Stereotactic Body Radiotherapy for Lung Tumours. Dr. Kaustav Talapatra Head, Radiation Oncology Kokilaben Dhirubhai Ambani Hospital Mumbai
|
|
|
- Dylan Tyler
- 5 years ago
- Views:
Transcription
1 Stereotactic Body Radiotherapy for Lung Tumours Dr. Kaustav Talapatra Head, Radiation Oncology Kokilaben Dhirubhai Ambani Hospital Mumbai
2 SBRT Definition SBRT is a method of External Beam Radiation that accurately delivers a high irradiation dose to an extracranial target in one of few treatmen t sessions
3 AAPM Task Group 101; (ASTRO and ACR); (CARO- SBRT) and the National Radiotherapy Implementation Group of the UK all agree on the following items: SBRT is (1) a method of external beam radiotherapy (EBRT) that (2) accurately delivers a (3) high dose of irradiation in (4) one or few treatment fractions to an (5) extracranial target.
4
5 Zone of the proximal bronchial tree. Patients with T3 tumors based on mediastinal invasion or < 2 cm toward carina invasion should be dealt with caution
6 Concepts and recommendations on patient selection ASTRO PRO 2017
7 When is SBRT appropriate for patients with T1-2, N0 NSCLC who are medically operable? Any patient with operable stage I NSCLC being considered for SBRT should be evaluated by a thoracic surgeon, preferably in a ultidisciplinary setting, to reduce specialty bias
8 For patients with standard operative risk (ie, with anticipated operative mortality of less than.5%) and stage I NSCLC, SBRT is not recommended as an alternative to surgery outside of a clinical trial. For this population, lobectomy with systematic mediastinal lymph node evaluation remains the recommended treatment, though a sublobar resection may be considered in select clinical scenarios For patients with high operative riskd discussions Regarding SBRT are encouraged
9 When is SBRT appropriate for medically inoperable patients with T1-2, N0 NSCLC: For centrally located tumours 3 fractions should be avoided Significant risks should be considered For more than 5 cm tumours Only if acceptable therapeutic ratio Volumetric, maximum dose constraints can be adhered to
10 For patients who underwent pneumonectomy and now have a new primary tumor in their remaining lung? SBRT may be considered a curative treatment option for patients with metachronous in a postpneumonectomy setting. While SBRT for metachronous MPLC appears to have equivalent rates of local control and acceptable toxicity compared to single tumors, SBRT in the postpneumonectomy setting might have a higher rate of toxicity than in patients with higher baseline lung capacity. Recommendation strength: Conditional Quality of evidence: Low
11 Contouring
12 Contouring: Challenges Respiration induced motion compromises the intention to deliver prescribed dose to tumours. Motion artefacts Erroneous Hounsfield unit (HU) causing insufficient dose coverage to tumours which may adversely affect hypofractionated stereotactic treatment especially for their small volume.
13 Planning: Image acquisition Computed tomography will be the primary image platform for targeting and treatment planning. Contrast to be used which will allow better distinction between tumor and adjacent vessels or atelectasis. spacing 3.0 mm between scans in the region of the tumor should be used. If equipped with 4 DCT system, this should be used.
14 Planning: Image acquisition In case of multiple measurements of ranges of motion (at simulations and/or at treatments, possibly pre- and posttreatments) provide information about the day and time when the data have been collected. When data for some patients/treatment fractions is not collected the record of the missing measurement has to be kept and reported. If there is a clinical reason for not collecting data, it needs to be reported as well. The reported range of motion has to be separated from setup errors
15

16 Moving direction of anatomy from exhale to inhale status

17 4D Treatment Planning Internal target `Volume (ITV) Concept PTV ITV Full Breathing Cycle Selected Phases only
18 Contouring: Patient specific tumor ITV to be determined in order to ensure adequate tumor coverage. 4 dimensional CT (4DCT) is the widely used method to obtain volumetric information due to tumor motion. Precise delineation of the target with a relatively tight Planning Target Volume (PTV), conformal RT planning with the management of target motion with respiration is pre-requisite to deliver high dose per fraction.

19 Contouring Due to respiratory motion there s image distortion GTV on single respiratory phase can under or overestimate the tumor volume Also mean tumour position can be misrepresented. Respiratory motion management should be considered if available.
20 Contouring: Simulation: Supine Contrast : IV contrast Non 4DCT system : PTV should be expanded 5 mm axially and 1 cm craniocaudally 4 DCT system: To generate ITV based on 4DCT data set and to give 5 mm symmetrical margin over the ITV to generate PTV
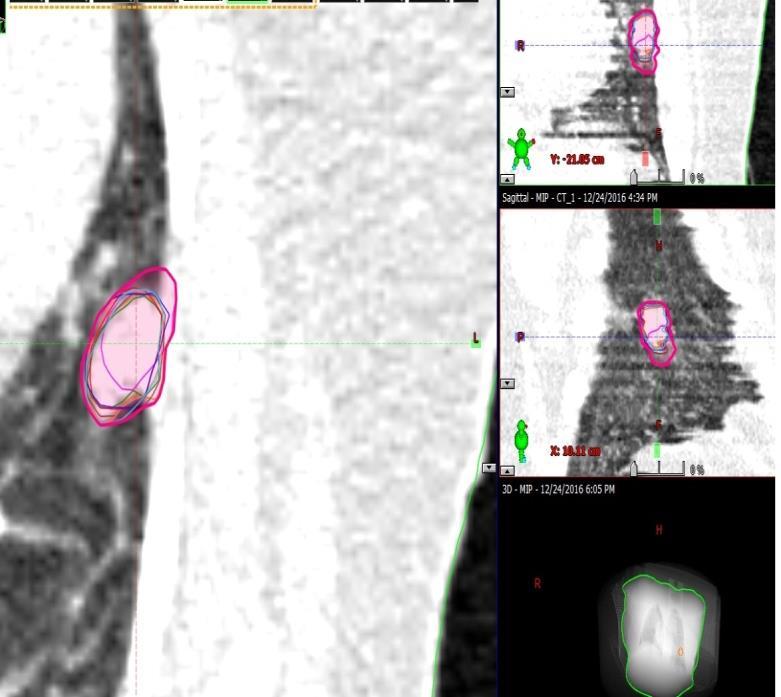
21 Contouring: Methods of ITV generation: -GTV to be contoured in all respiratory phases, then to draw the boolean structure to generate ITV -ITV can be drawn based on maximum intensity projection -In case of inhale, exhale and free breathing scan taking, GTV can be contoured in all these 3 phases an then to boolean hem o generate ITV.
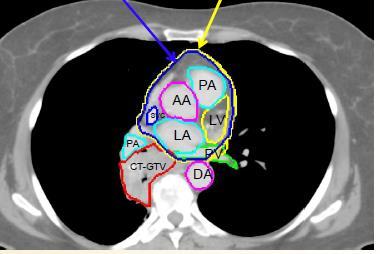
22 Contouring: Tumor The target will generally be drawn using CT pulmonary windows; Soft tissue windows with contrast may be used to avoid inclusion of adjacent vessels, atelectasis, or mediastinal or chest wall structures within the GTV. This target will not be enlarged whatsoever for prophylactic treatment (including no margin for presumed microscopic extension) Rather, include only abnormal CT signal consistent with gross tumor (i.e., the GTV and the clinical target volume [CTV] are identical).
23 Motion management and CT simulation: - Forced shallow breathing techniques (Compression paddle, Pressure belt) - Respiratory gated CT and 4DCT - Free Breathing and slow CT Scanners - Free Breathing and Fast CT Scanners - Breath Hold CT Scans

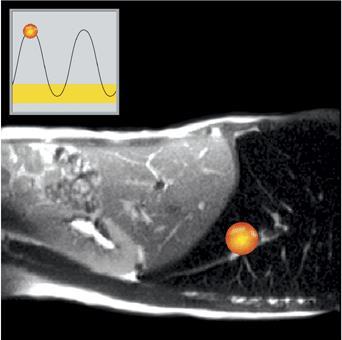
24 Respiratory Motion management Device:
 signals Beacon")


25 Radio frequency (RF) signals Beacon Electromagnetic Transponder Electromagnetic Signals:Locate and Track Continuously

26 Real-time tracking of target motion
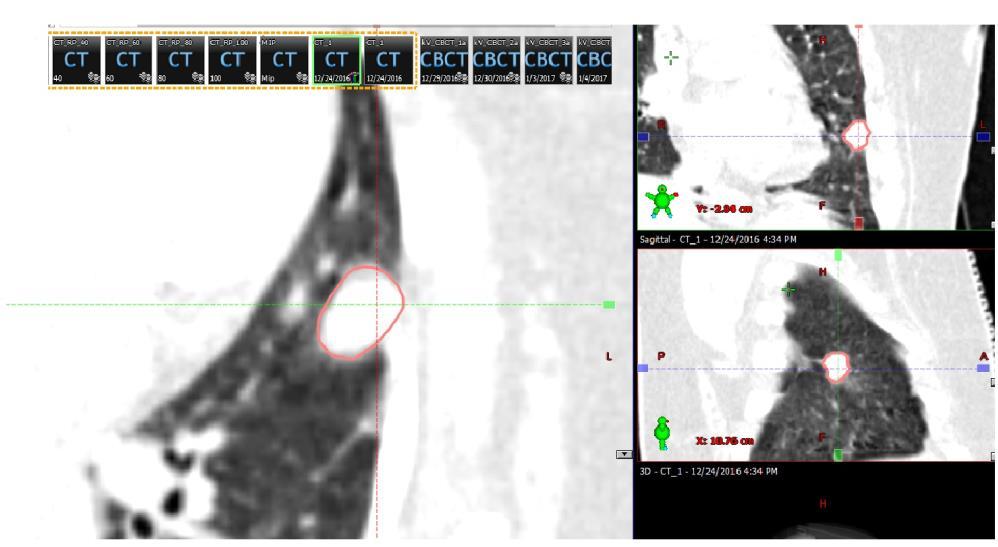
27 Contouring: Tumor
28 Contouring: Tumor

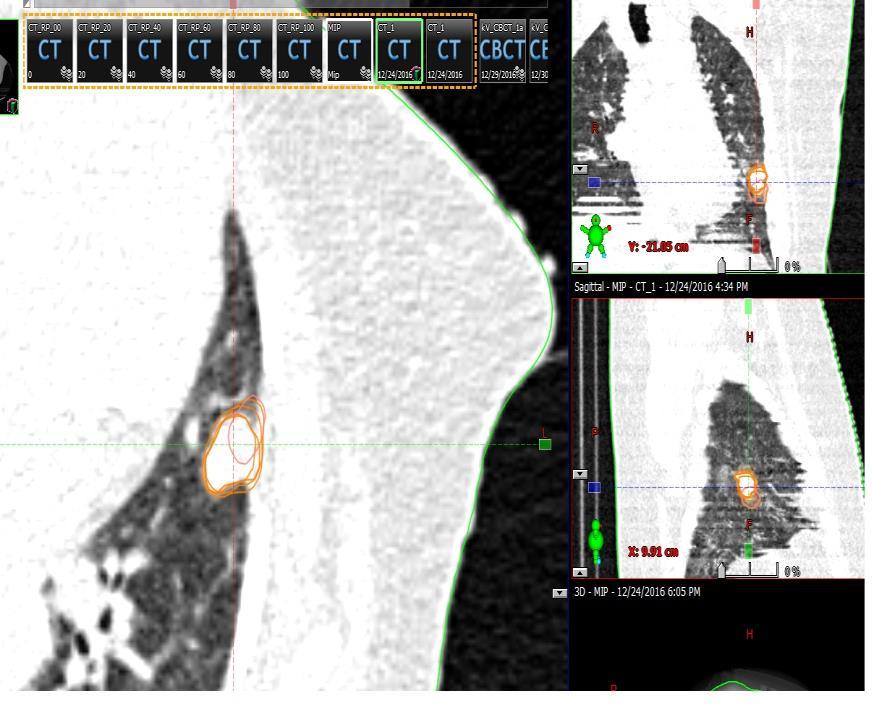
29 LUNG CONTOURING ON MIP :
30 This target will not be enlarged whatsoever for prophylactic treatment (including no margin for presumed microscopic extension) Only nly include abnormal CT signal consistent with gross tumor (i.e., the GTV and the Clinical Target Volume, CTV, are identical) An additional 0.5 cm in the axial plane and 1.0 cm in the longitudinal plane (cranio-caudal) will be added to the GTV to constitute the planning treatment volume (PTV)
31 Contorting: Normal structures Spinal Cord Contoured based on the bony limits of the spinal canal. The spinal cord should be contoured starting at least 10 cm above the superior extent of the PTV and continuing on every CT slice to at least 10 below the inferior extent of the PTV. Esophagus Contoured using mediastinal windowing on CT to correspond to the mucosal, submucosa, and all muscular layers out to the fatty adventitia. Extent as cord.
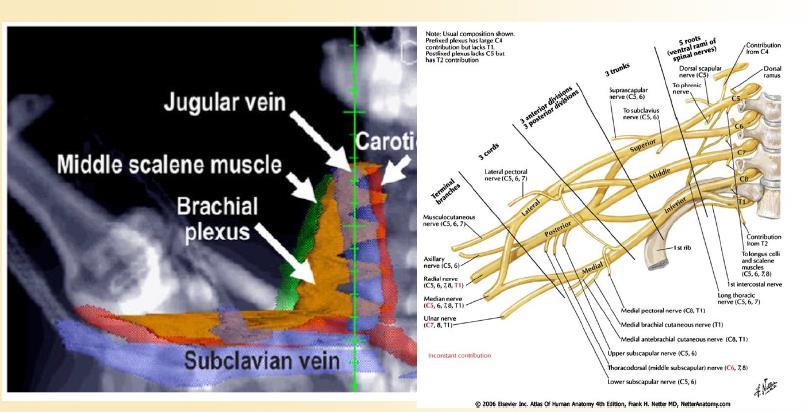
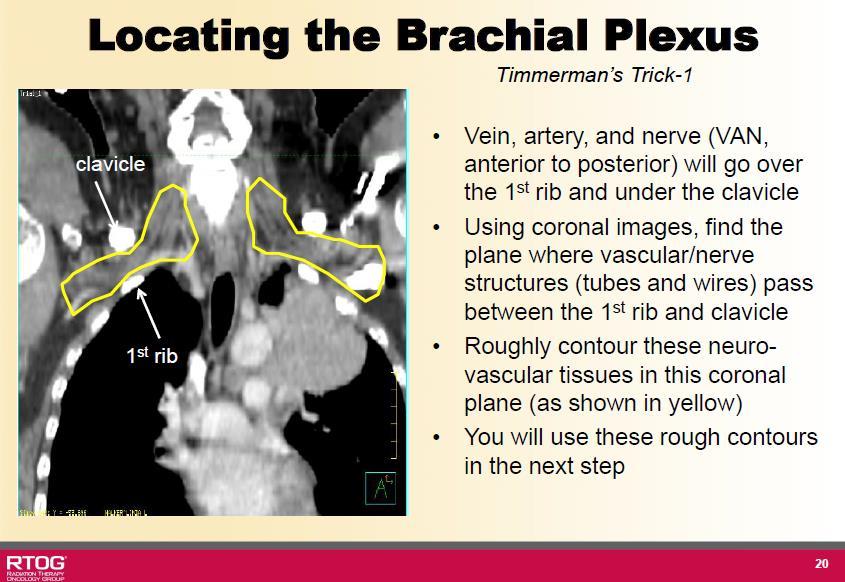
32 Contorting: Normal structures Brachial Plexus :The defined ipsilateral brachial plexus originates from the spinal nerves exiting the neuroforamine on the involved side from around C5 to T2. This neurovascular complex to be contoured starting proximally at the bifurcation of the brachiocephalic trunk into the jugular/subclavian veins (or carotid/subclavian arteries) and following along the route of the subclavian vein to the axillary vein ending after the neurovascular structures cross the second rib.
33
34
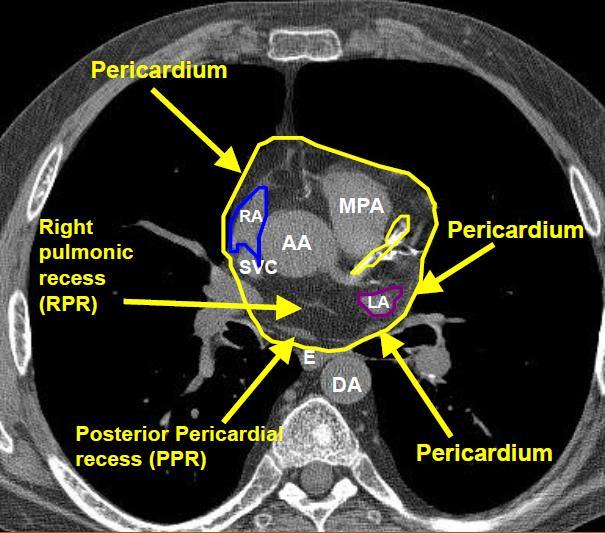
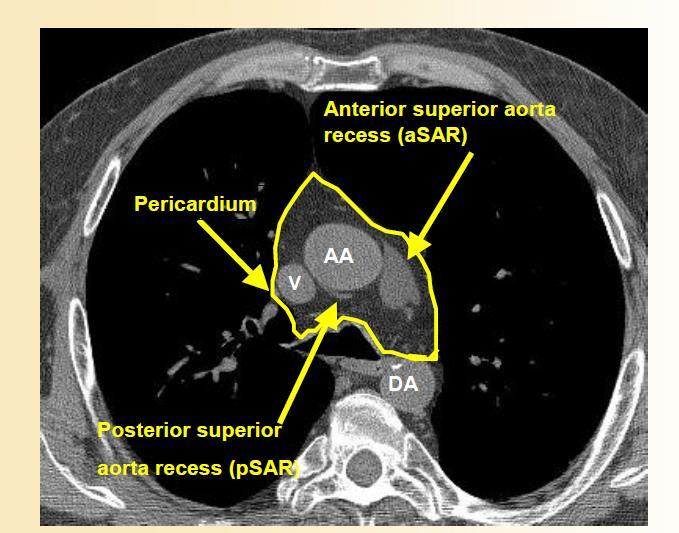
35 Contorting: Normal structures Heart to be contoured along with the pericardial sac. The superior aspect (or base) for purposes of contouring will begin at the level of the inferior aspect of the aortic arch (aortopulmonary window) Extend inferiorly to the apex of the heart / diaphragm.
36

37 RTOG Atlas
38
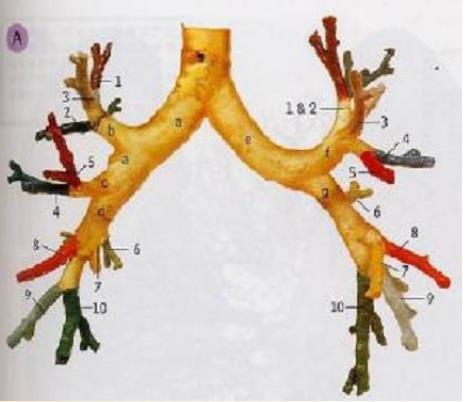
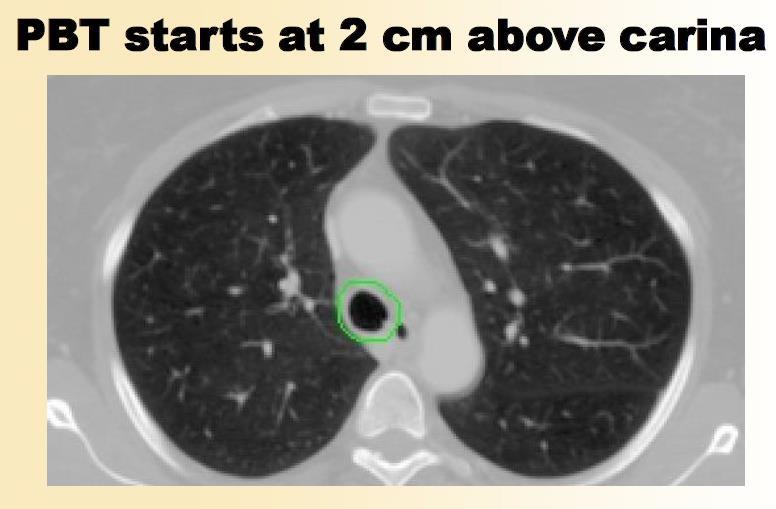
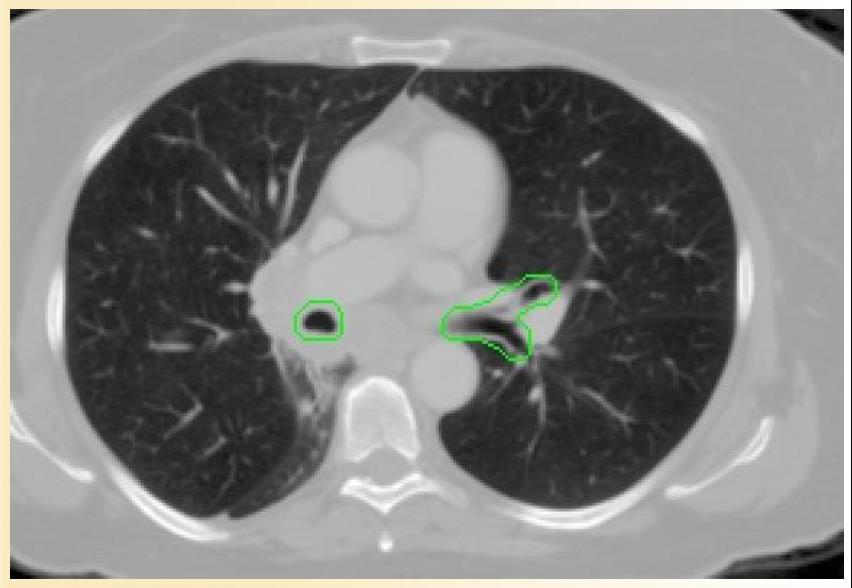
39 Contorting: Normal structures Trachea and Proximal Bronchial Tree to be contoured as two separate structures using Mediastinal windows on CT to correspond to the mucosal, submucosa and cartilage rings and airway channels associated with these structures. For this purpose, the trachea will be divided into two sections: Proximal trachea Distal 2 cm of trachea. The proximal trachea will be contoured as one structure, and the distal 2 cm of trachea will be included in the structure identified as proximal bronchial tree.
40 Contorting: Normal structures Contouring of the proximal trachea should begin at least 10 cm superior to the extent of the PTV or 5 cm superior to the carina (whichever is more superior) and continue inferiorly to the superior aspect of the proximal bronchial tree. The proximal bronchial tree will include the most inferior 2 cm of distal trachea and the proximal airways on both sides
41 Contorting: Normal structures The following airways will be included according to standard anatomic relationships: distal 2 cm of trachea the carina, the right and left mainstem bronchi the right and left upper lobe bronchi the intermedius bronchus, the right middle lobe bronchus, the lingular bronchus, and the right and left lower lobe bronchi. Contouring of the lobar bronchi will end immediately at the site of a segmental bifurcation. If there are parts of the proximal bronchial tree that are within GTV, they should be contoured separately, as proximal bronchial tree GTV
42
43
44

45

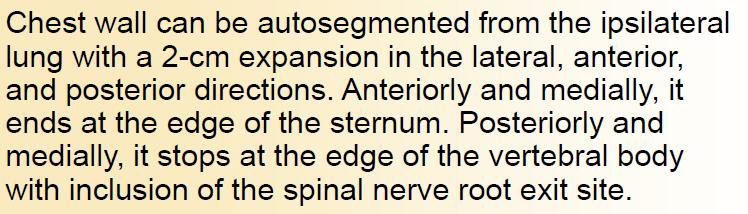
46 Chest wall
47 Contorting: Normal structures Whole Lung Both the right and left lungs should be contoured as one structure. Contouring should be carried out using pulmonary windows. All inflated and collapsed lung should be contoured Gross tumor (GTV) and trachea/ipsilateral bronchus as defined above should not be included in this structure.
48 Contorting: Normal structures The skin is the outer 0.5 cm of the body surface. As such it is a rind of uniform thickness (0.5 cm) which envelopes the entire body in the axial planes. The great vessels (aorta and vena cava, not the pulmonary artery or vein) contoured using mediastinal window on CT to correspond to the vascular wall and all muscular layers out to the fatty adventitia. The great vessel should be contoured starting at least 10 cm above the superior extent of the PTV and continuing on every CT slice to at least 10 cm below the inferior extent of the PTV. For right sided tumors, the vena cava will be contoured, and for left sided tumors, the aorta will be contoured.
49
50 Contorting: Normal structures Non-adjacent Wall of a Structure For the esophagus, trachea and proximal bronchial tree, and great vessels, corresponds to the half circumference of the tubular structure not immediately touching the GTV or PTV These contours would start and stop superiorly and inferiorly just as with the named structure. The half lumen of the structure should be included in this contour
51 Plan evaluation: Lung SBRT planning and evaluation has some basic principles. Based on RTOG 0813 it has been described.
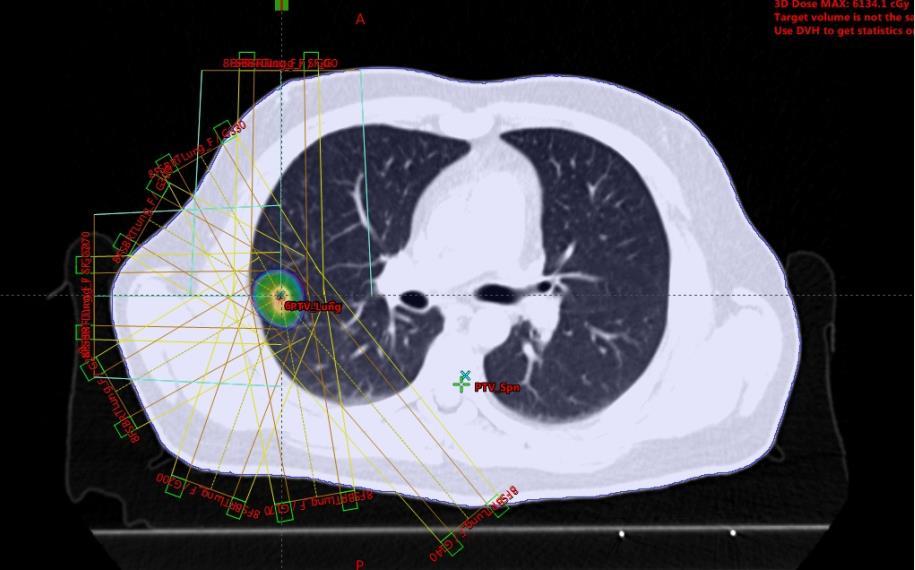
52 Planning: Dosimetry; 3D conformal planning 3 D coplanar or non-coplanar beam arrangements will be custom designed to deliver highly conformal prescription dose distributions. Non-opposing, noncoplanar beams are preferable. Typically, 7-10 beams of radiation will be used with roughly equal weighting. Generally, more beams are used for larger lesion sizes. When static beams are used, a minimum of seven non-opposing beams should be used. For arc rotation techniques, a minimum of 340 degrees (cumulative for all beams) should be utilized. For this protocol, the isocenter is defined as the common point of gantry and couch rotation for the treatment unit.
53 Planning: Dosimetry; 3D conformal planning Field aperture size and shape should correspond nearly identically to the projection of the PTV along a beam s eye view (i.e., no additional margin beyond the PTV). The only exception will be when observing the minimum field dimension of 3.5 cm when treating small lesions. Prescription lines covering the PTV will be the 60-90% line (rather than %); however, higher isodoses (hotspots) must be manipulated to occur within the target and not in adjacent normal tissue. The isocenter in stereotactic coordinates will be determined from system fiducials (or directly from the tumor in the case of volumetric imaging) and translated to the treatment record.
54 Planning: Dosimetry; 3D conformal planning The plan should be normalized to a defined point corresponding closely to the center of mass of the PTV (COMPTV). Typically, this point will be the isocenter of the beam rotation The point identified as COMPTV must have defined stereotactic coordinates and receive 100% of the normalized dose. Because the beam apertures coincide nearly directly with the edge of the PTV (little or no added margin).
55 Planning: Dosimetry; 3D conformal planning The external border of the PTV will be covered by a lower isodose surface than usually used in conventional radiotherapy planning, typically around 80% but ranging from 60-90%. The prescription dose will be delivered to the margin of the PTV and fulfill the requirements below. As such, a hotspot will exist within the PTV centrally at the COMPTV with a magnitude of prescribed dose times the reciprocal of the chosen prescription isodose line (i.e., 60-90%).
56 Planning: Dosimetry; IMRT IMRT should be considered only when target coverage, OAR dose limits, or dose spillage are not achievable with 3D conformal planning. The number of segments (control points) and the area of each segment should be optimized to ensure deliverability and avoid complex beam fluences. Ideally, the number of segments should be minimized (2-3 segments per beam should be adequate), and the area of each segment should be maximized (the aperture of one segment from each beam should correspond to the projection of the PTV along a beam s eye view).
57 Planning: Evaluation Successful treatment planning will require accomplishment of all of the following criteria: Normalization: The treatment plan should be normalized such that 100% corresponds to the center of mass of the PTV (COMPTV). This point will typically also correspond (but is not required to correspond) to the isocenter of the treatment beams. Prescription Isodose Surface Coverage: The prescription isodose surface will be chosen such that 95% of the target volume (PTV) is conformally covered by the prescription isodose surface and 99% of the target volume (PTV) receives a minimum of 90% of the prescription dose.
58 Planning: Evaluation Target Dose Heterogeneity: The prescription isodose surface selected must be o 60% of the dose at the center of mass of the PTV (COMPTV) and o 90% of the dose at the center of mass of the PTV (COMPTV). The COMPTV corresponds to the normalization point (100%) of the plan.

59
60 Planning: Evaluation High Dose Spillage: a. Location: Any dose > 105% of the prescription dose should occur primarily within the PTV itself and not within the normal tissues outside the PTV. Therefore, the cumulative volume of all tissue outside the PTV receiving a dose > 105% of prescription dose should be no more than 15% of the PTV volume. b. Volume: Conformality of PTV coverage will be judged such that the ratio of the volume of the prescription isodose to the volume of the PTV is ideally < 1.2. These criteria will not be required to be met in treating very small tumors (< 2.5 cm axial GTV dimension or < 1.5 cm craniocaudal GTV dimension) in which the required minimum field size of 3.5 cm.
61
62 Planning: Evaluation Low Dose Spillage: The falloff gradient beyond the PTV extending into normal tissue structures must be rapid in all directions and meet the following criteria: a. Location: The maximum total dose over all fractions in Gray (Gy) to any point 2 cm or greater away from the PTV in any direction must be no greater than D2cm where D2cm is given by the table below. b. Volume: The ratio of the volume of 50% of the prescription dose isodose to the volume of the PTV must be no greater than R50% where R50% is given.
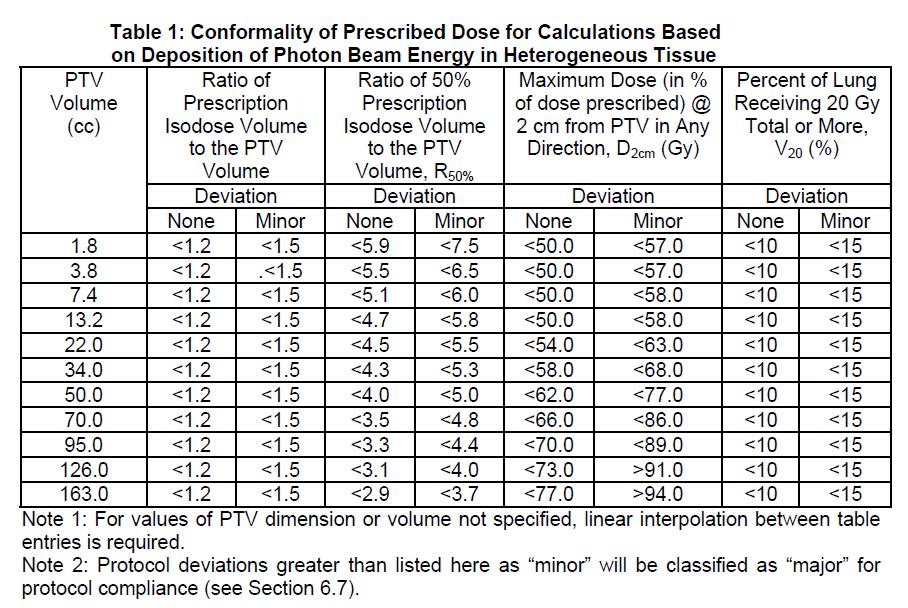
63 Planning: Evaluation
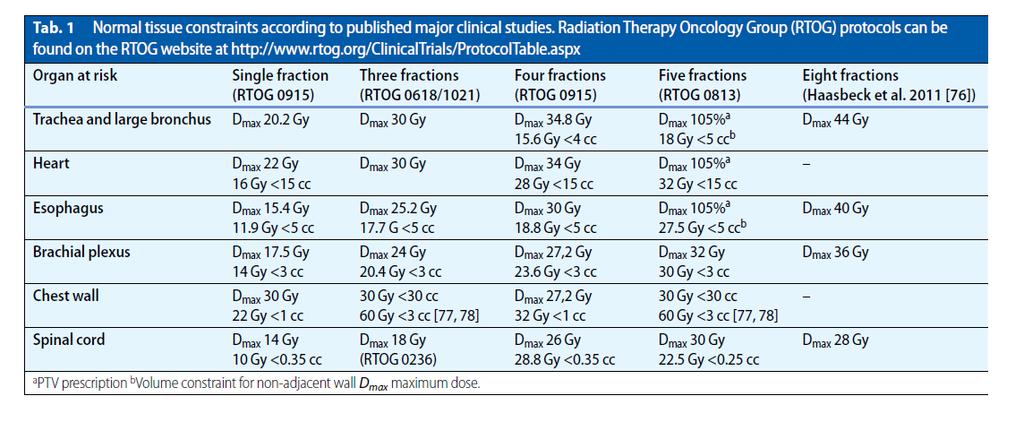
64 Planning: Evaluation The esophagus, trachea, bronchi and heart may be situated adjacent to the treated GTV/PTV. There is no specified limit as tumors that are immediately adjacent to that organ will not be able to be treated to any of the prescription doses without irradiating a small volume of that organ to the prescribed dose. In such a case, the planning needs to be done so that there is no hot spot within that organ, even if that organ is part of the PTV, i.e., that no part of any OAR receives more than 105% of the prescribed dose

65 Planning: Evaluation RTOG 0813, June 8, 2015

66 Planning: Evaluation RTOG 0813, June 8, 2015

67 Planning: Evaluation RTOG 0813, June 8, 2015
68
69 Toxicity documentation and reporting Cardiac and Pericardial injury Gastrointestinal/Esophageal Injury ( Esophagitis, ulceration,stenosis fistula ) The radiation effects on the esophagus can be acute: esophagitis Central Airway/Bronchial Injury This bronchial injury with subsequent focal collapse of lung may impair overall pulmonary status. The consequences of bronchial toxicity, e.g., cough, dyspnea, hypoxia, impairment of pulmonary function test parameters, pleural effusion or pleuritic pain
70 Lung Injury :Radiation pneumonitis is a subacute (weeks to months from treatment) inflammation of the end bronchioles and alveoli. Radiation fibrosis is a late manifestation of radiation injury to the irradiated lung. Rib Fracture
71 Thank You
Atlases for Organs at Risk (OARs) in Thoracic Radiation Therapy
 in Thoracic Radiation Therapy") Atlases for Organs at Risk (OARs) in Thoracic Radiation Therapy Feng-Ming (Spring) Kong MD PhD Leslie Quint MD Mitchell Machtay MD Jeffrey Bradley MD 1 Outline of Content Atlas for lung, esophagus, and
Atlases for Organs at Risk (OARs) in Thoracic Radiation Therapy Feng-Ming (Spring) Kong MD PhD Leslie Quint MD Mitchell Machtay MD Jeffrey Bradley MD 1 Outline of Content Atlas for lung, esophagus, and
Image Guided Stereotactic Radiotherapy of the Lung
 Image Guided Stereotactic Radiotherapy of the Lung Jamie Marie Harris, MS DABR Avera McKennan Radiation Oncology September 25, 2015 Stereotactic Body Radiotherapy - Clinical Dose/Fractionation - Normal
Image Guided Stereotactic Radiotherapy of the Lung Jamie Marie Harris, MS DABR Avera McKennan Radiation Oncology September 25, 2015 Stereotactic Body Radiotherapy - Clinical Dose/Fractionation - Normal
Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali
 Dr Raj K Shrimali") Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali Let us keep this simple and stick to some basic rules Patient positioning Must be reproducible Must be
Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali Let us keep this simple and stick to some basic rules Patient positioning Must be reproducible Must be
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR
 Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
Standard care plan for stereotactic body radiotherapy for non-small-cell lung cancer
 RADIOTHERAPY PROTOCOL Document Title: Document Type: Subject: Approved by: Stereotactic Body Radiotherapy for Non-Small Cell Lung Cancer (54-60 Gy in 3-8 fractions) Clinical Guideline Standard Care Plan
RADIOTHERAPY PROTOCOL Document Title: Document Type: Subject: Approved by: Stereotactic Body Radiotherapy for Non-Small Cell Lung Cancer (54-60 Gy in 3-8 fractions) Clinical Guideline Standard Care Plan
Defining Target Volumes and Organs at Risk: a common language
 Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
On the use of 4DCT derived composite CT images in treatment planning of SBRT for lung tumors
 On the use of 4DCT derived composite CT images in treatment planning of SBRT for lung tumors Zhe (Jay) Chen, Ph.D. Department of Therapeutic Radiology Yale University School of Medicine and Yale-New Haven
On the use of 4DCT derived composite CT images in treatment planning of SBRT for lung tumors Zhe (Jay) Chen, Ph.D. Department of Therapeutic Radiology Yale University School of Medicine and Yale-New Haven
Lung Cancer Radiotherapy
 Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Protocol of Radiotherapy for Small Cell Lung Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
4D Radiotherapy in early ca Lung. Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla
 4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
SBRT TREATMENT PLANNING: TIPS + TRICKS. Rachel A. Hackett CMD, RT(T)
") SBRT TREATMENT PLANNING: TIPS + TRICKS Rachel A. Hackett CMD, RT(T) OUTLINE Brief radiobiology review 3D CRT Tx Planning VMAT Tx Planning Protocols Other Sites Oligomets Spine Liver Kidney Adrenal Gland
SBRT TREATMENT PLANNING: TIPS + TRICKS Rachel A. Hackett CMD, RT(T) OUTLINE Brief radiobiology review 3D CRT Tx Planning VMAT Tx Planning Protocols Other Sites Oligomets Spine Liver Kidney Adrenal Gland
SBRT fundamentals. Outline 8/2/2012. Stereotactic Body Radiation Therapy Quality Assurance Educational Session
 Stereotactic Body Radiation Therapy Quality Assurance Educational Session J Perks PhD, UC Davis Medical Center, Sacramento CA SBRT fundamentals Extra-cranial treatments Single or small number (2-5) of
Stereotactic Body Radiation Therapy Quality Assurance Educational Session J Perks PhD, UC Davis Medical Center, Sacramento CA SBRT fundamentals Extra-cranial treatments Single or small number (2-5) of
REVISITING ICRU VOLUME DEFINITIONS. Eduardo Rosenblatt Vienna, Austria
 REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies USE OF STEREOTACTIC BODY RADIATION THERAPY FOR INOPERABLE NON- SMALL CELL LUNG TUMORS
 UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies USE OF STEREOTACTIC BODY RADIATION THERAPY FOR INOPERABLE NON- SMALL CELL LUNG TUMORS A Research Project Report Submitted in Partial Fulfillment of the
UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies USE OF STEREOTACTIC BODY RADIATION THERAPY FOR INOPERABLE NON- SMALL CELL LUNG TUMORS A Research Project Report Submitted in Partial Fulfillment of the
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Stereotaxy. Outlines. Establishing SBRT Program: Physics & Dosimetry. SBRT - Simulation. Body Localizer. Sim. Sim. Sim. Stereotaxy?
 Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical
 The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
Pitfalls in SBRT Treatment Planning for a Moving Target
 Pitfalls in SBRT Treatment Planning for a Moving Target Cynthia F. Chuang, Ph.D. Department of Radiation Oncology University of California-San Francisco I have no conflicts of interests to disclose In
Pitfalls in SBRT Treatment Planning for a Moving Target Cynthia F. Chuang, Ph.D. Department of Radiation Oncology University of California-San Francisco I have no conflicts of interests to disclose In
A Dosimetric Comparison of Whole-Lung Treatment Techniques. in the Pediatric Population
 A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
Specification of Tumor Dose. Prescription dose. Purpose
 Specification of Tumor Dose George Starkschall, Ph.D. Department of Radiation Physics U.T. M.D. Anderson Cancer Center Prescription dose What do we mean by a dose prescription of 63 Gy? Isocenter dose
Specification of Tumor Dose George Starkschall, Ph.D. Department of Radiation Physics U.T. M.D. Anderson Cancer Center Prescription dose What do we mean by a dose prescription of 63 Gy? Isocenter dose
Ashley Pyfferoen, MS, CMD. Gundersen Health Systems La Crosse, WI
 Ashley Pyfferoen, MS, CMD Gundersen Health Systems La Crosse, WI 3 Radiation Oncologists 3 Physicists 2 Dosimetrists 9 Radiation Therapists o o o o o o o o o Brachial Plexus Anatomy Brachial Plexopathy
Ashley Pyfferoen, MS, CMD Gundersen Health Systems La Crosse, WI 3 Radiation Oncologists 3 Physicists 2 Dosimetrists 9 Radiation Therapists o o o o o o o o o Brachial Plexus Anatomy Brachial Plexopathy
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS
 THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013
 Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
A dosimetric evaluation of VMAT for the treatment of non-small cell lung cancer
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 14, NUMBER 1, 2013 A dosimetric evaluation of VMAT for the treatment of non-small cell lung cancer Caitlin E. Merrow, a Iris Z. Wang, Matthew B. Podgorsak
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 14, NUMBER 1, 2013 A dosimetric evaluation of VMAT for the treatment of non-small cell lung cancer Caitlin E. Merrow, a Iris Z. Wang, Matthew B. Podgorsak
Silvia Pella, PhD, DABR Brian Doozan, MS South Florida Radiation Oncology Florida Atlantic University Advanced Radiation Physics Boca Raton, Florida
 American Association of Medical Dosimetrists 2015 Silvia Pella, PhD, DABR Brian Doozan, MS South Florida Radiation Oncology Florida Atlantic University Advanced Radiation Physics Boca Raton, Florida Most
American Association of Medical Dosimetrists 2015 Silvia Pella, PhD, DABR Brian Doozan, MS South Florida Radiation Oncology Florida Atlantic University Advanced Radiation Physics Boca Raton, Florida Most
Maria Golish, CMD, RTT, BS
 Maria Golish, CMD, RTT, BS Thank you auto-segmentation!! Had a limited role in early days of Radiotherapy Mostly based in Diagnostic Radiology department Slowly increased importance in RT department Currently
Maria Golish, CMD, RTT, BS Thank you auto-segmentation!! Had a limited role in early days of Radiotherapy Mostly based in Diagnostic Radiology department Slowly increased importance in RT department Currently
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI)
 for Craniospinal Irradiation (CSI)") Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases
 Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Therapy of Non-Operable early stage NSCLC
 SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
IGRT Protocol Design and Informed Margins. Conflict of Interest. Outline 7/7/2017. DJ Vile, PhD. I have no conflict of interest to disclose
 IGRT Protocol Design and Informed Margins DJ Vile, PhD Conflict of Interest I have no conflict of interest to disclose Outline Overview and definitions Quantification of motion Influences on margin selection
IGRT Protocol Design and Informed Margins DJ Vile, PhD Conflict of Interest I have no conflict of interest to disclose Outline Overview and definitions Quantification of motion Influences on margin selection
- In potentially operable patients -
 Lung Stereotactic Ablative Radiotherapy (SABR) - In potentially operable patients - Frank Lagerwaard VUMC Amsterdam Stereotactic Ablative Radiotherapy (SABR) 2003-2008 4DCT-based target definition Non-gated
Lung Stereotactic Ablative Radiotherapy (SABR) - In potentially operable patients - Frank Lagerwaard VUMC Amsterdam Stereotactic Ablative Radiotherapy (SABR) 2003-2008 4DCT-based target definition Non-gated
biij Initial experience in treating lung cancer with helical tomotherapy
 Available online at http://www.biij.org/2007/1/e2 doi: 10.2349/biij.3.1.e2 biij Biomedical Imaging and Intervention Journal CASE REPORT Initial experience in treating lung cancer with helical tomotherapy
Available online at http://www.biij.org/2007/1/e2 doi: 10.2349/biij.3.1.e2 biij Biomedical Imaging and Intervention Journal CASE REPORT Initial experience in treating lung cancer with helical tomotherapy
IROC Lung Phantom 3D CRT / IMRT. Guidelines for Planning and Irradiating the IROC Lung Phantom. Revised Dec 2015
 IROC Lung Phantom 3D CRT / IMRT Guidelines for Planning and Irradiating the IROC Lung Phantom. Revised Dec 2015 The IROC requests that each institution keep the phantom for no more than 2 weeks. During
IROC Lung Phantom 3D CRT / IMRT Guidelines for Planning and Irradiating the IROC Lung Phantom. Revised Dec 2015 The IROC requests that each institution keep the phantom for no more than 2 weeks. During
8/3/2016. Outline. Site Specific IGRT Considerations for Clinical Imaging Protocols. Krishni Wijesooriya, PhD University of Virginia
 Site Specific IGRT Considerations for Clinical Imaging Protocols Krishni Wijesooriya, PhD University of Virginia Outline Image registration accuracies for different modalities What imaging modality best
Site Specific IGRT Considerations for Clinical Imaging Protocols Krishni Wijesooriya, PhD University of Virginia Outline Image registration accuracies for different modalities What imaging modality best
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
Treatment Planning for Lung. Kristi Hendrickson, PhD, DABR University of Washington Dept. of Radiation Oncology
 Treatment Planning for Lung Kristi Hendrickson, PhD, DABR University of Washington Dept. of Radiation Oncology Outline of Presentation Dosimetric planning strategies for SBRT lung Delivery techniques Examples
Treatment Planning for Lung Kristi Hendrickson, PhD, DABR University of Washington Dept. of Radiation Oncology Outline of Presentation Dosimetric planning strategies for SBRT lung Delivery techniques Examples
Fiducial-Free Lung Tracking and Treatment with the CyberKnife System: A Non-Invasive Approach
 Fiducial-Free Lung Tracking and Treatment with the CyberKnife System: A Non-Invasive Approach Jesse McKay, MS, DABR Erlanger Health System Chattanooga, TN JASTRO 2014, Yokohama Japan Disclosure I have
Fiducial-Free Lung Tracking and Treatment with the CyberKnife System: A Non-Invasive Approach Jesse McKay, MS, DABR Erlanger Health System Chattanooga, TN JASTRO 2014, Yokohama Japan Disclosure I have
CPT code semantics 8/18/2011. SBRT Planning Case Studies. Spectrum of applications of SBRT. itreat
 Spectrum of applications of SBRT EDUCATIONAL COURSE Physics and Dosimetry of SBRT Part III: Planning Case Studies Brian D. Kavanagh, MD, MPH Department of Radiation Oncology University of Colorado School
Spectrum of applications of SBRT EDUCATIONAL COURSE Physics and Dosimetry of SBRT Part III: Planning Case Studies Brian D. Kavanagh, MD, MPH Department of Radiation Oncology University of Colorado School
Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas
 1 Carol Boyd Comprehensive Case Study July 11, 2013 Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas Abstract: Introduction:
1 Carol Boyd Comprehensive Case Study July 11, 2013 Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas Abstract: Introduction:
ASTRO econtouring for Lymphoma. Stephanie Terezakis, MD
 ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
Tecniche Radioterapiche U. Ricardi
 Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
BLADDER RADIOTHERAPY PLANNING DOCUMENT
 A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies
 UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies A SINGLE INSTITUTION S EXPERIENCE IN DEVELOPING A PURPOSEFUL AND EFFICIENT OFF-LINE TECHNIQUE FOR ADAPTIVE RADIOTHERAPY IN A CLINICAL ENVIRONMENT A Research
UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies A SINGLE INSTITUTION S EXPERIENCE IN DEVELOPING A PURPOSEFUL AND EFFICIENT OFF-LINE TECHNIQUE FOR ADAPTIVE RADIOTHERAPY IN A CLINICAL ENVIRONMENT A Research
Which Planning CT Should be Used for Lung SBRT? Ping Xia, Ph.D. Head of Medical Physics in Radiation Oncology Cleveland Clinic
 Which Planning CT Should be Used for Lung SBRT? Ping Xia, Ph.D. Head of Medical Physics in Radiation Oncology Cleveland Clinic Outline Image quality and image dose Free breathing CT, 4DCT, and synthetic
Which Planning CT Should be Used for Lung SBRT? Ping Xia, Ph.D. Head of Medical Physics in Radiation Oncology Cleveland Clinic Outline Image quality and image dose Free breathing CT, 4DCT, and synthetic
Implementing SBRT Protocols: A NRG CIRO Perspective. Ying Xiao, Ph.D. What is NRG Oncology?
 Implementing SBRT Protocols: A NRG CIRO Perspective Ying Xiao, Ph.D. What is NRG Oncology? One of five new NCI-supported National Clinical Trials Network (NCTN) groups. NCTN officially started March 1,
Implementing SBRT Protocols: A NRG CIRO Perspective Ying Xiao, Ph.D. What is NRG Oncology? One of five new NCI-supported National Clinical Trials Network (NCTN) groups. NCTN officially started March 1,
IROC Liver Phantom. Guidelines for Planning and Irradiating the IROC Liver Phantom. Revised July 2015
 IROC Liver Phantom Guidelines for Planning and Irradiating the IROC Liver Phantom. Revised July 2015 The study groups are requests that each institution keep the phantom for no more than 2 weeks. During
IROC Liver Phantom Guidelines for Planning and Irradiating the IROC Liver Phantom. Revised July 2015 The study groups are requests that each institution keep the phantom for no more than 2 weeks. During
Comparison of Interfacility Implementation of Essential SBRT Components. Keith Neiderer B.S. CMD RT(T) VCU Health System
 VCU Health System") Comparison of Interfacility Implementation of Essential SBRT Components Keith Neiderer B.S. CMD RT(T) VCU Health System Disclosures None Objectives Review essential components that characterize SBRT Compare
Comparison of Interfacility Implementation of Essential SBRT Components Keith Neiderer B.S. CMD RT(T) VCU Health System Disclosures None Objectives Review essential components that characterize SBRT Compare
UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies
 UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies AN ANALYSIS OF FOUR DIMENSIONAL STEREOTACTIC BODY RADIATION THERAPY FOR LUNG CANCER: ABDOMINAL COMPRESSION VERSUS FREE BREATHING A Research Project Report
UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies AN ANALYSIS OF FOUR DIMENSIONAL STEREOTACTIC BODY RADIATION THERAPY FOR LUNG CANCER: ABDOMINAL COMPRESSION VERSUS FREE BREATHING A Research Project Report
Chapters from Clinical Oncology
 Chapters from Clinical Oncology Lecture notes University of Szeged Faculty of Medicine Department of Oncotherapy 2012. 1 RADIOTHERAPY Technical aspects Dr. Elemér Szil Introduction There are three possibilities
Chapters from Clinical Oncology Lecture notes University of Szeged Faculty of Medicine Department of Oncotherapy 2012. 1 RADIOTHERAPY Technical aspects Dr. Elemér Szil Introduction There are three possibilities
Stereotactic Body Radiotherapy (SBRT) For HCC T A R E K S H O U M A N P R O F. R A D I A T I O N O N C O L O G Y N C I, C A I R O U N I V.
 For HCC T A R E K S H O U M A N P R O F. R A D I A T I O N O N C O L O G Y N C I, C A I R O U N I V.") Stereotactic Body Radiotherapy (SBRT) For HCC T A R E K S H O U M A N P R O F. R A D I A T I O N O N C O L O G Y N C I, C A I R O U N I V. Hepatocellular carcinoma (HCC), is a major health problem worldwide.
Stereotactic Body Radiotherapy (SBRT) For HCC T A R E K S H O U M A N P R O F. R A D I A T I O N O N C O L O G Y N C I, C A I R O U N I V. Hepatocellular carcinoma (HCC), is a major health problem worldwide.
Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain
 for treatment of post-operative high grade glioma in the right parietal region of brain") 1 Carol Boyd March Case Study March 11, 2013 Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain History of Present Illness:
1 Carol Boyd March Case Study March 11, 2013 Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain History of Present Illness:
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
Subject: Image-Guided Radiation Therapy
 04-77260-19 Original Effective Date: 02/15/10 Reviewed: 01/25/18 Revised: 01/01/19 Subject: Image-Guided Radiation Therapy THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
04-77260-19 Original Effective Date: 02/15/10 Reviewed: 01/25/18 Revised: 01/01/19 Subject: Image-Guided Radiation Therapy THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
Sarcoma and Radiation Therapy. Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington
 Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th & 12 th Eds.)
") PLEURAL CAVITY AND LUNGS Dr. Milton M. Sholley SELF STUDY RESOURCES Essential Clinical Anatomy 3 rd ed. (ECA): pp. 70 81 Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th &
PLEURAL CAVITY AND LUNGS Dr. Milton M. Sholley SELF STUDY RESOURCES Essential Clinical Anatomy 3 rd ed. (ECA): pp. 70 81 Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th &
CT Chest. Verification of an opacity seen on the straight chest X ray
 CT Chest Indications: To assess equivocal plain x-ray findings Staging of lung neoplasm Merastatic workup of extra thoraces malignancies Diagnosis of diffuse lung diseases with HRCT Assessment of bronchietasis
CT Chest Indications: To assess equivocal plain x-ray findings Staging of lung neoplasm Merastatic workup of extra thoraces malignancies Diagnosis of diffuse lung diseases with HRCT Assessment of bronchietasis
SBRT of Lung & Liver lesions using Novalis IGRT System. Patrick Silgen, M.S., DABR Park Nicollet Methodist Hospital
 SBRT of Lung & Liver lesions using Novalis IGRT System Patrick Silgen, M.S., DABR Park Nicollet Methodist Hospital It could be worse!!! Acknowledgements Michael Weber, M.S., DABR Brenden Garrity, M.S.,
SBRT of Lung & Liver lesions using Novalis IGRT System Patrick Silgen, M.S., DABR Park Nicollet Methodist Hospital It could be worse!!! Acknowledgements Michael Weber, M.S., DABR Brenden Garrity, M.S.,
CENTRAL3D: A CLINICAL TOOL FOR IMPROVED CHARACTERIZATION OF CENTRALLY LOCATED NON-SMALL CELL LUNG CANCER
 CENTRAL3D: A CLINICAL TOOL FOR IMPROVED CHARACTERIZATION OF CENTRALLY LOCATED NON-SMALL CELL LUNG CANCER Dominique Mathieu MD MSc, Vincent Cousineau Daoust MSc, Alexis Lenglet MD MSc, Édith Filion MD,
CENTRAL3D: A CLINICAL TOOL FOR IMPROVED CHARACTERIZATION OF CENTRALLY LOCATED NON-SMALL CELL LUNG CANCER Dominique Mathieu MD MSc, Vincent Cousineau Daoust MSc, Alexis Lenglet MD MSc, Édith Filion MD,
Advanced Technology Consortium (ATC) Credentialing Procedures for 3D Conformal Therapy Protocols 3D CRT Benchmark*
 Credentialing Procedures for 3D Conformal Therapy Protocols 3D CRT Benchmark*") Advanced Technology Consortium (ATC) Credentialing Procedures for 3D Conformal Therapy Protocols 3D CRT Benchmark* Purpose: To evaluate an institution s 3D treatment planning process and the institution
Advanced Technology Consortium (ATC) Credentialing Procedures for 3D Conformal Therapy Protocols 3D CRT Benchmark* Purpose: To evaluate an institution s 3D treatment planning process and the institution
Clinical outcomes of patients with malignant lung lesions treated with stereotactic body radiation therapy (SBRT) in five fractions
 in five fractions") J Radiat Oncol (2012) 1:57 63 DOI 10.1007/s13566-012-0008-0 ORIGINAL RESEARCH Clinical outcomes of patients with malignant lung lesions treated with stereotactic body radiation therapy (SBRT) in five fractions
J Radiat Oncol (2012) 1:57 63 DOI 10.1007/s13566-012-0008-0 ORIGINAL RESEARCH Clinical outcomes of patients with malignant lung lesions treated with stereotactic body radiation therapy (SBRT) in five fractions
New Radiation Treatment Modalities in the Treatment of Lung Cancer
 New Radiation Treatment Modalities in the Treatment of Lung Cancer David Perry, M.D. Chief, Radiation Oncology Medical Director, CyberKnife Radiosurgery Center Medstar Franklin Square Medical Center Definitions
New Radiation Treatment Modalities in the Treatment of Lung Cancer David Perry, M.D. Chief, Radiation Oncology Medical Director, CyberKnife Radiosurgery Center Medstar Franklin Square Medical Center Definitions
Corporate Medical Policy
 Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Head and Neck File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_head_and_neck
Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Head and Neck File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_head_and_neck
RTTs role in lung SABR
 RTTs role in lung SABR Bart van Baaren Lineke van der Weide VU Medical Centre SBRT symposium VUMC 16 December 2017 Flow chart lung SABR Pre-treatment imaging Treatment planning On-line imaging Treatment
RTTs role in lung SABR Bart van Baaren Lineke van der Weide VU Medical Centre SBRT symposium VUMC 16 December 2017 Flow chart lung SABR Pre-treatment imaging Treatment planning On-line imaging Treatment
Image Registration for Radiation Therapy Applications: Part 2: In-room Volumetric Imaging
 Image Registration for Radiation Therapy Applications: Part 2: In-room Volumetric Imaging Peter Balter Ph.D University of Texas M.D. Anderson Cancer Center Houston, TX, USA Disclosure Information Peter
Image Registration for Radiation Therapy Applications: Part 2: In-room Volumetric Imaging Peter Balter Ph.D University of Texas M.D. Anderson Cancer Center Houston, TX, USA Disclosure Information Peter
1.1. LUNG CANCER AND RADIATION THERAPY
 TABLE OF CONTENTS 1. INTRODUCTION... 1 1.1. LUNG CANCER AND RADIATION THERAPY... 1 1.1.1. Radiation induced complications following radiation therapy in the lungs... 2 1.1.2. Atelectasis... 2 1.2. STEREOTACTIC
TABLE OF CONTENTS 1. INTRODUCTION... 1 1.1. LUNG CANCER AND RADIATION THERAPY... 1 1.1.1. Radiation induced complications following radiation therapy in the lungs... 2 1.1.2. Atelectasis... 2 1.2. STEREOTACTIC
The External Anatomy of the Lungs. Prof Oluwadiya KS
 The External Anatomy of the Lungs Prof Oluwadiya KS www.oluwadiya.com Introduction The lungs are the vital organs of respiration Their main function is to oxygenate the blood by bringing inspired air into
The External Anatomy of the Lungs Prof Oluwadiya KS www.oluwadiya.com Introduction The lungs are the vital organs of respiration Their main function is to oxygenate the blood by bringing inspired air into
1 : : Medical Physics, Città della Salute e della Scienza, Torino, Italy
 Fusella M. 1, Badellino S. 2, Boschetti A. 1, Cadoni F. 1, Giglioli F. R. 1, Guarneri A. 3, Fiandra C. 2, Filippi A. 2, Ricardi U. 2, Ragona R. 2 1 : : Medical Physics, Città della Salute e della Scienza,
Fusella M. 1, Badellino S. 2, Boschetti A. 1, Cadoni F. 1, Giglioli F. R. 1, Guarneri A. 3, Fiandra C. 2, Filippi A. 2, Ricardi U. 2, Ragona R. 2 1 : : Medical Physics, Città della Salute e della Scienza,
IAEA RTC. PET/CT and Planning of Radiation Therapy 20/08/2014. Sarajevo (Bosnia & Hercegovina) Tuesday, June :40-12:20 a.
 Tuesday, June :40-12:20 a.") IAEA RTC PET/CT and Planning of Radiation Therapy Sarajevo (Bosnia & Hercegovina) Tuesday, June 17 2014 11:40-12:20 a.m María José García Velloso Servicio de Medicina Nuclear Clínica Universidad de Navarra
IAEA RTC PET/CT and Planning of Radiation Therapy Sarajevo (Bosnia & Hercegovina) Tuesday, June 17 2014 11:40-12:20 a.m María José García Velloso Servicio de Medicina Nuclear Clínica Universidad de Navarra
Chest and cardiovascular
 Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
Dr. Weyrich G07: Superior and Posterior Mediastina. Reading: 1. Gray s Anatomy for Students, chapter 3
 Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Credentialing for the Use of IGRT in Clinical Trials
 Credentialing for the Use of IGRT in Clinical Trials James M. Galvin, DSc Thomas Jefferson University Hospital Jefferson Medical College Philadelphia, PA and The Radiation Therapy Oncology Group RADIATION
Credentialing for the Use of IGRT in Clinical Trials James M. Galvin, DSc Thomas Jefferson University Hospital Jefferson Medical College Philadelphia, PA and The Radiation Therapy Oncology Group RADIATION
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors
 for locally advanced pancreatic tumors") Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast
 1 Angela Kempen February Case Study February 22, 2012 3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast History of Present Illness: JE is a 45 year-old Caucasian female who underwent
1 Angela Kempen February Case Study February 22, 2012 3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast History of Present Illness: JE is a 45 year-old Caucasian female who underwent
Sectional Anatomy Quiz - III
 Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
The Effects of DIBH on Liver Dose during Right-Breast Treatments: A Case Study Abstract: Introduction: Case Description: Conclusion: Introduction
 1 The Effects of DIBH on Liver Dose during Right-Breast Treatments: A Case Study Megan E. Sullivan, B.S., R.T.(T)., Patrick A. Melby, B.S. Ashley Hunzeker, M.S., CMD, Nishele Lenards, M.S., CMD, R.T. (R)(T),
1 The Effects of DIBH on Liver Dose during Right-Breast Treatments: A Case Study Megan E. Sullivan, B.S., R.T.(T)., Patrick A. Melby, B.S. Ashley Hunzeker, M.S., CMD, Nishele Lenards, M.S., CMD, R.T. (R)(T),
Treatment Planning & IGRT Credentialing for NRG SBRT Trials
 Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
RPC Liver Phantom Highly Conformal Stereotactic Body Radiation Therapy
 RPC Liver Phantom Highly Conformal Stereotactic Body Radiation Therapy Guidelines for Planning and Irradiating the RPC Liver Phantom. Revised Dec 2005 Credentialing for this protocol requires four steps:
RPC Liver Phantom Highly Conformal Stereotactic Body Radiation Therapy Guidelines for Planning and Irradiating the RPC Liver Phantom. Revised Dec 2005 Credentialing for this protocol requires four steps:
Anatomy Lecture 8. In the previous lecture we talked about the lungs, and their surface anatomy:
 Anatomy Lecture 8 In the previous lecture we talked about the lungs, and their surface anatomy: 1-Apex:it lies 1 inch above the medial third of clavicle. 2-Anterior border: it starts from apex to the midpoint
Anatomy Lecture 8 In the previous lecture we talked about the lungs, and their surface anatomy: 1-Apex:it lies 1 inch above the medial third of clavicle. 2-Anterior border: it starts from apex to the midpoint
Variable Dose Rate Dynamic Conformal Arc Therapy (DCAT) for SABR Lung: From static fields to dynamic arcs using Monaco 5.10
 for SABR Lung: From static fields to dynamic arcs using Monaco 5.10") Variable Dose Rate Dynamic Conformal Arc Therapy (DCAT) for SABR Lung: From static fields to dynamic arcs using Monaco 5.10 Simon Goodall Radiation Oncology Physicist Genesis Care Western Australia Introduction
Variable Dose Rate Dynamic Conformal Arc Therapy (DCAT) for SABR Lung: From static fields to dynamic arcs using Monaco 5.10 Simon Goodall Radiation Oncology Physicist Genesis Care Western Australia Introduction
This is not a required assignment but it is recommended.
 SU 12 Name: This is not a required assignment but it is recommended. BIO 116 - Anatomy & Physiology II Practice Assignment 2 - The Respiratory and Cardiovascular Systems 1. The exchange of oxygen and carbon
SU 12 Name: This is not a required assignment but it is recommended. BIO 116 - Anatomy & Physiology II Practice Assignment 2 - The Respiratory and Cardiovascular Systems 1. The exchange of oxygen and carbon
THE GOOFY ANATOMIST QUIZZES
 THE GOOFY ANATOMIST QUIZZES 7. LUNGS Q1. Fill in the blanks: the lung has lobes and fissures. A. Right, three, two. B. Right, two, one. C. Left, three, two. D. Left, two, three. Q2. The base of the lung
THE GOOFY ANATOMIST QUIZZES 7. LUNGS Q1. Fill in the blanks: the lung has lobes and fissures. A. Right, three, two. B. Right, two, one. C. Left, three, two. D. Left, two, three. Q2. The base of the lung
Lung Spine Phantom. Guidelines for Planning and Irradiating the IROC Spine Phantom. MARCH 2014
 Lung Spine Phantom Guidelines for Planning and Irradiating the IROC Spine Phantom. MARCH 2014 The study groups are requesting that each institution keep the phantom for no more than 2 week. During this
Lung Spine Phantom Guidelines for Planning and Irradiating the IROC Spine Phantom. MARCH 2014 The study groups are requesting that each institution keep the phantom for no more than 2 week. During this
The Effects of DIBH on Liver Dose during Right-Breast Treatments Introduction
 1 The Effects of DIBH on Liver Dose during Right-Breast Treatments Megan E. Sullivan B.S.R.T.(T)., Patrick A. Melby, B.S. Ashley Hunzeker, M.S., CMD, Nishele Lenards, M.S., CMD Medical Dosimetry Program
1 The Effects of DIBH on Liver Dose during Right-Breast Treatments Megan E. Sullivan B.S.R.T.(T)., Patrick A. Melby, B.S. Ashley Hunzeker, M.S., CMD, Nishele Lenards, M.S., CMD Medical Dosimetry Program
slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments
 Done By : Rahmeh Alsukkar Date : 26 /10/2017 slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments Each segmental bronchus passes to a structurally
Done By : Rahmeh Alsukkar Date : 26 /10/2017 slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments Each segmental bronchus passes to a structurally
Right lung. -fissures:
 -Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
-Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
Efficient SIB-IMRT planning of head & neck patients with Pinnacle 3 -DMPO
 Investigations and research Efficient SIB-IMRT planning of head & neck patients with Pinnacle 3 -DMPO M. Kunze-Busch P. van Kollenburg Department of Radiation Oncology, Radboud University Nijmegen Medical
Investigations and research Efficient SIB-IMRT planning of head & neck patients with Pinnacle 3 -DMPO M. Kunze-Busch P. van Kollenburg Department of Radiation Oncology, Radboud University Nijmegen Medical
Protocol of Radiotherapy for Breast Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
Mediastinum and pericardium
 Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
A TREATMENT PLANNING STUDY COMPARING VMAT WITH 3D CONFORMAL RADIOTHERAPY FOR PROSTATE CANCER USING PINNACLE PLANNING SYSTEM *
 Romanian Reports in Physics, Vol. 66, No. 2, P. 394 400, 2014 A TREATMENT PLANNING STUDY COMPARING VMAT WITH 3D CONFORMAL RADIOTHERAPY FOR PROSTATE CANCER USING PINNACLE PLANNING SYSTEM * D. ADAM 1,2,
Romanian Reports in Physics, Vol. 66, No. 2, P. 394 400, 2014 A TREATMENT PLANNING STUDY COMPARING VMAT WITH 3D CONFORMAL RADIOTHERAPY FOR PROSTATE CANCER USING PINNACLE PLANNING SYSTEM * D. ADAM 1,2,
Josh Howard CMD Upendra Parvathaneni MBBS, FRANZCR
 Anatomic and Dosimetric Correlation in the Treatment of Advanced Larynx Cancer- When is the Brachial Plexus at Risk? Josh Howard CMD Upendra Parvathaneni MBBS, FRANZCR AAMD 39th Annual Meeting - Seattle
Anatomic and Dosimetric Correlation in the Treatment of Advanced Larynx Cancer- When is the Brachial Plexus at Risk? Josh Howard CMD Upendra Parvathaneni MBBS, FRANZCR AAMD 39th Annual Meeting - Seattle
Automated Plan Quality Check with Scripting. Rajesh Gutti, Ph.D. Clinical Medical Physicist
 Automated Plan Quality Check with Scripting Rajesh Gutti, Ph.D. Clinical Medical Physicist Veera.Gutti@BSWHealth.org Outline Introduction - BSW Automation in Treatment planning Eclipse Scripting API Script
Automated Plan Quality Check with Scripting Rajesh Gutti, Ph.D. Clinical Medical Physicist Veera.Gutti@BSWHealth.org Outline Introduction - BSW Automation in Treatment planning Eclipse Scripting API Script