New Hope for VTE Burden in Ambulatory Cancer Patients
|
|
|
- Daniela Lang
- 6 years ago
- Views:
Transcription
1 New Hope for VTE Burden in Ambulatory Cancer Patients Essam Abo-El-Nazar MS, FRCS Consultant Liver Surgeon King Fahd Hospital Jeddah-KSA Prof. of Surgery Imperial College London-UK

2 My talk today What is the burden of VTE in cancer patients? What are the risk factors for VTE in cancer patients? What is the risk of VTE in cancer patients receiving chemotherapy? What is the new hope for VTE prophylaxis in those patients. VTE = venous thromboembolism.
3 KSA VTE Experts Meeting 2008 VTE epidemiology and risk factors in cancer patients
4 VTE and cancer Of all cases of VTE 1 ~20% of VTE occur in cancer patients Of all cancer patients % will experience VTE as many as 50% have VTE at autopsy Compared to patients without cancer 3.2-fold higher risk of recurrent VTE and rate as high as 21% at 1 year fold higher risk of bleeding with incidence of 12.5% at 1 year fold higher mortality 3 1. Lee AY, et al. Circulation. 2003;107:23 Suppl 1:I17-I Prandoni P, et al. Blood. 2002;100: Sorensen HT, et al. N Engl J Med. 2000;343:
5 Venous thromboembolism (VTE) is a major complication of cancer, occurring in 4% to 20% of patients, and is one of the leading causes of death in patients with cancer. The risk of VTE including deep venous thrombosis (DVT) and pulmonary embolism (PE) is increased several-fold in patients with cancer. Hospitalized patients with cancer and those receiving active therapy seem to be at the greatest risk for development of VTE.

6 Of all patients with VTE, patients with cancer account for 20%, with patients receiving chemotherapy accounting for as much as 13% of the total burden of VTE.



7 CONSEQUENCES OF CANCER-ASSOCIATED VTE Hospitalized patients with VTE have a greater in-hospital mortality rate (odds ratio, 2.01; 95% CI 1.83 to 2.22; P < 0001). The risk of fatal PE in patients with cancer undergoing surgery is three-fold greater than in patients without cancer undergoing similar surgery. Reducing VTE in patients with cancer could therefore have a significant impact on morbidity, outcomes, use of health care resources and mortality.

8 RISK FACTORS FOR CANCER-ASSOCIATED VTE In a population-based study, chemotherapy was associated with a 6.5-fold increased risk of VTE. The risk of VTE increases significantly when patients with cancer are hospitalized

9 Risk Factors for VTE in Patients With Malignant Disease
10 Venous thrombosis in cancer patients is increasing VTE rate in cancer the National Hospital Discharge Survey indicates VTE rates in hospitalized cancer patients doubled from VTE in hospitalized cancer and non-cancer patients(%) Year Cancer patients Non-cancer patients Stein PD. Am J Med. 2006;119:60-8.
11 Impact of cancer on PE frequency Cancer No cancer OR Surgical (%) Non-surgical (%) Total Adapted from Huber O, et al. Arch Surg. 1992;127:310-3.

12 Risk for VTE by type of malignancy Fold increase in risk vs patients without malignancy. Blom JW,et al. JAMA. 2005;293:
13 Activation of coagulation in cancer patients No cancer Cancer p (n = 72) (n = 106) value Tissue factor, pg/ml Factor VIIa, mu/ml TAT, μg/l PF 1+2, nmol/ml Factor XIIa, ng/ml PF = prothrombin factor; TAT = thrombin-antithrombin complex. Kakkar AK, et al. Lancet. 1995;346:
14 Risk factors for VTE in patients with malignant disease Patient-related factors older age (esp. > 65) race (Black/Asian > Hispanic/ Caucasian) comorbid conditions (obesity, infection, renal disease, pulmonary disease, arterial thrombosis) prior history of VTE heritable prothrombotic mutations Cancer-related factors primary site of cancer (pancreatic, GI, brain, lung, gynaecological, renal, haematological) initial 3 6 months after diagnosis current metastatic disease Treatment-related factors recent major surgery current hospitalization active chemotherapy active hormonal therapy current or recent antiangiogenic therapy (thalidomide, lenalidomide, bevacizumab) current erythropoiesis-stimulating agents presence of central venous catheters Lyman GH, et al. J Clin Oncol. 2007;25:
15 Mechanisms of chemotherapyinduced VTE The prothrombotic effects of chemotherapy Chemotherapy TF Platelet activation TF VEGF Tumour cell cytokine secretion Direct vascular endothelial toxicity Monocyte/macrophage expression of TF Decrease protein C and S Decrease ATIII Increase PAI-1 Alterations in coagulation and fibrinolytic molecules Endothelial cell apoptosis and increase in TF activity TNF-α IL-1β TF TF TF Increase in endothelial TF expression Haddad TC, Greeno EW. Thromb Res. 2006;118:555-
16 Risk of VTE is highest in first months after cancer diagnosis The highest risk of venous thrombosis is in the first 3 months after diagnosis (adjusted OR, 53.5; 95% CI, ) Patients (%) to 3 months > 3 months to 1 year > 1 to 3 years > 3 to 5 years > 5 to 10 years > 10 to 15 years > 15 years 0 Time after diagnosis of malignancy Adjusted OR = odds ratio adjusted for age and sex. Blom JW, et al. JAMA. 2005;293:
17 Independent risk factors for DVT/PE Risk factor/characteristic Odds ratio Recent surgery with institutionalization Trauma Institutionalization without recent surgery 7.98 Malignancy with chemotherapy 6.53 Prior CVC or transvenous pacemaker 5.55 Prior superficial vein thrombosis 4.32 Malignancy without chemotherapy 4.05 Neurological disease with extremity paresis 3.04 Serious liver disease 0.10 CVC = central venous catheter. Heit JA, et al. Thromb Haemost. 2001;86:
18 Venous thromboembolic events with chemotherapy according to cancer type Pooled analysis of patients in randomized Phase II and III studies (N = 6,055 patients/10 RCT) Incidence of VTE (% patients) Bevacizumab all grade No bevacizumab all grade Bevacizumab grade 3 5 No bevacizumab grade 3 5 All Breast cancer NSCLC NSCLC = non-small-cell lung cancer; RCT = randomized controlled trial. Pancreatic cancer 5% Renal cell cancer 10% Colorectal cancer Hurwitz HI, et al. J Clin Oncol. 2011;29:
19 Risk for VTE in cancer patients with angiogenesis agents Tumour type Incidence and relative risk of all-grade VTE with bevacizumab among patients with various tumour types Number of studies All-grade VTE, n/n Bevacizumab Control Overall 6 155/1, /1,083 Colorectal cancer Non-small-cell lung carcinoma 3 108/564 85/ /66 3/32 Breast cancer 1 17/229 12/215 Renal cell carcinoma 1 20/337 6/304 Incidence, % (95% CI) 11.9 ( ) 19.1 ( ) 14.9 ( ) 7.3 ( ) 3.0 ( ) RR (95% CI) 1.29 ( ) 1.19 ( ) 1.59 ( ) 1.30 ( ) 3.00 ( ) Nalluri SR, et al. JAMA. 2008;300:
20 Cisplatin-associated VTE Retrospective analysis of 932 patients treated with cisplatin-based chemotherapy 169 (18.1%) patients had a thromboembolic event (TE) DVT alone: 49.7% PE alone: 25.4% DVT+PE: 13.6% TEs occurred within 100 days of initiation of treatment in 88% of patients Moore RA, et al. J Clin Oncol. 2011;29:
21 What is the true burden of VTE in medical oncology? IHCIS Database search on the same population as SAVE-ONCO N VTE rate 30, % at 3.5 months IHCIS = Integrated Health Care Information Solutions. Lyman GH, et al. The European Multidisciplinary Cancer Congress, Stockholm, Sweden, September 2011: [abstract 3002].

22 What is the true burden of VTE in medical oncology? Medical oncology versus other settings 60% to 70% of fatal PE detected post-mortem are not suspected or diagnosed 1,2 70% Picture modified f from Ralph A. Clevenger Fatal PE is the leading cause of sudden death among hospitalized patients and contributes to up to 10% of in-hospital deaths 3 1. Stein PD, et al. Chest. 1995;110: Sandler DA, et al. J R Soc Med. 1989;82: Nicolaides AN, et al. Int Angiology. 2006;25:
 1/3 1/3 2/3 Upper limbs DVT 8% Iliac-cava vein 4% Lower limbs DVT + SVT* 6% Portal or splanchnic veins 10% Lower")
23 Atypical localization of VTE in cancer compared to major surgery setting Natural history following major surgery 1 Incidental VTE in cancer with chemotherapy 2 Retrospective, single institution cohort study N = 1,921 medical records of cancer patients (solid T + chemotherapy) 1/3 1/3 2/3 Upper limbs DVT 8% Iliac-cava vein 4% Lower limbs DVT + SVT* 6% Portal or splanchnic veins 10% Lower limbs DVT alone 31% PE alone 26% Renal veins 2% PE with lower limbs DVT 13% 1. Kakkar VV, et al. Lancet. 1969;2: DVT = deep vein thrombosis; SVT = superficial vein thrombosis. 2. Di Nisio M, et al. Thromb Haemost. 2010;104:
24 Conclusions Venous thromboembolism is an important complication Frequency may be underestimated Impact on clinical outcome frequently not appreciated Important opportunities for pharmacological prophylaxis
 Should ambulatory patients with cancer receive anticoagulation for VTE prophylaxis during systemic chemotherapy?")
25 GUIDELINE QUESTIONS (1) Should hospitalized patients with cancer receive anticoagulation for VTE prophylaxis? (2) Should ambulatory patients with cancer receive anticoagulation for VTE prophylaxis during systemic chemotherapy? (3) Should patients with cancer undergoing surgery receive perioperative VTE prophylaxis? (4) What is the best method for treatment of patients with cancer with established VTE to prevent recurrence? (5) Should patients with cancer receive anticoagulants in the absence of established VTE to improve survival?


26 1. SHOULD HOSPITALIZED PATIENTS WITH CANCER RECEIVE ANTICOAGULATION FOR VTE PROPHYLAXIS? Recommendation: Hospitalized patients with cancer should be considered candidates for VTE prophylaxis with anticoagulants in the absence of bleeding or other contraindications to anticoagulation.
 Routine prophylaxis with an antithrombotic agent is not recommended.")
27 2. SHOULD AMBULATORY PATIENTS WITH CANCER RECEIVE ANTICOAGULATION FOR VTE PROPHYLAXIS DURING SYSTEMIC CHEMOTHERAPY? (1) Routine prophylaxis with an antithrombotic agent is not recommended. (2) Patients receiving thalidomide or lenalidomide with chemotherapy or dexamethasone are at high risk for thrombosis and warrant prophylaxis.
 All patients undergoing major surgical intervention for malignant disease should be considered for thromboprophylaxis.")
 Prophylaxis should be commenced preoperatively, or as early as possible in the postoperative period.")
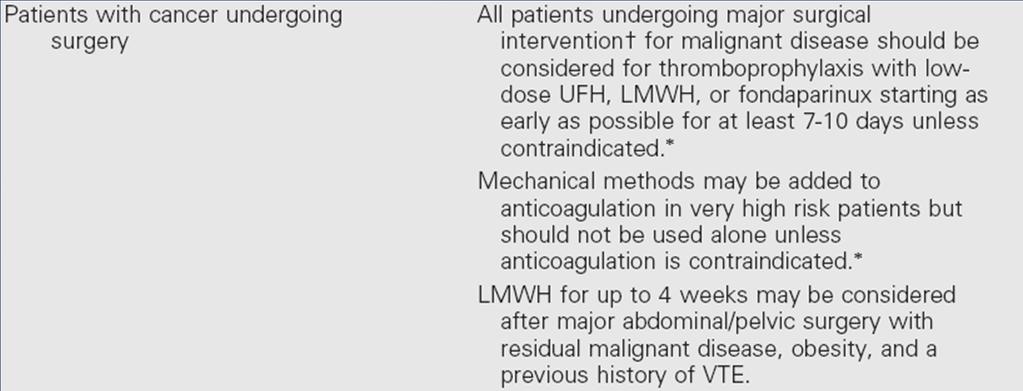
28 3. SHOULD PATIENTS WITH CANCER UNDERGOING SURGERY RECEIVE PERIOPERATIVE VTE PROPHYLAXIS? Recommendations (1) All patients undergoing major surgical intervention for malignant disease should be considered for thromboprophylaxis. (2) Patients undergoing laparotomy, laparoscopy, or thoracotomy lasting greater than 30 minutes should receive pharmacologic thromboprophylaxis with either low-dose UFH or LMWH unless contraindicated because of a high risk of bleeding or active bleeding. (3) Prophylaxis should be commenced preoperatively, or as early as possible in the postoperative period. (4) Mechanical methods may be added to pharmacologic methods, but should not be used as monotherapy for VTE prevention unless pharmacologic methods are contraindicated because of active bleeding.



29 (6) Prophylaxis should be continued for at least 7 to 10 days postoperatively. (7) Prolonged prophylaxis for up to 4 weeks may be considered in patients undergoing major abdominal or pelvic surgery for cancer with high-risk features such as residual malignant disease after operation, obese patients, and those with a previous history of VTE.
 LMWH is the preferred approach for the initial 5 to 10 days of anticoagulant treatment of the cancer patient with established VTE.")
30 4. WHAT IS THE BEST TREATMENT FOR PATIENTS WITH CANCER WITH ESTABLISHED VTE TO PREVENT RECURRENT VTE? Recommendations (1) LMWH is the preferred approach for the initial 5 to 10 days of anticoagulant treatment of the cancer patient with established VTE. (2) LMWH given for at least 6 months is also the preferred approach for long-term anticoagulant therapy. (3) Vitamin K antagonists with a targeted INR of 2 to 3 are acceptable for long-term therapy when LMWH is not available. (4) The insertion of a vena cava filter is only indicated for patients with contraindications to anticoagulant therapy and in those with recurrent VTE despite adequate long-term therapy with LMWH.
 or coagulopathy.")

31 (5) Anticoagulation should be avoided in the presence of active intracranial bleeding, preexisting bleeding diathesis such as thrombocytopenia (platelet count 50,000/L) or coagulopathy. (6) For elderly patients, anticoagulation is recommended for established VTE as described for other patients with cancer. Careful monitoring and dose adjustment is necessary to avoid excessive anticoagulation and further increase in the risk of bleeding.
 all hospitalized cancer patients should be considered for VTE prophylaxis with anticoagulants in the absence of bleeding or other contraindications.")
32 American Society of Clinical Oncology Guideline: Recommendations for Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer Recommendations of the American Society of Clinical Oncology VTE Guideline Panel include (1) all hospitalized cancer patients should be considered for VTE prophylaxis with anticoagulants in the absence of bleeding or other contraindications. (2) routine prophylaxis of ambulatory cancer patients with anticoagulation is not recommended, with the exception of patients receiving thalidomide or lenalidomide (3) Patients undergoing major surgery for malignant disease should be considered for pharmacologic thromboprophylaxis. (4) low molecular weight heparin represents the preferred agent for both the initial and continuing treatment of cancer patients with established VTE. (5) The impact of anticoagulants on cancer patient survival requires additional study and cannot be recommended at present.

33 Summary of recommendations
34 Summary of recommendations
35 Summary of recommendations
36 Prophylaxis Guidelines in cancer patients Guidelines recommend VTE prophylaxis in «hospitalized medical patients» & by NCCN only for «ambulatory cancer patients receiving chemotherapy» NCCN V ASCO 2007 ESMO May 2010 ACCP 2008 ICS 2006 Hospitalized medical patients VTE prophylaxis with anticoagulants if no contra indication from admission to discharge [I] VTE prophylaxis with anticoagulants if no contra indication or bleeding Prophylaxis with UFH, LMWH or Fonda for cancer patients confined to bed with an acute medical complication [I, A] Routine thromboprophylaxis in bedridden patient with an acute medical illness [Grade 1A) For patients with acute medical illness, thrombopx based on the risk of VTE (acute medical co-morbidity) LMWH or LDUH should be used [Grade A] Ambulatory patients receiving chemotherapy VTE prophylaxis in high risk settings (antiangiogenic therapy = myeloma patients thalidomide/lenalidomide + high dosedexamethasone) VTE prophylaxis in high risk outpatients on chemotherapy with risk factors [IIa] -Active cancers associated with high incidence of VTE: stomach, pancreas, lung, lymphoma, gynecologic, bladder and testicular -Prechemotherapy platelet count > 300,000/mcL -Hemoglobin < 10g/Dl -Use of erythropoietic stimulating agents -Body mass index 35kg/m2 -Prior VTE No routine prophylaxis. Multiple myeloma patients receiving thalidomide or lenalidomide with CT or dexamethasone are at high risk of thrombosis and warrant VTE prophylaxis with LMWH or adjusted-dose warfarin (INR~1.5) Extensive, routine prophylaxis for advanced cancer patients receiving CT not recommended. Consider LMWH or adjusted-dose warfarin in myeloma patients receiving thalidomide + dexamethasone or thalidomide + chemotherapy [IIB] Px in cancer patients receiving adjuvant chemotherapy and/or hormone therapy not recommended [I, A] Recommendation against routine thromboprophylaxis for the primary prevention of VTE in patients receiving CT or hormonal therapy [Grade 1C] Value of routine primary thromboprophylaxis not yet established (only for those with advanced breast cancer: use of AVK) [Grade B] NCCN: National Comprehensive Cancer Network/ ASCO: American Society of Clinical Oncology/ ESMO: European Society of Medical Oncology / AOIM: Italian Association of Medical Oncology/ SOR: Standards, Options: Recommendations, from the French National Cancer Institute/ ACCP: American College of Chest Physicians/ ICS: International Consensus Statement



37 The ultra-low-molecular-weight heparin (ULMWH) Semuloparin for prevention of Venous Thromboembolism (VTE) in Cancer patients receiving Chemotherapy: SAVE-ONCO study
38 Study rationale Patients with cancer are at increased risk for VTE 1,2 Chemotherapy represents an additional risk factor for VTE 3,4 Certain tumor types and late-stage disease are associated with even higher VTE risk 2,3,5,6 Currently, routine thromboprophylaxis in ambulatory patients with cancer receiving chemotherapy is not recommended 7,8,9,10 due to several randomized controlled trials reporting inconclusive results 11 Large, randomized, placebo-controlled, VTE-prevention trials are needed 1 Heit JA, et al. Arch Intern Med. 2000;160:809-15; 2 Khorana AA, et al. Cancer. 2007;110: ; 3 Blom JW, et al. J Thromb Haemost. 2006;4:529-35; 4 Kröger K, et al. Ann Oncol. 2006;17: ; 5 Chew HK, et al. Arch Intern Med. 2006;166:458-64; 6 Stein PD, et al. Am J Med. 2006;119:60-8; 7 Lyman G, et al. J Clin Oncol. 2007;34:1-16; 8 Geerts WH, et al. Chest. 2008;133:381S-453S; 9 Mandalà M, et al. Ann Oncol. 2010;21 Suppl 5:v274-6; 10 National Comprehensive Cancer Network (2010) 11 Kuderer N, et al. J Clin Oncol ASCO Annual Meeting Proceedings (Post-Meeting Edition); 27(15S): 9537.
39 Semuloparin Ultra-low-molecular-weight heparin (ULMWH): Molecular weight Da High anti-factor Xa activity with anti-factor IIa activity Half-life hours 98% bioavailability after subcutaneous injection C max reached at 3 hours Excretion mainly renal
40 Study objectives In patients with locally advanced or metastatic solid tumor receiving chemotherapy to: Compare the efficacy of semuloparin with placebo for the prevention of VTE Evaluate the safety of semuloparin
41 Study design Multinational, randomized, double-blind, parallel-group study N = 3200 Standard of care chemotherapy Placebo sc once daily Post-treatment follow-up Randomization Stratified by: - Cancer type - Cancer stage - Geographical location 1:1 Standard of care chemotherapy Semuloparin 20mg sc once daily End of treatment Treatment Duration: End of treatment + 1 month Patients were treated for the length of chemotherapy If chemotherapy changed prior to 3 months, patients were allowed to continue semuloparin or placebo treatment If chemotherapy changed or stopped after 3 months then semuloparin or placebo treatment was discontinued clinicaltrials.gov: NCT
42 Eligibility Criteria Main inclusion criteria Metastatic or locally advanced solid tumor of lung, pancreas, stomach, colon/rectum, bladder or ovary Initiating a chemotherapy regimen with a minimum intent of 3 months* Main exclusion criteria ECOG (Eastern Cooperative Oncology Group) Performance status of 3 or 4 Estimated creatinine clearance < 30mL/min Contraindication to anticoagulation Requirement for systemic anticoagulation or thrombolysis *Prior chemotherapy was allowed
43 Study endpoints Primary efficacy endpoint: Time to first occurrence of: Any symptomatic DVT Any PE Non-fatal VTE-related deaths (fatal PE or unexplained death) Primary safety endpoint Clinically relevant bleeding, composite of Major bleeding* Clinically relevant non-major bleeding (CRNM)** *Major bleeding defined as any of the following: fatal bleeding, bleeding in a critical area or organ, or clinically overt and causing a drop in hemoglobin 2 g/dl, or requiring 2 units of blood transfusion 1 **CRNM defined as bleeding requiring medical intervention and not meeting criteria for major bleeding 1 ISTH criteria DVT = deep-vein thrombosis, PE = pulmonary embolism
44 Statistical assumptions VTE event rate ~4% in placebo group Risk reduction (RR) with semuloparin ~50% Power = 90% Alpha = 0.05 Intent-to-treat analysis of primary efficacy endpoint
45 Analysis populations Randomized n = 3212 Placebo n = 1604 (100%) Efficacy population Intent-to-treat Semuloparin n = 1608 (100%) Treated n = 1583 (98.7%) Safety population Treated n = 1589 (98.8%)
46 Baseline characteristics Placebo Semuloparin n = 1604 n = 1608 Median age (range), years 60.0 (18-87) 60.0 (20-89) Male, % Median BMI (range), kg/m² 24.1 (13-54) 24.4 (12-57) CVL at baseline, n (%) 302 (18.8) 316 (19.7) Metastatic / locally advanced, % 68.3 / / 31.8 Primary tumor location, % Lung Colon / Rectum Stomach Ovary Pancreas Bladder

47 Treatment duration Treatment duration was approximately 3.5 months, with no difference between the semuloparin and placebo groups
48 Primary efficacy endpoint Composite of symptomatic DVT and any PE Cumulative incidence (%) 5.0% 4.0% 3.0% 2.0% 1.0% Placebo : 3.4% (55/1604) Semuloparin 1.2% (20/1608) HR : 0.36 [ ]; p < Placebo RR 64% Semuloparin 0.0% Time (Months) Number at Risk Placebo Semuloparin HR = hazard ratio
49 Components of the primary efficacy endpoint OR 0.32 [ ] Placebo Semuloparin 2.1 OR 0.41 [ ] OR 0.20 [ ] OR 0.77 [ ] / / / /1604 3/1608 9/1604 7/1608 Symptomatic DVT Any PE Non-fatal PE VTE-related death OR = odds ratio [95% CI]
50 Bleeding Placebo OR 1.41 [ ] 2.8 OR 1.05 [ ] OR 1.86 [ ] / / / / / /1589 Clinically relevant Major* Non-major** *Includes 6 fatal bleedings (4 [0.3%] in placebo and 2 [0.1%] in semuloparin),and 5 (0.3%) non-fatal bleedings into critical area or organ in the semuloparin group **6 events in placebo and 9 in semuloparin caused study drug discontinuation; 2 events in placebo and 3 in semuloparin were serious and caused study drug discontinuation; 13 events in placebo and 25 in semuloparin recovered
51 Summary Semuloparin, compared to placebo, showed: 64% risk reduction in the composite of symptomatic DVT and any PE (p < ) 59% risk reduction in any PE; OR 0.41, [ ] Incidence of clinically relevant bleeding of 2.8% vs 2.0% Similar low incidence of major bleeding; 1.2% vs 1.1%
52 Conclusions Semuloparin 20 mg demonstrated a favourable benefit-risk profile for VTE prevention in cancer patients receiving chemotherapy Which cancer patients should we now consider for thromboprophylaxis? Undergoing surgery Hospitalized/acutely ill Receiving chemotherapy : Semuloparin is efficient and safe for VTE prophylaxis in ambulatory cancer patients receiving chemotherapy.
53 Thank you
PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES
 PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES Mario Mandalà, MD Unit of Clinical Research Department of Oncology and Haematology Papa Giovanni XXIII Hospital Cancer Center
PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES Mario Mandalà, MD Unit of Clinical Research Department of Oncology and Haematology Papa Giovanni XXIII Hospital Cancer Center
Venous Thrombo-Embolism. John de Vos Consultant Haematologist RSCH
 Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Is There a Role for Prophylaxis in Cancer Patients During Therapy?
 Victor F. Tapson, MD, FCCP, FRCP Professor of Medicine Director, Center for Pulmonary Vascular Disease Division of Pulmonary and Critical Care Duke University Medical Center Durham, N.C. USA Is There a
Victor F. Tapson, MD, FCCP, FRCP Professor of Medicine Director, Center for Pulmonary Vascular Disease Division of Pulmonary and Critical Care Duke University Medical Center Durham, N.C. USA Is There a
In the Clinic: Annals Sweta Kakaraparthi 1/23/15
 In the Clinic: Annals Sweta Kakaraparthi 1/23/15 Case Scenerio 56 year old female with breast cancer presents to the clinic for her 3 month followup! She is concerned about blood clots and asks you about
In the Clinic: Annals Sweta Kakaraparthi 1/23/15 Case Scenerio 56 year old female with breast cancer presents to the clinic for her 3 month followup! She is concerned about blood clots and asks you about
RISK FACTORS. Cancer type. Cancer stage
 CANCER ASSOCIATED THROMBOSIS RISK FACTORS The link between cancer and thrombosis is well established, with malignancy recognised as the most important individual risk factor for venous thromboembolism
CANCER ASSOCIATED THROMBOSIS RISK FACTORS The link between cancer and thrombosis is well established, with malignancy recognised as the most important individual risk factor for venous thromboembolism
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
Epidemiology of Thrombosis in Patients with Malignancy. Cancer and Venous Thromboembolism. Chew HK, Arch Int Med, Feb Blom et al, JAMA, Feb 2005
 Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
Cancer and Thrombosis
 Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Profilassi e trattamento del tromboembolismo venoso nei pazienti con neoplasia: le nuove linee guida
 Profilassi e trattamento del tromboembolismo venoso nei pazienti con neoplasia: le nuove linee guida Anna Falanga Dipartimento di Medicina Trasfusionale ed Ematologia Centro Trombosi ed Emostasi Ospedale
Profilassi e trattamento del tromboembolismo venoso nei pazienti con neoplasia: le nuove linee guida Anna Falanga Dipartimento di Medicina Trasfusionale ed Ematologia Centro Trombosi ed Emostasi Ospedale
VTE Risk Assessment. Challenges of Hemostasis in Cancer Patients. Cihan Ay, MD Associate Professor
 Challenges of Hemostasis in Cancer Patients VTE Risk Assessment Cihan Ay, MD Associate Professor Clinical Division of Haematology and Haemostaseology Department of Medicine I, Comprehensive Cancer Center
Challenges of Hemostasis in Cancer Patients VTE Risk Assessment Cihan Ay, MD Associate Professor Clinical Division of Haematology and Haemostaseology Department of Medicine I, Comprehensive Cancer Center
THROMBOPROPHYLAXIS IN CANCER PATIENTS
 CANCER ASSOCIATED THROMBOSIS THROMBOPROPHYLAXIS IN CANCER PATIENTS Cancer is an important risk factor for venous thromboembolism (VTE). Research has shown that 4-20% of 1 patients with cancer experience
CANCER ASSOCIATED THROMBOSIS THROMBOPROPHYLAXIS IN CANCER PATIENTS Cancer is an important risk factor for venous thromboembolism (VTE). Research has shown that 4-20% of 1 patients with cancer experience
Cancer Associated Thrombosis: six months and beyond. Farzana Haque Hull York Medical School
 Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
Are guidelines for anticoagulation useful in cancer patients?
 Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
GLIOMA - VENOUS THROMBOEMBOLISM. Miguel Navarro. Hospital Universitario de Salamanca-IBSAL
 GLIOMA - VENOUS THROMBOEMBOLISM Miguel Navarro. Hospital Universitario de Salamanca-IBSAL GLIOMA - VTE GLIOMA - VTE The two string problem Substantial risk for developing VTE Concern antithrombotic agents
GLIOMA - VENOUS THROMBOEMBOLISM Miguel Navarro. Hospital Universitario de Salamanca-IBSAL GLIOMA - VTE GLIOMA - VTE The two string problem Substantial risk for developing VTE Concern antithrombotic agents
The risk of venous thromboembolism is four to seven times as
 review article Dan L. Longo, M.D., Editor Prophylaxis against Venous Thromboembolism in Ambulatory Patients with Cancer Jean M. Connors, M.D. The risk of venous thromboembolism is four to seven times as
review article Dan L. Longo, M.D., Editor Prophylaxis against Venous Thromboembolism in Ambulatory Patients with Cancer Jean M. Connors, M.D. The risk of venous thromboembolism is four to seven times as
Dr. Pierpaolo Di Micco Internal Medicine and Emergency Room Fatebenefratelli Hospital of Naples, Italy
 ? Para què sirve el recuento de leucocitos en lospacientescon cancer? Dr. Pierpaolo Di Micco Internal Medicine and Emergency Room Fatebenefratelli Hospital of Naples, Italy ? Para què sirve el recuento
? Para què sirve el recuento de leucocitos en lospacientescon cancer? Dr. Pierpaolo Di Micco Internal Medicine and Emergency Room Fatebenefratelli Hospital of Naples, Italy ? Para què sirve el recuento
Cancer Associated Thrombosis An update.
 Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
PROGNOSIS AND SURVIVAL
 CANCER ASSOCIATED THROMBOSIS PROGNOSIS AND SURVIVAL Since French internist Armand Trousseau reported the occurrence of mysterious thrombotic disorders in cancer patients in the mid-19th century, the link
CANCER ASSOCIATED THROMBOSIS PROGNOSIS AND SURVIVAL Since French internist Armand Trousseau reported the occurrence of mysterious thrombotic disorders in cancer patients in the mid-19th century, the link
New oral anticoagulants and Palliative Care.
 New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
Cancer and the Heparins
 Cancer and the Heparins Wim P Ceelen, MD, PhD, FACS Department of GI Surgery - UZ Gent Senior Clinical Researcher - FWO Overview Mechanisms of cancer induced thrombosis Guidelines for prevention and treatment
Cancer and the Heparins Wim P Ceelen, MD, PhD, FACS Department of GI Surgery - UZ Gent Senior Clinical Researcher - FWO Overview Mechanisms of cancer induced thrombosis Guidelines for prevention and treatment
Cancer Associated Thrombosis
 Cancer Associated Thrombosis Pantep Angchaisuksiri, MD Professor of Medicine Mahidol University, Thailand Adjunct Associate Professor University of North Carolina, Chapel Hill, USA Piccioli A. J Thromb
Cancer Associated Thrombosis Pantep Angchaisuksiri, MD Professor of Medicine Mahidol University, Thailand Adjunct Associate Professor University of North Carolina, Chapel Hill, USA Piccioli A. J Thromb
Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders
 SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation
 ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation Stephan Moll Department of Medicine, Division of Hematology-Oncology, University of North Carolina School of
ASH 2011: Clinically Relevant Highlights Regarding Venous Thromboembolism and Anticoagulation Stephan Moll Department of Medicine, Division of Hematology-Oncology, University of North Carolina School of
Management of Cancer Associated Thrombosis (CAT) where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth
 where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth") Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Tissue Factor-positive Microparticles in Cancerassociated
 Tissue Factor-positive Microparticles in Cancerassociated Thrombosis Nigel Mackman, Ph.D., FAHA John C. Parker Distinguished Professor of Medicine Director of the UNC McAllister Heart Institute Co-Director
Tissue Factor-positive Microparticles in Cancerassociated Thrombosis Nigel Mackman, Ph.D., FAHA John C. Parker Distinguished Professor of Medicine Director of the UNC McAllister Heart Institute Co-Director
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Factor Xa Inhibition in the Management of Venous Thromboembolism: Important Safety Information. Important Safety Information (cont d)
") Factor Xa Inhibition in the Management of Venous Thromboembolism: The Role of Fondaparinux WARNING: SPINAL/EPIDURAL HEMATOMAS Epidural or spinal hematomas may occur in patients who are anticoagulated with
Factor Xa Inhibition in the Management of Venous Thromboembolism: The Role of Fondaparinux WARNING: SPINAL/EPIDURAL HEMATOMAS Epidural or spinal hematomas may occur in patients who are anticoagulated with
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies
 VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
Cancer associated thrombosis. 17 th November 2016 Simon Noble Clinical Professor Palliative Medicine Cardiff University Wales, UK
 Cancer associated thrombosis 17 th November 2016 Simon Noble Clinical Professor Palliative Medicine Cardiff University Wales, UK Today What is VTE? How does CAT differ? Initial anticoagulation Anticoagulation
Cancer associated thrombosis 17 th November 2016 Simon Noble Clinical Professor Palliative Medicine Cardiff University Wales, UK Today What is VTE? How does CAT differ? Initial anticoagulation Anticoagulation
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS
 EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
incidence of cancer-associated thrombosis (CAT) is further increased by additional risk factors such as chemotherapeutic 2
 is further increased by additional risk factors such as chemotherapeutic 2") CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
J Clin Oncol 31: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 31 NUMBER 17 JUNE 10 2013 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E Gary H. Lyman, Nicole M. Kuderer, and Jeffrey M. Clarke, Duke University and Duke Cancer Institute, Durham;
VOLUME 31 NUMBER 17 JUNE 10 2013 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E Gary H. Lyman, Nicole M. Kuderer, and Jeffrey M. Clarke, Duke University and Duke Cancer Institute, Durham;
Prophylaxie primaire sur le patient ambulatoire. Marc Carrier
 Prophylaxie primaire sur le patient ambulatoire Marc Carrier Marc Carrier In compliance with COI policy, SSVQ requires the following disclosures to the session audience: Research Support/P.I. Employee
Prophylaxie primaire sur le patient ambulatoire Marc Carrier Marc Carrier In compliance with COI policy, SSVQ requires the following disclosures to the session audience: Research Support/P.I. Employee
Venous Thromboembolism (VTE) in Myeloma. Christine Chen May 2017
 in Myeloma. Christine Chen May 2017") Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1
 CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
Thromboembolism and cancer: New practices. Marc Carrier
 Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Prevention of Venous Thromboembolism
 Prevention of Venous Thromboembolism Surgical Care Improvement Project Dale W. Bratzler, DO, MPH President and CEO Dale W. Bratzler, DO, MPH Oklahoma Foundation for Medical Quality QIOSC Medical Director
Prevention of Venous Thromboembolism Surgical Care Improvement Project Dale W. Bratzler, DO, MPH President and CEO Dale W. Bratzler, DO, MPH Oklahoma Foundation for Medical Quality QIOSC Medical Director
Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski. Department of Surgery Grand Rounds March 24, 2008
 Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski Department of Surgery Grand Rounds March 24, 2008 History of Vena Cava Filters Virchow-1846-Proposes PE originate from veins
Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski Department of Surgery Grand Rounds March 24, 2008 History of Vena Cava Filters Virchow-1846-Proposes PE originate from veins
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Report dei gruppi di lavoro >> [ Trombosi e cancro ]
![Report dei gruppi di lavoro >> [ Trombosi e cancro ]](/thumbs/91/106293601.jpg "Report dei gruppi di lavoro >> [ Trombosi e cancro ]") Report dei gruppi di lavoro >> [ Trombosi e cancro ] Relatori: A. FALANGA, M. MARCHETTI 27-28 ottobre 2008 Borgo S. Luigi Monteriggioni (Siena) Trombosi e cancro - Copyright FSE 1 Gruppo di lavoro 2 [
Report dei gruppi di lavoro >> [ Trombosi e cancro ] Relatori: A. FALANGA, M. MARCHETTI 27-28 ottobre 2008 Borgo S. Luigi Monteriggioni (Siena) Trombosi e cancro - Copyright FSE 1 Gruppo di lavoro 2 [
How long to continue anticoagulation after DVT?
 How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement. Marilyn Szekendi, PhD, RN
 Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
10/8/2012. Disclosures. Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines. Goals and Objectives. Outline
 Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
General. Recommendations. Guideline Title. Bibliographic Source(s) Guideline Status. Major Recommendations
 Guideline Status. Major Recommendations") General Guideline Title Prevention of deep vein thrombosis and pulmonary embolism. Bibliographic Source(s) American College of Obstetricians and Gynecologists (ACOG). Prevention of deep vein thrombosis
General Guideline Title Prevention of deep vein thrombosis and pulmonary embolism. Bibliographic Source(s) American College of Obstetricians and Gynecologists (ACOG). Prevention of deep vein thrombosis
Novità dall EHA >> [ Trombosi e cancro ]
![Novità dall EHA >> [ Trombosi e cancro ]](/thumbs/91/106293367.jpg "Novità dall EHA >> [ Trombosi e cancro ]") Novità dall EHA >> [ Trombosi e cancro ] Relatore: A. FALANGA 27-28 ottobre 2008 Borgo S. Luigi Monteriggioni (Siena) Trombosi e cancro - Copyright FSE 1 TROMBOSI E CANCRO 2 SIMPOSIO EDUCAZIONALE: LMWH
Novità dall EHA >> [ Trombosi e cancro ] Relatore: A. FALANGA 27-28 ottobre 2008 Borgo S. Luigi Monteriggioni (Siena) Trombosi e cancro - Copyright FSE 1 TROMBOSI E CANCRO 2 SIMPOSIO EDUCAZIONALE: LMWH
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Anticoagulation in Special populations. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Venous Thromboembolism and Cancer: In Brief
 1 Venous Thromboembolism and Cancer: In Brief Ever since the landmark clinical observations of Trousseau linking venous thrombosis and malignancy, this association has fascinated generations of physicians
1 Venous Thromboembolism and Cancer: In Brief Ever since the landmark clinical observations of Trousseau linking venous thrombosis and malignancy, this association has fascinated generations of physicians
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Duration of Anticoagulant Therapy. Linda R. Kelly PharmD, PhC, CACP September 17, 2016
 Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
10/24/2013. Heparin-Induced Thrombocytopenia (HIT) Anticoagulation Management in ECMO Therapy:
 Anticoagulation Management in ECMO Therapy:") Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
La terapia del TEV nel paziente oncologico nell'era dei DOAC
 XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
CANCER-ASSOCIATED THROMBOSIS Prediction, Prevention and Treatment
 CANCER-ASSOCIATED THROMBOSIS Prediction, Prevention and Treatment Alok A. Khorana, MD, FACP Sondra and Stephen Hardis Chair in Oncology Research Vice-Chair, Taussig Cancer Institute Case Comprehensive
CANCER-ASSOCIATED THROMBOSIS Prediction, Prevention and Treatment Alok A. Khorana, MD, FACP Sondra and Stephen Hardis Chair in Oncology Research Vice-Chair, Taussig Cancer Institute Case Comprehensive
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients. David Liff MD Oklahoma Heart Institute Vascular Center
 DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Supplementary Online Content
 Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Prevention and management of venous thromboembolism M. AAPRO
 Prevention and management of venous thromboembolism M. AAPRO Thromboprophylaxisof DVT and PE in AmbulatoryCancerPatients Zurich, February 2017 M. AAPRO Based on a lesson in April 2016 by M. DICATO M.D.,
Prevention and management of venous thromboembolism M. AAPRO Thromboprophylaxisof DVT and PE in AmbulatoryCancerPatients Zurich, February 2017 M. AAPRO Based on a lesson in April 2016 by M. DICATO M.D.,
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT
 VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School
 Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
Anticoagulation in Special populations. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Fatal P.E. Historic 1-2% Current %
 Dr. (Prof.) Anil Arora MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London, UK) Senior
Dr. (Prof.) Anil Arora MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London, UK) Senior
Frequently Asked Questions about Cancer Associated Thrombosis
 + Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
+ Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
Acute and long-term treatment of VTE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Frequency, demographics and risk (according to tumour type or site) of cancer-associated thrombosis among patients seen at outpatient DVT clinics
 of cancer-associated thrombosis among patients seen at outpatient DVT clinics") 338 Schattauer 2010 Blood Coagulation, Fibrinolysis and Cellular Haemostasis Frequency, demographics and risk (according to tumour type or site) of cancer-associated thrombosis among patients seen at outpatient
338 Schattauer 2010 Blood Coagulation, Fibrinolysis and Cellular Haemostasis Frequency, demographics and risk (according to tumour type or site) of cancer-associated thrombosis among patients seen at outpatient
Non commercial use only. The treatment of venous thromboembolism with new oral anticoagulants. Background
 Italian Journal of Medicine 2013; volume 7(s8):29-35 The treatment of venous thromboembolism with new oral anticoagulants Davide Imberti AUSL Piacenza, Italy ABSTRACT Traditional anticoagulants, such as
Italian Journal of Medicine 2013; volume 7(s8):29-35 The treatment of venous thromboembolism with new oral anticoagulants Davide Imberti AUSL Piacenza, Italy ABSTRACT Traditional anticoagulants, such as
Results from RE-COVER RE-COVER II RE-MEDY RE-SONATE EXECUTIVE SUMMARY
 Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in the treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and the prevention of recurrent DVT and PE Results from
Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in the treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE) and the prevention of recurrent DVT and PE Results from
Venous Thromboembolism. Prevention
 Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS
 ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
Clinical practice guidelines for prophylaxis of venous thomboembolism in cancer patients
 618 Theme Issue Article Clinical practice guidelines for prophylaxis of venous thomboembolism in cancer patients Corinne Frere 1 ; Dominique Farge 2 1 Assistance Publique Hôpitaux de Marseille, Timone
618 Theme Issue Article Clinical practice guidelines for prophylaxis of venous thomboembolism in cancer patients Corinne Frere 1 ; Dominique Farge 2 1 Assistance Publique Hôpitaux de Marseille, Timone
Update on the Management of Cancer Associated VTE
 Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Venous thromboembolism in cancer patients: an underestimated major health problem
 Khalil et al. World Journal of Surgical Oncology (2015) 13:204 DOI 10.1186/s12957-015-0592-8 WORLD JOURNAL OF SURGICAL ONCOLOGY REVIEW Venous thromboembolism in cancer patients: an underestimated major
Khalil et al. World Journal of Surgical Oncology (2015) 13:204 DOI 10.1186/s12957-015-0592-8 WORLD JOURNAL OF SURGICAL ONCOLOGY REVIEW Venous thromboembolism in cancer patients: an underestimated major
Anticoagulation for prevention of venous thromboembolism
 Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism
 Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
Once-Daily, Oral LIXIANA (edoxaban) Met Primary Endpoint in Investigational Hokusai-VTE CANCER Study
 Met Primary Endpoint in Investigational Hokusai-VTE CANCER Study") Once-Daily, Oral LIXIANA (edoxaban) Met Primary Endpoint in Investigational Hokusai-VTE CANCER Study Hokusai-VTE CANCER study is a phase 3b, prospective, randomised, open-label, blind end-point (PROBE)
Once-Daily, Oral LIXIANA (edoxaban) Met Primary Endpoint in Investigational Hokusai-VTE CANCER Study Hokusai-VTE CANCER study is a phase 3b, prospective, randomised, open-label, blind end-point (PROBE)
Cancer Associated Thrombosis Review and Update. Family Practice Oncology CME Day November 21 st 2015 Erica Peterson
 Cancer Associated Thrombosis Review and Update Family Practice Oncology CME Day November 21 st 2015 Erica Peterson Disclosures No conflicts of interest to declare Objectives To review evidence in cancer-associated
Cancer Associated Thrombosis Review and Update Family Practice Oncology CME Day November 21 st 2015 Erica Peterson Disclosures No conflicts of interest to declare Objectives To review evidence in cancer-associated
TRANSPARENCY COMMITTEE OPINION. 18 April 2007
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 April 2007 ARIXTRA 2.5 mg/0.5 ml, solution for injection in prefilled syringe Pack of 2 (CIP: 359 225-4) Pack of
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 April 2007 ARIXTRA 2.5 mg/0.5 ml, solution for injection in prefilled syringe Pack of 2 (CIP: 359 225-4) Pack of
Expanding the treatment options of Superficial vein thrombosis with Rivaroxaban
 Expanding the treatment options of Superficial vein thrombosis with Rivaroxaban Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Expanding the treatment options of Superficial vein thrombosis with Rivaroxaban Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Acute and long-term treatment of PE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Effectiveness and Safety of Direct Oral Anticoagulants and Warfarin Among Patients with Sickle Cell Disease: A Retrospective Cohort Study
 Effectiveness and Safety of Direct Oral Anticoagulants and Warfarin Among Patients with Sickle Cell Disease: A Retrospective Cohort Study Megan Roberts, PharmD, BCPS MUSC Medical Center and South Carolina
Effectiveness and Safety of Direct Oral Anticoagulants and Warfarin Among Patients with Sickle Cell Disease: A Retrospective Cohort Study Megan Roberts, PharmD, BCPS MUSC Medical Center and South Carolina
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Venous Thromboembolism Prophylaxis: Checked!
 Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
Venous Thromboembolism Prophylaxis: Checked! William Geerts, MD, FRCPC Director, Thromboembolism Program, Sunnybrook HSC Professor of Medicine, University of Toronto National Lead, VTE Prevention, Safer
Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital Foundation Trust
 MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Venous Thromboembolism (VTE) Prevention
 Prevention") Venous Thromboembolism (VTE) Prevention 7 VTE Risk Assessment: General Patient Population Assess VTE risk at admission, post-op, and transfer See page 2 for VTE risk assessment among Obstetrical (OB) patients
Venous Thromboembolism (VTE) Prevention 7 VTE Risk Assessment: General Patient Population Assess VTE risk at admission, post-op, and transfer See page 2 for VTE risk assessment among Obstetrical (OB) patients
DOACs in CAT. Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD
 DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Menopausal Hormone Therapy & Haemostasis
 Menopausal Hormone Therapy & Haemostasis The Haematologist Perspective Dr. Batia Roth-Yelinek Coagulation unit Hadassah MC Menopausal Hormone Therapy & Hemostasis Hemostatic mechanism Mechanism of estrogen
Menopausal Hormone Therapy & Haemostasis The Haematologist Perspective Dr. Batia Roth-Yelinek Coagulation unit Hadassah MC Menopausal Hormone Therapy & Hemostasis Hemostatic mechanism Mechanism of estrogen
Dr Fahad Al-Hameed MD, FCCP, FRCPC Consultant Intensivist & Pulmonologist Professor Asst. of Medicine/Critical Care KSAU-HS Deputy chairman,
 Dr Fahad Al-Hameed MD, FCCP, FRCPC Consultant Intensivist & Pulmonologist Professor Asst. of Medicine/Critical Care KSAU-HS Deputy chairman, Intensive Care Department, Director, Ambulatory Care Center
Dr Fahad Al-Hameed MD, FCCP, FRCPC Consultant Intensivist & Pulmonologist Professor Asst. of Medicine/Critical Care KSAU-HS Deputy chairman, Intensive Care Department, Director, Ambulatory Care Center
New Oral Anticoagulant Drugs in the Prevention of DVT
 New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
New Oral Anticoagulants Prevention and Treatment of DVT and PE
 New Oral Anticoagulants Prevention and Treatment of DVT and PE Grigoris T Gerotziafas Groupe de Thrombose Equipe de recherche ER2UPMC Interactions cellulaires tumorales et leur environnement et réponses
New Oral Anticoagulants Prevention and Treatment of DVT and PE Grigoris T Gerotziafas Groupe de Thrombose Equipe de recherche ER2UPMC Interactions cellulaires tumorales et leur environnement et réponses