Gout: Let s Be Crystal Clear. Dr. Philip A. Baer Seacourses Asia CME December 2017
|
|
|
- Gwen McDaniel
- 6 years ago
- Views:
Transcription

1
2 Gout: Let s Be Crystal Clear Dr. Philip A. Baer Seacourses Asia CME December 2017
3 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law. Sea Courses is not responsible for any speaker or participant s statements, materials, acts or omissions.
4 Objectives Diagnose crystal-induced arthritis correctly Correctly treat acute gout Prevent recurrences of gout Deal with comorbidities associated with gout
5 Gout facts The most common inflammatory arthritis in men Increasingly common cause of inflammatory arthritis in women More common overall than RA


: The")
6 Gout: The disease of kings James Gillray( ): The Gout George Cruikshank ( ): The Gout, The King, and the Doctors
7 The victim goes to bed and sleeps in good health. About 2 a.m. in the morning he is awakened by a severe pain in the great toe; more rarely in the heel, ankle or instep. This pain is like that of a dislocation, and yet the parts feel as if cold water were poured over them. Then follow chills and shivers and a little fever. The pain, which was at first moderate, becomes more intense. After a time this comes to its full height, accommodating itself to the bones and ligaments of the tarsus and metatarsus. Violent stretching and tearing of the ligaments and the gnawing feeling of a dog. So exquisite the pain that it cannot bear the weight of bedclothes or the jar of a person walking in the room. The night is passed in torture, sleeplessness and the perpetual change of posture. T. Sydenham 1717
8


9 Gout: Clinical and X-ray Findings
10 Gout: Misdiagnosis is Common 9,108 Patients 1.7% Had gout 1.8% Had been misdiagnosed as having gout 76% treated with allopurinol Wolfe and Cathey, J. Rheum. 1991
11 Mathematics of Gout Elevated Serum Uric Acid Joint Pain GOUT

12 Gout not a priority in training Diagnostic methods not optimal Long-term complications underestimated Treatment not titrated to target serum uric acid levels Patients need more information Management guidelines not followed
13 Incidence of Gout: Doubled in 20 Years Increased longevity Increased prevalence of hypertension Dietary trends Increased obesity and metabolic syndrome Increased end-stage renal disease Increased survival in CAD and CHF
14 Percent of population Epidemiology: Prevalence of Gout 20% 16% 12% 8% 4% 0% Protective effect of estrogen in premenopausal women through increased renal clearance of uric acid 5.9% 2.0% 0.4% 12.6% Men Women years 80+ years Zhu Y, et al. Arth Rheum 2011; 63(10):



15 Pathophysiology of Gout Renal excretion (2/3) Alimentary excretion (1/3) HYPERURICEMIA Serum urate > 360 μmol/l URIC ACID XO Xanthine XO Over-production ~10% Under-excretion ~90% Urate crystal deposit in joint & tissue Inflammation Hypoxanthine Purine Acute Gout Attacks/flares Chronic Gout Tophi Chronic synovitis Bone erosion Cartilage loss Other Comorbidities Nephrolithiasis Nephropathy Metabolic S. XO = xanthine oxidase Hochberg MC. et al, eds. Rheumatology. 4th ed. Philadelphia, Pa: Mosby; 2007; Koopman WJ, ed. Arthritis and Allied Conditions. 15th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2005.
16 Uric Acid in Steady State Uric Acid level Steady State: Production = Excretion Sink is working perfectly
17 Hyperuricemia: Overproduction % of cases: Diet Malignancy Hemolysis Psoriasis Obesity Enzyme defects
18 Hyperuricemia: Underexcretion % of cases: Drugs: Low dose ASA, diuretics (increasing use) Toxins: Lead, ethanol Renal disease Endocrine disease Hypothyroidism Dehydration, starvation, ketosis Idiopathic
19 Underexcretion of Uric Acid Uric Acid level Under Excretion The Sink is Clogged The most common reason for hyperuricemia Lots of people with hyperuricemia but not acute gout

20 Gout: The Sink Overflows! Uric Acid level Acute Gout: When the sink overflows!

21
22 Nonpharmacologic ULT Measures in Gout Establish Diagnosis of Gout General Health, Diet and Lifestyle Measures for Gout Patients C Weight loss for obese patients achieve BMI that promotes general health Healthy overall diet Exercise (achieve physical fitness) Smoking cessation Stay well hydrated

23

24


25 Dietary Measures in Gout Avoid Limit Encourage Organ meats high in purine e.g. sweetbreads, liver, kidney B Serving sizes of: Beef, lamb, pork Seafood with high purine content e.g. sardines, shellfish B Low fat or non-fat dairy products B High fructose corn syrup foods sweetened sodas other beverages or foods C Servings of: Naturally sweet fruit juices Table sugar (beverages and desserts) Table salt (sauces and gravies) C Vegetables C Alcohol overuse in all gout patients Male >2 servings per day Female >1 serving per day B Alcohol Particularly beer Also wine and spirits B ANY alcohol use during periods of: Frequent gout attacks Advanced gout under poor control C
26 DASH Diet Lowers Serum Uric Acid The DASH diet can lower uric acid by 1.3 mg/dl in adults with an elevated uric acid, an effect similar to that of medication, where allopurinol, for example, the first-line urate-lowering medication, lowers uric acid by about 2 to 3 mg/dl. DOI: /art , American College of Rheumatology


27 Gout and Alcohol

28 What is the serum uric acid level at which the risk of gout starts to increase?
29 The relationship between serum uric acid levels and the incidence of gout 360 µmol/l = 6 mg/dl

30 Gout: Tip of the Uric Acid Iceberg
31 Stages of Gout

32 Dual Contour Sign on Ultrasound

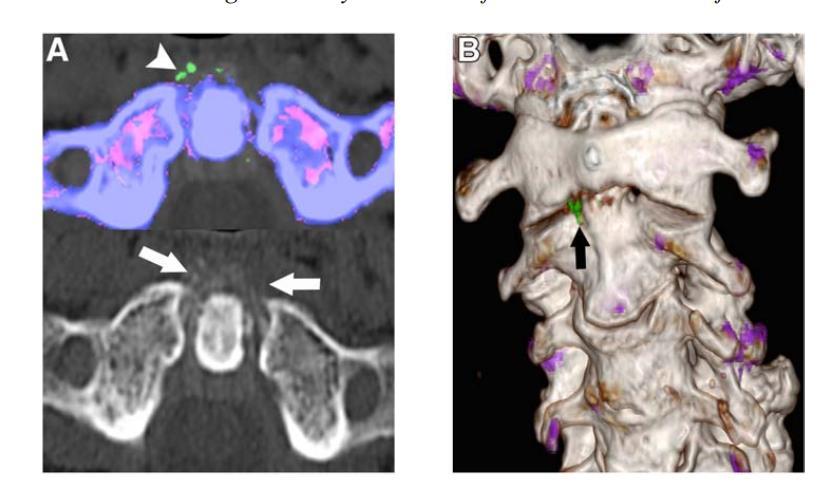
33 Dual Energy CT (DECT)

34 X-ray: Typical Gouty Erosions The characteristic gouty erosion is both destructive and hypertrophic, leading to overhanging edges The joint space often preserved until very late in the disease process

35 Acute Gout

36 Acute Gout: Mechanism
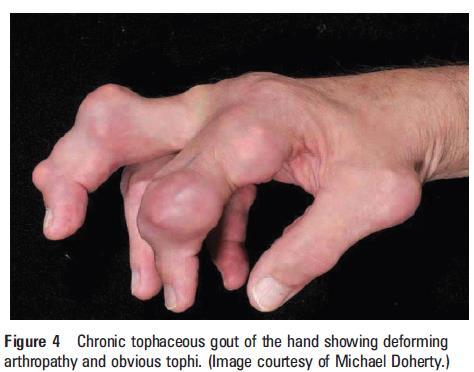


37 Chronic Tophaceous Gout




38 Chronic Tophaceous Gout

39 Gout: Tophi

40 Milk of Urate Bulla
41 NEJM 2016
42 Gout: Diagnosis Typical presentation Monosodium urate crystals in joint fluid Elevated serum uric acid X-ray changes

43 Pathophysiology of Gout: Acute Flares Common Characteristics Acute inflammation with rapid development of intense pain and tenderness, swelling, and with overlying shiny erythema Monoarticular ~ 90% of first attacks Podagra ~ 50% of first attacks Frequently involving lower extremities Often occurring at night Possible + family history As disease progresses, attacks occur more frequently and can become polyarticular and chronic Common Sites Frequency: Big toe 76% Ankle/foot 50% Knee 32% Finger 25% Elbow/wrist 10% >1 site simult.11% Mandell BF. Cleve Clin J Med. 2008;75:S5-S8. Gibson T. In Rheumatology. 4th ed. Mosby Elsevier limited 2008:

44 Gout: Synovial Fluid Analysis Compensated Polarized Light Microscopy Gold standard in diagnosis Urate crystals identified by Strong negative birefringence Needle and rod shapes 1
45 Clinical Diagnosis of Gout Establish Diagnosis of Gout Without Joint Fluid Analysis Predefined variable Clinical score Male sex 2.0 Previous patient-reported arthritis attack 2.0 Onset within one day 0.5 Joint redness st MTP involvement 2.0 Hypertension or 1 cardiovascular disease 1.5 Serum uric acid level >350 µmol/l 3.5 Maximum score 13.0 Janssens HJ et al,arch Intern Med (13)
46 Clinical Diagnosis of Gout Establish Diagnosis of Gout Gout confirmed in 80% of patients with score 8 Predefined variable Clinical score Male sex 2.0 Previous patient-reported arthritis attack 2.0 Onset within one day 0.5 Joint redness st MTP involvement 2.0 Hypertension or 1 cardiovascular disease 1.5 Serum uric acid level >350 µmol/l 3.5 Maximum score 13.0 Janssens HJ et al,arch Intern Med (13)

47 ACR-EULAR Gout Calculator
48 sua Levels as a Diagnostic Marker sua levels may be normal ~50% of the time during a flare Normal sua at the time of a flare does not rule out a gout diagnosis The best time to measure sua is after a flare has resolved, which may take up to 2 weeks Laboratories often report hyperuricemia based on population norms Population norms may be higher than biologically significant hyperuricemia ( 360 µmol/l) Best Time to Measure sua 0 Days (start of flare) 4 Days 8 Days 14 Days 20 Days Urano W. et al. J Rheumatol. 2002; 29: Zhang W. et al. Ann Rheum Dis. 2006; 65:

49 Gout Treatment Goals: From Toe Pain to No Pain Urate-lowering therapies Treat the acute attack

50
51 Management of an Acute Gout Attack General Principles Acute gouty arthritis attacks should be treated with pharmacologic therapy. C To provide optimal care, pharmacological treatment should be initiated within 24 hours of acute gout attack onset. C Ongoing pharmacologic ULT should not be interrupted during an acute gout attack. C
52 Management of an Acute Gout Attack Assess Severity Mild-moderate pain, particularly for an attack affecting only 1 or a few small joints, or 1-2 large joints Severe pain, particularly for a polyarticular attack or an attack affecting multiple large joints Monotherapy A Option: Initial combination therapy C NSAID (^or COX-2 inhibitor) A A A Systemic Corticosteroids Supplement with topical ice as needed B Colchicine COX=cyclooxygenase Colchicine was recommended as an appropriate option for acute gout if started within 36 hours of symptom onset. COX-2 inhibition therapy with celecoxib (Evidence B) requires high doses and has unclear risk-benefit ratio at this time.
53 Management of an Acute Gout Attack: NSAID or Selective COX-2 Inhibitor A Full FDA- or EMA-approved dose of NSAID or a COX-2 inhibitor C Continue initial treatment at full dose** until the gouty attack has fully resolved C FDA=Food and Drug Administration; EMA=European Medical Agency ** The option to taper the dose in patients with multiple comorbidities/hepatic or renal impairment was reinforced by the TFP, without specific TFP voting or more prescriptive guidance.
54 What is the recommended colchicine dose schedule for acute gout?
55 Management of an Acute Gout Attack: Oral Colchicine Is patient on prophylactic colchicine already? Yes No Oral Colchicine^ 1.2mg, then 0.6mg 1 hour later, then gout attack prophylaxis dosing can be started, beginning 12 hours or later, and continued until the acute attack resolves B Has patient received acute gout regimen colchicine therapy in the last 14 days? No Choose other therapy (NSAID or corticosteroid) B Yes ^The doses recommended need to be adjusted down in the presence of significant drug interactions, and moderate to severe renal or hepatic impairment.
56 Gout: Colchicine Therapy AGREE Trial: 1.8 mg vs 4.8 mg Colchicine Arthritis & Rheumatism Vol. 62, No. 4, April 2010, pp
57 Management of an Acute Gout Attack: Corticosteroids Extent of joint involvement Options: For all cases of gout Option: 1-2 large joints Consider IA corticosteroids B Start Initial Treatment Oral: Prednisone 0.5mg/kg per day A Duration of Rx: 5-10 days at full dose then stop OR for 2-5 days at full dose then taper for 7-10 days then stop IA: Dose depends on joint size (with or without oral treatment) IM: Triamcinolone acetonide 60mg, then oral prednisone as above* B C C IA = intra-articular; IM=intramuscular *IM triamcinolone acetonide monotherapy lack of consensus
58 PAIN GENERAL DISABILITY WALKING DISABILITY Prednisone 35 mg/day x 5 days vs. Naproxen 500 mg BID x 5 days Janssens et al Lancet 2008; 371:
59 Gout: Indications for Pharmacologic ULT Indications for Pharmacologic ULT Any patient with established diagnosis of gouty arthritis and Tophus or tophi by clinical exam or imaging study Frequent attacks of acute gouty arthritis ( 2 attacks/year) Chronic kidney disease (CKD) stage 2 or worse Past urolithiasis C C A A

60 Chronic Kidney Disease: Definitions
61 EULAR 2016: Gout Guideline ULT should be considered and discussed with every patient with a definite diagnosis of gout from the first presentation. ULT is indicated in all patients with recurrent flares, tophi, urate arthropathy and/or renal stones. Initiation of ULT is recommended close to the time of first diagnosis in patients presenting at a young age (<40 years) or with a very high SUA level (>8.0 mg/dl; 480 mmol/l) and/or comorbidities (renal impairment, hypertension, ischemic heart disease, heart failure). Patients with gout should receive full information and be fully involved in decision-making concerning the use of ULT.

62
63 Gout: Individual Targets TREAT TO SERUM URATE TARGET defined for individual patient The minimum serum urate target is <360µmol/L Serum urate lowering below 300µmol/L may be needed to improve gout signs and symptoms

64

65
66 Gout: Urate Lowering Therapy (ULT) TREAT TO SERUM URATE TARGET defined for individual patient The minimum serum urate target is < 360µmol/L Serum urate lowering below 300µmol/L may be needed to improve gout S/S Select First Line ULT agent Xanthine Oxidase Inhibitor (XOI) A Allopurinol OR Febuxostat If at least one XOI is contraindicated or not tolerated Alternative First Line ULT B Uricosuric Agent Probenecid* C *Probenecid is not recommended as a first line or alternative first line ULT agent if the CrCl is <50
67 Gout: ULT and Attack Prophylaxis TREAT TO SERUM URATE TARGET defined for individual patient The minimum serum urate target is < 360µmol/L Serum urate lowering below 300µmol/L may be needed to improve gout S/S Select First Line ULT agent Xanthine Oxidase Inhibitor (XOI) Allopurinol OR Febuxostat If at least one XOI is contraindicated or not tolerated Alternative First Line ULT B A Acute Gout Prophylaxis Initiate concomitant pharmacologic anti-inflammatory gout attack prophylaxis A Uricosuric Agent Probenecid* C *Probenecid is not recommended as a first line or alternative first line ULT agent if the CrCl is <50
68 Uric Acid Metabolism Xanthine XO X Uric Acid (insoluble) Xanthine Oxidase (XO) Inhibitors Uricase (inactive in humans and apes) Allantoin (soluble)
69 What is the starting dose of allopurinol?
70 Allopurinol Dosing and Titration Starting dosage should be no greater than 100 mg/day for any patient, and start at 50 mg/day in stage 4 or worse CKD. B Gradually titrate maintenance dose upward every 2 5 weeks to appropriate maximum dose in order to treat to chosen sua target. C sua=serum uric acid
71 Allopurinol Dosing and Pharmacogenetics Dose can be raised above 300 mg daily, even with renal impairment, as long as it is accompanied by adequate patient education and monitoring for drug toxicity (e.g., pruritus, rash, elevated hepatic transaminases). B Prior to initiation, consider HLA B*5801 in selected patients, specifically in subpopulations at higher risk for severe allopurinol hypersensitivity reaction (e.g. Koreans with stage 3 or worse CKD, and Han Chinese and Thai irrespective of renal function). A sua=serum uric acid
72 Febuxostat Nonpurine Selective XO Inhibitor OH OH OH N N N N N H C N N N H N N H OH N N H Hypoxanthine Allopurinol Oxypurinol O N NC CH 3 Febuxostat S COOH
 *p<.001 vs. allopurinol. p<.001 vs. febuxostat 40 mg Allopurinol 300 mg efficacy: 44% Allopurinol 200 mg efficacy: 32% Becker MA. et al.")
73 % of Subjects Efficacy of XO Inhibitors Proportion of Subjects with sua Level < 360 µmol/l at Final Visit 67% % 42% Febuxostat 40 mg (n=757) Febuxostat 80 mg (n=756) Febuxostat Allopurinol 300/200 mg (n=755) *p<.001 vs. allopurinol. p<.001 vs. febuxostat 40 mg Allopurinol 300 mg efficacy: 44% Allopurinol 200 mg efficacy: 32% Becker MA. et al. Arth Res & Ther 2010; 12:R63.
74 Chronic Gout Management Benefits of Continuous ULT Intermittent therapy or cessation of therapy can lead to recurrent flares. Continuous urate-lowering therapy controls flares better than intermittent therapy Bull PW, Scott JT. J Rheumatol. 1989; 16:


75 Benefits of Long-Term ULT Before Urate-Lowering Therapy 22 years with gout After Urate-Lowering Therapy 1 year with sua <240 µmol/l Images Fernando Perez-Ruiz, MD. All rights reserved.
76 Pharmacologic Antiinflammatory Prophylaxis of Gout Attacks Initiate Prophylaxis With, or just prior to initiating ULT Medication choices: First Line: Low dose Colchicine : e.g. colchicine 0.6 mg once or twice daily OR C Low dose NSAIDs with PPI (where indicated): e.g. naproxen 250 mg twice daily A * *Second Line: Low dose Prednisone or Prednisolone ( 10mg/day) C (if colchicine and NSAIDs both are not indicated, contraindicated, or ineffective) * Lack of consensus: Prednisone/prednisolone at doses above 10mg/day. The TFP did not specifically address case scenarios involving renal impairment adjusted colchicine dosing for gout attack prophylaxis
77 Duration of Anti-inflammatory Prophylaxis of Acute Gout Attacks Evaluate gout symptoms while on ULT No signs/symptoms Activity of gout S/S^ Continue pharmacologic antiinflammatory prophylaxis Duration: Treatment for the greater of A At least 6 months OR 3 months after achieving target serum urate appropriate for the patient (No tophi detected on physical exam) 6 months after achieving target serum urate appropriate for the patient (One or more tophi detected on physical exam) B C ^Examples include: acute gouty arthritis in the past 3 months, presence of palpable tophus or tophi, chronic tophaceous gouty arthropathy (with chronic synovitis) in the past 3 months
78 Subjects, % Reduction in Gout Flares Febuxostat 40 mg Febuxostat 80 mg Allopurinol 300/200 mg Time interval (weeks) Prophylaxis Prophylaxis: colchicine (0.6 mg daily) or naproxen (250 mg BID) Becker MA. et al. Arth Res & Ther 2010; 12:R63.

79 Uric Acid is Associated with Many Cardiovascular Risk Factors hypertension ethnicity obesity Uric Acid renal disease diuretics insulin resistance post-menopausal female male

80 Gout and the Metabolic Syndrome
81 GOUT: What s Coming
82 Urate transport systems in the proximal tubule The kidney excretes 70% of the daily urate production Urate anion transport function of URAT1 in renal proximal tubule epithelial cells. The organic anion transporter URAT1 exchanges tubular lumen urate with anions inside proximal tubular epithelial cells. URAT1 is targeted by uricosuric and antiuricosuric agents.
83 Lesinurad: FDA Approved (Zurampic) A selective uric acid re-absorption inhibitor (SURI) Inhibits the URAT1 transporter, increasing uric acid excretion and thereby lowering serum uric acid (sua) Phase 3 studies (CLEAR, CRYSTAL, LIGHT): used in combination with allopurinol or febuxostat Not to be used as monotherapy Approved by FDA in Dec Duzallo, a fixed-dose oral combination of lesinurad 200mg and allopurinol 200 or 300 mg, approved by FDA in

84 Arhalofenate First developed as an insulin sensitizer for type 2 diabetes Showed significant reductions in serum urate of 13 29% Inhibits URAT1, OAT 4 and OAT 10 involved in renal urate reabsorption without any effect on xanthine oxidase Antiinflammatory activity through inhibition of interleukin-1beta? the first ULAFT urate-lowering, antiflare therapy.
85
86 Resources
87
88

89

90

91


92

93

94 EULAR 2016 Gout Guideline
95 BSR 2017 Gout Guideline
96 Gout: PEARLs Serum urate concentrations can go down to normal levels during an attack of gout Oral steroids may be a safer alternative to NSAIDs or colchicine for the management of acute gout Urate lowering drugs are usually needed only for patients with frequent attacks of gout Asymptomatic hyperuricemia does not require pharmacologic treatment
97 Barriers to Change: Gout Gout is more common and more complex than usually appreciated Crystal analysis is gold standard for diagnosis but rarely performed Confusion between treatment of acute gout and chronic gout Patient and physician reluctance to start and continue urate lowering therapy (ULT)


98

99 Questions??
Gout 2.0. Scott Vogelgesang, M.D. Division of Immunology: Rheumatology & Allergy
 Gout 2.0 Scott Vogelgesang, M.D. Division of Immunology: Rheumatology & Allergy Case 48 year old man presents with swollen, painful left toe that started overnight. Didn t hurt when he went to bed. No
Gout 2.0 Scott Vogelgesang, M.D. Division of Immunology: Rheumatology & Allergy Case 48 year old man presents with swollen, painful left toe that started overnight. Didn t hurt when he went to bed. No
1. To review the diagnosis of gout and its differential. 2. To understand the four stages of gout
 Objectives 1. To review the diagnosis of gout and its differential GOUT 2. To understand the four stages of gout 3. To develop an approach for the acute treatment of gout Anthony Lim 9/13/12 Cycle 3 4.
Objectives 1. To review the diagnosis of gout and its differential GOUT 2. To understand the four stages of gout 3. To develop an approach for the acute treatment of gout Anthony Lim 9/13/12 Cycle 3 4.
Enhanced Primary Care Pathway: Gout
 Enhanced Primary Care Pathway: Gout 1. Focused summary of gout relevant to primary care Significance: Gout is a chronic, progressive, inflammatory disease requiring appropriate long-term management. Gout
Enhanced Primary Care Pathway: Gout 1. Focused summary of gout relevant to primary care Significance: Gout is a chronic, progressive, inflammatory disease requiring appropriate long-term management. Gout
Gout A rapid review. Jeremy Jones
 Gout A rapid review Jeremy Jones The Hyperuricemia Cascade Dietary purines Tissue nucleic acids Urate Endogenous purine synthesis Overproduction Hyperuricemia Underexcretion Silent tissue deposition Gout
Gout A rapid review Jeremy Jones The Hyperuricemia Cascade Dietary purines Tissue nucleic acids Urate Endogenous purine synthesis Overproduction Hyperuricemia Underexcretion Silent tissue deposition Gout
OBJECTIVES GOUT GOUTY INFLAMMATION 6/10/2016 GOUT INCIDENCE AND PREVALENCE MONOSODIUM URATE CRYSTAL DEPOSITION DISEASE
 GOUT Lisa Talbert, MD Family Medicine Update June 15, 2016 OBJECTIVES To be familiar with the clinical presentation and pathophysiology of gouty arthritis Be able to incorporate current guidelines when
GOUT Lisa Talbert, MD Family Medicine Update June 15, 2016 OBJECTIVES To be familiar with the clinical presentation and pathophysiology of gouty arthritis Be able to incorporate current guidelines when
Case presentation. serum uric acid = 11.5 mg/dl 24-hour uric acid excretion = 300 mg
 GOUT 55 y/o male 12 hours pain in my big toe & ankle went to bed last night feeling fine felt as if had broken toe this morning similar problems in right ankle & left wrist Case presentation lab studies
GOUT 55 y/o male 12 hours pain in my big toe & ankle went to bed last night feeling fine felt as if had broken toe this morning similar problems in right ankle & left wrist Case presentation lab studies
GOUT. Dr Krishnan Baburaj West herts NHS Trust
 GOUT Dr Krishnan Baburaj West herts NHS Trust podagra Gout A disease of kings, the king of diseases History Louis XIV Emperor Augustus Henry VIII Introduction Gout an inflammatory arthritic condition that
GOUT Dr Krishnan Baburaj West herts NHS Trust podagra Gout A disease of kings, the king of diseases History Louis XIV Emperor Augustus Henry VIII Introduction Gout an inflammatory arthritic condition that
Gout Treatment Guidelines
 Gout Treatment Guidelines Gout is a disorder that manifests as a spectrum of clinical and pathologic features built on a foundation of an excess body burden of uric acid, manifested in part by hyperuricemia,
Gout Treatment Guidelines Gout is a disorder that manifests as a spectrum of clinical and pathologic features built on a foundation of an excess body burden of uric acid, manifested in part by hyperuricemia,
Gout Hanan Abdel Rehim
 Review article 35 Gout Hanan Abdel Rehim Department of Internal Medicine, Kasr-Al Aini School of Medicine, Cairo University, Cairo, Egypt Correspondence to Hanan Abdel Rehim, MD, 11 Ismaiel Wahby Street,
Review article 35 Gout Hanan Abdel Rehim Department of Internal Medicine, Kasr-Al Aini School of Medicine, Cairo University, Cairo, Egypt Correspondence to Hanan Abdel Rehim, MD, 11 Ismaiel Wahby Street,
Gout -revisited. Shrenik Shah
 Gout -revisited Shrenik Shah definition Monosodium urate (MSU) crystal deposition episodic and later persistent joint inflammation and tophi All MSU crystal deposition- broader definition EULAR- European
Gout -revisited Shrenik Shah definition Monosodium urate (MSU) crystal deposition episodic and later persistent joint inflammation and tophi All MSU crystal deposition- broader definition EULAR- European
Achieving Gout Goals in Your Practice An Interview with Paul P. Doghramji, MD, FAAFP
 Achieving Gout Goals in Your Practice An Interview with Paul P. Doghramji, MD, FAAFP Dr. Paul Doghramji is attending physician at the Pottstown Memorial Medical Center and medical director of Health Services
Achieving Gout Goals in Your Practice An Interview with Paul P. Doghramji, MD, FAAFP Dr. Paul Doghramji is attending physician at the Pottstown Memorial Medical Center and medical director of Health Services
Crystal induced arthropathies. Dr. Amitesh Aggarwal
 Crystal induced arthropathies Dr. Amitesh Aggarwal 1 Crystal induced Arthropathies Gout Pseudogout Debilitating illnesses; Recurrent episodes of pain and joint inflammation; Formation and deposition of
Crystal induced arthropathies Dr. Amitesh Aggarwal 1 Crystal induced Arthropathies Gout Pseudogout Debilitating illnesses; Recurrent episodes of pain and joint inflammation; Formation and deposition of
Podcast (Video Recorded Lecture Series): Gout for the USMLE Step One Exam. Howard J. Sachs, MD
: Gout for the USMLE Step One Exam. Howard J. Sachs, MD") Podcast (Video Recorded Lecture Series): Gout for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com Podcast (Video Recorded Lecture Series): Gout for the
Podcast (Video Recorded Lecture Series): Gout for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com Podcast (Video Recorded Lecture Series): Gout for the
For more information about how to cite these materials visit
 Author(s): Seetha Monrad, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Seetha Monrad, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
A Patient s Guide to Gout. Foot and Ankle Center of Massachusetts, P.C.
 A Patient s Guide to Gout Welcome to Foot and Ankle Center of Massachusetts, where we believe in accelerating your learning curve with educational materials that are clearly written and professionally
A Patient s Guide to Gout Welcome to Foot and Ankle Center of Massachusetts, where we believe in accelerating your learning curve with educational materials that are clearly written and professionally
3/2/2014. Got Gout? Get a Plumber. Objectives. Disclosures
 Got Gout? Get a Plumber. Heidi Garcia, PA-C Department of Rheumatology Division of Internal Medicine Mayo Clinic Arizona 2013 MFMER slide-1 Objectives Recall some of the history of Gout. Describe the pathophysiology
Got Gout? Get a Plumber. Heidi Garcia, PA-C Department of Rheumatology Division of Internal Medicine Mayo Clinic Arizona 2013 MFMER slide-1 Objectives Recall some of the history of Gout. Describe the pathophysiology
Gout: Update in therapeutics
 Summary Gout: Update in therapeutics 29/11/14 Caroline van Durme CHU de Liège Maastricht University Medical Centre+ Why treating gout? Guidelines: ACR 12 Drugs: Colchicine Allopurinol: what about the kidney?
Summary Gout: Update in therapeutics 29/11/14 Caroline van Durme CHU de Liège Maastricht University Medical Centre+ Why treating gout? Guidelines: ACR 12 Drugs: Colchicine Allopurinol: what about the kidney?
Update on Gout for GPs
 Update on Gout for GPs Dr Patrick Kiely PhD FRCP Consultant Physician and Rheumatologist St George s, London 2/3 1/3 Gut bacteria have uricase Chronic erosive arthropathy Clinical spectrum Making the diagnosis
Update on Gout for GPs Dr Patrick Kiely PhD FRCP Consultant Physician and Rheumatologist St George s, London 2/3 1/3 Gut bacteria have uricase Chronic erosive arthropathy Clinical spectrum Making the diagnosis
Gout: Develop treatment plan in William Jones, MS, RPh
 Gout: Develop treatment plan in 2013 William Jones, MS, RPh (wnjones49@cox.net) Objectives Describe acute gouty arthritis Tx Describe Tx of chronic gouty arthritis. Define the target serum uric acid concentration
Gout: Develop treatment plan in 2013 William Jones, MS, RPh (wnjones49@cox.net) Objectives Describe acute gouty arthritis Tx Describe Tx of chronic gouty arthritis. Define the target serum uric acid concentration
Rheumatoid arthritis, seronegative spondylarthritides and gout. György Nagy
 Rheumatoid arthritis, seronegative spondylarthritides and gout György Nagy Dec 4, 2017 Rheumatoid arthritis Rheumatoid arthritis Chronic, progressive, autoimmune disorder of the joints with extra-articular
Rheumatoid arthritis, seronegative spondylarthritides and gout György Nagy Dec 4, 2017 Rheumatoid arthritis Rheumatoid arthritis Chronic, progressive, autoimmune disorder of the joints with extra-articular
Gout. Clinical features Most commonly affects middle-aged males. It is an acute and usually relapsing selflimiting
 Gout Gout is a syndrome caused by an inflammatory response to the formation of monosodium urate monohydrate crystals which develop secondary to hyperuricemia. Acute and chronic forms are recognized. Hyperuricemia
Gout Gout is a syndrome caused by an inflammatory response to the formation of monosodium urate monohydrate crystals which develop secondary to hyperuricemia. Acute and chronic forms are recognized. Hyperuricemia
CHAPTER:2 GOUT. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:2 GOUT BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY DEFINITION Gout is defined as a peripheral arthritis, resulting from the deposition of MSU crystals
CHAPTER:2 GOUT BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY DEFINITION Gout is defined as a peripheral arthritis, resulting from the deposition of MSU crystals
New Drug Evaluation: lesinurad tablet, oral
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Gout- Treatment Updates. Harinder Singh, MD Rheumatology Mercy Internal Medicine Clinic Mason City, IA
 Gout- Treatment Updates Harinder Singh, MD Rheumatology Mercy Internal Medicine Clinic Mason City, IA Gout Outline of purine metabolism: (1) amidophosphoribosyltransferase (2) hypoxanthine-guanine phosphoribosyltransferase
Gout- Treatment Updates Harinder Singh, MD Rheumatology Mercy Internal Medicine Clinic Mason City, IA Gout Outline of purine metabolism: (1) amidophosphoribosyltransferase (2) hypoxanthine-guanine phosphoribosyltransferase
Crystal-Induced Arthritis. Rajesh Kataria, D.O. Southern Ohio Rheumatology
 Crystal-Induced Arthritis Rajesh Kataria, D.O. Southern Ohio Rheumatology Disclosures Speaker: Rajesh Kataria, D.O. Relationships with commercial interests: Speakers Bureau - Horizon Presentation will
Crystal-Induced Arthritis Rajesh Kataria, D.O. Southern Ohio Rheumatology Disclosures Speaker: Rajesh Kataria, D.O. Relationships with commercial interests: Speakers Bureau - Horizon Presentation will
Managing Gout A Review of the Research for Adults
 Managing Gout A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional* has said that you have gout. You are age 18 or
Managing Gout A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional* has said that you have gout. You are age 18 or
Rheumatology Cases for the Internist
 Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
GOUT & PSEUDOGOUT OPSC 2018 HOWARD L. FEINBERG, D.O., F.A.C.O.I.., F.A.C.R.
 GOUT & PSEUDOGOUT OPSC 2018 HOWARD L. FEINBERG, D.O., F.A.C.O.I.., F.A.C.R. Everything in excess is opposed by nature Eunuchs do not take the gout, nor become bald. GOUT Hyperuricemia is not gout Gout
GOUT & PSEUDOGOUT OPSC 2018 HOWARD L. FEINBERG, D.O., F.A.C.O.I.., F.A.C.R. Everything in excess is opposed by nature Eunuchs do not take the gout, nor become bald. GOUT Hyperuricemia is not gout Gout
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: Gout and Pseudogout Wayne Blount MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: Gout and Pseudogout Wayne Blount MD Speaker has no disclosures
Acute hot swollen joint. Dr Edward Roddy Senior Lecturer in Rheumatology and Consultant Rheumatologist
 Acute hot swollen joint Dr Edward Roddy Senior Lecturer in Rheumatology and Consultant Rheumatologist Acute monoarthritis: differential diagnosis Septic arthritis Crystal arthritis (gout, pseudogout) Haemarthrosis
Acute hot swollen joint Dr Edward Roddy Senior Lecturer in Rheumatology and Consultant Rheumatologist Acute monoarthritis: differential diagnosis Septic arthritis Crystal arthritis (gout, pseudogout) Haemarthrosis
Lecture 8 Gout Hinch. Pathogenesis of acute attacks
 Gout: disease characterized by deposition of monosodium crystals in soft tissues (cartilage, tendons, bursa) recurrent episodes of acute joint pain & inflammation Pathogenesis of acute attacks Epidemiology:
Gout: disease characterized by deposition of monosodium crystals in soft tissues (cartilage, tendons, bursa) recurrent episodes of acute joint pain & inflammation Pathogenesis of acute attacks Epidemiology:
GOUT IN THE ELDERLY. Learning Objectives. Disclosure. Geriatric Grand Rounds. Geriatric Grand Rounds
 Visit web sites: Tuesday, June 2, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this event
Visit web sites: Tuesday, June 2, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this event
Uloric Step Therapy Program
 Uloric Step Therapy Program Policy Number: 5.01.584 Last Review: 7/2017 Origination: 7/2014 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for brand
Uloric Step Therapy Program Policy Number: 5.01.584 Last Review: 7/2017 Origination: 7/2014 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for brand
An update on the management of gout
 An update on the management of gout 8 The management of gout involves treatment of an acute attack, lifestyle modification and urate lowering treatment to achieve a target serum urate level. Recent evidence
An update on the management of gout 8 The management of gout involves treatment of an acute attack, lifestyle modification and urate lowering treatment to achieve a target serum urate level. Recent evidence
What will happen in the future? How will gout be diagnosed? How is gout treated? prevent
 Rheumatology Day Unit Dr J Hamilton 0191 4458359 0191 4455240 (9-5 Mon-Fri) Dr C Heycock 0191 4452198 Answer phone on 24hours Dr C Kelly 0191 4452193 Dr V Saravanan 0191 4456055 Dr M Rynne 0191 4458359
Rheumatology Day Unit Dr J Hamilton 0191 4458359 0191 4455240 (9-5 Mon-Fri) Dr C Heycock 0191 4452198 Answer phone on 24hours Dr C Kelly 0191 4452193 Dr V Saravanan 0191 4456055 Dr M Rynne 0191 4458359
Gout basics. Update on Gout. Production of uric acid. Gout basics. Crystal induced inflammation. Gout calculator. The important role of ultrasound
 Update on Gout The important role of ultrasound Cheung C Yue, M.D. Gout basics Hyperuricemia gout Over 5 years, 22% >9 mg/dl develop gout Man 3-4 times more than women Risks: thiazide, cyclosporin, low
Update on Gout The important role of ultrasound Cheung C Yue, M.D. Gout basics Hyperuricemia gout Over 5 years, 22% >9 mg/dl develop gout Man 3-4 times more than women Risks: thiazide, cyclosporin, low
Cost-effectiveness of lesinurad (Zurampic ) for the treatment of adult patients with gout
 for the treatment of adult patients with gout") Cost-effectiveness of lesinurad (Zurampic ) for the treatment of adult patients with gout The NCPE has issued a recommendation regarding the cost-effectiveness of Lesinurad (Zurampic ) in combination with
Cost-effectiveness of lesinurad (Zurampic ) for the treatment of adult patients with gout The NCPE has issued a recommendation regarding the cost-effectiveness of Lesinurad (Zurampic ) in combination with
New Drugs for the Primary Care Provider: What You Need to Know
 4:00 4:35 pm New Drugs for the Primary Care Provider: What You Need to Know SPEAKER Gerald W. Smetana, MD Presenter Disclosure Information The following relationships exist related to this presentation:
4:00 4:35 pm New Drugs for the Primary Care Provider: What You Need to Know SPEAKER Gerald W. Smetana, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Drugs Used to Treat Gout. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used to Treat Gout Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Gout is a metabolic disease characterized by recurrent episodes of acute arthritis
Drugs Used to Treat Gout Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Gout is a metabolic disease characterized by recurrent episodes of acute arthritis
Urate Lowering Efficacy of Febuxostat Versus Allopurinol in Hyperuricemic Patients with Gout
 Philippine Journal of Internal Medicine Meta-Analysis Urate Lowering Efficacy of Febuxostat Versus Allopurinol in Hyperuricemic Patients with Gout Erika Bianca S. Villazor-Isidro, M.D.*; John Carlo G.
Philippine Journal of Internal Medicine Meta-Analysis Urate Lowering Efficacy of Febuxostat Versus Allopurinol in Hyperuricemic Patients with Gout Erika Bianca S. Villazor-Isidro, M.D.*; John Carlo G.
GOUT GO FOR SIX WITH. Everything You Need to Know About Gout & Uric Acid PLUS:
 GO FOR SIX WITH Everything You Need to Know About Gout & Uric Acid GOUT PLUS: How to gain control of symptoms A gout-friendly eating style Medication recommendations to discuss with your doctor Lifestyle
GO FOR SIX WITH Everything You Need to Know About Gout & Uric Acid GOUT PLUS: How to gain control of symptoms A gout-friendly eating style Medication recommendations to discuss with your doctor Lifestyle
Subject: Krystexxa (pegloticase) Original Effective Date: 06/26/13. Policy Number: MCP-138. Revision Date(s):
 Original Effective Date: 06/26/13. Policy Number: MCP-138. Revision Date(s):") Subject: Krystexxa (pegloticase) Original Effective Date: 06/26/13 Policy Number: MCP-138 Revision Date(s): Review Date(s): 12/16/15; 6/15/2016; 3/21/2017 DISCLAIMER This Molina Clinical Policy (MCP) is
Subject: Krystexxa (pegloticase) Original Effective Date: 06/26/13 Policy Number: MCP-138 Revision Date(s): Review Date(s): 12/16/15; 6/15/2016; 3/21/2017 DISCLAIMER This Molina Clinical Policy (MCP) is
Zurampic. (lesinurad) New Product Slideshow
 New Product Slideshow") Zurampic (lesinurad) New Product Slideshow Introduction Brand name: Zurampic Generic name: Lesinurad Pharmacological class: URAT1 inhibitor Strength and Formulation: 200mg; tablets Manufacturer: Ironwood
Zurampic (lesinurad) New Product Slideshow Introduction Brand name: Zurampic Generic name: Lesinurad Pharmacological class: URAT1 inhibitor Strength and Formulation: 200mg; tablets Manufacturer: Ironwood
GOUT GO FOR SIX WITH. Everything You Need to Know about Gout & Uric Acid PLUS:
 GO FOR SIX WITH Everything You Need to Know about Gout & Uric Acid GOUT PLUS: How to gain control of symptoms A gout-friendly eating style Medication recommendations to discuss with your doctor Lifestyle
GO FOR SIX WITH Everything You Need to Know about Gout & Uric Acid GOUT PLUS: How to gain control of symptoms A gout-friendly eating style Medication recommendations to discuss with your doctor Lifestyle
GOUT disease spectrum including
 GOUT disease spectrum including *hyperuricemia, *recurrent attacks of acute arthritis associated with monosodium urate crystals in leukocytes found in synovial fluid, *deposits of monosodium urate crystals
GOUT disease spectrum including *hyperuricemia, *recurrent attacks of acute arthritis associated with monosodium urate crystals in leukocytes found in synovial fluid, *deposits of monosodium urate crystals
COPYRIGHT. Update in Internal Medicine December 4, 2016
 Update in Internal Medicine December 4, 2016 Fadi Badlissi, MD, MSc Director of the Musculoskeletal Medicine Unit The Orthopedic Department & Rheumatology Division Beth Israel Deaconess Medical Center
Update in Internal Medicine December 4, 2016 Fadi Badlissi, MD, MSc Director of the Musculoskeletal Medicine Unit The Orthopedic Department & Rheumatology Division Beth Israel Deaconess Medical Center
New Drug Evaluation: lesinurad tablet, oral
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Lesinurad in Combination With a Xanthine Oxidase Inhibitor for Treatment of Hyperuricemia Associated With Gout
 Lesinurad in Combination With a Xanthine Oxidase Inhibitor for Treatment of Hyperuricemia Associated With Gout Briefing Document for the Arthritis Advisory Committee Meeting Date: 23 October 215 Ardea
Lesinurad in Combination With a Xanthine Oxidase Inhibitor for Treatment of Hyperuricemia Associated With Gout Briefing Document for the Arthritis Advisory Committee Meeting Date: 23 October 215 Ardea
LECTURE 5: DRUGS IN GOUT
 Red : important Black : in male / female slides Pink : in female s slides only Blue : in male s slides only Green : Dr s notes Grey: Extra information, explanation Editing File LECTURE 5: DRUGS IN GOUT
Red : important Black : in male / female slides Pink : in female s slides only Blue : in male s slides only Green : Dr s notes Grey: Extra information, explanation Editing File LECTURE 5: DRUGS IN GOUT
Class Update: Drugs for Gout
 Copyright 2012 Oregon State University. ll Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. ll Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2016 Wolters Kluwer Health, Inc. All rights reserved.
 14 The Nurse Practitioner Vol. 41, No. 14 www.tnpj.com 2.5 CONTACT HOURS 2.5 CONTACT HOURS Gout An update on for primary care providers Abstract: This article discusses the current beliefs regarding the
14 The Nurse Practitioner Vol. 41, No. 14 www.tnpj.com 2.5 CONTACT HOURS 2.5 CONTACT HOURS Gout An update on for primary care providers Abstract: This article discusses the current beliefs regarding the
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Krystexxa) Reference Number: CP.PHAR.115 Effective Date: 06.01.13 Last Review Date: 02.19 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important Reminder
Clinical Policy: (Krystexxa) Reference Number: CP.PHAR.115 Effective Date: 06.01.13 Last Review Date: 02.19 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important Reminder
COMPARATIVE EVALUATION OF EFFICACY AND SAFETY PROFILE OF FEBUXOSTAT WITH ALLOPURINOL IN PATIENTS WITH HYPERURICEMIA AND GOUT
 Int. J. Pharm. Med. & Bio. Sc. 2013 P K Agarwal and Bijay Kumar, 2013 Research Paper ISSN 2278 5221 www.ijpmbs.com Vol. 2, No. 4, October 2013 2013 IJPMBS. All Rights Reserved COMPARATIVE EVALUATION OF
Int. J. Pharm. Med. & Bio. Sc. 2013 P K Agarwal and Bijay Kumar, 2013 Research Paper ISSN 2278 5221 www.ijpmbs.com Vol. 2, No. 4, October 2013 2013 IJPMBS. All Rights Reserved COMPARATIVE EVALUATION OF
Clinical Practice Guideline. Gout. Version
 Clinical Practice Guideline Gout Version 1.1.2017 August 2017 Table of Contents Introduction...5 Stages of Gout...7 Asymptomatic Hyperuricemia... 7 Acute Intermittent Gout... 7 Advanced Gout... 8 Diagnosis...8
Clinical Practice Guideline Gout Version 1.1.2017 August 2017 Table of Contents Introduction...5 Stages of Gout...7 Asymptomatic Hyperuricemia... 7 Acute Intermittent Gout... 7 Advanced Gout... 8 Diagnosis...8
4/1/2011. New Developments in Gout. Conflict of Interest Declaration. Objectives
 New Developments in Gout Tatum N. Mead, Pharm.D. Clinical Assistant Professor UMKC SOP meadt@umkc.edu April 16, 2011 1 Conflict of Interest Declaration I have no actual or potential conflict of interest
New Developments in Gout Tatum N. Mead, Pharm.D. Clinical Assistant Professor UMKC SOP meadt@umkc.edu April 16, 2011 1 Conflict of Interest Declaration I have no actual or potential conflict of interest
Dose of celecoxib in gout attack attack
 Dose of celecoxib in gout attack Gout is a disease characterized by an abnormal metabolism of uric acid, resulting in an excess of uric acid in the tissues and blood. People with gout either produce too
Dose of celecoxib in gout attack Gout is a disease characterized by an abnormal metabolism of uric acid, resulting in an excess of uric acid in the tissues and blood. People with gout either produce too
Drugs for Gout, osteoarthritis and osteoporosis
 MMS Pharmacology Lecture 3 Drugs for Gout, osteoarthritis and osteoporosis Dr Sura Al Zoubi Revision Gout The term gout describes a disease spectrum including hyperuricemia, recurrent attacks of acute
MMS Pharmacology Lecture 3 Drugs for Gout, osteoarthritis and osteoporosis Dr Sura Al Zoubi Revision Gout The term gout describes a disease spectrum including hyperuricemia, recurrent attacks of acute
Therapy for Gout: The Past
 Advances in Therapy for Gout: 2011 The Past, Present, and Future Therapy for Gout: The Past May 22, 1997 Pity a Tyrannosaur? Sue Had Gout By MALCOLM W. BROWNE Jonathan Graf, M.D. Associate Professor of
Advances in Therapy for Gout: 2011 The Past, Present, and Future Therapy for Gout: The Past May 22, 1997 Pity a Tyrannosaur? Sue Had Gout By MALCOLM W. BROWNE Jonathan Graf, M.D. Associate Professor of
MEDICAL POLICY PEGLOTICASE (KRYSTEXXA ) POLICY NUMBER MP POLICY TITLE. Original Issue Date (Created): January 1, 2011
 POLICY NUMBER MP POLICY TITLE. Original Issue Date (Created): January 1, 2011") Original Issue Date (Created): January 1, 2011 Most Recent Review Date (Revised): September 24, 2013 Effective Date: November 1, 2013 I. POLICY PREAUTHORIZATION REQUIRED Note: Requests for pegloticase
Original Issue Date (Created): January 1, 2011 Most Recent Review Date (Revised): September 24, 2013 Effective Date: November 1, 2013 I. POLICY PREAUTHORIZATION REQUIRED Note: Requests for pegloticase
Gout. Edward Roddy, 1 Christian D Mallen, 1 Michael Doherty 2 CLINICAL REVIEW
 Gout Edward Roddy, 1 Christian D Mallen, 1 Michael Doherty 2 1 Arthritis Research UK Primary Care Centre, Primary Care Sciences, Keele University, Keele ST5 5BG, UK 2 Academic Rheumatology, University
Gout Edward Roddy, 1 Christian D Mallen, 1 Michael Doherty 2 1 Arthritis Research UK Primary Care Centre, Primary Care Sciences, Keele University, Keele ST5 5BG, UK 2 Academic Rheumatology, University
Diagnosis and Management of Gout in 2011
 October 18, 2011 Early and accurate gout diagnosis and disease management are essential. Making the clinical diagnosis takes into consideration the differential diagnosis supported by the use of clinical,
October 18, 2011 Early and accurate gout diagnosis and disease management are essential. Making the clinical diagnosis takes into consideration the differential diagnosis supported by the use of clinical,
D espite reasonable understanding of its pathogenesis
 1312 EXTENDED REPORT EULAR evidence based recommendations for gout. Part II: Management. Report of a task force of the EULAR Standing Committee For International Clinical Studies Including Therapeutics
1312 EXTENDED REPORT EULAR evidence based recommendations for gout. Part II: Management. Report of a task force of the EULAR Standing Committee For International Clinical Studies Including Therapeutics
2.0. Copyright 2015 Wolters Kluwer Health, Inc. All rights reserved. 24 The Nurse Practitioner Vol. 40, No. 8
 2.0 CONTACT HOURS 24 The Nurse Practitioner Vol. 40, No. 8 www.tnpj.com Treatment and gout prevention of o leva Abstract: Gout is a disorder of purine metabolism that primarily occurs in adult males. Elevated
2.0 CONTACT HOURS 24 The Nurse Practitioner Vol. 40, No. 8 www.tnpj.com Treatment and gout prevention of o leva Abstract: Gout is a disorder of purine metabolism that primarily occurs in adult males. Elevated
Plus: How to gain control of symptoms A gout-friendly eating style Lifestyle changes that can help prevent future attacks
 about Gout What You Need to Know about Gout & Uric Acid Plus: How to gain control of symptoms A gout-friendly eating style Lifestyle changes that can help prevent future attacks We re doing everything
about Gout What You Need to Know about Gout & Uric Acid Plus: How to gain control of symptoms A gout-friendly eating style Lifestyle changes that can help prevent future attacks We re doing everything
Current treatment options for acute and chronic gout
 DRUG REVIEW n Current treatment options for acute and chronic gout Kelsey Jordan FRCP and Andrew Jeffries PGDip, MRCP Gout is the only curable form of arthritis, yet only a third of patients with chronic
DRUG REVIEW n Current treatment options for acute and chronic gout Kelsey Jordan FRCP and Andrew Jeffries PGDip, MRCP Gout is the only curable form of arthritis, yet only a third of patients with chronic
Gout: A Clinical Update. Why talk about Gout? Why talk about Gout? Populations at risk: Why is Gout Less Common in Women? US Gout Population: 2009
 Gout: A Clinical Update Peng Thim Fan, MD, FACP Clinical Professor of Medicine Division of Rheumatology David Geffen School of Medicine at UCLA Why talk about Gout? Large increase in gout in the last 20
Gout: A Clinical Update Peng Thim Fan, MD, FACP Clinical Professor of Medicine Division of Rheumatology David Geffen School of Medicine at UCLA Why talk about Gout? Large increase in gout in the last 20
uric acid Non electrolytes of the plasma
 73 uric acid Non electrolytes of the plasma 1 Purines and uric acid Fig 2 JFI Uric acid is the major product of catabolism of the purine nucleosides adenosine and guanosine, Uric acid is sparingly soluble
73 uric acid Non electrolytes of the plasma 1 Purines and uric acid Fig 2 JFI Uric acid is the major product of catabolism of the purine nucleosides adenosine and guanosine, Uric acid is sparingly soluble
Novel uricosurics RHEUMATOLOGY. Thomas Bardin 1,2 and Pascal Richette 1,2. Abstract. Introduction REVIEW
 RHEUMATOLOGY Rheumatology 2018;57:i42 i46 doi:10.1093/rheumatology/kex433 Novel uricosurics Thomas Bardin 1,2 and Pascal Richette 1,2 REVIEW Abstract Objective. According to recent guidelines, the mainstay
RHEUMATOLOGY Rheumatology 2018;57:i42 i46 doi:10.1093/rheumatology/kex433 Novel uricosurics Thomas Bardin 1,2 and Pascal Richette 1,2 REVIEW Abstract Objective. According to recent guidelines, the mainstay
Mono-articular Joint Complaints
 Mono-articular Joint Complaints Derrick J. Todd, M.D., Ph.D. Associate Physician Department of Rheumatology, Immunology, and Allergy Brigham and Women s Hospital Instructor of Medicine Harvard Medical
Mono-articular Joint Complaints Derrick J. Todd, M.D., Ph.D. Associate Physician Department of Rheumatology, Immunology, and Allergy Brigham and Women s Hospital Instructor of Medicine Harvard Medical
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Krystexxa) Reference Number: CP.CPA.57 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Krystexxa) Reference Number: CP.CPA.57 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Pharmacological Management of Knee Pain
 Pharmacological Management of Knee Pain Dr Indi Rasaratnam Consultant Rheumatologist, Epworth Health Care & The Alfred Senior Lecturer, Department of Medicine, Monash University Outline of Presentation
Pharmacological Management of Knee Pain Dr Indi Rasaratnam Consultant Rheumatologist, Epworth Health Care & The Alfred Senior Lecturer, Department of Medicine, Monash University Outline of Presentation
PART MUSCULOSKELETAL DISORDERS
 PART 12 MUSCULOSKELETAL DISORDERS CASE STUDY 77 GOUT For the Patient Case for this case study, see the printed book. DISEASE SUMMARY Definitions Gout is a syndrome of abnormal purine (i.e., DNA nucleotide
PART 12 MUSCULOSKELETAL DISORDERS CASE STUDY 77 GOUT For the Patient Case for this case study, see the printed book. DISEASE SUMMARY Definitions Gout is a syndrome of abnormal purine (i.e., DNA nucleotide
Gout Goals Are Not Being Achieved!! Strengthening The Provider/Patient Alliance Featuring PEPtools TM JointsAflame
 Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance QS Priorities Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance Paul P. Doghramji, MD, FAAFP
Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance QS Priorities Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance Paul P. Doghramji, MD, FAAFP
Krystexxa (pegloticase) Document Number: IC-0158
 Document Number: IC-0158") Krystexxa (pegloticase) Document Number: IC-0158 Last Review Date: 06/27/2017 Date of Origin: 02/07/20103 Dates Reviewed: 11/2013, 08/2014, 07/2015, 07/2016, 09/2016, 12/2016, 03/2017, 06/2017 I. Length
Krystexxa (pegloticase) Document Number: IC-0158 Last Review Date: 06/27/2017 Date of Origin: 02/07/20103 Dates Reviewed: 11/2013, 08/2014, 07/2015, 07/2016, 09/2016, 12/2016, 03/2017, 06/2017 I. Length
Rheumatology Updates for the Primary Care Provider
 Rheumatology Updates for the Primary Care Provider Jean Tayar, MD, RhMSUS Associate Professor Section of Rheumatology and Clinical Immunology Department of General Internal Medicine UT MD Anderson Cancer
Rheumatology Updates for the Primary Care Provider Jean Tayar, MD, RhMSUS Associate Professor Section of Rheumatology and Clinical Immunology Department of General Internal Medicine UT MD Anderson Cancer
Long-term Treatment of Gout: New Opportunities for Improved Outcomes
 Long-term Treatment of Gout: New Opportunities for Improved Outcomes Paul P. Doghramji, MD, FAAFP CONTINUING MEDICAL EDUCATION LEARNING OBJECTIVES Make a presumptive diagnosis of gout based on history
Long-term Treatment of Gout: New Opportunities for Improved Outcomes Paul P. Doghramji, MD, FAAFP CONTINUING MEDICAL EDUCATION LEARNING OBJECTIVES Make a presumptive diagnosis of gout based on history
Study of Febuxostat for the Management of Hyperuricemia in Gout
 Human Journals Review Article October 2015 Vol.:4, Issue:3 All rights are reserved by Sachin S. Shinde et al. Study of Febuxostat for the Management of Hyperuricemia in Gout Keywords: Febuxostat, Hyperuricemia,
Human Journals Review Article October 2015 Vol.:4, Issue:3 All rights are reserved by Sachin S. Shinde et al. Study of Febuxostat for the Management of Hyperuricemia in Gout Keywords: Febuxostat, Hyperuricemia,
Gout Goals Are Not Being Achieved!! Strengthening The Provider/Patient Alliance Featuring PEPtools JointsAflame
 Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance QS Priorities Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance Featuring PEPtools TM JointsAflame
Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance QS Priorities Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance Featuring PEPtools TM JointsAflame
Evidence Based Medicine and the Treatment of Gout
 Evidence Based Medicine and the Treatment of Gout DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine GORDON K. LAM, MD,
Evidence Based Medicine and the Treatment of Gout DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine GORDON K. LAM, MD,
Gout Goals Are Not Being Achieved!! Strengthening The Provider/Patient Alliance Featuring PEPtools JointsAflame
 Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance QS Priorities Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance Featuring PEPtools TM JointsAflame
Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance QS Priorities Gout Goals Are ot Being Achieved!! Strengthening The Provider/Patient Alliance Featuring PEPtools TM JointsAflame
Clinical Biochemistry department/ College of medicine / AL-Mustansiriyah University
 Clinical Biochemistry department/ College of medicine / AL-Mustansiriyah University Dr. Ali al-bayati NUCLEOTIDE METABOLISM Lec. 3 The salvage pathway of purine synthesis Purines that result from the normal
Clinical Biochemistry department/ College of medicine / AL-Mustansiriyah University Dr. Ali al-bayati NUCLEOTIDE METABOLISM Lec. 3 The salvage pathway of purine synthesis Purines that result from the normal
Febuxostat: a safe and effective therapy for hyperuricemia and gout
 DRUG EVALUATIO Febuxostat: a safe and effective therapy for hyperuricemia and gout atasha Jordan & Geraldine M McCarthy Author for correspondence Mater Misericordiae University Hospital, Eccles St. Dublin
DRUG EVALUATIO Febuxostat: a safe and effective therapy for hyperuricemia and gout atasha Jordan & Geraldine M McCarthy Author for correspondence Mater Misericordiae University Hospital, Eccles St. Dublin
Implementing AHRQ Effective Health Care Reviews Helping Clinicians Make Better Treatment Choices
 Implementing AHRQ Effective Health Care Reviews Helping Clinicians Make Better Treatment Choices Gout: Diagnosis and Management Practice Pointers by MATTHEW R. NOSS, DO, MSEd, U.S. Army Health Clinic,
Implementing AHRQ Effective Health Care Reviews Helping Clinicians Make Better Treatment Choices Gout: Diagnosis and Management Practice Pointers by MATTHEW R. NOSS, DO, MSEd, U.S. Army Health Clinic,
Essence of the Revised Guideline for the Management of Hyperuricemia and Gout
 Research and Reviews Essence of the Revised Guideline for the Management of Hyperuricemia and Gout JMAJ 55(4): 324 329, 2012 Hisashi YAMANAKA,* 1 The Guideline Revising Committee of Japanese Society of
Research and Reviews Essence of the Revised Guideline for the Management of Hyperuricemia and Gout JMAJ 55(4): 324 329, 2012 Hisashi YAMANAKA,* 1 The Guideline Revising Committee of Japanese Society of
Therapy for Gout: The Past
 Advances in Therapy for Gout: 2015 The Past, Present, and Future Therapy for Gout: The Past Jonathan Graf, M.D. Professor of Clinical Medicine UCSF Division of Rheumatology, SFGH May 22, 1997 Pity a Tyrannosaur?
Advances in Therapy for Gout: 2015 The Past, Present, and Future Therapy for Gout: The Past Jonathan Graf, M.D. Professor of Clinical Medicine UCSF Division of Rheumatology, SFGH May 22, 1997 Pity a Tyrannosaur?
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 24 June 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 24 June 2009 ADENURIC 80 mg, film-coated tablets B/28 (CIP code: 385 724-4) B/84 (CIP code: 572 820-3) ADENURIC 120
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 24 June 2009 ADENURIC 80 mg, film-coated tablets B/28 (CIP code: 385 724-4) B/84 (CIP code: 572 820-3) ADENURIC 120
Clinical Policy: Colchicine (Colcrys) Reference Number: CP.PMN.123 Effective Date: Last Review Date: 05.18
 Reference Number: CP.PMN.123 Effective Date: Last Review Date: 05.18") Clinical Policy: (Colcrys) Reference Number: CP.PMN.123 Effective Date: 05.01.11 Last Review Date: 05.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Colcrys) Reference Number: CP.PMN.123 Effective Date: 05.01.11 Last Review Date: 05.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Therapy for Gout: The Past
 Advances in Therapy for Gout: 2014 The Past, Present, and Future Therapy for Gout: The Past May 22, 1997 Pity a Tyrannosaur? Sue Had Gout By MALCOLM W. BROWNE Jonathan Graf, M.D. Associate Professor of
Advances in Therapy for Gout: 2014 The Past, Present, and Future Therapy for Gout: The Past May 22, 1997 Pity a Tyrannosaur? Sue Had Gout By MALCOLM W. BROWNE Jonathan Graf, M.D. Associate Professor of
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ABCG2 gene, in gout, 283 285 Acetaminophen, for CPP crystal deposition, 347 ACTH (corticotropin), for gout, 335 336, 383 ADAMTS proteins,
Index Note: Page numbers of article titles are in boldface type. A ABCG2 gene, in gout, 283 285 Acetaminophen, for CPP crystal deposition, 347 ACTH (corticotropin), for gout, 335 336, 383 ADAMTS proteins,
Limitations of Use: (1) Duzallo is not recommended for the treatment of asymptomatic hyperuricemia.
 Duzallo is not recommended for the treatment of asymptomatic hyperuricemia.") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.63 Subject: Duzallo Page: 1 of 5 Last Review Date: December 8, 2017 Duzallo Description Duzallo (lesinurad
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.63 Subject: Duzallo Page: 1 of 5 Last Review Date: December 8, 2017 Duzallo Description Duzallo (lesinurad
THE BURDEN OF SUBCLINICAL SYNOVITIS IN GOUT
 THE BURDEN OF SUBCLINICAL SYNOVITIS IN GOUT PRIYA CHOWALLOOR, MBBS, FRACP This thesis is presented for the degree of Masters of Clinical Research of The University of Western Australia SCHOOL OF MEDICINE
THE BURDEN OF SUBCLINICAL SYNOVITIS IN GOUT PRIYA CHOWALLOOR, MBBS, FRACP This thesis is presented for the degree of Masters of Clinical Research of The University of Western Australia SCHOOL OF MEDICINE
Update on the Management of Gout
 Update on the Management of Gout Professor Anthony D Woolf Duke of Cornwall Department of Rheumatology Royal Cornwall Hospital, Truro, UK Peninsular Medical School Universities of Exeter and Plymouth People
Update on the Management of Gout Professor Anthony D Woolf Duke of Cornwall Department of Rheumatology Royal Cornwall Hospital, Truro, UK Peninsular Medical School Universities of Exeter and Plymouth People
The 2010 Competency Standards addressed by this activity include (but may not be limited to): 4.2.2, 4.2.3, 6.1.2, 6.2.1, 7.1.2, 7.1.3,
: 4.2.2, 4.2.3, 6.1.2, 6.2.1, 7.1.2, 7.1.3,") UPDATE ON GOUT Learning objectives: After completing this activity, pharmacists should be able to: 1. describe the mechanisms underlying hyperuricaemia 2. state the risk factors for development of gout
UPDATE ON GOUT Learning objectives: After completing this activity, pharmacists should be able to: 1. describe the mechanisms underlying hyperuricaemia 2. state the risk factors for development of gout
Oxford Kidney Unit. Dietary advice for managing gout Information for patients
 Oxford Kidney Unit Dietary advice for managing gout Information for patients page 2 This leaflet is for you if you are suffering from gout. It will give you information to help manage your symptoms. What
Oxford Kidney Unit Dietary advice for managing gout Information for patients page 2 This leaflet is for you if you are suffering from gout. It will give you information to help manage your symptoms. What
Gout FACTSHEET REAL LIFE STORY
 1 What is gout? Gout is a type of arthritis where swelling and severe pain develops rapidly in joints, especially at the base of the big toe. Gout affects approximately one in 30 adults, most commonly
1 What is gout? Gout is a type of arthritis where swelling and severe pain develops rapidly in joints, especially at the base of the big toe. Gout affects approximately one in 30 adults, most commonly
Gout Prevention Project. Simplifying Gout Prevention Management for GPs and Patients
 Gout Prevention Project Simplifying Gout Prevention Management for GPs and Patients Gout Prevalance 2 Gout Management primary care level 52.8% of PCP provided optimal medication treatment for acute attack
Gout Prevention Project Simplifying Gout Prevention Management for GPs and Patients Gout Prevalance 2 Gout Management primary care level 52.8% of PCP provided optimal medication treatment for acute attack
ZURAMPIC (lesinurad) oral tablet
 oral tablet") ZURAMPIC (lesinurad) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ZURAMPIC (lesinurad) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES
 Generic Brand HICL GCN Exception/Other PEGLOTICASE KRYSTEXXA 37154 GUIDELINES FOR USE 1. Does the patient have a diagnosis of symptomatic chronic gout (prior to initiating Krystexxa therapy) with clinical
Generic Brand HICL GCN Exception/Other PEGLOTICASE KRYSTEXXA 37154 GUIDELINES FOR USE 1. Does the patient have a diagnosis of symptomatic chronic gout (prior to initiating Krystexxa therapy) with clinical
ACR Meeting November, 2012
 ACR Meeting November, 212 Arhalofenate is a Novel Dual-Acting Agent with Uricosuric and Anti-Inflammatory Properties Yun-Jung Choi, Vanina Larroca, Annette Lucman, Vic Vicena, Noe Abarca, Tim Rantz, Brian
ACR Meeting November, 212 Arhalofenate is a Novel Dual-Acting Agent with Uricosuric and Anti-Inflammatory Properties Yun-Jung Choi, Vanina Larroca, Annette Lucman, Vic Vicena, Noe Abarca, Tim Rantz, Brian