Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013
|
|
|
- Loren McLaughlin
- 5 years ago
- Views:
Transcription

1 Revised Anti- Retroviral Treatment Guideline Update For Frontline Clinical Health Professionals 3/13/2013 The following document highlights the changes National department of Health ARV treatment guidelines that will take effect on 2 April 2013
2 Table of Contents Objectives... 3 Expected Results... 3 Training Agenda... 3 Rationale For The FDC Implementation... 4 Revised ARV Treatment Guideline... 7 PMTCT Guideline PMTCT Indicators PMTCT Data Elements Infants and Children Guidelines Adults and Adolescent Guidelines Key Updates in 2013 Guidelines Risks and Benefits of Earlier Initiation of ART Guidelines Moving Toward Early Treatment Adults and Adolescent Eligibility to Start ART Standardised national ART regimens for adults and adolescents Standardized National Monitoring for Adults and Adolescents with HIV Indications for urgent up- referral prior to initiation or when on therapy Case Studies Group Work Instructions PMTCT Cases Case Study 1: Unbooked Pregnant Women Case Study 3: Return Visit Case Study 4: 6 days Postnatal Visit Case Study 5: TB and HIV Case Study 6: Failure to Thrive Baby Infant and Children Cases Case Study 1: Eligibility For Art Case Study 2: Nancy: infant (<1yr) Case Study 3: Thabo: Child (1-5Yrs) Case Study 4: Sara (Adolescent): case targeted at Drs Case Study 5: Providing ART follow- up care Adult and Adolescent Cases Page
3 Case Case Case Case Case Overview on ART Treatment Regimen Changes Background: What are FDCs? What are the programmatic benefits of FDCs? What do the guideline changes mean for women and children? What are the changes in the new guidelines? PMTCT Regimen P age
4 Objectives 1. To update frontline clinical staff implementing PMTCT, paediatric and adult ARV treatment guidelines 2. Develop the capacity of frontline clinical staff to implement the revised ARV treatment guidelines 3. To update frontline clinical staff on the PMTCT national indicator data set (NIDS) 2013 Expected Results 1. Frontline clinical health professionals are fully informed about the revised PMTCT, pediatric and adult treatment guidelines and the use of fixed- dose combination (FDC) - what is different now. 2. Frontline clinical staff have the necessary knowledge and information to implement the revised treatment guidelines 3. Frontline clinical health professionals are fully briefed on the roll out of FDC and the eligibility criteria for each category of recipient 4. Frontline clinical staff are updated and informed on the workers the PMTCT national indicator data set (NIDS) 2013 Training Agenda Time Topic Resource Material Welcome and Introductions :00 Rationale for revised Treatment Guidelines Drug regimen FDC Laboratory M & E Integrated management (TB,FP, Cervical screening, Breast feeding) 10:00 10: 15 Refreshment break 10:15-13:00 Revised ARV Treatment Guidelines What are the changes? PMTCT (Including data collection, laboratory testing) Paediatrics Slides 1-8 PMTCT Guidelines 2013 Combined ARV Treatment Guidelines Adult Combined ARV Treatment Guidelines :45 1:30 Lunch 1:30 2:30 Group work and Case Studies Pages :30 3:30 Group Work Presentations & Discussion 3:30-3: 45 Summary and Key take home messages for Pages Frontline Health Workers on the revised Treatment Guidelines 3: 45-3:50 Closure 3 P age
5 Rationale For The FDC Implementation Current status in SA SA has highest HIV burden 2011 ANC Sero prevalence showing women still highly affected High mortality due to HIV and AIDS Largest HIV and AIDS program, but morbidity and mortality still high Strong political commitment to increase life expectancy of SA. Rationale for revised Treatment Guidelines South Africa is committed to improving the health status of the citizens- NSDA Responded to the Global call to eliminate HIV and AIDS- May 2011 SA to reduce morbidity & mortality due to HIV and AIDS Call to move to more efficacious regimens- IAS 2012 The Mandates NSP 2012/2016 NSDA the four outcomes Action Framework for elimination by 2015 o Scale up coverage and improve quality of PMTCT to reduce MTCT to less than 5% MDGs 4,5 and 6 o (4)Two thirds reduction in infant mortality o (5)Three quarters reduction in maternal deaths o (6)Combat HIV and AIDS Important Areas For The Change Drug regimens FDC Laboratory M & E Integrated management (TB, SRH- FP, Cervical screening, Breast ) Key Updates Timing of ART initiation in treatment- naive patients remains at cd4 <= 350 Guidance on introduction of the fixed dose combination Considerations for patients with co morbidity 4 P age
6 Considerations for HIV- infected women of childbearing age Timing of ART initiation in patients with TB Guidance on management of patients requiring salvage therapy Guidance on management of stable patients and on new guidelines to improve adherence to treatment Key Changes to 2013 ARV Treatment Guidelines Phasing out separate Pre ART literacy sessions for ART eligible patients and Introduction of concurrent adherence literacy to strengthen adherence support It is mandatory that patients are started on treatment within 14 days after being assessed as eligible for ART Introduced management of patients with co morbidity Early treatment offered to prevent transmission to uninfected patients Fixed Dose combination The Minister announced that fixed dose combination (FDC) therapy will be introduced on the 1 April 2013 (see Figure 1) FDCs will be available in facilities on 1 April 2013 The FDC will be introduce in phased manner over period of 1 year On the 1 April 2013 HIV positive pregnant women and those breast feeding and patients initiating ART for the first time will be prioritized Patients with co infections and co morbidities will be the next priority group Finally patients requiring switching and patients who are virally suppressed requiring switching from three drugs to FDC 5 P age
7 PRIORITY 7 PRIORITY 6 PRIORITY 5 PRIORITY 4 PRIORITY 3 PRIORITY 2 PRIORITY 1 New patients (adults, adolescents and pregnant women) eligible to start ART 1. All pregnant women needing triple therapy 2. Breast feeding mothers currently stable on a FDC compatible regimen. Virally suppressed patients currently on first line regimen, requiring a switch due to toxicity (e.g. stavudine) Patients currently stable on a FDC compatible regimen, with TB comorbidity Patients currently stable on a FDC compatible regimen with other comorbidities (e.g. hypertension, diabetes mellitus, etc.) Patients currently stable on TDF-based regimen and who request a switch to a FDC Patients currently stable on TDF-based regimen who, after counseling, agree to a switch to a FDC Figure 1 Roll Out Plan 6 P age
8 Revised ARV Treatment Guideline PMTCT Guideline (Refer to Attached PMTCT Guidelines) Encourage all women to book as early as possible in pregnancy, preferably before 14 weeks gestation Do not turn women away when trying to book All women coming to the clinic for first antenatal booking must be seen on the same day Baseline screening and ANC Group HIV pre- test counseling Opt- out approach Booking bloods should include RPR, Rh, Hb check and HIV For HIV: Individual testing with rapid test kit Individual post- test counseling Tetanus Iron, folic acid, vit C, Calcium HIV Negative Test If negative, repeat 12 weeks after first test or at 32 weeks gestation or later o Counsel about condom use and partner testing o Consider re- testing at delivery, at 6/52 post natal EPI visit, 3 monthly while breastfeeding and then at least annually HIV Positive Test If positive and confirmed positive with 2nd rapid test kit o Post- test counseling o Baseline bloods (CD4, Creatinine) o Initiate ART with the FDC on the same day regardless of CD4 cell count or gestational age. Do not wait for blood results to initiate! o Bring client back within 7 days for CD4 and Creatinine results Also Discuss: Partner testing/status/treatment Infant feeding Continue condom use and counsel about future contraception plan after delivery Cervical screening 6/52 postpartum On- going adherence 7 P age
9 Screen for TB Active TB disease is common in women living with HIV. All pregnant women should be actively screened for TB symptoms. If an HIV positive patient has symptoms suggestive of TB, a sputum specimen must be collected for GeneXpert testing, and the TB Xpert diagnostic algorithm followed. Although it is important to investigate patients for TB before starting ART, in most pregnant patients, initiation of ART prophylaxis or lifelong treatment should not be delayed for TB investigations. The healthcare provider should suspect TB in a woman living with HIV if any of the following 4 symptoms are present: o Current cough of any duration. o Fever o Night sweats o Weight loss or poor weight gain Any woman living with HIV who has none of these symptoms can be considered for eligibility for isoniazid preventive therapy by performing a tuberculin skin test. Screen For Neuropsychiatric Illness Use of efavirenz is contraindicated in individuals with active psychiatric illness. In practice, any woman with an active psychiatric illness should not receive an efavrienz- containing antiretroviral regimen without consultation. Mild depression is not a contraindication to efavirenz Screen For Renal Disease Use of tenofovir is contraindicated in individuals with renal disease. Renal disease is uncommon in HIV- infected pregnant women. At the first antenatal visit, women at increased risk of renal disease may be identified through a pre- pregnancy history of: o diabetes or hypertension, o a previous kidney condition requiring hospitalization, o 2+ proteinuria on urine dipstix. A serum creatinine of >85 µmol/l is considered abnormal in pregnancy (other methods of estimating renal function, including estimated glomelurlar filatration rate from the Cockroft- Gault equation, are inaccurate in pregnancy). How To Initiate ART All pregnant women, regardless of CD4 cell count, will be initiated on a fixed- dose- combination of FTC+TDF+EFV (one tablet) on the same day that they are diagnosed HIV positive Tablet to be taken once a day o In the evening o At the same time Routine antenatal booking bloods must be done (HB, RPR, Rh) at booking. 8 P age
10 Creatinine and CD4 are done on that same day and the patient must return for the results within 7 days. ART is initiated on ALL HIV positive pregnant women immediately. There is no need to wait for the CD4 and Creatinine results before initiation. Counsel Women On FDC Use Itself Screen for contra- indications to FDC o Known renal disease o Previous or current history of psychiatric illness (psychosis) o Symptomatic for TB Explain what monitoring bloods will be required (CD4, VL, Creatinine see later slide) and when they will be done Counsel that EFV is safe in pregnancy (many clients will read the package insert and panic) Common side effects: most self- limiting or develop tolerance o Somnolence/dizziness/strange dreams common, but usually improve o Shift workers need reassurance that symptoms of somnolence/dizziness usually improve o Client must be aware of potential renal toxicity but that this will be monitored o Explain that FDC unlikely to cause rash o Seek attention at clinic/hospital immediately if there is a problem, but emphasise importance to continue treatment regardless NB!!! DO NOT WAIT FOR CD4 AND CREATININE RESULTS BEFORE STARTING THE PATIENT ON TREATMENT If CD4 350 cells/mm³: lifelong ART If CD4>350 cells/mm³: continue ART for duration of pregnancy and FOR ONE WEEK AFTER cessation of breastfeeding Already On ART And Pregnant Check when CD4, VL and monitoring bloods last done Check if virally suppressed Continue regimen if suppressed Assess adherence if not suppressed o Consider second- line ART If on EFV- containing regimen, NO need to switch If on 3 individual drugs (3TC+TDF+EFV) prioritise to FDC Already on AZT Check CD4 cell count has been done. If no count in past 6 months re- do CD4 Take blood for Creatinine Change to FDC HIV Unknown Status In Labour Or Last Negative Test <32 Weeks Or >3 Months Ago 9 P age
11 Offer HIV counseling intrapartum for the benefit of mum and baby Diagnosed HIV Positive Intrapartum Stat NVP and Truvada and 3 hourly AZT Start FDC as soon as possible if mom plans to breast feed CD4 and Creatinine tests To return to clinic/health facility within 7 days for results Diagnosed HIV Positive Postpartum If breastfeeding, start FDC, take CD4 and Creatinine, come back for results within 7 days Counsel about EXCLUSIVE breastfeeding If seroconverts while breastfeeding o Start FDC immediately and do baseline bloods o Baby gets NVP for 6/52 o PCR test for baby in case high degree of suspicion of infection (LBW, Sick baby) o If not breastfeeding there is no need to start ART. Take CD4 and come back for results: if CD4<350 refer for lifelong ART: o If infant<6 weeks old start NVP Infant Feeding HIV infected mothers (and whose infants are HIV uninfected or of unknown HIV status) should exclusively breastfeed their infants for the first 6 months of life while introducing appropriate complementary foods thereafter, and continue breastfeeding for the first 12 months of life. Breastfeeding should then only stop if a nutritionally adequate and safe diet without breast milk is possible Mothers known to be HIV- infected should only give commercial infant formula milk as a replacement feed to their HIV uninfected infants or infants who are of unknown HIV status, when specific conditions are met: (referred to as AFASS - affordable, feasible, acceptable, sustainable and safe in the 2007 WHO recommendations on HIV and Infant Feeding) a) safe water and sanitation are assured at the household level and in the community, and, b) the mother, or other caregiver can reliably provide sufficient infant formula milk to support normal growth and development of the infant, and, c) the mother or caregiver can prepare it cleanly and frequently enough so that it is safe and carries a low risk of diarrhoea and malnutrition, and d) the mother or caregiver can, in the first six months, exclusively give infant formula milk, and, e) the family is supportive of this practice, and, f) the mother or caregiver can access health care that offers comprehensive child health services. 10 P age
12 Infant Nevirapine All HIV exposed infants would take Nevirapine syrup for only 6 weeks irrespective of feeding choice Birth weight >2500g: 1,5ml daily at the same time everyday Birth weight<2500g: 1ml daily at the same time everyday Infant Testing 6 week PCR teting for all HIV exposed infants If breastfed, repeat PCR 6 weeks after cessation of breastfeeding 18 month ELISA Test at any age if symptomatic Please note: A negative PCR test any time before 6 weeks of age needs to be repeated at 6 weeks Monitoring Bloods Creatinine o If on TDF o Baseline, 3 months, 6 months, 12 months then annually CD4 o Baseline and then annually VL o 6 months, 12 months and then annually Remind mom to take ART to the hospital / clinic when in labour Remind mom to take ART at usual time during labour and delivery or caesarean section Remind mom to have enough for the entire hospital stay Never to run out of medication Go to the clinic before the tablets run out, not after Have enough until the follow up visit post delivery Know where to follow up before discharge from hospital Key Messages for PMTCT Key Message 1 All ANC clients (newly diagnosed as HIV positive and those pregnant but not yet on HAART) to start FDC (single pill)/art on the same day as 1st visit CD4 and creatinine test to be done and client asked to return within 7 days Further management based on CD4 counts, creatinine levels see algorithms in the PMTCT guidelines Key message - 2 All ANC clients that test HIV negative during pregnancy to repeat test every 12 weeks/3 months after 1 test, and/or at 32 weeks of gestation or later, at labour, during the postnatal period throughout period of breastfeeding Infant testing algorithm in the revised guidelines to be followed. 11 P age

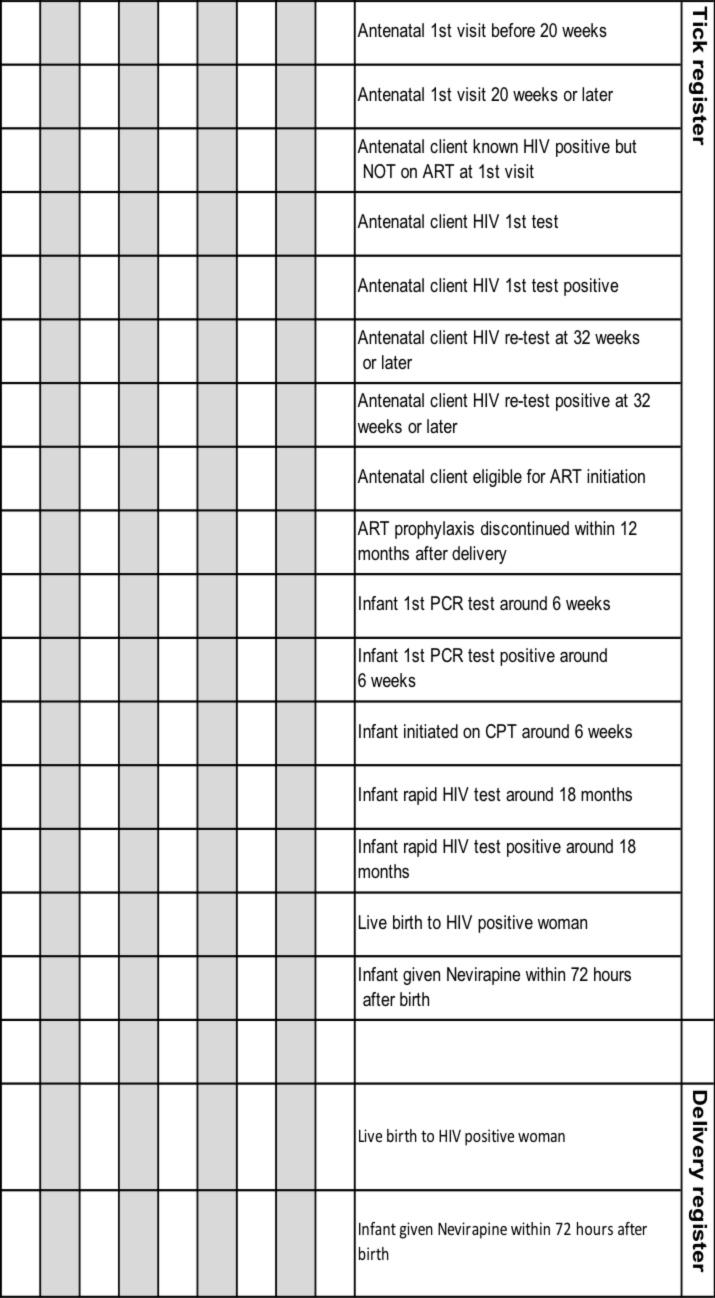
13 2013 PMTCT Indicators 12 P age
14 2013 PMTCT Data Elements 13 P age
15 14 P age
16 Infants and Children Guidelines Criteria to Start ART Eligible to Start ART o All children less than 5 years of age o Children 5 years to 15 years with WHO clinical stage 3 or 4 or CD4 < 350 cells/µl Criteria for Fast Tracking for ART Require Fast- Track (i.e. start ART within 7 days of being eligible) o Children less than 1 year of age o WHO clinical Stage 4 o MDR or XDR- TB o CD4 Count < 200 cells/ul or < 15% What ART To Start Children On First Line Regimen All infants and children under 3 years (and < 10kg) Children 3 years (and 10kg) Currently on d4tbased regimen ABC + 3TC + LPV/r ABC + 3TC + EFV Change d4t to ABC if Viral Load is undetectable If Viral load >1000 copies/ml manage as treatment failure If Viral load between copies/ml consult with expert for advise Note: Children 3 years and exposed to NVP for 6 weeks or longer (PMTCT) should be initiated on ABC + 3TC + LPV/r 15 P age
17 Second Line Regimen Failed First line Protease Inhibitor (PI) based regimen Failed First line PI Based regimen ABC + 3TC + LPV/r D4T + 3TC + LPV/r Recommended Second line regimen Consult with expert for advice* Unboosted PI based regimen Failed First line NNRTI based regimen (discuss with expert before changing) Failed First line NNRTI Based regimen ABC + 3TC + EFV (or NVP) d4t + 3TC + EFV (or NVP) Recommended Second line regimen AZT + 3TC + LPV/r AZT + ABC + LPV/r Advice For The Expert *Recommended Second Line regimen under expert advice ABC + 3TC + LPV/r No previous daily NVP for PMTCT AZT + 3TC + EFV* + LPV/r * Use NVP if < 3 years or <10kg Previous Daily NVP for PMTCT Treat with Third line regimen D4T + 3TC + LPV/r No previous daily NVP for PMTCT AZT + ABC + EFV* + LPV/r * Use NVP if < 3 years or <10kg Previous Daily NVP for PMTCT Treat with Third line regimen Previously on a regimen with unboosted PI (e.g. ritonavir alone), or with rifampicin while on LPV/r Must be managed by an expert on basis of genotype resistance testing to confirm PI susceptibility. 16 P age
18 Third line regimens Failing any 2 nd line regimen Refer for specialist opinion Regimen based on genotype resistance testing, expert opinion and supervised care. Access to third line ART will be managed centrally by the National Dept of Health. Investigations At Diagnosis At initial Diagnosis of HIV Verify HIV status Document weight, height, head circumference (<2yrs) and development Screen for TB symptoms WHO Clinical Staging Do the CD4 count Purpose Ensure that national testing algorithm has been followed To monitor growth and development + identify eligibility for ART To identify TB/HIV co-infected To determine if patient is eligible for ART Children < 5 years Baseline, DO NOT wait for CD4 count to start ART Children 5 years - To determine eligibility for ART and start cotrimoxazole prophylaxis as per national guideline Hb or FBC if available To detect anaemia or neutropenia Investigations Baseline At Initiation of ART (Baseline) Hb or FBC CD4 count (if not performed in last 6 months) HIV Viral Load (VL) Cholesterol + Triglyceride if on PI based regimen Purpose If less than 8 g/dl start ART and refer for specialist opinion Baseline assessment Baseline assessment Baseline assessment 17 P age
19 Creatinine + urine dipstix if on TDF regimen ALT (if Jaundice or on TB treatment) If abnormal refer for specialist opinion To assess for liver dysfunction Monitoring Treatment Response On ART Height, weight, head circumference (<2yrs) and development Clinical assessment CD4 at 1 year into ART, and then every 12 months VL at month 6, 1 year into ART, then every 6 monthly in children < 5 years / 12 monthly in children 5 years to 15 years Purpose To monitor growth and development stages To monitor response to ART and exclude adverse effects To monitor response to ART, stop cotrimoxazole prophylaxis as per national guideline To monitor viral suppression response to ART To identify treatment failure and to identify problems with adherence Monitoring Adverse Events On ART Hb or FBC at month 1, 2, 3 and then annually if on AZT Cholesterol + Triglyceride at 1 year and then every 12 months if on PI based regimen Clinical drug-related adverse events Purpose To identify AZT-related anaemia To monitor for PI-related metabolic side-effects To identify drug-related adverse events If develops jaundice or rash on EFV or NVP do Liver function test and refer to specialist 18 P age
20 Adults and Adolescent Guidelines Key Updates in 2013 Guidelines Timing of ART initiation in treatment- naive patients remains at cd4 count at 350 Treatment as prevention based on early initiation and adherence support Guidance on introduction of the fixed dosed combination Considerations for patients with co morbidity Considerations for HIV- infected women of childbearing age Timing of ART initiation in patients with TB Guidance on management of patients requiring salvage therapy Guidance on management of stable patients and on new guidelines to improve adherence to treatment Risks and Benefits of Earlier Initiation of ART Delayed ART Drug toxicity Preservation of limited Rx options Risk of resistance (and transmission of resistant virus) Early ART potency, durability, simplicity, safety of current regimens emergence of resistance toxicity with earlier therapy Risk of uncontrolled viremia Near normal survival if CD4+ count > 500 transmission Guidelines Moving Toward Early Treatment Early diagnosis, timely treatment can change the course of the epidemic 19 P age
21 Changes to guidelines reflect these goals Evolution toward treatment of essentially all patients Inclusion of treatment as prevention Adults and Adolescent Eligibility to Start ART Eligible to start ART CD4 count <350 cells/mm3 irrespective of WHO clinical stage Irrespective of CD4 count o o OR All types of TB (In patients with TB/HIV drug resistant or sensitive TB, including extra pulmonary TB) HIV positive women who are pregnant or breast feeding Patients with Cryptococcus meningitis or TB meningitis (defer ART for 4-6 weeks) OR WHO stage 3 or 4 irrespective of CD4 count Require fast track (i.e. ART initiation within 7 days of being eligible) HIV positive women who are pregnant or breast feeding OR Patients with low CD4 <200 OR Patients with Stage 4, irrespective of CD4 count OR Patients with TB/HIV co morbidity with CD4 count < 50 Patients with CD4 above 350, Not yet eligible for ART Transfer to a wellness programme for regular follow-up and repeat CD4 testing 6-monthly. Advise on how to avoid HIV transmission to sexual partners and children Initiate INH prophylaxis if asymptomatic for TB Provide counselling on nutrition and contraceptive and do annual pap smear Standardised national ART regimens for adults and adolescents All new patients needing treatment, including pregnant women 1 st Line TDF + FTC (or 3TC) +EFV FDC preferred Replace EFV with NVP in patients with significant psychiatric co-morbidity or intolerance to EFV and where the neuropsychiatric toxicity of EFV may impair daily functioning, e.g. shift workers. Contraindications to EFV TDF + (FTC or 3TC) + NVP Use NVP based regimen: In patients with significant psychiatric co morbidity or intolerance to EFV and where the neuropsychiatric toxicity of EFV may impair daily functioning, e.g. shift workers. 20 P age
22 1 st Line Contraindication to TDF AZT+ 3TC +EFV or (NVP) Renal disease or the use of other nephrotoxic drugs e.g. aminoglycosides Contraindication to TDF and AZT Contraindication to TDF, AZT and d4t Currently on d4t-based regimen Management of virological failure Failing on a TDF-based 1 st line regimen Failing on a d4t-based 1 st line regimen Dyslipidaemia or diarrhoea associated with LPV/r Failing any 2 nd line regimen Should be expert and genotype resistance testing based decision and supervised care Patients failing on second line therapy will be managed by an expert panel. The drugs for third line will be managed centrally. More discussion is required to deal with the modalities d4t + 3TC+ EFV (or NVP) ABC + 3TC + EFV (or NVP) TDF + FTC(or 3TC) + EFV FDC preferred AZT+3TC+ LPV/r 2 nd Line TDF+3TC (or FTC) and LPV/r Switch LPV/r to ATV/r Third line Specialist referral Most likely regimen would be Raltegravir/Darunavir/ /Etravirine adjusted according to genotype Interpretation. Should be by expert and take into account prior exposure and predictable mutations Renal disease and anaemia or the use of other nephrotoxic drugs, aminoglycosides Renal disease, anaemia, peripheral neuropathy, the use of other nephrotoxic drugs Mandatory if patients experience toxicity and patients who are at high risk of toxicity (high BMI or pregnant). Switch to TDF if virally suppressed and the patient has normal creatinine clearance, even if well tolerated. If plasma HIV RNA >1000 copies, Check for adherence, compliance, tolerability and drug- drug interaction and assess psychological issues. Repeat VL test 2 months later. If plasma VL confirmed >1000copies change regime to second line therapy Patients with anaemia and renal failure switch to ABC 21 P age
23 Standardized National Monitoring for Adults and Adolescents with HIV At initial Diagnosis of HIV Confirm HIV result with rapid antibody test Do CD4 count if HIV positive and WHO clinical staging Screen for pregnancy or ask if planning to conceive Screen for TB symptoms using the WHO questionnaire Do the CD4 count on the same day Do HB or FBC if requires AZT Purpose Ensure that national testing algorithm has been followed To assess eligibility for ART To assess eligibility for fast-tracking To identify women who need ART for life or ARV prophylaxis for PMTCT (see section 6) To identify TB/HIV co-infected To identify eligibility for ART or ARVs for prophylaxis if pregnant To detect anaemia or neutropenia, Creatinine if requires TDF To detect renal insufficiency For patients initiated on Nevirapine based regime do ALT To exclude liver disease On ART CD4 at 1 year on ART VL at month 6, 1 year on ART and then every 12 months ALT only if on NVP and develops rash or symptoms of hepatitis FBC at month 3 and 6 if on AZT Creatinine at month 3 and 6, 1 year then every 12 months if on TDF Fasting cholesterol and triglycerides at month 3 if on LPV/r Purpose To monitor immune response to ART To identify treatment failures and problems with adherence To identify NVP toxicity To identify AZT toxicity To identify TDF toxicity To identify LPV/r toxicity At Routine Follow-Up Visits for those not yet eligible for ART Purpose Repeat CD4 count at 6 months WHO clinical staging at every visit Screen for TB symptoms to identify TB suspects Offer IPT if no TB symptoms Offer prevention for HIV positives To see if they have become eligible for ART To see if they have become eligible for ART To identify TB/HIV co-infection To prevent TB activation To prevent HIV transmission and re-infection To prevent STIs 22 P age
24 Indications for urgent up- referral prior to initiation or when on therapy egfr less than 60 ml/min Hb less than 8 g/dl BMI less than 18.5 kg/m2 In a patient with TB, poor response to TB treatment 23 P age
25 24 P age
26 Case Studies Group Work Instructions 1. Participants to form a team of 4-5 persons 2. Each team will receive a different case study to work on 3. The purpose of the case studies is to apply the technical information to real life settings 4. Each team will have 30 minutes to discuss the case study and answer the key questions. i. One group member should be selected to facilitate the group discussion; ii. one to take notes on a flip chart (if available) and iii. one to present to the plenary. 5. Each team will prepare a 10 minute presentation of their findings For each case the team members must answer 4 questions : 1. How would you treat the patient today? (give a detailed account of clinical practice) 2. What follow- up treatment is required? 3. What referrals would you make for the patient? 4. What is the data element you would need to capture/ note in each case? These questions must be applied to the woman and if she has a new born baby the questions will also apply to the baby Present Back to Plenary: Each group will have 10 minutes to present back to the plenary Discussion: the presentation will be followed by 5 minutes of discussion per case study including questions of clarification 25 P age
27 PMTCT Cases Case Study 1: Unbooked Pregnant Women Lebo has not had any antenatal care. She is 38 weeks pregnant and is starting to have contractions. She asks her mother to take her to the nearest health facility. 1. How would you treat the patient today? (give a detailed account of clinical practice) 2. What follow- up treatment is required? 3. What referrals would you make for the patient 4. What is the data element you would need to capture/ note in each case? 26 P age
28 Case Study 2: First ANC Visit Thandi is 18 weeks pregnant. She goes to her clinic for her first antenatal care visit. At this visit she is offered an HIV test and the result is positive. 1. How would you treat the patient today? (give a detailed account of clinical practice) 2. What follow- up treatment is required? 3. What referrals would you make for the patient? 4. What is the data element you would need to capture/ note in each case? 27 P age
29 Case Study 3: Return Visit Thandi has had two previous antenatal care visits. The first visit was at approximately 20 weeks and another visit at 28 weeks. At her first ANC visit she had an HIV test. At that time, she tested negative. She is now 34 weeks pregnant. Her partner has been very sick for the past 4 weeks but refuses to go to the doctor. 1. How would you treat the patient today? (give a detailed account of clinical practice) 2. What follow- up treatment is required? 3. What referrals would you make for the patient 4. What is the data element you would need to capture/ note in each case? 28 P age
30 Case Study 4: 6 days Postnatal Visit Tsipwe s has been breastfeeding her baby since birth. She has brought her baby to the clinic for a checkup at 6 days. During pregnancy, Tsipwe was enrolled in the PMTCT programme 1. How would you treat the patient today? (give a detailed account of clinical practice) 2. What follow- up treatment is required? 3. What referrals would you make for the patient 4. What is the data element you would need to capture/ note in each case? 29 P age
31 Case Study 5: TB and HIV Lerato is pregnant with her first baby. She is approximately 16 weeks pregnant, but has not had any antenatal care yet. She has not been feeling very well, she thinks it may be because she is pregnant. Her symptoms include a cough, fever, night sweats and weight loss despite being pregnant. She comes to the health facility for antenatal care. 1. How would you treat the patient today? (give a detailed account of clinical practice) 2. What follow- up treatment is required? 3. What referrals would you make for the patient 4. What is the data element you would need to capture/ note in each case? 30 P age
32 Case Study 6: Failure to Thrive Baby Sesupo s baby is 8 weeks old. She has noticed that the baby is not gaining weight and appears to be sick. Sesupo was in the PMTCT programme during pregnancy, but because she has no help with the baby she has not taken the baby back to the facility for check- ups since birth. She takes her baby to the clinic. 1. How would you treat the patient today? (give a detailed account of clinical practice) 2. What follow- up treatment is required? 3. What referrals would you make for the patient 4. What is the data element you would need to capture/ note in each case? 31 P age
33 Infant and Children Cases Case Study 1: Eligibility For Art Decide whether or not the following children are eligible to receive ART. Assume that age- appropriate HIV test has been done and HIV infection has been confirmed. AGE STAGE CD4 COUNT/PERCENTAGE ANSWER 1. 4 years cells/mm 3 or 40% 2. 6 months cells/mm 3 or 15% 3. 9 months cells/mm 3 or 45% 4. 3 years 3 Not known 5. 9 years cells/mm years cells/mm month 1 Not known years cells/mm months cells/mm 3 or 20% month old cells/mm 3 32 P age
34 Case Study 2: Nancy: infant (<1yr) Nancy is three months old and weighs 6 kg. Her mother was found to be HIV- infected during pregnancy. Nancy was tested for HIV at six weeks and PCR results are positive. A full blood count done at the same time, showed that her Hb is 11g/dL. She is breastfeeding and is generally well. Her length is 60 cm and her head circumference is 41 cm. Her temperature was recorded as C. She lifts her head when her mother carries her with support, responds to sounds and follows close objects with both eyes. Her mother has not disclosed her own or Nancy s HIV status to anyone at home, but is a regular member of the clinic support group. She has been counselled regarding adherence, and is available and committed in ensuring that Nancy receives HIV care and Support. a) Is Nancy eligible for ART? List the eligibility criteria that you have considered. b) If you decide that she is eligible for ART, provide clinical management. 33 P age
35 Case Study 3: Thabo: Child (1-5Yrs) Thabo is a 4 year old boy. He has severe oral thrush. His temperature is C and his weight now is 12.3 kg. For the past 3 months his weight was 9.8 kg he has not received any treatment for poor weight gain. A rapid test was done which shows that he is HIV positive. The diagnosis is confirmed with a second rapid test which is also positive and his blood was sent to the laboratory for a CD4 count and Viral Load today. Thabo s mother has been on ART for the past 4 years. She has been taking her medication every day and is very motivated to take care of herself and of Thabo. She is supported by her mother who know that she is HIV- infected and on treatment. She now asks that Thabo should also receive ART. Thabo lives with his mother. She runs a spaza shop from home and looks after Thabo as well. a) Is Thabo eligible for ART? List the eligibility criteria that you have considered.. b) If you decide that he is eligible for ART, how are going to manage Thabo 34 P age
36 Case Study 4: Sara (Adolescent): case targeted at Drs Sara is a 14 years old girl in high school. She was born with HIV and has been on ARVs (ABC + 3TC+ EFV) for 7 years. Her mom who is also on ARVs reports that she (Sara) comes back home late this days- probably because she is at adolescent stage, she was no longer adhering to her treatment, and at times she missed clinic visits. Three months ago her, VL was 1100 and today is 1 200, she looks sick and her mom is worried. Last month she has joined her mom in a support group and improvement on adherence has been noted. 35 P age
37 Case Study 5: Providing ART follow- up care Sipho is 23 months old boy, currently 18 months on ARVs (1 st regimen), CD4 count, VL, Cholesterol + Triglycerides was done 12 months ago. He is responding well to treatment. No side effects ever reported by his mom. Today he came for his routine follow- up visit. a) Provide routine follow- up care to him 36 P age
38 Adult and Adolescent Cases Case 1 A 47 year- old male presents at your clinic. He is HIV- infected. He weighs 62 kg, has CD4 count 170 cells/mm 3. He does not have active TB or any other opportunistic infections at present. He is taking cotrimoxazole prophylaxis without any notable side effects. Is this patient eligible for ART? Why or why not? If the patient is eligible for ART, what regimen should he start? What is the appropriate dose of each medication? What lab tests should be obtained at baseline and when should they be repeated? Case 2 A 26 year- old female presents at your clinic. She is HIV- infected. Her weight is 65 kg, who was treated for PCP 6 weeks ago. She is not currently pregnant and declines contraceptives. No active TB and no other opportunistic infections at present. She is taking cotrimoxazole prophylaxis without any apparent side effects. Is this patient eligible for ART? Why or why not? If the patient is eligible for ART, what regimen should they start? What is the appropriate dose of each medication? What labs should be obtained at baseline and when should they be repeated? 37 P age
39 Case 3 A 35 year- old male presents at your clinic. He is HIV- infected. He weighs 70 kg and has no history of recent weight loss. He has a current CD4 count of 400 cells/mm 3. He has a history of herpes zoster 2 years ago. No active TB at present or other opportunistic infections. He is taking cotrimoxazole with no apparent side effects. Is this patient eligible for ART? Why or why not? If the patient is eligible for ART, what regimen should they start? What is the appropriate dose of each medication? What follow- up labs should be obtained? Case 4 A 30 year- old female presents at your clinic. She is HIV- infected. She weighs 55kg, with a CD4 of 156 cells/ mm 3. She is on an injectable contraceptive. She was diagnosed with pulmonary TB and started on TB therapy a week ago. She does not appear to have any significant adverse events related to the medications. 1. Is this patient eligible for ART? Why or why not? If the patient is eligible for ART, what regimen should they start? What is the appropriate dose of each medication? What labs should be obtained at baseline and when should they be repeated? 38 P age
40 Case 5 A 26 year- old male presents with a history of ART for one year and one month. Current regimen: stavudine, lamivudine and efavirenz. He has no symptoms today and reluctantly reports missing several doses over the past several months. Vitals: Temp: 37C, Respiratory Rate: 16, Pulse: 67, Blood Pressure: 110/75 Exam: Within Normal Limits Baseline CD4/VL: 130 cells/mm 3, 100,580 copies/ml 6 month CD4/VL: 250 cells/mm 3, < 400 copies/ml 1 year CD4/VL: 175 cells/mm 3, 10,890 copies /Ml What do you suspect is occurring? Is there an indication for switching or stopping a regimen? Why or why not? If so, what should take place next and if the regimen needs to be changed, what part of the regimen should be switched/ stopped? 39 P age
41 Overview on ART Treatment Regimen Changes As of April 1 st, 2013, changes to the ART treatment regimens will be implemented across the country. The target audience for this communication brief are all cadres of health care workers who interact with pregnant women, mothers and infants, and children. Background: On December 1, 2012, the Minister of Health announced the inclusion of fixed drug combinations (FDCs) for the national ART programme. This is a positive change for the programme and will benefit the patient and the health system, resulting in a more effective programme. What are FDCs? FDC are combinations of two or more active drugs in a single dosage form What are the programmatic benefits of FDCs? For the patient: One Pill convenient dosage regimen Easier to take Compliance Fewer side effects For the health service: Easier storage Easier logistics What do the guideline changes mean for women and children? All HIV positive pregnant women will start the triple drug prophylaxis from 14 weeks of pregnancy and continue throughout the breastfeeding period. Following the breast feeding period, women with CD4 counts less than 350 will continue on the triple drug prophylaxis. The fixed dose combination is more effective than dual therapy and has fewer side effects for the pregnant mother, in addition to its convenient dosage regimen. 40 P age
42 What are the changes in the new guidelines? PMTCT Regimen All pregnant women: Encourage all women to book early in pregnancy, preferably before 14 weeks gestation. All women coming to the clinic for first antenatal booking must be seen on the same day Booking bloods should include RPR, Rh, Hb check and HIV testing Tetanus; Iron, folic acid, vitamin C, Calcium should also be given at the first visit For women who test negative at first ANC visit: Retest (12 weeks after the first HIV test) and/or at 32 weeks of gestation, in labour; 6 weeks postpartum; every 3 months while breastfeeding; and thereafter annually. For women who test positive at first ANC visit: All pregnant women, regardless of CD4 cell count, will be initiated on a fixed-dosecombination of FTC+TDF+EFV (one tablet) on the same day that they are diagnosed HIV positive This tablet to be taken once a day, in the evening at the same time Creatinine and CD4 are done on that same day and the patient must return for the results within 7 days. ART is initiated on ALL HIV positive pregnant women immediately. There is no need to wait for the CD4 and Creatinine results before giving the FDC. This must take place on the same day. Depending on CD4 test results, treatment options are: If CD4 350 cells/mm³: lifelong ART If CD4>350 cells/mm³: continue ART for duration of pregnancy and FOR ONE WEEK AFTER cessation of breastfeeding THEN STOP ART For women who are on AZT at first ANC visit: Check CD4 cell count has been done. If not done in the past 6 months, repeat CD4 cell counts Take blood for Creatinine levels Change to FDC regimen on the same day as the ANC visit and ask women to return within 7 days for the blood results. For women who are already on ART and pregnant Check when CD4, VL and monitoring bloods were last done Check if virally suppressed o Continue regimen if suppressed o Assess adherence if not suppressed If on 3 individual drugs (3TC+TDF+EFV) prioritise to FDC 41 P age
43 For women who are diagnosed HIV positive during the intrapartum period Stat NVP and Truvada and 3 hourly AZT Start FDC as soon as possible if mom plans to breast feed CD4 and Creatinine tests To return to clinic within 7 days for results All HIV Exposed Infants Nevirapine syrup for 6 weeks irrespective of feeding choice Birth weight >2500g: 1,5ml daily at the same time everyday Birth weight<2500g: 1ml daily at the same time everyday 6 week PCR tests for all HIV exposed infants In case a PCR test was done before 6 weeks due to any reason and was negative, repeat PCR test at 6 weeks for the infant If breastfed, repeat PCR tests 6 weeks after cessation of breastfeeding Exclusive breast feeding is the recommended feeding choice. 18 month rapid HIV tests done for all HIV exposed infants Test at any age if symptomatic (if < 18 months do a PCR test, and if >18 months do a HIV rapid test for diagnosis) 42 P age
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE
 UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
Updates on Revised Antiretroviral Treatment Guidelines Overview 27 March 2013
 Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
WESTERN CAPE ART GUIDELINES PRESENTATION 2013
 WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
The NEW ARV Guidelines FAQs
 The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
The NEW ARV Guidelines FAQs Dr Madeleine Muller MBChB (Pret).MRCGP(Lon).Dip Hiv Man IYDSA Clinical Advisor Acknowledgments IYDSA for materials and support NDOH for slides CDC our funder HIV Clinician Society
Figure S1: Overview of PMTCT Options A and B. Prevention of Mother to Child HIV Transmission (PMTCT)
") Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
Paediatric ART: eligibility criteria and first line regimens. (revised) Dave le Roux 13 August 2016
 Dave le Roux 13 August 2016") Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
Update on global guidelines. and emerging issues on perinatal HIV prevention. WHO 2013 Consolidated ARV Guidelines
 WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
The New National Guidelines. Feeding in the Context of HIV. Dr. Godfrey Esiru; National PMTCT Coordinator
 The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and
, Children, Adolescents and") The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2018 (Amended Version) The Western Cape Consolidated
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2018 (Amended Version) The Western Cape Consolidated
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and
, Children, Adolescents and") The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2015 (Amended Version) The Western Cape Consolidated
The Western Cape Consolidated Guidelines for HIV Treatment: Prevention of Mother- to- Child Transmission of HIV (PMTCT), Children, Adolescents and Adults. 2015 (Amended Version) The Western Cape Consolidated
hiv/aids Programme Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants
 hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
hiv/aids Programme Programmatic update Use of Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants EXECUTIVE SUMMARY April 2012 EXECUTIVE SUMMARY Recent developments
INITIATING ART IN CHILDREN: Follow the six steps
 INITIATING ART IN CHILDREN: Follow the six steps STEP 1: DECIDE IF THE CHILD HAS CONFIRMED HIV INFECTION Child < 18 months: HIV infection is confirmed if the PCR is positive and the VL is more than 10,000
INITIATING ART IN CHILDREN: Follow the six steps STEP 1: DECIDE IF THE CHILD HAS CONFIRMED HIV INFECTION Child < 18 months: HIV infection is confirmed if the PCR is positive and the VL is more than 10,000
Outline. Aim with PMTCT. How are children transmitted. Prevention of mother-to-child transmission of HIV. How does HIV transmit to children?
 Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV
 TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
DEPARTMENT. Treatment Recommendations for. Pregnant and Breastfeeding Women: Critical Issues Consolidated ARV Guidelines. Dr.
 2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
2013 Consolidated ARV Guidelines H I V / A I D S Treatment Recommendations for DEPARTMENT Pregnant and Breastfeeding Women: Critical Issues Dr. Nathan Shaffer Objectives of Presentation obackground ooverview
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015
 MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015 HIV & MDR :Impact of early ART initiation Adjusted HR: 0.14; p = 0.042 86% reduction in mortality with ART Initiation during MDR-TB treatment 2015
MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015 HIV & MDR :Impact of early ART initiation Adjusted HR: 0.14; p = 0.042 86% reduction in mortality with ART Initiation during MDR-TB treatment 2015
Tunisian recommendations on ART : process and results
 Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
James Nuttall Paediatric Infectious Diseases Unit Red Cross Children s Hospital
 James Nuttall Paediatric Infectious Diseases Unit Red Cross Children s Hospital Paediatric HIV Infection Symposium, August 21, 2010, Red Cross Children s Hospital Overview of talk The 2010 paediatric guidelines
James Nuttall Paediatric Infectious Diseases Unit Red Cross Children s Hospital Paediatric HIV Infection Symposium, August 21, 2010, Red Cross Children s Hospital Overview of talk The 2010 paediatric guidelines
ARV Consolidated Guidelines 2015
 ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
2009 Revisions of WHO ART Guidelines. November 2009
 2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
Management of HIV Infected Children and Adolescents: Public Sector Approach in Kenya
 Management of HIV Infected Children and Adolescents: Public Sector Approach in Kenya KPA 2018 24-04-2018 Dr. Margaret Wainaina- Wafula Outline Introduction Evaluation of a child living with HIV. Standard
Management of HIV Infected Children and Adolescents: Public Sector Approach in Kenya KPA 2018 24-04-2018 Dr. Margaret Wainaina- Wafula Outline Introduction Evaluation of a child living with HIV. Standard
The 2017 Namibia ART Guidelines. Tadesse T. Mekonen, MD, MPH, AAF-HIV
 The 2017 Namibia ART Guidelines Tadesse T. Mekonen, MD, MPH, AAF-HIV Q1-Table 1 List at least four key new recommendations in the 2017 Namibian ART Guidelines Q2-Table-2 46yo, Male, on AZT/TDF/FTC/ATVr
The 2017 Namibia ART Guidelines Tadesse T. Mekonen, MD, MPH, AAF-HIV Q1-Table 1 List at least four key new recommendations in the 2017 Namibian ART Guidelines Q2-Table-2 46yo, Male, on AZT/TDF/FTC/ATVr
PMTCT UPDATE. AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM
 PMTCT UPDATE AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM Outline Background Risk of MTCT Historical ARV interventions SA PMTCT program Rationale for changes
PMTCT UPDATE AWACC CONFERENCE DURBAN SEPT 2013 Dr HM Sebitloane Chief Specialist, Dept of O+G, NRMSM Outline Background Risk of MTCT Historical ARV interventions SA PMTCT program Rationale for changes
Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20
 Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
Introduction Pregnancies amongst adolescents and young women 16% of all births - 19% will have repeat pregnancies before age 20 Proportions HIV infections 19% amongst adolescents (- 29.5% nationally 15
ESSENTIAL PACKAGE FOR HIV CARE AND TREATMENT. Essential Package for HIV Care and Treatment
 ESSENTIAL PACKAGE FOR HIV CARE AND TREATMENT Essential Care & Treatment Package for Adult PLHIV 1. All patients should have a confirmed and documented HIV diagnosis in their file 2. All HIV infected adults
ESSENTIAL PACKAGE FOR HIV CARE AND TREATMENT Essential Care & Treatment Package for Adult PLHIV 1. All patients should have a confirmed and documented HIV diagnosis in their file 2. All HIV infected adults
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM
 Dept of O+G NRMSM") Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
Dr HM Sebitloane Chief Specialist (Outreach) Dept of O+G NRMSM SA Background Population: 48m Annual number of deliveries:1,2m 97% of women attend the first ANC 71% of women attend 5 th ANC visit 97% of
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES?
 WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
WHAT S NEW IN THE 2015 PERINATAL HIV GUIDELINES? Today s Webinar will be starting soon For the audio portion of this meeting: Dial 1-855-702-5382 Enter participant code 596-825-4701# Guidelines for online
Adolescents Living with HIV
 Adolescents Living with HIV Gary Reubenson Polokwane 22 August 2015 Conflicts of Interest No relevant conflicts of interest to declare Acknowledgements Karl Technau Lee Fairlie Gill Sorour HIV Clinicians
Adolescents Living with HIV Gary Reubenson Polokwane 22 August 2015 Conflicts of Interest No relevant conflicts of interest to declare Acknowledgements Karl Technau Lee Fairlie Gill Sorour HIV Clinicians
Clinical guidelines for antiretroviral management of HIV disease. Origins and history of the HIV epidemic
 Clinical guidelines for antiretroviral management of HIV disease Origins and history of the HIV epidemic Both known species of HIV, viz. HIV-1 and HIV-2 originated in Africa (HIV-1 from Central Africa
Clinical guidelines for antiretroviral management of HIV disease Origins and history of the HIV epidemic Both known species of HIV, viz. HIV-1 and HIV-2 originated in Africa (HIV-1 from Central Africa
ANTIRETROVIRAL THERAPY IN NAMIBIA
 ANTIRETROVIRAL THERAPY IN NAMIBIA SAHIVCS CONFERENCE CAPETOWN 25-28- NOVEMBER 2012 DR. F. MUGALA MUKUNGU M.MED (INT.MED) SPECIALIST PHYSICIAN KATUTURA STATE HOSPITAL WINDHOEK NAMIBIA Current status in
ANTIRETROVIRAL THERAPY IN NAMIBIA SAHIVCS CONFERENCE CAPETOWN 25-28- NOVEMBER 2012 DR. F. MUGALA MUKUNGU M.MED (INT.MED) SPECIALIST PHYSICIAN KATUTURA STATE HOSPITAL WINDHOEK NAMIBIA Current status in
PMTCT Counseling Support Flipchart
 PMTCT Counseling Support Flipchart HOW TO USE THE COUNSELING CUE CARDS FLIPCHART The counseling cue cards flipchart was developed to support a range of providers (trained counselors, lay counselors, peer
PMTCT Counseling Support Flipchart HOW TO USE THE COUNSELING CUE CARDS FLIPCHART The counseling cue cards flipchart was developed to support a range of providers (trained counselors, lay counselors, peer
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Dr Wendy Mphatswe SA HIV Clinician s Society Meeting 15 July 2017 Overview 1. HIV epidemic 2. HIV response (Fast Track) 3. Goal of therapy in pregnant and breastfeeding women
Using new ARVs in pregnancy Dr Wendy Mphatswe SA HIV Clinician s Society Meeting 15 July 2017 Overview 1. HIV epidemic 2. HIV response (Fast Track) 3. Goal of therapy in pregnant and breastfeeding women
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Positive health, dignity and prevention for women and their babies
 FLIPCHART Positive health, dignity and prevention for women and their babies A treatment literacy guide for pregnant women and mothers living with HIV Module 1: Human rights in healthcare settings 1 Knowing
FLIPCHART Positive health, dignity and prevention for women and their babies A treatment literacy guide for pregnant women and mothers living with HIV Module 1: Human rights in healthcare settings 1 Knowing
Goal of this chapter. 6.1 Introduction Good practices for linkage to care General care for people living with HIV 84
 Clinical guidelines across THE CONTINuUM OF CARE: LINKING PEOPLE DIAGNOSEd WiTH hiv infection to hiv care and treatment 06 6.1 Introduction 84 6.2 Good practices for linkage to care 84 6.3 General care
Clinical guidelines across THE CONTINuUM OF CARE: LINKING PEOPLE DIAGNOSEd WiTH hiv infection to hiv care and treatment 06 6.1 Introduction 84 6.2 Good practices for linkage to care 84 6.3 General care
Clinical Management Guidelines 2012
 Central American Course Monitoring and Evaluation for HIV/AIDS Policy and Program Management 1 2 3 4 Module 1 Unit 1 Clinical Management Guidelines 2012 National TB, HIV/AIDS & other STIs Programme Ministry
Central American Course Monitoring and Evaluation for HIV/AIDS Policy and Program Management 1 2 3 4 Module 1 Unit 1 Clinical Management Guidelines 2012 National TB, HIV/AIDS & other STIs Programme Ministry
SA HIV Clinicians Society Adult ART guidelines
 SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
Rajesh T. Gandhi, M.D.
 HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
PLANNING INTEGRATED HIV SERVICES AT THE HEALTH CENTRE
 CHAPTER 2 PLANNING INTEGRATED HIV SERVICES AT THE HEALTH CENTRE 2.1 INTRODUCTION Achieving quality integrated HIV services at your health centre is dependant on good planning and management. This chapter
CHAPTER 2 PLANNING INTEGRATED HIV SERVICES AT THE HEALTH CENTRE 2.1 INTRODUCTION Achieving quality integrated HIV services at your health centre is dependant on good planning and management. This chapter
HIV. Transmission modes. Transmission modes in children. Prevention of mother-to-child transmission of HIV. HIV identified in 1983
 Prevention of mother-to-child transmission of HIV HIV identified in 1983 HIV AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia and wasting often combined Retrospectively,
Prevention of mother-to-child transmission of HIV HIV identified in 1983 HIV AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia and wasting often combined Retrospectively,
Care of the HIV-Exposed Infant
 Care of the HIV-Exposed Infant Use of Flipchart To promote quality and consistency of counseling Why use the counseling flipchart? To improve HIV-exposed infant outcomes through high quality counseling.
Care of the HIV-Exposed Infant Use of Flipchart To promote quality and consistency of counseling Why use the counseling flipchart? To improve HIV-exposed infant outcomes through high quality counseling.
Clinical guidelines for the management of HIV/AIDS in adults and adolescents 15 years. SAHIVCS - CME 13/06/15 DR.Henry Sunpath
 Clinical guidelines for the management of HIV/AIDS in adults and adolescents 15 years SAHIVCS - CME 13/06/15 DR.Henry Sunpath 1 Introduction What is new? Goals and objectives Guiding principles HIV continuum
Clinical guidelines for the management of HIV/AIDS in adults and adolescents 15 years SAHIVCS - CME 13/06/15 DR.Henry Sunpath 1 Introduction What is new? Goals and objectives Guiding principles HIV continuum
Infertility Treatment and HIV
 Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Infertility Treatment and HIV Infertility Treatment by IVF Or Intra-cytoplasmic Sperm Injections (ICSC) In Chronic HIV-1 Sero- discordant Couples (Poster 670) Retrospective study of outcome of IVF or ICSC
Anti Retroviral Traitment (ARVs)
") Anti Retroviral Traitment (ARVs) IEC material for People With Disabilities UPHLS - 2015 - Anti Retroviral Traitment Booklet Produced by AZ MEDIA No part of this publication may be reproduced without prior
Anti Retroviral Traitment (ARVs) IEC material for People With Disabilities UPHLS - 2015 - Anti Retroviral Traitment Booklet Produced by AZ MEDIA No part of this publication may be reproduced without prior
Clinical skills building - HIV drug resistance
 Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
Clinical skills building - HIV drug resistance Richard Lessells Clinical case 44-year old HIV-positive male HIV diagnosis 2010 Pre-treatment CD4+ count not known Initiated first-line ART (TDF/FTC/EFV)
treatment during pregnancy and breastfeeding
 treatment during pregnancy and breastfeeding Topics covered Introduction. Preventing parent-to-child transmission. AZT as a single therapy. Treatment begun late in pregnancy. Nevirapine for mothers and
treatment during pregnancy and breastfeeding Topics covered Introduction. Preventing parent-to-child transmission. AZT as a single therapy. Treatment begun late in pregnancy. Nevirapine for mothers and
2016 Perinatal Treatment Guidelines Update
 Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
Case year old single gay man First contact with clinic in Nov Unprotected sex 60 hours previously Received PEP Remained HIV-negative
 PrEP Case Studies Case 1 62 year old single gay man First contact with clinic in Nov 2011 Unprotected sex 60 hours previously Received PEP Remained HIV-negative Repeat exposures requiring PEP in 2013,
PrEP Case Studies Case 1 62 year old single gay man First contact with clinic in Nov 2011 Unprotected sex 60 hours previously Received PEP Remained HIV-negative Repeat exposures requiring PEP in 2013,
Breast Feeding for Women with HIV?
 Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
Breast Feeding for Women with HIV? CHIVA / BHIVA Hermione Lyall Imperial Healthcare NHS Trust 17.11.17 Acknowledgements: Nell Freeman-Romilly, Pat Tookey, Claire Townsend, Claire Thorne, Kate Francis,
HIV/AIDS Prenatal Care for HIV+ Mothers. 1. Algorithm for Prenatal Screening & Care (Antepartum)
") 7/10/18 njm 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+
7/10/18 njm 1. Algorithm for Prenatal Screening & Care (Antepartum) 2. Algorithm for Prenatal HIV Screening and Care (Mother refuses screening) 3. Algorithm for Intrapartum Care 4. Prenatal Care for HIV+
Family Planning and Sexually Transmitted. Infections, including HIV
 Infections, including HIV Family Planning and Sexually Transmitted Introduction To protect themselves, people need correct information about sexually transmitted infections (STIs), including HIV. Women
Infections, including HIV Family Planning and Sexually Transmitted Introduction To protect themselves, people need correct information about sexually transmitted infections (STIs), including HIV. Women
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT
 PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
Advancing Treatment 2.0: Progress on the 2013 Consolidated Guidelines What s new
 Advancing Treatment 2.0: Progress on the 2013 Consolidated Guidelines What s new H I V / A I D S D e p a r t m e n t WHO HQ Meg Doherty, MD, MPH, PhD Coordinator Treatment and Care November 5, 2012 1 Overview
Advancing Treatment 2.0: Progress on the 2013 Consolidated Guidelines What s new H I V / A I D S D e p a r t m e n t WHO HQ Meg Doherty, MD, MPH, PhD Coordinator Treatment and Care November 5, 2012 1 Overview
Important Safety Information About Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP)
") Important Safety Information About Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) For Healthcare Providers About Emtricitabine/Tenofovir Disoproxil
Important Safety Information About Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) For Healthcare Providers About Emtricitabine/Tenofovir Disoproxil
Overview of 2013 WHO consolidated ARV guidelines and update plans. Marco Vitoria HIV/AIDS Department WHO Geneva September 2014
 AMDS ANNUAL STAKEHOLDERS AND PARTNERS MEETING Overview of 2013 WHO consolidated ARV guidelines and update plans Marco Vitoria HIV/AIDS Department WHO Geneva September 2014 AMDS ANNUAL STAKEHOLDERS AND
AMDS ANNUAL STAKEHOLDERS AND PARTNERS MEETING Overview of 2013 WHO consolidated ARV guidelines and update plans Marco Vitoria HIV/AIDS Department WHO Geneva September 2014 AMDS ANNUAL STAKEHOLDERS AND
GLOBAL AIDS MONITORING REPORT
 KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
KINGDOM OF SAUDI ARABIA MINISTRY OF HEALTH GLOBAL AIDS MONITORING REPORT COUNTRY PROGRESS REPORT 2017 KINGDOM OF SAUDI ARABIA Submission date: March 29, 2018 1 Overview The Global AIDS Monitoring 2017
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA. Date
 CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
Infant feeding in the ARV era. Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital
 Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
Infant feeding in the ARV era Gerhard Theron Gerhard Theron Department of Obstetrics and Gynaecology Faculty of Health Sciences and Tygerberg Hospital Global HIV infections: 2007 12 countries account for
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES
 POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
POLICY BRIEF HIV TREATMENT TRANSITION TO NEW ANTIRETROVIRALS IN HIV PROGRAMMES JULY 2017 WHO This policy brief provides advice on a phased approach to transitioning to new WHO-recommended HIV treatment
The Global Fund s role as a strategic and responsible investor in HIV/AIDS: Paediatrics and PMTCT
 The Global Fund s role as a strategic and responsible investor in HIV/AIDS: Paediatrics and PMTCT Peter McDermott Managing Director, CIFF 19 th Board meeting, Geneva 6 th May 2009 Investment Criteria Measurable...change
The Global Fund s role as a strategic and responsible investor in HIV/AIDS: Paediatrics and PMTCT Peter McDermott Managing Director, CIFF 19 th Board meeting, Geneva 6 th May 2009 Investment Criteria Measurable...change
SA TB Guidelines The interface with Advanced Clinical Care
 SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
First line ART Rilpirivine A New NNRTI. Chris Jack Physician, Durdoc Centre ethekwini
 First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Malaysian Consensus Guidelines on Antiretroviral Therapy Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh
 Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
treatment VIRAL SUPPRESSION SUPPORT ART IS THE ONLY WAY TO CONTROL HIV TIPS FOR TAKING ART ADHERENCE Benefits of ART Start Know Your ARVs today ARVs
 treatment Benefits of ART Know Your ARVs Start ARVs today SUPPORT VIRAL SUPPRESSION TIPS FOR TAKING ART ART IS THE ONLY WAY TO CONTROL HIV ADHERENCE HIV: BASIC FACTS HIV stands for the Human Immunodeficiency
treatment Benefits of ART Know Your ARVs Start ARVs today SUPPORT VIRAL SUPPRESSION TIPS FOR TAKING ART ART IS THE ONLY WAY TO CONTROL HIV ADHERENCE HIV: BASIC FACTS HIV stands for the Human Immunodeficiency
2nd line failure, provincial evaluation process for 3rd line therapy, 3rd line treatment options James Nuttall
 2nd line failure, provincial evaluation process for 3rd line therapy, 3rd line treatment options James Nuttall Paediatric Infectious Diseases Unit, Red Cross War Memorial Children s Hospital & University
2nd line failure, provincial evaluation process for 3rd line therapy, 3rd line treatment options James Nuttall Paediatric Infectious Diseases Unit, Red Cross War Memorial Children s Hospital & University
Prioritized research questions for adolescent HIV testing, treatment and service delivery
 Prioritized research questions for adolescent HIV testing, treatment and service delivery The World Health Organization (WHO) and the Collaborative Initiative for Paediatric HIV Education and Research
Prioritized research questions for adolescent HIV testing, treatment and service delivery The World Health Organization (WHO) and the Collaborative Initiative for Paediatric HIV Education and Research
Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive:
 Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive: Rationale for the call to action, progress to date and dealing with realities Rene Ekpini, MD, MPH Senior Adviser,
Elimination of New HIV Infections among Children by 2015 and Keeping their Mothers Alive: Rationale for the call to action, progress to date and dealing with realities Rene Ekpini, MD, MPH Senior Adviser,
Scaling Up Treatment in Zimbabwe: The path to high coverage
 Scaling Up Treatment in Zimbabwe: The path to high coverage IAS Conference Dr. Tsitsi Mutasa-Apollo ART Programme Coordinator, Zimbabwe 30 th June, 2013 Kuala Lumpur, Malaysia Outline Introduction Background
Scaling Up Treatment in Zimbabwe: The path to high coverage IAS Conference Dr. Tsitsi Mutasa-Apollo ART Programme Coordinator, Zimbabwe 30 th June, 2013 Kuala Lumpur, Malaysia Outline Introduction Background
Objectives. Outline. Section 1: Interaction between HIV and pregnancy. Effects of HIV on Pregnancy. Section 2: Mother-to-Child-Transmission (MTCT)
") Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
HIV AND INFANT FEEDING
 HIV AND INFANT FEEDING UPDATED WHO GUIDELINES, 2016 Nigel Rollins Maternal, Newborn, Child and Adolescent Health WHO guidelines http://www.who.int/hiv/en/ Setting national recommendations for infant feeding
HIV AND INFANT FEEDING UPDATED WHO GUIDELINES, 2016 Nigel Rollins Maternal, Newborn, Child and Adolescent Health WHO guidelines http://www.who.int/hiv/en/ Setting national recommendations for infant feeding
Considerations for the Introduction of TLD in National Programs: PEPFAR Guidance on Developing Clinical and Programmatic Recommendations
 Considerations for the Introduction of TLD in National Programs: PEPFAR Guidance on Developing Clinical and Programmatic Recommendations December 2018 2 Table of Contents ACRONYMS... 3 INTRODUCTION...
Considerations for the Introduction of TLD in National Programs: PEPFAR Guidance on Developing Clinical and Programmatic Recommendations December 2018 2 Table of Contents ACRONYMS... 3 INTRODUCTION...
Objectives. Types of HIV Tests. Age Appropriateness of Tests. Breastfeeding and HIV Testing. Why are there different tests for different ages?
 Objectives At the end of the lesson participants will be able to: Identify the types of HIV tests available in Botswana State who should be tested Identify which tests are used for infants and children
Objectives At the end of the lesson participants will be able to: Identify the types of HIV tests available in Botswana State who should be tested Identify which tests are used for infants and children
CONSOLIDATED GUIDELINES ON THE USE OF ANTIRETROVIRAL DRUGS FOR TREATING AND PREVENTING HIV INFECTION WHAT S NEW
 POLICY BRIEF CONSOLIDATED GUIDELINES ON THE USE OF ANTIRETROVIRAL DRUGS FOR TREATING AND PREVENTING HIV INFECTION WHAT S NEW NOVEMBER 2015 WHO Library Cataloguing-in-Publication Data Policy brief: consolidated
POLICY BRIEF CONSOLIDATED GUIDELINES ON THE USE OF ANTIRETROVIRAL DRUGS FOR TREATING AND PREVENTING HIV INFECTION WHAT S NEW NOVEMBER 2015 WHO Library Cataloguing-in-Publication Data Policy brief: consolidated
Contraception for Women and Couples with HIV. Knowledge Test
 Contraception for Women and Couples with HIV Knowledge Test Instructions: For each question below, check/tick all responses that apply. 1. Which statements accurately describe the impact of HIV/AIDS in
Contraception for Women and Couples with HIV Knowledge Test Instructions: For each question below, check/tick all responses that apply. 1. Which statements accurately describe the impact of HIV/AIDS in
2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents. When to Start and What ART to Use in 1 st and 2 nd Line December 2009
 2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents When to Start and What ART to Use in 1 st and 2 nd Line December 2009 Historic Evolution of CD4 Criteria for ART Initiation in
2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents When to Start and What ART to Use in 1 st and 2 nd Line December 2009 Historic Evolution of CD4 Criteria for ART Initiation in
Dr Graham P Taylor Reader in Communicable Diseases
 HIV in Pregnancy Joint RCOG/BHIVA Multidisciplinary Conference Dr Graham Taylor Imperial College London Friday 20 January 2012, Royal College of Obstetricians and Gynaecologist, London Prevention of post-partum
HIV in Pregnancy Joint RCOG/BHIVA Multidisciplinary Conference Dr Graham Taylor Imperial College London Friday 20 January 2012, Royal College of Obstetricians and Gynaecologist, London Prevention of post-partum
What Women Need to Know: The HIV Treatment Guidelines for Pregnant Women
 : The HIV Treatment Guidelines for Pregnant Women : The HIV Treatment Guidelines for Pregnant Women What Women Need to Know: Prepared by Elaine Gross, RN, MS, CNS-C National Pediatric & Family HIV Resource
: The HIV Treatment Guidelines for Pregnant Women : The HIV Treatment Guidelines for Pregnant Women What Women Need to Know: Prepared by Elaine Gross, RN, MS, CNS-C National Pediatric & Family HIV Resource
Use of a Multidisciplinary Care Model for Pregnant Women Living with HIV & Their Infants Sarah McBeth, MD MPH
 Use of a Multidisciplinary Care Model for Pregnant Women Living with HIV & Their Infants Sarah McBeth, MD MPH University of Pittsburgh Medical Center Disclosures Presenter has no financial interests to
Use of a Multidisciplinary Care Model for Pregnant Women Living with HIV & Their Infants Sarah McBeth, MD MPH University of Pittsburgh Medical Center Disclosures Presenter has no financial interests to
European Guidelines. for the Clinical Management and Treatment of HIV Infected Adults
 European Guidelines for the Clinical Management and Treatment of HIV Infected Adults 2005 These Euroguidelines result from the comparison of guidelines from several European countries and from a discussion
European Guidelines for the Clinical Management and Treatment of HIV Infected Adults 2005 These Euroguidelines result from the comparison of guidelines from several European countries and from a discussion
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
Using new ARVs in pregnancy Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 3 June 2017 We have effective drugs. There is no reason why any mother should die of AIDS. There
Difference of opinion? Michelle Moorhouse 24 Sep 2014
 Difference of opinion? Michelle Moorhouse 24 Sep 2014 Meet NN 52 years, female Nurse in pre-art clinic Referred Feb 2012 by dermatologist History of severe reactions to ART Erythema and bullous eruptions
Difference of opinion? Michelle Moorhouse 24 Sep 2014 Meet NN 52 years, female Nurse in pre-art clinic Referred Feb 2012 by dermatologist History of severe reactions to ART Erythema and bullous eruptions
Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) Training Guide for Healthcare Providers
 Training Guide for Healthcare Providers") Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) Training Guide for Healthcare Providers About emtricitabine/tenofovir disoproxil fumarate for HIV-1 PrEP
Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) Training Guide for Healthcare Providers About emtricitabine/tenofovir disoproxil fumarate for HIV-1 PrEP
What s New. In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group
 What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
Mother to Child HIV Transmission
 Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
Koff WC. NEJM 2010;363:e7 Mother to Child HIV Transmission Why We Still Need New Prevention Modalities Lynne M. Mofenson, M.D. Maternal and Pediatric Infectious Disease Branch Eunice Kennedy Shriver National
Paediatric HIV Resistance Referal Pathway. Mohern Archary Paediatric Infectious Diseases Unit King Edward VIII Hospital / University of KwaZulu Natal
 Paediatric HIV Resistance Referal Pathway Mohern Archary Paediatric Infectious Diseases Unit King Edward VIII Hospital / University of KwaZulu Natal Third line Antiretroviral treatment options in HIV positive
Paediatric HIV Resistance Referal Pathway Mohern Archary Paediatric Infectious Diseases Unit King Edward VIII Hospital / University of KwaZulu Natal Third line Antiretroviral treatment options in HIV positive
The Pregnancy Journey...
 The Pregnancy Journey... when you are living with HIV Authors: Angelina Namiba, Jo Manchester and Lucy Osman If you, or your partner, is HIV positive and you want to get pregnant, or you are pregnant or
The Pregnancy Journey... when you are living with HIV Authors: Angelina Namiba, Jo Manchester and Lucy Osman If you, or your partner, is HIV positive and you want to get pregnant, or you are pregnant or
The CQUIN Learning Network
 The CQUIN Learning Network Adolescents Living with HIV: National Guidelines, Minimum Package, Challenges and Priorities Swaziland Ms Nobuhle Mthethwa MOH- SWAZILAND October 24-27, 2017 Johannesburg, South
The CQUIN Learning Network Adolescents Living with HIV: National Guidelines, Minimum Package, Challenges and Priorities Swaziland Ms Nobuhle Mthethwa MOH- SWAZILAND October 24-27, 2017 Johannesburg, South
CLAUDINE HENNESSEY & THEUNIS HURTER
 HIV/AIDS/TB CLAUDINE HENNESSEY & THEUNIS HURTER KEY TERMS Do these sound familiar? What strange terms do you hear in the clinics? Any others to add?? HIV AIDS Viral Load & suppression CD4 count Regimen
HIV/AIDS/TB CLAUDINE HENNESSEY & THEUNIS HURTER KEY TERMS Do these sound familiar? What strange terms do you hear in the clinics? Any others to add?? HIV AIDS Viral Load & suppression CD4 count Regimen
Using new ARVs in pregnancy
 Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
Using new ARVs in pregnancy Dr Kerry Uebel Slides courtesy of Linda-Gail Bekker With thanks to CN Mnyani SA HIV Clinician s Society Meeting 5 August 2017 We have effective drugs. There is no reason why
Emerging Issues in HIV and Pregnancy. Lynne M. Mofenson, MD. HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation
 Emerging Issues in HIV and Pregnancy Lynne M. Mofenson, MD HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation Perinatal Transmission in the ART Era What s New? Antepartum ARV drug
Emerging Issues in HIV and Pregnancy Lynne M. Mofenson, MD HIV Senior Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation Perinatal Transmission in the ART Era What s New? Antepartum ARV drug
When to start: guidelines comparison
 The editorial staff When to start: guidelines comparison The optimal time to begin antiretroviral therapy remains a critical question for the HIV field, and consensus about the appropriate CD4+ cell count
The editorial staff When to start: guidelines comparison The optimal time to begin antiretroviral therapy remains a critical question for the HIV field, and consensus about the appropriate CD4+ cell count
Technical Guidance Note for Global Fund HIV Proposals. TREATMENT - Antiretroviral Treatment-infants, children and adults
 Technical Guidance Note for Global Fund HIV Proposals TREATMENT - Antiretroviral Treatment-infants, children and adults May 2010 This technical brief is designed to provide key technical information to
Technical Guidance Note for Global Fund HIV Proposals TREATMENT - Antiretroviral Treatment-infants, children and adults May 2010 This technical brief is designed to provide key technical information to
Living Positively with HIV
 Living Positively with HIV Pregnancy and Planning a Family How do I avoid pregnancy and STI? What is this booklet for? This booklet gives basic information about planning a family if you are living with
Living Positively with HIV Pregnancy and Planning a Family How do I avoid pregnancy and STI? What is this booklet for? This booklet gives basic information about planning a family if you are living with