Novita da EHA 2016 Copenhagen Linfomi
|
|
|
- Buddy Esmond Young
- 5 years ago
- Views:
Transcription
1 Firenze, 16th September 2016 Marco Ladetto MD, Az Osp Santi Antonio e Biagio e Cesare Arrigo, Alessandria, Italy EU Novita da EHA 2016 Copenhagen Linfomi
2 THREE QUESTIONS TO ADDRESS: 1. Is ASCT still the golden standard for MCL? And how to challenge it in the future? 2. What is new in relapsed follicular lymphoma? Is benda-obinotuzumab a major step forward? Which are the alternatives? 3. Ultra high-risk lymphoma patients: Can we identify them? And where shall we go for treatment?
3 THREE QUESTIONS TO ADDRESS: 1. Is ASCT still the golden standard for MCL? And how to challenge it in the future? 2. What is new in relapsed follicular lymphoma? Is benda-obinotuzumab a major step forward? Which are the alternatives? 3. Ultra high-risk lymphoma patients: Can we identify them? And where shall we go for treatment?


4
5 MCL Educational session Points raised by prof E Zucca in the educational session EHA2016 Copenhagen 1. Watch and wait? 2. Prognosticators and prognostic models 3. Role of MRD 4. Role of PET
6 MCL Educational session Conclusions from prof T. Robak in the educational session EHA2016 Copenhagen 1. Heterogeneity and personalization 2. OS is improving 3. Target drugs are effective in the R/R setting 4. Auto ASCT and allo-sct should be considered also at relapse



7 Haematologica, 2016
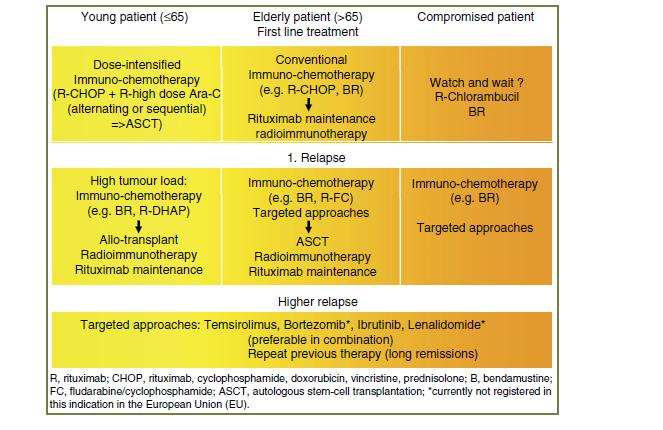
8 YOUNG PATIENTS PROBABLY NOT DESERVING ASCT Patients with major comorbidities Patients with limited stage MCL Indolent MCL Primary refractory patients For specific prognostic subgroups.

9 Adapted from Dreyling M and Ferrero S, 2016
10 MRD response after induction 100% RR 86% CR 34% Elderly 78% 90% 40% 25% Younger 94% 38% 20 80% % 40% % % R-CHOP R-FC R-CHOP MRD- MRD+ R-CHOP/ R-DHAP Courtesy of Christiane Pott
11 Eskeund CW S YEAR FOLLOW-UP OF THE NORDIC MCL2-TRIAL: DESPITE LONG-TERM RESPONSES LATE RELAPSES STILL OCCUR BACKGROUND Outcome of MCL has has improved thanks to Ara-C and R the Nordic trial showed a projected 10-year OS and PFS of 58% and 43% Updated results at a median follow-up of 11.4 years METHODS 160 untreated stage II-IV MCL pts. maxi-chop alternated to high-dose Ara-C, BEAM/BEAC and ASCT in responders (n=145). Use of pre-emptive rituximab (Andersen, JCO, 2009) RESULTS the median OS and PFS were 12.7 and 8.5 years. RD of the 145 patients who underwent ASCT was 12.4 years micro-rna-18b (MIPI-B-miR) remains highly significant and identifies a high-risk group of an exceedingly poor prognosis with OS and PFS of only 1.6 and 1.0 years
12 CONCLUSIONS a pattern of continuing relapse is observed, seemingly precluding cure. MIPI, MIPI-B and, in particular, MIPI-B-miR remain valid prognosticators that clearly separate patients into risk groups with different outcomes. All risk groups might benefit from addition of novel agents.
13 Rule S et al S438 OS OUTCOMES IN PTS WITH MCL TREATED WITH IBRUTINIB IN A POOLED ANALYSIS OF 370 PATIENTS FROM 3 INTERNATIONAL OPEN-LABEL STUDIES BACKGROUND pooled analysis from 3 ibrutinib studies (PCYC-1104, MCL2001 [SPARK] and MCL3001 [RAY]) METHODS ibrutinib 560 mg orally Inclusion and exclusion criteria were similar Simple descriptive statistics and exploratory analyses were done for PFS and OS with univariate and multivariate analyses RESULTS 370 patients were included in this analysis; median age was 67.5 years, 94%. 27%, 29%, 22% had 1, 2, 3 prior lines of therapy. Overall response rate (ORR) was 66% (20% CR; 46% PR), ORR for patients with 1, 2 and 3 prior lines of therapy was 77%, 71% and 64% DOR, PFS and OS of 18.6, 12.8 and 25.0 months, CR pts, had a PFS of 70% and OS of 90% at 2 years. ECOG, smipi, bulky disease and blastoid histology impacts OS
14 CONCLUSIONS OS is better patients who are younger and who have fewer prior lines of therapy Ibrutinib is an effective agent in blastoid MCL to achieve a response and potentially provide a bridge transplant. Data support the preferential use of ibrutinib after initial vs later relapse
15 Rule S et al P699 REAL-WORLD EXPERIENCE OF IBRUTINIB IN >700 PATIENTS WITH MANTLE-CELL LYMPHOMA: DATA FROM A GLOBAL NAMED PATIENT PROGRAM NPP program to allow access to ibrutinib for eligible patients R/E MCL This program provides real-world data on estimated outcomes with ibrutinib across a large, global MCL population.
16 Lenz G et al S439 SEQUENCE VARIANTS IN PATIENTS WITH PRIMARY AND ACQUIRED RESISTANCE TO IBRUTINIB IN THE PHASE 3 MCL3001 (RAY) TRIAL BACKGROUND To identify specific mechanisms of ibrutinib resistance in MCL, and to correlate genetic signatures with patient response. METHODS Primary resistance analysis, Acquired resistance analysis. RESULTS Mutations associated with primary resistance to ibrutinib were identified in NF-kB signaling pathways, both canonical (e.g., A20) and non-canonical (e.g., BIRC2). Other mutations were found in epigenetic modifiers and in the EGFR family. Acquired resistence: Mutations in epigenetic modifiers and alternate NF-kB or PI3K/mTOR pathways were found after a short treatment duration (<4 months). No primary or secondary BTK C481S mutations CONCLUSIONS Understanding both primary and acquired resistance patterns is key in order to improve outcomes and define the populations that benefit from ibrutinib treatment
17 THREE QUESTIONS TO ADDRESS: 1. Is ASCT still the golden standard for MCL? And how to challenge it in the future? 2. What is new in relapsed follicular lymphoma? Is benda-obinotuzumab a major step forward? Which are the alternatives? 3. Ultra high-risk lymphoma patients: Can we identify them? And where shall we go for treatment?

18 THE GADOLIN TRIAL Sehn L et al, Lancet 2016
19
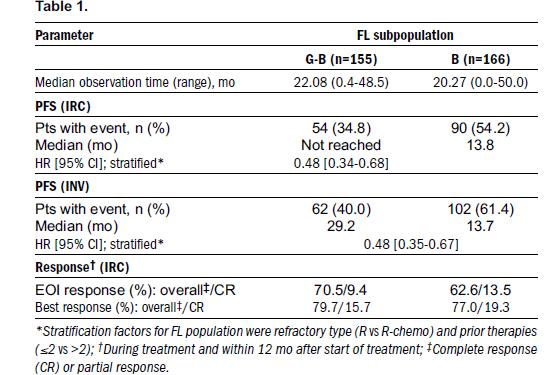
20 Trneny M et al S440 OBINUTUZUMAB PLUS BENDAMUSTINE VERSUS BENDAMUSTINE ALONE IN PATIENTS WITH RITUXIMAB-REFRACTORY FOLLICULAR LYMPHOMA: RESULTS FROM THE GADOLIN STUDY BACKGROUND FL subset analysis of GADOLIN pts. 321 (81%) of 396 inhl pts enrolled had FL. METHODS Pts received either G + B90 or B120 RESULTS Median number of prior therapies was 2. 94% pts were refractory to their last prior rituximab (R)-containing regimen and 88% double-refractory to R and an alkylating agent. According to IRC PFS is not reached in the G-B arm and 13.8 mo in the B arm (Figure 1), Survival data were immature at the time of analysis. Safety profiles were comparable.
21
22 Jiménez Ubieto A et al S441 ANALYSIS OF SECONDARY NEOPLASIAS AFTER HIGH DOSE THERAPY SUPPORTED BY AUTOLOGOUS STEM CELL TRANSPLANTATION IN FOLICULAR LYMPHOMA PATIENTS. A LONG TERM FOLLOW-UP ANALYSIS FROM THE GELTAMO REGISTRY. BACKGROUND HDT/ASCTis effective in FL Secondary neoplasia is one the major cncern To evaluate the cumulative incidence and characteristics of smds/saml and solid tumors after HDT/ASCT in a very long-term follow-up analysis of FL patients. METHODS A total of 655 FL patients (GELTAMO registry) RESULTS Median follow-up 12 years. The median OS were 21.3 years from HDT/ASCT and 22.6 years from the time of FL diagnosis. 12.5% developed a second malignancy: solid tumors (47.5%), smds/saml (42.5%). The accumulated incidence at 5, 10 and 15 years was 1.8%, 3.5% and 4.9% for solid tumors and 2.6%, 4.3% and 5% for smds/saml. Male sex and BM as stem cell source were associated to an increased risk.

23 the incidence of secondary neoplasia will probably not diminish the benefit of HDT/ASCT in relapsed FL. CONCLUSIONS FL pts are at an increased risk of second malignancy but not as high as reported. Low percentage of TBI and early transplant could explain these good results. Once a secondary neoplasia is diagnosed prognosis is dismal.
24 Hatake et al P686 INTERIM ANALYSIS OF POST MARKETING SURVEILLANCE OF YTTRIUM-90 IBRITUMOMAB TIUXETAN IN JAPANESE PATIENTS WITH RELAPSED OR REFRACTORY INDOLENT B-CELL NON-HODGKIN LYMPHOMA OR MANTLE CELL LYMPHOMA. RESULTS 413 pts enrolled. Good safety confirmed. ORR in 354 evaluable pts was 76.8%, CR rate 47.7%. ORR and CR for those receiving 2 or less prior regimens were 86.0% and 56.1% respectively, while ORR and CR for those receiving more than 2 prior regimens were 69.3% and 40.7% CONCLUSIONS 90YITis a tolerable and efficacious treatment option for pts with R/R B-cell NHL or MCL in Japan, It demonstrates good benefit-risk balance
25 Li JJ et al P317 IDELALISIB MONOTHERAPY IN RELAPSED/REFRACTORY FOLLICULAR LYMPHOMA (FL): EXPERIENCE THROUGH AN EARLY ACCESS PROGRAM IN EUROPE AND AUSTRALIA RESULTS Results: 66 pts with refractory FL who had documented prior treatment regimens. A total of 12 pts (20%) ASCT. With a median follow up of 109 days IDELA monotherapy was well-tolerated with 6/66 pts (9.1%) reporting an SAE. (Febrile neutropenia, neutropenia, diarrhea, gastrointestinal inflammatory disorder, pancytopenia, progressive disease, liver enzyme elevation, hypotension and colon cancer). CONCLUSIONS: The results confirm the acceptable tolerability profile of IDELA.
26 THREE QUESTIONS TO ADDRESS: 1. Is ASCT still the golden standard for MCL? And how to challenge it in the future? 2. What is new in relapsed follicular lymphoma? Is benda-obinotuzumab a major step forward? Which are the alternatives? 3. Ultra high-risk lymphoma patients: Can we identify them? And where shall we go for treatment?
27 Casasnovas O et al S105 BASELINE TOTAL METABOLIC VOLUME (TMTV) PREDICTS THE OUTCOME OF PATIENTS WITH ADVANCED HODGKIN LYMPHOMA (HL) ENROLLED IN THE AHL2011 LYSA TRIAL. BACKGROUND The TMTV assessed on the baseline FDG-PET assessed prospectively in pts enrolled in a phase III randomized trial (PET-driven) RESULTS follow-up of 16 months, 2y-PFS was 81% vs 93% in pts with high and low TMTV Using also PET-2 3 groups could be identified having a 61%, 88%, 94% 2y-PFS respectively (p<0.0001). CONCLUSIONS The TMTV predicts the outcome of young advanced HL pts. The combination of TMTV and PET2 allows identifying 3 subsets of HL pts
28 Stewart D et al S479 A BIOCLINICAL PROGNOSTIC MODEL INCORPORATING MYC AND BCL2 PREDICTS OUTCOME TO SALVAGE THERAPY IN RELAPSED/ REFRACTORY DIFFUSE LARGE B-CELL LYMPHOMA: AN NCIC CTG LY12 CORRELATIVE SCIENCE STUDY. BACKGROUND To determine clinical and molecular predictors of EFS and OS for rrdlbcl pts treated with R-GDP or R-DHAP followed by ASCT (Canadian Ly12 study) METHODS 91 pts had DLBCL immunohistochemical (IHC) testing for CD10, BCL6, MUM1, FOXP1, LMO2, BCL2, CMYC, P53, pystat3 expression. In addition, 97 formalin-fixed, had GEP with NanoString to evaluate Cell of Origin (COO) by the Lymph2Cx assay, as well as BCL2, MYC, P53, STAT3, PDL1 and PD1 expression. RESULTS Expression of both MYC and BCL2 was associated to poor outcome. Dual expressing (DE) lymphomas (MYC+/BCL+) had significantly worse 3y EFS (0% vs 40%, p=0.0009) and OS rates (20% vs 54%, p=0.0004)
29 Stewart D et al S479 A BIOCLINICAL PROGNOSTIC MODEL INCORPORATING MYC AND BCL2 PREDICTS OUTCOME TO SALVAGE THERAPY IN RELAPSED/ REFRACTORY DIFFUSE LARGE B-CELL LYMPHOMA: AN NCIC CTG LY12 CORRELATIVE SCIENCE STUDY. MYC and BCL2 expression using NanoString GEP (>1.5xmean) were significantly associated with inferior OS and EFS, and no patient who expressed both markers achieved 2y EFS or OS. Concordance rate of 79% was seen for MYC and 57% for BCL2. In multivariate analyses, primary refractory DLBCL, LDH at relapse, MYC expression and BCL2 expression (assessed by either IHC or GEP). CONCLUSIONS MYC and BCL2 expression, determined by IHC or Nanostring GEP, are independent poor prognostic factors for rrdlbcl, and dual expression predicts dismal prognosis.
30 Tchernonog E et al S788 CLINICAL CHARACTERISTICS AND PROGNOSTIC FACTORS OF IMMUNOCOMPROMISED AND NON IMMUNOCOMPROMISED PLASMABLASTIC LYMPHOMA PATIENTS: ANALYSIS OF 135 PATIENTS TREATED IN THE LYSA GROUP. BACKGROUND PBL remains a diagnostic and therapeutic challenge with an aggressive clinical course. Aim of this study was to specify the clinical, biological, pathological features and outcome of patients with PBL. METHODS AND RESULTS 135 patients with PBL diagnosed after 2000 within LYSA. The median age was 58, male predominance. 56 HIV-positive patients, 17 post-transplant patients, and 62 immunocompetent. However also this subtype of patients may present some degree of immunodepression. Immunophenotype showed CD138 positivity in 88% of cases and CD20 negativity in 90% of cases. EBER expression was observed in 62% of cases. Chemotherapy was administered to 108 of 135 patients, with a complete response rate of 55%. Rituximab, had a trend towards improved CR rate. The median overall survival was 32 mos. HIV positive status showed better overall survival. DISCUSSION Specific guidelines to clarify all the treatment options are lacking
31 Festuccia M et al 796 ALLOGENEIC STEM CELL TRANSPLANTATION AND BRENTUXIMAB VEDOTIN IN RELAPSED/REFRACTORY HODGKIN LYMPHOMA: A MULTICENTER EXPERIENCE BACKGROUND allo-hct has been used in RR HL with controversial results. Aim of our study is to investigate the role of allo-hct in RR HL METHODS 69 patients with RR HL, median age 34 (range, 18-64), 52 patients (75%) were at least in PR. The remaining 16 patients (23%) had progressive disease (non-responsive). Brentuximab Vedotin (BV) was given as bridge to transplant in 11 patients. Moreover, 7 patients received BV after allo-hct. The majority of patients underwent reduced intensity allo-hct, 64 patients (93%). MUD in 57%. The stem cells source was PB in 61 patients (88%).
32 RESULTS Median OS of 5.1 years (range, ) and RFS of, 1.3 years. The 5-year cumulative incidence of treatment related mortality (TRM) and relapse were 17.7% and 43.4%, respectively. The 5-year estimated of RFS was significantly higher in responsive compared to nonresponsive patients, 46.9% versus 12.5%, respectively, p= Eleven patients received BV as bridge to allo-hct for a median of 6 cycles.. All patients achieved at least PR. None of patients treated with BV had unexpected toxicity or GVHD worsening. DISCUSSION Allo-HCT is a feasible and effective option for RR HL. BV showed efficacy as a bridge to allo- HCT as well as post allo-hct rescue.


33 CHALLENGING HIGH-RISK PATIENTS TRADITIONAL BACKBONE TREATMENT Poor diagnostic profile Failure to achieve MRD/PET negativity or MRD loss Innovative or potentiated treatment
34











35 TRIANGLE study Flow chart
36 FLAZ-12: STUDY DESIGN MRD 3 R-CHEMO REGIMENS (R-CHOP, R-DHAP, R-FM, R-ICE, R-IEV, R-B) MRD CR-PR SD-PD BLIND RANDOMIZATION Pts stratified based on Center characteristics and response ARA-C 2g/sqm b.i.d. 2 days with Rituximab in vivo purging PBSC harvest MRD Randomization unblinding Arm A consolidation with RIT MRD Arm B: consolidation with ASCT Rituximab maintenance every three months for 8 courses (starting three months after consolidation) Rituximab maintenance every three months for 8 courses (starting three months after consolidation) At relapse MRD At relapse ASCT With Previously collected PBSC Any salvage treatment


 (24 cycles) R alone Rituximab 375 mg/m2 day 1 q 90 days")
37 FIL protocols in relapsed FL: Renoir RELAPSED/REFRACTORY FOLLICULAR LYMPHOMA NEED TO THERAPY R-Bendamustine x 4 once a month Rituximab 375 mg/m 2 day 2 day 0 or 0 1 or (day 1 (day 8 on 8 cycle on cycle 1) 1) Bendamustine mg/m mg/m 2 iv 2 days iv days CR/PR Random NR OFF R2 Rituximab 375 mg/m2 day 1 q 90 days (8 cycles) Lenalidomide (10 mg dd 1-21 q 28) (24 cycles) R alone Rituximab 375 mg/m2 day 1 q 90 days (8 cycles)
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Aggressive lymphomas ASH Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV
 Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients
 Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
Lymphoma- Med A-new drugs and treatments
 Lymphoma- Med A-new drugs and treatments Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Disclosures: Roche, Gilead Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Outline Lymphoma- what is
Lymphoma- Med A-new drugs and treatments Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Disclosures: Roche, Gilead Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Outline Lymphoma- what is
Mantle cell lymphoma An update on management
 Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Diffuse Large B-Cell Lymphoma (DLBCL)
") Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
GLSG/OSHO Study Group. Supported by Deutsche Krebshilfe
 GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
Mantle Cell Lymphoma: Update in Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency
 Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
What are the hurdles to using cell of origin in classification to treat DLBCL?
 What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University
 Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
MANTLE CELL LYMPHOMA
 MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma
 How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
Management of high-risk diffuse large B cell lymphoma: case presentation
 Management of high-risk diffuse large B cell lymphoma: case presentation Daniel J. Landsburg, MD Assistant Professor of Clinical Medicine Perelman School of Medicine University of Pennsylvania January
Management of high-risk diffuse large B cell lymphoma: case presentation Daniel J. Landsburg, MD Assistant Professor of Clinical Medicine Perelman School of Medicine University of Pennsylvania January
Treatment Nodal Marginal Zone Lymphoma
 Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Aggressive B and T cell lymphomas: Treatment paradigms in 2018
 Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate
Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate
POST ICML Indolent lymphomas relapse treatment
 POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting?
 Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
SEQUENCING FOLLICULAR LYMPHOMA
 SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL
 Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège. 14 th post-ash meeting, January 6 th 2011, Brussels
 Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Follicular Lymphoma 2016:
 Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
A CME-certified Oncology Exchange Program
 A CME-certified Oncology Exchange Program Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Seattle Genetics, Inc. Re-treatment with BV Bartlett
A CME-certified Oncology Exchange Program Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Seattle Genetics, Inc. Re-treatment with BV Bartlett
Dr Claire Burney, Lymphoma Clinical Fellow, Bristol Haematology and Oncology Centre, UK
 EMBT LWP 2017-R-05 Research Protocol: Outcomes of patients treated with Ibrutinib post autologous stem cell transplant for mantle cell lymphoma. A retrospective analysis of the LWP-EBMT registry. Principle
EMBT LWP 2017-R-05 Research Protocol: Outcomes of patients treated with Ibrutinib post autologous stem cell transplant for mantle cell lymphoma. A retrospective analysis of the LWP-EBMT registry. Principle
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA
 Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Targeted Radioimmunotherapy for Lymphoma
 Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
State of the Art Treatment for Relapsed Mantle Cell Lymphoma
 Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin
 What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
Bendamustine for Hodgkin lymphoma. Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service
 Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Front-line treatment in young. Role of maintenance therapy. Rome 2017 Prof Le Gouill S.
 Front-line treatment in young patients with MCL: Role of maintenance therapy Rome 2017 Prof Le Gouill S. Is there a need for maintenance for young MCL patients? Is there a need for maintenance for young
Front-line treatment in young patients with MCL: Role of maintenance therapy Rome 2017 Prof Le Gouill S. Is there a need for maintenance for young MCL patients? Is there a need for maintenance for young
Bendamustine: A Transversal * Chemotherapy Agent
 Bendamustine: A Transversal * Chemotherapy Agent Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, D.C., USA *Def Cutting across two lines, intersecting
Bendamustine: A Transversal * Chemotherapy Agent Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, D.C., USA *Def Cutting across two lines, intersecting
Obinutuzumab in combination with bendamustine for treating rituximab-refractory follicular lymphoma
 Obinutuzumab in combination with bendamustine for treating rituximab-refractory follicular lymphoma 1 st Appraisal Committee meeting Background and Clinical Effectiveness Committee A Lead team John Watkins
Obinutuzumab in combination with bendamustine for treating rituximab-refractory follicular lymphoma 1 st Appraisal Committee meeting Background and Clinical Effectiveness Committee A Lead team John Watkins
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Jonathan W Friedberg, MD, MMSc
 I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents
 Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
Post-ESMO Berne
 Post-ESMO Berne 23.10.2015 Lymphoma Update Panagiotis Samaras Department of Oncology Hemato-Oncology Center University Hospital Zurich Diffuse Large B-Cell Lymphoma (DLBCL) PCNSL Hodgkin s Lymphoma Mantle
Post-ESMO Berne 23.10.2015 Lymphoma Update Panagiotis Samaras Department of Oncology Hemato-Oncology Center University Hospital Zurich Diffuse Large B-Cell Lymphoma (DLBCL) PCNSL Hodgkin s Lymphoma Mantle
Firenze, settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo
 Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
Open questions in the treatment of Follicular Lymphoma. Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland
 Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
MMAE disrupts cell division and triggers apoptosis. Pola binds to cell surface antigen CD79b. Pola is internalized; linker cleaves, releasing MMAE
 Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Diffuse Large B-Cell Lymphoma Front line Therapy John P. Leonard, MD Weill Cornell Medicine New York, New York USA
 Diffuse Large B-Cell Lymphoma Front line Therapy John P. Leonard, MD Weill Cornell Medicine New York, New York USA Disclosures Consulting advice: Hospira, Bayer, Juno Therapeutics, Teva, Oncotracker, Gilead
Diffuse Large B-Cell Lymphoma Front line Therapy John P. Leonard, MD Weill Cornell Medicine New York, New York USA Disclosures Consulting advice: Hospira, Bayer, Juno Therapeutics, Teva, Oncotracker, Gilead
Immune checkpoint inhibitors in lymphoma. Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust
 Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
The treatment of DLBCL. Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona
 The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
R/R DLBCL Treatment Landscape
 An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
Mathias J Rummel, MD, PhD
 I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
Linfoma de Hodgkin. Novos medicamentos. Otavio Baiocchi CRM-SP
 Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth
 Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth") VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
Highlights of ICML 2015
 Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
The case for maintenance rituximab in FL
 New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
Challenges in the Treatment of Follicular Lymphoma
 Challenges in the Treatment of Follicular Lymphoma Prof. Michele Ghielmini Clinical Director Oncology Institute of Southern Switzerland Bellinzona ESMO guidelines 2014 (simplified) Low tumor burden High
Challenges in the Treatment of Follicular Lymphoma Prof. Michele Ghielmini Clinical Director Oncology Institute of Southern Switzerland Bellinzona ESMO guidelines 2014 (simplified) Low tumor burden High
MCL comprises less than 10% of all cases of non-hodgkin
 COHEN, ZAIN, AND KAHL Current Approaches to Mantle Cell Lymphoma: Diagnosis, Prognosis, and Therapies Jonathon B. Cohen, MD, Jasmine M. Zain, MD, and Brad S. Kahl, MD OVERVIEW Mantle cell lymphoma (MCL)
COHEN, ZAIN, AND KAHL Current Approaches to Mantle Cell Lymphoma: Diagnosis, Prognosis, and Therapies Jonathon B. Cohen, MD, Jasmine M. Zain, MD, and Brad S. Kahl, MD OVERVIEW Mantle cell lymphoma (MCL)
Treatment Landscape in R/R DLBCL Novel Targets and Strategies. Wyndham H. Wilson, M.D., Ph.D. Senior Investigator
 Treatment Landscape in R/R DLBCL Novel Targets and Strategies Wyndham H. Wilson, M.D., Ph.D. Senior Investigator Gene-expression profiling of DLBCL subtypes Roschewski, M. et al. (2013) Nat. Rev. Clin.
Treatment Landscape in R/R DLBCL Novel Targets and Strategies Wyndham H. Wilson, M.D., Ph.D. Senior Investigator Gene-expression profiling of DLBCL subtypes Roschewski, M. et al. (2013) Nat. Rev. Clin.
CME Information. Y-ibritumomab tiuxetan to that of rituximab maintenance for patients with newly diagnosed follicular lymphoma (FL).
.") CME Information LEARNING OBJECTIVES Compare the efficacy of consolidation therapy with a single dose of 90 Y-ibritumomab tiuxetan to that of rituximab maintenance for patients with newly diagnosed follicular
CME Information LEARNING OBJECTIVES Compare the efficacy of consolidation therapy with a single dose of 90 Y-ibritumomab tiuxetan to that of rituximab maintenance for patients with newly diagnosed follicular
Brentuximab, Nivolumab: L esperienza Real Word della REP. Dr.ssa Clara De Risi Az. Osp. Card. G. Panico - Tricase
 Brentuximab, Nivolumab: L esperienza Real Word della REP Dr.ssa Clara De Risi Az. Osp. Card. G. Panico - Tricase MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY IMPROVE
Brentuximab, Nivolumab: L esperienza Real Word della REP Dr.ssa Clara De Risi Az. Osp. Card. G. Panico - Tricase MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY IMPROVE
Brad S Kahl, MD. Tracks 1-21
 I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
New developments in the treatment of FL. Massimo Federico University of Modena and Reggio Emilia Italy
 New developments in the treatment of FL Massimo Federico University of Modena and Reggio Emilia Italy Common Questions Asked by The Patient I would like to know what is the best therapeutic option and
New developments in the treatment of FL Massimo Federico University of Modena and Reggio Emilia Italy Common Questions Asked by The Patient I would like to know what is the best therapeutic option and
OSCO/OU ASH-SABC Review. Lymphoma Update. Mohamad Cherry, MD
 OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
International Conference on Malignant Lymphoma (ICML) June 14-17, 2017
 June 14-17, 2017") International Conference on Malignant Lymphoma (ICML) June 14-17, 2017 INTERIM REPORT FROM A PHASE 2 MULTICENTER STUDY OF TAZEMETOSTAT, AN EZH2 INHIBITOR: CLINICAL ACTIVITY AND FAVORABLE SAFETY IN PATIENTS
International Conference on Malignant Lymphoma (ICML) June 14-17, 2017 INTERIM REPORT FROM A PHASE 2 MULTICENTER STUDY OF TAZEMETOSTAT, AN EZH2 INHIBITOR: CLINICAL ACTIVITY AND FAVORABLE SAFETY IN PATIENTS
Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center
 Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Today, how many PTCL patients are cured? Some but not as many
Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Today, how many PTCL patients are cured? Some but not as many
The case against maintenance rituximab in Follicular lymphoma. Jonathan W. Friedberg M.D., M.M.Sc.
 The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
Confronto Real world e studi registrativi
 Confronto Real world e studi registrativi V. Pavone San Giovanni Rotondo 8 Novembre 2018 U.O Ematologia Az.Osp.Card.G.Panico MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY
Confronto Real world e studi registrativi V. Pavone San Giovanni Rotondo 8 Novembre 2018 U.O Ematologia Az.Osp.Card.G.Panico MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY
Linfoma mantellare: terapia del paziente anziano. Francesco Zaja Trieste
 Linfoma mantellare: terapia del paziente anziano Francesco Zaja Trieste Dramatic demographic changes Increasing proportion of elderly persons In 2015 19% of the population in the European Union were 65
Linfoma mantellare: terapia del paziente anziano Francesco Zaja Trieste Dramatic demographic changes Increasing proportion of elderly persons In 2015 19% of the population in the European Union were 65
MARIO PETRINI Ematologia PISA UO Ematologia - Pisa
 I LINFOMI NON HODGKIN A BASSO GRADO DI MALIGNITA PESCARA 2008 linfomi mantellari MARIO PETRINI Ematologia PISA Mantle Cell Lymphoma Typical (Classic) small to medium-sized Ly with scanty cytoplasm, irregular
I LINFOMI NON HODGKIN A BASSO GRADO DI MALIGNITA PESCARA 2008 linfomi mantellari MARIO PETRINI Ematologia PISA Mantle Cell Lymphoma Typical (Classic) small to medium-sized Ly with scanty cytoplasm, irregular
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes
 Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
BENDAMUSTINE + RITUXIMAB IN CLL
 BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
AGRESSIVE LYMPHOMAS - FUTURE. Dr Stéphane Doucet CHUM
 AGRESSIVE LYMPHOMAS - FUTURE Dr Stéphane Doucet CHUM What are clinical trials? Clinical trials are carefully planned research studies where the most-promising discoveries and results from laboratory studies
AGRESSIVE LYMPHOMAS - FUTURE Dr Stéphane Doucet CHUM What are clinical trials? Clinical trials are carefully planned research studies where the most-promising discoveries and results from laboratory studies
Emerging targeted therapies for follicular lymphoma A future without chemotherapy
 Emerging targeted therapies for follicular lymphoma A future without chemotherapy Pier Luigi Zinzani Institute of Hematology L. e A. Seràgnoli University of Bologna FOLLICULAR LYMPHOMA: GENERAL ASPECTS
Emerging targeted therapies for follicular lymphoma A future without chemotherapy Pier Luigi Zinzani Institute of Hematology L. e A. Seràgnoli University of Bologna FOLLICULAR LYMPHOMA: GENERAL ASPECTS
Options in Mantle Cell Lymphoma Therapy
 Options in Mantle Cell Lymphoma Therapy Carlo Visco, MD Dept of Cell Therapy and Hematology San Bortolo Hospital, Vicenza, taly My Disclosures: ADVSOR OR ADVSORY BOARDS: Lundbeck Canada nc, Celgene Europe,
Options in Mantle Cell Lymphoma Therapy Carlo Visco, MD Dept of Cell Therapy and Hematology San Bortolo Hospital, Vicenza, taly My Disclosures: ADVSOR OR ADVSORY BOARDS: Lundbeck Canada nc, Celgene Europe,
Genomics in diffuse large B cell lymphoma (DLBCL) not as useful as we thought. OR IS IT?
 not as useful as we thought. OR IS IT?") Genomics in diffuse large B cell lymphoma (DLBCL) not as useful as we thought. OR IS IT? Matt McKinney MD Instructor in Medicine, Division of Hematologic Malignancies, Department of Medicine Duke University
Genomics in diffuse large B cell lymphoma (DLBCL) not as useful as we thought. OR IS IT? Matt McKinney MD Instructor in Medicine, Division of Hematologic Malignancies, Department of Medicine Duke University
Angioimmunoblastic T-cell lymphoma: nobody knows what to do...
 Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
MANTLE CELL LYMPHOMA MTOR-INHIBITION
 MANTLE CELL LYMPHOMA MTOR-INHIBITION Rome, 23. March 2017 Prof. Dr. med. Georg Heß III. Med. Klinik Universitäres Centrum für Tumorerkrankungen Universitätsmedizin der Johannes Gutenberg-Universität Mainz
MANTLE CELL LYMPHOMA MTOR-INHIBITION Rome, 23. March 2017 Prof. Dr. med. Georg Heß III. Med. Klinik Universitäres Centrum für Tumorerkrankungen Universitätsmedizin der Johannes Gutenberg-Universität Mainz
Simposio COSA È CAMBIATO NELL APPROCCIO TERAPEUTICO DEI LINFOMI NON HODGKIN DEL PAZIENTE ANZIANO?
 58 Congresso Nazionale Società Italiana di Gerontologia e Geriatria Torino 27-30 novembre 2013 Simposio COSA È CAMBIATO NELL APPROCCIO TERAPEUTICO DEI LINFOMI NON HODGKIN DEL PAZIENTE ANZIANO? C è un ruolo
58 Congresso Nazionale Società Italiana di Gerontologia e Geriatria Torino 27-30 novembre 2013 Simposio COSA È CAMBIATO NELL APPROCCIO TERAPEUTICO DEI LINFOMI NON HODGKIN DEL PAZIENTE ANZIANO? C è un ruolo
UBS European Conference 2013
 UBS European Conference 2013 Tuesday, 12 November 2013 Karl Mahler, Head of Investor Relations Stefan Frings, Oncology/Immunology Therapeutic Area Head,Roche Partnering Group: Continued strong sales growth
UBS European Conference 2013 Tuesday, 12 November 2013 Karl Mahler, Head of Investor Relations Stefan Frings, Oncology/Immunology Therapeutic Area Head,Roche Partnering Group: Continued strong sales growth
LYSA PET adapted programs. O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France
 LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
FCR and BR: When to use, how to use?
 FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
Relapsed/Refractory Diffuse Large B-Cell Lymphoma John Kuruvilla, MD Princess Margaret Cancer Centre University of Toronto
 Relapsed/Refractory Diffuse Large B-Cell Lymphoma John Kuruvilla, MD Princess Margaret Cancer Centre University of Toronto Disclosures Research Support Employee Leukemia and Lymphoma Society US, Rasch
Relapsed/Refractory Diffuse Large B-Cell Lymphoma John Kuruvilla, MD Princess Margaret Cancer Centre University of Toronto Disclosures Research Support Employee Leukemia and Lymphoma Society US, Rasch
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES
 How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma
 12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma
 Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
What is the best approach to the initial therapy of PTCL? standards of treatment? Should all
 What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
Highlights in chronic lymphocytic leukemia
 Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
MEETING SUMMARY ASH 2018, San Diego, USA
 MEETING SUMMARY ASH 2018, San Diego, USA Prof. Stefano Luminari University of Modena and Reggio Emilia, Italy AN UPDATE ON PROGNOSTIC FACTORS IN INDOLENT LYMPHOMAS 2 DISCLAIMER Please note: The views expressed
MEETING SUMMARY ASH 2018, San Diego, USA Prof. Stefano Luminari University of Modena and Reggio Emilia, Italy AN UPDATE ON PROGNOSTIC FACTORS IN INDOLENT LYMPHOMAS 2 DISCLAIMER Please note: The views expressed
Updates in the Treatment of Non-Hodgkin Lymphoma: ASH Topics
 Updates in the Treatment of Non-Hodgkin Lymphoma: ASH 2008 Joseph Tuscano, M.D. UC Davis Cancer Center 1 Topics Mantle Cell Lymphoma What is the standard of care for younger patients? (abstracts 581, 769,
Updates in the Treatment of Non-Hodgkin Lymphoma: ASH 2008 Joseph Tuscano, M.D. UC Davis Cancer Center 1 Topics Mantle Cell Lymphoma What is the standard of care for younger patients? (abstracts 581, 769,
Bcl-2 inhibition in NHL. Jonathan W. Friedberg M.D., M.M.Sc.
 Bcl-2 inhibition in NHL Jonathan W. Friedberg M.D., M.M.Sc. BCL-2, BH3 and apoptosis: Rational therapeutic targets in NHL Antiapoptotic proteins, prevent activation of Bax and Bak, thus inhibiting apoptosis.
Bcl-2 inhibition in NHL Jonathan W. Friedberg M.D., M.M.Sc. BCL-2, BH3 and apoptosis: Rational therapeutic targets in NHL Antiapoptotic proteins, prevent activation of Bax and Bak, thus inhibiting apoptosis.
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
The role of stem cell transplant for lymphoma in 2017
 DOI: 10.1002/hon.2396 SUPPLEMENT ARTICLE The role of stem cell transplant for in 2017 John G. Gribben Barts Cancer Institute, Queen Mary University of London, London, UK Correspondence John G. Gribben,
DOI: 10.1002/hon.2396 SUPPLEMENT ARTICLE The role of stem cell transplant for in 2017 John G. Gribben Barts Cancer Institute, Queen Mary University of London, London, UK Correspondence John G. Gribben,
Background. Outcomes in refractory large B-cell lymphoma with traditional standard of care are extremely poor 1
 2-Year Follow-Up and High-Risk Subset Analysis of ZUMA-1, the Pivotal Study of Axicabtagene Ciloleucel (Axi-Cel) in Patients with Refractory Large B Cell Lymphoma Abstract 2967 Neelapu SS, Ghobadi A, Jacobson
2-Year Follow-Up and High-Risk Subset Analysis of ZUMA-1, the Pivotal Study of Axicabtagene Ciloleucel (Axi-Cel) in Patients with Refractory Large B Cell Lymphoma Abstract 2967 Neelapu SS, Ghobadi A, Jacobson
State of the art: CAR-T cell therapy in lymphoma
 State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
BACKGROUND AND RATIONALE
 SYNOPSIS Observational study on the use of B cell receptor kinase inhibitors and BCL2 antagonists prior to allogeneic hematopoietic stem cell transplantation for B cell malignancies: A joint project of
SYNOPSIS Observational study on the use of B cell receptor kinase inhibitors and BCL2 antagonists prior to allogeneic hematopoietic stem cell transplantation for B cell malignancies: A joint project of
Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009
 Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations