Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects
|
|
|
- Meghan Singleton
- 6 years ago
- Views:
Transcription

1 Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC
2 Benefits and Limitations of Pulmonary Function Testing Benefits Useful for diagnosing cause of unexplained respiratory symptoms and monitoring patients with known disease Can be used to identify the pattern and severity of an abnormality Limitations Generally cannot distinguish among the potential causes of the abnormalities when used alone Must be interpreted within the context of a proper history, physical examination, and ancillary diagnostic tests
3 Indications for Pulmonary Function Testing Evaluate symptoms and signs of lung disease (eg, cough, dyspnea, cyanosis, wheezing, hyperinflation, hypoxemia, hypercapnia) Assess the progression of lung disease Monitor effectiveness of therapy Evaluate preoperative patients in selected situations Screen at risk individuals for pulmonary disease such as smokers or people with occupational exposure to toxic substances Monitor for potentially toxic effects of certain drugs or chemicals (eg, amiodarone, beryllium)
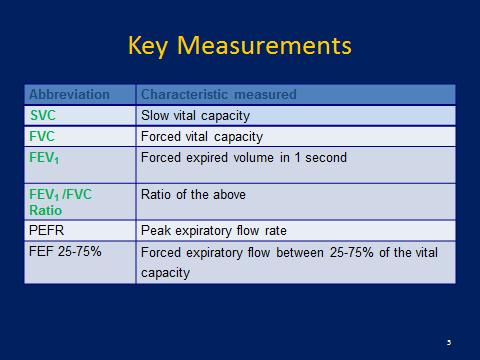
 Slow vital capacity Maximal inhalation or exhalation followed by maximal inhalation/exhalation without regard to time FVC Maximal inhalation followed by maximal exhalation as long and")
 Measures ability")
 and conditions that alter permeability or increase membrane thickness (pulmonary fibrosis) Residual Volume, Total Lung Capacity Must be measured indirectly")
4 Components of Pulmonary Function Tests Spirometry Measures volume and speed of air movement in and out of lungs during various respiratory maneuvers The four most important respiratory parameters are: VC (SVC) Slow vital capacity Maximal inhalation or exhalation followed by maximal inhalation/exhalation without regard to time FVC Maximal inhalation followed by maximal exhalation as long and forcefully as possible FEV1 Amount of air exhaled during the first second of the FVC maneuver. Tends to be lower in obstructive diseases such as asthma and emphysema FEV1/FVC ratio Used to determine if the pattern is obstructive, restrictive or normal Diffusing Capacity (DLCO) Measures ability of lung to transfer gas Decreased in conditions that minimize the ability of blood to accept and bind the gas that is diffusing (anemia), conditions that decrease surface area of alveolar-capillary membrane (emphysema, pulmonary embolism) and conditions that alter permeability or increase membrane thickness (pulmonary fibrosis) Residual Volume, Total Lung Capacity Must be measured indirectly (inert gas, plethysmography) Can demonstrate air trapping and hyperinflation in obstructive diseases and confirm true restriction
5
6 Factors to Confirm Before Interpreting PFTs 1. The volume-time curve reaches a plateau, and expiration lasts at least six seconds V o l u m e L Time (seconds
7 Factors to Confirm Before Interpreting PFTs 2. Results of the 2 best efforts on the FVC are within 0.2 L. of each other

8 Factors to Confirm Before Interpreting PFTs 3. The flow-volume loops are free of artifacts and abnormalities If the patient s efforts yield flattened flow-volume loops, submaximal effort is most likely; however, central or upper airway obstruction should be considered.
9 Step 1: Determine If the FEV1/FVC Ratio Is Low Low FEV1/FVC Ratio indicates an obstructive defect Two options: Follow GOLD Criteria Uses a cutoff of less than 70% For patients five to 18 years of age, the National Asthma Education and Prevention Program guideline says that a ratio of less than 85% is consistent with an obstructive defect as long as the patient has symptoms consistent with obstructive lung disease. Follow the ATS criteria, which use the lower limit of normal (LLN) as the cutoff for adults. The LLN is a measurement less than the fifth percentile of spirometry data obtained from the Third National Health and Nutrition Examination Survey (NHANES III).
10 Defining Normal - Lower Limit of Normal (LLN) Obtained by analyzing some measure (FVC, FEV1, etc.) in healthy subjects, then determining the variability of that measurement. 5 th percentile is often defined as the lower limit of normal in clinical medicine because it represents the segment of normal subjects farthest below the average
11 Defining Normal Fixed Percentage Uses the measured value divided by the reference value X % is often used as the limit of normal This method leads to errors because the variability around the predicted value is relatively constant in adults (scatter of normal values does not vary with the size of the predicted value
12 GOLD VS. ATS Criteria Eur Respir J 2005; 26: DOI: / Copyright ERS Journals Ltd 2005 SERIES ATS/ERS TASK FORCE: STANDARDISATION OF LUNG FUNCTION TESTING Edited by V. Brusasco, R. Crapo and G. Viegi Number 5 in this Series Interpretative strategies for lung function tests R. Pellegrino, G. Viegi, V. Brusasco, R.O. Crapo, F. Burgos, R. Casaburi, A. Coates, C.P.M. van der Grinten, P. Gustafsson, J. Hankinson, R. Jensen, D.C. Johnson, N. MacIntyre, R. McKay, M.R. Miller, D. Navajas, O.F. Pedersen and J. Wanger
13
14 GOLD VS. ATS CRITERIA A large cohort study found that using the GOLD criteria (FEV 1 /FVC less than 70%) for diagnosis of chronic obstructive pulmonary disease (COPD) in U.S. adults 65 years and older was more sensitive for COPD-related obstructive lung disease than using the ATS criteria (FEV 1 /FVC less than the LLN). Adults who met the GOLD criteria but not the ATS criteria (FEV 1 /FVC less than 70% but greater than the LLN) had greater risk of COPD-related hospitalization (hazard ratio = 2.6; 95% confidence interval, 2.0 to 3.3) and mortality (hazard ratio = 1.3; 95% confidence interval, 1.1 to 1.5). Another cohort study looking at adults 65 years and older found that, compared with the ATS criteria, the GOLD criteria had higher clinical agreement with an expert panel diagnosis for COPD and better identified patients with clinically relevant events (e.g., COPD exacerbation, hospitalization, mortality). Until better criteria for the diagnosis of COPD are found, physicians should use the GOLD criteria to diagnose obstructive lung disease in patients 65 years and older with respiratory symptoms who are at risk of COPD (i.e., current or previous smoker). Other studies have found that using the GOLD criteria can miss up to 50% of young adults with obstructive lung disease and leads to overdiagnosis in healthy non-smokers. Based on these studies, physicians should use the ATS criteria to diagnose obstructive lung disease in patients younger than 65 years regardless of smoking status, and in nonsmokers who are 65 years and older.
15 Summary of the usage of reference values Item Reference values General Predicted values should be obtained from studies of normal or healthy subjects with the same anthropometric (e.g. sex, age and height) and ethnic characteristics of the patient being tested. Height and weight should be measured for each patient at the time of testing If possible, all parameters should be taken from the same reference source When comparing selected reference equations with measurements performed on a sample of healthy subjects in a laboratory, it is suggested to choose the reference equation that provides the sum of residuals (observed predicted computed for each adult subject, or log observed log predicted for each subject in the paediatric age range) closest to zero When using a set of reference equations, extrapolation beyond the size and age of the investigated subjects should be avoided For each lung function index, values below the 5th percentile of the frequency distribution of values measured in the reference population are considered to be below the expected normal range Spirometry In the USA, ethnically appropriate NHANES III reference equations published in 1999 for those aged 8 80 yrs, and the equations of WANG et al. [29] for children aged 8 yrs are recommended In Europe, the ECCS combined reference equations published in 1993 [8] are often used for yr-old people, and those from QUANJER et al. [30] for paediatric ages. Currently, a specific set of equations is not recommendable for use in Europe. A new Europe-wide study to derive updated reference equations for lung function is needed Table 1 includes reference equations published from 1995 to August 2004 Lung volumes No specific set of equations can be recommended In practice, many USA and European laboratories use the reference equations for TLC, FRC and RV recommended by the 1995 ATS/ERS workshop [7] or by the ECCS in 1993 [8] Diffusing capacity No specific set of equations is generally recommended Commonly used equations appear to be those by the ECCS in 1993 [38] and those of CRAPO and MORRIS [40]. In Europe, equations from COTES et al. [41], PAOLETTI et al. [42] and ROCA et al. [43] are also used
16 Step 2: Determine If the FVC Is Low An FVC less than the LLN for adults or less than 80% of predicted for those five to 18 years of age, indicates a restrictive pattern A restrictive pattern can indicate restrictive lung disease, a mixed pattern (if a patient has an obstructive defect and a restrictive pattern), or pure obstructive lung disease with air trapping
17 Pulmonary Function Test Interpretation Test results based on age Suggested diagnosis FVC FEV1/FVC ratio* 5 to 18 years: 80% 5 to 18 years: 85% Normal Adults: LLN Adults: LLN or 70% 5 to 18 years: 80% 5 to 18 years: < 85% Obstructive defect Adults: LLN Adults: < LLN or < 70% 5 to 18 years: < 80% 5 to 18 years: 85% Restrictive pattern Adults: < LLN Adults: LLN or 70% 5 to 18 years: < 80% 5 to 18 years: < 85% Adults: < LLN Adults: < LLN or < 70% Mixed pattern FEV1 = forced expiratory volume in one second; FVC = forced vital capacity; LLN = lower limit of normal (defined as below the fifth percentile of spirometry data obtained from the Third National Health and Nutrition Examination Survey). * The 70% criteria should be used only for patients 65 years and older who have respiratory symptoms and are at risk of chronic obstructive pulmonary disease (i.e., current or previous smoker)
18 Step 3: Confirm the Restrictive Pattern If the patient s initial PFT results indicate a restrictive pattern or a mixed pattern that is not corrected with bronchodilators, the patient should be referred for full PFTs with DLCO testing DLCO is a quantitative measurement of gas transfer in the lungs Diseases that decrease blood flow to the lungs or damage alveoli will cause less efficient gas exchange, resulting in a lower DLCO measurement
19 Step 4: Grade the Severity of the Abnormality If an obstructive defect, a restrictive pattern, or a mixed pattern is present, as defined by steps 1 and 2, the physician should grade the severity of the abnormality based on the FEV1 percentage of predicted
20 Table 3. American Thoracic Society Grades for Severity of a Pulmonary Function Test Abnormality Severity FEV1 percentage of predicted Mild > 70 Moderate 60 to 69 Moderately severe 50 to 59 Severe 35 to 49 Very severe < 35 FEV1 = forced expiratory volume in one second. Adapted with permission from Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005; 26(5):957.
21 Step 5: Determine Reversibility of the Obstructive Defect Is defect reversible based on the increase in FEV1 or FVC after administration of a bronchodilator Increase of more than12% in patients five to 18 years of age More than 12% and more than 200 ml in adults Obstructive defects in asthma are usually fully reversible, whereas defects in COPD are not fully reversible If PFTs show a mixed pattern, and FVC corrects to >80% patients five to 18 or to the LLN or more in adults, patient is likely to have pure obstructive lung disease with air trapping
22
23 Step 6: Bronchoprovication If PFT results are normal but exercise or allergeninduced asthma is suspected consider bronchoprovocation Methacholine (Positive response = Greater than 20% fall in FEV1 at or before administration of 4 mg per ml of inhaled methacholine) Mannitol Exercise testing Eucapnic voluntary hyperpnea If FEV1 is <70%, trial of a bronchodilator may be considered
24 Step 7: Establish the Differential Diagnosis Obstructive Disease Airflow limitation Increased lung volumes with air trapping Normal or increased compliance Restrictive Disease Reduced lung volumes Increase in overall stiffness of lungs (decreased compliance) Common Obstructive Lung Diseases Asthma Asthmatic bronchitis Chronic obstructive bronchitis Chronic obstructive pulmonary disease (includes asthma, asthmatic bronchitis, chronic bronchitis, emphysema, overlap syndrome) Common Restrictive Lung Diseases Beryllium disease Congestive heart failure Idiopathic pulmonary fibrosis Infectious inflammation (histoplasmosis, mycobacterium infection) Interstitial pneumonitis Neuromuscular diseases Sarcoidosis Thoracic deformities
25 Differential Diagnosis Based on DLCO Results DLCO results Differential diagnosis High DLCO Asthma, left-to-right intracardiac shunts, polycythemia, pulmonary hemorrhage Normal DLCO Kyphoscoliosis, morbid obesity, neuromuscular weakness, with restrictive pattern pleural effusion Normal DLCO with α1-antitrypsin deficiency, asthma, bronchiectasis, chronic obstructive component bronchitis Low DLCO with restriction Asbestosis, berylliosis, hypersensitivity pneumonitis, idiopathic pulmonary fibrosis, Langerhans cell histiocytosis (histiocytosis X), lymphangitic spread of tumor, miliary tuberculosis, sarcoidosis, silicosis (late) Low DLCO with obstruction Cystic fibrosis, emphysema, silicosis (early) Low DLCO with normal Chronic pulmonary emboli, congestive heart failure, pulmonary function test results connective tissue disease with pulmonary involvement, dermatomyositis/polymyositis, inflammatory bowel disease, interstitial lung disease (early), primary pulmonary hypertension, rheumatoid arthritis, systemic lupus erythematosus, systemic sclerosis, Wegener granulomatosis (also called granulomatosis with polyangiitis) Interpretation: High = greater than 120% of predicted; Normal = LLN to 120% of predicted; Low (mild decrease) = greater than 60% of predicted and less than LLN; Low (moderate decrease) = 40% to 60% of predicted; Low (severe decrease) = less than 40% of predicted. If the laboratory does not report LLN, observational studies indicate that the LLN for men is approximately 80%, and the LLN for women is approximately 76% 11

26
27
28
29
30
31 1. Mannino DM, Sonia Buist A, Vollmer WM. Chronic obstructive pulmonary disease in the older adult: what defines abnormal lung function? Thorax. 2007;62(3): National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): Guidelines for the diagnosis and management of asthma summary report 2007 [published correction appears in J Allergy Clin Immunol. 2008;121(6):1330]. J Allergy Clin Immunol. 2007;120(5 suppl):s94-s Vesbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013; 187(4): Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5): Mannino DM, Sonia Buist A, Vollmer WM. Chronic obstructive pulmonary disease in the older adult: what defines abnormal lung function? Thorax. 2007;62(3): Güder G, Brenner S, Angermann CE, et al. GOLD or lower limit of normal definition? A comparison with expert-based diagnosis of chronic obstructive pulmonary disease in a prospective cohort-study. Respir Res. 2012;13(1):13 7. Hansen JE, Sun XG, Wasserman K. Spirometric criteria for airway obstruction: use percentage of FEV1/FVC ratio below the fifth percentile, not < 70%. Chest. 2007;131(2):
32 8. Hansen JE, Sun XG, Wasserman K. Spirometric criteria for airway obstruction: use percentage of FEV1/FVC ratio below the fifth percentile, not < 70%. Chest. 2007;131(2): Swanney MP, Ruppel G, Enright PL, et al. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Thorax. 2008;63(12): Crapo RO, Forster RE II. Carbon monoxide diffusing capacity. Clin Chest Med. 1989;10(2): Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2017 Report.
33
Interpreting pulmonary function tests: Recognize the pattern, and the diagnosis will follow
 REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
PFT Interpretation and Reference Values
 PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
Understanding the Basics of Spirometry It s not just about yelling blow
 Understanding the Basics of Spirometry It s not just about yelling blow Carl D. Mottram, RRT RPFT FAARC Technical Director - Pulmonary Function Labs and Rehabilitation Associate Professor of Medicine -
Understanding the Basics of Spirometry It s not just about yelling blow Carl D. Mottram, RRT RPFT FAARC Technical Director - Pulmonary Function Labs and Rehabilitation Associate Professor of Medicine -
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Impact of the new ATS/ERS pulmonary function test interpretation guidelines
 Respiratory Medicine (2007) 101, 2336 2342 Impact of the new ATS/ERS pulmonary function test interpretation guidelines Mary Elizabeth Kreider a,, Michael A. Grippi a,b a Division of Pulmonary, Allergy,
Respiratory Medicine (2007) 101, 2336 2342 Impact of the new ATS/ERS pulmonary function test interpretation guidelines Mary Elizabeth Kreider a,, Michael A. Grippi a,b a Division of Pulmonary, Allergy,
Pulmonary Function Testing
 In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
PULMONARY FUNCTION TESTS
 Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Basic approach to PFT interpretation. Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic
 Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Pulmonary Function Testing. Ramez Sunna MD, FCCP
 Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
PULMONARY FUNCTION TESTING. Purposes of Pulmonary Tests. General Categories of Lung Diseases. Types of PF Tests
 PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
Int. J. Pharm. Sci. Rev. Res., 34(2), September October 2015; Article No. 24, Pages: Role of Spirometry in Diagnosis of Respiratory Diseases
, September October 2015; Article No. 24, Pages: Role of Spirometry in Diagnosis of Respiratory Diseases") Review Article Role of Spirometry in Diagnosis of Respiratory Diseases Dipti Mohapatra 1, Tapaswini Mishra 1, Manasi Behera 1, Nibedita Priyadarsini 1, Arati Mohanty 1, *Prakash Kumar Sasmal 2 1 Department
Review Article Role of Spirometry in Diagnosis of Respiratory Diseases Dipti Mohapatra 1, Tapaswini Mishra 1, Manasi Behera 1, Nibedita Priyadarsini 1, Arati Mohanty 1, *Prakash Kumar Sasmal 2 1 Department
Pulmonary Function Tests. Mohammad Babai M.D Occupational Medicine Specialist
 Pulmonary Function Tests Mohammad Babai M.D Occupational Medicine Specialist www.drbabai.com Pulmonary Function Tests Pulmonary Function Tests: Spirometry Peak-Flow metry Bronchoprovocation Tests Body
Pulmonary Function Tests Mohammad Babai M.D Occupational Medicine Specialist www.drbabai.com Pulmonary Function Tests Pulmonary Function Tests: Spirometry Peak-Flow metry Bronchoprovocation Tests Body
Spirometric protocol
 Spirometric protocol Spirometry is the most common of the Pulmonary Function Test, that measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled.
Spirometric protocol Spirometry is the most common of the Pulmonary Function Test, that measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled.
Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology
 Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Assessment of the Lung in Primary Care
 Assessment of the Lung in Primary Care Andrew G Veale FRACP Auckland, New Zealand Presentation Cough (productive or dry) Haemoptysis Shortness of breath / dyspnea Wheeze (or noisy breathing) Chest pain
Assessment of the Lung in Primary Care Andrew G Veale FRACP Auckland, New Zealand Presentation Cough (productive or dry) Haemoptysis Shortness of breath / dyspnea Wheeze (or noisy breathing) Chest pain
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
Pulmonary Function Testing
 Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Content Indica c tion Lung v olumes e & Lung Indica c tions i n c paci c ties
 Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
PULMONARY FUNCTION. VOLUMES AND CAPACITIES
 PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
A Primer on Reading Pulmonary Function Tests. Joshua Benditt, M.D.
 A Primer on Reading Pulmonary Function Tests Joshua Benditt, M.D. What Are Pulmonary Function Tests Used For? Pulmonary function testing provides a method for objectively assessing the function of the
A Primer on Reading Pulmonary Function Tests Joshua Benditt, M.D. What Are Pulmonary Function Tests Used For? Pulmonary function testing provides a method for objectively assessing the function of the
Spirometry. Obstruction. By Helen Grim M.S. RRT. loop will have concave appearance. Flows decreased consistent with degree of obstruction.
 1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
Spirometry is the most frequently performed. Obstructive and restrictive spirometric patterns: fixed cut-offs for FEV1/FEV6 and FEV6
 Eur Respir J 2006; 27: 378 383 DOI: 10.1183/09031936.06.00036005 CopyrightßERS Journals Ltd 2006 Obstructive and restrictive spirometric patterns: fixed cut-offs for FEV1/ and J. Vandevoorde*, S. Verbanck
Eur Respir J 2006; 27: 378 383 DOI: 10.1183/09031936.06.00036005 CopyrightßERS Journals Ltd 2006 Obstructive and restrictive spirometric patterns: fixed cut-offs for FEV1/ and J. Vandevoorde*, S. Verbanck
Using Spirometry to Rule Out Restriction in Patients with Concomitant Low Forced Vital Capacity and Obstructive Pattern
 44 The Open Respiratory Medicine Journal, 2011, 5, 44-50 Using Spirometry to Rule Out Restriction in Patients with Concomitant Low Forced Vital Capacity and Obstructive Pattern Open Access Imran Khalid
44 The Open Respiratory Medicine Journal, 2011, 5, 44-50 Using Spirometry to Rule Out Restriction in Patients with Concomitant Low Forced Vital Capacity and Obstructive Pattern Open Access Imran Khalid
Coexistence of confirmed obstruction in spirometry and restriction in body plethysmography, e.g.: COPD + pulmonary fibrosis
 Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
3 COPD Recognition and Diagnosis: Approach to the Patient with Respiratory Symptoms
 William L. Eschenbacher, MD 3 COPD Recognition and Diagnosis: Approach to the Patient with Respiratory Symptoms Key Points 1. Patients who present with respiratory symptoms such as cough, sputum production,
William L. Eschenbacher, MD 3 COPD Recognition and Diagnosis: Approach to the Patient with Respiratory Symptoms Key Points 1. Patients who present with respiratory symptoms such as cough, sputum production,
Assessment of Bronchodilator Response in Various Spirometric Patterns
 Original Article 2013 NRITLD, National Research Institute of Tuberculosis and Lung Disease, Iran ISSN: 1735-0344 TANAFFOS Assessment of Bronchodilator Response in Various Spirometric Patterns Amir Houshang
Original Article 2013 NRITLD, National Research Institute of Tuberculosis and Lung Disease, Iran ISSN: 1735-0344 TANAFFOS Assessment of Bronchodilator Response in Various Spirometric Patterns Amir Houshang
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE
 The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
6- Lung Volumes and Pulmonary Function Tests
 6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
Office Based Spirometry
 Osteopathic Family Physician (2014)1, 14-18 Scott Klosterman, DO; Woodson Crenshaw, OMS4 Spartanburg Regional Family Medicine Residency Program; Edward Via College of Osteopathic Medicine - Virginia Campus
Osteopathic Family Physician (2014)1, 14-18 Scott Klosterman, DO; Woodson Crenshaw, OMS4 Spartanburg Regional Family Medicine Residency Program; Edward Via College of Osteopathic Medicine - Virginia Campus
Clinical Study Bronchial Responsiveness in Patients with Restrictive Spirometry
 BioMed Research International Volume 2013, Article ID 498205, 5 pages http://dx.doi.org/10.1155/2013/498205 Clinical Study Bronchial Responsiveness in Patients with Restrictive Spirometry Jean I. Keddissi,
BioMed Research International Volume 2013, Article ID 498205, 5 pages http://dx.doi.org/10.1155/2013/498205 Clinical Study Bronchial Responsiveness in Patients with Restrictive Spirometry Jean I. Keddissi,
Interpretative strategies for lung function tests
 Eur Respir J 2005; 26: 948 968 DOI: 10.1183/09031936.05.00035205 CopyrightßERS Journals Ltd 2005 SERIES ATS/ERS TASK FORCE: STANDARDISATION OF LUNG FUNCTION TESTING Edited by V. Brusasco, R. Crapo and
Eur Respir J 2005; 26: 948 968 DOI: 10.1183/09031936.05.00035205 CopyrightßERS Journals Ltd 2005 SERIES ATS/ERS TASK FORCE: STANDARDISATION OF LUNG FUNCTION TESTING Edited by V. Brusasco, R. Crapo and
S P I R O M E T R Y. Objectives. Objectives 2/5/2019
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
Lung Pathophysiology & PFTs
 Interpretation of Pulmonary Function Tests (PFTs) Course # 1612 2:00 5:00pm Friday February 22, 2013 Lung Pathophysiology & PFTs Mark F. Sands MD, FCCP, FAAAAI Division of Allergy, Immunology & Rheumatology
Interpretation of Pulmonary Function Tests (PFTs) Course # 1612 2:00 5:00pm Friday February 22, 2013 Lung Pathophysiology & PFTs Mark F. Sands MD, FCCP, FAAAAI Division of Allergy, Immunology & Rheumatology
behaviour are out of scope of the present review.
 explained about the test, a trial may be done before recording the results. The maneuver consists initially of normal tidal breathing. The subject then inhales to maximally fill the lungs. This is followed
explained about the test, a trial may be done before recording the results. The maneuver consists initially of normal tidal breathing. The subject then inhales to maximally fill the lungs. This is followed
PFTs ACOI Board Review 2018
 PFTs ACOI Board Review 2018 Thomas F. Morley, DO, MACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary, Critical Care and Sleep Medicine
PFTs ACOI Board Review 2018 Thomas F. Morley, DO, MACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary, Critical Care and Sleep Medicine
#8 - Respiratory System
 Page1 #8 - Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Equipment: Remember to bring photographic atlas. Figure 1. Structures of the respiratory system.
Page1 #8 - Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Equipment: Remember to bring photographic atlas. Figure 1. Structures of the respiratory system.
Spirometry Workshop for Primary Care Nurse Practitioners
 Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Adjunct Professor
Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Adjunct Professor
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation. Susan Blonshine RRT, RPFT, AE-C, FAARC
 Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Difference Between The Slow Vital Capacity And Forced Vital Capacity: Predictor Of Hyperinflation In Patients With Airflow Obstruction
 ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 4 Number 2 Difference Between The Slow Vital Capacity And Forced Vital Capacity: Predictor Of Hyperinflation In Patients With Airflow Obstruction
ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 4 Number 2 Difference Between The Slow Vital Capacity And Forced Vital Capacity: Predictor Of Hyperinflation In Patients With Airflow Obstruction
COMPREHENSIVE RESPIROMETRY
 INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
An Approach to Interpreting Spirometry
 COVER ARTICLE OFFICE PROCEDURES: An Approach to Interpreting Spirometry TIMOTHY J. BARREIRO, D.O., and IRENE PERILLO, M.D. University of Rochester School of Medicine and Dentistry, Rochester, New York
COVER ARTICLE OFFICE PROCEDURES: An Approach to Interpreting Spirometry TIMOTHY J. BARREIRO, D.O., and IRENE PERILLO, M.D. University of Rochester School of Medicine and Dentistry, Rochester, New York
Interpreting Spirometry. Vikki Knowles BSc(Hons) RGN Respiratory Nurse Consultant G & W`CCG
 RGN Respiratory Nurse Consultant G & W`CCG") Interpreting Spirometry Vikki Knowles BSc(Hons) RGN Respiratory Nurse Consultant G & W`CCG Why Spirometry? supports diagnosis classifies defect - obstructive/restrictive assesses -severity of defect -
Interpreting Spirometry Vikki Knowles BSc(Hons) RGN Respiratory Nurse Consultant G & W`CCG Why Spirometry? supports diagnosis classifies defect - obstructive/restrictive assesses -severity of defect -
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C
 MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene
 Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Outline FEF Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications?
 Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Using the lower limit of normal for the FEV 1 /FVC ratio reduces the misclassification of airway obstruction
 See Editorial, p 1031 c Supplementary reference values data are published online only at http://thorax.bmj.com/ content/vol63/issue12 1 Respiratory Physiology Laboratory, Christchurch Hospital, Canterbury
See Editorial, p 1031 c Supplementary reference values data are published online only at http://thorax.bmj.com/ content/vol63/issue12 1 Respiratory Physiology Laboratory, Christchurch Hospital, Canterbury
Effect Of Byrates (Barium Sulphate) On Pulmonary Function In Byrates Mine Workers
 On Pulmonary Function In Byrates Mine Workers") IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. I January. (2018), PP 46-50 www.iosrjournals.org Effect Of Byrates (Barium Sulphate)
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. I January. (2018), PP 46-50 www.iosrjournals.org Effect Of Byrates (Barium Sulphate)
SPIROMETRY. Marijke Currie (CRFS) Care Medical Ltd Phone: Copyright CARE Medical ltd
 Care Medical Ltd Phone: Copyright CARE Medical ltd") SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
Spirometry: an essential clinical measurement
 Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
Chapter. Diffusion capacity and BMPR2 mutations in pulmonary arterial hypertension
 Chapter 7 Diffusion capacity and BMPR2 mutations in pulmonary arterial hypertension P. Trip B. Girerd H.J. Bogaard F.S. de Man A. Boonstra G. Garcia M. Humbert D. Montani A. Vonk Noordegraaf Eur Respir
Chapter 7 Diffusion capacity and BMPR2 mutations in pulmonary arterial hypertension P. Trip B. Girerd H.J. Bogaard F.S. de Man A. Boonstra G. Garcia M. Humbert D. Montani A. Vonk Noordegraaf Eur Respir
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
SPIROMETRY METHOD. COR-MAN IN / EN Issue A, Rev INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark
 SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
DLCO versus DLCO/VA as predictors of pulmonary gas exchange $
 Respiratory Medicine (2007) 101, 989 994 DLCO versus DLCO/VA as predictors of pulmonary gas exchange $ David A. Kaminsky a,, Todd Whitman b, Peter W. Callas c a Pulmonary Disease and Critical Care Medicine,
Respiratory Medicine (2007) 101, 989 994 DLCO versus DLCO/VA as predictors of pulmonary gas exchange $ David A. Kaminsky a,, Todd Whitman b, Peter W. Callas c a Pulmonary Disease and Critical Care Medicine,
Spirometry and Interpretation of Spirometry
 Spirometry and Interpretation of Spirometry Chicago Asthma Consortium June 21, 2017 William Clapp MD, FCCP Medical Director Pulmonary Physiology Laboratories Cook County Health and Hospital Systems Disclosures
Spirometry and Interpretation of Spirometry Chicago Asthma Consortium June 21, 2017 William Clapp MD, FCCP Medical Director Pulmonary Physiology Laboratories Cook County Health and Hospital Systems Disclosures
CIRCULAR INSTRUCTION REGARDING ESTABLISHMENT OF IMPAIRMENT DUE TO OCCUPATIONAL LUNG DISEASE FOR THE PURPOSES OF AWARDING PERMANENT DISABLEMENT
 Circular Instruction 195 CIRCULAR INSTRUCTION REGARDING ESTABLISHMENT OF IMPAIRMENT DUE TO OCCUPATIONAL LUNG DISEASE FOR THE PURPOSES OF AWARDING PERMANENT DISABLEMENT COMPENSATION FOR OCCUPATIONAL INJURIES
Circular Instruction 195 CIRCULAR INSTRUCTION REGARDING ESTABLISHMENT OF IMPAIRMENT DUE TO OCCUPATIONAL LUNG DISEASE FOR THE PURPOSES OF AWARDING PERMANENT DISABLEMENT COMPENSATION FOR OCCUPATIONAL INJURIES
In order to diagnose lung diseases doctors
 You Take My Breath Away Activity 5C NOTE: This activity is designed to follow You Really Are Full of Hot Air! Activity Objectives: After completing You Really Are Full of Hot Air! Activity 5B, students
You Take My Breath Away Activity 5C NOTE: This activity is designed to follow You Really Are Full of Hot Air! Activity Objectives: After completing You Really Are Full of Hot Air! Activity 5B, students
Grading the Severity of Obstruction in Mixed Obstructive-Restrictive Lung Disease
 CHEST Original Research PULMONARY FUNCTION TESTING Grading the Severity of Obstruction in Mixed Obstructive-Restrictive Lung Disease Zechariah S. Gardner, MD ; Gregg L. Ruppel, MEd, RRT, RPFT ; and David
CHEST Original Research PULMONARY FUNCTION TESTING Grading the Severity of Obstruction in Mixed Obstructive-Restrictive Lung Disease Zechariah S. Gardner, MD ; Gregg L. Ruppel, MEd, RRT, RPFT ; and David
S P I R O M E T R Y. Objectives. Objectives 3/12/2018
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
Chapter 3. Pulmonary Function Study Assessments. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Relationship between Methacholine Challenge Testing and exhaled Nitric Oxide in adult patients with suspected bronchial asthma
 O R I G I N A L A R T I C L E S Eur Ann Allergy Clin Immunol Vol 46, N 3, 109-113, 2014 M. Giovannini, M. Valli, V. Ribuffo, R. Melara, G. Cappiello, E. Businarolo, A. Andreani Relationship between Methacholine
O R I G I N A L A R T I C L E S Eur Ann Allergy Clin Immunol Vol 46, N 3, 109-113, 2014 M. Giovannini, M. Valli, V. Ribuffo, R. Melara, G. Cappiello, E. Businarolo, A. Andreani Relationship between Methacholine
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD)
 Instructions for the Pulmonary Diagnosis Form (PLD)") Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Supplementary Online Content
 Supplementary Online Content Regan EA, Lynch DA, Curran-Everett D, et al; Genetic Epidemiology of COPD (COPDGene) Investigators. Clinical and radiologic disease in smokers with normal spirometry. Published
Supplementary Online Content Regan EA, Lynch DA, Curran-Everett D, et al; Genetic Epidemiology of COPD (COPDGene) Investigators. Clinical and radiologic disease in smokers with normal spirometry. Published
PULMONARY FUNCTION TEST(PFT)
") PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
QUALITY OF LIFE MEASURED BY THE ST GEORGE'S RESPIRATORY QUESTIONNAIRE AND SPIROMETRY
 ERJ Express. Published on January 22, 2009 as doi: 10.1183/09031936.00116808 QUALITY OF LIFE MEASURED BY THE ST GEORGE'S RESPIRATORY QUESTIONNAIRE AND SPIROMETRY 1 Mark Weatherall, 2 Suzanne Marsh, 2 Philippa
ERJ Express. Published on January 22, 2009 as doi: 10.1183/09031936.00116808 QUALITY OF LIFE MEASURED BY THE ST GEORGE'S RESPIRATORY QUESTIONNAIRE AND SPIROMETRY 1 Mark Weatherall, 2 Suzanne Marsh, 2 Philippa
The objectives of the pre-anaesthetic assessment
 Dr Gerard Meachery The objectives of the pre-anaesthetic assessment! Evaluate the patient s medical condition from medical history, physical examination, investigations and, when appropriate, past medical
Dr Gerard Meachery The objectives of the pre-anaesthetic assessment! Evaluate the patient s medical condition from medical history, physical examination, investigations and, when appropriate, past medical
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Peak Expiratory Flow Is Not a Quality Indicator for Spirometry*
 Original Research PULMONARY FUNCTION TESTING Peak Expiratory Flow Is Not a Quality Indicator for Spirometry* Peak Expiratory Flow Variability and FEV 1 Are Poorly Correlated in an Elderly Population Matthew
Original Research PULMONARY FUNCTION TESTING Peak Expiratory Flow Is Not a Quality Indicator for Spirometry* Peak Expiratory Flow Variability and FEV 1 Are Poorly Correlated in an Elderly Population Matthew
Spirometry, Static Lung Volumes, and Diffusing Capacity
 Spirometry, Static Lung Volumes, and Diffusing Capacity Carlos A Vaz Fragoso MD, Hilary C Cain MD, Richard Casaburi MD PhD, Patty J Lee MD, Lynne Iannone MSc, Linda S Leo-Summers MPH, and Peter H Van Ness
Spirometry, Static Lung Volumes, and Diffusing Capacity Carlos A Vaz Fragoso MD, Hilary C Cain MD, Richard Casaburi MD PhD, Patty J Lee MD, Lynne Iannone MSc, Linda S Leo-Summers MPH, and Peter H Van Ness
Clinical pulmonary physiology. How to report lung function tests
 Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Objectives. Pulmonary Assessment 12/13/2017
 Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Pulmonary Function Test
 Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Use of Lambda-Mu-Sigma-Derived Z Score for Evaluating Respiratory Impairment in Middle-Aged Persons
 Use of Lambda-Mu-Sigma-Derived Z Score for Evaluating Respiratory Impairment in Middle-Aged Persons Carlos A Vaz Fragoso MD, Thomas M Gill MD, Gail McAvay PhD, Peter H Van Ness PhD, H Klar Yaggi MD, and
Use of Lambda-Mu-Sigma-Derived Z Score for Evaluating Respiratory Impairment in Middle-Aged Persons Carlos A Vaz Fragoso MD, Thomas M Gill MD, Gail McAvay PhD, Peter H Van Ness PhD, H Klar Yaggi MD, and
POSITION STATEMENT BACKGROUND INTRODUCTION
 POSITION STATEMENT Reference values for spirometry and their use in test interpretation: A Position Statement from the Australian and New Zealand Society of Respiratory Science DANNY BRAZZALE, 1 GRAHAM
POSITION STATEMENT Reference values for spirometry and their use in test interpretation: A Position Statement from the Australian and New Zealand Society of Respiratory Science DANNY BRAZZALE, 1 GRAHAM
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Office Spirometry Guide
 Office Spirometry Guide MD Spiro 803 Webster Street, Lewiston ME 04240 Telephone 207-786-7808 1-800-588-3381 Fax 207-786-7280 www.mdspiro.com e-mail: sales@mdspiro.com Why should you perform spirometry
Office Spirometry Guide MD Spiro 803 Webster Street, Lewiston ME 04240 Telephone 207-786-7808 1-800-588-3381 Fax 207-786-7280 www.mdspiro.com e-mail: sales@mdspiro.com Why should you perform spirometry
Spirometry and Flow Volume Measurements
 Spirometry and Flow Volume Measurements Standards & Guidelines December 1998 To serve the public and guide the medical profession Revision Dates: December 1998 Approval Date: June 1998 Originating Committee:
Spirometry and Flow Volume Measurements Standards & Guidelines December 1998 To serve the public and guide the medical profession Revision Dates: December 1998 Approval Date: June 1998 Originating Committee:
Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma
 Original Article Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma Feng-Jia Chen, Huai Liao, Xin-Yan Huang, Can-Mao Xie Department of Respiratory
Original Article Importance of fractional exhaled nitric oxide in diagnosis of bronchiectasis accompanied with bronchial asthma Feng-Jia Chen, Huai Liao, Xin-Yan Huang, Can-Mao Xie Department of Respiratory
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities
 Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
PREDICTION EQUATIONS FOR LUNG FUNCTION IN HEALTHY, LIFE TIME NEVER-SMOKING MALAYSIAN POPULATION
 Prediction Equations for Lung Function in Healthy, Non-smoking Malaysian Population PREDICTION EQUATIONS FOR LUNG FUNCTION IN HEALTHY, LIFE TIME NEVER-SMOKING MALAYSIAN POPULATION Justin Gnanou, Brinnell
Prediction Equations for Lung Function in Healthy, Non-smoking Malaysian Population PREDICTION EQUATIONS FOR LUNG FUNCTION IN HEALTHY, LIFE TIME NEVER-SMOKING MALAYSIAN POPULATION Justin Gnanou, Brinnell
Relationship Between FEV1& PEF in Patients with Obstructive Airway Diseases
 OBSTRUCTIVE THE IRAQI POSTGRADUATE AIRWAY MEDICAL DISEASES JOURNAL Relationship Between FEV1& PEF in Patients with Obstructive Airway Diseases Muhammed.W.AL.Obaidy *, Kassim Mhamed Sultan*,Basil Fawzi
OBSTRUCTIVE THE IRAQI POSTGRADUATE AIRWAY MEDICAL DISEASES JOURNAL Relationship Between FEV1& PEF in Patients with Obstructive Airway Diseases Muhammed.W.AL.Obaidy *, Kassim Mhamed Sultan*,Basil Fawzi
Research Article Subjects with Discordant Airways Obstruction: Lost between Spirometric Definitions of COPD
 Pulmonary Medicine Volume 2011, Article ID 780215, 6 pages doi:10.1155/2011/780215 Research Article Subjects with Discordant Airways Obstruction: Lost between Spirometric Definitions of COPD Bernd Lamprecht,
Pulmonary Medicine Volume 2011, Article ID 780215, 6 pages doi:10.1155/2011/780215 Research Article Subjects with Discordant Airways Obstruction: Lost between Spirometric Definitions of COPD Bernd Lamprecht,
Spirometry: Introduction
 Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
Epidemiology of COPD Prof. David M. Mannino, M.D.
 Epidemiology of COPD David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health College of Public Health University of Kentucky 1 Outline Definitions Severity Progression
Epidemiology of COPD David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health College of Public Health University of Kentucky 1 Outline Definitions Severity Progression
Pulmonary Function Tests
 Ulster Med J 2011;80(2):84-90 Grand Rounds Pulmonary Function Tests Harpreet Ranu, Michael Wilde, Brendan Madden Accepted 16 December 2010 Abstract Pulmonary function tests are valuable investigations
Ulster Med J 2011;80(2):84-90 Grand Rounds Pulmonary Function Tests Harpreet Ranu, Michael Wilde, Brendan Madden Accepted 16 December 2010 Abstract Pulmonary function tests are valuable investigations
UNIT TWO: OVERVIEW OF SPIROMETRY. A. Definition of Spirometry
 UNIT TWO: OVERVIEW OF SPIROMETRY A. Definition of Spirometry Spirometry is a medical screening test that measures various aspects of breathing and lung function. It is performed by using a spirometer,
UNIT TWO: OVERVIEW OF SPIROMETRY A. Definition of Spirometry Spirometry is a medical screening test that measures various aspects of breathing and lung function. It is performed by using a spirometer,
WORKSHOP OF LUNG FUNCTION TEST. Dr. Lo Iek Long, Department of Respiratory Medicine, CHCSJ, Macau
 WORKSHOP OF LUNG FUNCTION TEST Dr. Lo Iek Long, Department of Respiratory Medicine, CHCSJ, Macau Big three in Respiratory Medicine Lung Function Test Chest imaging Bronchoscopy Table of Content Section
WORKSHOP OF LUNG FUNCTION TEST Dr. Lo Iek Long, Department of Respiratory Medicine, CHCSJ, Macau Big three in Respiratory Medicine Lung Function Test Chest imaging Bronchoscopy Table of Content Section
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Chronic Cough. Abhishek Kumar, MD, MPH Pulmonary and Critical Care Mercy Medical Center, Cedar Rapids, IA
 Chronic Cough Abhishek Kumar, MD, MPH Pulmonary and Critical Care Mercy Medical Center, Cedar Rapids, IA What we shall discuss? Cough anatomy and pathophysiology Common etiologies Work-up Role of spirometry/pulmonary
Chronic Cough Abhishek Kumar, MD, MPH Pulmonary and Critical Care Mercy Medical Center, Cedar Rapids, IA What we shall discuss? Cough anatomy and pathophysiology Common etiologies Work-up Role of spirometry/pulmonary
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
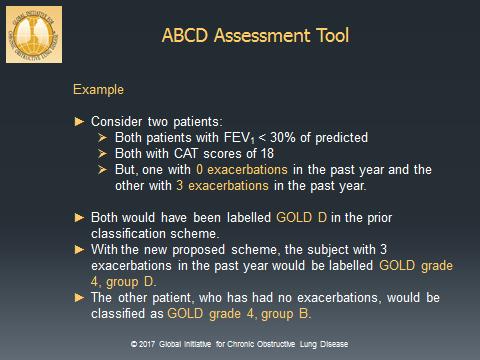
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Pulmonary Func-on Tes-ng. Chapter 8
 Pulmonary Func-on Tes-ng Chapter 8 Pulmonary Func-on Tes-ng Which of the following is the true pulmonary func-on test? Spirometry Lung volumes Diffusion capacity ABG Pulmonary Func-on Tes-ng Process of
Pulmonary Func-on Tes-ng Chapter 8 Pulmonary Func-on Tes-ng Which of the following is the true pulmonary func-on test? Spirometry Lung volumes Diffusion capacity ABG Pulmonary Func-on Tes-ng Process of
Triennial Pulmonary Workshop 2012
 Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Respiratory Physiology In-Lab Guide
 Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
PomPom SHOOTER. Activity Background: Common Obstructive Lung Disorders:
 CAUTION: Students with asthma or other respiratory problems should NOT perform the breathing exercises in this activity because they involve repeated maximal inhalations and exhalations and use of a breathing
CAUTION: Students with asthma or other respiratory problems should NOT perform the breathing exercises in this activity because they involve repeated maximal inhalations and exhalations and use of a breathing