RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER
|
|
|
- Jonah Bryant
- 6 years ago
- Views:
Transcription
1 RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER
2 INTRODUCTION
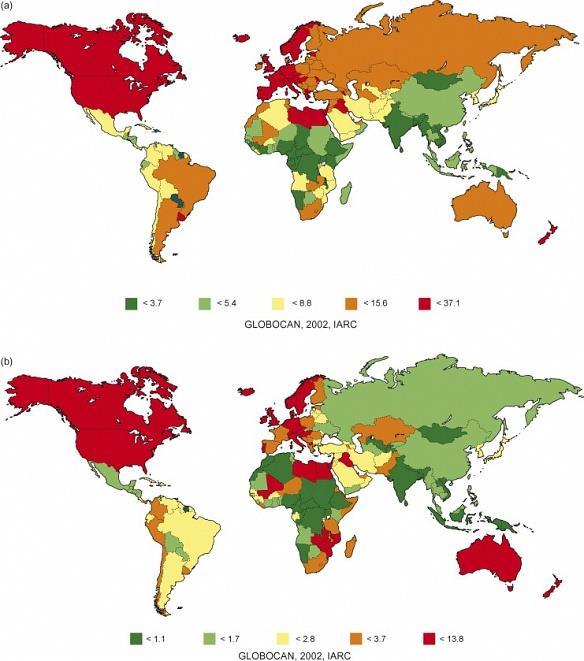
3 Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality: 12.1 Seventh most common cancer in women Incidence: 9.5 mortality: 4.5 At diagnosis >70%: > 65 y of age
4
5 Histology 90-95% 3% 2% <1% transitional-cell carcinoma squamous-cell carcinoma adenocarcinoma small-cell carcinoma
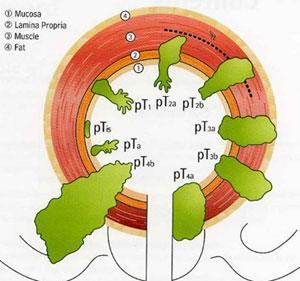
6 Entities 75-85% 10-15% 5% superficial bladder cancer pta, ptis, pt1 muscle-invasive bladder cancer pt2, pt3, pt4 metastatic bladder cancer N+, M+
7

8 Stage and Prognosis Stage TNM 5-y. Survival 0 Ta/Tis NoMo >85% I T1NoMo 65-75% II T2a-b NoMo 57% III T3a-4aNoMo 31% IV T4bNoMo 24% each T N+Mo 14% each T M+ med. 6-9 Mo
9 Treatment of choice for: Superficial Bladder tumours: The most common presentation is of Ta and T1 tumor. TURBT is the treatment of choice for Ta, G1 tumors High grade lesions may require adjuvant intra-vesical BCG. Muscle Invasive Bladder cancers: Radical cystectomy has been standard of care for two decades But organ-preserving regimens using multiple-modality therapy, consisting of TUR followed by irradiation and concurrent chemotherapy, emerging as viable alternatives. The ultimate goal is to maximize the quality of life by refining the treatment choice.
10 Results of radical cystectomy Stage Recurrence-Free / Overall Survival 5 years Organ-confined (<pt2pno) 73% 62% non-organ-confined (>pt2pno) 56% 49% Positive lymph nodes (pt1-4, pn+) 33% 24% Madersbacher et al JCO 2003;21:690
11 RADIOTHERAPY IN BLADDER CANCERS
12 Why radiotherapy? In a large series of high risk T1 cancers treated with either TURBT plus RT/RCT (University of Erlangen), only 15% of patients progressed to muscle-invasive disease after 5 years and more than 80% of those alive at 5 years preserved their bladder. In patients with unifocal T2-T3a disease, <5cm size, no hydronephrosis, good initial bladder function and visibly complete TURBT.. bladder preserving approach is preferred. Radiotherapy alone is being used less frequently in the management of patients with bladder cancer. It became, however, an important part of a multimodality bladder preservation program.
13 The five year control ranged from 31% to 45% for the entire population and from 49% to 79% for patients with complete response. Factors reported as having a significant favorable effect on local control with RT include: Early clinical stage (T2 and T3a) Absence of ureteral obstruction Complete response Visibly complete TURBT Absence of coexisting CIS Small tumor size (<5cm in diameter) Solitary tumors Tumor configuration (papillary vs. sessile) Hemoglobin level (>10g/dl)
14 When is radiotherapy delivered?? Radiation therapy for cancers of the urinary bladder can be delivered as external beam or as brachytherapy; and the intent of treatment can be: Pre-operative Post-operative Concurrent chemo-radiation as a part of multi-modality bladder sparing protocol Radiotherapy alone especially in elderly patients Palliative radiotherapy
15 Pre-operative Radiotherapy The aims of preoperative radiotherapy include: Tumor size reduction in locally advanced, muscleinvasive disease, resulting in down staging and make surgery easier, Decrease in the incidence of local recurrence following radical cystectomy, Decrease in the incidence of distant metastasis, Improvement of survival No increase in the incidence of surgical complications.
16 Evidence for pre-operative radiation Study of 724 bladder cancer patients at M.D. Anderson Hospital. Radiotherapy: 50 Gy/25 #/5 weeks, followed 6 weeks later by radical cystectomy. Treatment results in this group (I) were compared with patients who received definitive radiotherapy alone (group II) and postoperative irradiation (group III). The 5- and 10-year survival were 23% and 20%, respectively, for group I; 16% and 8% for group II; and 40% and 14%, respectively, for group III patients. Benefit seen in: Improving overall survival and disease-free survival Increase in freedom from distant metastasis Recommended in young patients with T3 disease However when compared to definitive chemo-radiation, there is no significant improvement in bladder preservation.
17 Post-operative Radiotherapy Indicated when there is extravesical disease or positive surgical margins. Administration of adjuvant irradiation decreases probability of tumor recurrence following radical cystectomy. However morbidity of post operative radiation is high due to small bowel toxicity that occupies pelvis after cystectomy.
18 TUR and adjuvant Radio-Chemotherapy 5 year Survival 50-65% Preservation of Bladder 38-43%
19 Radiotherapy in the Elderly These patients may also have coexisting medical conditions contraindicating the use of conventional bladder-sparing therapy or radical cystectomy. Radiotherapy alone consisting of a 6- to 7-week course of daily treatments may create a hardship on the patient On the other hand no-treatment option is likely to lead to distressing symptoms and signs of progressive disease such as pain, gross hematuria, frequency, and dysuria. Duchesne et al conducted a prospective randomized trial in 500 patients to compare the outcome in hypofractionated RT. There was no significant difference between the two treatment groups (35 Gy/10 # Vs 21 Gy / 7 #) in important study end points, including palliative effect, toxicity, and survival
20 Bladder-sparing therapy for invasive bladder cancer High probability of subsequent distant metastasis after cystectomy or radiotherapy alone (50% within 2 years) Radiotherapy alone in comparison with cystectomy has inferior results (local control 40%) Muscle-invasive bladder cancer is often a systemic disease HENCE... Need for combined modality therapy
21 Bladder-sparing protocol Transurthral resection Induction Therapy: Radiation + chemotherapy (cisplatin, paclitaxel) Cystoscopy after 1 month no tumor tumor Consolidation: RT + CT cystectomy
22 Combined Radio- and Chemotherapy CR 5y.OS Radiotherapy 57% 47% RT and cisplatin 85% 69% RT and carboplatin 70% 57% Birkenhake et al. Strahlenther Onkol 1998;174:121
23 Combined-modality treatment and organ preservation in invasive bladder cancer Rödel et al. JCO 2002;20: patients with T1 high-risk, T1-4, No-1 Treatment: 1. Transurethral resection 2. RT (n=126), RCT (n=289) RT median 54 Gy, CT cisplatin week 1, 5 3. Restaging-TUR
24 Combined-modality treatment and organ preservation in invasive bladder cancer Rödel et al. JCO 2002;20:3061 Complete remission 72% Local control after CR distant metastasis Disease-specific survival 64% (10 y.) 35% (10 y.) 42% (10 y.) Preservation of bladder >80%
25 Local control Distant metastasis Rödel et al. JCO 2002;20:3061
26 Table 1. Trials of Combined Modality Treatment and Selective Organ Preservation Study/Author ( Reference) Combined Therapy Used No. of Patients 5-Year Overall Survival (%) 5-Year Survival with Bladder Preservation (%) Erlangen-German y/rodel et al. [27] TURBT, EBRT ± chemo (Cisplatin, carboplatin,or cisplatin and 5-FU) 415 (RCT: cisplatin, 82; carboplatin, 61; 5FU/cisplatin, 87) MGH Shipley 2003 [28] TURBT, ± MCV, EBRT + cisplatin RTOG 8903/Shipley et al. [29] TURBT, ± MCV, EBRT + cisplatin Univ. Paris/Housset et al. [30] TURBT, 5-FU, EBRT + cisp latin NA EBRT, external beam radiotherapy; 5-FU, 5-fluorouracil; MCV, methotrexate, Cisplatin, Vinblastine; MGH, Massachusetts General Hospital; RTOG, Radiation Therapy Oncology Group; TURBT, transurethral resection of bladder tumor.
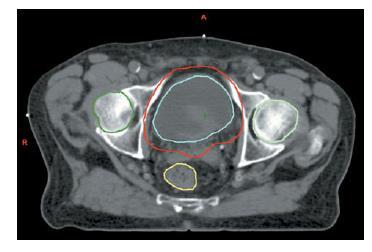
27 How is Radiotherapy delivered? Radiotherapy can be either External Beam or Brachytherapy. For external beam radiotherapy, initial treatment volume includes the whole bladder, proximal urethra, and, in male patients, the prostate with the prostatic urethra and the regional lymphatics. The regional lymphatics adjacent to the bladder include hypogastric, external iliac, and obturator lymph nodes. Boost volume usually includes the bladder or part of bladder with a 2-cm margin.
28 Anatomic extent of the radiation portals: The anterior posterior fields extend laterally about 1.5 cm to the bony pelvis at its widest section with inferior corners shielded to protect the femoral heads. The lateral fields extend anteriorly to about 1.5 to 2 cm from the most anterior aspect of the bladder as seen CT. The posterior border lies about 2.5 cm posterior to the most posterior aspect of the bladder and falls within the rectum. Inferiorly, the tissue above the symphysis and the anal canal is shielded. The inferior border is placed below the middle of the obturator foramen. The superior border is usually at the L5-S1 disc space
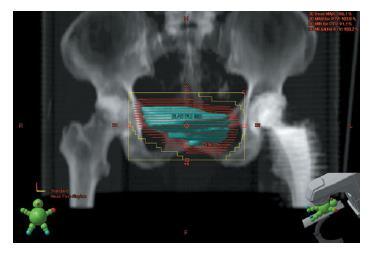
29 A four-field box technique is used most frequently as it provides a relatively homogeneous dose distribution over the treated volume, while keeping the radiation dose outside this volume to about 50% of the intended tumor dose. Because much of the bladder is anterior to the coronal midplane, anterior weightage is given, relative to the posterior one. The boost fields include either the whole bladder or only the involved part of the bladder with at least a 2-cm margin. Techniques may include 4 field box, two lateral fields, three or four oblique fields, or rotational arc techniques. Commonly accepted treatment schedule is cgy per day to a total of 45 to 50 Gy to the whole pelvis, followed by a boost to a smaller volume to a combined total dose of 60 to 65 Gy
30 For treatment planning, a CT scan is performed with the patient supine in the treatment position with arms folded across the chest with ankle supports to stabilise the legs and pelvis, and a knee support for comfort. The bladder should be emptied immediately before scanning and treatment, to reduce the volume irradiated and doses to normal tissues. The rectum should be empty to reduce organ motion and interfractional variations. A small volume of oral contrast is given 1 h before the planning CT scan to show the small bowel. The scan is performed with 3 5 mm slices from the lower border of L5 to the inferior border of the ischial tuberosities.
31 The GTV is the primary bladder tumour CTV is the GTV and the whole bladder. In patients with tumours at the bladder base, the proximal urethra and (in men) the prostate and prostatic urethra is included in the CTV PTV is the CTV with a cm margin.
32
33
34 Newer treatment techniques Teletherapy 3D Conformal Radiotherapy Intensity Modulated Radiotherapy (IMRT) Image Guided Radiotherapy (IGRT) Brachytherapy Advanced High Dose Rate systems
35 Due to the mobility of the bladder, strictly conformal radiotherapy of bladder tumors needs to be given with great care to ensure targeting accuracy for every treatment. Advanced localization techniques such as implanted markers and gating technology may make conformal therapy possible. Portal imaging systems are helpful in real-time monitoring of treatment accuracy.
36 IMRT with inverse planning can reduce the dose to normal tissues, and allow the delivery of a synchronous boost needed for partial bladder irradiation and permit dose escalation to the tumour. However, IMRT for this tumour site requires excellent immobilisation, with IGRT to locate and minimise PTV at the time of treatment. It has been shown that without IGRT an isotropic margin of 3 cm is required, but with IGRT this can be reduced to 12 mm. Organs At Risk (OAR) should be outlined including rectum, femoral heads and small bowel. Recommended dose constraints are: rectum V50 60 per cent, V60 50 per cent; femoral heads V50 50 per cent; small bowel V cm3.
37
38 The bladder is mobile and can change shape as well as position during treatment.verification is therefore very important. The current standard is EPI comparing bony anatomy with the AP and lateral DRRs daily for the first 3 5 days, and then once weekly correcting for systematic errors. Verification that allows visualisation of soft tissues at the time of treatment delivery, such as kv cone beam imaging, MV imaging with tomotherapy and MV imaging of gold seed markers cystoscopically implanted into the bladder, significantly improves accuracy of radiotherapy. Arc RT, which modifies treatment plans to account for variations in individual patients, or gated radiotherapy based on delivery of treatment only when the bladder is in the correct position may be useful techniques.

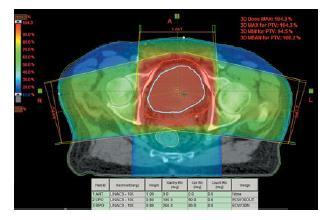
39 DVH for conformal plan for bladder cancer showing PTV, rectum and femoral heads.
40 Brachytherapy Interstitial therapy is not a common part of management of patients with bladder cancer. Brachytherapy for bladder cancer is limited almost exclusively to afterloaded interstitial therapy with iridium-192 ( 192 Ir) sources. A commonly accepted dimension of bladder tumors selected for brachytherapy is <5cm. The tumor usually is treated with a single plane implant of three to five line sources: needles or catheters into which the radioactive sources will be loaded (30 Gy at 58 cgy per hour). The distance between line sources is about 1 cm. A single plane implant can be used to treat a 2- to 2.5-cm thick lesion; beyond that two-plane implants may become necessary.
41 Palliative Radiotherapy 21 Gy in 3 fractions given on alternate days in 1 week or 36 Gy in 6 fractions of 6 Gy given once weekly for 6 weeks. In most cases 21 Gy in 3 fractions on alternate days over 1 week is as effective as longer schedules for palliation as shown by the MRC BA09 trial. A weekly hypofractionated regimen of 6 Gy weekly for 6 fractions has been shown to effectively palliate symptoms in patients unfit for radical treatment and may be preferred by some patients.
42 Treatment delivery and patient care Before radiation starts the patient should be made as fit as possible. Urinary infection should be treated, anaemia should be corrected to haemoglobin 12 g/dl and a low residue diet advised. Radiation cystitis is common; infection should always be excluded and a high fluid intake advised. Catheterisation should be avoided if possible to minimise the risk of infection.
43 Side effects of Radiotherapy Acute complications mainly consist of bladder irritability, resulting from mucositis with decreased bladder capacity, which is manifested by frequency, urge incontinence, dysuria, diarrhea (usually mild) and anal irritation Mild proctitis and lethargy are common. Late side effects include fibrosis and shrinkage of the bladder, haematuria due to bladder telangiectasia, late bowel damage, vaginal dryness and stenosis in women and impotence in men.

44 Thank you
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer
 Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Subject Index. Androgen antiandrogen therapy, see Hormone ablation therapy, prostate cancer synthesis and metabolism 49
 OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Androgen antiandrogen therapy, see Hormone ablation therapy, synthesis and metabolism 49 Bacillus Calmette-Guérin adjunct therapy with transurethral resection
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Androgen antiandrogen therapy, see Hormone ablation therapy, synthesis and metabolism 49 Bacillus Calmette-Guérin adjunct therapy with transurethral resection
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
BLADDER RADIOTHERAPY PLANNING DOCUMENT
 A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
GYNECOLOGIC CANCER and RADIATION THERAPY. Jon Anders M.D. Radiation Oncology
 GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
Radiation Therapy: From Fallacy to Science
 27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
Bladder Preservation Protocols in the Treatment of Muscle-Invasive Bladder Cancer
 Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
Dr. Tareq Salah Ahmed,MD,ESMO. Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate
 Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
DICHIARAZIONE Relatore: Andrea Vavassori
 ! DICHIARAZIONE Relatore: Andrea Vavassori Come da nuova regolamentazione della Commissione Nazionale per la Formazione Continua del Ministero della Salute, è richiesta la trasparenza delle fonti di finanziamento
! DICHIARAZIONE Relatore: Andrea Vavassori Come da nuova regolamentazione della Commissione Nazionale per la Formazione Continua del Ministero della Salute, è richiesta la trasparenza delle fonti di finanziamento
Cochrane metaanalysis 5 year OS Intent to treat
 RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
First, how does radiation work?
 Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Breast cancer Can I still keep my breast?
 Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
Case 1. Receives induction BCG weekly x 6 without significant toxicity Next step should be:
 Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
The Evolution of RT Techniques for Gynaecological Cancers in a developing country context
 The Evolution of RT Techniques for Gynaecological Cancers in a developing country context Hannah Simonds Stellenbosch University/ Tygerberg Academic Hospital ESMO Africa 2017 I have no disclosures External
The Evolution of RT Techniques for Gynaecological Cancers in a developing country context Hannah Simonds Stellenbosch University/ Tygerberg Academic Hospital ESMO Africa 2017 I have no disclosures External
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
September 10, Dear Dr. Clark,
 September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer. Scott Boulet BSc, RT(T)
 for Rectal Cancer. Scott Boulet BSc, RT(T)") Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer Scott Boulet BSc, RT(T) Outline Background Objectives Design Results Discussion Conclusion Acknowledgements Questions Background
Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer Scott Boulet BSc, RT(T) Outline Background Objectives Design Results Discussion Conclusion Acknowledgements Questions Background
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Point-Counterpoint: Radiation & Bladder Cancer
 Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
8/1/2017. Clinical Indications and Applications of Realtime MRI-Guided Radiotherapy
 Clinical Indications and Applications of Realtime MRI-Guided Radiotherapy Michael F Bassetti MD PhD Assistant Professor, Department of Human Oncology University of Wisconsin, Madison. Carbone Cancer Center
Clinical Indications and Applications of Realtime MRI-Guided Radiotherapy Michael F Bassetti MD PhD Assistant Professor, Department of Human Oncology University of Wisconsin, Madison. Carbone Cancer Center
4D Radiotherapy in early ca Lung. Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla
 4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
CBCT of the patient in the treatment position has gained wider applications for setup verification during radiotherapy.
 Gülcihan CÖDEL Introduction The aim of this study is to evaluate the changes in bladder doses during the volumetric modulated arc therapy (VMAT) treatment of prostate cancer patients using weekly cone
Gülcihan CÖDEL Introduction The aim of this study is to evaluate the changes in bladder doses during the volumetric modulated arc therapy (VMAT) treatment of prostate cancer patients using weekly cone
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 6, NUMBER 2, SPRING 2005 Advantages of inflatable multichannel endorectal applicator in the neo-adjuvant treatment of patients with locally advanced
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
20 Prostate Cancer Dan Ash
 20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Organ-sparing treatment of invasive transitional cell bladder carcinoma
 Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
IMRT for Prostate Cancer
 IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
IMRT for Cancer All patients are simulated in the supine position. Reproducibility is achieved using a custom alpha cradle cast that extends from the mid-back to mid-thigh. The feet are positioned in a
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
BRACHYTHERAPY FOR PROSTATE CANCER. Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital
, FRANZCR Radiation Oncologist, The Canberra Hospital") BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
MRI in Cervix and Endometrial Cancer
 28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer
 Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
UCL. Rectum Adenocarcinoma. Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans
 Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer
 Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer") Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Partial Cystectomy for Invasive Bladder Cancer
 European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
Changing Paradigms in Radiotherapy
 Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Outline - MRI - CT - US. - Combinations of imaging modalities for treatment planning
 Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Imaging Outline - MRI - CT - US - Combinations of imaging modalities for treatment planning Imaging Part 1: MRI MRI for cervical cancer high soft tissue contrast multiplanar imaging MRI anatomy: the normal
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Technological Advances in Radiotherapy for the Treatment of Localized Prostate Cancer - A Systematic Review
 Technological Advances in Radiotherapy for the Treatment of Localized Prostate Cancer - A Systematic Review Jayatissa R.M.G.C.S.B. (B.Sc.) Department of Radiography/Radiotherapy, Faculty of Allied Health
Technological Advances in Radiotherapy for the Treatment of Localized Prostate Cancer - A Systematic Review Jayatissa R.M.G.C.S.B. (B.Sc.) Department of Radiography/Radiotherapy, Faculty of Allied Health
Bladder Cancer in Primary Care. Dr Penny Kehagioglou Consultant Clinical Oncologist
 Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy
 Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Nordic Society for Gynecological Oncology Advisory Board of Radiotherapy Guidelines for postoperative irradiation of cervical cancer Contents: 1. Treatment planning for EBRT. 2 2. Target definition for
Radiotherapy What are our options and what is on the horizon. Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology
 Radiotherapy What are our options and what is on the horizon Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology Outline Advances in radiotherapy technique Oligo - disease Advancements
Radiotherapy What are our options and what is on the horizon Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology Outline Advances in radiotherapy technique Oligo - disease Advancements
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases
 Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
The role of Radiation Oncologist: Hi-tech treatments for liver metastases
 The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
La Pianificazione e I Volumi di Trattamento
 TRATTAMENTI INTEGRATI NEL CARCINOMA DELLA VULVA La Pianificazione e I Volumi di Trattamento PAOLO MUTO Direttore UOC Radioterapia ISTITUTO NAZIONALE TUMORI IRCCS Fondazione Pascale di Napoli Minimize collateral
TRATTAMENTI INTEGRATI NEL CARCINOMA DELLA VULVA La Pianificazione e I Volumi di Trattamento PAOLO MUTO Direttore UOC Radioterapia ISTITUTO NAZIONALE TUMORI IRCCS Fondazione Pascale di Napoli Minimize collateral
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology
 Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Principles of radiotherapy and radiochemotherapy. Polgár Cs. 1,2 National Institute of Oncology 1, Chair of Oncology, Semmelweis University 2
 Principles of radiotherapy and radiochemotherapy of malignant tumours Polgár Cs. 1,2 National Institute of Oncology 1, Chair of Oncology, Semmelweis University 2 Multidisciplinary treatment of malignant
Principles of radiotherapy and radiochemotherapy of malignant tumours Polgár Cs. 1,2 National Institute of Oncology 1, Chair of Oncology, Semmelweis University 2 Multidisciplinary treatment of malignant
Chemo-radiotherapy in muscle invasive bladder cancer. Dr Paula Wells St Bartholomew s Hospital London
 Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
Chemotherapy and Bladder Cancer. Blayne Welk UBC Urology Grand Rounds June 4, 2008
 Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
University of Kentucky. Markey Cancer Center
 University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
University of Kentucky Markey Cancer Center Invasive Cancer of the Vagina and Urethra Fred Ueland, MD No matter what you accomplish in your life, the size of your funeral will still be determined by the
The New ICRU/GEC ESTRO Report in Clinical Practice. Disclosures
 The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
The New ICRU/GEC ESTRO Report in Clinical Practice Christian Kirisits, MSc, PhD; Richard Pötter, MD Medical University of Vienna, Vienna, Austria On behalf of the Committee: B. Erickson, C. Haie Meder,
UPDATE ON RADIOTHERAPY
 1 Miriam Kleiter UPDATE ON RADIOTHERAPY Department for Companion Animals and Horses, Plattform Radiooncology and Nuclear Medicine, University of Veterinary Medicine Vienna Introduction Radiotherapy has
1 Miriam Kleiter UPDATE ON RADIOTHERAPY Department for Companion Animals and Horses, Plattform Radiooncology and Nuclear Medicine, University of Veterinary Medicine Vienna Introduction Radiotherapy has
Introduction to clinical Radiotherapy
 Introduction to clinical Radiotherapy Sarah Brothwood Radiotherapy Practice Educator Rosemere Cancer Centre Sarah.brothwood@lthtr.nhs.uk 01772 522694 Radiotherapy We have been able to see and document
Introduction to clinical Radiotherapy Sarah Brothwood Radiotherapy Practice Educator Rosemere Cancer Centre Sarah.brothwood@lthtr.nhs.uk 01772 522694 Radiotherapy We have been able to see and document
Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do?
 Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
ART for Cervical Cancer: Dosimetry and Technical Aspects
 ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
ART for Cervical Cancer: Dosimetry and Technical Aspects D.A. Jaffray, Ph.D. Radiation Therapy Physics Princess Margaret Cancer Centre/Techna/Ontario Cancer Institute Professor Departments of Radiation
Hypofractionated RT in Cervix Cancer. Anuja Jhingran, MD
 Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer Center Contemporary Experience
 International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer