Clinical Radiological Pathological Conference
|
|
|
- Albert Sparks
- 5 years ago
- Views:
Transcription
1 Clinical Radiological Pathological Conference
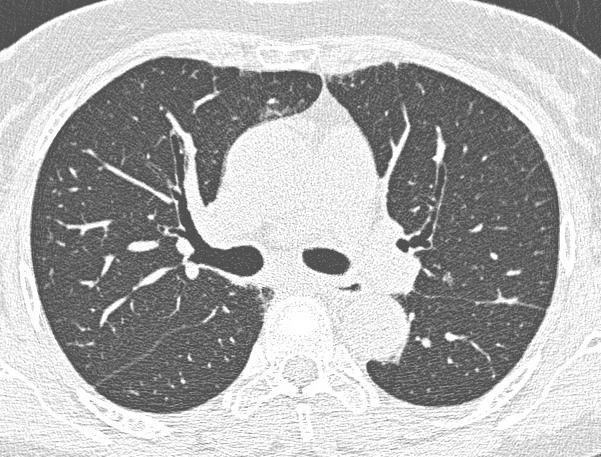
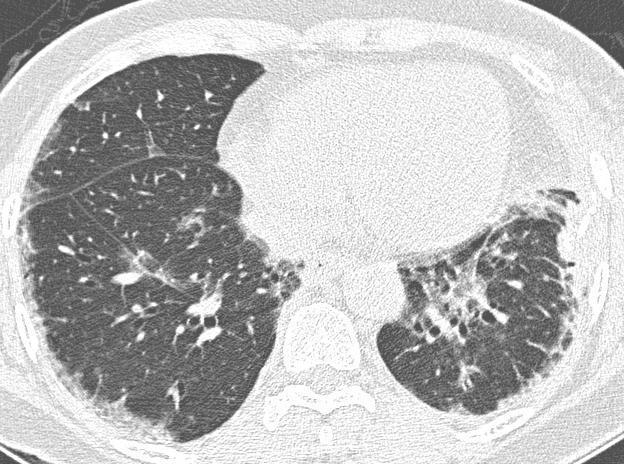
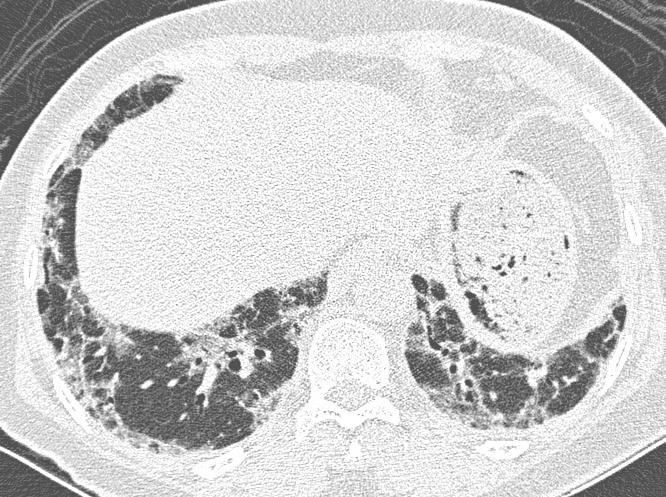
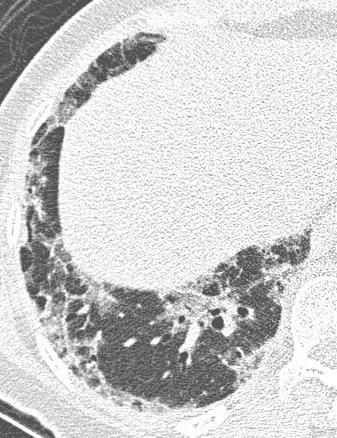
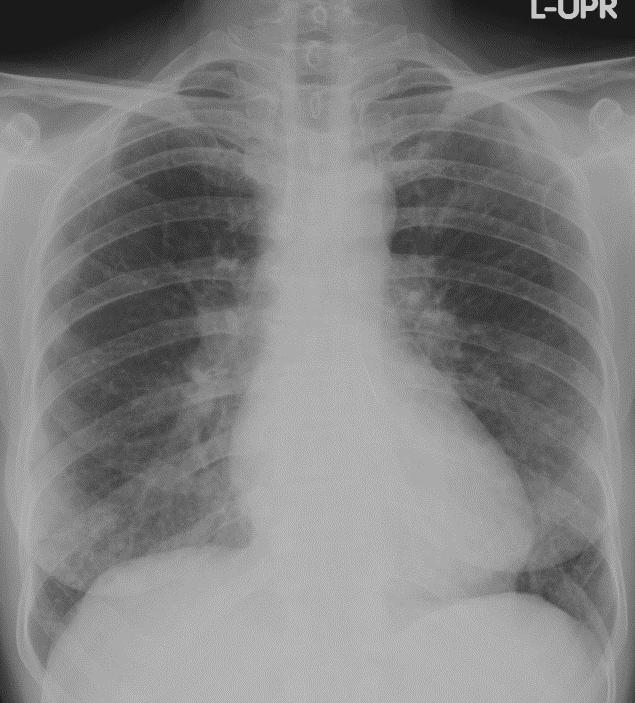
2 CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year
3 Present illness 1 year PTA : She developed dyspnea on exertion She had dry cough without hemoptysis, anorexia with weight loss 4 kgs. She denied arthritis, rash or fever. Due to her abnormal CXR, she had to collect sputum for AFB stains and the results were negative.
4 Past history Underlying disease : HT; on Amlodipine 5 mg/day No other medication use No smoking No history of contact TB No any pets No family history of cancer, genetic disease, connective tissue disease
5 Physical examination GA: Good consciousness V/S: BT 37 c RR 20/min PR 86/min BP 140/80 mmhg HEENT: not pale, no jaundice, no malar rash, no discoid rash, no oral ulcer, no peripheral lymphadenopathy Heart: normals1s2, no murmur, no loud P₂ Lungs: clear, normal breath sound both lungs Abdomen: no distension, normoactive bowel sound, soft, not tender, no organomegaly Ext: no pitting edema, no rash, no petechiae, no arthritis Neuro sign: grossly intact

6

7
8
9
10
11
12 Question (1) Are there any useful investigations? A. Anti-HIV B. Serology profile for connective tissue disease C. Bronchoscopy with BAL D. All of them
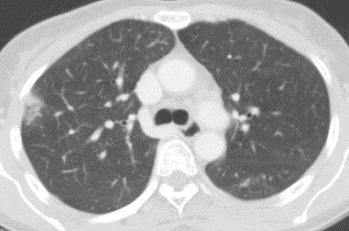
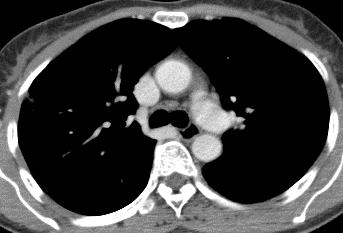
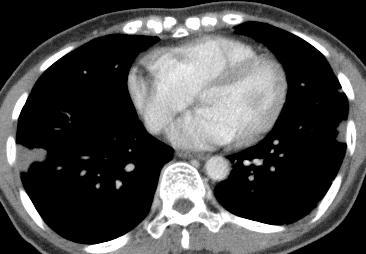
13 Question (2) Can we provide the diagnosis from HRCT?
14 Question (3) Do we need tissue diagnosis? A. Yes B. No C. I am not sure
15 Question (4) Is this disease likely reversible? A. Yes B. No C. I don t know
16 CASE 2: A 72-year-old male Gardener Live in Songkhla, Thailand Chronic cough for 3 months
17 Present illness 4 years PTA : He had chronic cough which was diagnosed pulmonary tuberculosis After complete treatment, his clinical was improved. 1 year PTA : He developed right pleural effusion then pleural tapping was performed which was considered to be parapneumonic effusion. The patient was admitted for intravenous antibiotic. 3 months PTA : He developed chronic cough again with abnormal CXR. He had uncertain weight loss but no fever.
18 Past history Underlying disease: Old myocardial infarction, on antiplatelet Smoking 20 packs-year
19 Physical examination GA : Good consciousness V/S: BT 36.5 c RR 28/min PR 60/min BP 132/60 mmhg HEENT: not pale, no jaundice, no peripheral lymphadenopathy Lungs: decrease breath sound at right lung with dullness on percussion Heart : normal S1S2, no murmur Abdomen: soft, not tender, no organomegaly Ext: no rash, no petechiae

20

21

22

23

24
25

26
27 Question (1) What is the most likely diagnosis of RLL infiltration? A. Pulmonary tuberculosis B. Aspergillosis C. Aspiration pneumonia D. Actinomycosis
28 Question (2) Where is normal site of the inhabited organisms? A. Teeth B. Gingival margins C. Upper lobes D. Nasal cavity
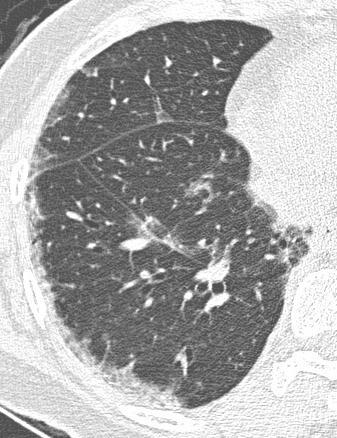
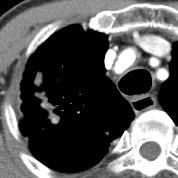
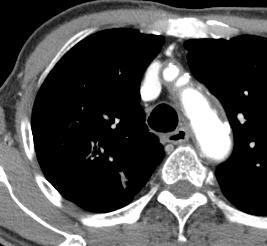
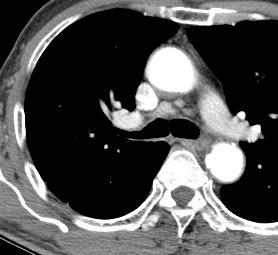
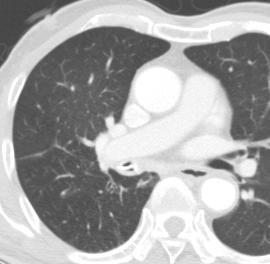
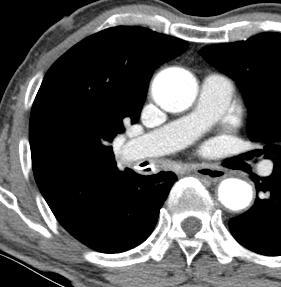
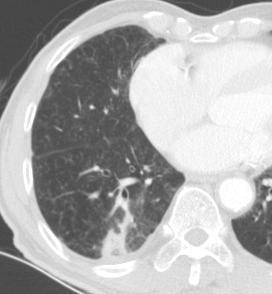
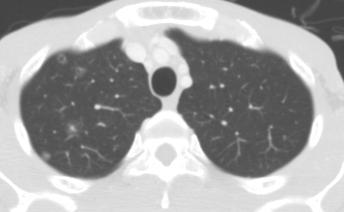
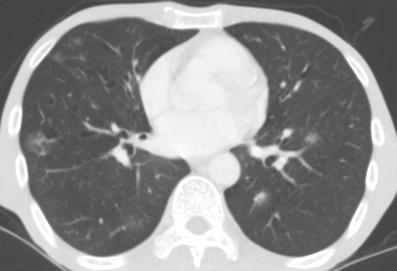
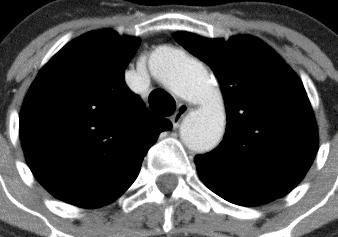
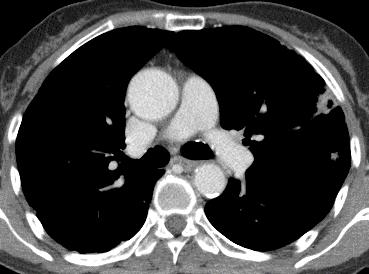
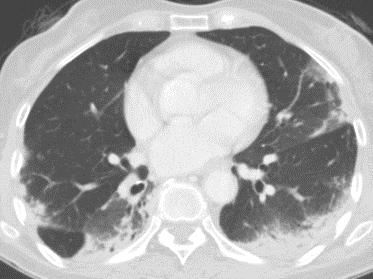
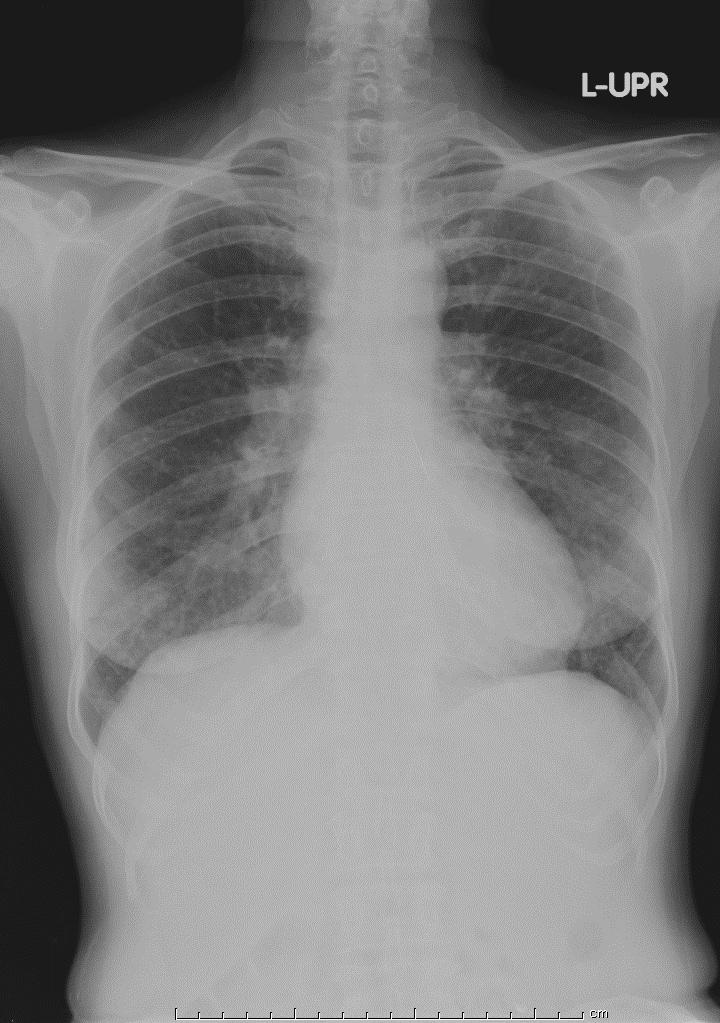
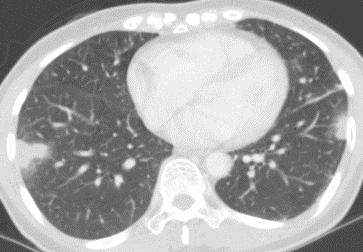
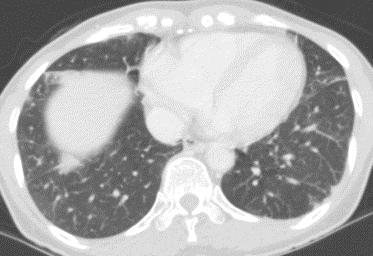
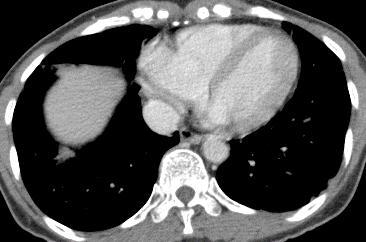
29 CASE 3: A 49-year-old male Employee Live in Pattani, Thailand Incidentally found abnormal CXR during admission
30 Present illness Known case of intrahepatic duct stones S/P ERCP with stone removal x 4 times Admitted due to chronic abdominal pain with significant weight loss (10 kgs in 2 months)
31 Physical examination GA: A Thai male, cachexia, no dyspnea V/S : BT 36 c BP 110/70 mmhg PR 85/min RR 20/min SpO₂ room air 100% BW 30 kgs HEENT: mildly pale, no jaundice Lungs: clear both lungs, no adventitious sound Heart: normal S1S2, no murmur Abdomen: normoactive bowel sound, soft, not tender, hepatomegaly 2 cm below RCM, no splenic dullness, no shifting dullness
32 Past history No other underlying disease Smoking 15 packs-year, quitted 6 months ago No alcohol used Herbal used due to chronic abdominal pain
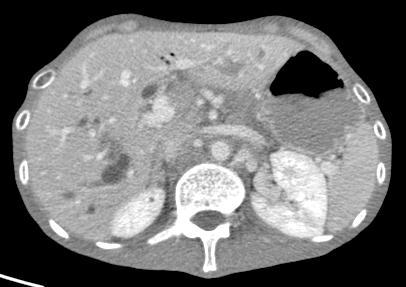
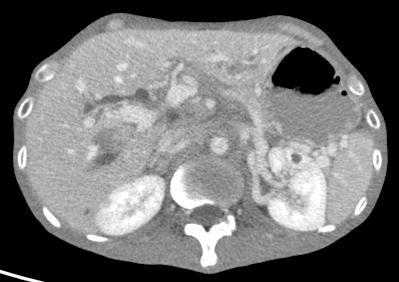
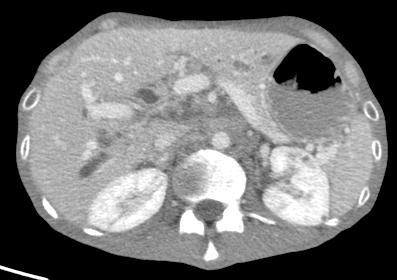
33 Investigations CT abdomen An ill-defined hepatic mass of progressive delayed enhancement and associated upstream dilated bile ducts in lateral segment of right lobe A few residual IHDs stones in lateral left hepatic lobe Multiple necrotic nodes
34 Investigations Failed EUS Consult IVR for mesenteric lymph node biopsy : USG revealed multiple cystic lesions around the mesenteric root, thrombosis of the SMV and partially extension to the main portal vein. Biopsy of the mesenteric cystic lesion -> 3 ml of mucous content was obtained. Cytology-Pathology report : suspicious for mucinous tumor
35 Consult Chest due to abnormal CXR and chest CT



36 23/9/2012 (Before admission) 23/12/2013 (admission) 7/1/2014
37 Chest CT 25/12/2013
38

39
40

41
42 Whole abdominal CT 25/12/2013
43
44
45
46 Question (1) What is the etiology of lung parenchymal abnormality? A. Septic emboli B. BAC C. Hematogenous metastasis D. Lymphoma
47 CASE 4: A 71-year-old female Housekeeper Live in Patthalung, Thailand Chronic cough for 6 months
48 Present illness 6 Months PTA : She had productive cough (more than one glass per day) without hemoptysis. Her symptom was predominant at night. Her sputum exams for AFB smears were negative. She took medications from a private clinic but her symptoms got worse. She had weight loss 2 kg recently.
49 Past history Underlying disease : HT, Dyslipidemia Passive smoker for 30 years No known drug allergy
50 Physical examination GA : no cachexia, afebrile V/S : BP 142/86 mmhg PR 94/min RR 20/min BW 44 kg Height 155 cm HEENT: not pale, no jaundice, no cervical lymphadenopathy Heart: normal S1S2, no murmur Lungs: coarse crepitation both basal lungs

51 13/9/2011

52 13/9/2011

53 13/9/2011


54 13/9/2011
55 Question (1) What is the most likely diagnosis? A. PAP B. BAC C. BOOP D. CEP
56 CASE 5: A 52-year-old female Housekeeper Live in Pattani, Thailand Chronic cough for 3 months
57 Present illness 3 months PTA: She had a cough with purulent sputum She had no hemoptysis or dyspnea. 1 month PTA: She had a progressively worsening cough with recurrent non-massive hemoptysis. She developed progressive dyspnea, weight loss 6 kgs but no fever. She was received bronchodilators and cough suppressant but her symptoms were not improved. Her sputum exams for AFB smears were negative.
58 Physical examination GA : Good consciousness, afebrile V/S : RR 26/min PR 96 bpm BP 120/70 mmhg SpO₂ room air 88% BW 43 kgs HEENT: not pale, no jaundice, no cervical lymphadenopathy Breast : no mass Heart : normal S1S2, no murmur Lungs: clear both lungs Ext: no clubbing of fingers
59 02/11/2011


60 02/11/2011
61 02/11/2011
62 02/11/2011
63 02/11/2011
64 Question (1) What is the most likely diagnosis? A. Pulmonary infarction from pulmonary embolism B. Pulmonary metastasis C. Tumor emboli D. BOOP
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION
 BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
Mechanical versus bioprosthetic valve. Intern: Supervisor: VS
 Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive abdominal distension 3 months Failure
 Dr Rajasree S Dr Srinivas S, Dr Bagdi RK, Dr Satheesh C Apollo Childrens Hospital, Chennai 1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive
Dr Rajasree S Dr Srinivas S, Dr Bagdi RK, Dr Satheesh C Apollo Childrens Hospital, Chennai 1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Presentation. Dr.N.Bhanu teja Final year postgraduate Department of pulmonology
 Case Presentation Dr.N.Bhanu teja Final year postgraduate Department of pulmonology A 60 year old male patient resident of miryalguda referred to pulmonary medicine outpatient department with complaints
Case Presentation Dr.N.Bhanu teja Final year postgraduate Department of pulmonology A 60 year old male patient resident of miryalguda referred to pulmonary medicine outpatient department with complaints
Fever in Lupus. 21 st April 2014
 Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION. OSCE 5: Cough
 BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 5: Cough This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. So Ms. Chen, tell me what is your average
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 5: Cough This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. So Ms. Chen, tell me what is your average
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Case presentation. Dr REESAUL R
 Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
PCCSS, LLP Pulmonary, Critical Care & Sleep Specialists
 NAME: AGE: DOB: DATE: REQUESTING PHYSICIAN: NOTE: Please help us find out about you by filling out the Patient side of this form on pages 1 3. If you don t know the answer to one of the questions, ask
NAME: AGE: DOB: DATE: REQUESTING PHYSICIAN: NOTE: Please help us find out about you by filling out the Patient side of this form on pages 1 3. If you don t know the answer to one of the questions, ask
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
APPROACH TO PLEURAL EFFUSIONS. Raed Alalawi, MD, FCCP
 APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Immune Reconstitution Inflammatory Syndrome. Dr. Lesego Mawela
 Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Rehuka Khurana, MD, MPH has the following disclosures to make:
 Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB
 The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB Harvey H. Wong, MD FRCPC MScCH Assistant Professor Department of Medicine Division of Respirology University of Toronto Financial
The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB Harvey H. Wong, MD FRCPC MScCH Assistant Professor Department of Medicine Division of Respirology University of Toronto Financial
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis
 All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Lung Cancer Case Study
 Lung Cancer Case Study Presented by s GP Education Programme 2 Part One Initial presentation 60 year old lady, presents with a 6 week history of right sided chest pain. The pain is like a dull ache, but
Lung Cancer Case Study Presented by s GP Education Programme 2 Part One Initial presentation 60 year old lady, presents with a 6 week history of right sided chest pain. The pain is like a dull ache, but
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
2017 Chicago CAPA meeting Case Discussion
 2017 Chicago CAPA meeting Case Discussion Case 1 (Presented by Haiyan Chen) 25 yo M, h/o melanoma diagnosed 2 months ago before presenting severe abdominal pain Left colon biopsy, low power Left colon
2017 Chicago CAPA meeting Case Discussion Case 1 (Presented by Haiyan Chen) 25 yo M, h/o melanoma diagnosed 2 months ago before presenting severe abdominal pain Left colon biopsy, low power Left colon
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
Enlarging TB Lymph Node Improving or Deteriorating? History. History. Physical examination. Distribution of lymph nodes
 Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
Case 5 15-year-old male
 Case 5 15-year-old male Present illness: Six months ago, abnormality of ECG was incidentally detected by annual health check. His blood level of γ-gtp, HbA1c and norepinephrine were elevated; however,
Case 5 15-year-old male Present illness: Six months ago, abnormality of ECG was incidentally detected by annual health check. His blood level of γ-gtp, HbA1c and norepinephrine were elevated; however,
Management of Pleural Effusion
 Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Patient to complete this information
 Patient to complete this information Patient s Name Birth date Today s date Referring Physician Primary Care Physician Age Occupation Retired, how long? Prior operations Medications Type Date Name Dose
Patient to complete this information Patient s Name Birth date Today s date Referring Physician Primary Care Physician Age Occupation Retired, how long? Prior operations Medications Type Date Name Dose
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
Index No. All five (05) questions should be answered. All questions carry equal marks.
 questions should be answered. All questions carry equal marks.") POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
Complicated echinococcal cyst to Biopsy or not to biopsy. V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center
 Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
BGS Spring Conference 2015
 TB in the elderly Dr Anna Rich Respiratory Consultant, Nottingham University Hospitals Outline Why relevant? Elderly vs young adults Diagnosis Treatment Side effects TB in the 21 st century Stats 2013;
TB in the elderly Dr Anna Rich Respiratory Consultant, Nottingham University Hospitals Outline Why relevant? Elderly vs young adults Diagnosis Treatment Side effects TB in the 21 st century Stats 2013;
Resident Case Review CHEST. Daria Manos CAR 2016
 Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Case Presentation. Faysal Ghazzay Ahmed
 Faysal Ghazzay Ahmed Case Presentation He is 49 years old male living in Al-Qaem Town (Al-Anbar Gov.), Muslim, and was previously serving in the army, but now he is idle. He was admitted to Al-Jumhoory
Faysal Ghazzay Ahmed Case Presentation He is 49 years old male living in Al-Qaem Town (Al-Anbar Gov.), Muslim, and was previously serving in the army, but now he is idle. He was admitted to Al-Jumhoory
Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma
 Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Looking Outside the Box: Incidental Extracardiac Finding in Echo
 Looking Outside the Box: Incidental Extracardiac Finding in Echo Dr. Aijaz Shah Head of Division, Adult Echocardiography Laboratory Prince Sultan Cardiac Centre Riyadh Case 1 17 year old boy presented
Looking Outside the Box: Incidental Extracardiac Finding in Echo Dr. Aijaz Shah Head of Division, Adult Echocardiography Laboratory Prince Sultan Cardiac Centre Riyadh Case 1 17 year old boy presented
Broward Oncology Associates, P.A. PATIENT INFORMATION
 NAME: BIRTHDATE: AGE: LOCAL ADDRESS (Street city state zip): HOME TELEPHONE# CELL # SOCIAL SECURITY #: - - SEX MARITAL STATUS WHAT IS YOUR HT? WHAT IS YOUR WT? EMPLOYER WORK# SPOUSE'S NAME SPOUSE'S EMPLOYER
NAME: BIRTHDATE: AGE: LOCAL ADDRESS (Street city state zip): HOME TELEPHONE# CELL # SOCIAL SECURITY #: - - SEX MARITAL STATUS WHAT IS YOUR HT? WHAT IS YOUR WT? EMPLOYER WORK# SPOUSE'S NAME SPOUSE'S EMPLOYER
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Pleural Effusions. Kyle J Henry, MD Pulmonary/ CCM Fellow PGY4 (210) (602)
 (602)") Pleural Effusions Kyle J Henry, MD Pulmonary/ CCM Fellow PGY4 (210) 275 8583 (602) 202 0351 None Disclosures Objectives Understand the presentation of a pleural effusion How to diagnose and treat Differentiate
Pleural Effusions Kyle J Henry, MD Pulmonary/ CCM Fellow PGY4 (210) 275 8583 (602) 202 0351 None Disclosures Objectives Understand the presentation of a pleural effusion How to diagnose and treat Differentiate
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
THE CONNECTIVE TISSUE AND EPITHELIUM
 THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
Management of acute alcoholic hepatitis
 Management of acute alcoholic hepatitis Yesim ALAHDAB Marmara University Hospital, Istanbul/TURKEY 5 th European Young Hepatologists Workshop August, 27-29, 2015 Moulin de Vernègues, France 1.4L ALCOHOL
Management of acute alcoholic hepatitis Yesim ALAHDAB Marmara University Hospital, Istanbul/TURKEY 5 th European Young Hepatologists Workshop August, 27-29, 2015 Moulin de Vernègues, France 1.4L ALCOHOL
Pulmonary TB aspects
 Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Long Case Set 02. Dr Raviraj Uppoor. Dr Sameer Shamshuddin. Consultant Radiologist Cumberland Infirmary, Carlisle, UK
 Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
PEARLS IN PULMONARY MEDICINE. Kellie R. Jones, MD Associate Professor University of Oklahoma Health Sciences Center
 PEARLS IN PULMONARY MEDICINE Kellie R. Jones, MD Associate Professor University of Oklahoma Health Sciences Center Case 1 While moonlighting in the ER, you are asked to evaluate a lady for shortness of
PEARLS IN PULMONARY MEDICINE Kellie R. Jones, MD Associate Professor University of Oklahoma Health Sciences Center Case 1 While moonlighting in the ER, you are asked to evaluate a lady for shortness of
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
NEUROLOGICAL SURGERY, P.C.
 NEUROLOGICAL SURGERY, P.C. PATIENT INFORMATION Name Date of Birth Age Address City Sate NY Zip Home ( ) - Cell ( ) - Work ( ) - Ext: Email Address _ Sex M F Soc. Sec. #: / / Single Married Widowed Separated
NEUROLOGICAL SURGERY, P.C. PATIENT INFORMATION Name Date of Birth Age Address City Sate NY Zip Home ( ) - Cell ( ) - Work ( ) - Ext: Email Address _ Sex M F Soc. Sec. #: / / Single Married Widowed Separated
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
HIV-associated Pulmonary Disease. Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond QUESTION: HIV-associated Pulmonary Diseases
 Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1).
.") PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
Bacterial pneumonia with associated pleural empyema pleural effusion
 EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
By Your Sis: Ghada Odeh :)
") By Your Sis: Ghada Odeh :) Hx: Chest pain ACS. Hx.: Cough Bronchiectasis. Hx: Epigastric pain Peptic ulcer disease. Hx: Joints Pain SLE. Hx: Hematurea post-strep Glomerulonephritis. Hx: Jaundice Chronic
By Your Sis: Ghada Odeh :) Hx: Chest pain ACS. Hx.: Cough Bronchiectasis. Hx: Epigastric pain Peptic ulcer disease. Hx: Joints Pain SLE. Hx: Hematurea post-strep Glomerulonephritis. Hx: Jaundice Chronic
2017/04/21 R1 歐宗頴. Case Discussion
 2017/04/21 R1 歐宗頴 Case Discussion Case Demography Name: 18143xxx Age: 14y/o Gender: boy Admission: 2017/04/07 Chief complaint: recurrent fever with RUQ pain for 6 weeks Past History G3P3 full term NSD
2017/04/21 R1 歐宗頴 Case Discussion Case Demography Name: 18143xxx Age: 14y/o Gender: boy Admission: 2017/04/07 Chief complaint: recurrent fever with RUQ pain for 6 weeks Past History G3P3 full term NSD
NORTHERN VIRGINIA PULMONARY AND CRITICAL CARE ASSOCIATES, P.C.
 NORTHERN VIRGINIA PULMONARY AND CRITICAL CARE ASSOCIATES, P.C. Past Medical History AIDS/HIV disease Anemia Asthma Bronchitis Cancer Date of last Chest X-ray Diabetes Mellitus, Type I Diabetes Mellitus,
NORTHERN VIRGINIA PULMONARY AND CRITICAL CARE ASSOCIATES, P.C. Past Medical History AIDS/HIV disease Anemia Asthma Bronchitis Cancer Date of last Chest X-ray Diabetes Mellitus, Type I Diabetes Mellitus,
Case 1: Clinical Presentation
 Impostors and Preconceived Notions: Lessons Learned in TB Diagnosis & Treatment Tuberculosis Nursing Workshop June 1, 2015 Christopher Spitters, MD, MPH Tuberculosis Clinic Public Health Seattle & King
Impostors and Preconceived Notions: Lessons Learned in TB Diagnosis & Treatment Tuberculosis Nursing Workshop June 1, 2015 Christopher Spitters, MD, MPH Tuberculosis Clinic Public Health Seattle & King
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
Cardiovascular and Respiratory Disorders
 Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
TB in Children. The diagnostic challenge. Ralph Diedericks Red Cross Hospital
 TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS
 MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
September 2014 Imaging Case of the Month. Michael B. Gotway, MD. Department of Radiology Mayo Clinic Arizona Scottsdale, AZ
 September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
A 43year old man presented with cough and breathlessness. Presented by Dr. Enayet-Ul-Islam Dhaka Medical College Hospital
 A 43year old man presented with cough and breathlessness Presented by Dr. Enayet-Ul-Islam Dhaka Medical College Hospital PARTICULARS OF THE PATIENT: Patients name : Mr. Md. Ismail,43 years. Address : Chittagong.
A 43year old man presented with cough and breathlessness Presented by Dr. Enayet-Ul-Islam Dhaka Medical College Hospital PARTICULARS OF THE PATIENT: Patients name : Mr. Md. Ismail,43 years. Address : Chittagong.
CASE-BASED SMALL GROUP DISCUSSION
 MHD II, Session XII, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION Session XII MHD II April 21, 2014 STUDENT COPY Helpful Resource: ACP Medicine online available through LUHS Library Infectious
MHD II, Session XII, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION Session XII MHD II April 21, 2014 STUDENT COPY Helpful Resource: ACP Medicine online available through LUHS Library Infectious
Evaluation of Chest Pain in the Primary Care Setting. Joseph Hackler, DO. Disclosures
 Evaluation of Chest Pain in the Primary Care Setting Joseph Hackler, DO Disclosures I have no relevant relationships with commercial interests to disclose. 1 Objectives 1. Discuss the different etiologies
Evaluation of Chest Pain in the Primary Care Setting Joseph Hackler, DO Disclosures I have no relevant relationships with commercial interests to disclose. 1 Objectives 1. Discuss the different etiologies
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
REDDY & ASSOCIATES LLC D/B/A Reddy Medical Group D/B/A Reddy Urgent Care. Reddy Urgent Care Pre-Employment Physical Form
 REDDY & ASSOCIATES LLC D/B/A Reddy Medical Group D/B/A Reddy Urgent Care 132 Franklin Springs St. 1061 Dowdy Road STE 100 280 General Daniels Ave. Royston, GA 30662 Athens, GA 30606 Danielsville, GA 30633
REDDY & ASSOCIATES LLC D/B/A Reddy Medical Group D/B/A Reddy Urgent Care 132 Franklin Springs St. 1061 Dowdy Road STE 100 280 General Daniels Ave. Royston, GA 30662 Athens, GA 30606 Danielsville, GA 30633
A case of acute liver failure in HIV/HBV co-infection
 A case of acute liver failure in HIV/HBV co-infection Lukun zhang Department of Infectious Disease The Third People s Hospital of Shenzhen May 12th,2017 History of present illness Patient basic information
A case of acute liver failure in HIV/HBV co-infection Lukun zhang Department of Infectious Disease The Third People s Hospital of Shenzhen May 12th,2017 History of present illness Patient basic information
B. Cystic Teratoma: Refer to virtual microscope slide p_223 ovary, teratoma and compare to normal virtual microscope slide 086 ovary.
 LAB 2: THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
LAB 2: THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
Instructions: Please bring these forms to your Physical Examination & TB Test and have the Doctor fill them out. (Where applicable)
") Instructions: Please bring these forms to your Physical Examination & TB Test and have the Doctor fill them out. (Where applicable) 1. The physician s examination certification form. Ask your doctor to
Instructions: Please bring these forms to your Physical Examination & TB Test and have the Doctor fill them out. (Where applicable) 1. The physician s examination certification form. Ask your doctor to
Case 1. Case Discussion. History. Present Illness. Impression. Physical Examination
 Case 1 Case Discussion R1 林吉倡 2013 / 01 / 02 13-yo Male BW: 45 kg DAY1 16:35 pm C/C: Epigastric pain since this morning TPR: 36.5/94/18 BP:133/83 SpO2: 100% GCS: 15 Triage: 2 Present Illness Sudden-onset
Case 1 Case Discussion R1 林吉倡 2013 / 01 / 02 13-yo Male BW: 45 kg DAY1 16:35 pm C/C: Epigastric pain since this morning TPR: 36.5/94/18 BP:133/83 SpO2: 100% GCS: 15 Triage: 2 Present Illness Sudden-onset
Reinventing Report: How You Can Develop Resident Expertise in High- Value Clinical Reasoning
 Reinventing Report: How You Can Develop Resident Expertise in High- Value Clinical Reasoning Jason H. Maley, MD, Kathleen M. Murphy, MD, and Erin M. Haley, MD, PhD Chief Medicine Residents Department of
Reinventing Report: How You Can Develop Resident Expertise in High- Value Clinical Reasoning Jason H. Maley, MD, Kathleen M. Murphy, MD, and Erin M. Haley, MD, PhD Chief Medicine Residents Department of
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD. November 18, 2017
 Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations