Drug Allergy: A Rash ionale for Treatment
|
|
|
- Bartholomew Paul
- 5 years ago
- Views:
Transcription



1
2 Drug Allergy: A Rash ionale for Treatment Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Jordan O. Powell, PharmD Clinical Pharmacist Remote Order Verification Advocate Health Care
3 Disclosure and Conflict of Interest Heather and Jordan Powell declare no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings and honoraria.
4 Pharmacist Objectives At the conclusion of this program, the pharmacist will be able to: 1. Recognize hallmark signs and symptoms of IgE-mediated allergic reactions. 2. Select appropriate and effective pharmacologic treatments for drug allergy reactions. 3. Discuss the risks and benefits of implementing angiotensin II receptor blocker therapy after experiencing angiotensinconverting enzyme-inhibitor angioedema. 4. Describe the cross-reactivity of various antibiotic classes for patients with documented beta-lactam antibiotic allergies.
5 Technician Objectives At the conclusion of this program, the technician will be able to: 1. Recognize hallmark signs and symptoms of IgE-mediated allergic reactions. 2. Describe pharmacologic treatments for drug allergy reactions. 3. Discuss the risks and benefits of implementing angiotensin II receptor blocker therapy after experiencing angiotensinconverting enzyme-inhibitor angioedema. 4. Describe the cross-reactivity of various antibiotic classes for patients with documented beta-lactam antibiotic allergies.
6 Pre-Test Question #1 Which of the following is not an IgE-mediated reaction? A. Urticaria B. Anaphylaxis C. Angioedema D. Stevens Johnson Syndrome
7 Pre-Test Question #2 Which of the following situations would warrant use of an oral steroid for a patient with contact dermatitis? A. Dermatitis covering >20% of BSA B. Erythema and pruritus C. Dermatitis limited to areas not including the face or feet D. Duration < 4 days
8 Pre-Test Question #3 Angiotensin Receptor Blocker (ARB) administration is an absolute contraindication for anyone with documented Angiotensin Converting Enzyme Inhibitor (ACE-I) induced angioedema. A. True B. False
9 Pre-Test Question #4 The cross-reactivity of an IgE-mediated drug reaction occurring upon administration of a cephalosporin in a patient with a true penicillin allergy is approximately what percentage? A. 2% B. 10% C. 40% D. 100%
10 Drug Allergy: A Rash ionale for Treatment
11 Adverse Drug Reactions (ADRs) Type A (Predictable) Dose dependent Related to known pharmacologic actions of the drug Type B (Unpredictable) Dose independent Unrelated to known pharmacologic mechanism Occurs only in susceptible individuals Ann of Allergy Asthma Immun. 2015; 3: S1-S39
12 Type B ADRs Subclass Drug intolerance Drug idiosyncrasy Drug allergy Pseudo-allergy Description Undesirable pharmacologic effect that occurs at low, sometimes sub-therapeutic doses, without underlying abnormalities of metabolism, excretion, or bioavailability Abnormal or unexpected effect that is unrelated to the intended pharmacologic action of the drug Immunologically mediated responses that result in production of drug-specific antibodies, T cells, or both Manifestations mimic IgE-mediated allergic reactions but are due to direct release of mediators from mast cells and basophils; do not require a preceding period of sensitization Ann of Allergy Asthma Immun. 2015; 3: S1-S39
13 Drug Allergy Diagnosis Considerations 1. The symptoms and physical findings are compatible with an immune drug reaction 2. Temporal relationship between administration of the drug and an adverse event 3. Class and/or structure of the drug have been associated with immune reactions 4. Patient received the drug (or a cross-reacting drug) on 1 or more occasion 5. No other clear cause for the presenting manifestations 6. Skin test and/or laboratory findings are compatible with drug hypersensitivity Ann of Allergy Asthma Immun. 2015; 115:
14 Drug Allergy Classifications Gell-Coombs Classification o Type I: IgE-mediated o Type II: Cytotoxic o Type III: Immune complex o Type IV: Cellular mediated Mixed Drug Reactions o Drug rash with eosinophilia and systemic symptoms (DRESS) syndrome o Steven s Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN) o Red Man s Syndrome Ann of Allergy Asthma Immun. 2015; 115: Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78.
15 IgE-mediated Mechanism: Onset: Common drugs: Examples: Release of mediators (histamine, prostaglandins, leukotrienes, acid hydrolases, neutral proteases, proteoglycans, cytokines) from sensitized basophils and mast cells on contact with allergens Within minutes of exposure Biologics Antibiotics Heparin Protamine Insulin Urticaria Bronchospasm Anaphylaxis Angioedema Ann of Allergy Asthma Immun. 2015; 115: Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78.
16 Anaphylaxis Life threatening systemic hypersensitivity reaction upon contact with an allergen Signs/Symptoms Respiratory Cardiovascular Cutaneous Gastrointestinal Central Nervous System Mucous membrane swelling, hoarseness, stridor, wheezing Tachycardia, hypotension, chest pain Pruritus, urticaria, angioedema, flushing N/V, pain, diarrhea, dysphagia Aura of impending doom, dizziness, headache, confusion, seizure Ann of Allergy Asthma Immun. 2015; 115: Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78.
 Place in the supine position Ann of Allergy Asthma Immun. 2015; 115: 341-384. Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78.")
17 Anaphylaxis: Treatment Airway Support o Respiratory collapse: Intubate Nebulized ß2 agonists (albuterol) Administer 1-5 mg glucagon IV over 5 minutes for those on ß- blockers not responding to epinephrine Oxygen Remove the allergen (if possible) Place in the supine position Ann of Allergy Asthma Immun. 2015; 115: Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78. Image:
18 Anaphylaxis: Treatment Epinephrine o α1, ß1, ß2 adrenergic agonist vasoconstriction and bronchodilation o Prompt, early use should be considered given long onset of antihistamines and corticosteroids even in patients with mild symptoms o Dosing: Self-injectors IM or SubQ depending on brand: 0.3 mg into the anterolateral aspect of the middle third of the thigh every minutes until arrival at ED Circulatory collapse: IV normal saline Ann of Allergy Asthma Immun. 2015; 115: Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78.
19 Anaphylaxis: Treatment Antihistamines (H 1 or H 2 ) optional o Not useful for acute manifestations o H 1 : No direct evidence to support their use in this population evidence extrapolated from use in urticarial or allergic rhinitis mg diphenhydramine if IV 10 mg cetirizine if PO o H 2 : Not supported by RCT evidence Glucocorticoids - optional o Not useful for acute manifestations but thought to control prolonged symptoms 1-2 mg/kg (max 125 mg) IV methylprednisolone (or PO equivalent) o Do not administer if symptoms are managed by epinephrine alone Ann of Allergy Asthma Immun. 2015; 115: Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78.

20 Angioedema Diffuse vasodilation and increased vascular permeability Signs/Symptoms: Asymmetric, non-pitting edema of the subcutaneous or submucosal tissues of the lips, tongue, and face Diffuse abdominal pain and diarrhea Treatment: Airway support Drug discontinuation Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78. Image:
21 ACE-I Induced Angioedema Mechanism: Time frame: Incidence: Bradykinin elevation (inflammatory vasoactive peptide) diffuse vasodilation and increased vascular permeability May occur at any time Will take at least 24 hours to resolve post drug discontinuation % of all recipients Not related to specific agent or dose Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78.
22 ACE-I Angioedema Treatment Airway Support Icatibant (FIRAZYR ) selective bradykinin ß2 receptor antagonist Off-label use Antihistamines Fresh Frozen Plasma Corticosteroids? Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78.
23 TRANSCEND Trial Angiotensin II receptor blocker (ARB) or placebo in ACE-I intolerant patients Primary outcome was not ARB tolerance, but the composite of cardiovascular death, myocardial infarction, stroke, or hospitalization for heart failure Intolerability was mostly due to cough (88.2%), not angioedema (1.3%) Treatment-period angioedema occurrence not significantly different in ARB (0.07%) vs placebo (0.10%) groups (p > 0.05) Study not powered for sub-group analysis Lancet 2008; 372:
24 ARBs following ACE-I Angioedema Controversial Unreliable results from the TRANSCEND trial Risk of developing ARB induced angioedema after ACE-I angioedema ranges anywhere from 2-17% risk Recommendation: Reserve for patients with definite indications for ARBs, avoid use if patient needed airway support for angioedema Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78.
25 Drug Allergy Classifications Gell-Coombs Classification Type I: IgE-mediated Type II: Cytotoxic Type III: Immune complex Type IV: Cellular mediated Mixed Drug Reactions Drug rash with eosinophilia and systemic symptoms (DRESS) syndrome Steven s Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN) Red Man s Syndrome Ann of Allergy Asthma Immun. 2015; 115:
 Topical bacitracin Neomycin Glucocorticoids Local anesthetics Antihistamines Oral penicillins and sulfonamides Ann of Allergy Asthma Immun.")
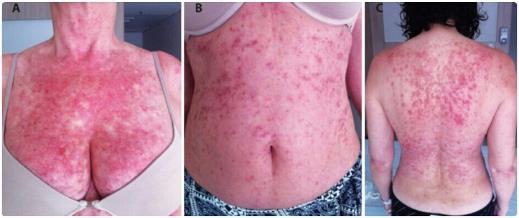
26 Cellular mediated Example Symptoms: Common drugs: Contact dermatitis (topical induction and elicitation of sensitization by a drug is limited to the skin) Delayed cutaneous eruptions (maculopapular exanthems, vesicles, and crusted lesions) Topical bacitracin Neomycin Glucocorticoids Local anesthetics Antihistamines Oral penicillins and sulfonamides Ann of Allergy Asthma Immun. 2015; 3: S1-S39 Image:

27 Cellular Mediated Allergy Treatment Drug/Irritant discontinuation Aluminum acetate compresses, calamine lotion, and/or colloidal oatmeal compresses or baths for pruritus reduction Ann of Allergy Asthma Immun. 2015; 3: S1-S39 Image:
28 Cellular Mediated Allergy Treatment Topical Corticosteroids o Long term use should be avoided o Potency depends on vehicle and increases if steroid is applied after shower/bath and/or if application site is covered AAFP. 2009; 79(2): Ann of Allergy Asthma Immun. 2015; 3: S1-S39 Image:
29 Cellular Mediated Allergy Treatment Topical Corticosteroids (cont.) o High potency For dermatitis NOT involving the face or flexural areas once or twice daily for 2-4 weeks Should be used for long-term control of chronic dermatitis of the hands, feet, or non-flexural areas once daily 3x/week on alternate days o Medium or low-potency For dermatitis of the face and flexural areas once or twice daily for 1-2 weeks Ann of Allergy Asthma Immun. 2015; 3: S1-S39

30 Cellular Mediated Allergy Treatment Steroid Vehicle Pros Cons Ointment Creams Lotions Gels (+) lubrication and occlusion (+) absorption (+) lubrication Vanish into the skin Drying effects for exudative inflammation Least greasy and occlusive Contain alcohol for drying effects Good for hairy areas where they can penetrate easily and leave little residue Quick drying effects for exudative inflammation Good for hairy areas where they can penetrate easily and leave little residue Cannot use in hairy areas May cause maceration and folliculitis on intertriginous areas Greasy Less potent than ointments Contain preservatives Less potent than ointments and creams Less potent than ointments and creams AAFP. 2009; 79(2): Ann of Allergy Asthma Immun. 2015; 3: S1-S39 Image:
31 Cellular Mediated Allergy Treatment Topic Steroid Potency Ultra high (I) High (II) Medium to high (III) Generic Augmented betamethasone dipropionate 0.05% Clobetasol propionate 0.05% Diflorasone diacetate 0.05% Fluocinonide 0.1% Flurandrenolide 4 mcg per m 2 Halobetasol propionate 0.05% Amcinonide 0.1% Augmented betamethasone dipropionate 0.05% Desoximetasone 0.25% and 0.05% Diflorasone diacetate 0.05% Fluocinonide 0.05% Halcinonide 0.1% Betamethasone dipropionate 0.05% Fluticasone propionate 0.005% Vehicles available Ointment, gel Ointment, cream, lotion, gel Ointment Cream Tape Ointment, Cream Ointment Cream, lotion Ointment, cream, gel Cream Ointment, cream, gel Ointment, cream Cream Ointment AAFP. 2009; 79(2):
32 Cellular Mediated Allergy Treatment Topic Steroid Potency Medium (IV and V) Low (VI) Least potent (VII) Generic Betamethasone valerate 0.1% Desoximetasone 0.05% Fluticasone propionate 0.05% Hydrocortisone butyrate 0.1% Hydrocortisone probutate 0.1% Hydrocortisone valerate 0.2% Mometasone furoate 0.1% Triamcinolone acetonide 0.1% Alclometasone dipropionate 0.05% Desonide 0.05% Fluocinolone 0.01% Hydrocortisone butyrate 0.1% Hydrocortisone 1% and 2.5% Vehicles available Cream, lotion Cream Cream Ointment Cream Ointment, cream Ointment, cream, lotion Ointment, cream, lotion Ointment, cream Ointment, cream, lotion, gel Cream Cream Ointment, cream, lotion AAFP. 2009; 79(2):
33 Cellular Mediated Allergy Treatment Oral Corticosteroids o Prednisone mg/kg (max 60 mg/day) for 7 days then tapered over two weeks for dermatitis >20% of BSA or when disabling (hands, feet, genitalia) Topical tacrolimus Use for contact dermatitis that is chronic and resistant to topical steroids or induced by topical steroids Ann of Allergy Asthma Immun. 2015; 3: S1-S39
34 Drug Allergy Classifications Gell-Coombs Classification Type I: IgE-mediated Type II: Cytotoxic Type III: Immune complex Type IV: Cellular mediated Mixed Drug Reactions Drug rash with eosinophilia and systemic symptoms (DRESS) syndrome Steven s Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN) Red Man s Syndrome Ann of Allergy Asthma Immun. 2015; 115:
35 DRESS Syndrome Drug-induced, multi-organ inflammatory response that may be life-threatening Symptoms Time frame: Common Drugs: Cutaneous eruptions (exanthems, erythema multiforme, purpura) Fever Eosinophilia Hepatic and renal dysfunction Lymphadenopathy Facial edema 2 8 weeks after therapy initiation Anticonvulsants (carbamazepine, phenytoin, lamotrigine) Sulfa drugs Allopurinol Minocycline Abacavir Hydroxychloroquine Ann of Allergy Asthma Immun. 2015; 115:
36 DRESS Syndrome Image:
37 DRESS Syndrome Treatment Drug discontinuation Symptoms may worsen after drug therapy is discontinued and may persist for weeks to months (average recovery time is 6-9 weeks) Warm, humid environment with gentle skin care Corticosteroids Questionable efficacy High or super high potency topical corticosteroids 2-3x/week for relief of pruritus and skin inflammation Ann of Allergy Asthma Immun. 2015; 115:
38 Drug Allergy Classifications Gell-Coombs Classification Type I: IgE-mediated Type II: Cytotoxic Type III: Immune complex Type IV: Cellular mediated Mixed Drug Reactions Drug rash with eosinophilia and systemic symptoms (DRESS) syndrome Steven s Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN) Red Man s Syndrome Ann of Allergy Asthma Immun. 2015; 115:

39 Steven s Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN) Image: clinical?pa=rdemmpkmicdrpntbrqnpups%2bmoh8keo592uslzeumrprouzmrmimkpao7%2bflceso7aggkhqrdhuwe sz5%2ff2u4ywfkdv4rj2qcl5b1yazcpo%3d
40 Steven s Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN) Symptoms Time frame: Common Drugs: Confluent purpuric macules on face and trunk Severe, mucosal erosions on more than one mucosal surface with fever and organ involvement SJS is less severe with < 10% of body surface involved TEN involves detachment of > 30% of body surface with mucosal membrane involvement 4-28 days after therapy initiation Sulfonamides Cephalosporins Imidazole agents Quinolones Aromatic anticonvulsants (Carbamazepine, ethosuximide, lamotrigine, oxcarbazepine, phenobarbital, and primidone) Valproic acid Glucocorticoids Ann of Allergy Asthma Immun. 2015; 115:
41 SJS and TEN Treatment Drug discontinuation Wound care/referral to burn unit Fluids and nutrition Pain control Systemic corticosteroids (prednisone 1 mg/kg/day) o Controversial due to increased infection/mortality risk o Use within 3 days of onset at high doses IVIG (1mg/kg per day for 3 days) Controversial due to no high-quality evidence Use within hours of onset Ann of Allergy Asthma Immun. 2015; 115:
42 Drug Allergy Classifications Gell-Coombs Classification Type I: IgE-mediated Type II: Cytotoxic Type III: Immune complex Type IV: Cellular mediated Mixed Drug Reactions Drug rash with eosinophilia and systemic symptoms (DRESS) syndrome Steven s Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN) Red Man s Syndrome Ann of Allergy Asthma Immun. 2015; 115:

43 Red Man s Syndrome Image:
44 Red Man s Syndrome Vasoactive mediator (histamine) release from non-specific mast cell activation due to IV vancomycin administration causing an ADR that mimics an allergic reaction Symptoms Time frame: Treatment Pruritus Erythema and flushing of the face, neck, trunk, and/or upper extremities Hypotension May be immediate Slow infusion rate to over hours and increase the dilution volume -OR- Slow infusion rate to < 10 mg/min or run a 1 gm dose over 100 minutes (whichever is a slower infusion) Antihistamines (H1 and H2) Ann of Allergy Asthma Immun. 2015; 115:
45 Penicillin (PCN) Allergy Up to 10% of the population has a documented PCN allergy Up to 90% of these patients are not at risk of IgE mediated reactions Immunogenicity wanes over time Product of previously impure drug formulations Ann Intern Med. 2000;160(18): Ann Allergy Asthma Immunol. 2010;105(4):
 Carbapenems: ~ 0.9-1% Aztreonam Ceftazidime Ann Allergy Asthma Immunol. 2010;105(4):259-273. Ann Allergy Asthma Immunol. 2016;17(1):67-71.")
46 Penicillin (PCN) Allergy Cross-reactivity of ß-lactams: More dependent on side chains Cephalosporins (2 nd or 3 rd generation): ~1-2.5% Avoid early generations with AMOXICILLIN allergy (Rgroup side chain) Carbapenems: ~ 0.9-1% Aztreonam Ceftazidime Ann Allergy Asthma Immunol. 2010;105(4): Ann Allergy Asthma Immunol. 2016;17(1): J Allergy Clin Immunol. 2016;137(2):354.
47 Penicillin (PCN) Allergy Immediate (Type 1/IgE mediated) reactions are relative contraindications for re-exposure to PCNs Urticaria, angioedema, pruritis, flushing, anaphylaxis, hypotension, edema, wheezing Occur within 1 4 hours of drug exposure Late reactions warrant clinical judgement before reexposure to PCNs depending on severity Rash (maculopapular or morbilliform or contact dermatitis), RBC, WBC, and platelet destruction, and serum sickness Occur days to weeks after drug exposure Not predicted by skin tests Ann Intern Med. 2000;160(18): Ann Allergy Asthma Immunol. 2010;105(4):
48 Post-Test Question #1 Which of the following is not an IgE-mediated reaction? A. Urticaria B. Anaphylaxis C. Angioedema D. Stevens Johnson Syndrome
49 Post-Test Question #1 Which of the following is not an IgE-mediated reaction? A. Urticaria B. Anaphylaxis C. Angioedema D. Stevens Johnson Syndrome
50 Post-Test Question #2 Which of the following situations would warrant use of an oral steroid for a patient with contact dermatitis? A. Dermatitis covering >20% of BSA B. Erythema and pruritus C. Dermatitis limited to areas not including the face or feet D. Duration < 4 days
51 Post-Test Question #2 Which of the following situations would warrant use of an oral steroid for a patient with contact dermatitis? A. Dermatitis covering >20% of BSA B. Erythema and pruritus C. Dermatitis limited to areas not including the face or feet D. Duration < 4 days
52 Post-Test Question #3 Angiotensin Receptor Blocker (ARB) administration is an absolute contraindication for anyone with documented Angiotensin Converting Enzyme Inhibitor (ACE-I) induced angioedema. A. True B. False
53 Post-Test Question #3 Angiotensin Receptor Blocker (ARB) administration is an absolute contraindication for anyone with documented Angiotensin Converting Enzyme Inhibitor (ACE-I) induced angioedema. A. True B. False
54 Post-Test Question #4 The cross-reactivity of an IgE-mediated drug reaction occurring upon administration of a cephalosporin in a patient with a true penicillin allergy is approximately what percentage? A. 2% B. 10% C. 40% D. 100%
55 Post-Test Question #4 The cross-reactivity of an IgE-mediated drug reaction occurring upon administration of a cephalosporin in a patient with a true penicillin allergy is approximately what percentage? A. 2% B. 10% C. 40% D. 100%
56 Take Home Points Airway support should be the first step taken for IgE-mediated allergic reactions Choosing an appropriate topical steroid based on vehicle, potency, and application site is crucial to preventing unwanted side effects for contact dermatitis A history of ACE-I induced angioedema is not a absolute contraindication to treatment with an ARB but should likely be considered as one if the airway was compromised Of the 10% of the population with a reported penicillin allergy, 90% of these patients will tolerate a penicillin without an IgE-mediated allergic reaction
57 Resources & References Bernstein DI, et al. Drug allergy: an updated practice parameter. Ann of Allergy Asthma Immun. 2010; 105: 273.e2-e78. Ference JD, Last AR. Choosing topical corticosteroids. AAFP. 2009; 79(2): Fonacier L, et al. Contact dermatitis: a practice parameter update Ann of Allergy Asthma Immun. 2015; 3: S1-S39. Lieberman P, et al. Anaphylaxis a practice parameter update Ann of Allergy Asthma Immun. 2015; 115:
58 Speaker Contact Information Heather A. Powell, PharmD, BCPS o hpowell01@roosevelt.edu Jordan O. Powell, PharmD o jopowell15@gmail.com
VACCINE-RELATED ALLERGIC REACTIONS
 VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis IERHA Immunization Program September 2016 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever, lymphadenopathy
VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis IERHA Immunization Program September 2016 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever, lymphadenopathy
VACCINE-RELATED ALLERGIC REACTIONS
 VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis Public Health Immunization Program June 2018 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever,
VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis Public Health Immunization Program June 2018 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever,
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
Medication Policy Manual. Topic: Dupixent, dupilumab Date of Origin: March 10, Committee Approval: March 10, 2017 Next Review Date: May 2018
 Independent licensees of the Blue Cross and Blue Shield Association Medication Policy Manual Policy No: dru493 Topic: Dupixent, dupilumab Date of Origin: March 10, 2017 Committee Approval: March 10, 2017
Independent licensees of the Blue Cross and Blue Shield Association Medication Policy Manual Policy No: dru493 Topic: Dupixent, dupilumab Date of Origin: March 10, 2017 Committee Approval: March 10, 2017
Eucrisa. Eucrisa (crisaborole) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.25 Subject: Eucrisa Page: 1 of 6 Last Review Date: September 15, 2017 Eucrisa Description Eucrisa
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.25 Subject: Eucrisa Page: 1 of 6 Last Review Date: September 15, 2017 Eucrisa Description Eucrisa
Eucrisa. Eucrisa (crisaborole) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Eucrisa Page: 1 of 7 Last Review Date: June 22, 2018 Eucrisa Description Eucrisa (crisaborole)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Eucrisa Page: 1 of 7 Last Review Date: June 22, 2018 Eucrisa Description Eucrisa (crisaborole)
Allergic Emergencies and Anaphylaxis. George Porfiris MD, CCFP(EM),FCFP TEGH
,FCFP TEGH") Allergic Emergencies and Anaphylaxis George Porfiris MD, CCFP(EM),FCFP TEGH Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Allergic Emergencies and Anaphylaxis George Porfiris MD, CCFP(EM),FCFP TEGH Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
ALLERGIC EMERGENCIES 5/8/2015. Objectives for Pharmacists. Patient Case. Objectives for Technicians. Definition of Anaphylaxis.
 ALLERGIC EMERGENCIES Kristina Dawson, PharmD, BCPS Objectives for Pharmacists Describe the immunologic pathways to cause an allergic response Identify the most common triggers to cause Choose the appropriate
ALLERGIC EMERGENCIES Kristina Dawson, PharmD, BCPS Objectives for Pharmacists Describe the immunologic pathways to cause an allergic response Identify the most common triggers to cause Choose the appropriate
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Drug Allergy A Guide to Diagnosis and Management
 Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
Adverse Drug Reactions. Navigating the World of. Adverse Drug Reactions. Definition. Essential History Taking. Essential History Taking
 Adverse Drug Reactions Navigating the World of Adverse Drug Reactions Jason Knuffman, M.D. Quincy Medical Group Quincy, IL Allergy and Immunology Section Upon completion of this activity, the participant
Adverse Drug Reactions Navigating the World of Adverse Drug Reactions Jason Knuffman, M.D. Quincy Medical Group Quincy, IL Allergy and Immunology Section Upon completion of this activity, the participant
The safety and effectiveness of Dupixent in pediatric patients have not been established (1).
.") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.30 Subject: Dupixent Page: 1 of 6 Last Review Date: September 15, 2017 Dupixent Description Dupixent
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.30 Subject: Dupixent Page: 1 of 6 Last Review Date: September 15, 2017 Dupixent Description Dupixent
Pharmacologic Treatment of Atopic Dermatitis
 J KMA Pharmacotherapeutics Pharmacologic Treatment of Atopic Dermatitis Chun Wook Park, MD Department of Dermatology, Hallym University College of Medicine E mail : dermap@paran.com J Korean Med Assoc
J KMA Pharmacotherapeutics Pharmacologic Treatment of Atopic Dermatitis Chun Wook Park, MD Department of Dermatology, Hallym University College of Medicine E mail : dermap@paran.com J Korean Med Assoc
Supplementary Online Content
 Supplementary Online Content Shenoy E, Macy E, Rowe TA, Blumenthal KG. Evaluation and management of penicillin allergy. JAMA. doi:10.1001/jama.2018.19283 Table 1. Hypersensitivity reaction types Table
Supplementary Online Content Shenoy E, Macy E, Rowe TA, Blumenthal KG. Evaluation and management of penicillin allergy. JAMA. doi:10.1001/jama.2018.19283 Table 1. Hypersensitivity reaction types Table
Texas Children's Hospital Dermatology Service PCP Referral Guidelines- Atopic Dermatitis (AD)
") Diagnosis: ATOPIC DERMATITIS (AD) Texas Children's Hospital Dermatology Service PCP Referral Guidelines- Atopic Dermatitis (AD) PATIENT ADVICE: Unfortunately, there is no cure for atopic dermatitis, so
Diagnosis: ATOPIC DERMATITIS (AD) Texas Children's Hospital Dermatology Service PCP Referral Guidelines- Atopic Dermatitis (AD) PATIENT ADVICE: Unfortunately, there is no cure for atopic dermatitis, so
8/8/2016. Overview. Back to Basics: Immunology. Adverse Reactions to Drugs: Dispelling Myths
 Adverse Reactions to Drugs: Dispelling Myths Allison Ramsey, MD NPA Annual Conference September 30, 2016 Overview Review of types of hypersensitivity reactions Penicillin allergy IV contrast allergy Local
Adverse Reactions to Drugs: Dispelling Myths Allison Ramsey, MD NPA Annual Conference September 30, 2016 Overview Review of types of hypersensitivity reactions Penicillin allergy IV contrast allergy Local
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2116-3 Program Prior Authorization/Medical Necessity Medications Dupixent (dupilumab) P&T Approval Date 1/2017, 5/2017, 7/2017
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2116-3 Program Prior Authorization/Medical Necessity Medications Dupixent (dupilumab) P&T Approval Date 1/2017, 5/2017, 7/2017
Chapter 8. Learning Objectives. Learning Objectives 9/11/2012. Anaphylaxis. List symptoms of anaphylactic shock
 Chapter 8 Anaphylaxis Learning Objectives List symptoms of anaphylactic shock Discuss role of immune system in fighting antigens Define allergic response Learning Objectives Describe body s response to
Chapter 8 Anaphylaxis Learning Objectives List symptoms of anaphylactic shock Discuss role of immune system in fighting antigens Define allergic response Learning Objectives Describe body s response to
Recognition & Management of Anaphylaxis in the Community. S. Shahzad Mustafa, MD, FAAAAI
 Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures None Outline Define anaphylaxis Pathophysiology Common causes Recognition and Management Definition Acute,
Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures None Outline Define anaphylaxis Pathophysiology Common causes Recognition and Management Definition Acute,
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
7/25/2016. Use of Epinephrine in the Community. Knowledge Amongst Paramedics. Knowledge Amongst Paramedics survey of 3479 paramedics
 Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures Speaker s bureau Genentech, Teva Consultant Genentech, Teva Outline Knowledge gap Definition Pathophysiology
Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures Speaker s bureau Genentech, Teva Consultant Genentech, Teva Outline Knowledge gap Definition Pathophysiology
Chapter 65 Allergy and Immunology for the Internist. ingestion provoke an IgE antibody response and clinical symptoms in sensitive individuals.
 Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke
Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke
Anaphylaxis: Treatment in the Community
 : Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
: Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
Dupixent (dupilumab)
") Dupixent (dupilumab) Line(s) of Business: HMO; PPO; QUEST Integration Effective Date: TBD POLICY A. INDICATIONS The indications below including FDA-approved indications and compendial uses are considered
Dupixent (dupilumab) Line(s) of Business: HMO; PPO; QUEST Integration Effective Date: TBD POLICY A. INDICATIONS The indications below including FDA-approved indications and compendial uses are considered
PM-03 PED ALLERGY/ANAPHYLAXIS. Protocol SECTION: PM-03 PROTOCOL TITLE: PED ALLERGY/ANAPHYLAXIS REVISED: 01MAY2018
 SECTION: PROTOCOL TITLE: REVISED: 01MAY2018 BLS SPECIFIC CARE: See General Pediatric Care Protocol PM-1 - Determine patient s color category on length based resuscitation tape (Broselow Tape) Epi Pen Protocol
SECTION: PROTOCOL TITLE: REVISED: 01MAY2018 BLS SPECIFIC CARE: See General Pediatric Care Protocol PM-1 - Determine patient s color category on length based resuscitation tape (Broselow Tape) Epi Pen Protocol
Urticaria Moderate Allergic Reaction Mild signs/symptoms with any of following: Dyspnea, possibly with wheezes Angioneurotic edema Systemic, not local
 Allergic Reactions & Anaphylaxis Incidence In USA - 400 to 800 deaths/year Parenterally administered penicillin accounts for 100 to 500 deaths per year Hymenoptera stings account for 40 to 100 deaths per
Allergic Reactions & Anaphylaxis Incidence In USA - 400 to 800 deaths/year Parenterally administered penicillin accounts for 100 to 500 deaths per year Hymenoptera stings account for 40 to 100 deaths per
Drug allergy and Skin Disorders. Timothy Craig, DO, FACOI Professor of Medicine and Pediatrics Distinguished Educator Penn State University, Hershey
 Drug allergy and Skin Disorders Timothy Craig, DO, FACOI Professor of Medicine and Pediatrics Distinguished Educator Penn State University, Hershey The best screening test for anaphylaxis is? A. histamine
Drug allergy and Skin Disorders Timothy Craig, DO, FACOI Professor of Medicine and Pediatrics Distinguished Educator Penn State University, Hershey The best screening test for anaphylaxis is? A. histamine
Cutaneous Drug Reactions
 Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
EPIPEN INSERVICE Emergency Administration of Epinephrine for the Basic EMT. Michael J. Calice MD, FACEP St. Mary Mercy Hospital
 EPIPEN INSERVICE Emergency Administration of Epinephrine for the Basic EMT Michael J. Calice MD, FACEP St. Mary Mercy Hospital Case #1 NR is an 8 yo male c/o hot mouth and stomach ache after eating jelly
EPIPEN INSERVICE Emergency Administration of Epinephrine for the Basic EMT Michael J. Calice MD, FACEP St. Mary Mercy Hospital Case #1 NR is an 8 yo male c/o hot mouth and stomach ache after eating jelly
Emergency Department Guideline. Anaphylaxis
 Emergency Department Guideline Inclusion criteria: 1. Acute onset of an illness (minutes to hours) with a AND (b OR c): a. Skin and/or mucosa (pruritus, flushing, hives, angioedema) b. Respiratory compromise
Emergency Department Guideline Inclusion criteria: 1. Acute onset of an illness (minutes to hours) with a AND (b OR c): a. Skin and/or mucosa (pruritus, flushing, hives, angioedema) b. Respiratory compromise
Anaphylaxis: The Atypical Varieties
 Anaphylaxis: The Atypical Varieties John Johnson, D.O., PGY-4 Allergy/Immunology Fellow University Hospitals of Cleveland Case Western Reserve University School of Medicine Disclosures: None What is Anaphylaxis?
Anaphylaxis: The Atypical Varieties John Johnson, D.O., PGY-4 Allergy/Immunology Fellow University Hospitals of Cleveland Case Western Reserve University School of Medicine Disclosures: None What is Anaphylaxis?
An unpredictable, dose-independent adverse drug reaction which is immunologically or IgEmediated.
 R H E U M A T I S M D I S O R D E R S A N D A L L E R G I E S APPROACH TO DRUG ALLERGY Dr Bernard Thong DEFINITION OF DRUG ALLERGY An unpredictable, dose-independent adverse drug reaction which is immunologically
R H E U M A T I S M D I S O R D E R S A N D A L L E R G I E S APPROACH TO DRUG ALLERGY Dr Bernard Thong DEFINITION OF DRUG ALLERGY An unpredictable, dose-independent adverse drug reaction which is immunologically
Drug induced allergy and hypersensitivity
 Drug induced allergy and hypersensitivity Yunita Sari Pane, Aznan Lelo Dept. Pharmacology & Therapeutic School of Medicine Universitas Sumatera Utara 13 Mei 2009, KBK-FK USU, Medan Drug Allergy Adverse
Drug induced allergy and hypersensitivity Yunita Sari Pane, Aznan Lelo Dept. Pharmacology & Therapeutic School of Medicine Universitas Sumatera Utara 13 Mei 2009, KBK-FK USU, Medan Drug Allergy Adverse
Objectives 8/30/2012. How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Adverse Drug Reactions
 Drug Allergies? Adverse Drug Reactions") How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Faoud Ishmael, MD, PhD Assistant Professor of Medicine Section of Allergy and Immunology Penn State College of Medicine I have no conflicts
How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Faoud Ishmael, MD, PhD Assistant Professor of Medicine Section of Allergy and Immunology Penn State College of Medicine I have no conflicts
Penicillin Allergy Guidance Document
 Key Points Penicillin Allergy Guidance Document Background Careful evaluation of antibiotic allergy and prior tolerance history is essential to providing optimal treatment The true incidence of penicillin
Key Points Penicillin Allergy Guidance Document Background Careful evaluation of antibiotic allergy and prior tolerance history is essential to providing optimal treatment The true incidence of penicillin
Adverse drug reactions
 Medications William Smith Adverse drug reactions Allergy? Side-effect? Intolerance? Background Adverse drug reactions (ADRs) vary from life-threatening anaphylaxis to minor common side-effects. Objective
Medications William Smith Adverse drug reactions Allergy? Side-effect? Intolerance? Background Adverse drug reactions (ADRs) vary from life-threatening anaphylaxis to minor common side-effects. Objective
Cutaneous Adverse Drug Reactions in Domestic Animals. Katherine Doerr, DVM, Dip. ACVD. Veterinary Dermatology Center
 Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Introduction: Severe adverse reactions:
 Immunotherapy and Anaphylaxis: Risks, Prevention, Recognition and Treatment by Frederick M. Schaffer, M.D. Associate Professor, The Medical University of South Carolina Introduction: Immunotherapy (IT)
Immunotherapy and Anaphylaxis: Risks, Prevention, Recognition and Treatment by Frederick M. Schaffer, M.D. Associate Professor, The Medical University of South Carolina Introduction: Immunotherapy (IT)
Systemic Allergic & Immunoglobulin Disorders
 Systemic Allergic & Immunoglobulin Disorders Bryan L. Martin, DO, MMAS, FACAAI, FAAAAI, FACP, FACOI Emeritus Professor of Medicine and Pediatrics President, American College of Allergy, Asthma & Immunology
Systemic Allergic & Immunoglobulin Disorders Bryan L. Martin, DO, MMAS, FACAAI, FAAAAI, FACP, FACOI Emeritus Professor of Medicine and Pediatrics President, American College of Allergy, Asthma & Immunology
KDIGO Conference San Francisco March KDIGO. Mechanisms of drug hypersensitivity. A. J. Bircher Dermatology/Allergology
 Conference San Francisco March 27 30 2014 Mechanisms of drug hypersensitivity A. J. Bircher Dermatology/Allergology University Hospital Basel Switzerland andreas.bircher@unibas.ch Disclosure of Interests
Conference San Francisco March 27 30 2014 Mechanisms of drug hypersensitivity A. J. Bircher Dermatology/Allergology University Hospital Basel Switzerland andreas.bircher@unibas.ch Disclosure of Interests
Pediatric Dermatology
 Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
DUPIXENT (dupilumab) subcutaneous injection
 subcutaneous injection") DUPIXENT (dupilumab) subcutaneous injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
DUPIXENT (dupilumab) subcutaneous injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
The Medical Letter. on Drugs and Therapeutics
 The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
Management of an immediate adverse event following immunisation
 Management of an immediate adverse event following immunisation The vaccinated person should remain under observation for a short interval to ensure that they do not experience an immediate adverse event.
Management of an immediate adverse event following immunisation The vaccinated person should remain under observation for a short interval to ensure that they do not experience an immediate adverse event.
The mechanisms of common drug hypersensitivities and implications for testing
 The mechanisms of common drug hypersensitivities and implications for testing R J Heddle 17 May 2016 Adverse Drug Reactions (ADR) Type A 85-90% of ADR Any individual, given sufficient dose & exposure Predictable
The mechanisms of common drug hypersensitivities and implications for testing R J Heddle 17 May 2016 Adverse Drug Reactions (ADR) Type A 85-90% of ADR Any individual, given sufficient dose & exposure Predictable
Penicillin Allergy and Use of Other Antibiotics
 Penicillin Allergy and Use of Other Antibiotics 7300-646PT Policy No.: 7310-646PT 8790-646PT Original Policy Date: 10/10/2016 Revision Date(s): Review Date(s): Approval: 11/17/16 Pharmacy & Therapeutics
Penicillin Allergy and Use of Other Antibiotics 7300-646PT Policy No.: 7310-646PT 8790-646PT Original Policy Date: 10/10/2016 Revision Date(s): Review Date(s): Approval: 11/17/16 Pharmacy & Therapeutics
: ALLERGIC REACTION
 6208.05: ALLERGIC REACTION INTRODUCTION Allergic (hypersensitivity) reactions are most often secondary to an exaggerated immune system response to a harmless foreign antigen (e.g. insect bite or sting,
6208.05: ALLERGIC REACTION INTRODUCTION Allergic (hypersensitivity) reactions are most often secondary to an exaggerated immune system response to a harmless foreign antigen (e.g. insect bite or sting,
Future of Pediatrics: Blisters, Hives and Other Tales from the Emergency Room June 14 th, 2016
 A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
Lecture 03: Drug allergy
 Lecture 03: Drug allergy 1. Basic Information Author: Netherlands Pharmacovigilance Centre Lareb Version date: 17 Nov 2017 Content: This hand-out describes Drug allergy and provides background information
Lecture 03: Drug allergy 1. Basic Information Author: Netherlands Pharmacovigilance Centre Lareb Version date: 17 Nov 2017 Content: This hand-out describes Drug allergy and provides background information
Skin Manifestations of Drug Reactions
 Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
Mast Cell Disorders. Andrew M. Smith, MD, MS
 Mast Cell Disorders Andrew M. Smith, MD, MS Division of Immunology, Allergy, and Rheumatology University of Cincinnati and Cincinnati VA Medical Centers August 10 and 11, 2012 Disclosures None The contents
Mast Cell Disorders Andrew M. Smith, MD, MS Division of Immunology, Allergy, and Rheumatology University of Cincinnati and Cincinnati VA Medical Centers August 10 and 11, 2012 Disclosures None The contents
Terms What is Anaphylaxis? Causes Signs & Symptoms Management Education Pictures Citations. Anaphylaxis; LBodak
 Leslie Bodak, EMT-P Terms What is Anaphylaxis? Causes Signs & Symptoms Management Education Pictures Citations Allergic Reaction: an abnormal immune response the body develops when a person has been previously
Leslie Bodak, EMT-P Terms What is Anaphylaxis? Causes Signs & Symptoms Management Education Pictures Citations Allergic Reaction: an abnormal immune response the body develops when a person has been previously
Who Should Be Premediciated for Contrast-Enhanced Exams?
 Who Should Be Premediciated for Contrast-Enhanced Exams? Jeffrey C. Weinreb, MD,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Types of Intravenous Contrast Media Iodinated Contrast Agents
Who Should Be Premediciated for Contrast-Enhanced Exams? Jeffrey C. Weinreb, MD,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Types of Intravenous Contrast Media Iodinated Contrast Agents
Allergy Immunotherapy in the Primary Care Setting
 Allergy Immunotherapy in the Primary Care Setting New York State College Health Association 2008 COMBINED ANNUAL MEETING October 2008 Mary Madsen RN BC University of Rochester Issues in Primary Care Practice
Allergy Immunotherapy in the Primary Care Setting New York State College Health Association 2008 COMBINED ANNUAL MEETING October 2008 Mary Madsen RN BC University of Rochester Issues in Primary Care Practice
Annex I: Proposed Core Safety Profile (CSP) 4.3 Contraindications
 4.3 Contraindications") Annex I: Proposed Core Safety Profile (CSP) 4.3 Contraindications Hypersensitivity to cefuroxime or to any of the excipients listed in section 6.1. Patients with known hypersensitivity to cephalosporin
Annex I: Proposed Core Safety Profile (CSP) 4.3 Contraindications Hypersensitivity to cefuroxime or to any of the excipients listed in section 6.1. Patients with known hypersensitivity to cephalosporin
Anaphylaxis: treatment in the community
 : treatment in the community Item Type Guideline Authors Health Service Executive Citation Health Service Executive. : treatment in the community. Dublin: Health Service Executive;. 5p. Publisher Health
: treatment in the community Item Type Guideline Authors Health Service Executive Citation Health Service Executive. : treatment in the community. Dublin: Health Service Executive;. 5p. Publisher Health
Student Health Center
 Referring Allergist Agreement Your patient is requesting that the University of Mary Washington Student Health Center (UMWSHC) administer allergy extracts provided by your office. Consistent with our policies
Referring Allergist Agreement Your patient is requesting that the University of Mary Washington Student Health Center (UMWSHC) administer allergy extracts provided by your office. Consistent with our policies
Antibiotic allergy in the Intensive Care. Sanjay Swaminathan Clinical Immunologist, Westmead and Blacktown Hospitals September 28, 2017
 Antibiotic allergy in the Intensive Care Sanjay Swaminathan Clinical Immunologist, Westmead and Blacktown Hospitals September 28, 2017 Outline of talk True or false? Case example Types of drug allergy
Antibiotic allergy in the Intensive Care Sanjay Swaminathan Clinical Immunologist, Westmead and Blacktown Hospitals September 28, 2017 Outline of talk True or false? Case example Types of drug allergy
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity. Disclosure Statement. Learning Objectives
 Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
DERMATOLOGIC EMERGENCIES. Mary Evers D.O., F.A.O.C.D. Georgetown, Texas
 DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
Emergency Dermatology. Emergency Dermatology
 Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
Anaphylaxis. Choosing Wisely with Academic Detailing Conference October 21, 2017
 Anaphylaxis Choosing Wisely with Academic Detailing Conference October 21, 2017 Disclosure Natasha Rodney-Cail, Pharmacist, Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance of Nova Scotia
Anaphylaxis Choosing Wisely with Academic Detailing Conference October 21, 2017 Disclosure Natasha Rodney-Cail, Pharmacist, Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance of Nova Scotia
VI.2 Elements for a public summary. VI.2.1 Overview of disease epidemiology
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Sinus infection (Acute bacterial sinusitis) Sinus infection (upper respiratory infection) is short-lived infection of the sinuses,
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Sinus infection (Acute bacterial sinusitis) Sinus infection (upper respiratory infection) is short-lived infection of the sinuses,
About the immune system
 The immune system and anaphylaxis edward.purssell@kcl.ac.uk About the immune system The immune system Protects the body from infectious organisms, foreign bodies and malignancies Surface barriers Innate
The immune system and anaphylaxis edward.purssell@kcl.ac.uk About the immune system The immune system Protects the body from infectious organisms, foreign bodies and malignancies Surface barriers Innate
Allergic Reactions and Anaphylaxis. William Mapes, NRP, I/C Chief, Brandon Area Rescue Squad Brandon, VT
 Allergic Reactions and Anaphylaxis William Mapes, NRP, I/C Chief, Brandon Area Rescue Squad Brandon, VT Allergy to Anaphylaxis Defined as a histamine-mediated spectrum of physiologic events that include:
Allergic Reactions and Anaphylaxis William Mapes, NRP, I/C Chief, Brandon Area Rescue Squad Brandon, VT Allergy to Anaphylaxis Defined as a histamine-mediated spectrum of physiologic events that include:
PERIOPERATIVE ANAPHYLAXIS: A BRIEF REVIEW
 PERIOPERATIVE ANAPHYLAXIS: A BRIEF REVIEW DEC 2011 ANDREW TRIEBWASSER DEPARTMENT OF ANESTHESIA HASBRO CHILDREN S HOSPITAL ADVERSE DRUG REACTIONS (ADR) IN THE PERIOPERATIVE ENVIRONMENT: OVERVIEW most perioperative
PERIOPERATIVE ANAPHYLAXIS: A BRIEF REVIEW DEC 2011 ANDREW TRIEBWASSER DEPARTMENT OF ANESTHESIA HASBRO CHILDREN S HOSPITAL ADVERSE DRUG REACTIONS (ADR) IN THE PERIOPERATIVE ENVIRONMENT: OVERVIEW most perioperative
Allergic rhinitis (Hay fever) Asthma Anaphylaxis Urticaria Atopic dermatitis
 Asthma Anaphylaxis Urticaria Atopic dermatitis") Hypersensitivity Disorders Hypersensitivity Disorders Immune Response IgE Disease Example Ragweed hay fever IgG Cytotoxic Immune complex T Cell Hemolytic anemia Serum sickness Poison ivy IgE-mediated Diseases
Hypersensitivity Disorders Hypersensitivity Disorders Immune Response IgE Disease Example Ragweed hay fever IgG Cytotoxic Immune complex T Cell Hemolytic anemia Serum sickness Poison ivy IgE-mediated Diseases
Managing Penicillin Allergy
 Managing Penicillin Allergy Brian T. Kelly, MD MA April 12, 2019 Objectives Review penicillin allergy prevalence, morbidity, and management Describe the penicillin testing and oral challenge process Provide
Managing Penicillin Allergy Brian T. Kelly, MD MA April 12, 2019 Objectives Review penicillin allergy prevalence, morbidity, and management Describe the penicillin testing and oral challenge process Provide
Five things to know about anaphylaxis
 Five things to know about anaphylaxis Magdalena Berger, MD FRCPC Allergist and Clinical Immunologist New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation
Five things to know about anaphylaxis Magdalena Berger, MD FRCPC Allergist and Clinical Immunologist New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation
ASDIN 10th Annual Scientific Meeting Final. COI Disclosure Statement. Intravenous Contrast Media: Basics
 COI Disclosure Statement There are no financial relationships or conflicts of interest to disclose with this presentation Melissa Hicks, BA, RT(R)(VI) Vascular Interventional Technologist University of
COI Disclosure Statement There are no financial relationships or conflicts of interest to disclose with this presentation Melissa Hicks, BA, RT(R)(VI) Vascular Interventional Technologist University of
TOPCORT Cream/Ointment (Mometasone furoate 0.1%)
") Published on: 10 Jul 2014 TOPCORT Cream/Ointment (Mometasone furoate 0.1%) Composition TOPCORT Cream Mometasone Furoate, IP... 0.1% w/w In a cream base... q.s. TOPCORT Ointment Mometasone Furoate, IP...
Published on: 10 Jul 2014 TOPCORT Cream/Ointment (Mometasone furoate 0.1%) Composition TOPCORT Cream Mometasone Furoate, IP... 0.1% w/w In a cream base... q.s. TOPCORT Ointment Mometasone Furoate, IP...
Omalizumab (Xolair ) ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication
 ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication") ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to
( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to
CENTENE PHARMACY AND THERAPEUTICS NEW DRUG REVIEW 3Q17 July August
 BRAND NAME Dupixent GENERIC NAME dupilumab MANUFACTURER Regeneron DATE OF APPROVAL March 28, 2017 PRODUCT LAUNCH DATE First week of April 2017 REVIEW TYPE Review type 1 (RT1): New Drug Review Full review
BRAND NAME Dupixent GENERIC NAME dupilumab MANUFACTURER Regeneron DATE OF APPROVAL March 28, 2017 PRODUCT LAUNCH DATE First week of April 2017 REVIEW TYPE Review type 1 (RT1): New Drug Review Full review
Transfusion Reactions
 Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
EL DORADO COUNTY EMS AGENCY PREHOSPITAL PROTOCOLS
 EL DORADO COUNTY EMS AGENCY PREHOSPITAL PROTOCOLS Effective: July 1, 2017 Reviewed: November 9, 2016 Revised: November 9, 2016 EMS Agency Medical Director ALLERGIC REACTION/ANAPHYLAXIS ADULT BLS TREATMENT
EL DORADO COUNTY EMS AGENCY PREHOSPITAL PROTOCOLS Effective: July 1, 2017 Reviewed: November 9, 2016 Revised: November 9, 2016 EMS Agency Medical Director ALLERGIC REACTION/ANAPHYLAXIS ADULT BLS TREATMENT
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Anaphylaxis in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Anaphylaxis in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Local Omalizumab Treatment Protocol (For children 6 to <12 years of age)
") Local Omalizumab Treatment Protocol (For children 6 to
Local Omalizumab Treatment Protocol (For children 6 to
Title: Management of Allergic Reactions after IV Contrast in Magnetic Resonance Imaging
 ABSTRACT FOR SPS POSTER CASE PRESENTATION K Singer Title: Management of Allergic Reactions after IV Contrast in Magnetic Resonance Imaging Introduction: Children undergoing radiologic imaging frequently
ABSTRACT FOR SPS POSTER CASE PRESENTATION K Singer Title: Management of Allergic Reactions after IV Contrast in Magnetic Resonance Imaging Introduction: Children undergoing radiologic imaging frequently
Endocarditis. By : Mehrnoush. dianatkhah
 Endocarditis By : Mehrnoush. dianatkhah Case 5.31, 31 years old woman CC : Fever, dyspnea, 3 days postpartum PMH : Mitral prolapse Fever 38.5 WBC : 8900 ESR : 84 CRP : 10.4 Cr : 0.6 NT Pro BNP: 5469 Physical
Endocarditis By : Mehrnoush. dianatkhah Case 5.31, 31 years old woman CC : Fever, dyspnea, 3 days postpartum PMH : Mitral prolapse Fever 38.5 WBC : 8900 ESR : 84 CRP : 10.4 Cr : 0.6 NT Pro BNP: 5469 Physical
Anaphylaxis in the Community
 Anaphylaxis in the Community ACES101210 Copyright 2010, AANMA www.aanma.org ACES2015 ACES101210 Copyright Copyright 2015 2010, Allergy AANMA & Asthma www.aanma.org Network AllergyAsthmaN Anaphylaxis Community
Anaphylaxis in the Community ACES101210 Copyright 2010, AANMA www.aanma.org ACES2015 ACES101210 Copyright Copyright 2015 2010, Allergy AANMA & Asthma www.aanma.org Network AllergyAsthmaN Anaphylaxis Community
ANAPHYLAXIS EMET 2015
 ANAPHYLAXIS EMET 2015 ANA = AGAINST PHYLAX = PROTECTION No standardised definition (they re working on it) All include the similar concept of: A serious, generalised or systemic, allergic or hypersensitivity
ANAPHYLAXIS EMET 2015 ANA = AGAINST PHYLAX = PROTECTION No standardised definition (they re working on it) All include the similar concept of: A serious, generalised or systemic, allergic or hypersensitivity
Antiallergics and drugs used in anaphylaxis
 Antiallergics and drugs used in anaphylaxis Antiallergics and drugs used in anaphylaxis The H 1 -receptor antagonists are generally referred to as antihistamines. They inhibit the wheal, pruritus, sneezing
Antiallergics and drugs used in anaphylaxis Antiallergics and drugs used in anaphylaxis The H 1 -receptor antagonists are generally referred to as antihistamines. They inhibit the wheal, pruritus, sneezing
PACKAGE INSERT USP ANTIBIOTIC
 Pr AMPICILLIN for Injection USP ANTIBIOTIC ACTIONS AND CLINICAL PHARMACOLOGY Ampicillin has a broad spectrum of bactericidal activity against many gram-positive and gramnegative aerobic and anaerobic bacteria.
Pr AMPICILLIN for Injection USP ANTIBIOTIC ACTIONS AND CLINICAL PHARMACOLOGY Ampicillin has a broad spectrum of bactericidal activity against many gram-positive and gramnegative aerobic and anaerobic bacteria.
Adverse drug reactions. Dr. Mark Haworth MBChB DA MRCA
 Adverse drug reactions Dr. Mark Haworth MBChB DA MRCA Types of drug reaction The appearance of known side effects to a drug e.g. respiratory depression following the administration of opioid analgesics
Adverse drug reactions Dr. Mark Haworth MBChB DA MRCA Types of drug reaction The appearance of known side effects to a drug e.g. respiratory depression following the administration of opioid analgesics
The Diagnosis and Management of Anaphylaxis
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-allergy/the-diagnosis-and-management-of-anaphylaxis/3919/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/focus-on-allergy/the-diagnosis-and-management-of-anaphylaxis/3919/
Anaphylaxis/Latex Allergy
 Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Sign up to receive ATOTW weekly -
 ANAPHYLAXIS ANAESTHESIA TUTORIAL OF THE WEEK 38 1 th DECEMBER 2006 Dr. Sara Rees Cardiff, UK Case History You are anaesthetising a fit and well 40 year old woman for total abdominal hysterectomy for menorrhagia.
ANAPHYLAXIS ANAESTHESIA TUTORIAL OF THE WEEK 38 1 th DECEMBER 2006 Dr. Sara Rees Cardiff, UK Case History You are anaesthetising a fit and well 40 year old woman for total abdominal hysterectomy for menorrhagia.
Drug Allergy HSJ 19/09/2011
 Drug Allergy HSJ 19/09/2011 BSACI Guidelines Definitions Mechanisms Clinical Features Risk factors Diagnosis Investigations Criteria for referral/investigation Mirakian et al. Clin Exp All 2008 ; 39: 43-61
Drug Allergy HSJ 19/09/2011 BSACI Guidelines Definitions Mechanisms Clinical Features Risk factors Diagnosis Investigations Criteria for referral/investigation Mirakian et al. Clin Exp All 2008 ; 39: 43-61
Eczema & Dermatitis Clinical features: Histopathological features: Classification:
 Eczema & Dermatitis Eczema is an inflammatory reactive pattern of skin to many and different stimuli characterized by itching, redness, scaling and clustered papulovesicles. Eczema and dermatitis are synonymous
Eczema & Dermatitis Eczema is an inflammatory reactive pattern of skin to many and different stimuli characterized by itching, redness, scaling and clustered papulovesicles. Eczema and dermatitis are synonymous
Myth: Prior Episodes Predict Future Reactions REALITY: No predictable pattern Severity depends on: Sensitivity of the individual Dose of the allergen
 Myth: Prior Episodes Predict Future Reactions REALITY: No predictable pattern Severity depends on: Sensitivity of the individual Dose of the allergen Anaphylaxis Fatalities Estimated 500 1000 deaths annually
Myth: Prior Episodes Predict Future Reactions REALITY: No predictable pattern Severity depends on: Sensitivity of the individual Dose of the allergen Anaphylaxis Fatalities Estimated 500 1000 deaths annually
Adverse Drug Reactions (ADRs) Outline
 Outline") Adverse Drug Reactions (ADRs) Outline 1. What are Adverse Drug Reactions (ADRs)? WHAT WHY HOW 2. How important are ADRs and are they preventable? 3. What are the classifications and mechanisms of ADRs?
Adverse Drug Reactions (ADRs) Outline 1. What are Adverse Drug Reactions (ADRs)? WHAT WHY HOW 2. How important are ADRs and are they preventable? 3. What are the classifications and mechanisms of ADRs?
Emergency Dermatology Dr Melissa Barkham
 Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Anaphylaxis. Perceive the differences between anaphylactic shock and other types of shock. Recognize its nature, causes & characteristics.
 Anaphylaxis Red : important Black : in male / female slides Pink : in female s slides only Blue : in male s slides only Females doctor notes Grey: Males doctor notes OBJECTIVES: By the end of this lecture,
Anaphylaxis Red : important Black : in male / female slides Pink : in female s slides only Blue : in male s slides only Females doctor notes Grey: Males doctor notes OBJECTIVES: By the end of this lecture,
Anaphylaxis for House Staff: Rapid Recognition and Treatment
 8/2/14 2:00 am Rapid Response Anaphylaxis for House Staff: Rapid Recognition and Treatment You are covering a patient with urosepsis. She is receiving her second dose of ceftriaxone. You are called for
8/2/14 2:00 am Rapid Response Anaphylaxis for House Staff: Rapid Recognition and Treatment You are covering a patient with urosepsis. She is receiving her second dose of ceftriaxone. You are called for
NEOFEN 60 mg suppository
 PACKAGE LEAFLET: INFORMATION FOR THE USER NEOFEN 60 mg suppository IBUPROFEN This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for a medicine, which outlines
PACKAGE LEAFLET: INFORMATION FOR THE USER NEOFEN 60 mg suppository IBUPROFEN This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for a medicine, which outlines
Allergy Skin Prick Testing
 Allergy Skin Prick Testing What is allergy? The term allergy is often applied erroneously to a variety of symptoms induced by exposure to a wide range of environmental or ingested agents. True allergy
Allergy Skin Prick Testing What is allergy? The term allergy is often applied erroneously to a variety of symptoms induced by exposure to a wide range of environmental or ingested agents. True allergy
Allergy & Anaphylaxis
 Allergy & Anaphylaxis (why, where, and what to do) Robert H. Brown, M.D., M.P.H. Professor Departments of Anesthesiology, Environmental Health Sciences, Medicine, and Radiology The Johns Hopkins Medical
Allergy & Anaphylaxis (why, where, and what to do) Robert H. Brown, M.D., M.P.H. Professor Departments of Anesthesiology, Environmental Health Sciences, Medicine, and Radiology The Johns Hopkins Medical
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October
 Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
GROUP 15 TOPICAL PREPARATIONS
 - 105 - GROUP 15 15.1 DERMATOLOGICAL PREPARATIONS 15.1.1 TOPICAL ANTIFUNGALS CLOTRIMAZOLE Indication: Treatment of susceptible fungal infections, dermatophytoses, superficial mycoses, and cutaneous candidiasis
- 105 - GROUP 15 15.1 DERMATOLOGICAL PREPARATIONS 15.1.1 TOPICAL ANTIFUNGALS CLOTRIMAZOLE Indication: Treatment of susceptible fungal infections, dermatophytoses, superficial mycoses, and cutaneous candidiasis
Michaela Lucas. Clinical Immunologist/Immunopathologist. Pathwest, QE2 Medical Centre, Princess Margaret Hospital
 Michaela Lucas Clinical Immunologist/Immunopathologist Pathwest, QE2 Medical Centre, Princess Margaret Hospital School of Medicine and Pharmacology, School of Pathology and Laboratory Medicine University
Michaela Lucas Clinical Immunologist/Immunopathologist Pathwest, QE2 Medical Centre, Princess Margaret Hospital School of Medicine and Pharmacology, School of Pathology and Laboratory Medicine University