Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy?
|
|
|
- Grace Spencer
- 5 years ago
- Views:
Transcription




1 Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure Yasuo Yoshioka, MD, does not have any financial relationships or products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months. 1
2 Background Typical IMRT (1.8 2 Gy/fr) has problems of Long treatment period of 2 months Burden to patients Burden to medical staff Burden to machine resources Difficulty in controlling intra fraction error Wider margin Toxicity concern Moderate dose escalation Not utilizing low α/β ratio of prostate caner HDR brachytherapy (especially monotherapy) solution SBRT solution?? Aim To discuss similarity and difference between HDR monotherapy and SBRT, in terms of radiation physics (dose distribution) radiobiology (dose, dose-fractionation) reported clinical results in the context of extreme hypofractionation. 2




3 Where Are HDR and SBRT Standing? 3






4 Where Are HDR and SBRT Standing? Classics of Prostate Hypofractionation (Era of 2D or Early 3D. No IMRT) Carcinoma of prostate treated by radical external beam radiotherapy using hypofractionation. Twenty two years' experience ( ). Lloyd Davies RW, et al. Urology. 1990;36: (UK) 36 Gy/6 fr (6 Gy/fr),n = 209 Randomized trial comparing two fractionation schedules for patients with localized prostate cancer. (Canada) Lukka H, et al. J Clin Oncol. 2005;23: Gy/20 fr (2.625 Gy/fr) vs 66 Gy/33 fr (2 Gy/fr), n = 936 Hypofractionated versus conventionally fractionated radiotherapy for prostate carcinoma: final results of phase III randomized trial. (Australia) Yeoh EE, et al. Int J Radiat Oncol Biol Phys. 2011;81: Gy/20 fr (2.75 Gy/fr) vs 64 Gy/32 fr (2 Gy/fr), n = 217 4
 Modern Clinical Trials,")




")

5 Moderate Hypofractionation (2.4 4 Gy/fr) Modern Clinical Trials, Using IGRT + 3D CRT or IMRT Cabrera AR, Lee WR. Hypofractionation for clinically i ll localized li prostate tt cancer. Semin Radiat Oncol. 2013;23: In near future, 70 Gy/2.5 Gy or 60 Gy/3 Gy (IGRT + IMRT) may become the standard Extreme Hypofractionation Trials (6 Gy/fr or More, Excluding HDR Brachy) Cabrera AR, Lee WR. Hypofractionation for clinically localized prostate cancer. Semin Radiat Oncol. 2013;23:


")
 (2 implants) (3 implants) (2 days)")
: 94% Low risk: 95% Intermediate: 93%")
![High: 93% Hormone therapy (median mo [range]) Low: 4 (3 6)](/docs-images/92/110342308/images/6-8.jpg "Inter: 6 (6 10) High: 9 (9 14) Overall: 9 (3 14) Toxicity")

6 N = Gy/6 fr. CET 38 Gy/4 fr. WBH Median follow up: 5.2 years 97% biochemical control at 8 years 3% GU Grade 3 10% GU Grade 2 <1% GI Demanes DJ, Martinez AA, et al. Int J Radiat Oncol Biol Phys. 2011;81: Largest Series of HDR Monotherapy for Low, Intermediate, and High Risk Prostate Cancer 718 patients (low high risk) treated by HDR monotherapy 9.5 Gy x 4 fr 9.5 Gy x 4fr 11.5 Gy x 3 fr (1 implant) (2 implants) (3 implants) (2 days) (2 weeks) (3 weeks) Median follow up: 52.8 mo 5 y bned (all): 94% Low risk: 95% Intermediate: 93% High: 93% Hormone therapy (median mo [range]) Low: 4 (3 6) Inter: 6 (6 10) High: 9 (9 14) Overall: 9 (3 14) Toxicity (per event) Acute GU G3: 5.4% Acute GI G3: 0.2% Late GU G3: 3.5% Late GI G3: 1.6% (None G4 5) Zamboglou N, et al. Int J Radiat Oncol Biol Phys. 2013;85: (Offenbach, Germany) 6
 High 106 (60%) Hormone P = 0.047 Yes 133 (75%) No 44 (25%) Follow up period (years) Median 6.8 Intermediate risk: 89% at 7 years Range 1.5 17.")

![5 Gy/7 fr/ 5 days Presented at ESTRO 2014 (Vienna) by Yoshioka Y (Osaka, Japan) Author [Country] Rogers [USA] Zamboglou [Germany] Hoskin [UK] Present study [Japan] Literature on HDR Monotherapy](/docs-images/92/110342308/images/7-2.jpg "for Intermediate /High Risk Prostate Cancer Total dose/ Fractions No. of patients Follow up (y) PSA control rate/ Risk group Late toxicity Grade 2* GU GI 39 Gy/6 Fr. 284 2.")
/Intermediate 36 Gy/4 Fr. 25 3.5 40.0% 4.0% 87% (3y)/High 31.5 Gy/3 Fr. 55 34.0% 7.0% 48 Gy/8 Fr. 89% (7y)/Intermediate 54 Gy/9 Fr. 177 6.8 76% (7y)/High 45.5 Gy/7 Fr. 12.4% 4.")
7 HDR Monotherapy for Intermediate /High Risk Prostate Cancer: the Longest Follow up Series Patient characteristics Biochemical control rate Treatment period No. of patients 177 Risk category Intermediate 71 (40%) High 106 (60%) Hormone P = Yes 133 (75%) No 44 (25%) Follow up period (years) Median 6.8 Intermediate risk: 89% at 7 years Range High risk: 76% at 7 years Definitions of intermediate: T2b c, GS=7 or 10<PSA<20 (Definition of PSA failure: Nadir + 2 ng/ml) high: T3 4, GS>8 or PSA>20 HDR monotherapy regimen Gy/8 fr/ 5 days 54 Gy/9 fr/ 5 days 45.5 Gy/7 fr/ 5 days Presented at ESTRO 2014 (Vienna) by Yoshioka Y (Osaka, Japan) Author [Country] Rogers [USA] Zamboglou [Germany] Hoskin [UK] Present study [Japan] Literature on HDR Monotherapy for Intermediate /High Risk Prostate Cancer Total dose/ Fractions No. of patients Follow up (y) PSA control rate/ Risk group Late toxicity Grade 2* GU GI 39 Gy/6 Fr % (5y)/Intermediate 7.7% 0.0% 38 Gy/4 Fr % (5y)/Low 38 Gy/4 Fr % (5y)/Intermediate 27.5% 2.6% 34.5 Gy/3 Fr % (5y)/High 34 Gy/4 Fr % 13.0% 95% (3y)/Intermediate 36 Gy/4 Fr % 4.0% 87% (3y)/High 31.5 Gy/3 Fr % 7.0% 48 Gy/8 Fr. 89% (7y)/Intermediate 54 Gy/9 Fr % (7y)/High 45.5 Gy/7 Fr. 12.4% 4.5% *Scored per event not per patient. Rogers CL, et al. J Urol. 2012;187: Zamboglou N, et al. Int J Radiat Oncol Biol Phys. 2013;85: Hoskin P, et al. Int J Radiat Oncol Biol Phys. 2012;82:
")




 Fuller, et al.")




")


8 Virtual HDR (CyberKnife) Indeed, this 150% arrangement of 125% isodose lines 75% resembles HDR 50% (cf. Real HDR at Osaka Univ.) Fuller, et al. Int J Radiat Oncol Biol Phys. 2008;70; Influence of Interplay Effect 2D < 3D CRT < IMRT < SBRT+IMRT? Small field (segment) irradiation would be easily influenced by interplay effect, which never be adjusted by re registration before irradiation 8


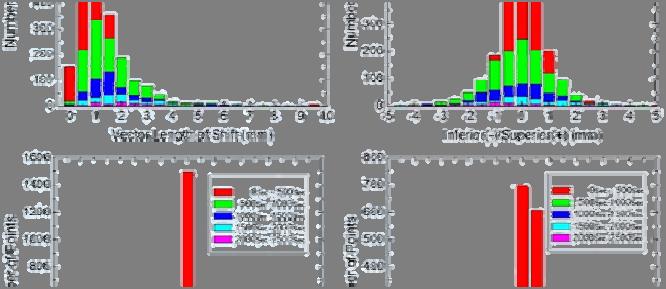
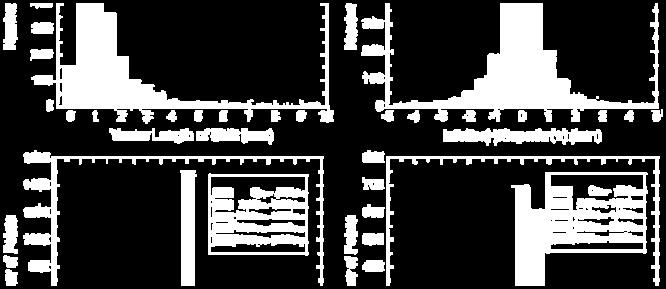
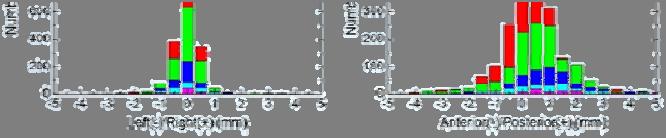
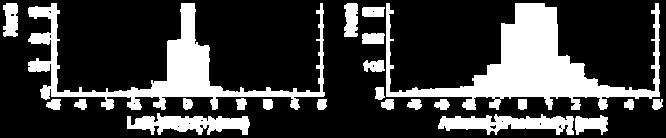
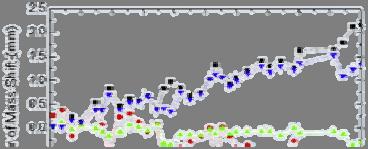




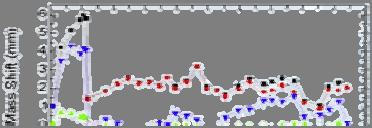
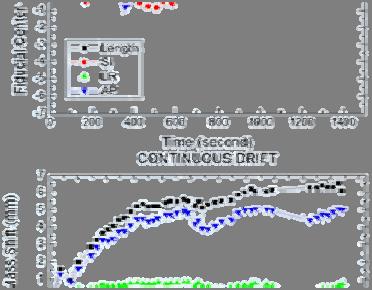
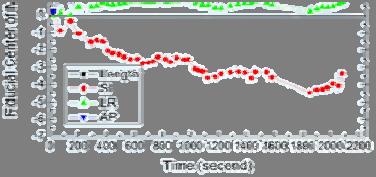
9 Stanford 2008 Intrafractional motion of the prostate during hypofractionated radiotherapy. Xie Y, et al. Int J Radiat Oncol Biol Phys. 2008;72: Fig. 4. A smaller shift observed for a shorter interval (red), whereas a larger shift for a longer interval (green, blue) Fig. 5. The amount of shift increases according to time Intra fractional Motion Is Not Constant Fig. 6(a), (b).different patterns among different patients Xie Y, et al. Int J Radiat Oncol Biol Phys. 2008;72: Fig. 7(d), (j). Different patterns among different fractions in the same patient 9





, the")





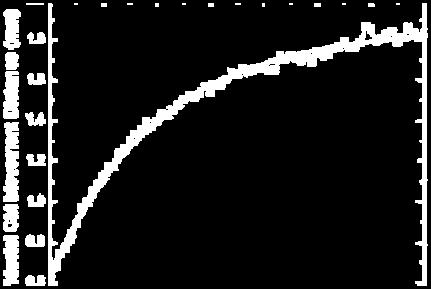
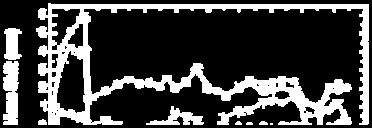
10 Ignorance Is Bliss What You Don t Know Never Hurts You Fig. 9(b). If the interval of imaging becomes twice (ie, shot frequency is 1/2), the shift looks smaller significantly Fig. 10. Shorter interval imaging is needed to detect a smaller shift with less probability Xie Y, et al. Int J Radiat Oncol Biol Phys. 2008;72:


 2012 McBride SM, et")


 4 centers, phase")



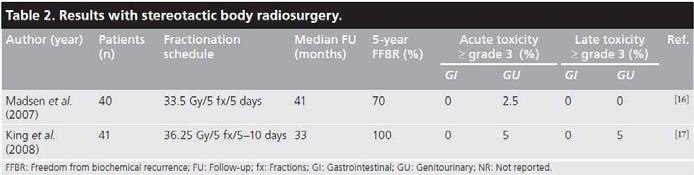
11 King, et al. Radiother Oncol. 2013;109; Stanford 2012 King CR, et al. Int J Radiat Oncol Biol Phys. 2012;82: Harvard, others (multicenter) 2012 McBride SM, et al. Cancer. 2012;118: low risk patients Median follow up: 2.7 years Gy/5 fractions (7.25 Gy/fraction) 4 centers, phase I trial 45 low risk patients 34 pts: 7.5 Gy x 5 fractions 9 pts: 7.25 Gy x 5 fractions 2 pts: other regimens Median follow up: 44.5 months bpfs rate at 3 years: 97.7% G3 late GU: 1 pt (stricture TUR P) G3 late GI: 2 pts (rectal bleed APC) G2 late GU: 7 pts (17%) G2 late GI: 3 pts (7%) 11
 Median follow up: 18.")
: Whole pelvis IMRT 45 50 Gy + 9.")
 Risk group GU GI King Stanford 67 27 2.7 94% at 4y/Low 9% 2% McBride 4 centers 45 3.")
12 UCSF 2012 Stereotactic body radiotherapy as monotherapy or post external beam radiotherapy boost for prostate cancer: technique, early toxicity, and PSA response. Jabbari S, et al. Int J Radiat Oncol Biol Phys. 2012;82: prostate cancer (low high risk) Median follow up: 18.3 months 100% biochemical control (hormone used for 47% pts) 20 patients (mainly lowintermediate risk): 9.5 Gy x 4 fractions 18 patients (mainly high risk): Whole pelvis IMRT Gy Gy x 2 fractions Margin: 0/0 mm for first 15 pts, 2/0 2 mm for latter 23 pts 60 80% isodose line prescription Reported Clinical Results of Robotic SBRT Author Institution No. of patients Median Follow up Biochemical control/ Late toxicity Grade 2 (years) Risk group GU GI King Stanford % at 4y/Low 9% 2% McBride 4 centers % at 3y/Low 19% 12% (multicenter, Prospective) Katz Flushing % at 5y/Low, 4% 2% % at 5y/Inter, 74% at 5y/High 11% 5% Ju Georgetown % at 2y/Inter 44% 7% King (multicenter, pooled) 8 centers % at 5y/Low, 84% at 5y/Inter, 81% at 5y/High NA NA 12
13 Representative Dose fractionations and BEDs of SBRT or HDR Physical dose BED (Gy) EQD 2Gy (Gy) Method Author Dose/fr (Gy) SBRT McBride (multicenter, prospective) No. of fractions Total dose (Gy) α/β =1.5 α/β =3.0 α/β =1.5 α/β = SBRT Katz SBRT King (multicenter, pooled) 7 8, Median , Median HDR Yoshioka HDR Yoshioka HDR Yoshioka HDR Rogers HDR Demanes HDR Mark HDR Martinez HDR Zamboglou HDR Hoskin HDR Ghilezan HDR Hoskin IMRT Zelefsky Clinical Trial: Robotic SBRT Mimicking HDR Dose Distribution and Fractionation Official Title: Virtual HDR CyberKnife Radiosurgery for Localized Prostatic Carcinoma: A Phase II Study Intervention Radiation: CyberKnife Radiosurgery 38 Gy in 4 fractions of 9.5 Gy/fx, over 4 5 days Status Recruiting: Start date: Primary completion date: (Anticipated) Inclusion Criteria: T1b T2b, NX/N0, M0 Gleason Sum <7 Prostate specific antigen <10 ng/ml Prostate volumes by TRUS 80 cc Principal Investigator: Donald B Fuller, MD, CyberKnife Centers of San Diego/Radiation Medical Group 13
 (73.")
 CTV =Prostate PTV = + 4 10 mm Daily target")
 is required for this protocol.")
.")
 (Note: both arms are experimental) CTV =prostate PTV")
14 Patients: low risk group Primary endpoint: Non inferiority in disease free survival (PSA fail included) (73.8 Gy is considered as equivalent to 78 Gy at isocenter prescription) CTV =Prostate PTV = mm Daily target localization (fiducial markers, transabdominal ultrasound or other) is required for this protocol. Principal Investigator: Lee WR Patients: low risk group Primary endpoint: 1y HRQOL (EPIC). To show non inferiority of either arm to RTOG 0415 (EPIC measure) (Note: both arms are experimental) CTV =prostate PTV = + 5 mm/3 mm(rectum) IMRT: mandatory Fiducial: mandatory Principal Investigator: Lukka H 14








15 Cost Comparison (USA) Technologic evolution in the treatment of prostate cancer. Clinical, financial, and legal implications for managed care organizations. Quang TS, et al. Oncology. 2007;21: , Urologists' use of intensity modulated radiation therapy for prostate cancer. Mitchell JM. N Engl J Med. 2013;369: Samples from Medicare beneficiaries age >66 1,335 SBRT patients 2,670 IMRT patients $13,645 SBRT cost $21,023 $ IMRT costt GU toxicity at 24 months 43.9% (SBRT) vs 36.3% (IMRT) (P = 0.001) (measured by Medicare claims) 15

 Inter")
![fraction error [organ motion] Intra fraction](/docs-images/92/110342308/images/16-4.jpg "error [organ motion] Gating or Chasing [Extreme]")



16 Conclusion: SBRT or HDR? Key words at the forefront of EBRT SBRT solution HDR solution IGRT (image guided radiotherapy) SBRT (stereotactic body radiotherapy) Inter fraction error [organ motion] Intra fraction error [organ motion] Gating or Chasing [Extreme] Hypofractionation [>6 Gy/fr.] Any unknown uncertainty? Or perfect substitute for HDR? OK with device OK OK Fiducial tracking? Robot? (Clinical results) Coming after, but rapidly growing OK OK Need applicator adjustment OK OK (Clinical results) Preceding, but slow accumulation Optimal dose fractionation? Slightly low? Optimal or high? 16
LDR Monotherapy vs. HDR Monotherapy
 Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT
 Donald B. Fuller, M.D. 1, John Naitoh, M.D. 2, Mark Reilly, M.D. 3, Chad Lee, Ph.D 1. 1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT Typically,
Donald B. Fuller, M.D. 1, John Naitoh, M.D. 2, Mark Reilly, M.D. 3, Chad Lee, Ph.D 1. 1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT Typically,
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer
 Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
Stereotactic ablative body radiation for prostate cancer SABR
 Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments
 Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Section: Therapy Effective Date: October 15, 2016 Subsection: Therapy Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT)
") Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Embracing Technology & Timing of Salvage Hormones
 Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE
 CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
An Update on Radiation Therapy for Prostate Cancer
 An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
PACE Study. Hypofractionation 17/12/2014. Traditional Model of Fractionation 200 Response. What s the fraction sensitivity of prostate cancer?
 0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
Hypofractionated RT in Cervix Cancer. Anuja Jhingran, MD
 Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica
 Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica 2014 HYPOFRACTIONATION & PROSTATE CANCER HYPOFRACTIONATION & PROSTATE CANCER: TECHNOLOGY: HIGH CONFORMAL DOSE & IMAGING
Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica 2014 HYPOFRACTIONATION & PROSTATE CANCER HYPOFRACTIONATION & PROSTATE CANCER: TECHNOLOGY: HIGH CONFORMAL DOSE & IMAGING
Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update
 Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update DONALD B. FULLER, M.D. RADIATION ONCOLOGIST GENESIS HEALTHCARE Disclosure & Disclaimer The
Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update DONALD B. FULLER, M.D. RADIATION ONCOLOGIST GENESIS HEALTHCARE Disclosure & Disclaimer The
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR RADIOACTIVE SEED IMPLANTATION FOR PROSTATE CANCER
 MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation. Roberto Alonzi Mount Vernon Cancer Centre
 The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
External Beam Radiation Therapy for Low/Intermediate Risk Prostate Cancer
 External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
MEDICAL POLICY. SUBJECT: BRACHYTHERAPY OR RADIOACTIVE SEED IMPLANTATION FOR PROSTATE CANCER POLICY NUMBER: CATEGORY: Technology Assessment
 MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
HDR Brachytherapy: Results and Future Studies in Monotherapy
 HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
HDR Brachytherapy: Results and Future Studies in Monotherapy Nikolaos Zamboglou and Nikolaos Tselis Strahlenklinik Klinikum Offenbach - Germany Prostate Brachytherapy UK & Ireland Conference 2013 Comparison
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Has radiotherapy the potential being focal?
 Has radiotherapy the potential being focal? György Kovács & Alexander Schlaefer* Interdisciplinary Brachytherapy Unit and *Institute of Robotics and Cognitive Systems, University of Lübeck / 1 100% 90%
Has radiotherapy the potential being focal? György Kovács & Alexander Schlaefer* Interdisciplinary Brachytherapy Unit and *Institute of Robotics and Cognitive Systems, University of Lübeck / 1 100% 90%
Hypofractionated SBRT versus conventionally fractionated EBRT for prostate cancer: comparison of PSA slope and nadir
 Anwar et al. Radiation Oncology 2014, 9:42 RESEARCH Open Access Hypofractionated SBRT versus conventionally fractionated EBRT for prostate cancer: comparison of PSA slope and nadir Mekhail Anwar *, Vivian
Anwar et al. Radiation Oncology 2014, 9:42 RESEARCH Open Access Hypofractionated SBRT versus conventionally fractionated EBRT for prostate cancer: comparison of PSA slope and nadir Mekhail Anwar *, Vivian
CyberKnife Radiotherapy For Localized Prostate Cancer: Rationale And Technical Feasibility
 Open Access Article The authors, the publisher, and the right holders grant the right to use, reproduce, and disseminate the work in digital form to all users. Technology in Cancer Research & Treatment
Open Access Article The authors, the publisher, and the right holders grant the right to use, reproduce, and disseminate the work in digital form to all users. Technology in Cancer Research & Treatment
Evaluation of Normal Tissue Complication Probability and Risk of Second Primary Cancer in Prostate Radiotherapy
 Evaluation of Normal Tissue Complication Probability and Risk of Second Primary Cancer in Prostate Radiotherapy Rungdham Takam Thesis submitted for the degree of Doctor of Philosophy in The School of Chemistry
Evaluation of Normal Tissue Complication Probability and Risk of Second Primary Cancer in Prostate Radiotherapy Rungdham Takam Thesis submitted for the degree of Doctor of Philosophy in The School of Chemistry
Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division
 IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High-Dose Rate Temporary Prostate Brachytherapy. Original Policy Date
 MP 8.01.15 High-Dose Rate Temporary Prostate Brachytherapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return
MP 8.01.15 High-Dose Rate Temporary Prostate Brachytherapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
Propensity score matched comparison of SBRT versus IMRT for the treatment of localized prostate cancer
 J Radiat Oncol (2016) 5:187 195 DOI 10.1007/s13566-015-0237-0 ORIGINAL RESEARCH Propensity score matched comparison of SBRT versus IMRT for the treatment of localized prostate cancer Caspian Oliai 1 &
J Radiat Oncol (2016) 5:187 195 DOI 10.1007/s13566-015-0237-0 ORIGINAL RESEARCH Propensity score matched comparison of SBRT versus IMRT for the treatment of localized prostate cancer Caspian Oliai 1 &
Medical Policy. MP High-Dose Rate Temporary Prostate Brachytherapy
 Medical Policy MP 8.01.33 BCBSA Ref. Policy: 8.01.33 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 7.01.79 Cryoablation of Prostate Cancer 8.01.10 Charged-Particle
Medical Policy MP 8.01.33 BCBSA Ref. Policy: 8.01.33 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 7.01.79 Cryoablation of Prostate Cancer 8.01.10 Charged-Particle
Future Directions in Prostate Cancer: The Case for Protons. John J. Coen, MD Helen & Harry Gray Cancer Center
 Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Prostate Cancer in comparison to Radiotherapy alone:
 Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
How can we best use HDR brachytherapy to escalate dose in intermediate and high risk disease? Gerard Morton Associate Professor
 How can we best use HDR brachytherapy to escalate dose in intermediate and high risk disease? Gerard Morton Associate Professor Objectives Why should we escalate dose? What HDR dose and fractionation should
How can we best use HDR brachytherapy to escalate dose in intermediate and high risk disease? Gerard Morton Associate Professor Objectives Why should we escalate dose? What HDR dose and fractionation should
Description. Section: Therapy Effective Date: October 15, 2015 Subsection: Therapy Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2015 Page: 1 of 14 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Last Review Status/Date: September 2015 Page: 1 of 14 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
The role of Radiation Oncologist: Hi-tech treatments for liver metastases
 The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
Name of Policy: High-Dose Rate Temporary Prostate Brachytherapy
 Name of Policy: High-Dose Rate Temporary Prostate Brachytherapy Policy #: 024 Latest Review Date: June 2014 Category: Therapy Policy Grade: C Background/Definitions: As a general rule, benefits are payable
Name of Policy: High-Dose Rate Temporary Prostate Brachytherapy Policy #: 024 Latest Review Date: June 2014 Category: Therapy Policy Grade: C Background/Definitions: As a general rule, benefits are payable
Prostate Cancer. 3DCRT vs IMRT : Hasan Murshed
 Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
SRO Tutorial: Prostate Cancer Clinics
 SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Salvage HDR Brachytherapy. Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK
 Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Three-year outcomes of 324 prostate carcinoma patients treated with combination high-dose-rate brachytherapy and intensity modulated radiation therapy
 Original Article Three-year outcomes of 324 prostate carcinoma patients treated with combination high-dose-rate brachytherapy and intensity modulated radiation therapy Jekwon Yeh, Brandon Lehrich, Albert
Original Article Three-year outcomes of 324 prostate carcinoma patients treated with combination high-dose-rate brachytherapy and intensity modulated radiation therapy Jekwon Yeh, Brandon Lehrich, Albert
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER
 PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
High-dose-rate brachytherapy as monotherapy for prostate cancer: technique, rationale and perspective
 Review paper Educational Activity High-dose-rate brachytherapy as monotherapy for prostate cancer: technique, rationale and perspective Yasuo Yoshioka, MD, PhD 1, Osamu Suzuki, MD, PhD 1, Yuki Otani, PhD
Review paper Educational Activity High-dose-rate brachytherapy as monotherapy for prostate cancer: technique, rationale and perspective Yasuo Yoshioka, MD, PhD 1, Osamu Suzuki, MD, PhD 1, Yuki Otani, PhD
Changing Paradigms in Radiotherapy
 Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
SBRT in early stage NSCLC
 SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER
 CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER Klinikum Offenbach Nucletron April 27 th 28 th, 2014 History HDR Protocols for Boost and Monotherapy, Results, Logistics and Practical
CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER Klinikum Offenbach Nucletron April 27 th 28 th, 2014 History HDR Protocols for Boost and Monotherapy, Results, Logistics and Practical
University of California, Los Angeles, Los Angeles, CA, 2 FROS Radiation Oncology and CyberKnife Center, Flushing, NY, 3
 Long-Term Outcomes of Stereotactic Body Radiation Therapy for Low- and Intermediate-Risk Prostate Adenocarcinoma: A Multi-Institutional Consortium Study A. U. Kishan 1, A. Katz 2, C. A. Mantz 3, F. I.
Long-Term Outcomes of Stereotactic Body Radiation Therapy for Low- and Intermediate-Risk Prostate Adenocarcinoma: A Multi-Institutional Consortium Study A. U. Kishan 1, A. Katz 2, C. A. Mantz 3, F. I.
Fractionation: why did we ever fractionate? The Multiple Fractions School won! Survival curves: normal vs cancer cells
 1 Basic Radiobiology for the Radiotherapy Physicist Colin G. Orton, Ph.D. Professor Emeritus, Wayne State University, Detroit, Michigan, USA Fractionation: why did we ever fractionate? Actually, initially
1 Basic Radiobiology for the Radiotherapy Physicist Colin G. Orton, Ph.D. Professor Emeritus, Wayne State University, Detroit, Michigan, USA Fractionation: why did we ever fractionate? Actually, initially
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
Particle (proton) Therapy Randomized trials vs. Prospective registry. Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology
 Therapy Randomized trials vs. Prospective registry. Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology") Particle (proton) Therapy Randomized trials vs. Prospective registry Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Should we do randomized trials? Are randomized trials needed
Particle (proton) Therapy Randomized trials vs. Prospective registry Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Should we do randomized trials? Are randomized trials needed
Disclosures. Proton therapy advantages. Why are comparing therapies difficult? Proton Therapy for Low Risk Prostate Cancer
 Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
LA TOMOTERAPIA IN ITALIA: ESPERIENZE A CONFRONTO
 LA TOMOTERAPIA IN ITALIA: ESPERIENZE A CONFRONTO BARD 20 NOVEMBRE 2010 DI MUZIO NADIA H. S. RAFFAELE MILANO PHASE I-II STUDY OF HYPOFRACTIONATED SIMULTANEOUS INTEGRATED BOOST WITH TOMOTHERAPY FOR PROSTATE
LA TOMOTERAPIA IN ITALIA: ESPERIENZE A CONFRONTO BARD 20 NOVEMBRE 2010 DI MUZIO NADIA H. S. RAFFAELE MILANO PHASE I-II STUDY OF HYPOFRACTIONATED SIMULTANEOUS INTEGRATED BOOST WITH TOMOTHERAPY FOR PROSTATE
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update
 BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Table of Contents Data Supplement 1: Additional Evidence Table(s) Table
BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Table of Contents Data Supplement 1: Additional Evidence Table(s) Table
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
OPTIMIZATION OF COLLIMATOR PARAMETERS TO REDUCE RECTAL DOSE IN INTENSITY-MODULATED PROSTATE TREATMENT PLANNING
 Medical Dosimetry, Vol. 30, No. 4, pp. 205-212, 2005 Copyright 2005 American Association of Medical Dosimetrists Printed in the USA. All rights reserved 0958-3947/05/$ see front matter doi:10.1016/j.meddos.2005.06.002
Medical Dosimetry, Vol. 30, No. 4, pp. 205-212, 2005 Copyright 2005 American Association of Medical Dosimetrists Printed in the USA. All rights reserved 0958-3947/05/$ see front matter doi:10.1016/j.meddos.2005.06.002
Margins in SBRT. Mischa Hoogeman
 Margins in SBRT Mischa Hoogeman MARGIN CONCEPTS Why do we use margins? Target / tumor To a-priori compensate for (unknown) deviations between the intended target position and the real target position during
Margins in SBRT Mischa Hoogeman MARGIN CONCEPTS Why do we use margins? Target / tumor To a-priori compensate for (unknown) deviations between the intended target position and the real target position during
Results of Stereotactic radiotherapy for Stage I and II NSCLC Is There a Need for Image Guidance?
 Results of Stereotactic radiotherapy for Stage I and II NSCLC Is There a Need for Image Guidance? Frank Zimmermann Institute of Radiation Oncolgy University Clinic Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch
Results of Stereotactic radiotherapy for Stage I and II NSCLC Is There a Need for Image Guidance? Frank Zimmermann Institute of Radiation Oncolgy University Clinic Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch
BRACHYTHERAPY FOR PROSTATE CANCER. Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital
, FRANZCR Radiation Oncologist, The Canberra Hospital") BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
Research Article Implant R100 Predicts Rectal Bleeding in Prostate Cancer Patients Treated with IG-IMRT to 45 Gy and Pd-103 Implant
 Radiotherapy, Article ID 130652, 6 pages http://dx.doi.org/10.1155/2014/130652 Research Article Implant R100 Predicts Rectal Bleeding in Prostate Cancer Patients Treated with IG-IMRT to 45 Gy and Pd-103
Radiotherapy, Article ID 130652, 6 pages http://dx.doi.org/10.1155/2014/130652 Research Article Implant R100 Predicts Rectal Bleeding in Prostate Cancer Patients Treated with IG-IMRT to 45 Gy and Pd-103
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy combined HDR + EBRT 574 HDR monotherapy Total Patients
 Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Overview of Advanced Techniques in Radiation Therapy
 Overview of Advanced Techniques in Radiation Therapy Jacob (Jake) Van Dyk Manager, Physics & Engineering, LRCP Professor, UWO University of Western Ontario Acknowledgements Glenn Bauman Jerry Battista
Overview of Advanced Techniques in Radiation Therapy Jacob (Jake) Van Dyk Manager, Physics & Engineering, LRCP Professor, UWO University of Western Ontario Acknowledgements Glenn Bauman Jerry Battista
Current and Emerging Standards in Radiation Therapy for Prostate Cancer
 Current and Emerging Standards in Radiation Therapy for Prostate Cancer Amandeep R. Mahal, BS, and James B. Yu, MD, MHS Abstract Improved radiation technology has allowed physicians to precisely target
Current and Emerging Standards in Radiation Therapy for Prostate Cancer Amandeep R. Mahal, BS, and James B. Yu, MD, MHS Abstract Improved radiation technology has allowed physicians to precisely target
4D Radiotherapy in early ca Lung. Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla
 4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
GRANDANGOLO: CA PROSTATA
 GRANDANGOLO: CA PROSTATA AIRO 2014, Padova Alessio G. Morganti RT dose-effect Creak A et al. Br J Cancer 2013! randomized study:! 126 patients! med. FUP: 13.7 years! T1b-T3b! neoadjuv. ADT + 3D-RT! 64
GRANDANGOLO: CA PROSTATA AIRO 2014, Padova Alessio G. Morganti RT dose-effect Creak A et al. Br J Cancer 2013! randomized study:! 126 patients! med. FUP: 13.7 years! T1b-T3b! neoadjuv. ADT + 3D-RT! 64
PROSTATE CANCER TREATMENT
 PROSTATE CANCER TREATMENT INFORMATION GUIDE Several effective treatment options exist today for men diagnosed with prostate cancer. Each man s particular cancer, overall health, age, and lifestyle will
PROSTATE CANCER TREATMENT INFORMATION GUIDE Several effective treatment options exist today for men diagnosed with prostate cancer. Each man s particular cancer, overall health, age, and lifestyle will
Stereotaxy. Outlines. Establishing SBRT Program: Physics & Dosimetry. SBRT - Simulation. Body Localizer. Sim. Sim. Sim. Stereotaxy?
 Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
Department of Radiotherapy & Nuclear Medicine, National Cancer Institute, Cairo University, Cairo, Egypt.
 Original article Res. Oncol. Vol. 12, No. 1, Jun. 2016:10-14 Dosimetric comparison of 3D conformal conventional radiotherapy versus intensity-modulated radiation therapy both in conventional and high dose
Original article Res. Oncol. Vol. 12, No. 1, Jun. 2016:10-14 Dosimetric comparison of 3D conformal conventional radiotherapy versus intensity-modulated radiation therapy both in conventional and high dose
Credentialing for the Use of IGRT in Clinical Trials
 Credentialing for the Use of IGRT in Clinical Trials James M. Galvin, DSc Thomas Jefferson University Hospital Jefferson Medical College Philadelphia, PA and The Radiation Therapy Oncology Group RADIATION
Credentialing for the Use of IGRT in Clinical Trials James M. Galvin, DSc Thomas Jefferson University Hospital Jefferson Medical College Philadelphia, PA and The Radiation Therapy Oncology Group RADIATION
Questions may be submitted anytime during the presentation.
 Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Radiotherapy Advances
 Radiotherapy Advances Not Radiotherapy Principles IMRT IGRT Image Fusion Planning Introduction IMRT = Intensity Modulated RadioTherapy Restriction: IMRT with photon beams IMRT: Highly conformal technique
Radiotherapy Advances Not Radiotherapy Principles IMRT IGRT Image Fusion Planning Introduction IMRT = Intensity Modulated RadioTherapy Restriction: IMRT with photon beams IMRT: Highly conformal technique
Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center
 Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center Seungtaek Choi, MD Assistant Professor Department tof fradiation
Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center Seungtaek Choi, MD Assistant Professor Department tof fradiation
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR
 Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Maurizio Valeriani, Stefano Bracci *, Mattia Falchetto Osti, Teresa Falco, Linda Agolli, Vitaliana De Sanctis and Riccardo Maurizi Enrici
 Valeriani et al. Radiation Oncology 2013, 8:137 RESEARCH Open Access Intermediate-risk prostate cancer patients treated with androgen deprivation therapy and a hypofractionated radiation regimen with or
Valeriani et al. Radiation Oncology 2013, 8:137 RESEARCH Open Access Intermediate-risk prostate cancer patients treated with androgen deprivation therapy and a hypofractionated radiation regimen with or
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Will CyberKnife M6 Multileaf collimator offer advantages over IRIS collimator in prostate SBRT?
 Will CyberKnife M6 Multileaf collimator offer advantages over collimator in prostate SBRT? Vindu Kathriarachchi Professional Science Master in Medical Physics Department of Physics, Florida Atlantic University,
Will CyberKnife M6 Multileaf collimator offer advantages over collimator in prostate SBRT? Vindu Kathriarachchi Professional Science Master in Medical Physics Department of Physics, Florida Atlantic University,
Dosimetric impacts of endorectal balloon in CyberKnife stereotactic body radiation therapy (SBRT) for early-stage prostate cancer
 for early-stage prostate cancer") Received: 31 October 2016 Revised: 24 January 2017 Accepted: 7 February 2017 DOI: 10.1002/acm2.12063 RADIATION ONCOLOGY PHYSICS Dosimetric impacts of endorectal balloon in CyberKnife stereotactic body
Received: 31 October 2016 Revised: 24 January 2017 Accepted: 7 February 2017 DOI: 10.1002/acm2.12063 RADIATION ONCOLOGY PHYSICS Dosimetric impacts of endorectal balloon in CyberKnife stereotactic body
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD
 Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
Erectile Dysfunction (ED) after Radiotherapy (RT) for Prostate Cancer. William M. Mendenhall, MD
 after Radiotherapy (RT) for Prostate Cancer. William M. Mendenhall, MD") Erectile Dysfunction (ED) after Radiotherapy (RT) for Prostate Cancer William M. Mendenhall, MD Meta-Analysis of Probability of Maintaining Erectile Function after Treatment of Localized Cancer Treatment
Erectile Dysfunction (ED) after Radiotherapy (RT) for Prostate Cancer William M. Mendenhall, MD Meta-Analysis of Probability of Maintaining Erectile Function after Treatment of Localized Cancer Treatment
Outcomes Following Negative Prostate Biopsy for Patients with Persistent Disease after Radiotherapy for Prostate Cancer
 Clinical Urology Post-radiotherapy Prostate Biopsy for Recurrent Disease International Braz J Urol Vol. 36 (1): 44-48, January - February, 2010 doi: 10.1590/S1677-55382010000100007 Outcomes Following Negative
Clinical Urology Post-radiotherapy Prostate Biopsy for Recurrent Disease International Braz J Urol Vol. 36 (1): 44-48, January - February, 2010 doi: 10.1590/S1677-55382010000100007 Outcomes Following Negative
STUDY CHAIR. Arica Hirsch, MD Advocate Lutheran General Hospital 1700 Luther Lane, Suite 204 Park Ridge, IL 60068
 PROSPECTIVE EVALUATION OF CYBERKNIFE AS MONOTHERAPY OR BOOST STEREOTACTIC BODY RADIOTHERAPY FOR INTERMEDIATE OR HIGH RISK LOCALIZED PROSTATE CANCER: AN OBSERVATIONAL STUDY STUDY CHAIR Arica Hirsch, MD
PROSPECTIVE EVALUATION OF CYBERKNIFE AS MONOTHERAPY OR BOOST STEREOTACTIC BODY RADIOTHERAPY FOR INTERMEDIATE OR HIGH RISK LOCALIZED PROSTATE CANCER: AN OBSERVATIONAL STUDY STUDY CHAIR Arica Hirsch, MD
Neoplasie prostatiche Radioterapia: le nuove strategie
 Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Therapy of Non-Operable early stage NSCLC
 SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical