Ductal Carcinoma-in-Situ: New Concepts and Controversies
|
|
|
- Godfrey Andrews
- 5 years ago
- Views:
Transcription
1 Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
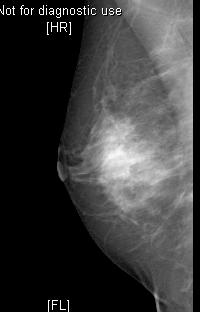
2 Case Presentation 51 y.o. woman referred for recent diagnosis of Ductal Carcinoma-in-Situ Presented to her surgeon with mass in right breast Prior mammogram (two years earlier) negative Current mammogram

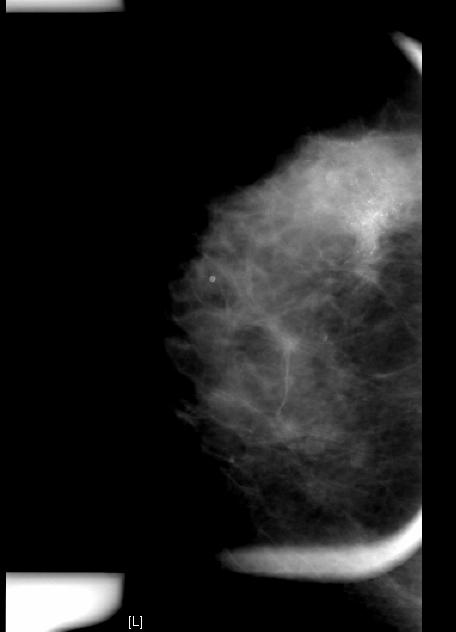
3 Large area of microcalcifications
4 Case Presentation 51 y.o. woman referred for recent diagnosis of Ductal Carcinoma-in-Situ Presented to Dr. Chang with mass in right breast Prior mammogram (two years earlier) negative Current mammogram. Needle biopsy.dcis
5 Case, continued Past history unremarkable No history of hormone replacement therapy Natural menopause several years ago Exam: residual 2-3 cm mass adjacent to needle biopsy mark only abnormality Surgical therapy discussed with her surgeon Calcifications extensive so he recommended mastectomy feeling that margins would be difficult to achieve Underwent modified radical mastectomy Pathology: sentinel LN negative but additional lymph node positive; no invasive cancer seen on mastectomy specimen
6 Case, continued Biochemical markers: ER and PR both negative Her-2/neu 6.9 interpreted as overexpressed Received therapy with Taxotere, Adriamycin and Cytoxan followed by Herceptin Ejection fraction fell from 75% to 60% after Herceptin but otherwise she feels well and is without evidence of cancer at present 18 months after initial diagnosis
7 Case #2 50 y.o. lady developed breast mass which she watched for three years Mammogram
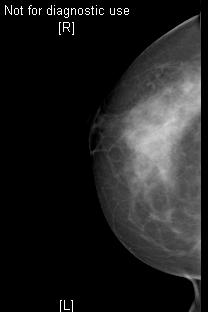
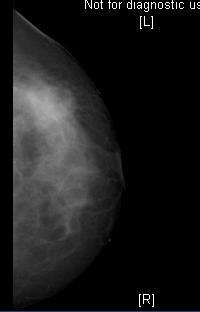
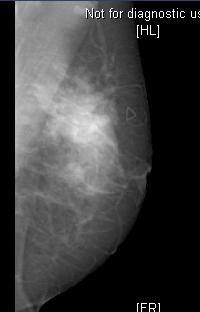
8 Obliteration of normal clear space
9 Case #2 50 y.o. lady developed breast mass which she watched for three years Mammogram Underwent lumpectomy 3 cm tumor: all DCIS; margins close Re-excision of margins...pathology: DCIS with microinvasion; margins now negative
10 Case #2 Biochemistry of microinvasive component: ER, PR negative Her-2/neu overexpressed at 10.7 Referred for medical oncology consultation; decision made not to treat further, e.g., with chemo or herceptin See subsequent discussion for rationale Pathology at issue..

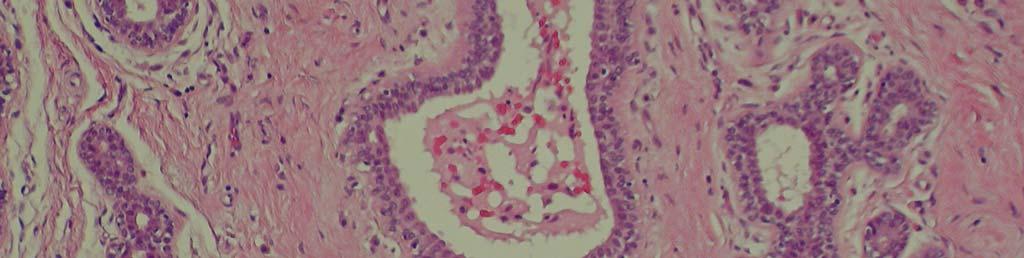
11 Normal Breast Architecture


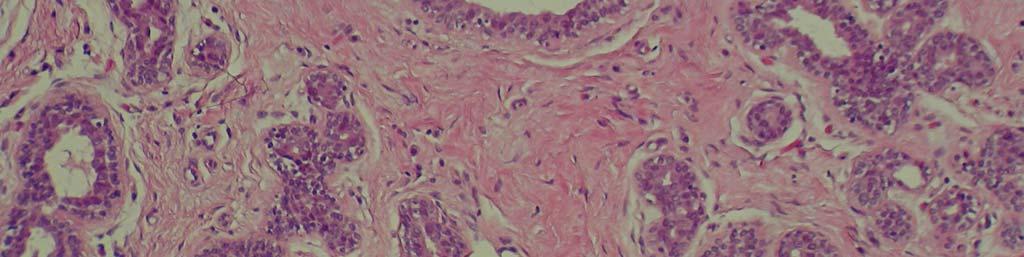
12 Double cell layer: beginnings of atypia

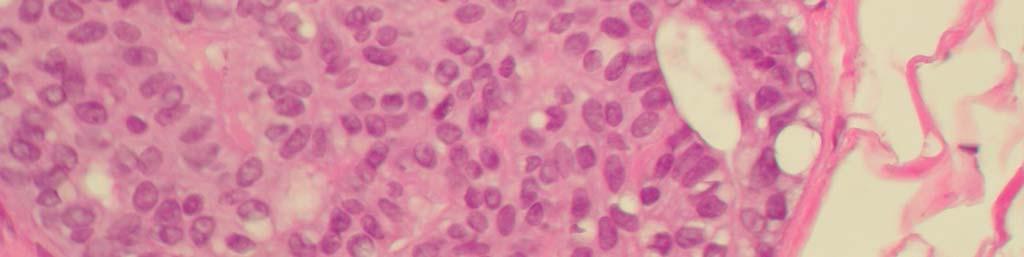
13 Very cellular: Atypia

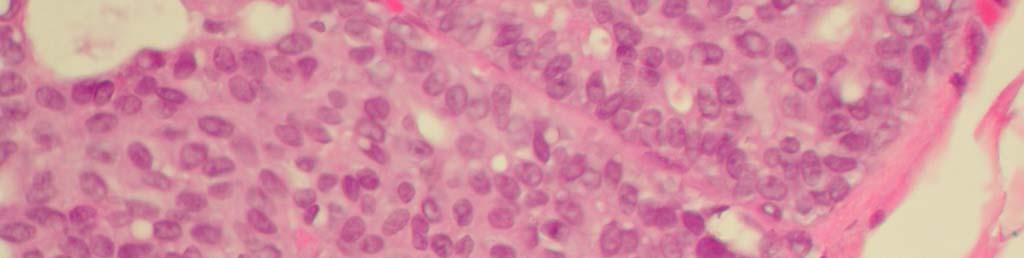
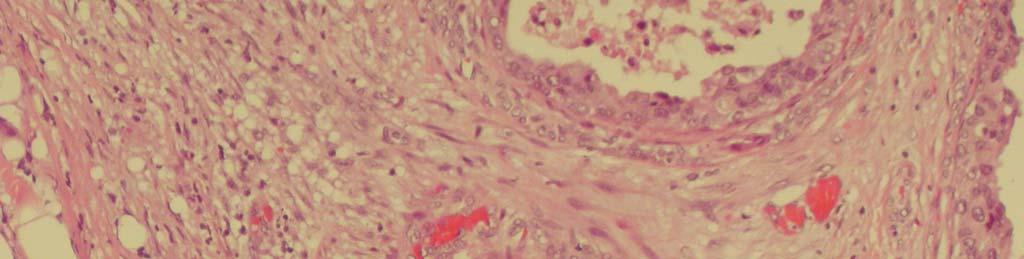
14 Ductal Carcinoma in-situ

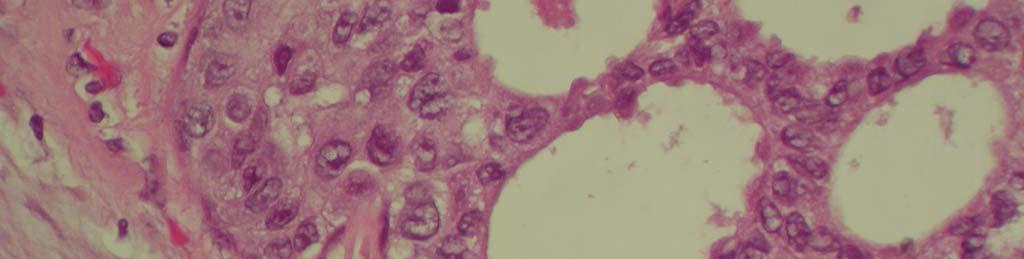
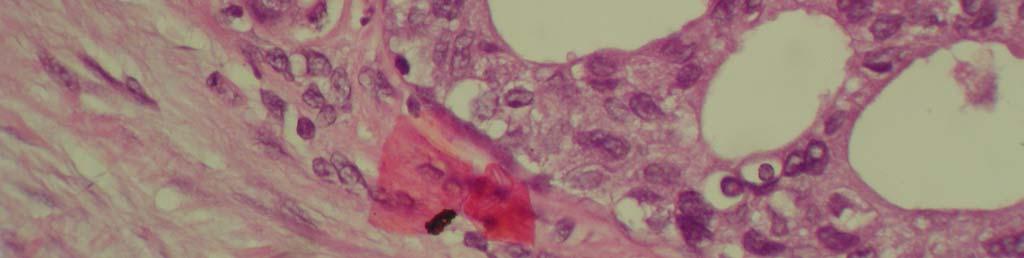
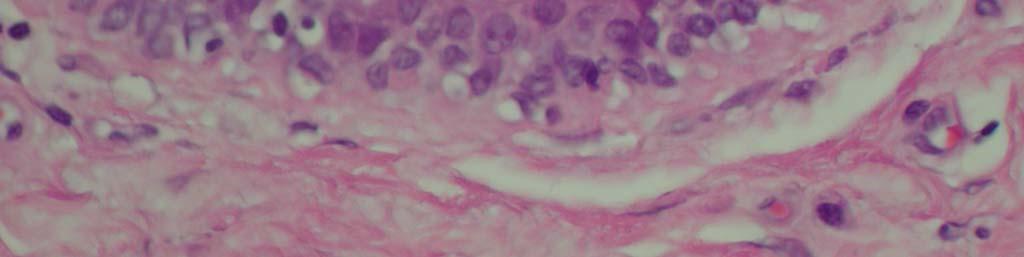
15 Crowding of odd-shaped cells DCIS


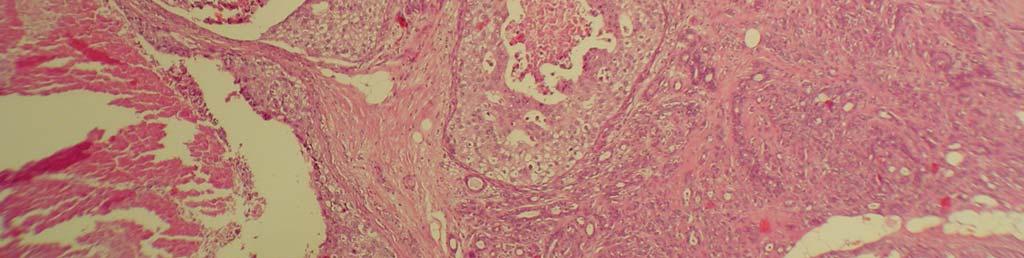
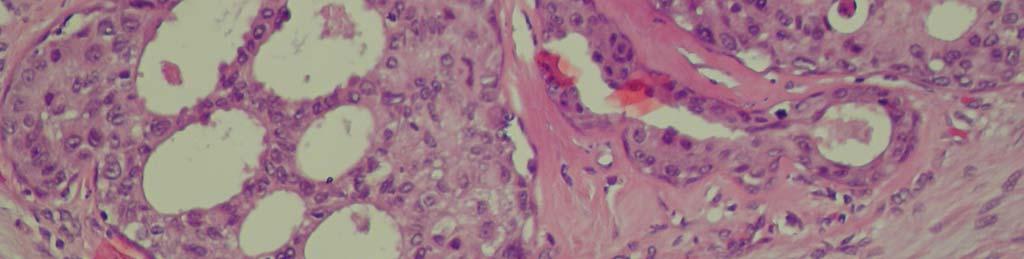
16 Nest of necrotic debris Comedo necrosis
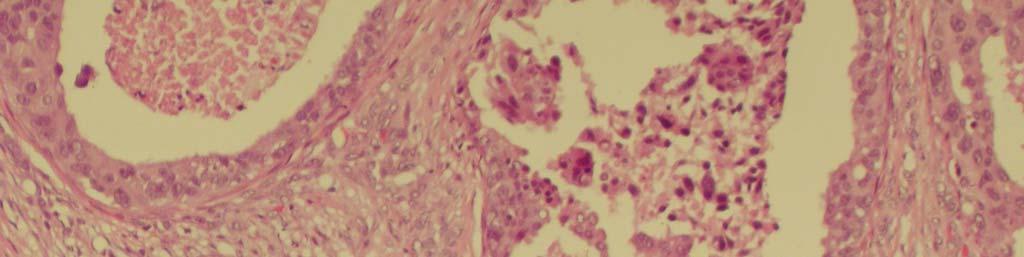
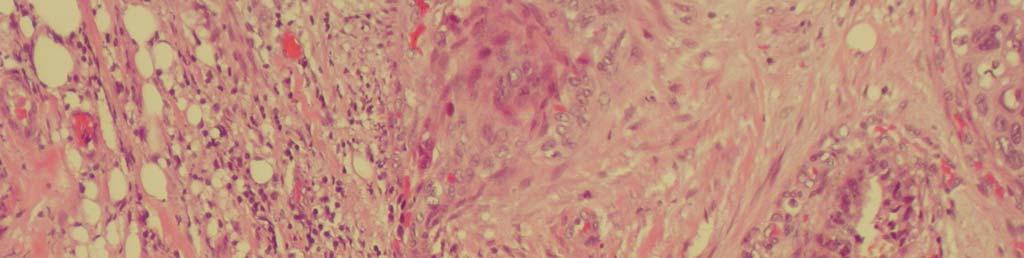
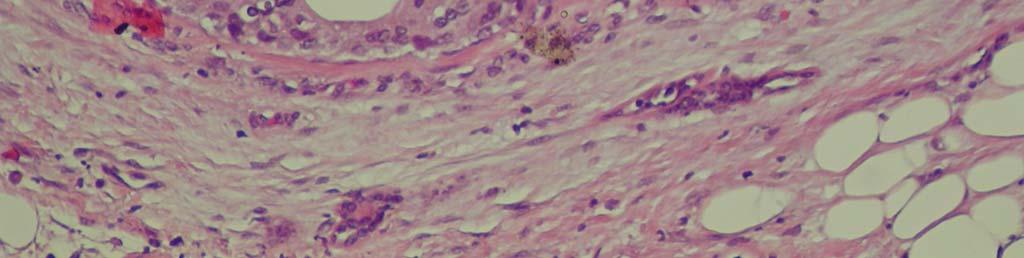
17 Area of microinvasion Microinvasive Ductal Carcinoma
18 DCIS -- Background <1% of all breast neoplasms in 1978 prior to widespread screening mammography Percentage of all breast neoplasms that are DCIS has skyrocketed in mammography era Now at least 20% of all breast neoplasms are in situ; most are picked up by mammography only and are not palpable
19 Background, continued Risk factors same as for invasive breast cancer (FH, nulliparity, etc.) Part of BRCA 1 and 2 syndromes Not related to hormone replacement therapy What is the natural history of this entity? What percentage of these tumors would go on to develop full-blown invasive cancer? No one knows the answer to this but there are powerful clues in the literature
20 Natural history of 28 women with small low-grade DCIS tumors treated with biopsy only (path originally misread by current standards) 5/28 women treated with biopsy only died of breast cancer eventually small series but sobering Time since biopsy (yrs) Sanders et al CANCER 103:2481, 2005
21 The Nurses Health Study Huge longitudinal health study conducted by the Harvard School of Public Health involving 237,000 female nurses over 20 years 1877 benign breast biopsies reviewed 13 cases of previously unrecognized DCIS uncovered All treated by biopsy only
22 Collins et al CANCER 103:1778, 2005
23 What happened to the women with recurrent DCIS?
24 What happened to the women who subsequently developed invasive cancer? Of 13 women whose tumors were misread, 10 developed subsequent events, 6 with invasive cancer; one died
25 Untreated DCIS, cont. Relative risk (versus biopsied patients with truly benign histology) in this group of 13 women of developing: Subsequent invasive cancer: 13.5 Either DCIS or invasive cancer: 20 Take-home message from these two studies: DCIS is worth treating!
26 What About DCIS Treated Properly (to be defined) After simple lumpectomy only, the majority of patients never suffer a recurrence One half of all recurrences are with invasive cancer 90% of patients with invasive cancer and 100% of patients with pure DCIS recurrence survive the second event
27 How to Treat DCIS in 2008: Factors in Decision Making What determines likelihood of local recurrence: Grade (high-grade or with necrosis) Margin width (10 mm is usual cut-off) Microinvasion How do the above contribute to treatment recommendations?
28 What is the Optimal Treatment for DCIS? Surgery: breast-conserving surgery is adequate if margins can be achieved; can be difficult in DCIS where disease is often multifocal (several foci in the same quadrant versus multicentric) Mastectomy virtually eliminates local recurrence but is too much treatment for most women
29 Results of Largest Series of DCIS treated non-randomly (1,115 pts): freedom from local recurrence Surgery does solve the problem but is probably too much treatment for most women Silverstein, MJ.. Oncology 2003; 17:1519.
30 Optimal Treatment of DCIS, continued What about radiation? Several studies have addressed this issue NSABP B-17: study with long follow-up Radiation halves rate of in-breast invasive and noninvasive recurrence but has no impact on survival because salvage therapy is so good Two other smaller studies from Europe and Asia confirm the above findings Some authors believe that for highly favorable lesions (small, low-grade) radiation can be eliminated
31 Optimal Treatment of DCIS, continued What about the role of hormonal suppression? Tamoxifen vs. Placebo added to RT in large trial (NSABP B-24) Benefit of tamoxifen small Largely confined to women whose DCIS expressed the estrogen receptor UK/ANZ trial failed to confirm Nonetheless most large centers recommend tamoxifen as an adjunct to lumpectomy and radiation for DCIS No data on Aromatase Inhibitors but two large trials are ongoing which will attempt to assess Tamoxifen vs. Arimidex in DCIS
32 The Van-Nuys Scoring System Size Margin (mm) Pathologic Classification Age (yr) Score 1 <15 mm >10 low-grade no necrosis mm 1-9 low-grade with necrosis >40 mm <1 high-grade with necrosis <50 Add up the score from the four columns: that is the "Van-Nuys" Score
33 Validation of Van-Nuys Van Nuys Score Average Size (mm) Avg Nucl Grade % Recurrences % Inv. Recurrences %10-year Survival
34 Van Nuys, contined Has stood up as best way to estimate risk of future events Useful as way to stratify patients for future randomized trials To some extent helps guide contemporary treatment, especially for women with the highest scores
35 What is the Significance of Microinvasive Cancer? Uncommon finding Hotly debated One large series * 425 patients: pt1a, pt1b and pt1mic 24 had pt1mic: Of these 24 all had negative axillary or sentinel lymph node 5/14 were Her-2/neu + (not done on the rest) Ki-67 elevated in half 15/23 were ER+ or PR + or both + None of these patients received adjuvant chemotherapy Patients who were ER or PR + were offered adjuvant hormones All 24 patients were alive and cancer-free at the time the article was written; years at risk not stated in paper Colleoni et al Annals of Oncology 15:
36 Survival of Three Groups Microinvasive subset Number of patients at risk at each unit of time not stated Colleoni et al Annals of Oncology 15:
37 What about DCIS that overexpresses Her-2/neu? A high percentage of ER-negative DCIS tumors overexpress the Her-2/neu oncogene Associated with higher incidence of comedo necrosis (recall this predicts for local recurrence) Not yet standard-of-care to add Herceptin to treatment regimen of such patients but question is being actively studied at major institutions Editorial comment: Expense and potential for cardiac toxicity limit value of this approach in patients in whom survival is already virtually assured with appropriate treatment
38 What about DCIS with positive lymph node(s) case 1 Not a trivial issue as many as 10% of patients with DCIS have positive sentinel lymph node 11% of patients with DCIS on biopsy will have invasive component at mastectomy Most patients with + sentinel node did not have invasive cancer found at subsequent mastectomy What to do about all of this is unclear Argues for more liberal use of sentinel LN procedure in DCIS
39 What is in store long-term for patients with DCIS? Large MD Anderson study looking at 799 women with DCIS Characteristics
40 Therapy Administered at MD Anderson Dawood et al Annals of Surgical Oncology 15:244, 2008
41 45/799 patients had second event
42 Gradual Nature of Subsequent Events
43 Conclusions DCIS is a very common diagnosis Overall prognosis very good Even with subset analysis it is difficult to identify patient group with bad outcome Adequate surgery and radiation contribute to risk reduction for second event Role of adjuvant hormonal antagonism less certain Genetic subset analysis will become important in the future
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Breast Cancer Basics. Clinical Oncology for Public Health Professionals. Ben Ho Park, MD, PhD
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Breast Cancer. Excess Estrogen Exposure. Alcohol use + Pytoestrogens? Abortion. Infertility treatment?
 Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
4/13/2010. Silverman, Buchanan Breast, 2003
 Tailoring Breast Cancer Treatment: Has Personalized Medicine Arrived? Judith Luce, M.D. San Francisco General Hospital Avon Comprehensive Breast Care Center Outline First, treatment of DCIS Sorting risk
Tailoring Breast Cancer Treatment: Has Personalized Medicine Arrived? Judith Luce, M.D. San Francisco General Hospital Avon Comprehensive Breast Care Center Outline First, treatment of DCIS Sorting risk
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Evolving Practices in Breast Cancer Management
 Evolving Practices in Breast Cancer Management The Georgia Tumor Registrars Association 2016 Priscilla R. Strom, MD, FACS Objectives 1. understand newer indications for neoadjuvant treatment 2. understand
Evolving Practices in Breast Cancer Management The Georgia Tumor Registrars Association 2016 Priscilla R. Strom, MD, FACS Objectives 1. understand newer indications for neoadjuvant treatment 2. understand
A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues
- Test slide, Breast cancer tissues with corresponding normal tissues") A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Ductal Carcinoma in Situ (DCIS)
") Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /
Disclosure. Objectives 03/19/2019. Current Issues in Management of DCIS Radiation Oncology Considerations
 Current Issues in Management of DCIS Radiation Oncology Considerations Fariba Asrari, M.D. Director. Johns Hopkins Breast Center at Green Spring Station Department of Radiation Oncology & Molecular Sciences
Current Issues in Management of DCIS Radiation Oncology Considerations Fariba Asrari, M.D. Director. Johns Hopkins Breast Center at Green Spring Station Department of Radiation Oncology & Molecular Sciences
LOBULAR CARCINOMA IN SITU: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE
 : WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
Minimizing Errors in Diagnostic Pathology
 Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville Medical Director, Shands Jacksonville Breast Health Center
Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville Medical Director, Shands Jacksonville Breast Health Center
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
BREAST SURGERY PROGRESS TEST Name:
 General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
Breast Cancer FAQ. How does Breast Cancer spread? Breast cancer spreads by invading into
 FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
Adjuvant Systemic Therapy in Early Stage Breast Cancer
 Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Ductal Carcinoma in Situ. Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA
 Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Speaker s Bureau. Travel expenses. Advisory Boards. Stock. Genentech Invuity Medtronic Pacira. Faxitron. Dune TransMed7 Genomic Health.
 Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
It is a malignancy originating from breast tissue
 59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
A DEEPER DIVE INTO DUCTAL CARCINOMA IN SITU: CLINICAL AND PATHOLOGIC CONSIDERATIONS IN 2015
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 A DEEPER DIVE INTO DUCTAL CARCINOMA IN SITU: CLINICAL AND PATHOLOGIC CONSIDERATIONS IN 2015
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 A DEEPER DIVE INTO DUCTAL CARCINOMA IN SITU: CLINICAL AND PATHOLOGIC CONSIDERATIONS IN 2015
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction
 Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
 in Locally Advanced Breast Cancer") Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Invasive Papillary Breast Carcinoma
 410 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the
410 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the
What is the recommended regimen for adjuvant radiation therapy? Tata Memorial Centre s opinion is summarized as follows:
 February 3 rd 2015 Dear Ms., Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online consultation
February 3 rd 2015 Dear Ms., Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online consultation
My Personalized Breast Cancer Worksheet
 My Personalized Breast Cancer Worksheet KNOW For Early-Stage Breast Cancer. No Questions. Only Results. No two tumors are alike. What are the characteristics of your breast cancer and how will that effect
My Personalized Breast Cancer Worksheet KNOW For Early-Stage Breast Cancer. No Questions. Only Results. No two tumors are alike. What are the characteristics of your breast cancer and how will that effect
In Situ Breast Carcinoma. James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA
 In Situ Breast Carcinoma James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA Content In Situ Ductal Carcinoma In Situ Lobular Carcinoma
In Situ Breast Carcinoma James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA Content In Situ Ductal Carcinoma In Situ Lobular Carcinoma
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER. B.Zandi Professor of Radiology
 ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights
 2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights Mylin A. Torres, M.D. Director, Glenn Family Breast Center Associate Professor Department of Radiation Oncology Winship Cancer Institute
2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights Mylin A. Torres, M.D. Director, Glenn Family Breast Center Associate Professor Department of Radiation Oncology Winship Cancer Institute
Promise of a beautiful day
 Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
Conservative Surgery and Radiation Stage I and II Breast Cancer
 Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
Breast Cancer Breast Managed Clinical Network
 Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Diseases of the breast (2 of 2) Breast cancer
 Breast cancer") Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Table of contents. Page 2 of 40
 Page 1 of 40 Table of contents Introduction... 4 1. Background Information... 6 1a: Referral source for the New Zealand episodes... 6 1b. Invasive and DCIS episodes by referral source... 7 1d. Age of the
Page 1 of 40 Table of contents Introduction... 4 1. Background Information... 6 1a: Referral source for the New Zealand episodes... 6 1b. Invasive and DCIS episodes by referral source... 7 1d. Age of the
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Ahmad Elahi*, Gholamreza Toogeh,Habibollah Mahmoodzadeh, Behnaz Jahanbin, Farhad Shahi,
 Clinical Experience Open Access DOI: 10.1187/abc.20185258-62 Ductal Carcinoma In Situ Close to the Inked Margin: A Case Presented in Multidisciplinary Session With Clinical Discussion and Decision Making
Clinical Experience Open Access DOI: 10.1187/abc.20185258-62 Ductal Carcinoma In Situ Close to the Inked Margin: A Case Presented in Multidisciplinary Session With Clinical Discussion and Decision Making
Breast Cancer: Who Gets It? Who Survives? The Latest Information
 Breast Cancer: Who Gets It? Who Survives? The Latest Information James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine
Breast Cancer: Who Gets It? Who Survives? The Latest Information James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
SFMC Breast Cancer Site Study: 2011
 SFMC Breast Cancer Site Study: 2011 Introduction Breast cancer is the most frequently diagnosed cancer among American women, except for skin cancers. It is the second leading cause of cancer death in women,
SFMC Breast Cancer Site Study: 2011 Introduction Breast cancer is the most frequently diagnosed cancer among American women, except for skin cancers. It is the second leading cause of cancer death in women,
Clinical Management Guideline for Breast Cancer
 Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Adjuvant Treatment Less than 4 positive lymph nodes ER Positive HER2 Negative (see page 2 & 3 ) Primary Diagnosis:
Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Adjuvant Treatment Less than 4 positive lymph nodes ER Positive HER2 Negative (see page 2 & 3 ) Primary Diagnosis:
Female Genital Tract Lab. Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan
 Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Mammographic imaging of nonpalpable breast lesions. Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand
 Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP
 Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Pathology: Grade 1 infiltrating ductal carcinoma with associated DCIS, Lymphvascular invasion present. ER+, PR+. Her 2/ IHC 1+, negative
 GATRA 2016 Breast Case Demographics Name: Autumn Leaf Sex: F Date of Birth: 3/26/75 SSN: 098765432 Race: African American Marital Status: Single Address: 3615 Burnt Hickory Trail, Helen, GA 37285, White
GATRA 2016 Breast Case Demographics Name: Autumn Leaf Sex: F Date of Birth: 3/26/75 SSN: 098765432 Race: African American Marital Status: Single Address: 3615 Burnt Hickory Trail, Helen, GA 37285, White
Breast Cancer? Breast cancer is the most common. What s New in. Janet s Case
 Focus on CME at The University of Calgary What s New in Breast Cancer? Theresa Trotter, MD, FRCPC Breast cancer is the most common malignancy affecting women in Canada, accounting for almost a third of
Focus on CME at The University of Calgary What s New in Breast Cancer? Theresa Trotter, MD, FRCPC Breast cancer is the most common malignancy affecting women in Canada, accounting for almost a third of
Tata Memorial Centre s opinion is summarized as follows:
 February 2 nd 2015 Dear Ms., Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online consultation
February 2 nd 2015 Dear Ms., Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online consultation
DCIS: Margins and the USC/VNPI
 DCIS: Margins and the USC/VNPI Van Nuys USC Hoag Melvin J. Silverstein, M.D Gross Endowed Chair in Oncoplastic Surgery Director, Hoag Breast Program Newport Beach, CA Clinical Professor of Surgery Keck
DCIS: Margins and the USC/VNPI Van Nuys USC Hoag Melvin J. Silverstein, M.D Gross Endowed Chair in Oncoplastic Surgery Director, Hoag Breast Program Newport Beach, CA Clinical Professor of Surgery Keck
Case 1. BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care
 BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
Disclosures. Premalignant Lesions of the Breast: What Clinicians Want and Why. NY Times: Prone to Error: Earliest Steps to Find Cancer.
 Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Bruno CUTULI Policlinico Courlancy REIMS. WORKSHOP SULL IRRADIAZIONE MAMMARIA IPOFRAZIONATA Il carcinoma duttale in situ
 Bruno CUTULI Policlinico Courlancy REIMS WORKSHOP SULL IRRADIAZIONE MAMMARIA IPOFRAZIONATA Il carcinoma duttale in situ XXI CONGRESSO AIRO GENOVA 22.11.2011 INTRODUCTION Due to wide diffusion of mammography,
Bruno CUTULI Policlinico Courlancy REIMS WORKSHOP SULL IRRADIAZIONE MAMMARIA IPOFRAZIONATA Il carcinoma duttale in situ XXI CONGRESSO AIRO GENOVA 22.11.2011 INTRODUCTION Due to wide diffusion of mammography,
Neoadjuvant Treatment of. of Radiotherapy
 Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Breast Cancer. For breast cancer, the mortality risk varies with the stage of the cancer.
 CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Breast Cancer Breast cancer is the most common cancer in women in the United States and second only to lung cancer as a cause of cancer deaths.
CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Breast Cancer Breast cancer is the most common cancer in women in the United States and second only to lung cancer as a cause of cancer deaths.
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Breast Cancer MultiDisciplinary Approach
 Breast Cancer MultiDisciplinary Approach October 30, 2012 Kristi Dolcetti RN, CON, CBPNC-IC OTN Bookings Regional Cancer Care is booking indirect Patient visits for our Multidisciplinary Cancer Conferences
Breast Cancer MultiDisciplinary Approach October 30, 2012 Kristi Dolcetti RN, CON, CBPNC-IC OTN Bookings Regional Cancer Care is booking indirect Patient visits for our Multidisciplinary Cancer Conferences
Interpretation of Breast Pathology in the Era of Minimally Invasive Procedures
 Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
Insights and Updates in Breast Cancer. No Disclosures. Learning Objectives. Mountain States Cancer Conference 2017 Regina Jeanise Brown MD
 Insights and Updates in Breast Cancer Mountain States Cancer Conference 2017 Regina Jeanise Brown MD 10/14/17 No Disclosures Learning Objectives Understand screening recommendations Understand the effectiveness
Insights and Updates in Breast Cancer Mountain States Cancer Conference 2017 Regina Jeanise Brown MD 10/14/17 No Disclosures Learning Objectives Understand screening recommendations Understand the effectiveness
Breast cancer staging update. Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director
 Breast cancer staging update Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director 1 1 Review of the AJCC 8 th edition breast cancer staging Review of genomic assays as stage modifiers
Breast cancer staging update Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director 1 1 Review of the AJCC 8 th edition breast cancer staging Review of genomic assays as stage modifiers
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
RADIOTHERAPY IN BREAST CANCER :
 RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
Cancer Endorsement Maintenance 2011-Maintenance Measures
 Measure Number Title Description Measure Steward 0210 Proportion receiving chemotherapy in the last 14 days of life 0211 Proportion with more than one emergency room visit in the last days of life 0212
Measure Number Title Description Measure Steward 0210 Proportion receiving chemotherapy in the last 14 days of life 0211 Proportion with more than one emergency room visit in the last days of life 0212
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Q&A. Fabulous Prizes. Collecting Cancer Data: Breast 4/4/13. NAACCR Webinar Series Collecting Cancer Data Breast
 Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Breast Cancer: Selected Topics for the Primary Care Clinician
 Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
So, Who are the appropriate individuals that should consider genetic counseling and genetic testing?
 Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
Journal of Breast Cancer
 CSE REPORT Journal of reast Cancer J reast Cancer 2016 December; 19(4): 459-464 Increased Malignant Microcalcifications after Neoadjuvant Chemotherapy in dvanced reast Cancer Gi Won Shin, Young Mi Park,
CSE REPORT Journal of reast Cancer J reast Cancer 2016 December; 19(4): 459-464 Increased Malignant Microcalcifications after Neoadjuvant Chemotherapy in dvanced reast Cancer Gi Won Shin, Young Mi Park,
Systemic Treatment of Breast Cancer. Hormone Therapy and Chemotherapy, Curative and Palliative
 Systemic Treatment of Breast Cancer Hormone Therapy and Chemotherapy, Curative and Palliative Systemic Therapy Invasive breast cancers Two forms Curative Palliative Curative Systemic Therapy Adjuvant Therapy
Systemic Treatment of Breast Cancer Hormone Therapy and Chemotherapy, Curative and Palliative Systemic Therapy Invasive breast cancers Two forms Curative Palliative Curative Systemic Therapy Adjuvant Therapy
Measure Definition Benchmark Endorsed By. Measure Definition Benchmark Endorsed By
 Process Risk Assessment Tumor Site: Breast Process Presence or Risk absence Assessment of cancer in first-degree blood relatives documented in patients with invasive breast Presence cancer or absence of
Process Risk Assessment Tumor Site: Breast Process Presence or Risk absence Assessment of cancer in first-degree blood relatives documented in patients with invasive breast Presence cancer or absence of
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery
 Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
BREAST CANCER PATHOLOGY
 BREAST CANCER PATHOLOGY FACT SHEET Version 4, Aug 2013 This fact sheet was produced by Breast Cancer Network Australia with input from The Royal College of Pathologists of Australasia I m a nurse and know
BREAST CANCER PATHOLOGY FACT SHEET Version 4, Aug 2013 This fact sheet was produced by Breast Cancer Network Australia with input from The Royal College of Pathologists of Australasia I m a nurse and know
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Jose A Torres, MD 1/12/2017
 Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer
 The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer Le défi des traitements locorégionaux individualisés pour les patientes présentant un cancer du sein
The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer Le défi des traitements locorégionaux individualisés pour les patientes présentant un cancer du sein
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
BREAST CANCER SITE STUDY REPORT By Robert O. Maganini, M.D., F.A.C.S. Breast Surgeon, Alexian Brothers Medical Group
 BREAST CANCER SITE STUDY REPORT By Robert O. Maganini, M.D., F.A.C.S. Breast Surgeon, Alexian Brothers Medical Group Breast cancer is the most common cancer diagnosed in women around the world. In the
BREAST CANCER SITE STUDY REPORT By Robert O. Maganini, M.D., F.A.C.S. Breast Surgeon, Alexian Brothers Medical Group Breast cancer is the most common cancer diagnosed in women around the world. In the
Page 1. AHN-JHU Breast Cancer Symposium. Novel Local Regional Clinical Trials. Background. Neoadjuvant Chemotherapy Benefit.
 AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Watchful Waiting: Well Behaved Breast Cancers Non-Surgical Management of Breast Cancer
 Case Report imedpub Journals http://www.imedpub.com Journal of Adenocarcinoma DOI: 10.21767/2572-309X.10002 Watchful Waiting: Well Behaved Breast Cancers Non-Surgical Management of Breast Cancer Received:
Case Report imedpub Journals http://www.imedpub.com Journal of Adenocarcinoma DOI: 10.21767/2572-309X.10002 Watchful Waiting: Well Behaved Breast Cancers Non-Surgical Management of Breast Cancer Received:
RUTGERS CANCER INSTITUTE OF NEW JERSEY - ROBERT WOOD JOHNSON MEDICAL SCHOOL INTERDISCIPLINARY BREAST SURGERY FELLOWSHIP CORE EDUCATIONAL OBJECTIVES
 RUTGERS CANCER INSTITUTE OF NEW JERSEY - ROBERT WOOD JOHNSON MEDICAL SCHOOL INTERDISCIPLINARY BREAST SURGERY FELLOWSHIP CORE EDUCATIONAL OBJECTIVES At the completion of Breast Fellowship training, the
RUTGERS CANCER INSTITUTE OF NEW JERSEY - ROBERT WOOD JOHNSON MEDICAL SCHOOL INTERDISCIPLINARY BREAST SURGERY FELLOWSHIP CORE EDUCATIONAL OBJECTIVES At the completion of Breast Fellowship training, the
Breast Surgery: Yesterday, Today and Tomorrow
 Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
Collecting Cancer Data: Breast. Prizes! Collecting Cancer Data: Breast 8/4/ NAACCR Webinar Series 1. NAACCR Webinar Series
 Collecting Cancer Data: Breast NAACCR 2008 2009 Webinar Series Prizes! Question of the Month! The participant that submits the best question of the session will receive a fbl fabulous Pi Prize! Shannon
Collecting Cancer Data: Breast NAACCR 2008 2009 Webinar Series Prizes! Question of the Month! The participant that submits the best question of the session will receive a fbl fabulous Pi Prize! Shannon
Follow-up Care of Breast Cancer Patients
 Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 19 April 2018 Disclosures
Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 19 April 2018 Disclosures