Case Conference April 1, Melissa Spera, MD
|
|
|
- Esmond Waters
- 6 years ago
- Views:
Transcription
1 Case Conference April 1, 2014 Melissa Spera, MD
2 Chief Complaint Throat pain and neck swelling x 3 months
3 HPI 24 yr old man with no known past medical history who presented to ILH on 2/3/14 complaining of persistent throat and neck pain since November The patient reports that in Nov 2013 he began to experience right ear pain with bilateral ear fullness. He presented to OSH #1 at that time and was diagnosed with uvulitis and treated with a course of Amoxicillin/Clavulanate.
4 HPI The patient reported slight improvement in his symptoms following antibiotics His symptoms then continued to progress to include dysphagia to solids then to liquids with associated odynophagia. Other associated symptoms were night sweats, fevers, chills, fatigue and 30 lb weight loss attributed to decreased appetite and ability to eat. He presented to OSH #2 for further evaluation on 12/31/13 CT neck showed possible pharyngeal abscess and the patient was transferred to OSH #3 for ENT evaluation on 12/31/13
5 HPI On 1/3/14 he underwent bilateral tympanostomy tube placement with the finding of bilateral purulent otitis media During the procedure, the right tonsil was noted to be inflamed with evidence of parapharyngeal cellulitis Right sided tonsillectomy was also performed with exploration of the right upper parapharyngeal space No masses or abscesses were encountered Culture of ear drainage => slight coagulase negative staph The patient was treated with unknown IV antibiotics during hospitalization
6 HPI Repeat imaging of the neck was performed on 1/6/14 and showed possible mastoiditis with continued ill defined area of low attenuation in the right neck. The patient was discharged 1/6/14 with PO antibiotics and prednisone taper prescribed Referral was sent to LSU ENT from OSH #3
7 HPI The patient reported slight improvement in his symptoms following D/C with antibiotics and prednisone. Once treatment was completed his symptoms returned and progressed to include the following: Bilateral conjunctivitis Decreased vision in right eye Difficulty opening his mouth with right facial droop Nausea Dysuria Polyarthritis in his bilateral shoulders, knees, elbows and ankles
8 HPI The patient was seen in LSU ENT Clinic on 2/3/14 for his head and neck symptoms Sent by ENT to the ED for admission to establish a diagnosis and direct therapy
9 HPI Past medical history: as above Past surgical history : as above Family History Mother-alive-50 yo with asthma, bronchitis Father alive- 72 yo with CAD s/p stent placement
10 HPI-Social history Tobacco: 1 ppd x 5-10 years, quit Nov 2013 ETOH: 1-2 beers/day on weekends Illicit drug use: Marijuana Employment: Previously employed as a crab fisherman on Lake Pontchartrain Sexual History: Previous monogamous relationship with woman Currently lives with his mother in Robert, La Hobbies include hunting and fishing No pets, sick contacts, recent travel or insect bites
11 HPI Allergies: NKDA Medications: Hydrocodone acetaminophen mg syrup q6 hrs PRN pain Promethazine 6.25mg/ 5ml syrup q6 hrs PRN nausea Health Care Maintenance- Tdap, influenza -not up to date ROS-per HPI
12 Physical Exam BP 118/78 Pulse 107 Temp 99.5 F Resp 20 SpO2 99% Ht 1.88 m (6' 2") Wt kg (236 lb) BMI kg/m2 BP 116/70 Pulse 95 Temp F Resp 17 SpO2 97% General: AAOx4, appeared uncomfortable HEENT: Ophtho: Bilateral mild ptosis, right pupil 3mm to 2mm, left 5mm to 3mm both reactive to light, bilateral conjunctivitis without exudate No papilledema, no AV nicking, macula flat OP: Evidence of right tonsillectomy, good dentition, no oral lesions noted, + trismus Neck: Trachea midline, slight swelling of right neck, no masses palpated Cardiac: Regular rate and rhythm, no murmurs, no rubs, no S3, no S4 Resp: Clear to auscultation bilaterally, no wheezes, no rhonchi, no crackles, symmetric chest expansion
13 Physical Exam continued Abdomen: Non distended; normoactive bowel sounds; soft, non tender, no rebound, no guarding GU: Negative for penile lesions, and discharge. No testicular masses or lesions Rectal: Good rectal tone, no stool in the vault, no masses palpated, no blood or melena present Lower extremities: No clubbing, cyanosis or edema, 2+ DP pulse bilaterally Neuro: Intact eye closure, head turn and shoulder shrug, smile limited by trismus, tongue midline, intact sensation in V1, 2, 3, 5/5 strength in bilateral upper and lower extremities Skin: No rashes, wounds, or jaundice Lymph: No cervical, axillary or inguinal lymphadenopathy
14 Laboratory Findings Na K Cl CO2 BUN Cr Gluc Ca 132 meq/l ( meq/l) 4.5 meq/l 96 meq/l 25 meq/l 15 mg/dl 0.71mg/dL 107 mg/dl 9.2 mg/dl
15 Laboratory Findings WBC 9.8 K/uL Hemoglobin 11.8 g/dl ( g/dl) Hematocrit 35.2% (40-51%) Platelets 565 K/uL ( K/uL) MCV 88.7fL RDW 12.6% Neutrophils 78 % Bands 0 % Lymphocytes 10 % Monocytes 6 % Eosinophils 5 % (AEC >450)
16 Laboratory Findings Total protein 7.2 g/dl Albumin 3.0 g/dl ( g/dl) Total bilirubin 1.2 mg/dl AST 19 IU/L Alkaline Phosphatase 70 IU/L ALT 25 IU/L PT 16.1 sec ( sec) INR 1.5 ( ) CRP LDH 21.9 mg/dl (<0.90 mg/dl) 139 IU/L
17 Laboratory Findings Urinalysis ph 8.0 SG Clear, yellow Protein 25 Glucose normal Ketones negative Blood 250 Nitrites negative Uro bilinogen 4.0 Leukocytes negative Urine Microscopic > 100 RBC 6-10 WBC Sqam. epithelial cells 2-20 Bacteria negative Casts 0-2
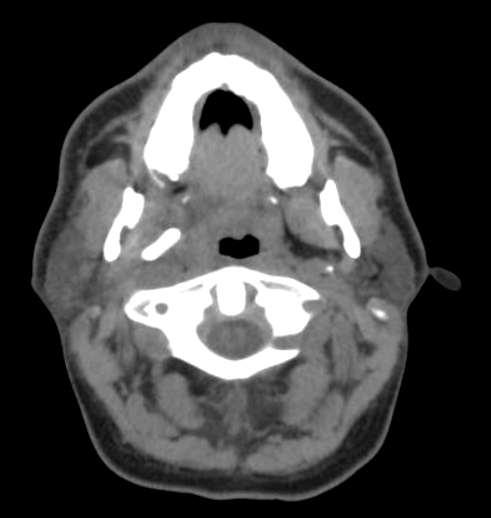
18 CT head with IV contrast


19
20 Hospital Course Admitted to ENT on the evening of 2/3/14 General Medicine Consult Service, Infectious Disease, Hematology Oncology, Ophthalmology and IR consulted
21 Hospital Course 2/4/14 IR felt the mass was too ill defined for ultrasound or CT guided tissue biopsy All services agreed tissue biopsy was necessary to establish diagnosis
22 Hospital Course 2/4 Ophthalmology evaluation Conjunctivitis likely due to blepharitis vs Dry Eye Syndrome Could not rule out iritis Artificial tears with erythromycin ointment started Anisocoria Idiopathic vs due to pharyngeal mass involvement
23 Hospital Course evening 2/5 Temperature of F recorded Vancomycin and piperacillin-tazobactam started Blood cultures drawn 2/3 were NGTD Patient with persistent eosinophilia: >450 absolute eosinophil count on 2/4 and 2/5 Further imaging including MRI orbit, face and neck performed
24 MRI Head with and without IV contrast


25


26
27 Hospital Course 2/6/14 Taken to OR on 2/6/14 by ENT for full neck exploration Reactive parapharyngeal lymph nodes and parapharyngeal fat were noted No obvious abscess found Tissue specimens sent to pathology Samples included parapharyngeal mass, lymph nodes and medial pterygoid JP drain was left in place
28
29 Pathology from neck exploration

30 Lymph node, reactive lymphoid hyperplasia, sinus histiocytosis, presence of neutrophils and eosinophils.

31 Lymph node, reactive lymphoid hyperplasia, highpower view, abundant eosinophils in the sinuses.

32 Pterygoid muscle, eosinophilic myositis, skeletal muscle with eosinophilic infiltration, muscle destruction and regeneration.

33 Pterygoid muscle, eosinophilic myositis, highpower view, abundant eosinophils evidence of muscle destruction

34 Parapharyngeal mass. Fibroadipose tissue with mixed inflammation including plasma cells and abundant eosinophils.

35 Parapharyngeal mass. High-power view. Mixed inflammatory infiltrate with abundant eosinophils.
36 Hospital Course 2/7/14 Preliminary comments from pathology => possible vasculitis Further work up for vasculitis initiated Tissue cultures and blood cultures remained NGTD; AFB smear negative
37 Hospital Course 2/7/14 Renal function worsened overnight from Cr 0.81 to 1.99 Work up for AKI was initiated FENA was 0.43 => thought to be pre renal azotemia from decreased PO intake vs contrast induced UA was repeated and hematuria was still present No urine eosinophils were present Renal ultrasound => non specific echo texture of the renal parenchyma likely due to medical renal disease.
38 Hospital Course 2/8/14 Creatinine continued to worsen => increasing from 1.99 to 2.63 despite IVF Vancomycin and piperacillin-tazobactam discontinued Renally dosed imipenem-cilastatin was initiated at 250mg IV q 8 hours Nephrology was consulted
39 Hospital Course 2/9/14 Creatinine peaked at 3.28 Urine specimen centrifuged by Nephrology Too numerous to count RBC s with dysmorphic RBC s present Serologic work up to further evaluate renal failure was initiated

40 Creatinine trend
41 Hospital Course 2/10-2/11 Worsening creatinine, proteinura and hematuria Patient consents to renal biopsy INR found to be 1.8 Patient received FFP and vitamin K INR decreased to 1.5 IR plans for renal biopsy
42 Hospital Course 2/11 Anti proteinase 3 antibody returns as positive Concern for underlying ANCA associated vasculitis Patient is questioned further He reports recurrent sinusitis symptoms which began at age 18 yrs History of nasal crusting Occasional epistaxis No history of asthma, nasal polyps, or necrotizing nasal lesions
43 Hospital Course Methylprednisolone 1 gram IV daily was started x 3 days by renal on 2/11 to prevent further worsening of renal function Renal biopsy performed 2/12
44 Renal Biopsy Slides courtesy of S Meleg-Smith, MD, Tulane nephropathology

45 Glomerulus tubules HE stain

46 ATN RBC Granular cast Epith necrosis HE stain

47 Loops OK Inflammation Epithelial proliferation Fibrin necrosis HE stain

48 Epithelial proliferation necrosis OK Silver stain

49 Necrosis Red cell cast OK Jones Silver stain Epithelial proliferation

50 Antiserum to human fibrin Antiserum to human fibrin Crescent Crescent Negative Negative glomerulus glomerulus

51 Fibrin Positive In Segmental necrosis of glomerulus

52 suggestive of fibrin thrombi in glomerulus cannot rule out segmental necrosis

53 Loops with well preserved foot processes
54 R Final diagnosis: Focal segmental necrotizing glomerulonephritis pauci -IC, i.e. neg IC
55 Laboratory Findings C3 complement 160mg/dl C4 complement 12mg/dl (18-55mg/dl) Anti streptolysin O titer 61 IU/mL ANA Screen Negative Anti mitochondrial antibody 5.7 Units Anti proteinase (PR-3) antibody >8 AI (<1.0 AI) Anti myeloperoxidase antibody <0.2 AI (<1.0 AI) Anti GBM antibody <0.2 AI Rheumatoid Factor 948 IU/mL (<20 IU/mL) TP/Creatinine ratio 849mg/g (<200mg/g) Serum protein electrophoresis Negative Urine protein electrophoresis Negative
56 Laboratory Finding C-ANCA 1:80 (<1:20) P-ANCA <1:20 Atypical ANCA <1:20 Serum IgG 839 mg/dl IgG1 412 mg/dl( mg/dl) IgG2 355 mg/dl IgG3 55 mg/dl IgG4 94 mg/dl T Spot TB Negative IgE 723 IU/mL
57 Preliminary Diagnosis 2/13 Once renal biopsy preliminary results known => Rheumatology was consulted ANCA associated vasculitis Eosinophilic Granulomatosis Polyangiitis (EGPA) vs Granulomatosis Polyangiitis (GPA) Patient underwent echo to evaluate for EGPA cardiac involvement Echo 2/14 showed left ventricular enlargement with normal valves, normal systolic and diastolic function, LVEF> 55%, PAP < 35 mm Hg
58 Treatment 2/13 The patient was started on prednisone 60mg PO q 24 hours with plans to taper with azathioprine 50mg PO q 12 hours The patient was discharged 2/14/14 with follow up
59 Hospital Follow up 2/26-2/27 Follow up in Rheumatology and Renal Clinics Patient reports feeling better with improved swallowing He has noticed facial and lower extremity edema and a 30lb weight gain He was noted to have 2+ pitting edema on physical exam
60 Laboratory Findings 2/26 Na K Cl CO2 BUN Cr Gluc Ca 142 meq/l 4.6 meq/l 106 meq/l 29 meq/l 47mg/dL 2.32mg/dL (2 weeks prior 1.85 mg/dl) 115 mg/dl 8.9 mg/dl
61 Follow up 2/26-2/27 Nephrotic range proteinuria with protein/creatinine ration 4235 mg/g Azathioprine was increased to 100mg BID Prednisone continued at 60mg daily Furosemide 40mg daily initiated
62 Follow up 3/6-3/10 Labs drawn 3/6/14 shows creatinine increased from 2.32 to 2.44 mg/dl Worsening TP/Cr ratio from 4235 to 5221 mg/g Rituximab infusion was initiated on 3/10/14, second dose received 3/17/14, and third dose on 3/24/14
63 Final Diagnosis ANCA associated vasculitis
64 ANCA Associated Vasculitis ANCA are highly specific for a group of disorders associated with vascular inflammation Include the following: Granulomatosis Polyangiitis (GPA) Microscopic polyangiitis (MPA) Churg-Strauss syndrome. The term "ANCA-associated vasculitis" may be misleading since NOT all patients with clinical (and even histopathologically proven) diagnoses have ANCA. 85% with GPA have ANCA 70% with MPA have ANCA 50% with Churg-Strauss syndrome have ANCA
65 Granulomatous Polyangiitis (GPA) Complex, immune-mediated disorder Tissue injury results from: Interplay of an initiating inflammatory event and Highly specific immune response. Part of this response is directed against previously shielded epitopes of neutrophil granule proteins Leading to autoantibodies known as antineutrophil cytoplasmic antibodies (ANCA). ANCA are directed against antigens present within the primary granules of neutrophils and monocytes The most commonly identified and evaluated antigens in GPA are: Proteinase 3 (PR3) Observed in 70 to 80 percent of patients Myeloperoxidase (MPO) Observed in 10 percent of patients These antibodies produce tissue damage via interactions with primed neutrophils and endothelial cells.
66 Granulomatous Polyangiitis (GPA) The events that MAY lead to the initiation of GPA are obscure and include: Infection Genetic factors Met with limited success Environmental factors Drugs Exact relationships between environmental exposures and vasculitis are complicated by difficulties in obtaining reliable measurements of exposures Rifampicin, allopurinol, hydralazine, propylthiouracil, aminoguanidine reported to cause ANCA seroconversion Particularly thiol and hydrazine containing compounds Combo of all
67 Granulomatous Polyangiitis (GPA) GPA and MPA have similar clinical presentations Mostly occur in older adults and both genders are equally affected. Far more common among white individuals. Typically present with constitutional symptoms including: Fever, migratory arthralgias, malaise, anorexia and weight loss. Prodromal symptoms may last for weeks to months without evidence of specific organ involvement.
68 Granulomatous Polyangiitis (GPA) Specific Organ System involvement Ears, Nose, and Throat manifestations include: Crusting, sinusitis, otitis media, persistent rhinorrhea, and purulent/bloody nasal discharge More common in patients with GPA Estimated frequency 90% in GPA versus 35% in MPA GPA more typically have evidence of: Bony and cartilage destruction resulting in saddle nose deformity Upper airway and orbital masses Cranial nerve entrapment and Subglottic disease
69 Granulomatous Polyangiitis (GPA) Pulmonary manifestations Either GPA or MPA may present with involvement of airways or pulmonary parenchyma causing: Hoarseness, cough, dyspnea, stridor, wheezing, hemoptysis or pleuritic pain Sometimes accompanied by signs of tracheal or subglottic stenosis, pulmonary consolidation and/or pleural effusion. The chest x-ray findings are variable. Common manifestations include nodules, patchy or diffuse opacities and fleeting pulmonary infiltrates, and hilar adenopathy
70 Granulomatous Polyangiitis (GPA) Renal manifestations is common in GPA and MPA Can present as: Asymptomatic hematuria or Acute kidney injury with hematuria and cellular casts, Variable degree of proteinuria that is usually subnephrotic. Histologically, renal biopsy findings in GPA and MPA generally parallel the severity of the clinical presentation ranging from: Mild focal and segmental glomerulonephritis in Patients with asymptomatic hematuria and normal or near-normal renal function Diffuse necrotizing and crescentic glomerulonephritis Patients with acute kidney injury In most patients, the glomerulonephritis is associated with few or no immune deposits in the glomeruli Pauci-immune glomerulonephritis
71 Granulomatous Polyangiitis (GPA) Cutaneous manifestations occur in about one-half of patients with GPA or MPA. The most common skin lesion is leukocytoclastic angiitis Causes purpura involving the lower extremities May be accompanied by focal necrosis and ulceration. Skin lesions may also include urticaria, livida reticularis, and tender nodules Other manifestations include: Eyes Conjunctivitis, corneal ulceration, episcleritis/scleritis, optic neuropathy, nasolacrimal duct obstruction, proptosis, diplopia, retinal vasculitis, and uveitis Nervous system Mononeuritis multiplex, cranial nerve abnormalities, central nervous system mass lesions, external ophthalmoplegia, hearing loss Patients with ANCA vasculitis have a high incidence of DVT.
72 Granulomatous Polyangiitis (GPA) Prompt diagnosis of GPA or MPA is important to permit initiation of therapy that may be life saving and organ sparing. Diagnosis of vasculitis is strongly suggested in patients with: Suggestive clinical findings Positive ANCA test False positive and negative results may be obtained. Ultimately histologic examination of tissue is needed to make definitive diagnosis Obtained by biopsy of an affected organ Generally either skin, kidney or lung. Patients should be treated empirically if: Clinical suspicion for ANCA vasculitis is high and Tissue diagnosis cannot be obtained in a timely manner.
73 Granulomatous Polyangiitis (GPA) Several attempts made to standardize the classification and diagnostic criteria for small vessel vasculitis. Classification algorithms have important limitations. None of the algorithms reliably distinguish between GPA and MPA in all patients. Alternative approach to classification based upon ANCA serology uses the terms: "proteinase 3 ANCA disease," "myeloperoxidase ANCA disease," and "seronegative ANCA disease." With this approach, no diagnostic criteria are needed other than serological findings. Proteinase 3 ANCA and myeloperoxidase ANCA have more prognostic significance than the terms MPA and GPA with respect to response to therapy, propensity for relapse, and patient outcome
74 Granulomatous Polyangiitis (GPA) The American College of Rheumatology (ACR) 1990 criteria Chapel Hill Consensus Conference (CHCC) criteria European Medicines Agency algorithm The distinction of ANCA vasculitis from other systemic rheumatic diseases is a frequent clinical problem. Includes diseases with similar general clinical features, similar lung and/or renal signs, and/or positive ANCA serologies Evaluation must be undertaken to assess other potential diagnoses
75 Granulomatous Polyangiitis (GPA) Induction of complete remission is the goal of immunosuppressive therapy in GPA or MPA Defined as the absence of active disease. Approach to initial therapy depends upon the severity of the disease and the organ systems involved. From an initial therapeutic perspective, there are essentially two groups: Mild disease No evidence for "active" glomerulonephritis Normal serum creatinine and no red cell casts or proteinuria No organ-threatening or life-threatening manifestations Absence of pulmonary hemorrhage, cerebral vasculitis, progressive neuropathy, orbital pseudotumor, gastrointestinal bleeding, pericarditis, or myocarditis Moderate to severe disease Other patients with GPA or MPA are classified into this group for the purposes of initial therapy. May have organ-threatening or life-threatening manifestations, including (but not limited to) marked pulmonary hemorrhage or rapidly deteriorating renal function.
76 Granulomatous Polyangitis (GPA) Choice of Therapy Mild disease Glucocorticoids in combination with methotrexate (Grade 2C). Rather than other therapies or glucocorticoids alone Failure to respond to methotrexate or who have progressive disease should be treated with: Either cyclophosphamide or rituximab.
77 Granulomatous Polyangiitis (GPA) Choice of Therapy Moderate to severe disease Glucocorticoids in combination with either cyclophosphamide (oral or intravenous) or rituximab (Grade 1A). Rather than other therapies or glucocorticoids alone Cannot take or refuse to take cyclophosphamide then initial immunosuppressive therapy with rituximab and glucocorticoids (Grade 1B). Plasma exchange in addition to cyclophosphamide and glucocorticoid therapy (Grade 2C) for patients with GPA or MPA who have one or more of the following: Serum creatinine above 5.7 Requirement for dialysis Pulmonary hemorrhage And/or a positive anti-glomerular basement membrane (anti-gbm) antibody. Consider prophylaxis against opportunistic infections during induction therapy Suggested regimen varies with the regimen used for initial immunosuppression.
78 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) Previously called the Churg-Strauss syndrome (CSS) or allergic granulomatosis and angiitis Multisystem disorder characterized by: Allergic rhinitis Asthma Prominent peripheral blood eosinophilia cells/microl and/or >10% eosinophils on differential leukocyte count The most commonly involved organ is the lung, followed by the skin. Can affect any organ system, including: Cardiovascular, gastrointestinal, renal, and central nervous systems. Vasculitis of extrapulmonary organs is largely responsible for the morbidity and mortality associated with EGPA.
79 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) The exact etiology is unknown. ANCA is detected in about 40 to 60 percent of patients EGPA is classified among the ANCA-positive vasculitides. Least common of the three (MPA and GPA) Several other abnormalities in immunologic function occur, including: Heightened Th1 and Th2 lymphocyte function Determined by prominence of allergic features (allergic rhinitis, asthma, and positive skin tests) and pulmonary angiocentric granulomatosis respectively Increased eosinophil recruitment and Decreased eosinophil apoptosis.
80 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) Genetic factors HLA class and certain interleukin-10 polymorphisms may play a role pathogenesis. Association with Medications Leukotriene modifying agents, inhaled glucocorticoids, and omalizumab Appears association most likely due to unmasking of the underlying disease or intensification of therapy in a patient with escalating EGPA, rather than a causal relationship. Cocaine EGPA-like illness can rarely occur after the use of free base cocaine. ANCAs associated with cocaine use recognize different target proteases than the typical ANCAs associated with EGPA.
81 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) The major histopathologic findings of EGPA from any affected organ include the following: May not all be present Eosinophilic infiltration Prominent and sometimes extensive areas of necrosis Eosinophilic, giant cell vasculitis Especially of the small arteries and veins Interstitial and perivascular necrotizing granulomas
82 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) Clinical features typically develop in several sequential phases Although these phases are not always clearly distinguishable Prodromal phase Occurs in the second and third decades of life Characterized by atopic disease, allergic rhinitis, and asthma. Eosinophilic phase Features include peripheral blood eosinophilia and eosinophilic infiltration of multiple organs Especially the lung and gastrointestinal tract. Almost 40 percent of patients with EGPA present with pulmonary opacities, asthma, and peripheral eosinophilia prior to the development of a systemic vasculitis (polyangiitis). Vasculitic phase Third and fourth decades of life Life-threatening systemic vasculitis of the medium and small vessels Often associated with vascular and extravascular granulomatosis. May be heralded by nonspecific constitutional symptoms and signs Especially fever, weight loss, malaise, and lassitude.
83 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) Pulmonary disease Asthma is the cardinal clinical feature and present in more than 90% of patients Usually precedes the vasculitic phase by approximately 8 to 10 years Suspect in patients whose asthma is poorly controlled on moderate doses of inhaled glucocorticoids Prolonged treatment of asthma with glucocorticoid therapy may partially or totally suppress the usual clinical signs of untreated EGPA. Disease may therefore not become evident until glucocorticoids are reduced or stopped Other pulmonary findings are reported in 50 to 70 percent of patients include: Pulmonary opacities with eosinophilia, pleural effusion (often eosinophilic), nodules that are rarely cavitary, and alveolar hemorrhage
84 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) Other organ involvement Ears, Nose and Throat Serous otitis, allergic rhinitis, nasal obstruction, recurrent sinusitis, and nasal polyposis, is reported in 48 percent of patients Neurologic A peripheral neuropathy, usually mononeuritis multiplex, is seen in up to 75 percent of patients with EGPA. Skin Two-thirds of EGPA patients have skin involvement ranging from palpable purpura to subcutaneous nodules. Skin biopsy is often helpful for confirming the diagnosis. Renal Varies in studies with largest having 22% involvement GI Can have eosinophilic gastroenteritis Cardiac One of the more serious manifestations, accounting for approximately one-half of deaths attributable to EGPA. Suspected in the presence of refractory dyspnea, clinical evidence of heart failure, or cardiac rhythm abnormalities, but can also be asymptomatic.
85 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) Labs There are no laboratory tests that are specific for EGPA Although eosinophilia is characteristic Obtain a complete cell count with differential, a total eosinophil count, and an IgE level. Also usually obtain an ANCA test Imaging Although the sensitivity and specificity are low Chest radiographic abnormalities are variable and diverse. High resolution computed tomography (HRCT) of chest findings include: Patchy parenchymal consolidation or ground glass opacification; nodules may also be noted
86 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) The ACR has established six criteria for the classification of EGPA in a patient with documented vasculitis The presence of four or more of these criteria had a sensitivity of 85 percent and a specificity of 99.7 percent: Asthma (a history of wheezing or the finding of diffuse high pitched wheezes on expiration) Greater than 10 percent eosinophils on the differential leukocyte count Mononeuropathy (including multiplex) or polyneuropathy Migratory or transient pulmonary opacities detected radiographically Paranasal sinus abnormality Biopsy containing a blood vessel showing the accumulation of eosinophils in extravascular areas

87
88 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) The diagnosis of EGPA is typically suspected based on the clinical findings Eosinophilia 1500/microL, asthma, allergic rhinitis. Confirming the diagnosis is often difficult because of the following confounding factors: Individual manifestations of the syndrome can occur in isolation. Lung parenchymal involvement is not universal. Some manifestations can exist for many years before additional features become clinically apparent. Classified as a vasculitis but only 40 to 60% have ANCA. Many biopsies do not show a necrotizing vasculitis or granuloma, but rather an apparently nondestructive infiltration of vessel walls by eosinophils
89 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) EGPA patients with evidence of systemic vasculitis Systemic glucocorticoid therapy (Grade 1A) daily for 6 to 12 weeks, or until disease remission is attained, and then gradually tapered. Patients with fulminant disease may require initial therapy with intravenous glucocorticoids. For patients with severe disease manifest by a FFS of 2: Addition of cyclophosphamide to systemic glucocorticoid therapy (Grade 1B). For patients with a FFS of 1 Especially with cardiac or central nervous system involvement Addition of cyclophosphamide to systemic glucocorticoids (Grade 2C).
90 Eosinophilic Granulomatosis with Polyangiitis (EGPA/Churg-Strauss) After induction of remission with cyclophosphamide Transition to maintenance therapy with azathioprineto sustain the remission (Grade 1B). Methotrexate and leflunomide are alternative agents that can be used if azathioprine is not tolerated or is not effective. These drugs are preferred to long-term cyclophosphamide therapy Associated with significantly greater toxicity Continue maintenance immunosuppressive therapy for 12 to 18 months. Longer term or indefinite maintenance therapy may be warranted in patients with multiple relapses Concurrent glucocorticoid therapy (prednisone or equivalent) (Grade 1C) is recommended for maintenance therapy. Glucocorticoid is gradually tapered to the lowest dose required for control of symptoms and signs of active EGPA
91 References Levine, SM, Stone, JH; Pathogenesis of granulomatosis with polyangiitis (Wegener's) and related vasculitides; UpToDate; 12/2013. Falk, RJ, King TE, Stone, JH; Clinical manifestations and diagnosis of granulomatosis with polyangiitis (Wegener's) and microscopic polyangiitis, UpToDate; 1/2014. Stone, JH, Kaplan, AA, Falk RJ; Initial immunosuppressive therapy in granulomatosis with polyangiitis and microscopic polyangiitis; Uptodate; 3/2014. King, TE; Epidemiology, pathogenesis, and pathology of eosinophilic granulomatosis with polyangiitis (Churg- Strauss); UpToDate, 1/2014. King, TE; Clinical features and diagnosis of eosinophilic granulomatosis with polyangiitis (Churg-Strauss); UpToDate; 1/2014. King, TE; Treatment and prognosis of eosinophilic granulomatosis with polyangiitis (Churg-Strauss); UpToDate; 7/2013.
SHO Teaching. Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth
 SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
Case Presentation. Rafid Asfar, MD
 Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Management of Acute Vasculitis. CMT teaching 3 rd June 2015 Caroline Wroe
 Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
VASCULITIS. Case Presentation. Case Presentation
 VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Case Presentation VASCULITIS. Case Presentation. Case Presentation. Vasculitis
 Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Atlas of the Vasculitic Syndromes
 CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
PAEDIATRIC VASCULITIS
 PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
Rituximab treatment for ANCA-associated vasculitis in childhood
 Rituximab treatment for ANCA-associated vasculitis in childhood DISCLOSURE I have no relevant financial relationships to disclose Katharine Moore MD Nov 14, 2012 University of Colorado School of Medicine
Rituximab treatment for ANCA-associated vasculitis in childhood DISCLOSURE I have no relevant financial relationships to disclose Katharine Moore MD Nov 14, 2012 University of Colorado School of Medicine
RAPIDLY FAILING KIDNEYS. Dr Paul Johny 2 nd yr DNB Medicine Resident
 RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS
 GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
Vasculitis. Edward Dwyer, M.D. Division of Rheumatology. Vasculitis
 Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Granulomatosis with Polyangiitis (Wegener s)
") August 2011 Granulomatosis with Polyangiitis (Wegener s) Andrew Noll, Harvard Medical School, Year III Agenda Patient presentation Overview of granulomatosis with polyangiitis (Wegener s), abbreviated
August 2011 Granulomatosis with Polyangiitis (Wegener s) Andrew Noll, Harvard Medical School, Year III Agenda Patient presentation Overview of granulomatosis with polyangiitis (Wegener s), abbreviated
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
CHECK LIST FORM-MONTH 27 (Please note Month 27 is from enrolment not randomisation)
") CHECK LIST FORM-MONTH 27 (Please note Month 27 is from enrolment not randomisation) Participant Initials: Date of Birth: Were the following forms completed for this visit? Follow Up Form Done t Done BVASWG
CHECK LIST FORM-MONTH 27 (Please note Month 27 is from enrolment not randomisation) Participant Initials: Date of Birth: Were the following forms completed for this visit? Follow Up Form Done t Done BVASWG
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Scleritis LEN V KOH OD
 Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Disclosures. Objectives. Vasculitis: What The Primary Care Physician Needs To Know. Definition & Classification of Vasculitis
 Vasculitis: What The Primary Care Physician Needs To Know Lynn Fussner, MD Assistant Professor - Clinical Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Vasculitis: What The Primary Care Physician Needs To Know Lynn Fussner, MD Assistant Professor - Clinical Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Vasculitis: What The Primary Care Physician Needs To Know. Lynn Fussner, MD
 Vasculitis: What The Primary Care Physician Needs To Know Lynn Fussner, MD Assistant Professor - Clinical Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Vasculitis: What The Primary Care Physician Needs To Know Lynn Fussner, MD Assistant Professor - Clinical Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
RATIONALE. K Without therapy, ANCA vasculitis with GN is associated. K There is high-quality evidence for treatment with
 http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
December 6, 2010 Asthma and Rheumatic Disorders and Vasculitis
 December 6, 2010 Asthma and Rheumatic Disorders and Vasculitis Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
December 6, 2010 Asthma and Rheumatic Disorders and Vasculitis Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
AKI Case study -Vasculitis. Sarah Mackie Renal Practice Development Nurse King s College Hospital - London
 AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
VCRC-OMERACT ANCA-Vasculitis Outcome Measure Initiative Comparative Outcome Measure Exercise-Training Cases
 Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
CARDIOVASCULAR CASE-BASED SMALL GROUP DISCUSSION
 MHD I Session VIII Student Copy Page 1 CARDIOVASCULAR CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION VIII OCTOBER 22, 2014 STUDENT COPY MHD I Session VIII Student Copy Page 2 Case 1 Chief Complaint I
MHD I Session VIII Student Copy Page 1 CARDIOVASCULAR CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION VIII OCTOBER 22, 2014 STUDENT COPY MHD I Session VIII Student Copy Page 2 Case 1 Chief Complaint I
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
Small Vessel Vasculitis
 Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
EULAR/ERA-EDTA recommendations for the management of ANCAassociated
 EULAR/ERA-EDTA recommendations for the management of ANCAassociated vasculitis Dr. Meharunnisha Syed III year DNB Resident (General Medicine) Narayana Health-MSH Fifteen recommendations were developed,
EULAR/ERA-EDTA recommendations for the management of ANCAassociated vasculitis Dr. Meharunnisha Syed III year DNB Resident (General Medicine) Narayana Health-MSH Fifteen recommendations were developed,
Wegener s Granulomatosis JUN-KI PARK
 Wegener s Granulomatosis JUN-KI PARK Definition History Epidemiology Clinical symptoms Pathophysiology Treatment Wegener granulomatosis (WG) is a complex, immunemediated disorder, which along with microscopic
Wegener s Granulomatosis JUN-KI PARK Definition History Epidemiology Clinical symptoms Pathophysiology Treatment Wegener granulomatosis (WG) is a complex, immunemediated disorder, which along with microscopic
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
GPA & MPA GRANULOMATOSIS WITH POLYANGIITIS &MICROSCOPIC POLYANGIITIS. What you need to know about GPA & MPA
 GRANULOMATOSIS WITH POLYANGIITIS &MICROSCOPIC POLYANGIITIS GPA & MPA This medical guide is designed for educational purposes to help patients understand GPA & MPA. Please consult your doctor on specific
GRANULOMATOSIS WITH POLYANGIITIS &MICROSCOPIC POLYANGIITIS GPA & MPA This medical guide is designed for educational purposes to help patients understand GPA & MPA. Please consult your doctor on specific
VASCULITIC SYNDROMES. Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018
 VASCULITIC SYNDROMES Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018 2012 REVISED CHAPEL HILL CONSENSUS CONFERENCE Large vessel Takayasu arteritis Giant cell arteritis Medium Vessel Polyarteritis
VASCULITIC SYNDROMES Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018 2012 REVISED CHAPEL HILL CONSENSUS CONFERENCE Large vessel Takayasu arteritis Giant cell arteritis Medium Vessel Polyarteritis
Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management
 Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management") AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Rheumatology Primer: What Labs and When
 Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Protocol Version 2.0 Synopsis
 Protocol Version 2.0 Synopsis Title Short Title Plasma exchange and glucocorticoid dosing in anti-neutrophil cytoplasm antibody associated vasculitis: a randomized controlled trial. PEXIVAS PEXIVAS Clinical
Protocol Version 2.0 Synopsis Title Short Title Plasma exchange and glucocorticoid dosing in anti-neutrophil cytoplasm antibody associated vasculitis: a randomized controlled trial. PEXIVAS PEXIVAS Clinical
GRANULOMATOSIS WITH POLYANGIITIS
 What is granulomatosis with polyangiitis (GPA)? Granulomatosis with polyangiitis (GPA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict
What is granulomatosis with polyangiitis (GPA)? Granulomatosis with polyangiitis (GPA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict
EDITORIAL. Issue Seventeen, October Editorial Team. Issue Seventeen. Info link
 EDITORIAL, October 2004 Welcome to the Spring 2004 Edition of InfoLink. The feature article in this edition has been written by Dr Rodger Laurent, Head of Department, PaLMS Rheumatology Laboratory. The
EDITORIAL, October 2004 Welcome to the Spring 2004 Edition of InfoLink. The feature article in this edition has been written by Dr Rodger Laurent, Head of Department, PaLMS Rheumatology Laboratory. The
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Pharmacy Management Drug Policy
 SUBJECT: : Nucala (mepolizumab), Cinqair (reslizumab), & Fasenra (benralizumab) POLICY NUMBER: Pharmacy-62 EFFECTIVE DATE: 12/15 LAST REVIEW DATE: 3/5/2018 If the member s subscriber contract excludes
SUBJECT: : Nucala (mepolizumab), Cinqair (reslizumab), & Fasenra (benralizumab) POLICY NUMBER: Pharmacy-62 EFFECTIVE DATE: 12/15 LAST REVIEW DATE: 3/5/2018 If the member s subscriber contract excludes
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ANCA-associated systemic vasculitis (AASV)
") PAPER 2007 Royal College of Physicians of Edinburgh ANCA-associated systemic vasculitis (AASV) 1 DC Kluth, 2 J Hughes 1 Reader in Nephrology, MRC Centre for Inflammation Research, University of Edinburgh,
PAPER 2007 Royal College of Physicians of Edinburgh ANCA-associated systemic vasculitis (AASV) 1 DC Kluth, 2 J Hughes 1 Reader in Nephrology, MRC Centre for Inflammation Research, University of Edinburgh,
a mimicker of Wegener s Granulomatosis
 a mimicker of Wegener s Granulomatosis Combined Meeting October 2009 a story of 2 ladies Madam JA 56 year-old Madam RH 36 year-old Madam JA 56 year-old Apr 2008 May Jun Jul Aug Sept Oct Nov 2008 Madam
a mimicker of Wegener s Granulomatosis Combined Meeting October 2009 a story of 2 ladies Madam JA 56 year-old Madam RH 36 year-old Madam JA 56 year-old Apr 2008 May Jun Jul Aug Sept Oct Nov 2008 Madam
The Vasculitis Syndromes
 The Vasculitis Syndromes Definition Inflammation and damage of blood vessels Single organ skin Several organ systems Primary Secondary Heterogeneity Overlap Primary Vasculitis Syndromes Wegener s granulomatosis
The Vasculitis Syndromes Definition Inflammation and damage of blood vessels Single organ skin Several organ systems Primary Secondary Heterogeneity Overlap Primary Vasculitis Syndromes Wegener s granulomatosis
Overview. = inflammation of vessel wall. Symptoms and signs depend on the tissue of which the vessels are affected
 Vasculitis (1+2) Overview = inflammation of vessel wall Symptoms and signs depend on the tissue of which the vessels are affected Often with systemic symptoms fever, myalgia, arthralgia, malaise etc. Most
Vasculitis (1+2) Overview = inflammation of vessel wall Symptoms and signs depend on the tissue of which the vessels are affected Often with systemic symptoms fever, myalgia, arthralgia, malaise etc. Most
Immune-mediated lung disease. Ian Sabroe
 Immune-mediated lung disease Ian Sabroe It s all immune? Diseases that doesn t have immune involvement? The processes of response to injury and tissue repair are key homeostatic pathways involved in all
Immune-mediated lung disease Ian Sabroe It s all immune? Diseases that doesn t have immune involvement? The processes of response to injury and tissue repair are key homeostatic pathways involved in all
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session 13, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION SESSION 13 MHD I Autoimmunity November 10, 2016 STUDENT COPY MHD I, Session 13, STUDENT Copy Page 2 Case 1 CHIEF COMPLAINT: I am
MHD I, Session 13, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION SESSION 13 MHD I Autoimmunity November 10, 2016 STUDENT COPY MHD I, Session 13, STUDENT Copy Page 2 Case 1 CHIEF COMPLAINT: I am
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION
 BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
A TRICKY PROBLEM. Presenter-Dr Lakshmi PK
 A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
Patient: Becky Smith DOB: 01/26/XXXX Age: 5 y/o Attending: Dr. D. Miles Allergies: NKA MR#: 203. Patient Chart #203 Becky Smith
 Patient Chart #203 Becky Smith 1 Property of CSCLV CSCLV Rev: 06/04/2018 Chief Complaint: Abdominal pain. Informant: Parents. HISTORY & PHYSICAL HPI: Ill looking patient, healthy until 2 days ago when
Patient Chart #203 Becky Smith 1 Property of CSCLV CSCLV Rev: 06/04/2018 Chief Complaint: Abdominal pain. Informant: Parents. HISTORY & PHYSICAL HPI: Ill looking patient, healthy until 2 days ago when
USAID Health Care Improvement Project. pneumonia) respiratory infections through improved case management (amb/hosp)
 respiratory infections through improved case management (amb/hosp)") Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
CASE CONFERENCE Arif Shahzad, M.D. PGYIII Internal Medicine / Pediatrics
 CASE CONFERENCE Arif Shahzad, M.D. PGYIII Internal Medicine / Pediatrics Chief Complaint I feel very weak and dizzy History of Present Illness 54 yr man with PMHX DM-II and depression who was in his USOH
CASE CONFERENCE Arif Shahzad, M.D. PGYIII Internal Medicine / Pediatrics Chief Complaint I feel very weak and dizzy History of Present Illness 54 yr man with PMHX DM-II and depression who was in his USOH
CASE-BASED SMALL GROUP DISCUSSION MHD II SESSION 6. Friday, MARCH 18, 2016 STUDENT COPY
 MHD II, Session 6, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II SESSION 6 Friday, MARCH 18, 2016 STUDENT COPY Resource for cases: ACP Medicine (Scientific American Medicine) - Vaginitis
MHD II, Session 6, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II SESSION 6 Friday, MARCH 18, 2016 STUDENT COPY Resource for cases: ACP Medicine (Scientific American Medicine) - Vaginitis
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
Tell me more about vasculitis. Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital
 Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
RARE JUVENILE PRIMARY SYSTEMIC VASCULITIS
 www.pediatric-rheumathology.printo.it RARE JUVENILE PRIMARY SYSTEMIC VASCULITIS WHAT IS IT? Vasculitis is an inflammation of blood vessels. Vasculitides cover a wide group of diseases. Primary vasculitis
www.pediatric-rheumathology.printo.it RARE JUVENILE PRIMARY SYSTEMIC VASCULITIS WHAT IS IT? Vasculitis is an inflammation of blood vessels. Vasculitides cover a wide group of diseases. Primary vasculitis
Eosinophils and effusion: a clinical conundrum
 Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
CHECK LIST FORM-SCREENING
 CHECK LIST FORM-SCREENING Participant Initials: Date of Birth: Evaluation Date: Were the following forms completed for this visit? Eligibility Form Done t Done Baseline medical History Form Done t Done
CHECK LIST FORM-SCREENING Participant Initials: Date of Birth: Evaluation Date: Were the following forms completed for this visit? Eligibility Form Done t Done Baseline medical History Form Done t Done
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Done by: Shatha Khtoum
 Done by: Shatha Khtoum Overview Vasculitis -Vasculitis is a general term for vessel wall inflammation -Symptoms and signs depend on the tissue of which the vessels are affected. (slide 2) -There are usually
Done by: Shatha Khtoum Overview Vasculitis -Vasculitis is a general term for vessel wall inflammation -Symptoms and signs depend on the tissue of which the vessels are affected. (slide 2) -There are usually
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Clinical Grand Rounds. Vasishta Tatapudi, MD August 28, 2012
 Clinical Grand Rounds Vasishta Tatapudi, MD August 28, 2012 Case Summary History Chief complaint: A 49 year old African American male patient presented with progressively worsening shortness of breath
Clinical Grand Rounds Vasishta Tatapudi, MD August 28, 2012 Case Summary History Chief complaint: A 49 year old African American male patient presented with progressively worsening shortness of breath
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
CASE REPORT. Abstract. Introduction. Case Reports
 CASE REPORT Efficacy of Early Intravenous Immunoglobulin for Eosinophilic Granulomatosis with Polyangiitis with Drastically Progressive Neuropathy: A Synopsis of Two Cases Takeshi Matsumoto 1, Kojiro Otsuka
CASE REPORT Efficacy of Early Intravenous Immunoglobulin for Eosinophilic Granulomatosis with Polyangiitis with Drastically Progressive Neuropathy: A Synopsis of Two Cases Takeshi Matsumoto 1, Kojiro Otsuka
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Review Article. Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis. Milind Aurangabadkar
 associated Vasculitis. Milind Aurangabadkar") Review Article Vidarbha Journal of Internal Medicine Volume 23 July 207 Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis Milind Aurangabadkar ABSTRACT Anti-neutrophil
Review Article Vidarbha Journal of Internal Medicine Volume 23 July 207 Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis Milind Aurangabadkar ABSTRACT Anti-neutrophil
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
PUFF THE MAGIC DRAGON
 PUFF THE MAGIC DRAGON AN UNUSUAL CASE OF A PUFFY FACE MA ACP Annual Scientific Meeting Gurbir Gill, M.D., PGY-3 (Associate) George M. Abraham, MD, MPH, FACP Department of Medicine, Saint Vincent Hospital,
PUFF THE MAGIC DRAGON AN UNUSUAL CASE OF A PUFFY FACE MA ACP Annual Scientific Meeting Gurbir Gill, M.D., PGY-3 (Associate) George M. Abraham, MD, MPH, FACP Department of Medicine, Saint Vincent Hospital,
*HSP is a common vasculitis of small vessels with cutaneous & systemic complications. Its etiology is unknown& often follows URTIs.
 BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018
 SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
Managing Acute Medical Problems, Birmingham Vasculitis. David Jayne. University of Cambridge
 Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
TREATMENT OF ANCA-ASSOCIATED VASCULITIS
 TREATMENT OF ANCA-ASSOCIATED VASCULITIS Loïc Guillevin Hôpital Cochin, Université Paris Descartes Cours DU, 11 mars 2016 1 Disclosure of interest regarding this presentation Roche has provided, in part,
TREATMENT OF ANCA-ASSOCIATED VASCULITIS Loïc Guillevin Hôpital Cochin, Université Paris Descartes Cours DU, 11 mars 2016 1 Disclosure of interest regarding this presentation Roche has provided, in part,
Small Vessel Vasculitis
 Banff- Rocky Mountain Barry Kassen, MD, FRCPC,FACP Head, Division of Internal Medicine UBC/VGH/SPH Acting Head, Division of Community Internal Medicine November, 2009 Objectives 1. To understand small
Banff- Rocky Mountain Barry Kassen, MD, FRCPC,FACP Head, Division of Internal Medicine UBC/VGH/SPH Acting Head, Division of Community Internal Medicine November, 2009 Objectives 1. To understand small
Case report Fever in a patient with ANCA-associated vasculitis
 Case report Fever in a patient with ANCA-associated vasculitis 73 years-old white woman PRIOR MEDICAL HISTORY *Hypertension: Enalapril, Furosemide *Dyslipidemia: Pravastatin *Ischemic heart disease: 2008
Case report Fever in a patient with ANCA-associated vasculitis 73 years-old white woman PRIOR MEDICAL HISTORY *Hypertension: Enalapril, Furosemide *Dyslipidemia: Pravastatin *Ischemic heart disease: 2008
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session 13, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION SESSION 13 MHD I November 12, 2015 STUDENT COPY MHD I, Session 13, STUDENT Copy Page 2 Case 1 CHIEF COMPLAINT: I am very tired and
MHD I, Session 13, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION SESSION 13 MHD I November 12, 2015 STUDENT COPY MHD I, Session 13, STUDENT Copy Page 2 Case 1 CHIEF COMPLAINT: I am very tired and
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
Atopic Pulmonary Disease: Findings on Thoracic Imaging
 July 2003 Atopic Pulmonary Disease: Findings on Thoracic Imaging Rebecca G. Breslow Harvard Medical School Year IV Churg-Strauss Syndrome Hypersensitivity Pneumonitis Asthma Atopic Pulmonary Disease Allergic
July 2003 Atopic Pulmonary Disease: Findings on Thoracic Imaging Rebecca G. Breslow Harvard Medical School Year IV Churg-Strauss Syndrome Hypersensitivity Pneumonitis Asthma Atopic Pulmonary Disease Allergic
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
Date of Admission: [DATE]. Date of Discharge:
![Date of Admission: [DATE]. Date of Discharge:](/thumbs/74/71277118.jpg "Date of Admission: [DATE]. Date of Discharge:") Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Subject ID: I N D # # U A * Consent Date: Day Month Year
 IND Study # Eligibility Checklist Pg 1 of 15 Instructions: Check the appropriate box for each Inclusion and Exclusion Criterion below. Each criterion must be marked and all protocol criteria have to be
IND Study # Eligibility Checklist Pg 1 of 15 Instructions: Check the appropriate box for each Inclusion and Exclusion Criterion below. Each criterion must be marked and all protocol criteria have to be
Sinonasal involvement in systemic vasculitides and cocaine-induced midline destructive lesions: Diagnostic controversies
 Sinonasal involvement in systemic vasculitides and cocaine-induced midline destructive lesions: Diagnostic controversies M. Armengot, M.D., Ph.D., A. García-Lliberós, M.D., M. J. Gómez, M.D., A. Navarro,
Sinonasal involvement in systemic vasculitides and cocaine-induced midline destructive lesions: Diagnostic controversies M. Armengot, M.D., Ph.D., A. García-Lliberós, M.D., M. J. Gómez, M.D., A. Navarro,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session XIII, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION SESSION XIII MHD I November 13, 2014 STUDENT COPY MHD I, Session XIII, STUDENT Copy Page 2 Case 1 CHIEF COMPLAINT: I am very tired
MHD I, Session XIII, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION SESSION XIII MHD I November 13, 2014 STUDENT COPY MHD I, Session XIII, STUDENT Copy Page 2 Case 1 CHIEF COMPLAINT: I am very tired
CASE-BASED SMALL GROUP DISCUSSION
 MHD II, Session XII, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION Session XII MHD II April 21, 2014 STUDENT COPY Helpful Resource: ACP Medicine online available through LUHS Library Infectious
MHD II, Session XII, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION Session XII MHD II April 21, 2014 STUDENT COPY Helpful Resource: ACP Medicine online available through LUHS Library Infectious
Case Report Crescentic Glomerulonephritis with Anti-GBM and p-anca Antibodies
 Case Reports in Nephrology Volume 2012, Article ID 132085, 4 pages doi:10.1155/2012/132085 Case Report Crescentic Glomerulonephritis with Anti-GBM and p-anca Antibodies TariqJavedandParagVohra Department
Case Reports in Nephrology Volume 2012, Article ID 132085, 4 pages doi:10.1155/2012/132085 Case Report Crescentic Glomerulonephritis with Anti-GBM and p-anca Antibodies TariqJavedandParagVohra Department
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
* Final Report * ED Triage Entered On: 01/16/2014 8:45 EST Performed On: 01/16/2014 8:42 EST by
 Result date: Result status: 16 January 2014 8:42 EST Auth (Verified) * Final Report * ED Triage Entered On: 01/16/2014 8:45 EST Performed On: 01/16/2014 8:42 EST by Assessment I Chief Complaint : Diarrhea
Result date: Result status: 16 January 2014 8:42 EST Auth (Verified) * Final Report * ED Triage Entered On: 01/16/2014 8:45 EST Performed On: 01/16/2014 8:42 EST by Assessment I Chief Complaint : Diarrhea
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine