Pediatric Mood Dysregulation: Irritability, Disruptive Mood Dysregulation Disorder, and Bipolar Disorder
|
|
|
- Julianna Parks
- 6 years ago
- Views:
Transcription
1 Pediatric Mood Dysregulation: Irritability, Disruptive Mood Dysregulation Disorder, and Bipolar Disorder William P. French, MD PAL Conference Everett, WA February 10, 2018
2 Disclosure of Potential Conflicts Source Research Funding Books, Intellectual Property Advisor/ Consultant Speakers Bureau Employee In-kind Services (example: travel) Stock or Equity Honorarium or expenses for this presentation or meeting Disclosure Pfizer, Shire, & Supernus Pharmaceuticals none none Symposia Medicus none Symposia Medicus none Symposia Medicus
3 Today s agenda Irritability Disruptive Mood Dysregulation Disorder Severe Mood Dysregulation Pediatric Bipolar Disorder Yes, its controversial and rare, but it does exist DSM 5 diagnostic criteria Assessment Medication and non-medication treatments Take home message
4 Key Points in Today s Presentation Irritability and/or mood swings don t equal pediatric bipolar disorder (PBD). Irritability (a potential presenting complaint in bipolar mania) is a non-specific, common symptom present in many childhood psychiatric illnesses. Multiple factors have led to a significant increase the diagnosis of PBD, leading to inappropriate prescribing of medications (e.g., antipsychotics) with serious side effect burdens. NIMH research has worked to clarify unique neurobiological substrates and clinical courses in youth presenting with chronic vs. episodic irritability PBD, while a zebra and not a horse does occur in youth, especially in the context of a strong family history. Youth presenting with acute mania, ideally, should be referred for hospitalization and to specialists, such as child and adolescent psychiatrists (CAPs).

5 Irritability For mental health providers, our version of fever in children with psychiatric issues
6 What s Up With All the Irritability? Irritability can be defined as an elevated proneness to anger relative to peers Involves dysfunction of reward system: frustrative nonreward and threat system: bias toward perception of environmental threats and relative default to fight/attack (versus freezing or fleeing), which leads to maladaptive emotional and behavioral responses These two systems, when dysfunctional, can potentiate each other in situations where both frustrative nonreward and perception of threat exist Neural substrates such as PFC, striatum, amygdala, etc. are implicated

7 What Going On in My Kid s Brain?
 PTSD Anxiety/OCD ODD Conduct Disorder Substance Use ASD rigidity Attachment Disorder Borderline Personality Disorder/Traits ADHD with")
8 Differential Diagnoses With Mood Dysregulation & Irritability Bipolar Disorder Depression (esp. kids) PTSD Anxiety/OCD ODD Conduct Disorder Substance Use ASD rigidity Attachment Disorder Borderline Personality Disorder/Traits ADHD with emotional lability Complex Developmental Trauma DMDD
9 But There Are Ways to Tease This Apart Disorder ADHD with emotional lability ODD Disruptive Mood Dysregulation Disorder Depression Bipolar Disorder Definition ADHD + problems with mood regulation Angry/Irritable Argumentative/ Defiant/Vindictive Recurrent temper outbursts Persistently irritable and angry between outbursts Depressed mood, loss of interest, irritable mood, poor sleep BP I: Mania BP II: Mania + Depression BP Other Specified BP Unspecified Cyclothymia Mood Quality Easily irritated, low frustration tolerance, excitable Irritable Loses temper Easily annoyed Angry and resentful Persistently irritable or angry mood Extreme temper outbursts Irritability (in kids) or depressed mood for most of the day Persistent elevated, expansive, or irritable mood Typical Age of Onset Same as ADHD: preschool to school-age Bimodal: early onset with ADHD or later onset during adolescence By definition, should not be diagnosed before 6 but should be present by 10 yrs of age Early to late adolescence Mid to late adolescence Associated Features Distractible, overactive, impulsive, poor sleep at times Difficult temperament, low frustration tolerance, substance use May co-occur with ADHD with depressive disorders May present with psychosis Increase in energy, decreased need for sleep, grandiosity, distractibility, risk taking behavior Prevalence 38 to 75% of kids with ADHD 2% to 16% 1-3%?? 11 percent of youth by age % Exclusions Cannot occur exclusively during psychosis Concurrent DMDD Concurrent ODD (if both, choose DMDD); and BPD Cannot have a history of (hypo) mania Substance-induced BPD; and due to medical condition
10 Chronic versus Episodic Irritability Objective: Test validity of distinction between chronic and episodic irritability. (Central debate in pediatric bipolar) Method: Community sample of 776 children and adolescents interviewed at 3 points in time (T0, T2y, T7y). Irritability rating scales used to tease out chronic versus episodic irritability. Association with age, gender and diagnosis were examined. (Liebenluft et al, 2006)
11 Irritability and Later Psychopathology Chronic irritability at TI - associated with ADHD at T2 and depression at T3 Episodic Irritability associate with simple phobia at T2 and mania at T3 Conclusions: - Episodic and chronic irritability are distinct constructs. - Episodic irritability is associated with bipolar disorder and confers higher risk of future manic episodes than chronic irritability. (Liebenluft et al, 2006)
12 Chronic vs Episodic Irritability Those with episodic irritability were more likely than those with chronic irritability to have: A parent diagnosed with Bipolar Disorder Experienced elation and/or grandiosity More symptoms of mania Psychotic symptoms Had a depressive episode Made a suicide attempt (Liebenluft et al, 2006)
13 Disruptive Mood Dysregulation Disorder Symptoms in search of a diagnosis
14 Disruptive Mood Dysregulation D/O A. Severe recurrent temper outbursts manifested verbally and/or behaviorally that are grossly out of proportion in intensity or duration to the situation or provocation. B. Temper outbursts are inconsistent with developmental level. C. Temper outbursts occur, on average, > 3X per week. D. The mood between temper outbursts is persistently irritable or angry most of the day, nearly every day, and observable by others E. Criteria A-D have been present for >12 mo. Throughout that time, the individual has not had a period > 3 consecutive months without all of the symptoms in A-D. F. Criteria A and D are present in at least two of three settings and are severe in at least one of these. G. Dx should not be made 1 st before age 6 or after age 18. H. Age at onset of Criteria A-E is before 10 years.
15 Disruptive Mood Dysregulation D/O I. There has never been a distinct period lasting more than one day during which the full symptom criteria, except duration, for a manic or hypomanic episode have been met. J. The behaviors do not occur exclusively during an episode of major depressive disorder and are not better explained by another mental disorder. K. The symptoms are not attributable to the physiological effects of a substance or to another medical or neurological condition. Note: This diagnosis cannot co-exist with Oppositional Defiant Disorder or Bipolar Disorder, though it can co-exist with ADHD, Conduct Disorder, and Substance Use Disorders.
16 BTW, How Did We Get DMDD as a New Diagnosis?
17 Severe Mood Dysregulation (SMD) Clinical syndrome not a diagnosis (3.3% lifetime prevalence ages 9-19) Served as research framework for DMDD chronically irritable children whose diagnosis is in doubt. (This is the type of kid, who would previously, but hopefully less frequently now, is diagnosed with Bipolar, NOS) IS real and confers risk of psychopathology down the line, but NOT for bipolar disorder Presence of SMD increases risk of depressive disorder and GAD at 20 year follow-up. Stringaris et al, 2010
18 Core Features of SMD Chronic: persistent symptoms; no distinct episodes of mania Unusually intense, frequent, prolonged negative reactivity (e.g., temper tantrums) to negative emotional stimuli > 3x/wk Baseline mood between tantrums: anger/sadness 3 or more ADHD-like Hyperarousal symptoms: insomnia, agitation, distractibility, racing thoughts or flight of ideas, pressured speech, and intrusiveness. Very impairing Leibenluft et al, 2003
19 SMD Definition (Leibenluft) Age 7-17, onset by 12 Anger or sadness at least half day most days Hyperarousal Symptoms (differs from DMDD) Increased reactivity to negative emotional stimuli (tantrum, rage, aggression) 12 months in length Multiple settings (1 severe) No cardinal Bipolar Sx: expansive mood, grandiosity, episodic sleep deficits
20 Is SMD related to Bipolar? Follow-up studies of SMD from age 10 to 18 generally show subsequent incidence of MDD at age 18 far more than BD Another study showed that after an average of 2.4 years, only 1.2% of SMD patients experienced a manic episode, compared to 62.4% of patients with BD Parental history for Bipolar far greater in BD group (33%) than SMD group (2.7%)
21 Data from the Smokey Mountain Cohort: Parents of BPD youth more likely to have BD than are parents of SMD children % BPD BPD (n=34) SMD (n=30) OR 15.82, CI , p=.01; Chi-square p<.01 Brotman et al, submitted
22 Can SMD Be Treated? National Institute of Mental Health (NIMH) A Controlled Trial of Serotonin Reuptake Inhibitors Added to Stimulant Medication in Youth With Severe Mood Dysregulation This study will evaluate the effectiveness of the stimulant medication methylphenidate (MPH) when combined (or not combined) with the antidepressant citalopram (Celexa) in treating symptoms of SMD in children and adolescents
23 Not-Bipolar Take-Home Message #1 The diagnosis of bipolar disorder should be reserved for children who have clear episodes of mania. Elation during mania is common in children with bipolar disorder, so be skeptical of presentations with only a history of irritability, especially if the parent report is that irritability is a baseline condition Children with severe, chronic irritability and hyperarousal are at high risk for major depression or anxiety disorders, not necessarily bipolar disorder.
24 Not-Bipolar Take-Home Message #2 Currently, there is no single diagnosis for chronically dysregulated or irritable kids. Evidence is more suggestive of current and/or future depressive or anxiety disorders Kids with severe, non-episodic irritability differ from those with bipolar in course, family history, and research findings Still a major role for parent support/training and mental health support. These are ill kids, who can be draining and are high risk There can be a role for medications to decrease maladaptive aggression and affective instability
25 Pediatric Bipolar Disorder Horses move over, bring on the Zebra
26 But First a Little More About the Controversy
27 Bipolar Is (maybe was) A Hot Topic Bipolar disorder in kids is/has been much talked about Child Anxiety Illness on Google About 31,000,000 hits in 2014 down to 28.7 million on 1/14/2018 Child Bipolar Illness on Google About 40,100,000 hits down to 6.3 million on 1/14/2018 (French, 3/26/2014) Child anxiety disorders are actually about 10 times more common than child bipolar disorder 40 fold increase in office visits for child bipolar disorder from 1994 to 2003 (Also 40-fold increase in diagnosis.) National Center for Health Statistics
28 Frequency of Childhood Bipolar Very controversial Some popular books by well established clinicians assert a very high incidence The Bipolar Child by Papolos and Papolos Assert 1/3 of all children with ADHD States about 6% of all children are bipolar Is Your Child Bipolar by McDonnell and Wozniak States more than 3 million US kids have it Based on their estimates, incidence is 4%.
29 Bipolar Disorder Frequency Depends On Where You Look Prevalence of true adolescent bipolar 0.6% of high school students 1% in general outpatient practice 6 % of child psychiatry outpatients 22% incarcerated adolescents 26-34% of child psychiatry inpatients presenting with manic symptoms ( CDC survey of discharge diagnosis) Youngstrom et al, CAPC Vol 18
30 Quoted Child Rates Don t Match Our Adult Knowledge Adult Lifetime prevalence rates of bipolar disorder 1 to 2% Greater diagnostic certainty with adults Bipolar disorder is a lifelong diagnosis need plausible explanation of what happens to these kids if pediatric bipolar is 3-6X > adult bipolar Lessons from Great Smoky Mountain data set child bipolar NOS bipolar adult Kids with bad mood swings cannot all have true bipolar disorder
31 Why is diagnosis so challenging? Symptom overlap + high rates of co-morbidity Confounding developmental issues Environmental influences Limited ability of (many) children to verbalize emotions Many different expert opinions Influence of popular media/pharmaceutical industry Requires extensive history assessment of both current symptoms and past episodes (subject to recall bias)
32 Rapid Cycling Controversy Typical adult pattern is episodic. Rapid cycling is rare in adult bipolar populations Kids are more reactive and more common to get story of rapid cycling Consider rapid cycling in kids if there is no trigger identifiable for the mood changes Where many episodes become static, chronic mood state is controversial. ADHD plus irritability should not generate a bipolar diagnosis Youth with BP do spend more time cycling and have more changes in mood polarity than adult populations. (Birmaher et al, 2006)
33 DSM 5 Bipolar Diagnostic Criteria
34 DSM-5 defines a manic episode as: A distinct period of abnormally and persistently elevated, expansive, or irritable mood, and abnormally and persistently increased goal-directed activity or energy, lasting at least 1 week and present most of the day, nearly every day (or any duration if hospitalization is necessary). Manic symptoms include inflated self-esteem or grandiosity, decreased need for sleep, rapid pressured speech, flight of ideas, racing thoughts, or excessive involvement in activities that have a high potential for painful consequences
35 DSM-5 defines hypomania as: A episode similar to a manic episode, except the episode is not severe enough to cause a marked impairment in social or occupational functioning. Mood and functional disturbances are observable to others, and minimum duration of symptoms is 4 days
36 DSM-5 Bipolar and Related Disorders To enhance the accuracy of diagnosis and facilitate earlier detection, Criterion A for manic and hypomanic episodes now requires, not only persistently elevated, expansive, or irritable mood, but also persistently increased goal-directed activity or energy DSM-IV diagnosis of Bipolar I Disorder, mixed episode, has been removed. Instead, with mixed features, has been added as a specifier; applied to episodes of mania or hypomania when depressive symptoms exist, & vice-versa Other specifiers: With Anxious Distress With Melancholic Features With Seasonal Pattern (Seattle?) With Rapid Cycling (4 in 1 yr)
37 DSM-5 Bipolar and Related Disorders Other Specified Bipolar and Related Disorder Specify particular conditions for other specified bipolar and related disorder, including categorization for individuals with a past history of a major depressive disorder who meet all criteria for hypomania except the duration criterion (i.e., at least 4 consecutive days). A second condition may be that too few symptoms of hypomania are present to meet criteria for the full bipolar II syndrome, although the duration is sufficient at 4 or more days.
38 Other Specified Bipolar and Related Disorder Recurrent hypomanic episodes w/o depressive symptoms Short-duration (< 4 days) hypomanic episodes and MDE Short-duration cyclothymia (less than 24 months in adults and 12 months in children) You document this by specifying Other and then the reason (e.g., short-duration cyclothymia )
39 Unspecified Bipolar and Related Disorder Patient presents with symptoms characteristic of a bipolar disorder and related disorder that causes significant impairment, but does not meet full criteria for any of the disorders in the bipolar diagnostic class Unlike as is done in the Other Specified Bipolar and Related Disorder, here the clinician chooses not to specify the reason the criteria are not met Recommended for presentations where there is insufficient information to make a more specific diagnosis (e.g., emergency room setting)
40 Unspecified (Formerly: Bipolar Disorder, NOS) BD Contributes to the bipolar epidemic Label often given to impulsive, aggressive kids with pervasive irritable mood Prognosis could be normal, MDD, or (rarely) true bipolar Diagnosis confused with: ADHD Depression Abuse (current and PTSD) Anxiety Disorders Disruptive Behaviors Disorders (ODD irritable subtype) Reactive Attachment Disorder Intermittent Explosive Disorder
41 Why are/were these unspecified/nos Bipolar, NOS so commonly used? Broad category/catch-all Only recently another more suitable diagnosis that captures complex behavioral picture (SMD, DMDD) Sounds better to us than I don t know Justifies the medication treatment options If we give a child medicine as if bipolar, parents often report improvement Bipolar medicines have many non-specific effects All can potentially decrease impulsivity and aggression
42 However, Some Youth with BPD, NOS Will Transition To Bipolar I or II Over Time 140 children who met operationalized criteria for BP- NOS Diagnostic conversion to BP-I or BP-II occurred in 63 subjects (45%) Median time from intake to conversion was 58 weeks First- or second-degree family history of mania or hypomania was the strongest baseline predictor of diagnostic conversion (p.006) Children and adolescents referred with mood symptoms that meet operationalized criteria for BP-NOS, particularly those with a family history of BP, frequently progress to BP-I or BP-II Axelson DA et al. J. Am. Acad. Child Adolesc. Psychiatry, 2011;50(10):
43 What to Look For When Considering Bipolar as a Potential Diagnosis?
44 What To Do? What role should a primary care provider take regarding the question of child bipolar disorder? Psychoeducation? Referral? Treatment? How do you assess for childhood bipolar disorder? When does it make sense to Wait? Prescribe a mood stabilizer? Refer to a therapist? Refer to a (child and adolescent) psychiatrist?
45 Diagnostic Perspective Experience with adult mania helps but can be challenging to translate to kids Compare child to a prototypic manic patient Pressured speech -- not just talkative Having no doubt about their grandiose ideas -- impaired reality testing/lack of insight) Thought process is fast and jumping around Episodes that most commonly last days not minutes or hours Little need for sleep (versus poor sleep.)
46 Look for Hallmark Symptoms Increased specificity More likely bipolar Elation Hyperactivity Grandiosity Hypersexuality Decreased need for sleep
47 What about Family History? Mom says she has been diagnosed with bipolar and his uncle is bipolar, just like him Avoid overcalling a positive family history many adults who call themselves bipolar may not have that illness first degree relative bipolar disorder, increases OR by 5 second degree relative bipolar, increase OR by 2.5 given a generous prevalence of 2% bipolar in the population, most children of a bipolar parent (~90%) will not have bipolar disorder Youngstrom E & Duax J, JAACAP 44:7, 2005
48 Look for Episodes and Patterns Individual episodes represent a clear departure from baseline with hallmark symptoms Hopefully, the presence of hallmark symptoms will help distinguish irritable mania from irritability due to other causes The correct mood diagnosis (and treatment) requires establishing the pattern of mood episodes, not just presenting (current) episode
49 Remember to keep your differential broad. Consider the large differential for each of these Mania symptoms in kids: Distractible Indiscretions/risk taking Grandiose Flight of ideas/racing thoughts Activity (goal directed) increase Sleep need decreased Talkative (pressured speech) Which can mimic ADHD symptoms, for example?
50 Manic symptoms versus ADHD (Kowatch et al, 2005) Symptom ADHD PBD* Irritability 72% 98% Accelerated Speech 82% 97% Distractibility 96% 94% Unusual Energy 95% 100% * Pediatric Bipolar Disorder
51 Bipolar Assessment--questions Question Relevance Flag? Is there a confirmed history of BPD in a parent or (twin) sibling? Is there a history of increased energy and decreased need for sleep? Is there a history of episodic irritability? % that patient will develop a BPD disorder This could represent a history of hypomania Without evidence of clear environmental trigger and with evidence of additional cardinal changes from baseline, this could represent a risk for BPD Red Yellow Yellow Is there evidence of chronic irritability only? Does the patient have a history of early onset depression or have a history of previous psychotic symptoms presenting early in the course of a depressive illness? Does the patient have any evidence of irritability, activation, or intolerability of previous trials on SSRIs Is there a seasonal pattern to previous mood/depressive episodes? Research indicates that these patients are more likely at risk for a depressive or anxiety disorder? May increase likelihood of developing bipolar Could any of these responses to an SSRI trial represent switching? Does this represent episodic mood disturbance consistent with BPD, especially if there is some evidence of hypomania/irritability during seasonal swings? No Yellow Yellow Yellow
52 Bipolar Diagnostic Aides Rating Scales Young Mania Rating Scale Useful for monitoring symptoms over time Not a diagnostic tool (very low specificity) DISC or KSADS Used in research, have flaws Impractical for your office practice Rating scales are too misleading to recommend for diagnostic use and are intentionally excluded from the PAL guide
53 Looking back at adult bipolar. Several studies have asked adults with bipolar about onset of their symptoms retrospectively Bipolar adults look back and note symptoms became bipolar-like in their teen years (50-66%) Many bipolar adults had major depression episodes as children The younger the child s first major depression, the more likely bipolar disorder is in the future
54 Bipolar Treatment
55 What if a Bipolar Child Really is Bipolar? Though rare in a PCP practice, becomes more likely the older the child. Typical pattern is early onset depression, and during teenage years getting first symptoms of mania. Expect mood episodes. COBY study established validity of episodic course. Assemble a team. Real deal bipolar disorder is a big problem and requires multi-modal treatment.
56 Course Of True Bipolar Disorder If clearly manic, strongly recommend hospitalization and/or referral to CAP Suicidalilty up to 15% eventually complete suicide Substance Abuse in up to 60% Anxiety disorders in up to 50% Psychotic features in up to 50% Relationship Disruptions Work Disruptions Hospitalizations Stern TA and Herman JB, 2004; Brent et al, 1988, 1993
57 Bipolar Treatment If clear manic episodes, strongly recommend referral to child psychiatrist Management difficult because: High rate of substance abuse High rate of medication non-compliance Even with medication, recurrences happen High rates of family disruption from the illness Suicidal behavior is common Brent et al, 1988, 1993
58 If No Child Psychiatrist Can Assume Care, Then What? Get collateral information to help establish correct diagnosis Strongly advise against rushing to offer diagnosis of bipolar disorder. This may require separate/designated appointment(s) with caregivers and/or patient to get sufficient history Seek consultant advice on medication (PAL) Advocate for multimodal care Specialist for medication management Parent/caregiver involvement School support (IEP if attendance/performance impacted) Individual support
59 Bipolar Treatments (for when you are left holding the bag) Medication management (acute and maintenance) Safety monitoring and crisis planning Individual Support (symptom management, coping skills, adherence monitoring, psychoeducation) Family support (psychoeducation, risk assessment/response, adherence/relapse prevention) Lifestyle coaching and support (stress mitigation, sleep hygiene, drug/alcohol risks, exercise, interpersonal and social rhythm therapy)
60 Resources for Non-pharmacologic Interventions Boris Birmaher, MD: New Hope for Children and Teens with Bipolar Disorder. Three Rivers Press, New York, 2004 David Miklowitz PhD: The Bipolar Disorder Survival Guide, 2 nd edition. The Guilford Press, 2011 Ellen Frank PhD:Treating Bipolar Disorder: A Clinician's Guide to Interpersonal and Social Rhythm Therapy. The Guilford Press, 2005 Mary Fristad PhD: Interpersonal and Social Rhythm Therapy:
61 Bipolar Medications
62 Classes of Medication Mood Stabilizers Antipsychotic Medications Anticonvulsants (AEDs) Depression Medications (SSRIs, SNRI) Sleep Aides
63 What Is A Mood Stabilizer? Includes both atypical anti-psychotics and anti-epileptic drugs (AEDs) Generic term clarify what they mean when taking history and what you mean when proposing treatment. FDA does not recognize this term As relates to treatment of bipolar disorder, ideally treats both depressive and manic episodes as well as prevents recurrence of mood episodes. Since no one compound does this well, multiple meds are often used together (but little evidence base to support it)
64 Mood Stabilizers are Non-Specific to PBD Maladaptive aggression Intellectual Disability (lithium, risperidone) Autism (risperidone, aripiprazole) Conduct Disorder (risperidone, valproic acid, lithium) ADHD with impulsive aggression (risperidone) Seizure Disorders kindling hypothesis; neuroprotective effects in mood disorders (lithium) Depression (aripiprazole, quetiapine, lamotrigine) Psychosis (primary, mood disorder, delirium) OCD (refractory) PTSD (intrusive thoughts)
65 Bipolar Medications Pearls Look for a family history of positive response to a specific medication/medication class Classic mania: Acutely: Lithium +/- neuroleptic; add neuroleptic if severe mania and need quick response and/or if the patient is psychotic and then try to remove neuroleptic over time Mixed states/rapid cycling/seizure D/O: Depakote Bipolar depression: Lamictal; second choice Latuda BPD with severe agitation/anxiety: add BDZ or other anxiolytic Avoid SSRI if possible even when very depressed; if have to add: Wellbutrin Neuroleptic choices more mania : Risperdal > Abilify > Zyprexa = Seroquel Most kids will need to be on > 1 med to adequately treat.
66 Pharmacotherapy: Evidence-base Medication Bipolar I, Manic, Mixed, w/o Psychosis Lithium* A A Divalproex* A A Carbamazepine B B Oxcarbazepine A (no benefit) C Bipolar I, Manic, Mixed, w/ Psychosis Topiramate B (trial discontinued) B (trial discontinued) Lamotrigene* B B Risperidone* B B Olanzapine B B Quetiapine B; D B Ziprasidone B B Aripiprazole B ND A=Placebo-controlled, randomized trials; B=Open child/adolescent trials and retrospective analyses; C=child/adolescent case reports or panel consensus; D=as adjunctive Tx; ND=no data; * Randomized clinical trials in progress
67 Second-Generation Antipsychotics (SGAs)
68 Atypical Antipsychotics in the treatment of Pediatric Bipolar FDA approval for pediatric use: Acute Mania, ages 10 years and older Risperidone, Aripiprazole, Quetiapine, Olanzapine (13 and older), Ziprasidone, Asenapine
69 Risks common to all Atypical Antipsychotics (Correll, JAACAP. 2008) Sedation (olanzapine, quetiapine) Tardive Dyskinesia (0.4% annual incidence) Increased Cholesterol/ Triglycerides (olanzapine) Akathisia (aripiprazole) (youth<adults) Increase glucose (olanzapine, quetiapine) EPS (risperidone) Lower seizure threshold (mildly) QT interval change (~20ms for ziprasidone) Weight gain (olanzapine > quetiapine, risperidone >the rest) Neuroleptic Malignant Syndrome
70 SGAs: Adverse Effects Common Side Effects (>10%) Weight gain Muscle rigidity Parkinsonism Constipation Dry mouth Dizziness Somnolence/fatigue Less Common Side Effects Tremors Nausea or abdominal pain Akathisia (restlessness) Headache Agitation Orthostasis Elevated glucose Elevated cholesterol/triglycerides Notable Rare Reactions ( 2% ) Tardive Dyskinesia Neuroleptic Malignant Syndrome Lowered blood cell counts Elevated liver enzymes Prolonged QT interval Tachycardia
71 SGAs: Monitoring Monitoring recommendation Height and weight Fasting blood sugar Fasting triglyceride/cholesterol Screen for movement disorder or tardive dyskinesia CBC with Diff BP/Pulse Cardiac history Determine if treatment response Frequency Suggestion At baseline and at each follow-up (at least every 6 months) At least every 6 months At least every 6 months At least every 6 months Once to catch if any suppression, a few months after initiation At least once after starting medication At baseline, get EKG if in doubt about risk from a mild QT increase Repeat disorder specific rating scale(s) until remission is achieved. Increase at 4-6 week intervals if insufficient benefit.
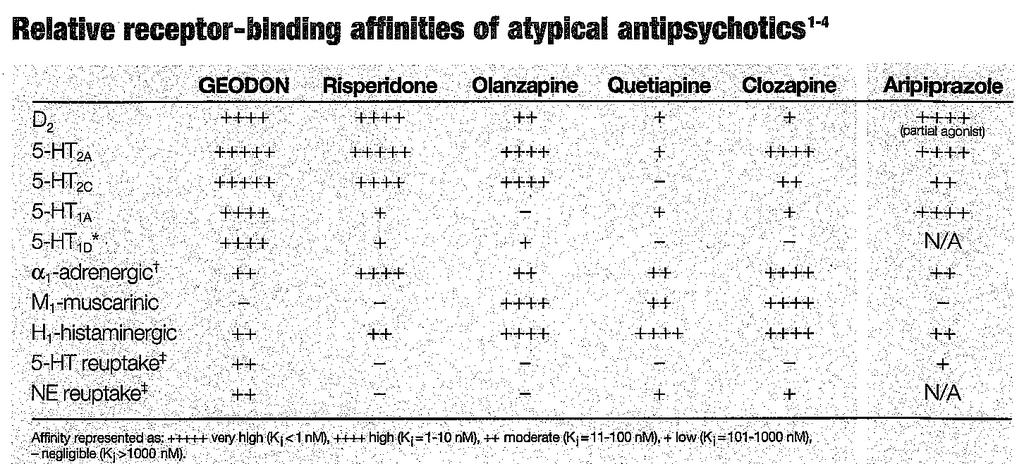
72 Atypical Heterogeneity
73 Adverse and Therapeutic Effects of Occupancy and Withdrawal (Correll, JAACAP. 2008)
74 Risperidone (Risperdal) PROS QD-BID dosing (T½ = 20 hours) FDA for mania > 10 years old, irritability/aggression in ASD Multiple dosage forms (liquid, dissolving tab, tabs, depot) Low doses (<2 mg) adequate for non-specific aggression TD incidence reported less than 0.5% CONS Weight gain and sedation common Hyperprolactinemia risk Relatively high rates of dystonic reactions/eps
75 Aripiprazole (Abilify) PROS QD-BID dosing ( T½=75 hrs) but kids may do better BID FDA for mania (>10 yrs) and limited RCT support Mixed agonist/antagonist (less dystonia/eps) Often less sedation CONS Limited dosage forms Misperception of less weight gain/metabolic SE Agitation/activation not uncommon Higher rates of akathisia Long T ½ -may take longer to see impact of changes
76 Quetiapine (Seroquel) PROS Lower potency - may be experienced as milder FDA approval (>10 years old) limited RCT evidence Effective anxiolytic Cross indication for bipolar and unipolar depression CONS Short half-life (T½ = 6 hours); multiple daily dose; mixed results w/ XR preparation Large tablets - may be hard to swallow Effective sleep aide (high risk, high cost sleep aide) Cataract risk
77 Olanzapine (Zyprexa) PROS QD-BID dosing (T½ = 30 hours) FDA approval (> 13 years) and limited RCT evidence Multiple dosage forms (tablets, oral disintegrating, IM) Very effective for acute stabilization of mania and psychosis CONS Weight gain (dose related, less of plateau than others) High rates of metabolic side effects Sedation common
78 Ziprasidone (Geodon) PROS Often less sedating Most weight neutral Fewer metabolic side effects Unique receptor profile CONS BID-QID dosing (T ½ = 7 hrs) No FDA approval for pediatric mania No pediatric RCT support Concern for EKG changes has lowered its usage
79 Anticonvulsants and Lithium
80 Lithium PROS FDA approved for mania >12 years Some evidence in refractory depression Anti-suicide properties Some EB dosing guidelines (adjust for age/gfr) CONS Narrow therapeutic index (close monitoring for toxicity w/ illness/dehydration; no NSAIDs) Usually best in combination, so committing to polypharmacy if you start here (best w/ atypical or VPA) SE in therapeutic range similar to early toxicity (tremor, diarrhea) SE often limit use (weight gain, acne, GI); HS dosing can minimize Hard to predict who will respond No evidence for maintenance treatment /slow anti-manic effects
81 Lithium In adults, best documented treatment for classic manic depressive illness Open trials support lithium for pediatric bipolar, either as monotherapy or with other mood stabilizers or antipsychotics Risperidone more effective than lithium or valproate for pediatric mania (ages 6 15 years) (Geller et al., 2012) Lithium FDA Approved for Youth 12 years of age or older with Bipolar, based on adult literature
82 Valproic Acid (Depakote) PROS Single daily dosing can be effective (Depakote ER) Can be useful for maladaptive/non-specific aggression Studies suggest helpful, usually in combination CONS Requires blood draws (levels, LFTs, amylase, CBC) Risk of hepatotoxicity (highest in first 6 months) High side-effect burden (weight gain, GI, tremor, sedation, rash) Less ideal for females (risk of birth defects (NTD), PCOS)
83 Depakote How well does it work? Fair, usually works best in adolescents in combination with an antipsychotic (better than either one alone) Some RCT s have suggested that it works better than lithium on acute manic symptoms Broad effects: also used for externalizing behavior disorders, conduct disorder Lost in head-to-head trial with quetiapine Similar long-term stabilizing effect to Lithium after stabilization with both divalproex and lithium DelBello MP et al, 2002, 2006, Bowden C et al, 2004, Rana M et al, 2005, Findling, R et al 2005
84 Carbamazepine (Tegretol) PROS Some empirical supports for aggression 2 Open trials Similar response rates as Li and VPA (38%) (Kowatch et al, 2005) CONS Drug/drug interactions (OCPs, Lithium) Blood draws to check levels (auto-induced metabolism) Weak evidence of benefit in bipolar (McClellan and Werry, 1997) Risk of aplasia and liver failure
85 Lamotrigine (Lamictal) PROS Bipolar depression treatment Less sedation and lower side effect profile in general CONS Not helpful for manic phase Requires monitoring of CBC and liver function Significant rash risk Slow titration (age >12)
86 Oxcarbazepine (Trileptal) PROS FDA approval for adults bipolar disorder Weight neutral Less risks/side effects than carbamazepine Monitoring of levels not required CONS Levels do not correlate well with efficacy or toxicity Negative adolescent bipolar trial (Cochrane Review. Vasudev et al. 2008) Hyponatremia not uncommon
87 Sleep Needs to Happen
88 Sleep Aides Lifestyle changes: limit caffeine, exercise, no drugs/alcohol Sleep hygiene education Melatonin (mild sleep aide, can help regulate sleep cycle) Anti-histamines Trazodone Benzodiazepines
89 In Summary
90 Bipolar Take-Home Message Diagnosis of bipolar disorder made with relative confidence in the presence of manic (Bipolar I) or hypomanic (Bipolar II) episodes. It gets tricky after that Mood episodes involve distinct change from baseline with alternations in behavior and evidence of impairment Bipolar diagnosis is a serious diagnosis that has a lifelong course and many management challenges True bipolar has high rates of morbidity and mortality If suspected, strongly recommend involving a child and adolescent psychiatrist If you, as PCP, are playing central role in management, check-in frequently to monitor side effects of medication(s) and surveillance of mood symptoms
91 At PCP level, recommend. keeping in mind many possible causes of mood swings and irritability resisting temptation to label impulsive, difficult kids as bipolar reminding yourself and parents who are struggling that most disruptive, irritable children do not have bipolar disorder but can still benefit from help getting help with diagnostic and treatment questions as often as necessary
92 Selected Bibliography Pharmacologic Treatments for Pediatric Bipolar Disorder: A Review and Meta-Analysis. Liu et al. JAACAP. August Practitioner Review: The Assessment of Bipolar Disorder in Children and Adolescents. Baroni et al. JCPP Antipsychotic Use in Children and Adolescents:Minimizing Adverse Effects to Maximize Outcomes. Correll. JAACAP. January 2008.
Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder,
 Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder, Journal of the Academy of Child and Adolescent Psychiatry, 1997 Primary Authors: Jon McClellan MD
Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder, Journal of the Academy of Child and Adolescent Psychiatry, 1997 Primary Authors: Jon McClellan MD
Kelly Godecke, MD Department of Psychiatry University of Utah
 Kelly Godecke, MD Department of Psychiatry University of Utah Epidemiology and Impact -module 2 session 1 overview of mood disorders Diagnostic Criteria of Bipolar Disorders Medications Used in Bipolar
Kelly Godecke, MD Department of Psychiatry University of Utah Epidemiology and Impact -module 2 session 1 overview of mood disorders Diagnostic Criteria of Bipolar Disorders Medications Used in Bipolar
Differentiating Unipolar vs Bipolar Depression in Children
 Differentiating Unipolar vs Bipolar Depression in Children Mai Uchida, M.D. Director, Center for Early Identification and Prevention of Pediatric Depression Massachusetts General Hospital Assistant Professor
Differentiating Unipolar vs Bipolar Depression in Children Mai Uchida, M.D. Director, Center for Early Identification and Prevention of Pediatric Depression Massachusetts General Hospital Assistant Professor
Differentiating MDD vs. Bipolar Depression In Youth
 Differentiating MDD vs. Bipolar Depression In Youth Mai Uchida, M.D. Staff Physician Clinical and Research Programs in Pediatric Psychopharmacology Massachusetts General Hospital Disclosures Neither I
Differentiating MDD vs. Bipolar Depression In Youth Mai Uchida, M.D. Staff Physician Clinical and Research Programs in Pediatric Psychopharmacology Massachusetts General Hospital Disclosures Neither I
Pediatric Bipolar Disorder and ADHD
 Pediatric Bipolar Disorder and ADHD Janet Wozniak, M.D. Director, Pediatric Bipolar Disorder Research Program Associate Professor Psychiatry Massachusetts General Hospital Harvard Medical School Disclosures
Pediatric Bipolar Disorder and ADHD Janet Wozniak, M.D. Director, Pediatric Bipolar Disorder Research Program Associate Professor Psychiatry Massachusetts General Hospital Harvard Medical School Disclosures
PEDIATRIC BIPOLAR DISORDER
 PEDIATRIC BIPOLAR DISORDER Swapna Deshpande, MD Clinical Assistant Professor Associate Training Director, Child/Adolescent Fellowship Program Department of Psychiatry & Behavioral Sciences University of
PEDIATRIC BIPOLAR DISORDER Swapna Deshpande, MD Clinical Assistant Professor Associate Training Director, Child/Adolescent Fellowship Program Department of Psychiatry & Behavioral Sciences University of
Comprehensive Quick Reference Handout on Pediatric Bipolar Disorder By Jessica Tomasula
 Comprehensive Quick Reference Handout on Pediatric Bipolar Disorder By Jessica Tomasula Official Name Bipolar Disorder; also referred to as Manic Depression Definitions (DSM-IV-TR, 2000) Bipolar I Disorder
Comprehensive Quick Reference Handout on Pediatric Bipolar Disorder By Jessica Tomasula Official Name Bipolar Disorder; also referred to as Manic Depression Definitions (DSM-IV-TR, 2000) Bipolar I Disorder
Mood Disorders for Care Coordinators
 Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
5/2/2017. By Pamela Pepper PMH, CNS, BC. DSM-5 Growth and Development
 By Pamela Pepper PMH, CNS, BC DSM-5 Growth and Development The idea that diagnosis is based on subjective criteria and that those criteria should fall neatly into a set of categories is not sustainable,
By Pamela Pepper PMH, CNS, BC DSM-5 Growth and Development The idea that diagnosis is based on subjective criteria and that those criteria should fall neatly into a set of categories is not sustainable,
RANZCP 2010 AUCKLAND, NEW ZEALAND
 RANZCP 2010 AUCKLAND, NEW ZEALAND Dr Veronica Stanganelli et al. RANZCP 2010 1 INTRODUCTION Bipolar disorder within young people has been debated for years. It is still controversial in DSM V (1), whether
RANZCP 2010 AUCKLAND, NEW ZEALAND Dr Veronica Stanganelli et al. RANZCP 2010 1 INTRODUCTION Bipolar disorder within young people has been debated for years. It is still controversial in DSM V (1), whether
CASE 5 - Toy & Klamen CASE FILES: Psychiatry
 CASE 5 - Toy & Klamen CASE FILES: Psychiatry A 14-year-old boy is brought to the emergency department after being found in the basement of his home by his parents during the middle of a school day. The
CASE 5 - Toy & Klamen CASE FILES: Psychiatry A 14-year-old boy is brought to the emergency department after being found in the basement of his home by his parents during the middle of a school day. The
Psychiatric Medications. Positive and negative effects in the classroom
 Psychiatric Medications Positive and negative effects in the classroom Teaching the Medicated Child Beverly Bryant, M.D. Hattiesburg Clinic 9/17/14 Introduction According to the National Survey of Children
Psychiatric Medications Positive and negative effects in the classroom Teaching the Medicated Child Beverly Bryant, M.D. Hattiesburg Clinic 9/17/14 Introduction According to the National Survey of Children
BIPOLAR DISORDER AND ADHD IN CHILDREN
 BIPOLAR DISORDER AND ADHD IN CHILDREN BIPOLAR I DISORDER IS BEING DIAGNOSED WITH INCREASING FREQUENCY (INTENSITY) IN PRE-PUBERTAL CHIDREN WITH THE CAVEAT (WARNING / STIPULATION) THAT CLASSIC MANIC EPISODES
BIPOLAR DISORDER AND ADHD IN CHILDREN BIPOLAR I DISORDER IS BEING DIAGNOSED WITH INCREASING FREQUENCY (INTENSITY) IN PRE-PUBERTAL CHIDREN WITH THE CAVEAT (WARNING / STIPULATION) THAT CLASSIC MANIC EPISODES
Mood swings in young people
 Mood swings in young people Bipolar I & II Disorders are uncommon before puberty; Mood Dysregulation (MD) is very common before puberty Are they the same problem? What are the beginnings of bipolar? What
Mood swings in young people Bipolar I & II Disorders are uncommon before puberty; Mood Dysregulation (MD) is very common before puberty Are they the same problem? What are the beginnings of bipolar? What
Chronic irritability in youth that may be misdiagnosed as bipolar disorder. Ellen Leibenluft, M.D.
 Chronic irritability in youth that may be misdiagnosed as bipolar disorder Ellen Leibenluft, M.D. Chief, Section on Bipolar Spectrum Disorders Emotion and Development Branch National Institute of Mental
Chronic irritability in youth that may be misdiagnosed as bipolar disorder Ellen Leibenluft, M.D. Chief, Section on Bipolar Spectrum Disorders Emotion and Development Branch National Institute of Mental
Treatment of Bipolar Disorder in Youth
 Treatment of Bipolar Disorder in Youth Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts General Hospital
Treatment of Bipolar Disorder in Youth Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts General Hospital
Pediatric Bipolar Disorder: Advances in Diagnosis and Research
 Pediatric Bipolar Disorder: Advances in Diagnosis and Research Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts
Pediatric Bipolar Disorder: Advances in Diagnosis and Research Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts
Bipolar Disorder Demystified. Cerrone Cohen, MD FABPN, FABFM Duke Departments of Family Medicine and Psychiatry
 Bipolar Disorder Demystified Cerrone Cohen, MD FABPN, FABFM Duke Departments of Family Medicine and Psychiatry Underdiagnoses of Depression In Primary Care 2005 Study of 650 primary care patients on antidepressants
Bipolar Disorder Demystified Cerrone Cohen, MD FABPN, FABFM Duke Departments of Family Medicine and Psychiatry Underdiagnoses of Depression In Primary Care 2005 Study of 650 primary care patients on antidepressants
Brief Notes on the Mental Health of Children and Adolescents
 Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
Brief Notes on the Mental Health of Children and Adolescents The future of our country depends on the mental health and strength of our young people. However, many children have mental health problems
5 COMMON QUESTIONS WHEN TREATING DEPRESSION
 5 COMMON QUESTIONS WHEN TREATING DEPRESSION Do Antidepressants Increase the Possibility of Suicide? Will I Accidentally Induce Mania if I Prescribe an SSRI? Are Depression Medications Safe and Effective
5 COMMON QUESTIONS WHEN TREATING DEPRESSION Do Antidepressants Increase the Possibility of Suicide? Will I Accidentally Induce Mania if I Prescribe an SSRI? Are Depression Medications Safe and Effective
Bipolar Disorder in Youth
 Bipolar Disorder in Youth Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts General Hospital Pediatric-Onset
Bipolar Disorder in Youth Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric Bipolar Disorder Research Program Harvard Medical School Massachusetts General Hospital Pediatric-Onset
Post Traumatic Stress Disorder (PTSD) versus Bipolar Disorder: Confusion in the face of chaos.
 versus Bipolar Disorder: Confusion in the face of chaos.") Post Traumatic Stress Disorder (PTSD) versus Bipolar Disorder: Confusion in the face of chaos. Randall Ricardi D.O. Child and Adolescent Psychiatry Phoenix Children s Hospital 6-24-17 10:50am Disclosures
Post Traumatic Stress Disorder (PTSD) versus Bipolar Disorder: Confusion in the face of chaos. Randall Ricardi D.O. Child and Adolescent Psychiatry Phoenix Children s Hospital 6-24-17 10:50am Disclosures
Depressive and Bipolar Disorders
 Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Ohio Psychotropic Medication Quality Improvement Collaborative. Minds Matter. Toolkit. for You and Your Family. This is the property of
 Minds Matter Ohio Psychotropic Medication Quality Improvement Collaborative Minds Matter Toolkit for You and Your Family This is the property of About Minds Matter Minds Matter is a project to help teens,
Minds Matter Ohio Psychotropic Medication Quality Improvement Collaborative Minds Matter Toolkit for You and Your Family This is the property of About Minds Matter Minds Matter is a project to help teens,
Bipolar Disorder. Other Organic Diagnoses. Assessment/Diagnosis of Bipolar Disorder 2/6/2018 1
 Bipolar Disorder 2/6/2018 1 Assessment/Diagnosis of Bipolar Disorder Complicated; mimicking other disorders and has comorbidity (presents with other disorders) Half of bipolar children have relatives with
Bipolar Disorder 2/6/2018 1 Assessment/Diagnosis of Bipolar Disorder Complicated; mimicking other disorders and has comorbidity (presents with other disorders) Half of bipolar children have relatives with
Clinical Guideline for the Management of Bipolar Disorder in Adults
 Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine June 10-12, 2011
 Adelaide Robb, MD Associate Professor Psychiatry and Pediatrics Source Advisory Board Disclosure Speaker s Bureau Bristol Myers Squibb Yes Yes Yes Epocrates Research Contract Royalties Yes Stock Janssen
Adelaide Robb, MD Associate Professor Psychiatry and Pediatrics Source Advisory Board Disclosure Speaker s Bureau Bristol Myers Squibb Yes Yes Yes Epocrates Research Contract Royalties Yes Stock Janssen
Bipolar disorder and severe irritability in youth: Diagnosis and treatment. Ellen Leibenluft, M.D.
 Bipolar disorder and severe irritability in youth: Diagnosis and treatment Ellen Leibenluft, M.D. Chief, Section on Bipolar Spectrum Disorders Emotion and Development Branch National Institute of Mental
Bipolar disorder and severe irritability in youth: Diagnosis and treatment Ellen Leibenluft, M.D. Chief, Section on Bipolar Spectrum Disorders Emotion and Development Branch National Institute of Mental
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care
 Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
Pediatric Behavior Problems: ODD and DMDD. Stanley Brewer, DO Pediatrics Assistant Professor (Clinical) Psychiatry Adjunct Instructor
 Psychiatry Adjunct Instructor") Pediatric Behavior Problems: ODD and DMDD Stanley Brewer, DO Pediatrics Assistant Professor (Clinical) Psychiatry Adjunct Instructor Acting out: What to call it Externalizing disorders Oppositional Defiant
Pediatric Behavior Problems: ODD and DMDD Stanley Brewer, DO Pediatrics Assistant Professor (Clinical) Psychiatry Adjunct Instructor Acting out: What to call it Externalizing disorders Oppositional Defiant
Criteria for Child Psychiatrist on the Use of Selected Psychotropic Medications in Children & Adolescents
 Criteria for Child Psychiatrist on the Use of Selected Psychotropic Medications in Children & Adolescents DRUG NAME INDICATIONS / ACCEPTABLE USES PRIOR STIMULANT/ADHD DRUGS Daytrana (methylphenidate) ADHD
Criteria for Child Psychiatrist on the Use of Selected Psychotropic Medications in Children & Adolescents DRUG NAME INDICATIONS / ACCEPTABLE USES PRIOR STIMULANT/ADHD DRUGS Daytrana (methylphenidate) ADHD
MOOD DISORDERS 101: A primer for recognizing and intervening with children with DMDD JULIE T. STECK, PH.D., HSPP CRG/CHILDREN S RESOURCE GROUP
 MOOD DISORDERS 101: A primer for recognizing and intervening with children with DMDD JULIE T. STECK, PH.D., HSPP CRG/CHILDREN S RESOURCE GROUP OBJECTIVES Participants will develop an understanding of Disruptive
MOOD DISORDERS 101: A primer for recognizing and intervening with children with DMDD JULIE T. STECK, PH.D., HSPP CRG/CHILDREN S RESOURCE GROUP OBJECTIVES Participants will develop an understanding of Disruptive
Severe Mood Dysregulation in Children and Adolescents Research Findings Support Diagnostic Validity of Pediatric Bipolar Disorder
 Severe Mood Dysregulation in Children and Adolescents Research Findings Support Diagnostic Validity of Pediatric Bipolar Disorder Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric
Severe Mood Dysregulation in Children and Adolescents Research Findings Support Diagnostic Validity of Pediatric Bipolar Disorder Janet Wozniak, M.D. Associate Professor of Psychiatry Director, Pediatric
PSYCH 235 Introduction to Abnormal Psychology. Agenda/Overview. Mood Disorders. Chapter 11 Mood/Bipolar and Related disorders & Suicide
 PSYCH 235 Introduction to Abnormal Psychology Chapter 11 Mood/Bipolar and Related disorders & Suicide 1 Agenda/Overview Mood disorders Major depression Persistent Depressive Disorder (Dysthymia) Bipolar
PSYCH 235 Introduction to Abnormal Psychology Chapter 11 Mood/Bipolar and Related disorders & Suicide 1 Agenda/Overview Mood disorders Major depression Persistent Depressive Disorder (Dysthymia) Bipolar
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XV, 2013 INDEX
 A acceptance and commitment therapy Posttraumatic Stress, 69 ADHD Adjunctive Fatty Acids, 5 Adjunctive Guanfacine Pharmacokinetics, 27 Amantadine, 21 Atomoxetine, 23 Cancer Risk, 31 CBT for Comorbid Anxiety,
A acceptance and commitment therapy Posttraumatic Stress, 69 ADHD Adjunctive Fatty Acids, 5 Adjunctive Guanfacine Pharmacokinetics, 27 Amantadine, 21 Atomoxetine, 23 Cancer Risk, 31 CBT for Comorbid Anxiety,
2013 Virtual AD/HD Conference 1
 Medication for & Coexisting Conditions Part 2 Dr. Kenny Handelman Child, Adolescent & Adult Psychiatrist Halton Healthcare Adjunct Professor of Psychiatry, University of Western Ontario www.drkenny.com
Medication for & Coexisting Conditions Part 2 Dr. Kenny Handelman Child, Adolescent & Adult Psychiatrist Halton Healthcare Adjunct Professor of Psychiatry, University of Western Ontario www.drkenny.com
Disclosure Statement. A Rational Approach to Psychopharmacology. Goals 10/28/2013
 A Rational Approach to Psychopharmacology Disclosure Statement Full time employed physician with MaineGeneral Medical Center in Waterville and Augusta No conflicts of interest to disclose Goals Promote
A Rational Approach to Psychopharmacology Disclosure Statement Full time employed physician with MaineGeneral Medical Center in Waterville and Augusta No conflicts of interest to disclose Goals Promote
Kelly E. Williams, Pharm.D. PGY2 Psychiatric Pharmacy Resident April 16,2009
 Kelly E. Williams, Pharm.D. PGY2 Psychiatric Pharmacy Resident April 16,2009 List the antipsychotics most often prescribed Compare and contrast the use and adverse effects experienced in the pediatric
Kelly E. Williams, Pharm.D. PGY2 Psychiatric Pharmacy Resident April 16,2009 List the antipsychotics most often prescribed Compare and contrast the use and adverse effects experienced in the pediatric
J. Indian Assoc. Child Adolesc. Ment. Health 2012; 8(1):1-5. Editorial
:1-5. Editorial") 1 J. Indian Assoc. Child Adolesc. Ment. Health 2012; 8(1):1-5 Editorial Controversies in Paediatric Bipolar Disorder Vivek Agarwal 1, Sivakumar T 2 1.Editor JIACAM & Associate Professor, Department of
1 J. Indian Assoc. Child Adolesc. Ment. Health 2012; 8(1):1-5 Editorial Controversies in Paediatric Bipolar Disorder Vivek Agarwal 1, Sivakumar T 2 1.Editor JIACAM & Associate Professor, Department of
RCHC Case Presentation
 Michael Kennedy, MFT Division Director RCHC Case Presentation Starring Melissa Ladrech as Susan and Michael Kozart as Dr. Keigh The following case is presented in three video installments. After each installment,
Michael Kennedy, MFT Division Director RCHC Case Presentation Starring Melissa Ladrech as Susan and Michael Kozart as Dr. Keigh The following case is presented in three video installments. After each installment,
April 2016 Prepared By: Kimberly D. Griego, PharmD, CGP
 April 2016 Prepared By: Kimberly D. Griego, PharmD, CGP Bipolar disorder (BD), also referred to as manic-depression, presents with dramatic swings in a person s mood and energy level, which affects their
April 2016 Prepared By: Kimberly D. Griego, PharmD, CGP Bipolar disorder (BD), also referred to as manic-depression, presents with dramatic swings in a person s mood and energy level, which affects their
HealthyPlace s Introductory Guide to Bipolar Disorder. By Natasha Tracy
 HealthyPlace s Introductory Guide to Bipolar Disorder By Natasha Tracy 1 Index Introduction Chapter One Bipolar Disorder Basics Chapter Two Bipolar Disorder Diagnosis Chapter Three Treatment of Bipolar
HealthyPlace s Introductory Guide to Bipolar Disorder By Natasha Tracy 1 Index Introduction Chapter One Bipolar Disorder Basics Chapter Two Bipolar Disorder Diagnosis Chapter Three Treatment of Bipolar
Class Update: Oral Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
6/22/2012. Co-morbidity - when two or more conditions occur together. The two conditions may or may not be causally related.
 Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
Riding the Waves: Tools for the Management of Bipolar Disorder
 Riding the Waves: Tools for the Management of Bipolar Disorder Jacintha S. Cauffield, Pharm.D., BCPS, CDE Associate Professor of Pharmacy Practice Palm Beach Atlantic University Lloyd L. Gregory School
Riding the Waves: Tools for the Management of Bipolar Disorder Jacintha S. Cauffield, Pharm.D., BCPS, CDE Associate Professor of Pharmacy Practice Palm Beach Atlantic University Lloyd L. Gregory School
Mood Disorders.
 Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Medications for Anxiety & Behavior in Williams Syndrome. Disclosure of Potential Conflicts. None 9/22/2016. Evaluation
 Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
To Give or not to Give Medication: That is the Question
 To Give or not to Give Medication: That is the Question Charmi Patel Rao, MD September 14, 2018 Introduction Board Certified Child & Adolescent Psychiatrist Clinical expertise in ECMH and Developmental
To Give or not to Give Medication: That is the Question Charmi Patel Rao, MD September 14, 2018 Introduction Board Certified Child & Adolescent Psychiatrist Clinical expertise in ECMH and Developmental
11/11/2018. The ABCs of Medication Management for Autism Spectrum Disorder. ABC Logging (FBA) First. ABC Logging HOW TO COMPLEMENT BEHAVIORAL THERAPY
 First. ABC Logging HOW TO COMPLEMENT BEHAVIORAL THERAPY") The ABCs of Medication Management for Autism Spectrum Disorder OR HOW TO COMPLEMENT BEHAVIORAL THERAPY ABC Logging (FBA) First We need to know what, when, where and why behaviors happen. Antecedent: What
The ABCs of Medication Management for Autism Spectrum Disorder OR HOW TO COMPLEMENT BEHAVIORAL THERAPY ABC Logging (FBA) First We need to know what, when, where and why behaviors happen. Antecedent: What
Pediatric Bipolar Disorder
 Pediatric Bipolar Disorder Jason J. Washburn, Ph.D., ABPP 1 Overview of Talk Bipolar Disorder Understanding Differences between Adults & Children Diagnosis of Pediatric Bipolar Disorder Treatment of Pediatric
Pediatric Bipolar Disorder Jason J. Washburn, Ph.D., ABPP 1 Overview of Talk Bipolar Disorder Understanding Differences between Adults & Children Diagnosis of Pediatric Bipolar Disorder Treatment of Pediatric
Goal: To recognize and differentiate abnormal reactions involving depressed and manic moods
 Goal: To recognize and differentiate abnormal reactions involving depressed and manic moods Moods versus emotions DSM-IV mood disorders are now two separate categories in DSM-5 Depressive disorders Bipolar
Goal: To recognize and differentiate abnormal reactions involving depressed and manic moods Moods versus emotions DSM-IV mood disorders are now two separate categories in DSM-5 Depressive disorders Bipolar
Drugs for Emotional and Mood Disorders Chapter 16
 Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
4/29/2016. Psychosis A final common pathway. Early Intervention in Psychotic Disorders: Necessary, Effective, and Overdue
 Early Intervention in Psychotic Disorders: Necessary, Effective, and Overdue Disclosures Financial relationships with commercial interests Douglas R. Robbins, M.D. Maine Medical Center Tufts University
Early Intervention in Psychotic Disorders: Necessary, Effective, and Overdue Disclosures Financial relationships with commercial interests Douglas R. Robbins, M.D. Maine Medical Center Tufts University
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*
 DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*") COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
Treating Disruptive Behavior Disorders in Children and Teens. A Review of the Research for Parents and Caregivers
 Treating Disruptive Behavior Disorders in Children and Teens A Review of the Research for Parents and Caregivers e Is This Information Right for Me? This information is for you if: A health care professional*
Treating Disruptive Behavior Disorders in Children and Teens A Review of the Research for Parents and Caregivers e Is This Information Right for Me? This information is for you if: A health care professional*
BIPOLAR DISORDERS DIAGNOSTIC AND TREATMENT ISSUES RICHARD RIES MD
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences BIPOLAR DISORDERS DIAGNOSTIC AND TREATMENT ISSUES RICHARD RIES MD PROFESSOR DEPARTMENT OF PSYCHIATRY UNIVERSITY
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences BIPOLAR DISORDERS DIAGNOSTIC AND TREATMENT ISSUES RICHARD RIES MD PROFESSOR DEPARTMENT OF PSYCHIATRY UNIVERSITY
Bipolar Disorder 4/6/2014. Bipolar Disorder. Symptoms of Depression. Mania. Depression
 Bipolar Disorder J. H. Atkinson, M.D. Professor of Psychiatry HIV Neurobehavioral Research Programs University of California, San Diego KETHEA, Athens Slides courtesy of John Kelsoe, M.D. Bipolar Disorder
Bipolar Disorder J. H. Atkinson, M.D. Professor of Psychiatry HIV Neurobehavioral Research Programs University of California, San Diego KETHEA, Athens Slides courtesy of John Kelsoe, M.D. Bipolar Disorder
Index. Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) b-adrenergic blockers
 b-adrenergic blockers") Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Jonathan Haverkampf BIPOLAR DISORDR BIPOLAR DISORDER. Dr. Jonathan Haverkampf, M.D.
 BIPOLAR DISORDER Dr., M.D. Abstract - Bipolar disorder is a condition affecting an individual s affective states (mood). The different flavors of bipolar disorder have in common that there are alterations
BIPOLAR DISORDER Dr., M.D. Abstract - Bipolar disorder is a condition affecting an individual s affective states (mood). The different flavors of bipolar disorder have in common that there are alterations
Bipolar Disorders. Disclosure Statement. I have no financial disclosures or conflicts of interest
 Bipolar Disorders Ahsan Naseem, MD Diplomate American Board of Psychiatry and Neurology Adult and Geriatric Psychiatry Medical Director Bryan Heartland Psychiatry Bryan Physician Network Partner Cheney
Bipolar Disorders Ahsan Naseem, MD Diplomate American Board of Psychiatry and Neurology Adult and Geriatric Psychiatry Medical Director Bryan Heartland Psychiatry Bryan Physician Network Partner Cheney
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression
 Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Crisis Intervention Team (CIT) Training
 Training") Crisis Intervention Team (CIT) Training Student Guide Bipolar Disorder Created by: Nils Rosenbaum Matthew Tinney Lawrence Saavedra Bipolar Disorder What is bipolar disorder? Bipolar disorder is a brain
Crisis Intervention Team (CIT) Training Student Guide Bipolar Disorder Created by: Nils Rosenbaum Matthew Tinney Lawrence Saavedra Bipolar Disorder What is bipolar disorder? Bipolar disorder is a brain
D I A G N O S I S ADD/ADHD. Conduct Disorder. Oppositional. Oppositional Defiant Disorder. Defiant. Anxiety Disorder. Adjustment.
 Dr. Crismon has no potential conflicts of interest to disclose with regard to this presentation. M. Lynn Crismon, Pharm.D., FCCP, BCPP Dean James T. Doluisio Regents Chair & Behrens Centennial Professor
Dr. Crismon has no potential conflicts of interest to disclose with regard to this presentation. M. Lynn Crismon, Pharm.D., FCCP, BCPP Dean James T. Doluisio Regents Chair & Behrens Centennial Professor
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XIV, 2012 INDEX
 A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
Childhood Rage: Diagnosis and Treatment Strategies for Severe Mood Dysregulation - Part 2: Diagnosis and Treatment
 Liberty University DigitalCommons@Liberty University Faculty Publications and Presentations Department for Counselor Education and Family Studies 2013 Childhood Rage: Diagnosis and Treatment Strategies
Liberty University DigitalCommons@Liberty University Faculty Publications and Presentations Department for Counselor Education and Family Studies 2013 Childhood Rage: Diagnosis and Treatment Strategies
Mood disorders. Carolyn R. Fallahi, Ph. D.
 Mood disorders Carolyn R. Fallahi, Ph. D. Childhood bipolar disorder Dramatic mood swings Occur in cycles Exhilaration and agitation = mania Depression Normal mood The typical adult cycle How do children
Mood disorders Carolyn R. Fallahi, Ph. D. Childhood bipolar disorder Dramatic mood swings Occur in cycles Exhilaration and agitation = mania Depression Normal mood The typical adult cycle How do children
Disruptive mood dysregulation disorder (DMDD) a
 a") Disruptive mood dysregulation disorder: A better understanding Recognizing key differences in DMDD can help distinguish it from similar pediatric disorders Disruptive mood dysregulation disorder (DMDD)
Disruptive mood dysregulation disorder: A better understanding Recognizing key differences in DMDD can help distinguish it from similar pediatric disorders Disruptive mood dysregulation disorder (DMDD)
A Brief Overview of Psychiatric Pharmacotherapy. Joel V. Oberstar, M.D. Chief Executive Officer
 A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
Piecing the Puzzle Together: Pharmacologic Approaches to Behavioral Management in Autism Spectrum Disorder
 Piecing the Puzzle Together: Pharmacologic Approaches to Behavioral Management in Autism Spectrum Disorder Hannah Sauer, PharmD PGY1 Pediatric Pharmacy Resident Mayo Clinic 2015 MFMER slide-1 Objectives
Piecing the Puzzle Together: Pharmacologic Approaches to Behavioral Management in Autism Spectrum Disorder Hannah Sauer, PharmD PGY1 Pediatric Pharmacy Resident Mayo Clinic 2015 MFMER slide-1 Objectives
Guidelines for the Utilization of Psychotropic Medications for Children in Foster Care. Illinois Department of Children and Family Services
 Guidelines for the Utilization of Psychotropic Medications for Children in Foster Care Illinois Department of Children and Family Services Introduction With few exceptions, children and adolescents in
Guidelines for the Utilization of Psychotropic Medications for Children in Foster Care Illinois Department of Children and Family Services Introduction With few exceptions, children and adolescents in
Judges Reference Table for the March 2016 Psychotropic Medication Utilization Parameters for Foster Children
 Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Schedule FDA & literature based indications
 Psychotropic Medication List Recommended dosages are intended to serve only as a guide for children. Recommended doses are literature based. Clinicians should consult package insert of medications for
Psychotropic Medication List Recommended dosages are intended to serve only as a guide for children. Recommended doses are literature based. Clinicians should consult package insert of medications for
Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents
 BadgerCare Plus Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice
BadgerCare Plus Preferred Practice Guidelines Bipolar Disorder in Children and Adolescents These Guidelines are based in part on the following: American Academy of Child and Adolescent Psychiatry s Practice
ADHD and. Shaw Wendi Fortuchang, M.D. Board certified in Child & Adolescent, Adult, and Forensic Psychiatry
 ADHD and Beyond Shaw Wendi Fortuchang, M.D. Board certified in Child & Adolescent, Adult, and Forensic Psychiatry Overview Use of medications in children How do medications work in the brain? Risperdal?
ADHD and Beyond Shaw Wendi Fortuchang, M.D. Board certified in Child & Adolescent, Adult, and Forensic Psychiatry Overview Use of medications in children How do medications work in the brain? Risperdal?
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults
 Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Bipolar Disorder Michael Coudreaut, MD
 Bipolar Disorder Michael Coudreaut, MD Consultation liaison psychiatry at Intermountain Medical Center; Adjuctive assistant professor, Departments of psychiaitry, University of Utah; Salt Lake City, Utah
Bipolar Disorder Michael Coudreaut, MD Consultation liaison psychiatry at Intermountain Medical Center; Adjuctive assistant professor, Departments of psychiaitry, University of Utah; Salt Lake City, Utah
Treat mood, cognition, and behavioral disturbances associated with psychological disorders. Most are not used recreationally or abused
 Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Adult Depression - Clinical Practice Guideline
 1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
3/9/2017. A module within the 8 hour Responding to Crisis Course. Our purpose
 A module within the 8 hour Responding to Crisis Course Our purpose 1 What is mental Illness Definition of Mental Illness A syndrome characterized by clinically significant disturbance in an individual
A module within the 8 hour Responding to Crisis Course Our purpose 1 What is mental Illness Definition of Mental Illness A syndrome characterized by clinically significant disturbance in an individual
4/2/13 COMMON CLASSES OF MEDICATIONS. Child & Adolescent Behavioral Medicine & Medication Therapies. Behavioral Medicine & Medication Therapies
 Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Depression Management
 Depression Management Ulka Agarwal, M.D. Adjunct Psychiatrist Pine Rest Christian Mental Health Disclosures The presenter and all planners of this education activity do not have a financial/arrangement
Depression Management Ulka Agarwal, M.D. Adjunct Psychiatrist Pine Rest Christian Mental Health Disclosures The presenter and all planners of this education activity do not have a financial/arrangement
Aggression (Severe) in Children under Age 6
 in Children under Age 6") Aggression (Severe) in Children under Age 6 Level 0 Comprehensive diagnostic assessments. Refer to Principles of Practice on page 6. Evaluate and treat comorbid conditions (i.e. medical, other psychiatric
Aggression (Severe) in Children under Age 6 Level 0 Comprehensive diagnostic assessments. Refer to Principles of Practice on page 6. Evaluate and treat comorbid conditions (i.e. medical, other psychiatric
Goal: To recognize and differentiate abnormal reactions involving depressed and manic moods
 Key Dates TH Feb 9 Begin Dimensions-Behavior, Units IIB, 8 through page 147; MW Ch 9 Betty, Elvis TU Feb 14 Unit 8 147-end and Unit 9; MW Ch 8 Jeffrey and Ch 10 Diana TH Feb 16 Unit 10; MW Ch 11 Theodore
Key Dates TH Feb 9 Begin Dimensions-Behavior, Units IIB, 8 through page 147; MW Ch 9 Betty, Elvis TU Feb 14 Unit 8 147-end and Unit 9; MW Ch 8 Jeffrey and Ch 10 Diana TH Feb 16 Unit 10; MW Ch 11 Theodore
ANXIETY: FAST FACTS AND SKILLS FOR THE PRIMARY CARE PHYSICIAN
 UW PACC Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANXIETY: FAST FACTS AND SKILLS FOR THE PRIMARY CARE PHYSICIAN RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL
UW PACC Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANXIETY: FAST FACTS AND SKILLS FOR THE PRIMARY CARE PHYSICIAN RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL
Promoting and Monitoring Evidenced-Based Antipsychotic Prescribing Practices in Children and Adolescents: Florida Medicaid Initiatives
 Promoting and Monitoring Evidenced-Based Antipsychotic Prescribing Practices in Children and Adolescents: Florida Medicaid Initiatives Mary Elizabeth Jones, Pharm BSc, RPh Senior Pharmacist AHCA Pharmacy
Promoting and Monitoring Evidenced-Based Antipsychotic Prescribing Practices in Children and Adolescents: Florida Medicaid Initiatives Mary Elizabeth Jones, Pharm BSc, RPh Senior Pharmacist AHCA Pharmacy
PSYCHIATRIC DRUGS. Mr. D.Raju, M.pharm, Lecturer
 PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
DSM5: How to Understand It and How to Help
 DSM5: How to Understand It and How to Help Introduction: The DSM5 is a foreign language! Three Questions: I. The first was, What the key assumptions made to determine the organization of the DSM5? A. Mental
DSM5: How to Understand It and How to Help Introduction: The DSM5 is a foreign language! Three Questions: I. The first was, What the key assumptions made to determine the organization of the DSM5? A. Mental
4/29/2015. Dr. Carman Gill Wednesday, April 29th
 Dr. Carman Gill Wednesday, April 29th 1 Impacted diagnoses Major changes and rationale Special considerations Implications for counselors A sustained condition of prolonged emotional dejection, sadness,
Dr. Carman Gill Wednesday, April 29th 1 Impacted diagnoses Major changes and rationale Special considerations Implications for counselors A sustained condition of prolonged emotional dejection, sadness,
CONTROVERSIES AND NEW DIRECTIONS
 BIPOLAR Introduction DISORDER IN CHILDHOOD AND EARLY ADOLESCENCE Introduction MELISSA P. D ELBELLO, DAVID AXELSON, and BARBARA GELLER CONTROVERSIES AND NEW DIRECTIONS Although the existence and diagnostic
BIPOLAR Introduction DISORDER IN CHILDHOOD AND EARLY ADOLESCENCE Introduction MELISSA P. D ELBELLO, DAVID AXELSON, and BARBARA GELLER CONTROVERSIES AND NEW DIRECTIONS Although the existence and diagnostic
ATTENTION DEFICIT HYPERACTIVITY DISORDER COMORBIDITIES 23/02/2011. Oppositional Defiant Disorder
 ATTENTION DEFICIT HYPERACTIVITY DISORDER COMORBIDITIES The comorbidity of ADHD with other disorders is between 60% and 80% The most commonly comorbid disorder that occur alongside ADHD are: Oppositional
ATTENTION DEFICIT HYPERACTIVITY DISORDER COMORBIDITIES The comorbidity of ADHD with other disorders is between 60% and 80% The most commonly comorbid disorder that occur alongside ADHD are: Oppositional
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Disruptive Mood Dysregulation Disorder
 Walden University ScholarWorks School of Counseling Publications College of Social and Behavioral Sciences 2015 Disruptive Mood Dysregulation Disorder Brandy L. Gilea Walden University Rachel M. O Neill
Walden University ScholarWorks School of Counseling Publications College of Social and Behavioral Sciences 2015 Disruptive Mood Dysregulation Disorder Brandy L. Gilea Walden University Rachel M. O Neill
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D.
 HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
HDSA Annual Convention June 2013 Behavior Issues: Irritability and Depression Peg Nopoulos, M.D. Professor of Psychiatry, Neurology, and Pediatrics University of Iowa, Iowa City, Iowa The information provided
Primary Care: Referring to Psychiatry
 Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
White Paper: The Treatment of Schizophrenia and Bipolar Disorder
 White Paper: The Treatment of Schizophrenia and Bipolar Disorder in Children: What is Medically Necessary? For Health Plans, Medical Management Organizations and TPAs Trends in the Diagnosis and Treatment
White Paper: The Treatment of Schizophrenia and Bipolar Disorder in Children: What is Medically Necessary? For Health Plans, Medical Management Organizations and TPAs Trends in the Diagnosis and Treatment
Deficits in Emotional Regulation in ADHD
 Deficits in Emotional Regulation in ADHD Joseph Biederman, MD Professor of Psychiatry Harvard Medical School Chief, Clinical and Research Programs in Pediatric Psychopharmacology and Adult ADHD Massachusetts
Deficits in Emotional Regulation in ADHD Joseph Biederman, MD Professor of Psychiatry Harvard Medical School Chief, Clinical and Research Programs in Pediatric Psychopharmacology and Adult ADHD Massachusetts
Handout for the Neuroscience Education Institute (NEI) online activity: Juvenile Bipolar Disorder: Further Complicated by Comorbidity
 online activity: Juvenile Bipolar Disorder: Further Complicated by Comorbidity") Handout for the Neuroscience Education Institute (NEI) online activity: Juvenile Bipolar Disorder: Further Complicated by Comorbidity Learning Objectives Utilize evidence-based strategies to accurately
Handout for the Neuroscience Education Institute (NEI) online activity: Juvenile Bipolar Disorder: Further Complicated by Comorbidity Learning Objectives Utilize evidence-based strategies to accurately