Case 1. Receives induction BCG weekly x 6 without significant toxicity Next step should be:
|
|
|
- Derek Underwood
- 5 years ago
- Views:
Transcription
1 Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two suspicious flat lesion remote from the primary tumors that are normal by white light Final path TaG3Tis urothelial cancer
2 Case 1 Receives induction BCG weekly x 6 without significant toxicity Next step should be: Follow up cysto and cytology in 6 weeks Bladder biopsies and cytology in 6 weeks



3 Case 1 Patient is taken back to operating room for bladder biopsies 6 weeks after completing BCG What additional imaging should be included in order to accurately stage the response to BCG? BJUI 2010: 105, 789
4 Case 1 Site directed biopsies of prior areas of CIS were negative/bcg related inflammation and cytology was negative. False positives can occur with PDD after BCG. OCT showed normal urothelium Next step is: Surveillance cysto every 3 months Second induction course of BCG Monthly maintenance BCG 3 weeks of BCG at 3 months
5 Case 1 Patient receives 3 weeks of BCG at 3 and 6 months, becomes BCG intolerant and maintains a complete response for 2.5 years. He now presents with significant microhematuria and 2 months of dysuria. Urinalysis is otherwise normal. Cysto shows a 2 cm tumor with papillary and sessile features with some surface necrosis Cytology is positive and voided FISH is abnormal


6 Case 1 Patient has a complete TURBT into muscle and biopsy of prior sites of CIS are positive Path T1G3Tis
7 Case 1 Next step is: BCG weekly for 6 weeks BCG + Interferon MMC Gem/MMC Re-resection with biopsies of prostatic urethra


8 Case 1 Patient has re-resection and prostatic urethra biopsies No residual tumor at previous tumor site but there is CIS of the urethra and prostatic ducts Next step is? TURP to determine extent of CIS and open bladder neck for intravesical therapy P ducts Verumontanum CIS
9 Case 1 Patient would like to avoid cystectomy and his TURP shows residual CIS of the prostatic urethra, ducts and acini Next step should be: Radical cysto prostatectomy BCG weekly for 6 weeks BCG + Interferon MMC Gem/MMC
10 Case 1 Patient decides on cystectomy Final pathology: 2 focal areas of CIS of the bladder Diffuse CIS of the prostatic ducts and acini with possible focus of stromal invasions
11 Case 2 62 yo female with T2aTis urothelial cancer with squamous differentiation involving bladder neck and proximal urethra. Fullness at bladder neck but no palpable dimensional mass. She is sexually active and desires to continue. egfr is 50 and she takes Cytoxan for chronic rheumatoid arthritis.
12 Case 2 Treatment should be: Neoadjuvant cisplatin based chemotherapy Neoadjuvant carboplatin based chemotherapy Radical cystectomy Radiation therapy with radiosensitizing chemotherapy Integrated trimodal therapy with cisplatin based chemotherapy and radiotherapy
13 Case 2 She elects to go ahead with cystectomy. What are technical considerations with muscle invasive cancer of bladder neck and urethra? Vaginal reconstruction? Diversion type? Radical cystectomy with en bloc inferior pubectomy, bilateral pelvic lymphadenectomy including pre-sacral nodes, Indiana pouch and anterior vaginal wall reconstruction with rectus flap
14 Case 2 The final path was pt4ag2tisn0 with squamous differentiation. The tumor was involving the anterior vaginal wall, bladder neck and urethra with negative margins. What is her risk of occult metastatic disease and progression? Should she get adjuvant chemothrapy? Pre-op egfr 50 and no change after surgery
15 Case 2 She was felt to be at high risk for progression based on pt4a stage and was treated with adjuvant chemotherapy with 4 cycles of carboplatin and paclitaxel. She has been continuously free of disease since the surgery for 13 years.
16 Case 3 - Localized Bladder Cancer 62 y/o healthy male First occurrence ct2 high grade urothelial Single 4 cm tumor, left posterior wall Complete TUR (R0) according to local urologist no mass on EUA no hydronephrosis no adenopathy egfr 74 ml/min (MDRD)


17 Case 3 ct2nxmx Localized Bladder Cancer


18 Invasion of muscularis propria TCC with squamous cell features
19 Case 3 T2 High Grade Mixed Histology What is the appropriate management of this case? 1) Radical TURBT alone 2) Initial cystectomy ± adjuvant chemotherapy 3) Neoadjuvant chemotherapy + cystectomy 4) Bladder sparing chemo/radiation therapy
20 Case 3 Why Neoadjuvant Chemotherapy? Can we risk stratify when deciding between upfront definitive treatment vs. neoadjuvant chemotherapy? What chemotherapy regimen? Number of cycles? Does mixed histology affect response to neoadjuvant chemotherapy Neoadjuvant vs. adjuvant chemotherapy Why does it matter as long as we give it?
21 NCCN Guidelines (2010) First Line Chemotherapy Neoadjuvant for T2-4aN0 category 1 recommendation Level 1 evidence; uniform consensus MVAC is the historical standard of care GC de facto standard of care based on treatment of measurable metastatic disease
22 NCCN Guidelines (2010) First Line Chemotherapy 3 drug regimens (GC + taxane) not superior to GC alone Carboplatin should not be substituted for cisplatin in patients with normal renal function Split does cisplatin may be considered for patients with borderline renal function or minimal dysfunction
23 Neoadjuvant Selection Criteria Higher risk of relapse: 3-D mass on EUA Prostatic stroma, vaginal wall involvement LVI increased risk of occult nodal involvement Hydronephrosis Increased risk of extra-organ extension thin ureteral wall Upper tract tumor Ureteral or renal pelvis (requires G3 TCC or measurable mass on CT) Micropapillary tumor Small cell tumor (on small cell chemotherapy) Use of these criteria: 80% likelihood of upstaging to >=pt3b or N+ with initial surgery (Millikan et al. JCO 2001) MDACC criteria
24 Case 3 Why not Bladder Preservation Is patient a candidate for bladder preservation? What strategy?
25 Case 3 Definitive Loco-Regional Treatment 1) Radical cystectomy and standard pelvic lymphadenectomy 2) Radical cystectomy and extended pelvic lymphadenectomy 3) Laparascopic/Robotic assisted radical cystectomy and standard pelvic lymphadenectomy 4) Laparascopic/Robotic assisted radical cystectomy and extended pelvic lymphadenectomy 5) Bladder preservation with trimodal therapy Complete TURBT, integrated chemoradiation?
26 Case 3 Treatment and Outcome Neoadjuvant chemotherapy - gemcitabine and cisplatin x4 cycles Open radical cystectomy, BPLND - pt0 bladder specimen - 32 negative nodes Ileal neobladder Incidental adenocarcinoma prostate -pt1c, G6
, COPD (smoking), NIDDM ct3, TCC, mild left hydro")

27 Case 4 Locally advanced bladder cancer in unfit patient 84 y/o frail female Obese, HTN, CAD (stents x2), COPD (smoking), NIDDM ct3, TCC, mild left hydro No pelvic mass, mobile bladder Visibly complete TUR, deep fat invasion No adenopathy, or mets Severe LUTS, hematuria with clots, incontinence egfr 45 ml/min (MDRD)
28 Case 4 Questions? What is appropriate treatment for this lady? Is she a candidate for cystectomy? Can she receive chemotherapy? If yes, which regimen? If no, why not? Is chemoradiation an option for cure or palliation? How are unfit patients defined for curative therapy of advanced bladder cancer?
29 Case 4 Questions? What statement best reflects your view regarding her candidacy for cystectomy? 1) Her age and body habitus rule out surgery. 2) Her cardiopulmonary status (stents x2, COPD) and performance status rule out surgery. 3) She remains a surgical candidate and given her extent of disease and bladder function, I recommend surgery. 4) I don t know how to define unfit for surgery.
30 Who is Too Sick for Surgery Anyone can undergo surgery if the alternative is dying from their cancer. Poor surgical Candidates: Home oxygen Ejection fraction < 25% PS 2 or greater.
31 Cardiac Stents Bare metal Dual anti-platelet therapy for 90 days Drug eluting Dual anti-platelet therapy for 365 days. If therapy is stopped in these time periods 10 fold increase in major cardiac event Both require low-dose ASA for life, even during surgery.
32 Cystectomy alone: ~ 33% 3 yrs Grossman et al. NEJM 2003
33 Fig 2. Overall survival of all 140 registered patients by assigned therapy Millikan, R. et al. J Clin Oncol; 19: Copyright American Society of Clinical Oncology

34 Long-term MGH Experience Efstathiou et al ASTRO 2009; ASCO GU 2010

35 Bladder sparing trimodality therapy 74% 67% 63% 53% 49% 49% Efstathiou et al ASTRO 2009; ASCO GU 2010
36 Case 4 What is appropriate management for this patient? 1) Radical TURBT alone 2) Radical cystectomy ± chemotherapy 3) Trimodality therapy with TUR followed by radiation therapy and concurrent radiosensitizing chemotherapy 4) TUR followed by chemotherapy alone 5) TUR followed by radiation therapy alone
37 Case 4 Treatment and Outcome Radical cystectomy, BPLND - pt3 bladder (negative margins) - 16 negative lymph nodes No complications (hospital stay, 8 days) egfr 49 ml/min (MDRD) Significant palliation - no pelvic symptoms

38 Bladder Cancer Case 5 52 yo WM No prior history of urothelial cancer Hematuria Intravenous pyelogram Filling defect bladder Mild right hydronephrosis

39 Operative Findings Cystoscopy, bimanual exam under anesthesia and transurethral resection of bladder tumor Pathology T1G3Tis minor component Small Cell Small cell carcinoma involving 80-90% of tumor LVI Metastatic work up negative Chromogranin A normal
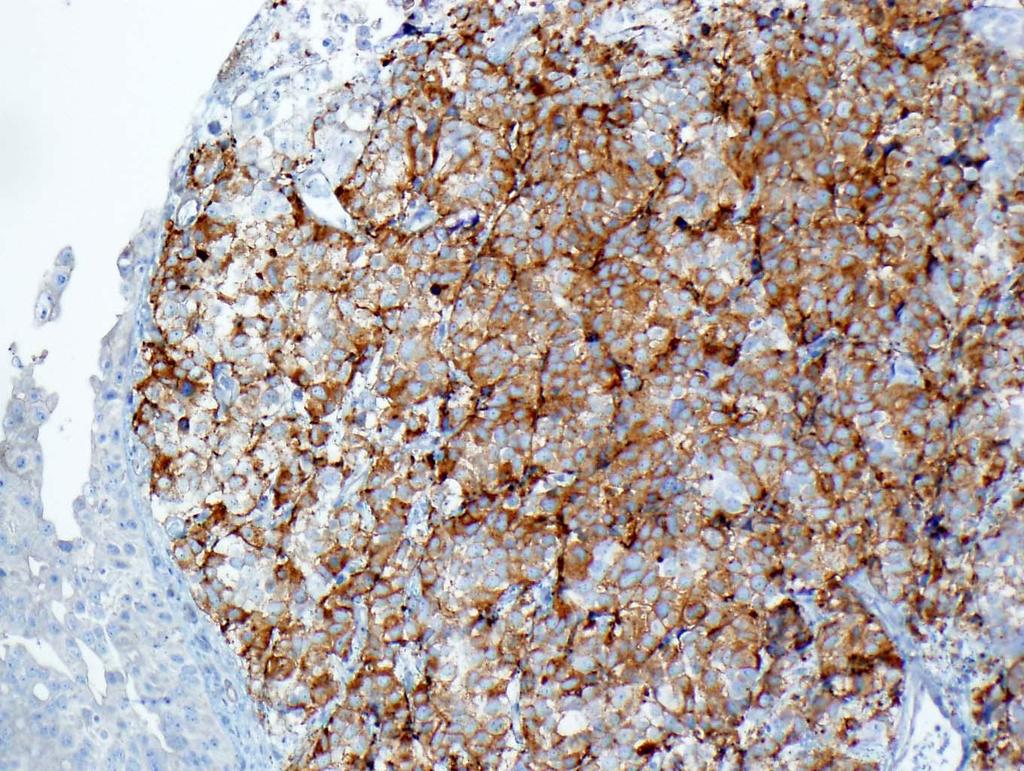
40 Synaptophysin
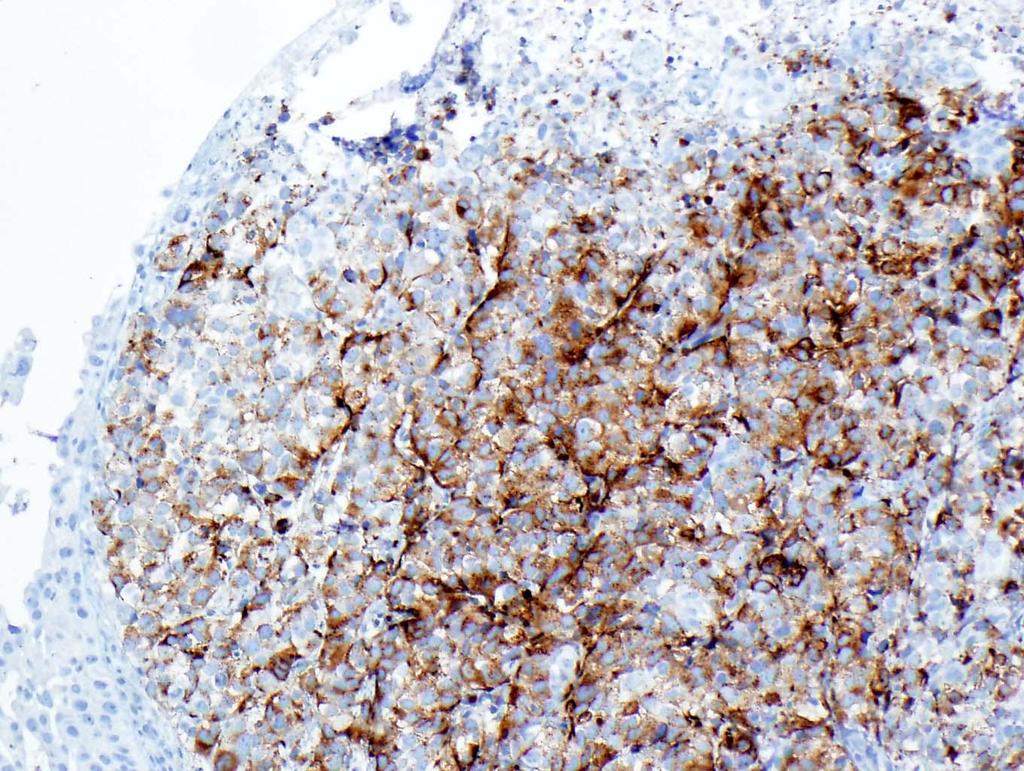
41 Chromogranin
42 What is the next step in management? T1G3Tis mixed TCC and predominant small cell carcinoma with LVI 1) Intravesical immunotherapy with BCG 2) Radical cystectomy and bilateral pelvic and iliac lymphadenectomy 3) Systemic chemotherapy 4) Radiation therapy with concurrent chemotherapy
43 Neoadjuvant chemotherapy recommended. What is the regimen of choice in patients with normal renal function? 1) M-VAC 2) GC 3) Ifosfamide and doxorubicin 4) Etoposide and cisplatin 5) Etoposide and carboplatin
44 Response to chemotherapy Re-staged Cystoscopy Small lesion consistent with scar Cytology and FISH negative Re-resection bladder biopsies negative Chest x-ray and CT abdomen and pelvis negative
45 The patient has had a complete clinical response to chemotherapy. What is the next step in management? 1) Close surveillance 2) Cystectomy and pelvic lymphadenectomy 3) Radiation therapy with concurrent chemotherapy
46 Post Chemotherapy Management Cystectomy with extended pelvic and iliac node dissection (IMA); Neobladder Pathology pt0n0m0 38 nodes all negative Management Adjunctive therapy? Surveillance Status Alive NED 6.5 years months post cystectomy


47 Case 6-57 year old male with microhematuria History of radical prostatectomy in 3 years prior to presentation pt3an0 Gleason Current PSA <.003 Cystoscopy shows 2 foci of papillary tumor right posterior wall Total diameter 2cm
 Muscularis propria in specimen CT Abdomen and pelvis")
48 Initial Surgery and Staging Compete TURBT T1aG3 micropapillary without CIS (100%) Muscularis propria in specimen CT Abdomen and pelvis negative
49 Does this patient need re-resection before deciding on therapy? 1) Yes 2) No
50 What is the next step in management? 1) BCG 2) BCG + Interferon 3) Neoadjuvant chemotherapy 4) Radical Cystectomy and bilateral pelvic and iliac lymphadenectomy 5) Radiation therapy with chemotherapy (bladder preservation)
51 Case 6 - Follow-up BCG 6 week induction course Follow-up cystoscopy shows a 1cm papillary tumor adjacent to previous resection site TURBT T1aG3 micropapillary
52 What is the next step in management? 1) Second induction course of BCG 2) BCG plus interferon 3) Intravesical Mitomycin C 4) Experimental Salvage Protocol - Gemcitabine, Eoquin, Abraxane, other? 5) Radical cystectomy and bilateral pelvic and iliac lymphadenectomy
53 Treatment and Follow up Radical cystectomy and bilateral iliac and pelvic lymphadenectomy pt0n0m0 0/31 nodes Follow-up Alive, NED 7 years post-op
Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016
 BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
Panel: A Case-based Approach to the Management of Bladder Cancer
 Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Neoplasms of the Prostate and Bladder
 Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
AUA Guidelines for Invasive Bladder Cancer: What s New?
 AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
Urinary Bladder Cancer
 Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer
 Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer
 Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Management of High-Risk Non-Muscle Invasive Bladder Cancer. Seth P. Lerner, MD, FACS
 Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
September 10, Dear Dr. Clark,
 September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
Point-Counterpoint: Radiation & Bladder Cancer
 Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Partial Cystectomy for Invasive Bladder Cancer
 European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
Bladder Cancer in Primary Care. Dr Penny Kehagioglou Consultant Clinical Oncologist
 Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer
 Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Chemotherapy and Bladder Cancer. Blayne Welk UBC Urology Grand Rounds June 4, 2008
 Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Disclosures. The Importance of Pathology? Pathologic, Morphologic and Clinical Features. Pathologic Reproducibility
 The Importance of Pathology? Seth P. Lerner, MD, FACS Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine Support for research Disclosures Photocure, Imalux,
The Importance of Pathology? Seth P. Lerner, MD, FACS Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine Support for research Disclosures Photocure, Imalux,
UROTHELIAL CELL CANCER
 UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
Invasive Bladder Transitional Cell Carcinoma OBJECTIVES
 Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER
 RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline
 Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
NMIBC. Piotr Jarzemski. Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland
 NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience. Paul Gellhaus Assistant Clinical Professor
 Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D.
 Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Bladder Cancer. Clinical Case Conference
 Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Cochrane metaanalysis 5 year OS Intent to treat
 RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer Center Contemporary Experience
 International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D.
 Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Part II: Treatment. A Woman-to-Woman Talk with Dr. Armine Smith. Wednesday, March 8, Presented by
 Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and
Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
PREVENTION & SCREENING
 A) PUBLIC HEALTH EPIDEMIOLOGY Incidence: 16 per 100,000 (males 26 per 100,000, females 7 per 100,000). Accounts for 6.1% of all new male cancer cases and 2.1% of all new female cancer cases in Canada.
A) PUBLIC HEALTH EPIDEMIOLOGY Incidence: 16 per 100,000 (males 26 per 100,000, females 7 per 100,000). Accounts for 6.1% of all new male cancer cases and 2.1% of all new female cancer cases in Canada.
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Case 1 SURGICAL PATHOLOGY REPORT. Procedure: Cystoscopy, transurethral resection of bladder tumor (TURBT)
") Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
UNDERSTANDING BLADDER CANCER
 UNDERSTANDING BLADDER CANCER Learn About Your Treatment Options After Your Diagnosis If your doctor has told you that you have bladder cancer, you likely have many questions and concerns. Learning about
UNDERSTANDING BLADDER CANCER Learn About Your Treatment Options After Your Diagnosis If your doctor has told you that you have bladder cancer, you likely have many questions and concerns. Learning about
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
Bladder Case # 1. Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia.
 DISCHARGE SUMMARY Bladder Case # 1 Date: 04/22/2010 Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia. Hospital Course: Mr.
DISCHARGE SUMMARY Bladder Case # 1 Date: 04/22/2010 Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia. Hospital Course: Mr.
10/23/2012 CASE STUDIES: RENAL AND UROLOGIC IMPAIRMENTS. 1) Are there any clues from this history that suggest a particular diagnosis?
 Are there any clues from this history that suggest a particular diagnosis?") Case # 1 An underwriter enters your office, hands you a sheet of paper, and asks What do you think? Can we make an offer? You look at the paper and see it s lab results on a 60 year male looking for $500,000
Case # 1 An underwriter enters your office, hands you a sheet of paper, and asks What do you think? Can we make an offer? You look at the paper and see it s lab results on a 60 year male looking for $500,000
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Open clinical uro-oncology trials in Canada
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Koji Ichihara Hiroshi Kitamura Naoya Masumori Fumimasa Fukuta Taiji Tsukamoto
 Int J Clin Oncol (2013) 18:75 80 DOI 10.1007/s10147-011-0346-8 ORIGINAL ARTICLE Transurethral prostate biopsy before radical cystectomy remains clinically relevant for decision-making on urethrectomy in
Int J Clin Oncol (2013) 18:75 80 DOI 10.1007/s10147-011-0346-8 ORIGINAL ARTICLE Transurethral prostate biopsy before radical cystectomy remains clinically relevant for decision-making on urethrectomy in
EAU MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 EAU MUSLE-INVASIVE AND METASTATI LADDER ANER (Limited text update March 2016) J.A. Witjes (hair), E. ompérat, N.. owan, M. De Santis, G. Gakis, N. James, T. Lebret, A.G. van der Heijden, M.J. Ribal Guidelines
EAU MUSLE-INVASIVE AND METASTATI LADDER ANER (Limited text update March 2016) J.A. Witjes (hair), E. ompérat, N.. owan, M. De Santis, G. Gakis, N. James, T. Lebret, A.G. van der Heijden, M.J. Ribal Guidelines
URETHRAL CANCER EPIDEMIOLOGY - 1
 URETHRAL CANCER Diagnosis & Management Case Conferences Jennie Mickelson Grand Rounds November 15, 2006 EPIDEMIOLOGY - 1 RARE 2200 reported cases F:M - 4:1 1 FEMALE URETHRAL CA any age but >60 most common
URETHRAL CANCER Diagnosis & Management Case Conferences Jennie Mickelson Grand Rounds November 15, 2006 EPIDEMIOLOGY - 1 RARE 2200 reported cases F:M - 4:1 1 FEMALE URETHRAL CA any age but >60 most common
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Bladder Cancer Basics For the Newly Diagnosed
 Bladder Cancer Basics For the Newly Diagnosed Bladder Cancer Advocacy Network The information in this patient guide is not intended to take the place of medical care or the advice of your doctor. Please
Bladder Cancer Basics For the Newly Diagnosed Bladder Cancer Advocacy Network The information in this patient guide is not intended to take the place of medical care or the advice of your doctor. Please
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Issues in the Management of High Risk Superficial Bladder Cancer
 Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
Pathology Driving Decisions
 Pathology Driving Decisions Part I: Understanding Your Diagnosis and Your Treatment Options May 7, 2018 Presented by: Dr. Matthew Mossanen completed his college and medical school training at UCLA. He
Pathology Driving Decisions Part I: Understanding Your Diagnosis and Your Treatment Options May 7, 2018 Presented by: Dr. Matthew Mossanen completed his college and medical school training at UCLA. He
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Q&A. Overview. Collecting Cancer Data: Prostate. Collecting Cancer Data: Prostate 5/5/2011. NAACCR Webinar Series 1
 Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
 A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
Open Radical Cystectomy Tips and Tricks in Males and Females
 Open Radical Cystectomy Tips and Tricks in Males and Females Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine
Open Radical Cystectomy Tips and Tricks in Males and Females Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine
Neodjuvant chemotherapy
 Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Hey Doc, there s blood in my urine Evaluation of hematuria. Christian S. Kuhr, MD FACS May 4, 2018
 Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
Chapter 8 Adenocarcinoma
 Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Case by Case: Critical Issues in Superficial Bladder Cancer Management 5/24/05 13:46 1
 Case by Case: Critical Issues in Superficial Bladder Cancer Management 5/24/05 13:46 1 Case Study 1 A 22-year-old man with a history of gross total painless hematuria: two times in two months, both after
Case by Case: Critical Issues in Superficial Bladder Cancer Management 5/24/05 13:46 1 Case Study 1 A 22-year-old man with a history of gross total painless hematuria: two times in two months, both after
MEDitorial March Bladder Cancer
 MEDitorial March 2010 Bladder Cancer Last month, my article addressed the issue of blood in the urine ( hematuria ). A concerning cause of hematuria is bladder cancer, a variably malignant tumor starting
MEDitorial March 2010 Bladder Cancer Last month, my article addressed the issue of blood in the urine ( hematuria ). A concerning cause of hematuria is bladder cancer, a variably malignant tumor starting
Dr. Tareq Salah Ahmed,MD,ESMO. Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate
 Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
Bladder replacement in men and women: when and when not? Outline. Continent Diversion History
 1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Non Muscle Invasive Bladder Cancer. Primary and Recurrent TCC 4/10/2010. Two major consequences: Strategies: High-Risk NMI TCC
 Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
EAU GUIDELINES ON NON-MUSCLE INVASIVE (TaT1, CIS) BLADDER CANCER
 BLADDER CANCER") EU GUIDELINES ON NON-MUSLE INVSIVE (TaT1, IS) LDDER NER (Limited text update March 2017) M. abjuk (hair), M. urger (Vice-hair), E. ompérat, P. Gontero,.H. Mostafid, J. Palou,.W.G. van Rhijn, M. Rouprêt,
EU GUIDELINES ON NON-MUSLE INVSIVE (TaT1, IS) LDDER NER (Limited text update March 2017) M. abjuk (hair), M. urger (Vice-hair), E. ompérat, P. Gontero,.H. Mostafid, J. Palou,.W.G. van Rhijn, M. Rouprêt,
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015
 Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
BACKGROUND. Many patients with invasive urothelial cell cancer are poor candidates
 2181 Treatment Options for Muscle-invasive Urothelial Cancer for Patients Who Were Not Eligible for Cystectomy or Neoadjuvant Chemotherapy With Methotrexate, Vinblastine, Doxorubicin, and Cisplatin Report
2181 Treatment Options for Muscle-invasive Urothelial Cancer for Patients Who Were Not Eligible for Cystectomy or Neoadjuvant Chemotherapy With Methotrexate, Vinblastine, Doxorubicin, and Cisplatin Report
Subject Index. Androgen antiandrogen therapy, see Hormone ablation therapy, prostate cancer synthesis and metabolism 49
 OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Androgen antiandrogen therapy, see Hormone ablation therapy, synthesis and metabolism 49 Bacillus Calmette-Guérin adjunct therapy with transurethral resection
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Androgen antiandrogen therapy, see Hormone ablation therapy, synthesis and metabolism 49 Bacillus Calmette-Guérin adjunct therapy with transurethral resection
Reviewing Immunotherapy for Bladder Carcinoma In Situ
 Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
BLADDER CANCER CONTENT CREATED BY. Learn more at
 BLADDER CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK TO YOUR DOCTOR Table of Contents WHAT IS BLADDER CANCER? 4 TYPES OF BLADDER CANCER 5 GRADING AND STAGING 8 TREATMENT OVERVIEW
BLADDER CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK TO YOUR DOCTOR Table of Contents WHAT IS BLADDER CANCER? 4 TYPES OF BLADDER CANCER 5 GRADING AND STAGING 8 TREATMENT OVERVIEW
Controversies in the management of Non-muscle invasive bladder cancer
 Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation *
 ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
Urology An introduction to cut up DR J R GOEPEL
 Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient
Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient