Netherlands, Atrium Medical Center, Heerlen, the Netherlands. Rheumatology Unit, Department of Medicine DIMED, University of Padova, Italy
|
|
|
- Domenic Green
- 5 years ago
- Views:
Transcription

1 DR. SOFIA RAMIRO (Orcid ID : ) Article type : Full Length Is it useful to repeat MRI of the sacroiliac joints after three months or one year in the diagnostic process of patients with chronic back pain suspected of axial spondyloarthritis? P.A. Bakker, MD 1, S. Ramiro, MD, PhD D 1 Z. Ez-Zaitouni, MD 1, M. van Lunteren, MSc 1, I.J. Berg, MD, PhD 2, R. Landewé, MD, PhD 3, R. Ramonda MD, PhD 4, M. van Oosterhout, MD, PhD 5, PhD, M. Reijnierse MD, PhD 6, F.A. van Gaalen MD, PhD 1, D. van der Heijde, MD, PhD 1 1 Department of Rheumatology, Leiden University Medical Center, Leiden, the Netherlands 2 Department of Rheumatology, Diakonhjemmet Hospital, Oslo, Norway 3 Department of Rheumatology, Amsterdam Medical Rheumatology Center AMC, the Netherlands, Atrium Medical Center, Heerlen, the Netherlands 4 Rheumatology Unit, Department of Medicine DIMED, University of Padova, Italy 5 Department of Rheumatology, Groene Hart Ziekenhuis, Gouda, the Netherlands 6 Department of Radiology, Leiden University Medical Center, Leiden, the Netherlands There are no conflicts of interests for all individual authors. Running head: Usefulness of repeating MRI-SI in the diagnostic process of axspa This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. Please cite this article as doi: /art.40718
2 Address for correspondence and reprint requests: P.A.C. Bakker, MD Leiden University Medical Centre, Department of Rheumatology P.O. Box RC Leiden The Netherlands Telephone: Abstract Objective: To investigate the value of repeating MRI of the sacroiliac joints (MRI-SI) in the diagnostic process of early chronic back pain patients (CBP) suspected of axial SpondyloArthritis (axspa) and study determinants of MRI-SI-positivity. Methods: Patients with CBP (duration: 3 months, 2 year, onset <45 years) with 1 SpA-feature included in the SPondyloArthritis Caught Early cohort underwent baseline, three months and one year visits with evaluation of all SpA-features and repeated MRI-SI. MRI-SI-positivity according to ASAS was assessed by two (or three) well-trained readers, blinded for clinical information. Factors determining MRI-SI-positivity over follow-up were calculated by GEE analysis. Results: Of the 188 patients (38.3% male, mean (SD) age 31.0 (8.2) years, symptom duration 13.2 (7.1) months), 31 (16.5%) were MRI-SI-positive at baseline. After three months and one year 3/27 (11.1%) and 11/29 (37.9%) patients changed from MRI-SI positive to negative, respectively which was partly induced by the start of anti-tnf therapy. Changes from negative to positive were seen in 5/116 (4.3%) and 10/138 (7.2%) patients, respectively. HLA-B27-positivity and male gender independently determined the likelihood of a positive MRI at any time point (42% in HLA-B27+ men and 6% in HLA-B27- females). If the baseline MRI is negative, the likelihood of a positive MRI during follow-up is very low (max 7%).
3 Conclusion: MRI-SI ASAS status changes are seen in a minority of the patients. Both male gender and HLA-B27-positivity are important predictors of MRI-positivity. Repeating MRI after three months or one year in the diagnostic work-up in early disease is not useful. Introduction: In the diagnostic process of axial spondyloarthritis (axspa), sacroiliac joint imaging plays a pivotal role (1). Conventional radiography has always been and still is the most commonly used method to detect sacroiliitis. However, it is known that radiographic abnormalities evolve over several years of time, which contributes to a reported delay of 8-9 years in diagnosis (2) (3). This substantial delay in diagnosis is problematic since effective treatments are available for patients with axspa (4) (5) (6). Over the last decade, Magnetic Resonance Imaging (MRI) rapidly gained ground and proved to be an important imaging technique in the diagnostic process of (non-radiographic) axial spondyloarthritis (7). It has been shown that MRI can detect the early inflammatory stages of sacroiliitis, months to years before structural damage can be detected on a conventional radiograph (8) (9). Besides the fact that MRI has substantial advantages in terms of sensitivity, MRI has the benefit of providing information on activity and structural damage by one imaging modality (10) (11) (12). Axial spondyloarthritis (axspa) should be considered in patients with chronic back pain (CBP) with an onset before 45 years of age. Regrettably, no formal diagnostic criteria exist and there is no single SpA-feature with sufficient specificity to establish the diagnosis. The modified Berlin algorithm is a helpful tool for rheumatologists in establishing an early diagnosis of axspa with greater confidence (1). According to this algorithm, MRI of the sacroiliac joints (MRI-SI) should be performed in a certain group of patients after obtaining conventional radiographs and HLA-B27 testing (13). The more recently published EULAR recommendations on imaging in SpA even state that in certain cases, such as young patients and those with short symptom duration, MRI of the SI-joints is an alternative first imaging method (14).
4 Although inflammation on MRI is now widely considered as an important manifestation in early axspa, not much evidence is available on how inflammatory lesions develop over time (outside clinical trials) (15) (16). Though, with the augmented interest of MRI in the early diagnosis of axspa this is important. We do know that inflammatory lesions (bone marrow edema, BME) can change over relatively short periods of time in patients diagnosed with SpA. But in patients with CBP and with a suspicion of axspa, it is unclear if BME-lesions newly develop or fluctuate over time. For example, a relevant clinical question is if an MRI is completely normal and there is still a clinical suspicion of axspa, should the MRI be repeated? And if so, after what period of follow-up? Or does this not contribute to the diagnostic process? The SPondyloArthritis Caught Early (SPACE) cohort is an ideal cohort to investigate this research question since it includes a population of patients with back pain of short duration referred to rheumatologists with a suspicion of SpA (but without the mandatory presence of a single or multiple SpA-features). With this study, we aim to investigate the evolution of MRI-lesions over a 3-month and 1-year time frame in the SPACE-cohort. Patients and Methods: Study design and patient population: SPACE is a multi-national ongoing cohort study, started in January Across five participating centres in Europe, patients with chronic back pain ( 3 months, 2 years, onset < 45 years; aged 16 years and older) are included. Before start of the study, approval was obtained by the local medical ethics committees. Before inclusion, written informed consent was obtained from all patients in accordance with the Declaration of Helsinki. A detailed description of the SPACE cohort has been given elsewhere (17). All patients underwent a diagnostic work-up at baseline. This includes a physical examination, MRI and radiographs of the SI-joints (MRI-SI, X-SI respectively), HLA-B27 testing and examination of all other SpAfeatures (13) (18). Patients fulfilling the Assessment of SpondyloArthritis international Society (ASAS) axspa-criteria at baseline or patients with possible axspa (i.e. the presence of SpA-features though not sufficient to be classified as axspa, defined as the presence of 1 SpA-feature) were included for follow-up visits. At three months and 1-year follow-up, clinical and laboratory data were again collected and another MRI-SI was performed. It was considered arbitrarily that three month MRI data of about 150 patients was sufficient to
5 answer the question about the change over three months and therefore decided to leave out the three month MRI in the patients included in the cohort after July Imaging and scoring methodology: MRI-SIs were performed on a 1.5 Tesla MRI-scanner at baseline and follow-up. Coronal oblique MRI images were obtained, with a slice thickness of 4 millimetres. Both short tau inversion recovery (STIR) and T1 weighted turbo spin echo (T1TSE) sequences were acquired and evaluated in the scoring process. At baseline, conventional radiographs of the pelvis (sacroiliac joints) in anterior-posterior view (X-SI) were performed. MRI-SIs and X-SIs were scored independently by two trained and well-calibrated readers, blinded for patient characteristics, clinical data, time sequence and the other imaging modality. In case of discrepancy on dichotomous scores a third reader scored the images (see below for details). A radiograph was marked positive for sacroiliitis according to the fulfilment of the modified New York (mny) criteria: at least bilateral grade 2 sacroiliitis or at least unilateral grade 3 sacroiliitis was mandatory (19). According to the ASAS definition for a positive MRI, an MRI- SI was marked positive if 1 bone marrow edema (BME) lesion highly suggestive of SpA was present on 2 consecutive slices or if several BME lesions highly suggestive of SpA are visible on a single slice (18) (7). MRIs were also scored according to the SPondyloArthritis Research Consortium of Canada (SPARCC) score which measures inflammation on a continuous scale (range: 0-72) (20). According to the SPARCC score, the presence of increased signal corresponding to BME lesions is marked on 6 consecutive slices of an MRI-SI. The maximum score for two SI-joints on each slice is 8. In addition to these 8 points per slice, a score for intensity (adding 1 point) may be assigned to each SI-joint if a so-called intense signal is seen in any quadrant on each slice. The signal from pre-sacral blood vessels defined a lesion that is scored as intense. Further, a score for depth (adding 1 point) may be assigned to each SIjoint if a homogeneous and unequivocal increase in signal is extending over a depth of at least 1 cm from the articular surface on each slice, resulting in a maximum score of 12 points per slice. For assessment of both the ASAS definition and the SPARCC score on the STIR sequence, the readers took into account the findings on the T1TSE sequences, looking at both sequences simultaneously.
6 In case of disagreement on the presence of radiographic sacroiliitis (mny) or a positive MRI (ASAS-definition) amongst the two initial readers, a third reader served as adjudicator (final score: two out of three agreeing readers). The SPARCC scores of the two agreeing readers on a positive MRI were used for further analysis. Statistical methods: Disease characteristics of patients were presented using descriptive statistics. Then, we described the MRI-SI ASAS-status over time in different ways. First, by depicting the course of MRI-SI ASAS status at the (two or three) available time points and second, by means of a two-by-tow table reflecting changes in MRI ASAS-status (positive-negative). Agreement on the absence or presence of MRI-SI ASAS inflammation was assessed by cross-tabulation and expressed as Cohen s kappa. Cumulative probability plots were used to visualize baseline and 1 year-sparcc-scores in which patients were grouped according to either positivity or negativity according to the ASAS-definition. Subsequently, patients of special interest, i.e. in which the MRI changed from positive to negative or vice versa after three months and oneyear follow-up, were described phenotypically: according to the presence of SpA-features and other disease characteristics. Thereafter, we investigated the likelihood of having a positive MRI at any time point during follow-up and identified which factors determine MRI- SI ASAS-positivity. After the analysis for the whole group of patients, we repeated this analysis in the subset of patients that have IBP according to the ASAS definition. Subsequently, we looked at the likelihood of having a positive MRI in the follow-up time points (3 months or 1 year), taking into account the baseline MRI (positive vs negative), first in all patients and secondly in the subgroup of patients with IBP. This was done by using generalised estimated equation (GEE) analysis for binomial outcome variables: MRI ASAS status was defined as the dependent variable, HLA-B27 and gender being independent explanatory variables. CRP was added to the model as a covariate, in order to assess the contribution of CRP in explaining a positive MRI. The likelihood of finding a positive MRI if the baseline MRI is either positive or negative was calculated, taking into account HLA-B27 status and gender. Odds ratios from the model were converted into probabilities (likelihood) (21). Data analysis was performed using Stata SE v. 14 software (StataCorp LP, College Station), TX, USA).
7 Results: Patient characteristics In total, 188 patients were included in the current study. Baseline characteristics were described in Table 1. The mean age of the included patients was 31.0 years (SD 8.2 years) and 38.3% were male. The mean symptom duration of back pain was 13.2 months (SD 7.1 months) and 139 patients (74.3%) had inflammatory back pain according to the ASAS criteria definition. Almost half of the patients (48.4 %) were HLA-B27 positive. MRI findings Agreement between the two readers regarding the definition of a positive MRI-SI according to the ASAS definition was good: kappa In 8 of the 188 cases (4.3%) adjudication was needed since reader 1 and reader 2 were in disagreement on the MRI-SI ASAS status. The course of MRI-SI ASAS positivity over time is visualised in table 2. In 122 out of 188 patients, all three time points were available: baseline, three months and one-year followup. In 66 out of 188 patients, MRI was performed at two time points: in 21/66 patients at baseline and three months follow-up and in 45/66 patients at baseline and one-year followup. In all three scenarios mentioned above, the vast majority of patients 77.1% (145/188) had a negative MRI according to the ASAS definition at baseline which did not change at the follow-up time point(s) (triple/double-negative). In patients with all three time points available, persistence of a positive MRI was seen in (15/122) 12.3% of the patients (triplepositive) and (21/122) 17.2% of the patients showed MRI fluctuations over time (for instance: 0-0-1; 1-1-0; etcetera). Changes in MRI-SI ASAS-status over time are depicted in another way by means of a two-bytwo table (table 3). In contrast to table 2, data are clustered, shown independently of the availability of the third time point. The upper part of the table reflects changes over three months and changes over one-year time are shown in the lower part of the table. In 8 out of 143 patients (5.6%) a change in MRI-SI ASAS status was seen after three months follow-up. After a year follow-up, the percentage with a change in MRI-SI status was slightly higher: 12.6% (21/167). The MRI of 10 of 138 patients (7.2%) turned from negative to positive after one year follow-up (compared to 5/116 (4.3%) patients after three months) and on the
8 other hand, 11 out of 29 (37.9%) patients with a positive MRI-SI ASAS at baseline were negative after one year of follow-up (compared to 3/27 (11.1%) patients after three months). Thus, relatively more patients become negative in comparison to patients that develop a positive MRI. To visualise the amount of BME, cumulative probability plots for each of the readers, of baseline and 1 year-sparcc-scores in which patients were grouped according to either positivity or negativity according to the ASAS-definition are given in figure 1 in the supplementary file. With special interest, we reviewed the patients with a change in MRI-SI-ASAS status; their disease characteristics are depicted in table 4. Three of the five patients that turned ASAS MRI-positive after three months (table 4, orange cells) were male (60%) and three patients (60%) were HLA-B27 positive. One patient had sacroiliitis on radiographs (mny-criteria) at baseline. After three months, two patients developed a new SpA-feature, namely good response on NSAIDs. One patient used NSAIDs on baseline, whilst three (60%) after three months. All three patients with an initial positive MRI according to the ASAS definition that turned negative (table 4, blue cells) were on NSAID treatment from baseline, were men and HLA-B27 positive. Of the 10 newly MRI-SI positive patients at one-year follow-up (table 4, green cells) 5 patients were male (50%) and the majority (n=8, 80%) was HLA-B27 positive. Sacroiliitis on radiographs (mny criteria at baseline) was present in 30% of the patients (3/10). Two patients developed new SpA-feature(s) over one-year time, which were not yet present at baseline (patient 10: good response on NSAIDs, patient 16: good response on NSAIDs, inflammatory back pain and dactylitis). All 10 patients used NSAIDs after one-year follow-up (50% at baseline) and there were no patients on anti-tnf treatment in this group. Of the 11 patients that started with a positive baseline MRI, which became negative at one year (table 4, red cells), the majority was male (n=7, 64%) and HLA-B27 (n=8, 73%) and developed new SpA features (n=6, 55%). Four patients had started anti-tnf therapy and one patient started an NSAID.
9 SPARCC scores are depicted in the last column of table 4. Overall, when comparing SPARCC scores between the two different readers, only modest differences are seen, which implies a high level of agreement. Reviewing patients becoming newly ASAS positive (after three months or one year: table 4, orange and green cells), half of the patients become marginally positive in terms of SPARCC scores whilst other patients become evidently positive with a marked raise in SPARCC scores up to 18. After one year, patients that were initially ASAS positive but became negative over time (table 4, red cells) had mostly low SPARCC scores except those that have been treated (patients were treated according to clinical practice). Four patients were on anti-tnf therapy which showed an important decrease in SPARCCscores at one-year follow-up. Factors determining a positive MRI According to the GEE analysis, both HLA-B27 positivity (OR: 2.36, 95% CI: , p=0.029) and male gender (OR: 5.63, 95% CI: , p<0.001) independently determined the likelihood of a positive MRI at any time point. Figure 1 displays the effects of HLA-B27 and sex in an absolute manner. The likelihood of a positive MRI in HLA-B27 negative women with CBP is only 7%, whereas in HLA-B27 positive men this is 43.0% (HLA-B27 positive women: 6%, HLA-B27 negative men: 14%). In men, HLA- B27 positivity or -negativity has a significant effect on the likelihood of having a positive MRI at any time point (OR: 4.54, 95% CI: , p=0.008) whereas this effect was not present in women (OR: 0.84, 95% CI: , p=0.800). Influences of CRP were investigated in all models, but correcting for CRP had only very minor influence. Therefore, data uncorrected for CRP are shown. Only minor differences were seen between patients with CBP and IBP according to the ASAS definition (data not shown). Likelihood of a positive MRI during follow-up The likelihood of finding a positive MRI at 3 months or 1 year according to the baseline MRI status (either positive or negative) was considered. Both HLA-B27 status (OR: 2.41, 95% CI: , p=0.067) and MRI baseline status (OR: 43.89, 95% CI: , p<0.001) were independently contributory to a positive MRI at follow-up. This analysis was repeated with sex instead of HLA-B27 status: both sex (OR: 2.54, 95% CI: , p=0.048) and MRI
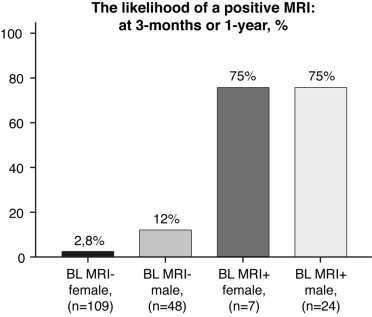
10 baseline status (OR: 36.04, 95% CI: , p<0.001) appeared to be independently contributory to a positive MRI over time. Again, only minor changes were seen between CBP and IBP patients, not reaching significance (data not shown). In figure 2, the likelihood of a positive MRI in relation to baseline MRI and HLA-B27 status (a) and sex (b) is visualized. In an HLA-B27 negative patient with a negative baseline MRI, the likelihood of a positive MRI at follow-up is negligible (1.5%). On the contrary, in an HLA-B27 positive patient with a positive baseline MRI-SI, the likelihood is rather high: 73%. In patients with a positive MRI on baseline, HLA-B27 status does not influence the likelihood of a positive MRI at any follow-up time point (OR: 0.65, 95% CI: , p=0.582). However, in MRI baseline negative patients, HLA-B27 positivity or negativity has a significant effect on the likelihood of a positive MRI at follow-up (OR: 8.12, 95% CI: , p=0.010). For sex, in a male or female patient with a positive baseline MRI the likelihood of having a positive MRI at 3 months or 1 year follow-up is 75%, whereas it is only 2.8% in a female patient with a negative baseline MRI and 12% in a male patient with a negative MRI at baseline. In patients with a negative baseline MRI, there is a significant effect of sex (OR: 4.67, 95% CI: , p=0.01) while this is absent in patients with a positive MRI on baseline (OR: 0.96, 95% CI: , p=0.959). As an example, MRI-SIs of patients with an ASAS status change over 1 year time are depicted in figure 2 in the supplementary file: two patients being MRI-SI ASAS positive at baseline, but negative after 1 year (Figure 2a, supplementary file) and two patients being MRI-SI ASAS negative at baseline, but positive after 1 year (Figure 2b, supplementary file). Discussion: In this study of patients with chronic back pain suspicious for axial SpA, 83.5% of the patients (157/188) had a negative MRI at baseline. Of these patients, only (12/157) 7.6 % had a positive MRI at any follow-up time point. Twelve of the 31 patients (38.7% ) with a positive MRI at baseline had a negative MRI at any follow-up time point. Although changes are visible in both directions, relatively more patients become negative (4.3% after three months and 7.2% after one year) than positive (11.1% after 3 months and 37.9% after one
11 year). Nevertheless, it is important to realise that 36% of the patients that became negative after one year started anti-tnf therapy, which is known to decrease inflammation in the sacroiliac joints visible on MRI (16). This study showed that MRI status at baseline appeared to be strongly influencing the chance of having a positive MRI of the sacroiliac joints at follow-up. If the baseline MRI is positive, the likelihood that the MRI will be positive again at three months or one year is very high (75%). The usefulness of repeating a negative MRI in terms of diagnostic yield is low, but there are different risks related to sex and HLA-B27 status. In baseline MRI negative patients, HLA-B27 status has a significant effect on the likelihood of a positive MRI at follow-up. In HLA-B27 negative patients with a negative MRI at baseline, sacroiliitis at follow-up can be excluded with a high level of confidence. The likelihood of a positive MRI at follow-up is only 1.5%. In HLA-B27 positive patients with a negative MRI at baseline, the likelihood of a positive MRI at three months or one year is still low, though somewhat higher (namely 11%). Of course, we can debate on the clinical relevance of this small difference in terms of percentage and, in general, chances of MRI positivity at followup are very low when the baseline MRI is negative. But, if a clinical suspicion about the diagnosis axial spondyloarthritis remains (for example a patient develops other SpA features) it might be worthwhile to consider re-doing an MRI in HLA-B27 positive patients. Likewise, there is a statistically significant difference between male and female patients with a negative baseline MRI, namely that in male patients more often a positive MRI at followup is seen (difference: 12% in men, 3% in women). Of course, interpretation of MRI findings should always be determined in the context of all clinical, laboratory and other imaging parameters available, for example other SpA-features that enhance diagnostic confidence. Also, other findings on MRI (for example the presence of structural lesions) can be supportive in the diagnostic process. However, in this group of patients with short symptom duration, the frequency of structural changes in SI-joints is relatively low and only discriminates between patients with and without axial SpA if at least 5 structural lesions (especially erosions and fatty lesions) are present. (11) This indicates that at this phase of the disease, BME is the most important feature.
12 Van Onna et al. performed a two-year follow-up study (22), which observed MRI status changes in 15% of the patients with recent-onset inflammatory back pain (IBP) that can be seen as relatively similar to our data, although follow-up time is considerably shorter in our study. On the other hand, in our study substantially more patients are included and two validated scoring methods are used. Like in our study, in the study by van Onna et al. relatively more patients became negative in comparison to patients that developed a positive MRI over time: 30% became negative (while positive at baseline) and 15% became positive (while negative at baseline) at one or two years follow-up. They also found that male gender and HLA-B27 positivity were predictive of a positive MRI-SI at follow up. In our study too, male gender and HLA-B27 positivity determined independently the likelihood of a positive MRI at any time point. HLA-B27 positive male patients with chronic back pain, have the highest chance of a positive MRI at any time. Other studies have investigated the natural history of MRI-determined BME in individuals with suspected axspa as well. Sengupta et al. concluded that in patients fulfilling the ASAS IBP criteria repeat MRI scans within a 12-week period should only be considered in HLA-B27 positive males; since there were no HLA-B27- negative patients changed from MRI-negative to positive in this study. Although this was a considerably smaller group of patients, data are in line with our findings that HLA-B27 positivity determines the likelihood of a positive MRI (23). Marzo-Ortega et al. also reported a higher chance of a positive MRI at one year in early, untreated IBP patients being HLA-B27 positive (24). Regarding sex differences, historically ankylosing spondylitis (AS) was considered as a predominantly male disease, but it has been reported that 46% of the patients diagnosed since 1990 were female compared to 10% in 1960 (25). This suggests that the male predominance in AS and axspa may be (at least in part) induced by missing the diagnosis of AS among women in earlier times and more data become available that the percentage female patients with non-radiographic axial SpA and AS is substantial. Another reason for the higher male/female ratio in AS may be that men develop more often radiographic sacroiliitis compared to females. This is also in line with our findings that male patients are more likely to have a positive MRI at any time point, as a positive MRI is a predictor of development of radiographic sacroiliitis (9).
13 Another issue is timing: when to re-do an MRI in case of persistent axspa suspicion and after what period of follow-up. With this study, we looked at both three months and oneyear follow-up, and at both time points the additional value is very limited. Given the low diagnostic yield, taking costs and feasibility into account, repeating an MRI after 3 months or 1 year should not be performed routinely. Two-year data on the SPACE cohort will become available in the future, which will provide information on a longer interval. In general, MRI has become an important tool in the evaluation of patients with axspa and relevant improvements in the field have taken place: such as the standardization of imaging protocols, and the development and validation of standardized descriptions of lesions. These lesions include not only inflammatory lesions, but also structural lesions: by means of fatty lesions, erosions, sclerosis and ankylosis. MRI has the unique potential of visualizing both inflammatory and structural lesions by means of one imaging technique and it is hypothesized that structural lesions could enhance sensitivity and/or specificity which could be helpful when in diagnostic doubts. Research on the incremental value of structural lesions is ongoing. Looking at methodological aspects, the fact that we have repeated MRI in all patients irrespective of the diagnosis is an important strength of our study compared to studies doing this in a selected population of patients. Moreover, the follow-up is quite complete avoiding unintentional bias in leaving out patients with a low likelihood of axial SpA. Another strength of our study is our scoring process with two readers with adjudication in case of discrepancy, which adds to the credibility of the findings. Moreover, the fact that we used two well-validated scoring methods (ASAS and SPARCC) provides additional insight. On the other hand, limitations of the current study are the limited duration of follow-up and the fact that we could not compare these findings with an external standard. Diagnosis is influenced by MRI findings and would lead to circular reasoning. Moreover, we lack another imaging technique like low-dose CT or histology. Prospective evaluation over a sufficient time frame with a longer follow-up should enhance confidence in the diagnosis of this sometimes slowly evolving disease.
14 In conclusion, MRI-SI ASAS status changes are seen in a minority of the patients of the SPACE cohort and both changes from negative to positive and from positive to negative occur. Especially a very small percentage of patients become positive (4.3% and 7.2% after three months and one year, respectively), which indicates that the usefulness of repeating an MRI-SI in the diagnostic process after three months or one year is very limited. Relatively more patients become negative (37.9% after one year) and one should realize that resolution of inflammation is partly induced by the use of anti-tnf therapy. Male gender and HLA-B27 positivity determine independently the likelihood of a positive MRI at any time point, while MRI-SI status at baseline strongly predicts MRI-SI status at follow-up. Reference List (1) van den Berg R, de Hooge M., Rudwaleit M, Sieper J, van GF, Reijnierse M, et al. ASAS modification of the Berlin algorithm for diagnosing axial spondyloarthritis: results from the SPondyloArthritis Caught Early (SPACE)-cohort and from the Assessment of SpondyloArthritis international Society (ASAS)-cohort. Ann Rheum Dis 2013; 72(10): (2) Feldtkeller E, Bruckel J, Khan MA. Scientific contributions of ankylosing spondylitis patient advocacy groups. Curr Opin Rheumatol 2000; 12(4): (3) Rudwaleit M, Khan MA, Sieper J. The challenge of diagnosis and classification in early ankylosing spondylitis: do we need new criteria? Arthritis Rheum 2005; 52(4): (4) Kroon FP, van der Burg LR, Ramiro S, Landewe RB, Buchbinder R, Falzon L, et al. Nonsteroidal Antiinflammatory Drugs for Axial Spondyloarthritis: A Cochrane Review. J Rheumatol 2016; 43(3): (5) van der Heijde D, Ramiro S, Landewe R, Baraliakos X, Van den Bosch F, Sepriano A, et al update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann Rheum Dis 2017; 76(6): (6) Smolen JS, Schols M, Braun J, Dougados M, FitzGerald O, Gladman DD, et al. Treating axial spondyloarthritis and peripheral spondyloarthritis, especially psoriatic arthritis, to target: 2017 update of recommendations by an international task force. Ann Rheum Dis (7) Lambert RG, Bakker PA, van der Heijde D, Weber U, Rudwaleit M, Hermann KG, et al. Defining active sacroiliitis on MRI for classification of axial spondyloarthritis: update by the ASAS MRI working group. Ann Rheum Dis 2016; 75(11): (8) Oostveen J, Prevo R, den Boer J., van de Laar M. Early detection of sacroiliitis on magnetic resonance imaging and subsequent development of sacroiliitis on plain radiography. A prospective, longitudinal study. J Rheumatol 1999; 26(9):
15 (9) Dougados M, Sepriano A, Molto A, van Lunteren M., Ramiro S, de Hooge M., et al. Sacroiliac radiographic progression in recent onset axial spondyloarthritis: the 5-year data of the DESIR cohort. Ann Rheum Dis 2017; 76(11): (10) Weber U, Lambert RG, Pedersen SJ, Hodler J, Ostergaard M, Maksymowych WP. Assessment of structural lesions in sacroiliac joints enhances diagnostic utility of magnetic resonance imaging in early spondylarthritis. Arthritis Care Res (Hoboken) 2010; 62(12): (11) de Hooge M., van den Berg R, Navarro-Compan V, Reijnierse M, van GF, Fagerli K, et al. Patients with chronic back pain of short duration from the SPACE cohort: which MRI structural lesions in the sacroiliac joints and inflammatory and structural lesions in the spine are most specific for axial spondyloarthritis? Ann Rheum Dis 2016; 75(7): (12) Bakker PA, van den Berg R, Lenczner G, Thevenin F, Reijnierse M, Claudepierre P, et al. Can we use structural lesions seen on MRI of the sacroiliac joints reliably for the classification of patients according to the ASAS axial spondyloarthritis criteria? Data from the DESIR cohort. Ann Rheum Dis 2017; 76(2): (13) Rudwaleit M, van der Heijde D, Khan MA, Braun J, Sieper J. How to diagnose axial spondyloarthritis early. Ann Rheum Dis 2004; 63(5): (14) Mandl P, Navarro-Compan V, Terslev L, Aegerter P, van der Heijde D, D'Agostino MA, et al. EULAR recommendations for the use of imaging in the diagnosis and management of spondyloarthritis in clinical practice. Ann Rheum Dis 2015; 74(7): (15) Pedersen SJ, Poddubnyy D, Sorensen IJ, Loft AG, Hindrup JS, Thamsborg G, et al. Course of Magnetic Resonance Imaging-Detected Inflammation and Structural Lesions in the Sacroiliac Joints of Patients in the Randomized, Double-Blind, Placebo-Controlled Danish Multicenter Study of Adalimumab in Spondyloarthritis, as Assessed by the Berlin and Spondyloarthritis Research Consortium of Canada Methods. Arthritis Rheumatol 2016; 68(2): (16) Maksymowych WP, Dougados M, van der Heijde D, Sieper J, Braun J, Citera G, et al. Clinical and MRI responses to etanercept in early non-radiographic axial spondyloarthritis: 48-week results from the EMBARK study. Ann Rheum Dis 2016; 75(7): (17) van den Berg R, de Hooge M., van GF, Reijnierse M, Huizinga T, van der Heijde D. Percentage of patients with spondyloarthritis in patients referred because of chronic back pain and performance of classification criteria: experience from the Spondyloarthritis Caught Early (SPACE) cohort. Rheumatology (Oxford) 2013; 52(8): (18) Rudwaleit M, Jurik AG, Hermann KG, Landewe R, van der Heijde D, Baraliakos X, et al. Defining active sacroiliitis on magnetic resonance imaging (MRI) for classification of axial spondyloarthritis: a consensual approach by the ASAS/OMERACT MRI group. Ann Rheum Dis 2009; 68(10): (19) van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum 1984; 27(4): (20) Maksymowych WP, Inman RD, Salonen D, Dhillon SS, Williams M, Stone M, et al. Spondyloarthritis research Consortium of Canada magnetic resonance imaging index for assessment of sacroiliac joint inflammation in ankylosing spondylitis. Arthritis Rheum 2005; 53(5):703-9.
16 (21) P.Mean: Calculating predicted probabilities from a logistic regression model (created ). www pmean com/13/predicted html [ 2013 Available from: URL: (22) van Onna M., Jurik AG, van der Heijde D, van Tubergen A., Heuft-Dorenbosch L, Landewe R. HLA-B27 and gender independently determine the likelihood of a positive MRI of the sacroiliac joints in patients with early inflammatory back pain: a 2-year MRI follow-up study. Ann Rheum Dis 2011; 70(11): (23) Sengupta R, Marzo-Ortega H, McGonagle D, Wadeley A, Bennett AN. Short-term Repeat Magnetic Resonance Imaging Scans in Suspected Early Axial Spondyloarthritis Are Clinically Relevant Only in HLA-B27-positive Male Subjects. J Rheumatol 2018; 45(2): (24) Marzo-Ortega H, McGonagle D, O'Connor P, Hensor EM, Bennett AN, Green MJ, et al. Baseline and 1-year magnetic resonance imaging of the sacroiliac joint and lumbar spine in very early inflammatory back pain. Relationship between symptoms, HLA-B27 and disease extent and persistence. Ann Rheum Dis 2009; 68(11): (25) Stolwijk C, van Onna M., Boonen A, van TA. Global Prevalence of Spondyloarthritis: A Systematic Review and Meta-Regression Analysis. Arthritis Care Res (Hoboken) 2016; 68(9):
17 Table 1: Baseline characteristics Total number (n=188) Age (years) at inclusion, mean (SD) 31.0 (8.2) Male, n (%) 72 (38.3%) Symptom duration (months) at first visit, mean (SD) 13.2 (7.1) Good response to NSAIDs, n (%) 76 (41.3%) IBP, n (%) 139 (74.3%) Positive family history SpA, n (%) 96 (51.3%) Peripheral arthritis, n (%) 34 (18.2%) Dactylitis, n (%) 15 (8.0%) Enthesitis, n (%) 41 (21.9%) Uveitis, n (%) 16 (8.6%) IBD, n (%) 17 (9.1%) Psoriasis, n (%) 25 (13.4%) Elevated CRP, n (%) 35 (18.9%) HLA-B27 positive, n (%) 91 (48.4%) Sacroiliitis present on radiograph, n (%) 19 (11.1%) Positive MRI (ASAS definition), n (%) 31 (16.5%) Diagnosis axspa according to rheumatologist, n (%)* 74 (39.6%) ASAS, Assessment of SpondyloArthritis; axspa, axial spondyloarthritis; CRP, C-reactive protein; HLA-B27, human leukocyte antigen-b27; IBD, inflammatory bowel disease; IBP, inflammatory back pain; MRI, magnetic resonance imaging; NSAIDs, non-steroidal anti-inflammatory drugs; SD, standard deviation; *Confidence level 7 (NRS 0-10)
18 Table 2: Course of MRI-SI ASAS positivity over one-year time: Patients with MRI-SI available at baseline & 3 months & 1 year (a) Patients with MRI-SI available at baseline & 3 months (b) Patients with MRI-SI available at baseline & 1 year (c) *0=MRI ASAS negative; 1 = MRI ASAS positive MRI-SI ASAS definition over Number of patients time Total Total Total 45 Cases with all three time points available (a), cases with baseline & 3 months available (b) and cases with 3 months & 1 year available (c)
19 Table 3: Changes in MRI-SI ASAS positivity over three months and one-year time MRI 3 months ASAS positive MRI 3 months ASAS negative Total MRI baseline positive MRI baseline negative Total MRI 1 year ASAS positive MRI 1 year ASAS negative Total MRI baseline positive MRI baseline negative Total
20 ccepted Article Table 4: Disease characteristics of patients with a change in MRI-SI-ASAS status over 3 months and 1 year mny + HLA-B27 Age Sex + SpA-features* CRP ASDAS Medication SPARCC score reader 1 - reader 2 Baseline 3 months Baseline 3 months Baseline 3 months Baseline 3 months Baseline 3 months 1 1 Positive 19 M 1, 2 Idem /0 5/6 2 0 Negative 38 F 1, 3 Idem NSAID NSAID 1/1 2/2 3 0 Positive 25 M 2, 8 Idem NSAID 0/0 10/7 4 0 Negative 29 F 1 Idem /0 9/ Positive 26 M 1, 2 Idem NSAID 0/0 5/5 6 1 Positive 21 M 1, 9 Idem NSAD NSAID 3/5 0/3 7 0 Positive 32 M 1, 6, 9 Idem NSAID NSAID 2/4 0/0 8 0 Positive 31 M 1, 6, 8, 9 Idem NSAID NSAID 2/2 0/0 mny + SPARCC-score HLA-B27 Age Sex + SpA-features* CRP ASDAS Medication reader 1 reader 2 Baseline 1 year Baseline 1 year Baseline 1 year Baseline 1 year Baseline 1 year 9 0 Positive 21 F 1, 2, 5, 9 Idem NSAID NSAID 0/0 4/ Positive 33 M 1, 4 Idem NSAID 0/0 5/ Positive 19 M 1, 2 Idem NSAID 0/0 16/ Positive 31 M 1,2 Idem NSAID NSAID 0/2 2/ Positive 32 M 1 Idem NSAID NSAID 0/0 3/ Positive 19 F 2 Idem NSAID NSAID 0/0 2/ Negative 32 F 1, 2, 6, 9 Idem NSAID NSAID 1/0 5/ Positive 25 M 2, 8 Idem + 1, 7, NSAID 0/0 10/ Positive 35 F 9 Idem NSAID 1/0 14/ Negative 29 F 1 Idem NSAID 0/0 13/ Negative 43 F 1, 6 Idem /2 0/ Positive 29 F 1 Idem NSAID NSAID +anti-tnf 14/14 0/ Positive 31 M 1, 6, 8, 9 Idem NSAID NSAID 2/2 0/ Negative 40 F 1 Idem + 4, Anti-TNF 8/8 0/ Positive 22 M - 1, 2, NSAID NSAID 9/13 1/ Positive 32 M 1, 6, 9 Idem NSAID NSAID 2/4 0/ Positive 33 M 1, 8, 9 Idem NSAID Anti-TNF 7/5 0/ Negative 46 M 1, 9 Idem NSAID NSAID 4/2 1/0
21 ccepted Article 27 1 Positive 24 F 2, 5, 6 Idem + 1, NSAID NSAID +anti-tnf 46/44 0/ Positive 42 M 6, 9 Idem NSAID NSAID 10/9 0/ Positive 26 M 1, 2 Idem NSAID 18/16 2/0 * 1=IBP; 2=positive family history; 3=uveitis; 4=IBD; 5=psoriasis; 6=enthesitis; 7=dactylitis; 8=peripheral arthritis; 9=NSAID resp. + mny status and age at baseline Orange cells: reflect patients in which a negative MRI-SI at baseline turned positive after 3 months follow-up Blue cells: reflect patients in which a positive MRI-SI at baseline turned negative after 3 months follow-up Green cells: reflect patients in which a negative MRI-SI at baseline turned positive after 1 year follow-up Red cells: reflect patients in which a positive MRI-SI at baseline turned negative after 1 year follow-up
22 Figure 1: Likelihood of a positive MRI at any time point in CBP patients investigated at baseline, 3 months and 1-year follow-up in the subgroups of patients according to HLA- B27 status and gender. Figure 2: Likelihood of a positive MRI at three months or 1-year follow-up in CBP patients, in the subgroups of patients according to the result of the baseline MRI (negative or positive) and HLA-B27 status or sex.
23
24
ARD Online First, published on October 11, 2005 as /ard
 ARD Online First, published on October 11, 2005 as 10.1136/ard.2005.044206 Combining information obtained from MRI and conventional radiographs in order to detect sacroiliitis in patients with recent-onset
ARD Online First, published on October 11, 2005 as 10.1136/ard.2005.044206 Combining information obtained from MRI and conventional radiographs in order to detect sacroiliitis in patients with recent-onset
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/29572 holds various files of this Leiden University dissertation. Author: Berg, Rosaline van den Title: Spondyloarthritis : recognition, imaging, treatment
Cover Page The handle http://hdl.handle.net/1887/29572 holds various files of this Leiden University dissertation. Author: Berg, Rosaline van den Title: Spondyloarthritis : recognition, imaging, treatment
Department of Radiology, Aarhus University Hospital, Aarhus, Denmark; 4. Key words MRI, sacroiliitis, ankylosing spondylitis, axial spondyloarthritis.
 Gadolinium contrast-enhanced MRI sequence does not have an incremental value in the assessment of sacroiliitis in patients with early inflammatory back pain by using MRI in combination with pelvic radiographs:
Gadolinium contrast-enhanced MRI sequence does not have an incremental value in the assessment of sacroiliitis in patients with early inflammatory back pain by using MRI in combination with pelvic radiographs:
Diakonhjemmet Hospital, Oslo, Norway;
 ARTHRITIS & RHEUMATOLOGY Vol. 70, No. 7, July 2018, pp 1042 1048 DOI 10.1002/art.40475 2018 The Authors. Arthritis & Rheumatology published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
ARTHRITIS & RHEUMATOLOGY Vol. 70, No. 7, July 2018, pp 1042 1048 DOI 10.1002/art.40475 2018 The Authors. Arthritis & Rheumatology published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Introduction SCIENTIFIC ARTICLE
 Skeletal Radiol (2017) 46:633 639 DOI 10.1007/s00256-017-2581-1 SCIENTIFIC ARTICLE Prevalence and clinical significance of lumbosacral transitional vertebra (LSTV) in a young back pain population with
Skeletal Radiol (2017) 46:633 639 DOI 10.1007/s00256-017-2581-1 SCIENTIFIC ARTICLE Prevalence and clinical significance of lumbosacral transitional vertebra (LSTV) in a young back pain population with
Imaging of axial spondyloarthritis including ankylosing spondylitis
 Imaging of axial spondyloarthritis including ankylosing spondylitis ACR 2012 Prof. Dr. med. J. Braun Rheumazentrum Ruhrgebiet, Herne Ruhr-Universität Bochum Germany Modified New York Criteria 1984 for
Imaging of axial spondyloarthritis including ankylosing spondylitis ACR 2012 Prof. Dr. med. J. Braun Rheumazentrum Ruhrgebiet, Herne Ruhr-Universität Bochum Germany Modified New York Criteria 1984 for
Progression of Nonradiographic Axial Spondyloarthritis to Ankylosing Spondylitis
 ARTHRITIS & RHEUMATOLOGY Vol. 68, No. 6, June 2016, pp 1415 1421 DOI 10.1002/art.39542 VC 2016, American College of Rheumatology Progression of Nonradiographic Axial Spondyloarthritis to Ankylosing Spondylitis
ARTHRITIS & RHEUMATOLOGY Vol. 68, No. 6, June 2016, pp 1415 1421 DOI 10.1002/art.39542 VC 2016, American College of Rheumatology Progression of Nonradiographic Axial Spondyloarthritis to Ankylosing Spondylitis
SpA non-radiografica: fase precoce di spondilite anchilosante o altro?
 Rheumatology Department of Lucania, S. Carlo Hospital of Potenza and Madonna delle Grazie Hospital of Matera SpA non-radiografica: fase precoce di spondilite anchilosante o altro? Ignazio Olivieri Disclosures
Rheumatology Department of Lucania, S. Carlo Hospital of Potenza and Madonna delle Grazie Hospital of Matera SpA non-radiografica: fase precoce di spondilite anchilosante o altro? Ignazio Olivieri Disclosures
2016 update of the ASAS/EULAR recommendations for the management of axial spondyloarthritis. Online supplementary material
 2016 update of the ASAS/EULAR recommendations for the management of axial spondyloarthritis Online supplementary material 1. Introduction A systematic literature review (SLR) was performed to inform the
2016 update of the ASAS/EULAR recommendations for the management of axial spondyloarthritis Online supplementary material 1. Introduction A systematic literature review (SLR) was performed to inform the
Are gender-specific approaches needed in diagnosing early axial spondyloarthritis? Data from the SPondyloArthritis Caught Early cohort
 Ortolan et al. Arthritis Research & Therapy (2018) 20:218 https://doi.org/10.1186/s13075-018-1705-x RESEARCH ARTICLE Are gender-specific approaches needed in diagnosing early axial spondyloarthritis? Data
Ortolan et al. Arthritis Research & Therapy (2018) 20:218 https://doi.org/10.1186/s13075-018-1705-x RESEARCH ARTICLE Are gender-specific approaches needed in diagnosing early axial spondyloarthritis? Data
Do HLA-B27 positive patients differ from HLA-B27 negative patients in clinical presentation
 Do HLA-B27 positive patients differ from HLA-B27 negative patients in clinical presentation and imaging? Results from the DESIR cohort of patients with recent onset axial spondyloarthritis Ho Yin Chung
Do HLA-B27 positive patients differ from HLA-B27 negative patients in clinical presentation and imaging? Results from the DESIR cohort of patients with recent onset axial spondyloarthritis Ho Yin Chung
NIH Public Access Author Manuscript Curr Opin Rheumatol. Author manuscript; available in PMC 2011 January 20.
 NIH Public Access Author Manuscript Published in final edited form as: Curr Opin Rheumatol. 2010 September ; 22(5): 603 607. doi:10.1097/bor.0b013e32833c7255. Early axial spondyloarthritis Robert A Colbert
NIH Public Access Author Manuscript Published in final edited form as: Curr Opin Rheumatol. 2010 September ; 22(5): 603 607. doi:10.1097/bor.0b013e32833c7255. Early axial spondyloarthritis Robert A Colbert
Evaluation of multiple referral strategies for axial spondyloarthritis in the SPondyloArthritis Caught Early (SPACE) cohort
 cohort") To cite: Abawi O, van den Berg R, van der Heijde D, et al. Evaluation of multiple referral strategies for axial spondyloarthritis in the SPondyloArthritis Caught Early (SPACE) cohort. RMD Open 2017;3:e000389.
To cite: Abawi O, van den Berg R, van der Heijde D, et al. Evaluation of multiple referral strategies for axial spondyloarthritis in the SPondyloArthritis Caught Early (SPACE) cohort. RMD Open 2017;3:e000389.
What is Axial Spondyloarthritis?
 Physiotherapist Module 2 What is Axial Spondyloarthritis? How does it apply to physiotherapists? Claire Harris, Senior Physiotherapist, London North West Healthcare NHS Trust Susan Gurden, Advanced Physiotherapy
Physiotherapist Module 2 What is Axial Spondyloarthritis? How does it apply to physiotherapists? Claire Harris, Senior Physiotherapist, London North West Healthcare NHS Trust Susan Gurden, Advanced Physiotherapy
Current Concept of Spondyloarthritis: Special Emphasis on Early Referral and Diagnosis
 DOI 10.1007/s11926-012-0274-2 SERONEGATIVE ARTHRITIS (MA KHAN, SECTION EDITOR) Current Concept of Spondyloarthritis: Special Emphasis on Early Referral and Diagnosis Salih Ozgocmen & Muhammad Asim Khan
DOI 10.1007/s11926-012-0274-2 SERONEGATIVE ARTHRITIS (MA KHAN, SECTION EDITOR) Current Concept of Spondyloarthritis: Special Emphasis on Early Referral and Diagnosis Salih Ozgocmen & Muhammad Asim Khan
Ankylosing spondylitis: Assessment and analysis of long-term outcome Ramiro, S.
 UvA-DARE (Digital Academic Repository) Ankylosing spondylitis: Assessment and analysis of long-term outcome Ramiro, S. Link to publication Citation for published version (APA): Antunes da Cunha Oliveira
UvA-DARE (Digital Academic Repository) Ankylosing spondylitis: Assessment and analysis of long-term outcome Ramiro, S. Link to publication Citation for published version (APA): Antunes da Cunha Oliveira
T he spondyloarthritides (SpA) comprise five subtypes:
 comprise five subtypes:") 1305 EXTENDED REPORT Magnetic resonance imaging of the spine and the sacroiliac joints in ankylosing spondylitis and undifferentiated spondyloarthritis during treatment with etanercept M Rudwaleit*, X
1305 EXTENDED REPORT Magnetic resonance imaging of the spine and the sacroiliac joints in ankylosing spondylitis and undifferentiated spondyloarthritis during treatment with etanercept M Rudwaleit*, X
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Secukinumab for treating ankylosing spondylitis after inadequate response to non-steroidal anti-inflammatory drugs
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Secukinumab for treating ankylosing spondylitis after inadequate response to non-steroidal anti-inflammatory drugs
Axial Spondyloarthritis: Issues & Controversies
 Axial Spondyloarthritis: Issues & Controversies Atul Deodhar, MD Professor of Medicine Oregon Health & Science University Portland, OR WRA 2018 Annual Meeting, Leavenworth, WA. 16 th September, 2018 Disclosures:
Axial Spondyloarthritis: Issues & Controversies Atul Deodhar, MD Professor of Medicine Oregon Health & Science University Portland, OR WRA 2018 Annual Meeting, Leavenworth, WA. 16 th September, 2018 Disclosures:
van der Heijde et al. Arthritis Research & Therapy (2018) 20:61 https://doi.org/ /s
 20:61 https://doi.org/ /s") van der Heijde et al. Arthritis Research & Therapy (2018) 20:61 https://doi.org/10.1186/s13075-018-1556-5 RESEARCH ARTICLE Clinical and MRI remission in patients with nonradiographic axial spondyloarthritis
van der Heijde et al. Arthritis Research & Therapy (2018) 20:61 https://doi.org/10.1186/s13075-018-1556-5 RESEARCH ARTICLE Clinical and MRI remission in patients with nonradiographic axial spondyloarthritis
Anti-CD74 antibodies have no diagnostic value in early axial spondyloarthritis: data from the spondyloarthritis caught early (SPACE) cohort
 cohort") de Winter et al. Arthritis Research & Therapy (2018) 20:38 https://doi.org/10.1186/s13075-018-1535-x RESEARCH ARTICLE Open Access Anti-CD74 antibodies have no diagnostic value in early axial spondyloarthritis:
de Winter et al. Arthritis Research & Therapy (2018) 20:38 https://doi.org/10.1186/s13075-018-1535-x RESEARCH ARTICLE Open Access Anti-CD74 antibodies have no diagnostic value in early axial spondyloarthritis:
Axial Spondyloarthritis. Doug White, Rheumatologist Waikato Hospital
 Axial Spondyloarthritis Doug White, Rheumatologist Waikato Hospital Disclosures Presentations / Consulting Abbott Laboratories AbbVie MSD Novartis Roche Clinical Trials Abbott Laboratories AbbVie Actelion
Axial Spondyloarthritis Doug White, Rheumatologist Waikato Hospital Disclosures Presentations / Consulting Abbott Laboratories AbbVie MSD Novartis Roche Clinical Trials Abbott Laboratories AbbVie Actelion
Clinical and spinal radiographic outcome in axial spondyloarthritis Maas, Fiona
 University of Groningen Clinical and spinal radiographic outcome in axial spondyloarthritis Maas, Fiona IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen Clinical and spinal radiographic outcome in axial spondyloarthritis Maas, Fiona IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/43590 holds various files of this Leiden University dissertation Author: Machado, Pedro Title: Health and imaging outcomes in axial spondyloarthritis Issue
Cover Page The handle http://hdl.handle.net/1887/43590 holds various files of this Leiden University dissertation Author: Machado, Pedro Title: Health and imaging outcomes in axial spondyloarthritis Issue
Maksymowych et al. Arthritis Research & Therapy (2017) 19:126 DOI /s
 19:126 DOI /s") Maksymowych et al. Arthritis Research & Therapy (2017) 19:126 DOI 10.1186/s13075-017-1342-9 RESEARCH ARTICLE Open Access MRI evidence of structural changes in the sacroiliac joints of patients with nonradiographic
Maksymowych et al. Arthritis Research & Therapy (2017) 19:126 DOI 10.1186/s13075-017-1342-9 RESEARCH ARTICLE Open Access MRI evidence of structural changes in the sacroiliac joints of patients with nonradiographic
Feasibility and reliability of the Spondyloarthritis Research Consortium of Canada sacroiliac joint inflammation score in children
 Weiss et al. Arthritis Research & Therapy (2018) 20:56 https://doi.org/10.1186/s13075-018-1543-x RESEARCH ARTICLE Feasibility and reliability of the Spondyloarthritis Research Consortium of Canada sacroiliac
Weiss et al. Arthritis Research & Therapy (2018) 20:56 https://doi.org/10.1186/s13075-018-1543-x RESEARCH ARTICLE Feasibility and reliability of the Spondyloarthritis Research Consortium of Canada sacroiliac
Nonradiographic axial spondyloarthritis: clinical and therapeutic relevance
 Ghosh and Ruderman Arthritis Research & Therapy (2017) 19:286 DOI 10.1186/s13075-017-1493-8 REVIEW Nonradiographic axial spondyloarthritis: clinical and therapeutic relevance Nilasha Ghosh and Eric M.
Ghosh and Ruderman Arthritis Research & Therapy (2017) 19:286 DOI 10.1186/s13075-017-1493-8 REVIEW Nonradiographic axial spondyloarthritis: clinical and therapeutic relevance Nilasha Ghosh and Eric M.
Chapter 2. Overview of ankylosing spondylitis
 Chapter 2 Overview of ankylosing spondylitis The concept and classification of spondyloarthritis The term spondyloarthritis (SpA) comprises AS, reactive arthritis, arthritis/spondylitis associated with
Chapter 2 Overview of ankylosing spondylitis The concept and classification of spondyloarthritis The term spondyloarthritis (SpA) comprises AS, reactive arthritis, arthritis/spondylitis associated with
Radiographic sacroiliitis develops predictably over time in a cohort of familial spondyloarthritis followed longitudinally
 RHEUMATOLOGY Rheumatology 2017;56:811 817 doi:10.1093/rheumatology/kew496 Advance Access publication 4 February 2017 Original article Radiographic sacroiliitis develops predictably over time in a cohort
RHEUMATOLOGY Rheumatology 2017;56:811 817 doi:10.1093/rheumatology/kew496 Advance Access publication 4 February 2017 Original article Radiographic sacroiliitis develops predictably over time in a cohort
Clinical and spinal radiographic outcome in axial spondyloarthritis Maas, Fiona
 University of Groningen Clinical and spinal radiographic outcome in axial spondyloarthritis Maas, Fiona IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen Clinical and spinal radiographic outcome in axial spondyloarthritis Maas, Fiona IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
Sacroiliac joints MR: Finally a universal language for the sacroiliitis diagnosis
 Sacroiliac joints MR: Finally a universal language for the sacroiliitis diagnosis Poster No.: C-1836 Congress: ECR 2013 Type: Scientific Exhibit Authors: M. E. Banegas Illescas, C. López Menéndez, M. L.
Sacroiliac joints MR: Finally a universal language for the sacroiliitis diagnosis Poster No.: C-1836 Congress: ECR 2013 Type: Scientific Exhibit Authors: M. E. Banegas Illescas, C. López Menéndez, M. L.
Imaging and intervention of sacroiliac joint. Dr Ryan Lee Ka Lok Associate Consultant Prince of Wales Hospital
 Imaging and intervention of sacroiliac joint Dr Ryan Lee Ka Lok Associate Consultant Prince of Wales Hospital Introduction 15%-25% of low back pain is related to sacroiliac joint (SIJ) pain SIJ pain is
Imaging and intervention of sacroiliac joint Dr Ryan Lee Ka Lok Associate Consultant Prince of Wales Hospital Introduction 15%-25% of low back pain is related to sacroiliac joint (SIJ) pain SIJ pain is
New developments in the diagnosis and treatment of axial spondyloarthritis
 Review: Clinical Trial Outcomes New developments in the diagnosis and treatment of axial spondyloarthritis Clin. Invest. (2013) 3(2), 153 171 Spondyloarthritis (SpA) is an umbrella term for a group of
Review: Clinical Trial Outcomes New developments in the diagnosis and treatment of axial spondyloarthritis Clin. Invest. (2013) 3(2), 153 171 Spondyloarthritis (SpA) is an umbrella term for a group of
adalimumab, 40mg/0.8mL, solution for injection (Humira ) SMC No. (858/13) AbbVie Ltd (previously part of Abbott)
 SMC No. (858/13) AbbVie Ltd (previously part of Abbott)") adalimumab, 40mg/0.8mL, solution for injection (Humira ) SMC No. (858/13) AbbVie Ltd (previously part of Abbott) 08 March 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the
adalimumab, 40mg/0.8mL, solution for injection (Humira ) SMC No. (858/13) AbbVie Ltd (previously part of Abbott) 08 March 2013 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Concept of Spondyloarthritis (SpA)
") Concept of Spondyloarthritis (SpA) Spondyloarthritis: Characteristic Parameters Used for Diagnosis I Symptoms Inflammatory back pain Imaging Lab ESR/CRP Patient s history Good response to NSAIDs Spondyloarthritis-Characteristic
Concept of Spondyloarthritis (SpA) Spondyloarthritis: Characteristic Parameters Used for Diagnosis I Symptoms Inflammatory back pain Imaging Lab ESR/CRP Patient s history Good response to NSAIDs Spondyloarthritis-Characteristic
Spine MRI in SpA What is the rheumatologist interested in? Personal use only
 Spine MRI in SpA What is the rheumatologist interested in? 4th Musculoskeletal MRI Meeting 2017: Spine MRI Ospedale Regionale di Lugano May 6th 2017 Ulrich Weber MD Consultant, King Christian 10th Hospital,
Spine MRI in SpA What is the rheumatologist interested in? 4th Musculoskeletal MRI Meeting 2017: Spine MRI Ospedale Regionale di Lugano May 6th 2017 Ulrich Weber MD Consultant, King Christian 10th Hospital,
ABSTRACT Objective: To validate and refine two sets of candidate criteria for the classification/diagnosis of axial spondyloarthritis
 1 Rheumatology, Med Klinik I, Charité, Campus Benjamin Franklin, Berlin, Germany; 2 Leiden University Medical Center, Leiden, The Netherlands; 3 Maastricht University Medical Center, Maastricht, The Netherlands;
1 Rheumatology, Med Klinik I, Charité, Campus Benjamin Franklin, Berlin, Germany; 2 Leiden University Medical Center, Leiden, The Netherlands; 3 Maastricht University Medical Center, Maastricht, The Netherlands;
Dr Tracey Kain. Associate Professor Ed Gane
 Associate Professor Ed Gane New Zealand Liver Transplant Unit Auckland Dr Tracey Kain Consultant Rheumatologist Grace Orthopaedic Centre Tauranga Hospital Tauranga 7:00-7:55 Abbvie Breakfast Session 1.
Associate Professor Ed Gane New Zealand Liver Transplant Unit Auckland Dr Tracey Kain Consultant Rheumatologist Grace Orthopaedic Centre Tauranga Hospital Tauranga 7:00-7:55 Abbvie Breakfast Session 1.
Anja Weiß 1*, In-Ho Song 2, Hildrun Haibel 2, Joachim Listing 1 and Joachim Sieper 1,2
 Weiß et al. Arthritis Research & Therapy 2014, 16:R35 RESEARCH ARTICLE Open Access Good correlation between changes in objective and subjective signs of inflammation in patients with short- but not long
Weiß et al. Arthritis Research & Therapy 2014, 16:R35 RESEARCH ARTICLE Open Access Good correlation between changes in objective and subjective signs of inflammation in patients with short- but not long
Gender differences in effectiveness of treatment in rheumatic diseases
 Gender differences in effectiveness of treatment in rheumatic diseases Irene van der Horst-Bruinsma Associate Professor Rheumatology Center of Excellence of Axial Spondyloarthritis ARC/VU University Medical
Gender differences in effectiveness of treatment in rheumatic diseases Irene van der Horst-Bruinsma Associate Professor Rheumatology Center of Excellence of Axial Spondyloarthritis ARC/VU University Medical
The evidence for whole-spine MRI in the assessment of axial spondyloarthropathy
 RHEUMATOLOGY Rheumatology 2010;49:426 432 doi:10.1093/rheumatology/kep427 Advance Access publication 11 January 2010 Review The evidence for whole-spine MRI in the assessment of axial spondyloarthropathy
RHEUMATOLOGY Rheumatology 2010;49:426 432 doi:10.1093/rheumatology/kep427 Advance Access publication 11 January 2010 Review The evidence for whole-spine MRI in the assessment of axial spondyloarthropathy
Diagnostic value of pelvic enthesitis on MRI of the sacroiliac joints in spondyloarthritis
 Eur Radiol (2014) 24:866 871 DOI 10.1007/s00330-013-3074-9 MUSCULOSKELETAL Diagnostic value of pelvic enthesitis on MRI of the sacroiliac joints in spondyloarthritis L. Jans & C. van Langenhove & L. Van
Eur Radiol (2014) 24:866 871 DOI 10.1007/s00330-013-3074-9 MUSCULOSKELETAL Diagnostic value of pelvic enthesitis on MRI of the sacroiliac joints in spondyloarthritis L. Jans & C. van Langenhove & L. Van
Clinical and spinal radiographic outcome in axial spondyloarthritis Maas, Fiona
 University of Groningen Clinical and spinal radiographic outcome in axial spondyloarthritis Maas, Fiona IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen Clinical and spinal radiographic outcome in axial spondyloarthritis Maas, Fiona IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
Golimumab, compared to placebo, significantly improved symptoms in adults with active nonradiographic
 golimumab 50mg/0.5mL solution for injection in pre-filled pen or syringe and 100mg/mL solution for injection in pre-filled pen (Simponi ) SMC No. (1124/16) Merck Sharp & Dohme Limited 8 January 2016 The
golimumab 50mg/0.5mL solution for injection in pre-filled pen or syringe and 100mg/mL solution for injection in pre-filled pen (Simponi ) SMC No. (1124/16) Merck Sharp & Dohme Limited 8 January 2016 The
Clinical and MRI responses to etanercept in early non-radiographic axial spondyloarthritis: 48-week results from the EMBARK study
 EXTENDED REPORT Clinical and MRI responses to etanercept in early non-radiographic axial spondyloarthritis: 48-week results from the EMBARK study Walter P Maksymowych, 1 Maxime Dougados, 2 Désirée van
EXTENDED REPORT Clinical and MRI responses to etanercept in early non-radiographic axial spondyloarthritis: 48-week results from the EMBARK study Walter P Maksymowych, 1 Maxime Dougados, 2 Désirée van
ABSTRACT ORIGINAL RESEARCH. Laure Tant. Nadine Delmotte. Maria Van den Enden. Valerie Gangji. Herman Mielants
 Rheumatol Ther (2017) 4:121 132 DOI 10.1007/s40744-016-0051-1 ORIGINAL RESEARCH High Prevalence of Undiagnosed Axial Spondyloarthritis in Patients with Chronic Low Back Pain Consulting Non-Rheumatologist
Rheumatol Ther (2017) 4:121 132 DOI 10.1007/s40744-016-0051-1 ORIGINAL RESEARCH High Prevalence of Undiagnosed Axial Spondyloarthritis in Patients with Chronic Low Back Pain Consulting Non-Rheumatologist
A mong the inflammatory rheumatic diseases
 659 REVIEW Early referral recommendations for ankylosing spondylitis (including pre-radiographic and radiographic forms) in primary care J Sieper, M Rudwaleit... An earlier diagnosis of ankylosing spondylitis
659 REVIEW Early referral recommendations for ankylosing spondylitis (including pre-radiographic and radiographic forms) in primary care J Sieper, M Rudwaleit... An earlier diagnosis of ankylosing spondylitis
Walter P. Maksymowych, Robert G. Lambert, L. Steven Brown and Aileen L. Pangan
 The Journal of Rheumatology Defining the Minimally Important Change for the SpondyloArthritis Research Consortium of Canada Spine and Sacroiliac Joint Magnetic Resonance Imaging Indices for Ankylosing
The Journal of Rheumatology Defining the Minimally Important Change for the SpondyloArthritis Research Consortium of Canada Spine and Sacroiliac Joint Magnetic Resonance Imaging Indices for Ankylosing
37 year old male with several year history of back pain
 37 year old male with several year history of back pain Inflammatory Low Back Pain Clues onset before the age of 40 years insidious onset, chronic (>3 months) pain morning stiffness for longer than 30
37 year old male with several year history of back pain Inflammatory Low Back Pain Clues onset before the age of 40 years insidious onset, chronic (>3 months) pain morning stiffness for longer than 30
ORIGINAL ARTICLE INTRODUCTION
 Arthritis & Rheumatism (Arthritis Care & Research) Vol. 53, No. 5, October 15, 2005, pp 703 709 DOI 10.1002/art.21445 2005, American College of Rheumatology ORIGINAL ARTICLE Spondyloarthritis Research
Arthritis & Rheumatism (Arthritis Care & Research) Vol. 53, No. 5, October 15, 2005, pp 703 709 DOI 10.1002/art.21445 2005, American College of Rheumatology ORIGINAL ARTICLE Spondyloarthritis Research
Assessing the Signs, Symptoms, and Clinical Manifestations of Axial SpA
 Physiotherapist Module 3 Assessing the Signs, Symptoms, and Clinical Manifestations of Axial SpA Enhance your patient examination skills Claire Harris, Senior Physiotherapist, London North West Healthcare
Physiotherapist Module 3 Assessing the Signs, Symptoms, and Clinical Manifestations of Axial SpA Enhance your patient examination skills Claire Harris, Senior Physiotherapist, London North West Healthcare
Overview of axial spondyloarthritis
 Chapter 2 Overview of axial spondyloarthritis The concept and classification of spondyloarthritis The term spondyloarthritis (SpA) comprises ankylosing spondylitis (AS), reactive arthritis, arthritis/spondylitis
Chapter 2 Overview of axial spondyloarthritis The concept and classification of spondyloarthritis The term spondyloarthritis (SpA) comprises ankylosing spondylitis (AS), reactive arthritis, arthritis/spondylitis
Characterization of Patients With Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis in the US-Based Corrona Registry
 Arthritis Care & Research Vol. 70, No. 11, November 2018, pp 1661 1670 DOI 10.1002/acr.23534 2018, The Authors. Arthritis Care & Research published by Wiley Periodicals, Inc. on behalf of American College
Arthritis Care & Research Vol. 70, No. 11, November 2018, pp 1661 1670 DOI 10.1002/acr.23534 2018, The Authors. Arthritis Care & Research published by Wiley Periodicals, Inc. on behalf of American College
Performance of the Ankylosing Spondylitis Disease Activity Score (ASDAS) in patients under biological therapies
 in patients under biological therapies") Performance of the Ankylosing Spondylitis Disease Activity Score (ASDAS) in patients under biological therapies 1. Introduction The Ankylosing Spondylitis Disease Activity Score (ASDAS) is a new instrument
Performance of the Ankylosing Spondylitis Disease Activity Score (ASDAS) in patients under biological therapies 1. Introduction The Ankylosing Spondylitis Disease Activity Score (ASDAS) is a new instrument
Eligibility criteria for TNFi therapy in axspa: BASDAI vs ASDAS
 Eligibility criteria for TNFi therapy in axspa: BASDAI vs ASDAS Abstract Background The Ankylosing Spondylitis Disease Activity Score (ASDAS) has been developed as a composite disease activity measure
Eligibility criteria for TNFi therapy in axspa: BASDAI vs ASDAS Abstract Background The Ankylosing Spondylitis Disease Activity Score (ASDAS) has been developed as a composite disease activity measure
Muhammad Haroon 1* Oliver FitzGerald 4. , Muddassar Ahmad 1, Muhammad Nouman Baig 2, Olivia Mason 3, John Rice 2 and
 Haroon et al. Arthritis Research & Therapy (2018) 20:73 https://doi.org/10.1186/s13075-018-1565-4 RESEARCH ARTICLE Inflammatory back pain in psoriatic arthritis is significantly more responsive to corticosteroids
Haroon et al. Arthritis Research & Therapy (2018) 20:73 https://doi.org/10.1186/s13075-018-1565-4 RESEARCH ARTICLE Inflammatory back pain in psoriatic arthritis is significantly more responsive to corticosteroids
Hierarchy of Impairment of Spinal Mobility Measures in Ankylosing Spondylitis: Twelve-Year Data
 Arthritis Care & Research Vol. 67, No. 11, November 2015, pp 1571 1577 DOI 10.1002/acr.22614 VC 2015, American College of Rheumatology ORIGINAL ARTICLE Hierarchy of Impairment of Spinal Mobility Measures
Arthritis Care & Research Vol. 67, No. 11, November 2015, pp 1571 1577 DOI 10.1002/acr.22614 VC 2015, American College of Rheumatology ORIGINAL ARTICLE Hierarchy of Impairment of Spinal Mobility Measures
Assessing the Signs, Symptoms, and Clinical Manifestations of Axial SpA
 This resource was organised and funded by AbbVie. It has been developed in collaboration with Claire Harris, Susan Gurden, Dr Jane Martindale, Claire Jeffries and NASS. For UK healthcare professionals
This resource was organised and funded by AbbVie. It has been developed in collaboration with Claire Harris, Susan Gurden, Dr Jane Martindale, Claire Jeffries and NASS. For UK healthcare professionals
I J Sørensen,15 R Valle-Oñate,16 U Weber,17 J Wei,18 J Sieper,1,19
 See Editorial, pg 1 Additional data (supplementary table) are published online only. To view these fi les please visit the journal online (http://ard.bmj. com). 1 Department of Medicine, Charité University
See Editorial, pg 1 Additional data (supplementary table) are published online only. To view these fi les please visit the journal online (http://ard.bmj. com). 1 Department of Medicine, Charité University
MRI of the Sacroiliac Joints in Patients with Moderate to Severe Ankylosing Spondylitis
 MRI of Sacroiliac Joints in Patients with nkylosing Spondylitis Musculoskeletal Imaging Original Research M E D E N T U R I L I M G I N G JR 2006; 187:1420 1426 0361 803X/06/1876 1420 merican Roentgen
MRI of Sacroiliac Joints in Patients with nkylosing Spondylitis Musculoskeletal Imaging Original Research M E D E N T U R I L I M G I N G JR 2006; 187:1420 1426 0361 803X/06/1876 1420 merican Roentgen
ESPONDILOARTROPATÍAS. Dr. Julio Ramírez García
 ESPONDILOARTROPATÍAS Dr. Julio Ramírez García Bloque 1: Caracterización de los pacientes con SpA axial ABSTRACT NUMBER: 1509 Similarities and Differences between Non-Radiographic and Radiographic Axial
ESPONDILOARTROPATÍAS Dr. Julio Ramírez García Bloque 1: Caracterización de los pacientes con SpA axial ABSTRACT NUMBER: 1509 Similarities and Differences between Non-Radiographic and Radiographic Axial
Update - Imaging of the Spondyloarthropathies. Spondyloarthropathies. Spondyloarthropathies
 Update - Imaging of the Spondyloarthropathies Donald J. Flemming, M.D. Dept of Radiology Penn State Hershey Medical Center Spondyloarthropathies Family of inflammatory arthritides of synovium and entheses
Update - Imaging of the Spondyloarthropathies Donald J. Flemming, M.D. Dept of Radiology Penn State Hershey Medical Center Spondyloarthropathies Family of inflammatory arthritides of synovium and entheses
Spondyloarthritis: Practice. New Concepts in. Epidemiology and Clinical
 New Concepts in Spondyloarthritis: Epidemiology and Clinical Practice Atul Deodhar MD Professor of Medicine Oregon Health & Science University Portland, OR Northwest Rheumatism Society, Seattle, April
New Concepts in Spondyloarthritis: Epidemiology and Clinical Practice Atul Deodhar MD Professor of Medicine Oregon Health & Science University Portland, OR Northwest Rheumatism Society, Seattle, April
Evaluation of treatments for sacroiliitis in spondyloarthropathy using the Spondyloarthritis Research Consortium Canada scoring system
 Cui et al. Arthritis Research & Therapy (2016) 18:38 DOI 10.1186/s13075-016-0916-2 RESEARCH ARTICLE Open Access Evaluation of treatments for sacroiliitis in spondyloarthropathy using the Spondyloarthritis
Cui et al. Arthritis Research & Therapy (2016) 18:38 DOI 10.1186/s13075-016-0916-2 RESEARCH ARTICLE Open Access Evaluation of treatments for sacroiliitis in spondyloarthropathy using the Spondyloarthritis
Magnetic Resonance Imaging of Inflammatory Lesions in the Spine in Ankylosing Spondylitis Clinical Trials: Is Paramagnetic Contrast Medium Necessary?
 Magnetic Resonance Imaging of Inflammatory Lesions in the Spine in Ankylosing Spondylitis Clinical Trials: Is Paramagnetic Contrast Medium Necessary? KAY-GEERT A. HERMANN, ROBERT B.M. LANDEWÉ, JÜRGEN BRAUN,
Magnetic Resonance Imaging of Inflammatory Lesions in the Spine in Ankylosing Spondylitis Clinical Trials: Is Paramagnetic Contrast Medium Necessary? KAY-GEERT A. HERMANN, ROBERT B.M. LANDEWÉ, JÜRGEN BRAUN,
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP)
") European Medicines Agency Pre-Authorisation Evaluation of Medicines for Human Use London, 23 April 2009 Doc. Ref. CPMP/EWP/4891/03 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON CLINICAL
European Medicines Agency Pre-Authorisation Evaluation of Medicines for Human Use London, 23 April 2009 Doc. Ref. CPMP/EWP/4891/03 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON CLINICAL
ACR Appropriateness Criteria Chronic Back Pain Suspected Sacroiliitis Spondyloarthropathy EVIDENCE TABLE
 1. Underwood MR, Dawes P. Inflammatory back pain in primary care. Br J Rheumatol. 1995;(11):107-1077.. Sieper J, van der Heijde D, Landewe R, et al. New criteria for inflammatory back pain in patients
1. Underwood MR, Dawes P. Inflammatory back pain in primary care. Br J Rheumatol. 1995;(11):107-1077.. Sieper J, van der Heijde D, Landewe R, et al. New criteria for inflammatory back pain in patients
Heel pain in spondyloarthritis: results of a cross-sectional study of 275 patients
 Heel pain in spondyloarthritis: results of a cross-sectional study of 275 patients E. Koumakis, L. Gossec, M. Elhai, V. Burki, A. Durnez, I. Fabreguet, M. Meyer, J. Payet, F. Roure, S. Paternotte, M. Dougados
Heel pain in spondyloarthritis: results of a cross-sectional study of 275 patients E. Koumakis, L. Gossec, M. Elhai, V. Burki, A. Durnez, I. Fabreguet, M. Meyer, J. Payet, F. Roure, S. Paternotte, M. Dougados
Magnetic resonance imaging in ankylosing spondylitis
 REVIEW Magnetic resonance imaging in ankylosing spondylitis Xenofon Baraliakos, Robert Landewé & Juergen Braun Author for correspondence Ruhr-University, Rheumazentrum Ruhrgebiet Herne, Bochum, Germany
REVIEW Magnetic resonance imaging in ankylosing spondylitis Xenofon Baraliakos, Robert Landewé & Juergen Braun Author for correspondence Ruhr-University, Rheumazentrum Ruhrgebiet Herne, Bochum, Germany
 www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
Classifying Back Pain and Peripheral Joint Complaints in Inflammatory Bowel Disease Patients: A Prospective Longitudinal Followup
 Journal of Crohn's and Colitis, 2016, 166 175 doi:10.1093/ecco-jcc/jjv195 Advance Access publication October 28, 2015 Original Article Original Article Classifying Back Pain and Peripheral Joint Complaints
Journal of Crohn's and Colitis, 2016, 166 175 doi:10.1093/ecco-jcc/jjv195 Advance Access publication October 28, 2015 Original Article Original Article Classifying Back Pain and Peripheral Joint Complaints
Navarro-Compán et al. Arthritis Research & Therapy (2015) 17:265 DOI /s y
 17:265 DOI /s y") Navarro-Compán et al. Arthritis Research & Therapy (2015) 17:265 DOI 10.1186/s13075-015-0779-y RESEARCH ARTICLE Sponyloarthritis features forecasting the presence of HLA-B27 or sacroiliitis on magnetic
Navarro-Compán et al. Arthritis Research & Therapy (2015) 17:265 DOI 10.1186/s13075-015-0779-y RESEARCH ARTICLE Sponyloarthritis features forecasting the presence of HLA-B27 or sacroiliitis on magnetic
Active (acute) inflammation on MRI highly suggestive of sacroiliitis associated with SpA
 inflammation on MRI highly suggestive of sacroiliitis associated with SpA") MRI findings of active and chronic sacroiliitis in light of recent ASAS criteria for diagnosing axial spondyloarthritis: what the radiologist should know Poster No.: C-1955 Congress: ECR 2012 Type: Educational
MRI findings of active and chronic sacroiliitis in light of recent ASAS criteria for diagnosing axial spondyloarthritis: what the radiologist should know Poster No.: C-1955 Congress: ECR 2012 Type: Educational
Ez-Zaitouni et al. Arthritis Research & Therapy (2017) 19:118 DOI /s
 19:118 DOI /s") Ez-Zaitouni et al. Arthritis Research & Therapy (2017) 19:118 DOI 10.1186/s13075-017-1335-8 RESEARCH ARTICLE Open Access Is the current ASAS expert definition of a positive family history useful in identifying
Ez-Zaitouni et al. Arthritis Research & Therapy (2017) 19:118 DOI 10.1186/s13075-017-1335-8 RESEARCH ARTICLE Open Access Is the current ASAS expert definition of a positive family history useful in identifying
Referral Strategy for Axial Spondyloarthritis
 Referral Strategy for Axial Spondyloarthritis Development, validation and impact in a chronic low back pain population Lonneke van Hoeven Referral Strategy for Axial Spondyloarthritis Development, validation
Referral Strategy for Axial Spondyloarthritis Development, validation and impact in a chronic low back pain population Lonneke van Hoeven Referral Strategy for Axial Spondyloarthritis Development, validation
Chapter 2 Criteria and Disease Activity Measures in Axial Spondyloarthropathies
 Chapter 2 Criteria and Disease Activity Measures in Axial Spondyloarthropathies Jose Aliling 1 and Lawrence H Brent 1* Einstein Medical Center, USA * Corresponding Author: Lawrence H Brent, Einstein Medical
Chapter 2 Criteria and Disease Activity Measures in Axial Spondyloarthropathies Jose Aliling 1 and Lawrence H Brent 1* Einstein Medical Center, USA * Corresponding Author: Lawrence H Brent, Einstein Medical
Multiple Technology Appraisal (MTA)
") National Institute for Health and Care Excellence Multiple Technology Appraisal (MTA) TNF-alpha inhibitors for ankylosing spondylitis and axial spondyloarthritis without radiographic evidence of ankylosing
National Institute for Health and Care Excellence Multiple Technology Appraisal (MTA) TNF-alpha inhibitors for ankylosing spondylitis and axial spondyloarthritis without radiographic evidence of ankylosing
Clinical and Imaging Efficacy of Infliximab in HLA B27 Positive Patients With Magnetic Resonance Imaging Determined Early Sacroiliitis
 ARTHRITIS & RHEUMATISM Vol. 60, No. 4, April 2009, pp 946 954 DOI 10.1002/art.24408 2009, American College of Rheumatology Clinical and Imaging Efficacy of Infliximab in HLA B27 Positive Patients With
ARTHRITIS & RHEUMATISM Vol. 60, No. 4, April 2009, pp 946 954 DOI 10.1002/art.24408 2009, American College of Rheumatology Clinical and Imaging Efficacy of Infliximab in HLA B27 Positive Patients With
ARTHRITIS ADVISORY COMMITTEE MEETING
 ARTHRITIS ADVISORY COMMITTEE MEETING July 23, 2013 sbla 125057/323: adalimumab for the treatment of Active non-radiographic axial spondyloarthritis in adults with objective signs of inflammation by elevated
ARTHRITIS ADVISORY COMMITTEE MEETING July 23, 2013 sbla 125057/323: adalimumab for the treatment of Active non-radiographic axial spondyloarthritis in adults with objective signs of inflammation by elevated
MRI of the sacroiliac joints: what to report and its pitfalls
 MRI of the sacroiliac joints: what to report and its pitfalls Poster No.: C-1920 Congress: ECR 2016 Type: Educational Exhibit Authors: J. Goncalves, A. Y. Aihara, C. Longo, H. Guidorizzi, P. Aguiar, 1
MRI of the sacroiliac joints: what to report and its pitfalls Poster No.: C-1920 Congress: ECR 2016 Type: Educational Exhibit Authors: J. Goncalves, A. Y. Aihara, C. Longo, H. Guidorizzi, P. Aguiar, 1
BRIEF REPORT. Denis Poddubnyy, 1 Hildrun Haibel, 1 J urgen Braun, 2 Martin Rudwaleit, 3 and Joachim Sieper 1
 ARTHRITIS & RHEUMATOLOGY Vol. 67, No. 9, September 2015, pp 2369 2375 DOI 10.1002/art.39225 VC 2015, American College of Rheumatology BRIEF REPORT Clinical Course Over Two Years in Patients With Early
ARTHRITIS & RHEUMATOLOGY Vol. 67, No. 9, September 2015, pp 2369 2375 DOI 10.1002/art.39225 VC 2015, American College of Rheumatology BRIEF REPORT Clinical Course Over Two Years in Patients With Early
6/6/2017. Spondyloarthritis and Osteopathic Primary Care: Facts and Challenges. Progression of Ankylosing Spondylitis Classic Disease
 1 Outline Talk 1 Introduction of spondyloarthritis (SpA) Clinical case challenge The problem of low back pain (LBP) in primary care and in osteopathic primary care Talk 2 What is SpA today? How many people
1 Outline Talk 1 Introduction of spondyloarthritis (SpA) Clinical case challenge The problem of low back pain (LBP) in primary care and in osteopathic primary care Talk 2 What is SpA today? How many people
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/43590 holds various files of this Leiden University dissertation Author: Machado, Pedro Title: Health and imaging outcomes in axial spondyloarthritis Issue
Cover Page The handle http://hdl.handle.net/1887/43590 holds various files of this Leiden University dissertation Author: Machado, Pedro Title: Health and imaging outcomes in axial spondyloarthritis Issue
Do extra-articular manifestations influence outcome in ankylosing spondylitis? 12-year results from OASIS
 Do extra-articular manifestations influence outcome in ankylosing spondylitis? 12-year results from OASIS I. Essers 1, S. Ramiro 2, C. Stolwijk 1, M. Blaauw 1, R. Landewé 3, D. van der Heijde 2, F. Van
Do extra-articular manifestations influence outcome in ankylosing spondylitis? 12-year results from OASIS I. Essers 1, S. Ramiro 2, C. Stolwijk 1, M. Blaauw 1, R. Landewé 3, D. van der Heijde 2, F. Van
Quantifying bone marrow inflammatory edema in the spine and sacroiliac joints with thresholding
 Chronaiou et al. BMC Musculoskeletal Disorders (2017) 18:497 DOI 10.1186/s12891-017-1861-1 RESEARCH ARTICLE Open Access Quantifying bone marrow inflammatory edema in the spine and sacroiliac joints with
Chronaiou et al. BMC Musculoskeletal Disorders (2017) 18:497 DOI 10.1186/s12891-017-1861-1 RESEARCH ARTICLE Open Access Quantifying bone marrow inflammatory edema in the spine and sacroiliac joints with
SPARTAN NEWS. Greetings!
 Volume 3 Issue 1 SPARTAN NEWS Greetings! I am looking forward to seeing you at our Annual Meeting in Cambridge, MA and encourage you to register for the meeting as soon as possible if you haven't had the
Volume 3 Issue 1 SPARTAN NEWS Greetings! I am looking forward to seeing you at our Annual Meeting in Cambridge, MA and encourage you to register for the meeting as soon as possible if you haven't had the
Optimisation of rheumatology assessments the actual situation in axial spondyloarthritis including ankylosing spondylitis
 Optimisation of rheumatology assessments the actual situation in axial spondyloarthritis including ankylosing spondylitis J. Braun, U. Kiltz, X. Baraliakos, D. van der Heijde Rheumazentrum Ruhrgebiet,
Optimisation of rheumatology assessments the actual situation in axial spondyloarthritis including ankylosing spondylitis J. Braun, U. Kiltz, X. Baraliakos, D. van der Heijde Rheumazentrum Ruhrgebiet,
2014 Update on the CRA/SPARCC Treatment Recommendations for the Management of Spondyloarthritis
 2014 Update on the CRA/SPARCC Treatment Recommendations for the Management of Spondyloarthritis Dr. Sherry Rohekar May 24, 2014 Learning Objectives Learn about proposed principles of the management of
2014 Update on the CRA/SPARCC Treatment Recommendations for the Management of Spondyloarthritis Dr. Sherry Rohekar May 24, 2014 Learning Objectives Learn about proposed principles of the management of
A nkylosing spondylitis (AS) is a common chronic
 is a common chronic") 1046 EXTENDED REPORT Analysing chronic spinal changes in ankylosing spondylitis: a systematic comparison of conventional x rays with magnetic resonance imaging using established and new scoring systems
1046 EXTENDED REPORT Analysing chronic spinal changes in ankylosing spondylitis: a systematic comparison of conventional x rays with magnetic resonance imaging using established and new scoring systems
Guideline on the Clinical Investigation of Medicinal Products for the Treatment of Axial Spondyloarthritis
 12 October 2017 EMA/CPMP/EWP/4891/03 Rev.1 Committee for Medicinal Products for Human Use (CHMP) Guideline on the Clinical Investigation of Medicinal Products for the Treatment of Axial Draft agreed by
12 October 2017 EMA/CPMP/EWP/4891/03 Rev.1 Committee for Medicinal Products for Human Use (CHMP) Guideline on the Clinical Investigation of Medicinal Products for the Treatment of Axial Draft agreed by
Prevalence of Human Leucocyte Antigen B17 in Spondyloarthritis Patients in a Tertiary Care Center in South India Detected Microlymphocytotoxicity Test
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 7 (2016) pp. 592-598 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.507.066
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 7 (2016) pp. 592-598 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.507.066
The Clinical Usefulness of Multidetector Computed Tomography of the Sacroiliac Joint for Evaluating Spondyloarthropathies
 The Korean Journal of Internal Medicine : 22:171-177, 2007 The Clinical Usefulness of Multidetector Computed Tomography of the Sacroiliac Joint for Evaluating Spondyloarthropathies You-Hyun Lee, M.D.,
The Korean Journal of Internal Medicine : 22:171-177, 2007 The Clinical Usefulness of Multidetector Computed Tomography of the Sacroiliac Joint for Evaluating Spondyloarthropathies You-Hyun Lee, M.D.,
SPARCC Abstracts and Publications
 SPARCC Abstracts and Publications 2006 Papers 1. Siannis F, Farewell VT, Cook RJ, Schentag CT, Gladman DD. Clinical and radiological damage in psoriatic arthritis. Ann Rheum Dis online 2006;65 478-481
SPARCC Abstracts and Publications 2006 Papers 1. Siannis F, Farewell VT, Cook RJ, Schentag CT, Gladman DD. Clinical and radiological damage in psoriatic arthritis. Ann Rheum Dis online 2006;65 478-481
CLOSER LOOK AT SpA. Dr. Mohamed Bedaiwi. Consultant Rheumatologist Rheumatology Unit - KKUH
 CLOSER LOOK AT SpA Dr. Mohamed Bedaiwi Consultant Rheumatologist Rheumatology Unit - KKUH Closer look at SpA I. Categories II. SIGN & SYMPTOMS III. X-RAY IV. MRI V. MANAGMENT Spondyloarthritis (SpA)
CLOSER LOOK AT SpA Dr. Mohamed Bedaiwi Consultant Rheumatologist Rheumatology Unit - KKUH Closer look at SpA I. Categories II. SIGN & SYMPTOMS III. X-RAY IV. MRI V. MANAGMENT Spondyloarthritis (SpA)
Identification of Psoriatic Arthritis and Ankylosing Spondylitis Early Detection to Facilitate Appropriate Care
 Identification of Psoriatic Arthritis and Ankylosing Spondylitis Early Detection to Facilitate Appropriate Care Joy Schechtman D.O. Professor Midwestern University 64C-1876207 Disclosures None 3 64C-1876207
Identification of Psoriatic Arthritis and Ankylosing Spondylitis Early Detection to Facilitate Appropriate Care Joy Schechtman D.O. Professor Midwestern University 64C-1876207 Disclosures None 3 64C-1876207
B Freundlich,7 M Rudwaleit,1 J Sieper 1
 1 Department of Rheumatology, Charité Medical University, Campus Benjamin Franklin, Berlin, Germany 2 Department of Radiology, Charité Medical University, Campus Charité Mitte, Berlin, Germany 3 German
1 Department of Rheumatology, Charité Medical University, Campus Benjamin Franklin, Berlin, Germany 2 Department of Radiology, Charité Medical University, Campus Charité Mitte, Berlin, Germany 3 German
ARTHRITIS ADVISORY COMMITTEE MEETING
 ARTHRITIS ADVISORY COMMITTEE MEETING July 23, 2013 sbla 125160/215: Cimzia (certolizumab) for the treatment of active axial spondyloarthritis, including patients with ankylosing spondylitis Disclaimer
ARTHRITIS ADVISORY COMMITTEE MEETING July 23, 2013 sbla 125160/215: Cimzia (certolizumab) for the treatment of active axial spondyloarthritis, including patients with ankylosing spondylitis Disclaimer
SPONDYLOARTHRITIS: PATHOGENESIS, CLINICAL MANIFESTATIONS, DIAGNOSIS, AND MANAGEMENT
 SPONDYLOARTHRITIS: PATHOGENESIS, CLINICAL MANIFESTATIONS, DIAGNOSIS, AND MANAGEMENT *Pilar S. del Río-Martínez Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain *Correspondence to psdelrio@yahoo.es
SPONDYLOARTHRITIS: PATHOGENESIS, CLINICAL MANIFESTATIONS, DIAGNOSIS, AND MANAGEMENT *Pilar S. del Río-Martínez Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain *Correspondence to psdelrio@yahoo.es
The Challenge of Diagnosis and Classification in Early Ankylosing Spondylitis
 ARTHRITIS & RHEUMATISM Vol. 52, No. 4, April 2005, pp 1000 1008 DOI 10.1002/art.20990 2005, American College of Rheumatology COMMENTARY The Challenge of Diagnosis and Classification in Early Ankylosing
ARTHRITIS & RHEUMATISM Vol. 52, No. 4, April 2005, pp 1000 1008 DOI 10.1002/art.20990 2005, American College of Rheumatology COMMENTARY The Challenge of Diagnosis and Classification in Early Ankylosing