Management of Colorectal Liver Metastases
|
|
|
- Angel Tucker
- 5 years ago
- Views:
Transcription


1 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town
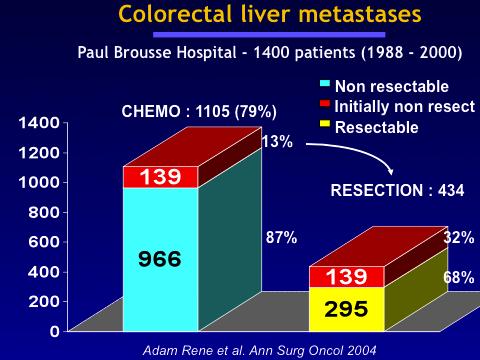
2 50% of patients with colorectal cancer develop liver metastasis 30% present with synchronous liver metastasis In 40% of cases the liver is the only site of metastasis Liver metastasis resectable in 10-20% of cases
3 Rationale for surgery in colorectal Five year survival after resection of liver metastasis is 30% liver metastasis Only chance of long term survival J Clin Oncol 2009;27:3677
4 Years
 Extraheptic disease None are")
5 Resectability Complete (R0) resection with a liver remnant consisting of at least two segments with preserved inflow, outflow and biliary drainage. Volume of liver remnant should not be less than 20-30% of total liver volume Traditional Contraindications Bilobar disease > 4 liver metastases Large tumours (>10cm) Extraheptic disease None are considered an absolute contraindication although they do have prognostic significance Primary and extra hepatic disease should be resectable
 Extensive intra-hepatic disease Inadequate residual volume after an R0 resection Caudate lobe involving the IVC Portal vein confluence")
6 When is surgery contraindicated Unfit for surgery Uncontrolled primary disease Untreatable extra-hepatic disease Untreatable extra-hepatic disease includes Widespread pulmonary disease Peritoneal disease Extensive nodal disease (retroperitoneal or portal) Extensive intra-hepatic disease Inadequate residual volume after an R0 resection Caudate lobe involving the IVC Portal vein confluence Hepatic veins and IVC involved

7
8 When is surgery appropriate? Controllable extrahepatic disease Resectable/ablatable pulmonary disease Resectable isolated extrahepatic sites, spleen adrenal Local direct extension involving diaphragm, adrenal
9 Preoperative evaluation Accurate staging is essential Biopsy of a liver lesion is not necessary CT Sensitivity 75% J Clin Oncol 2010;102:909 MRI Sensitivity 81% Contrast MRI is the best modality for detection and charecterisation of liver lesions FDG-PET most sensitive means of demonstrating extra hepatic disease May restage up to 28% of patients More likely to change management with increasing disease severity

10 Uni- or bilobar mets? Hepatic veins clear? Portal vein clear? Hepatic artery clear? Bile duct clear? Residual liver volume? Rule of thumb: 2 segments plus caudate 30% if normal liver 40% if chemotherapy

11 Chemotherapy Recurrence = Achilles heel of liver resection Recurrent disease develops in 70% of patients who undergo a liver resection Chemotherapy has been shown to improve survival Timing of the chemotherapy remains controversial Conversion chemotherapy - chemotherapy is given to downsize potentially resectable metastasis into resectable disease
12 Chemotherapy related liver toxicity Irinotecan chemotherapy-associated steatohepatitis (CASH) Oxaliplatin sinusoidal obstruction syndrome Bevacizumab impaired wound healing and liver regeneration

13 Steatosis and sinusoidal dilatation Balance between an adequate resection margin and sufficient residual liver volume Preserve residual liver volume after chemotherapy
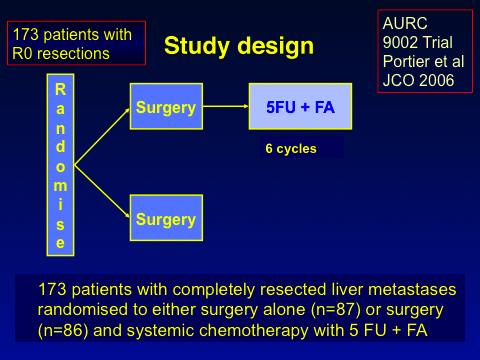
14 Postoperative Chemotherapy
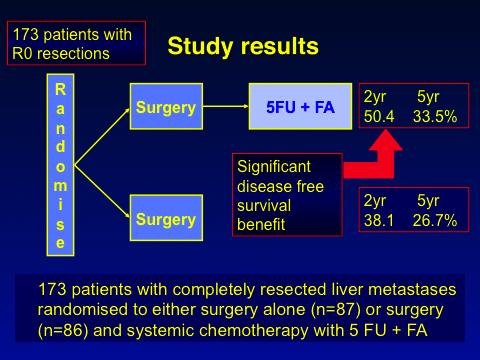
15 Postoperative Chemotherapy

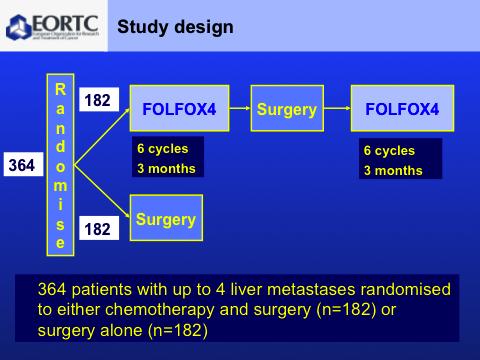
16 Preoperative chemotherapy
17
18
19 Results Surgery only 84% had successful resections 11% non-therapeutic laparotomy rate 5y progression free survival 28% 5y overall survival 48% Perioperative chemotherapy 83% had successful resections 67/182 had an objective response (4 complete) 11/182 progressed on chemo 5% non-therapeutic laparotomy rate 5y progression free survival 35% 5y overall survival 52%



20 Conversion Chemotherapy Conversion of initially irresectable hepatic metastasis into resectable disease ( Conversion Chemo) Definition of initially unresectable is subjective Conversion rates of 5-40%
21

22 Complete Radiological Response
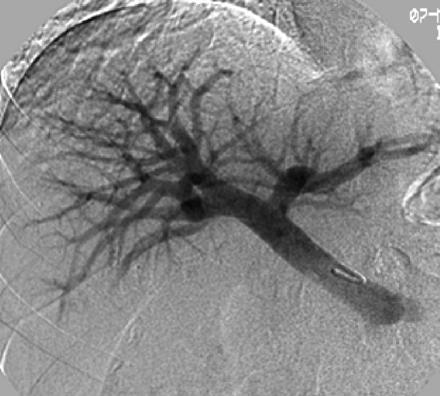
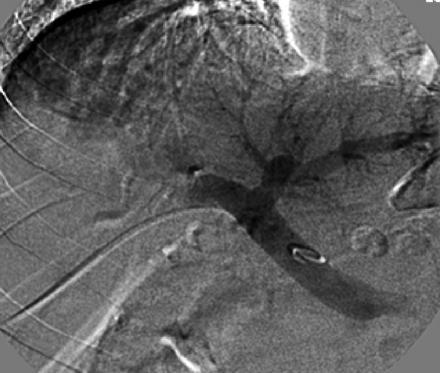
23 Strategies to prevent postoperative liver failure Risk of postoperative liver failure is greatest with extensive liver resections functional residual volume < 30% Portal Vein Embolisation Ipsilateral atrophy, contralateral hypertrophy Gelfoam, lipiodol, cyanoacrylate, fibrin Increase in volume 15% of total liver volume Maximum effect 3-9weeks Staged resection Multiple bilobar disease Clearance of one hemiliver followed by embolistion of the contralateral side Resection of the contralateral side
24
25 Timing of Resection Patients with synchronous liver metastasis have traditionally had staged surgery Synchronous resection can be safely performed Usually reserved for simple resections E.g. Right hemicolectomy/ segment 2/3 resection
 Ethanol Microwave")
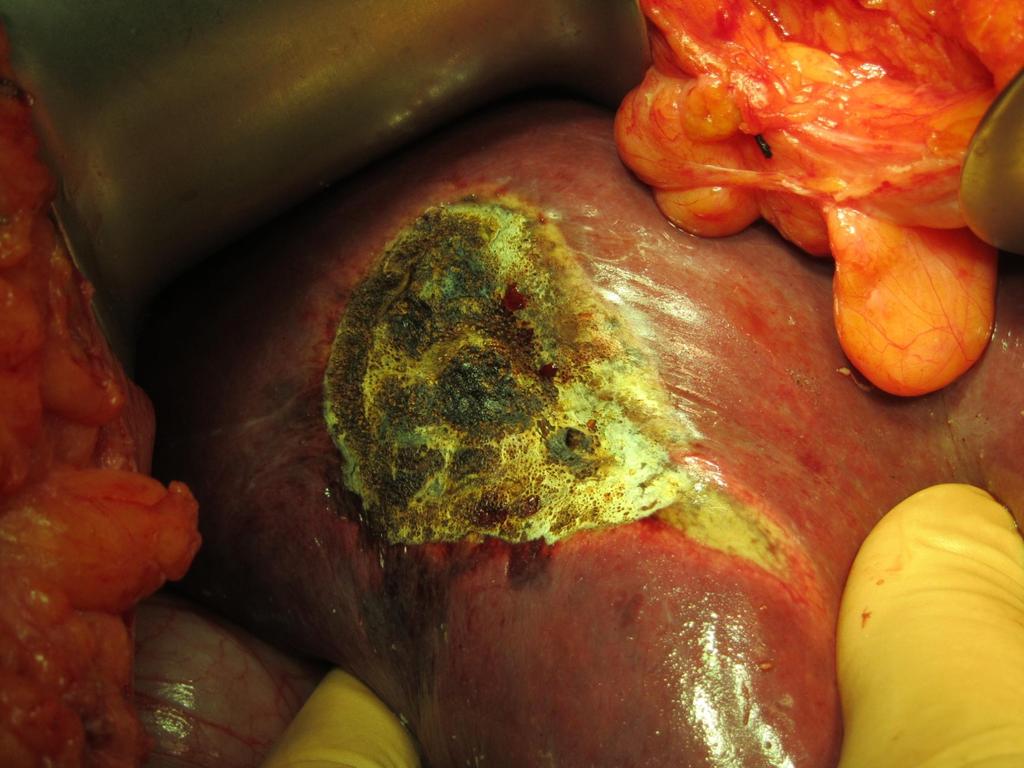
26 Ablative Therapy Thermo-ablative Chemo-ablative Cryotherapy Acetic acid Radiofrequency ablation (RFA) Ethanol Microwave Ablation


27 Ablative Therapy Radiofrequency Ablation Alternating current with frequency of KHz Oscillation of tissue ions causes frictional heat coagulative necrosis Microwave Ablation Microwaves with a frequency of 900MHz Agitate water molecules causing frictional heat and coagulative necrosis Quicker than RFA Not limited by tissue desiccation
28 Ablative Therapy Open, laparoscopic or percutaneous Lack of good evidence. No randomised trial comparing ablation to resection Higher local recurrence rate, inferior disease free survival Liver metastasis not amenable to curative resection Location Multifocality Inadequate hepatic reserve
29 Complications Biloma Abscess Thermal injury to surrounding structures Haemorrhage Haemobilia


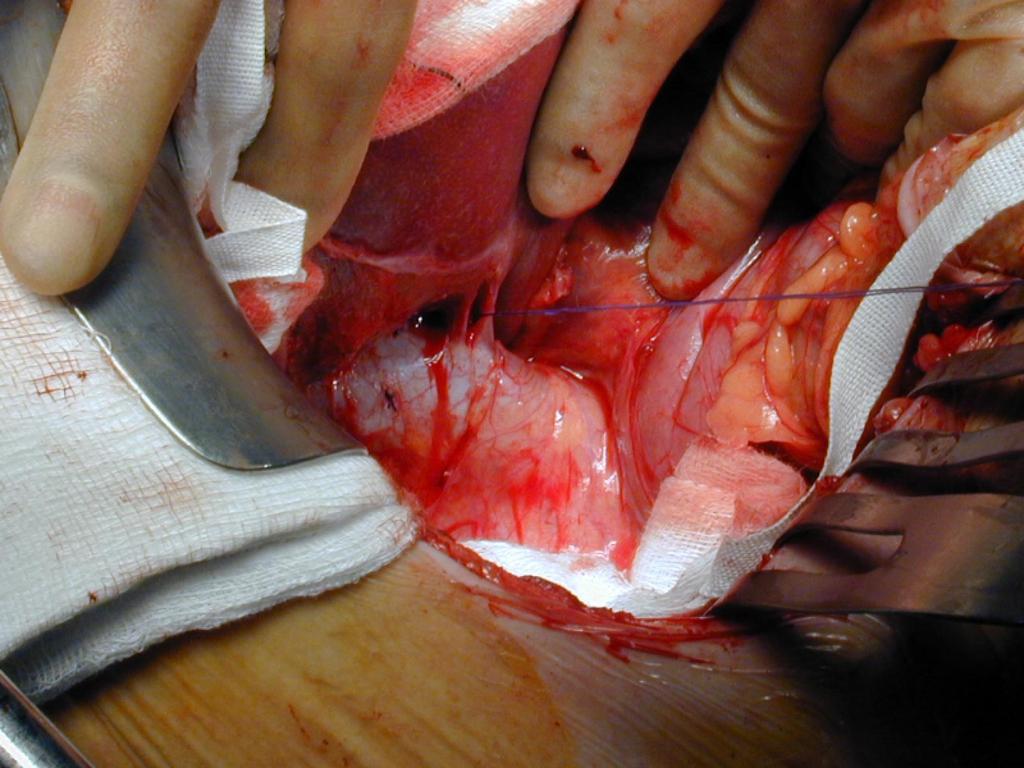
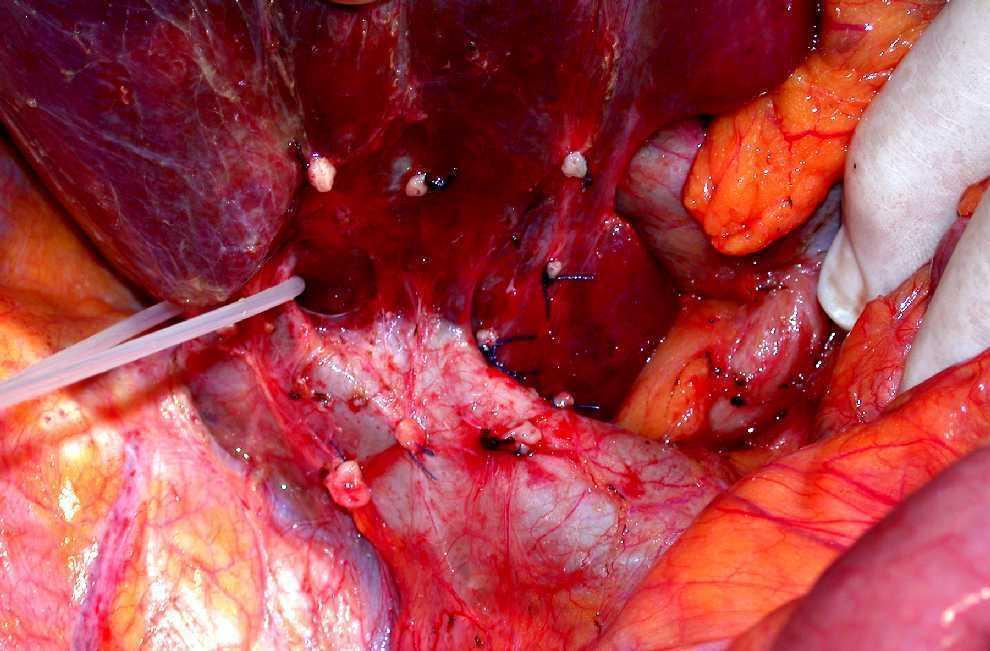
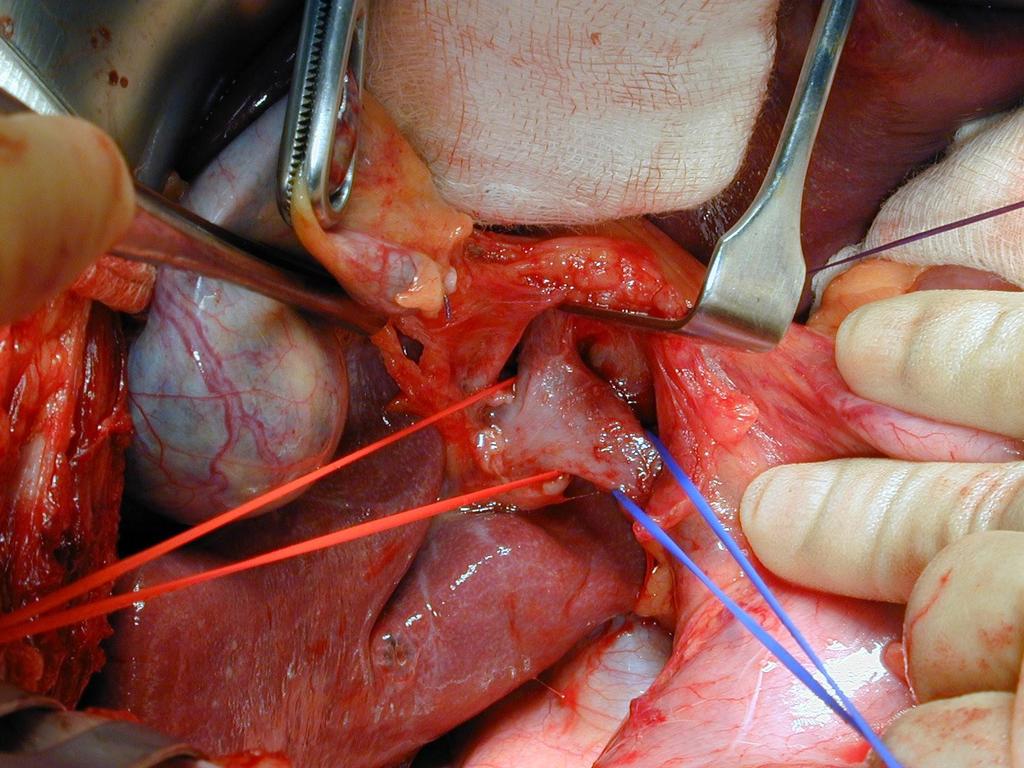
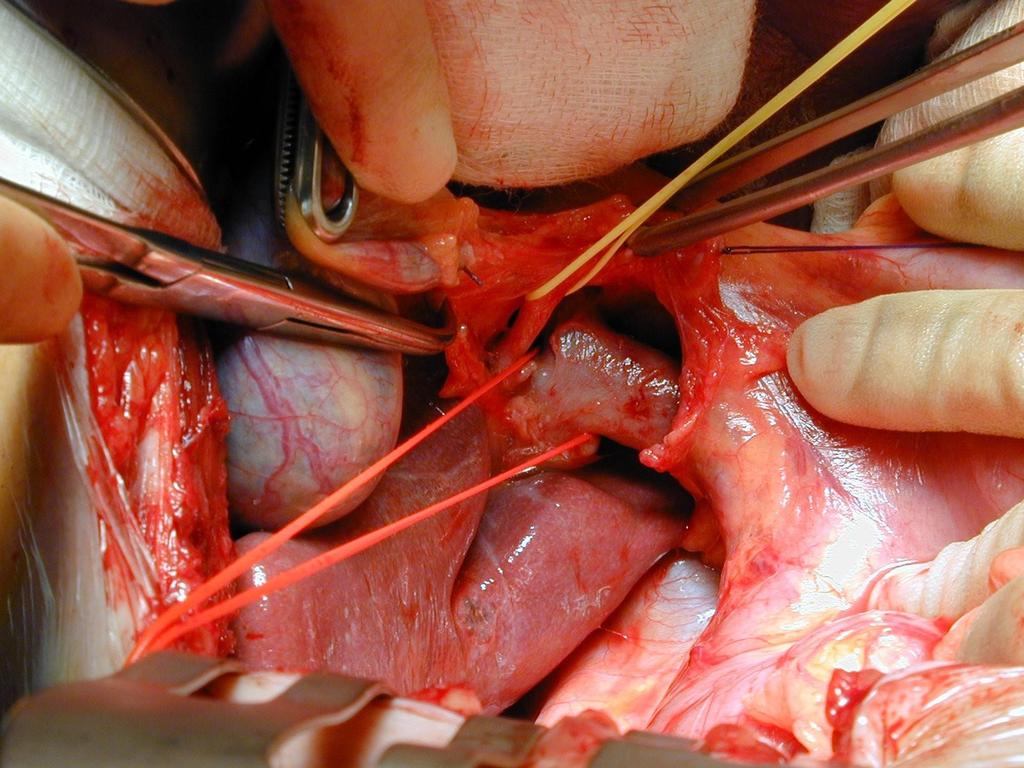
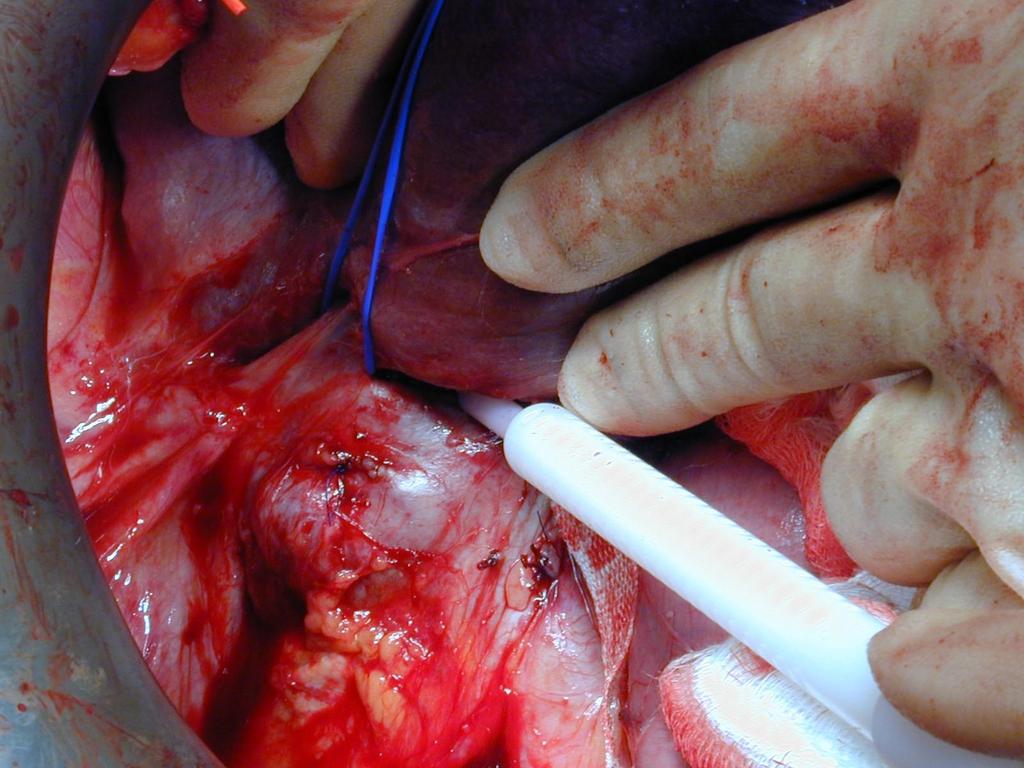
30 53 y old female T3 Rectal adenocarcinoma 7cm above anal verge Synchronous liver met Pre-operative radiotherapy


31 Synchronous anterior resection and microwave ablation of liver lesion
32


33 Developed a liver abscess 14 days after the procedure

34 Managed with percutaneous drainage

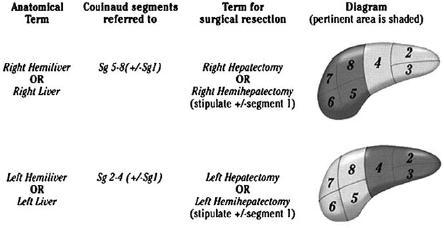
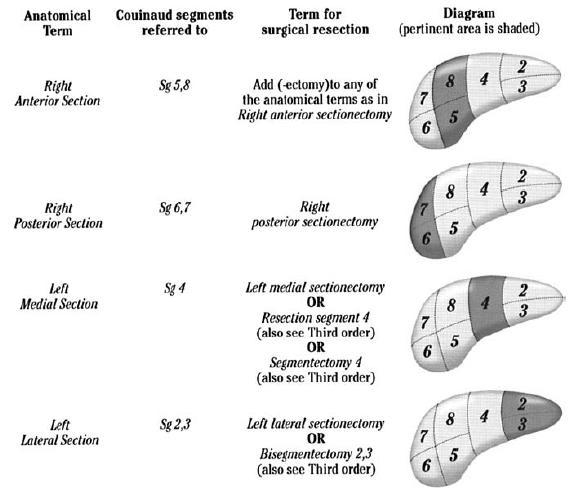
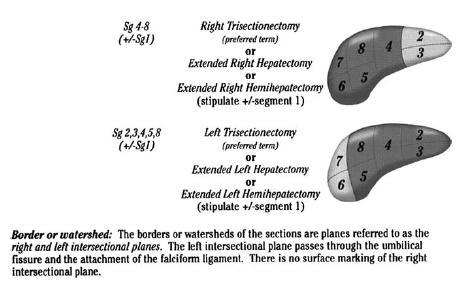
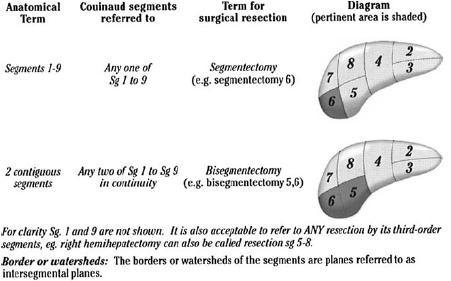
35 Hepatic anatomy and nomenclature of resections
36
37
38
39
40 Technique Basic steps in liver resection Exposure/Mobilise liver Intra-operative assessment (including intraoperative ultrasound) Vascular control Parenchymal transection Seal cut surface/haemostasis
41

42
43
44
45
46
47
48
49

50 Parenchymal Transection

51 How to stay out of trouble Minimise blood loss Avoid prolonged ischaemia Resect tumour with adequate margin Preserve sufficient functional residual liver

52 LIVER RESECTION ACCORDING TO PATHOLOGY n = 356 GSH + UCT PAH - HPB unit All liver resections entered on a prospective data base which includes 1º and 2º pathology, operative details, blood loss, transfusion requirements, complications, survival, etc THE BIG THREE n = 240 Accurate audit and assessment of performance


53 Complications Series of 173 patients at Groote Schuur Peri-operative mortality 2.9% Major Morbidity -19% Bile leak Subphrenic/perihepatic collection Bleeding requiring re-laparotomy Liver failure all patients had extended resections

")
54 Complications Major vs. Minor Resections (%) 122/173 (70.9)
55 Complex procedures best carried out in high volume centers with the appropriate expertise Conclusion Liver resection for colorectal liver metastasis prolongs survival and is the only treatment associated with long term survival A multimodality approach offers the best results and patients should be discussed in multi disciplinary team meeting
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
The Surgical Management of Colorectal Metastases
 11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
How to integrate surgery in the treatment of patients with liver-only metastatic disease
 How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy
 Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
TIMOTHY M. PAWLIK, RICHARD D. SCHULICK, MICHAEL A. CHOTI
 The Oncologist Hepatobiliary Expanding Criteria for Resectability of Colorectal Liver Metastases TIMOTHY M. PAWLIK,RICHARD D. SCHULICK,MICHAEL A. CHOTI Department of Surgery, Johns Hopkins University School
The Oncologist Hepatobiliary Expanding Criteria for Resectability of Colorectal Liver Metastases TIMOTHY M. PAWLIK,RICHARD D. SCHULICK,MICHAEL A. CHOTI Department of Surgery, Johns Hopkins University School
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Trattamento chirurgico delle lesioni epatiche secondarie difficili. Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica
 Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
LiverGroup.org. Case Report Form (CRF) for STAGED procedures
 for STAGED procedures") Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Liver surgery for colorectal liver metastases. Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham
 Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers
 Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Colorectal Liver Metastases Metachronous
 Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer
 Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
LIVER SURGERY 2. Case 1. Med 5 Refresher Course (Surgery) 2013/14. Dr Sunny Cheung
 2013/14. Dr Sunny Cheung") LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
Dr Adam Bartlett. General Surgeon Senior Lecturer University of Auckland Auckland City Hospital
 Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Radiofrequency Ablation of Liver Tumors
 Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases
 Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Radiofrequency Ablation versus Microwave Ablation in HCC and Liver Metastases Thomas J. Vogl, B. Panahi, N. Nour-Eldin I D I R: Institute of Diagnostic and Interventional Radiology Goethe University Frankfurt,
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D.
 Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
6 th August 2018 Day 1 - Gallbladder & Bile duct Topic
 Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Ruolo della interventistica per le secondarietà epatiche e di altre sedi
 Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
How to deal with synchronous primary and liver metastases
 How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
Patient Selection for Ablative Therapies. Adrian D Joyce Leeds UK
 Patient Selection for Ablative Adrian D Joyce Leeds UK Therapy Renal Cell Ca USA: 30,000 new cases annually >12,000 deaths RCC accounts for 3% of all adult malignancy 40% of patients will die from their
Patient Selection for Ablative Adrian D Joyce Leeds UK Therapy Renal Cell Ca USA: 30,000 new cases annually >12,000 deaths RCC accounts for 3% of all adult malignancy 40% of patients will die from their
Management of Stage IV Colorectal Cancer: Expanding the Horizon
 Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
RF Ablation: indication, technique and imaging follow-up
 RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
Regional Therapy for Metastatic Neuroendocrine Tumors. Janette Durham, MD Professor of Radiology University of Colorado School of Medicine
 Regional Therapy for Metastatic Neuroendocrine Tumors Janette Durham, MD Professor of Radiology University of Colorado School of Medicine Introduce regional therapy for mnet Arterial therapies Injection
Regional Therapy for Metastatic Neuroendocrine Tumors Janette Durham, MD Professor of Radiology University of Colorado School of Medicine Introduce regional therapy for mnet Arterial therapies Injection
Original article: new surgical approaches to the Klatskin tumour
 Alimentary Pharmacology & Therapeutics Original article: new surgical approaches to the Klatskin tumour T. M. VAN GULIK*, S. DINANT*, O. R. C. BUSCH*, E. A. J. RAUWS, H. OBERTOP* & D. J. GOUMA Departments
Alimentary Pharmacology & Therapeutics Original article: new surgical approaches to the Klatskin tumour T. M. VAN GULIK*, S. DINANT*, O. R. C. BUSCH*, E. A. J. RAUWS, H. OBERTOP* & D. J. GOUMA Departments
Synchronous Hepatic Cryotherapy and Resection
 HPB Surgery, 2000, Vol. 11, pp. 379-382 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
HPB Surgery, 2000, Vol. 11, pp. 379-382 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age. Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010
 Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Aintree University Hospital
 Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
pitfall Table 1 4 disorientation pitfall pitfall Table 1 Tel:
 11 687 692 2002 pitfall 1078 29 17 9 1 2 3 dislocation outflow block 11 1 2 3 9 1 2 3 4 disorientation pitfall 11 687 692 2002 Tel: 075-751-3606 606-8507 54 2001 8 27 2002 10 31 29 4 pitfall 16 1078 Table
11 687 692 2002 pitfall 1078 29 17 9 1 2 3 dislocation outflow block 11 1 2 3 9 1 2 3 4 disorientation pitfall 11 687 692 2002 Tel: 075-751-3606 606-8507 54 2001 8 27 2002 10 31 29 4 pitfall 16 1078 Table
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
General summary GENERAL SUMMARY
 General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
HOW I DO IT Feasibility of Bisegmentectomy 7 8 is Independent of the Presence of a Large Inferior Right Hepatic Vein
 Journal of Surgical Oncology 2006;93:338 342 HOW I DO IT Feasibility of Bisegmentectomy 7 8 is Independent of the Presence of a Large Inferior Right Hepatic Vein MARCEL AUTRAN C. MACHADO, MD, 1,2 * PAULO
Journal of Surgical Oncology 2006;93:338 342 HOW I DO IT Feasibility of Bisegmentectomy 7 8 is Independent of the Presence of a Large Inferior Right Hepatic Vein MARCEL AUTRAN C. MACHADO, MD, 1,2 * PAULO
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
Liver surgery, acute GI tract bleeding
 Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
HEPATECTOMY. Surgical Potpourri Session. ACS NSQIP National Conference Salt Lake City 2012
 HEPATECTOMY Surgical Potpourri Session ACS NSQIP National Conference Salt Lake City 2012 Pascal Fuchshuber, MD, PhD, FACS Kaiser Permanente Medical Center Walnut Creek - California Hepatic Resection Is
HEPATECTOMY Surgical Potpourri Session ACS NSQIP National Conference Salt Lake City 2012 Pascal Fuchshuber, MD, PhD, FACS Kaiser Permanente Medical Center Walnut Creek - California Hepatic Resection Is
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Management of Patients with Suspected Cholangiocarcinoma CLINICAL GUIDELINES
 London Cancer Hepatic Pancreatic and Biliary (HPB) Faculty Management of Patients with Suspected Cholangiocarcinoma CLINICAL GUIDELINES JULY 2014 This operational policy is agreed and accepted by: Designated
London Cancer Hepatic Pancreatic and Biliary (HPB) Faculty Management of Patients with Suspected Cholangiocarcinoma CLINICAL GUIDELINES JULY 2014 This operational policy is agreed and accepted by: Designated
RFA of Tumors of the Lung: How and Why. Radiofrequency Ablation. Radiofrequency Ablation. RFA of pulmonary metastases. Radiofrequency Ablation of Lung
 RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Disclosure. Nothing to Disclose Will not be discussing off label use of any of the medications
 Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
Liver Cancer: Diagnosis and Treatment Options
 Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Metastatic Liver Cancer
 4 Metastatic Liver Cancer ANDREW J. SMITH, MD, FRCSC RONALD P. DEMATTEO, MD YUMAN FONG, MD, FACS LESLIE H. BLUMGART, MD, FACS, FRCS (ENG, EDIN, GLAS) The management of hepatic metastases has become more
4 Metastatic Liver Cancer ANDREW J. SMITH, MD, FRCSC RONALD P. DEMATTEO, MD YUMAN FONG, MD, FACS LESLIE H. BLUMGART, MD, FACS, FRCS (ENG, EDIN, GLAS) The management of hepatic metastases has become more
Published: Address correspondence to Vidal-Jove Joan:
 Oncothermia Journal 7:111-114 (2013) Complete responses after hyperthermic ablation by ultrasound guided high intensity focused ultrasound (USgHIFU) plus cystemic chemotherapy (SC) for locally advanced
Oncothermia Journal 7:111-114 (2013) Complete responses after hyperthermic ablation by ultrasound guided high intensity focused ultrasound (USgHIFU) plus cystemic chemotherapy (SC) for locally advanced
Corporate Medical Policy
 Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
Therapeutic Value of Radiofrequency Ablation of Hepatic Malignant Tumors
 Therapeutic Value of Radiofrequency Ablation of Hepatic Malignant Tumors Student: Shazia Hussain, V-01 Supervisor: Trond Buanes (Ullevål universitetssykehus) Universitetet i Oslo Det medisinske fakultet
Therapeutic Value of Radiofrequency Ablation of Hepatic Malignant Tumors Student: Shazia Hussain, V-01 Supervisor: Trond Buanes (Ullevål universitetssykehus) Universitetet i Oslo Det medisinske fakultet
3/28/2012. Periampullary Tumors. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Eric K. Nakakura Ko Olina, HI
 Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies
 HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Liver related complications in unresectable disease after portal vein embolization
 Original Article Liver related complications in unresectable disease after portal vein embolization Floor Huisman 1, Kasia P. Cieslak 1, Krijn P. van Lienden 2, Roelof J. Bennink 3, Thomas M. van Gulik
Original Article Liver related complications in unresectable disease after portal vein embolization Floor Huisman 1, Kasia P. Cieslak 1, Krijn P. van Lienden 2, Roelof J. Bennink 3, Thomas M. van Gulik
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Behandeling van colorectale levermetastasen. Rol van beeldvorming van de lever bij colorectaal carcinoom
 Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Primary tumor with synchronous metastases
 Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
Horizon Scanning in Surgery: Application to Surgical Education and Practice
 Horizon Scanning in Surgery: Application to Surgical Education and Practice Microwave ablation for hepatic metastases December 2012 American College of Surgeons Division of Education Prepared by the Australian
Horizon Scanning in Surgery: Application to Surgical Education and Practice Microwave ablation for hepatic metastases December 2012 American College of Surgeons Division of Education Prepared by the Australian
Long R. Jiao, David N. Hakim, Tamara M. H. Gall, Ana Fajardo, Tim D. Pencavel, Ruifang Fan, Mikael H. Sodergren
 How We Do It A totally laparoscopic associating liver partition and portal vein ligation for staged hepatectomy assisted with radiofrequency (radiofrequency assisted liver partition with portal vein ligation)
How We Do It A totally laparoscopic associating liver partition and portal vein ligation for staged hepatectomy assisted with radiofrequency (radiofrequency assisted liver partition with portal vein ligation)
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
RADIOFREQUENCY ABLATION
 RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Variations in portal and hepatic vein branching of the liver
 Yamagata Med J (ISSN 0288-030X)2015;33(2):115-121 DOI 10.15022/00003476 Variations in portal and hepatic vein branching of the liver Wataru Kimura, Tsuyoshi Fukumoto, Toshihiro Watanabe, Ichiro Hirai First
Yamagata Med J (ISSN 0288-030X)2015;33(2):115-121 DOI 10.15022/00003476 Variations in portal and hepatic vein branching of the liver Wataru Kimura, Tsuyoshi Fukumoto, Toshihiro Watanabe, Ichiro Hirai First
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
To evaluate 792 patients with malignant biliary obstruction after inner-stents drainage procedure
 To evaluate 792 patients with malignant biliary obstruction after inner-stents drainage procedure Zhu wei, Zhang xiquan, Pan xiaolin, Dong ge, Guo feng. The Cardio-Interventional Center, The 148th PLA
To evaluate 792 patients with malignant biliary obstruction after inner-stents drainage procedure Zhu wei, Zhang xiquan, Pan xiaolin, Dong ge, Guo feng. The Cardio-Interventional Center, The 148th PLA
Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy
 Original Article Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy Rebecca C. Auer, MD 1 ; Rebekah R. White, MD 2 ; Nancy E. Kemeny, MD
Original Article Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy Rebecca C. Auer, MD 1 ; Rebekah R. White, MD 2 ; Nancy E. Kemeny, MD
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Colorectal Cancer and FDG PET/CT
 Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Current Treatment Strategies for Hilar and Intrahepatic Cholangiocarcinoma
 Current Treatment Strategies for Hilar and Intrahepatic Cholangiocarcinoma Jean-Nicolas Vauthey, MD, FACS Professor of Surgery Chief Hepato-Pancreato-Biliary Section Department of Surgical Oncology Crescent
Current Treatment Strategies for Hilar and Intrahepatic Cholangiocarcinoma Jean-Nicolas Vauthey, MD, FACS Professor of Surgery Chief Hepato-Pancreato-Biliary Section Department of Surgical Oncology Crescent
Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma
 Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma Taylor S. Riall, MD, PhD CERCIT Workshop October 19, 2012 Department of Surgery Center for Comparative Effectiveness
Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma Taylor S. Riall, MD, PhD CERCIT Workshop October 19, 2012 Department of Surgery Center for Comparative Effectiveness
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Guidelines on Renal Cell
 Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
SECONDARIES: A PRELIMINARY REPORT
 HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical management of HCC. Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London
 Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE METASTASES
 LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
Posthepatectomy Liver Failure. C. Jeske
 Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following
Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following