Cancer Associated Thrombosis Review and Update. Family Practice Oncology CME Day November 21 st 2015 Erica Peterson
|
|
|
- Francine Pearson
- 6 years ago
- Views:
Transcription
1 Cancer Associated Thrombosis Review and Update Family Practice Oncology CME Day November 21 st 2015 Erica Peterson
2 Disclosures No conflicts of interest to declare
3 Objectives To review evidence in cancer-associated VTE Epidemiology VTE risk factors/risk stratification Primary prophylaxis Treatment of cancer-associated VTE VTE and thrombocytopenia VTE and bleeding Incidental VTE
4 Case 1: Ms. P.E. 65 year old female PMHx hypertension, hypothyroidism and obesity Recently diagnosed with unresectable locally advanced pancreatic cancer ECOG 2 Plan to place port-a-cath and start multi-agent chemotherapy What is this patient s risk of VTE? Is the risk high enough to need primary prophylaxis?
5 Cancer-Associated VTE (CAT) ~20% of all VTE cases are associated with cancer VTE is associated with higher mortality 2nd leading cause of death in cancer patients Significant burden on the health care community Increased hospitalization Health care costs and resource utilization Can cause treatment discontinuation/delays Heit Arch Intern Med Heit Arch Intern Med Sorensen NEJM Pradoni N Engl J Med Sorensen N Engl J Med Chew Arch Intern Med Khorana J Thromb Haemost 2007.
6 Pathogenesis of CAT Multifactorial etiology Venous stasis Endothelial Dysfunction Hypercoagulability
7 Pathogenesis of CAT Multifactorial etiology Venous stasis Endothelial Dysfunction Hypercoagulability Genetic mutations in cancer cells Cytokines Adhesion molecules Tissue factor microparticles
8 Risk Factors for VTE in Cancer Divided into 3 main categories Patient-related risk factors Treatment-related risk factors Cancer-related risk factors Overall risk is not static and varies over time Acquisition of new risk factors Disease progression Initiation of new therapies
9 Risk Factors for VTE in Cancer Patient-related Older age Race Prior VTE Platelet count Obesity Comorbid conditions Cancer-related Primary site Histology Stage Grade Time interval since diagnosis Treatment-related Surgery Chemotherapy Hormonal therapy Anti-angiogenic agents ESA Hospitalization Catheters Lyman J Clin Oncol Heit Arch Intern Med Blom JAMA 2005.
10 Tumour Type and VTE Risk RR of VTE ranges from 1.02 to 4.34 Stein P.D. et al Am J Med
11 CAT is Increasing Over Time Stein P.D. et al Am J Med
12 Risk of VTE with Age Annual incidence of VTE varies with age Overall 1/1000 < 30 y 1/10,000 ~ 80 y 1/100 After age 50 Risk doubles with each decade Men have higher risk than women Silverstein M.D. Arch Intern Med 1998
13 Who Are At Risk for CAT? Highest VTE risk in: Older patients Pancreatic, brain, upper GI tumours and lymphoma Metastatic disease First 3 months after cancer diagnosis First month after surgery Systemic chemotherapy (especially cisplatin, anthracyclines, thal/lenalidomide, bevacizumab) How do we identify individual patient risk?
14 Risk Stratification in CAT Khorana risk model 5-independent risk factors identified Patient Characteristic Score Site of cancer Very high risk (stomach, pancreas) High risk (lung, lymphoma, gyne and GU) 2 1 Pre-chemo platelet count Hemoglobin < 100 or use of ESA 1 Pre-chemo WBC > 11 1 BMI 35 1 Low risk =0 Moderate Risk=1-2 High Risk 3 Khorana A. et al Blood 2008
15 Risk Stratification in CAT Khorana risk model 5-independent risk factors identified Patient Characteristic Score Site of cancer Very high risk (stomach, pancreas) High risk (lung, lymphoma, gyne and GU) 2 1 Pre-chemo platelet count Hemoglobin < 100 or use of ESA 1 Pre-chemo WBC > 11 1 BMI 35 1 Low risk 0.3% Moderate Risk 2.0% High Risk 6.7% Khorana A. et al Blood 2008
16 Risk Stratification in CAT Khorana risk model 5-independent risk factors identified Patient Characteristic Score Site of cancer Very high risk (stomach, pancreas) High risk (lung, lymphoma, gyne and GU) 2 1 Pre-chemo platelet count Hemoglobin < 100 or use of ESA 1 Pre-chemo WBC > 11 1 BMI 35 1 For Ms. P.E Score=3/6 HIGH RISK Khorana A. et al Blood 2008
17 Who Should Get Primary Prophylaxis ASCO 2013 Guideline Routine primary prophylaxis not indicated in outpatients LMWH should be considered case-by-case basis in highly selected outpatients with solid tumours receiving chemo ASA or LMWH should be given to those with myeloma receiving thalidomide or lenalidomide regimens with chemo/dex Educate patient regarding signs and symptoms of VTE, particularly in high risk patients

18 Case 1: Ms. P.E. Returns to clinic for assessment prior to cycle 2 Complains of a 1 week history of worsening calf pain and swelling Worsening SOB on exertion On exam left leg, swollen, tender to palpation and erythematous US confirms a left leg DVT What do you do now?
19 Treatment of CAT All major consensus guidelines recommend LMWH monotherapy as the preferred treatment for CAT Recommendations based on results of 3 open-label RCTs CANTHANOX study: enoxaparin vs. warfarin CLOT study: dalteparin vs. warfarin/acenocoumarol LITE study: tinzaparin vs. warfarin Kearon et al Chest ACCP 9 th edition NCCN Lyman et al J Clin Oncol ESMO 2011.
20 Risk of Recurrent VTE with LMWH Recurrent VTE Cochrane Review Outcome HR (95% CI) Recurrent VTE 0.47 ( ) Major bleeding 1.07 ( ) Survival 0.96 ( ) Dalteparin 200 u/kg x 1 mo then 150 u/kg x 5 mo Tinzaparin 175 u/kg (3 mo LITE; 6 mo CATCH) Enoxaparin 1.5 mg/kg x 3 mo Warfarin to target INR 2.0 to 3.0 Lee A.Y.Y. et al NEJM 2003; Hull R.D. et al Am J Med 2006; Meyer G. et al Arch Intern Med 2002; Lee A.Y.Y. et al JAMA 2015 Akl E. et al Cochrane Database Syst Rev 2014
21 Risk of Bleeding with LMWH Major Bleeding Cochrane Review Outcome HR (95% CI) Recurrent VTE 0.47 ( ) Major bleeding 1.07 ( ) Survival 0.96 ( ) Dalteparin Tinzaparin Enoxaparin Warfarin to target INR 2.0 to 3.0 Bleeding rates decrease over time 3.6% in the first month 1.1 % for months % for months 7-12 Lee A.Y.Y. et al NEJM 2003; Hull R.D. et al Am J Med 2006; Meyer G. et al Arch Intern Med 2002; Lee A.Y.Y. et al JAMA 2015 Francis C.W. et al J Thromb Haemost 2015
22 Tolerability of LMWH in Cancer Qualitative studies indicate that cancer patients Are usually accepting of daily injections Find LMWH convenient and empowering Prefer efficacy and safety over the route of administration Do not want the anticoagulant to interfere with their cancer treatment Noble S. et al Hematologica 2015; Noble S. et al Palliat Med 2005
23 Case 1: Ms. P.E. 1 month follow-up Significant bruising and subcutaneous hematomas at injection sites Wants to know if it is possible to switch to the new oral pill she saw advertised on CNN Are the new oral anticoagulants a suitable option in cancer patients?
24 Anticoagulant Sites of Action Unfractionated Heparin XII XI IX VIII fondaparinux X VII Direct Factor Xa Inhibitors Rivaroxaban Apixaban Edoxaban Betrixaban Darexaban Low Molecular Weight Heparin V Warfarin II I Fibrin Clot Direct Thrombin (IIa) Inhibitors Bivalirudin Lepirudin Argatroban Dabigatran Courtesy of Dr. J Ansell.
25 DOAC Pharmacology Dabigatran Rivaroxaban Apixaban Warfarin Target Thrombin Factor Xa Factor Xa Vit K dependent factors Action onset 1 2 h 2 4 h 1 3 h 4-5 days Half life h 5-13 h h 40 h Renal clearance 80% 33% 25% 0% Dosing BID OD (BID) BID OD Lab monitoring No No No YES Antidote No No No YES Drug interactions P-gp P-gp/CYP3A4 P-gp/CYP3A4 MANY
26 DOAC Drug Interactions antifungals ritonavir amiodarone verapamil clarithromycin quinidine tamoxifen TKIs cyclosporin tacrolimus Inhibitors Increase Drug Levels Inducers rifampicin phenytoin carbamazepine phenobarbitone dexamethasone doxorubicin vinblastine St. John s wort Decrease Drug Levels
27 DOAC trials for VTE treatment Dabigatran: RE-COVER and RE-COVER II Rivaroxaban: EINSTEIN DVT AND EINSTEIN PE UFH/LMWH Dabigatran 150 mg BID Rivaroxaban 15 mg BID x 21 days then 20 mg OD R R UFH/LMWH + Warfarin Warfarin Enoxaparin + Warfarin Warfarin Apixaban: AMPLIFY Apixaban 10mg BID x 1 week then 5 mg BID R Enoxaparin + Warfarin Warfarin Schulman S. et al N Engl J Med Buller H. et al N Engl J Med Agnelli G. et al N Engl J Med 2013
28 DOAC trials for VTE treatment Dabigatran: RE-COVER and RE-COVER II Rivaroxaban: EINSTEIN DVT AND EINSTEIN PE UFH/LMWH Dabigatran 150 mg BID Rivaroxaban 15 mg BID x 21 days then 20 mg OD R R UFH/LMWH + Warfarin Warfarin Enoxaparin + Warfarin Warfarin 9.5% active cancer 9.2% active cancer Apixaban: AMPLIFY All cancer patients were highly selected Well No bleeding No significant renal/hepatic dysfunction R Apixaban 10mg BID x 1 week then 5 mg BID Enoxaparin + Warfarin Warfarin 5.3% active cancer Schulman S. et al N Engl J Med Buller H. et al N Engl J Med Agnelli G. et al N Engl J Med 2013
29 DOAC trials for VTE treatment TTR 60% TTR 58% TTR 61% DOACs = Warfarin But LMWH>Warfarin in cancer patients Schulman S. et al NEJM Buller H. et al NEJM Agnelli NEJM 2013
30 DOAC Limitations in Cancer Patients Unreliable administration and absorption in patients with n/v, diarrhea and mucosal erosion Higher risk of GI bleed for dabigatran Liver and renal dysfunction is common in cancer Drug interactions may be clinically important Lack of measurement (therapeutic range) and antidote Lack of experience on management for procedures and thrombocytopenia No comparison against long-term LMWH for treatment Paucity of clinical trial data
31 Practical Pearls about LMWH Get over YOUR fear/reluctance of injections Have patient do his/her first injection in clinic Allow alcohol to dry before injection Inject SLOWLY (over 5-10 seconds) Firm pressure for 2 5 min after injection Reduces bruising, hematomas and pain DO NOT RUB Insulin syringe offers greater comfort than prefilled syringes

32 Practical Pearls about LMWH Rotate sites and use love handles Round UP on dose to nearest prefilled syringe Dose based on body weight No capping for weight
33 Case 1: Ms. P.E. 2 months later Patient presents to ER with UGIB Hb 90 Platelets 42 What do you do with her anticoagulation? Does she require an IVC filter?
34 VTE and Bleeding Multiple reasons for bleeding in cancer patients In patients with bleeding who also require anticoagulation, need to consider: Severity and source of bleed (e.g. epistaxis vs ICH) Whether source can be treated or eliminated How long is the bleeding event likely to last Likelihood of recurrence of bleeding event Indication for anticoagulation
35 VTE and Bleeding No evidence-based guidance on management Treat bleeding source whenever possible Active, serious bleeding: Hospitalize and withhold anticoagulation Insert retrievable filter only if risk of recurrent VTE is very high (within first 4 weeks after VTE diagnosis) Start anticoagulation and remove filter when bleeding stops When restarting anticoagulation restart prophylactic doses and uptitrate as tolerated
36 IVC Filters Efficacy and safety remain ill-defined after 40 years of use Long-term data shows no reduction in total VTE or mortality Short and long-term complications are common Thrombosis (6 36%) Filter tilt, fracture, migration or embolization (3 69%) IVC perforation (3 86%) Post-thrombotic syndrome (5 70%) Streiff Blood Decousus et al N Engl J Med PREPIC investigators Circulation Hammond et al Clin Radiol Imberti et al J Thromb Thrombolysis 2012.

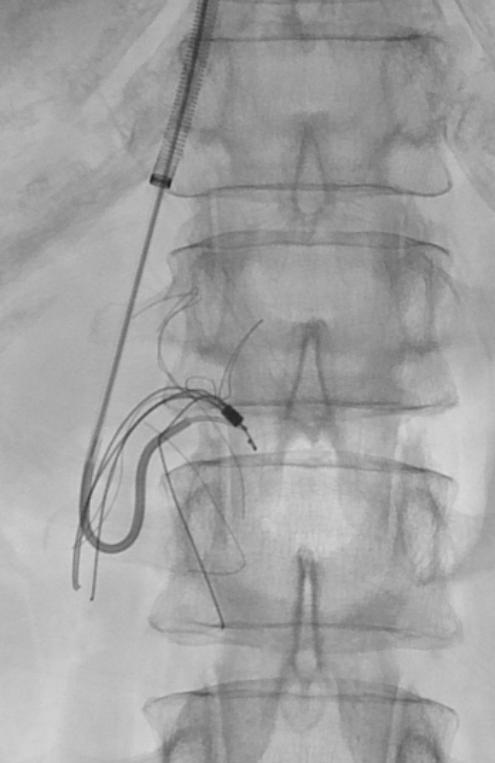
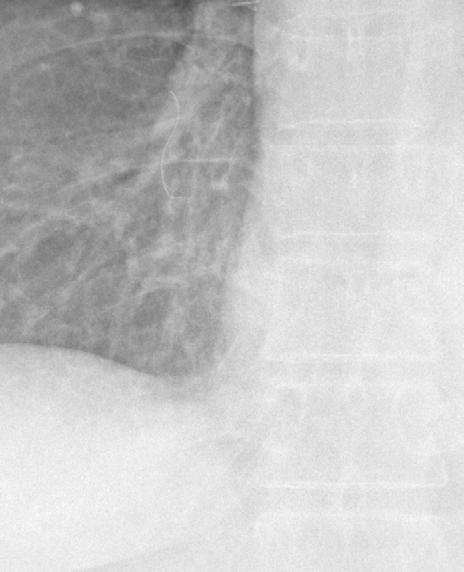
37 IVC Filter Complications
38 VTE and thrombocytopenia If platelet count less than 50x10 9 /L: Transfuse platelets if VTE recent (< 30 days) Reduce dose of LMWH if VTE established (> 30days)

39 VTE and thrombocytopenia VTE within last 4 weeks Lee AY Blood 2013;122:2310

40 VTE and thrombocytopenia VTE >4 weeks Lee AY Blood 2013;122:2310
41 Case 2: Mr. D.v.T. 71 y.o. male with metastatic colon cancer Recent surgery and hospitalization for intestinal obstruction Large saddle embolus seen on CT scan performed for complete cancer staging Clinically and hemodynamically stable Currently asymptomatic according to his oncologist Should we initiate anticoagulation? Does this affect the patient s overall prognosis?
42 Incidental VTE Indirect evidence suggests that incidental and symptomatic VTE share the same risk factors: older age hospitalization previous VTE elevated WBC cancer recent chemotherapy metastatic disease first 3-6 months after cancer diagnosis Gosseline et al Radiology Ritchie at al Thorax Larici et al Radiology Browne et al J Thorac Oncol Cronin et al AJR DiNisio et al Thromb Haemost O Connell et al J Clin Oncol 2006.
43 Incidental VTE Retrospective studies in oncology patients Douma et al: incidental VTE 2.5%, PE/DVT 1.3% and abdominal vein thrombosis 1.1% Cronin et al: incidental VTE 6%, DVT 6.8% and PE 3.3% Prospective studies Shah et al: incidental VTE 2% Observed rates are increasing over time due Improved imaging techniques More scans Cronin C.G. et al AJR 2007; Douma R.A. et al Thromb Res 2007; Shah M.A. et al J Thromb Haemost 2010


44 Incidental VTE Di Nisio M. et al Thromb Haemost 2010
45 Incidental PE: Clinically Significant? Thrombus burden/location of emboli are similar to symptomatic PE When compared to matched controls incidental PE patients were more likely to have: Fatigue (54% vs. 20% p=0.0002) SOB (22% vs. 8% p=0.02) Incidental and symptomatic PE are both associated with increased mortality Patients with incidental PE have similar rates of recurrent VTE, bleeding and mortality compared to those with symptomatic PE O Connell C. L. et al JCO 2006; Palla et al Cancer Investigation 2012; Shinagare et al Cancer 2011.
46 Management Strategy for Incidental PE Incidental PE Segmental or larger PE Subsegmental PE Consider risk for bleeding Positive for PE Review with chest radiologist or do CTPA If uncertain do US of pelvis and legs Anticoagulation if no contraindication Positive for DVT Negative for DVT Consider serial imaging Withhold anticoagulation
47 Incidental VTE in Cancer Prevalence increasing due to improved imaging, greater awareness and likely true rise in incidence Must confirm diagnosis Prognosis appears to be similar to symptomatic VTE in terms of VTE recurrence and mortality Role of anticoagulation is unclear Currently recommended by ACCP guideline (2B) and 2013 ASCO guideline Kearon et al Chest Huisman et al Chest Lyman et al J Clin Oncol 2013.
48 Conclusions CAT is a common, costly and potentially fatal VTE risk assessment and patients education should be done routinely prior to starting chemotherapy Primary prophylaxis is not routinely indicated but should be discussed with patients at high risk Incidental VTE should be treated with standard therapy LMWH is still the treatment of choice but we need to encourage research using DOACs
49 Questions?
My Cancer Patient Has a Clot- Can I prescribe a Direct Oral Anticoagulant (DOAC)?
?") My Cancer Patient Has a Clot- Can I prescribe a Direct Oral Anticoagulant (DOAC)? November 24, 2018 Erica Peterson MD, FRCPC University of British Columbia Disclosures I participate in clinical research
My Cancer Patient Has a Clot- Can I prescribe a Direct Oral Anticoagulant (DOAC)? November 24, 2018 Erica Peterson MD, FRCPC University of British Columbia Disclosures I participate in clinical research
La terapia del TEV nel paziente oncologico nell'era dei DOAC
 XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
Venous Thrombo-Embolism. John de Vos Consultant Haematologist RSCH
 Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Venous Thromboembolism (VTE) in Myeloma. Christine Chen May 2017
 in Myeloma. Christine Chen May 2017") Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Cancer Associated Thrombosis An update.
 Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
New oral anticoagulants and Palliative Care.
 New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
Epidemiology of Thrombosis in Patients with Malignancy. Cancer and Venous Thromboembolism. Chew HK, Arch Int Med, Feb Blom et al, JAMA, Feb 2005
 Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES
 PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES Mario Mandalà, MD Unit of Clinical Research Department of Oncology and Haematology Papa Giovanni XXIII Hospital Cancer Center
PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES Mario Mandalà, MD Unit of Clinical Research Department of Oncology and Haematology Papa Giovanni XXIII Hospital Cancer Center
Update on the Management of Cancer Associated VTE
 Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Frequently Asked Questions about Cancer Associated Thrombosis
 + Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
+ Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
Cancer associated thrombosis. 17 th November 2016 Simon Noble Clinical Professor Palliative Medicine Cardiff University Wales, UK
 Cancer associated thrombosis 17 th November 2016 Simon Noble Clinical Professor Palliative Medicine Cardiff University Wales, UK Today What is VTE? How does CAT differ? Initial anticoagulation Anticoagulation
Cancer associated thrombosis 17 th November 2016 Simon Noble Clinical Professor Palliative Medicine Cardiff University Wales, UK Today What is VTE? How does CAT differ? Initial anticoagulation Anticoagulation
Cancer Associated Thrombosis: six months and beyond. Farzana Haque Hull York Medical School
 Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
Cancer Associated Thrombosis
 Cancer Associated Thrombosis Can we use DOACs? D R. C Y N T H I A W U MD F R C P ( C ) D I V I S I O N O F H E M A T O L O G Y F A M I L Y P H Y S I C I A N S A N D C A N C E R C O N T R O L A P R I L
Cancer Associated Thrombosis Can we use DOACs? D R. C Y N T H I A W U MD F R C P ( C ) D I V I S I O N O F H E M A T O L O G Y F A M I L Y P H Y S I C I A N S A N D C A N C E R C O N T R O L A P R I L
Management of Cancer Associated Thrombosis (CAT) where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth
 where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth") Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
incidence of cancer-associated thrombosis (CAT) is further increased by additional risk factors such as chemotherapeutic 2
 is further increased by additional risk factors such as chemotherapeutic 2") CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
Updates in Management of Venous Thromboembolic Disease
 Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Updates in Management of Venous Thromboembolic Disease November 7 th 2018 UHN Emergency Conference Susan Jenkins RN(EC) NP-Adult Thrombosis and Hemostasis Program University Health Network Disclosures
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1
 CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
Management of Cancer Associated VTE
 Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS
 ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
DOACs in CAT. Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD
 DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
Prophylaxie primaire sur le patient ambulatoire. Marc Carrier
 Prophylaxie primaire sur le patient ambulatoire Marc Carrier Marc Carrier In compliance with COI policy, SSVQ requires the following disclosures to the session audience: Research Support/P.I. Employee
Prophylaxie primaire sur le patient ambulatoire Marc Carrier Marc Carrier In compliance with COI policy, SSVQ requires the following disclosures to the session audience: Research Support/P.I. Employee
Thromboembolism and cancer: New practices. Marc Carrier
 Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
Cancer and Venous Thromboembolism
 125 34 Cancer and Venous Thromboembolism Stephan Moll, MD University of North Carolina Chapel Hill, NC GASCO, Atlanta Sept 8 th, 2017 Disclosures Consultant: Speaker bureau: none Janssen, Boehringer-Ingelheim,
125 34 Cancer and Venous Thromboembolism Stephan Moll, MD University of North Carolina Chapel Hill, NC GASCO, Atlanta Sept 8 th, 2017 Disclosures Consultant: Speaker bureau: none Janssen, Boehringer-Ingelheim,
New Oral Anticoagulant Drugs in the Prevention of DVT
 New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
Cancer and the Heparins
 Cancer and the Heparins Wim P Ceelen, MD, PhD, FACS Department of GI Surgery - UZ Gent Senior Clinical Researcher - FWO Overview Mechanisms of cancer induced thrombosis Guidelines for prevention and treatment
Cancer and the Heparins Wim P Ceelen, MD, PhD, FACS Department of GI Surgery - UZ Gent Senior Clinical Researcher - FWO Overview Mechanisms of cancer induced thrombosis Guidelines for prevention and treatment
Cancer and Thrombosis
 Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer Associated Thrombosis
 Cancer Associated Thrombosis Pantep Angchaisuksiri, MD Professor of Medicine Mahidol University, Thailand Adjunct Associate Professor University of North Carolina, Chapel Hill, USA Piccioli A. J Thromb
Cancer Associated Thrombosis Pantep Angchaisuksiri, MD Professor of Medicine Mahidol University, Thailand Adjunct Associate Professor University of North Carolina, Chapel Hill, USA Piccioli A. J Thromb
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI
 10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI Cleveland Clinic Heart and Vascular Institute Heather L. Gornik, MD has the following relationships to disclose:
10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI Cleveland Clinic Heart and Vascular Institute Heather L. Gornik, MD has the following relationships to disclose:
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Venous Thromboembolic Disease Update
 Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Abstract. Background. Methods
 Abstract Background Malignancy is a major risk factor for developing venous thromboembolism (VTE), and thus cancer patients are at high risk for deep vein thrombosis (DVT) and/or pulmonary embolism (PE).
Abstract Background Malignancy is a major risk factor for developing venous thromboembolism (VTE), and thus cancer patients are at high risk for deep vein thrombosis (DVT) and/or pulmonary embolism (PE).
In the Clinic: Annals Sweta Kakaraparthi 1/23/15
 In the Clinic: Annals Sweta Kakaraparthi 1/23/15 Case Scenerio 56 year old female with breast cancer presents to the clinic for her 3 month followup! She is concerned about blood clots and asks you about
In the Clinic: Annals Sweta Kakaraparthi 1/23/15 Case Scenerio 56 year old female with breast cancer presents to the clinic for her 3 month followup! She is concerned about blood clots and asks you about
Update on thrombosis 13/07/2017. To focus on
 Update on thrombosis Oxford Advanced Course 2017 Simon Noble Clinical Professor Palliative and Supportive Medicine Cardiff University Wales, UK To focus on Changing thrombogenicity of cancer What is the
Update on thrombosis Oxford Advanced Course 2017 Simon Noble Clinical Professor Palliative and Supportive Medicine Cardiff University Wales, UK To focus on Changing thrombogenicity of cancer What is the
A Brief History of the World of Anticoagulation
 A Brief History of the World of Anticoagulation Allison Burnett, PharmD, CACP, PhC Clinical Assistant Professor- UNM College of Rx Antithrombosis Stewardship Pharmacist University of New Mexico Hospital
A Brief History of the World of Anticoagulation Allison Burnett, PharmD, CACP, PhC Clinical Assistant Professor- UNM College of Rx Antithrombosis Stewardship Pharmacist University of New Mexico Hospital
Cancer associated thrombosis
 Cancer associated thrombosis Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University Take home messages 1. Clots are cool
Cancer associated thrombosis Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University Take home messages 1. Clots are cool
New Hope for VTE Burden in Ambulatory Cancer Patients
 New Hope for VTE Burden in Ambulatory Cancer Patients Essam Abo-El-Nazar MS, FRCS Consultant Liver Surgeon King Fahd Hospital Jeddah-KSA Prof. of Surgery Imperial College London-UK My talk today What is
New Hope for VTE Burden in Ambulatory Cancer Patients Essam Abo-El-Nazar MS, FRCS Consultant Liver Surgeon King Fahd Hospital Jeddah-KSA Prof. of Surgery Imperial College London-UK My talk today What is
Is There a Role for Prophylaxis in Cancer Patients During Therapy?
 Victor F. Tapson, MD, FCCP, FRCP Professor of Medicine Director, Center for Pulmonary Vascular Disease Division of Pulmonary and Critical Care Duke University Medical Center Durham, N.C. USA Is There a
Victor F. Tapson, MD, FCCP, FRCP Professor of Medicine Director, Center for Pulmonary Vascular Disease Division of Pulmonary and Critical Care Duke University Medical Center Durham, N.C. USA Is There a
The risk of venous thromboembolism is four to seven times as
 review article Dan L. Longo, M.D., Editor Prophylaxis against Venous Thromboembolism in Ambulatory Patients with Cancer Jean M. Connors, M.D. The risk of venous thromboembolism is four to seven times as
review article Dan L. Longo, M.D., Editor Prophylaxis against Venous Thromboembolism in Ambulatory Patients with Cancer Jean M. Connors, M.D. The risk of venous thromboembolism is four to seven times as
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
THROMBOPROPHYLAXIS IN CANCER PATIENTS
 CANCER ASSOCIATED THROMBOSIS THROMBOPROPHYLAXIS IN CANCER PATIENTS Cancer is an important risk factor for venous thromboembolism (VTE). Research has shown that 4-20% of 1 patients with cancer experience
CANCER ASSOCIATED THROMBOSIS THROMBOPROPHYLAXIS IN CANCER PATIENTS Cancer is an important risk factor for venous thromboembolism (VTE). Research has shown that 4-20% of 1 patients with cancer experience
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015
 Clinical Practice Guideline August 2015") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Top 5 (or so) Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE
 Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE") Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum
 Online Data Supplement Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum Stacey M. Kassutto, C. Jessica Dine, Maryl Kreider, Rupal
Online Data Supplement Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum Stacey M. Kassutto, C. Jessica Dine, Maryl Kreider, Rupal
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
VTE Management in Oncology Patients
 VTE Management in Oncology Patients October 24, 2014 Dr. Rufaro Chitsike MD MMed Haem, FCPath(Haem), Cert Clin(Haem) St. John s, Newfoundland Dr. Mary DeCarolis (Moderator) MD, GPO Housekeeping Sign the
VTE Management in Oncology Patients October 24, 2014 Dr. Rufaro Chitsike MD MMed Haem, FCPath(Haem), Cert Clin(Haem) St. John s, Newfoundland Dr. Mary DeCarolis (Moderator) MD, GPO Housekeeping Sign the
Rapid Fire-Top Articles You Need to Know
 Rapid Fire-Top Articles You Need to Know TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Rapid Fire-Top Articles You Need to Know TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
New Antithrombotic Agents DISCLOSURE
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
Venous Thromboembolism Prophylaxis: Checked!
 Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
Are guidelines for anticoagulation useful in cancer patients?
 Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for
: Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for") The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING
 DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
Choosing and Managing Direct Oral Anticoagulants (DOACs)
") Choosing and Managing Direct Oral Anticoagulants (DOACs) Ana G. Antun, MD, MSc Assistant Professor, Department of Hematology and Medical Oncology Winship Cancer Institute of Emory University 1 Outline
Choosing and Managing Direct Oral Anticoagulants (DOACs) Ana G. Antun, MD, MSc Assistant Professor, Department of Hematology and Medical Oncology Winship Cancer Institute of Emory University 1 Outline
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL
 PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
New antithrombotic agents in the treatment of VTE; a subgroup analysis of the Phase III randomized clinical trials.
 Interactions cellulaires tumorales et leur environnement et réponses aux agents anticancéreux. New antithrombotic agents in the treatment of VTE; a subgroup analysis of the Phase III randomized clinical
Interactions cellulaires tumorales et leur environnement et réponses aux agents anticancéreux. New antithrombotic agents in the treatment of VTE; a subgroup analysis of the Phase III randomized clinical
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
VTE General Background
 VTE General Background VTE incidence is about 1:1000 persons annually >250,000 admissions for VTE annually >100,000 people die of PE annually >90% of PE s arise from lower limb DVT 50% of DVT at diagnosis
VTE General Background VTE incidence is about 1:1000 persons annually >250,000 admissions for VTE annually >100,000 people die of PE annually >90% of PE s arise from lower limb DVT 50% of DVT at diagnosis
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren
 Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren Paul Kyrle Allgemeines Krankenhaus Wien Disclosures relevant for this presentation Consultancies, member of advisory boards, speaker
Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren Paul Kyrle Allgemeines Krankenhaus Wien Disclosures relevant for this presentation Consultancies, member of advisory boards, speaker
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
DOACs and CAT. 05 May 2017 NTW St Thomas Hospital
 DOACs and CAT Alexander (Ander) Cohen Vascular Medicine / Haematology Guy s and St Thomas Hospitals, King s College, London 05 May 2017 NTW St Thomas Hospital Disclosures for Dr. Alexander (Ander) T. Cohen
DOACs and CAT Alexander (Ander) Cohen Vascular Medicine / Haematology Guy s and St Thomas Hospitals, King s College, London 05 May 2017 NTW St Thomas Hospital Disclosures for Dr. Alexander (Ander) T. Cohen
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
DOAC for VTE. Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University
 DOAC for VTE Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University No disclosures Direct Oral Anticoagulants Understand VTE and the ACCP s position on it List the DOACs available in the US
DOAC for VTE Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University No disclosures Direct Oral Anticoagulants Understand VTE and the ACCP s position on it List the DOACs available in the US
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
ADVANCES IN HEMATOLOGY
 ADVANCES IN HEMATOLOGY Current Developments in the Management of Hematologic Disorders Section Editor: Craig M. Kessler, MD Are Direct Acting Oral Anticoagulants Ready for Prime-Time Use in Cancer-Related
ADVANCES IN HEMATOLOGY Current Developments in the Management of Hematologic Disorders Section Editor: Craig M. Kessler, MD Are Direct Acting Oral Anticoagulants Ready for Prime-Time Use in Cancer-Related
New Strategies and New Data- Beyond Guidelines
 New Strategies and New Data- Beyond Guidelines Anthony Maraveyas GESCAT Lisbon 13 th October 2018 G.MA.GM.XA.12.2017.1962 Conflict of Interest Statement 2 u Research Support: Bayer, Boehringer Ingelheim,
New Strategies and New Data- Beyond Guidelines Anthony Maraveyas GESCAT Lisbon 13 th October 2018 G.MA.GM.XA.12.2017.1962 Conflict of Interest Statement 2 u Research Support: Bayer, Boehringer Ingelheim,
UC SF. Division of General Internal Medicine UNIVERSITY OF CALIFORNIA SAN FRANCISCO, DIVISION OF HOSPITAL MEDICINE
 Updates in the Management of Venous Thromboembolism Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic Venous Thromboembolism
Updates in the Management of Venous Thromboembolism Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic Venous Thromboembolism
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Reversal of Direct Oral Anticoagulants. Why are we now seeing so many patients on DOACs? Objectives. DOAC: Recurrent VTE. DOAC: Intracranial Bleeding
 Reversal of Direct Oral Anticoagulants Cameron D Griffiths, MD, FRCPC Clinical Assistant Professor Division of Hematology UBC Objectives Review efficacy and safety data for Direct Oral Anticoagulants (DOACs)
Reversal of Direct Oral Anticoagulants Cameron D Griffiths, MD, FRCPC Clinical Assistant Professor Division of Hematology UBC Objectives Review efficacy and safety data for Direct Oral Anticoagulants (DOACs)
DOACs in SPECIAL POPULATIONS
 DOACs in SPECIAL POPULATIONS Ann K Wittkowsky PharmD, CACP, FASHP, FCCP Clinical Professor University of Washington School of Pharmacy Director, Anticoagulation Services UWMedicine Department of Pharmacy
DOACs in SPECIAL POPULATIONS Ann K Wittkowsky PharmD, CACP, FASHP, FCCP Clinical Professor University of Washington School of Pharmacy Director, Anticoagulation Services UWMedicine Department of Pharmacy
Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders
 SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Reversal of Novel Oral Anticoagulants. Angelina The, MD March 22, 2016
 Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Perioperative Management of the Anticoagulated Patient
 Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS
 NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
Primary VTE Thromboprophylaxis
 Primary VTE Thromboprophylaxis Controversies in Hematology 53 rd Annual Meeting of Thai Society of Hematology Bundarika Suwanawiboon, MD Division of Hematology Department of Medicine Faculty of Medicine
Primary VTE Thromboprophylaxis Controversies in Hematology 53 rd Annual Meeting of Thai Society of Hematology Bundarika Suwanawiboon, MD Division of Hematology Department of Medicine Faculty of Medicine
Warfarin for Long-Term Anticoagulation. Disadvantages of Warfarin. Narrow Therapeutic Window. Warfarin vs. NOACs. Challenges Monitoring Warfarin
 1 2:15 pm The Era of : Selecting the Best Approach to Treatment SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza,
1 2:15 pm The Era of : Selecting the Best Approach to Treatment SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza,
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Anticoagulation Forum: Management of Tiny Clots
 Anticoagulation Forum: Management of Tiny Clots Casey O Connell, MD FACP Associate Professor Jane Anne Nohl Division of Hematology Keck School of Medicine USC DISCLOSURES None 4/11/2017 Objectives Define
Anticoagulation Forum: Management of Tiny Clots Casey O Connell, MD FACP Associate Professor Jane Anne Nohl Division of Hematology Keck School of Medicine USC DISCLOSURES None 4/11/2017 Objectives Define
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
10/6/2016. Objectives. Abbreviations. Patient Case: K.T. Cancer-Associated Thrombosis. Etiology
 0/6/206 DOACs for VTE Treatment and Secondary Prophylaxis in Patients: A New Direction Samantha Vogel, PharmD PGY Pharmacy Resident Seton Healthcare Family The University of Texas College of Pharmacy Objectives
0/6/206 DOACs for VTE Treatment and Secondary Prophylaxis in Patients: A New Direction Samantha Vogel, PharmD PGY Pharmacy Resident Seton Healthcare Family The University of Texas College of Pharmacy Objectives
10/8/2012. Disclosures. Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines. Goals and Objectives. Outline
 Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Non commercial use only. The treatment of venous thromboembolism with new oral anticoagulants. Background
 Italian Journal of Medicine 2013; volume 7(s8):29-35 The treatment of venous thromboembolism with new oral anticoagulants Davide Imberti AUSL Piacenza, Italy ABSTRACT Traditional anticoagulants, such as
Italian Journal of Medicine 2013; volume 7(s8):29-35 The treatment of venous thromboembolism with new oral anticoagulants Davide Imberti AUSL Piacenza, Italy ABSTRACT Traditional anticoagulants, such as