THE EFFECT OF SALBUTAMOL ON LUNG FUNCTION AND CHEST WALL VOLUMES AT REST AND DURING EXERCISE IN COPD
|
|
|
- Polly Farmer
- 5 years ago
- Views:
Transcription
1 Thorax Online First, published on June 30, 2005 as /thx THE EFFECT OF SALBUTAMOL ON LUNG FUNCTION AND CHEST WALL VOLUMES AT REST AND DURING EXERCISE IN COPD Aliverti A. (1), Rodger K. (2), Dellacà R.L. (1), Stevenson N. (2), Lo Mauro A. (1), Pedotti A. (1), Calverley P.M.A. (2) (1) Dipartimento di Bioingegneria, Politecnico di Milano, Italy (2) University Department of Medicine, University Hospital Aintree, Liverpool, UK. The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence on a worldwide basis to the BMJ Publishing Group Ltd and its Licensees to permit this article to be published in THORAX and any other BMJPGL products to exploit all subsidiary rights, as set out in our licence ( Corresponding Author: Aliverti Andrea, PhD Dipartimento di Bioingegneria - TBMLab Politecnico di Milano P.zza Leonardo da Vinci, Milano Italy Ph: Fax: andrea.aliverti@polimi.it This work was supported in part by the European Community CARED FP5 project (contract n. QLG5-CT ) Running head: chest wall volumes after salbutamol in COPD Keywords: COPD; breathing pattern; bronchodilators; chest wall volume; exercise Copyright Article author (or their employer) Produced by BMJ Publishing Group Ltd (& BTS) under licence.
2 ABSTRACT Background. Inhaled bronchodilators can increase exercise capacity in COPD by reducing dynamic hyperinflation but treatment is not always effective. This may reflect the degree to which the abdomen allows dynamic hyperinflation to occur. Method. We conducted a blinded randomised cross-over trial of 5 mg nebulised salbutamol or saline on endurance exercise time in 18 COPD patients (age 67.1 (6.3SD) yrs; FEV 1 = 40.6 %pred (15.0 SD). We recorded breathing pattern, metabolic variables, dyspnoea intensity and total and regional chest wall volumes non-invasively with opto-electronic plethysmography (OEP) at rest and during exercise. Results. Salbutamol increased FEV 1, FVC and inspiratory capacity and reduced FRC and residual volume significantly. OEP showed the change in resting FRC to be mainly in the abdominal compartment. Although end-expiratory chest wall volume was 541 ml (118 SE) lower (p<0.001) at end-exercise, endurance time was unchanged by the bronchodilator. Changes in resting lung volumes were smaller when exercise duration did not improve but FEV 1 still rose significantly after active drug. Post-bronchodilator these patients tried to reduce EELV when exercising while those exercising longer continued to allow end-expiratory abdominal wall volume to rise. This change to a more euvolumic breathing pattern was associated with a lower oxygen pulse and a significant fall in endurance time with higher iso-time levels of dyspnoea. Conclusions. Nebulised salbutamol improved forced expiratory flow in most COPD patients but less hyperinflated patients tried to reduce abdominal compartmental volume after active therapy and this reduced their exercise capacity. Identifying these patients has important therapeutic implications as does the understanding of the mechanisms that control chest wall muscle activation. INTRODUCTION Chronic obstructive pulmonary disease (COPD) is characterised by the presence of persistent and usually progressive airflow obstruction (1). When expiratory airflow limitation develops during tidal breathing patients must allow the end-expiratory lung volume (EELV) to rise to permit a higher expiratory flow rate (dynamic hyperinflation) or stop exercising relatively quickly (euvolumic response) (2). Either way the patient s exercise tolerance is limited and this is associated with a worse health status (3). Bronchodilator drugs like salbutamol, a short-acting beta agonist, are widely prescribed for the symptomatic relief of breathlessness in COPD (4). Unfortunately, not all patients benefit from bronchodilator therapy and the relationship between the change in spirometry and the subsequent exercise capacity is weak (5). A reduction in end-expiratory lung volume during exercise has been reported with short acting inhaled drugs (6), and long acting anticholinergics and beta agonists (7,8) and this relates to the reported reduction in dyspnoea. However exercise duration does not always increase even when lung mechanics improve (9). We have previously described two different patterns of chest wall volume change during exercise in COPD euvolumic patients who try to reduce end-expiratory chest wall volume during when exercise and hyperinflators who let chest wall volume rise, mainly by a change in abdominal compartmental volume (2). Bronchodilators can reduce total chest wall volume at rest (10) but nothing is known about how these drugs affect the breathing strategy adopted during exercise and whether this relates to the subsequent exercise performance. We hypothesised that bronchodilator therapy would reduce chest wall volumes at rest and during exercise. Moreover we anticipated that patients who increased their end-expiratory abdominal compartmental volume during exercise after the active drug would be able to exercise for longer. To 2
3 test these ideas we conducted a double blind randomised cross-over trial of the effect of nebulised salbutamol on lung function, chest wall volume and endurance exercise capacity in patients with stable COPD. METHODS Subjects The study recruited 18 patients with clinically stable COPD diagnosed by accepted criteria (1, 11). All had been smokers and complained of exertional dyspnoea. None had clinical or physiological features of bronchial asthma or a history of exacerbation in the last 6 weeks. There were no comorbid conditions limiting exercise. Patients were studied before pulmonary rehabilitation and were unfamiliar with physiological exercise testing and they discontinued routine bronchodilator drugs for 4 hours (short-acting) or 12 hours (long-acting) before attendance. The protocol was approved by the district research ethics committee and informed consent was obtained by all patients. Study design The study had a randomized double-blind cross-over design. During an initial screening visit, patients were thoroughly familiarized with all procedures and symptom rating scales, and pulmonary function testing and symptom-limited incremental cycle exercise testing was performed to determine maximum workload (Wmax). Then subjects were randomised to receive either highdose nebulised salbutamol or placebo. Each subject attended twice within a period of 3 to 10 days. At each visit pulmonary function, subdivisions of lung and chest wall volumes and resting breathing pattern were measured. Then, either salbutamol or placebo treatment was administered by inhalation over approximately 15 min. Thirty minutes after the treatment finished, pulmonary function, subdivisions of lung and chest wall volumes and resting breathing pattern measurements were repeated. Finally, a symptom limited submaximal (70% Wmax) constant-load cycle exercise testing was performed. Procedures and measurements - Resting Lung Function testing Spirometry and body plethysmography were performed using automated testing equipment (Medgraphic Autolink 1085D, Medical Graphics, St Paul, MN) according to recommended standards (12). Specialised flow/volume loop software was used to measure the FEV 1, FVC and maximal expiratory flow indices (FEF25% and FEF75%) during spirometry. Thoracic gas volume (TGV) was measured with patients seated in the body plethysmograph and panting against a closed shutter at a frequency of ~1 Hz with their cheeks supported. TLC was obtained as the sum of TGV and the inspiratory capacity measured soon after re-opening the shutter; RV was calculated as the difference between TLC and a slow expiratory vital capacity; FRC was obtained from TGV corrected for any difference between the volume at which the shutter was closed and the average end-expiratory volume of the four preceding tidal breaths. - Chest wall volumes Procedures for measuring chest wall volumes by Opto-Electronic Plethysmography (OEP), have been described in detail in our previous publications (2, 13). The position of 89 retro-reflective markers placed front and back over the chest wall from clavicles to pubis was recorded at 60 Hz by six calibrated video cameras (Smart system BTS, Milan), placed three in front of the subject and three behind. From the three-dimensional co-ordinates of the markers, obtained by stereophotogrammetry, a specialised software based on Gauss s theorem provided the continuous 3
4 measurement of the volume of the total chest wall (V CW ), the rib cage (V RC ) and the abdomen (V AB ), with V CW = V RC + V AB. The markers were placed on the patients after the first spirometric and body box evaluation. Then, they were asked to sit on an unsupported chair and OEP measurement were taken during 3 minutes of spontaneous breathing at rest and during a series of 3-4 slow vital capacity (SVC) manoeuvres. From the breath-by-breath measurements of Vcw during quiet breathing, the ventilatory pattern including tidal volume (V T ), breathing frequency (f B ), minute ventilation (V E ), inspiratory (T I ) and expiratory (T E ) time, mean inspiratory (V T /T I ) and expiratory (V T /T E ) flow, was determined by calculating the average values of these variables. From the OEP measurements carried out during the SVC manoeuver, the average operating total and compartmental chest wall volumes (i.e., V CW, V RC and V AB at TLC, FRC and RV) were obtained. - Treatment Treatments were administered using a face mask from an Acorn nebuliser at a flow rate of 4 L/min over a period of 15 min. The total volume of nebulised solution was 2.5 ml for all patients: salbutamol (5 mg) was compared with a placebo, which consisted of sterile 0.9% sodium chloride solution. - Exercise testing The two exercise tests were performed on an electrically braked cycle ergometer at 70% of the maximum work rate achieved during the incremental exercise test. During exercise, standard measurements (V O 2, V CO 2, HR, SaO 2 ) were collected using a cardiopulmonary exercise testing system (Medical Graphics, St Paul, MN) with patients wearing a noseclip and breathing though a mass flow sensor (70 ml dead space). The tests consisted of a steady-state resting period of 90 seconds, a subsequent 90 seconds warming-up by unloaded pedalling, followed by an immediate increase in work-rate; pedalling frequencies were maintained at approximately 60 revolutions per minute. Initial and end-exercise values ( 1 min and stop in the following text and figures) were defined respectively as the mean over the period between 45 and 75 sec from the beginning of loaded exercise and over the last 30 s of loaded exercise. OEP measurements were also performed during constant workload exercise with the patients wearing the previously positioned markers. To keep the arms from obscuring relevant markers, the chest the patient grasped handles positioned laterally at mid-sternum level. Special care was taken to allow the visibility of the markers placed on the thoraco-abdominal surface and to analyze the patients with the same posture (trunk position) during the two different tests. From OEP measurements, the ventilatory pattern was determined, including breath-by-breath variations of endexpiratory and end-inspiratory volumes of V CW, V RC and V AB. At rest, every 1 min during exercise and at end-exercise, subjects rated the intensity of their breathing and leg discomfort using the modified Borg scale (14). Statistical Analysis Data are presented as mean (SE) unless otherwise stated. Paired or unpaired t-student tests were used as appropriate to respectively compare placebo vs salbutamol and improvers vs nonimprovers group. A statistical significance of 0.05 was used for all analyses, with appropriate Bonferroni corrections for multiple comparisons. Randomisation was performed using a table of random numbers to generate a concealed subject allocation card. As we did not have data about the effect of bronchodilators on abdominal compartmental volume change before this study, the trial was powered on an expected difference in inspiratory capacity of 200 ml between treatment groups and our 18 subjects had a 90% power to detect this difference at the 5% level of significance. To identify the mechanisms determining the response to therapy we decided a priori to arbitrarily classify patients whose post-salbutamol exercise duration was greater as improvers and those where it was equal to / less than exercise duration after saline as nonimprovers, irrespective of the 4
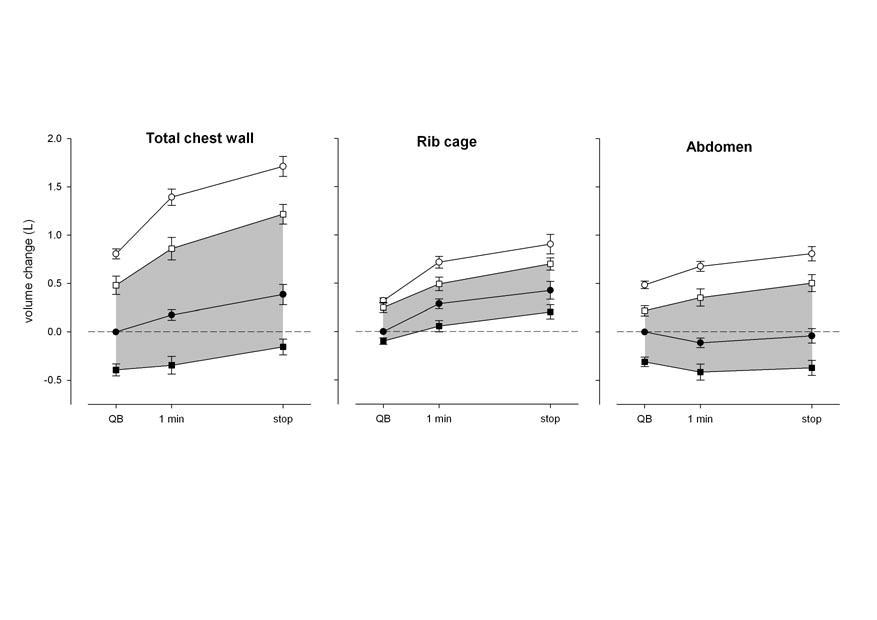
5 magnitude of the difference after the drug. Statistical analysis of these secondary endpoints is included to aid future hypothesis generation and should be treated with caution given the number involved. RESULTS Demographic data for the patients studied are shown in table 1. They were an elderly group with moderate to severe airflow limitation, significantly raised lung volumes, and markedly impaired exercise capacity. Treatment effects resting data The effect of treatment on baseline pulmonary function is shown in fig. 1 as changes from pre- to post-treatment. Comparing the changes in spirometry and lung volumes after placebo and salbutamol in the whole population of patients, statistically significant differences were found in FEV 1 (p<0.001), FVC (p<0.05), FEF25% (p<0.01), FEF75% (p<0.01), FRC (p<0.01) and IC (p<0.001). The changes in the subdivisions of lung volume, measured by total body plethysmography, were not statistically different from the changes in the chest wall at the corresponding volumes (TLC, FRC and RV) measured by OEP (fig. 2). The decrease in functional residual capacity induced by salbutamol was accomplished by a decrease in abdominal volume rather than rib cage volume. The decrease in residual volume was instead the result of the decrease of both rib cage and abdominal volume (fig. 2). Although the thoraco-abdominal configuration at FRC could be considered relaxed, at RV it was active. Hence the greater reduction of Vab compared to Vrc at FRC shown in fig. 2 is likely to represent a greater compliance of the abdominal compared to the rib cage compartment. In this situation the thoraco-abdominal configurational change at active RV reflects the actions of the expiratory muscles on the two compartments, and not only their inherent mechanical properties. The ventilatory pattern analysed at rest after placebo and bronchodilator drug is shown in table 2. There were no changes in the timing or frequency of respiration after any treatment, but mean expiratory flow (V T /T E ) and minute ventilation (V E ) showed significant increases after salbutamol (p<0.05). Treatment effects exercise data At the end of the symptom-limited constant workload exercise after placebo treatment, endexpiratory Vcw increased by 386 (106) ml (fig 3, left panel). End-expiratory Vrc increased by 426 (91) ml (fig 3, middle panel). In contrast, end expiratory Vab remained practically constant throughout exercise with the end-inspiratory volumes rising to accommodate the increases in Vrc (fig 3, right panel). End-inspiratory Vcw approached the TLC values measured before exercise and this was accomplished by increases in both Vrc and Vab. The dynamic behaviour of chest wall volume after salbutamol in the overall population of patients was very similar to that observed after placebo, with the only difference being that the operating volumes were shifted toward lower values. After placebo end-expiratory chest wall volume (EEVcw) fell in 4 patients (mean change 64 ml) while a decrease in EEVcw occurred in 5 subjects (mean change 172 ml) after salbutamol. As a result, after bronchodilator treatment end-inspiratory Vcw did not reached the TLC values and at end-exercise a significant inspiratory reserve volume was still present. The ventilatory pattern at end-exercise did not show differences after placebo and bronchodilator apart from a significant prolongation in expiratory time at end-exercise after salbutamol, in keeping 5
6 with the lower end-expiratory chest wall volume (table 2). There were no differences in the degree of oxygen desaturation during exercise between placebo and salbutamol days. Considering the overall population of patients, symptom-limited exercise endurance time did not improve significantly after salbutalmol compared with placebo (330 (35) sec and 316 (53) sec, respectively). Treatment effects responder analysis In 12 patients endurance time increased by 106 (23) sec (a mean improvement of 86 (30)%), while in the other 6 patients it decreased by 170 (42) sec (-34 (10) %). Individual changes are reported in fig. 4. Table 3 illustrates baseline data and the response to bronchodilator treatment. Nonimprovers tended to have smaller Wmax (but longer endurance times) and better pulmonary function (FEV1, FVC, expiratory flows) than those improving their exercise duration, although only baseline FRC and RV achieved statistical significance (p<0.05), the improvers exhibiting more hyperinflation and gas trapping before the bronchodilator. After salbutamol those whose exercise performance improved had significantly increased FEV 1 (p<0.001), FVC (p<0.001), forced expiratory flows (p<0.01), IC (p<0.001) and decreased FRC (p<0.01) and RV (p<0.01). In contrast, patients who did not increase their exercise capacity increased their FEV1 (p<0.01) and reduced FRC (p<0.05) post-salbutamol, the other variables trending to improvement but not significantly so. An improvement in resting IC of more than 200 ml (the day to day reproducibility) was present in 50% of these patients. At rest, the ventilatory pattern, metabolic rate and dyspnea intensity were similar in the two groups after both placebo and salbutamol treatment (tables 3 and 4). After the saline placebo patients not improving stopped exercise at a lower minute ventilation and a lower dyspnoea intensity compared to those who benefited from therapy. The peak minute ventilation was unaffected by the test drug but the oxygen pulse fell significantly (p<0.01) at endexercise post-salbutamol in the non-improvers (table 4). End-inspiratory and end-expiratory volumes of the entire chest wall (fig. 5, left) and of rib cage and abdominal compartment (data not shown) during rest and exercise after placebo treatment were very similar in the two groups. In contrast, two different patterns of change in Vcw occurred during exercise after bronchodilator treatment. While the improvers continued to increase both end-inspiratory and end-expiratory chest wall volume, the nonimprovers maintained a significantly lower total chest wall volume (fig. 5, right) (p<0.05). This was entirely due to a difference in the abdominal compartmental volume (fig. 6). Ensemble averages of flow-volume curves during forced expiratory maneuvers and tidal breathing at rest and end-exercise are shown in fig. 7 for improvers (left) and non-improvers (right). Volume data reported in the graphs have been obtained by integrating the flow measured at the mouth and then aligning it to the volume of the chest wall measured by OEP. These data show a shift in the average maximum expiratory flow-volume envelope which did not achieve significance for the group as a whole. Patients improving their endurance time (left) reduced their resting endexpiratory lung volume (EELV) post-bronchodilator and this change persisted at end-exercise (middle-left panel vs. lower-left panel). Those not improving (right) had a lower EELV during resting breathing relative to their predicted TLC. After exercise post-bronchodilator, ELLV did not rise and the gas compression artefact (area beyond the MEFV curve) was more evident in keeping with the increased action of the expiratory muscles in the abdominal compartment (middle-right panel vs. right-lower panel). The values of dyspnoea reported by the nonimprovers at the end of exercise were significantly lower (p<0.05) than those reported by the improvers both after placebo and after bronchodilators (see table 4). Within the two groups, bronchodilator therapy did not change the values of both dyspnea and leg effort at the end of exercise. However, these similar values were obtained after a time longer in the improvers and shorter in the nonimprovers. 6
7 DISCUSSION Evaluating the effect of bronchodilator therapy on exercise capacity and dyspnea has proven surprisingly difficult in COPD with contradictory data being reported with different drug classes in different studies (15). More recent studies using long acting inhaled agents have demonstrated improvements in both breathlessness and endurance time (8), although not all workers have confirmed the latter effect (9). These differences are usually attributed to differences in the exercise protocol used and to random variation in the patient s ability to perform the test. Our data before and after salbutamol suggest an alternative explanation for these findings. While our group as a whole showed the improvement in dynamic hyperinflation reported by others, the one third of patients who failed to improve their endurance time were less severely affected by COPD and showed smaller volume changes at rest. They also adopted a very different pattern of chest wall volume distribution on exercise that we believe helps to explain the unexpected worsening of their exercise performance. Nebulised salbutamol produced statistically significant increases in FEV1, FVC and resting IC with a reduction in FRC and RV. Neither TLC nor FEV1/FVC changed significantly suggesting that the improvements in expiratory flow were related to change in operating volume. The constant FEV1/FVC ratio suggests that the time constant (resistance x compliance) of the respiratory system did not change after the bronchodilator and that the reduction in gas trapping indicated by the increase in FVC was due to the opening of lung units with similar mechanical properties to those functioning prior to bronchodilation. The total fall in end-expiratory chest wall volume measured by OEP at rest was similar to that identified by body plethysmography confirming the accuracy of the OEP data (10). The change in dynamically regulated volume corresponding to FRC was accompanied by a fall in the volume of the abdominal compartment at rest, while the reduction in RV was equally distributed between rib cage and abdominal compartments. This change in chest wall shape after the bronchodilator suggests that at rest the diaphragm was relatively longer and potentially capable of greater force generation as observed previously (9). It is also likely that the change of lung volume influenced the length of the abdominal muscles with consequences on their activation in response to loading (16). The pooled end-expiratory and end-inspiratory total chest wall volume data during endurance exercise, resemble those seen with other bronchodilator drugs where end-expiratory lung volume has been measured indirectly (8). Despite the improved lung and chest wall mechanics, we saw no significant difference in exercise duration or end-exercise symptoms in this patient group. We examined a range of characteristics at rest and during exercise that might explain this heterogeneous response to the bronchodilator. Separating patients into improvers and non improvers highlighted several important differences. Patients who improved were older, had worse airflow obstruction, higher resting lung volumes and better exercise performance after the placebo compared to non-improvers. Only FEV1 (both absolute and %predicted) was significantly higher after the bronchodilator. However, there was an ~18% increase in FVC post-bronchodilator compared with an ~8% change in improvers. This greater reduction in gas trapping may reflect the greater degree of hyperinflation seen at rest in the improvers. Most of our patients would not be considered reversible using currently recommended criteria (17) despite the statistically significant improvement in expiratory flow in the group as a whole. Reliance on changes in IC would have been better but an improvement in resting IC of more than 200 ml (the day to day reproducibility) (18) was still seen in subjects who subsequently failed to improve their exercise capacity. Non-improvers had better spirometry post-salbutamol than those whose performance improved. It is unlikely that they stopped exercising because of a limited ventilatory reserve. We believe that differences in the activation of the chest wall muscles after the bronchodilator explain this apparently paradoxical behaviour. The results during the placebo test were similar irrespective of 7
8 the subsequent response to bronchodilator. However patients whose exercise endurance improved after treatment showed a significant fall in chest wall volume after the bronchodilator but adopted the same pattern of progressive hyperinflation during exercise at this lower operating volume. In contrast those with worse post-bronchodilator exercise performance were now able to reduce their end-expiratory chest wall volume after one minute of exercise, although this tended to rise as exercise ended. These changes in chest wall volume were due to differences in the volume of the abdominal but not the rib cage compartment. The distribution of volume during the exercise after the bronchodilator resembles that seen in some healthy subjects when exercising while breathing through a Starling resistor (19, 20) and is qualitatively similar to the euvolumic pattern reported previously (2). Figure 7 indicates that there was dynamic gas compression/blood shift occurring at maximal exercise in the non-improvers after salbutamol. Previous work suggests that excessive abdominal muscle activation can impair venous return, decrease cardiac output (21, 22) and shift blood from the thorax to the extremities (2, 19, 20). Oxygen pulse, an indirect measure of cardiac output and a reliable guide to exercise performance in COPD (23), fell in the nonimprovers suggesting that this mechanism might be operative in our patients. Why these breathing patterns should be adopted is not clear. One possibility could be that the reduction in functional residual capacity in the less severely affected patients changed either the ability of the diaphragm to generate force and displace volume or the way in which expiratory muscles are acting. There may be variable degrees of abdominal muscle recruitment by reflex mechanisms in COPD patients which explain these differing responses (24). Alternatively the breathing strategy adopted when patients develop expiratory flow limitation during tidal breathing may be a learned response that is influenced by the degree of expiratory flow reserve, as suggested previously (2). Future studies should examine the relationship between abdominal muscle use and expiratory flow limitation which can now be studied noninvasively and continuously (25). In our study the end-exercise Borg score was not influenced by treatment. However there was a clear positive effect on the iso-time Borg score compared to placebo and no evidence of benefit in this variable in the nonimprover group. This is not likely to be due to a simple regression to the mean effect as the order of placebo therapy was randomised. Patients adopting a euvolumic breathing pattern spontaneously before bronchodilatation are as breathless when they stop as hyperinflating patients who exercise for longer (2). Whether this reflects the greater degree of expiratory muscle activation, as suggested in studies of healthy individuals (26) or has some other mechanism is still to be determined. Our data require some qualification. Although this was a blinded cross-over trial the data only apply to one post-bronchodilator exercise study and it would be unwise to extrapolate further until the consistency of the response pattern on repeated testing and on different days is established. We used a large dose of salbutamol high on the dose-response curve established using a spirometric outcome (27) and the relevance of this to lower doses is less certain. The complexity of the protocol limited the number of patients recruited and the number of nonimprovers selected by our arbitrary response criterion was underpowered to exclude a difference in several of the explanatory variables. However the large differences in the chest wall volume response to exercise is unlikely to have arisen by chance given the small variation in these variables after the placebo treatment which was itself administered in random order. In summary we have confirmed that nebulised beta-agonists reduce end-expiratory chest wall volume during endurance exercise in stable COPD. However the ability to exercise soon after receiving active treatment is influenced by the degree of pre-bronchodilator pulmonary hyperinflation and the way in which the chest wall muscles adapt to the change in lung mechanics produced by the bronchodilator. Patients with less hyperinflation may, paradoxically, do worse after treatment by adopting a physiologically inappropriate breathing strategy. These data help explain 8
9 why the patients subjective report of the effectiveness of therapy is more valuable than reliance on spirometric change. Additionally it demonstrates that a deterioration in exercise performance after active therapy can have a physiological rather than just a statistical basis. It also highlights the need to understand how and in what circumstances COPD patients permit their end-expiratory lung volume to rise during exercise. REFERENCES 1. Chronic obstructive pulmonary disease. National clinical guideline on management of chronic obstructive pulmonary disease in adults in primary and secondary care. Thorax 2004;59 Suppl 1: Aliverti A, Stevenson N, Dellacà RL, Lo Mauro A, Pedotti A, Calverley PMA. Regional Chest Wall Volumes during exercise in Chronic Obstructive Pulmonary Disease. Thorax 2004; Jones PW. Health status measurement in chronic obstructive pulmonary disease. Thorax, 2001; 56: Sutherland ER, Cherniack RM. Management of chronic obstructive pulmonary disease (review). N Engl J Med, 2004; 24; 350: Hay JG, Stone P, Carter J, Church S, Eyre-Brook A, Pearson M, Woodcock A, Calverley PM. Bronchodilator reversibility, exercise performance and breathlessness in stable chronic obstructive pulmonary disease. Eur Respir J 1992; 5:659 64, O Donnell DE, Fluge T, Gerken F, Hamilton A, Webb K, Aguilaniu B, Make B, Magnussen H. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD. Eur Respir J 2004; 23: O Donnell DE, Lam M, Webb KA. Spirometric correlates of improvement in exercise performance after anticholinergic therapy in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1999; 160: O Donnell DE, Voduc N, Fitzpatrick M, Webb KA. Effect of salmeterol on the ventilatory response to exercise in chronic obstructive pulmonary disease. Eur Respir J 2004, 24: Man WD, Mustfa N, Nikoletou D, Kaul S, Hart N, Rafferty GF, Donaldson N, Polkey MI, Moxham J. Effect of salmeterol on respiratory muscle activity during exercise in poorly reversible COPD, Thorax 2004; 59: Duranti R, Filippelli M, Bianchi R, Romagnoli I, Pellegrino R, Brusasco V, Scano G. Inspiratory capacity and decrease in lung hyperinflation with albuterol in COPD. Chest, 2002; 122: Anonymous. BTS guidelines for the management of chronic obstructive pulmonary disease. The COPD Guidelines Group of the Standards of Care Committee of the BTS. Thorax 1997;52 Suppl 5:S American Thoracic Society. ATS Statement. Snowbird Workshop on Standardization of Spirometry. Am Rev Respir Dis 1979;
10 13. Cala SJ, Kenyon CM, Ferrigno G, Carnevali P, Aliverti A, Pedotti A, Macklem PT and Rochester DF. Chest wall and lung volume estimation by optical reflectance motion analysis. J Appl Physiol 1996; 81: Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc 1982; 14: Liesker JJ, Wijkstra PJ, Ten Hacken NH, Koeter GH, Postma DS, Kerstjens HA. Systematic Review of the Effects of Bronchodilators on Exercise Capacity in Patients With COPD. Chest 2002;121: Iscoe S. Control of abdominal muscles (review). Prog Neurobiol. 1998; 56(4): Pauwels RA, Buist AS, Calverley PMA, Jenkins CR, Hurd SS. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med 2001, 163: Hadcroft J,.Calverley PM. Alternative methods for assessing bronchodilator reversibility in chronic obstructive pulmonary disease. Thorax 2001;56: Iandelli I, Aliverti A, Kayser B, Dellacà R, Cala S, Duranti R, Kelly S, Scano G, Sliwinski P, Yan S, Macklem PT, Pedotti A. Determinants of exercise performance in normal men with externally imposed expiratory flow-limitation. J Appl Physiol 2002, 92(5): Aliverti A, Iandelli I, Duranti R, Cala S, Kayser B, Kelly S, Misuri G, Pedotti A, Scano G, Sliwinski P, Yan S, Macklem PT. Respiratory muscle dynamics and control during exercise with externally imposed expiratory flow-limitation. J Appl Physiol 2002; 92(5): Stark-Leyva, Kristy N., Ken C. Beck, and Bruce D. Johnson. Influence of expiratory loading and hyperinflation on cardiac output during exercise. J Appl Physiol 2004; 96: Simon M, LeBlanc P, Jobin J, Desmeules M, Sullivan MJ, Maltais F. Limitation of lower limb V O2 during cycling exercise in COPD patients. J Appl Physiol 2001;90: Montes de Oca M, Rassulo J, Celli BR. Respiratory muscle and cardiopulmonary function during exercise in very severe COPD. Am J Respir Crit Care Med 1996;154: Polkey MI, Kyroussis D, Hamnegard CH, Mills GH, Hughes PD, Green M, Moxham J. Diaphragm performance during maximal voluntary ventilation in Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med 1997;155: Dellacà RL, Santus P, Aliverti A, Stevenson N, Centanni S, Macklem PT, Pedotti A, Calverley PMA. Detection of expiratory flow limitation in COPD using the forced oscillation technique. Eur Respir J 2004, 23: Kayser B, Sliwinski S, Yan S, Tobiasz M, and Macklem PT. Respiratory effort sensation during exercise with induced expiratory flow limitation in healthy humans. J Appl Physiol 1997; 83: Vathenen AS, Britton JR, Ebden P, Cookson JB, Wharrad HJ, Tattersfield AE. High-dose inhaled albuterol in severe chronic airflow limitation. Am Rev Respir Dis 1988, 138:
11 FIGURE LEGENDS Fig. 1 - Effect of nebulised agent on pulmonary function and lung volumes. ***: p<0.001; **: p<0.01; *: p<0.05; n.s.= not significant Fig. 2 - Effect of nebulised agent on lung and chest wall volume changes at total lung capacity (TLC), functional residual capacity (FRC) and residual volume (RV). **: p<0.01; n.s.= not significant Fig. 3 - End-Expiratory (closed symbols) and end-inspiratory (open symbols) volume changes after placebo (circles) and bronchodilator (squares) during quiet breathing (QB), after 1 min of exercise and in the 30 sec before stopping exercise (stop). All values are referred to end-expiratory volumes during quiet breathing after placebo treatment. The shaded area indicates the range of volume changes during the test after bronchodilator. Data are expressed as mean±se (n=18). Fig. 4 Left panel: Group mean and individual data for constant workload exercise endurance time after the placebo and salbutamol nebulisation. The lines connect data from the same patient. Errors bars represent standard error of the mean. Right panel: Mean, SE, 5% and 95% confidence intervals of the difference in endurance time in all subjects and in those where endurance time increased (IMP) or did not improve (NIMP) after salbutamol. Fig. 5 - End-Expiratory (closed symbols) and end-inspiratory (open symbols) volume changes after placebo (left) and bronchodilator (right) during quiet breathing (QB), after 1 min of exercise and in the 30 sec before stopping exercise (stop). Data are divided into two groups of patients, those who improved exercise time after bronchodilator, i.e. the improvers (circles, n=12) and those who did not, i.e. nonimprovers (squares, n=6). All values are referred to end-expiratory volumes during quiet breathing after placebo treatment. Data are expressed as mean±se. *p<0.05 (improvers vs nonimprovers). Fig. 6 - End-Expiratory (closed symbols) and end-inspiratory (open symbols) volume changes of the rib cage (left) and the abdomen (right) during quiet breathing (QB), after 1 min of exercise and in the 30 sec before stopping exercise (stop) of the improvers (circles, n=12) and nonimprovers (squares, n=6) patients after salbutamol. All values are referred to end-expiratory volumes during quiet breathing after placebo treatment. Data are expressed as mean±se. *p<0.05 (improvers vs nonimprovers). Fig. 7 Flow- volume curves obtained during forced expiratory manoeuvre (upper panels), tidal breathing at rest (middle panels) and end-exercise (lower panels). Maximal expiratory flow-volume (MEFV) curves are repeated in the middle and lower panels for reference. Left panels refer to patients who improved exercise endurance time after salbutamol (improvers) and right panels to patients who did not (non-improvers). Each curve is the ensemble average of the individual curves of all patients belonging to these two groups. In each graph the data obtained after placebo (thin lines) and salbutamol (thick lines) treatment are reported, while error bars represent standard error of mean flow and volume at 0, 20, 40, 60, 80 and 100% of the duration of the manoeuvre or the tidal breath. See text for details. 11
12 Table 1 - Patients baseline anthropometric, spirometric, lung function, exercise and resting breathing pattern data Value (SD) Subjects n 18 Males / Females 15 / 3 Age (yrs) 67.1 (6.3) Body mass index (kg m -2 ) 24.3 (4.2) % predicted (SD) Lung function FEV 1 (L) 1.14 (0.41) 40.6 (15.0) FVC (L) 2.74 (0.72) 74.5 (17.2) FEV 1 / FVC (%) 42.4 (11.6) FEF 25% (L sec -1 ) 1.20 (0.90) 19.2 (13.6) FEF 75% (L sec -1 ) 0.20 (0.07) 17.8 (5.9) TLC (L) 7.87 (1.04) (11.6) FRC (L) 5.86 (1.10) (26.0) RV (L) 4.80 (1.03) (47.1) IC (L) 2.02 (0.47) 68.2 (16.7) Resting breathing pattern V T (L) (0.221) f R (breaths min -1 ) 23.9 (9.5) T I (sec) 1.17 (0.29) T E (sec) 1.99 (0.73) V T /T I (L sec -1 ) (0.081) V T /T E (L sec -1 ) (0.102) V E (L min -1 ) 15.9 (0.8) Exercise performance Wmax (watt) 66.8 (16.2) Exercise time at 70% Wmax (sec) 318 (224) 12
13 Table 2 Resting and end-exercise ventilatory pattern, metabolic and cardiac variables after placebo and salbutamol treatment. Values are expressed as means (SD). *: p<0.05 (salbutamol vs placebo) After placebo After Salbutamol exercise time (sec) 316 (52) 330 (35) Rest End-exercise Rest End-exercise V T (L) (0.052) (0.074) (0.065) (0.064) f R (breaths min -1 ) 23.9 (2.2) 34.3 (1.8) 25.2 (2.2) 32.7 (2.1) T I (sec) 1.17 (0.07) 0.82 (0.05) 1.18 (0.08) 0.90 (0.07) T E (sec) 1.99 (0.17) 1.08 (0.06) 1.94 (0.21) 1.26 (0.13)* V T /T I (L sec -1 ) 0.71 (0.04) 1.71 (0.10) 0.75 (0.04) 1.65 (0.10) V T /T E (L sec -1 ) 0.43 (0.02) 1.30 (0.07) 0.48 (0.03)* 1.25 (0.09) V E (L min -1 ) 15.9 (0.8) 43.7 (2.5) (0.99)* 41.6 (2.8) V O 2 (L min -1 ) 0.34 (0.02) 0.93 (0.05) 0.33 (0.02) 0.95 (0.05) V CO 2 (L min -1 ) 0.29 (0.02) 0.87 (0.05) 0.28 (0.01) 0.91 (0.06) RER 0.84 (0.02) 0.93 (0.02) 0.86 (0.03) 0.96 (0.03)* HR (beats min -1 ) 91.1 (3.6) (4.4) 89.1 (2.0) (4.1) V O 2 /HR (ml/beat) 3.6 (0.2) 8.7 (0.4) 3.7 (0.2) 8.3 (0.6) SaO 2 (%) 96.0 (0.6) 93.6 (0.5) 96.2 (0.5) 94.5 (0.6) Breathlessness 0.75 (0.25) 5.61 (0.48) 1.00 (0.30) 6.28 (0.52) Leg effort 0.72 (0.24) 5.33 (0.56) 0.83 (0.23) 6.03 (0.68) Thorax: first published as /thx on 30 June Downloaded from on 19 November 2018 by guest. Protected by copyright. 13
14 Table 3 - Anthropometric, spirometric, lung function, exercise and resting breathing pattern data pre- and post- bronchodilator (BD) treatment by salbutamol divided in the group of patients who increased exercise time after treatment (improvers) and those who did not (nonimprovers). Values are expressed as means (SD) and as differences between post- and pre-bronchodilator (95% confidence intervals, CI). ***,**,*: p<0.001, 0.01, 0.05 (Pre-BD vs Post-BD);,, : p<0.001, 0.01, 0.05 (Improvers vs Nonimprovers) Improvers group Nonimprovers group Subjects n 12 6 Males / Females 11/1 4/2 Age (yrs) 67.6 (1.9) 66.0 (2.7) Body mass index (kg m -2 ) 23.9 (1.2) 25.2 (2.0) Maximum workload (watt) 65.9 (4.8) 49.0 (6.6) Pre-BD Post-BD Difference (95% CI) Pre-BD Post-BD Difference (95% CI) exercise time (sec) 212 (38) 319 (33) 107 (56 to 157) 524 (95) 354 (85) -171 (-280 to -62) FEV 1 (L) 1.06 (0.12) 1.27 (0.13) *** 0.21 (0.14 to 0.27) 1.30 (0.15) 1.42 (0.14) ** 0.12 (0.04 to 0.19) FEV 1 (%pred) 37.3 (4.4) 44.7 (4.9) *** 7.4 (4.8 to 10.0) 47.2 (5.2) 51.5 (5.1) ** 4.3 (1.5 to 7.2) FVC (L) 2.66 (0.16) 3.15 (0.17) *** 0.49 (0.27 to 0.71) 2.88 (0.41) 3.12 (0.37) 0.24 ( to 0.58) FVC (%pred) 72.1 (3.9) 85.7 (5.3) *** 13.7 (7.0 to 20.3) 79.3 (9.7) 86.2 (8.3) 6.8 (-2.4 to 16.0) FEV 1 / FVC (%) 39.4 (2.9) 40.3 (3.2) 0.9 (-2.0 to 3.8) 47.8 (5.4) 48.0 (5.0) 0.2 (-6.6 to 6.9) FEF 25% (L sec -1 ) 1.08 (0.29) 1.44 (0.39) ** 0.36 (0.13 to 0.60) 1.42 (0.26) 1.57 (0.22) 0.15 (-0.11 to 0.42) FEF 75% (L sec -1 ) 0.18 (0.02) 0.27 (0.35) ** 0.09 (0.03 to 0.15) 0.22 (0.03) 0.27 (0.06) 0.05 (-0.05 to 0.15) TLC (L) 8.17 (0.26) 8.05 (0.35) (-0.61 to 0.36) 7.27 (0.45) 6.24 (1.24) (-4.09 to 2.03) TLC (% pred) (3.3) (4.5) -2.2 (-9.6 to 5.3) (5.6) (5.1) 2.2 (-7.5 to 11.9) FRC (L) 6.27 (0.28) 5.98 (0.34) ** (-0.57 to -0.15) 5.04 (0.38) 4.91 (0.29) (-0.79 to 0.54) FRC (% pred) (6.6) (8.0) ** (-18.4 to -4.2) (10.4) (9.4) -2.3 (-25.3 to 20.6) RV (L) 5.20 (0.26) 4.74 (0.26) ** (-0.85 to -0.20) 4.01 (0.34) 4.13 (0.22) 0.12 (-0.75 to 1.00) RV (% pred) (12.7) (11.8) (-39.4 to -8.8) (18.7) (7.5) 6.5 (-34.7 to 47.7) IC (L) 1.91 (0.13) 2.23 (0.12) *** 0.42 (0.23 to 0.60) 2.23 (0.19) 2.45 (0.30) 0.22 (-0.12 to 0.57) IC (% pred) 63.7 (4.7) 77.1 (4.7) *** 13.4 (8.2 to 18.7) 76.2 (7.2) 89.6 (7.3) 9.7 (-6.1 to 25.4) V T (L) 0.81 (0.04) 0.91 (0.07) 0.10 (-0.01 to 0.21) 0.80 (0.14) 0.80 (0.14) 0.01 (-0.09 to 0.10) f R (breaths min -1 ) 21.8 (2.4) 23.7 (2.7) 1.9 (-2.4 to 6.1) 28.0 (4.5) 28.4 (3.8) 0.5 (-3.5 to 4.5) T I (sec) 1.21 (0.09) 1.22 (0.12) 0.01 (-0.16 to 0.19) 1.09 (0.10) 1.10 (0.07) 0.01 (-0.10 to 0.11) T E (sec) 2.04 (0.21) 2.01 (0.28) (-0.42 to 0.36) 1.88 (0.32) 1.78 (0.26) (-0.67 to 0.47) V T /T I (L sec -1 ) 0.69 (0.04) 0.77 (0.04) 0.07 (0.01 to 0.13) 0.74 (0.10) 0.74 (0.11) (-0.13 to 0.12) V T /T E (L sec -1 ) 0.43 (0.03) 0.49 (0.04) 0.07 (0.02 to 0.11) 0.44 (0.05) 0.46 (0.05) 0.02 (-0.08 to 0.11) Thorax: first published as /thx on 30 June Downloaded from on 19 November 2018 by guest. Protected by copyright.
15 Table 4 Ventilatory pattern and metabolic data in resting conditions and at end-exercise post-placebo and port-bronchodilator (BD) treatment by salbutamol divided in improvers and nonimprovers. Values are expressed as means (SD). **: p<0.01 (BD vs placebo) : p<0.05 (Improvers vs Nonimprovers) Improvers group Nonimprovers group Placebo BD Placebo BD REST V E (L min -1 ) 15.6 (0.8) 16.4 (1.9) 17.7 (1.1) 16.6 (2.2) V O 2 (L min -1 ) 0.39 (0.08) 0.35 (0.02) 0.35 (0.03) 0.29 (0.02) V CO 2 (L min -1 ) 0.28 (0.02) 0.30 (0.02) 0.30 (0.04) 0.25 (0.03) RER 0.84 (0.02) 0.86 (0.03) 0.84 (0.05) 0.85 (0.06) HR (beats min -1 ) 95.3 (4.1) 87.0 (2.0) 82.6 (6.1) 92.3 (3.9) V O 2 /HR (ml/beat) 3.5 (0.3) 4.1 (0.2) ( ) 4.0 (0.4) 3.2 (0.3) Breathlessness 0.9 (0.4) 1.2 (0.4) 0.5 (0.2) 0.8 (0.3) Leg effort 0.9 (0.3) 0.8 (0.3) 0.4 (0.2) 0.9 (0.5) EXERCISE V E (L min -1 ) 47.3 (2.9) 43.8 (3.7) 36.3 (3.4) 37.1 (3.1) V O 2 (L min -1 ) 0.94 (0.06) 0.99 (0.07) 0.92 (0.08) 0.86 (0.06) V CO 2 (L min -1 ) 0.90 (0.07) 0.96 (0.08) ( ) 0.82 (0.06) 0.82 (0.06) RER 0.95 (0.03) 0.97 (0.04) 0.90 (0.03) 0.95 (0.01) HR (beats min -1 ) (6.2) (6.3) (3.2) (3.3) V O 2 /HR (ml/beat) 8.4 (0.5) 8.7 (0.9) 9.4 (0.8) 7.6 (0.8)** Breathlessness 6.4 (0.5) 7.0 (0.6) 4.0 (0.6) 4.8 (0.7) Leg effort 6.0 (0.7) 6.5 (0.9) 4.0 (0.6) 5.0 (0.5) Thorax: first published as /thx on 30 June Downloaded from on 19 November 2018 by guest. Protected by copyright.
16
17
18
19
20
21
22
C hronic obstructive pulmonary disease (COPD) is characterised
 is characterised") 96 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Effect of salbutamol on lung function and chest wall volumes at rest and during exercise in COPD A Aliverti, K Rodger, R L Dellacà, N Stevenson, A Lo Mauro, A Pedotti,
96 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Effect of salbutamol on lung function and chest wall volumes at rest and during exercise in COPD A Aliverti, K Rodger, R L Dellacà, N Stevenson, A Lo Mauro, A Pedotti,
E xercise limitation is a major cause of disability in
 210 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Regional chest wall volumes during exercise in chronic obstructive pulmonary disease A Aliverti, N Stevenson, R L Dellacà, A Lo Mauro, A Pedotti, P M A Calverley...
210 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Regional chest wall volumes during exercise in chronic obstructive pulmonary disease A Aliverti, N Stevenson, R L Dellacà, A Lo Mauro, A Pedotti, P M A Calverley...
PARADOXICAL MOVEMENT OF THE LOWER RIB CAGE AT REST AND DURING EXERCISE IN COPD PATIENTS. Andre Luis Pereira Albuquerque 2,3 and Peter M.
 ERJ Express. Published on September 17, 2008 as doi: 10.1183/09031936.00141607 PARADOXICAL MOVEMENT OF THE LOWER RIB CAGE AT REST AND DURING EXERCISE IN COPD PATIENTS Andrea Aliverti 1, Marco Quaranta
ERJ Express. Published on September 17, 2008 as doi: 10.1183/09031936.00141607 PARADOXICAL MOVEMENT OF THE LOWER RIB CAGE AT REST AND DURING EXERCISE IN COPD PATIENTS Andrea Aliverti 1, Marco Quaranta
Increased difference between slow and forced vital capacity is associated with reduced exercise tolerance in COPD patients
 Yuan et al. BMC Pulmonary Medicine 2014, 14:16 RESEARCH ARTICLE Open Access Increased difference between slow and forced vital capacity is associated with reduced exercise tolerance in COPD patients Wei
Yuan et al. BMC Pulmonary Medicine 2014, 14:16 RESEARCH ARTICLE Open Access Increased difference between slow and forced vital capacity is associated with reduced exercise tolerance in COPD patients Wei
B reathlessness is the most disabling symptom associated
 8 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Effect of oxygen on recovery from maximal exercise in patients with chronic obstructive pulmonary disease N J Stevenson, P M A Calverley... See end of article for
8 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Effect of oxygen on recovery from maximal exercise in patients with chronic obstructive pulmonary disease N J Stevenson, P M A Calverley... See end of article for
In patients with symptomatic COPD, desirable. Assessment of Bronchodilator Efficacy in Symptomatic COPD* Is Spirometry Useful?
 Assessment of Bronchodilator Efficacy in Symptomatic COPD* Is Spirometry Useful? Denis E. O Donnell, MD, FCCP Bronchodilator therapy in COPD is deemed successful if it improves ventilatory mechanics to
Assessment of Bronchodilator Efficacy in Symptomatic COPD* Is Spirometry Useful? Denis E. O Donnell, MD, FCCP Bronchodilator therapy in COPD is deemed successful if it improves ventilatory mechanics to
Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology
 Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Optoelectronic plethysmography demonstrates abrogation of regional chest wall motion dysfunction in patients with pectus excavatum after Nuss repair
 Journal of Pediatric Surgery (2012) 47, 160 164 www.elsevier.com/locate/jpedsurg Optoelectronic plethysmography demonstrates abrogation of regional chest wall motion dysfunction in patients with pectus
Journal of Pediatric Surgery (2012) 47, 160 164 www.elsevier.com/locate/jpedsurg Optoelectronic plethysmography demonstrates abrogation of regional chest wall motion dysfunction in patients with pectus
Exercise limitation and the breathlessness. Exercise and dyspnoea in COPD. P.M.A. Calverley
 Eur Respir Rev 2006; 15: 100, 72 79 DOI: 10.1183/09059180.00010004 CopyrightßERSJ Ltd 2006 Exercise and dyspnoea in COPD P.M.A. Calverley ABSTRACT: Dyspnoea provoked either by exercise or during a disease
Eur Respir Rev 2006; 15: 100, 72 79 DOI: 10.1183/09059180.00010004 CopyrightßERSJ Ltd 2006 Exercise and dyspnoea in COPD P.M.A. Calverley ABSTRACT: Dyspnoea provoked either by exercise or during a disease
Study No.: Title: Rationale: Phase: Study Period Study Design: Centres: Indication: Treatment: Objectives : Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Content Indica c tion Lung v olumes e & Lung Indica c tions i n c paci c ties
 Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
H Wilkens, 1 B Weingard, 1 A Lo Mauro, 2 E Schena, 2 A Pedotti, 2 G W Sybrecht, 1 A Aliverti 2. Lung transplantation
 < Supplementary tables are published online only. To view these files please visit the journal online (http://thorax.bmj. com). 1 Innere Medizin V, Universitätsklinikum des Saarlandes, Homburg/Saar, Germany
< Supplementary tables are published online only. To view these files please visit the journal online (http://thorax.bmj. com). 1 Innere Medizin V, Universitätsklinikum des Saarlandes, Homburg/Saar, Germany
Diaphragm Activation during Exercise in Chronic Obstructive Pulmonary Disease
 Diaphragm Activation during Exercise in Chronic Obstructive Pulmonary Disease CHRISTER SINDERBY, JADRANKA SPAHIJA, JENNIFER BECK, DAREK KAMINSKI, SHENG YAN, NORMAN COMTOIS, and PAWEL SLIWINSKI Guy-Bernier
Diaphragm Activation during Exercise in Chronic Obstructive Pulmonary Disease CHRISTER SINDERBY, JADRANKA SPAHIJA, JENNIFER BECK, DAREK KAMINSKI, SHENG YAN, NORMAN COMTOIS, and PAWEL SLIWINSKI Guy-Bernier
Respiratory muscle dynamics and control during exercise with externally imposed expiratory flow limitation
 J Appl Physiol 92: 1953 1963, 2002. First published February 1, 2002; 10.1152/japplphysiol.01222.2000. Respiratory muscle dynamics and control during exercise with externally imposed expiratory flow limitation
J Appl Physiol 92: 1953 1963, 2002. First published February 1, 2002; 10.1152/japplphysiol.01222.2000. Respiratory muscle dynamics and control during exercise with externally imposed expiratory flow limitation
PULMONARY FUNCTION TESTING. Purposes of Pulmonary Tests. General Categories of Lung Diseases. Types of PF Tests
 PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
TORCH: Salmeterol and Fluticasone Propionate and Survival in COPD
 TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
TORCH: and Propionate and Survival in COPD April 19, 2007 Justin Lee Pharmacy Resident University Health Network Outline Overview of COPD Pathophysiology Pharmacological Treatment Overview of the TORCH
André Luis Pereira de Albuquerque 1, Marco Quaranta 2, Biswajit Chakrabarti 3, Andrea Aliverti 2, Peter M. Calverley 3
 http://dx.doi.org/10.1590/s1806-37562015000000078 ORIGINAL ARTICLE Exercise performance and differences in physiological response to pulmonary rehabilitation in severe chronic obstructive pulmonary disease
http://dx.doi.org/10.1590/s1806-37562015000000078 ORIGINAL ARTICLE Exercise performance and differences in physiological response to pulmonary rehabilitation in severe chronic obstructive pulmonary disease
Spirometry: an essential clinical measurement
 Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
DOI: /chest This information is current as of February 6, 2006
 Arm Exercise and Hyperinflation in Patients With COPD: Effect of Arm Training Francesco Gigliotti, Claudia Coli, Roberto Bianchi, Michela Grazzini, Loredana Stendardi, Carla Castellani and Giorgio Scano
Arm Exercise and Hyperinflation in Patients With COPD: Effect of Arm Training Francesco Gigliotti, Claudia Coli, Roberto Bianchi, Michela Grazzini, Loredana Stendardi, Carla Castellani and Giorgio Scano
PFT Interpretation and Reference Values
 PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
Spirometric Correlates of Improvement in Exercise Performance after Anticholinergic Therapy in Chronic Obstructive Pulmonary Disease
 Spirometric Correlates of Improvement in Exercise Performance after Anticholinergic Therapy in Chronic Obstructive Pulmonary Disease DENIS E. O DONNELL, MIU LAM, and KATHERINE A. WEBB Respiratory Investigation
Spirometric Correlates of Improvement in Exercise Performance after Anticholinergic Therapy in Chronic Obstructive Pulmonary Disease DENIS E. O DONNELL, MIU LAM, and KATHERINE A. WEBB Respiratory Investigation
6- Lung Volumes and Pulmonary Function Tests
 6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
Farmaci inalatori e dispnea nell asma e nella BPCO. Federico Lavorini
 Farmaci inalatori e dispnea nell asma e nella BPCO Federico Lavorini Dept. Experimental and Clinical Medicine Careggi University Hospital Florence - Italy Presenter Disclosures F.L. has received in the
Farmaci inalatori e dispnea nell asma e nella BPCO Federico Lavorini Dept. Experimental and Clinical Medicine Careggi University Hospital Florence - Italy Presenter Disclosures F.L. has received in the
Treatment. Assessing the outcome of interventions Traditionally, the effects of interventions have been assessed by measuring changes in the FEV 1
 58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
Modulation of operational lung volumes with the use of salbutamol in COPD patients accomplishing upper limbs exercise tests
 Respiratory Medicine (2009) 103, 251e257 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed Modulation of operational lung volumes with the use of salbutamol in COPD patients
Respiratory Medicine (2009) 103, 251e257 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed Modulation of operational lung volumes with the use of salbutamol in COPD patients
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
Diagnostic value of post-bronchodilator pulmonary function testing to distinguish between stable, moderate to severe COPD and asthma
 ORIGINAL RESEARCH Diagnostic value of post-bronchodilator pulmonary function testing to distinguish between stable, moderate to severe COPD and asthma Daphne C Richter 1 James R Joubert 1 Haylene Nell
ORIGINAL RESEARCH Diagnostic value of post-bronchodilator pulmonary function testing to distinguish between stable, moderate to severe COPD and asthma Daphne C Richter 1 James R Joubert 1 Haylene Nell
Difference Between The Slow Vital Capacity And Forced Vital Capacity: Predictor Of Hyperinflation In Patients With Airflow Obstruction
 ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 4 Number 2 Difference Between The Slow Vital Capacity And Forced Vital Capacity: Predictor Of Hyperinflation In Patients With Airflow Obstruction
ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 4 Number 2 Difference Between The Slow Vital Capacity And Forced Vital Capacity: Predictor Of Hyperinflation In Patients With Airflow Obstruction
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Spirometry: FEVER DISEASE DIABETES HOW RELIABLE IS THIS? 9/2/2010 BUT WHAT WE PRACTICE: Spirometers are objective tools
 SPIROMETRY PRINCIPLES, PROCEDURE AND QA Spirometry: Dr. Rahul Kodgule CHEST RESEARCH FOUNDATION, PUNE FEVER ISCHAEMIC HEART DISEASE DIABETES BUT WHAT WE PRACTICE: Spirometers are objective tools to diagnose
SPIROMETRY PRINCIPLES, PROCEDURE AND QA Spirometry: Dr. Rahul Kodgule CHEST RESEARCH FOUNDATION, PUNE FEVER ISCHAEMIC HEART DISEASE DIABETES BUT WHAT WE PRACTICE: Spirometers are objective tools to diagnose
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
S P I R O M E T R Y. Objectives. Objectives 3/12/2018
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
Accurately Measuring Airway Resistance in the PFT Lab
 Accurately Measuring Airway Resistance in the PFT Lab Angela Lorenzo, MS, RRT, RPFT Adjunct Faculty, Long Island University Respiratory Care Division Disclaimer The views in this lecture are those of the
Accurately Measuring Airway Resistance in the PFT Lab Angela Lorenzo, MS, RRT, RPFT Adjunct Faculty, Long Island University Respiratory Care Division Disclaimer The views in this lecture are those of the
COMPREHENSIVE RESPIROMETRY
 INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
Pulmonary Function Testing
 In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
PULMONARY FUNCTION TESTS
 Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Impacting patient-centred outcomes in COPD: breathlessness and exercise tolerance
 Eur Respir Rev 2006; 15: 99, 37 41 DOI: 10.1183/09059180.00009903 CopyrightßERSJ Ltd 2006 Impacting patient-centred outcomes in COPD: breathlessness and exercise tolerance D.E. O Donnell ABSTRACT: The
Eur Respir Rev 2006; 15: 99, 37 41 DOI: 10.1183/09059180.00009903 CopyrightßERSJ Ltd 2006 Impacting patient-centred outcomes in COPD: breathlessness and exercise tolerance D.E. O Donnell ABSTRACT: The
DECLINE OF RESTING INSPIRATORY CAPACITY IN COPD: THE IMPACT ON BREATHING PATTERN, DYSPNEA AND VENTILATORY CAPACITY DURING EXERCISE
 Page 1 of 29 Body of text word count: 2,836 Abstract word count: 250 DECLINE OF RESTING INSPIRATORY CAPACITY IN COPD: THE IMPACT ON BREATHING PATTERN, DYSPNEA AND VENTILATORY CAPACITY DURING EXERCISE Authors:
Page 1 of 29 Body of text word count: 2,836 Abstract word count: 250 DECLINE OF RESTING INSPIRATORY CAPACITY IN COPD: THE IMPACT ON BREATHING PATTERN, DYSPNEA AND VENTILATORY CAPACITY DURING EXERCISE Authors:
Bronchodilator responsiveness in patients with COPD
 Eur Respir J 28; 31: 742 75 DOI: 1.1183/931936.12967 CopyrightßERS Journals Ltd 28 Bronchodilator responsiveness in patients with COPD D.P. Tashkin*, B. Celli #, M. Decramer ", D. Liu +, D. Burkhart +,
Eur Respir J 28; 31: 742 75 DOI: 1.1183/931936.12967 CopyrightßERS Journals Ltd 28 Bronchodilator responsiveness in patients with COPD D.P. Tashkin*, B. Celli #, M. Decramer ", D. Liu +, D. Burkhart +,
Ventilatory functions response to breathing training versus aerobic training in asthmatic children
 Egypt J Pediatr Allergy Immunol 2012;10(1):33-37. Original article Ventilatory functions response to breathing training versus aerobic training in asthmatic children Background: There is worldwide public
Egypt J Pediatr Allergy Immunol 2012;10(1):33-37. Original article Ventilatory functions response to breathing training versus aerobic training in asthmatic children Background: There is worldwide public
Coexistence of confirmed obstruction in spirometry and restriction in body plethysmography, e.g.: COPD + pulmonary fibrosis
 Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
SPIROMETRY. Marijke Currie (CRFS) Care Medical Ltd Phone: Copyright CARE Medical ltd
 Care Medical Ltd Phone: Copyright CARE Medical ltd") SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
Spirometry. Obstruction. By Helen Grim M.S. RRT. loop will have concave appearance. Flows decreased consistent with degree of obstruction.
 1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
Author's response to reviews
 Author's response to reviews Title:Aclidinium improves exercise endurance, dyspnea, lung hyperinflation, and physical activity in patients with COPD: a randomized, placebo-controlled, crossover trial Authors:
Author's response to reviews Title:Aclidinium improves exercise endurance, dyspnea, lung hyperinflation, and physical activity in patients with COPD: a randomized, placebo-controlled, crossover trial Authors:
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C
 MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Breathing and pulmonary function
 EXPERIMENTAL PHYSIOLOGY EXPERIMENT 5 Breathing and pulmonary function Ying-ying Chen, PhD Dept. of Physiology, Zhejiang University School of Medicine bchenyy@zju.edu.cn Breathing Exercise 1: Tests of pulmonary
EXPERIMENTAL PHYSIOLOGY EXPERIMENT 5 Breathing and pulmonary function Ying-ying Chen, PhD Dept. of Physiology, Zhejiang University School of Medicine bchenyy@zju.edu.cn Breathing Exercise 1: Tests of pulmonary
SPIROMETRY METHOD. COR-MAN IN / EN Issue A, Rev INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark
 SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
Postural and Musculoskeletal Impairments Contributing to Increased Work of Breathing
 Postural and Musculoskeletal Impairments Contributing to Increased Work of Breathing Jordon Metcalf, Tiffany Sheffield, Katherine Sullivan, Ashley Williams Objectives Review the normal mechanics of breathing
Postural and Musculoskeletal Impairments Contributing to Increased Work of Breathing Jordon Metcalf, Tiffany Sheffield, Katherine Sullivan, Ashley Williams Objectives Review the normal mechanics of breathing
Effect of Pulmonary Rehabilitation on Quadriceps Fatiguability during Exercise
 Effect of Pulmonary Rehabilitation on Quadriceps Fatiguability during Exercise M. JEFFERY MADOR, THOMAS J. KUFEL, LILIBETH A. PINEDA, ANN STEINWALD, AJAY AGGARWAL, AMITA M. UPADHYAY, and MOHAMMED A. KHAN
Effect of Pulmonary Rehabilitation on Quadriceps Fatiguability during Exercise M. JEFFERY MADOR, THOMAS J. KUFEL, LILIBETH A. PINEDA, ANN STEINWALD, AJAY AGGARWAL, AMITA M. UPADHYAY, and MOHAMMED A. KHAN
aclidinium 322 micrograms inhalation powder (Eklira Genuair ) SMC No. (810/12) Almirall S.A.
 SMC No. (810/12) Almirall S.A.") aclidinium 322 micrograms inhalation powder (Eklira Genuair ) SMC No. (810/12) Almirall S.A. 05 October 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and
aclidinium 322 micrograms inhalation powder (Eklira Genuair ) SMC No. (810/12) Almirall S.A. 05 October 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and
Evaluation of acute bronchodilator reversibility in patients with symptoms of GOLD stage I COPD
 c Additional Methods data are published online only at http:// thorax.bmj.com/content/vol64/ issue3 1 Respiratory Investigation Unit, Department of Medicine, Queen s University and Kingston General Hospital,
c Additional Methods data are published online only at http:// thorax.bmj.com/content/vol64/ issue3 1 Respiratory Investigation Unit, Department of Medicine, Queen s University and Kingston General Hospital,
Short burst oxygen therapy after activities of daily living in the home in chronic obstructive pulmonary disease
 Thorax Online First, published on February 20, 2007 as 10.1136/thx.2006.063636 Short burst oxygen therapy after activities of daily living in the home in chronic obstructive pulmonary disease S J Quantrill,
Thorax Online First, published on February 20, 2007 as 10.1136/thx.2006.063636 Short burst oxygen therapy after activities of daily living in the home in chronic obstructive pulmonary disease S J Quantrill,
Pulmonary Function Testing. Ramez Sunna MD, FCCP
 Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation. Susan Blonshine RRT, RPFT, AE-C, FAARC
 Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
COPD is a progressive disorder leading to increasing
 Improvement in Exercise Tolerance With the Combination of Tiotropium and Pulmonary Rehabilitation in Patients With COPD* Richard Casaburi, MD, PhD, FCCP; David Kukafka, MD, FCCP; Christopher B. Cooper,
Improvement in Exercise Tolerance With the Combination of Tiotropium and Pulmonary Rehabilitation in Patients With COPD* Richard Casaburi, MD, PhD, FCCP; David Kukafka, MD, FCCP; Christopher B. Cooper,
Lung mechanics in subjects showing increased residual volume without bronchial obstruction
 Lung mechanics in subjects showing increased residual volume without bronchial obstruction S VULTERINI, M R BIANCO, L PELLICCIOTTI, AND A M SIDOTI From the Divisione di Medicina Generale, Ospedale Fatebenefratelli,
Lung mechanics in subjects showing increased residual volume without bronchial obstruction S VULTERINI, M R BIANCO, L PELLICCIOTTI, AND A M SIDOTI From the Divisione di Medicina Generale, Ospedale Fatebenefratelli,
roflumilast 500 microgram tablets (Daxas ) SMC No. (635/10) Nycomed Ltd
 SMC No. (635/10) Nycomed Ltd") roflumilast 500 microgram tablets (Daxas ) SMC No. (635/10) Nycomed Ltd 06 August 2010 (Issued 10 September 2010) The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
roflumilast 500 microgram tablets (Daxas ) SMC No. (635/10) Nycomed Ltd 06 August 2010 (Issued 10 September 2010) The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Repeated abdominal exercise induces respiratory muscle fatigue
 Journal of Sports Science and Medicine (2009) 8, 543-547 http://www.jssm.org Research article Repeated abdominal exercise induces respiratory muscle fatigue Christopher L. Gomez, Lisa M. Strongoli and
Journal of Sports Science and Medicine (2009) 8, 543-547 http://www.jssm.org Research article Repeated abdominal exercise induces respiratory muscle fatigue Christopher L. Gomez, Lisa M. Strongoli and
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Supramaximal flow in asthmatic patients
 Eur Respir J ; 19: 13 17 DOI: 1.113/93193..51 Printed in UK all rights reserved Copyright #ERS Journals Ltd European Respiratory Journal ISSN 93-193 Supramaximal flow in asthmatic patients H. Sala*, A.
Eur Respir J ; 19: 13 17 DOI: 1.113/93193..51 Printed in UK all rights reserved Copyright #ERS Journals Ltd European Respiratory Journal ISSN 93-193 Supramaximal flow in asthmatic patients H. Sala*, A.
C hronic obstructive pulmonary disease (COPD) is a
 is a") 288 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Altered thoracic gas compression contributes to improvement in spirometry with lung volume reduction surgery A Sharafkhaneh, S Goodnight-White, T M Officer, J
288 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Altered thoracic gas compression contributes to improvement in spirometry with lung volume reduction surgery A Sharafkhaneh, S Goodnight-White, T M Officer, J
Effect of N-Acetylcysteine on Air Trapping in COPD. A Randomized Placebo-Controlled Study
 CHEST Effect of N-Acetylcysteine on Air Trapping in COPD A Randomized Placebo-Controlled Study David Stav, MD; and Meir Raz, MD Original Research COPD Background: FEV 1 is used for the classification of
CHEST Effect of N-Acetylcysteine on Air Trapping in COPD A Randomized Placebo-Controlled Study David Stav, MD; and Meir Raz, MD Original Research COPD Background: FEV 1 is used for the classification of
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
Effects of a multidisciplinary body weight reduction program on static and dynamic thoraco-abdominal volumes in obese adolescents
 Applied Physiology, Nutrition, and Metabolism Effects of a multidisciplinary body weight reduction program on static and dynamic thoraco-abdominal volumes in obese adolescents Journal: Applied Physiology,
Applied Physiology, Nutrition, and Metabolism Effects of a multidisciplinary body weight reduction program on static and dynamic thoraco-abdominal volumes in obese adolescents Journal: Applied Physiology,
Aclidinium Bromide: Clinical Benefit in Patients with Moderate to Severe COPD
 Send Orders of Reprints at bspsaif@emirates.net.ae 150 The Open Respiratory Medicine Journal, 2012, 6, 150-154 Aclidinium Bromide: Clinical Benefit in Patients with Moderate to Severe COPD Charlotte Suppli
Send Orders of Reprints at bspsaif@emirates.net.ae 150 The Open Respiratory Medicine Journal, 2012, 6, 150-154 Aclidinium Bromide: Clinical Benefit in Patients with Moderate to Severe COPD Charlotte Suppli
Spirometry: Introduction
 Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
S P I R O M E T R Y. Objectives. Objectives 2/5/2019
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
Cardiopulmonary Exercise Testing Cases
 Canadian Respiratory Conference - 217 Cardiopulmonary Exercise Testing Cases Darcy D Marciniuk, MD FRCPC FCCP Associate Vice-President Research, University of Saskatchewan Professor, Respirology, Critical
Canadian Respiratory Conference - 217 Cardiopulmonary Exercise Testing Cases Darcy D Marciniuk, MD FRCPC FCCP Associate Vice-President Research, University of Saskatchewan Professor, Respirology, Critical
Performing a Methacholine Challenge Test
 powder for solution, for inhalation Performing a Methacholine Challenge Test Provocholine is a registered trademark of Methapharm Inc. Copyright Methapharm Inc. 2016. All rights reserved. Healthcare professionals
powder for solution, for inhalation Performing a Methacholine Challenge Test Provocholine is a registered trademark of Methapharm Inc. Copyright Methapharm Inc. 2016. All rights reserved. Healthcare professionals
H ospitalisation due to an exacerbation of chronic
 713 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Intravenous aminophylline in patients admitted to hospital with non-acidotic exacerbations of chronic obstructive pulmonary disease: a prospective randomised controlled
713 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Intravenous aminophylline in patients admitted to hospital with non-acidotic exacerbations of chronic obstructive pulmonary disease: a prospective randomised controlled
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE
 The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
EVect of breathing circuit resistance on the measurement of ventilatory function
 9 Department of Respiratory Medicine, The Alfred Hospital and Monash University Medical School, Melbourne, Victoria, Australia 311 D P Johns C M Ingram S Khov P D Rochford E H Walters Correspondence to:
9 Department of Respiratory Medicine, The Alfred Hospital and Monash University Medical School, Melbourne, Victoria, Australia 311 D P Johns C M Ingram S Khov P D Rochford E H Walters Correspondence to:
B ronchodilators are the mainstay of treatment in chronic
 471 RESPIRATORY MUSCLES Effect of salmeterol on respiratory muscle activity during exercise in poorly reversible COPD W D C Man, N Mustfa, D Nikoletou, S Kaul, N Hart, G F Rafferty, N Donaldson, M I Polkey,
471 RESPIRATORY MUSCLES Effect of salmeterol on respiratory muscle activity during exercise in poorly reversible COPD W D C Man, N Mustfa, D Nikoletou, S Kaul, N Hart, G F Rafferty, N Donaldson, M I Polkey,
Minimal important difference of the transition dyspnoea index in a multinational clinical trial
 Eur Respir J 2003; 21: 267 272 DOI: 10.1183/09031936.03.00068503a Printed in UK all rights reserved Copyright #ERS Journals Ltd 2003 European Respiratory Journal ISSN 0903-1936 Minimal important difference
Eur Respir J 2003; 21: 267 272 DOI: 10.1183/09031936.03.00068503a Printed in UK all rights reserved Copyright #ERS Journals Ltd 2003 European Respiratory Journal ISSN 0903-1936 Minimal important difference
PULMONARY FUNCTION. VOLUMES AND CAPACITIES
 PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น
 รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
umeclidinium, 55 micrograms, powder for inhalation (Incruse ) SMC No. (1004/14) GlaxoSmithKline
 SMC No. (1004/14) GlaxoSmithKline") umeclidinium, 55 micrograms, powder for inhalation (Incruse ) SMC No. (1004/14) GlaxoSmithKline 07 November 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
umeclidinium, 55 micrograms, powder for inhalation (Incruse ) SMC No. (1004/14) GlaxoSmithKline 07 November 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Physiological Effects of Roflumilast at Rest and during Exercise in COPD
 ERJ Express. Published on September 29, 2011 as doi: 10.1183/09031936.00096511 Physiological Effects of Roflumilast at Rest and during Exercise in COPD Authors: Denis E. O Donnell 1, MD; Dirk Bredenbröker
ERJ Express. Published on September 29, 2011 as doi: 10.1183/09031936.00096511 Physiological Effects of Roflumilast at Rest and during Exercise in COPD Authors: Denis E. O Donnell 1, MD; Dirk Bredenbröker
Effect of bronchoscopic lung volume reduction on dynamic hyperinflation and
 Effect of bronchoscopic lung volume reduction on dynamic hyperinflation and exercise in emphysema Nicholas S Hopkinson, Tudor P Toma, David M Hansell, Peter Goldstraw, John Moxham, Duncan M Geddes & Michael
Effect of bronchoscopic lung volume reduction on dynamic hyperinflation and exercise in emphysema Nicholas S Hopkinson, Tudor P Toma, David M Hansell, Peter Goldstraw, John Moxham, Duncan M Geddes & Michael
COPD Manual Diaphragm Manipulation
 COPD Manual Diaphragm Manipulation Journal of Physiotherapy 61 (2015) 182 189 Journal of PHYSIOTHERAPY journal homepage: www.elsevier.com/locate/jphys Research The Manual Diaphragm Release Technique improves
COPD Manual Diaphragm Manipulation Journal of Physiotherapy 61 (2015) 182 189 Journal of PHYSIOTHERAPY journal homepage: www.elsevier.com/locate/jphys Research The Manual Diaphragm Release Technique improves
Respiro: le nuove tecnologie
 Dipartimento di Elettronica, Informazione e Bioingegneria Respiro: le nuove tecnologie Andrea Aliverti Respiratory function Total ventilation (O 2 consumption) alveolar ventilation diffusion/gas exchange
Dipartimento di Elettronica, Informazione e Bioingegneria Respiro: le nuove tecnologie Andrea Aliverti Respiratory function Total ventilation (O 2 consumption) alveolar ventilation diffusion/gas exchange
Basic approach to PFT interpretation. Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic
 Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
A comparison of global questions versus health status questionnaires as measures of the severity and impact of asthma
 Eur Respir J 1999; 1: 591±596 Printed in UK ± all rights reserved Copyright #ERS Journals Ltd 1999 European Respiratory Journal ISSN 93-1936 A comparison of global questions versus health status questionnaires
Eur Respir J 1999; 1: 591±596 Printed in UK ± all rights reserved Copyright #ERS Journals Ltd 1999 European Respiratory Journal ISSN 93-1936 A comparison of global questions versus health status questionnaires
Comparison of the effects of nebulised and inhaled salbutamol on breathlessness in severe COPD
 Respiratory Medicine (2005) 99, 372 376 Comparison of the effects of nebulised and inhaled salbutamol on breathlessness in severe COPD P.J. Poole, R. Saini, S.M. Brodie, P.N. Black Department of Medicine,
Respiratory Medicine (2005) 99, 372 376 Comparison of the effects of nebulised and inhaled salbutamol on breathlessness in severe COPD P.J. Poole, R. Saini, S.M. Brodie, P.N. Black Department of Medicine,
Effect of tiotropium bromide on the cardiovascular response to exercise in COPD
 Respiratory Medicine (27) 11, 217 224 Effect of tiotropium bromide on the cardiovascular response to exercise in COPD J. Travers a, P. Laveneziana a, K.A. Webb a, S. Kesten b, D.E. O Donnell a, a Respiratory
Respiratory Medicine (27) 11, 217 224 Effect of tiotropium bromide on the cardiovascular response to exercise in COPD J. Travers a, P. Laveneziana a, K.A. Webb a, S. Kesten b, D.E. O Donnell a, a Respiratory
GE Healthcare. Non Invasive Ventilation (NIV) For the Engström Ventilator. Relief, Relax, Recovery
 For the Engström Ventilator. Relief, Relax, Recovery") GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects
 Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Effect of salbutamol on dynamic hyperinflation in chronic obstructive pulmonary disease patients
 Eur Respir J 1998; 12: 799 84 DOI: 1.1183/931936.98.124799 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1998 European Respiratory Journal ISSN 93-1936 Effect of salbutamol on dynamic
Eur Respir J 1998; 12: 799 84 DOI: 1.1183/931936.98.124799 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1998 European Respiratory Journal ISSN 93-1936 Effect of salbutamol on dynamic
Key words: computer administration; continuous method for rating breathlessness; exercise testing
 Comparison of Continuous and Discrete Measurements of Dyspnea During Exercise in Patients With COPD and Normal Subjects* Gustavo Fierro-Carrion, MD; Donald A. Mahler, MD, FCCP; Joseph Ward, RCPT; and John
Comparison of Continuous and Discrete Measurements of Dyspnea During Exercise in Patients With COPD and Normal Subjects* Gustavo Fierro-Carrion, MD; Donald A. Mahler, MD, FCCP; Joseph Ward, RCPT; and John
European Respiratory & Pulmonary Diseases. Satellite Symposium Proceedings
 Satellite Symposium Proceedings Non-invasive Screening of Expiratory Flow Limitation in Chronic Obstructive Pulmonary Disease Proceedings of a Philips Respironics sponsored satellite symposium held during
Satellite Symposium Proceedings Non-invasive Screening of Expiratory Flow Limitation in Chronic Obstructive Pulmonary Disease Proceedings of a Philips Respironics sponsored satellite symposium held during
PULMONARY FUNCTION TESTING. By: Gh. Pouryaghoub. MD Center for Research on Occupational Diseases (CROD) Tehran University of Medical Sciences (TUMS)
 Tehran University of Medical Sciences (TUMS)") PULMONARY FUNCTION TESTING By: Gh. Pouryaghoub. MD Center for Research on Occupational Diseases (CROD) Tehran University of Medical Sciences (TUMS) PULMONARY FUNCTION TESTS CATEGORIES Spirometry Lung volumes
PULMONARY FUNCTION TESTING By: Gh. Pouryaghoub. MD Center for Research on Occupational Diseases (CROD) Tehran University of Medical Sciences (TUMS) PULMONARY FUNCTION TESTS CATEGORIES Spirometry Lung volumes
Workshop: Pulmonary rehabilitation and NIV
 Workshop: Pulmonary rehabilitation and NIV Jean-Christian Borel INSERM U 1042, HP2 Laboratory, Université Joseph Fourier, Faculté de Médecine, Grenoble, France, AGIRadom, Research and Development department,
Workshop: Pulmonary rehabilitation and NIV Jean-Christian Borel INSERM U 1042, HP2 Laboratory, Université Joseph Fourier, Faculté de Médecine, Grenoble, France, AGIRadom, Research and Development department,
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially