Embracing Technology & Timing of Salvage Hormones
|
|
|
- Crystal Anthony
- 5 years ago
- Views:
Transcription

1 Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October 13, 2009

2 The Future of Prostate Cancer

3
4
:1853; June 19, 2007")
5 No Normal PSAs Thompson IM, Ankerst D. CMAJ 176(13):1853; June 19, 2007

6 Risk of Ca P vs age

7 What s our Yardstick in Prostate Ca?
8 CURE WITHOUT 99 1 COMPROMISE
9 Advances in Technology

10 Iliac LN Seminal Vesicles Prostate
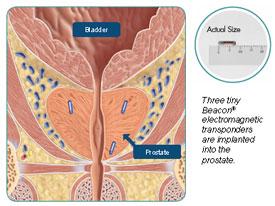
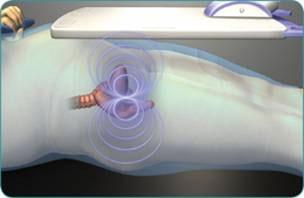
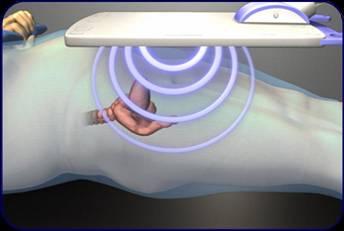
11 Radiotherapy Advances CT Plan LINAC IGRT Gold seed insert IMRT Plan


12 10 mm margin 4 mm margin Better Control Fewer visits more convenient for patient Higher capacity for RT centre Less side effects
13 Prostate Brachytherapy SEEDS Permanent Temporary HDR Monotherapy Combined with External Beam Low Risk Cancer IPSS < 15, Vol < 50 cc Intermediate / high risk IPSS < 15, Vol < 50


14 Minimally Invasive Surgery

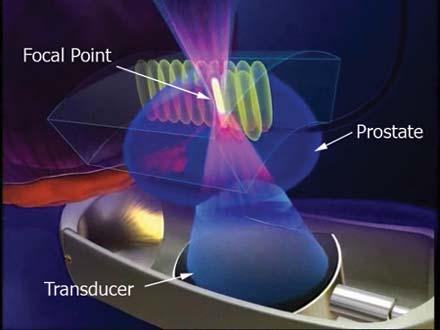
15 HIFU

16 Prostate Hypofractionation
17 Dose Escalated Radiation Therapy Pollack IJROBP 2002 n=305 Zeitman JAMA 2005 Sathya JCO 2005 Peeters JCO 2006
18 OCOG/NCIC PR5: RCT 66 Gy / 33f vs 52.5 Gy / 20f Probability of Failure HR = % CI = (0.993, 1.41) Short (n=466) n=936 mfu 5.7y Long (n=470) Years Post Randomization Lukka et al. J Clin Oncol 2005
19 Australian RCT: 64 Gy/32f vs 55 Gy/20f n = 217, median FU 48 mo Yeoh et al. IJROBP 2006; 66(4):
20 What is the α/β of prostate cancer? Brenner and Hall, 1999 n=367 Ext beam vs I-125 implant α/β = 1.5 (95% C.I ) Fowler et al, 2001 n=735 Ext Beam vs I-125/Pd-103 vs HDR α/β = 1.49 (95% CI ) Lukka et al, 2003 n=936 NCIC PR Gy/20 vs 66 Gy/33 RCT α/β = 0.9 Yeoh et al, 2003 n=120 Australian 64 Gy/32 vs 55 Gy/20 RCT α/β = 2.6 Overall n = 2158 weighted α/β = 1.3 Loblaw DA, Cheung P. Cdn J Urol 13(Suppl 1):62-6; 2006


21 Little Punches vs One Big KO! Prostate Ca HART Conventional HART
22 Hypofractionated Radiotherapy Protocol Menu Risk Category Trial Phase Duration Low risk phart3 1/2 5 f / 5 wk Intermediate risk HDR single 2 16 f / 5 wk PROFIT 3 20 f / 4 wk High Risk phart f / 5 wk Adjuvant Post-op phart f / 3 wk
23 Prostate HART 3 STUDY HYPOFRACTIONATED ACCELERATED RADIOTHERAPY FOR LOW RISK LOCALIZED PROSTATE CANCER Andrew Loblaw, Patrick Cheung Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto
24 phart3 Schema Gold feducial marker insert Primary Outcome: Secondary Outcomes: Helical Planning CT 1.5 mm slices IMRT Plan Acute GU/GI Toxicity Late GU/GI Toxicity at 3y Quality of Life (incl. ED) Positive 3y biopsy 5y bdfs Treatment On-Line Portal Imaging 35 Gy / 5 Fr 1 Fr / wk x 5 wk

25 Planning Objectives Target CTV D100% > 100% PTV D95% > 99% Normal Tissues Bladder V15% < 3300 V20% < 2800 Rectum V15% < 3180 V20% < 2800 P Bulb V90% < 2000
26 Accrual Statistics Opened October 2006 As of Sept 2009: 85 Consented Median F/U ~ 2 y
27
28
29
30
31 Virginia Mason HART Experience 33.5 / 5 / 1 wk 40 low risk patients Median follow-up 41 mo (21 67 mo) bdfs 90% Toxicity Grade 0 Grade 1-2 Grade 3 Acute GU 49% 49% 2% Acute GI 61% 39% 0% Late GU 55% 43% 2% Late GI 63% 35% 2% ED (new) 23% Madsen BL. IJROBP 67(4): ; 2007
32 Stanford Cyberknife Experience / 5f / 1-2 wks 41 low risk patients Median follow-up 33 mo (21 67 mo) bdfs 100% Benign bounce 29% G3 rectal less with qod (p = 0.003) Toxicity Grade 0 Grade 1-2 Grade 3 Acute GU (IPSS) 58% 0% 5% Acute GI (EPIC) 37% 63% 0% Late GU 71% 24% 5% Late GI 85% 15% 0% ED (new) King CR et al. IJROBP 73(4):1043-8; 2009
33 Naples Cyberknife Experience 35 / 5f / 5 days; LHRH 21/ patients (82 G6-, 29 G7, 1 G9) Median follow-up 24 mo bdfs 97% Toxicity Grade 0 Grade 1-2 Grade 3 Acute GU (IPSS) 6% Acute GI (RAS) Late GU 1% Late GI 1% ED (new) 82% Friedland JL et al. Tech Ca Res Treat 8(5):387-92; 2009
34 phart3.3

35 Seed Brachytherapy
36 SWOG 8794 pt3 Prostate Cancer N= eligible R A N D O M I Z E Adjuvant RT No RT* Outcomes bned Cause specific survival Overall survival Freedom from Distant Metastasis * 32% received delayed RT Thompson et al JAMA 2006
37 Adjuvant RT for pathologic T3 prostate cancer (SWOG 8794) Adjuvant RT Observation HR P value 10-yr bned 47% 23% 0.51 ( ) < yr FFDM 71% 61% 0.80 ( ) yr OS 74% 63% 0.76 ( ) 0.11 Thompson et al JAMA 2006 mfu = 10 years
38 SWOG 8794: mfu 12 years HR 0.71 (95% CI ), p = HR 0.72 (95% CI ), p = Thompson AUA, in press J Urol 2008

39 phart4 Schema Gold feducial marker insert Primary Outcome: Secondary Outcomes: Helical Planning CT 1.5 mm slices IMRT Plan Acute GU/GI Toxicity Late GU/GI Toxicity at 3y Quality of Life (incl. ED) 5y bdfs Treatment On-Line Portal Imaging 51 Gy / 17 Fr 3.5 wk

40 Seed Brachytherapy



41 Prostate Brachytherapy SEEDS Permanent Temporary HDR Monotherapy Combined with External Beam Low Risk Cancer IPSS < 15, Vol < 50 cc Intermediate / high risk IPSS < 15, Vol < 50
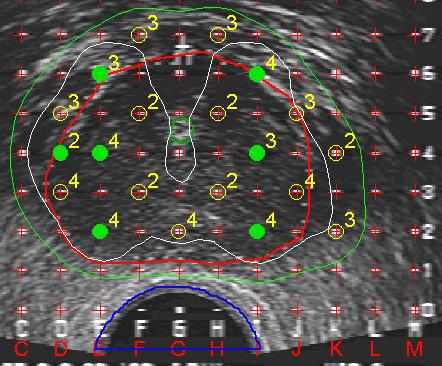
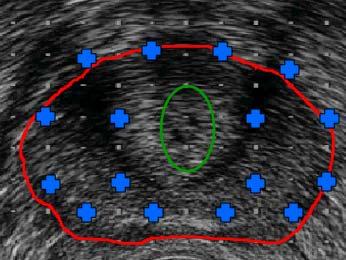
42 Pre-Implant Planning 100% isodose


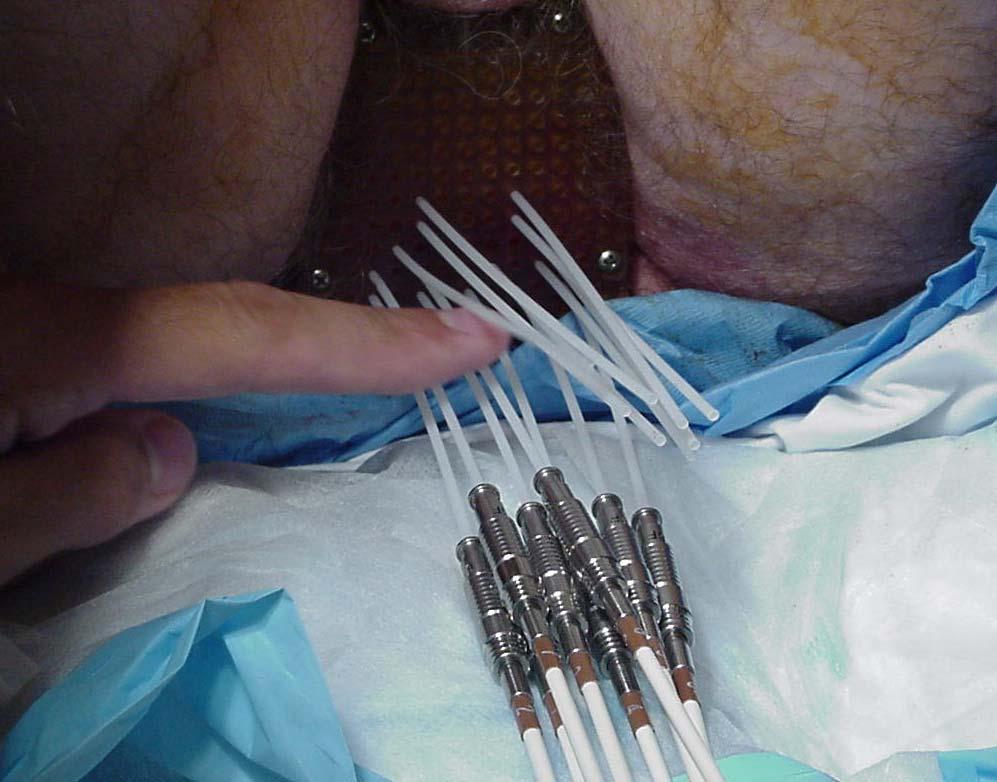
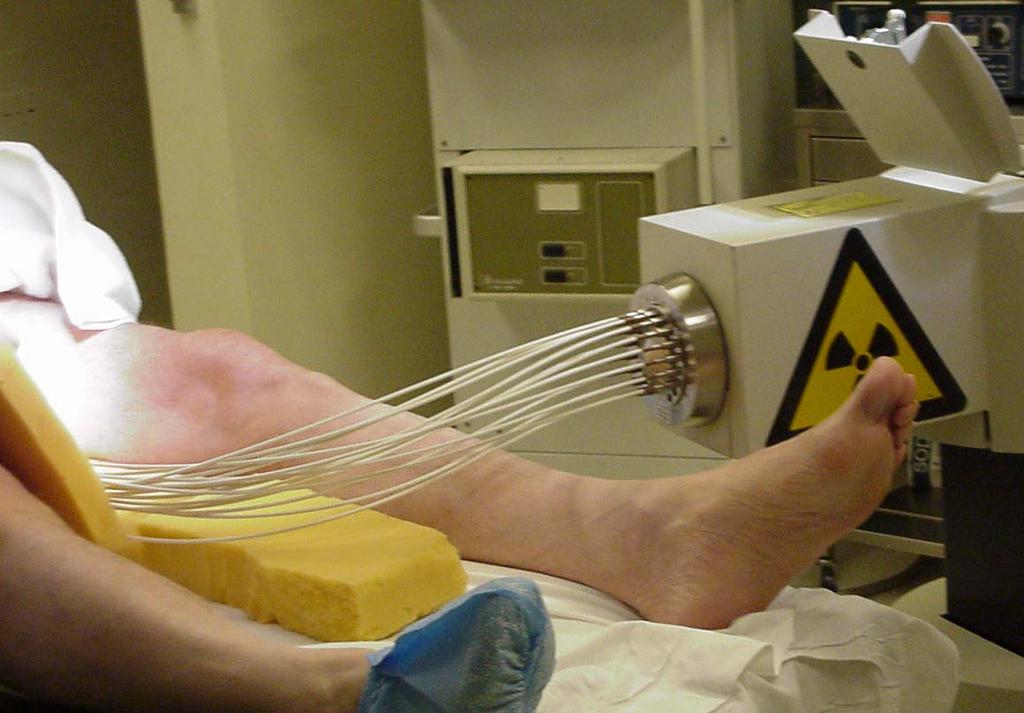
43 Anaesthesia and Positioning Spinal Positioning

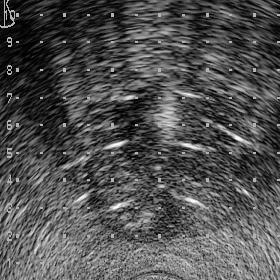
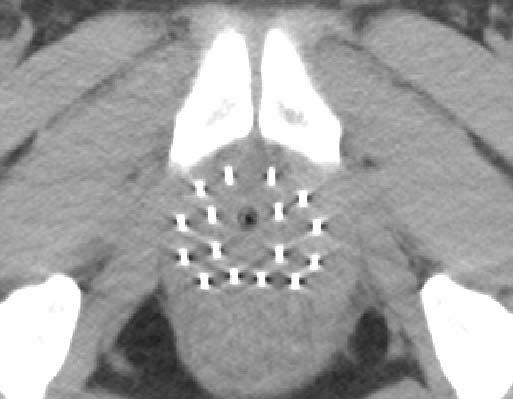
44 Needle Insertion

45 Seed Brachy Post-Implant Day 1 Thundering Waters, 11 th Hole, Niagara Falls
46 Seattle Prostate Institute Grimm,et al. Int J Radiat Oncol Biol Phys 51:31-40, 2001
47 Canadian Data Centre Started 5-yr bdfs Quebec % Sunnybrook % BCCA % PMH %
48 Disease Control (n=201) Median Follow-up = 69 months (4-102 months) 5-year Disease-Free Survival = 94% 18 failures 5 distant metastases (2.5%) 2 deaths from disease 5 local recurrence (2.5%) 3 salvage prostatectomy 1 salvage cryotherapy 8 biochemical failure only (nadir+2) (4%)

49 HDR Brachytherapy

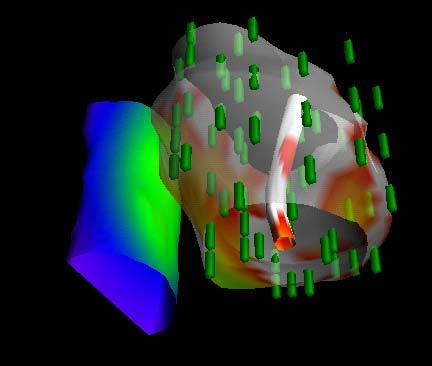
50 HDR Stepping Source Dose Distributions along single catheter

51 Treatment Administered
52 Study Schema Conventional Fractionated Gy Gy 45 Gy / 25f Single/Hypofractionated 15 Gy 37.5 Gy / 15f months




53 HDR Procedure: Outpatient, Spinal Anaesthesia Catheter Insertion CT Planning QA and Treatment Dose Optimisation

54 External Beam RT Prostate High Dose Region
55 GU Toxicity 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Conventional: GU Toxicity CTCAE v2 and RTOG n = Months from HDR 10 Gy x Gy/25 Grade 0 Grade 1 Grade 2 Grade 3 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Single Fraction: GU Toxicity CTCAE v3 n = Gy x Gy/15 Months from HDR Less Acute Grade 3 with Single Fraction No difference in late effects, but different toxicity scales
56 GI Toxicity 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Conventional: GI Toxicity CTCAE v2 and RTOG n = Months from HDR 10 Gy x Gy/25 Grade 0 Grade 1 Grade 2 Grade 3 Single Fraction: GI Toxicity CTCAE v3 n = % 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Gy x Gy/15 Months from HDR Minimal GI toxicity with either protocol < 5% Grade 2 GI toxicity at 2 years
57 Efficacy- PSA PSA Failure: Conventional: 3/58 (5%) HDR Single: 0/ Mean PSA 8 6 NO DIFFERENCE HDR Single Conventional Time in months

58 Efficacy: 2 year biopsy
59 McGill HDR Experience 10 Gy + 50/20 EBRT (CTV + 7mm) Intermediate risk pr ca: n=137, 100 with FU > 2 y mfu = 59mo Biopsy: 95% negative (35/37) bdfs: 90% (7% mets) Toxicity Grade 2 Grade 3 Acute GU n/r 0% Acute GI n/r 0% Late GU 2% 1% Late GI 2% 1% Erectile Dys 31% Cury F et al., CARO 2009 abstract 34
60 HDR RCTs P = Hoskin et al Radioth Oncol /20 vs 36/ /2 HDR boost N = 220, mfu = 30 mo Sathya et al J Clin Oncol /33 vs 40/ Gy / 48 hrs N=104, 60% HR, 40% IR mfu = 8.2 y

61 HDR RCTs Guix et al., Am Brachy Soc pts, mfu 55mo 76/38 vs 46/ /2 HDR boost

62 Recurrent Prostate Cancer After Radical Radiotherapy
63 Post-Radiotherapy Failure Local therapies Radical prostatectomy Cryotherapy HiFU Seed brachytherapy* ANDROGEN DEPRIVATION THERAPY ASCO Androgen Sensitive Guideline 2006 Update available April 2007
64 Burden of Problem Extent of disease Incidence Localized Metastatic 17,225 3,151 (85%) (15%) Skarsgard D, Tonita J. Ca Cause Control 2000; Cdn Cancer Stats 2006
65 Burden of Problem Localized disease Incidence 5 yr Biochemical Failure At risk (n) Post-RT (n) Low risk 5391 (31%) Intermediate 4852 (28%) High risk 6982 (41%) % overall (2570 post-rt) Skarsgard D, Tonita J. Ca Cause Control 2000; Cdn Cancer Stats 2006
66 RCTs Timing of ADT Post Radical RT TROG Timing of Androgen Deprivation (TOAD) ongoing
67 Patterns of Care Survey Oncologists Survey (%) Trigger PSA (ng/ml) for starting ADT 1994 Canada 2000 USA 2004 Canada < > Skarsgard D, Tonita J. Ca Cause Control 2000; Cdn Cancer Stats 2006
68 ASCO Guidelines Until data from studies using modern medical diagnostic/ biochemical tests and standardized follow-up schedules become available, no specific recommendations can be issued regarding the question of early versus deferred ADT. A discussion about the pros and cons of early versus deferred ADT should occur. Loblaw DA et al J Clin Oncol 2004;14: In metastatic or progressive PCa, immediate versus symptomonset institution of ADT results in a moderate decrease (17%) in relative risk (RR) for PCa-specific mortality, a moderate increase (15%) in RR for non PCa-specific mortality, and no overall survival advantage. Therefore, the Panel cannot make a strong recommendation for early ADT initiation. For patients electing to wait until symptoms for ADT, regular monitoring visits are indicated. Loblaw DA et al J Clin Oncol 2007; 25(12):
69 Prostate Cancer Mortality
70 Overall Mortality
71 Unanswered Questions 1. What are the benefits of immediate ADT following radiation therapy Can we extrapolate from Watchful Waiting / Metastatic patient data? 2. What is the magnitude of detriment on QOL?
72 ADT Side Effects Vasomotor symptoms Decreased libido erectile dysfunction Decreased muscle mass Decreased energy Metabolic syndrome Osteopenic effects
 fracture (living >5 yr) bone metastases not")
73 50,613 men with Prostate Cancer in SEER database % vs 12% had (any) fracture (living >5 yr) bone metastases not excluded


74 73,197 men > 66 yr in SEER, Medicare 1/3 had LHRH agonist Excluded prevalent M1, DM, CAD In 10 years 9% 11% 3% 4%
75 Prognostic Factors Predictors Overall Mortality Cause specific Mortality Distant Metastases PSAdt (< 6months) D Amico 2006 Kim-Sing 2004 Pound 1999 Gleason Score (8-10) Pound 1999 PSA response to ADT D Amico 2006 Age < 75yr D Amico Does the effect of timing of ADT differ by PSAdt, Gleason?
76 Timing of ADT for Recurrent Prostate Cancer
77 ELAAT Survey 96 Canadian Specialists 42 GU Radiation Oncologists 50 Urologists 4 Medical Oncologists Current Practice Trigger: PSAdt (28%), PSA (3%), both (69%) Start treatment if PSAdt < 12months (95%) Start treatment if PSA (ng/ml) <10 (53%), (36%) Orchiectomy (0%)
78 ELAAT Survey Trial comfort zones to start ADT Lowest PSA to start ADT: 4ng/mL (58%) 5ng/mL (86%) Highest PSA to withhold ADT: 25ng/mL (61%) PSAdt trigger: < 12 months (71%) Need for Trial Moderate to very important (86%) Very important (51%) Number of patients per year: 1500+
79 ELAAT STUDY A Randomized Comparison of Immediate versus Deferred Androgen Deprivation Therapy using Goserelin for Recurrent Prostate Cancer after Radical Radiotherapy Andrew Loblaw, Sergio Faria, Himu Lukka, Tom Pickles, Patrick Cheung, Lawrence Klotz, Kathy Pritchard, Martin Gleave, Tulay Koru-Singul, Mark Levine
80 ELAAT Study Schema Localized Prostate Cancer Asymptomatic biochemical failure post RT n = 1100 R A N D O M I Z E Immediate LHRH Deferred LHRH (at symptom onset) (or PSA>25ng/mL) Outcomes Time to Androgen Independent Disease Cause specific survival Overall survival Quality of Life Complications of Advanced Malignancy Bone Fractures

81 ELAAT Enrolment Does Not Preclude Enrolment in Any Other Clinical Trial
82 ELAAT Study Status First Center Activated May 2007 # Centers Activated 14 # Patients entered (Sept 09) 67
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
LDR Monotherapy vs. HDR Monotherapy
 Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
An Update on Radiation Therapy for Prostate Cancer
 An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
When radical prostatectomy is not enough: The evolving role of postoperative
 When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy?
 Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Prostate cancer: Update from the BCCA
 Prostate cancer: Update from the BCCA Tom Pickles Clinical Professor, UBC Topics 1. Incidence & Utilization rates 2. New developments with External Beam RT IGRT, VMAT and other enhancements Optimizing
Prostate cancer: Update from the BCCA Tom Pickles Clinical Professor, UBC Topics 1. Incidence & Utilization rates 2. New developments with External Beam RT IGRT, VMAT and other enhancements Optimizing
Salvage HDR Brachytherapy. Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK
 Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy. Dr. Matt Andrews Supervisor: Dr. David Bowes
 The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
External Beam Radiation Therapy for Low/Intermediate Risk Prostate Cancer
 External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
PORT after RP. Adjuvant. Salvage
 PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
How to deal with patients who fail intracavitary treatment
 How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER
 PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
Timing of Androgen Deprivation: The Modern Debate Must be conducted in the following Contexts: 1. Clinical States Model
 Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Brachytherapy for Prostate Cancer
 Brachytherapy for Prostate Cancer Who should be thinking about this and why... Juanita Crook Professor Radiation Oncology University of Toronto Princess Margaret Hospital Many options watchful waiting?
Brachytherapy for Prostate Cancer Who should be thinking about this and why... Juanita Crook Professor Radiation Oncology University of Toronto Princess Margaret Hospital Many options watchful waiting?
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
The Spa Hotel, Tunbridge Wells Friday 23 rd March Platinum sponsor
 The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update
 BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Table of Contents Data Supplement 1: Additional Evidence Table(s) Table
BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Table of Contents Data Supplement 1: Additional Evidence Table(s) Table
Disclosures. Proton therapy advantages. Why are comparing therapies difficult? Proton Therapy for Low Risk Prostate Cancer
 Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER
 CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER Klinikum Offenbach Nucletron April 27 th 28 th, 2014 History HDR Protocols for Boost and Monotherapy, Results, Logistics and Practical
CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER Klinikum Offenbach Nucletron April 27 th 28 th, 2014 History HDR Protocols for Boost and Monotherapy, Results, Logistics and Practical
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
BRACHYTHERAPY FOR PROSTATE CANCER. Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital
, FRANZCR Radiation Oncologist, The Canberra Hospital") BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT
 Donald B. Fuller, M.D. 1, John Naitoh, M.D. 2, Mark Reilly, M.D. 3, Chad Lee, Ph.D 1. 1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT Typically,
Donald B. Fuller, M.D. 1, John Naitoh, M.D. 2, Mark Reilly, M.D. 3, Chad Lee, Ph.D 1. 1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT Typically,
How can we best use HDR brachytherapy to escalate dose in intermediate and high risk disease? Gerard Morton Associate Professor
 How can we best use HDR brachytherapy to escalate dose in intermediate and high risk disease? Gerard Morton Associate Professor Objectives Why should we escalate dose? What HDR dose and fractionation should
How can we best use HDR brachytherapy to escalate dose in intermediate and high risk disease? Gerard Morton Associate Professor Objectives Why should we escalate dose? What HDR dose and fractionation should
Neoplasie prostatiche Radioterapia: le nuove strategie
 Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy combined HDR + EBRT 574 HDR monotherapy Total Patients
 Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Stereotactic ablative body radiation for prostate cancer SABR
 Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
Prostate Cancer. GU Practice Guideline
 Prostate Cancer GU Practice Guideline This guideline is a statement of consensus of the GU Disease Site Team regarding their views of currently accepted approaches to treatment. It is not intended to replace
Prostate Cancer GU Practice Guideline This guideline is a statement of consensus of the GU Disease Site Team regarding their views of currently accepted approaches to treatment. It is not intended to replace
SRO Tutorial: Prostate Cancer Clinics
 SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE
 CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
Androgen Deprivation Therapy A Question of Timing
 Androgen Deprivation Therapy A Question of Timing James Johnston BSc MBChB FRACS (Urol) Disclosure 1 OUTLINE History Watchful waiting Node positive patient Recurrence Intermittent Androgen Suppression
Androgen Deprivation Therapy A Question of Timing James Johnston BSc MBChB FRACS (Urol) Disclosure 1 OUTLINE History Watchful waiting Node positive patient Recurrence Intermittent Androgen Suppression
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer
 Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD
 Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Prostate Cancer in comparison to Radiotherapy alone:
 Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April
 Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April 17, 2016 Discuss permanent prostate brachytherapy and
Trina Lynd, M.S. Medical Physicist Lifefirst Imaging & Oncology Cullman, AL Tri-State Alabama, Louisiana and Mississippi Spring 2016 Meeting April 17, 2016 Discuss permanent prostate brachytherapy and
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT)
") Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Prostate Cancer Appraisal Addendum: Stereotactic Body Radiation Therapy (SBRT) The Institute for Clinical and Economic Review (ICER) has published appraisals on multiple management options for clinically-localized,
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
GRANDANGOLO: CA PROSTATA
 GRANDANGOLO: CA PROSTATA AIRO 2014, Padova Alessio G. Morganti RT dose-effect Creak A et al. Br J Cancer 2013! randomized study:! 126 patients! med. FUP: 13.7 years! T1b-T3b! neoadjuv. ADT + 3D-RT! 64
GRANDANGOLO: CA PROSTATA AIRO 2014, Padova Alessio G. Morganti RT dose-effect Creak A et al. Br J Cancer 2013! randomized study:! 126 patients! med. FUP: 13.7 years! T1b-T3b! neoadjuv. ADT + 3D-RT! 64
Prostate Cancer. 3DCRT vs IMRT : Hasan Murshed
 Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
High-Dose Rate Temporary Prostate Brachytherapy. Original Policy Date
 MP 8.01.15 High-Dose Rate Temporary Prostate Brachytherapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return
MP 8.01.15 High-Dose Rate Temporary Prostate Brachytherapy Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return
Section: Therapy Effective Date: October 15, 2016 Subsection: Therapy Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
2018 ASTRO Refresher Course: Prostate Cancer. Timur Mitin, MD PhD Oregon Health and Science University
 2018 ASTRO Refresher Course: Prostate Cancer Timur Mitin, MD PhD Oregon Health and Science University Disclosures UpToDate Chapter author, royalties Oregon Health and Science University Practicing Radiation
2018 ASTRO Refresher Course: Prostate Cancer Timur Mitin, MD PhD Oregon Health and Science University Disclosures UpToDate Chapter author, royalties Oregon Health and Science University Practicing Radiation
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Prostatectomy as salvage therapy. Cases. Paul Cathcart - Guy s & St Thomas NHS Trust, London
 Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update
 Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update DONALD B. FULLER, M.D. RADIATION ONCOLOGIST GENESIS HEALTHCARE Disclosure & Disclaimer The
Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update DONALD B. FULLER, M.D. RADIATION ONCOLOGIST GENESIS HEALTHCARE Disclosure & Disclaimer The
Management. Localized Prostate Cancer. Andrew K. Lee, MD, MPH Associate Professor M.D. Anderson Cancer Center
 Management of Localized Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor M.D. Anderson Cancer Center Disclosure Information Ad Andrew K. KLee Dr. Lee has indicated no financial relationships,
Management of Localized Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor M.D. Anderson Cancer Center Disclosure Information Ad Andrew K. KLee Dr. Lee has indicated no financial relationships,
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Radiotherapy Considerations in Extremity Sarcoma
 Radiotherapy Considerations in Extremity Sarcoma Peter Chung Department of Radiation Oncology Princess Margaret Hospital University of Toronto Role of RT in STS Local tumour eradication while allowing
Radiotherapy Considerations in Extremity Sarcoma Peter Chung Department of Radiation Oncology Princess Margaret Hospital University of Toronto Role of RT in STS Local tumour eradication while allowing
Active surveillance for low-risk Prostate Cancer Compared with Immediate Treatment: A Canadian cost evaluation
 Active surveillance for low-risk Prostate Cancer Compared with Immediate Treatment: A Canadian cost evaluation Alice Dragomir, PhD Fabio Cury, MD Armen Aprikian, MD Introduction Clinical and economic burden
Active surveillance for low-risk Prostate Cancer Compared with Immediate Treatment: A Canadian cost evaluation Alice Dragomir, PhD Fabio Cury, MD Armen Aprikian, MD Introduction Clinical and economic burden
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Salvage low-dose-rate 125 I partial prostate brachytherapy after dose-escalated external beam radiotherapy
 Case report Salvage low-dose-rate 125 I partial prostate brachytherapy after dose-escalated external beam radiotherapy Lynn Chang, MD 1, Mark K. Buyyounouski, MD, MS 2 Case Report 1 Department of Radiation
Case report Salvage low-dose-rate 125 I partial prostate brachytherapy after dose-escalated external beam radiotherapy Lynn Chang, MD 1, Mark K. Buyyounouski, MD, MS 2 Case Report 1 Department of Radiation
Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica
 Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica 2014 HYPOFRACTIONATION & PROSTATE CANCER HYPOFRACTIONATION & PROSTATE CANCER: TECHNOLOGY: HIGH CONFORMAL DOSE & IMAGING
Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica 2014 HYPOFRACTIONATION & PROSTATE CANCER HYPOFRACTIONATION & PROSTATE CANCER: TECHNOLOGY: HIGH CONFORMAL DOSE & IMAGING
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Prognostic Factors for Overall Survival and Risk Stratification of Prostate Cancer Patients with Biochemical Failure
 Western University Scholarship@Western Electronic Thesis and Dissertation Repository September 2015 Prognostic Factors for Overall Survival and Risk Stratification of Prostate Cancer Patients with Biochemical
Western University Scholarship@Western Electronic Thesis and Dissertation Repository September 2015 Prognostic Factors for Overall Survival and Risk Stratification of Prostate Cancer Patients with Biochemical
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
The benefit of a preplanning procedure - view from oncologist. Dorota Kazberuk November, 2014 Otwock
 The benefit of a preplanning procedure - view from oncologist Dorota Kazberuk 21-22 November, 2014 Otwock Brachytherapy is supreme tool in prostate cancer management with a wide range of options in every
The benefit of a preplanning procedure - view from oncologist Dorota Kazberuk 21-22 November, 2014 Otwock Brachytherapy is supreme tool in prostate cancer management with a wide range of options in every
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Radical Prostatectomy:
 Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
Medical Policy. MP High-Dose Rate Temporary Prostate Brachytherapy
 Medical Policy MP 8.01.33 BCBSA Ref. Policy: 8.01.33 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 7.01.79 Cryoablation of Prostate Cancer 8.01.10 Charged-Particle
Medical Policy MP 8.01.33 BCBSA Ref. Policy: 8.01.33 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Therapy Related Policies 7.01.79 Cryoablation of Prostate Cancer 8.01.10 Charged-Particle
Salvage prostatectomy for post-radiation adenocarcinoma with treatment effect: Pathological and oncological outcomes
 ORIGINAL RESEARCH Salvage prostatectomy for post-radiation adenocarcinoma with treatment effect: Pathological and oncological outcomes Michael J. Metcalfe, MD ; Patricia Troncoso, MD 2 ; Charles C. Guo,
ORIGINAL RESEARCH Salvage prostatectomy for post-radiation adenocarcinoma with treatment effect: Pathological and oncological outcomes Michael J. Metcalfe, MD ; Patricia Troncoso, MD 2 ; Charles C. Guo,
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer