Cancer Programme Update The 100,000 Genomes Project and Forwards
|
|
|
- Eustace Morris
- 6 years ago
- Views:
Transcription


1 Cancer Programme Update The 100,000 Genomes Project and Forwards Clare Turnbull Clinical Lead for Cancer Genomics, Genomics England Reader in Genomic Medicine, Institute of Cancer Research and Queen Mary University of London Honorary Consultant in Cancer Genetics, Guys and St Thomas NHS Trust ACGS Annual Meeting, Birmingham, June 26th 2017
2 To cover. Recruitment Sample Handling and Consensus statement Experimental work Haemato-oncology samples Return of results Germline Findings Genomics England Cancer Transition Group 10 July
3 Cancer Programme Phased roll-out Pilot Phase: 6 CRUK sites, 5 BRC sites Experimental Phase Gear 1 Gear 2 Gear 3 General recruitment Surgical resections (establish protocols) IIP Biopsies Focused cohorts (multiple samples in space and time) Individualised patient management (clinical turnaround time) 75x for tumour; 35x for germline ctdna pre-surgery Main Programme WAVE 1 WAVE 2 WAVE 3 Breast Renal Brain Prostate Sarcoma Upper GI Colorectal Germ Cell Tumours Ovarian Endometrial Lung Melanoma CLL Bladder Haem Onc 10 July
4 Recruitment
5 GMC self-reported recruitment to 2 nd June (including Pilot and IIP) 5,176 cancer samples (inc. tumour sample and germline) 4 weekly average = 110 samples 5
6 Number of participants registered per tumour type to 8 th June As of 4th May 2017 As of 8th June
7 Sample Handling
")


.")
8 New FFPE guideline conditions (early 2016) GeL402 Fresh-Frozen GeL402 FFPE, new guidelines (NBF 80ºC) SUMMARY There are significant improvements with the new guidelines when compared to previous methods employing formal saline. However, data quality is still significantly worse than fresh-frozen (lower coverage uniformity and rate of somatic variant overcalling). ~ ~640,000 GeL402 FFPE, previous conditions (FS 80ºC) Confidential - Not for further distribution
9 Mutational burden in paired FFPE vs FF samples FFPE samples show increased mutational burden of small variants, both SNVs and indels This is an artefact of FFPE samples


10 Monitoring quality
11 Bench marking quality between centres

12 Bench marking quality between centres
13 Consensus Statement Detailed consent is still required to agree to the research aspects of the 100,000 Genomes Project and to state opinions on how a patient's germline findings should be handled. Implications of the Consensus Statement: 1.Laboratories which do not have a research HTA licence can still store tissue for the diagnostic arm of the 100,000 Genomes Project. 2.Samples can be handled in a genomic friendly way by not putting them into formalin as part of the diagnostic pathway without specific consent required to do this. 3.Consent for participation in the 100,000 Genomes Project can be taken after tissue has been sampled. 13
14 Number of Biopsies Proportion of biopsy/surgical resections St George s Hospital, South London GMC Number of FF samples collected (Biopsy vs Resection) September October November December January February March April May Joint Statement Implementation Resection Biopsy Number of biopsies as a proportion of total samples has been increasing After introduction of the Joint Statement biopsies accounted for 49% of samples in May 2017 The graph to the right provides a breakdown of biopsies by tumour type Biopsy numbers by tumour type Number of biopsies Breast Colorectal Bladder 14
15 Experimental Work
16 SOP development group Molecular Pathology Working Group: experiments, protocols, implementation GMC implementation group EXPERIMENTAL GROUP Q Initiation Implementation phase Q Main program up o gr t n e pm ol e v de P O S WS 1: upstream tumour handling WS 3: tumour assessment WS 5: DNA quantification and quality assessment WS 2: tumour processing, fixative, embedding WS 4: DNA extraction WS 6: Library preparation and sequencing *Led by Prof Louise Jones. Includes molecular pathology representation from BRC-GMC centres. Consultation with Joint Molecular Pathology Group

17 Alternative Freezing Strategies # Treatment (T:0 4h) Details 1 Liquid Nitrogen onto dry ice 2 Isopentane onto dry ice 3 Cryospray (indirect) onto dry ice 4 Cryospray (direct) onto dry ice Aim: To provide flexibility in freezing samples, particularly biopsies in clinic setting 5 Dry ice 6 Wet ice 7 Phosphate Buffered Saline 8 RPMI Culture Medium Storage at 4 C/RT Storage at 4 C/RT 1,1,1,2 tetrafluoroethane supplied in pressurised canister Widely used in pathology for rapid freezing for frozen section analysis Gives excellent morphology (for FF) 10 July
18 DNA Quality (Tapestation) cryospray cryospray Sample N2 N2 F1 A1 E1 B1 C1 D1 A2 E2 C2 B2 D2 S2 B3 A3 F3 DIN X X Confidential - Not for further distribution



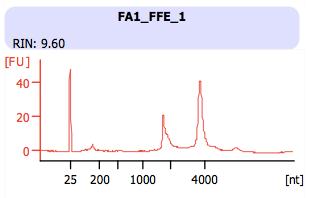
19 RNA Quality



20 Alternative freezing: sequencing results No evidence of a negative impact of alternative freezing strategies % aligned reads Library insert size Coverage uniformity Numbers of somatic SV calls Somatic SNV number and distribution Number of small somatic variant calls and their distribution across repeat classes are similar in all conditions See example, right Confidential - Not for further distribution Data courtesy of Illumina

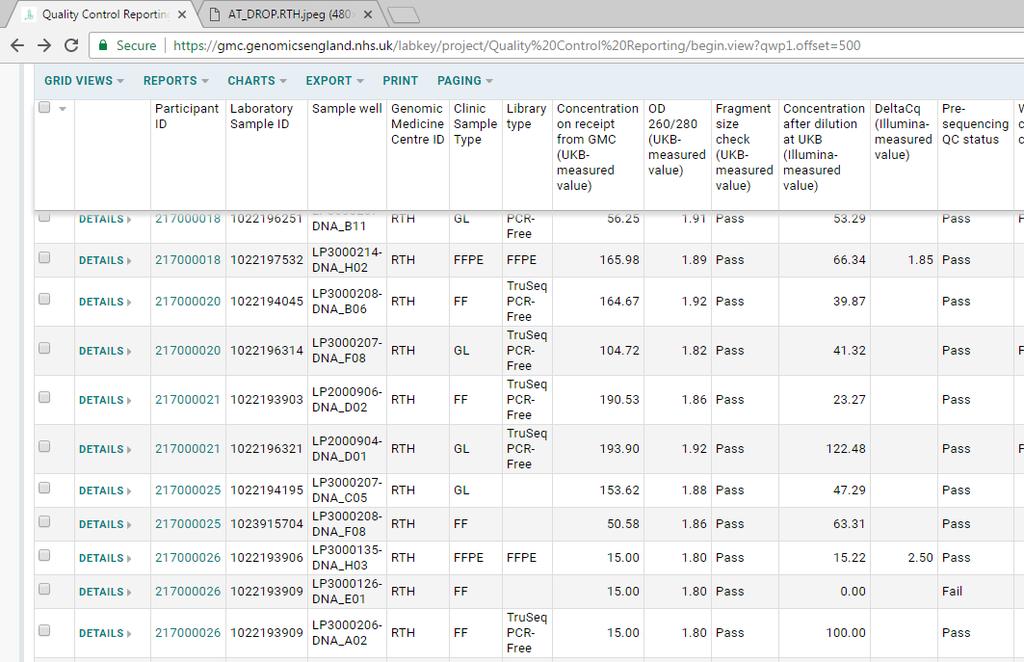
21 Paxgene: Alternative Fixatives PAXgene Tissue System Dual chamber system Tissue fixation Methanol based Tissue Stabiliser Requires formalin-free processing Morphology, IHC and ISH reported to be comparable to FFPE (Kap M et al. PLoS ONE 2011) 8 patients from 1 GMC PCR-based library prep for FFPE samples PCR-based library prep PAXgene samples PCR-free library prep for FF PCR-free library prep PAXgene samples Delta Cq values are good for all PAXgene samples; Delta Cq variable for FFPE Confidential - Not for further distribution Data courtesy of Illumina


22 Paxgene Sequencing QC runs PCR-free PAXgene libraries resemble FF most closely High-AT regions are under represented in FFPE; better with PAXgene High-GC regions are over represented with PAXgene (FFPE prep); FFPE samples are variable Confidential - Not for further distribution Data courtesy of Illumina
23 Full build data: (colorectal) purity estimate evenness score 39% 95.49% PAXgene PCR-free prep 21% 95.29% PAXgene PCR prep 48% 94.45% FFPE 45% 90.1% FF Confidential - Not for further distribution
24 PAX PCR-free PAX PCR-free PAX PCR-free PAX PCR-free Full build data: (colorectal) Somatic small variant distribution Somatic SNVs Somatic Indels Confidential - Not for further distribution Data courtesy of Illumina
25 Haemato-oncology
26 Haem-onc: Myeloid Disorders Disease Eligibility Criteria Tumour / Germline samples Additional samples High risk Myelodysplastic syndromes [MDS] / Acute myeloid Leukaemia [AML] Chronic Myeloid Leukaemia [CML] Unclassified Newly diagnosed (i.e. untreated): - MDS (blasts 10-19%) - AML (blasts >=20%) Extreme responders: - BCR-ABL transcript level using International Standards [IS] of <1% or >10% Patients who present in accelerated or blast phase (>10% blasts in PB or BMA) Patients present with cytogenetic abnormality in addition to t(9;22) Patients who progress after initial response: - Progress from chronic to accelerated / blast phase - BCR-ABL transcript level using IS reduced to <1% before increasing to >40% (on treatment) Difficult to define! But examples would include - Myelodysplastic/Myeloproliferative overlap syndromes [MDS/MPN} - Triple negative MPN - Others where mismatch between clinical diagnosis and pathological findings contact service desk if in doubt Tumour: DNA from pre-treatment peripheral blood [PB] / bone marrow aspirate [BMA] (2 ug / 500 ng) Germline intensive treatment: DNA from saliva taken at D5 of treatment (10 ug / 4 ug) Non-intensive treatment: DNA from cultured fibroblasts (10 ug / 4 ug) *alternative options being pursued Tumour: DNA from pre-treatment PB or BMA (2 ug / 500 ng) Germline: good responder: DNA from saliva at time BCR-ABL <1% (10 ug / 4 ug) All other categories: DNA from cultured fibroblasts (10 ug / 4 ug) *alternative options being pursued Tumour: DNA from pre-treatment PB or BMA (2 ug / 500 ng) Germline: DNA from cultured fibroblasts (10 ug / 4 ug) *alternative options being pursued Pre-treatment RNA (in form of GTC lysate) Pre-treatment RNA (in form of GTC lysate) Pre-treatment RNA (in form of GTC lysate) 26
27 Haem-onc: Lymphoid Disorders (1) Disease Eligibility Criteria Tumour / Germline samples Additional samples Chronic Lymphocytic Leukaemia [CLL] Myeloma - Any patient enrolled in FLAIR trial - Any untreated patient who has severe enough disease that they would meet the criteria for enrolment in the FLAIR trial and are fit enough for chemoimmunotherapy (including a purine analogue: either fludarabine or bendamustine) but have not been recruited to FLAIR for logistical, medical (e.g. poor renal function), genomic (i.e. TP53 abnormality in >20% cells) or patient choice reasons Any newly diagnosed untreated myeloma patient from whom sufficient CD138+ cells can be isolated from the BMA to make the minimum purity (>40%) and DNA requirements (>=500 ng minimum) Tumour: DNA from pre-treatment PB if lymphocytosis >25x10 9 /L, DNA from pretreatment BMA if lymphocytosis <25x10 9 /L (2 ug / 500 ng) Germline: DNA from saliva taken at a time when PB lymphocytosis is lymphocytosis <25x10 9 /L (10 ug / 4 ug) Tumour: DNA from pre-treatment CD138+ selected cells (e.g. post-column enrichment) aiming for purity >80% but will consider >40% if enrichment step undertaken (2 ug / 500 ng) Germline: DNA from PB or saliva (10 ug / 4 ug) Pre-treatment RNA (in form of GTC lysate) Baseline plasma for ctdna Follow up plasma for ctdna taken at 3/12 intervals for year 1, 6/12 intervals for year 2, time of any relapse Pre-treatment RNA (in form of GTC lysate) High grade lymphoma - Any newly diagnosed, untreated high grade lymphoma including )but not limited to): Diffuse Large B cell Lymphoma, Burkitt s lymphoma, Primary mediastinal B cell lymphoma, T cell lymphomas, Lymphoblastic lymphoma High grade lymphomas NOS - High grade [HG] transformation of a lower grade lymphoma or CLL Tumour: DNA from pre-treatment fresh frozen resection / biopsy with malignant cell percentage >=40% (2 ug / 500 ng) Germline: DNA from PB or saliva (10 ug / 4 ug) Pre-treatment RNA (in form of GTC lysate) Baseline plasma for ctdna Follow up plasma for ctdna taken at 3/12 intervals for year 1, 6/12 intervals for year 2, time of any relapse 27
28 Haem-onc: Lymphoid Disorders (2) Disease Eligibility Criteria Tumour / Germline samples Additional samples Paediatric Acute Lymphoblastic Leukaemia [ALL] Children & young adults (i.e. <25 years old at time of diagnosis) with ALL who have failed to obtain Minimal Residual Disease [MRD] levels of <5% at the D28 BMA Tumour: DNA from pre-treatment PB or BMA where blasts >=40% nucleated cells (NB will need to have DNA stored from diagnosis as will not know patient is eligible until post-d28 assessment (2 ug / 500 ng) Germline: DNA from saliva when there are no circulating blasts (morphological assessment of the peripheral blood) (10 ug / 4 ug) Pre-treatment RNA (in form of GTC lysate) 28
29 Returning Results


30 Preliminary analysis



31 Supplementary analysis Supplementary analysis Mutational signatures Structural variants Mutational density Coverage and copy number Mutation context Hypermutation rain plots
32 Cancer Analysis: Flow Main Programme (Fresh Frozen) 3,000 Cancer FF DNA Sample progress 2,500 2,511 2,000 1,687 1,500 1,000 1,276 1,194 Change to SRV Return of remaining 222 reports late June Samples at GMCs 2.1 Samples at Biobanks 2.2 DNA Dispatched to illumina 3.1 DNA passed QC 3.2 WGS Completed 4.1 WGS received by GEL 4.2 Ready for interpretation 6.1 Dispatched to GMCs Feedback received from GMCs

33 WGS with somatic small variants in 72 actionable genes Median 2.4 actionable genes across tumour types 33

34 Somatic small variants in 72 actionable genes across tumour types Breast Ovarian Colorectal Lung Renal Sarcoma Prostate Bladder 10 July
35 Cancer Analysis & Interpretation for Main Programme (for Fresh Frozen samples) 3,000 Cancer FF DNA Sample progress 2,500 2,511 2,000 1,687 1,500 1,000 1,276 1,194 Change to SRV Return of remaining 222 reports late June Samples at GMCs 2.1 Samples at Biobanks 2.2 DNA Dispatched to illumina 3.1 DNA passed QC 3.2 WGS Completed 4.1 WGS received by GEL 4.2 Ready for interpretation 6.1 Dispatched to GMCs Feedback received from GMCs
36 Interpretation in Cancer programme DNA Patient Tumour type NHS clinical team Validation Outcomes GeCIP(s) Gene Panels Report QC Reporting portal Genome sequence Annotated VCFs Gene Groups Variant filtering Variants Domains Clinical Review Knowledge Bases Annotation Providers


37 Illumina BaseSpace Variant Interpreter Associations Associations Column On/Off Tumor Type based on matching ontology term Four possible fields: Prediction: Based off ClinVar value and only possible with the Germline analysis Knowledge Base: only possible when in a workgroup BaseSpace Knowledge Network ClinVar Tiles indicate significance and number of entries: 3 7
38 Return of Germline findings
39 Proposal for expansion in return of germline variants Tier 1: high confidence pathogenic vars in gene set pertinent to tumour type susceptibility (current). Pre-annotation of pathogenic vars for childhood, Haem-Onc and other rare tumour types will be problematic?additional susceptibility variants?tier 2(OPTIONAL)*: (a) all (low freq) vars in gene set pertinent to tumour type susceptibility (b) all (low freq) vars in universal tumour type susceptibility gene set (~50 for adult solid tumours; many additional genes if expanding to haemonc and/or childhood)?addtional germline content to inform oncology management?tier 3(OPTIONAL)*: (a) all (low freq) vars in universal gene set relevant to therapy (DNA repair: HRD and BER genes) (b) all (low freq) vars in universal cancer gene set (eg cancer gene census; 572) To annotate germline var if var present in same gene or deletion spanning gene (LOH) on subtracted somatic analysis. * for local review. Molecular pathology lab receiving cancer reports should agree approach to analysis and management of these data with their molecular genetics laboratory and clinical cancer genetics service.
40 Pertinent Findings: genes Tumour Type Genes analysed Breast cancer BRCA1, BRCA2, PALB2, PTEN, TP53 Colorectal cancer MLH1, MSH2, MSH6, MUTYH (bi), PMS2, POLD1, POLE, PTEN, SMAD4, STK11 Ovarian cancer BRCA1, BRCA2, MLH1, MSH2, MSH6, PMS2, RAD51C, RAD51D Prostate cancer BRCA2 Renal Cancer FH, FLCN, PTEN, SDHB, VHL, MET Sarcoma TP53 Melanoma BAP1, (CDK4), CDKN2A Endometrial cancer FH, MLH1, MSH2, MSH6, PMS2, PTEN Adult Glioma APC, ATM (bi), MLH1, MSH2, MSH6, PMS2, TP53 Upper GI MLH1, MSH2, MSH6, PMS2 40
41 Proposal for expansion in return of germline variants Tier 1: high confidence pathogenic vars in gene set pertinent to tumour type susceptibility (current). Pre-annotation of pathogenic vars for childhood, Haem-Onc and other rare tumour types will be problematic?additional susceptibility variants?tier 2(OPTIONAL)*: (a) all (low freq) vars in gene set pertinent to tumour type susceptibility (b) all (low freq) vars in universal tumour type susceptibility gene set (~50 for adult solid tumours; many additional genes if expanding to haemonc and/or childhood)?addtional germline content to inform oncology management?tier 3(OPTIONAL)*: (a) all (low freq) vars in universal gene set relevant to therapy (DNA repair: HRD and BER genes) (b) all (low freq) vars in universal cancer gene set (eg cancer gene census; 572) To annotate germline var if var present in same gene or deletion spanning gene (LOH) on subtracted somatic analysis. * for local review. Molecular pathology lab receiving cancer reports should agree approach to analysis and management of these data with their molecular genetics laboratory and clinical cancer genetics service.
42 NHSE Cancer Transition Working Group
43 The molecular context: a dynamic field Single gene/ Standalone test Small panel (eg hot spot Amplicon ) Genome Test required Number of markers Complexity of markers Larger generic panel (eg Hybridisationcapture) Bespoke, customdesigned tumourspecific panel Other nongenetic tests Technology Cost (for depth) Chemistry/Performance TAT Whole genome sequencing: a dynamic value proposition for each tumour context
 +/-biopsy +/-biopsy LOCAL/REGIONAL DISEASE METASTATIC DISEASE neoadjuvant chemo-radiorx Adjuvant chemo-radiorx chemo-rx targeted drug chemo-rx")
44 The clinical context: a dynamic field When do we undertake molecular testing on patients? diagnostic biopsy surgery Biopsy (diagnostic/recurrence) +/-biopsy +/-biopsy LOCAL/REGIONAL DISEASE METASTATIC DISEASE neoadjuvant chemo-radiorx Adjuvant chemo-radiorx chemo-rx targeted drug chemo-rx Phase II/III Clinical trial Phase I clinical trial/ Experimental/compassi onate use drug Why do we undertake molecular testing on patients? Standard Care Diagnostic Prognostic Monitoring Targeted Drugs Clinical Trials Single new agent vs SOC Multi-arm umbrella/basket Molecular genomics-drug matching Discovery Research Longitudinal patient studies
45 Principles of evaluation capture CLINICAL; by tumour type Which genes have clinical utility for testing? What type of molecular markers in that gene? Type of actionability? Predictive, prognostic What is the level of evidence and impact: clinical (NHS) or research How widely is test implemented in NHS at the moment? LABORATORY; global What is the sensitivity of different standalone tests/ngs approaches in testing for each type of molecular marker? How well does that test/ngs approach perform wrt important metrics? Failure rate, TAT, DNA req, tolerance for DNA quality etc CLINICAL-LABORATORY; integrated; by tumour type What is the total palette of markers undertaken for that tumour type? For standard of care clinically? If we also think about entry to clinical trials/research? How well can different NGS-based approaches (panels, genomes) better deliver the palette of markers? Are standalone tests still needed? What are the INDIRECT IMPACTS of each approach (eg molecular pathology, complexity of laboratory workflow, ongoing requirement for redevelopment and redesign) CLINICAL-LABORATORY-ECONOMIC; integrated; by tumour type What is the costing for the different approaches IMMEDIATE COSTS: reagents, labcoats (INDIRECT IMPACTS: (re) development, molecular pathology) ADDITIONAL NON-LAB COSTS: data storage etc 45
46 Tumour Type experts consulted Sought input from >1 tumour type expert Tumour type Experts approached AML Anna Schuh, Angela Hamblin, Shirley Henderson Haem onc other Anna Schuh, Angela Hamblin, Shirley Henderson Sarcoma Nischalan Pillay, Adrienne Flanagan Breast Nick Turner+ NCRI clin studies group Ian Tomlinson, Gary Middleton, Phil Quirke, Nirupa Colorectal Murugaesu Ovarian James Brenton, Iain McNneish Prostate Johann De Bono, Mark Linch Crispin Hiley (cc Charlie Swanton), Andrew Hudson, Lung Gary Middleton, Nirupa Murugaesu Renal James Larkin, Samra Turajlic Brain Ashkan Keyoumars, Richard Houlston Endometrial David Church Bladder Simon Crabb John Bridgewater, Tim Meyer, Jeff Evans, Chrissie Upper GI Thirlwell Melanoma Paul Lorigan, James Larkin Childhood 46

47 40 different marker tests, 16 in standard of care testing
48 Laboratory Evaluation Gene molecular marker profile Scoring Stand alone tests Single fragment molecular marker test (e.g cobas, pyrosequencing) FISH karyotype Full gene screen (eg sanger of multiple fragments) MLPA/dosage analysis Single mutation(snv, small indel) o 3 NS NS 2 NS Oligo hot spots in same gene 3:excellent (FP and FN rate <1%, 3 NS NS 2 NS All disparate mutations across a gendetection >95% for VRF<5%) NS NS NS 2 NS Suitability/ CNV/amplification/loss 2: good (acceptable) NS 1 NS NS 2 sensitivity SV with known partner 1: poor NS NS SV with mutiple partner 0/NS: technology not suitable NS NS SV with any partner NS NS 2 NS NS Mutational signature NS NS NS NS NS High (tally score 5) DNA requirements (amount) Medium (tally score 3) Low (tally score 1) Low Medium High medium Medium tolerance of test to low quality DNA (ieffpe) 3: Good performance using poor quality DNA (ie FFPE) 2: Acceptable performance using poor quality DNA 1: Equivoval performance using 3 poor quality DNA: high quality DNA 2 NS 2 2 preferable 0: high quality DNA essential N/A: liquid tumour Needs live cells Typical TAT Failure rate 3: not required 0: required N/A: solid tumour 3: <3 days 2: <1 week 1: < 2 weeks 0: >2 weeks 3: <1% 2: 1-5% 1: 5-20% 0: >20%
49 PANELS Suitability/ sensitivity DNA requirements (amount) Gene molecular marker profile Scoring Single mutation(snv, small indel) or h Oligo hot spots in same gene 3:excellent (FP and FN rate <1%, All disparate mutations across a genedetection >95% for VRF<5%) CNV/amplification/loss 2: good (acceptable) SV with known partner 1: poor SV with mutiple partner 0/NS: technology not suitable SV with any partner Mutational signature Very High (tally score 10) High (tally score 5) Medium (tally score 3) Low (tally score 1) NGS DNA Amplicon Hot spot panel ( 200x) NGS large gene panel (Capture, generic) eg Illumina 170 genes ( 200x) NGS bespoke specific panel ( 200x) WGS at (tumour ~75x) NS NS NS NS NS NS NS 2 3 NS WGS at (tumour ~150x) Low Medium High Very High Very High tolerance of test to low quality DNA (ieffpe) 3: Good performance using poor quality DNA (ie FFPE) 2: Acceptable performance using poor quality DNA 1: Equivoval performance using poor quality DNA: high quality DNA preferable 0: high quality DNA essential N/A: liquid tumour Needs live cells Typical TAT Failure rate 3: not required 0: required N/A: solid tumour 3: <3 days 2: <1 week 1: < 2 weeks 0: >2 weeks 3: <1% 2: 1-5% 1: 5-20% 0: >20% ?? 49
50 Clinical Laboratory Integrator Context: STEP 1: SUMMARY OF MOLECULAR MARKERS FROM CLINICAL EVALUATION Standard Clinical Care count (Standard sensitivity) count (High sensitivity) Single mutation(snv, small indel) or hotspot 6 1 Oligo hot spots in same gene 0 All disparate mutations across a gene 2 CNV/amplification/loss 0 SV with known partner 8 SV with mutiple partner 0 SV with any partner 0 Mutational signature 0 STEP 2: BRINGING TESTS TOGETHER AS 5 APPROACHES Additional stand-alone non-ngs tests Single fragment molecular marker test (e.g cobas, pyro, qpcr) Full gene screen (eg sanger of multiple fragments) MLPA/dosage analysis karyotype FISH Approach1: all standalone tests Approach 2: hotspot panel(+ additional tests) Approach 3: generic gene panel(+ additional tests) Approach 4: bespoke gene panel (+ additional tests) Approach 5: (+ additional tests) Approach 6: (+ additional tests) Count of additional tests required by this approach
51 Consultation meeting: 23 rd May 2017 Adrienne Flanagan Dr Pippa Corrie Lucy Side Andrew Protheroe Fiona Carragher Manuel Salto-Tellez Anna Schuh Fiona Lalloo Mark Davies Clare Verrill Gareth Thomas Martin Gore Crispin Hiley Harpeet Wasan Nick Turner Darren Hargrave Ian Chau Nischalan Pillay David Church Ian Lewis Peter Clark David Thomson Ian Tomlinson Prof Karin Oien Dion Morton Ian Walker Rachael Hough Dr Alison Birtle Jacquie Westwood Rachel Butler Dr Andrew Biankin James Brenton Richard Edmondson Dr Andrew Pettitt James Larkin Richard Stephens Dr Colin Watts Jane Moorhead Rory Harvey Dr Daniel Rea Jo Martin Sarah Coupland Dr Lee Jeys Johann Debono Simon Crabb Dr Matt Hatton John Bridgewater Tony Williams Dr Meriel Jenney John Radford Wailup Wong 51

52 Secondary phase of data collection Review of proposed marker set Numbers, subtypes, patient journey, emerging technologies/approaches Key molecular targets going into Phase 3 To return by 26/6/17 10 July
53 Acknowledgements PILOTS/EXPERIMENTS Lab Leads: Anna Schuh Shirley Henderson Gerry Thomas Adrienne Flannagan Andrew Wallace David Gonzalez de C James Brenton Francesca Ciccarelli Emily Shaw Louise Jones Clare Verrill Pauline Robbe Dimitris Vavoulis James Hadfield ILLUMINA R&D team: Mark Ross Jenn Becq Zoya Kingsbury Sean Humphray David Bentley CANCER WORKING GROUP Dion Morton (pan cancer) James Brenton (ovary) Charles Swanton (lung) Johann de Bono (prostate) Nick Turner (breast) Ian Tomlinson (colorectal) Adrienne Flanagan (sarcoma) Josef Vormoor (childhood) James Larkin (renal) Anna Schuh (haem-onc) Crispin Hiley Mark Linch Samra Turajlicy Nischalan Pillay David Gonzalez (Imperial GMC) Frank McCaughan (SL GMC) Paul Cane (SL GMC) Tim Helliwell (NWcoast GMC) John McGrath (Wessex GMC) John Radford (Manchester GMC) Sean Grimmond (ICGC) David Cameron (clinical trials) Ian Cree (RCPath) Rowena Sharpe (CRUK) VALIDATION, INTERPRETATION AND FEEDBACK WORKING GROUP David Gonzalez de Castro (ICR/RMH) Phil Bennet (UCL) Angela Hamblin (Oxford) Shirley Henderson (Oxford) Manuel Salto-Tellez (Belfast) Andrew Wallace (Manchester) Gert Attard (Imperial) Gary Middleton (Birmingham) Rachel Butler (Cardiff) GENOMICS ENGLAND CANCER TEAM Louise Jones Alice Tuff Lacey Nirupa Murugaesu Joanne Mason Clare Craig Jason Chattoo Kay Lawson Cristina Aguilera Shirley Henderson Amanda O Neill Angela Hamblin Nancy Horseman Alona Sosinsky James Hadfield Augusto Rendon James Peach Simon Thompson Mark Caulfield Tom Fowler



54 Following the #genomes100k Like the Genomics England page Follow Genomics England /sign-up
55 FF vs FFPE by GMC as of 6 th June March June June June FF FFPE 55
Cancer Validation in the 100,000 genomes project. Dr Shirley Henderson ACGS spring meeting 06/07/16
 Cancer Validation in the 100,000 genomes project Dr Shirley Henderson ACGS spring meeting 06/07/16 Cancer is a lesion of the Genome Diagnosis Cancer Molecular Lesions Prognosis Disease Monitoring Why is
Cancer Validation in the 100,000 genomes project Dr Shirley Henderson ACGS spring meeting 06/07/16 Cancer is a lesion of the Genome Diagnosis Cancer Molecular Lesions Prognosis Disease Monitoring Why is
100,000 Genomes Project Update: The Cancer Programme Cancer Testing Strategy & NHS Genomic Medicine Service
 100,000 Genomes Project Update: The Cancer Programme Cancer Testing Strategy & NHS Genomic Medicine Service Nirupa Murugaesu Consultant Medical Oncologist at St George s Hospital Clinical Lead for Molecular
100,000 Genomes Project Update: The Cancer Programme Cancer Testing Strategy & NHS Genomic Medicine Service Nirupa Murugaesu Consultant Medical Oncologist at St George s Hospital Clinical Lead for Molecular
AVENIO family of NGS oncology assays ctdna and Tumor Tissue Analysis Kits
 AVENIO family of NGS oncology assays ctdna and Tumor Tissue Analysis Kits Accelerating clinical research Next-generation sequencing (NGS) has the ability to interrogate many different genes and detect
AVENIO family of NGS oncology assays ctdna and Tumor Tissue Analysis Kits Accelerating clinical research Next-generation sequencing (NGS) has the ability to interrogate many different genes and detect
The 100,000 Genomes Project Harnessing the power of genomics for NHS rare disease and cancer patients
 The 100,000 Genomes Project Harnessing the power of genomics for NHS rare disease and cancer patients Dr Richard Scott, Clinical Lead for Rare Disease Dr Nirupa Murugaesu, Clinical Lead for Cancer Four
The 100,000 Genomes Project Harnessing the power of genomics for NHS rare disease and cancer patients Dr Richard Scott, Clinical Lead for Rare Disease Dr Nirupa Murugaesu, Clinical Lead for Cancer Four
AVENIO ctdna Analysis Kits The complete NGS liquid biopsy solution EMPOWER YOUR LAB
 Analysis Kits The complete NGS liquid biopsy solution EMPOWER YOUR LAB Analysis Kits Next-generation performance in liquid biopsies 2 Accelerating clinical research From liquid biopsy to next-generation
Analysis Kits The complete NGS liquid biopsy solution EMPOWER YOUR LAB Analysis Kits Next-generation performance in liquid biopsies 2 Accelerating clinical research From liquid biopsy to next-generation
5 th July 2016 ACGS Dr Michelle Wood Laboratory Genetics, Cardiff
 5 th July 2016 ACGS Dr Michelle Wood Laboratory Genetics, Cardiff National molecular screening of patients with lung cancer for a national trial of multiple novel agents. 2000 NSCLC patients/year (late
5 th July 2016 ACGS Dr Michelle Wood Laboratory Genetics, Cardiff National molecular screening of patients with lung cancer for a national trial of multiple novel agents. 2000 NSCLC patients/year (late
Dr Yvonne Wallis Consultant Clinical Scientist West Midlands Regional Genetics Laboratory
 Dr Yvonne Wallis Consultant Clinical Scientist West Midlands Regional Genetics Laboratory Personalised Therapy/Precision Medicine Selection of a therapeutic drug based on the presence or absence of a specific
Dr Yvonne Wallis Consultant Clinical Scientist West Midlands Regional Genetics Laboratory Personalised Therapy/Precision Medicine Selection of a therapeutic drug based on the presence or absence of a specific
The 100,000 Genomes Project
 The 100,000 Genomes Project Dr Matina Prapa, Scientific co ordinator Genomics England Clinical Interpretation Partnership William Harvey Research Institute Queen Mary University of London Genomics England
The 100,000 Genomes Project Dr Matina Prapa, Scientific co ordinator Genomics England Clinical Interpretation Partnership William Harvey Research Institute Queen Mary University of London Genomics England
The Next Generation of Hereditary Cancer Testing
 The Next Generation of Hereditary Cancer Testing Why Genetic Testing? Cancers can appear to run in families. Often this is due to shared environmental or lifestyle patterns, such as tobacco use. However,
The Next Generation of Hereditary Cancer Testing Why Genetic Testing? Cancers can appear to run in families. Often this is due to shared environmental or lifestyle patterns, such as tobacco use. However,
The Cancer Research UK Stratified Medicine Programme: Phases One and Two Dr Emily Shaw
 The Cancer Research UK Stratified Medicine Programme: Phases One and Two Dr Emily Shaw Introduction The CRUK Stratified Medicine Programme: SMP1 rationale, design and implementation The role of the cellular
The Cancer Research UK Stratified Medicine Programme: Phases One and Two Dr Emily Shaw Introduction The CRUK Stratified Medicine Programme: SMP1 rationale, design and implementation The role of the cellular
CentoCancer STRIVE FOR THE MOST COMPLETE INFORMATION
 CentoCancer STRIVE FOR THE MOST COMPLETE INFORMATION CentoCancer our most comprehensive oncogenetics panel for hereditary mutations Hereditary pathogenic variants confer an increased risk of developing
CentoCancer STRIVE FOR THE MOST COMPLETE INFORMATION CentoCancer our most comprehensive oncogenetics panel for hereditary mutations Hereditary pathogenic variants confer an increased risk of developing
TGL clinical User Guide
 TGL clinical User Guide The Institute of Cancer Research Brookes Lawley Building 15 Cotswold Road Sutton, Surrey SM2 5NG Page 1 of 7 TGL clinical This document describes the services provided by TGL clinical
TGL clinical User Guide The Institute of Cancer Research Brookes Lawley Building 15 Cotswold Road Sutton, Surrey SM2 5NG Page 1 of 7 TGL clinical This document describes the services provided by TGL clinical
NCRI Biomarkers & Imaging CSG Cell-free DNA workshop
 NCRI Biomarkers & Imaging CSG Cell-free DNA workshop Workshop Report Christie Education Centre, Manchester 30th January 2014 Sponsored by Workshop summary 86 delegates from a variety of specialities attended
NCRI Biomarkers & Imaging CSG Cell-free DNA workshop Workshop Report Christie Education Centre, Manchester 30th January 2014 Sponsored by Workshop summary 86 delegates from a variety of specialities attended
Enabling Personalized
 Molecular Enabling Personalized Diagnostics Medicine- Targeted Sequencing: NGS-based solutions Silvia Dorn Roel Reinders- Andreas Diplas Friday, 19.06.2015 Company Overview Founded in April 2011 Development
Molecular Enabling Personalized Diagnostics Medicine- Targeted Sequencing: NGS-based solutions Silvia Dorn Roel Reinders- Andreas Diplas Friday, 19.06.2015 Company Overview Founded in April 2011 Development
WHAT IS A GENE? CHROMOSOME DNA PROTEIN. A gene is made up of DNA. It carries instructions to make proteins.
 WHAT IS A GENE? CHROMOSOME E GEN DNA A gene is made up of DNA. It carries instructions to make proteins. The proteins have specific jobs that help your body work normally. PROTEIN 1 WHAT HAPPENS WHEN THERE
WHAT IS A GENE? CHROMOSOME E GEN DNA A gene is made up of DNA. It carries instructions to make proteins. The proteins have specific jobs that help your body work normally. PROTEIN 1 WHAT HAPPENS WHEN THERE
BriTROC personalised biomarkers in relapsed ovarian high grade serous carcinoma
 BriTROC personalised biomarkers in relapsed ovarian high grade serous carcinoma GCIG Translational Committee 4 th June 2016 Iain McNeish Professor of Gynaecological Oncology Wolfson Wohl Cancer Research
BriTROC personalised biomarkers in relapsed ovarian high grade serous carcinoma GCIG Translational Committee 4 th June 2016 Iain McNeish Professor of Gynaecological Oncology Wolfson Wohl Cancer Research
Supplementary Tables. Supplementary Figures
 Supplementary Files for Zehir, Benayed et al. Mutational Landscape of Metastatic Cancer Revealed from Prospective Clinical Sequencing of 10,000 Patients Supplementary Tables Supplementary Table 1: Sample
Supplementary Files for Zehir, Benayed et al. Mutational Landscape of Metastatic Cancer Revealed from Prospective Clinical Sequencing of 10,000 Patients Supplementary Tables Supplementary Table 1: Sample
Analysis of Massively Parallel Sequencing Data Application of Illumina Sequencing to the Genetics of Human Cancers
 Analysis of Massively Parallel Sequencing Data Application of Illumina Sequencing to the Genetics of Human Cancers Gordon Blackshields Senior Bioinformatician Source BioScience 1 To Cancer Genetics Studies
Analysis of Massively Parallel Sequencing Data Application of Illumina Sequencing to the Genetics of Human Cancers Gordon Blackshields Senior Bioinformatician Source BioScience 1 To Cancer Genetics Studies
Enterprise Interest Thermo Fisher Scientific / Employee
 Enterprise Interest Thermo Fisher Scientific / Employee A next-generation sequencing assay to estimate tumor mutation load from FFPE research samples Fiona Hyland. Director of R&D, Bioinformatics Clinical
Enterprise Interest Thermo Fisher Scientific / Employee A next-generation sequencing assay to estimate tumor mutation load from FFPE research samples Fiona Hyland. Director of R&D, Bioinformatics Clinical
Germline Multigene Panel Testing in Oncology: Genetic Counseling Perspective
 Germline Multigene Panel Testing in Oncology: Genetic Counseling Perspective Sarah L. Campian, MS CGC Certified Genetic Counselor Nancy & James Grosfeld Cancer Genetics Center Objectives Identify patients/families
Germline Multigene Panel Testing in Oncology: Genetic Counseling Perspective Sarah L. Campian, MS CGC Certified Genetic Counselor Nancy & James Grosfeld Cancer Genetics Center Objectives Identify patients/families
WHAT IS A GENE? CHROMOSOME DNA PROTEIN. A gene is made up of DNA. It carries instructions to make proteins.
 WHAT IS A GENE? CHROMOSOME GENE DNA A gene is made up of DNA. It carries instructions to make proteins. The proteins have specific jobs that help your body work normally. PROTEIN 1 WHAT HAPPENS WHEN THERE
WHAT IS A GENE? CHROMOSOME GENE DNA A gene is made up of DNA. It carries instructions to make proteins. The proteins have specific jobs that help your body work normally. PROTEIN 1 WHAT HAPPENS WHEN THERE
Your Health Topic : Genomics and Clinical Practice How genetics is improving care for patients
 Your Health Topic : Genomics and Clinical Practice How genetics is improving care for patients Speaker Dr Kevin Monahan FRCP PhD Consultant Gastroenterologist, Family History of Bowel Cancer Clinic, Chelsea
Your Health Topic : Genomics and Clinical Practice How genetics is improving care for patients Speaker Dr Kevin Monahan FRCP PhD Consultant Gastroenterologist, Family History of Bowel Cancer Clinic, Chelsea
NGS in Cancer Pathology After the Microscope: From Nucleic Acid to Interpretation
 NGS in Cancer Pathology After the Microscope: From Nucleic Acid to Interpretation Michael R. Rossi, PhD, FACMG Assistant Professor Division of Cancer Biology, Department of Radiation Oncology Department
NGS in Cancer Pathology After the Microscope: From Nucleic Acid to Interpretation Michael R. Rossi, PhD, FACMG Assistant Professor Division of Cancer Biology, Department of Radiation Oncology Department
The benefit of. knowing. Genetic testing for hereditary cancer. A patient support guide
 The benefit of knowing Genetic testing for hereditary cancer A patient support guide Does cancer run in your family? Cancer is more common in some families. Sometimes cancer is caused by a change in a
The benefit of knowing Genetic testing for hereditary cancer A patient support guide Does cancer run in your family? Cancer is more common in some families. Sometimes cancer is caused by a change in a
NGS for Cancer Predisposition
 NGS for Cancer Predisposition Colin Pritchard MD, PhD University of Washington Dept. of Lab Medicine AMP Companion Society Meeting USCAP Boston March 22, 2015 Disclosures I am an employee of the University
NGS for Cancer Predisposition Colin Pritchard MD, PhD University of Washington Dept. of Lab Medicine AMP Companion Society Meeting USCAP Boston March 22, 2015 Disclosures I am an employee of the University
Greater Manchester Genomics Medicine Centre 100,000 genomes project - cancer newsletter No 2 March 2017
 Introduction Welcome to the edition of the cancer newsletter for The 100,000 Genomes Project (100KGP) for Greater Manchester Genomic Medicine Centre (GMC). Since the last newsletter, the Genome Teams at
Introduction Welcome to the edition of the cancer newsletter for The 100,000 Genomes Project (100KGP) for Greater Manchester Genomic Medicine Centre (GMC). Since the last newsletter, the Genome Teams at
Be Ready Pack Learn more about how Myriad myrisk is revolutionizing hereditary cancer testing.
 Be Ready Pack Learn more about how Myriad myrisk is revolutionizing hereditary cancer testing. Hereditary cancer and you Approximately 5% to 10% of all cancers develop because a person inherited a genetic
Be Ready Pack Learn more about how Myriad myrisk is revolutionizing hereditary cancer testing. Hereditary cancer and you Approximately 5% to 10% of all cancers develop because a person inherited a genetic
Characterisation of structural variation in breast. cancer genomes using paired-end sequencing on. the Illumina Genome Analyser
 Characterisation of structural variation in breast cancer genomes using paired-end sequencing on the Illumina Genome Analyser Phil Stephens Cancer Genome Project Why is it important to study cancer? Why
Characterisation of structural variation in breast cancer genomes using paired-end sequencing on the Illumina Genome Analyser Phil Stephens Cancer Genome Project Why is it important to study cancer? Why
Fluxion Biosciences and Swift Biosciences Somatic variant detection from liquid biopsy samples using targeted NGS
 APPLICATION NOTE Fluxion Biosciences and Swift Biosciences OVERVIEW This application note describes a robust method for detecting somatic mutations from liquid biopsy samples by combining circulating tumor
APPLICATION NOTE Fluxion Biosciences and Swift Biosciences OVERVIEW This application note describes a robust method for detecting somatic mutations from liquid biopsy samples by combining circulating tumor
Supplementary Figure 1. Estimation of tumour content
 Supplementary Figure 1. Estimation of tumour content a, Approach used to estimate the tumour content in S13T1/T2, S6T1/T2, S3T1/T2 and S12T1/T2. Tissue and tumour areas were evaluated by two independent
Supplementary Figure 1. Estimation of tumour content a, Approach used to estimate the tumour content in S13T1/T2, S6T1/T2, S3T1/T2 and S12T1/T2. Tissue and tumour areas were evaluated by two independent
Accel-Amplicon Panels
 Accel-Amplicon Panels Amplicon sequencing has emerged as a reliable, cost-effective method for ultra-deep targeted sequencing. This highly adaptable approach is especially applicable for in-depth interrogation
Accel-Amplicon Panels Amplicon sequencing has emerged as a reliable, cost-effective method for ultra-deep targeted sequencing. This highly adaptable approach is especially applicable for in-depth interrogation
NGS in tissue and liquid biopsy
 NGS in tissue and liquid biopsy Ana Vivancos, PhD Referencias So, why NGS in the clinics? 2000 Sanger Sequencing (1977-) 2016 NGS (2006-) ABIPrism (Applied Biosystems) Up to 2304 per day (96 sequences
NGS in tissue and liquid biopsy Ana Vivancos, PhD Referencias So, why NGS in the clinics? 2000 Sanger Sequencing (1977-) 2016 NGS (2006-) ABIPrism (Applied Biosystems) Up to 2304 per day (96 sequences
SureSelect Cancer All-In-One Custom and Catalog NGS Assays
 SureSelect Cancer All-In-One Custom and Catalog NGS Assays Detect all cancer-relevant variants in a single SureSelect assay SNV Indel TL SNV Indel TL Single DNA input Single AIO assay Single data analysis
SureSelect Cancer All-In-One Custom and Catalog NGS Assays Detect all cancer-relevant variants in a single SureSelect assay SNV Indel TL SNV Indel TL Single DNA input Single AIO assay Single data analysis
Molecular. Oncology & Pathology. Diagnostic, Prognostic, Therapeutic, and Predisposition Tests in Precision Medicine. Liquid Biopsy.
 Molecular Oncology & Pathology Hereditary Cancer Somatic Cancer Liquid Biopsy Next-Gen Sequencing qpcr Sanger Sequencing Diagnostic, Prognostic, Therapeutic, and Predisposition Tests in Precision Medicine
Molecular Oncology & Pathology Hereditary Cancer Somatic Cancer Liquid Biopsy Next-Gen Sequencing qpcr Sanger Sequencing Diagnostic, Prognostic, Therapeutic, and Predisposition Tests in Precision Medicine
A guide to genetic testing for hereditary cancers
 Cancer Testing Solutions A guide to genetic testing for hereditary cancers The benefit of knowing TM Hereditary cancer genetic testing can play a critical role in managing health Cancer touches millions
Cancer Testing Solutions A guide to genetic testing for hereditary cancers The benefit of knowing TM Hereditary cancer genetic testing can play a critical role in managing health Cancer touches millions
Introduction of an NGS gene panel into the Haemato-Oncology MPN service
 Introduction of an NGS gene panel into the Haemato-Oncology MPN service Dr. Anna Skowronska, Dr Jane Bryon, Dr Samuel Clokie, Dr Yvonne Wallis and Professor Mike Griffiths West Midlands Regional Genetics
Introduction of an NGS gene panel into the Haemato-Oncology MPN service Dr. Anna Skowronska, Dr Jane Bryon, Dr Samuel Clokie, Dr Yvonne Wallis and Professor Mike Griffiths West Midlands Regional Genetics
MSI positive MSI negative
 Pritchard et al. 2014 Supplementary Figure 1 MSI positive MSI negative Hypermutated Median: 673 Average: 659.2 Non-Hypermutated Median: 37.5 Average: 43.6 Supplementary Figure 1: Somatic Mutation Burden
Pritchard et al. 2014 Supplementary Figure 1 MSI positive MSI negative Hypermutated Median: 673 Average: 659.2 Non-Hypermutated Median: 37.5 Average: 43.6 Supplementary Figure 1: Somatic Mutation Burden
Illumina Trusight Myeloid Panel validation A R FHAN R A FIQ
 Illumina Trusight Myeloid Panel validation A R FHAN R A FIQ G E NETIC T E CHNOLOGIST MEDICAL G E NETICS, CARDIFF To Cover Background to the project Choice of panel Validation process Genes on panel, Protocol
Illumina Trusight Myeloid Panel validation A R FHAN R A FIQ G E NETIC T E CHNOLOGIST MEDICAL G E NETICS, CARDIFF To Cover Background to the project Choice of panel Validation process Genes on panel, Protocol
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer
 status in Colorectal Cancer") Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
Breast and ovarian cancer in Serbia: the importance of mutation detection in hereditary predisposition genes using NGS
 Breast and ovarian cancer in Serbia: the importance of mutation detection in hereditary predisposition genes using NGS dr sc. Ana Krivokuća Laboratory for molecular genetics Institute for Oncology and
Breast and ovarian cancer in Serbia: the importance of mutation detection in hereditary predisposition genes using NGS dr sc. Ana Krivokuća Laboratory for molecular genetics Institute for Oncology and
Using the Bravo Liquid-Handling System for Next Generation Sequencing Sample Prep
 Using the Bravo Liquid-Handling System for Next Generation Sequencing Sample Prep Tom Walsh, PhD Division of Medical Genetics University of Washington Next generation sequencing Sanger sequencing gold
Using the Bravo Liquid-Handling System for Next Generation Sequencing Sample Prep Tom Walsh, PhD Division of Medical Genetics University of Washington Next generation sequencing Sanger sequencing gold
Please Silence Your Cell Phones. Thank You
 Please Silence Your Cell Phones Thank You Utility of NGS and Comprehensive Genomic Profiling in Hematopathology Practice Maria E. Arcila M.D. Memorial Sloan Kettering Cancer Center New York, NY Disclosure
Please Silence Your Cell Phones Thank You Utility of NGS and Comprehensive Genomic Profiling in Hematopathology Practice Maria E. Arcila M.D. Memorial Sloan Kettering Cancer Center New York, NY Disclosure
Personalised medicine: Past, present and future
 Kathmandu, Bir Hospital visit, August 2018 Personalised medicine: Past, present and future Rodney J. Scott University of Newcastle, NSW, Australia & Hunter Area Pathology Service Current Medical Care Started
Kathmandu, Bir Hospital visit, August 2018 Personalised medicine: Past, present and future Rodney J. Scott University of Newcastle, NSW, Australia & Hunter Area Pathology Service Current Medical Care Started
ACE ImmunoID. ACE ImmunoID. Precision immunogenomics. Precision Genomics for Immuno-Oncology
 ACE ImmunoID ACE ImmunoID Precision immunogenomics Precision Genomics for Immuno-Oncology Personalis, Inc. A universal biomarker platform for immuno-oncology Patient response to cancer immunotherapies
ACE ImmunoID ACE ImmunoID Precision immunogenomics Precision Genomics for Immuno-Oncology Personalis, Inc. A universal biomarker platform for immuno-oncology Patient response to cancer immunotherapies
100,000 genomes RD Validation and Reporting Working Groups - Overview - Dom McMullan Chair Association for Clinical Genomic Science
 100,000 genomes RD Validation and Reporting Working Groups - Overview - Dom McMullan Chair Association for Clinical Genomic Science What? More Working Groups? Post January 20 th meeting Volunteers for
100,000 genomes RD Validation and Reporting Working Groups - Overview - Dom McMullan Chair Association for Clinical Genomic Science What? More Working Groups? Post January 20 th meeting Volunteers for
Personalised cancer care Information for Medical Specialists. A new way to unlock treatment options for your patients
 Personalised cancer care Information for Medical Specialists A new way to unlock treatment options for your patients Contents Optimised for clinical benefit 4 Development history 4 Full FIND IT panel vs
Personalised cancer care Information for Medical Specialists A new way to unlock treatment options for your patients Contents Optimised for clinical benefit 4 Development history 4 Full FIND IT panel vs
End of Grant Report. Registered Charity
 End of Grant Report Dr Sally George. Report at the end of the grant by Christopher s Smile for the 3 year position of Clinical research Fellow in the Paediatric Solid Tumour Biology Team at The Institute
End of Grant Report Dr Sally George. Report at the end of the grant by Christopher s Smile for the 3 year position of Clinical research Fellow in the Paediatric Solid Tumour Biology Team at The Institute
Session 4 Rebecca Poulos
 The Cancer Genome Atlas (TCGA) & International Cancer Genome Consortium (ICGC) Session 4 Rebecca Poulos Prince of Wales Clinical School Introductory bioinformatics for human genomics workshop, UNSW 20
The Cancer Genome Atlas (TCGA) & International Cancer Genome Consortium (ICGC) Session 4 Rebecca Poulos Prince of Wales Clinical School Introductory bioinformatics for human genomics workshop, UNSW 20
What do blood cancer patients want? (And what do we need and expect too?)
") What do blood cancer patients want? (And what do we need and expect too?) John Reeve, Consumer Rep Haem. Onc. CSG Richard Stephens, Patient Member, NCIN Haematology SSCRG Delivering clinical research to
What do blood cancer patients want? (And what do we need and expect too?) John Reeve, Consumer Rep Haem. Onc. CSG Richard Stephens, Patient Member, NCIN Haematology SSCRG Delivering clinical research to
plasma MATCH Andrew Wardley,
 in partnership with plasma MATCH A multiple parallel cohort, open-label, multi-centre phase IIa clinical trial of circulating tumour DNA screening to direct targeted therapies in patients with advanced
in partnership with plasma MATCH A multiple parallel cohort, open-label, multi-centre phase IIa clinical trial of circulating tumour DNA screening to direct targeted therapies in patients with advanced
GYNplus. genetic testing for hereditary ovarian and/or uterine cancer
 GYNplus genetic testing for hereditary ovarian and/or uterine cancer What Are the Causes of Hereditary Ovarian and Uterine Cancer? uterine cancer ovarian cancer sporadic 70-80% hereditary 5% Lynch syndrome
GYNplus genetic testing for hereditary ovarian and/or uterine cancer What Are the Causes of Hereditary Ovarian and Uterine Cancer? uterine cancer ovarian cancer sporadic 70-80% hereditary 5% Lynch syndrome
NeoTYPE Cancer Profiles
 NeoTYPE Cancer Profiles Multimethod Analysis of 25+ Hematologic Diseases and Solid Tumors Anatomic Pathology FISH Molecular The next generation of diagnostic, prognostic, and therapeutic assessment NeoTYPE
NeoTYPE Cancer Profiles Multimethod Analysis of 25+ Hematologic Diseases and Solid Tumors Anatomic Pathology FISH Molecular The next generation of diagnostic, prognostic, and therapeutic assessment NeoTYPE
An innovative multi-dimensional NGS approach to understanding the tumor microenvironment and evolution
 An innovative multi-dimensional NGS approach to understanding the tumor microenvironment and evolution James H. Godsey, Ph.D. Vice President, Research & Development Clinical Sequencing Division (CSD) Life
An innovative multi-dimensional NGS approach to understanding the tumor microenvironment and evolution James H. Godsey, Ph.D. Vice President, Research & Development Clinical Sequencing Division (CSD) Life
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
The Role of genetic Testing for Inherited Prostate Cancer Risk
 FOIU July 2018 The Role of genetic Testing for Inherited Prostate Cancer Risk Leonard G. Gomella, MD Chairman, Department of Urology Sidney Kimmel Cancer Center Thomas Jefferson University Philadelphia,
FOIU July 2018 The Role of genetic Testing for Inherited Prostate Cancer Risk Leonard G. Gomella, MD Chairman, Department of Urology Sidney Kimmel Cancer Center Thomas Jefferson University Philadelphia,
GYNplus: A Genetic Test for Hereditary Ovarian and/or Uterine Cancer
 GYNplus: A Genetic Test for Hereditary Ovarian and/or Uterine Cancer Causes of Hereditary Ovarian and Uterine Cancer uterine cancer ovarian cancer Sporadic 75-90% Sporadic 70-80% Hereditary, 5% Lynch syndrome
GYNplus: A Genetic Test for Hereditary Ovarian and/or Uterine Cancer Causes of Hereditary Ovarian and Uterine Cancer uterine cancer ovarian cancer Sporadic 75-90% Sporadic 70-80% Hereditary, 5% Lynch syndrome
Abstract. Optimization strategy of Copy Number Variant calling using Multiplicom solutions APPLICATION NOTE. Introduction
 Optimization strategy of Copy Number Variant calling using Multiplicom solutions Michael Vyverman, PhD; Laura Standaert, PhD and Wouter Bossuyt, PhD Abstract Copy number variations (CNVs) represent a significant
Optimization strategy of Copy Number Variant calling using Multiplicom solutions Michael Vyverman, PhD; Laura Standaert, PhD and Wouter Bossuyt, PhD Abstract Copy number variations (CNVs) represent a significant
Evaluation of BRCA1/2 and homologous recombination defects in ovarian cancer and impact on clinical outcomes
 Evaluation of BRCA1/2 and homologous recombination defects in ovarian cancer and impact on clinical outcomes Melinda S. Yates, PhD Department of Gynecologic Oncology & Reproductive Medicine University
Evaluation of BRCA1/2 and homologous recombination defects in ovarian cancer and impact on clinical outcomes Melinda S. Yates, PhD Department of Gynecologic Oncology & Reproductive Medicine University
Cytogenetics 101: Clinical Research and Molecular Genetic Technologies
 Cytogenetics 101: Clinical Research and Molecular Genetic Technologies Topics for Today s Presentation 1 Classical vs Molecular Cytogenetics 2 What acgh? 3 What is FISH? 4 What is NGS? 5 How can these
Cytogenetics 101: Clinical Research and Molecular Genetic Technologies Topics for Today s Presentation 1 Classical vs Molecular Cytogenetics 2 What acgh? 3 What is FISH? 4 What is NGS? 5 How can these
Learn your genetic risk for the most common hereditary cancers.
 Learn your genetic risk for the most common hereditary cancers. color.com Color analyzes 30 genes including BRCA1 and BRCA2 to help women and men understand their risk for the most common hereditary cancers,
Learn your genetic risk for the most common hereditary cancers. color.com Color analyzes 30 genes including BRCA1 and BRCA2 to help women and men understand their risk for the most common hereditary cancers,
Objectives. Morphology and IHC. Flow and Cyto FISH. Testing for Heme Malignancies 3/20/2013
 Molecular Markers in Hematologic Malignancy: Ways to locate the needle in the haystack. Objectives Review the types of testing for hematologic malignancies Understand rationale for molecular testing Marcie
Molecular Markers in Hematologic Malignancy: Ways to locate the needle in the haystack. Objectives Review the types of testing for hematologic malignancies Understand rationale for molecular testing Marcie
Schedule of Accreditation issued by United Kingdom Accreditation Service 2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK
 2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK NW Thames Regional Genetics Laboratory Northwick Park Hospital Watford Road Harrow HA1 3UJ United Kingdom Contact: Caroline Sullivan Tel:
2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK NW Thames Regional Genetics Laboratory Northwick Park Hospital Watford Road Harrow HA1 3UJ United Kingdom Contact: Caroline Sullivan Tel:
The Value of Panel Testing in Inherited Breast Cancer Risk Assessment. Rodney J. Scott Division of Molecular Medicine
 The Value of Panel Testing in Inherited Breast Cancer Risk Assessment Rodney J. Scott Division of Molecular Medicine Mutation Detection Next Generation DNA sequencing has revolutionised mutation detection
The Value of Panel Testing in Inherited Breast Cancer Risk Assessment Rodney J. Scott Division of Molecular Medicine Mutation Detection Next Generation DNA sequencing has revolutionised mutation detection
Molecular Diagnostics Centre
 Directorate of Central Manchester Haematology Service Molecular Diagnostics Centre Haemato-Oncology User Guide 2014 Page 1 of 13 Directorate of CONTENTS About Us 3 Contact Details 3 Location 3 Postal Address
Directorate of Central Manchester Haematology Service Molecular Diagnostics Centre Haemato-Oncology User Guide 2014 Page 1 of 13 Directorate of CONTENTS About Us 3 Contact Details 3 Location 3 Postal Address
TP53 mutational profile in CLL : A retrospective study of the FILO group.
 TP53 mutational profile in CLL : A retrospective study of the FILO group. Fanny Baran-Marszak Hopital Avicenne Bobigny France 2nd ERIC workshop on TP53 analysis in CLL, Stresa 2017 TP53 abnormalities :
TP53 mutational profile in CLL : A retrospective study of the FILO group. Fanny Baran-Marszak Hopital Avicenne Bobigny France 2nd ERIC workshop on TP53 analysis in CLL, Stresa 2017 TP53 abnormalities :
Multi-drug, genetic-marker-directed, non-comparative, multi-centre, multi-arm phase II trial in non-small cell lung cancer
 Multi-drug, genetic-marker-directed, non-comparative, multi-centre, multi-arm phase II trial in non-small cell lung cancer Sponsor: University of Birmingham Chief Investigator: Gary Middleton Chief Biostatistician:
Multi-drug, genetic-marker-directed, non-comparative, multi-centre, multi-arm phase II trial in non-small cell lung cancer Sponsor: University of Birmingham Chief Investigator: Gary Middleton Chief Biostatistician:
A complete next-generation sequencing workfl ow for circulating cell-free DNA isolation and analysis
 APPLICATION NOTE Cell-Free DNA Isolation Kit A complete next-generation sequencing workfl ow for circulating cell-free DNA isolation and analysis Abstract Circulating cell-free DNA (cfdna) has been shown
APPLICATION NOTE Cell-Free DNA Isolation Kit A complete next-generation sequencing workfl ow for circulating cell-free DNA isolation and analysis Abstract Circulating cell-free DNA (cfdna) has been shown
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
Introduction to liquid biopsies. Rachel Butler All Wales Genetics Laboratory
 Introduction to liquid biopsies Rachel Butler All Wales Genetics Laboratory What is cell free DNA? Non-Invasive Prenatal Testing (NIPT) Extract DNA Genetic alterations detectable in circulating cell-free
Introduction to liquid biopsies Rachel Butler All Wales Genetics Laboratory What is cell free DNA? Non-Invasive Prenatal Testing (NIPT) Extract DNA Genetic alterations detectable in circulating cell-free
The Center for PERSONALIZED DIAGNOSTICS
 The Center for PERSONALIZED DIAGNOSTICS Precision Diagnostics for Personalized Medicine A joint initiative between The Department of Pathology and Laboratory Medicine & The Abramson Cancer Center The (CPD)
The Center for PERSONALIZED DIAGNOSTICS Precision Diagnostics for Personalized Medicine A joint initiative between The Department of Pathology and Laboratory Medicine & The Abramson Cancer Center The (CPD)
QIAGEN Complete Solutions for Liquid Biopsy Molecular Testing
 QIAGEN Complete Solutions for Liquid Biopsy Molecular Testing Christopher Swagell, PhD Market Development Manager, Advanced Molecular Pathology QIAGEN 1 Agenda QIAGEN Solid Tumor Testing and Liquid Biopsy
QIAGEN Complete Solutions for Liquid Biopsy Molecular Testing Christopher Swagell, PhD Market Development Manager, Advanced Molecular Pathology QIAGEN 1 Agenda QIAGEN Solid Tumor Testing and Liquid Biopsy
Germline Testing for Hereditary Cancer with Multigene Panel
 Germline Testing for Hereditary Cancer with Multigene Panel Po-Han Lin, MD Department of Medical Genetics National Taiwan University Hospital 2017-04-20 Disclosure No relevant financial relationships with
Germline Testing for Hereditary Cancer with Multigene Panel Po-Han Lin, MD Department of Medical Genetics National Taiwan University Hospital 2017-04-20 Disclosure No relevant financial relationships with
ACE ImmunoID Biomarker Discovery Solutions ACE ImmunoID Platform for Tumor Immunogenomics
 ACE ImmunoID Biomarker Discovery Solutions ACE ImmunoID Platform for Tumor Immunogenomics Precision Genomics for Immuno-Oncology Personalis, Inc. ACE ImmunoID When one biomarker doesn t tell the whole
ACE ImmunoID Biomarker Discovery Solutions ACE ImmunoID Platform for Tumor Immunogenomics Precision Genomics for Immuno-Oncology Personalis, Inc. ACE ImmunoID When one biomarker doesn t tell the whole
Multigene Panel Testing for Hereditary Cancer Risk
 Multigene Panel Testing for Hereditary Cancer Risk Dana Zakalik, M.D. Director, Nancy and James Grosfeld Cancer Genetics Center Professor, OUWB Medical School MCC Annual Meeting November 4, 2015 Outline
Multigene Panel Testing for Hereditary Cancer Risk Dana Zakalik, M.D. Director, Nancy and James Grosfeld Cancer Genetics Center Professor, OUWB Medical School MCC Annual Meeting November 4, 2015 Outline
COMPUTATIONAL OPTIMISATION OF TARGETED DNA SEQUENCING FOR CANCER DETECTION
 COMPUTATIONAL OPTIMISATION OF TARGETED DNA SEQUENCING FOR CANCER DETECTION Pierre Martinez, Nicholas McGranahan, Nicolai Juul Birkbak, Marco Gerlinger, Charles Swanton* SUPPLEMENTARY INFORMATION SUPPLEMENTARY
COMPUTATIONAL OPTIMISATION OF TARGETED DNA SEQUENCING FOR CANCER DETECTION Pierre Martinez, Nicholas McGranahan, Nicolai Juul Birkbak, Marco Gerlinger, Charles Swanton* SUPPLEMENTARY INFORMATION SUPPLEMENTARY
NGS Gateway Lab Services
 TM NGS Gateway Lab Services Accelerating Precision Medicine Design a Complete Genomic Testing Portfolio with Turnkey Assays About NGS Gateway Lab Services TM Designed to provide a gateway to your own in-house
TM NGS Gateway Lab Services Accelerating Precision Medicine Design a Complete Genomic Testing Portfolio with Turnkey Assays About NGS Gateway Lab Services TM Designed to provide a gateway to your own in-house
patient guide CancerNext-Expanded genetic testing for hereditary cancer Because knowing your risk can mean early detection and prevention
 patient guide CancerNext-Expanded genetic testing for hereditary cancer Because knowing your risk can mean early detection and prevention Know the Basics Cancer occurs in about 1 in 3 adults in their lifetime
patient guide CancerNext-Expanded genetic testing for hereditary cancer Because knowing your risk can mean early detection and prevention Know the Basics Cancer occurs in about 1 in 3 adults in their lifetime
Are you at risk of Hereditary Cancer? Your Guide to the Answers
 Are you at risk of Hereditary Cancer? Your Guide to the Answers What is Hereditary Cancer? The genes we are born with may contribute to our risk of developing certain types of cancer, including breast,
Are you at risk of Hereditary Cancer? Your Guide to the Answers What is Hereditary Cancer? The genes we are born with may contribute to our risk of developing certain types of cancer, including breast,
Molecular Testing Updates. Karen Rasmussen, PhD, FACMG Clinical Molecular Genetics Spectrum Medical Group, Pathology Division Portland, Maine
 Molecular Testing Updates Karen Rasmussen, PhD, FACMG Clinical Molecular Genetics Spectrum Medical Group, Pathology Division Portland, Maine Keeping Up with Predictive Molecular Testing in Oncology: Technical
Molecular Testing Updates Karen Rasmussen, PhD, FACMG Clinical Molecular Genetics Spectrum Medical Group, Pathology Division Portland, Maine Keeping Up with Predictive Molecular Testing in Oncology: Technical
Anna Schuh, MD, Ph.D.
 Anna Schuh, MD, Ph.D. Current position: Associate Professor and Director of Molecular Diagnostics in the Department of Oncology University of Oxford Honorary Consultant Hematologist at Oxford University
Anna Schuh, MD, Ph.D. Current position: Associate Professor and Director of Molecular Diagnostics in the Department of Oncology University of Oxford Honorary Consultant Hematologist at Oxford University
Clinical Grade Genomic Profiling: The Time Has Come
 Clinical Grade Genomic Profiling: The Time Has Come Gary Palmer, MD, JD, MBA, MPH Senior Vice President, Medical Affairs Foundation Medicine, Inc. Oct. 22, 2013 1 Why We Are Here A Shared Vision At Foundation
Clinical Grade Genomic Profiling: The Time Has Come Gary Palmer, MD, JD, MBA, MPH Senior Vice President, Medical Affairs Foundation Medicine, Inc. Oct. 22, 2013 1 Why We Are Here A Shared Vision At Foundation
Transform genomic data into real-life results
 CLINICAL SUMMARY Transform genomic data into real-life results Biomarker testing and targeted therapies can drive improved outcomes in clinical practice New FDA-Approved Broad Companion Diagnostic for
CLINICAL SUMMARY Transform genomic data into real-life results Biomarker testing and targeted therapies can drive improved outcomes in clinical practice New FDA-Approved Broad Companion Diagnostic for
Frequency(%) KRAS G12 KRAS G13 KRAS A146 KRAS Q61 KRAS K117N PIK3CA H1047 PIK3CA E545 PIK3CA E542K PIK3CA Q546. EGFR exon19 NFS-indel EGFR L858R
 KRAS G12 KRAS G13 KRAS A146 KRAS Q61 KRAS K117N PIK3CA H1047 PIK3CA E545 PIK3CA E542K PIK3CA Q546. EGFR exon19 NFS-indel EGFR L858R") Frequency(%) 1 a b ALK FS-indel ALK R1Q HRAS Q61R HRAS G13R IDH R17K IDH R14Q MET exon14 SS-indel KIT D8Y KIT L76P KIT exon11 NFS-indel SMAD4 R361 IDH1 R13 CTNNB1 S37 CTNNB1 S4 AKT1 E17K ERBB D769H ERBB
Frequency(%) 1 a b ALK FS-indel ALK R1Q HRAS Q61R HRAS G13R IDH R17K IDH R14Q MET exon14 SS-indel KIT D8Y KIT L76P KIT exon11 NFS-indel SMAD4 R361 IDH1 R13 CTNNB1 S37 CTNNB1 S4 AKT1 E17K ERBB D769H ERBB
Circulating Tumor DNA in GIST and its Implications on Treatment
 Circulating Tumor DNA in GIST and its Implications on Treatment October 2 nd 2017 Dr. Ciara Kelly Assistant Attending Physician Sarcoma Medical Oncology Service Objectives Background Liquid biopsy & ctdna
Circulating Tumor DNA in GIST and its Implications on Treatment October 2 nd 2017 Dr. Ciara Kelly Assistant Attending Physician Sarcoma Medical Oncology Service Objectives Background Liquid biopsy & ctdna
Genetic testing for hereditary cancer
 Genetic testing for hereditary cancer THE GENETICS OF HEREDITARY CANCER About half of all men and one-third of all women in the US will develop cancer during their lifetimes. Approximately 5% to 10% of
Genetic testing for hereditary cancer THE GENETICS OF HEREDITARY CANCER About half of all men and one-third of all women in the US will develop cancer during their lifetimes. Approximately 5% to 10% of
IntelliGENSM. Integrated Oncology is making next generation sequencing faster and more accessible to the oncology community.
 IntelliGENSM Integrated Oncology is making next generation sequencing faster and more accessible to the oncology community. NGS TRANSFORMS GENOMIC TESTING Background Cancers may emerge as a result of somatically
IntelliGENSM Integrated Oncology is making next generation sequencing faster and more accessible to the oncology community. NGS TRANSFORMS GENOMIC TESTING Background Cancers may emerge as a result of somatically
NeoTYPE Cancer Profiles
 NeoTYPE Cancer Profiles 30+ Multimethod Assays for Hematologic Diseases and Solid Tumors Molecular FISH Anatomic Pathology The next generation of diagnostic, prognostic, and therapeutic assessment What
NeoTYPE Cancer Profiles 30+ Multimethod Assays for Hematologic Diseases and Solid Tumors Molecular FISH Anatomic Pathology The next generation of diagnostic, prognostic, and therapeutic assessment What
The use of diagnostic FFPE material in cancer epidemiology research
 The use of diagnostic FFPE material in cancer epidemiology research Neil O Callaghan Genetic Epidemiology Laboratory Department of Pathology The University of Melbourne www.pedigree.org.au Overview Who
The use of diagnostic FFPE material in cancer epidemiology research Neil O Callaghan Genetic Epidemiology Laboratory Department of Pathology The University of Melbourne www.pedigree.org.au Overview Who
Molecular Pathology Evaluation Panel and Molecular Pathology Consortium Advice Note
 Molecular Pathology Evaluation Panel and Molecular Pathology Consortium Advice Note MPEP/MPC Advice Note 2016-02 June 2016 Test evaluated: Tumour Protein p53 (TP53) Molecular Pathology Evaluation Panel
Molecular Pathology Evaluation Panel and Molecular Pathology Consortium Advice Note MPEP/MPC Advice Note 2016-02 June 2016 Test evaluated: Tumour Protein p53 (TP53) Molecular Pathology Evaluation Panel
Genetic Risk Assessment for Cancer
 Genetic Risk Assessment for Cancer Jennifer Siettmann, MS CGC Certified Genetic Counselor Banner MD Anderson Cancer Center Objectives Describe the role of genetic counseling and genetic testing in patient
Genetic Risk Assessment for Cancer Jennifer Siettmann, MS CGC Certified Genetic Counselor Banner MD Anderson Cancer Center Objectives Describe the role of genetic counseling and genetic testing in patient
Assessment and Management of Genetic Predisposition to Breast Cancer. Dr Munaza Ahmed Consultant Clinical Geneticist 2/7/18
 Assessment and Management of Genetic Predisposition to Breast Cancer Dr Munaza Ahmed Consultant Clinical Geneticist 2/7/18 Overview The role of the Cancer Genetics team NICE guidelines for Familial Breast
Assessment and Management of Genetic Predisposition to Breast Cancer Dr Munaza Ahmed Consultant Clinical Geneticist 2/7/18 Overview The role of the Cancer Genetics team NICE guidelines for Familial Breast
A Patient s Guide to Hereditary Cancer. Is Hereditary Cancer Testing Right for You?
 A Patient s Guide to Hereditary Cancer Is Hereditary Cancer Testing Right for You? What is Hereditary Cancer? Most cancers occur in people who do not have a strong family history of that cancer. This is
A Patient s Guide to Hereditary Cancer Is Hereditary Cancer Testing Right for You? What is Hereditary Cancer? Most cancers occur in people who do not have a strong family history of that cancer. This is
Genomic Medicine: What every pathologist needs to know
 Genomic Medicine: What every pathologist needs to know Stephen P. Ethier, Ph.D. Professor, Department of Pathology and Laboratory Medicine, MUSC Director, MUSC Center for Genomic Medicine Genomics and
Genomic Medicine: What every pathologist needs to know Stephen P. Ethier, Ph.D. Professor, Department of Pathology and Laboratory Medicine, MUSC Director, MUSC Center for Genomic Medicine Genomics and
Molecular Markers. Marcie Riches, MD, MS Associate Professor University of North Carolina Scientific Director, Infection and Immune Reconstitution WC
 Molecular Markers Marcie Riches, MD, MS Associate Professor University of North Carolina Scientific Director, Infection and Immune Reconstitution WC Overview Testing methods Rationale for molecular testing
Molecular Markers Marcie Riches, MD, MS Associate Professor University of North Carolina Scientific Director, Infection and Immune Reconstitution WC Overview Testing methods Rationale for molecular testing
Consensus statement between CM-Path, CRUK and the PHG Foundation following on from the Liquid Biopsy workshop on the 8th March 2018
 Consensus statement between CM-Path, CRUK and the PHG Foundation following on from the Liquid Biopsy workshop on the 8th March 2018 Summary: This document follows on from the findings of the CM-Path The
Consensus statement between CM-Path, CRUK and the PHG Foundation following on from the Liquid Biopsy workshop on the 8th March 2018 Summary: This document follows on from the findings of the CM-Path The
Performance Characteristics BRCA MASTR Plus Dx
 Performance Characteristics BRCA MASTR Plus Dx with drmid Dx for Illumina NGS systems Manufacturer Multiplicom N.V. Galileïlaan 18 2845 Niel Belgium Table of Contents 1. Workflow... 4 2. Performance Characteristics
Performance Characteristics BRCA MASTR Plus Dx with drmid Dx for Illumina NGS systems Manufacturer Multiplicom N.V. Galileïlaan 18 2845 Niel Belgium Table of Contents 1. Workflow... 4 2. Performance Characteristics
Out-Patient Billing CPT Codes
 Out-Patient Billing CPT Codes Updated Date: August 3, 08 Client Billed Molecular Tests HPV DNA Tissue Testing 8764 No Medicare Billed - Molecular Tests NeoARRAY NeoARRAY SNP/Cytogenetic No 89 NeoLAB NeoLAB
Out-Patient Billing CPT Codes Updated Date: August 3, 08 Client Billed Molecular Tests HPV DNA Tissue Testing 8764 No Medicare Billed - Molecular Tests NeoARRAY NeoARRAY SNP/Cytogenetic No 89 NeoLAB NeoLAB