Malignant Breast disorders
|
|
|
- Noah Gaines
- 5 years ago
- Views:
Transcription
1 Malignant Breast disorders
2 RISK FACTORS FOR BREAST CANCER Family Hx.: first- and second-degree relatives with breast cancer and their age at diagnosis.
3 RISK FACTORS FOR BREAST CANCER (cont.) Hormonal Risk Factors exposure to estrogen risk for breast cancer: -factors that increase the number of menstrual cycles, such as early menarche, nulliparity, and late menopause, are associated with increased risk. -obesity is associated increased breast cancer risk. Because the major source of estrogen in postmenopausal women is the conversion of androstenedione to estrone by adipose tissue, obesity is associated with a long-term increase in estrogen exposure. -so older age at first live birth is associated with an increased risk of breast cancer whereas exposure thought to be protective. -Moderate levels of exercise and a longer lactation period, factors that decrease the total number of menstrual cycles, are protective. -The terminal differentiation of breast epithelium associated with a full-term pregnancy is also protective, so older age at first live birth is associated with an increased risk of breast cancer.
4 RISK FACTORS FOR BREAST CANCER (cont.) Nonhormonal Risk Factors radiation exposure. Survivors of the atomic bomb blasts in Japan during World War II have a very high incidence of breast cancer, radiation exposure during adolescence, a period of active breast development, magnifies the deleterious effect. alcohol consumption increases the risk of breast cancer. Alcohol consumption is known to increase serum levels of estradiol. long-term consumption of foods with a high fat contributes to an increased risk of breast cancer by increasing serum estrogen levels.
5 Risk Management e.g. when to use postmenopausal hormone replacement therapy. at what age to begin mammography screening or incorporate magnetic resonance imaging (MRI) screening. When to use tamoxifen to prevent breast cancer. when to perform prophylactic mastectomy to prevent breast cancer. Breast Cancer Screening. When Risk-reducing salpingo-oophorectomy When Chemoprevention.
6 EPIDEMIOLOGY AND NATURAL HISTORY OF BREAST CANCER Epidemiology Breast cancer is the most common sitespecific cancer in women and is the leading cause of death from cancer for women aged 20 to 59 years. The increase in breast cancer incidence occurred primarily in women 55 years. There is a 10-fold variation in breast cancer incidence among different countries worldwide.
7 Natural History Bloom and colleagues described the natural history of breast cancer based on the records of 250 women with untreated breast cancers who were cared for on charity wards in the Middlesex Hospital, London, between 1805 and 1933.
8 Primary Breast Cancer. More than 80% of breast cancers show productive fibrosis that involves the epithelial and stromal tissues. entraps and shortens Cooper s suspensory ligaments to produce a characteristic skin retraction. Localized edema (peaud orange) develops when drainage of lymph fluid from the skin is disrupted. cancer cells invade the skin, and eventually ulceration occurs. As new areas of skin are invaded, small satellite nodules appear near the primary ulceration.
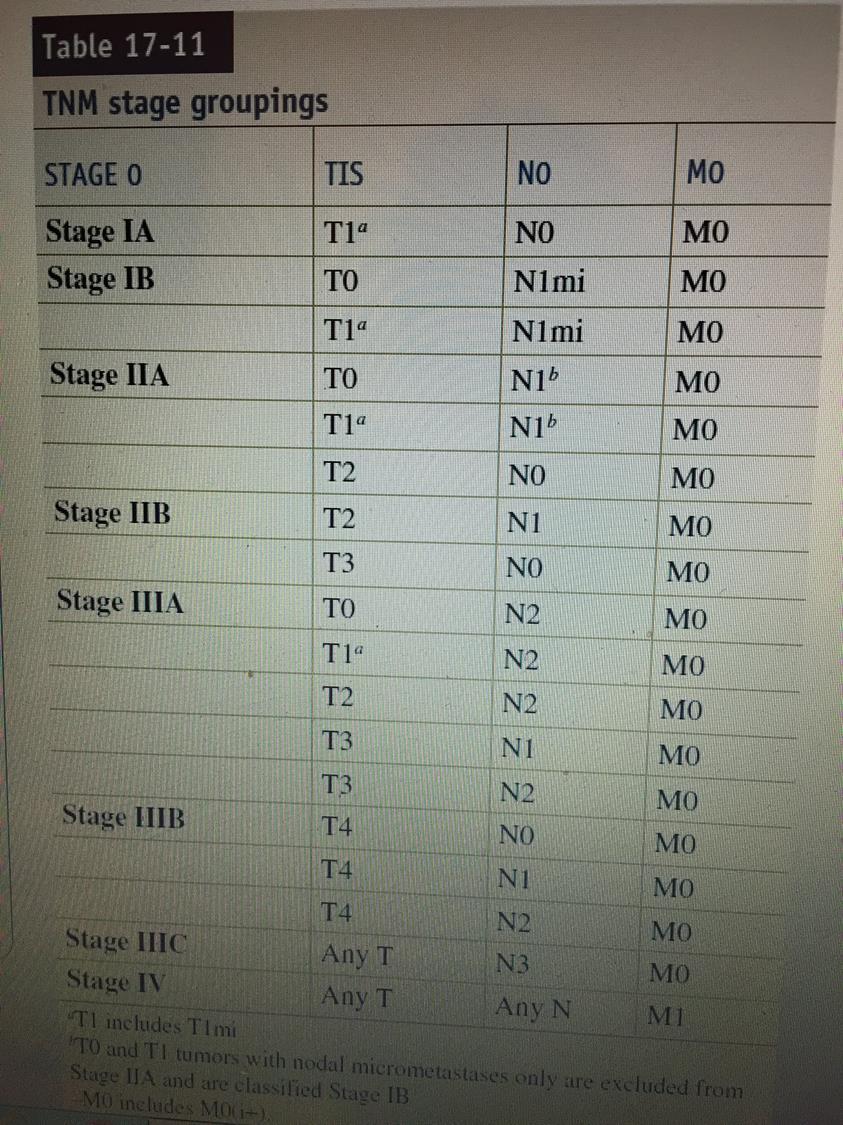
9 Axillary Lymph Node Metastases As primary breast cancer increases, some cancer cells are shed into cellular spaces and transported via the lymphatics the to the regional lymph nodes, especially axillary LNs. LNs that contain mets cancer are at first illdefined and soft but become firm or hard with continued growth of the mets. Eventually LNs adhere to each other and form a conglomerate mass. Cancer cells may grow through LN capsule and fix to structures in the axilla, including the chest wall.
10 Distant Metastases At approximately the twentieth cell doubling, breast cancers acquire their own blood supply (neovascularization). Thereafter, cancer cells may be shed directly into the systemic venous blood to seed the pulmonary circulation via the axillary and intercostal veins or the vertebral column. These cells are scavenged by natural killer lymphocytes and macrophages. Successful mets foci from breast cancer predictably occurs after the primary cancer exceeds 0.5 cm in diameter, which corresponds to the twenty-seventh cell doubling. For 10 years after initial treatment, distant metastases are the most common cause of death in breast cancer patients. Metastases may become evident as late as 20 to 30 years after treatment Common sites of involvement, in order of frequency, are bone, lung, pleura, soft tissues, and liver. Brain metastases are less
11 HISTOPATHOLOGY OF BREAST CANCER Carcinoma In Situ Cancer cells are in situ or invasive depending on whether or not they invade through the basement membrane. ductal and alveolar. Lobular Carcinoma In Situ. LCIS: originates from the terminal duct lobular units and develops only in the female breast. Ductal Carcinoma In Situ (DCIS): Although DCIS is predominantly seen in the female breast, it accounts for 5% of male breast cancers. Histologically, DCIS is characterized by a proliferation of the epithelium that lines the minor ducts, resulting in papillary growths within the duct lumina.
12 HISTOPATHOLOGY OF BREAST CANCER Invasive Breast Carcinoma ldescribed as lobular or ductal in origin. invasive ductal carcinoma of no special type (NST). Foote and Stewart originally proposed the following classification for invasive breast cancer125: 1. Paget s disease of the nipple 2. Invasive ductal carcinoma Adenocarcinoma with productive fibrosis (scirrhous, simplex, NST), 80% 3. Medullary carcinoma, 4% 4. Mucinous (colloid) carcinoma, 2% 5. Papillary carcinoma, 2% 6. Tubular carcinoma, 2% 7. Invasive lobular carcinoma, 10% 8. Rare cancers (adenoid cystic, squamous cell, apocrine)
13 Paget s disease of the nipple: frequently presents as a chronic, eczematous eruption of the nipple, which may be subtle but may progress to an ulcerated, weeping lesion. Paget s disease usually is associated with extensive DCIS and may be associated with an invasive cancer. Invasive ductal carcinoma of the breast with productive fibrosis (scirrhous, simplex, NST): accounts accounts for 80% of breast cancers. Medullary carcinoma is a special-type breast cancer; it Accounts for 4%. Grossly, the cancer is soft and hemorrhagic. A rapid increase in size may occur secondary to necrosis and hemorrhage. Bilaterality is reported in 20% of cases. Mucinous carcinoma (colloid carcinoma),: another specialtype breast cancer, accounts for 2% of all invasive breast cancers. defined by extracellular pools of mucin. Papillary carcinoma: accounts for 2% of all invasive breast cancers. defined by papillae with fibrovascular stalks and multilayered epithelium. showed a low frequency of axillary lymph node metastases
14 Tubular carcinoma: accounts for 2%. Under low-power magnification, a haphazard array of small, randomly arranged tubular elements is seen. Invasive lobular carcinoma: accounts for 10%. It is frequently multifocal, multicentric, and bilateral.
15 DIAGNOSIS OF BREAST CANCER Discussed in benign breast disorders. Hx Physical Examination Investigations.
16 Breast Cancer Staging The clinical stage of breast cancer is determined primarily through physical examination of the skin, breast tissue, and regional lymph nodes (axillary, supraclavicular, and internal mammary). Ultrasound (US) is more sensitive than physical examination alone in determining axillary lymph node involvement. Fine-needle aspiration (FNA) or core biopsy of sonographically indeterminate or suspicious lymph nodes can provide a more definitive diagnosis than US alone. Sentinel node dissection is the preferred method for staging of the regional lymph nodes in women with clinically nodenegative invasive breast cancer. Axillary dissection may be avoided in women with 1 to 2 positive sentinel nodes who are treated with breast conserving surgery. whole breast radiation and systemic therapy.a frequently used staging system is the TNM (tumor, nodes, and metastasis) system.
17
18 SURGICAL APPROACHES TO CANCER THERAPY Multidisciplinary Approach to Cancer Although surgery is an effective therapy for most solid tumors, patients who die from cancer usually die of metastatic disease. In most instances, a multidisciplinary approach beginning at the patient s initial presentation is likely to yield the best result.
19 Surgical Management of Primary Tumors The goal of surgical therapy for cancer is to achieve oncologic cure. A curative operation presupposes that the tumor is confined to the organ of origin or to the organ and the regional lymph node basin. Patients in whom the primary tumor is not resectable with negative surgical margins are considered to have inoperable disease. The operability of primary tumors is best determined before surgery with appropriate imaging studies. Disease involving multiple distant metastases is deemed inoperable because it is usually not curable with surgery of th primary tumor. On occasion, primary tumors are resected in these patients for palliative reasons,
20 It is important to determine optimum surgical margins for each cancer type so that adjuvant radiation and systemic therapy can be offered to patients There are also ongoing studies on approaches to assess margins intraoperatively, to allow immediate intraoperative reexcisions as needed, and maximizing local control.
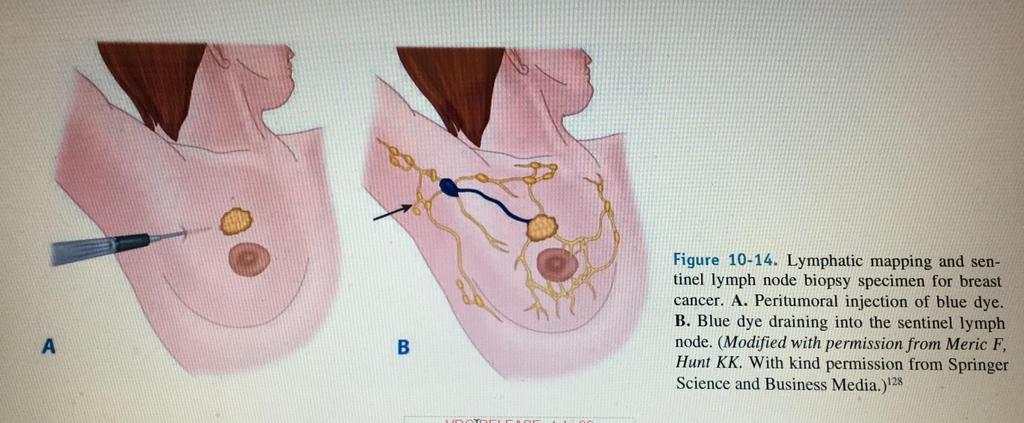
21 Surgical Management of the Regional Lymph Node Basin Most neoplasms have the ability to metastasize via the lymphatics. most oncologic operations have been designed to remove the primary tumor and draining lymphatics en bloc. Surgical management of the clinically negative regional lymph node has evolved with the introduction of lymphatic mapping technology. Lymphatic mapping and sentinel lymph node biopsy specimen were first reported in 1977 by Cabanas for penile cancer. Now, sentinel node biopsy specimen is the standard of care for the management of melanoma and breast cancer. The first node to receive drainage from the tumor site is termed the sentinel node. It is the node most likely to contain metastases, if metastases to that regional lymph node are present.
22
23 Surgical Management of Distant Metastases The treatment of a patient with distant metastases depends on the number and sites of metastases, the cancer type, the rate of tumor growth, the previous treatments delivered and the responses to these treatments, and the patient s age, physical condition, and desires.
24 CHEMOTHERAPY Clinical Use of Chemotherapy In patients with documented distant metastatic disease, chemotherapy is usually the primary modality of therapy. Adjuvant therapy can be administered after surgery (postoperative chemotherapy), or before surgery (preoperative chemotherapy neoadjuvant chemotherapy, or inductio therapy). Chemotherapy destroys cells by first-order kinetics, which means that with the administration of a drug a constan percentage of cells is killed, not a constant number of cells. Cell- cycle phase-nonspecific agents (e.g., alkylating agents) have a linear dose-response curve, such that the fraction of cells killed increases with the dose of the drug. In contrast, the cell-cycle phase-specific drugs have a plateau with respect to cell killing ability, and cell kill will not increase with further increases in drug dose.
25 Anticancer Agents: Alkylating Agents Antitumor Antibiotics. Antimetabolites. Plant Alkaloids. Combination Chemotherapy
26 RADIATION THERAPY Radiation therapy may be used as the primary modality for palliation in certain patients with metastatic disease, primarily patients with bony metastases. Adjuvant radiation therapy can be given before surgery, after surgery, or, in selected cases, during surgery.
27 HORMONAL THERAPY The first attempts at hormonal therapy were through surgical ablation of the organ producing the hormones involved, such as oophorectomy for breast cancer. Currently, hormonal anticancer agents include androgens, antiandrogens, antiestrogens, estrogens, glucocorticoids, gonadotropin inhibitors, progestins. such as with the estrogen antagonist tamoxifen. In breast cancer, estrogen and progesterone receptor status is used to predict the success of hormonal therapy. Androgen receptor is also being pursued as a therapeutic target for breast cancer treatment.
28 TARGETED THERAPY: Over the past decade, increased understanding of cancer biologyhas fostered the emerging field of molecular therapeutics.the basic principle of molecular therapeutics is to exploit themolecular differences between normal cells and cancer cells todevelop targeted therapies. IMMUNOTHERAPY: The aim of immunotherapy is to induce or potentiate inherent antitumor immunity that can destroy cancer cells. GENE THERAPY: Gene therapy is being pursued as a possible approach to modifying the genetic program of cancer cells as well as treating metabolic diseases.
29 Breast Cancer Prognosis Survival rates for women diagnosed with breast cancer in the United States can be obtained from the SEER Program of the National Cancer Institute. The overall 5-year relative survival for breast cancer patients from the time period of from 18 SEER geographic areas was 89.2%. The 5-year relative survival by race was reported to be 90.4% for white women and 78.7% for black women. The 5-year survival rate for patients with localized disease (61% of patients) is 98.6%; for patients with regional disease (32% of patients), 84.4%; and for patients with distant metastatic disease (5% of patients), 24.3%.
30 Local-Regional Recurrence Women with local-regional recurrence of breast cancer may be separated into two groups: those who have had mastectomy and those who have had lumpectomy. Women treated previously with mastectomy undergo surgical resection of the local-regional recurrence and appropriat reconstruction. Chemotherapy and antiestrogen therapy are considered, and adjuvant radiation therapy is given if the chest wall has not previously received radiation therapy or if the radiation oncologist feels that there is scope for further radiation therapy, particularly if this is palliative. Women treated previously with a breast conservation procedure undergo a mastectomy and appropriate reconstruction. Chemotherapy and antiestrogen therapy are considered.
31
32 Local-Regional Recurrence: Women with local-regional recurrence of breast cancer may be separated into two groups: those who have had mastectomy and those who have had lumpectomy. Women treated previously with mastectomy undergo surgical resection of the local-regional recurrence and appropriate reconstruction. Chemotherapy and antiestrogen therapy are considered, and adjuvant radiation therapy is given if the chest wall has not previously received radiation therapy or if the radiation oncologist there is scope for further radiation therapy, particularly if this is palliative. Women treated previously with a breast conservation procedure undergo a mastectomy and appropriate reconstruction. Chemotherapy and antiestrogen therapy are considered.
33 SURGICAL TECHNIQUES IN BREAST CANCER THERAPY Excisional Biopsy with Needle Localization Excisional biopsy implies complete removal of a breast lesion with a margin of normal-appearing breast tissue. important to consider the options for local therapy (lumpectomy vs. mastectomy with or without reconstruction) and the need for nodal assessment with SLN dissection. After excision of a suspicious breast lesion, the specimen should be x-rayed to confirm the lesion has been excised with appropriate margins.
34 Breast Conservation Breast conservation involves resection of the primary breast cancer with a margin of normal-appearing breast tissue, adjuvant radiation therapy, and assessment of regional lymph node status. Resection of the primary breast cancer is alternatively called segmental mastectomy, lumpectomy, partial mastectomy, wide local excision, and tylectomy.
35 Mastectomy and Axillary Dissection A skin-sparing mastectomy removes all breast tissue, the nipple-areola complex, and scars from any prior biopsy procedures A total (simple) mastectomy without skin sparing removes all breast tissue, the nipple-areola complex, and skin. An extended simple mastectomy removes all breast tissue, the nipple-areola complex, skin, and the level I axillary lymph nodes. A modified radical ( Patey ) mastectomy removes all breast tissue, the nipple-areola complex, skin, and the levels I, II and III axillary lymph nodes: the pectoralis minor which was divided and removed by Patey may be simply divided, giving improved access to level III nodes, and then left in-situ or occasionally the axillary clearance can be performed without dividing pectoralis minor. The Halsted radical mastectomy Nipple-areolar sparing mastectomy
36
DISORDERS OF THE BREAST Dated. FIBROADENOSIS Other common names: mastitis, fibrocystic disease, cystic mammary dysplasia.
 DISORDERS OF THE BREAST Dated BENIGN BREAST DISORDERS (Essential Surg 2 nd Ed, pp 540) FIBROADENOSIS Other common names: mastitis, fibrocystic disease, cystic mammary dysplasia. Fibroadenosis is the distortion
DISORDERS OF THE BREAST Dated BENIGN BREAST DISORDERS (Essential Surg 2 nd Ed, pp 540) FIBROADENOSIS Other common names: mastitis, fibrocystic disease, cystic mammary dysplasia. Fibroadenosis is the distortion
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
It is a malignancy originating from breast tissue
 59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
BREAST SURGERY PROGRESS TEST Name:
 General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
Invasive Papillary Breast Carcinoma
 410 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the
410 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR
 INTERNAL MAMMARY SUPRACLAVICULAR") BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
Q&A. Fabulous Prizes. Collecting Cancer Data: Breast 4/4/13. NAACCR Webinar Series Collecting Cancer Data Breast
 Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
BREAST PATHOLOGY MCQS
 BREAST PATHOLOGY MCQS 1) :The most important factor in breast enlargement during pregnancy is A. stromal edema B. secretion of chorionic gonadotropin C. glandular hyperplasia D. proliferation of stroma
BREAST PATHOLOGY MCQS 1) :The most important factor in breast enlargement during pregnancy is A. stromal edema B. secretion of chorionic gonadotropin C. glandular hyperplasia D. proliferation of stroma
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST CANCER SURGERY. Dr. John H. Donohue
 Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery
 Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
Classification System
 Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
Breast Pathology. Breast Development
 Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Cancer. Excess Estrogen Exposure. Alcohol use + Pytoestrogens? Abortion. Infertility treatment?
 Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
General Information Key Points
 The content of this booklet was adapted from content originally published by the National Cancer Institute. Male Breast Cancer Treatment (PDQ ) Patient Version. Updated September 29,2017. https://www.cancer.gov/types/breast/patient/male-breast-treatment-pdq
The content of this booklet was adapted from content originally published by the National Cancer Institute. Male Breast Cancer Treatment (PDQ ) Patient Version. Updated September 29,2017. https://www.cancer.gov/types/breast/patient/male-breast-treatment-pdq
Table of contents. Page 2 of 40
 Page 1 of 40 Table of contents Introduction... 4 1. Background Information... 6 1a: Referral source for the New Zealand episodes... 6 1b. Invasive and DCIS episodes by referral source... 7 1d. Age of the
Page 1 of 40 Table of contents Introduction... 4 1. Background Information... 6 1a: Referral source for the New Zealand episodes... 6 1b. Invasive and DCIS episodes by referral source... 7 1d. Age of the
COPE Library Sample
 Breast Anatomy LOBULE LOBE ACINI (MILK PRODUCING UNITS) NIPPLE AREOLA COMPLEX ENLARGEMENT OF DUCT AND LOBE LOBULE SUPRACLAVICULAR NODES INFRACLAVICULAR NODES DUCT DUCT ACINI (MILK PRODUCING UNITS) 8420
Breast Anatomy LOBULE LOBE ACINI (MILK PRODUCING UNITS) NIPPLE AREOLA COMPLEX ENLARGEMENT OF DUCT AND LOBE LOBULE SUPRACLAVICULAR NODES INFRACLAVICULAR NODES DUCT DUCT ACINI (MILK PRODUCING UNITS) 8420
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Presented by: Lillian Erdahl, MD
 Presented by: Lillian Erdahl, MD Learning Objectives What is Breast Cancer Types of Breast Cancer Risk Factors Warning Signs Diagnosis Treatment Options Prognosis What is Breast Cancer? A disease that
Presented by: Lillian Erdahl, MD Learning Objectives What is Breast Cancer Types of Breast Cancer Risk Factors Warning Signs Diagnosis Treatment Options Prognosis What is Breast Cancer? A disease that
Breast Cancer FAQ. How does Breast Cancer spread? Breast cancer spreads by invading into
 FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
CPC 4 Breast Cancer. Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast.
 CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
Advances in Localized Breast Cancer
 Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Diseases of the breast (2 of 2) Breast cancer
 Breast cancer") Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Breast Cancer. Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology
 Breast Cancer Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology Muscles Muscles underneath the breasts separating them from the ribs Breast has no muscle tissue 2 Female Breast Anatomy
Breast Cancer Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology Muscles Muscles underneath the breasts separating them from the ribs Breast has no muscle tissue 2 Female Breast Anatomy
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e
 Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 60: Caring for Clients With Breast Disorders Slide 1 Infectious and Inflammatory Breast Disorders: Mastitis Pathophysiology and Etiology
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 60: Caring for Clients With Breast Disorders Slide 1 Infectious and Inflammatory Breast Disorders: Mastitis Pathophysiology and Etiology
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Breast Cancer Basics. Clinical Oncology for Public Health Professionals. Ben Ho Park, MD, PhD
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Breast Surgery: Yesterday, Today and Tomorrow
 Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate surgical options
 across Ontario: Patient indications and appropriate surgical options") A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
Excerpts from the American College of Surgeons Educational Courses about Breast Disease:
 1 Excerpts from the American College of Surgeons Educational Courses about Breast Disease: Gynecomastia Gynecomastia is a benign enlargement of the male breast that can be unilateral or bilateral. It typically
1 Excerpts from the American College of Surgeons Educational Courses about Breast Disease: Gynecomastia Gynecomastia is a benign enlargement of the male breast that can be unilateral or bilateral. It typically
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
RUTGERS CANCER INSTITUTE OF NEW JERSEY - ROBERT WOOD JOHNSON MEDICAL SCHOOL INTERDISCIPLINARY BREAST SURGERY FELLOWSHIP CORE EDUCATIONAL OBJECTIVES
 RUTGERS CANCER INSTITUTE OF NEW JERSEY - ROBERT WOOD JOHNSON MEDICAL SCHOOL INTERDISCIPLINARY BREAST SURGERY FELLOWSHIP CORE EDUCATIONAL OBJECTIVES At the completion of Breast Fellowship training, the
RUTGERS CANCER INSTITUTE OF NEW JERSEY - ROBERT WOOD JOHNSON MEDICAL SCHOOL INTERDISCIPLINARY BREAST SURGERY FELLOWSHIP CORE EDUCATIONAL OBJECTIVES At the completion of Breast Fellowship training, the
So, we already talked about that recognition is the key to optimal treatment and outcome.
 Hi, I m Dr. Anthony Lucci from the University of Texas MD Anderson Cancer Center in Houston. And today, I d like to talk to you about the role of surgery in inflammatory breast cancer patients. So, there
Hi, I m Dr. Anthony Lucci from the University of Texas MD Anderson Cancer Center in Houston. And today, I d like to talk to you about the role of surgery in inflammatory breast cancer patients. So, there
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018)
 Test Content Outline (Effective 2018)") Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Chapter 2 Staging of Breast Cancer
 Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
Ductal Carcinoma-in-Situ: New Concepts and Controversies
 Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Armed Forces Institute of Pathology.
 Armed Forces Institute of Pathology www.radpath.com Armed Forces Institute of Pathology Breast Disease www.radpath.org Armed Forces Institute of Pathology Interpretation of Breast MRI Leonard M. Glassman
Armed Forces Institute of Pathology www.radpath.com Armed Forces Institute of Pathology Breast Disease www.radpath.org Armed Forces Institute of Pathology Interpretation of Breast MRI Leonard M. Glassman
Breast Cancer Task Force of the Greater Miami Valley A collaborative effort of health care professionals and breast cancer survivors in the Greater
 Breast Cancer Task Force of the Greater Miami Valley A collaborative effort of health care professionals and breast cancer survivors in the Greater Dayton Area Last Updated Fall 2014 TABLE OF CONTENTS
Breast Cancer Task Force of the Greater Miami Valley A collaborative effort of health care professionals and breast cancer survivors in the Greater Dayton Area Last Updated Fall 2014 TABLE OF CONTENTS
Jose A Torres, MD 1/12/2017
 Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Completing the Puzzle AJCC TNM Staging Breast. Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017
 Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
BREAST CANCER BREAST CANCER
 BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
Diagnosis and staging of breast cancer and multidisciplinary team working
 1 Diagnosis and staging of breast cancer and multidisciplinary team working Common symptoms and signs Over 90% of breast cancers (BCs) are local or regional when first detected. At least 60% of patients
1 Diagnosis and staging of breast cancer and multidisciplinary team working Common symptoms and signs Over 90% of breast cancers (BCs) are local or regional when first detected. At least 60% of patients
Chapter 13 Cancer of the Female Breast
 Lynn A. Gloeckler Ries and Milton P. Eisner INTRODUCTION This study presents survival analyses for female breast cancer based on 302,763 adult cases from the Surveillance, Epidemiology, and End Results
Lynn A. Gloeckler Ries and Milton P. Eisner INTRODUCTION This study presents survival analyses for female breast cancer based on 302,763 adult cases from the Surveillance, Epidemiology, and End Results
5.1 Breast, Anatomy. 70
 Chapter 5 Breast 5.1 Breast, Anatomy Breasts, also called Mamma are mammary glands, subcutaneously placed on the ventral side of the trunk in mammalian species, and develop for the sole purpose of secreting
Chapter 5 Breast 5.1 Breast, Anatomy Breasts, also called Mamma are mammary glands, subcutaneously placed on the ventral side of the trunk in mammalian species, and develop for the sole purpose of secreting
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
BREAST CANCER d an BREAST SELF EXAM
 BREAST CANCER and BREAST SELF EXAM American Cancer Society Statistics: 2009 Invasive breast cancer will be diagnosed in over 192,370 women Carcinoma in situ will be diagnosed in 62,280 women More than
BREAST CANCER and BREAST SELF EXAM American Cancer Society Statistics: 2009 Invasive breast cancer will be diagnosed in over 192,370 women Carcinoma in situ will be diagnosed in 62,280 women More than
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Seventh Edition Staging 2017 Breast
 Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction
 Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Mammographic imaging of nonpalpable breast lesions. Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand
 Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Case 1. BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care
 BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
PATIENT INFORMATION. about BREAST CANCER
 PATIENT INFORMATION about BREAST CANCER What is Breast Cancer? The female breast is made up mainly of: Lobules (milk-producing glands) Ducts (tiny tubes that carry the milk from the lobules to the nipple)
PATIENT INFORMATION about BREAST CANCER What is Breast Cancer? The female breast is made up mainly of: Lobules (milk-producing glands) Ducts (tiny tubes that carry the milk from the lobules to the nipple)
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Collecting Cancer Data: Breast. Prizes! Collecting Cancer Data: Breast 8/4/ NAACCR Webinar Series 1. NAACCR Webinar Series
 Collecting Cancer Data: Breast NAACCR 2008 2009 Webinar Series Prizes! Question of the Month! The participant that submits the best question of the session will receive a fbl fabulous Pi Prize! Shannon
Collecting Cancer Data: Breast NAACCR 2008 2009 Webinar Series Prizes! Question of the Month! The participant that submits the best question of the session will receive a fbl fabulous Pi Prize! Shannon
Case Scenario 1: Breast
 Case Scenario 1: Breast A 63 year old white female presents with a large mass in her left breast. 4/15/13 Mammogram/US: 1. Left breast mammographic and sonographic at 3:00 measuring 7.1 cm highly suggestive
Case Scenario 1: Breast A 63 year old white female presents with a large mass in her left breast. 4/15/13 Mammogram/US: 1. Left breast mammographic and sonographic at 3:00 measuring 7.1 cm highly suggestive
Pathology: Grade 1 infiltrating ductal carcinoma with associated DCIS, Lymphvascular invasion present. ER+, PR+. Her 2/ IHC 1+, negative
 GATRA 2016 Breast Case Demographics Name: Autumn Leaf Sex: F Date of Birth: 3/26/75 SSN: 098765432 Race: African American Marital Status: Single Address: 3615 Burnt Hickory Trail, Helen, GA 37285, White
GATRA 2016 Breast Case Demographics Name: Autumn Leaf Sex: F Date of Birth: 3/26/75 SSN: 098765432 Race: African American Marital Status: Single Address: 3615 Burnt Hickory Trail, Helen, GA 37285, White
Health Bites Breast Cancer. Breast Cancer. Normal breast
 Health Bites Breast Cancer Breast Cancer Normal breast The normal breast tissue varies in size and shape. The breasts rest in front of the rib cage. The breasts are made up of fatty tissue, milk ducts
Health Bites Breast Cancer Breast Cancer Normal breast The normal breast tissue varies in size and shape. The breasts rest in front of the rib cage. The breasts are made up of fatty tissue, milk ducts
Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy
 Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy Mitsui Memorial Hospital Department of Breast and Endocine surgery Daisuke Ota No financial support
Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy Mitsui Memorial Hospital Department of Breast and Endocine surgery Daisuke Ota No financial support
Breast Cancer. What is breast cancer?
 Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
Types of Breast Cancer
 IOWA RADIOLOGY 1 Types of Breast Cancer 515-226-9810 Ankeny Clive Downtown Des Moines IOWA RADIOLOGY 1 Table of Contents Introduction... 1 Ductal Carcinoma... 2 Paget s Disease of the Nipple... 8 Lobular
IOWA RADIOLOGY 1 Types of Breast Cancer 515-226-9810 Ankeny Clive Downtown Des Moines IOWA RADIOLOGY 1 Table of Contents Introduction... 1 Ductal Carcinoma... 2 Paget s Disease of the Nipple... 8 Lobular
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
BreastScreen Victoria Annual Statistical Report
 BreastScreen Victoria Annual Statistical Report 29 BREASTSCREEN VICTORIA: ANNUAL STATISTICAL REPORT, 29 Produced by: BreastScreen Victoria Coordination Unit Level, 3 Pelham Street, Carlton South Victoria
BreastScreen Victoria Annual Statistical Report 29 BREASTSCREEN VICTORIA: ANNUAL STATISTICAL REPORT, 29 Produced by: BreastScreen Victoria Coordination Unit Level, 3 Pelham Street, Carlton South Victoria
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Breast Cancer Pathway Map
 Care Ontario Pathway Map 03.18 Printer Friendly Version Note: print 11x17 landscape for best results, some features and content are only available on web version of pathway map Prevention Screening Diagnosis
Care Ontario Pathway Map 03.18 Printer Friendly Version Note: print 11x17 landscape for best results, some features and content are only available on web version of pathway map Prevention Screening Diagnosis
The Alvin & Lois Lapidus Cancer Institute BREAST CANCER
 The Alvin & Lois Lapidus Cancer Institute BREAST CANCER What is breast cancer? Breast cancer is a disease in which cancer cells form in the tissues of the breast. The breast is made up of lobes and ducts.
The Alvin & Lois Lapidus Cancer Institute BREAST CANCER What is breast cancer? Breast cancer is a disease in which cancer cells form in the tissues of the breast. The breast is made up of lobes and ducts.
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Pathology Report Patient Companion Guide
 Pathology Report Patient Companion Guide Breast Cancer - Understanding Your Pathology Report Pathology Reports can be overwhelming. They contain scientific terms that are unfamiliar and might be a bit
Pathology Report Patient Companion Guide Breast Cancer - Understanding Your Pathology Report Pathology Reports can be overwhelming. They contain scientific terms that are unfamiliar and might be a bit
Case Report Synchronous Bilateral Solid Papillary Carcinomas of the Breast
 Case Reports in Surgery Volume 2013, Article ID 812129, 4 pages http://dx.doi.org/10.1155/2013/812129 Case Report Synchronous Bilateral Solid Papillary Carcinomas of the Breast Noriko Yoshimura, 1 Shigeru
Case Reports in Surgery Volume 2013, Article ID 812129, 4 pages http://dx.doi.org/10.1155/2013/812129 Case Report Synchronous Bilateral Solid Papillary Carcinomas of the Breast Noriko Yoshimura, 1 Shigeru
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST
 COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast