Zahra Jahangard Clinical pharmacy Resident
|
|
|
- Domenic Cunningham
- 5 years ago
- Views:
Transcription
1 Zahra Jahangard Clinical pharmacy Resident
2 OA, or degenerative joint disease, is the most common form of arthritis A clinical syndrome of joint pain accompanied by varying degrees of functional limitation and reduced quality of life. The single most common cause of rheumatic symptoms Any synovial joint can develop osteoarthritis but knees, hips and small hand joints are the peripheral sites most commonly affected. Patients with OA are more dependent on others in climbing stairs and walking than any other disease

3 The prevalence of OA rises dramatically with age. In those younger than age 45 years, about one-fifth have OA of the hands, whereas of those ages 75 to 79 years, 85% have OA of the hands. OA of the knee occurs in less than 0.1% of those ages 25 to 34 years, but in 10% to 20% of those ages 65 to 74 years. Women are more often affected by OA, with older women being twice as likely as men to have OA of the knee and hands


4
5 Human cartilage is a connective tissue composed of cartilage cells (chondrocytes) and the extracellular matrix The extracellular matrix accounts for nearly 90% of articular cartilage and is predominantly avascular. Chondrocyte nutrients and waste products are transported by diffusion through the blood supply of trabecular bone, blood and synovial fluid.
6 The extracellular matrix of cartilage serves as the anchor for chondrocytes and imparts structural stability. Is composed of collagen, hyaluronic acid, and proteoglycans (PGs). PGs are macromolecules composed of a protein core covalently linked to sulfated glucosaminoglycan (GAG) side chains. two types of GAGs are linked to the protein core: chondroitin sulfate and keratan sulfate
7 Hyaluronate serves as a link protein, which is bound to the PG subunit ionically. The strength of articular cartilage largely depends on collagen, hyaluronate, and the GAGs of the PG aggregates (mostly chondroitin). During cartilage synthesis, cations and water are bound to PG. This forms a viscous layer, which cushions and lubricates the joint.

8 GAG and PG structures in human cartilage
9 OA is characterized by a loss of PGs and GAGs and an increase in cartilage degradation, leading to joint stiffness and decreased elasticity.
10 1- hypertrophic phase: OA most commonly begins with damage to articular cartilage, through trauma or other injury, excess joint loading from obesity or other reasons, or instability or injury of the joint that causes abnormal loading damage to cartilage dramatically increases the metabolic activity of chondrocytes This leads to increased synthesis of matrix constituents, with swelling of cartilage
11 2- Increased turnover increased collagen synthesis and destruction, but with destruction outpacing formation, with net loss of cartilage Key players in this destruction are the matrix metalloproteinases (MMPs) chondrocytes in OA cartilage undergo apoptosis, likely as a result of induction of nitric oxide synthase and production of toxic metabolites.

12 The net result of all of these processes is that there is a progressive cycle of cartilage destruction and loss of chondrocytes. Substantial loss of cartilage causes joint space narrowing and leads to a painful, deformed joint Accompanying the changes in cartilage and subchondral bone, local inflammatory changes and pathologic changes can occur in the joint capsule and synovium. With inflammatory changes in the synovium, effusions and synovial thickening occur

13 joint space narrowing

14 Primary (idiopathic) OA: The most common type, without identifiable cause Localized OA involving one or two sites Generalized OA, affecting three or more sites Secondary OA: associated with a known cause such as rheumatoid or another inflammatory arthritis, trauma, metabolic or endocrine disorders, and congenital factors

15 Age Female versus male sex Obesity Occupation Sports activities Genetic susceptibility developmental abnormalities(acromegaly)
16 Advanced age is one of the strongest risk factors associated with osteoarthritis. prevalence of this disease is less than 0.1 percent in 25 to 34 years old versus a rate of over 80 percent in people over age 55.

17 Innumerable studies have found that female sex is associated with an increased risk of osteoarthritis. Women with OA are also more likely than men to experience rapid structural damage and to undergo total hip arthroplasty The reason for these increased risks in women remains unclear, but may be related to hormones, genetics, or other undetermined factors

18 Obesity is perhaps the strongest modifiable risk factor for the development of osteoarthritis It is likely that even modest weight loss will provide some benefit. metabolic factors may also play a role in the development of OA in obese individuals. Excess adipose tissue can produce abnormal levels of hormones or growth factors that can affect cartilage or underlying bone, predisposing individuals to OA. A weight loss of 5 kg is associated with a 50% reduction in the odds of developing symptomatic knee OA.
19 Wrestling (cervical spine, knees, and elbows) Boxing (carpometacarpal joints) Cycling (patellofemoral joints) Recreational parachuting (spine, knees, and ankles) Cricket (fingers) Gymnastics (shoulders, wrists, and elbows) Ballet dancing (talar joints) Soccer (hips, knees, ankles, cervical spine, and talar joints) Football (knees, feet, and ankles)

20 Acromegaly has been associated with the development of secondary osteoarthritis, presumably due to the effects of elevated growth hormone levels on bone and cartilage
21 The clinical presentation of OA is variable and depends on the particular joints involved The primary symptom is a deep aching pain localized to the affected joint(s) morning stiffness and stiffness after rest during the day lasting less than 20 to 30 minutes, limited to involved joints. Joint motion may be limited secondary to loss of integrity of the joint surfaces, intra-articular loose bodies, and protective muscle spasm.
22 Crepitus, a palpable grating or crackling due to roughened articular surfaces, may be associated with both passive and active motion of involved joints. Occasionally, secondary synovial inflammation can contribute to symptoms The Heberden's nodes, bony protuberances (osteophytes) at the margins on the dorsal surfaces of the DIP joints are more common in women, have a genetic predisposition, and often are associated with a more severe disease course involving multiple joints

23 Heberden's nodes
24 The prognosis for patients with primary OA is variable and depends on the joint involved. If a weight-bearing joint or the spine is involved, considerable morbidity and disability are possible. In the case of secondary OA, the prognosis depends on the underlying cause. Treatment of OA may relieve pain or improve function, but does not reverse preexisting damage to the articular cartilage

25 Treatment of OA may relieve pain or improve function, but does not reverse preexisting damage to the articular cartilage OA treatment goals are to relieve pain, maintain or improve joint function, minimize disability, enhance quality of life and functional independence and minimize risks of therapy
26 Because of the degenerative nature of OA, nonpharmacologic interventions aimed at preserving joint function and ROM while maintaining muscle strength are essential.
27 exercises that avoid stress on joints while strengthening periarticular muscles (e.g., aerobic aquatic exercises, stationary bicycle) avoidance of excessive loading of the hip or knee joints by using assistive devices (e.g., canes, walkers, orthopedic shoe) weight reduction for obese individuals thermal modalities
28 Drug therapy in OA is targeted at relief of pain. For mild or moderate pain, topical analgesics or acetaminophen can be used. If these measures fail, or if there is inflammation, NSAIDs may be useful. Even when drug therapy is initiated, appropriate nondrug therapies should be continued and reinforced. Nondrug modalities are the cornerstone of OA management and may provide as much relief as drug therapy
29
30 The American College of Rheumatology (ACR) recommends acetaminophen as first-line drug therapy for pain management in OA because of its relative safety, efficacy, and lower cost compared to NSAID Pain relief with acetaminophen has been reported as similar to that obtained with aspirin, naproxen, ibuprofen, and other NSAIDs, although many patients respond better to NSAIDs
31 Acetaminophen prevents prostaglandin synthesis by blocking the action of central cyclooxygenase. The treatment of choice for mild pain because of a lower risk of GI complications compared with NSAIDs Comparable relief of mild to moderate OA pain has been demonstrated for acetaminophen at 2.6 to 4 g/day, aspirin 650 mg four times daily, and NSAIDS, including ibuprofen at 1,200 or 2,400 mg daily, and naproxen 750 mg daily
32 Adverse effects: hepatotoxicity The maximum dose of acetaminophen should be not be exceeded in any patient population, and chronic use of even the maximum 4 g/day can affect the liver. Acetaminophen should be used cautiously in patients with liver disease or in those who abuse alcohol.
33 Adverse effects: possibly renal toxicity with long-term use The cumulative amount (at least 1 to 2 kg of acetaminophen), rather than the duration of analgesic intake, is the primary risk factor for developing chronic analgesic nephropathy The National Kidney Foundation strongly discourages the use of nonprescription combination analgesic products (e.g., acetaminophen and NSAIDs) because this is associated with an increased prevalence of renal failure

34 Dosing and Administration Acetaminophen can be taken at 325 to 650 mg every 4 to 6 hours, but total dose must not exceed 4 g daily in the setting of chronic alcohol intake or in those with underlying hepatic disease, the duration should be limited and the dose should not exceed 2 g daily

35
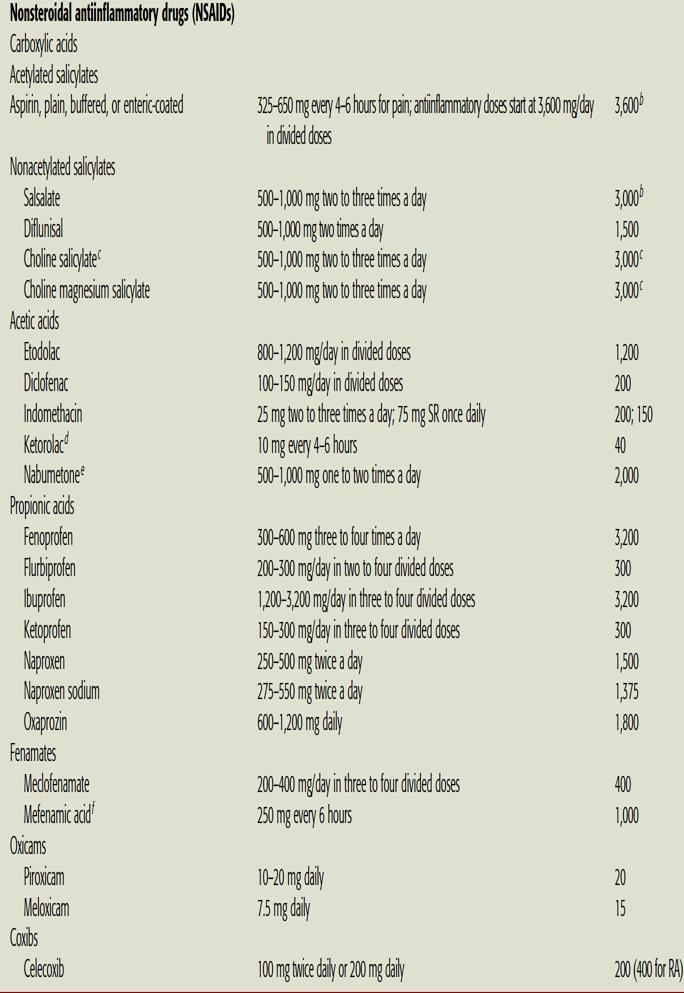
36 The American College of Rheumatology recommends consideration of NSAIDs for OA patients in whom acetaminophen is ineffective. NSAIDs have analgesic properties at lower doses and antiinflammatory effects at higher doses. There is no significant difference among the NSAIDs in efficacy. The selection of an NSAID is based primarily on patient preference, convenience, cost, and safety.
37 Blockade of prostaglandin synthesis by inhibiting cyclooxygenase enzymes (COX-1 and COX-2) is thought to account for the ability of NSAIDs to relieve pain and inflammation
38 Pathway of synthesis for prostaglandins and leukotrienes

39
40 exhibit several pharmacokinetic similarities, including high oral availability, high protein binding, and absorption as active drugs (except for sulindac and nabumetone, which require hepatic conversion for activity) The most important difference in NSAIDs is a serum half-life ranging from 1 hour for tolmetin to 50 hours for piroxicam, impacting the frequency of dosing and, potentially, compliance with therapy NSAIDs penetrate joint fluid, reaching approximately 60% of blood levels

41
42 nausea, dyspepsia, anorexia, abdominal pain, flatulence, and diarrhea(in 10% to 60% of patients) To minimize these symptoms, NSAIDs should be taken with food or milk, except for enteric-coated products, which should not be taken with milk or antacids
43 All NSAIDs have the potential to cause GI bleeding Un-ionized NSAIDs enter gastric mucosal cells, release hydrogen ions, and are concentrated ( ion trapped ) within cells, with cell death or damage. Gastric mucosal injury can also result from NSAID inhibition of gastroprotective prostaglandins.
44 In a meta-analysis of controlled trials involving some of the most commonly prescribed NSAIDs,The risk of gastrointestinal complications was highest with indomethacin followed by naproxen, diclofenac, piroxicam, tenoxicam, ibuprofen, and meloxicam.
45 risk factors for NSAID-induced GI bleeding : Prior history of a gastrointestinal event (ulcer, hemorrhage) Age >60 High dosage of a NSAID Concurrent use of glucocorticoid Concurrent use of anticoagulants concurrent use of more than one NSAID or aspirin at any dose
46 prevention therapy in high risk patients: Misoprostol (200 mcg three or four times daily) PPI are effective in preventing NSAID-induced gastroduodenal mucosal injury PPI cotherapy is more commonly prescribed because of the convenience of once-daily dosing and better tolerability
47 The development of NSAIDs highly selective for COX-2 introduced the potential to reduce inflammation without the worrisome adverse effects of nonselective NSAIDs, particularly gastropathy there is variable evidence that COX-2 inhibitors pose a decreased risk of GI toxicity compared to nonspecific NSAIDs, an especially important consideration when treating those at risk for clinically significant GI adverse effects

48
49 Two large multicenter clinical trials evaluated the GI safety of COX-2 inhibitors. The initial 6-month analysis of celecoxib in the CLASS trial revealed a lower rate of ulcer complications, but evaluation of the data at 13 months indicated that celecoxib did not have a GI safety advantage over ibuprofen or diclofenac. The most likely explanation for these results is that celecoxib is not as highly a selective COX-2 inhibitor as was originally anticipated VIGOR trial indicated that ulcers and related complications were lower with rofecoxib than with naproxen.
50 The COX-2 enzyme, found in blood vessel endothelial cells, leads to production of prostaglandin I2, which has antithrombotic effects. The COX-1 found in platelets forms thromboxane A2 a prothrombotic molecule. some researchers postulate that blocking COX-2 alone could upset the hemostatic balance, in favor of thromboxane A2, with prothrombotic events possible.
51 In meta analysis of RCTs the relative risk for vascular events compared to placebo was 0.92 with naproxen, 1.51 with ibuprofen, and 1.63 with diclofenac diclofenac is the most selective for COX-2 compared with COX-1 (and similar to celecoxib), naproxen is the least selective for COX-2 compared with COX-1, and ibuprofen has intermediate selectivity for COX-2 compared with COX-1
52 Several COX-2 selective inhibitors (eg, rofecoxib) have been withdrawn from the market because of an increased risk of ischemic cardiovascular events

53 Increasing degrees of selectivity for COX-2 are associated with augmented cardiovascular risk, whereas increasing degrees of selectivity for COX-1 are associated with augmented GI risk
54 Mild fluid retention occurs in approximately 5% of NSAID users, and NSAID-induced kidney disease occurs in <1% of patients Risk factors: heart failure, liver disease with associated ascites, compromised renal function, or when diuretics are administered concomitantly

55
56 Indomethacin is associated with the highest risk of NSAIDsinduced renal ischemia, whereas aspirin appears to have the lowest risk. Naproxen, ibuprofen, piroxicam, and diclofenac are considered intermediate in their relative capacities to acutely compromise renal perfusion. Sulindac may offer a renal-sparing effect COX-2 selective agents do not offer any benefit over nonselective NSAID with regard to renovascular effects
57 All NSAIDs may raise blood pressure and diminish the antihypertensive efficacy of all classes of antihypertensive drugs, except calcium channel blockers Aspirin, in the low dose that is used as an antithrombotic agent, does not affect blood pressure or interfere with the efficacy of antihypertensive drugs
58 Administration of NSAIDs must be tailored to the individual patient with OA. It usually takes about two to four weeks to evaluate the efficacy of a NSAID. Individual patient response differs among NSAIDs, So if an inadequate response is obtained with one NSAID, another NSAID may yet provide benefit
59

60 NSAIDs and cardioprotective doses of aspirin Ibuprofen, used at doses of 400 mg or more, may block aspirin s antiplatelet effect if it is taken prior to aspirin. Patients are advised to take a single dose of ibuprofen at least 2 hours after taking aspirin, or they should take their aspirin at least 8 hours after taking ibuprofen

61

62 topical NSAIDs (diclofenac, ibuprofen) have been as effective as oral NSAIDs, particularly in patients with OA of the knee. The mechanism of action of topical NSAIDs is thought to be primarily by local inhibition of COX-2 enzymes. This mode of delivery minimizes systemic exposure and may decrease the risk of the serious adverse events associated with oral NSAIDs. However, the efficacy of topical NSAIDs appears to be of relatively short duration
63 Capsaicin cream, derived from vanillyl alkaloids found in hot peppers and related plants, induces analgesic effects by depleting local sensory nerve endings of substance P. Evidence supporting the use of capsaicin cream is not as strong as topical NSAIDs, but is better than placebo in providing pain relief.

64 To be effective, capsaicin must be used regularly, and it may take up to 2 weeks to take effect. Although use is recommended four times a day, a twice-daily application may enhance long-term adherence and still provide adequate pain relief. Adverse events associated with capsaicin are primarily local, with 1 in 3 patients experiencing burning, stinging, and/or erythema that usually subsides with repeated application.
65 Topical salicylates are not effective for relief of OA symptoms





66
67 Endogenous glucosamine, an aminomonosaccharide synthesized from glucose, is integral to the biosynthesis of proteoglycans and the glycosaminoglycans, which are building blocks of cartilage. Chondroitin sulfate reportedly provides substrate for the formation of a healthy joint matrix and blocks enzymes responsible for breaking down old cartilage.
68 These products are often sold as combination products for the treatment of OA, but there is no evidence that the combination produces better results than glucosamine sulfate alone.
69 As a result of the widespread promotion and use of glucosamine with or without chondroitin for OA and the lack of strong clinical trial evidence, the National Institutes of Health sponsored a large study to end all speculation. The Glucosamine/chondroitin Arthritis Intervention Trial evaluated 1,583 patients randomized to receive either placebo, celecoxib, glucosamine, chondroitin, or glucosamine with chondroitin.
70 At 24-week follow-up, glucosamine and chondroitin, either alone or in combination, were found to be no different than placebo at achieving the primary endpoint of a 20% reduction in knee pain from baseline. A preplanned subgroup analysis of 354 patients with baseline moderate to severe pain revealed a significantly higher response rate with combination glucosamine and chondroitin versus placebo.
71 The combination of glucosamine and chondroitin is well-tolerated and may only be beneficial for moderate to severe OA. However, clinicians and patients should keep in mind that these are natural products unregulated by the FDA and, as a result, consistency in potency, safety, purity, and efficacy cannot be assured.
72 Because of the relative safety of these agents, a trial of glucosamine chondroitin may be reasonable in patients considering alternatives to traditional OA treatments. Dosing should be at least 1,500 mg/day of glucosamine and 1,200 mg/day of chondroitin. Keep in mind that the addition of other ingredients might increase the potential for adverse effects and may add to the cost of the product
73 Glucosamine-related adverse events are generally mild and include gastrointestinal symptoms (gas, bloating, cramps). he initial concerns regarding glucosamine-induced hyperglycemia had likely been overstated as later safety data in both healthy subjects and those with type 2 diabetes mellitus did not show significant elevations in blood glucose. Chondroitin is extremely well tolerated with the most common adverse effect being nausea
74 Systemic corticosteroids are not commonly prescribed for patients with OA because inflammation is not a primary component of OA pathophysiology. Intra-articular injection of a corticosteroid can be of value when isolated joints with effusions are painful and swollen
75 The aspiration of effusion fluid followed by an injection of a corticosteroid such as triamcinolone hexacetonide (up to 40 mg) can be effective for reducing pain and increasing muscle strength The initial relief of pain may permit more effective physical therapy and appropriate balance of rest and exercise, thus attenuating the need for repeated injections. On the other hand, symptomatic improvement may lead to overuse of the joint and potentially accelerate the degenerative process
76 The intra-articular injection of crystalline steroid suspension can precipitate a flare of synovitis, which usually is temporary and can be relieved with cold compresses and analgesics. Other potential, but rare, complications of intraarticular injections include osteonecrosis, tendon rupture, microcrystalline corticosteroid deposition in the synovial fluid, and joint capsule calcification. Thus, frequent injections into the same joint, particularly weight-bearing joints, should be avoided
77 High-molecular-weight HA is an important constituent of synovial fluid. Endogenous HA may also have antiinflammatory effects. Because the concentration and molecular size of synovial HA decrease in OA, administration of exogenous HA products has been studied, with the theory that this could reconstitute synovial fluid and reduce symptoms
78 In fact, HA injections temporarily and modestly increase viscosity. HA products are injected once weekly for either 3 or 5 weeks, depending on the specific agent administered. Hyalgan (20 mg sodium hylaronate/2 ml) is administered weekly for five injections. Synvisc (16 mg hylan polymers/2 ml) is administered weekly for three injections
79 HA injections may be beneficial for patients with knee OA unresponsive to other therapies. These agents are expensive because the treatment includes both drug costs and administration costs. improvement can begin within 3 to 4 weeks and can last several months
80 Low-dose opioid analgesics can be useful in patients who experience no relief with acetaminophen, NSAIDs, intraarticular injections, or topical therapy. Tramadol relieves moderate to severe pain and is comparable to ibuprofen for the treatment of OA of the hip and knee, and may be used as adjunctive therapy to NSAIDs tramadol seems to be safest for the short-term treatment of acute pain. If tramadol is used for chronic pain, closes monitoring for abuse or addiction



81
82 Tetracycline or doxycycline Appear to inhibit metalloproteinases In knee OA, doxycycline has been seen to delay loss of articular cartilage (joint space narrowing) in humans when compared with placebo. Diacerein An interleukin-1β inhibitor This agent decreased pain to a modest but statistically significant extent compared to placebo. In long-term studies, diacerein appeared to show a significant slowing of progression of joint space narrowing at the hip, but not at the knee
83 Oily fractions of avocado unsaponifiables decrease production of nitric oxide and stimulate production of plasminogen activator inhibitor-1 that can decrease MMPs Several short-term studies have demonstrated that the use of avocado/soy unsaponifiables at a dose of 300 mg to 600 mg daily led to decreases in the use of NSAIDS for pain control, but one long-term (2 years) study failed to replicate these results.

84 Treatment algorithm for osteoarthritis

85 Treatment algorithm for osteoarthritis

86
4 2 Osteoarthritis 1
 Osteoarthritis 1 Osteoarthritis ( OA) Osteoarthritis is a chronic disease and the most common of all rheumatological disorders. It particularly affects individuals over the age of 65 years. The prevalence
Osteoarthritis 1 Osteoarthritis ( OA) Osteoarthritis is a chronic disease and the most common of all rheumatological disorders. It particularly affects individuals over the age of 65 years. The prevalence
High Impact Rheumatology
 High Impact Rheumatology Evaluation and Management of Osteoarthritis Osteoarthritis: Case 1 A 65-year-old man comes to your office complaining of knee pain that began insidiously about a year ago. He has
High Impact Rheumatology Evaluation and Management of Osteoarthritis Osteoarthritis: Case 1 A 65-year-old man comes to your office complaining of knee pain that began insidiously about a year ago. He has
Osteoarthritis. Dr Anthony Feher. With special thanks to Dr. Tim Williams and Dr. Bhatia for allowing me to use some of their slides
 Osteoarthritis Dr Anthony Feher With special thanks to Dr. Tim Williams and Dr. Bhatia for allowing me to use some of their slides No Financial Disclosures Number one chronic disability in the United States
Osteoarthritis Dr Anthony Feher With special thanks to Dr. Tim Williams and Dr. Bhatia for allowing me to use some of their slides No Financial Disclosures Number one chronic disability in the United States
Osteoarthritis What is new? Dr Peter Cheung, Rheumatologist, NUHS
 Osteoarthritis What is new? Dr Peter Cheung, Rheumatologist, NUHS Objective Outline some clinical features that are not well appreciated in OA patients Recent advances in knowledge and management of OA
Osteoarthritis What is new? Dr Peter Cheung, Rheumatologist, NUHS Objective Outline some clinical features that are not well appreciated in OA patients Recent advances in knowledge and management of OA
Some illustrations are from the internet and intended for educational purpose only
 Some illustrations are from the internet and intended for educational purpose only นพ. ส หธ ช งามอ โฆษ ภาคว ชา ออร โธป ด กส คณะแพทย ศาสตร จ ฬาลงกรณ มหาว ทยาล ย Knee anatomy Femur Pathophysiology Symptoms
Some illustrations are from the internet and intended for educational purpose only นพ. ส หธ ช งามอ โฆษ ภาคว ชา ออร โธป ด กส คณะแพทย ศาสตร จ ฬาลงกรณ มหาว ทยาล ย Knee anatomy Femur Pathophysiology Symptoms
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Definition and Risk Factors Idiopathic vs. Secondary OA Clinical Features Diagnosis Radiologic Features ACR OA
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Definition and Risk Factors Idiopathic vs. Secondary OA Clinical Features Diagnosis Radiologic Features ACR OA
Non-Steroidal Anti- Inflammatory Drugs. ATPE 410 Chapter 6
 Non-Steroidal Anti- Inflammatory Drugs ATPE 410 Chapter 6 Inflammatory Process A normal, beneficial process that begins immediately after injury to facilitate repair and return the tissue to normal function
Non-Steroidal Anti- Inflammatory Drugs ATPE 410 Chapter 6 Inflammatory Process A normal, beneficial process that begins immediately after injury to facilitate repair and return the tissue to normal function
For more information about how to cite these materials visit
 Author(s): Seetha Monrad, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Seetha Monrad, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
The New Science of Osteoarthritis
 The New Science of Osteoarthritis What it means in managing our patients Terence W. Starz MD Clinical Professor of Medicine University of Pittsburgh School of Medicine Osteoarthritis: Key Points Perspective:
The New Science of Osteoarthritis What it means in managing our patients Terence W. Starz MD Clinical Professor of Medicine University of Pittsburgh School of Medicine Osteoarthritis: Key Points Perspective:
DISEASES AND DISORDERS
 DISEASES AND DISORDERS 9. 53 10. Rheumatoid arthritis 59 11. Spondyloarthropathies 69 12. Connective tissue diseases 77 13. Osteoporosis and metabolic bone disease 95 14. Crystal arthropathies 103 15.
DISEASES AND DISORDERS 9. 53 10. Rheumatoid arthritis 59 11. Spondyloarthropathies 69 12. Connective tissue diseases 77 13. Osteoporosis and metabolic bone disease 95 14. Crystal arthropathies 103 15.
Elements for a Public Summary
 VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Osteoarthritis Osteoarthritis is the most common type of joint disease. It represents a group of conditions that result in changes
VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Osteoarthritis Osteoarthritis is the most common type of joint disease. It represents a group of conditions that result in changes
Prevention Diagnosis Assessment Prescription and /or application of wide range of interventions and PRM program management
 OA PATHOLOGY Characterized by progressive deterioration and ultimate loss of articular cartilage Reactive changes of joint margins and joint thickening of the capsule When OA symptomatic leads to: Pain
OA PATHOLOGY Characterized by progressive deterioration and ultimate loss of articular cartilage Reactive changes of joint margins and joint thickening of the capsule When OA symptomatic leads to: Pain
Pain or stiffness in joints after periods of inactivity or excessive use
 Arthritis Awareness* Some older adults call it Arthur ; others refer to it as their constant compassion, but most describe it as extremely painful Arthritis is a chronic joint disease It is commonly believed
Arthritis Awareness* Some older adults call it Arthur ; others refer to it as their constant compassion, but most describe it as extremely painful Arthritis is a chronic joint disease It is commonly believed
Types of osteoarthritis
 ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
UPDATES ON MANAGEMENT OF OSTEOARTHRITIS
 UPDATES ON MANAGEMENT OF OSTEOARTHRITIS August 10, 2014 Dr. Suneil Kapur Assistant Professor of Medicine, University of Ottawa Associate Staff Rheumatologist, The Ottawa Hospital Learning Objectives Upon
UPDATES ON MANAGEMENT OF OSTEOARTHRITIS August 10, 2014 Dr. Suneil Kapur Assistant Professor of Medicine, University of Ottawa Associate Staff Rheumatologist, The Ottawa Hospital Learning Objectives Upon
Your Joint Pain and Treatment Options
 Your Joint Pain and Treatment Options Pinnacle Orthopedics Pinnacle Medical Network About Pinnacle Orthopedics and Pinnacle Medical Network South Louisiana s Premier System for the Delivery of Musculoskeletal
Your Joint Pain and Treatment Options Pinnacle Orthopedics Pinnacle Medical Network About Pinnacle Orthopedics and Pinnacle Medical Network South Louisiana s Premier System for the Delivery of Musculoskeletal
Dr. Howard C. H. Chen Athlete s Care Sports Medicine Centres DFCM University of Toronto
 Dr. Howard C. H. Chen Athlete s Care Sports Medicine Centres DFCM University of Toronto Faculty: Dr. Howard C. H. Chen Program: 51 st Annual Scientific Assembly Relationships with commercial interests:
Dr. Howard C. H. Chen Athlete s Care Sports Medicine Centres DFCM University of Toronto Faculty: Dr. Howard C. H. Chen Program: 51 st Annual Scientific Assembly Relationships with commercial interests:
Overcoming joint pain and arthritis
 Overcoming joint pain and arthritis The 9 things you need to know to get moving again This guide provides an overview about managing joint pain, stiffness and swelling without sacrificing your quality
Overcoming joint pain and arthritis The 9 things you need to know to get moving again This guide provides an overview about managing joint pain, stiffness and swelling without sacrificing your quality
Arthritis of the Knee
 Arthritis of the Knee There are three basic types of arthritis that may affect the knee joint. Osteoarthritis Osteoarthritis (OA) is the most common form of knee arthritis. OA is usually a slowly progressive
Arthritis of the Knee There are three basic types of arthritis that may affect the knee joint. Osteoarthritis Osteoarthritis (OA) is the most common form of knee arthritis. OA is usually a slowly progressive
Pain in Osteoarthritis
 Pain in Osteoarthritis By Edward L. Treadwell, MD Professor of Medicine- Rheumatology/Immunology Brody School of Medicine at East Carolina University School of Medicine Greenville, NC 27834 E-mail: treadwelle@ecu.edu
Pain in Osteoarthritis By Edward L. Treadwell, MD Professor of Medicine- Rheumatology/Immunology Brody School of Medicine at East Carolina University School of Medicine Greenville, NC 27834 E-mail: treadwelle@ecu.edu
Risk Management Plan Etoricoxib film-coated tablets
 VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Osteoarthritis (OA): OA is a condition in which the cartilage of the joints is broken down. This causes stiffness, pain and leads
VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Osteoarthritis (OA): OA is a condition in which the cartilage of the joints is broken down. This causes stiffness, pain and leads
OSTEOARTHRITIS An introduction to aging science brought to you by the American Federation for Aging Research
 infoaging guides DISEASES OF AGING OSTEOARTHRITIS An introduction to aging science brought to you by the American Federation for Aging Research WHAT IS OSTEOARTHRITIS? Osteoarthritis (OA) is the most common
infoaging guides DISEASES OF AGING OSTEOARTHRITIS An introduction to aging science brought to you by the American Federation for Aging Research WHAT IS OSTEOARTHRITIS? Osteoarthritis (OA) is the most common
Osteoarthritis. Dr. Siddharth Kumar Das M. D. Professor and Head, Department of Rheumatology, Chhatrapati Shahu Maharaj Medical University, Lucknow
 Osteoarthritis Dr. Siddharth Kumar Das M. D. Professor and Head, Department of Rheumatology, Chhatrapati Shahu Maharaj Medical University, Lucknow Das S.K. Osteoarthritis In Wagh S. (Ed). Rheumatology
Osteoarthritis Dr. Siddharth Kumar Das M. D. Professor and Head, Department of Rheumatology, Chhatrapati Shahu Maharaj Medical University, Lucknow Das S.K. Osteoarthritis In Wagh S. (Ed). Rheumatology
NSAIDs Overview. Souraya Domiati, Pharm D, MS
 NSAIDs Overview Souraya Domiati, Pharm D, MS Case A 32 years old shows up into your pharmacy asking for an NSAID for his ankle pain He smokes1 pack/day His BP is 125/75mmHg His BMI is 35kg/m2 His is on
NSAIDs Overview Souraya Domiati, Pharm D, MS Case A 32 years old shows up into your pharmacy asking for an NSAID for his ankle pain He smokes1 pack/day His BP is 125/75mmHg His BMI is 35kg/m2 His is on
Effective Health Care Program
 Comparative Effectiveness Review Number 38 Effective Health Care Program Analgesics for Osteoarthritis: An Update of the 2006 Comparative Effectiveness Review Executive Summary Background Osteoarthritis
Comparative Effectiveness Review Number 38 Effective Health Care Program Analgesics for Osteoarthritis: An Update of the 2006 Comparative Effectiveness Review Executive Summary Background Osteoarthritis
Osteoarthritis - An Overview and Visual Guide to OA
 Osteoarthritis - An Overview and Visual Guide to OA Osteoarthritis: What Is It? Also called "wear and tear" arthritis or degenerative joint disease, osteoarthritis (OA) is the progressive breakdown of
Osteoarthritis - An Overview and Visual Guide to OA Osteoarthritis: What Is It? Also called "wear and tear" arthritis or degenerative joint disease, osteoarthritis (OA) is the progressive breakdown of
Osteoarthritis. RA Hughes
 Osteoarthritis RA Hughes Osteoarthritis (OA) OA is the most common form of arthritis and the most common joint disease Most of the people who have OA are older than age 45, and women are more commonly
Osteoarthritis RA Hughes Osteoarthritis (OA) OA is the most common form of arthritis and the most common joint disease Most of the people who have OA are older than age 45, and women are more commonly
Is Viscosupplementation Effective in Reducing Osteoarthritis Knee Pain?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2016 Is Viscosupplementation Effective in
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2016 Is Viscosupplementation Effective in
Guide to Understanding and Managing Arthritis
 Guide to Understanding and Managing Arthritis The content in this guide is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician
Guide to Understanding and Managing Arthritis The content in this guide is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician
Osteoarthritis of the Hip
 Osteoarthritis of the Hip Sometimes called "wear-and-tear" arthritis, osteoarthritis is a common condition that many people develop during middle age or older. Osteoarthritis of the hip causes pain and
Osteoarthritis of the Hip Sometimes called "wear-and-tear" arthritis, osteoarthritis is a common condition that many people develop during middle age or older. Osteoarthritis of the hip causes pain and
ARTHRITIS. What Is Arthritis?
 There are many types of arthritic processes that can cause joint changes, pain and loss of motion and strength in the hands. Many excellent and detailed resources are available and will be listed under
There are many types of arthritic processes that can cause joint changes, pain and loss of motion and strength in the hands. Many excellent and detailed resources are available and will be listed under
Pain therapeutics. Acetaminophen/NSAIDs Acute pain Osteoarthritis Migraine Acute Gout Neuropathic pain
 Pain therapeutics Acetaminophen/NSAIDs Acute pain Osteoarthritis Migraine Acute Gout Neuropathic pain James McCormack, Pharm.D. Professor Faculty of Pharmaceutical Sciences, UBC Common types of pain killers
Pain therapeutics Acetaminophen/NSAIDs Acute pain Osteoarthritis Migraine Acute Gout Neuropathic pain James McCormack, Pharm.D. Professor Faculty of Pharmaceutical Sciences, UBC Common types of pain killers
STRIDE PLUS STRIDE PLUS. Nutritional Maintenance of Healthy Cartilage and Joints in Dogs. 100%
 STRIDE STRIDE Nutritional Maintenance of Healthy Cartilage and Joints in Dogs. WITH HYALURONIC ACID NATURAL YEAST FLAVOURING CERTIFIED VEGAN 100% The Joint The joint is where two or more bones meet. Each
STRIDE STRIDE Nutritional Maintenance of Healthy Cartilage and Joints in Dogs. WITH HYALURONIC ACID NATURAL YEAST FLAVOURING CERTIFIED VEGAN 100% The Joint The joint is where two or more bones meet. Each
Joint Health Optimum Flex Plus, Hi- Victory, Yucca, Herbal Respond
 Joint Health Optimum Flex Plus, Hi- Victory, Yucca, Herbal Respond May Educational Webinar 2018 Dr Tania Cubitt Performance Horse Nutrition COMPARATIVE ANATOMY 2 JOINT A joint is defined as a structure
Joint Health Optimum Flex Plus, Hi- Victory, Yucca, Herbal Respond May Educational Webinar 2018 Dr Tania Cubitt Performance Horse Nutrition COMPARATIVE ANATOMY 2 JOINT A joint is defined as a structure
TRANSPARENCY COMMITTEE OPINION. 26 November 2008
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 26 November 2008 CHONDROSULF 400 mg, capsule Box containing 84 capsules (CIP: 335 917-3) CHONDROSULF 400 mg, granules
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 26 November 2008 CHONDROSULF 400 mg, capsule Box containing 84 capsules (CIP: 335 917-3) CHONDROSULF 400 mg, granules
Hyaluronic Acid Derivatives
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.11.04 Subject: Hyaluronic Acid Page: 1 of 6 Last Review Date: March 13, 2014 Hyaluronic Acid Derivatives
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.11.04 Subject: Hyaluronic Acid Page: 1 of 6 Last Review Date: March 13, 2014 Hyaluronic Acid Derivatives
NSAIDs: Side Effects and Guidelines
 NSAIDs: Side Effects and James J Hale FY1 Department of Anaesthetics Introduction The non-steroidal anti-inflammatory drugs (NSAIDs) are a diverse group of drugs that have analgesic, antipyretic and anti-inflammatory
NSAIDs: Side Effects and James J Hale FY1 Department of Anaesthetics Introduction The non-steroidal anti-inflammatory drugs (NSAIDs) are a diverse group of drugs that have analgesic, antipyretic and anti-inflammatory
RISK MANAGEMENT PLAN (RMP) PUBLIC SUMMARY ETORICOXIB ORION (ETORICOXIB) 30 MG, 60 MG, 90 MG & 120 MG FILM-COATED TABLET DATE: , VERSION 1.
 PUBLIC SUMMARY ETORICOXIB ORION (ETORICOXIB) 30 MG, 60 MG, 90 MG & 120 MG FILM-COATED TABLET DATE: , VERSION 1.") RISK MANAGEMENT PLAN (RMP) PUBLIC SUMMARY ETORICOXIB ORION (ETORICOXIB) 30 MG, 60 MG, 90 MG & 120 MG FILM-COATED TABLET DATE: 07-10-2016, VERSION 1.2 VI.2 Elements for a Public Summary Etoricoxib Orion
RISK MANAGEMENT PLAN (RMP) PUBLIC SUMMARY ETORICOXIB ORION (ETORICOXIB) 30 MG, 60 MG, 90 MG & 120 MG FILM-COATED TABLET DATE: 07-10-2016, VERSION 1.2 VI.2 Elements for a Public Summary Etoricoxib Orion
Etoricoxib STADA 30 mg, 60 mg, 90 mg and 120 mg film-coated tablets , Version V1.2 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN
 Etoricoxib STADA 30 mg, 60 mg, 90 mg and 120 mg film-coated tablets 23.5.2016, Version V1.2 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN VI.2 Elements for a Public Summary Etoricoxib STADA 30 mg film-coated
Etoricoxib STADA 30 mg, 60 mg, 90 mg and 120 mg film-coated tablets 23.5.2016, Version V1.2 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN VI.2 Elements for a Public Summary Etoricoxib STADA 30 mg film-coated
R. Krishna Chaganti, MD, MS Associate Clinical Professor UCSF Division of Rheumatology
 R. Krishna Chaganti, MD, MS Associate Clinical Professor UCSF Division of Rheumatology No Disclosures Causes of OA Knowledge gaps Treatment options Medication Non-Medication Holy Grail : Disease Modifying
R. Krishna Chaganti, MD, MS Associate Clinical Professor UCSF Division of Rheumatology No Disclosures Causes of OA Knowledge gaps Treatment options Medication Non-Medication Holy Grail : Disease Modifying
Evaluation and Treatment of Knee Arthritis Classification of Knee Arthritis Osteoarthritis Osteoarthritis Osteoarthritis of Knee
 1 2 Evaluation and Treatment of Knee Arthritis John Zebrack, MD Reno Orthopaedic Clinic Classification of Knee Arthritis Non-inflammatory Osteoarthritis Primary Secondary Post-traumatic, dysplasia, neuropathic,
1 2 Evaluation and Treatment of Knee Arthritis John Zebrack, MD Reno Orthopaedic Clinic Classification of Knee Arthritis Non-inflammatory Osteoarthritis Primary Secondary Post-traumatic, dysplasia, neuropathic,
Salicylates: Interactions 10/14/2009. Salicylates DRUGS USED IN THE MANAGEMENT OF MUSCULOSKELETAL DISORDERS. Chapters 17, 18, 34 & Pages 577 &
 DRUGS USED IN THE MANAGEMENT OF MUSCULOSKELETAL DISORDERS Chapters 17, 18, 34 & Pages 577 & 579-586 Salicylates aspirin Have analgesic, antipyretic, and anti-inflammatory effects. Inhibits the production
DRUGS USED IN THE MANAGEMENT OF MUSCULOSKELETAL DISORDERS Chapters 17, 18, 34 & Pages 577 & 579-586 Salicylates aspirin Have analgesic, antipyretic, and anti-inflammatory effects. Inhibits the production
Inflammatory rheumatic diseases
 Learning objectives Inflammatory rheumatic diseases Bruce Kidd Barts & The London, Queen Mary, University of London To understand: 1. prevalence and range of the rheumatological s 2. clinical features
Learning objectives Inflammatory rheumatic diseases Bruce Kidd Barts & The London, Queen Mary, University of London To understand: 1. prevalence and range of the rheumatological s 2. clinical features
Drug Class Review Nonsteroidal Antiinflammatory Drugs (NSAIDs)
") Drug Class Review Nonsteroidal Antiinflammatory Drugs (NSAIDs) Preliminary Scan Report #2 May 2014 Last Report: Update #4 (November 2010) Last Preliminary Scan: July 2013 The purpose of reports is to make
Drug Class Review Nonsteroidal Antiinflammatory Drugs (NSAIDs) Preliminary Scan Report #2 May 2014 Last Report: Update #4 (November 2010) Last Preliminary Scan: July 2013 The purpose of reports is to make
o Total knee arthroplasty is projected to grow 85% o Other studies predict up to 3.48 million TKA o 17% adults over age 45 have symptomatic OA
 NONOPERATIVE TREATMENT OF KNEE ARTHRITIS DAVID M SCHALL MD Knee Arthritis o Total knee arthroplasty is projected to grow 85% to 1.26 million procedures per year by 2030 o Other studies predict up to 3.48
NONOPERATIVE TREATMENT OF KNEE ARTHRITIS DAVID M SCHALL MD Knee Arthritis o Total knee arthroplasty is projected to grow 85% to 1.26 million procedures per year by 2030 o Other studies predict up to 3.48
Month/Year of Review: January 2012 Date of Last Review: February 2007
 Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Month/Year of Review: January 2012 Date of Last Review:
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-945-5220 Fax 503-947-1119 Month/Year of Review: January 2012 Date of Last Review:
DECREASE JOINT PAIN IMPROVE JOINT FUNCTION Treatment of Osteoarthritis with Ostenil
 PATIENT - INFORMATION DECREASE JOINT PAIN IMPROVE JOINT FUNCTION Treatment of Osteoarthritis with Ostenil What is osteoarthritis? Osteoarthritis is a degenerative joint disease that mainly occurs due to
PATIENT - INFORMATION DECREASE JOINT PAIN IMPROVE JOINT FUNCTION Treatment of Osteoarthritis with Ostenil What is osteoarthritis? Osteoarthritis is a degenerative joint disease that mainly occurs due to
Hyaluronic Acid Derivatives
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.09 Subject: Hyaluronic Acid Derivatives Page: 1 of 6 Last Review Date: December 2, 2016 Hyaluronic
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.09 Subject: Hyaluronic Acid Derivatives Page: 1 of 6 Last Review Date: December 2, 2016 Hyaluronic
Joint Health: Arthritis Prevention Non-operative Treatments and Replacement Surgery
 Joint Health: Arthritis Prevention Non-operative Treatments and Replacement Surgery John A. Abraham, MD Orthopedic Oncology Service and Arthroplasty Service, Rothman Institute Director, Jefferson Sarcoma
Joint Health: Arthritis Prevention Non-operative Treatments and Replacement Surgery John A. Abraham, MD Orthopedic Oncology Service and Arthroplasty Service, Rothman Institute Director, Jefferson Sarcoma
KNEE PAIN MANAGEMENT
 KNEE PAIN MANAGEMENT Mr D Raj FRCS (Tr & Orth) Consultant Lower Limb Orthopaedic Surgeon BostoniaN Private Wing Pilgrim Hospital, Boston Lincolnshire PE21 9QS Boston treatment Centre, West Business Park,
KNEE PAIN MANAGEMENT Mr D Raj FRCS (Tr & Orth) Consultant Lower Limb Orthopaedic Surgeon BostoniaN Private Wing Pilgrim Hospital, Boston Lincolnshire PE21 9QS Boston treatment Centre, West Business Park,
GLUCOSAMINE SP TABLETS
 Executive Executive Summary Summary GLUCOSAMINE SP TABLETS WHAT IS GLUCOSAMINE? Glucosamine is widely used in Europe and is popular as a health food ingredient in Japan. Glucosamine is originally produced
Executive Executive Summary Summary GLUCOSAMINE SP TABLETS WHAT IS GLUCOSAMINE? Glucosamine is widely used in Europe and is popular as a health food ingredient in Japan. Glucosamine is originally produced
REVIEW I-Flex and Management of Inflammation in Osteoarthritis
 1 REVIEW I-Flex and Management of Inflammation in Osteoarthritis Tammy Wolhuter, RD (SA) & Anne Till, RD(SA) From: Anne Till & Associates, Registered Dietitians 1. Introduction Osteoarthritis (OA) is a
1 REVIEW I-Flex and Management of Inflammation in Osteoarthritis Tammy Wolhuter, RD (SA) & Anne Till, RD(SA) From: Anne Till & Associates, Registered Dietitians 1. Introduction Osteoarthritis (OA) is a
ASPIRIN. Session Two of TIP Assignment
 ASPIRIN Session Two of TIP Assignment History Behind Aspirin Development 2 Pain relief is something that has been sought after since the ancient Greeks and Egyptians used bark and dried leaves of the poplar
ASPIRIN Session Two of TIP Assignment History Behind Aspirin Development 2 Pain relief is something that has been sought after since the ancient Greeks and Egyptians used bark and dried leaves of the poplar
Arthritis of the Shoulder
 Arthritis of the Shoulder Simply defined, arthritis is inflammation of one or more of your joints. In a diseased shoulder, inflammation causes pain and stiffness. Although there is no cure for arthritis
Arthritis of the Shoulder Simply defined, arthritis is inflammation of one or more of your joints. In a diseased shoulder, inflammation causes pain and stiffness. Although there is no cure for arthritis
Non-operative Treatment of Osteoarthritis. Health Chat June 21 & 22, 2016 Aaron Leininger, MD
 Non-operative Treatment of Osteoarthritis Health Chat June 21 & 22, 2016 Aaron Leininger, MD About Me Aaron Leininger, MD Clemson University Mechanical Engineering Varsity Soccer, Formula SAE race car
Non-operative Treatment of Osteoarthritis Health Chat June 21 & 22, 2016 Aaron Leininger, MD About Me Aaron Leininger, MD Clemson University Mechanical Engineering Varsity Soccer, Formula SAE race car
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 20 November 2013 FLEXEA 625 mg, tablet Box of 60 tablets (CIP: 34009 380 534 2 5) Box of 180 tablets (CIP: 34009 380
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 20 November 2013 FLEXEA 625 mg, tablet Box of 60 tablets (CIP: 34009 380 534 2 5) Box of 180 tablets (CIP: 34009 380
Joint Injuries and Disorders
 Joint Injuries and Disorders Introduction A joint is where two or more bones come together. Your joints include the knees, hips, elbows and shoulders. There are many types of joint disorders, including
Joint Injuries and Disorders Introduction A joint is where two or more bones come together. Your joints include the knees, hips, elbows and shoulders. There are many types of joint disorders, including
Hyaluronic Acid Derivatives
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.09 Subject: Hyaluronic Acid Derivatives Page: 1 of 6 Last Review Date: March 20, 2015 Hyaluronic Acid
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.09 Subject: Hyaluronic Acid Derivatives Page: 1 of 6 Last Review Date: March 20, 2015 Hyaluronic Acid
Drug Class Review on Cyclo-oxygenase (COX)-2 Inhibitors and Non-steroidal Anti-inflammatory Drugs (NSAIDs)
-2 Inhibitors and Non-steroidal Anti-inflammatory Drugs (NSAIDs)") Drug Class Review on Cyclo-oxygenase (COX)-2 Inhibitors and Non-steroidal Anti-inflammatory Drugs (NSAIDs) Final Report Update 3 Evidence Tables November 2006 Original Report Date: May 2002 Update 1 Report
Drug Class Review on Cyclo-oxygenase (COX)-2 Inhibitors and Non-steroidal Anti-inflammatory Drugs (NSAIDs) Final Report Update 3 Evidence Tables November 2006 Original Report Date: May 2002 Update 1 Report
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 9 January 2013
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 January 2013 The opinion adopted by the Transparency Committee on 4 July 2012 was given a hearing on 5 December
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 January 2013 The opinion adopted by the Transparency Committee on 4 July 2012 was given a hearing on 5 December
Hyaluronic Acid Derivatives
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.09 Subject: Hyaluronic Acid Derivatives Page: 1 of 6 Last Review Date: March 16, 2018 Hyaluronic Acid
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.09 Subject: Hyaluronic Acid Derivatives Page: 1 of 6 Last Review Date: March 16, 2018 Hyaluronic Acid
NOTOPAIN CAPLETS. Diclofenac Sodium + Paracetamol. Composition. Each tablet contains: Diclofenac Sodium BP 50mg Paracetamol BP 500mg.
 NOTOPAIN CAPLETS Diclofenac Sodium + Paracetamol Composition Each tablet contains: Diclofenac Sodium BP 50mg Paracetamol BP 500mg Pharmacology Phamacodynamics Diclofenac relieves pain and inflammation
NOTOPAIN CAPLETS Diclofenac Sodium + Paracetamol Composition Each tablet contains: Diclofenac Sodium BP 50mg Paracetamol BP 500mg Pharmacology Phamacodynamics Diclofenac relieves pain and inflammation
Safety and efficacy of flavocoxid compared with naproxen in subjects with osteoarthritis of the knee: a pilot study
 Osteoarthritis and Cartilage. 15(suppl B):B91 Safety and efficacy of flavocoxid compared with naproxen in subjects with osteoarthritis of the knee: a pilot study Levy R*, Saikovsky R, Shmidt E, Khokhlov
Osteoarthritis and Cartilage. 15(suppl B):B91 Safety and efficacy of flavocoxid compared with naproxen in subjects with osteoarthritis of the knee: a pilot study Levy R*, Saikovsky R, Shmidt E, Khokhlov
Matthew Husa, MD Assistant Professor of Medicine
 Evidence-based Review of Non-surgical Management of Osteoarthritis Matthew Husa, MD Assistant Professor of Medicine Division i i of Rheumatlogy and Immunology The Ohio State University Wexner Medical Center
Evidence-based Review of Non-surgical Management of Osteoarthritis Matthew Husa, MD Assistant Professor of Medicine Division i i of Rheumatlogy and Immunology The Ohio State University Wexner Medical Center
Canadian Chiropractic Guideline Initiative (CCGI) Guideline Summary
 Guideline Summary") Canadian Chiropractic Guideline Initiative (CCGI) Guideline Summary Title of guideline Osteoarthritis: care and management Clinical guideline Author of guideline National Institute for Health and Care
Canadian Chiropractic Guideline Initiative (CCGI) Guideline Summary Title of guideline Osteoarthritis: care and management Clinical guideline Author of guideline National Institute for Health and Care
Non-Operative Options for Articular Cartilage Issues in the Athlete s Knee
 Non-Operative Options for Articular Cartilage Issues in the Athlete s Knee Sourav Poddar, MD Associate Professor Director, Primary Care Sports Medicine University of Colorado School of Medicine OBJECTIVES
Non-Operative Options for Articular Cartilage Issues in the Athlete s Knee Sourav Poddar, MD Associate Professor Director, Primary Care Sports Medicine University of Colorado School of Medicine OBJECTIVES
SIMPLE Targets of OA Therapy
 SIMPLE Targets of OA Therapy Helping your patient with their osteoarthritis symptoms is SIMPLE. Remember these steps to prevent and treat osteoarthritis. Symptom management (e.g. reduce pain and stiffness)
SIMPLE Targets of OA Therapy Helping your patient with their osteoarthritis symptoms is SIMPLE. Remember these steps to prevent and treat osteoarthritis. Symptom management (e.g. reduce pain and stiffness)
Bursitis. Other joints are found between the different bones of your fingers and toes. You also have joints that allow your vertebrae to move.
 Bursitis Introduction Bursitis is a common condition that causes swelling around muscles and bones. It happens most often in the shoulder, elbow, hip, or knee. Bursitis is usually caused by overusing a
Bursitis Introduction Bursitis is a common condition that causes swelling around muscles and bones. It happens most often in the shoulder, elbow, hip, or knee. Bursitis is usually caused by overusing a
THAT S PROVEN FOR THE LONG RUN
 A GUIDE FOR PATIENTS KNEE PAIN RELIEF THAT S PROVEN FOR THE LONG RUN TREATMENT OPTIONS FOR OA KNEE PAIN There are several things you can do to help reduce knee pain due to OA. Lifestyle changes Losing
A GUIDE FOR PATIENTS KNEE PAIN RELIEF THAT S PROVEN FOR THE LONG RUN TREATMENT OPTIONS FOR OA KNEE PAIN There are several things you can do to help reduce knee pain due to OA. Lifestyle changes Losing
CARDIOVASCULAR RISK and NSAIDs
 CARDIOVASCULAR RISK and NSAIDs Dr. Syed Ghulam Mogni Mowla Assistant Professor of Medicine Shaheed Suhrawardy Medical College, Dhaka INTRODUCTION NSAIDs are most commonly prescribed drugs Recent evidence
CARDIOVASCULAR RISK and NSAIDs Dr. Syed Ghulam Mogni Mowla Assistant Professor of Medicine Shaheed Suhrawardy Medical College, Dhaka INTRODUCTION NSAIDs are most commonly prescribed drugs Recent evidence
A GUIDE FOR PATIENTS KNEE PAIN RELIEF THAT JUST CAN T WAIT
 A GUIDE FOR PATIENTS KNEE PAIN RELIEF THAT JUST CAN T WAIT TREATMENT OPTIONS FOR OA KNEE PAIN There are several things you can do to help reduce knee pain due to OA. Lifestyle changes Losing weight, if
A GUIDE FOR PATIENTS KNEE PAIN RELIEF THAT JUST CAN T WAIT TREATMENT OPTIONS FOR OA KNEE PAIN There are several things you can do to help reduce knee pain due to OA. Lifestyle changes Losing weight, if
1. Understand the basic epidemiology of OA 2. Understand challenges facing OA therapy development
 Evidence-based Review of Non-surgical Management of Osteoarthritis Matthew Husa, MD Assistant Professor of Medicine Division of Rheumatlogy and Immunology The Ohio State University Wexner Medical Center
Evidence-based Review of Non-surgical Management of Osteoarthritis Matthew Husa, MD Assistant Professor of Medicine Division of Rheumatlogy and Immunology The Ohio State University Wexner Medical Center
MUSCULOSKELETAL PHARMACOLOGY. A story of the inflamed
 MUSCULOSKELETAL PHARMACOLOGY A story of the inflamed 1 INFLAMMATION Pathophysiology Inflammation Reaction to tissue injury Caused by release of chemical mediators Leads to a vascular response Fluid and
MUSCULOSKELETAL PHARMACOLOGY A story of the inflamed 1 INFLAMMATION Pathophysiology Inflammation Reaction to tissue injury Caused by release of chemical mediators Leads to a vascular response Fluid and
Is Tanezumab More Effective than a Placebo in Reducing Pain in Patients with Osteoarthritis?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2018 Is Tanezumab More Effective than a Placebo
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2018 Is Tanezumab More Effective than a Placebo
Osteoarthritis of the Hip
 Osteoarthritis of the Hip Information on hip osteoarthritis is also available in Spanish: Osteoartritis de cadera (topic.cfm?topic=a00608). Sometimes called "wear and tear" arthritis, osteoarthritis is
Osteoarthritis of the Hip Information on hip osteoarthritis is also available in Spanish: Osteoartritis de cadera (topic.cfm?topic=a00608). Sometimes called "wear and tear" arthritis, osteoarthritis is
10 April 2014 Osteoarthritis SSalman 2
 10 April 2014 Osteoarthritis SSalman 2 Updates on therapies of knee Osteoarthritis Prof Sami Salman, FRCP, MRCP, DMR, CES, MB ChB College of Medicine University of Baghdad Introduction Investigational
10 April 2014 Osteoarthritis SSalman 2 Updates on therapies of knee Osteoarthritis Prof Sami Salman, FRCP, MRCP, DMR, CES, MB ChB College of Medicine University of Baghdad Introduction Investigational
This document has not been circulated to either the industry or Consultants within the Suffolk system.
 New Medicine Report Document Status COX II Inhibitors In Acute Analgesia For Suffolk Drug & Therapeutics Committee Date of Last Revision 15 th February 2002 Reviewer s Comments There seems to be a growing
New Medicine Report Document Status COX II Inhibitors In Acute Analgesia For Suffolk Drug & Therapeutics Committee Date of Last Revision 15 th February 2002 Reviewer s Comments There seems to be a growing
Osteoarthritis. What is osteoarthritis? Understanding joints. What causes osteoarthritis?
 Page 1 of 6 Osteoarthritis Osteoarthritis causes pain and stiffness in joints. Symptoms may be helped by exercises, some physical devices and treatments, and losing weight if you are overweight. Paracetamol
Page 1 of 6 Osteoarthritis Osteoarthritis causes pain and stiffness in joints. Symptoms may be helped by exercises, some physical devices and treatments, and losing weight if you are overweight. Paracetamol
PATIENT EDUCATION TOTAL HIP REPLACEMENT
 PATIENT EDUCATION TOTAL HIP REPLACEMENT WHY ORTHO DEVELOPMENT? Ortho Development is passionate about making the best, clinically proven, high-performance orthopedic devices in the world. All of our implants
PATIENT EDUCATION TOTAL HIP REPLACEMENT WHY ORTHO DEVELOPMENT? Ortho Development is passionate about making the best, clinically proven, high-performance orthopedic devices in the world. All of our implants
Diagnosis and treatment of osteoarthritisos4_
 Orthopaedic Surgery (2010), Volume 2, No. 1, 1 6 GUIDELINE Diagnosis and treatment of osteoarthritisos4_55 1..6 Chinese Orthopaedic Association Background Osteoarthritis (OA) is the most common form of
Orthopaedic Surgery (2010), Volume 2, No. 1, 1 6 GUIDELINE Diagnosis and treatment of osteoarthritisos4_55 1..6 Chinese Orthopaedic Association Background Osteoarthritis (OA) is the most common form of
Pain Management in the Canine Patient 10/31/16
 Laurie Edge-Hughes, BScPT, MAnimSt(Animal Physio), CAFCI, CCRT Laurie Edge-Hughes, BScPT, MAnimSt, CAFCI, CCRT 1 Thermal Therapy - HEAT Conduction e.g. Hot water bottle Convection e.g. Hair dryer or water
Laurie Edge-Hughes, BScPT, MAnimSt(Animal Physio), CAFCI, CCRT Laurie Edge-Hughes, BScPT, MAnimSt, CAFCI, CCRT 1 Thermal Therapy - HEAT Conduction e.g. Hot water bottle Convection e.g. Hair dryer or water
Available Strengths. Cost per Rx 325 mg tablet - $ mg tablet - $ mg ER tablet - $ mg capsule - $ mg chewable tablet
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY Non-Opioids LAST REVIEW 5/9/2017 THERAPEUTIC CLASS Pain REVIEW HISTORY 2/16, 5/15 LOB AFFECTED Medi-Cal (MONTH/YEAR) This
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY Non-Opioids LAST REVIEW 5/9/2017 THERAPEUTIC CLASS Pain REVIEW HISTORY 2/16, 5/15 LOB AFFECTED Medi-Cal (MONTH/YEAR) This
Osteoarthritis (OA), Safety & Efficacy of Glucosamine & Chondroitin in Osteoarthritis. Clinical studies. show these. agents are very.
, Safety & Efficacy of Glucosamine & Chondroitin in Osteoarthritis. Clinical studies. show these. agents are very.") FEATURE Safety & Efficacy of Glucosamine & Chondroitin in Osteoarthritis by DARRELL T. HULISZ, Pharm.D., R.Ph. Assistant Professor of Family Medicine Case Western Reserve University School of Medicine;
FEATURE Safety & Efficacy of Glucosamine & Chondroitin in Osteoarthritis by DARRELL T. HULISZ, Pharm.D., R.Ph. Assistant Professor of Family Medicine Case Western Reserve University School of Medicine;
Osteoarthritis: recent advances in diagnosis and management
 n DRUG REVIEW Osteoarthritis: recent advances in diagnosis and management Andrew Barr MRCP and Philip Conaghan PhD, FRACP, FRCP SPL Osteoarthritis represents a failure of joint tissue repair and can be
n DRUG REVIEW Osteoarthritis: recent advances in diagnosis and management Andrew Barr MRCP and Philip Conaghan PhD, FRACP, FRCP SPL Osteoarthritis represents a failure of joint tissue repair and can be
Managing Osteoarthritis Pain With Medicines. A Review of the Research for Adults
 Managing Osteoarthritis Pain With Medicines A Review of the Research for Adults Is This Summary Right for Me? Yes, if: A doctor* said you have osteoarthritis (pronounced ah-stee-oharth-rye-tis). Osteoarthritis
Managing Osteoarthritis Pain With Medicines A Review of the Research for Adults Is This Summary Right for Me? Yes, if: A doctor* said you have osteoarthritis (pronounced ah-stee-oharth-rye-tis). Osteoarthritis
ARTHRITIS. What happens when Arthritis goes untreated? Often people take arthritis to be a natural part of aging and do not seek medical advice.
 ARTHRITIS Move again with Life ARTHRITIS needn't control your life anymore Now you can control it. Joint pain, restricted joint mobility, joint swelling and inflammation can steal happiness from your life.
ARTHRITIS Move again with Life ARTHRITIS needn't control your life anymore Now you can control it. Joint pain, restricted joint mobility, joint swelling and inflammation can steal happiness from your life.
The causes of OA of the knee are multiple and include aging (wear and tear), obesity, and previous knee trauma or surgery. OA affects usually the
, obesity, and previous knee trauma or surgery. OA affects usually the") The Arthritic Knee The causes of OA of the knee are multiple and include aging (wear and tear), obesity, and previous knee trauma or surgery. OA affects usually the medial compartment of the knee, and
The Arthritic Knee The causes of OA of the knee are multiple and include aging (wear and tear), obesity, and previous knee trauma or surgery. OA affects usually the medial compartment of the knee, and
Anti-inflammatory drugs
 Anti-inflammatory drugs 1 Inflammatory process 1. stimulus (cut) 2. Initial local vasoconstriction( blood loss) 3. vasodilation, local immune/inflammatory reaction (heat, redness) 4. swelling and pain
Anti-inflammatory drugs 1 Inflammatory process 1. stimulus (cut) 2. Initial local vasoconstriction( blood loss) 3. vasodilation, local immune/inflammatory reaction (heat, redness) 4. swelling and pain
Update on Osteoarthritis
 Update on Osteoarthritis Ian McLeod, MS, MEd, PA-C, ATC Department of Physician Assistant Studies Northern Arizona University ASAPA Fall CME Conference 2018 ian.mcleod@nau.edu Objectives 1. Identify risk
Update on Osteoarthritis Ian McLeod, MS, MEd, PA-C, ATC Department of Physician Assistant Studies Northern Arizona University ASAPA Fall CME Conference 2018 ian.mcleod@nau.edu Objectives 1. Identify risk
WHAT S OSTEOARTHRITIS AND HOW CAN I MANAGE IT?
 WHAT S OSTEOARTHRITIS AND HOW CAN I MANAGE IT? What Osteoarthritis (OA)? Commonly referred to also as Degenerative Joint Disease (DJD) It is wear and tear arthritis very common in most of us as we age
WHAT S OSTEOARTHRITIS AND HOW CAN I MANAGE IT? What Osteoarthritis (OA)? Commonly referred to also as Degenerative Joint Disease (DJD) It is wear and tear arthritis very common in most of us as we age
Algorithm for Use of Non-steroidal Anti-inflammatories (NSAIDs)
") Algorithm for Use of Non-steroidal Anti-inflammatories (NSAIDs) Page 3 Publisher Conseil du médicament www.cdm.gouv.qc.ca Coordination Anne Fortin, Pharmacist Development Conseil du médicament Fédération
Algorithm for Use of Non-steroidal Anti-inflammatories (NSAIDs) Page 3 Publisher Conseil du médicament www.cdm.gouv.qc.ca Coordination Anne Fortin, Pharmacist Development Conseil du médicament Fédération
Best Practices in the Diagnosis and Management of OA
 Best Practices in the Diagnosis and Management of OA 1 Disclosure None 2 Objective To provide an approach to identify and treat people with OA in primary care clinical practice American College of Physicians
Best Practices in the Diagnosis and Management of OA 1 Disclosure None 2 Objective To provide an approach to identify and treat people with OA in primary care clinical practice American College of Physicians
Medications for Degenerative Arthritis
 House Paws Home Veterinary Care (651) 283-7216 housepawsmn@gmail.com Medications for Degenerative Arthritis Degenerative joint disease is the number one cause of chronic pain in dogs and cats. This condition
House Paws Home Veterinary Care (651) 283-7216 housepawsmn@gmail.com Medications for Degenerative Arthritis Degenerative joint disease is the number one cause of chronic pain in dogs and cats. This condition
Joint Injection Challenge The art of good injection therapy is to place the appropriate amount of the appropriate medication into the exact site of th
 The Art of the Injection By Jon C. Brillhart PA-C Daivd Lannik MD Portsmouth Orthopedics, Inc Joint Injection Challenge The art of good injection therapy is to place the appropriate amount of the appropriate
The Art of the Injection By Jon C. Brillhart PA-C Daivd Lannik MD Portsmouth Orthopedics, Inc Joint Injection Challenge The art of good injection therapy is to place the appropriate amount of the appropriate
LESSON ASSIGNMENT. Analgesic, Anti-Inflammatory, and Antigout Agents.
 LESSON ASSIGNMENT LESSON 4 Analgesic, Anti-Inflammatory, and Antigout Agents. TEXT ASSIGNMENT Paragraphs 4-1 through 4-8. LESSON OBJECTIVES 4-1. Given one of the following terms: analgesic, antipyretic,
LESSON ASSIGNMENT LESSON 4 Analgesic, Anti-Inflammatory, and Antigout Agents. TEXT ASSIGNMENT Paragraphs 4-1 through 4-8. LESSON OBJECTIVES 4-1. Given one of the following terms: analgesic, antipyretic,
Total Joint Replacement. Hip and Knee Pain Lawrence P. Johnson, MD Merrimack Valley Orthopedic Associates Lowell General Hospital
 Hip and Knee Pain Lawrence P. Johnson, MD Merrimack Valley Orthopedic Associates Lowell General Hospital This talk will touch upon the following topics: Understanding the Causes of Hip and Knee pain Treatment
Hip and Knee Pain Lawrence P. Johnson, MD Merrimack Valley Orthopedic Associates Lowell General Hospital This talk will touch upon the following topics: Understanding the Causes of Hip and Knee pain Treatment
Arthritis of the Knee
 Copyright 2007 American Academy of Orthopaedic Surgeons Arthritis of the Knee There are three basic types of arthritis that may affect the knee joint. Osteoarthritis Osteoarthritis (OA) is the most common
Copyright 2007 American Academy of Orthopaedic Surgeons Arthritis of the Knee There are three basic types of arthritis that may affect the knee joint. Osteoarthritis Osteoarthritis (OA) is the most common
COLCRYS-PST. Products Affected Step 1: Mitigare 0.6 mg capsule. Details. Step 2: Colcrys 0.6 mg tablet
 COLCRYS-PST Mitigare 0.6 mg capsule Colcrys 0.6 mg tablet Criteria If the patient has tried one Step 1 product, authorization for a Step 2 product may be given. Exceptions can be made for a step 2 drug
COLCRYS-PST Mitigare 0.6 mg capsule Colcrys 0.6 mg tablet Criteria If the patient has tried one Step 1 product, authorization for a Step 2 product may be given. Exceptions can be made for a step 2 drug
Diagnosis & Nonoperative Treatment of the Osteoarthritic Knee. Randall R Wroble MD Orthopedic One Columbus OH
 Diagnosis & Nonoperative Treatment of the Osteoarthritic Knee Randall R Wroble MD Orthopedic One Columbus OH There are 2 things a good doctor does First Step: Finds out what's wrong Second step Makes the
Diagnosis & Nonoperative Treatment of the Osteoarthritic Knee Randall R Wroble MD Orthopedic One Columbus OH There are 2 things a good doctor does First Step: Finds out what's wrong Second step Makes the
Elements for a Public Summary Overview of disease epidemiology
 VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Acute pain usually responds to medication and should settle in less than three months. Inadequate pain relief may lead to other
VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Acute pain usually responds to medication and should settle in less than three months. Inadequate pain relief may lead to other