High Risk or High Reward: Breast Cancer Prevention and Screening in Primary Care: New Challenges and Opportunities
|
|
|
- Archibald Stevenson
- 5 years ago
- Views:
Transcription
1 High Risk or High Reward: Breast Cancer Prevention and Screening in Primary Care: New Challenges and Opportunities Section 1 Jamie Stern, MD, MPH: Mammography in the 40s and 50s: the Data and the Controversy Case: A 43 year old woman wants to discuss breast cancer screening. She is asymptomatic with respect to her breasts. She had menarche at age 13, gave birth to her first child at age 29, is of normal body weight and drinks wine socially. She has no FH of breast or ovarian cancer. She has never had a mammogram before, but has heard from her friends that they are very painful. What would you recommend? 1) Which statement is true regarding this patient? A. USPSTF guidelines recommend routine screening in her age group B. The NNS to prevent death in year olds is 1904 C. It is rare for women in their 40 s to have a false positive mammography D. Biopsies rarely occur as a result of false positive mammography 2) If our patient opts to have a mammogram at age 43 (her current age), she should be screened again: A. in 5 years B. in 1-2 years C. At age 50 D. At age 60 Section 2 Jennifer Corbelli, MD: Routine Screening: Considerations Outside the Controversy 1) A 38 year old woman with no significant PMHx or FHx presents to your office and asks if she should be doing self-breast exams (SBE). You advise her: A. Most guidelines continue to recommend that women be instructed to perform a structured monthly self-breast exam B. Some guidelines now recommend against instructing women to perform the SBE C. Although the SBE has not been shown to decrease breast cancer mortality, these studies were observational, and therefore it is unclear if the findings are valid 2) A 51 year old premenopausal woman presents for her first mammogram. She requests a digital mammogram because she read in a magazine that it is superior to traditional (film) mammography. How would you counsel her about the difference between these options? A. Breast cancer detection rates are overall superior with digital mammography vs. film B. Digital mammography has no indications for screening mammography but can be a useful modality for diagnostic mammography C. Digital mammography is more sensitive than film in pre- and peri-menopausal women
2 3) A 45 woman undergoes screening mammography. Her mammogram report reads: No evidence of malignancy. Breasts are heterogeneously very dense. How should this finding impact your plan for screening? A. This finding has no impact on her cancer risk and therefore does not impact her screening B. This finding has no impact on her cancer risk, but it means film mammography will be less sensitive. Digital mammography is the test of choice for screening C. She is at increased cancer risk, and per guidelines should be screened more aggressively than women without dense breasts D. She is at increased cancer risk but no guidelines state that she should be screened differently than women without dense breasts Section 3 Rachel Bonnema, MD, MS: Identification of High-Risk Women 1) A 43 year old Caucasian patient who has not been seen since her last child was born presents for a check-up because both her mother and sister were diagnosed with breast cancer in the last 2 years. You determine her Gail score to be 2.7%. You tell her this is: A. Lower than average risk B. Average risk C. Higher than average risk 2) You discuss with this patient that the best management at this point is: A. Continuing with usual screening patterns as she is average risk for breast cancer. B. Referral for genetic counseling for further delineation of risks, including possible genetic evaluation, as she is high risk for breast cancer. C. Referral to a breast surgeon for evaluation of possible mastectomy as she is high risk for breast cancer. D. Managing her increased risks for breast cancer, but no need for genetic evaluation as it will not add further information to her already known high risk for breast cancer.
3 Section 4 Annie Im, MD: Breast Cancer Primary Prevention For the following patients, choose one of the following options for prevention: A. Tamoxifen B. Raloxifene C. Neither D. Either tamoxifen or raloxifene Patient #1: 42 year old Caucasian female, mother with breast cancer age 50, personal history of breast biopsy with atypical hyperplasia, Gail 5-year risk score = 4.6% Patient #2: 66 year old female, sister with breast cancer age 60, Gail 5-year risk score = 3.3%, personal history of DVT 2 years ago Patient #3: 64 year old female, Gail 5-year risk 1.8%, history of osteoporosis, no history of thrombotic events or other comordities Patient #4: 47 year old female, premenopausal, paternal grandmother and 2 paternal aunts with breast cancer, Gail 5-year risk 1%
4 Section 5 Sarah Tilstra, MD: Screening in High-Risk Women Case: 37 yo female presents to your office for a routine visit. Her PMH is significant for NHL s/p chemo and mediastinal radiation at age 22, currently in remission. She is nulliparous, menarche at age 11 and underwent early menopause due to primary gonadal failure. FHX is significant for a paternal aunt with breast CA at age 35, paternal GM with belly cancer deceased at age 40, and a maternal aunt with breast CA at age Which factors make this woman high risk for developing breast CA? History of mediastinal radiation History of early menarche History of nulliparity Early menopause Family history of paternal aunt with breast CA age 35 Family history of paternal GM with belly cancer deceased age 40 Family history of maternal aunt with breast CA age Should she be tested for BRCA? A. Yes B. No 3. How should our patient be screened for breast cancer? A. Yearly mammography B. Yearly MRI C. Yearly mammography + MRI D. Alternating mammography and MRI q6m 4. When should screening start in this patient? A. Should have started at age 25 B. Should have started at age 30 C. Should have started at age 35 D. Start at age 40

5 High Risk or High Reward? Breast Cancer Prevention and Screening in Primary Care: New Challenges and Opportunities Rachel Bonnema, MD, MS Jennifer Corbelli, MD Annie Im, MD Jamie Stern, MD MPH Sarah Tilstra, MD
6 Workshop Format Introductions and Brainstorm (10 minutes) 5 Content Subsections (15 minutes each) 5 Minutes Questions/Answers in Small Groups 10 Minutes Content Discussion (10 minutes)
7 Workshop Objectives: By the end of this workshop, participants will be able to Counsel patients on risks and benefits of: Starting breast cancer screening at age 40 vs. 50 Continuing screening after age 70 Chemoprevention Recognize: Indications for genetic counseling Implications of breast density on cancer risk Patients at high risk for breast cancer Indications for breast MRI Incorporate Gail model into clinical practice
8 Brainstorm What challenges do you face when deciding how and when to screen your patients for breast cancer? What do you see as the barriers to using breast cancer preventive therapy?
9 Mammography in the 40s and 50s: The Data and the Controversy Jamie Stern, MD, MPH University of Pittsburgh Medical Center
10 Case A 43 year old woman wants to discuss breast cancer screening. She is asymptomatic with respect to her breasts. She had menarche at age 13, gave birth to her first child at age 29, is of normal body weight and drinks wine socially. She has no FH of breast or ovarian cancer. She has never had a mammogram before, but has heard from her friends that they are very painful. What would you recommend?
11 Question #1 Which statement is true regarding this patient?: A. USPSTF guidelines recommend routine screening in her age group B. The NNS to prevent death in year olds is 1904 C. It is rare for women in their 40 s to have a false positive mammography D. Biopsies rarely occur as a result of false positive mammography
12 Question #2 If our patient opts to have a mammogram at age 43 (her current age), she should be screened again: A. in 5 years B. in 1 2 years C. at age 50 D. At age 60
13 2009 USPSTF Mammography Guidelines Age recommends against routine screening (C), net benefit is small, NNS to prevent death 1904 Age recommends biennial screening (B), net benefit is moderate, NNS to prevent death is 1339 for women in their 50 s and 377 for women in their 60 s Age >75 insufficient evidence (I), net benefit unknown, NNS unknown Melson HD. Screening for breast cancer: an update for the USPSTF. Ann Intern Med 2009; 151:
14 USPSTF guidelines 2 major changes in guidelines from Reclassification of screening women in their 40 s from a B to a C recommendation Frequency of screening of women changed from 1 2 years to every 2 years Nelson HD. Screening for breast cancer: an update for the USPSTF. Ann Intern Med 2009;151:
15 Other Organizations The American Cancer Society, American College of Radiology, AMA, NCI, ACOG, National Comprehensive Cancer Network, American Academy of Family Physicians all recommend starting routine screening at 40 ACP and the Canadian Task Force on the Periodic Health Examination recommend starting routine screening at 50 Warner, Ellen. Breast cancer screening. NEJM 365;
16 Harms of Screening Unnecessary imaging tests and biopsies Breast discomfort Radiation exposure Inconvenience Overdiagnosis harms associated with treatment of cancer that would not become clinically apparent during a women s lifetime Harms of unnecessary earlier treatment of breast cancer that would have become clinically apparent, but would not have shortened a women s life
17 Overdiagnosis Recent study in the Annals of Internal Medicine estimated the percentage of overdiagnosis of breast cancer attributable to screening mammography in year old women in Norway Results show that the estimated rate of overdiagnosis was 15 25%, p <0.001 This translates to 6 10 women overdiagnosed for every 2,500 women invited to screen Kalager, M, Overdiagnosis of invasive breast cancer due to mammography screening:results from the Norwegian screening program. Ann int med 2012;156:
18 Data: Women Screening for women in this age group is universally recommended A USPSTF meta analysis (2009) showed significant reductions in the number of deaths due to breast cancer in this age group 14% for women in their 50 s 32% for women in their 60 s The greater reduction in the older age group is due to Increased sensitivity of mammography with age Decreased breast density Slower tumor growth Nelson HD. Screening for breast cancer: an update for the USPSTF. Ann Intern Med 2009;151:
19 Data: Women No single RCT has clearly shown a reduction in mortality from mammography in this age group Several meta analyses have shown a 15 20% reduction in breast cancer mortality, though USPSTF conducted its own meta analysis published in 2002 which showed that mammography decreased death from breast cancer with a RR 0.85, 95% CI Therefore, the USPSTF previously recommended routine screening mammography in this age group (2002 recommendations) Preventive Service Task Force: Screening for breast cancer: recommendations and rationale. Ann Intern Med 2002;137:344 6.
20 Data: Women Age Trial Randomized trial that assessed the effects of screening among 161,000 women aged 39 41, mean follow up was 10.7 years Those assigned to annual mammography had a nonsignificant decreased risk of death from breast cancer RR 0.83, 95% CI RR of death from any cause was 0.97, 95% CI , NNS to prevent one death from breast cancer was 2512 Moss SM. Effect of mammographic screening from age 40 years on breast cancer mortality at 10 years follow up: a randomised controlled trial. Lancet 2006;368:
21 Data: Women An updated USPSTF meta analysis (2009) which included results from the Age Trial provided results similar to the first metaanalysis. RR of death from breast cancer 0.85, 95% CI , NNS 1904 The USPSTF guideline included the following statement, The USPSTF recommends against routine screening mammography in women aged years Nelson HD. Screening for breast cancer: an update for the USPSTF. Ann Intern Med 2009;151:
22 Data: Women The decision to change the USPSTF recommendations was based on Negative results of the Age Trial (the only trial that specifically focused on women in their 40 s) Lower breast cancer risk Lower mammographic sensitivity (greater breast density) Higher rate of false positives Warner, Ellen. Breast cancer screening. NEJM 2011; 365:
23 Frequency of Screenings Another controversial change from the 2002 USPSTF guidelines was a switch from 1 2 year screening to 2 year screening Supporting this change was the observation that there was little difference in the likelihood of detecting advanced breast cancer with annual versus biennial screening Wai ES. Comparison of 1 and 2 year screening intervals for women undergoing screening mammography. Br J Cancer 2005;92:961 6.
24 Frequency of Screening In statistical models, screening of women every 2 years maintained 81% of the benefit associated with annual screening and decreased the number of false positive results by almost half As compared with screening every 2 years, annual screening prevented about 2 additional deaths from breast cancer per 1000 women screened Mendelblatt, JS. Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms. Ann Intern Med 2009;151:
25 The Bottom Line Age Shared decision making Still recommend mammography if the patient is willing Would recommend screening every 1 2 years due to rapid tumor growth in young women Age Strongly recommend mammography Based on my review of the literature, I have changed my recommendation from yearly to biennial
26 Routine Screening: Considerations Outside the Controversy Jennifer Corbelli, MD University of Pittsburgh Medical Center
27 Question #1 A 38 year old woman with no significant PMHx or FHx presents to your office and asks if she should be doing self breast exams (SBE). You advise her: A. Most guidelines continue to recommend that women be instructed to perform a structured monthly selfbreast exam B. Some guidelines now recommend against instructing women to perform the SBE C. Although the SBE has not been shown to decrease breast cancer mortality, these studies were observational, and therefore it is unclear if the findings are valid
28 Question #2 A 51 year old premenopausal woman presents for her first mammogram. She requests a digital mammogram because she read in a magazine that it is superior to traditional (film) mammography. How would you counsel her about the difference between these options? A. Breast cancer detection rates are overall superior with digital mammography vs. film B. Digital mammography has no indications for screening mammography but can be a useful modality for diagnostic mammography C. Digital mammography is more sensitive than film in pre and peri menopausal women
29 Question #3 A 45 woman undergoes screening mammography. Her mammogram report reads: No evidence of malignancy. Breasts are heterogeneously dense (>75%). How should this finding impact your plan for screening? A. This finding has no impact on her cancer risk and therefore does not impact her screening B. This finding has no impact on her cancer risk, but it means film mammography will be less sensitive. Digital mammography is the test of choice for screening. C. She is at increased cancer risk, & per guidelines should be screened more aggressively than women without dense breasts D. She is at increased cancer risk but no guidelines state that she should be screened differently than women w/o dense breasts
30 Clinical Breast Exam (CBE): Guidelines USPSTF: Insufficient evidence to assess additional benefits of CBE beyond screening mammography (Nelson Annals 2009) ACOG: CBE yearly after age 40 (Smith Cancer Journal 2010) ACS: CBE yearly after age 40, every 3 years ages (ACOG Practice Bulletin, Obstet Gynecol 2011)
31 Clinical Breast Exam Sensitivity 54%, Specificity 94% Limitations in data: No trials compare CBE alone to no screening (unethical) Studies did not specify/standardize exam techniques Bottom Line for CBE: Unable to quantify CBE benefit in addition to mammogram Most studies show independent contribution of CBE to cancer detection (offset by harms?) UPMC algorithm: Housestaff need to learn (normal vs. abnormal) Generally done every 1 2 years Barton JAMA 1999
32 Key Points, JAMA Rational Clinical Exam The vertical strip method ("lawnmower ) is more thorough than the circular method Nipple should NOT be squeezed Spontaneous discharge associated with increased cancer risk Expressed discharge is not Increased time per breast increases sensitivity Recommended 3 min/breast (average size, i.e. B cup) Based on expert consensus Average clinician spends 1.8 minutes for both breasts
33 Self Breast Exam (SBE) USPSTF: Recommends against advising regular SBE ACOG: Encourage breast self awareness, which may include SBE ACS: SBE an option for women starting age 20, emphasis on breast awareness 2 large RCTs (11 year follow up) showed no mortality benefit to monthly SBE Associated with higher biopsy rates for benign findings Bottom Line: Breast awareness should be emphasized over a structured, monthly SBE Thomas JNCI 2002 Semiglazov Vopr Onkol 1999 Hackshaw BJCa 2003
34 Digital vs. Film Mammography Film is traditional method, many centers have now moved to all digital Digital: increased contrast between tumor & breast Digital mammography (DMIST trial): 50,000 asymptomatic women > 40, screened with digital and film Overall no significant difference in sensitivity Digital significantly more sensitive than film if: Pre and peri menopausal Dense breasts Age <50 No difference in specificity (both 92%) all 3 present Pisano Radiology 2008
35 Digital vs. Film Mammography Total Sensitivity NEJM Editorial, Sept Recommends digital for (any one): Women being screened in their 40s Women of any age with dense breasts Premenopausal women >50 Sensitivity: Women <50, premenopause, dense breasts Digital 70% 78% Film 66% 51% Pisano Radiology 2008 Warner, NEJM 2011
36 Breast Density Dense breast tissue (mammographic, not Pex finding) increases cancer risk (not included in Gail) Nested case control vs <10% density: (Boyd NEJM 2007) 10 25% density= RR 1.8 >75% density = RR 4.7 Increased risk both for cancers detected both by mammogram and within 12 months of negative test Attributable risk of >50% density: 16% all breast cancers 40% found within 12 mos. of negative mammogram No recommendations for different screening
37 Breast Density and Screening Two Annals papers (May 2012) Modeling study: women in 40s with cancer risk 2x average have harm to benefit ratio comparable to women Meta analysis, 2x inc breast cancer risk with either: Extremely dense breasts (>50%) One first degree relative with breast cancer Conclusion (?): Women with dense breasts should start mammography at age 40 But won t know until first mammogram
38 Stopping Mammograms USPSTF: Insufficient evidence to recommend for or against screening after 75 ACS: continue mammograms while in good health ACOG: consider life expectancy in patients >75 Issues: Data limited Shorter life expectancy decreases benefit of screening Not all women want to know/treat Cost: Benefit Ratio (as always)
39 Data: Stopping Mammograms Only one RCT Swedish study, included women up to 75 RR of death from Br CA: 1.12, 95% CI No NNS calculated (total # deaths not reported) National Cancer Institute: 2 additional cancer deaths prevented per 1000 women screened ages Expert opinion: screening may be indicated if estimated >10 years life expectancy (if patient would desire and be candidate for treatment) NystromLancet 2002 Nelson Annals 2009
40 Take Home Points Benefit of clinical breast exam remains unclear (sensitivity 54%): use vertical strip method if you do it Advise breast self awareness rather than monthly SBE Generally opt for digital over film mammogram in women <50, with dense breasts, and/or pre or peri menopausal Breast density increases cancer risk, independently of decreased mammography sensitivity Hot off the press: Women <50 with dense breasts should potentially begin mammography starting at age 40 (but you won t know until you screen)
41 Identification of High Risk Women Rachel Bonnema, MD, MS University of Nebraska Medical Center
42 A 43 year old Caucasian patient who has not been seen since her last child was born presents for a check up because both her mother and sister were diagnosed with breast cancer in the last 2 years. You determine her Gail score to be 2.7%. You tell her this is: A. Lower than average risk B. Average risk C. Higher than average risk
43 You discuss with this patient that the best management at this point is: A. Continuing with usual screening patterns as she is average risk for breast cancer. B. Referral for genetic counseling for further delineation of risks, including possible genetic evaluation, as she is high risk for breast cancer. C. Referral to a breast surgeon for evaluation of possible mastectomy as she is high risk for breast cancer. D. Managing her increased risks for breast cancer, but no need for genetic evaluation as it will not add further information to her already known high risk for breast cancer.
44 Importance of Appropriate Risk Assessment Appropriately managing women with BRCA1/2 mutations decrease breast cancer incidence by 80 95% Adherence to recommendations for genetic testing and counseling for high risk women is low 41% in recent vignette based survey Average risk women often mislabeled as high risk Important barrier is lack of knowledge in genetic risk and risk reduction skills Trivers KF, et al. Cancer, 2011
45 Quantitative Risk Assessment The Gail Model: Projects the absolute risk of invasive breast cancer over five years for women >35 years Factors included in calculating risk: Age Age at menarche Number of first degree female relatives with breast cancer Number of previous breast biopsies Age at first live birth (or nulliparity) Race Personal history of atypical hyperplasia Gail MH, et al. J Natl Cancer Inst 1989; 81:1879
46 Gail Model We recommend using the computer program available at: Most commonly used breast cancer prediction tool National Cancer Institute. Accessed May 2012 Vachon CM, et al. Breast Ca Res, 2007
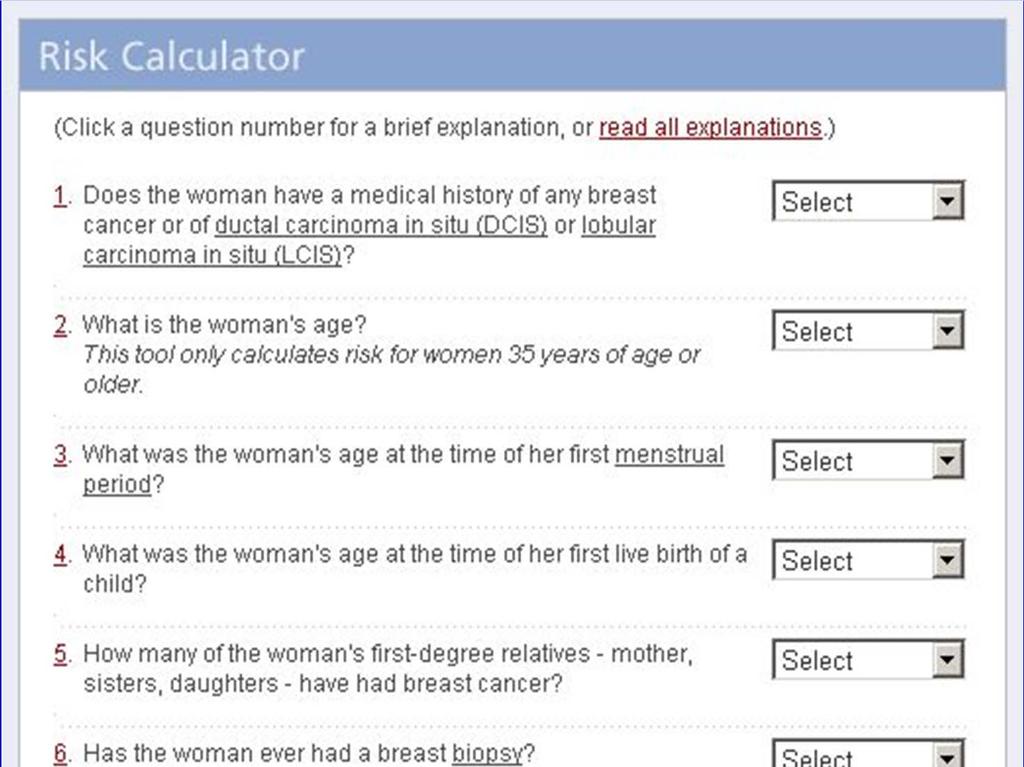
47
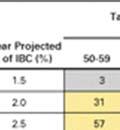
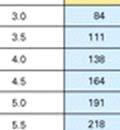
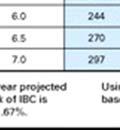
48 Gail Model An increased risk of developing breast cancer is defined as a Gail Score of 1.66% or greater
49 Gail Model Is the Gail Model valid? Breast Cancer Prevention Trial Nurses Health Study In the above studies, the Gail Model s expected number of breast cancer cases closely approximated the actual number of breast cancer cases Has been validated in white, African American, Asian and Pacific Islander women Costantino JP, et al. J Natl Cancer Inst 1999; 91: Roskhill B, et al. J Natl Cancer Inst 2001; 93: tool.aspx. Accessed April 29, 2012.
50 Gail Model Shortcomings of the Gail Model: Does not incorporate family history outside of first degree relatives or presence in paternal lineage BRCAPRO model, CLAUS model PAT (Pedigree Assessment Tool) Does not account for young age of breast cancer onset Does not incorporate estrogen use, alcohol use Does not account for breast density Does not account for risks due to previous thoracic radiation Not valid in women under age 35
51 Gail Score Not static throughout patient s life Should be reassessed periodically No recommendations on interval Our practice calculate Gail score: Anyone > age 35 with any FHx of breast cancer Anytime a patient s family member is newly diagnosed with breast cancer New diagnosis of atypical hyperplasia, DCIS, LCIS In general: ~age 50 if not done prior, repeat ~q 5 years especially if prior 5 year risk close to 1.66% (depending on comorbidities, life expectancy, etc)
52 Other Risks Genetic disorder Li Fraumeni, Cowden, Bannayan Riley Ruvalcada Syndromes Previous thoracic radiation treatment Dense breasts
53 Hereditary Breast Cancer A positive family history is reported in up to 20% of women with breast cancer Only 5 6% of all breast cancers are associated with an inherited mutation Two major susceptibility genes for breast cancer are BRCA1 and BRCA2 General population prevalence % Ashkenazi Jewish prevalence 2.5% Struewing JP, et al. N Engl J Med 1997; 336:1401 Tung N. JAMA, 2011.
54 BRCA1 and BRCA2 BRCA genes encode for proteins which function to repair breaks in double stranded DNA Mutations in these genes account for the majority of inherited breast cancers Mutations are inherited in an autosomal dominant fashion Lifetime estimate of breast cancer in BRCA ½ is 36 90% Antoniou A, et al. Am J Hum Genet 2003; 72:1117.
55 Referring for Genetic Counseling Indications for referral: Known BRCA ½ mutation in family 2 breast cancers from same side of family Breast + ovarian cancer from same side of family 1 ovarian cancer from same side of family Breast cancer occurring before age 50 Male relatives with breast cancer Ashkenazi Jewish heritage and a family history of breast or ovarian cancer Smith RA, et al. CA Cancer J Clin 2003; 53; NCCN Guidelines, Version
56 Referral for Genetic Counseling Genetic Counselor may or may not say patient is appropriate for genetic testing Does not change Gail score or risk of developing breast cancer Patient may not be tested, still remain high risk Patient tested and negative for BRCA, still remains high risk
57 Breast Cancer Primary Prevention Annie Im, MD Hematology/Oncology Fellow University of Pittsburgh Cancer Institute
58 High risk or High reward? For the following patients, choose one of the following options for prevention: A) Tamoxifen B) Raloxifene C) Neither D) Either tamoxifen or raloxifene
59 Patient #1 42 year old Caucasian female, mother with breast cancer age 50, personal history of breast biopsy with atypical hyperplasia, Gail 5 year risk score = 4.6% A) Tamoxifen B) Raloxifene C) Neither D) Either tamoxifen or raloxifene
60 Patient #2 66 year old female, sister with breast cancer age 60, Gail 5 year risk score = 3.3%, personal history of DVT 2 years ago A) Tamoxifen B) Raloxifene C) Neither D) Either tamoxifen or raloxifene
61 Patient #3 64 year old female, Gail 5 year risk 1.8%, history of osteoporosis, no history of thrombotic events or comorbidities A) Tamoxifen B) Raloxifene C) Neither D) Either tamoxifen or raloxifene
62 Patient #4 47 year old female, premenopausal, paternal grandmother and 2 paternal aunts with breast cancer, Gail 5 year risk 1% A) Tamoxifen B) Raloxifene C) Neither D) Either tamoxifen or raloxifene
63 Risk Reduction Strategies Risk reduction mastectomy* Preventive therapy Tamoxifen Raloxifene Aromatase Inhibitors Lifestyle modifications Weight loss Exercise Alcohol intake
64 Tamoxifen Selective Estrogen Receptor Modulator (SERM) Role in prevention developed after shown to decrease contralateral breast cancer incidence when used as adjuvant hormonal therapy for early stage breast cancer Anti estrogenic properties in breast tissue Estrogenic properties in uterus, bone, coagulation
65 Prevention Guideline #1: Tamoxifen 20mg daily x 5 years reduces risk of ER positive breast cancer by 50% for 10 years Recommended: Premenopausal or postmenopausal women age>35 with Gail 5 year breast cancer risk >/=1.7% History of LCIS Contraindicated: History of DVT/PE, TIA, or stroke Not recommended: Postmenopausal women with uterus History of cataracts
66 Tamoxifen: Adverse effects Increased risk of uterine cancer Increased risk of DVT/PE and stroke, especially in postmenopausal women Increased risk of cataracts Hot flashes, sexual side effects, gynecologic symptoms
67 Tamoxifen: Tips Benefit of 5 years therapy lasts up to 10 years, with decreasing risk of toxicities and side effects NNT to prevent 1 cancer over 5 years = 95, over 10 years = 56 Only chemoprevention option for premenopausal women, and benefit/risk ratio more favorable
68 Raloxifene Second generation SERM, initially studied as an osteoporotic agent Anti estrogenic properties in breast and uterus Estrogenic properties in bone and coagulation
69 Prevention Guideline #2: Raloxifene 60mg daily x 5 years reduces risk of ERpositive breast cancer by 40% Recommended: Postmenopausal women age>35 with Gail 5 year breast cancer risk >/=1.7% History of LCIS Contraindicated: History of DVT/PE, TIA, or stroke
70 Raloxifene: Adverse effects Compared to tamoxifen: Does not increase risk of uterine cancer Does not increase risk of cataracts Less risk of DVT and PE (30%), but similar risk of stroke Hot flashes, musculoskeletal complaints, weight gain
71 Raloxifene: Tips Toxicity profile is better for postmenopausal NNT to prevent 1 cancer over 4 years = 96, over 8years = 52 Decreases risk of vertebral fractures and increases bone density, and may be used longer for osteoporosis
72 The Future of Preventive Therapy: Aromatase Inhibitors AIs (anastrozole, exemestane, letrozole) block estrogen production in peripheral tissue in postmenopausal women Currently used in early stage breast cancer for adjuvant hormonal therapy Benefits no increased risk of thromboembolic events, stroke, uterine malignancies, cataracts Risks no estrogenic effect on bone Recent phase III study shows risk reduction of 65% for ER positive cancers in high risk women
73 Prevention Guideline #3: Lifestyle Modifications Evidence for risk reduction: Weight loss and avoiding postmenopausal weight gain Exercise >5hrs vigorous exercise or >10 hours brisk walking per week, >10 hours per week, regular strenuous activity Alcohol consumption <1 drink/day Evidence unclear: Low fat diet/nutrition but in general a good thing! HRT recommend to limit long term use
74 Risk Reduction Strategies Gail score>1.7% or LCIS? N Postmenopausal? Y N History of DVT/PE or stroke? Y N History of DVT/PE or stroke? Y Tamoxifen Lifestyle modifications N Uterus? Y Lifestyle modifications Osteoporosis? Raloxifene N Raloxifene or Tamoxifen Y Raloxifene
75 Risk Reduction Strategies Strong family history Gail score >1.7% Gail score <1.7% Indications for genetic screening? Use previous algorithm N Indications for genetic screening? Y Refer to genetic counseling Lifestyle modifications Refer to genetic counseling
76 Risk/benefit Counseling
77 Take Home Message Recommendations for prevention strategies should be individualized based on patient s baseline breast cancer risk, comorbidities, and personal preference Preventive therapy is safe and effective, and plays an essential role in the primary care setting
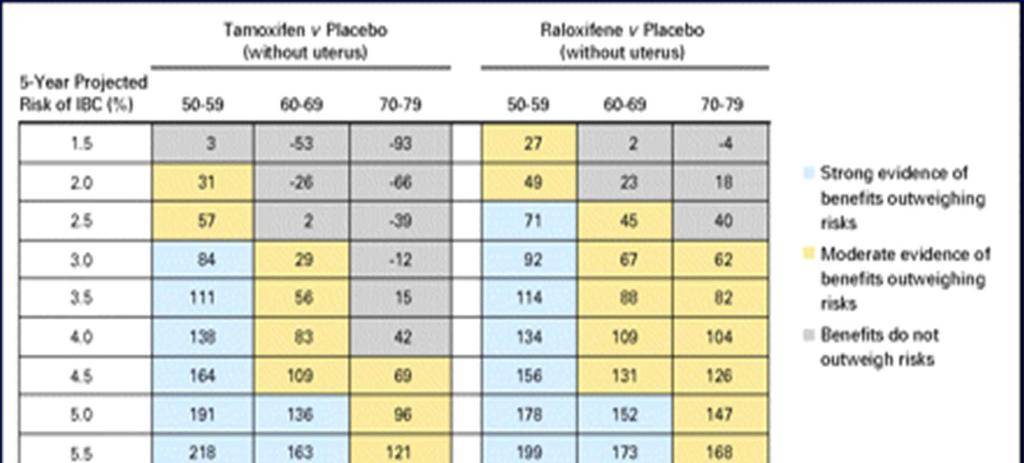
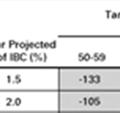
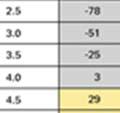
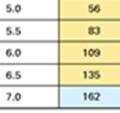
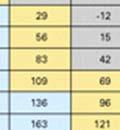
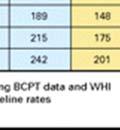
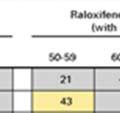
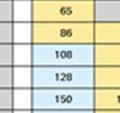
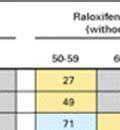
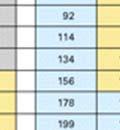
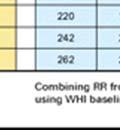
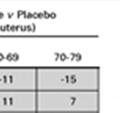
78 References *Freedman A, et al. Benefit/Risk Assessment for Breast Cancer Chemoprevention With Raloxifene or Tamoxifen for Women Age 50 or Older. J Clin Oncol, 2011:29: NCCN Clinical Practice Guidelines Bevers TB, et al. J Natl Compr Canc Netw 2010;8: ASCO Clinical Practice Guidelines Visvanathan K, et al. J Clin Oncol 2009;27:
79 Screening for Breast Cancer in High Risk Women Sarah Tilstra, MD University of Pittsburgh Medical Center
80 Case 37 yo female presents to your office for a routine visit. Her PMH is significant for NHL s/p chemo and mediastinal radiation at age 22, currently in remission. She is nulliparous, menarche at age 11 and underwent early menopause due to primary gonadal failure. FHX is significant for a paternal aunt with breast CA at age 35, paternal GM with belly cancer deceased at age 40, and a maternal aunt with breast CA at age 60.
81 Questions 1. What makes this women at high risk for breast cancer? Will get to this 2. Should she be tested for BRCA? A = Yes, B = No 3. How should she be screened? A. Yearly mammography B. Yearly MRI C. Yearly mammography + MRI D. Alternating mammography and MRI q6m 4. At what age should screening start? A = 25, B = 30, C = 35, D = 40
82 High Risk 1. BRCA1 or BRCA2 carrier (RR 5 30) 2. BRCA1 or BRCA2 carrier in first degree relative, unknown patient carrier status 3. Strong family history of breast/ovarian CA (RR 3 4) Mother/sister diagnosed <40 2+ first degree relatives with breast or ovarian cancers 4. Radiation treatment to chest area ages (RR 4 11) 5. Known genetic syndrome predisposing pt to breast CA (Li Fraumeni, Cowden, Bannayan Riley Ruvalcada Syndromes) Or >20% lifetime risk of breast CA American Cancer Society ww5.komen.org
83 Question 1: Which factors make this woman high risk for developing breast CA? Hx of mediastinal radiation Hx of early menarche Hx of nulliparity Early menopause FHx of paternal aunt with breast CA age 35 FHx of paternal GM with belly cancer deceased age 40 FHx of maternal aunt with breast CA age 60
84 Moderate Risk Lifetime breast CA risk 15 20% according to risk assessment tools Personal hx of breast CA, ductal CA in situ (DCIS), lobular CA in situ (LCIS), atypical ductal hyperplasia (ADH), atypical lobular hyperplasia (ALH) Extremely dense breasts Unevenly dense breasts on mammography American Cancer Society ww5.komen.org
85 Question 2: Test for BRCA? Yes! Paternal aunt with breast CA at age 35 Paternal GM with belly cancer deceased age 40 Suspicious for BRCA Maternal aunt with breast CA at age 60 not an indication
86 BRCA1/BRCA2 If inherited, 50 85% lifetime risk of breast CA Harder to detect in families with no female members >45 Weitzel JN et al. Limited Family Structure and BRCA Gene Mutation Status in Single Cases of Breast Cancer. JAMA. 2007; 297(23):
87 Who Should Definitely Be Tested Known BRCA ½ mutation in family 2 breast cancers from same side of family Breast + ovarian cancer from same side of family 1 ovarian cancer from same side of family Breast cancer occurring before age 50 Male relatives with breast cancer Ashkenazi Jewish heritage and a family history of breast or ovarian cancer Smith RA, et al. CA Cancer J Clin 2003; 53; NCCN Guidelines, Version
88 Who Should You Consider for Testing Patients with Cancer Breast CA <40 Ovarian CA Bilateral breast CA Breast CA <50 with close relative breast CA <50 Breast CA any age with 2+ relatives breast CA ACOG Routine Screening for Hereditary Breast and Ovarian Cancer, 2009
89 Who Should You Consider for Testing Patients Without Cancer Two first degree relatives with breast CA, one diagnosed <50 First degree relative with bilateral CA or male breast CA First/second degree relative with both breast and ovarian CA 3+ first/second degree relative with breast CA 2+ first/second degree relatives with ovarian CA ACOG Routine Screening for Hereditary Breast and Ovarian Cancer 2009 National Cancer Institute at the NIH
90 Question 3: How Should Our Patient Be Screened? A. Yearly mammography B. Yearly MRI C. Yearly mammography + MRI D. Alternating mammography and MRI q6m
91 Screening MRI + Mammography Complementary, sensitivity MRI + mammo > MRI alone Q6m vs. yearly no evidence to support one over the other. All trials obtained imaging at the same time Sensitivity in high risk women: % MRI 16 40% Mammography/Ultrasound MRI: more false+, more call backs, more biopsies (3 15%) ACS Guidelines. Saslow et al, CA Cancer J Clin, 2007
92 Evidence: MRI BRCA mutation, first degree BRCA carrier, but untested, lifetime risk >20% Expert consensus: Chest radiation, genetic syndromes Insufficient evidence for/against: Hx CA (mammo occult..), lifetime risk 15 20%, dense breasts, DCIS, LCIS, ALH, ADH Against MRI: <15% lifetime risk ACS Guidelines. Saslow et al, CA Cancer J Clin, 2007.
93 Question 4: When Should Screening Start? A. Should have started at age 25 B. Should have started at age 30 C. Should have started at age 35 D. Start at age 40
94 When to Start Screening High Risk Women BRCA: age 25, yearly MRI + mammography Strong family history: 5 10 years before earliest breast CA in the family Radiation: 8 10 years after radiation or age 25, whatever comes last OR.. Age 30 ACS Guidelines. Saslow et al, CA Cancer J Clin, 2007.
95 Breast Cancer Survivors Caveat: requires a workshop in itself SBE: Survivors should perform monthly Physical exam (CBE implied but not specified) q3 6 months for first three years q6 12 months years 4 5 Annually thereafter Mammography: Breast conserving tx: q6 12 months s/p mastectomy: yearly if stable mammography findings MRI: not recommended for routine surveillance No evidence of improved outcomes 2006 ASCO guidelines
96 Discussion













97





98 References: * Freedman A, et al. Benefit/Risk Assessment for Breast Cancer Chemoprevention With Raloxifene or Tamoxifen for Women Age 50 or Older. J Clin Oncol,, 2011:29: NCCN Clinical Practice Guidelines Bevers TB, et al. Breast Cancer Risk Reduction. J Natl Compr Canc Netw 2010;8: ASCO Clinical Practice Guidelines Visvanathan K, et al. American Society of Clinical Oncology Clinical Practice Guideline Update on the Use of Pharmacologic Interventions Including Tamoxifen, Raloxifene, and Aromatase Inhibition for Breast Cancer Risk Reduction. J Clin Oncol 2009;27:
99 Top Ten Clinical Pearls for Breast Cancer Screening and Prevention in Primary Care 1. For average risk women aged 40-49, USPSTF recommends against routine screening with mammography (class C). The number needed to screen to prevent 1 death is Harms include overdiagnosis and false positive mammograms. 2. For average risk women aged 50-74, USPSTF recommends biennial screening with mammography (class B) The number needed to screen to prevent one death is 1339 for women in their 50 s and 377 for women in their 60 s. Patients should be counseled regarding reasons for this controversy, and engaged in shared-decision making when discussing screening. 3. There is no overall difference in sensitivity between digital and film mammography. However, digital mammography is significantly more sensitive (78% vs 51%) than film in women under age 50, who have dense breasts, and who are premenopausal. 4. Women with dense breasts are at an independently increased risk for breast cancer. There are no clear recommendations to guide screening in this population. However, recently published data shows that women in their 40s with extremely dense breasts may have a screening harm:benefit ratio that is comparable to women over 50. These data suggest that these women may benefit from initiating mammography at age 40 more so than agematched women without dense breasts. (Nelson HD et al. Risk Factors for Breast Cancer for Women Aged 40 to 49 Years: A Systematic Review and Meta-analysis. Ann Intern Med May 1, : Van Ravesteyn NT et al. Tipping the Balance of Benefits and Harms to Favor Screening Mammography Starting at Age 40 Years. A Comparative Modeling Study of Risk. Ann Intern Med May 1, : ) 5. Women with a Gail score >1.7% should be considered at increased risk for breast cancer, whether or not they meet criteria for genetic counseling. Although there are no recommendations on when to first calculate the Gail score or how often to repeat it, it should be reassessed periodically throughout a woman s life. 6. Absolute indications for genetic counseling include: Known BRCA mutation in family >2 breast cancers on same side of the family >1 ovarian cancers in family Breast cancer <age 50 in close relative Ashkenazi Jewish heritage and a family history of breast or ovarian cancer Male relatives with breast cancer
100 7. Women who fit into one of more of the following categories should be considered at very high risk for breast cancer: Known BRCA carrier Mother/sister diagnosed <40 2+ first-degree relatives with breast or ovarian cancers Known genetic syndrome predisposing to breast cancer Radiation treatment to chest area ages >20% average lifetime risk of breast cancer per risk-analysis tools 8. High-risk women should be screened for breast cancer with yearly mammography and MRI. Alternating mammography and MRI every 6 months is also acceptable. Breast cancers survivors are not considered part of this high-risk group, and should not undergo MRI for routine surveillance. 9. Recommendations for breast cancer prevention strategies should be individualized based on a patient's baseline breast cancer risk, comorbidities, and personal preference. 10. Preventive therapy is safe and effective, and counseling of the benefits and risks plays an essential role in the primary care setting. It should be considered in all women with a 5- year risk of invasive breast cancer >1.7% based on the Gail score, and in women with LCIS. Rachel Bonnema, MD, MS Jennifer Corbelli, MD Annie Im, MD Jamie Stern, MD, MPH Sarah Tilstra, MD
Risk Assessment, Genetics, and Prevention
 Risk Assessment, Genetics, and Prevention Katherine D. Crew, MD MS Director, Clinical Breast Cancer Prevention Program Columbia University Medical Center 1 Outline Breast cancer risk factors Hereditary
Risk Assessment, Genetics, and Prevention Katherine D. Crew, MD MS Director, Clinical Breast Cancer Prevention Program Columbia University Medical Center 1 Outline Breast cancer risk factors Hereditary
Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program
 Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program A B C D USPSTF recommends the service. There is high certainty that Offer or provide
Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program A B C D USPSTF recommends the service. There is high certainty that Offer or provide
Increased Risk of Breast Cancer: Screening and Prevention. Elizabeth Pritchard, MD 4/5/2017
 Increased Risk of Breast Cancer: Screening and Prevention Elizabeth Pritchard, MD 4/5/2017 No disclosures Defining Risk Risk Factors Modifiable Lifestyle obesity physical activity alcohol consumption breast
Increased Risk of Breast Cancer: Screening and Prevention Elizabeth Pritchard, MD 4/5/2017 No disclosures Defining Risk Risk Factors Modifiable Lifestyle obesity physical activity alcohol consumption breast
OBJECTIVES 8/25/2017. An attempt to organize the chaos
 High Risk for Breast Cancer and Genetics: Who? What? Where? When? An attempt to organize the chaos Presented at Winds of Change Conference November 3, 2017 by Carol Hager, MSN, CRNP and Allison Haener,
High Risk for Breast Cancer and Genetics: Who? What? Where? When? An attempt to organize the chaos Presented at Winds of Change Conference November 3, 2017 by Carol Hager, MSN, CRNP and Allison Haener,
So, Who are the appropriate individuals that should consider genetic counseling and genetic testing?
 Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
Chemo-endocrine prevention of breast cancer
 Chemo-endocrine prevention of breast cancer Andrea DeCensi, MD Division of Medical Oncology Ospedali Galliera, Genova; Division of Cancer Prevention and Genetics, European Institute of Oncology, Milano;
Chemo-endocrine prevention of breast cancer Andrea DeCensi, MD Division of Medical Oncology Ospedali Galliera, Genova; Division of Cancer Prevention and Genetics, European Institute of Oncology, Milano;
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond.
 HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
Melissa Hartman, DO Women s Health Orlando VA Medical Center
 Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
Current Strategies in the Detection of Breast Cancer. Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF
 Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow
 Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow Debra A. Walz, RN, MS, AOCNP, WHNP-BC, RNFA Advanced Oncology & Women s Health Nurse Practitioner Oneida
Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow Debra A. Walz, RN, MS, AOCNP, WHNP-BC, RNFA Advanced Oncology & Women s Health Nurse Practitioner Oneida
Imaging Guidelines for Breast Cancer Screening
 Imaging Guidelines for Breast Cancer Screening Sarah Colwick, MD Dr. Sarah Colwick was born and raised in Sikeston, MO. She attended college and medical school at the University of Missouri-Kansas City
Imaging Guidelines for Breast Cancer Screening Sarah Colwick, MD Dr. Sarah Colwick was born and raised in Sikeston, MO. She attended college and medical school at the University of Missouri-Kansas City
Breast Cancer Screening and Diagnosis
 Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
Breast Cancer Risk Assessment and Prevention
 Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Screening and High Risk
 Breast Cancer Screening and High Risk Mary Freyvogel, DO Breast Surgeon Clinical Assistant Professor of Surgery University Hospitals Case Medical Center St. John Medical Center / Elyria Medical Center
Breast Cancer Screening and High Risk Mary Freyvogel, DO Breast Surgeon Clinical Assistant Professor of Surgery University Hospitals Case Medical Center St. John Medical Center / Elyria Medical Center
MANAGEMENT OF DENSE BREASTS. Nichole K Ingalls, MD, MPH NW Surgical Specialists September 25, 2015
 MANAGEMENT OF DENSE BREASTS Nichole K Ingalls, MD, MPH NW Surgical Specialists September 25, 2015 No financial disclosures National Cancer Institute National Cancer Institute Increased Cancer Risk... DENSITY
MANAGEMENT OF DENSE BREASTS Nichole K Ingalls, MD, MPH NW Surgical Specialists September 25, 2015 No financial disclosures National Cancer Institute National Cancer Institute Increased Cancer Risk... DENSITY
Breast Cancer Risk Factors 8/3/2014
 Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Session Objectives Explain the rationale for initiation and frequency of clinical breast exams to clients
Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Session Objectives Explain the rationale for initiation and frequency of clinical breast exams to clients
Breast Cancer Screening: Changing Philosophies in Educating Women and Teens
 Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Disclosures Merck Nexplanon trainer Session Objectives Explain the rationale for initiation and frequency
Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Disclosures Merck Nexplanon trainer Session Objectives Explain the rationale for initiation and frequency
Spectrum of Care Options for Women at High Risk for Breast and Ovarian Cancer
 Spectrum of Care Options for Women at High Risk for Breast and Ovarian Cancer Sheryl G.A. Gabram, MD, MBA, FACS Professor of Surgery, Emory University Director, High Risk Assessment Program Winship Cancer
Spectrum of Care Options for Women at High Risk for Breast and Ovarian Cancer Sheryl G.A. Gabram, MD, MBA, FACS Professor of Surgery, Emory University Director, High Risk Assessment Program Winship Cancer
Prophylactic Mastectomy
 Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO 08/24/2012 Section: Surgery Place(s) of Service: Inpatient I.
Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO 08/24/2012 Section: Surgery Place(s) of Service: Inpatient I.
Breast Cancer: Selected Topics for the Primary Care Clinician
 Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Women s Health: Breast Cancer Screening. K. Rast, MD and E. McNany, MD
 Women s Health: Breast Cancer Screening K. Rast, MD and E. McNany, MD 2013 2017 Update: Who? How? When? Cases and Practice Questions Question 1 A 40 year old female comes to your office for a well woman
Women s Health: Breast Cancer Screening K. Rast, MD and E. McNany, MD 2013 2017 Update: Who? How? When? Cases and Practice Questions Question 1 A 40 year old female comes to your office for a well woman
NATIONAL GUIDELINE CLEARINGHOUSE (NGC) GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER
 GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER") NATIONAL GUIDELINE CLEARINGHOUSE (NGC) GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER Guidelines 1. American Cancer Society (ACS). (1) ACS guidelines for breast cancer screening: update 2003. (2) American
NATIONAL GUIDELINE CLEARINGHOUSE (NGC) GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER Guidelines 1. American Cancer Society (ACS). (1) ACS guidelines for breast cancer screening: update 2003. (2) American
RALOXIFENE Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA Is the request for the prevention (risk reduction) of breast cancer?
 of breast cancer?") Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA 16917 GUIDELINES FOR USE 1. Is the request for the prevention (risk reduction) of breast cancer? If yes, continue to #2. If no, approve by HICL
Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA 16917 GUIDELINES FOR USE 1. Is the request for the prevention (risk reduction) of breast cancer? If yes, continue to #2. If no, approve by HICL
Mammography and Other Screening Tests. for Breast Problems
 301.681.3400 OBGYNCWC.COM Mammography and Other Screening Tests What is a screening test? for Breast Problems A screening test is used to find diseases, such as cancer, in people who do not have signs
301.681.3400 OBGYNCWC.COM Mammography and Other Screening Tests What is a screening test? for Breast Problems A screening test is used to find diseases, such as cancer, in people who do not have signs
Screening Mammography: The Controversy, Risk Assessment and Individualized Screening recommendations. Jonathan T. Sims MD, MBA
 Screening Mammography: The Controversy, Risk Assessment and Individualized Screening recommendations. Jonathan T. Sims MD, MBA I have no relevant Financial Disclosures Agenda Discuss the recent studies
Screening Mammography: The Controversy, Risk Assessment and Individualized Screening recommendations. Jonathan T. Sims MD, MBA I have no relevant Financial Disclosures Agenda Discuss the recent studies
Case 1. BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care
 BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
Effective Health Care Program
 Comparative Effectiveness Review Number 17 Effective Health Care Program Comparative Effectiveness of Medications To Reduce Risk of Primary Breast Cancer in Women Executive Summary Background Breast cancer
Comparative Effectiveness Review Number 17 Effective Health Care Program Comparative Effectiveness of Medications To Reduce Risk of Primary Breast Cancer in Women Executive Summary Background Breast cancer
Update in Breast Cancer Screening
 Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute and Grail - and - Karla Kerlikowske,
Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute and Grail - and - Karla Kerlikowske,
Updates In Cancer Screening: Navigating a Changing Landscape
 Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Breast Cancer Risk Assessment: Genetics, Risk Models, and Screening. Amie Hass, MSN, ARNP, FNP-BC Hall-Perrine Cancer Center
 Breast Cancer Risk Assessment: Genetics, Risk Models, and Screening Amie Hass, MSN, ARNP, FNP-BC Hall-Perrine Cancer Center Disclosure- I DO NOT HAVE any relevant financial interest with any entity producing,
Breast Cancer Risk Assessment: Genetics, Risk Models, and Screening Amie Hass, MSN, ARNP, FNP-BC Hall-Perrine Cancer Center Disclosure- I DO NOT HAVE any relevant financial interest with any entity producing,
Breast Cancer: Key Issues for the Non-Oncologist
 Breast Cancer: Key Issues for the Non-Oncologist I have no financial disclosures I developed and validated one of the models that will be discussed. I hold no patents and derive no financial benefit from
Breast Cancer: Key Issues for the Non-Oncologist I have no financial disclosures I developed and validated one of the models that will be discussed. I hold no patents and derive no financial benefit from
Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008
 Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008 Breast Cancer Most common cancer in American women 180,000 new cases per year Second most common cause of cancer death 44,000
Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008 Breast Cancer Most common cancer in American women 180,000 new cases per year Second most common cause of cancer death 44,000
Assessing Your Patient s Breast Cancer Risk: Is Genetic Testing Necessary?
 May 16, 2016 Assessing Your Patient s Breast Cancer Risk: Is Genetic Testing Necessary? Presenter: Emily Kuchinsky, MS, CGC 1 Experiences with Genetic Testing Adverse Events in Cancer Genetic Testing:
May 16, 2016 Assessing Your Patient s Breast Cancer Risk: Is Genetic Testing Necessary? Presenter: Emily Kuchinsky, MS, CGC 1 Experiences with Genetic Testing Adverse Events in Cancer Genetic Testing:
This information explains the advice about familial breast cancer (breast cancer in the family) that is set out in NICE guideline CG164.
 that is set out in NICE guideline CG164.") Familial breast cancer (breast cancer in the family) Information for the public Published: 1 June 2013 nice.org.uk About this information NICE guidelines provide advice on the care and support that should
Familial breast cancer (breast cancer in the family) Information for the public Published: 1 June 2013 nice.org.uk About this information NICE guidelines provide advice on the care and support that should
Update in Breast Cancer Screening
 Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla Kerlikowske, MD
Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla Kerlikowske, MD
Evaluations & CE Credits
 Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. 1 Breast Density and Breast Cancer
Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. 1 Breast Density and Breast Cancer
Patient Education. Breast Cancer Prevention. Cancer Center
 Patient Education Breast cancer affects one in nine women in the US by the time they reach their 80 s. It is the result of several mutations or alterations in the genes found in the DNA of normal breast
Patient Education Breast cancer affects one in nine women in the US by the time they reach their 80 s. It is the result of several mutations or alterations in the genes found in the DNA of normal breast
Prophylactic Mastectomy
 Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO 07/22/2011 Section: Surgery Place(s) of Service: Inpatient I.
Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO 07/22/2011 Section: Surgery Place(s) of Service: Inpatient I.
Follow-up Issues for Early Stage Breast Cancer: The Role of Surveillance and Long-Term Care
 Follow-up Issues for Early Stage Breast Cancer: The Role of Surveillance and Long-Term Care Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of
Follow-up Issues for Early Stage Breast Cancer: The Role of Surveillance and Long-Term Care Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of
Risk Assessment and Risk Management
 Risk Assessment and Risk Management Epworth Benign Breast Disease Symposium Dr Laura Chin-Lenn 12 November 2016 Why identify those at increased risk of breast cancer? Should I be worried? 1 Why identify
Risk Assessment and Risk Management Epworth Benign Breast Disease Symposium Dr Laura Chin-Lenn 12 November 2016 Why identify those at increased risk of breast cancer? Should I be worried? 1 Why identify
Screening Mammography Policy and Politics. Kevin L. Piggott, MD, MPH August 29, 2015
 Screening Mammography Policy and Politics Kevin L. Piggott, MD, MPH August 29, 2015 Objectives 1. To review the current recommendations for screening mammography by various national groups 2. To provide
Screening Mammography Policy and Politics Kevin L. Piggott, MD, MPH August 29, 2015 Objectives 1. To review the current recommendations for screening mammography by various national groups 2. To provide
MANAGEMENT OF HIGH RISK BREAST PATIENTS DR PAMELA THOMPSON BREAST PHYSICIAN, FSH
 MANAGEMENT OF HIGH RISK BREAST PATIENTS DR PAMELA THOMPSON BREAST PHYSICIAN, FSH HIGH RISK MANAGEMENT OBJECTIVES Be alert to FHx Breast and/or Ovarian cancer Know how to perform a risk assessment Be aware
MANAGEMENT OF HIGH RISK BREAST PATIENTS DR PAMELA THOMPSON BREAST PHYSICIAN, FSH HIGH RISK MANAGEMENT OBJECTIVES Be alert to FHx Breast and/or Ovarian cancer Know how to perform a risk assessment Be aware
Prophylactic Mastectomy
 Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/01/2013 Section: Surgery Place(s) of Service:
Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/01/2013 Section: Surgery Place(s) of Service:
Evaluation & Management of PowerPoint Cover Title. the High Risk Population. High Risk Clinic
 Evaluation & Management of PowerPoint Cover Title the High Risk Population High Risk Clinic Subtitle Joanna Would Springman, Go Here PA-C Assessment Genetics Known genetic mutation Family history with
Evaluation & Management of PowerPoint Cover Title the High Risk Population High Risk Clinic Subtitle Joanna Would Springman, Go Here PA-C Assessment Genetics Known genetic mutation Family history with
Breast Evaluation & Management Guidelines
 Breast Evaluation & Management Guidelines Pamela L. Kurtzhals, M.D. F.A.C.S. Head, Dept. of General Surgery Scripps Clinic, La Jolla Objective Review screening & diagnostic guidelines Focused patient complaints
Breast Evaluation & Management Guidelines Pamela L. Kurtzhals, M.D. F.A.C.S. Head, Dept. of General Surgery Scripps Clinic, La Jolla Objective Review screening & diagnostic guidelines Focused patient complaints
Breast Cancer Screening
 Breast Cancer Screening Claire Frost, MD R3 Talks 1 Objective 1. Understand risks and benefits of screening by reviewing current literature 2. Evaluate major society recommendations on breast cancer screening
Breast Cancer Screening Claire Frost, MD R3 Talks 1 Objective 1. Understand risks and benefits of screening by reviewing current literature 2. Evaluate major society recommendations on breast cancer screening
Original Policy Date
 MP 7.01.06 Prophylactic Mastectomy Medical Policy Section Surgery Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature search/12:2013 Return to Medical Policy Index
MP 7.01.06 Prophylactic Mastectomy Medical Policy Section Surgery Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature search/12:2013 Return to Medical Policy Index
Breast Cancer Screening
 Breast Cancer Screening Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Breast Cancer Screening Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Host Factors that Increase Breast Cancer Risk
 Host Factors that Increase Breast Cancer Risk 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive
Host Factors that Increase Breast Cancer Risk 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive
2/9/2015. The high prevalence of breast disease and breast cancer (i.e. the problem is in every OB/GYN office, every day)
") Breast Cancer: What is the Gynecologist s Role in Detection, Management, and Surveillance? James W. Orr, Jr. M.D. FACOG, FACS Chair, Florida Board of Medicine Medical Director: Regional Cancer Center &
Breast Cancer: What is the Gynecologist s Role in Detection, Management, and Surveillance? James W. Orr, Jr. M.D. FACOG, FACS Chair, Florida Board of Medicine Medical Director: Regional Cancer Center &
RMF BREAST CARE MANAGEMENT ALGORITHM
 RMF BREAST CARE MANAGEMENT ALGORITHM IMPROVING BREAST PATIENT SAFETY 2003 Risk Management Foundation of the Harvard Medical Instititutions page 1 Improving Breast Patient Safety Failure to diagnose breast
RMF BREAST CARE MANAGEMENT ALGORITHM IMPROVING BREAST PATIENT SAFETY 2003 Risk Management Foundation of the Harvard Medical Instititutions page 1 Improving Breast Patient Safety Failure to diagnose breast
POSITION PAPER FOR HEALTH CARE PROVIDERS Use of Pharmacologic Intervention for Breast Cancer Risk Reduction
 P.O. Box 30195 Lansing, MI 48909 Phone: 877-588-6224 FAX: 517-335-9397 www.michigancancer.org Introduction POSITION PAPER FOR HEALTH CARE PROVIDERS Use of Pharmacologic Intervention for Breast Cancer Risk
P.O. Box 30195 Lansing, MI 48909 Phone: 877-588-6224 FAX: 517-335-9397 www.michigancancer.org Introduction POSITION PAPER FOR HEALTH CARE PROVIDERS Use of Pharmacologic Intervention for Breast Cancer Risk
Page 1. Selected Controversies. Cancer Screening! Selected Controversies. Breast Cancer Screening. ! Using Best Evidence to Guide Practice!
 Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Screening Mammograms: Questions and Answers
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
BSO, HRT, and ERT. No relevant financial disclosures
 BSO, HRT, and ERT Jubilee Brown, MD Professor & Associate Director, Gynecologic Oncology Levine Cancer Institute at the Carolinas HealthCare System Charlotte, North Carolina No relevant financial disclosures
BSO, HRT, and ERT Jubilee Brown, MD Professor & Associate Director, Gynecologic Oncology Levine Cancer Institute at the Carolinas HealthCare System Charlotte, North Carolina No relevant financial disclosures
Breast Imaging! Ravi Adhikary, MD!
 Breast Imaging! Ravi Adhikary, MD! ACS Estimated Cancers Statistics 2014! Breast! New Cases in Women! 232,670 (+67,570 in situ)! Deaths in Women! 40,000! Colon! 48,380! 24,040! Cervical! 12,360! 4,020!
Breast Imaging! Ravi Adhikary, MD! ACS Estimated Cancers Statistics 2014! Breast! New Cases in Women! 232,670 (+67,570 in situ)! Deaths in Women! 40,000! Colon! 48,380! 24,040! Cervical! 12,360! 4,020!
Breast Cancer. Breast Cancer. Established breast cancer risk factors. Established breast cancer risk factors. Cancer incidence.
 Breast Cancer A buffet of breast cancer topics Wendy Y. Chen, MD MPH Dana-Farber Cancer Institute Brigham and Women s Hospital Disclosures: none Not related to anything presented in this lecture Wendy
Breast Cancer A buffet of breast cancer topics Wendy Y. Chen, MD MPH Dana-Farber Cancer Institute Brigham and Women s Hospital Disclosures: none Not related to anything presented in this lecture Wendy
BREAST DENSITY WHAT IS IT? WHY IS IT IMPORTANT? & What IOWA SF250 Means to Patients and Providers
 BREAST DENSITY WHAT IS IT? WHY IS IT IMPORTANT? & What IOWA SF250 Means to Patients and Providers Arnold Honick, MD Radiology Consultants of Iowa, PLC ahonick@rciowa.com BREAST DENSITY LEGISLATION Nancy
BREAST DENSITY WHAT IS IT? WHY IS IT IMPORTANT? & What IOWA SF250 Means to Patients and Providers Arnold Honick, MD Radiology Consultants of Iowa, PLC ahonick@rciowa.com BREAST DENSITY LEGISLATION Nancy
Approximately 5% to 10% of breast cancer (BC) is hereditary in nature. Since. By Dawna Gilchrist, MD, FRCPC, FCCMG
 is hereditary in nature. Since. By Dawna Gilchrist, MD, FRCPC, FCCMG") By Dawna Gilchrist, MD, FRCPC, FCCMG Approximately 5% to 10% of breast cancer (BC) is hereditary in nature. Since the discovery of the genes BRCA 1 and 2 in the early 1990s, genetic counselling and testing
By Dawna Gilchrist, MD, FRCPC, FCCMG Approximately 5% to 10% of breast cancer (BC) is hereditary in nature. Since the discovery of the genes BRCA 1 and 2 in the early 1990s, genetic counselling and testing
CLINICAL GUIDELINES. Screening Mammography Guidelines
 CLINICAL GUIDELINES Screening Mammography Guidelines Paula George, M.D. and C. Todd Cunningham, M.D., Karen F. Goodhope, M.D., Valerie C. Reichert, M.D. Hayley Sheldon, M.D., Michelle Walters, D.O. 2/17/2016
CLINICAL GUIDELINES Screening Mammography Guidelines Paula George, M.D. and C. Todd Cunningham, M.D., Karen F. Goodhope, M.D., Valerie C. Reichert, M.D. Hayley Sheldon, M.D., Michelle Walters, D.O. 2/17/2016
Prophylactic Mastectomy
 Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/01/2015 Section: Surgery Place(s) of Service:
Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/01/2015 Section: Surgery Place(s) of Service:
WHAT DO GENES HAVE TO DO WITH IT? Breast Cancer Risk Assessment and Risk Reduction in 2016
 WHAT DO GENES HAVE TO DO WITH IT? Breast Cancer Risk Assessment and Risk Reduction in 2016 39 th Annual CANP Educational Conference March 17 20, 2016 Collaborate. Educate. Advocate. Karen Herold, DNP,
WHAT DO GENES HAVE TO DO WITH IT? Breast Cancer Risk Assessment and Risk Reduction in 2016 39 th Annual CANP Educational Conference March 17 20, 2016 Collaborate. Educate. Advocate. Karen Herold, DNP,
An Update on Breast Cancer Screening and Prevention.
 Thomas Jefferson University Jefferson Digital Commons Department of Family & Community Medicine Faculty Papers Department of Family & Community Medicine 6-2014 An Update on Breast Cancer Screening and
Thomas Jefferson University Jefferson Digital Commons Department of Family & Community Medicine Faculty Papers Department of Family & Community Medicine 6-2014 An Update on Breast Cancer Screening and
The best way of detection of and screening for breast cancer in women with genetic or hereditary risk
 The best way of detection of and screening for breast cancer in women with genetic or hereditary risk Ingrid Vogelaar Introduction Each year almost 1.2 million women are diagnosed with breast cancer worldwide.
The best way of detection of and screening for breast cancer in women with genetic or hereditary risk Ingrid Vogelaar Introduction Each year almost 1.2 million women are diagnosed with breast cancer worldwide.
SCREENING FOR BREAST CANCER BREAST IMAGING
 SCREENING FOR BREAST CANCER BREAST IMAGING Liane Philpotts, MD, FSBI, FACR Professor, Radiology and Biomedical Imaging Division Chief, Breast Imaging Dec. 5, 2017 Warner, E. NEJM 2011 Screening for
SCREENING FOR BREAST CANCER BREAST IMAGING Liane Philpotts, MD, FSBI, FACR Professor, Radiology and Biomedical Imaging Division Chief, Breast Imaging Dec. 5, 2017 Warner, E. NEJM 2011 Screening for
Primary Care Approach to Genetic Cancer Syndromes
 Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
This is a summary of what we ll be talking about today.
 Slide 1 Breast Cancer American Cancer Society Reviewed October 2015 Slide 2 What we ll be talking about How common is breast cancer? What is breast cancer? What causes it? What are the risk factors? Can
Slide 1 Breast Cancer American Cancer Society Reviewed October 2015 Slide 2 What we ll be talking about How common is breast cancer? What is breast cancer? What causes it? What are the risk factors? Can
SBI Breast Imaging Symposium 2016 Austin Texas, April 7, 2016
 Guidelines for Breast Cancer Screening: An Update SBI Breast Imaging Symposium 2016 Austin Texas, April 7, 2016 Robert A. Smith, PhD Cancer Control Department American Cancer Society Atlanta, GA I have
Guidelines for Breast Cancer Screening: An Update SBI Breast Imaging Symposium 2016 Austin Texas, April 7, 2016 Robert A. Smith, PhD Cancer Control Department American Cancer Society Atlanta, GA I have
Shared Decision Making in Breast and Prostate Cancer Screening. An Update and a Patient-Centered Approach. Sharon K. Hull, MD, MPH July, 2017
 Shared Decision Making in Breast and Prostate Cancer Screening An Update and a Patient-Centered Approach Sharon K. Hull, MD, MPH July, 2017 Overview Epidemiology of Breast and Prostate Cancer Controversies
Shared Decision Making in Breast and Prostate Cancer Screening An Update and a Patient-Centered Approach Sharon K. Hull, MD, MPH July, 2017 Overview Epidemiology of Breast and Prostate Cancer Controversies
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Breast MRI: Friend or Foe?
 Breast MRI: Friend or Foe? UCSF Postgraduate Course May 18, 2013 Cheryl Ewing, MD Clinical Professor of Surgery UCSF Department of Surgery APPLEGATE HAS DOUBLE MASTECTOMY IN CANCER SCARE DIAGNOSED WITH
Breast MRI: Friend or Foe? UCSF Postgraduate Course May 18, 2013 Cheryl Ewing, MD Clinical Professor of Surgery UCSF Department of Surgery APPLEGATE HAS DOUBLE MASTECTOMY IN CANCER SCARE DIAGNOSED WITH
Breast density: imaging, risks and recommendations
 Breast density: imaging, risks and recommendations Maureen Baxter, MD Radiologist Director of Ruth J. Spear Breast Center Providence St. Vincent Medical Center Alison Conlin, MD/MPH Medical Oncologist
Breast density: imaging, risks and recommendations Maureen Baxter, MD Radiologist Director of Ruth J. Spear Breast Center Providence St. Vincent Medical Center Alison Conlin, MD/MPH Medical Oncologist
BREAST CANCER SCREENING IS A CHOICE
 BREAST CANCER SCREENING IS A CHOICE by ELAINE SCHATTNER, MD no financial disclosures (ES) American Association for Cancer Research Typical headlines focus on controversy 2 Data: Breast Cancer Incidence
BREAST CANCER SCREENING IS A CHOICE by ELAINE SCHATTNER, MD no financial disclosures (ES) American Association for Cancer Research Typical headlines focus on controversy 2 Data: Breast Cancer Incidence
5/24/16. Current Issues in Breast Cancer Screening. Breast cancer screening guidelines. Outline
 Disclosure information: An Evidence based Approach to Breast Cancer Karla Kerlikowske, MDDis Current Issues in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla
Disclosure information: An Evidence based Approach to Breast Cancer Karla Kerlikowske, MDDis Current Issues in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla
So how much of breast and ovarian cancer is hereditary? A). 5 to 10 percent. B). 20 to 30 percent. C). 50 percent. Or D). 65 to 70 percent.
. 5 to 10 percent. B). 20 to 30 percent. C). 50 percent. Or D). 65 to 70 percent.") Welcome. My name is Amanda Brandt. I am one of the Cancer Genetic Counselors at the University of Texas MD Anderson Cancer Center. Today, we are going to be discussing how to identify patients at high
Welcome. My name is Amanda Brandt. I am one of the Cancer Genetic Counselors at the University of Texas MD Anderson Cancer Center. Today, we are going to be discussing how to identify patients at high
AN EXAMINATION OF CANADIAN FAMILY PHYSICIANS KNOWLEDGE AND PRACTICE PATTERNS REGARDING BREAST CANCER PREVENTION
 AN EXAMINATION OF CANADIAN FAMILY PHYSICIANS KNOWLEDGE AND PRACTICE PATTERNS REGARDING BREAST CANCER PREVENTION by Mary-Kathryn Tighe A thesis submitted to the Department of Community Health and Epidemiology
AN EXAMINATION OF CANADIAN FAMILY PHYSICIANS KNOWLEDGE AND PRACTICE PATTERNS REGARDING BREAST CANCER PREVENTION by Mary-Kathryn Tighe A thesis submitted to the Department of Community Health and Epidemiology
Hereditary Breast and Ovarian Cancer Rebecca Sutphen, MD, FACMG
 Hereditary Breast and Ovarian Cancer 2015 Rebecca Sutphen, MD, FACMG Among a consecutive series of 11,159 women requesting BRCA testing over one year, 3874 responded to a mailed survey. Most respondents
Hereditary Breast and Ovarian Cancer 2015 Rebecca Sutphen, MD, FACMG Among a consecutive series of 11,159 women requesting BRCA testing over one year, 3874 responded to a mailed survey. Most respondents
Hereditary breast cancer who to refer to a cancer genetics clinic and how to counsel patients with
 Hereditary breast cancer who to refer to a cancer genetics clinic and how to counsel patients with positive and negative results? SAMO Workshop Luzern 3./4.10.2014 Dr. med. Barbara Bolliger TumorTumor-
Hereditary breast cancer who to refer to a cancer genetics clinic and how to counsel patients with positive and negative results? SAMO Workshop Luzern 3./4.10.2014 Dr. med. Barbara Bolliger TumorTumor-
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Breast Cancer Screening Clinical Practice Guideline. Kaiser Permanente National Breast Cancer Screening Guideline Development Team
 NATIONAL CLINICAL PRACTICE GUIDELINE Breast Cancer Screening Clinical Practice Guideline Kaiser Permanente National Breast Cancer Screening Guideline Development Team This guideline is informational only.
NATIONAL CLINICAL PRACTICE GUIDELINE Breast Cancer Screening Clinical Practice Guideline Kaiser Permanente National Breast Cancer Screening Guideline Development Team This guideline is informational only.
Screening Mammography: Who, what, where, when, why and how?
 Screening Mammography: Who, what, where, when, why and how? Jillian Lloyd, MD, MPH Breast Surgical Oncologist University Surgical Oncology Department of Surgery University of Tennessee Medical Center Disclosures
Screening Mammography: Who, what, where, when, why and how? Jillian Lloyd, MD, MPH Breast Surgical Oncologist University Surgical Oncology Department of Surgery University of Tennessee Medical Center Disclosures
Breast Cancer. American Cancer Society
 Breast Cancer American Cancer Society Reviewed February 2017 What we ll be talking about How common is breast cancer? What is breast cancer? What causes it? What are the risk factors? Can breast cancer
Breast Cancer American Cancer Society Reviewed February 2017 What we ll be talking about How common is breast cancer? What is breast cancer? What causes it? What are the risk factors? Can breast cancer
Karen degenevieve MSN, FNP, BC
 Karen degenevieve MSN, FNP, BC Become more comfortable treating common breast complaints. Discuss recent controversial screening recommendations. Discuss oral medications used in breast cancer prevention
Karen degenevieve MSN, FNP, BC Become more comfortable treating common breast complaints. Discuss recent controversial screening recommendations. Discuss oral medications used in breast cancer prevention
Utilization of BRCA Testing. Breast and Ovarian Cancer in Texas
 Utilization of BRCA Testing in Older Ode Women with Breast and Ovarian Cancer in Texas Ana M. Rodriguez, MD Assistant Professor Department of Obstetrics and Gynecology University of Texas Medical Branch
Utilization of BRCA Testing in Older Ode Women with Breast and Ovarian Cancer in Texas Ana M. Rodriguez, MD Assistant Professor Department of Obstetrics and Gynecology University of Texas Medical Branch
Clinical guideline Published: 25 June 2013 nice.org.uk/guidance/cg164
 Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer Clinical guideline Published: 25 June 2013 nice.org.uk/guidance/cg164
Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer Clinical guideline Published: 25 June 2013 nice.org.uk/guidance/cg164
North American Menopause Society (NAMS)
") North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
BAYLOR SCOTT & WHITE HEALTH GENETICS QUESTIONNAIRE PATIENT INFORMATION
 PATIENT INFORMATION Name: Address: (Last) (First) (Middle) (Street) (City) (State) (Zip) Home Phone: Cell Phone: Email Address: Birth Date: Age: When is the best time to contact you? May we email you for
PATIENT INFORMATION Name: Address: (Last) (First) (Middle) (Street) (City) (State) (Zip) Home Phone: Cell Phone: Email Address: Birth Date: Age: When is the best time to contact you? May we email you for
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY
 EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
Tissue Breast Density
 Tissue Breast Density Reporting breast density within the letter to the patient is now mandated by VA law. Therefore, this website has been established by Peninsula Radiological Associates (PRA), the radiologists
Tissue Breast Density Reporting breast density within the letter to the patient is now mandated by VA law. Therefore, this website has been established by Peninsula Radiological Associates (PRA), the radiologists
Breast Cancer Risk Assessment among Bahraini Women. Majida Fikree, MD, MSc* Randah R Hamadeh, BSc, MSc, D Phil (Oxon)**
**") Bahrain Medical Bulletin, Vol. 35, No.1, March 2013 Breast Cancer Risk Assessment among Bahraini Women Majida Fikree, MD, MSc* Randah R Hamadeh, BSc, MSc, D Phil (Oxon)** Objective: To estimate breast
Bahrain Medical Bulletin, Vol. 35, No.1, March 2013 Breast Cancer Risk Assessment among Bahraini Women Majida Fikree, MD, MSc* Randah R Hamadeh, BSc, MSc, D Phil (Oxon)** Objective: To estimate breast
Breast Cancer Imaging
 Breast Cancer Imaging I. Policy University Health Alliance (UHA) will cover breast imaging when such services meet the medical criteria guidelines (subject to limitations and exclusions) indicated below.
Breast Cancer Imaging I. Policy University Health Alliance (UHA) will cover breast imaging when such services meet the medical criteria guidelines (subject to limitations and exclusions) indicated below.
BRCA Precertification Information Request Form
 BRCA Precertification Information Request Form Failure to complete this form in its entirety may result in the delay of review. Fax to: BRCA Precertification Department Fax number: 1-860-975-9126 Section
BRCA Precertification Information Request Form Failure to complete this form in its entirety may result in the delay of review. Fax to: BRCA Precertification Department Fax number: 1-860-975-9126 Section
Improving the Identification of Underserved Women at High Risk for Breast Cancer and Increasing the use of Breast MRI Screening in this Population
 Improving the Identification of Underserved Women at High Risk for Breast Cancer and Increasing the use of Breast MRI Screening in this Population Greenwood HI, Truong L, Price ER. UCSF Department or Radiology
Improving the Identification of Underserved Women at High Risk for Breast Cancer and Increasing the use of Breast MRI Screening in this Population Greenwood HI, Truong L, Price ER. UCSF Department or Radiology
Page 1. Cancer Screening for Women I have no conflicts of interest. Overview. Breast, Colon, and Lung Cancer. Jeffrey A.
 Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Current Status of Supplementary Screening With Breast Ultrasound
 Current Status of Supplementary Screening With Breast Ultrasound Stephen A. Feig, M.D., FACR Fong and Jean Tsai Professor of Women s Imaging Department of Radiologic Sciences University of California,
Current Status of Supplementary Screening With Breast Ultrasound Stephen A. Feig, M.D., FACR Fong and Jean Tsai Professor of Women s Imaging Department of Radiologic Sciences University of California,
Patient Information. Name: (Last) (First) (Middle) Address: (Street) (City) (State) (Zip) Home Phone: Cell Phone: address:
 (First) (Middle) Address: (Street) (City) (State) (Zip) Home Phone: Cell Phone: address:") Patient Information Name: (Last) (First) (Middle) Address: (Street) (City) (State) (Zip) Home Phone: Cell Phone: Email address: Birth date: _ Age: Social Security.: When is the best time to contact you?
Patient Information Name: (Last) (First) (Middle) Address: (Street) (City) (State) (Zip) Home Phone: Cell Phone: Email address: Birth date: _ Age: Social Security.: When is the best time to contact you?
Management of BRCA Positive Breast Cancer. Archana Ganaraj, MD February 17, 2018 UPDATE ON WOMEN S HEALTH
 Management of BRCA Positive Breast Cancer Archana Ganaraj, MD February 17, 2018 UPDATE ON WOMEN S HEALTH The number of American women who have lost their lives to breast cancer outstrips the total number
Management of BRCA Positive Breast Cancer Archana Ganaraj, MD February 17, 2018 UPDATE ON WOMEN S HEALTH The number of American women who have lost their lives to breast cancer outstrips the total number
Breast Cancer Prevention
 Breast Cancer Prevention TREVOR J. POWLES Royal Marsden NHS Trust, and Institute of Cancer Research, London, United Kingdom Key Words. Breast cancer Chemoprevention Tamoxifen Raloxifene ABSTRACT Epidemiological,
Breast Cancer Prevention TREVOR J. POWLES Royal Marsden NHS Trust, and Institute of Cancer Research, London, United Kingdom Key Words. Breast cancer Chemoprevention Tamoxifen Raloxifene ABSTRACT Epidemiological,
Follow-up Care of Breast Cancer Patients
 Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures
Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures