Evidence Based Medicine and the Treatment of Gout
|
|
|
- Ashley Miles
- 5 years ago
- Views:
Transcription
1 Evidence Based Medicine and the Treatment of Gout DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine GORDON K. LAM, MD, FACR NorthEast Rheumatology Medical Director, Northern Region Research Center Atrium Health, Concord, NC
2 CONFLICT OF INTEREST I have no conflicts of interest pertaining to the material presented in this lecture.
3 OUTLINE Gout from a Podiatric Physicians Perspective Gout from a Rheumatologists Perspective
4 OUTLINE Gout from a Podiatric Physicians Perspective Clinical Presentation Differential Diagnosis Risk Factors Clinical / Lab findings Radiographic Features Non Medical Treatment When to Refer
5 OUTLINE Gout from a Rheumatologist Perspective Treatment of Patient with Acute Gout Flare Colchicine Corticosteroids Indocin/NSAID s Long-term Management of Gout Peri-operative Management of the Gout Patient Management of the Recalcitrant Patient Newer Medication Options Lesinurad/Allopurinol Krystexxa

6 Famous Sufferers of Gout Leonardo da Vinci 1519 King Henry VIII 1547 Charles V 1558 Nostradamus 1566 Sir Isaac Newton 1727 Benjamin Franklin 1790 Beethoven 1827 Luciano Pavarotti

7 N Engl J Med 2006;355: Aug 2006

8 King Charles V Holy Roman Emperor. Abdicated throne due to effects of gout. Emperor had a voracious appetite, especially for meat. Drank large quantities of beer and wine. Ordered a specially designed four-handed drinking mug. N Engl J Med 2006;355: Aug 2006


9 King Charles V Pathological analysis of distal phalanx of fifth digit of hand was performed. Radiograph demonstrated erosive changes as well as softtissue calcification Massive chalky appearing soft tissue mass confirmed gout crystals via electron microscopy. N Engl J Med 2006;355: Aug 2006

10 James Gillray British caricaturist and printmaker 18 th Century Considered to be the Father of Political Cartoons 1799

11 Feb Napoleon vs. William Pitt Depicts England and France carving up the world.



12 James Gillray Gillray himself became an alcoholic and suffered from Gout.

13 GOUT Arthritic process which occurs secondary to hyperurecemia. Overproducers Under-excretors Estimated that greater than 5 Million people in the United States are affected by Gout.
14 Interesting fact: Not everyone with hyperuricemia develops gout up to two-thirds of people with hyperuricemia never develop symptoms.
15 Epidemiology Males > Females 10:1 ratio Highest incidence is in 5 th decade of life African Americans greater incidence than Caucasians Rare in pre-menopausal females Estrogen promotes the excretion of uric acid Post menopausal: Male:Female 3:1 ratio Most common cause of inflammatory arthritis in males > 30 years of age
. The incidence of secondary, diuretic related gout did not increase over time (p = 0.140).")
16 Is the Incidence of Gout Rising? There was a greater than 2-fold increase in the rate of primary gout (i.e., no history of diuretic exposure) in the recent compared to the older time periods (p = 0.002). The incidence of secondary, diuretic related gout did not increase over time (p = 0.140). Our results indicate that the incidence of primary gout has increased significantly over the past 20 years. While this increase might be a result of improved ascertainment of atypical gout, it may also be related to other, as yet unidentified, risk factors. Epidemiology of gout: is the incidence rising? J Rheumatol Nov;29(11): Arromdee E, Michet CJ, Crowson CS, O Fallon WM, Gabriel SE.
17 Is the Incidence of Gout Rising? a 26.8% increase in Acute Gout being primary presenting diagnosis. Men responsible for 78% of visits. J Charnow: Emergency Department Gout Visits Rise Dramatically. Renal and Urology News. June, 2018.
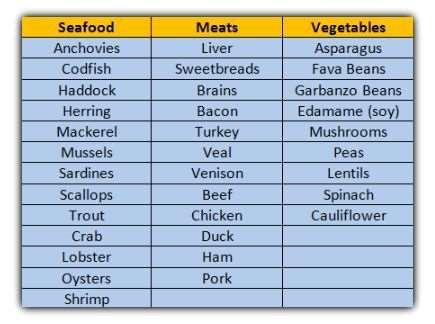
18 GOUT RISK FACTORS Obesity High Blood Pressure Chronic Kidney Disease EtOH Diet (Purine rich foods) Medications Diuretics Fasting Myelo-lymphoproliferative disorders Hypothyroidism Dehydration
19 MEDICATIONS SPEED Salicylates Pyrazinamide (TB) Ethambutol (TB) Ethanol Diuretics

20 Up To Date: Feb



21 Alcohol and Gout Risk of gout for various alcoholic beverages: Two or more beers/day = 2.5 fold increase risk. Two or more intake of spirits = 1.6 fold increased risk. Two 4 oz or more wine consumption was not associated with an increased risk of gout. These findings were independent of diet, age, BMI, hypertension or use of diuretics. The Lancet: Alcohol intake and risk of incident gout in men: a prospective study. H Choi, K

22
 Results Additional weekly serving of purine rich red meat 21% increase risk of gout Additional")
23 12 year retrospective study. 47,150 men with no h/o gout (> 40 years of age) Results Additional weekly serving of purine rich red meat 21% increase risk of gout Additional weekly serving of seafood 7% increase risk of gout (particularly in low BMI patients). N Engl J Med 2004; 350:
24 During 12 years of the study 730 confirmed new cases of gout. 88% of men reported podagra, with 35% demonstrating midfoot involvement. Other Findings Intake of low fat dairy as well as purine rich vegetable protein may be protective. N Engl J Med 2004; 350:
25 INDUCERS OF ACUTE ATTACK Trauma Surgery Diet Changes in EtOH intake Changes in Medications Dehydration
26
27 Diagnosis of Gout Gout (monosodium urate [MSU] crystal deposition disease) is characterized biochemically by extracellular fluid urate saturation, which is reflected in the blood by hyperuricemia, with serum or plasma urate concentrations exceeding 6.8 mg/dl (approximately 400 micromol/l); this level of urate is the approximate limit of urate solubility. ACR Guidelines (2012) recommend the goal of Gout management is to achieve < 6.0 mg/dl UptoDate.com/clinical manifestations and diagnosis of Gout: Feb. 2018

28 Clinical Presentation Red, Hot, Swollen! First Metatarsal Phalangeal Joint Pain started at night I can t even let the sheets touch my foot

29
30 It Woke me up! ARTHRITIS & RHEUMATOLOGY Vol. 67, No. 2, February 2015, pp DOI /art , American College of Rheumatology Conclusion. These findings provide the first prospective evidence that the risk of gout attacks during the night and early morning is 2.4 times higher than in the daytime. Further, these data support the purported mechanisms and historical descriptions of the nocturnal onset of gout attacks and may have implications for antigout prophylactic measures.

31 Why? Diurnal variations in body temperature ranges from 37.5 C between 10am and 6pm to 36.4 C between 2am and 6am leading to a higher risk if UA crystallization. Relative dehydration Diurnal variations of blood cortisol levels. Sleep Apnea ARTHRITIS & RHEUMATOLOGY Vol. 67, No. 2, February 2015, pp DOI /art , American College of Rheumatology
32 Sleep apnea hypoxia can enhance nucleotide turnover, thereby generating purines. Up to 50% of sleep apnea patients have been found to have hyperuricemia. Hasday JD, Grum CM. Nocturnal increase of urinary uric acid: creatinine ratio: a biochemical correlate of sleep-associated hypoxemia. Am Rev Respir Dis 1987;135:534 8.

33 Conclusions: Our findings support an association between gout and sleep disorders, although the association with obstructive sleep apnea syndrome does not appear to be independent of co-morbid confounding factors. However, the potential co-existence of these two common conditions is an important message for clinicians and deserves wider recognition. Future studies should focus on establishing the independence of this association and causality and examine whether treatment strategies benefit both conditions. Roddy E, Muller S, Hayward R, Mallen CD. The association of gout with sleep disorders: a cross-sectional study in primary care. BMC Musculoskelet Disord 2013;14:119.

34 Differential Diagnosis Gout Septic Joint Trauma

35 Imaging

36 Imaging

37

38

39

40 Courtesy: Leland Jaffe, DPM, North Chicago, IL
41 Definitive Diag. via Jt. Aspiration But Isn t this more commonly a Clinical Diagnosis? How commonly do you aspirate the joint? Always (100%) Mostly (75%) Commonly (50%) Rarely (25%) Never (0%)




42 I d Tap That!

43

44 Courtesy: Leland Jaffe, DPM, North Chicago, IL


45 Courtesy Gina Painter, DPM Great Falls, MT


46 Reductio Ad Absurdum Reduction to Absurdity History & Clinical Exam Labs Radiographs Ultrasound MRI DECT
47

48 Gouty Arthritis Acute Monoarticular Gout (3-10 days) Quick onset Severe crushing pain Affected joint (usually 1 st MPJ) edematous, hot and dry 10% will never experience another attack 60% experience a second attack within a year Red, hot, swollen joint, so why isn t Gout considered an Inflammatory Arthritide? *Inflammation is short-lived (7-10days)

49 Gouty Arthritis Polyarticular Gout Recurrent attacks may or may not affect joint initially involved Attacks less severe but prolonged X-ray changes in 33% of patients

50 Chronic Gout Gouty Arthritis Increasingly uncommon due to current medications Joints become stiff, enlarged and deformed with extensive bone and joint destruction Presence of tophi (large multiple urate deposits)


51 Gouty Arthritis Note the peri-articular swelling & erosions with sparing of the joint

52 Gouty Arthritis

53 First MPJ most often affected Gouty Arthritis Low ph (acidic) & low temperature can trigger urate crystal precipitation in tissues Arthritic degeneration and increased vascularity X-ray findings appear late in disease usually after several years and multiple attacks and diagnosis already established Radiographs of little diagnostic value early Rule out septic or infectious arthritis




54 Gouty Arthritis Tophi



55 Martel s Sign

56 Tophi forming away from the 1 st MPJ Gouty Arthritis

57 Note extra-articular erosions of lesser metatarsal heads.


58 Gout Masquerading as a Neuroma Courtesy Gina Painter, DPM Great Falls, MT



59 Gout Masquerading as a Neuroma Courtesy Gina Painter, DPM Great Falls, MT

60 Gouty Arthritis


61 Gouty Arthritis


62 Gout The Great Imitator

63 Lis Franc Joint involvement is under-reported. Advanced Imaging in Gout: Girish G, Glazebrook KN, Jacobson JA AJR:201, Sept. 2013


64 Gout The Great Imitator

65 Gout The Great Imitator

66 MRI
67 Advanced Imaging in Gout: Girish G, Glazebrook KN, Jacobson JA AJR:201, Sept DECT (Dual Energy CT) Scan Ct scan which utilizes both the normal X-ray as well as a second less powerful X-ray to make the images. (140 and 80 kvp). Assesses attenuation properties of Uric acid deposits. Able to differentiate monosodium urate crystals from calcification.


68 DECT Scan Advanced Imaging in Gout: Girish G, Glazebrook KN, Jacobson JA AJR:201, Sept. 2013

69 70 y/o referred for amputation of forefoot mass.
 consistent with tophaceous")
70 ECT: Dual Energy CT 3D rendered DECT with color mapping demonstrates MSU Crystals (green) consistent with tophaceous gout.

71 Dual-energy CT in Gout A review of current concepts and applications. H Chou, T Chin, W Peh. J Med Radiat Sci: 2017 Mar, 64(1): 41-51



72 TREATMENT
73 TREATMENT Rest Ice Elevation Avoid constrictive sheets/hose/shoe gear Gait assistive devices
74 Ice Therapy During Gout Attack OBJECTIVE: To evaluate the effect of local application of ice on duration and severity of acute gouty arthritis. METHODS: Nineteen patients with acute gout were enrolled and randomized into 2 groups. Group A (n = 10) received topical ice therapy, oral prednisone 30 mg PO tapered to 0 over 6 days and colchicine 0.6 mg/day. Group B was the control group (n = 9), given the same regimen but without the ice therapy. The patients were followed for one week. RESULTS: The mean reduction in pain for those patients treated with ice therapy was 7.75 cm (on 10 cm visual analog scale) with standard deviation +/ compared with 4.42 cm (+/- SD 2.96) for the control group. Using a Wilcoxon rank-sum test there was a significant difference (p = ) in pain reduction between the ice therapy and control groups. CONCLUSION: The group treated with ice had a significantly greater reduction in pain compared with the control group. Although the clinical improvement was impressive, due to the small sample size we could not show statistically significant improvement in all the variables that tended to suggest that effect was more than simply analgesic. Cold applications may be a useful adjunct to treatment of acute gouty arthritis. Local ice therapy during bouts of gouty arthritis: Schlesinger N, Detry MA, Holland BK, et.al. J Rheumatol Feb;29(2):33-14
75 Choi, Hk, Curhan G. Coffee, tea and caffeine consumption and serum uric acid: the Third National Health and Nutrition Examination Survey. Arthritis Rheum. June 2007 Males >40. Coffee and Gout Studied over a period of 12 years. N = 45,869 Drinking 1-3 cups/day lowered gout risk by 8%. Drinking 4-5 cups/day lowered gout risk by 40%. Drinking > 5 cups lowered gout risk by 59%. Drinking Decaf coffee lowered the effect. Drinking Tea did not appear to have a protective affect.
76 TREATMENT Indocin Colchicine NSAID s Corticosteroids Allopurinol
77 Podiatry Management Survey June 2018 Do you prescribe Uric Acid lowering drugs for the management of acute or chronic gout? Yes, for acute gout % Yes, for chronic gout. 6.18% Yes, for acute and chronic gout % No 40.27% N=971

78 Increased levels of Uric Acid and associated Systemic Disease. Systemic Risk
79 Evidence Based Medicine and the Treatment of Gout DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine GORDON K. LAM, MD, FACR NorthEast Rheumatology Medical Director, Northern Region Research Center Atrium Health, Concord, NC
80 CONFLICT OF INTEREST Horizon Pharm, Plc: Speakers Bureau; Advisory Board Selecta Biosciences: Advisory Board
81 OUTLINE Gout from a Rheumatologist s Perspective Treatment of Patient with Acute Gout Flare Colchicine Corticosteroids Indocin/NSAID s Long-term Management of Gout Management of the Recalcitrant Patient Newer Medication Options: Combination therapies, pegloticase Peri-operative Management of the Gout Patient
82 Collaboration between podiatrists & rheumatologists Podiatrists role in gout management today is critical Increased emphasis on comprehensive, collaborative and correlated care amongst healthcare providers First responders of gout flares Surgical management of refractory tophaceous gout Missing link between a patient s PCP & rheumatologist

83 Collaboration between podiatrists & rheumatologists Results Web-based survey demonstrated poor integration of podiatrists into multidisciplinary teams Only 16% reported being part of an established multidisciplinary team 95% expressed interest in professional development for the podiatric management of arthritides Conclusions There are barriers in the involvement of podiatrists in the management rheumatic
84 Overcoming barriers between podiatrists and rheumatologists in caring for gout patients Identify a local rheumatologist who has a common interest in gout Foster a collaborative relationship Establish a procedure for direct contact to refer patients in a timely manner Perform joint community outreach and education Create dual podiatry-rheumatology clinics Develop a co-management strategy Delineate roles Identify common ground
85 When to refer to a rheumatologist To confirm the diagnosis, particularly in patients with atypical presentations To treat chronic, uncontrolled gout Inability to achieve sua < 6.0 mgl with conventional uratelowering therapies at appropriate doses Recurrent flares despite adequate treatment Comorbidities that may limit therapy (e.g. chronic kidney disease, liver disease, heart disease) Complex cases refractory to conventional therapies Initiation of biologic therapy


86 Treatment of gout
87 Overcoming barriers between patients and providers in caring for gout Patients Misunderstand causes of gout Don t realize consequences of untreated gout May not view gout as a chronic disease Non-adherence to treatment plans Unwilling to adopt lifestyle modifications Providers Only manage acute attacks rather than treat gout as a chronic progressive disease Lack urgency to treat Don t adopt treat-to-target strategy Use only fixed doses No communication with patient s other providers

88 Strategy for gout management
89 2012 ACR Gout Treatment Guidelines Treat to Target At minimum, sua <6 mg/dl or sua <5 mg/dl for those with chronic tophaceous gout and Durable improvement in signs and symptoms of gout Reduced frequency of flares Clearance of tophi Urate-lowering therapy Xanthine oxidase inhibitors (Alternative if XOI contraindicated or not tolerated: probenecid) sua target not achieved, continuing disease activity Add uricosuric to XOI* sua target not achieved, continuing disease activity Biologic therapy: pegloticase



90 Maintaining sua <6 mg/dl is associated with reduced risk of recurrent gout flares


91 Appropriate management of gout requires control of both symptoms and urate burden Must address 2 processes simultaneously for successful outcomes: Control flares and symptoms Reduce urate burden
92 NSAIDs Treatment of acute gout: Anti-inflammatories indomethacin: 75 mg three times daily celecoxib: 200 mg twice daily ibuprofen: 800 mg three times daily naproxen 500 mg twice daily Colchicine: 1.2 mg at first sign, then 0.6 mg 1 hour later Steroids Prednisone 20 mg daily x 4 d, 15 mg daily x 4 d, 10 mg daily x 4 d, 5 mg daily x 4 d. Choice of therapy is dependent on patient s comorbidities
93 Treatment of chronic gout: Urate-lowering therapies (ULTs) Small molecules xanthine oxidase inhibitors uricosurics allopurinol probenecid febuxostat lesinurad combination XOIs and uricosurics Biologics allopurinol / lesinurad uricase (pegloticase)
94 Purine catabolism Purines Humans Almost All Other Mammals Hypoxanthine xanthine oxidase X Xanthine xanthine oxidase X Urate Allantoin allopurinol febuxostat allopurinol febuxostat C probenecid lesinurad Urinary Excretion Urinary Excretion



95 Management of refractory gout
96 Refractory gout: Definition Ongoing hyperuricemia or gout flares despite maximum appropriate doses of ULTs Recurrent and disabling gout flares Chronic gout arthropathy +/- bony erosions Visible progressive tophi Progressive physical disability Poor health-related quality of life The combination of severe gout, comorbidities, and polypharmacy can make refractory gout challenging to manage
97 Treatment options for refractory gout Dose escalation of conventional urate lowering therapies: allopurinol to 800 mg daily in divided doses febuxostat to mg daily probenecid to 1000 mg daily in divided doses lesinurad to 200 mg daily Combination therapy: xanthine oxidase inhibitor + uricosuric Lifestyle modifications diet - vitamin C - avoidance of high fructose corn syrup exercise - losartan for diuretics - low fat dairy products cherry extract - fenofibrate for niacin Biologic therapy pegloticase

98 Pegloticase: a biologic for the treatment of refractory gout pegloticase is recombinant modified porcine uricase surrounded by polyethylene glycol (PEG) Uricase PEG decreases immunogenicity and increases half-life of the molecule mpeg pegloticase catalyzes the breakdown of uric acid to allantoin allantoin is more water soluble than uric acid and is readily excreted by the kidneys, leading to lowering of sua levels Cross sectional image Figure courtesy of Toby Sannan and Christopher Hadad, Ohio State University.

99 Purine catabolism Purines Humans Almost All Other Mammals Hypoxanthine xanthine oxidase X Xanthine xanthine oxidase X Urate Allantoin allopurinol febuxostat allopurinol febuxostat C probenecid lesinurad Urinary Excretion Urinary Excretion
100 Pegloticase: phase III trials Two replicate, multicenter, randomized, double-blind, placebocontrolled trials of 6 months duration Subjects included adults with chronic refractory gout 8 mg pegloticase infusions every 2 weeks vs. placebo PRIMARY ENDPOINT Percentage of plasma uric acid (PUA) responders versus placebo Complete Responders Patients who achieved PUA <6 mg/dl for 80% of the time during months 3 and 6 Incomplete Responders Patients who did not sustain PUA <6 mg/dl throughout the trial Patients who withdrew before the final visit SECONDARY ENDPOINT Complete resolution (CR) of tophi Defined as 100% resolution of at least 1 target tophus, with no new or progressive tophi
101 Mean sua (mg/dl) Pooled trial results: Complete responders of patients had a complete response Time (Weeks) These patients maintained sua levels below 6 mg/dl 80% of the time at months 3 and 6 versus 0% for placebo (P<0.001)
102 Mean sua (mg/dl) Pooled trial results: Incomplete responders Loss of uric acid response Placebo (n=43) KRYSTEXXA incomplete responder (n=49) of patients had an incomplete response Time (Weeks) These patients achieved a reduction in sua for a mean of 7 weeks, allowing some clearance of the urate burden (P<0.001). The response was not durable; therefore, they did not meet the primary endpoint.

103 Baseline Secondary endpoint: Tophus resolution
104 Secondary endpoint: Tophus resolution Complete resolution of tophi Defined as 100% resolution of at least 1 tophus, with no new or progressive tophi 3 Months 22% of patients (n=62) achieved complete resolution of tophi (P=0.01) 3 6 Months 45% Complete resolution of tophi These results include patients who experienced a complete response as well as patients who experienced an incomplete response in the primary endpoint 3 45% (18/40) of patients treated with pegloticase achieved complete resolution of their target tophus versus 8% (2/25) of patients receiving placebo (P=0.002)


105 Secondary endpoint: Tophus resolution

106 Secondary endpoint: Tophus resolution

107 Secondary endpoint: Tophus resolution
108 Safety: Adverse events Most common adverse events (occurring >5% of patients) Gout flares Contusion or ecchymosis Infusion reactions Nasopharyngitis Nausea Constipation Vomiting Chest pain
109 Adverse events: Infusion reactions Most infusion reactions (IRs) occurred when sua levels were >6 mg/dl (91% vs 4.5%) If sua levels increase to >6 mg/dl on therapy, patient is likely to have anti-pegloticase antibodies, and may be at increased risk of infusion reactions If pegloticase is discontinued after the sua >6 mg/dl, most IRs could be avoided
110 Using sua as a predictive biomarker: Stopping rule Check a sua 48 hours before each pegloticase infusion: If SUA <6 mg/dl, infusion can be given If SUA >6 mg/dl, consider discontinuing treatment, particularly when 2 consecutive sua levels >6 mg/dl are observed If this stopping rule is utilized, the majority of infusion reactions can be avoided No other biologic in Rheumatology has a predictive biomarker
111 Safety: Pre-infusion protocol Infusion pre-medications Antihistamine the night before and the morning of each infusion Acetaminophen the morning of the infusion Corticosteroids prior to each infusion Gout flare prophylaxis Colchicine, NSAIDS, or both Initiate 1 week before starting pegloticase Continue for at least 6 months Oral urate-lowering therapy Discontinue any oral ULT the day before starting pegloticase to prevent confounding of the sua predictive biomarker effect May reinitiate once pegloticase course is completed



112 Perioperative management of the gout patient
113 Perioperative considerations Gout has many associated comorbidities: hypertenstion diabetes mellitus coronary heart disease hyperlipidemia congestive heart failure chronic kidney disease atrial fibrillation peripheral vascular disease Appropriate medical clearance should be obtained prior to any surgical intervention Post-operative gout flares are common
114 Perioperative management Optimize ULT preoperatively Risk of gout attacks decreases if sua <6 mg/dl Maintain ULT until NPO status on day of surgery Reinitiate as soon as appropriate postoperatively May consider short prophylactic course preoperatively Low-dose NSAIDs or colchicine 0.6 mg QD/BID If gout flares postoperatively, treat with anti-inflammatories High-dose NSAIDS, colchicine, or steroids
115 Summary Gout is a chronic, progressive arthritis caused by hyperuricemia with associated chronic inflammation Podiatrists play a critical role in the management of gout Collaboration between podiatrists and rheumatologists can lead to optimal care of the gout patient Appropriate treatment of gout includes treating acute flares with anti-inflammatories AND treating the underlying hyperuricemia with urate-lowering therapies
116 Summary Treatment for acute gout flares include NSAIDs, colchicine, and steroids ULTs include xanthine oxidase inhibitors (allopurinol, febuxostat), uricosurics (probenecid, lesinurad), combination therapies, and biologics (pegloticase) Pegloticase is the first biologic and only FDA-approved treatment option for patients with refractory gout Optimization sua <6 mg/dl preoperatively reduces risk of gout flares postoperatively
117 Questions??? Thank You! GORDON K. LAM, MD, FACR DANIEL P. EVANS, DPM, FACFAOM
1. To review the diagnosis of gout and its differential. 2. To understand the four stages of gout
 Objectives 1. To review the diagnosis of gout and its differential GOUT 2. To understand the four stages of gout 3. To develop an approach for the acute treatment of gout Anthony Lim 9/13/12 Cycle 3 4.
Objectives 1. To review the diagnosis of gout and its differential GOUT 2. To understand the four stages of gout 3. To develop an approach for the acute treatment of gout Anthony Lim 9/13/12 Cycle 3 4.
CHAPTER:2 GOUT. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:2 GOUT BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY DEFINITION Gout is defined as a peripheral arthritis, resulting from the deposition of MSU crystals
CHAPTER:2 GOUT BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY DEFINITION Gout is defined as a peripheral arthritis, resulting from the deposition of MSU crystals
OBJECTIVES GOUT GOUTY INFLAMMATION 6/10/2016 GOUT INCIDENCE AND PREVALENCE MONOSODIUM URATE CRYSTAL DEPOSITION DISEASE
 GOUT Lisa Talbert, MD Family Medicine Update June 15, 2016 OBJECTIVES To be familiar with the clinical presentation and pathophysiology of gouty arthritis Be able to incorporate current guidelines when
GOUT Lisa Talbert, MD Family Medicine Update June 15, 2016 OBJECTIVES To be familiar with the clinical presentation and pathophysiology of gouty arthritis Be able to incorporate current guidelines when
Gout 2.0. Scott Vogelgesang, M.D. Division of Immunology: Rheumatology & Allergy
 Gout 2.0 Scott Vogelgesang, M.D. Division of Immunology: Rheumatology & Allergy Case 48 year old man presents with swollen, painful left toe that started overnight. Didn t hurt when he went to bed. No
Gout 2.0 Scott Vogelgesang, M.D. Division of Immunology: Rheumatology & Allergy Case 48 year old man presents with swollen, painful left toe that started overnight. Didn t hurt when he went to bed. No
Achieving Gout Goals in Your Practice An Interview with Paul P. Doghramji, MD, FAAFP
 Achieving Gout Goals in Your Practice An Interview with Paul P. Doghramji, MD, FAAFP Dr. Paul Doghramji is attending physician at the Pottstown Memorial Medical Center and medical director of Health Services
Achieving Gout Goals in Your Practice An Interview with Paul P. Doghramji, MD, FAAFP Dr. Paul Doghramji is attending physician at the Pottstown Memorial Medical Center and medical director of Health Services
A Patient s Guide to Gout. Foot and Ankle Center of Massachusetts, P.C.
 A Patient s Guide to Gout Welcome to Foot and Ankle Center of Massachusetts, where we believe in accelerating your learning curve with educational materials that are clearly written and professionally
A Patient s Guide to Gout Welcome to Foot and Ankle Center of Massachusetts, where we believe in accelerating your learning curve with educational materials that are clearly written and professionally
Case presentation. serum uric acid = 11.5 mg/dl 24-hour uric acid excretion = 300 mg
 GOUT 55 y/o male 12 hours pain in my big toe & ankle went to bed last night feeling fine felt as if had broken toe this morning similar problems in right ankle & left wrist Case presentation lab studies
GOUT 55 y/o male 12 hours pain in my big toe & ankle went to bed last night feeling fine felt as if had broken toe this morning similar problems in right ankle & left wrist Case presentation lab studies
Gout Hanan Abdel Rehim
 Review article 35 Gout Hanan Abdel Rehim Department of Internal Medicine, Kasr-Al Aini School of Medicine, Cairo University, Cairo, Egypt Correspondence to Hanan Abdel Rehim, MD, 11 Ismaiel Wahby Street,
Review article 35 Gout Hanan Abdel Rehim Department of Internal Medicine, Kasr-Al Aini School of Medicine, Cairo University, Cairo, Egypt Correspondence to Hanan Abdel Rehim, MD, 11 Ismaiel Wahby Street,
Gout- Treatment Updates. Harinder Singh, MD Rheumatology Mercy Internal Medicine Clinic Mason City, IA
 Gout- Treatment Updates Harinder Singh, MD Rheumatology Mercy Internal Medicine Clinic Mason City, IA Gout Outline of purine metabolism: (1) amidophosphoribosyltransferase (2) hypoxanthine-guanine phosphoribosyltransferase
Gout- Treatment Updates Harinder Singh, MD Rheumatology Mercy Internal Medicine Clinic Mason City, IA Gout Outline of purine metabolism: (1) amidophosphoribosyltransferase (2) hypoxanthine-guanine phosphoribosyltransferase
Update on Gout for GPs
 Update on Gout for GPs Dr Patrick Kiely PhD FRCP Consultant Physician and Rheumatologist St George s, London 2/3 1/3 Gut bacteria have uricase Chronic erosive arthropathy Clinical spectrum Making the diagnosis
Update on Gout for GPs Dr Patrick Kiely PhD FRCP Consultant Physician and Rheumatologist St George s, London 2/3 1/3 Gut bacteria have uricase Chronic erosive arthropathy Clinical spectrum Making the diagnosis
Gout A rapid review. Jeremy Jones
 Gout A rapid review Jeremy Jones The Hyperuricemia Cascade Dietary purines Tissue nucleic acids Urate Endogenous purine synthesis Overproduction Hyperuricemia Underexcretion Silent tissue deposition Gout
Gout A rapid review Jeremy Jones The Hyperuricemia Cascade Dietary purines Tissue nucleic acids Urate Endogenous purine synthesis Overproduction Hyperuricemia Underexcretion Silent tissue deposition Gout
Rheumatoid arthritis, seronegative spondylarthritides and gout. György Nagy
 Rheumatoid arthritis, seronegative spondylarthritides and gout György Nagy Dec 4, 2017 Rheumatoid arthritis Rheumatoid arthritis Chronic, progressive, autoimmune disorder of the joints with extra-articular
Rheumatoid arthritis, seronegative spondylarthritides and gout György Nagy Dec 4, 2017 Rheumatoid arthritis Rheumatoid arthritis Chronic, progressive, autoimmune disorder of the joints with extra-articular
Gout -revisited. Shrenik Shah
 Gout -revisited Shrenik Shah definition Monosodium urate (MSU) crystal deposition episodic and later persistent joint inflammation and tophi All MSU crystal deposition- broader definition EULAR- European
Gout -revisited Shrenik Shah definition Monosodium urate (MSU) crystal deposition episodic and later persistent joint inflammation and tophi All MSU crystal deposition- broader definition EULAR- European
GOUT. Dr Krishnan Baburaj West herts NHS Trust
 GOUT Dr Krishnan Baburaj West herts NHS Trust podagra Gout A disease of kings, the king of diseases History Louis XIV Emperor Augustus Henry VIII Introduction Gout an inflammatory arthritic condition that
GOUT Dr Krishnan Baburaj West herts NHS Trust podagra Gout A disease of kings, the king of diseases History Louis XIV Emperor Augustus Henry VIII Introduction Gout an inflammatory arthritic condition that
Gout Treatment Guidelines
 Gout Treatment Guidelines Gout is a disorder that manifests as a spectrum of clinical and pathologic features built on a foundation of an excess body burden of uric acid, manifested in part by hyperuricemia,
Gout Treatment Guidelines Gout is a disorder that manifests as a spectrum of clinical and pathologic features built on a foundation of an excess body burden of uric acid, manifested in part by hyperuricemia,
Managing Gout A Review of the Research for Adults
 Managing Gout A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional* has said that you have gout. You are age 18 or
Managing Gout A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional* has said that you have gout. You are age 18 or
Rheumatology Cases for the Internist
 Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
MEDICAL POLICY PEGLOTICASE (KRYSTEXXA ) POLICY NUMBER MP POLICY TITLE. Original Issue Date (Created): January 1, 2011
 POLICY NUMBER MP POLICY TITLE. Original Issue Date (Created): January 1, 2011") Original Issue Date (Created): January 1, 2011 Most Recent Review Date (Revised): September 24, 2013 Effective Date: November 1, 2013 I. POLICY PREAUTHORIZATION REQUIRED Note: Requests for pegloticase
Original Issue Date (Created): January 1, 2011 Most Recent Review Date (Revised): September 24, 2013 Effective Date: November 1, 2013 I. POLICY PREAUTHORIZATION REQUIRED Note: Requests for pegloticase
Podcast (Video Recorded Lecture Series): Gout for the USMLE Step One Exam. Howard J. Sachs, MD
: Gout for the USMLE Step One Exam. Howard J. Sachs, MD") Podcast (Video Recorded Lecture Series): Gout for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com Podcast (Video Recorded Lecture Series): Gout for the
Podcast (Video Recorded Lecture Series): Gout for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com Podcast (Video Recorded Lecture Series): Gout for the
GOUT IN THE ELDERLY. Learning Objectives. Disclosure. Geriatric Grand Rounds. Geriatric Grand Rounds
 Visit web sites: Tuesday, June 2, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this event
Visit web sites: Tuesday, June 2, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this event
3/2/2014. Got Gout? Get a Plumber. Objectives. Disclosures
 Got Gout? Get a Plumber. Heidi Garcia, PA-C Department of Rheumatology Division of Internal Medicine Mayo Clinic Arizona 2013 MFMER slide-1 Objectives Recall some of the history of Gout. Describe the pathophysiology
Got Gout? Get a Plumber. Heidi Garcia, PA-C Department of Rheumatology Division of Internal Medicine Mayo Clinic Arizona 2013 MFMER slide-1 Objectives Recall some of the history of Gout. Describe the pathophysiology
Gout. Clinical features Most commonly affects middle-aged males. It is an acute and usually relapsing selflimiting
 Gout Gout is a syndrome caused by an inflammatory response to the formation of monosodium urate monohydrate crystals which develop secondary to hyperuricemia. Acute and chronic forms are recognized. Hyperuricemia
Gout Gout is a syndrome caused by an inflammatory response to the formation of monosodium urate monohydrate crystals which develop secondary to hyperuricemia. Acute and chronic forms are recognized. Hyperuricemia
Subject: Krystexxa (pegloticase) Original Effective Date: 06/26/13. Policy Number: MCP-138. Revision Date(s):
 Original Effective Date: 06/26/13. Policy Number: MCP-138. Revision Date(s):") Subject: Krystexxa (pegloticase) Original Effective Date: 06/26/13 Policy Number: MCP-138 Revision Date(s): Review Date(s): 12/16/15; 6/15/2016; 3/21/2017 DISCLAIMER This Molina Clinical Policy (MCP) is
Subject: Krystexxa (pegloticase) Original Effective Date: 06/26/13 Policy Number: MCP-138 Revision Date(s): Review Date(s): 12/16/15; 6/15/2016; 3/21/2017 DISCLAIMER This Molina Clinical Policy (MCP) is
Crystal-Induced Arthritis. Rajesh Kataria, D.O. Southern Ohio Rheumatology
 Crystal-Induced Arthritis Rajesh Kataria, D.O. Southern Ohio Rheumatology Disclosures Speaker: Rajesh Kataria, D.O. Relationships with commercial interests: Speakers Bureau - Horizon Presentation will
Crystal-Induced Arthritis Rajesh Kataria, D.O. Southern Ohio Rheumatology Disclosures Speaker: Rajesh Kataria, D.O. Relationships with commercial interests: Speakers Bureau - Horizon Presentation will
Gout: Develop treatment plan in William Jones, MS, RPh
 Gout: Develop treatment plan in 2013 William Jones, MS, RPh (wnjones49@cox.net) Objectives Describe acute gouty arthritis Tx Describe Tx of chronic gouty arthritis. Define the target serum uric acid concentration
Gout: Develop treatment plan in 2013 William Jones, MS, RPh (wnjones49@cox.net) Objectives Describe acute gouty arthritis Tx Describe Tx of chronic gouty arthritis. Define the target serum uric acid concentration
Lesinurad in Combination With a Xanthine Oxidase Inhibitor for Treatment of Hyperuricemia Associated With Gout
 Lesinurad in Combination With a Xanthine Oxidase Inhibitor for Treatment of Hyperuricemia Associated With Gout Briefing Document for the Arthritis Advisory Committee Meeting Date: 23 October 215 Ardea
Lesinurad in Combination With a Xanthine Oxidase Inhibitor for Treatment of Hyperuricemia Associated With Gout Briefing Document for the Arthritis Advisory Committee Meeting Date: 23 October 215 Ardea
pegloticase (Krystexxa )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Drugs Used to Treat Gout. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used to Treat Gout Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Gout is a metabolic disease characterized by recurrent episodes of acute arthritis
Drugs Used to Treat Gout Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Gout is a metabolic disease characterized by recurrent episodes of acute arthritis
Urate Lowering Efficacy of Febuxostat Versus Allopurinol in Hyperuricemic Patients with Gout
 Philippine Journal of Internal Medicine Meta-Analysis Urate Lowering Efficacy of Febuxostat Versus Allopurinol in Hyperuricemic Patients with Gout Erika Bianca S. Villazor-Isidro, M.D.*; John Carlo G.
Philippine Journal of Internal Medicine Meta-Analysis Urate Lowering Efficacy of Febuxostat Versus Allopurinol in Hyperuricemic Patients with Gout Erika Bianca S. Villazor-Isidro, M.D.*; John Carlo G.
Crystal induced arthropathies. Dr. Amitesh Aggarwal
 Crystal induced arthropathies Dr. Amitesh Aggarwal 1 Crystal induced Arthropathies Gout Pseudogout Debilitating illnesses; Recurrent episodes of pain and joint inflammation; Formation and deposition of
Crystal induced arthropathies Dr. Amitesh Aggarwal 1 Crystal induced Arthropathies Gout Pseudogout Debilitating illnesses; Recurrent episodes of pain and joint inflammation; Formation and deposition of
Cost-effectiveness of lesinurad (Zurampic ) for the treatment of adult patients with gout
 for the treatment of adult patients with gout") Cost-effectiveness of lesinurad (Zurampic ) for the treatment of adult patients with gout The NCPE has issued a recommendation regarding the cost-effectiveness of Lesinurad (Zurampic ) in combination with
Cost-effectiveness of lesinurad (Zurampic ) for the treatment of adult patients with gout The NCPE has issued a recommendation regarding the cost-effectiveness of Lesinurad (Zurampic ) in combination with
Therapy for Gout: The Past
 Advances in Therapy for Gout: 2011 The Past, Present, and Future Therapy for Gout: The Past May 22, 1997 Pity a Tyrannosaur? Sue Had Gout By MALCOLM W. BROWNE Jonathan Graf, M.D. Associate Professor of
Advances in Therapy for Gout: 2011 The Past, Present, and Future Therapy for Gout: The Past May 22, 1997 Pity a Tyrannosaur? Sue Had Gout By MALCOLM W. BROWNE Jonathan Graf, M.D. Associate Professor of
Enhanced Primary Care Pathway: Gout
 Enhanced Primary Care Pathway: Gout 1. Focused summary of gout relevant to primary care Significance: Gout is a chronic, progressive, inflammatory disease requiring appropriate long-term management. Gout
Enhanced Primary Care Pathway: Gout 1. Focused summary of gout relevant to primary care Significance: Gout is a chronic, progressive, inflammatory disease requiring appropriate long-term management. Gout
New Drug Evaluation: lesinurad tablet, oral
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
GOUT & PSEUDOGOUT OPSC 2018 HOWARD L. FEINBERG, D.O., F.A.C.O.I.., F.A.C.R.
 GOUT & PSEUDOGOUT OPSC 2018 HOWARD L. FEINBERG, D.O., F.A.C.O.I.., F.A.C.R. Everything in excess is opposed by nature Eunuchs do not take the gout, nor become bald. GOUT Hyperuricemia is not gout Gout
GOUT & PSEUDOGOUT OPSC 2018 HOWARD L. FEINBERG, D.O., F.A.C.O.I.., F.A.C.R. Everything in excess is opposed by nature Eunuchs do not take the gout, nor become bald. GOUT Hyperuricemia is not gout Gout
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Krystexxa) Reference Number: CP.CPA.57 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Krystexxa) Reference Number: CP.CPA.57 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Gout basics. Update on Gout. Production of uric acid. Gout basics. Crystal induced inflammation. Gout calculator. The important role of ultrasound
 Update on Gout The important role of ultrasound Cheung C Yue, M.D. Gout basics Hyperuricemia gout Over 5 years, 22% >9 mg/dl develop gout Man 3-4 times more than women Risks: thiazide, cyclosporin, low
Update on Gout The important role of ultrasound Cheung C Yue, M.D. Gout basics Hyperuricemia gout Over 5 years, 22% >9 mg/dl develop gout Man 3-4 times more than women Risks: thiazide, cyclosporin, low
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Krystexxa) Reference Number: CP.PHAR.115 Effective Date: 06.01.13 Last Review Date: 02.19 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important Reminder
Clinical Policy: (Krystexxa) Reference Number: CP.PHAR.115 Effective Date: 06.01.13 Last Review Date: 02.19 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important Reminder
Gout: Let s Be Crystal Clear. Dr. Philip A. Baer Seacourses Asia CME December 2017
 Gout: Let s Be Crystal Clear Dr. Philip A. Baer Seacourses Asia CME December 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Gout: Let s Be Crystal Clear Dr. Philip A. Baer Seacourses Asia CME December 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Uloric Step Therapy Program
 Uloric Step Therapy Program Policy Number: 5.01.584 Last Review: 7/2017 Origination: 7/2014 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for brand
Uloric Step Therapy Program Policy Number: 5.01.584 Last Review: 7/2017 Origination: 7/2014 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for brand
An update on the management of gout
 An update on the management of gout 8 The management of gout involves treatment of an acute attack, lifestyle modification and urate lowering treatment to achieve a target serum urate level. Recent evidence
An update on the management of gout 8 The management of gout involves treatment of an acute attack, lifestyle modification and urate lowering treatment to achieve a target serum urate level. Recent evidence
New Drug Evaluation: lesinurad tablet, oral
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Lecture 8 Gout Hinch. Pathogenesis of acute attacks
 Gout: disease characterized by deposition of monosodium crystals in soft tissues (cartilage, tendons, bursa) recurrent episodes of acute joint pain & inflammation Pathogenesis of acute attacks Epidemiology:
Gout: disease characterized by deposition of monosodium crystals in soft tissues (cartilage, tendons, bursa) recurrent episodes of acute joint pain & inflammation Pathogenesis of acute attacks Epidemiology:
Gout: Update in therapeutics
 Summary Gout: Update in therapeutics 29/11/14 Caroline van Durme CHU de Liège Maastricht University Medical Centre+ Why treating gout? Guidelines: ACR 12 Drugs: Colchicine Allopurinol: what about the kidney?
Summary Gout: Update in therapeutics 29/11/14 Caroline van Durme CHU de Liège Maastricht University Medical Centre+ Why treating gout? Guidelines: ACR 12 Drugs: Colchicine Allopurinol: what about the kidney?
Clinical Practice Guideline. Gout. Version
 Clinical Practice Guideline Gout Version 1.1.2017 August 2017 Table of Contents Introduction...5 Stages of Gout...7 Asymptomatic Hyperuricemia... 7 Acute Intermittent Gout... 7 Advanced Gout... 8 Diagnosis...8
Clinical Practice Guideline Gout Version 1.1.2017 August 2017 Table of Contents Introduction...5 Stages of Gout...7 Asymptomatic Hyperuricemia... 7 Acute Intermittent Gout... 7 Advanced Gout... 8 Diagnosis...8
Krystexxa (pegloticase) Document Number: IC-0158
 Document Number: IC-0158") Krystexxa (pegloticase) Document Number: IC-0158 Last Review Date: 06/27/2017 Date of Origin: 02/07/20103 Dates Reviewed: 11/2013, 08/2014, 07/2015, 07/2016, 09/2016, 12/2016, 03/2017, 06/2017 I. Length
Krystexxa (pegloticase) Document Number: IC-0158 Last Review Date: 06/27/2017 Date of Origin: 02/07/20103 Dates Reviewed: 11/2013, 08/2014, 07/2015, 07/2016, 09/2016, 12/2016, 03/2017, 06/2017 I. Length
Diagnosis and Management of Gout in 2011
 October 18, 2011 Early and accurate gout diagnosis and disease management are essential. Making the clinical diagnosis takes into consideration the differential diagnosis supported by the use of clinical,
October 18, 2011 Early and accurate gout diagnosis and disease management are essential. Making the clinical diagnosis takes into consideration the differential diagnosis supported by the use of clinical,
COMPARATIVE EVALUATION OF EFFICACY AND SAFETY PROFILE OF FEBUXOSTAT WITH ALLOPURINOL IN PATIENTS WITH HYPERURICEMIA AND GOUT
 Int. J. Pharm. Med. & Bio. Sc. 2013 P K Agarwal and Bijay Kumar, 2013 Research Paper ISSN 2278 5221 www.ijpmbs.com Vol. 2, No. 4, October 2013 2013 IJPMBS. All Rights Reserved COMPARATIVE EVALUATION OF
Int. J. Pharm. Med. & Bio. Sc. 2013 P K Agarwal and Bijay Kumar, 2013 Research Paper ISSN 2278 5221 www.ijpmbs.com Vol. 2, No. 4, October 2013 2013 IJPMBS. All Rights Reserved COMPARATIVE EVALUATION OF
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 24 June 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 24 June 2009 ADENURIC 80 mg, film-coated tablets B/28 (CIP code: 385 724-4) B/84 (CIP code: 572 820-3) ADENURIC 120
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 24 June 2009 ADENURIC 80 mg, film-coated tablets B/28 (CIP code: 385 724-4) B/84 (CIP code: 572 820-3) ADENURIC 120
Acute hot swollen joint. Dr Edward Roddy Senior Lecturer in Rheumatology and Consultant Rheumatologist
 Acute hot swollen joint Dr Edward Roddy Senior Lecturer in Rheumatology and Consultant Rheumatologist Acute monoarthritis: differential diagnosis Septic arthritis Crystal arthritis (gout, pseudogout) Haemarthrosis
Acute hot swollen joint Dr Edward Roddy Senior Lecturer in Rheumatology and Consultant Rheumatologist Acute monoarthritis: differential diagnosis Septic arthritis Crystal arthritis (gout, pseudogout) Haemarthrosis
What will happen in the future? How will gout be diagnosed? How is gout treated? prevent
 Rheumatology Day Unit Dr J Hamilton 0191 4458359 0191 4455240 (9-5 Mon-Fri) Dr C Heycock 0191 4452198 Answer phone on 24hours Dr C Kelly 0191 4452193 Dr V Saravanan 0191 4456055 Dr M Rynne 0191 4458359
Rheumatology Day Unit Dr J Hamilton 0191 4458359 0191 4455240 (9-5 Mon-Fri) Dr C Heycock 0191 4452198 Answer phone on 24hours Dr C Kelly 0191 4452193 Dr V Saravanan 0191 4456055 Dr M Rynne 0191 4458359
Therapy for Gout: The Past
 Advances in Therapy for Gout: 2014 The Past, Present, and Future Therapy for Gout: The Past May 22, 1997 Pity a Tyrannosaur? Sue Had Gout By MALCOLM W. BROWNE Jonathan Graf, M.D. Associate Professor of
Advances in Therapy for Gout: 2014 The Past, Present, and Future Therapy for Gout: The Past May 22, 1997 Pity a Tyrannosaur? Sue Had Gout By MALCOLM W. BROWNE Jonathan Graf, M.D. Associate Professor of
GOUT GO FOR SIX WITH. Everything You Need to Know About Gout & Uric Acid PLUS:
 GO FOR SIX WITH Everything You Need to Know About Gout & Uric Acid GOUT PLUS: How to gain control of symptoms A gout-friendly eating style Medication recommendations to discuss with your doctor Lifestyle
GO FOR SIX WITH Everything You Need to Know About Gout & Uric Acid GOUT PLUS: How to gain control of symptoms A gout-friendly eating style Medication recommendations to discuss with your doctor Lifestyle
Krystexxa. Krystexxa (pegloticase) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.14 Subject: Krystexxa Page: 1 of 5 Last Review Date: March 16, 2018 Krystexxa Description Krystexxa
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.14 Subject: Krystexxa Page: 1 of 5 Last Review Date: March 16, 2018 Krystexxa Description Krystexxa
Plus: How to gain control of symptoms A gout-friendly eating style Lifestyle changes that can help prevent future attacks
 about Gout What You Need to Know about Gout & Uric Acid Plus: How to gain control of symptoms A gout-friendly eating style Lifestyle changes that can help prevent future attacks We re doing everything
about Gout What You Need to Know about Gout & Uric Acid Plus: How to gain control of symptoms A gout-friendly eating style Lifestyle changes that can help prevent future attacks We re doing everything
uric acid Non electrolytes of the plasma
 73 uric acid Non electrolytes of the plasma 1 Purines and uric acid Fig 2 JFI Uric acid is the major product of catabolism of the purine nucleosides adenosine and guanosine, Uric acid is sparingly soluble
73 uric acid Non electrolytes of the plasma 1 Purines and uric acid Fig 2 JFI Uric acid is the major product of catabolism of the purine nucleosides adenosine and guanosine, Uric acid is sparingly soluble
Retreatment with Pegloticase after a Gap in Therapy in Patients with Gout: A Report of Four Cases
 Rheumatol Ther (2018) 5:583 594 https://doi.org/10.1007/s40744-018-0111-9 CASE SERIES Retreatment with Pegloticase after a Gap in Therapy in Patients with Gout: A Report of Four Cases Allan H. Morton.
Rheumatol Ther (2018) 5:583 594 https://doi.org/10.1007/s40744-018-0111-9 CASE SERIES Retreatment with Pegloticase after a Gap in Therapy in Patients with Gout: A Report of Four Cases Allan H. Morton.
Dose of celecoxib in gout attack attack
 Dose of celecoxib in gout attack Gout is a disease characterized by an abnormal metabolism of uric acid, resulting in an excess of uric acid in the tissues and blood. People with gout either produce too
Dose of celecoxib in gout attack Gout is a disease characterized by an abnormal metabolism of uric acid, resulting in an excess of uric acid in the tissues and blood. People with gout either produce too
Literature Scan: Analgesics for Gout. Month/Year of Review: April 2015 Date of Last Review: January 2014
 Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503 947 1119 Copyright 2012 Oregon State University. All Rights
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503 947 1119 Copyright 2012 Oregon State University. All Rights
Initial Phase 3 Studies Results for Rilonacept in the Prevention of Gout Flares in Patients Initiating Uric Acid-lowering Therapy and the Treatment
 Initial Phase 3 Studies Results for Rilonacept in the Prevention of Gout Flares in Patients Initiating Uric Acid-lowering Therapy and the Treatment of Patients in the Midst of an Acute Gout Attack Investor
Initial Phase 3 Studies Results for Rilonacept in the Prevention of Gout Flares in Patients Initiating Uric Acid-lowering Therapy and the Treatment of Patients in the Midst of an Acute Gout Attack Investor
ACP Rheumatology Pearls. Adam Q Carlson MD Assistant Professor UVA Rheumatology
 ACP Rheumatology Pearls Adam Q Carlson MD Assistant Professor UVA Rheumatology Disclosures I have no personal or professional disclosures Case #1 27 yo woman with a history of systemic lupus complicated
ACP Rheumatology Pearls Adam Q Carlson MD Assistant Professor UVA Rheumatology Disclosures I have no personal or professional disclosures Case #1 27 yo woman with a history of systemic lupus complicated
4/1/2011. New Developments in Gout. Conflict of Interest Declaration. Objectives
 New Developments in Gout Tatum N. Mead, Pharm.D. Clinical Assistant Professor UMKC SOP meadt@umkc.edu April 16, 2011 1 Conflict of Interest Declaration I have no actual or potential conflict of interest
New Developments in Gout Tatum N. Mead, Pharm.D. Clinical Assistant Professor UMKC SOP meadt@umkc.edu April 16, 2011 1 Conflict of Interest Declaration I have no actual or potential conflict of interest
Study of Febuxostat for the Management of Hyperuricemia in Gout
 Human Journals Review Article October 2015 Vol.:4, Issue:3 All rights are reserved by Sachin S. Shinde et al. Study of Febuxostat for the Management of Hyperuricemia in Gout Keywords: Febuxostat, Hyperuricemia,
Human Journals Review Article October 2015 Vol.:4, Issue:3 All rights are reserved by Sachin S. Shinde et al. Study of Febuxostat for the Management of Hyperuricemia in Gout Keywords: Febuxostat, Hyperuricemia,
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: Gout and Pseudogout Wayne Blount MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: Gout and Pseudogout Wayne Blount MD Speaker has no disclosures
Gout. Edward Roddy, 1 Christian D Mallen, 1 Michael Doherty 2 CLINICAL REVIEW
 Gout Edward Roddy, 1 Christian D Mallen, 1 Michael Doherty 2 1 Arthritis Research UK Primary Care Centre, Primary Care Sciences, Keele University, Keele ST5 5BG, UK 2 Academic Rheumatology, University
Gout Edward Roddy, 1 Christian D Mallen, 1 Michael Doherty 2 1 Arthritis Research UK Primary Care Centre, Primary Care Sciences, Keele University, Keele ST5 5BG, UK 2 Academic Rheumatology, University
Long-term Treatment of Gout: New Opportunities for Improved Outcomes
 Long-term Treatment of Gout: New Opportunities for Improved Outcomes Paul P. Doghramji, MD, FAAFP CONTINUING MEDICAL EDUCATION LEARNING OBJECTIVES Make a presumptive diagnosis of gout based on history
Long-term Treatment of Gout: New Opportunities for Improved Outcomes Paul P. Doghramji, MD, FAAFP CONTINUING MEDICAL EDUCATION LEARNING OBJECTIVES Make a presumptive diagnosis of gout based on history
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES
 Generic Brand HICL GCN Exception/Other PEGLOTICASE KRYSTEXXA 37154 GUIDELINES FOR USE 1. Does the patient have a diagnosis of symptomatic chronic gout (prior to initiating Krystexxa therapy) with clinical
Generic Brand HICL GCN Exception/Other PEGLOTICASE KRYSTEXXA 37154 GUIDELINES FOR USE 1. Does the patient have a diagnosis of symptomatic chronic gout (prior to initiating Krystexxa therapy) with clinical
Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved.
 14 The Nurse Practitioner Vol. 41, No. 14 www.tnpj.com 2.5 CONTACT HOURS 2.5 CONTACT HOURS Gout An update on for primary care providers Abstract: This article discusses the current beliefs regarding the
14 The Nurse Practitioner Vol. 41, No. 14 www.tnpj.com 2.5 CONTACT HOURS 2.5 CONTACT HOURS Gout An update on for primary care providers Abstract: This article discusses the current beliefs regarding the
For more information about how to cite these materials visit
 Author(s): Seetha Monrad, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Seetha Monrad, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Current treatment options for acute and chronic gout
 DRUG REVIEW n Current treatment options for acute and chronic gout Kelsey Jordan FRCP and Andrew Jeffries PGDip, MRCP Gout is the only curable form of arthritis, yet only a third of patients with chronic
DRUG REVIEW n Current treatment options for acute and chronic gout Kelsey Jordan FRCP and Andrew Jeffries PGDip, MRCP Gout is the only curable form of arthritis, yet only a third of patients with chronic
The 2010 Competency Standards addressed by this activity include (but may not be limited to): 4.2.2, 4.2.3, 6.1.2, 6.2.1, 7.1.2, 7.1.3,
: 4.2.2, 4.2.3, 6.1.2, 6.2.1, 7.1.2, 7.1.3,") UPDATE ON GOUT Learning objectives: After completing this activity, pharmacists should be able to: 1. describe the mechanisms underlying hyperuricaemia 2. state the risk factors for development of gout
UPDATE ON GOUT Learning objectives: After completing this activity, pharmacists should be able to: 1. describe the mechanisms underlying hyperuricaemia 2. state the risk factors for development of gout
Mono-articular Joint Complaints
 Mono-articular Joint Complaints Derrick J. Todd, M.D., Ph.D. Associate Physician Department of Rheumatology, Immunology, and Allergy Brigham and Women s Hospital Instructor of Medicine Harvard Medical
Mono-articular Joint Complaints Derrick J. Todd, M.D., Ph.D. Associate Physician Department of Rheumatology, Immunology, and Allergy Brigham and Women s Hospital Instructor of Medicine Harvard Medical
School of Health and Related Research (ScHARR), The University of Sheffield. Produced by
, The University of Sheffield. Produced by") Pegloticase for the treatment of hyperuricaemia in people with symptomatic gout whose disease is refractory to conventional uratelowering therapy, or in whom conventional urate-lowering therapy is contraindicated
Pegloticase for the treatment of hyperuricaemia in people with symptomatic gout whose disease is refractory to conventional uratelowering therapy, or in whom conventional urate-lowering therapy is contraindicated
Dual energy CT in diagnosis of Gout
 Dual energy CT in diagnosis of Gout Poster No.: R-0060 Congress: RANZCR ASM 2013 Type: Educational Exhibit Authors: F. Tabatabaie Moghadam, A. Moghaddam, F. Ghazanfari ; 1 1 1 2 2 Brisbane/AU, Melbourne/AU
Dual energy CT in diagnosis of Gout Poster No.: R-0060 Congress: RANZCR ASM 2013 Type: Educational Exhibit Authors: F. Tabatabaie Moghadam, A. Moghaddam, F. Ghazanfari ; 1 1 1 2 2 Brisbane/AU, Melbourne/AU
Therapy for Gout: The Past
 Advances in Therapy for Gout: 2015 The Past, Present, and Future Therapy for Gout: The Past Jonathan Graf, M.D. Professor of Clinical Medicine UCSF Division of Rheumatology, SFGH May 22, 1997 Pity a Tyrannosaur?
Advances in Therapy for Gout: 2015 The Past, Present, and Future Therapy for Gout: The Past Jonathan Graf, M.D. Professor of Clinical Medicine UCSF Division of Rheumatology, SFGH May 22, 1997 Pity a Tyrannosaur?
D espite reasonable understanding of its pathogenesis
 1312 EXTENDED REPORT EULAR evidence based recommendations for gout. Part II: Management. Report of a task force of the EULAR Standing Committee For International Clinical Studies Including Therapeutics
1312 EXTENDED REPORT EULAR evidence based recommendations for gout. Part II: Management. Report of a task force of the EULAR Standing Committee For International Clinical Studies Including Therapeutics
COPYRIGHT. Update in Internal Medicine December 4, 2016
 Update in Internal Medicine December 4, 2016 Fadi Badlissi, MD, MSc Director of the Musculoskeletal Medicine Unit The Orthopedic Department & Rheumatology Division Beth Israel Deaconess Medical Center
Update in Internal Medicine December 4, 2016 Fadi Badlissi, MD, MSc Director of the Musculoskeletal Medicine Unit The Orthopedic Department & Rheumatology Division Beth Israel Deaconess Medical Center
GOUT disease spectrum including
 GOUT disease spectrum including *hyperuricemia, *recurrent attacks of acute arthritis associated with monosodium urate crystals in leukocytes found in synovial fluid, *deposits of monosodium urate crystals
GOUT disease spectrum including *hyperuricemia, *recurrent attacks of acute arthritis associated with monosodium urate crystals in leukocytes found in synovial fluid, *deposits of monosodium urate crystals
GOUT GO FOR SIX WITH. Everything You Need to Know about Gout & Uric Acid PLUS:
 GO FOR SIX WITH Everything You Need to Know about Gout & Uric Acid GOUT PLUS: How to gain control of symptoms A gout-friendly eating style Medication recommendations to discuss with your doctor Lifestyle
GO FOR SIX WITH Everything You Need to Know about Gout & Uric Acid GOUT PLUS: How to gain control of symptoms A gout-friendly eating style Medication recommendations to discuss with your doctor Lifestyle
Journal of Advanced Scientific Research
 Bijoy Kumar Panda et al, J Adv Scient Res, 2012, 3(2): 03-11 3 Journal of Advanced Scientific Research Available online through http://www.sciensage.info/jasr ISSN 0976-9595 Review Article Febuxostat,
Bijoy Kumar Panda et al, J Adv Scient Res, 2012, 3(2): 03-11 3 Journal of Advanced Scientific Research Available online through http://www.sciensage.info/jasr ISSN 0976-9595 Review Article Febuxostat,
Drugs for Gout, osteoarthritis and osteoporosis
 MMS Pharmacology Lecture 3 Drugs for Gout, osteoarthritis and osteoporosis Dr Sura Al Zoubi Revision Gout The term gout describes a disease spectrum including hyperuricemia, recurrent attacks of acute
MMS Pharmacology Lecture 3 Drugs for Gout, osteoarthritis and osteoporosis Dr Sura Al Zoubi Revision Gout The term gout describes a disease spectrum including hyperuricemia, recurrent attacks of acute
New Drugs for the Primary Care Provider: What You Need to Know
 4:00 4:35 pm New Drugs for the Primary Care Provider: What You Need to Know SPEAKER Gerald W. Smetana, MD Presenter Disclosure Information The following relationships exist related to this presentation:
4:00 4:35 pm New Drugs for the Primary Care Provider: What You Need to Know SPEAKER Gerald W. Smetana, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Class Update: Drugs for Gout
 Copyright 2012 Oregon State University. ll Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. ll Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Gout is the most common inflammatory. Evolving Concepts in Gout Diagnosis and Treatment. Objectives
 C L I N I C A L I S S U E S Objectives Evolving Concepts in Gout Diagnosis and Treatment Here s the latest update on this most common inflammatory condition. 1) To examine the significant role of uric
C L I N I C A L I S S U E S Objectives Evolving Concepts in Gout Diagnosis and Treatment Here s the latest update on this most common inflammatory condition. 1) To examine the significant role of uric
Clinical Biochemistry department/ College of medicine / AL-Mustansiriyah University
 Clinical Biochemistry department/ College of medicine / AL-Mustansiriyah University Dr. Ali al-bayati NUCLEOTIDE METABOLISM Lec. 3 The salvage pathway of purine synthesis Purines that result from the normal
Clinical Biochemistry department/ College of medicine / AL-Mustansiriyah University Dr. Ali al-bayati NUCLEOTIDE METABOLISM Lec. 3 The salvage pathway of purine synthesis Purines that result from the normal
Osteoarthritis. Rheumatology Update. Gout 1/17/2013
 Osteoarthritis Rheumatology Update Richard Zweig, MD January, 2013 Degeneration of cartilage over time accompanied by increase in bone density and bone formation around the joint Risks include: aging,
Osteoarthritis Rheumatology Update Richard Zweig, MD January, 2013 Degeneration of cartilage over time accompanied by increase in bone density and bone formation around the joint Risks include: aging,
Women With Gout: Efficacy and Safety of Urate-Lowering With Febuxostat and Allopurinol
 Arthritis Care & Research Vol. 64, No. 2, February 2012, pp 256 261 DOI 10.1002/acr.20680 2012, American College of Rheumatology ORIGINAL ARTICLE Women With Gout: Efficacy and Safety of Urate-Lowering
Arthritis Care & Research Vol. 64, No. 2, February 2012, pp 256 261 DOI 10.1002/acr.20680 2012, American College of Rheumatology ORIGINAL ARTICLE Women With Gout: Efficacy and Safety of Urate-Lowering
Zurampic. (lesinurad) New Product Slideshow
 New Product Slideshow") Zurampic (lesinurad) New Product Slideshow Introduction Brand name: Zurampic Generic name: Lesinurad Pharmacological class: URAT1 inhibitor Strength and Formulation: 200mg; tablets Manufacturer: Ironwood
Zurampic (lesinurad) New Product Slideshow Introduction Brand name: Zurampic Generic name: Lesinurad Pharmacological class: URAT1 inhibitor Strength and Formulation: 200mg; tablets Manufacturer: Ironwood
Implementing AHRQ Effective Health Care Reviews Helping Clinicians Make Better Treatment Choices
 Implementing AHRQ Effective Health Care Reviews Helping Clinicians Make Better Treatment Choices Gout: Diagnosis and Management Practice Pointers by MATTHEW R. NOSS, DO, MSEd, U.S. Army Health Clinic,
Implementing AHRQ Effective Health Care Reviews Helping Clinicians Make Better Treatment Choices Gout: Diagnosis and Management Practice Pointers by MATTHEW R. NOSS, DO, MSEd, U.S. Army Health Clinic,
2.0. Copyright 2015 Wolters Kluwer Health, Inc. All rights reserved. 24 The Nurse Practitioner Vol. 40, No. 8
 2.0 CONTACT HOURS 24 The Nurse Practitioner Vol. 40, No. 8 www.tnpj.com Treatment and gout prevention of o leva Abstract: Gout is a disorder of purine metabolism that primarily occurs in adult males. Elevated
2.0 CONTACT HOURS 24 The Nurse Practitioner Vol. 40, No. 8 www.tnpj.com Treatment and gout prevention of o leva Abstract: Gout is a disorder of purine metabolism that primarily occurs in adult males. Elevated
Spondyloarthritis: A Gouty Display
 Spondyloarthritis: A Gouty Display Preetam Gongidi 1*, Shawn Gough-Fibkins 2 1. Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, FL, USA 2. Broward General Medical Center,
Spondyloarthritis: A Gouty Display Preetam Gongidi 1*, Shawn Gough-Fibkins 2 1. Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, FL, USA 2. Broward General Medical Center,
Febuxostat: a safe and effective therapy for hyperuricemia and gout
 DRUG EVALUATIO Febuxostat: a safe and effective therapy for hyperuricemia and gout atasha Jordan & Geraldine M McCarthy Author for correspondence Mater Misericordiae University Hospital, Eccles St. Dublin
DRUG EVALUATIO Febuxostat: a safe and effective therapy for hyperuricemia and gout atasha Jordan & Geraldine M McCarthy Author for correspondence Mater Misericordiae University Hospital, Eccles St. Dublin
CARDIOVASCULAR SAFETY OF FEBUXOSTAT OR ALLOPURINOL IN PATIENTS WITH GOUT AND CARDIOVASCULAR DISEASE (The CARES Trial)
") CARDIOVASCULAR SAFETY OF FEBUXOSTAT OR ALLOPURINOL IN PATIENTS WITH GOUT AND CARDIOVASCULAR DISEASE (The CARES Trial) William B. White, MD for the CARES Investigators Calhoun Cardiology Center University
CARDIOVASCULAR SAFETY OF FEBUXOSTAT OR ALLOPURINOL IN PATIENTS WITH GOUT AND CARDIOVASCULAR DISEASE (The CARES Trial) William B. White, MD for the CARES Investigators Calhoun Cardiology Center University
The Clinic a l Problem
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e Gout Tuhina Neogi, M.D., Ph.D. This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various
T h e n e w e ngl a nd j o u r na l o f m e dic i n e Gout Tuhina Neogi, M.D., Ph.D. This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various
Limitations of Use: (1) Duzallo is not recommended for the treatment of asymptomatic hyperuricemia.
 Duzallo is not recommended for the treatment of asymptomatic hyperuricemia.") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.63 Subject: Duzallo Page: 1 of 5 Last Review Date: December 8, 2017 Duzallo Description Duzallo (lesinurad
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.63 Subject: Duzallo Page: 1 of 5 Last Review Date: December 8, 2017 Duzallo Description Duzallo (lesinurad
Gout: A Clinical Update. Why talk about Gout? Why talk about Gout? Populations at risk: Why is Gout Less Common in Women? US Gout Population: 2009
 Gout: A Clinical Update Peng Thim Fan, MD, FACP Clinical Professor of Medicine Division of Rheumatology David Geffen School of Medicine at UCLA Why talk about Gout? Large increase in gout in the last 20
Gout: A Clinical Update Peng Thim Fan, MD, FACP Clinical Professor of Medicine Division of Rheumatology David Geffen School of Medicine at UCLA Why talk about Gout? Large increase in gout in the last 20
Rheumatology Review Update in Internal Medicine COPYRIGHT. Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center.
 Rheumatology Review Update in Internal Medicine Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston MA Case #1 True statement(s) regarding etanercept and leflunomide, for the treatment
Rheumatology Review Update in Internal Medicine Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston MA Case #1 True statement(s) regarding etanercept and leflunomide, for the treatment
RHEUMATOLOGY OVERVIEW. Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center
 RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
PART MUSCULOSKELETAL DISORDERS
 PART 12 MUSCULOSKELETAL DISORDERS CASE STUDY 77 GOUT For the Patient Case for this case study, see the printed book. DISEASE SUMMARY Definitions Gout is a syndrome of abnormal purine (i.e., DNA nucleotide
PART 12 MUSCULOSKELETAL DISORDERS CASE STUDY 77 GOUT For the Patient Case for this case study, see the printed book. DISEASE SUMMARY Definitions Gout is a syndrome of abnormal purine (i.e., DNA nucleotide