Clinical Study Retrospective Analysis of Cushing s Disease with or without Hyperprolactinemia
|
|
|
- Margaret Underwood
- 5 years ago
- Views:
Transcription
1 International Endocrinology, Article ID , 8 pages Clinical Study Retrospective Analysis of Cushing s Disease with or without Hyperprolactinemia Cheng Huan, 1 Chao Lu, 2 Guang-ming Xu, 1 Xin Qu, 3 and Yuan-ming Qu 1 1 Department of Neurosurgery, Shandong Provincial Hospital Affiliated to Shandong University, Jinan , China 2 Department of Laboratory Medicine, Shandong Provincial Hospital Affiliated to Shandong University, Jinan , China 3 Department of Intensive Care Unit, Shandong Provincial Hospital Affiliated to Shandong University, Jinan , China Correspondence should be addressed to Yuan-ming Qu; quyuanming2014@163.com Received 17 July 2014; Accepted 27 October 2014; Published 23 November 2014 Academic Editor: Ludwik K. Malendowicz Copyright 2014 Cheng Huan et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Objective. We compared the characteristics of patients with Cushing s disease alone with those of patients with Cushing s disease and hyperprolactinemia. Methods. Eighty-four patients were enrolled between 2002 and 2011, in a hospital in China. Clinical, endocrinological, and histopathological data, MRI scans, and surgical outcomes were reviewed throughout the follow-up period. Results. Patients with Cushing s disease and hyperprolactinemia had a younger age at diagnosis (30.28 ± versus ± years; P = 0.037) and a larger adenoma maximal diameter (2.44 ± 1.32 versus 1.44 ± 1.05 cm; P < 0.001) than patients with Cushing s disease alone. Menstrual disorders (P = 0.027) and visual field defects (P = 0.021) were more common and progressive obesity (P = 0.009)andhypertension(P < 0.001) were less common in patients with Cushing s disease and hyperprolactinemia. The rate of normalization of hormonal levels was lower (41.7% versus 91.7%; P < 0.001) and the recurrence rate was higher (36.1% versus 8.3%; P < 0.001) in patients with Cushing s disease and hyperprolactinemia. Conclusions. Careful long-term follow-up is needed of patients with Cushing s disease and hyperprolactinemia. 1. Introduction The most common etiology of spontaneous excess cortisol production is Cushing s disease due to hypersecretion of pituitary adrenocorticotropic hormone (ACTH) by a corticotroph adenoma [1]. Cushing s disease is a rare disorder, with an annual incidence of 1 3 per million and a female : male ratioof3:1,thatisresponsibleforsignificantmorbidity and mortality resulting from cardiovascular complications, infections, and psychiatric disturbances [2]. It is now recognized that, in a small proportion of cases, Cushing s disease is accompanied by an elevated prolactin (PRL) level. For example, Lado-Abeal and colleagues identified a mildly elevated serum PRL in 20% of women with Cushing s disease and menstrual abnormalities [3],andbothMahleretal.[4] and Sherry et al. [5] have presented a patient with Cushing s disease and symptomatic hyperprolactinemia. Although Cushing s disease with hyperprolactinemia due to mixed ACTH- and PRL-secreting adenomas occurs rarely, elevated preoperative PRL levels in Cushing s disease are of diagnostic significance. Despite the abundance of published data concerning various aspects of the clinical course and treatment of Cushing s disease, very few investigations have focused on the characteristics of patients with Cushing s disease and hyperprolactinemia, and there is a paucity of studies comparing the clinical features of patients with Cushing s disease and hyperprolactinemia and those with Cushing s disease but no hyperprolactinemia. This is particularly the case for patients in China, about whom very little information is available concerning clinical outcomes following transsphenoidal surgery. The aims of our investigation were to describe the prevalence and clinical features of Cushing s disease in patients treated with transsphenoidal surgery at our hospital in China and to evaluate the differences between patients with Cushing s disease and hyperprolactinemia and those with Cushing s disease alone. We therefore performed a retrospective analysis of patients with Cushing s disease, with or without concomitant hyperprolactinemia, to clarify the


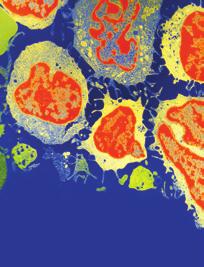
2 2 International Endocrinology (a) (b) Figure 1: Representative T1-weighted coronal MRI scans. (a) Microadenoma (arrow). (b) Macroadenoma expanding into the suprasellar cistern (arrow). clinical features and confirm the efficacy of transsphenoidal surgery for treatment of the disease. This study provides novel insights that extend our current knowledge and will help to improve the diagnosis and treatment of patients with Cushing s disease and hyperprolactinemia. 2. Materials and Methods 2.1. Patients. This was a retrospective study of patients diagnosed with Cushing s disease, who had been treated by primary transsphenoidal surgery between January 2002 and June 2011, at the Department of Neurosurgery, Shandong Provincial Hospital Affiliated to Shandong University, Jinan, Shandong,China.ThediagnosisofCushing sdiseasewas made on the basis of the medical history, symptoms, the levels of serum hormones, immunohistochemical staining, computer-aided tomographic (CT) imaging, and magnetic resonance imaging (MRI). Patients were divided into two groups, according to the preoperative hormonal levels and immunohistochemical results: a CD group (patients with elevatedcortisolonly)andacd+prlgroup(patientswithboth elevated cortisol and PRL levels). Due to the retrospective nature of this study, written informed consent was deemed not to be required. Oral informed consent was obtained from each participant, and the data were analyzed anonymously. The Ethics Committee of the Shandong Provincial Hospital Affiliated to Shandong University approved the research protocols. Patients were included in the study if all the following criteria were satisfied: classical signs and symptoms of Cushing s disease; increased serum cortisol levels; loss of diurnal rhythm of serum cortisol; increased 24-hour urinary free cortisol levels; normal or slightly elevated plasma ACTH levels; lack of suppression of urinary free cortisol and serum cortisol following oral 2 mg dexamethasone loading; suppression of urinary free cortisol and serum cortisol after oral 16 mg dexamethasone (urinary free cortisol and/or serum cortisol suppressed by >50% of the baseline value following oral administration of 2 mg dexamethasone every 6 hours for 48 hours); an adenoma staining positively for ACTH; the presence of a pituitary mass on MRI; treatment by surgery alone; and availability of a complete set of medical records. An additional inclusion criterion required for the CD + PRL group was an adenoma staining positive for PRL. The exclusion criteria for the CD group were patients with hypersecretion of two or more hormones; adenomas with positive immunohistochemical staining for two or more hormones; adrenal-derived Cushing s syndrome; ectopic Cushing s syndrome; and other potential causes of an elevated cortisol level. The exclusion criteria for the CD + PRL group were patients with hypersecretion of two or more hormones (except for cortisol and PRL); adenomas with positive immunohistochemical staining for two or more hormones (except for ACTH and PRL); and other causes of elevated cortisol and PRL levels. Microscopically assisted transsphenoidal pituitary tumor resection surgery was performed by two experienced neurosurgeons (Yuan-ming Qu and Guang-ming Xu), and the resection was considered subtotal or complete in all enrolled patients. In order to accurately assess the effects of surgery, only patients treated by surgery alone were included in this study Data Extracted from the Medical Records. The data collectedincludedtheageandgenderofthepatient,pastmedical history, clinical presentation, preoperative neurological, endocrine, and ophthalmological status, and postoperative outcomes. The time from the onset of symptoms and signs tothedateofdiagnosis(timetodiagnosis)wasnoted Investigations. The tumor size was measured using MRI. A microadenoma was defined as a tumor with a diameter of 10 mm or less, whereas a macroadenoma was defined as a tumor with a diameter of more than 10mm [6]. Representative T1-weighted coronal MRI scans showing an example of a microadenoma and a macroadenoma are shown in Figure 1. Cavernous sinus invasion was suspected when adenoma tissue was located lateral to the cavernous portion of
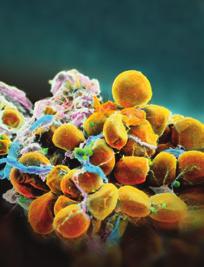
 H&E staining of tumor tissue from a patient in the CD + PRL group. (c) Immunohistochemistry: cells of the adenoma from a patient in the CD group were immunoreactive to antibodies against ACTH.")

, thyroid stimulating hormone (TSH), luteinizing hormone")
 with a functional sensitivity of <8.")
. The normal range for PRL is 2.64 13.13 ng/ml in males, 3.34 26.")
3 International Endocrinology 3 (a) (b) (d1) (c) (d2) (d) Figure 2: Surgical pathology analyses of the tumors. (a) H&E staining of tumor tissue from a patient in the CD group. (b) H&E staining of tumor tissue from a patient in the CD + PRL group. (c) Immunohistochemistry: cells of the adenoma from a patient in the CD group were immunoreactive to antibodies against ACTH. (d) Immunohistochemistry: cells of the adenoma from a patient in the CD + PRL group were immunoreactive to antibodies against ACTH (d1) and PRL (d2). the internal carotid artery on MRI. Definite diagnosis could be made when the medial wall of the cavernous sinus was found to be destroyed during surgery by invasion [7]. The Knosp grade from the radiology findings was classified for degree of invasion. Pituitary imaging was also performed three months after surgery. Endocrinological assessment was carried out in all patients, including measurements of the serum levels of cortisol, PRL, growth hormone (GH), thyroid stimulating hormone (TSH), luteinizing hormone (LH), follicle stimulating hormone (FSH), testosterone, estradiol, thyroxine, and progesterone. In this study, cortisol was measured using an electrochemiluminescent immunoassay kit (Roche Diagnostics GmbH, Mannheim, Germany) with a functional sensitivity of <8.5 nmol/l and intra-assay and interassay variation coefficients of <10% and <15%, respectively. The normal range for cortisol is nmol/l. The serum level of PRL was measured using a commercially available chemiluminescence kit (Beckman Coulter, Inc., Brea, CA, USA). The normal range for PRL is ng/ml in males, ng/ml in premenopausal females, and ng/ml in postmenopausal females. The analytical sensitivity for PRL was 0.25 ng/ml, and the intra-assay and interassay variation coefficients were <10% and <15%, respectively. Serum levels of cortisol and PRL were evaluated in all patients on three occasions: 3 days after surgery, approximately 3 months after surgery, and 12 months after surgery. The resected tumor fragments were fixed in 10% buffered formalin, stained with hematoxylin and eosin (H&E) using routine histochemical methods, and embedded in paraffin blocks. Immunohistochemical analysis was also performed on specimens, using specific antibodies against ACTH (rabbit polyclonal antibody; Maxin Co. Ltd., Fujian, China), GH (rabbit polyclonal antibody; Maxin Co. Ltd., Fujian, China), PRL (rabbit polyclonal antibody; Maxin Co. Ltd., Fujian, China), FSH (mouse monoclonal antibody; Maxin Co. Ltd., Fujian, China), LH (mouse monoclonal antibody; Maxin Co. Ltd., Fujian, China), and TSH (mouse monoclonal antibody; Maxin Co. Ltd., Fujian, China). An Olympus BX53 upright fluorescence microscope (Olympus Co. Ltd., Shinjuku, Japan) was used to view and record the images. Examples of images obtained using these pathological techniques are shown in Figure 2 (original magnification 400) Postoperative Complications. Postoperative complications were divided into major and minor categories. A major complication was considered to be a disease or injury diagnosed after surgery that was potentially fatal and/or resulted in a permanent defect. Less serious adverse events, including diabetes insipidus (DI) and hyponatremia, were counted as minor complications. Urine volume measurements and serum electrolyte analyses were carried out for all patients. Serum levels of sodium were measured immediately before surgery and on days 1, 3, and 7 after surgery; hyponatremia was diagnosed when the serum sodium level
4 4 International Endocrinology was 135 mmol/l, and, when present, its onset, frequency, and time course were monitored. Central DI includes both transient DI and permanent DI [8]; transient DI is diagnosed when hypotonic polyuria (40 ml/kg body weight daily) ensues soon after surgery and is usually self-remitting within a few days. Since permanent DI requires assessment of endocrine function several months after surgery, the incidence of DI in this study may only represent transient DI Follow-Up. Allpatientswerefollowedupasoutpatients for three months after surgery and then at annual or biannual intervals. Follow-up information for patients not attending our department was obtained by contacting the patients or their relatives by telephone or mail. Normalization was defined as a return of hormone levels to within the normal range without the requirement of any further treatment. Recurrence was diagnosed from the clinical features, hormonal function, or identification of residual tumor, based on the results of hormone and MRI examinations performed two years after surgery Statistical Analysis. Quantitative data are reported as the mean ± standard deviation (SD), and qualitative data are expressed as percentages. Quantitative and nonparametric data, such as mean age, time to diagnosis, and tumor size, were compared by Student s t-tests or Mann-Whitney U tests. Chi-square tests were used to compare qualitative data, including gender, invasiveness, the presence of pituitary apoplexy, tumor classification, remission rate, and recurrence rate. Statistical comparisons of endocrine outcomes at different follow-up times were adjusted for multiple testing using a Bonferroni correction. Differences between groups in endocrine outcome at the same follow-up time were assessed by Student s t-test. Correlationsbetween variables were evaluated using Pearson or Spearman correlation coefficients. Analyses were performed using Statistical Package for Social Sciences Version 16.0 (Chicago, IL, USA). All statistical tests were two-sided, and P < 0.05 was considered statistically significant. 3. Results 3.1. Baseline Characteristics. A total of 84 patients were enrolledinthestudy,withameanageof33.60± years (range: years); more than half the patients were female (n =59; 70.2%). The demographics and tumor characteristics of the two groups of patients are summarized in Tables 1 and 2. Of the 84 patients enrolled, 48 (15 males and 33 females) werecategorizedintothecdgroupand36(10malesand26 females) into the CD + PRL group. At the time of diagnosis, the patients in the CD + PRL group (mean age: ± years; range: years) were significantly younger than those in the CD group (mean age: ± years; range: years) (P = 0.037). Furthermore, maximal adenoma size was larger for patients in the CD + PRL group (mean diameter: 2.44 ± 1.32 cm; range: cm) than for those in the CD group (mean diameter: 1.44 ± 1.05;range: cm) (P < 0.001). The mean time to diagnosis did not differ Table 1: Preoperative demographic characteristics and tumor sizes of the patients in the two groups. Variable CD (n =48) PRL+CD(n =36) P Age (years) ± ± Time to diagnosis (months) 25.32± ± Tumor size (cm) 1.44 ± ± 1.32 <0.001 Data are expressed as the mean ± SD. P values were determined using a Student s t-test or a Mann-Whitney U test, as appropriate. P < 0.05 was considered statistically significant. Table 2: Gender, tumor invasiveness, and the presence of pituitary apoplexy in the two groups of patients. Variable CD (n =48) PRL+CD(n =36) P Gender Male 15 (31.3%) 10 (27.8%) Female 33 (68.8%) 26 (72.2%) Invasion + 11 (22.9%) 12 (33.3%) 37 (77.1%) 24 (66.7%) Apoplexy + 9 (18.8%) 6 (16.7%) 39 (81.3%) 30 (83.3%) Classification Knosp 0 25 (52.1) 7 (19.4) 1 7 (14.6) 9 (25.0) 2 6 (12.5) 7 (19.4) (16.7) 8 (22.2) 4 2 (4.2) 5 (13.9) Data are expressed as n (%). + and indicate the presence and absence, respectively, of the characteristic in the group. P values were determined using a chi-square test or a Mann-Whitney U tests. P < 0.05 was considered statistically significant. significantly between the CD group (25.32 ± months; range: months) and the CD + PRL group (33.68 ± months; range: months), and there were also no significant differences in the incidences of invasiveness or pituitary apoplexy between the two groups. The patients were classified according to the degree of invasion of the cavernous sinus according to Knosp classification, and the two groups showed significant differences with the CD + PRL group showing a tendency for higher grades reflecting higher rates of invasion (P = 0.005) Tumor Classification. IntheCDgroup,47.9%ofthe patients had microadenomas, and 52.1% had macroadenomas. The corresponding values for patients in the CD + PRL group were 5.6% and 94.4%, indicating that macroadenomas were more prevalent in the CD + PRL group than in the CD group (P < 0.001) Preoperative Clinical Manifestations. The most commonly presenting clinical manifestations in the two groups were menstrual disorders, headaches, and dizziness (Table 3).
5 International Endocrinology 5 Table 3: Preoperative clinical manifestations in the two groups of patients. Symptom CD (n =48) PRL+CD(n =36) P Headache/dizziness 27 (56.3%) 24 (66.7%) Progressive obesity 21 (43.8%) 6 (16.7%) Vomiting 4 (8.3%) 4 (11.1%) Visual impairment 19 (39.6%) 18 (50.0%) Visual field defects 6 (12.5%) 12 (33.3%) Menstrual disorders 16/28 (57.1%) 22/26 (84.6%) Galactorrhea 10/28 (35.7%) 14/26 (53.8%) Sexual dysfunction 4/10 (40.0%) 2/20 (10.0%) Polyuria/polydipsia 12 (25.0%) 8 (22.2%) Hypertension 40 (83.3%) 10 (27.8%) <0.001 Diabetes mellitus 5 (10.4%) 6 (16.7%) Data are expressed as n (%). P values were determined using a chi-square test. P < 0.05 was considered statistically significant. Menstrual disorders and visual field defects were more common in patients in the CD + PRL group than in patients in the CD group (P = and 0.021, resp.), whereas the incidences of progressive obesity and hypertension were muchlowerinpatientsinthecd+prlgroupthanin patients in the CD group (P = and P < 0.001,resp.) Endocrine Function before and after Surgery. Preoperative and postoperative serum cortisol and PRL levels were available for all patients (Table 4). Elevated preoperative levels of serum cortisol and PRL were detected in patients in the CD + PRL group, and these patients had lower cortisol levels and higher PRL levels than those in the CD group (P < 0.05 for both comparisons). The cortisol level of patients in the CD group decreased from ± nmol/l before surgery to ± nmol/l at 3days,320.64± nmol/l at 3 months, and ± nmol/l at 12 months after surgery. The preoperative andpostoperativeprllevelsinthecdgroupwereallwithin the normal range. In the CD + PRL group, the cortisol level decreased from ± nmol/l before surgery to ± nmol/l at 3 days, ± nmol/l at 3 months, and ± nmol/l at 12 months after surgery. Furthermore, the PRL levels of this group decreased from ± ng/ml before surgery to ± ng/ml at 3 days, ± ng/ml at 3 months, and ± ng/ml at 12 months after surgery. There were no significant differences in the postoperative cortisol levels betweenthecdandcd+prlgroups,butthepostoperative PRL levels in the CD + PRL group remained markedly higher than those in the CD group. Among the patients with microadenomas, the normalization rates (based on the postoperative hormone levels at three months) in the CD and CD + PRL groups were 95.7% and 100%, respectively (Figure 3(a)). For patients with macroadenomas, the corresponding normalization rates were 88.0% and 38.2%, respectively. Overall, normalization of hormonal levels was achieved in 44 patients (91.7%) in the CD group, but only 15 patients (41.7%) in the CD + PRL group (P < 0.001). In the CD + PRL group, normalization of both cortisol and PRL levels occurred in 41.7% of the patients (Figure 3(b)) Postoperative Complications. No deaths or major complications were observed, although some minor complications did occur, including transient DI and hyponatremia. Transient DI was observed in 26 of 48 patients (54.2%) in thecdgroupandin18of36patients(50.0%)inthecd+ PRL group. Hyponatremia occurred in 50% of the patients in both groups, with nadir serum sodium levels in the CD group ( mmol/l) similar to those in the CD + PRL group ( mmol/l). There were no significant differences in the incidences of transient DI and hyponatremia between the two groups Follow-Up. The median postoperative duration of hospitalization was 5 days (range: 3 15 days). Overall, 90% of the patients were discharged by postoperative day 5. The median duration of follow-up for the entire group was 45 months (range: months). Tumor recurrence was significantly less frequent in the CD group (4 patients, 8.3%) than in the CD + PRL group (13 patients; 36.1%) (P < 0.001). All recurrences arose within the first two years after surgery. 4. Discussion Cushing s disease, caused by excessive ACTH secretion from tumorous pituitary corticotrophs, is a potentially lifethreatening endocrine condition [9]. The first-line treatment for Cushing s disease is pituitary surgery to control excessive hormoneproductionandimprovepituitaryfunction[10]. Cases of pituitary adenoma associated with increased production of both ACTH and PRL, causing apparent Cushing s disease and hyperprolactinemia, are extremely rare [5, 11]. The present study has evaluated the clinical features and endocrine and surgical outcomes, over a relatively long follow-up period, of a large series of patients who underwent transsphenoidal surgery for Cushing s disease with or without hyperprolactinemia. The majority of our patients were diagnosed in their thirties and forties, with those in the CD + PRL group significantly younger at diagnosis than those in the CD group. In addition, our results revealed that the mean maximal diameter of the adenoma varied between the two groups, consistent with a previous report that patients with Cushing s disease alone usually present with small tumors [12]. The CD + PRL group also had a tendency for higher Knosp grades so the adenoma was more likely to have invaded the cavernous sinus space. Approximately half of the patients in the CD group were found to have microadenomas, and the other half were found to have macroadenomas, a finding similartothatofothers[13]. Although recent advances in imaging technologies, including MRI, can detect relatively small lesions within the pituitary gland, these methods can localize microadenomas in only 60 80% of patients with Cushing s disease, since most of the lesions are very small [8, 14]. In our study, the average diameter of the adenoma was
6 6 International Endocrinology Table 4: The levels of cortisol (nmol/l) and PRL (ng/ml) measured during follow-up of the patients in the two groups. Group Hormone Before surgery CD (n =48) PRL + CD (n =36) 3daysafter surgery 3monthsafter surgery 12 months after surgery Cortisol ± ± ± ± <0.001 PRL ± ± ± ± Cortisol ± ± ± ± <0.001 PRL ± ± ± ± <0.001 Data are expressed as the mean ± SD. indicates a significant difference in the cortisol level between the two groups at the same time point (P < 0.05). indicates a significant difference in the PRL level between the two groups at the same time point (P < 0.05). Each P value shown in the Table is for comparative analysis, within the CD or PRL + CD group, between values before surgery and those 3 days after surgery. F P P = P < % (%) % % 0 Microadenoma CD PRL + CD Macroadenoma PRL(N) and COR(N) PRLL(H) and COR(N) PRL(H) and COR(H) (a) (b) Figure 3: The rate of hormonal normalization in patients with Cushing s disease. (a) Comparisons of the normalization rates (%) after transsphenoidal surgery between microadenomas and macroadenomas, for patients in the CD and CD + PRL groups. (b) Distribution of the hormonal normalization rate in the CD + PRL group. H indicates hormone levels above normal after surgery; N indicates hormone levels in the normal range after surgery. less than 5 to 6 mm, in agreement with previous investigations [8, 15]. We also found that nearly 95% of patients in the CD + PRL group had macroadenomas; this higher incidence may be related to the higher levels of PRL. Menstrual disorders and visual field defects were more common in patients in the CD + PRL group (compared with the CD group), whereas the incidences of progressive obesity and hypertension were much lower. Hypersecretion of PRL has a variety of manifestations, including menstrual disorders in women [16], and our findings concurred with those of previous investigations [17]. Pituitary compression by a tumor may present with visual field defects; furthermore, patients in the CD + PRL group were much more likely to have macroadenomas, which are more commonly associated with the development of neurological deficits and visual disturbances. ACTH has antagonistic effects on protein and lipid metabolism that can lead to uncontrolled hypertension and other serious complications [18]. Overall, the clinical symptoms observed in our study agreed with those of previous reports in the literature [19 21]. Of the patients in the CD + PRL group who had hormonal symptoms, most were related to plurihormone production. Elevated preoperative cortisol and PRL levels were detected in patients in the CD + PRL group, with PRL levels improving after surgery; this is consistent with the findings of Ratliff and Oldfield [22]andWynneetal.[23]. We also found that patients in the CD + PRL group with high PRL levels often had a relatively low serum cortisol level. Yamaji and colleagues reported PRL elevation in 23% of patients with Cushing s disease [24], while Caufriez and coworkers found that 91% of patients with Cushing s disease had preoperative elevation of PRL levels that normalized after transsphenoidal surgery [25]. AlthoughWynneetal. reportedthatthepredictive value of preoperative PRL levels in Cushing s disease was limited [23], we found that patients in the CD group were more likely to achieve normalization of endocrine function. It was notable that, in the CD + PRL group, the normalization rate for patients with macroprolactinomas was significantly lower than that for patients with microprolactinomas. Since complete resection of microadenomas was possible, it is
7 International Endocrinology 7 perhaps not surprising that the normalization rates for patients with microadenomas exceeded 95% for both groups. Our results, together with those of previous investigations, indicate that surgery is a highly effective treatment for Cushing s disease, and transsphenoidal surgery is considered the definitive treatment method [26]. Thus, the discovery of patients with a plurihormonal tumor depends on the hormonal levels as well as pathological identification [27, 28]. Plurihormonal adenomas are defined as those that secrete two or more hormones that differ in chemical composition, immunoreactivity, and biologic effects [29, 30]. In every patient in the CD + PRL group, a mixed tumor with ACTHand PRL-positive cells was discovered by pathological investigations following surgery. Transsphenoidal surgery represents a relatively safe procedure for resecting tumors underlying Cushing s disease. However, even in the most experienced hands, postoperative complications are unavoidable. The occurrences of postoperative transient DI and hyponatremia correlate with intraoperative manipulation of the pituitary stalk and posterior lobe, multiple incisions in the gland, and partial hypophysectomy [31]. Since pituitary exploration may damage the normal gland, gland manipulation is always kept to the minimum necessary to identify and remove the adenoma. The rate of postoperative transient DI reported in the literature varies widely [32, 33]. Although there was no significant difference in the incidence of DI between the two groups in our study, relatively higher rates of DI were observed in our patients overall, likely due to an increased awareness regarding this potential complication. There was also no significant difference in the incidence of hyponatremia between the two groups. Future prospective studies of the impact of transsphenoidal surgery on transient DI and electrolyte abnormalities are merited. Wide variations in surgical outcomes and recurrence rates have been reported, depending on the tumor characteristics, the surgeon s experience, and the duration of the follow-up. The recurrence rate in the CD group was 8.3%, lower than that reported by others [34, 35], whereas it was 36.1% in the CD + PRL group. The lower recurrence rate in thecdgroupmayreflectlong-termremission.theelevated rate of recurrence in the CD + PRL group is an important finding, which suggests that careful long-term follow-up is needed in this subset of patients, even if surgery is considered successful. Mixed ACTH and PRL adenomas often manifest themselves as coexisting Cushing s disease and prolactinoma [5]. Several hypotheses have been proposed to explain the coexistence of two or more hormones within an adenoma. First, neoplastic transformation caused by stimulation could result in different cell types [36]. Second, different hormones could be derived from distinct cell types within the borders of a single adenoma [4, 37]; for example, two separate tumors growing in a small space could become conjoined as a single mass. Our study is not without its limitations. First, this was a retrospective cohort study in a single institution; prospective, multicenter studies are merited to extend our observations. Second, the follow-up period was relatively short for some patients, limiting the evaluation of the real recurrence rates. Hence, long-term postoperative follow-up of a similar cohort of patients is needed to better assess the effects of surgery and treatment outcomes. 5. Conclusion In summary, the current study has compared characteristics between patients with both Cushing s disease and hyperprolactinemia and those with Cushing s disease alone. We found that patients in the CD + PRL group were characterized by younger age, larger tumor size, more clinical manifestations (including a higher incidence of menstrual disorders caused by PRL secretion), lower endocrine normalization rate, and more frequent recurrence rate, compared with patients with Cushing s disease alone. Our observations extend our knowledge of the characteristics of patients with Cushing s disease and hyperprolactinemia and may provide insights that will help to improve the diagnosis and treatment of the disease. Conflict of Interests The authors declare no conflict of interests regarding the publication of this paper. Authors Contribution Cheng Huan and Chao Lu contributed equally to this work. Funding This work was supported by the Chinese National Natural Science Foundation ( ) and Shandong Provincial Scientific and Technological Development Projects Foundation (2010GSF10225). Acknowledgment theauthorswouldliketothanktheentirestaffofthedepartment of Neurosurgery of the Provincial Hospital Affiliated to Shandong University for their help. References [1] J. Egger, T. Kapur, C. Nimsky, and R. Kikinis, Pituitary adenoma volumetry with 3D Slicer, PLoS ONE, vol. 7, no. 12, Article ID e51788, [2]C.Steffensen,A.M.Bak,K.ZøylnerRubeck,andJ.O.L. Jørgensen, Epidemiology of Cushing s syndrome, Neuroendocrinology,vol.92,no.1,pp.1 5,2010. [3] J. Lado-Abeal, J. Rodriguez-Arnao, J. D. C. Newell-Price et al., Menstrual abnormalities in women with cushing s disease are correlated with hypercortisolemia rather than raised circulating androgen levels, Clinical Endocrinology and Metabolism, vol. 83, no. 9, pp , [4] C. Mahler, J. Verhelst, R. Klaes, and J. Trouillas, Cushing s disease and hyperprolactinemia due to a mixed ACTHand prolactin-secreting pituitary macroadenoma, Pathology: Research and Practice,vol.187,no.5,pp ,1991.
8 8 International Endocrinology [5] S.H.Sherry,A.T.Guay,A.K.Leeetal., Concurrentproduction of adrenocorticotropin and prolactin from two distinct cell lines in a single pituitary adenoma: a detailed immunohistochemical analysis, Clinical Endocrinology and Metabolism,vol. 55,no.5,pp ,1982. [6] A. Lania and P. Beck-Peccoz, Pituitary incidentalomas, Best Practice and Research: Clinical Endocrinology and Metabolism, vol. 26, no. 4, pp , [7] E. Knosp, K. Kitz, E. Steiner, and C. Matula, Pituitary adenomaswithparasellarinvasion., Acta Neurochirurgica, Supplement,vol.53,pp.65 71,1991. [8] T. J. Mampalam, J. B. Tyrrell, and C. B. Wilson, Transsphenoidal microsurgery for Cushing disease. A report of 216 cases, Annals of Internal Medicine, vol. 109, no. 6, pp , [9] M. Barbot, N. Albiger, S. Koutroumpi et al., Predicting late recurrence in surgically treated patients with Cushing s disease, Clinical Endocrinology,vol.79,no.3,pp ,2013. [10] V. Esposito, A. Santoro, G. Minniti et al., Transsphenoidal adenomectomy for GH-, PRL- and ACTH-secreting pituitary tumours: outcome analysis in a series of 125 patients, Neurological Sciences,vol.25,no.5,pp ,2004. [11] A. M. McNicol, Current topics in neuropathology. Cushing s disease, Neuropathology and Applied Neurobiology, vol. 11, no. 6, pp , [12] J. B. Tyrrell and C. B. Wilson, Cushing s disease. Therapy of pituitary adenomas, Endocrinology and Metabolism Cinics of North America,vol.23,pp ,1994. [13] R.A.Kristof,J.Schramm,L.Redel,G.Neuloh,M.Wichers,and D. Klingmüller, Endocrinological outcome following first time transsphenoidal surgery for GH-, ACTH-, and PRL-secreting pituitary adenomas, Acta Neurochirurgica, vol. 144, no. 6, pp , [14] J. L. Doppman, J. A. Frank, A. J. Dwyer et al., Gadolinium DTPA enhanced MR imaging of ACTH-secreting microadenomas of the pituitary gland, Computer Assisted Tomography, vol. 12, no. 5, pp , [15] A. B. Atkinson, The treatment of Cushing s syndrome, Clinical Endocrinology,vol.34,no.6,pp ,1991. [16] S. Isik, D. Berker, Y. A. Tutuncu et al., Clinical and radiological findings in macroprolactinemia, Endocrine, vol. 41, no. 2, pp , [17] S. Furuhata, T. Kameya, M. Otani, and S. Toya, Prolactin presents in all pituitary tumors of acromegalic patients, Human Pathology,vol.24,no.1,pp.10 15,1993. [18]D.K.Hamilton,M.L.Vance,P.T.Boulos,andE.R.Laws, Surgical outcomes in hyporesponsive prolactinomas: analysis of patients with resistance or intolerance to dopamine agonists, Pituitary,vol.8,no.1,pp.53 60,2005. [19] H. L. Fideleff, H. R. Boquete, M. G. Suárez, and M. Azaretzky, Prolactinoma in children and adolescents, Hormone Research, vol. 72, no. 4, pp , [20] A. G. Lania, S. Ferrero, R. Pivonello et al., Evolution of an aggressive prolactinoma into a growth hormone secreting pituitary tumor coincident with GNAS gene mutation, Journal of Clinical Endocrinology and Metabolism,vol.95,no.1,pp.13 17, [21] S. Melmed, Update in pituitary disease, The Clinical Endocrinology & Metabolism,vol.93,no.2,pp ,2008. [22] J. K. Ratliff and E. H. Oldfield, Multiple pituitary adenomas in Cushing s disease, Neurosurgery, vol. 93, no. 5, pp , [23] A. G. Wynne, B. W. Scheithauer, W. F. Young Jr. et al., Coexisting corticotroph and lactotroph adenomas: case report with reference to the relationship of corticotropin and prolactin excess, Neurosurgery, vol. 30, no. 6, pp , [24] T. Yamaji, M. Ishibashi, A. Teramoto, and T. Fukushima, Hyperprolactinemia in Cushing s disease and Nelson s syndrome, Clinical Endocrinology and Metabolism, vol. 58,no.5,pp ,1984. [25] A. Caufriez, D. Desir, M. Szyper, C. Robyn, and G. Copinschi, Prolactin secretion in Cushing s disease, The Clinical Endocrinology and Metabolism,vol.53,no.4,pp ,1981. [26]B.M.K.Biller,A.B.Grossman,P.M.Stewartetal., Treatment of adrenocorticotropin-dependent cushing s syndrome: a consensus statement, The Clinical Endocrinology and Metabolism,vol.93,no.7,pp ,2008. [27] G. Kontogeorgos, K. Kovacs, E. Horvath, and B. W. Scheithauer, Multiple adenomas of the human pituitary. A retrospective autopsy study with clinical implications, Neurosurgery,vol.74,no.2,pp ,1991. [28] A. D. Parent, J. Bebin, and R. R. Smith, Incidental pituitary adenomas, Neurosurgery,vol.54,no.2,pp , [29]K.Kovacs,E.Horvath,S.L.Asa,L.Stefaneanu,andT.Sano, Pituitary cells producing more than one hormone: human pituitary adenomas, Trends in Endocrinology and Metabolism, vol. 1, no. 2, pp , [30] D.M.Ho,C.Y.Hsu,L.T.Ting,andH.Chiang, Plurihormonal pituitary adenomas: immunostaining of all pituitary hormones is mandatory for correct classification, Histopathology,vol.39, no.3,pp ,2001. [31] B. R. Olson, J. Gumowski, D. Rubino, and E. H. Oldfield, Pathophysiology of hyponatremia after transsphenoidal pituitary surgery, Neurosurgery, vol. 87, no. 4, pp , [32] H.-D. Jho, Endoscopic transsphenoidal surgery, Neuro-Oncology,vol.54,no.2,pp ,2001. [33] P. Cappabianca, L. M. Cavallo, A. Colao, and E. de Divitiis, Surgical complications associated with the endoscopic endonasal transsphenoidal approach for pituitary adenomas, Neurosurgery, vol. 97, no. 2, pp , [34] J. H. Kim, C. S. Shin, S. H. Paek, H. W. Jung, S. W. Kim, and S. Y. Kim, Recurrence of Cushing s disease after primary transsphenoidal surgery in a university hospital in Korea, Endocrine Journal, vol. 59, no. 10, pp , [35] K. I. Alexandraki, G. A. Kaltsas, A. M. Isidori et al., Longterm remission and recurrence rates in Cushing s disease: predictive factors in a single-centre study, European Endocrinology / European Federation of Endocrine Societies,vol. 168, no. 4, pp , [36] K.Kovacs,E.Horvath,L.Stefaneanuetal., Pituitaryadenoma producing growth hormone and adrenocorticotropin: a histological, immunocytochemical, electron microscopic, and in situ hybridization study, Neurosurgery,vol.88, no.6,pp , [37] B. W. Scheithauer, E. Horvath, K. Kovacs, E. R. Laws Jr., R. V. Randall, and N. Ryan, Plurihormonal pituitary adenomas, Seminars in Diagnostic Pathology, vol. 3, no. 1, pp , 1986.












9 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Process / Evidence Class. Clinical Assessment / III
 Table 2: Endocrine Author Cozzi et al (2009) 1 Study Design: Prospectively followed case series. Fourteen patients had pre-op hypocortisolism. Patient Population: Seventy-two adult patients who underwent
Table 2: Endocrine Author Cozzi et al (2009) 1 Study Design: Prospectively followed case series. Fourteen patients had pre-op hypocortisolism. Patient Population: Seventy-two adult patients who underwent
Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution?
 Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
The characteristics of acromegalic patients with hyperprolactinemia and the differences with hyperprolactinemia patients
 The characteristics of acromegalic patients with hyperprolactinemia and the differences with hyperprolactinemia patients Cheng Huan 1, Guihua Cui 2 and Zongming Ren 3 * 1 Department of Neurosurgery, Shandong
The characteristics of acromegalic patients with hyperprolactinemia and the differences with hyperprolactinemia patients Cheng Huan 1, Guihua Cui 2 and Zongming Ren 3 * 1 Department of Neurosurgery, Shandong
Gender differences in presentation and outcome of patients with Cushing's disease in Han Chinese
 Bio-Medical Materials and Engineering 24 (2014) 3439 3446 DOI 10.3233/BME-141168 IOS Press 3439 Gender differences in presentation and outcome of patients with Cushing's disease in Han Chinese Cheng Huan
Bio-Medical Materials and Engineering 24 (2014) 3439 3446 DOI 10.3233/BME-141168 IOS Press 3439 Gender differences in presentation and outcome of patients with Cushing's disease in Han Chinese Cheng Huan
Pituitary Tumors and Incidentalomas. Bijan Ahrari, MD, FACE, ECNU Palm Medical Group
 Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Metoclopramide Domperidone. HYPER- PROLACTINAEMIA: the true and the false problems
 Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary Tumor Apoplexy
 Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Diseases of pituitary gland
 Diseases of pituitary gland A brief introduction Anterior lobe = adenohypophysis Posterior lobe = neurohypophysis The production of most pituitary hormones is controlled in large part by positively and
Diseases of pituitary gland A brief introduction Anterior lobe = adenohypophysis Posterior lobe = neurohypophysis The production of most pituitary hormones is controlled in large part by positively and
Sharon maslovitz Lis Maternity Hospital
 Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Medical background Healthy until 24yo
Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Medical background Healthy until 24yo
Imaging pituitary gland tumors
 November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
Case Report A Rare Corticotroph-Secreting Tumor with Coexisting Prolactin and Growth Hormone Staining Cells
 Case Reports in Endocrinology Volume 2012, Article ID 529730, 5 pages doi:10.1155/2012/529730 Case Report A Rare Corticotroph-Secreting Tumor with Coexisting Prolactin and Growth Hormone Staining Cells
Case Reports in Endocrinology Volume 2012, Article ID 529730, 5 pages doi:10.1155/2012/529730 Case Report A Rare Corticotroph-Secreting Tumor with Coexisting Prolactin and Growth Hormone Staining Cells
A survey of pituitary incidentaloma in Japan
 European Journal of Endocrinology (2003) 149 123 127 ISSN 0804-4643 CLINICAL STUDY A survey of pituitary incidentaloma in Japan Naoko Sanno, Ken ichi Oyama, Shigeyuki Tahara, Akira Teramoto and Yuzuru
European Journal of Endocrinology (2003) 149 123 127 ISSN 0804-4643 CLINICAL STUDY A survey of pituitary incidentaloma in Japan Naoko Sanno, Ken ichi Oyama, Shigeyuki Tahara, Akira Teramoto and Yuzuru
Endocrinological Outcome Among Treated Craniopharyngioma Patients
 Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas
Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
TABLES. Table 1: Imaging. Congress of Neurological Surgeons Author (Year) Description of Study Classification Process / Evidence Class
 Description of Study Classification Process / Evidence Class") TABLES Table 1: Imaging Kremer et al (2002) 2 Study Design: Prospective followed case series. Patient Population: Fifty adult patients with NFPA Study Description: Patients underwent MRI before surgery,
TABLES Table 1: Imaging Kremer et al (2002) 2 Study Design: Prospective followed case series. Patient Population: Fifty adult patients with NFPA Study Description: Patients underwent MRI before surgery,
Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report of Neoadjuvant Use Enabling Complete Surgical Resection
 Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Hypothalamus & Pituitary Gland
 Hypothalamus & Pituitary Gland Hypothalamus and Pituitary Gland The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and
Hypothalamus & Pituitary Gland Hypothalamus and Pituitary Gland The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and
CLINICALLY SILENT ACTH CROOKE S CELL ADENOMA PRESENTING AS UNILATERAL EAR PAIN
 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
Case Report Tortuous Common Carotid Artery: A Report of Four Cases Observed in Cadaveric Dissections
 Case Reports in Otolaryngology Volume 2016, Article ID 2028402, 4 pages http://dx.doi.org/10.1155/2016/2028402 Case Report Tortuous Common Carotid Artery: A Report of Four Cases Observed in Cadaveric Dissections
Case Reports in Otolaryngology Volume 2016, Article ID 2028402, 4 pages http://dx.doi.org/10.1155/2016/2028402 Case Report Tortuous Common Carotid Artery: A Report of Four Cases Observed in Cadaveric Dissections
Case Report Multiple Intracranial Meningiomas: A Review of the Literature and a Case Report
 Case Reports in Surgery Volume 2013, Article ID 131962, 4 pages http://dx.doi.org/10.1155/2013/131962 Case Report Multiple Intracranial Meningiomas: A Review of the Literature and a Case Report F. Koech,
Case Reports in Surgery Volume 2013, Article ID 131962, 4 pages http://dx.doi.org/10.1155/2013/131962 Case Report Multiple Intracranial Meningiomas: A Review of the Literature and a Case Report F. Koech,
Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male
 Case Reports in Radiology Volume 2016, Article ID 6434623, 4 pages http://dx.doi.org/10.1155/2016/6434623 Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male Jordan Nepute,
Case Reports in Radiology Volume 2016, Article ID 6434623, 4 pages http://dx.doi.org/10.1155/2016/6434623 Case Report Intracranial Capillary Hemangioma in the Posterior Fossa of an Adult Male Jordan Nepute,
Long-term results of treatment in patients with ACTH-secreting pituitary macroadenomas
 European Journal of Endocrinology (2003) 149 195 200 ISSN 0804-4643 CLINICAL STUDY Long-term results of treatment in patients with ACTH-secreting pituitary macroadenomas S Cannavò, B Almoto, C Dall Asta
European Journal of Endocrinology (2003) 149 195 200 ISSN 0804-4643 CLINICAL STUDY Long-term results of treatment in patients with ACTH-secreting pituitary macroadenomas S Cannavò, B Almoto, C Dall Asta
Enterprise Interest None
 Enterprise Interest None Plurihormonal cells of normal anterior pituitary Lubov Mitrofanova¹, Petr Konovalov¹, Julia Krylova², Igor Kvetnoy² ¹Federal Almazov North-West Medical Research Centre, St. Petersburg,
Enterprise Interest None Plurihormonal cells of normal anterior pituitary Lubov Mitrofanova¹, Petr Konovalov¹, Julia Krylova², Igor Kvetnoy² ¹Federal Almazov North-West Medical Research Centre, St. Petersburg,
Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC
 10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
Pathology of pituitary gland. By: Shifaa Qa qa
 Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary Disorders. Eiman Ali Basheir Mob: /1/2019
 Pituitary Disorders Eiman Ali Basheir Mob: 0915020385 31/1/2019 Objectives By the end of this lecture the students will be able to: Understand basic Pituitary axis physiology State the common causes of
Pituitary Disorders Eiman Ali Basheir Mob: 0915020385 31/1/2019 Objectives By the end of this lecture the students will be able to: Understand basic Pituitary axis physiology State the common causes of
Research Article Abdominal Aortic Aneurysms and Coronary Artery Disease in a Small Country with High Cardiovascular Burden
 ISRN Cardiology, Article ID 825461, 4 pages http://dx.doi.org/10.1155/2014/825461 Research Article Abdominal Aortic Aneurysms and Coronary Artery Disease in a Small Country with High Cardiovascular Burden
ISRN Cardiology, Article ID 825461, 4 pages http://dx.doi.org/10.1155/2014/825461 Research Article Abdominal Aortic Aneurysms and Coronary Artery Disease in a Small Country with High Cardiovascular Burden
Subject Index. hypothalamic-pituitary-adrenal axis 158. Atherosclerosis, ghrelin role AVP, see Arginine vasopressin.
 Subject Index Acromegaly, somatostatin analog therapy dopamine agonist combination therapy 132 efficacy 132, 133 overview 130, 131 receptor subtype response 131, 132 SOM30 studies 131, 132 ACTH, see Adrenocorticotropic
Subject Index Acromegaly, somatostatin analog therapy dopamine agonist combination therapy 132 efficacy 132, 133 overview 130, 131 receptor subtype response 131, 132 SOM30 studies 131, 132 ACTH, see Adrenocorticotropic
Clinical presentations of endocrine diseases
 Section I Chapter 1 Clinical approaches Clinical presentations of endocrine diseases Karen Gomez-Hernandez and Shereen Ezzat Endocrinology is a fascinating field that covers a wide range of diseases with
Section I Chapter 1 Clinical approaches Clinical presentations of endocrine diseases Karen Gomez-Hernandez and Shereen Ezzat Endocrinology is a fascinating field that covers a wide range of diseases with
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Research Article Comparison of Colour Duplex Ultrasound with Computed Tomography to Measure the Maximum Abdominal Aortic Aneurysmal Diameter
 International Vascular Medicine, Article ID 574762, 4 pages http://dx.doi.org/10.1155/2014/574762 Research Article Comparison of Colour Duplex Ultrasound with Computed Tomography to Measure the Maximum
International Vascular Medicine, Article ID 574762, 4 pages http://dx.doi.org/10.1155/2014/574762 Research Article Comparison of Colour Duplex Ultrasound with Computed Tomography to Measure the Maximum
Abstract. Introduction
 Clinical Features and Outcome of Surgery in 30 Patients with Acromegaly A. Chandna, N. Islam, A. Jabbar, L. Zuberi, N. Haque Endocrinology Section, Department of Medicine, Aga Khan University Hospital,
Clinical Features and Outcome of Surgery in 30 Patients with Acromegaly A. Chandna, N. Islam, A. Jabbar, L. Zuberi, N. Haque Endocrinology Section, Department of Medicine, Aga Khan University Hospital,
HYPOTHALAMO PITUITARY GONADAL AXIS
 HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease
 A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease Z Hussein, MRCP*, B Tress**, P G Cohnan, FRACP***... 'Department of Medicine, Hospital Putrajaya, Putrajaya, Presint 7, 62250
A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease Z Hussein, MRCP*, B Tress**, P G Cohnan, FRACP***... 'Department of Medicine, Hospital Putrajaya, Putrajaya, Presint 7, 62250
Surgical therapeutic strategy for giant pituitary adenomas.
 Biomedical Research 2017; 28 (19): 8284-8288 ISSN 0970-938X www.biomedres.info Surgical therapeutic strategy for giant pituitary adenomas. Han-Shun Deng, Zhi-Quan Ding, Sheng-fan Zhang, Zhi-Qiang Fa, Qing-Hua
Biomedical Research 2017; 28 (19): 8284-8288 ISSN 0970-938X www.biomedres.info Surgical therapeutic strategy for giant pituitary adenomas. Han-Shun Deng, Zhi-Quan Ding, Sheng-fan Zhang, Zhi-Qiang Fa, Qing-Hua
Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule
 Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
Case Reports in Oncological Medicine Volume 2013, Article ID 865032, 4 pages http://dx.doi.org/10.1155/2013/865032 Case Report PET/CT Imaging in Oncology: Exceptions That Prove the Rule M. Casali, 1 A.
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Research Article The Cost of Prolonged Hospitalization due to Postthyroidectomy Hypocalcemia: A Case-Control Study
 Advances in Endocrinology, Article ID 954194, 4 pages http://dx.doi.org/10.1155/2014/954194 Research Article The Cost of Prolonged Hospitalization due to Postthyroidectomy Hypocalcemia: A Case-Control
Advances in Endocrinology, Article ID 954194, 4 pages http://dx.doi.org/10.1155/2014/954194 Research Article The Cost of Prolonged Hospitalization due to Postthyroidectomy Hypocalcemia: A Case-Control
Case Report Pediatric Cushing s Disease and Pituitary Incidentaloma: Is This a Real Challenge?
 Case Reports in Endocrinology, Article ID 851942, 5 pages http://dx.doi.org/10.1155/2014/851942 Case Report Pediatric Cushing s Disease and Pituitary Incidentaloma: Is This a Real Challenge? Rosa Maria
Case Reports in Endocrinology, Article ID 851942, 5 pages http://dx.doi.org/10.1155/2014/851942 Case Report Pediatric Cushing s Disease and Pituitary Incidentaloma: Is This a Real Challenge? Rosa Maria
Pituitary Stalk Interruption Syndrome. Leena Shahla, MD, PGY5 Endocrinology, Diabetes and Metabolism Fellowship University of Massachusetts
 Pituitary Stalk Interruption Syndrome Leena Shahla, MD, PGY5 Endocrinology, Diabetes and Metabolism Fellowship University of Massachusetts 11/12/2016 Case: NP, 42 year old female, from Dominican Republic.
Pituitary Stalk Interruption Syndrome Leena Shahla, MD, PGY5 Endocrinology, Diabetes and Metabolism Fellowship University of Massachusetts 11/12/2016 Case: NP, 42 year old female, from Dominican Republic.
Spontaneous remission of acromegaly and Cushing s disease following pituitary apoplexy: Two case reports
 CASE REPORT Spontaneous remission of acromegaly and Cushing s disease following pituitary apoplexy: Two case reports S.H.P.P. Roerink 1 *, E.J. van Lindert 2, A.C. van de Ven 1 Departments of 1 Internal
CASE REPORT Spontaneous remission of acromegaly and Cushing s disease following pituitary apoplexy: Two case reports S.H.P.P. Roerink 1 *, E.J. van Lindert 2, A.C. van de Ven 1 Departments of 1 Internal
See the latest estimates for new cases of pituitary tumors in the US and what research is currently being done.
 About Pituitary Tumors Overview and Types If you have been diagnosed with a pituitary tumor or worried about it, you likely have a lot of questions. Learning some basics is a good place to start. What
About Pituitary Tumors Overview and Types If you have been diagnosed with a pituitary tumor or worried about it, you likely have a lot of questions. Learning some basics is a good place to start. What
Research Article Predictions of the Length of Lumbar Puncture Needles
 Computational and Mathematical Methods in Medicine, Article ID 732694, 5 pages http://dx.doi.org/10.1155/2014/732694 Research Article Predictions of the Length of Lumbar Puncture Needles Hon-Ping Ma, 1,2
Computational and Mathematical Methods in Medicine, Article ID 732694, 5 pages http://dx.doi.org/10.1155/2014/732694 Research Article Predictions of the Length of Lumbar Puncture Needles Hon-Ping Ma, 1,2
Pituitary for the General Practitioner. Marilyn Lee Consultant physician and endocrinologist
 Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
 Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Imaging The Turkish Saddle. Russell Goodman, HMS III Dr. Gillian Lieberman
 Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
Original Article. Abstract. Introduction. Thinesh Kumran 1,2, Saffari Haspani 1,2, Jafri Malin Abdullah 1,4, Azmi Alias 1,2, Fan Rui Ven 3
 Original Article Factors Influencing Disconnection Hyperprolactinemia and Reversal of Serum Prolactin after Pituitary Surgery in a Non-Functioning Pituitary Macroadenoma Thinesh Kumran 1,2, Saffari Haspani
Original Article Factors Influencing Disconnection Hyperprolactinemia and Reversal of Serum Prolactin after Pituitary Surgery in a Non-Functioning Pituitary Macroadenoma Thinesh Kumran 1,2, Saffari Haspani
Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child
 Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction
 Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction Mohammad Talha Rauf, MD Internal Medicine Resident PGY3 Dania AbuShanab, MD Julie Samantray,
Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction Mohammad Talha Rauf, MD Internal Medicine Resident PGY3 Dania AbuShanab, MD Julie Samantray,
Case Report Metyrapone for Long-Term Medical Management of Cushing s Syndrome
 Case Reports in Endocrinology Volume 2013, Article ID 782068, 4 pages http://dx.doi.org/10.1155/2013/782068 Case Report Metyrapone for Long-Term Medical Management of Cushing s Syndrome Andrea N. Traina,
Case Reports in Endocrinology Volume 2013, Article ID 782068, 4 pages http://dx.doi.org/10.1155/2013/782068 Case Report Metyrapone for Long-Term Medical Management of Cushing s Syndrome Andrea N. Traina,
Delayed Hyponatremia Following Transsphenoidal Surgery for Pituitary Adenoma
 Neurol Med Chir (Tokyo) 48, 489 494, 2008 Delayed Hyponatremia Following Transsphenoidal Surgery for Pituitary Adenoma Jae Il LEE, WonHoCHO*, ByungKwanCHOI, Seung Heon CHA, Geun Sung SONG, and Chang Hwa
Neurol Med Chir (Tokyo) 48, 489 494, 2008 Delayed Hyponatremia Following Transsphenoidal Surgery for Pituitary Adenoma Jae Il LEE, WonHoCHO*, ByungKwanCHOI, Seung Heon CHA, Geun Sung SONG, and Chang Hwa
Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
 Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
Case Reports in Orthopedics Volume 2016, Article ID 1834740, 4 pages http://dx.doi.org/10.1155/2016/1834740 Case Report Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Report Osteolysis of the Greater Trochanter Caused by a Foreign Body Granuloma Associated with the Ethibond Suture after Total Hip Arthroplasty
 Hindawi Volume 2017, Article ID 6082302, 4 pages https://doi.org/10.1155/2017/6082302 Case Report Osteolysis of the Greater Trochanter Caused by a Foreign Body Granuloma Associated with the Ethibond Suture
Hindawi Volume 2017, Article ID 6082302, 4 pages https://doi.org/10.1155/2017/6082302 Case Report Osteolysis of the Greater Trochanter Caused by a Foreign Body Granuloma Associated with the Ethibond Suture
Management of incidental pituitary microadenomas: a cost-effectiveness analysis King J T, Justice A C, Aron D C
 Management of incidental pituitary microadenomas: a cost-effectiveness analysis King J T, Justice A C, Aron D C Record Status This is a critical abstract of an economic evaluation that meets the criteria
Management of incidental pituitary microadenomas: a cost-effectiveness analysis King J T, Justice A C, Aron D C Record Status This is a critical abstract of an economic evaluation that meets the criteria
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
GLMS CME- Cell Group 5 10 April Greenlane Medical Specialists Pui-Ling Chan Endocrinologist
 GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
Case Report Overlap of Acute Cholecystitis with Gallstones and Squamous Cell Carcinoma of the Gallbladder in an Elderly Patient
 Case Reports in Surgery Volume 2015, Article ID 767196, 4 pages http://dx.doi.org/10.1155/2015/767196 Case Report Overlap of Acute Cholecystitis with Gallstones and Squamous Cell Carcinoma of the Gallbladder
Case Reports in Surgery Volume 2015, Article ID 767196, 4 pages http://dx.doi.org/10.1155/2015/767196 Case Report Overlap of Acute Cholecystitis with Gallstones and Squamous Cell Carcinoma of the Gallbladder
THE ANTERIOR PITUITARY. Embryology cont. Embryology of the pituitary BY MISPA ZUH HS09A179. Embryology cont. THE PITUIYARY GLAND Anatomy:
 THE ANTERIOR PITUITARY BY MISPA ZUH HS09A179 Embryology of the pituitary The pituitary is formed early in embryonic life from the fusion of the Rathke s pouch (anterior) and the diencephalon ( posterior)
THE ANTERIOR PITUITARY BY MISPA ZUH HS09A179 Embryology of the pituitary The pituitary is formed early in embryonic life from the fusion of the Rathke s pouch (anterior) and the diencephalon ( posterior)
Pituitary adenomas and menopause
 Pituitary adenomas and menopause Iulia Potorac Service d Endocrinologie Université de Liège CHU Liège RESULTATS Clinical case 1-38-year-old patient referred for exploration of premature ovarian failure
Pituitary adenomas and menopause Iulia Potorac Service d Endocrinologie Université de Liège CHU Liège RESULTATS Clinical case 1-38-year-old patient referred for exploration of premature ovarian failure
October 13, Surgical Nuances to Managing Cushing s Disease. Cortisol Regulation. Cushing s Syndrome Excess Cortisol. Sandeep Kunwar, M.D.
 Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication for Repeat Metastasectomy
 Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
Research Article Hb A1c Separation by High Performance Liquid Chromatography in Hemoglobinopathies
 Scientifica Volume 2016, Article ID 2698362, 4 pages http://dx.doi.org/10.1155/2016/2698362 Research Article Hb A1c Separation by High Performance Liquid Chromatography in Hemoglobinopathies Vani Chandrashekar
Scientifica Volume 2016, Article ID 2698362, 4 pages http://dx.doi.org/10.1155/2016/2698362 Research Article Hb A1c Separation by High Performance Liquid Chromatography in Hemoglobinopathies Vani Chandrashekar
MANAGEMENT OF PATIENTS WITH PITUITARY DISORDERS ON THE NEUROSUGERY WARDS RESPONSIBILITIES OF THE METABOLIC REGISTRAR
 MANAGEMENT OF PATIENTS WITH PITUITARY DISORDERS ON THE NEUROSUGERY WARDS RESPONSIBILITIES OF THE METABOLIC REGISTRAR We have clear links with DCN and a responsibility for the management of patients with
MANAGEMENT OF PATIENTS WITH PITUITARY DISORDERS ON THE NEUROSUGERY WARDS RESPONSIBILITIES OF THE METABOLIC REGISTRAR We have clear links with DCN and a responsibility for the management of patients with
Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy
 Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Mechanism of hyperprolactinemia
 Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
In some patients with pituitary macroadenoma, visual acuity
 ORIGINAL RESEARCH A.M. Tokumaru I. Sakata H. Terada S. Kosuda H. Nawashiro M. Yoshii Optic Nerve Hyperintensity on T2-Weighted Images among Patients with Pituitary Macroadenoma: Correlation with Visual
ORIGINAL RESEARCH A.M. Tokumaru I. Sakata H. Terada S. Kosuda H. Nawashiro M. Yoshii Optic Nerve Hyperintensity on T2-Weighted Images among Patients with Pituitary Macroadenoma: Correlation with Visual
3/22/2017. Disclosure of Relevant Financial Relationships. Disclosure of Relevant Financial Relationships
 Ki67 in Pituitary Tumors: What Information Could We Obtain? Robert Y. Osamura, MD International University of Health and Welfare Ki67 in Pituitary Tumors: What Information Could We Obtain? Robert Y. Osamura,
Ki67 in Pituitary Tumors: What Information Could We Obtain? Robert Y. Osamura, MD International University of Health and Welfare Ki67 in Pituitary Tumors: What Information Could We Obtain? Robert Y. Osamura,
CYSTIC PROLACTINOMA: A SURGICAL DISEASE?
 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
VARIABLE THYROID-STIMULATING HORMONE DYNAMICS IN SILENT THYROTROPH ADENOMAS
 Case Report VRILE THYROID-STIMULTING HORMONE DYNMICS IN SILENT THYROTROPH DENOMS Nigel Glynn, M 1 ; nne Marie Hannon, M 1 ; Michael Farrell, MD 2 ; Francesca rett, MD 2 ; Mohsen Javadpour, MD 3 ; mar gha,
Case Report VRILE THYROID-STIMULTING HORMONE DYNMICS IN SILENT THYROTROPH DENOMS Nigel Glynn, M 1 ; nne Marie Hannon, M 1 ; Michael Farrell, MD 2 ; Francesca rett, MD 2 ; Mohsen Javadpour, MD 3 ; mar gha,
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Pituitary Disorders Suranut Charoensri, MD
 Pituitary Disorders Suranut Charoensri, MD Division of Endocrinology and Metabolism Department of Medicine Faculty of Medicine, Khon Kaen University Anatomical Landmarks Nat Rev Endocrinol 2014;10:423-435
Pituitary Disorders Suranut Charoensri, MD Division of Endocrinology and Metabolism Department of Medicine Faculty of Medicine, Khon Kaen University Anatomical Landmarks Nat Rev Endocrinol 2014;10:423-435
Case Report A Rare Case of Near Complete Regression of a Large Cervical Disc Herniation without Any Intervention Demonstrated on MRI
 Case Reports in Radiology, Article ID 832765, 4 pages http://dx.doi.org/10.1155/2014/832765 Case Report A Rare Case of Near Complete Regression of a Large Cervical Disc Herniation without Any Intervention
Case Reports in Radiology, Article ID 832765, 4 pages http://dx.doi.org/10.1155/2014/832765 Case Report A Rare Case of Near Complete Regression of a Large Cervical Disc Herniation without Any Intervention
Studies on the diagnosis and treatment of canine Cushing s disease
 Studies on the diagnosis and treatment of canine Cushing s disease Summary of the Doctoral Thesis Asaka Sato (Supervised by Professor Yasushi Hara) Graduate School of Veterinary Medicine and Life Science
Studies on the diagnosis and treatment of canine Cushing s disease Summary of the Doctoral Thesis Asaka Sato (Supervised by Professor Yasushi Hara) Graduate School of Veterinary Medicine and Life Science
Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma of Thyroid
 Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Long term outcome following repeat transsphenoidal surgery for recurrent endocrine-inactive pituitary adenomas
 Pituitary (2010) 13:223 229 DOI 10.1007/s11102-010-0221-z Long term outcome following repeat transsphenoidal surgery for recurrent endocrine-inactive pituitary adenomas Edward F. Chang Michael E. Sughrue
Pituitary (2010) 13:223 229 DOI 10.1007/s11102-010-0221-z Long term outcome following repeat transsphenoidal surgery for recurrent endocrine-inactive pituitary adenomas Edward F. Chang Michael E. Sughrue
Silent ACTHoma: A subclinical presentation of Cushing s disease in a 79 year old male
 575 Silent ACTHoma: A subclinical presentation of Cushing s disease in a 79 year old male Meenal Malviya 1, Navneet Kumar 1*, Naseer Ahmad 2 1 MD; Department of Internal Medicine, Providence Hospital &
575 Silent ACTHoma: A subclinical presentation of Cushing s disease in a 79 year old male Meenal Malviya 1, Navneet Kumar 1*, Naseer Ahmad 2 1 MD; Department of Internal Medicine, Providence Hospital &
Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
62-year-old woman with severe headache. Celeste Thomas November 1, 2012
 62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis
 Advances in Orthopedics Volume 2015, Article ID 210972, 4 pages http://dx.doi.org/10.1155/2015/210972 Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis Hiroaki
Advances in Orthopedics Volume 2015, Article ID 210972, 4 pages http://dx.doi.org/10.1155/2015/210972 Research Article Relationship between Pain and Medial Meniscal Extrusion in Knee Osteoarthritis Hiroaki
Case Report Crossed Renal Ectopia without Fusion An Unusual Cause of Acute Abdominal Pain: A Case Report
 Case Reports in Urology Volume 2012, Article ID 728531, 4 pages doi:10.1155/2012/728531 Case Report Crossed Renal Ectopia without Fusion An Unusual Cause of Acute Abdominal Pain: A Case Report D. P. Ramaema,
Case Reports in Urology Volume 2012, Article ID 728531, 4 pages doi:10.1155/2012/728531 Case Report Crossed Renal Ectopia without Fusion An Unusual Cause of Acute Abdominal Pain: A Case Report D. P. Ramaema,
Research Article The Impact of the Menstrual Cycle on Perioperative Bleeding in Vitreoretinal Surgery
 Hindawi Ophthalmology Volume 2017, Article ID 9549284, 4 pages https://doi.org/10.1155/2017/9549284 Research Article The Impact of the Menstrual Cycle on Perioperative Bleeding in Vitreoretinal Surgery
Hindawi Ophthalmology Volume 2017, Article ID 9549284, 4 pages https://doi.org/10.1155/2017/9549284 Research Article The Impact of the Menstrual Cycle on Perioperative Bleeding in Vitreoretinal Surgery
Therapeutic Objectives. Cushing s Disease Surgical Results. Cushing s Disease Surgical Results: Macroadenomas 10/24/2015
 Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君
 Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君 Williams text book of endocrinology 11 th e Anterior pituitary hormone 10-20% of pituitary cells, increase to 40% during AP PRL releasing factors: TRH, oxytocin,
Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君 Williams text book of endocrinology 11 th e Anterior pituitary hormone 10-20% of pituitary cells, increase to 40% during AP PRL releasing factors: TRH, oxytocin,
Undetectable postoperative cortisol does not always. predict long-term remission in Cushing s disease: a single centre audit*
 Clinical Endocrinology (2002) 56, 25 31 Undetectable postoperative cortisol does not always Blackwell Science Ltd predict long-term remission in Cushing s disease: a single centre audit* L. B. Yap*, H.
Clinical Endocrinology (2002) 56, 25 31 Undetectable postoperative cortisol does not always Blackwell Science Ltd predict long-term remission in Cushing s disease: a single centre audit* L. B. Yap*, H.
Pituitary Macroadenoma with Superior Orbital Fissure Syndrome
 1 CASE REPORT OPEN ACCESS Pituitary Macroadenoma with Superior Orbital Fissure Syndrome Tapan Nagpal, Ankit Singhania ABSTRACT Introduction: Pituitary adenomas are benign tumours which arise within the
1 CASE REPORT OPEN ACCESS Pituitary Macroadenoma with Superior Orbital Fissure Syndrome Tapan Nagpal, Ankit Singhania ABSTRACT Introduction: Pituitary adenomas are benign tumours which arise within the
Binostril Endoscopic Trans-Sphenoidal Approach for Pituitary Adenomas
 Med. J. Cairo Univ., Vol. 85, No. 4, June: 1593-1600, 2017 www.medicaljournalofcairouniversity.net Binostril Endoscopic Trans-Sphenoidal Approach for Pituitary Adenomas HESHAM ABO RAHMA, M.D. and AHMED
Med. J. Cairo Univ., Vol. 85, No. 4, June: 1593-1600, 2017 www.medicaljournalofcairouniversity.net Binostril Endoscopic Trans-Sphenoidal Approach for Pituitary Adenomas HESHAM ABO RAHMA, M.D. and AHMED
ACROMEGALY OCCURRING IN A PATIENT WITH A PITUITARY ADENOMA, LYMPHOCYTIC HYPOPHYSITIS, AND A RATHKE CLEFT CYST
 Case Report ACROMEGALY OCCURRING IN A PATIENT WITH A PITUITARY ADENOMA, LYMPHOCYTIC HYPOPHYSITIS, AND A RATHKE CLEFT CYST Anupa Sharma, DO 1 ; Eric K.Richfield, MD, PhD 2 ; Sara E. Lubitz, MD 1 ABSTRACT
Case Report ACROMEGALY OCCURRING IN A PATIENT WITH A PITUITARY ADENOMA, LYMPHOCYTIC HYPOPHYSITIS, AND A RATHKE CLEFT CYST Anupa Sharma, DO 1 ; Eric K.Richfield, MD, PhD 2 ; Sara E. Lubitz, MD 1 ABSTRACT
Impact of Gamma Knife Radiosurgery on the neurosurgical management of skull-base lesions: The Combined Approach
 Radiosurgery as part of the neurosurgical armamentarium: Educational Symposium November 24 th 2011 Impact of Gamma Knife Radiosurgery on the neurosurgical management of skull-base lesions: The Combined
Radiosurgery as part of the neurosurgical armamentarium: Educational Symposium November 24 th 2011 Impact of Gamma Knife Radiosurgery on the neurosurgical management of skull-base lesions: The Combined
(3) Pituitary tumours
 Pituitary tumours") Hypopituitarism Diabetes Insipidus Pituitary tumours (2) Dr T Kemp - Endocrinology and Metabolism Unit - Steve Biko Academic Hospital (3) Pituitary tumours Pituitary microadenoma - intrasellar adenoma
Hypopituitarism Diabetes Insipidus Pituitary tumours (2) Dr T Kemp - Endocrinology and Metabolism Unit - Steve Biko Academic Hospital (3) Pituitary tumours Pituitary microadenoma - intrasellar adenoma
ABNORMAL PITUITARY FUNCTION
 Overview ABNORMAL PITUITARY FUNCTION Specialist Portfolio Seminar Katie Jones Sandwell and West Birmingham Hospitals NHS Trust Anterior pituitary overview Posterior pituitary overview Pituitary dysfunction
Overview ABNORMAL PITUITARY FUNCTION Specialist Portfolio Seminar Katie Jones Sandwell and West Birmingham Hospitals NHS Trust Anterior pituitary overview Posterior pituitary overview Pituitary dysfunction
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury
 Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to