TREATMENT UPDATES IN ACUTE LEUKEMIA. Shannon McCurdy, MD University of Pennsylvania
|
|
|
- Horace Carroll
- 6 years ago
- Views:
Transcription
1 TREATMENT UPDATES IN ACUTE LEUKEMIA Shannon McCurdy, MD University of Pennsylvania
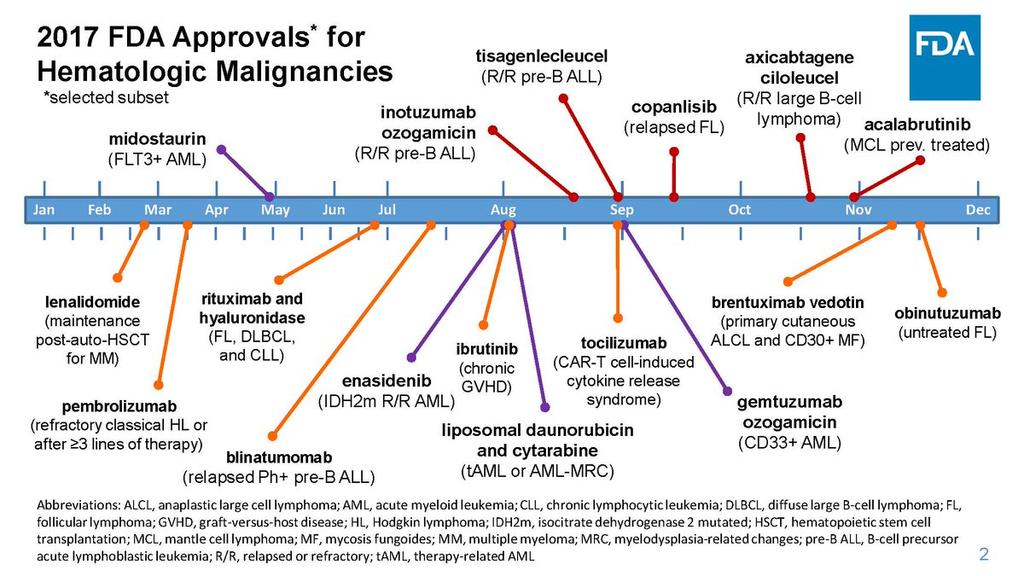
2 TIMELINE FOR FDA APPROVED AGENTS FOR AML Midostuarin Enasidenib Cytarabine + Daunorubicin (7+3) Gemtuzumab Ozogamicin approved Gemtuzumab Gemtuzumab Ozogamicin Ozogamicin withdrawn Liposomal Daunorubicin and Cytarabine
3
4 ACUTE MYELOID LEUKEMIA 4

5 MUTATIONAL LANDSCAPE: 200 CASES DE NOVO AML MUTATIONS: 1. FLT3 28% 2. NPM1 27% 3. DNMT3A 26% 4. IDH1 or IDH2 20% N Engl J Med 2013;368:
6 FLT3: MIDOSTAURIN Kinase inhibitor, including inhibition of FLT3 and KIT FDA Approved based on 717 patients with newly diagnosed AML with FLT3 ITD or FLT3 TKD (i.e. D835) Midostaurin 50mg PO BID Days 8-21 In combination with 7+3 induction In combination with HIDAC (ARA-C) consolidation Midostuarin 50mg daily continuous for up to 12 cycles (take with food) Approved as maintenance in Europe, but not in the U.S. 6
7 RATIFY/C10603 SCHEMA FLT3 SCREEN PRE-REGISTER Stratify* FLT3 ITD or TKD R A N D O M I Z E DNR 60 mg/m2 d1-3 ARA-C 200 mg/m2 d1-7 Midostaurin 50 mg BID d8-21 DNR 60 mg/m2 d1-3 ARA-C 200 mg/m2 d1-7 Placebo BID d8-21 CR CR HidAC Midostaurin HidAC Placebo X 4 X 4 Midostaurin MAINTENANCE 12 months Placebo MAINTENANCE 12 months FLT3 WILD TYPE not eligible for enrollment Stratification: TKD; ITD with allelic ratio <0.7 vs 0.7 Screened 3277 Age <60 to find 896 FLT3 mut+ patients; 717 randomized Stone RM, et al. NEJM 2017
 MIDOSTAURIN PLACEBO 44.3% (95%CI: 39, 50) PLACEBO SCT in CR1 HR 0.61 SCT, non-cr1 HR 0.98 Hazard Ratio*: 0.")
8 RATIFY/C10603 MIDOSTAURIN OVERALL SURVIVAL BENEFIT All patients Arm 4-year Survival Transplanted patients MIDOSTAURIN 51.4% (95%CI: 46, 57) MIDOSTAURIN PLACEBO 44.3% (95%CI: 39, 50) PLACEBO SCT in CR1 HR 0.61 SCT, non-cr1 HR 0.98 Hazard Ratio*: sided log-rank p-value*: Stone RM, et al. NEJM 2017
9 Forest Plot of OS by FLT3 status Mido effect on OS was similar across FLT3 subtypes
10 FLT3 Tyrosine Kinase Inhibitors in Development Quizartinib N O N O H Crenolanib O N N H O N H N S O N N O H 3 C CH 3 N OCH 3 Cl F F F Sorafenib O O O N H O N CH 3 Midostaurin N H N H N Gilteritinib
11 NEWER FLT3 INHIBITORS Drug Half life (dosing) D835 activity Selectivity Single agent Relapse/refractory Chemo combinations Quizartinib (AC220) Long (once daily) No Narrow, inhibits KIT Phase 3 enrollment complete Ph 1/2 completed, 1 Ph3 ongoing Crenolanib Short (TID) Yes Narrow, spares KIT N/A (Phase 3 with chemo ongoing) Ph 2 completed 2 Ph3 to open 2018 Gilteritinib (ASP2215) Long (once daily) Yes Narrow spares KIT Phase 3 ongoing Ph 1/2 ongoing 3 1. Altman JK, et al ASH abstracts 2013; Burnett AK, et al ASH abstracts Wang ES, et al. ASH Abstract 2017 # Pratz KW, et al. ASH Abstract 2017 #722
12 GILTERITINIB STUDY DESIGN AND TREATMENT Phase 1 study (NCT ): Patients aged 18 years with newly diagnosed AML Multicenter, open-label, 3+3 design Enrollment began 1/ 2015 Adult patients with newly diagnosed AML Dose-escalation cohorts of 40, 80, and 120 mg/day gilteritinib with 3 6 patients per cohort Dose Escalation Remission induction (1 2 cycles) Cytarabine (100 mg/m 2 ; Days 1 7) + Idarubicin (12 mg/m 2 ; Days 1 3) + Gilteritinib (once daily, Days 1 14 or 4 17*) Consolidation (1 3 cycles) DLT Observation More than 20 patients in the doseexpansion cohort, including 15 FLT3 Mut+ patients Cytarabine (1.5 g/m 2 q12h; Days 1, 3, and 5) + Gilteritinib (once daily, Days 1 14) Maintenance (up to 26 cycles) Gilteritinib (once daily) Pratz et al. ASH 2017
13 GILTERITINIB DOSE-LIMITING TOXICITIES AND TEAES Gilteritinib 40 mg/day Days 1 14, 2 patients had DLT with prolonged neutropenia and thrombocytopenia (n=1) and decreased ejection fraction (n=1) Subsequently modified to Days 4 17 with no further DLTs in 40 or 80mg/day The MTD was not reached Gilteritinib 120 mg/day was chosen as the first expansion dose Dose escalation in the 200 mg/day gilteritinib cohort is ongoing Grade 3 TEAEs in 10%: febrile neutropenia (36.7%), thrombocytopenia (18.4%), neutropenia (16.3%), and decreased platelet count (12.2%) Serious TEAEs: febrile neutropenia (n=8), sepsis (n=2), small intestinal obstruction (n=2), lung infection (n=2), and decreased ejection fraction (n=2), no deaths from TEAEs Pratz et al. ASH 2017
14 ANTILEUKEMIC RESPONSE: FLT3 MUT+ Response Parameter*, n (%) FLT3 Mut+ (n=21) CR 19 (90.5) CRp 1 (4.8) CRi 1 (4.8) PR 0 CRc 21 (100) CR, complete remission; CRc, composite complete remission; CRi, complete remission with incomplete hematologic recovery; CRp, complete remission with incomplete platelet recovery; FLT3, fms-like tyrosine kinase 3; Mut+, mutationpositive; PR, partial remission; WT, wild-type. *Response parameters were defined according to the International Working Group Criteria for AML (Cheson B, et al. J Clin Oncol. 2003;12(24): ). Two patients were excluded from the response analysis population: one patient was excluded due to favorable cytogenetic status and one patient was excluded due to refusal to undergo a bone marrow biopsy and withdrawal of consent. CRc included patients who achieved CR, CRp, and CRi. Pratz et al. ASH 2017

15 IDH2: ENASIDENIB FDA approved for the treatment of adult patients with relapsed or refractory AML with an IDH2 mutation Based on AG221-C-001 (NCT ) Single arm study of 199 adults with relapsed or refractory AML with an IDH2 mutation Enasidenib 100mg PO daily 23% CR/CRh lasting 8.2 months Median time to first response was 1.9 months Median time to best response was 3.7 months Stein EM, Dinardo CD, et. al. Blood % of transfusion-dependent patients became transfusion-independent 76% of transfusion-independent patients maintained transfusion independence Side effects >20%: Nausea, vomiting, diarrhea, elevated bilirubin, decreased appetite 15
 Bone pain (27%) Weight gain/edema (21%) Pleural (45%) or pericardial effusion (18%) Onset range: 10 days to 5 months Hyperleukocytosis not necessary to develop differentiation")
16 ENASIDENIB DIFFERENTIATION SYNDROME Differentiation Syndrome occurs in 14% associated with: Respiratory symptoms such as supplemental oxygen requirement (76%) Renal dysfunction (70%) Fever (36%) Lymphadenopathy (33%) Bone pain (27%) Weight gain/edema (21%) Pleural (45%) or pericardial effusion (18%) Onset range: 10 days to 5 months Hyperleukocytosis not necessary to develop differentiation syndrome Treatment: Dexamethasone 10mg BID and hemodynamic monitoring Taper steroids after symptom resolution If severe pulmonary symptoms (requiring intubation) and/or renal dysfunction >48 hours, stop Enasidenib 16
17 IDH1 INHIBITOR: IVOSIDENIB SINGLE-ARM, OPEN-LABEL, PHASE 1 study Dose escalation (n=78) Enrollment complete Patients with midh1+ advanced hematologic malignancies Oral ivosidenib daily in continuous 28-day cycles Doses included 100 mg BID, 300, 500, 800, 1200 mg QD Dose expansion (n=180) Enrollment complete: 500 mg QD in continuous 28-day cycles R/R AML in 2nd+ relapse, relapse after SCT, refractory to induction or reinduction, or relapse within 1 year, n=126 Untreated AML not eligible for SOC, n=25 Other non-aml midh1 R/R advanced hematologic malignancies, n=11 Other R/R AML not eligible for Arm 1, n=18 ClinicalTrials.gov NCT Dinardo et al. Abstract 725 ASH 2017
18 IVOSIDENIB MOST COMMON AES ( 15%) (N=258) All treated patients, N=258 Any grade, n (%) Grade 3, n (%) Any AE 255 (98.8) 200 (77.5) Diarrhea 86 (33.3) 6 (2.3) Leukocytosis 78 (30.2) 17 (6.6) Nausea 76 (29.5) 3 (1.2) Fatigue 74 (28.7) 8 (3.1) Febrile neutropenia 65 (25.2) 64 (24.8) Dyspnea 61 (23.6) 9 (3.5) Anemia 60 (23.3) 49 (19.0) Electrocardiogram QT prolonged 58 (22.5) 23 (8.9) Edema peripheral 56 (21.7) 0 (0.0) Pyrexia 53 (20.5) 4 (1.6) Decreased appetite 51 (19.8) 4 (1.6) Constipation 48 (18.6) 2 (0.8) Cough 48 (18.6) 1 (0.4) Hypokalemia 45 (17.4) 7 (2.7) Vomiting 45 (17.4) 3 (1.2) Arthralgia 41 (15.9) 5 (1.9) Thrombocytopenia 41 (15.9) 35 (13.6) Top 10 Adverse Events: 1. Diarrhea 33% 2. Leukocytosis 30% 3. Nausea 30% 4. Fatigue 29% 5. Neutropenic Fever 25% 6. Dyspnea 24% 7. Anemia 23% 8. QT prolongation 23% 9. Edema 22% 10. Decreased Appetite 20% Dizziness 40 (15.5) 1 (0.4) Epistaxis 39 (15.1) 2 (0.8) Dinardo et al. Abstract 725 ASH 2017
19 IVOSIDENIB AES OF INTEREST Leukocytosis Grade 3 leukocytosis reported in 10/125 patients (8%) Managed with hydroxyurea None were fatal QT prolongation Grade 3 QT prolongation reported in 10/125 patients (8%) Study drug was reduced in 1 patient and held in 5 patients (all grades) None were Grade 4 or fatal IDH-differentiation syndrome (IDH-DS) All grade reported in 12/125 patients (9.6%) 4/12 had co-occurring leukocytosis Managed with corticosteroids and diuretics, and hydroxyurea if accompanied by leukocytosis None were Grade 4 or fatal Best response for the 12 patients with IDH- Differentiation Syndrome: Best Response CR CRh CRi/CRp MLFS SD n= Grade 3 = WBC > 100,000/mm 3 ; Grade 4 = clinical manifestations of leukostasis, urgent intervention indicated Dinardo et al. Abstract 725 ASH 2017
20 IVOSIDENIB RESPONSE IN RELAPSED/REFRACTORY AML (N=125) Primary R/R AML Set (n=125) CR+CRh rate, n (%) [95% CI] 38 (30.4%) [22.5, 39.3] Time to CR/CRh, median (range) months 2.7 (0.9, 5.6) Duration of CR/CRh, median [95% CI] months 8.2 [5.5, 12.0] CR rate, n (%) [95% CI] 27 (21.6%) [14.7, 29.8] Time to CR, median (range) months 2.8 (0.9, 8.3) Duration of CR, median [95% CI] months 9.3 [5.6, 18.3] CRh rate, n (%) 11 (8.8%) Overall Response Rate, n (%) [95% CI] 52 (41.6%) [32.9, 50.8] Time to first response, median (range) months 1.9 (0.8, 4.7) Duration of response, median [95% CI] months 6.5 [4.6, 9.3] CRh = 6 patients with investigator assessed responses of CRi/CRp and 5 with MLFS Dinardo et al. Abstract 725 ASH 2017
21 IVOSIDENIB RESPONSE IN UNTREATED AML AND MDS Characteristic Untreated AML Arm 2 a (n=34) Women / men, n 15 / 19 Age in years, median (range) 76.5 (64 87) ECOG PS at screening, n (%) (23.5) 20 (58.8) Prior MDS, n (%) 18 ( 52.9) Response Overall Response Rate, n (%) [95% CI] 19 (55.9) [37.9, 72.8] MDS Arm 3 b (n=12) 3 / (52 78) 4 (33.3) 6 (50.0) NA 11 (91.7) [61.5, 99.8] Duration of response, median [95% CI] months Duration of CR, median [95% CI] months 9.2 [1.9, NE] NE [5.6, NE] NE [2.3, NE] NE [2.8, NE] a Untreated AML patients not eligible for standard of care therapies in expansion Arm 2 and from dose escalation whose starting dose was 500 mg QD b MDS patients in expansion Arm 3 and from dose escalation whose starting dose was 500 mg QD Dinardo et al. Abstract 725 ASH 2017
 PHASE 2 (2:1 RANDOMIZATION) Newly diagnosed AML Age 18")


 PRIMARY ENDPOINTS: Recommended")


; enrollment is now closed ClinicalTrials.")

22 IDH INHIBITORS WITH AZACITIDINE KEY ELIGIBILITY CRITERIA PHASE 1B (3+3 DESIGN) PHASE 2 (2:1 RANDOMIZATION) Newly diagnosed AML Age 18 Ineligible for intensive chemotherapy Pts with antecedent hematologic disorders allowed but prior HMA excluded midh1 midh2 Dose-finding* Ivosidenib + AZA n=7 Dose-finding* Enasidenib + AZA n=6 Expansion Ivosidenib + AZA n=15 Follow-up midh2 Randomization 2 1 Enasidenib 100mg QD + SC AZA n=66 SC AZA Monotherapy n=33 Follow-up SC AZA 75mg/m 2 /day x 7 days/ 28-day cycle (all study phases) PRIMARY ENDPOINTS: Recommended combination dose (RCD); safety KEY SECONDARY ENDPOINTS: Overall response rate PK/PD QOL outcomes PRIMARY ENDPOINT: PRIMARY ENDPOINT Overall response rate KEY SECONDARY ENDPOINTS: Safety Event-free survival Overall survival *Dose finding for enasidenib or ivosidenib; AZA dose remained constant 4 pts had enrolled in expansion as of data cutoff (1 Sep 2017); enrollment is now closed ClinicalTrials.gov NCT AML, acute myeloid leukemia; AZA, azacitidine; IC, induction chemotherapy; ORR, overall response rate; QOL, quality of life; RCD, recommended combination dose Dinardo et al. Abstract 639 ASH
23 ENASIDENIB + AZACITIDINE: TREATMENT-EMERGENT ADVERSE EVENTS Median enasidenib Tx cycles: 9 (range 1-13) Most common TEAEs (any grade): nausea, hyperbilirubinemia (n=4 each) IDH-differentiation syndrome (IDH-DS) occurred in 1 pt in the enasidenib 200-mg arm Grade 3-4 treatment-emergent adverse events Enasidenib 100 mg + AZA (n=3) Enasidenib 200 mg + AZA (n=3) Enasidenib + AZA Total (N=6) n (%) Hematological Neutropenia 0 2* (67) 2* (33) Thrombocytopenia 0 1* (33) 1* (17) Febrile neutropenia 0 1* (33) 1* (17) Anemia 0 1* (33) 1* (17) Lymphocyte count decreased 0 1 (33) 1 (17) WBC count decreased 0 1 (33) 1 (17) Non-hematological Pneumonia 1 (33) 1 (33) 2 (33) Hyperbilirubinemia 1 (33) 1* (33) 2* (33) Colitis 1 (33) 0 1 (17) Upper respiratory tract infection 1 (33) 0 1 (17) Hypocalcemia 1 (33) 0 1 (17) Hypokalemia 1 (33) 0 1 (17) Hypophosphatemia 1 (33) 0 1 (17) Hemorrhoidal hemorrhage 1 (33) 0 1 (17) Hypoxia 0 1 (33) 1 (17) Embolism 0 1* (33) 1* (17) Dinardo et al. Abstract 639 ASH 2017 *One event considered to be treatment-related 23
24 IVOSIDENIB (IDH1 INHBITOR) + AZACITIDINE Median ivosidenib Tx cycles: 3.0 (1-13) Most common TEAEs (any grade): nausea (n=8), constipation (6), fatigue (5), diarrhea (4) IDH-1 case of differentiation syndrome 1 death on-study d/t pneumonia Grade 3-4 treatment-emergent adverse events Hematological Anemia 2* (18) Febrile neutropenia 2 (18) Neutropenia 1* (9) Thrombocytopenia 1* (9) Non-hematological Pneumonia 2 (18) Constipation 1* (9) Dizziness 1 (9) Atrial fibrillation 1 (9) Blood creatinine increased 1* (9) IDH differentiation syndrome 1* (9) Parainfluenza virus infection 1 (9) Sepsis 1 (9) Cellulitis 1 (9) INR increased 1 (9) Gastrointestinal hemorrhage 1 (9) Ivosidenib 500 mg + AZA (N=11) n (%) 24 *One event was considered to be treatment-related Dinardo et al. Abstract 639 ASH 2017
25 OVERALL RESPONSE RATES FOR IDH INHBITORS + AZACITIDINE Overall response rate (ORR): CR + CRi/CRp + PR + MLFS (IWG 2003) Enasidenib + AZACITIDINE: ORR: 4 of 6 (67%) In the enasidenib 100 mg + AZA arm, 2 pts achieved CR In the enasidenib 200 mg + AZA arm, 1 pt achieved PR and 1 had MLFS Ivosidenib (IDH1 inhibitor) 500 mg + AZACITIDINE: ORR: 8 of 11 (73%) 4 pts achieved CR, 1 achieved CRi, 1 achieved PR, and 2 pts had MLFS CR = morphologic complete remission; CRi = morphologic complete remission with incomplete neutrophil recovery; CRp = morphologic complete remission with incomplete platelet recovery; PR = partial remission; MLFS = morphologic leukemia-free state; SD = stable disease; PD = progressive disease; MR = morphologic relapse after CR/CRi/CRp Dinardo et al. Abstract 639 ASH
 stopped early due to increased induction mortality and VOD 2010 GO pulled from the market 2015 Lower dose of GO with")
26 GEMTUZUMAB OZOGAMICIN (GO) FDA approved for adults with de novo CD33 + AML History: 2000 Granted accelerated approval as a single agent (9mg/m 2 x 2 14 days apart) for patients 60 years+ with relapsed CD33 + AML 2009 SWOG S0106 trial of GO with 7+3 (6mg/m 2 D4) stopped early due to increased induction mortality and VOD 2010 GO pulled from the market 2015 Lower dose of GO with 7+3 submitted based on ALFA-0701 (3mg/m 2 D1, D4, D7 of induction, D1 of consolidation cycles 1 and 2) Castaigne S, et al. Lancet yr EFS & OS 40.8% and 53.2% 2-yr EFS and OS 17.1% and 41.9% Schrama D, et al Nat Rev Drug Dev 2006
27 META-ANALYSIS: VOD RATE BY GO MONOTHERAPY DOSE IN PATIENTS WITH RELAPSED/REFRACTORY AML GO dose N VOD incidence (95% CI) 9 mg/m2 x 2 (10 studies combined) % (3.5, 8.1) 6 mg/m2 x 2 (7 studies combined) % (6.4, 26.4) 3 mg/m2 d1, 4, 7 (3 studies combined) 87 0% (0.0, 1.1) 27

28 GEMTUZUMAB OZOGAMICIN + INTENSIVE CHEMOTHERAPY Age <60, CBF+ Survival benefit Age >60 Survival benefit No benefit, used 6 mg/m2 No benefit, used 6 mg/m2 Age 50-70, Survival benefit Hills R, et al. Lancet Oncol, 2014
29 BENEFIT WITH GO SEEN IN CORE BINDING FACTOR (CBF) LEUKEMIA CBF t(8;21); inv(16) Intermediate Adverse Hills RK, et al. Lancet Oncol
30 SPLICING VARIANT FOR CD33 ASSOCIATED WITH ALTERNATE ISOFORM AND LACK OF BENEFIT FROM GO Eliminates CD33 IgV domain, which is the antibody-binding site for GO Lamba, et al. JCO
, AML with prior history of MDS, or AML with")

31 VYXEOS (CPX-531) Liposome-encapsulated combination of Ara-C and Dauno FDA approved for adults with newly-diagnosed therapy-related AML (t-aml), AML with prior history of MDS, or AML with cytogenetic abnormalities diagnostic for MDS 100 nm bilamellar liposomes 5:1 molar ratio of cytarabine to daunorubicin 1 unit = 1.0 mg cytarabine plus 0.44 mg daunorubicin Lancet et al. ASCO Abstract 2016

32 PHASE 3 STUDY CPX-351 VS STANDARD INDUCTION IN YEAR OLD PATIENTS WITH NEWLY DIAGNOSED TREATMENT RELATED, SECONDARY AML, OR AML-MRC CPX-351 n= unit = 1 mg cytarabine mg daunorubicin n=156 First Induction 100 units/m 2 Days 1, 3 and 5 First Induction Cytarabine: 100 mg/m 2 x 7 d Daunorubicin: 60 mg/m 2 x 3 d Re-induction 100 units/m 2 Days 1 and 3 Re-induction Cytarabine: 100 mg/m 2 x 5 d Daunorubicin: 60 mg/m 2 x 2 d Consolidation 65 units/m 2 Days 1 and 3 Consolidation Cytarabine: 100 mg/m 2 x 5 d Daunorubicin: 60 mg/m 2 x 2 d Lancet et al. ASCO Abstract
33 VYXEOS (CPX-351) IMPROVES OVERALL AND POST-TRANSPLANT SURVIVAL Lancet et al. ASCO Abstract 2016
34 VYXEOS (CPX-351) IMPROVED 30 AND 60 DAY MORTALITY AND CR RATES 60-day mortality CR rates Lancet J, et al. ASCO 2016
35 LONGER DURATION TO NEUTROPHIL AND PLATELET RECOVERY WITH VYEXOS ANC 500/uL Platelets 50,000/uL CPX CPX Patients Receiving 1 Induction n=58 n=34 n=58 n=34 Median (days) Patients Receiving 2 Inductions n=15 n=18 n=15 n=18 Median (days) Lancet et al. ASCO Abstract 2016 Lancet J, et al. ASCO
36 ACUTE LYMPHOBLASTIC LEUKEMIA 36
37 BLINATUMOMAB FDA approved for relapsed or refractory pre-b ALL in adults and children, confirmed clinical benefit after accelerated approval and expanded indication to Ph+ relapse or refractory pre-b ALL TOWER (NCT ) Blinatumomab at 9 mcg/day on days 1-7 and 28mcg/day on days 8-28 and for subsequent cycles Improved OS with median 7.7 months vs. 4.0 months in the SOC arm ALCANTARA (NCT ) Expanded indication to Ph+ with 45 patients with disease resistance or intolerance to second generation TKI and imatinib 36% complete remission rate, duration median 6.7 months Premedication with dexamethasone, very short half-life T cell CD3 BiTE B or pre-b CD19 cell T cell B or pre-b cell 37
38 BLINATUMOMAB TOWER STUDY FOR RELAPSED/REFRACTORY ALL N=189 Response Rate: CR and CRh: 43% of patients within the first 2 cycles 82% of whom were MRD negative 40% bridged to allo SCT, which led to durable remissions.now Being Studied Combined with Induction Chemotherapy in Newly Diagnosed Ph- Pre-B ALL Topp et al; Lancet Oncology, 2014 Toxicities Neurologic (delirium, seizure, other) 58% any grade; 13% Grade 3 or 4 Mostly in Cycle 1 Cytokine Release Syndrome 2% Grade 3 >50% blasts; pre-phase treatment with high dose dexamethasone Stepwise dosing for cycle 1 (9µg/d x 7 days then 28µg/d x 21 days) Pre-treatment 20mg Dexamethasone before D1 and Dose Escalations Fever occurs in 60% Mortality 23 (12%) fatal adverse events (mostly sepsis) No patient in remission died during therapy
39 INOTUZUMAB OZOGAMICIN FDA approved for relapsed/refractory pre-b ALL Dosing 0.8 mg/m2 on Day 1, then 0.5mg/m2 on Days 8 and 15 First cycle days, subsequent cycles 28 days with full dosing if CR not achieved Phase 3 INO-VATE ALL (NCT ) n= 326 Inotuzumab ozogamicin (n=164) vs. investigator s choice chemo (n=162) ITT 35.8% CR for median 8 months (89.7% MRD negative) vs. 17.4% CR for median 4.9 months (31.6% MRD negative) ITT analysis CR/CRi rate was 80.7% (78.4% MRD negative) vs. 29.4% (28.1% MRD negativity) PFS was 5 vs. 1.8 months; OS was 7.7 vs. 6.7 months KANTARJIAN HM ET AL. N ENGL J MED 2016;375:
40 INOTUZUMAB OZOGAMICIN CD22 MoAb bound to calicheamicin Adverse Reactions: Cytopenias Infection Hemorrhage Neutropenic fever/fever Nausea Headache Transaminitis, hyperbilirubinemia Abdominal pain VOD/SOS in 11% May prolong the QT when combined with other QT prolonging agents Thomas X. Blood and Lymphatic Cancer: Targets and Therapy
 Kantarjian et al.")
41 MINI-HYPERCVAD PLUS INOTUZUMAB OZOGAMICIN IN ALL PATIENTS 60 20% 5-yr survival in older patients SEER, 2013 American Cancer Society.: Cancer Facts and Figures, Also being studied in EWALL-INO NCT in a phase 2 in combination with the first two treatment cycles only (vs. 4 used above) Kantarjian et al. The Lancet Oncology Jan The Lancet Oncology DOI: ( /S (18) )


, which can be treated")


42 TISAGENLECLEUCEL (KYMRIAH) nd or later relapse for ALL age 25 years T cell Approval based on trial of 63 pediatric and young adult patients with an 83% remission rate at 3 months Black box warning for cytokine release syndrome (CRS), which can be treated with Tocilzumab, REMS program required Native TCR CTL019 cell CD19 Dead tumor cell Anti-CD19 CAR construct Black box warning for neurologic symptoms Tumor cell Milone, et al. Mol Ther 2009 Carpenito, et al. PNAS 2009
 CRS manageable with no deaths due to CRS CR/CRi 83% Grupp et al, ASH 2016:")
43 ELIANA: FIRST GLOBAL MULTI-CENTER CAR T CELL TRIAL IN PEDIATRIC ALL 94% of pts received CTL centers across 11 countries (US, EU, Canada, Australia, Japan) CRS manageable with no deaths due to CRS CR/CRi 83% Grupp et al, ASH 2016: Abstract 221

44 THERE IS ALWAYS HOPE 44

45 Slide Contributors: Mark Levis Keith Pratz Courtney Dinardo Alexander Perl Noelle Frey THANK YOU!

 Arm D1 (n=25) + Arm E1 (n=25)")
46 VENETOCLAX + HMAS PRATZ ET AL. ABSTRACT EHA Patients received DEC or AZA with VEN given as a continuous 400-mg dose versus 800- mg dose for 28 days during cycle 1 Shortened duration of 800-mg dose during subsequent cycles in patients with leukemia clearance to allow for recovery of the absolute neutrophil count (ANC) Arm D1 (n=25) + Arm E1 (n=25) Cycle 1 Ramp-Up Arm D2 (n=25) + Arm E2 (n=25) Cycle 1 Ramp-Up 46
47 PATIENT CHARACTERISTICS Characteristic N=100 Age, median (range), years 72.5 (65 86) 75 years, n (%) 39 (39) Male, n (%) 61 (61) ECOG performance score, n (%)* Baseline bone marrow blast count, n (%) >50 Cytogenetics, n (%) Intermediate Poor 26 (26) 58 (58) 15 (15) 32 (32) 32 (32) 36 (36) 47 (47) 53 (53) Secondary AML, n (%) 22 (22) *Data were missing for 1 patient. Defined in the 2014 NCCN guidelines, version 2. PRATZ ET 47 All AL. data ABSTRACT as of 17-Feb-2017 EHA 2017.

48 RESPONSE RATES BY IWG CRITERIA WITH 2 DOSING SCHEDULES OF VEN IN COMBINATION WITH HMAS 76% 68% 72% 56% 68% CR + CRi Arm VEN + DEC 400 mg n=25 * * * DEC 800 mg n=25 AZA 400 mg n=25 AZA 800 mg n=25 N=100 *One patient each in arms D1, D2, and E1 discontinued before assessment. Also in arm D2, 1 patient was still on active treatment at the time of this analysis and had no response reported. RD = resistant disease MLFS = morphological leukemia-free state PRATZ ET AL. ABSTRACT EHA
49 OS FOR ALL PATIENTS Median time since first dose of study drug: 9 months Survival estimates: 79% (95% CI: 70 86%) at 6 months 70% (95% CI: 59 79%) at 12 months Median OS has not been reached PRATZ ET AL. ABSTRACT EHA
50 CONCLUSIONS: IDH INHIBITORS + AZACITIDINE Enasidenib or Ivosidenib + AZA combinations well tolerated grade 1-2 GI events: indirect bilirubinemia in enasidenib-treated d/t off-target inhibition of UGT1A1 enzym11 pts remained on-study at data cutoff Phase 1b confirms 100 mg enasidenib + AZA and 500 mg ivosidenib + AZA for further study Ongoing studies of midh inhibitors + AZA: Randomized phase 2 portion of the current study of enasidenib + AZA (enrollment complete in the ivosidenib + AZA arm) Phase 3 placebo-controlled AGILE study of ivosidenib + AZA (NCT ) in newly diagnosed AML not suitable for intensive therapy Dinardo et al. Abstract 725 ASH
IDH1 AND IDH2 MUTATIONS
 Mutant Isocitrate Dehydrogenase (midh) Inhibitors, Enasidenib or Ivosidenib, in Combination with Azacitidine (AZA): Preliminary Results of a Phase 1b/2 Study in Patients with Newly Diagnosed Acute Myeloid
Mutant Isocitrate Dehydrogenase (midh) Inhibitors, Enasidenib or Ivosidenib, in Combination with Azacitidine (AZA): Preliminary Results of a Phase 1b/2 Study in Patients with Newly Diagnosed Acute Myeloid
Acute Myeloid Leukemia: State of the Art in 2018
 Acute Myeloid Leukemia: State of the Art in 2018 Harry P. Erba, MD, PhD Professor, Department of Medicine Director, Leukemia Program Duke University Durham, NC Treatment Paradigm of Adults with AML Fit
Acute Myeloid Leukemia: State of the Art in 2018 Harry P. Erba, MD, PhD Professor, Department of Medicine Director, Leukemia Program Duke University Durham, NC Treatment Paradigm of Adults with AML Fit
Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias
 Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias Relevant financial relationships in the past twelve months by presenter or spouse/partner. Speakers bureau: Novartis, Janssen, Gilead, Bayer The
Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias Relevant financial relationships in the past twelve months by presenter or spouse/partner. Speakers bureau: Novartis, Janssen, Gilead, Bayer The
Acute Myeloid and Lymphoid Leukemias
 Acute Myeloid and Lymphoid Leukemias Hugo F. Fernandez, MD Department of Malignant Hematology & Cellular Therapy Moffitt at Memorial Healthcare System April 29, 2018 15 th Annual Miami Cancer Meeting Objectives
Acute Myeloid and Lymphoid Leukemias Hugo F. Fernandez, MD Department of Malignant Hematology & Cellular Therapy Moffitt at Memorial Healthcare System April 29, 2018 15 th Annual Miami Cancer Meeting Objectives
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain
 June 22-25, 2017 Madrid, Spain") Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Enasidenib Monotherapy is Effective and Well-Tolerated in Patients with Previously Untreated Mutant-IDH2 Acute Myeloid Leukemia
 Enasidenib Monotherapy is Effective and Well-Tolerated in Patients with Previously Untreated Mutant-IDH2 Acute Myeloid Leukemia Pollyea DA 1, Tallman MS 2,3, de Botton S 4,5, DiNardo CD 6, Kantarjian HM
Enasidenib Monotherapy is Effective and Well-Tolerated in Patients with Previously Untreated Mutant-IDH2 Acute Myeloid Leukemia Pollyea DA 1, Tallman MS 2,3, de Botton S 4,5, DiNardo CD 6, Kantarjian HM
Acute Myeloid Leukemia
 Acute Myeloid Leukemia Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outline Molecular biology Chemotherapy and Hypomethylating agent Novel Therapy
Acute Myeloid Leukemia Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outline Molecular biology Chemotherapy and Hypomethylating agent Novel Therapy
Novel Induction and Targeted Strategies in Acute Myeloid Leukemia
 Novel Induction and Targeted Strategies in Acute Myeloid Leukemia Eytan M. Stein, MD Leukemia Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College New York, New York Current Paradigms
Novel Induction and Targeted Strategies in Acute Myeloid Leukemia Eytan M. Stein, MD Leukemia Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College New York, New York Current Paradigms
Acute Myeloid Leukemia Progress at last
 Acute Myeloid Leukemia Progress at last Bruno C. Medeiros, MD September 9, 217 Introduction Mechanisms of leukemogenesis Emerging therapies in AML Previously untreated AML Relapsed and refractory patients
Acute Myeloid Leukemia Progress at last Bruno C. Medeiros, MD September 9, 217 Introduction Mechanisms of leukemogenesis Emerging therapies in AML Previously untreated AML Relapsed and refractory patients
Summary of Key AML Abstracts Presented at the American Society of Hematology (ASH) December 2-6, San Diego CA
 December 2-6, San Diego CA") Summary of Key AML Abstracts Presented at the American Society of Hematology (ASH) December 2-6, 2016 - San Diego CA ASH 2016 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://ash.confex.com/ash/2016/webprogram/start.html
Summary of Key AML Abstracts Presented at the American Society of Hematology (ASH) December 2-6, 2016 - San Diego CA ASH 2016 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://ash.confex.com/ash/2016/webprogram/start.html
Ivosidenib (IVO; AG-120) in mutant IDH1 relapsed/refractory acute myeloid leukemia (R/R AML): Results of a phase 1 study
 in mutant IDH1 relapsed/refractory acute myeloid leukemia (R/R AML): Results of a phase 1 study") 7000 Ivosidenib (IVO; AG-120) in mutant IDH1 relapsed/refractory acute myeloid leukemia (R/R AML): Results of a phase 1 study Daniel A Pollyea 1, Courtney D DiNardo 2, Stéphane de Botton 3, Eytan M Stein
7000 Ivosidenib (IVO; AG-120) in mutant IDH1 relapsed/refractory acute myeloid leukemia (R/R AML): Results of a phase 1 study Daniel A Pollyea 1, Courtney D DiNardo 2, Stéphane de Botton 3, Eytan M Stein
ENASIDENIB IN MUTANT-IDH2 RELAPSED OR REFRACTORY ACUTE MYELOID LEUKEMIA (R/R AML): RESULTS OF A PHASE 1 DOSE- ESCALATION AND EXPANSION STUDY
: RESULTS OF A PHASE 1 DOSE- ESCALATION AND EXPANSION STUDY") ENASIDENIB IN MUTANT-IDH2 RELAPSED OR REFRACTORY ACUTE MYELOID LEUKEMIA (R/R AML): RESULTS OF A PHASE 1 DOSE- ESCALATION AND EXPANSION STUDY Eytan M. Stein, Courtney D. DiNardo, Daniel A. Pollyea, Amir
ENASIDENIB IN MUTANT-IDH2 RELAPSED OR REFRACTORY ACUTE MYELOID LEUKEMIA (R/R AML): RESULTS OF A PHASE 1 DOSE- ESCALATION AND EXPANSION STUDY Eytan M. Stein, Courtney D. DiNardo, Daniel A. Pollyea, Amir
Inotuzumab Ozogamicin in ALL. Hagop Kantarjian M.D. May 2016 Bologna, Italy
 Inotuzumab Ozogamicin in ALL Hagop Kantarjian M.D. May 2016 Bologna, Italy Immuno Oncology in ALL Monoclonals + cytotoxic agents e.g.inotuzumab Bispecific monoclonals (CD3 + CD19) e.g.blinatumomab Modified
Inotuzumab Ozogamicin in ALL Hagop Kantarjian M.D. May 2016 Bologna, Italy Immuno Oncology in ALL Monoclonals + cytotoxic agents e.g.inotuzumab Bispecific monoclonals (CD3 + CD19) e.g.blinatumomab Modified
How the Treatment of Acute Myeloid Leukemia is Changing in 2019
 How the Treatment of Acute Myeloid Leukemia is Changing in 2019 Guido Marcucci, M.D. Director, Gehr Family Center for Leukemia Research Chair, Dept. Hematologic Malignancies Translational Science City
How the Treatment of Acute Myeloid Leukemia is Changing in 2019 Guido Marcucci, M.D. Director, Gehr Family Center for Leukemia Research Chair, Dept. Hematologic Malignancies Translational Science City
New concepts in the management of elderly patients with AML
 New concepts in the management of elderly patients with AML Martha L. Arellano, MD Associate Professor of Hematology/Oncology Director, Hematology & Medical Oncology Fellowship Program Winship Cancer Institute
New concepts in the management of elderly patients with AML Martha L. Arellano, MD Associate Professor of Hematology/Oncology Director, Hematology & Medical Oncology Fellowship Program Winship Cancer Institute
Safety and Efficacy of Venetoclax Plus Low-Dose Cytarabine in Treatment-Naïve Patients Aged 65 Years With Acute Myeloid Leukemia
 Safety and Efficacy of Venetoclax Plus Low-Dose Cytarabine in Treatment-Naïve Patients Aged 65 Years With Acute Myeloid Leukemia Abstract 102 Wei AH, Strickland SA, Roboz GJ, Hou J-Z, Fiedler W, Lin TL,
Safety and Efficacy of Venetoclax Plus Low-Dose Cytarabine in Treatment-Naïve Patients Aged 65 Years With Acute Myeloid Leukemia Abstract 102 Wei AH, Strickland SA, Roboz GJ, Hou J-Z, Fiedler W, Lin TL,
Background CPX-351. Lancet J, et al. J Clin Oncol. 2017;35(suppl): Abstract 7035.
: Abstract 7035.") Overall Survival (OS) With Versus in Older Adults With Newly Diagnosed, Therapy-Related Acute Myeloid Leukemia (taml): Subgroup Analysis of a Phase 3 Study Abstract 7035 Lancet JE, Rizzieri D, Schiller
Overall Survival (OS) With Versus in Older Adults With Newly Diagnosed, Therapy-Related Acute Myeloid Leukemia (taml): Subgroup Analysis of a Phase 3 Study Abstract 7035 Lancet JE, Rizzieri D, Schiller
Hematologic Malignancies: Top Ten Advances Impacting Clinical Practice
 Hematologic Malignancies: Top Ten Advances Impacting Clinical Practice Adam D. Cohen, MD Abramson Cancer Center University of Pennsylvania June 14, 2018 Please note that some of the studies reported in
Hematologic Malignancies: Top Ten Advances Impacting Clinical Practice Adam D. Cohen, MD Abramson Cancer Center University of Pennsylvania June 14, 2018 Please note that some of the studies reported in
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014
![[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014](/thumbs/73/68853651.jpg "[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014") [ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
Leukemia. Andre C. Schuh. Princess Margaret Cancer Centre Toronto
 Leukemia Andre C. Schuh Princess Margaret Cancer Centre Toronto AGENDA Ø Overview Ø Key News This Year Ø Key News out of ASH 2016 Sessions Abstracts Ø Canadian Perspective Ø Overview 2015- Stone, R. et
Leukemia Andre C. Schuh Princess Margaret Cancer Centre Toronto AGENDA Ø Overview Ø Key News This Year Ø Key News out of ASH 2016 Sessions Abstracts Ø Canadian Perspective Ø Overview 2015- Stone, R. et
Molecularly Targeted Therapies - Strategies of the AMLSG
 Molecularly Targeted Therapies - Strategies of the AMLSG Richard Schlenk Department of Internal Medicine III Ulm University, Germany Genotype-adapted Leukemia Program NAPOLEON GIMEMA/AMLSG/SAL APL [t(15;17)]
Molecularly Targeted Therapies - Strategies of the AMLSG Richard Schlenk Department of Internal Medicine III Ulm University, Germany Genotype-adapted Leukemia Program NAPOLEON GIMEMA/AMLSG/SAL APL [t(15;17)]
ANCO: ASCO Highlights 2018 Hematologic Malignancies
 ANCO: ASCO Highlights 2018 Hematologic Malignancies Brian A. Jonas, M.D., Ph.D. UC Davis Comprehensive Cancer Center August 25, 2018 Brian Jonas, MD, PhD ANCO: ASCO Highlights 2018 Relevant financial relationships
ANCO: ASCO Highlights 2018 Hematologic Malignancies Brian A. Jonas, M.D., Ph.D. UC Davis Comprehensive Cancer Center August 25, 2018 Brian Jonas, MD, PhD ANCO: ASCO Highlights 2018 Relevant financial relationships
Updates in Treatment Strategies for Acute Leukemia. Alexander Perl, MD Assistant Professor, Hematology/Oncology University of Pennsylvania 1/22/2016
 Updates in Treatment Strategies for Acute Leukemia Alexander Perl, MD Assistant Professor, Hematology/Oncology University of Pennsylvania 1/22/2016 What is happening to standard of care in 2017? AML treatment
Updates in Treatment Strategies for Acute Leukemia Alexander Perl, MD Assistant Professor, Hematology/Oncology University of Pennsylvania 1/22/2016 What is happening to standard of care in 2017? AML treatment
ANCO Hematological Malignancies Update: The year in review. Midostaurin Vyxeos Gemtuzumab ozogamicin Enasidenib. The year in preview
 ANCO Hematological Malignancies Update: Gabriel Mannis, MD Assistant Professor, and Marrow Co-Director, Cancer Immunotherapy Clinic Acute Leukemia Sacramento, CA June 16, 2018 OVERVIEW Overview The year
ANCO Hematological Malignancies Update: Gabriel Mannis, MD Assistant Professor, and Marrow Co-Director, Cancer Immunotherapy Clinic Acute Leukemia Sacramento, CA June 16, 2018 OVERVIEW Overview The year
Neue zielgerichtete Behandlungsoptionen der neu diagnostizierten FLT3-positiven Akuten Myeloischen Leukämie (AML)
") Neue zielgerichtete Behandlungsoptionen der neu diagnostizierten FLT3-positiven Akuten Myeloischen Leukämie (AML) Prof. Hartmut Döhner Klinik für Innere Medizin III, Universitätsklinikum Ulm Midostaurin
Neue zielgerichtete Behandlungsoptionen der neu diagnostizierten FLT3-positiven Akuten Myeloischen Leukämie (AML) Prof. Hartmut Döhner Klinik für Innere Medizin III, Universitätsklinikum Ulm Midostaurin
Updates in the Management of Acute Myeloid Leukemia
 Updates in the Management of Acute Myeloid Leukemia Lydia Benitez, harmd, BCO 2017 TOA Conference I have no conflicts of interest with relation to the content of this presentation 4 Objectives Describe
Updates in the Management of Acute Myeloid Leukemia Lydia Benitez, harmd, BCO 2017 TOA Conference I have no conflicts of interest with relation to the content of this presentation 4 Objectives Describe
Best of ASH: Acute leukemia. Frédéric Baron
 Best of ASH: Acute leukemia Frédéric Baron I Acute Myeloid Leukemia Flt3 inhibitors (ratify, sorafenib after HCT) 5 other important abstracts (in brief) Mutated genes in AML FLT3: The Cancer Genome Atlas
Best of ASH: Acute leukemia Frédéric Baron I Acute Myeloid Leukemia Flt3 inhibitors (ratify, sorafenib after HCT) 5 other important abstracts (in brief) Mutated genes in AML FLT3: The Cancer Genome Atlas
2/10/2017. Updates in Acute Leukemia Therapy Blood Cancer Incidence in the United States, Leukemia Incidence in the Unites States, 2016
 Updates in Acute Leukemia Therapy 2017 Aaron Logan, MD, PhD UCSF Division of Malignant Hematology and Blood and Marrow Transplantation aaron.logan@ucsf.edu @hemedoc Blood Cancer Incidence in the United
Updates in Acute Leukemia Therapy 2017 Aaron Logan, MD, PhD UCSF Division of Malignant Hematology and Blood and Marrow Transplantation aaron.logan@ucsf.edu @hemedoc Blood Cancer Incidence in the United
Acute Myeloid Leukemia: Targets and Curability, so Close But a Journey So Far
 Acute Myeloid Leukemia: Targets and Curability, so Close But a Journey So Far Martin S. Tallman, M.D. Chief, Leukemia Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Cornell
Acute Myeloid Leukemia: Targets and Curability, so Close But a Journey So Far Martin S. Tallman, M.D. Chief, Leukemia Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Cornell
ANCO 2015: Treatment advances in acute leukemia
 ANCO 2015: Treatment advances in acute leukemia Michaela Liedtke, MD Stanford, CA September 12, 2015!" Disclosures Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Steering Committee
ANCO 2015: Treatment advances in acute leukemia Michaela Liedtke, MD Stanford, CA September 12, 2015!" Disclosures Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Steering Committee
M Y ELO I D D I FFER ENTIATI O N OPENS UP THE POSSIBILITIES
 IDHIFA (enasidenib) is indicated for the treatment of adult patients with relapsed or refractory (R/R) acute myeloid leukemia (AML) with an isocitrate dehydrogenase-2 (IDH2) mutation as detected by an
IDHIFA (enasidenib) is indicated for the treatment of adult patients with relapsed or refractory (R/R) acute myeloid leukemia (AML) with an isocitrate dehydrogenase-2 (IDH2) mutation as detected by an
Evolving Targeted Management of Acute Myeloid Leukemia
 Evolving Targeted Management of Acute Myeloid Leukemia Jessica Altman, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Learning Objectives Identify which mutations should be assessed
Evolving Targeted Management of Acute Myeloid Leukemia Jessica Altman, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Learning Objectives Identify which mutations should be assessed
Presented at the 58 th American Society of Hematology Annual Meeting and Exposition, December 5, 2016, San Diego, CA
 1070 Determination of IDH1 mutational burden and clearance via next-generation sequencing in patients with IDH1 mutation-positive hematologic malignancies receiving AG-120, a first-in-class inhibitor of
1070 Determination of IDH1 mutational burden and clearance via next-generation sequencing in patients with IDH1 mutation-positive hematologic malignancies receiving AG-120, a first-in-class inhibitor of
Immunotherapies in Acute Lymphoblastic Leukaemia. Professor David Ritchie Royal Melbourne Hospital
 Immunotherapies in Acute Lymphoblastic Leukaemia Professor David Ritchie Royal Melbourne Hospital Blinatumomab Cases Case 1: Mr BE 30 year old male Aged 17, diagnosed Philadelphia negative B-ALL in Nov
Immunotherapies in Acute Lymphoblastic Leukaemia Professor David Ritchie Royal Melbourne Hospital Blinatumomab Cases Case 1: Mr BE 30 year old male Aged 17, diagnosed Philadelphia negative B-ALL in Nov
Abstract 861. Stein AS, Topp MS, Kantarjian H, Gökbuget N, Bargou R, Litzow M, Rambaldi A, Ribera J-M, Zhang A, Zimmerman Z, Forman SJ
 Treatment with Anti-CD19 BiTE Blinatumomab in Adult Patients With Relapsed/Refractory B-Precursor Acute Lymphoblastic Leukemia (R/R ALL) Post-Allogeneic Hematopoietic Stem Cell Transplantation Abstract
Treatment with Anti-CD19 BiTE Blinatumomab in Adult Patients With Relapsed/Refractory B-Precursor Acute Lymphoblastic Leukemia (R/R ALL) Post-Allogeneic Hematopoietic Stem Cell Transplantation Abstract
Personalized Therapy for Acute Myeloid Leukemia. Patrick Stiff MD Loyola University Medical Center
 Personalized Therapy for Acute Myeloid Leukemia Patrick Stiff MD Loyola University Medical Center 708-327-3216 Major groups of Mutations in AML Targets for AML: Is this Achievable? Chronic Myeloid Leukemia:
Personalized Therapy for Acute Myeloid Leukemia Patrick Stiff MD Loyola University Medical Center 708-327-3216 Major groups of Mutations in AML Targets for AML: Is this Achievable? Chronic Myeloid Leukemia:
All patients with FLT3 mutant AML should receive midostaurin-based induction therapy. Not so fast!
 All patients with FLT3 mutant AML should receive midostaurin-based induction therapy Not so fast! Harry P. Erba, M.D., Ph.D. Professor, Internal Medicine Director, Hematologic Malignancy Program University
All patients with FLT3 mutant AML should receive midostaurin-based induction therapy Not so fast! Harry P. Erba, M.D., Ph.D. Professor, Internal Medicine Director, Hematologic Malignancy Program University
Emerging Therapeutics in Hematologic Malignancies
 Emerging Therapeutics in Hematologic Malignancies Brian A. Jonas, MD, PhD Assistant Professor of Medicine UC Davis Comprehensive Cancer Center September 26, 2015 16th Annual Advances in Oncology 2015 September
Emerging Therapeutics in Hematologic Malignancies Brian A. Jonas, MD, PhD Assistant Professor of Medicine UC Davis Comprehensive Cancer Center September 26, 2015 16th Annual Advances in Oncology 2015 September
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia
 Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Highlights in Acute Myeloid Leukemia From the 2017 American Society of Hematology Annual Meeting and Exposition
 March 2018 Volume 16, Issue 3, Supplement 8 A SPECIAL MEETING REVIEW EDITION Highlights in Acute Myeloid Leukemia From the 2017 American Society of Hematology Annual Meeting and Exposition A Review of
March 2018 Volume 16, Issue 3, Supplement 8 A SPECIAL MEETING REVIEW EDITION Highlights in Acute Myeloid Leukemia From the 2017 American Society of Hematology Annual Meeting and Exposition A Review of
AML in elderly. D.Selleslag AZ Sint-Jan Brugge, Belgium 14 December 2013
 AML in elderly D.Selleslag AZ Sint-Jan Brugge, Belgium 14 December 2013 AML is predominantly a disease of the elderly incidence 2 3/100.000 SEER Cancer Statistics, National Cancer Institute, USA 2002 2006
AML in elderly D.Selleslag AZ Sint-Jan Brugge, Belgium 14 December 2013 AML is predominantly a disease of the elderly incidence 2 3/100.000 SEER Cancer Statistics, National Cancer Institute, USA 2002 2006
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
Disclosure Slide. Research Support: Onconova Therapeutics, Celgene
 Oral Rigosertib Combined with Azacitidine in Patients with Acute Myeloid Leukemia (AML) and Myelodysplastic Syndromes (MDS): Effects in Treatment Naïve and Relapsed- Refractory Patients Shyamala C. Navada,
Oral Rigosertib Combined with Azacitidine in Patients with Acute Myeloid Leukemia (AML) and Myelodysplastic Syndromes (MDS): Effects in Treatment Naïve and Relapsed- Refractory Patients Shyamala C. Navada,
Remission induction in acute myeloid leukemia
 Int J Hematol (2012) 96:164 170 DOI 10.1007/s12185-012-1121-y PROGRESS IN HEMATOLOGY How to improve the outcome of adult acute myeloid leukemia? Remission induction in acute myeloid leukemia Eytan M. Stein
Int J Hematol (2012) 96:164 170 DOI 10.1007/s12185-012-1121-y PROGRESS IN HEMATOLOGY How to improve the outcome of adult acute myeloid leukemia? Remission induction in acute myeloid leukemia Eytan M. Stein
Disclosure. Study was sponsored by Karyopharm Therapeutics No financial relationships to disclose Other disclosures:
 Combination of Selinexor with High-Dose Cytarabine and Mitoxantrone for Remission Induction in Acute Myeloid Leukemia is Feasible and Tolerable A Phase I Study (NCT02573363) Amy Y. Wang, Howie Weiner,
Combination of Selinexor with High-Dose Cytarabine and Mitoxantrone for Remission Induction in Acute Myeloid Leukemia is Feasible and Tolerable A Phase I Study (NCT02573363) Amy Y. Wang, Howie Weiner,
BESPONSA (inotuzumab ozogamicin)
") BESPONSA (inotuzumab ozogamicin) Fact Sheet BESPONSA (inotuzumab ozogamicin) is an antibody-drug conjugate (ADC) composed of a monoclonal antibody (mab) targeting CD22, a cell surface antigen expressed
BESPONSA (inotuzumab ozogamicin) Fact Sheet BESPONSA (inotuzumab ozogamicin) is an antibody-drug conjugate (ADC) composed of a monoclonal antibody (mab) targeting CD22, a cell surface antigen expressed
Acute Leukemia From Precision Medicine to ImmunoRx
 Acute Leukemia From Precision Medicine to ImmunoRx Hagop M. Kantarjian, MD Professor and Chair, Department of Leukemia Samsung Distinguished Leukemia Chair in Cancer Medicine The University of Texas MD
Acute Leukemia From Precision Medicine to ImmunoRx Hagop M. Kantarjian, MD Professor and Chair, Department of Leukemia Samsung Distinguished Leukemia Chair in Cancer Medicine The University of Texas MD
Manufacturer: Wyeth Pharmaceuticals Inc., a subsidiary of Pfizer Inc.
 Brand Name: Mylotarg Generic Name: gentuzumab ozogamicin Manufacturer: Wyeth Pharmaceuticals Inc., a subsidiary of Pfizer Inc. Drug Class: CD33-directed antibody-drug conjugate Uses: Labeled Uses: Newly-diagnosed
Brand Name: Mylotarg Generic Name: gentuzumab ozogamicin Manufacturer: Wyeth Pharmaceuticals Inc., a subsidiary of Pfizer Inc. Drug Class: CD33-directed antibody-drug conjugate Uses: Labeled Uses: Newly-diagnosed
New drugs in first-line therapy
 New drugs in first-line therapy Gianantonio Rosti Dept of Hematology and Oncology Seràgnoli, Bologna University (Italy) GIMEMA (Gruppo Italiano Malattie Ematologiche dell Adulto) CML WORKING PARTY IRIS
New drugs in first-line therapy Gianantonio Rosti Dept of Hematology and Oncology Seràgnoli, Bologna University (Italy) GIMEMA (Gruppo Italiano Malattie Ematologiche dell Adulto) CML WORKING PARTY IRIS
CLINICAL STUDY REPORT SYNOPSIS
 CLINICAL STUDY REPORT SYNOPSIS Document No.: EDMS-PSDB-5412862:2.0 Research & Development, L.L.C. Protocol No.: R115777-AML-301 Title of Study: A Randomized Study of Tipifarnib Versus Best Supportive Care
CLINICAL STUDY REPORT SYNOPSIS Document No.: EDMS-PSDB-5412862:2.0 Research & Development, L.L.C. Protocol No.: R115777-AML-301 Title of Study: A Randomized Study of Tipifarnib Versus Best Supportive Care
CREDIT DESIGNATION STATEMENT
 CME Information LEARNING OBJECTIVES Recall the dose-limiting toxicity and preliminary clinical response results with 14- and 21-day extended treatment schedules of daily oral azacitidine. Apply new research
CME Information LEARNING OBJECTIVES Recall the dose-limiting toxicity and preliminary clinical response results with 14- and 21-day extended treatment schedules of daily oral azacitidine. Apply new research
How to Integrate the New Drugs into the Management of Multiple Myeloma
 How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
Oncology Highlights: Leukemia & Myelodysplastic Syndromes
 Oncology Highlights: Leukemia & Myelodysplastic Syndromes Jorge Cortes, MD Department of Leukemia The University of Texas, M.D. Anderson Cancer Center Highlights of the Day Leukemia & MDS AML: The field
Oncology Highlights: Leukemia & Myelodysplastic Syndromes Jorge Cortes, MD Department of Leukemia The University of Texas, M.D. Anderson Cancer Center Highlights of the Day Leukemia & MDS AML: The field
New Drug Updates in Hematologic Malignancies: CAR T Cells, Targeted Therapeutics, and Other Agents
 New Drug Updates in Hematologic Malignancies: CAR T Cells, Targeted Therapeutics, and Other Agents R. Donald Harvey, PharmD, BCOP, FCCP, FHOPA Associate Professor, Hematology/Medical Oncology and Pharmacology
New Drug Updates in Hematologic Malignancies: CAR T Cells, Targeted Therapeutics, and Other Agents R. Donald Harvey, PharmD, BCOP, FCCP, FHOPA Associate Professor, Hematology/Medical Oncology and Pharmacology
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: TAG IDAG Objectives:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Risk-adapted therapy of AML in younger adults. Sergio Amadori Tor Vergata University Hospital Rome
 Risk-adapted therapy of AML in younger adults Sergio Amadori Tor Vergata University Hospital Rome Pescara 11/2010 AML: treatment outcome Age CR % ED % DFS % OS %
Risk-adapted therapy of AML in younger adults Sergio Amadori Tor Vergata University Hospital Rome Pescara 11/2010 AML: treatment outcome Age CR % ED % DFS % OS %
CARs vs. BiTE in ALL. David L Porter, MD Jodi Fisher Horowitz Professor University of Pennsylvania Health System Abramson Cancer Center
 CARs vs. BiTE in ALL David L Porter, MD Jodi Fisher Horowitz Professor University of Pennsylvania Health System Abramson Cancer Center Disclosure Information David L Porter Speaker and members of study
CARs vs. BiTE in ALL David L Porter, MD Jodi Fisher Horowitz Professor University of Pennsylvania Health System Abramson Cancer Center Disclosure Information David L Porter Speaker and members of study
Department of Leukemia, The University of Texas M.D. Anderson Cancer Center, Houston, Texas; 2 Sunesis Pharmaceuticals, Inc, South San Francisco
 Phase I/II Study of Vosaroxin and Decitabine in Newly Diagnosed Older Patients with Acute Myeloid Leukemia (AML) and High Risk Myelodysplastic Syndrome (MDS) Naval Daver 1, Hagop Kantarjian 1, Guillermo
Phase I/II Study of Vosaroxin and Decitabine in Newly Diagnosed Older Patients with Acute Myeloid Leukemia (AML) and High Risk Myelodysplastic Syndrome (MDS) Naval Daver 1, Hagop Kantarjian 1, Guillermo
Current Strategies for Relapsed/Refractory ALL in AYAs and Adults: Where We Are Now
 Current Strategies for Relapsed/Refractory ALL in AYAs and Adults: Where We Are Now Eunice S. Wang, MD Roswell Park Cancer Institute Buffalo, New York, United States Relapsed ALL Carries a Poor Prognosis
Current Strategies for Relapsed/Refractory ALL in AYAs and Adults: Where We Are Now Eunice S. Wang, MD Roswell Park Cancer Institute Buffalo, New York, United States Relapsed ALL Carries a Poor Prognosis
The Evolving Treatment Landscape in AML
 The Evolving Treatment Landscape in AML Elias Jabbour, MD Associate Professor Section Chief, Acute Lymphocytic Leukemia Department of Leukemia Division of Cancer Medicine The University of Texas MD Anderson
The Evolving Treatment Landscape in AML Elias Jabbour, MD Associate Professor Section Chief, Acute Lymphocytic Leukemia Department of Leukemia Division of Cancer Medicine The University of Texas MD Anderson
Leukemia. Roland B. Walter, MD PhD MS. Fred Hutchinson Cancer Research Center University of Washington
 Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
Cautionary Note Regarding Forward-Looking Statements
 lndoximod Combined with Standard Induction Chemotherapy Is Well Tolerated and Induces a High Rate of Complete Remission with MRD-Negativity in Patients with Newly Diagnosed AML: Results from a Phase 1
lndoximod Combined with Standard Induction Chemotherapy Is Well Tolerated and Induces a High Rate of Complete Remission with MRD-Negativity in Patients with Newly Diagnosed AML: Results from a Phase 1
Emerging Treatment Options for Myelodysplastic Syndromes
 Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Treatments and Current Research in Leukemia. Richard A. Larson, MD University of Chicago
 Treatments and Current Research in Leukemia Richard A. Larson, MD University of Chicago 2 Acute (rapid progression) Myeloid Acute myeloid leukemia (AML) Acute promyelocytic leukemia (APL) Lymphoid Acute
Treatments and Current Research in Leukemia Richard A. Larson, MD University of Chicago 2 Acute (rapid progression) Myeloid Acute myeloid leukemia (AML) Acute promyelocytic leukemia (APL) Lymphoid Acute
BR is an established treatment regimen for CLL in the front-line and R/R settings
 Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Targeting CD20 and CD22 in B-cell ALL Daniel J. DeAngelo, MD, PhD
 Targeting CD20 and CD22 in B-cell ALL Daniel J. DeAngelo, MD, PhD Harvard/Dana-Farber Cancer Institute Boston, MA Disclosures for Daniel J. DeAngelo, MD, PhD Royalty Receipt of intellectual property/ Patent
Targeting CD20 and CD22 in B-cell ALL Daniel J. DeAngelo, MD, PhD Harvard/Dana-Farber Cancer Institute Boston, MA Disclosures for Daniel J. DeAngelo, MD, PhD Royalty Receipt of intellectual property/ Patent
NEW THERAPIES IN ACUTE MYELOID LEUKEMIA (AML) Maho Hibino, PharmD, BCOP Oncology Clinical Specialist Wake Forest Baptist Health August 3, 2018
 Maho Hibino, PharmD, BCOP Oncology Clinical Specialist Wake Forest Baptist Health August 3, 2018") NEW THERAPIES IN ACUTE MYELOID LEUKEMIA (AML) Maho Hibino, PharmD, BCOP Oncology Clinical Specialist Wake Forest Baptist Health August 3, 2018 OBJECTIVES Recognize new medications that received FDA approval
NEW THERAPIES IN ACUTE MYELOID LEUKEMIA (AML) Maho Hibino, PharmD, BCOP Oncology Clinical Specialist Wake Forest Baptist Health August 3, 2018 OBJECTIVES Recognize new medications that received FDA approval
AML Handout August 3, 2018
 NEW THERAPIES IN ACUTE MYELOID LEUKEMIA (AML) Maho Hibino, PharmD, BCOP Oncology Clinical Specialist Wake Forest Baptist Health August 3, OBJECTIVES Recognize new medications that received FDA approval
NEW THERAPIES IN ACUTE MYELOID LEUKEMIA (AML) Maho Hibino, PharmD, BCOP Oncology Clinical Specialist Wake Forest Baptist Health August 3, OBJECTIVES Recognize new medications that received FDA approval
Subset Specific Therapy in High Risk Myeloid Malignancies. Are We Making Progress? Olatoyosi Odenike, MD. The University of Chicago
 Subset Specific Therapy in High Risk Myeloid Malignancies. Are We Making Progress? Olatoyosi Odenike, MD The University of Chicago Disclosure Information 23 rd Annual Developmental Therapeutics Symposium
Subset Specific Therapy in High Risk Myeloid Malignancies. Are We Making Progress? Olatoyosi Odenike, MD The University of Chicago Disclosure Information 23 rd Annual Developmental Therapeutics Symposium
La lenalidomide: meccanismo d azione e risultati terapeutici. F. Ferrara
 La lenalidomide: meccanismo d azione e risultati terapeutici F. Ferrara MDS: new treatment goals Emerging treatment options expected to facilitate shift from supportive care to active therapy in MDS New
La lenalidomide: meccanismo d azione e risultati terapeutici F. Ferrara MDS: new treatment goals Emerging treatment options expected to facilitate shift from supportive care to active therapy in MDS New
Meet-the-Expert: AML Treating older patients with AML
 Meet-the-Expert: AML Treating older patients with AML Sergio Amadori Tor Vergata University Hospital Rome Istanbul 2012 AML in older patients Poor prognosis Minority treated with intensive Cx Treatment
Meet-the-Expert: AML Treating older patients with AML Sergio Amadori Tor Vergata University Hospital Rome Istanbul 2012 AML in older patients Poor prognosis Minority treated with intensive Cx Treatment
Department of Leukemia, The University of Texas M.D. Anderson Cancer Center, Houston, Texas; 2 Sunesis Pharmaceuticals, Inc, South San Francisco
 Phase I/II Study of Vosaroxin and Decitabine in Newly Diagnosed Older Patients with Acute Myeloid Leukemia (AML) and High Risk Myelodysplastic Syndrome (MDS) Naval Daver 1, Hagop Kantarjian 1, Guillermo
Phase I/II Study of Vosaroxin and Decitabine in Newly Diagnosed Older Patients with Acute Myeloid Leukemia (AML) and High Risk Myelodysplastic Syndrome (MDS) Naval Daver 1, Hagop Kantarjian 1, Guillermo
Highlights in acute leukemia
 CONGRESS HIGHLIGHTS 28 Highlights in acute leukemia T. Feys, MSc, MBA SPECIAL EDITION There has been a long period of time without any new acute myeloid leukemia (AML) treatments. However, the tide has
CONGRESS HIGHLIGHTS 28 Highlights in acute leukemia T. Feys, MSc, MBA SPECIAL EDITION There has been a long period of time without any new acute myeloid leukemia (AML) treatments. However, the tide has
NEW FDA DRUG APPROVALS
 NEW FDA DRUG APPROVALS Jennifer Peterson MSN, RN, OCN, BMTCN Jennifer Shamai MS, RN, AOCNS, BMTCN How the Experts Treat Hematologic Malignancies Las Vegas, NV March 15, 2018 Disclosures We have nothing
NEW FDA DRUG APPROVALS Jennifer Peterson MSN, RN, OCN, BMTCN Jennifer Shamai MS, RN, AOCNS, BMTCN How the Experts Treat Hematologic Malignancies Las Vegas, NV March 15, 2018 Disclosures We have nothing
A Phase II Study of the Combination of Oral Rigosertib and Azacitidine in Patients with Myelodysplastic Syndromes (MDS)
") A Phase II Study of the Combination of Oral Rigosertib and Azacitidine in Patients with Myelodysplastic Syndromes (MDS) Shyamala C. Navada, MD 1, Lewis R. Silverman, MD 1, Katherine Hearn, RN 2, Rosalie
A Phase II Study of the Combination of Oral Rigosertib and Azacitidine in Patients with Myelodysplastic Syndromes (MDS) Shyamala C. Navada, MD 1, Lewis R. Silverman, MD 1, Katherine Hearn, RN 2, Rosalie
2 Workshop Nazionale SIES Ematologia Traslazionale Nuovi Farmaci e Strategie Terapeutiche nelle LMA
 2 Workshop Nazionale SIES Ematologia Traslazionale Nuovi Farmaci e Strategie Terapeutiche nelle LMA Adriano Venditti Ematologia Universita Tor Vergata, Roma Current Treatment Results in AML AGE, y CR%
2 Workshop Nazionale SIES Ematologia Traslazionale Nuovi Farmaci e Strategie Terapeutiche nelle LMA Adriano Venditti Ematologia Universita Tor Vergata, Roma Current Treatment Results in AML AGE, y CR%
Learning Objectives. Case A: Presentation. Case A Question Not included in Activity Survey. Acute Leukemia: Diagnosis and Prognosis
 Learning Objectives Improve awareness of FDA-approved agents and/or therapies under development for the treatment of AML and ALL Incorporate FDA-approved agents and therapies under development into treatment
Learning Objectives Improve awareness of FDA-approved agents and/or therapies under development for the treatment of AML and ALL Incorporate FDA-approved agents and therapies under development into treatment
VYXEOS : CHEMOTHERAPY LIPOSOME INJECTION FOR ACUTE MYELOID LEUKEMIA
 VYXEOS : CHEMOTHERAPY LIPOSOME INJECTION FOR ACUTE MYELOID LEUKEMIA Sarah Mae Rogado PharmD Candidate 2017 Preceptors: Rozena Varghese, PharmD, CMPP; Rachel Brown, PharmD MedVal Scientific Information
VYXEOS : CHEMOTHERAPY LIPOSOME INJECTION FOR ACUTE MYELOID LEUKEMIA Sarah Mae Rogado PharmD Candidate 2017 Preceptors: Rozena Varghese, PharmD, CMPP; Rachel Brown, PharmD MedVal Scientific Information
2 nd Generation TKI Frontline Therapy in CML
 2 nd Generation TKI Frontline Therapy in CML Elias Jabbour, M.D. April 212 New York Frontline Therapy of CML in 212 - imatinib 4 mg daily - nilotinib 3 mg BID - dasatinib 1 mg daily Second / third line
2 nd Generation TKI Frontline Therapy in CML Elias Jabbour, M.D. April 212 New York Frontline Therapy of CML in 212 - imatinib 4 mg daily - nilotinib 3 mg BID - dasatinib 1 mg daily Second / third line
Acute Myeloid Leukemia
 Acute Myeloid Leukemia Guido Marcucci, M.D. Director, Gehr Family Center for Leukemia Research Hematologic Malignancies and Stem Cell Transplantation Institute City of Hope Acute Myeloid Leukemia Gene
Acute Myeloid Leukemia Guido Marcucci, M.D. Director, Gehr Family Center for Leukemia Research Hematologic Malignancies and Stem Cell Transplantation Institute City of Hope Acute Myeloid Leukemia Gene
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant
 Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
CAR T-Cell Therapy for Acute Lymphoblastic Leukemia: Identifying Appropriate Patients and Maximizing Outcomes. Shannon L.
 CAR T-Cell Therapy for Acute Lymphoblastic Leukemia: Identifying Appropriate Patients and Maximizing Outcomes Shannon L. Maude, MD, PhD CTL019 cell Lentiviral vector Anti-CD19 CAR construct CD19 Native
CAR T-Cell Therapy for Acute Lymphoblastic Leukemia: Identifying Appropriate Patients and Maximizing Outcomes Shannon L. Maude, MD, PhD CTL019 cell Lentiviral vector Anti-CD19 CAR construct CD19 Native
UMN request : information to be made public Page 1
 Product Name Active substance Indication and conditions of use Midostaurin (PKC412) Midostaurin (PKC412) soft gelatin capsules of 25 mg Compassionate Use Program with Midostaurin for newly diagnosed FLT3
Product Name Active substance Indication and conditions of use Midostaurin (PKC412) Midostaurin (PKC412) soft gelatin capsules of 25 mg Compassionate Use Program with Midostaurin for newly diagnosed FLT3
Phase 1 Study of ARRY-520 and Carfilzomib in Patients With Relapsed/Refractory Multiple Myeloma (RRMM)
") Phase 1 Study of ARRY-520 and Carfilzomib in Patients With Relapsed/Refractory Multiple Myeloma (RRMM) Jatin J Shah, MD, Sheeba Thomas, MD, Donna Weber, MD, Michael Wang, MD, Raymond Alexanian, MD, Robert
Phase 1 Study of ARRY-520 and Carfilzomib in Patients With Relapsed/Refractory Multiple Myeloma (RRMM) Jatin J Shah, MD, Sheeba Thomas, MD, Donna Weber, MD, Michael Wang, MD, Raymond Alexanian, MD, Robert
New drugs in Acute Leukemia. Cristina Papayannidis, MD, PhD University of Bologna
 New drugs in Acute Leukemia Cristina Papayannidis, MD, PhD University of Bologna Challenges to targeted therapy in AML Multiple subtypes based upon mutations/cytogenetic aberrations No known uniform genomic
New drugs in Acute Leukemia Cristina Papayannidis, MD, PhD University of Bologna Challenges to targeted therapy in AML Multiple subtypes based upon mutations/cytogenetic aberrations No known uniform genomic
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia
 Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
ESTABLISHED AND EMERGING THERAPIES FOR ACUTE MYELOID LEUKAEMIA. Dr Rob Sellar UCL Cancer Institute, London, UK
 ESTABLISHED AND EMERGING THERAPIES FOR ACUTE MYELOID LEUKAEMIA Dr Rob Sellar UCL Cancer Institute, London, UK OVERVIEW Main focus on patients fit for intensive treatment Biological and Clinical Heterogeneity
ESTABLISHED AND EMERGING THERAPIES FOR ACUTE MYELOID LEUKAEMIA Dr Rob Sellar UCL Cancer Institute, London, UK OVERVIEW Main focus on patients fit for intensive treatment Biological and Clinical Heterogeneity
(212) (347)
 (347)") EMBARGOED FOR MONDAY, JUNE 21, 2010: 3:00 P.M. EST For immediate release: June 21, 2010 Media Contact: Curtis Allen (212) 733-2096 (347) 443-5252 Investors Contact: Suzanne Harnett (212) 733-8009 Pfizer
EMBARGOED FOR MONDAY, JUNE 21, 2010: 3:00 P.M. EST For immediate release: June 21, 2010 Media Contact: Curtis Allen (212) 733-2096 (347) 443-5252 Investors Contact: Suzanne Harnett (212) 733-8009 Pfizer
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities
: Cytokine release syndrome and neurological toxicities") Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
CARE at ASH 2014 Leukemia. Julie Bergeron, MD Maisonneuve-Rosemont Hospital
 CARE at ASH 2014 Leukemia Julie Bergeron, MD Maisonneuve-Rosemont Hospital Acute Leukemias Dr. Julie Bergeron Hôpital Maisonneuve-Rosemont, Montréal Disclosures Advisory boards in 2014: AMGEN EUSA pharma
CARE at ASH 2014 Leukemia Julie Bergeron, MD Maisonneuve-Rosemont Hospital Acute Leukemias Dr. Julie Bergeron Hôpital Maisonneuve-Rosemont, Montréal Disclosures Advisory boards in 2014: AMGEN EUSA pharma
SUPPLEMENTAL APPENDIX
 SUPPLEMENTAL APPENDIX Table of Contents 1. Supplemental Tables 2. Supplemental Figures Nature Medicine: doi:1.138/nm.4441 Supplemental Table 1. Baseline Characteristics of Patients Treated with anti-cd22
SUPPLEMENTAL APPENDIX Table of Contents 1. Supplemental Tables 2. Supplemental Figures Nature Medicine: doi:1.138/nm.4441 Supplemental Table 1. Baseline Characteristics of Patients Treated with anti-cd22
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
5/21/2018. Disclosures. Objectives. Normal blood cells production. Bone marrow failure syndromes. Story of DNA
 AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
Actinium Pharmaceuticals, Inc.
 , Inc. Actimab-A MRD Consolidation Strategy in MRD+ AML July 10, 2018 1 Disclaimer and Safe Harbor Some of the information presented herein may contain projections or other forward-looking statements regarding
, Inc. Actimab-A MRD Consolidation Strategy in MRD+ AML July 10, 2018 1 Disclaimer and Safe Harbor Some of the information presented herein may contain projections or other forward-looking statements regarding
FACULTY TRAINING TRANSCRIPT
 FACULTY TRAINING TRANSCRIPT PROGRAM CURRICULUM REVIEWED BY: B. DOUGLAS SMITH, MD Professor of Oncology Johns Hopkins University, School of Medicine Baltimore, MD JONATHAN WEBSTER, MD Instructor of Oncology
FACULTY TRAINING TRANSCRIPT PROGRAM CURRICULUM REVIEWED BY: B. DOUGLAS SMITH, MD Professor of Oncology Johns Hopkins University, School of Medicine Baltimore, MD JONATHAN WEBSTER, MD Instructor of Oncology
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
New drugs and trials. Andreas Hochhaus
 New drugs and trials. Andreas Hochhaus Hadera I Oct 2018 Introduction ABL001 is a potent, specific inhibitor of BCR-ABL1 with a distinct allosteric mechanism of action BCR-ABL1 Protein Binds a distinct
New drugs and trials. Andreas Hochhaus Hadera I Oct 2018 Introduction ABL001 is a potent, specific inhibitor of BCR-ABL1 with a distinct allosteric mechanism of action BCR-ABL1 Protein Binds a distinct
Frontline Induc.on Therapy in 2017 Alan K Burne+
 Frontline Induc.on Therapy in 2017 Alan K Burne+ Ravenna, October 2017 Standard of Care Induc5on: 7+3 Ara-C / Daunorubicin Consolida5on: High Dose Ara-C (3g doses) Total of 4 courses. Myeloabla5ve allogral
Frontline Induc.on Therapy in 2017 Alan K Burne+ Ravenna, October 2017 Standard of Care Induc5on: 7+3 Ara-C / Daunorubicin Consolida5on: High Dose Ara-C (3g doses) Total of 4 courses. Myeloabla5ve allogral