Evidence and So Much More
|
|
|
- George Wood
- 5 years ago
- Views:
Transcription











1 Evidence and So Much More James McCormack, BSc(Pharm), PharmD Professor, Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC









2 Entire salary comes through the UBC Faculty of Pharmaceutical Sciences - also some legal/educational work I have received no honorarium or research money from the drug industry in the last 25 or so years ios apps (ipad/iphone) KidneyCalc and MyStudies - mystudies.org Premium podcast subscription Best Science (BS) Medicine podcast - therapeuticseducation.org
3 Our Agenda 1.Background and guiding principles 2.Evidence on new diabetes drugs 3.Lab reports and how to interpret them 4.Guidelines and how to use them 5.Medical cannabinoids

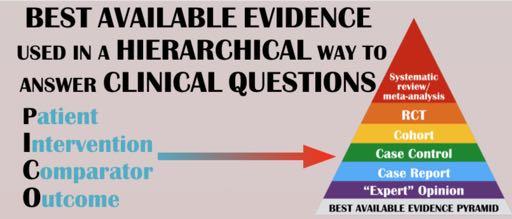
4 MY BELIEF All Health Care Providers should have their practice underpinned by the best available evidence Evidence-Based Practice (EBP)

5 The Bullshit Asymmetry The amount of energy needed to refute bullshit is an order of magnitude bigger than to produce it.


6

7


8

9 People want involvement in evidence and decisions Communicating with patients on health care evidence. Discussion Paper, Institute of Medicine, Washington, DC 2012

10 Satisfaction is linked to shared decisions Communicating with patients on health care evidence. Discussion Paper, Institute of Medicine, Washington, DC 2012
11 Most patients cannot recall a time when their care provider discussed scientific evidence as the basis for better care Communicating with patients on health care evidence. Discussion Paper, Institute of Medicine, Washington, DC 2012

12 PATIENT REVOLUTION = Clinicians and patients working in partnership KNOWING THE MAGNITUDE OF THE BENEFIT OF TREATMENT KNOWING the POTENTIAL HARMS - SIDE EFFECTS, COST AND INCONVENIENCE REALIZING HEALTH DECISIONS ARE YOUR DECISIONS
13 Evidence Issues Much of research is not going to be right One study likely proves nothing - need reproducibility The evidence for nonreproducibility in basic and preclinical biomedical research is compelling John Ioannidis Cohort trials don't prove causation Research does go unpublished - but large studies do get reported
14 Science can be used to inform clinical decisions, but cannot definitively inform value judgements, because the significance of potential benefits and harms of a therapy are in the eye of the beholder and will differ across individuals. Circulation. 2017;135: DOI: /CIRCULATIONAHA
15 Some clinical adages? Ask - how do you feel about being involved in making decisions about your treatment? It's OK if we say I don t know, let s look into it, it s your decision. You and your patient s perception are not necessarily right and likely not the same

16 BENEFIT - 88% of study authors concluded that participants overestimated benefits HARM - 67% underestimated harm JAMA Intern Med 2015;175:

17 Key steps to communicating evidence 1. Understand the patient s (and family members ) experiences and expectations. 2. Build partnerships. 3. Discuss the evidence, including a balanced discussion about uncertainties. 4. Present recommendations. 5. Check for understanding and agreement.

18 Risky Relative Adjectives HOW low is low moderate is moderate high is high
19 Misleading Terminology Significant Use with caution Use with extreme caution Monitor closely High risk Very high risk high risk
20 What is "High Risk" 40 Clinicians Patients % of respondents % Chance of a heart attack in the next 5 years (%)
21 Beware of qualitative quantification Lancet 2002;359:853 54
22 Evidence-based risk communication There is likely no single best method of communicating probabilities to patients but rather several good options with some better suited to certain risk scenarios. Ann Intern Med 2014;161:270-80
23 Recommended approaches Need a time frame, main endpoints, ask what they know GENERAL SUGGESTIONS - these are relative use percentages (5%) or natural frequencies (5 out of 100) - BOTH? use absolute terms add bar graphs or icon arrays use incremental risk format with icon arrays in the same array avoid use of NNTs if use relative risks add baseline risks Ann Intern Med 2014;161:270-80
24 Many courts (UK, US, CA) The reasonable-patient standard requires physicians and other health care practitioners to disclose all relevant information about the risks, benefits, and alternatives of a proposed treatment that an OBJECTIVE PATIENT would find material in making an intelligent decision as to whether to agree to the proposed procedure JAMA 2016;315:2063-4
25 It s all about figuring out The Chance WITH NO TREATMENT VS The Chance WITH TREATMENT Ballpark risk estimate Epidemiological data/cohort data - Framingham, QRISK, FRAX, CHA2DS2-VASc Ballpark benefit estimate RCT data 1.use the absolute benefit if people are similar to those in the studies or, 2.use the relative benefit and apply it to the baseline risk
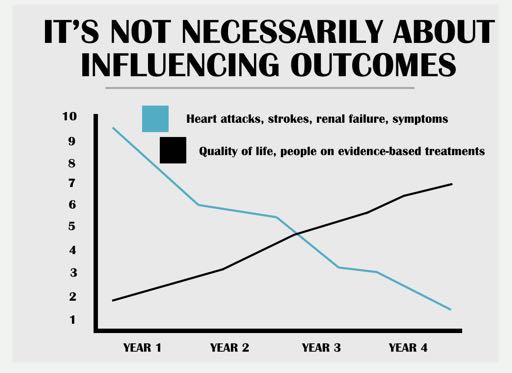
26 Approaches differ depending on outcome Every patient is an experiment - dose and effect Prevention - one will never know if it worked Symptoms - we can usually figure out if it is working - but it is tricky Diagnosis - pre- and post-test probabilities Expectations
27 Prevention



28 cvdcalculator.com 1. Calculate ballpark 10-yr risk of /fractures - BP, chol, diabetes, BMI. BMD 2. Make estimate of benefit based on the best available evidence 3. Gives a list of adverse effects to discuss


29 INITIAL COST NOW COSTS Baseline risk Relative benefit YOU SAVE New risk Absolute benefit

30 Misguided beliefs Patients believe CVD prevention drugs produce a 70% absolute benefit over 5 years when at most only ~ 20-30% benefit is possible over a lifetime LIFETIME FIVE YEARS Clin Med 2002;2:527-33
 Assume a")



31 Risk of future illness CVD risk/benefit (most people don t benefit despite a lifetime of treatment) Assume a person s lifetime risk of CVD is that of a male with two CVD risk factors - roughly 50% (NEJM 2012;366:321-9) Assume that with multiple risk factor modification we can reduce that risk relatively by 60% (VERY optimistic) Risk goes from 50% 20% 30% of individuals BENEFIT 70% DO NOT despite a LIFETIME of treatment Prescriber September 2015
32 Symptoms
33 You primarily need to know IF it works Safety, cost and convenience Older medications first - safety Head-to-head studies are uncommon Doses in the CPS are wrong N-of-1 studies Let the patient tell you
34 Symptom NNTs General anesthesia/local anesthesia - NNT ~1 PPIS, sildenafil - heartburn/ successful intercourse NNT ~2 NSAIDs, opioids - pain NNT ~3-5 Steroids - sore throat - NNT ~3, Bell s palsy - NNT ~10 Antibiotics - acute COPD exacerbation - NNT ~5 Topical antibiotics - bacterial conjunctivitis - NNT ~7 Antidepressants - severe depression - NNT ~10 Ipratropium - asthma attack - NNT ~11 Cholinesterase inhibitors - ADAS-Cog >4 - NNT ~10 Sleeping pills - improvement in sleep quality - NNT ~13
35 But you need to know what goes on in the placebo group Response in the placebo group If person responds, what is the % chance it was the medication If Benefit 10% - NNT 10 If Benefit 20% - NNT 5 0% ~100% ~100% 20% ~33% ~50% 40% ~20% ~33%
36 The Placebo Group Effect not the placebo effect and these are ballpark numbers ~0% - general anesthesia ~5% - psychosis ~10% - sildenafil, OCD ~20% - Alzheimer s meds, acetaminophen for headaches, side effects ~25% - menopausal symptoms, migraine (frequency/severity) ~30% - blood pressure goal, depression, anxiety, PTSD, PPIs/H2RA, sore throat, NSAIDs of OA, inhalers for COPD ~40% - panic disorders
37 When a medication has worked, if you were a betting person you would bet that it probably wasn't because the medication worked.
38 The Lancet Published online February 21, 2018 provides as good and balanced a synopsis as we will likely ever have of the results from the 522 trials of 21 antidepressants in 116,477 participants 82% of the included studies - moderate to high risk of bias 78% of studies were funded by drug companies, and many studies failed to report funding at all the authors report funding by industry was not associated with substantial differences in terms of response or dropout rates
39 The Lancet Published online February 21, 2018 patient population was limited to adults with moderate to severe depression and an average Hamilton depression score of 26.3 primary endpoint - 50% change in Hamilton depression score at 8 weeks also looked at remission rates at 8 weeks all-cause discontinuation - combines both efficacy and tolerability looked at drop-outs due to adverse events but didn t report data on specific adverse effects such as sedation, dry mouth, sexual dysfunction, and weight gain
40 The Lancet Published online February 21, 2018 all antidepressants worked 50% change - OR ~ 1.65 for all antidepressants combined remission - OR ~ 1.55 they found few differences between antidepressants when all data were considered confidence intervals around individual effect sizes were wide
41 The Lancet Published online February 21, % of placebo group participants report improvement or remission in trials of antidepressants an OR of ~ 1.6 means about 10-12% more people in the treatment group would benefit compared with the placebo group absolute response rates placebo ~40% and treatment ~50% 10 patients with moderate to severe depression take an antidepressant for two months five (50%) will report being better but in four of them the response will not be because of the medication
42 The Lancet Published online February 21, 2018 all-cause discontinuation rates were not statistically different from placebo for most antidepressants in this meta-analysis. active treatment increased the risk of dropping out because of side effect - OR of ~ 2.3 placebo typically 3-5% ~ 5% more people in treatment groups dropped out because of side effects
43 What the antidepressant MA doesn't answer 1. their effect on milder forms of depression 2. their effects beyond eight weeks of treatment 3. the harms associated with specific agents and their magnitude 4. the effectiveness of antidepressants outside the confines of randomised trials 5. the long-term adverse effects of antidepressants 6. the likelihood of withdrawal symptoms when treatment stops 7. comparative benefits and harms of antidepressants relative to non-drug treatments such as cognitive behavioural therapy 8. which antidepressant should be tried first 9. which one is likely to work best for an individual patient
44 Low doses
45 A sample of RCT Evidence 6.25 mg hydrochlorothiazide first marketed at 50 to 200 mg daily 6.25 mg captopril 25 mg PO TID is still a commonly recommended initial starting dose for hypertension 25 mg sildenafil (Viagra) effective dose for erectile dysfunction 25 mg sumatriptan (Imitrex) works as well as100 mg 5 mg daily fluoxetine (Prozac) similar effects to those seen at 20 mg and 40 mg daily 0.25 mg ezetimibe (Ezetrol) 15 mg elemental iron daily 150 mg daily bupropion (Zyban) 0.5 mg BID varenicline (Champix) 10 mg atorvastatin 1/40th of the recommended initial starting dose provides 50% of the LDL lowering effect as effective for anemia in the elderly as 50 mg and 150 mg with a lower incidence of side effects produces the same rate of smoking cessation at one year as 300 mg daily (1.0 mg BID) produces 2/3 of the effect on cholesterol as that seen with an 80 mg (8-fold increase) dose 200 mg ibuprofen (Motrin) as effective as 400 mg for migraine headache 25 mg ranitidine (Zantac) as effective as 125 mg for heartburn relief 1.8 mg colchicine as effective as 4.8mg for acute gout with less adverse events
46 60 DOSE increases do not lead to proportional EFFECT increases % reduction in LDL cholesterol mg 20mg 40mg 80mg 15 0 Rosuvastatin Atorvastatin Simvastatin Pravastatin 100% 95% 85% 75% 80 mg 40 mg 20 mg 10 mg Atorvastatin
47 KEEP CALM AND DO THE RIGHT THING
Polypharmacy: A Rational Evidence-informed Approach with a Touch of Common Sense
 Polypharmacy: A Rational Evidence-informed Approach with a Touch of Common Sense KEEP CALM BECAUSE LESS IS MORE James McCormack B.Sc. (Pharm), Pharm.D. Professor Faculty of Pharmaceutical Sciences University
Polypharmacy: A Rational Evidence-informed Approach with a Touch of Common Sense KEEP CALM BECAUSE LESS IS MORE James McCormack B.Sc. (Pharm), Pharm.D. Professor Faculty of Pharmaceutical Sciences University
James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada
, PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada") James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada My Agenda Discuss the best available evidence Put the evidence into
James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada My Agenda Discuss the best available evidence Put the evidence into
Welcome to the 19th Annual wow, almost 20 years Drug Therapy Decision Making Course
 Welcome to the 19th Annual wow, almost 20 years Drug Therapy Decision Making Course An interactive course on common and new drug therapy issues from an evidence based perspective Education should not be
Welcome to the 19th Annual wow, almost 20 years Drug Therapy Decision Making Course An interactive course on common and new drug therapy issues from an evidence based perspective Education should not be
James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada
, PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada") LESS IS MORE James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada MORE OR LESS therapeuticseducation.org medicationmythbusters.com
LESS IS MORE James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada MORE OR LESS therapeuticseducation.org medicationmythbusters.com
Lipid Lowering in patients with High Risk of Cardiovascular Disease (Primary Prevention)
") Lipid Lowering in patients with High Risk of Cardiovascular Disease (Primary Prevention) Policy Statement: October 2010 This policy defines the decision made by NHS Wirral following an evidence review
Lipid Lowering in patients with High Risk of Cardiovascular Disease (Primary Prevention) Policy Statement: October 2010 This policy defines the decision made by NHS Wirral following an evidence review
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
The who, what, why, where, and when of Clinical Practice Guidelines (CPGs)
") The who, what, why, where, and when of Clinical Practice Guidelines (CPGs) Appraisal of Guidelines for Research and Evaluation (AGREE) II DOMAIN 1. SCOPE AND PURPOSE DOMAIN 2. STAKEHOLDER INVOLVEMENT DOMAIN
The who, what, why, where, and when of Clinical Practice Guidelines (CPGs) Appraisal of Guidelines for Research and Evaluation (AGREE) II DOMAIN 1. SCOPE AND PURPOSE DOMAIN 2. STAKEHOLDER INVOLVEMENT DOMAIN
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Pain therapeutics. Acetaminophen/NSAIDs Acute pain Osteoarthritis Migraine Acute Gout Neuropathic pain
 Pain therapeutics Acetaminophen/NSAIDs Acute pain Osteoarthritis Migraine Acute Gout Neuropathic pain James McCormack, Pharm.D. Professor Faculty of Pharmaceutical Sciences, UBC Common types of pain killers
Pain therapeutics Acetaminophen/NSAIDs Acute pain Osteoarthritis Migraine Acute Gout Neuropathic pain James McCormack, Pharm.D. Professor Faculty of Pharmaceutical Sciences, UBC Common types of pain killers
Quantifying the Benefits and Harms of Interventions: Relative vs. Absolute Risk
 JOURNAL CLUB LECTURE SERIES: Quantifying the Benefits and Harms of Interventions: Relative vs. Absolute Risk Tuesday, May 12 th, 2015 Anil N. Makam, MD MAS Oanh K. Nguyen, MD MAS Division of General Internal
JOURNAL CLUB LECTURE SERIES: Quantifying the Benefits and Harms of Interventions: Relative vs. Absolute Risk Tuesday, May 12 th, 2015 Anil N. Makam, MD MAS Oanh K. Nguyen, MD MAS Division of General Internal
Calculating RR, ARR, NNT
 Calculating RR, ARR, NNT In a trial RR = Event rate (eg # of people with one stroke/ total people) in treatment group/event rate in the control group. ARR = Event rate in control group minus the event
Calculating RR, ARR, NNT In a trial RR = Event rate (eg # of people with one stroke/ total people) in treatment group/event rate in the control group. ARR = Event rate in control group minus the event
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
How to CRITICALLY APPRAISE
 How to CRITICALLY APPRAISE an RCT in 10 minutes James McCormack BSc(Pharm), Pharm D Professor Faculty of Pharmaceutical Sciences, UBC Vancouver, BC, Canada medicationmythbusters.com CRITICAL APPRAISAL
How to CRITICALLY APPRAISE an RCT in 10 minutes James McCormack BSc(Pharm), Pharm D Professor Faculty of Pharmaceutical Sciences, UBC Vancouver, BC, Canada medicationmythbusters.com CRITICAL APPRAISAL
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
TRANSCRIPT. Do Corticosteroids Decrease the Pain of Acute Pharyngitis? - Frankly Speaking EP 18
 Do Corticosteroids Decrease the Pain of Acute Pharyngitis? - Frankly Speaking EP 18 Transcript Details This is a transcript of an episode from the podcast series Frankly Speaking accessible at Pri- Med.com.
Do Corticosteroids Decrease the Pain of Acute Pharyngitis? - Frankly Speaking EP 18 Transcript Details This is a transcript of an episode from the podcast series Frankly Speaking accessible at Pri- Med.com.
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Hypertension and Cholesterol in the Elderly
 Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden
Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden
Evidence- and Value-based Solutions for Health Care Clinical Improvement Consults, Content Development, Training & Seminars, Tools
 Definition Key Points Key Problems Bias Choice Lack of Control Chance Observational Study Defined Epidemiological study in which observations are made, but investigators do not control the exposure or
Definition Key Points Key Problems Bias Choice Lack of Control Chance Observational Study Defined Epidemiological study in which observations are made, but investigators do not control the exposure or
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
If Not Opioids then LEAH EDMONDS CSHP OCTOBER 26, 2017
 If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
JAMA. 2011;305(24): Nora A. Kalagi, MSc
: Nora A. Kalagi, MSc") JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Understanding new international guidelines to tackle CV Risk: A practical model John Deanfield, MD UCL, London United Kingdom s
 Understanding new international guidelines to tackle CV Risk: A practical model John Deanfield, MD UCL, London United Kingdom s Ho Chi Minh City, Vietnam August 7, 2014 JBS 2 Risk Guidelines (2005) Based
Understanding new international guidelines to tackle CV Risk: A practical model John Deanfield, MD UCL, London United Kingdom s Ho Chi Minh City, Vietnam August 7, 2014 JBS 2 Risk Guidelines (2005) Based
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181)
") Putting NICE guidance into practice Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181) Published: July 2014 This costing report accompanies Lipid modification:
Putting NICE guidance into practice Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181) Published: July 2014 This costing report accompanies Lipid modification:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Overview
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Overview Ezetimibe for the treatment of primary (heterozygous familial and non-familial) hypercholesterolaemia The overview is written by members of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Overview Ezetimibe for the treatment of primary (heterozygous familial and non-familial) hypercholesterolaemia The overview is written by members of
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Making comparisons. Previous sessions looked at how to describe a single group of subjects However, we are often interested in comparing two groups
 Making comparisons Previous sessions looked at how to describe a single group of subjects However, we are often interested in comparing two groups Data can be interpreted using the following fundamental
Making comparisons Previous sessions looked at how to describe a single group of subjects However, we are often interested in comparing two groups Data can be interpreted using the following fundamental
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Pharmacology Challenges: Managing Statin Myalgia
 Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Dyslipidemia in women: Who should be treated and how?
 Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Tools for Targeting High Risk Patients in Your Practice. Statement of Disclosure
 Tools for Targeting High Risk Patients in Your Practice Joseph Vande Griend, PharmD, BCPS, CGP Assistant Professor, University of Colorado Departments of Clinical Pharmacy and Family Medicine Skaggs School
Tools for Targeting High Risk Patients in Your Practice Joseph Vande Griend, PharmD, BCPS, CGP Assistant Professor, University of Colorado Departments of Clinical Pharmacy and Family Medicine Skaggs School
Introduction: Case One. Commonly used agents 4/10/2015
 Introduction: Rates of herbal medications Source NHANEs 2007 17.9% current users PMID: 22030445 Surgical population 57% of population were ever users, PMID: 16% current users 15051013 Non-pregnant rural
Introduction: Rates of herbal medications Source NHANEs 2007 17.9% current users PMID: 22030445 Surgical population 57% of population were ever users, PMID: 16% current users 15051013 Non-pregnant rural
An example of a systematic review and meta-analysis
 An example of a systematic review and meta-analysis Sattar N et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet 2010; 375: 735-742. Search strategy
An example of a systematic review and meta-analysis Sattar N et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet 2010; 375: 735-742. Search strategy
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
A C A D E M I C D E TA I L I N G C H O O S I N G W I S E LY C O N F E R E N C E O C T 2 1, PA M M C L E A N - V E Y S E Y B S C P H A R M D R
 PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
Combining Individualized Treatment Options with Patient-Clinician Dialogue
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
50% reduction in strokes
 Now, let's look at some health messages. The next three questions are about the following advertisement for an imaginary drug called Gritagrel. Gritagrel 50% reduction in strokes Gritagrel is a new pill
Now, let's look at some health messages. The next three questions are about the following advertisement for an imaginary drug called Gritagrel. Gritagrel 50% reduction in strokes Gritagrel is a new pill
Evidence Based Medicine: Articles of Diagnosis
 Evidence Based Medicine: Articles of Diagnosis Duke University School of Medicine EBM Course March 5, 2013 Jamie Fox, MD David Ming, MD Departments of Internal Medicine and Pediatrics Diagnosis Diagnostic
Evidence Based Medicine: Articles of Diagnosis Duke University School of Medicine EBM Course March 5, 2013 Jamie Fox, MD David Ming, MD Departments of Internal Medicine and Pediatrics Diagnosis Diagnostic
Vascular Diseases. Overview: Selected Slides
 Vascular Diseases Overview: Selected Slides Total deaths and change in vascular death rates
Vascular Diseases Overview: Selected Slides Total deaths and change in vascular death rates
NCI Community Oncology Research Program Kansas City (NCORP-KC)
") NCI Community Oncology Research Program Kansas City (NCORP-KC) Consent Form Study Title for Study Participants: Comparing Two Dose Levels of Bupropion Versus Placebo for Sexual Desire Official Study Title
NCI Community Oncology Research Program Kansas City (NCORP-KC) Consent Form Study Title for Study Participants: Comparing Two Dose Levels of Bupropion Versus Placebo for Sexual Desire Official Study Title
Chantix Label Update 2018
 Chantix Label Update 2018 Chantix (varenicline) Prescribing Information Chantix Prescribing Info URL and Disclaimer Please refer to the full Prescribing Information on important treatment considerations
Chantix Label Update 2018 Chantix (varenicline) Prescribing Information Chantix Prescribing Info URL and Disclaimer Please refer to the full Prescribing Information on important treatment considerations
Mixing and Matching: Layering Medications as Family Physicians
 Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
CLINICAL DECISION USING AN ARTICLE ABOUT TREATMENT JOSEFINA S. ISIDRO LAPENA MD, MFM, FPAFP PROFESSOR, UPCM
 CLINICAL DECISION USING AN ARTICLE ABOUT TREATMENT JOSEFINA S. ISIDRO LAPENA MD, MFM, FPAFP PROFESSOR, UPCM Principles of Decision Making Knowing the patient s true state is often unnecessary Does my patient
CLINICAL DECISION USING AN ARTICLE ABOUT TREATMENT JOSEFINA S. ISIDRO LAPENA MD, MFM, FPAFP PROFESSOR, UPCM Principles of Decision Making Knowing the patient s true state is often unnecessary Does my patient
Suffolk PCT Drug & Therapeutics Committee New Medicine Report (Adopted by the CCG until review and further notice)
") Suffolk PCT Drug & Therapeutics Committee New Medicine Report (Adopted by the CCG until review and further notice) This drug has been reviewed because it is a product that may be prescribed in primary
Suffolk PCT Drug & Therapeutics Committee New Medicine Report (Adopted by the CCG until review and further notice) This drug has been reviewed because it is a product that may be prescribed in primary
SMOKING CESSATION IS HARD
 POWER TO BREAK THE HOLD OF NICOTINE ADDICTION 1 SMOKING CESSATION IS HARD Most smokers try to quit 5-7 times before they are successful. 2 Why is it so hard to quit? Typical withdrawal symptoms from stopping
POWER TO BREAK THE HOLD OF NICOTINE ADDICTION 1 SMOKING CESSATION IS HARD Most smokers try to quit 5-7 times before they are successful. 2 Why is it so hard to quit? Typical withdrawal symptoms from stopping
The All Wales Medicine Strategy Group (AWMSG) is asked to support implementation of the following prescribing indicators.
 is asked to support implementation of the following prescribing indicators.") ENCLOSURE 5 APPENDIX 1 Paper presented to AWMSG in June 2006 AWPAG considered comments recorded in AWMSG minutes in July 2006 Paper subsequently updated and brought back to AWMSG for endorsement This paper
ENCLOSURE 5 APPENDIX 1 Paper presented to AWMSG in June 2006 AWPAG considered comments recorded in AWMSG minutes in July 2006 Paper subsequently updated and brought back to AWMSG for endorsement This paper
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Addiction Overview. Diane A. Rothon MD. Causes Consequences Treatments. Methadone/Buprenorphine 101 April 1, 2017
 Addiction Overview Causes Consequences Treatments Methadone/Buprenorphine 101 April 1, 2017 Diane A. Rothon MD Why? would you listen to this presentation Review the definition and neurobiology of addiction
Addiction Overview Causes Consequences Treatments Methadone/Buprenorphine 101 April 1, 2017 Diane A. Rothon MD Why? would you listen to this presentation Review the definition and neurobiology of addiction
SESSION 5 2:20 3:35 PM
 SESSION 5 2:20 3:35 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 5 2:20 3:35 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
Addiction Medicine: What s new for primary care
 Addiction Medicine: What s new for primary care Dan Vinson, MD Family and Community Medicine How to talk so our patients listen, and listen so our patients talk. 1 2 Comfortably engaging your patient in
Addiction Medicine: What s new for primary care Dan Vinson, MD Family and Community Medicine How to talk so our patients listen, and listen so our patients talk. 1 2 Comfortably engaging your patient in
Outline. What is Evidence-Based Practice? EVIDENCE-BASED PRACTICE. What EBP is Not:
 Evidence Based Practice Primer Outline Evidence Based Practice (EBP) EBP overview and process Formulating clinical questions (PICO) Searching for EB answers Trial design Critical appraisal Assessing the
Evidence Based Practice Primer Outline Evidence Based Practice (EBP) EBP overview and process Formulating clinical questions (PICO) Searching for EB answers Trial design Critical appraisal Assessing the
OBSERVATION SHEET TOPIC CLINICAL SCENARIO. OBSERVATIONS MADE (Use the skills objectives/ provider tasks to evaluate the conversation)
") OBSERVATION SHEET TOPIC CLINICAL SCENARIO OBSERVATIONS MADE (Use the skills objectives/ provider tasks to evaluate the conversation) FEEDBACK: WHAT WENT WELL FEEDBACK: THINGS TO CONSIDER DEBRIEF: Observer
OBSERVATION SHEET TOPIC CLINICAL SCENARIO OBSERVATIONS MADE (Use the skills objectives/ provider tasks to evaluate the conversation) FEEDBACK: WHAT WENT WELL FEEDBACK: THINGS TO CONSIDER DEBRIEF: Observer
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Appendix D Survey Questions
 Appendix D Survey Questions 1. Age 2. Gender 3. These are the symptoms most commonly associated with hypothyroidism. Have you had/got any of these symptoms? Fatigue Menstrual changes Fertility problems
Appendix D Survey Questions 1. Age 2. Gender 3. These are the symptoms most commonly associated with hypothyroidism. Have you had/got any of these symptoms? Fatigue Menstrual changes Fertility problems
Cardiovascular Controversies: Exploring the ACC and AHA Guidelines on the Treatment of Blood Cholesterol
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Rational Medication Use in Dementia
 Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Providing High Value Cost-Conscious Care:
 Providing High Value Cost-Conscious Care: Biostatistical Concepts You Need to Know 2012-2013 Presentation #5 0f 10 http://hvc.acponline.org/ Learning Objectives Understand that a working knowledge of basic
Providing High Value Cost-Conscious Care: Biostatistical Concepts You Need to Know 2012-2013 Presentation #5 0f 10 http://hvc.acponline.org/ Learning Objectives Understand that a working knowledge of basic
Managing Back Pain. Faculty/Presenter Disclosure
 Managing Back Pain G. Michael Allan Evidence & CPD Program, Alberta College of Family Physicians Professor, Dept Family Med, U of A. Faculty/Presenter Disclosure Faculty/Presenter: G. Michael Allan Relationships
Managing Back Pain G. Michael Allan Evidence & CPD Program, Alberta College of Family Physicians Professor, Dept Family Med, U of A. Faculty/Presenter Disclosure Faculty/Presenter: G. Michael Allan Relationships
Metabolic Syndrome. Shon Meek MD, PhD Mayo Clinic Florida Endocrinology
 Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
The Healthy User Effect: Ubiquitous and Uncontrollable S. R. Majumdar, MD MPH FRCPC FACP
 The Healthy User Effect: Ubiquitous and Uncontrollable S. R. Majumdar, MD MPH FRCPC FACP Professor of Medicine, Endowed Chair in Patient Health Management, Health Scholar of the Alberta Heritage Foundation,
The Healthy User Effect: Ubiquitous and Uncontrollable S. R. Majumdar, MD MPH FRCPC FACP Professor of Medicine, Endowed Chair in Patient Health Management, Health Scholar of the Alberta Heritage Foundation,
Smoking Cessation. Disclosures. Thank You. None
 Smoking Cessation Dr. Jamie Kellar; BSc, BScPhm, PharmD Clinician Educator Centre for Addiction and Mental Health Assistant Professor Leslie Dan Faculty of Pharmacy Disclosures None Thank You Several slides
Smoking Cessation Dr. Jamie Kellar; BSc, BScPhm, PharmD Clinician Educator Centre for Addiction and Mental Health Assistant Professor Leslie Dan Faculty of Pharmacy Disclosures None Thank You Several slides
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Smoking Cessation: Where Are We Now? Nancy Rigotti, MD
 Smoking Cessation: Where Are We Now? Nancy Rigotti, MD Director, MGH Tobacco Research and Treatment Center Professor of Medicine, Harvard Medical School nrigotti@partners.org OVERVIEW The challenge for
Smoking Cessation: Where Are We Now? Nancy Rigotti, MD Director, MGH Tobacco Research and Treatment Center Professor of Medicine, Harvard Medical School nrigotti@partners.org OVERVIEW The challenge for
Thinking about giving up. Booklet 2
 Thinking about giving up Booklet 2 This booklet is written for people who are trying to make up their mind about giving up smoking. A lot of people who smoke have done so for a long time, and like smoking.
Thinking about giving up Booklet 2 This booklet is written for people who are trying to make up their mind about giving up smoking. A lot of people who smoke have done so for a long time, and like smoking.
Journal Club Critical Appraisal Worksheets. Dr David Walbridge
 Journal Club Critical Appraisal Worksheets Dr David Walbridge The Four Part Question The purpose of a structured EBM question is: To be directly relevant to the clinical situation or problem To express
Journal Club Critical Appraisal Worksheets Dr David Walbridge The Four Part Question The purpose of a structured EBM question is: To be directly relevant to the clinical situation or problem To express
We should stop using clinical practice guidelines when it comes to teaching health care providers -
 We should stop using clinical practice guidelines when it comes to teaching health care providers - or should we? James McCormack, BSc(Pharm), Pharm D Professor, Faculty of Pharmaceutical Sciences, UBC
We should stop using clinical practice guidelines when it comes to teaching health care providers - or should we? James McCormack, BSc(Pharm), Pharm D Professor, Faculty of Pharmaceutical Sciences, UBC
Is it worth offering cardiovascular disease prevention to the elderly? Prof. Dr. Helmut Gohlke Herz-Zentrum Bad Krozingen, Germany
 Is it worth offering cardiovascular disease prevention to the elderly? Prof. Dr. Helmut Gohlke Herz-Zentrum Bad Krozingen, Germany Is it worth offering cardiovascular disease prevention to the elderly?
Is it worth offering cardiovascular disease prevention to the elderly? Prof. Dr. Helmut Gohlke Herz-Zentrum Bad Krozingen, Germany Is it worth offering cardiovascular disease prevention to the elderly?
Pulmonary Year in Review
 Pulmonary Year in Review Rachel Givelber, MD University of Pittsburgh SOM Pulmonary, Allergy, Critical Care and Sleep Medicine Rachel Givelber, MD Assistant Professor of Medicine PACCM, UPSOM Disclosures
Pulmonary Year in Review Rachel Givelber, MD University of Pittsburgh SOM Pulmonary, Allergy, Critical Care and Sleep Medicine Rachel Givelber, MD Assistant Professor of Medicine PACCM, UPSOM Disclosures
Depression Assessment and Management. John Kern MD Clinical Professor University of Washington
 Depression Assessment and Management John Kern MD Clinical Professor University of Washington Handouts Antidepressant Treatment Flowchart Managing antidepressant nonresponse handouts 2 Diagnosis PHQ-9
Depression Assessment and Management John Kern MD Clinical Professor University of Washington Handouts Antidepressant Treatment Flowchart Managing antidepressant nonresponse handouts 2 Diagnosis PHQ-9
rosuvastatin, 5mg, 10mg, 20mg, film-coated tablets (Crestor ) SMC No. (725/11) AstraZeneca UK Ltd.
 SMC No. (725/11) AstraZeneca UK Ltd.") rosuvastatin, 5mg, 10mg, 20mg, film-coated tablets (Crestor ) SMC No. (725/11) AstraZeneca UK Ltd. 09 September 2011 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
rosuvastatin, 5mg, 10mg, 20mg, film-coated tablets (Crestor ) SMC No. (725/11) AstraZeneca UK Ltd. 09 September 2011 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Antidepressant does not relieve repetitive behaviors
 NEWS Antidepressant does not relieve repetitive behaviors BY KELLY RAE CHI 16 JUNE 2009 1 / 5 Bitter pill: Negative results from clinical trials of two antidepressants, Celexa and Prozac, challenge the
NEWS Antidepressant does not relieve repetitive behaviors BY KELLY RAE CHI 16 JUNE 2009 1 / 5 Bitter pill: Negative results from clinical trials of two antidepressants, Celexa and Prozac, challenge the
Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand
 Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand Presentation outline Strengths & weaknesses of short-term risk approach Strengths &
Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand Presentation outline Strengths & weaknesses of short-term risk approach Strengths &
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Common Antidepressant Medications for Adults
 (and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
(and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
What s New, What s True, and What s Poo Part 1
 What s New, What s True, and What s Poo Part 1 Tina Korowynk and Mike Kolber PEER Group What s New? What s True? What s Poo? 1 Anti-Depressants Meta-Analysis (Network): 522 RCTs (116477 pts) Mean duration
What s New, What s True, and What s Poo Part 1 Tina Korowynk and Mike Kolber PEER Group What s New? What s True? What s Poo? 1 Anti-Depressants Meta-Analysis (Network): 522 RCTs (116477 pts) Mean duration
#s in EVERYDAY LIFE OUTLINE Class 3: Medical and Health Studies Ricki Lewis
 #s in EVERYDAY LIFE OUTLINE Class 3: Ricki Lewis (RALEWIS@NYCAP.RR.COM) The slides for this presentation are unavailable. We provide herewith A detailed summary of the material presented. A preliminary
#s in EVERYDAY LIFE OUTLINE Class 3: Ricki Lewis (RALEWIS@NYCAP.RR.COM) The slides for this presentation are unavailable. We provide herewith A detailed summary of the material presented. A preliminary
Section 4 Decision-making
 Decision-making : Decision-making Summary Conversations about treatments Participants were asked to describe the conversation that they had with the clinician about treatment at diagnosis. The most common
Decision-making : Decision-making Summary Conversations about treatments Participants were asked to describe the conversation that they had with the clinician about treatment at diagnosis. The most common
Benzodiazepines: risks, benefits or dependence
 Benzodiazepines: risks, benefits or dependence A re-evaluation Council Report CR 59 January 1997 Royal College of Psychiatrists, London Due for review: January 2002 1 Contents A College Statement 3 Benefits
Benzodiazepines: risks, benefits or dependence A re-evaluation Council Report CR 59 January 1997 Royal College of Psychiatrists, London Due for review: January 2002 1 Contents A College Statement 3 Benefits
Cost-effectiveness of smoking cessation in Australia with varenicline, a novel pharmacotherapy
 Cost-effectiveness of smoking cessation in Australia with varenicline, a novel pharmacotherapy Alissa Brown 1, Kate Webb 1, Hansoo Kim 1, Danny Liew 2 1 Pfizer Australia Pty Ltd 2 St Vincent s Hospital,
Cost-effectiveness of smoking cessation in Australia with varenicline, a novel pharmacotherapy Alissa Brown 1, Kate Webb 1, Hansoo Kim 1, Danny Liew 2 1 Pfizer Australia Pty Ltd 2 St Vincent s Hospital,
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
FREEDOM FROM SMOKING INFORMATIONAL SESSION
 FREEDOM FROM SMOKING INFORMATIONAL SESSION How to Quit Tobacco Presented by Laura Frick, MSW Health Promotions Coordinator American Lung Association of the Plains-Gulf Region AMERICAN LUNG ASSOCIATION
FREEDOM FROM SMOKING INFORMATIONAL SESSION How to Quit Tobacco Presented by Laura Frick, MSW Health Promotions Coordinator American Lung Association of the Plains-Gulf Region AMERICAN LUNG ASSOCIATION
Section 4 - Dealing with Anxious Thinking
 Section 4 - Dealing with Anxious Thinking How do we challenge our unhelpful thoughts? Anxiety may decrease if we closely examine how realistic and true our unhelpful/negative thoughts are. We may find
Section 4 - Dealing with Anxious Thinking How do we challenge our unhelpful thoughts? Anxiety may decrease if we closely examine how realistic and true our unhelpful/negative thoughts are. We may find
Mapping the Informed Health Choices (IHC) Key Concepts (KC) to core concepts for the main steps of Evidence-Based Health Care (EBHC).
 Key Concepts (KC) to core concepts for the main steps of Evidence-Based Health Care (EBHC).") KC No KC Short Title KC Statement EBHC concept EBHC sub concept EBHC statement EBHC Step Reported 1.01 Treatments can harm Treatments may be harmful Explain the use of harm/aetiologies for (rare) adverse
KC No KC Short Title KC Statement EBHC concept EBHC sub concept EBHC statement EBHC Step Reported 1.01 Treatments can harm Treatments may be harmful Explain the use of harm/aetiologies for (rare) adverse
Smoking. know the facts
 Smoking know the facts DID YOU KNOW? In Northern Ireland, 2,300 people die each year from smoking-related illness more than six people per day. Why stop? Smoking is the main cause of illness and early
Smoking know the facts DID YOU KNOW? In Northern Ireland, 2,300 people die each year from smoking-related illness more than six people per day. Why stop? Smoking is the main cause of illness and early
Psychiatric Consultant Role in Collaborative Care Sept 12, 2013
 New York State Collaborative Care Initiative Psychiatric Consultant Role in Collaborative Care Sept 12, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Psychiatric Consultant Role in Collaborative Care Sept 12, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
MEDICINES ADHERENCE The Role of the Pharmacist
 BROUGHT TO YOU BY MEDICINES ADHERENCE The Role of the Pharmacist Developed by Pfizer 15 May, 2017 This learning module is intended for UK healthcare professionals only. Job code; PP-GEP-GBR-0682. Date
BROUGHT TO YOU BY MEDICINES ADHERENCE The Role of the Pharmacist Developed by Pfizer 15 May, 2017 This learning module is intended for UK healthcare professionals only. Job code; PP-GEP-GBR-0682. Date