accumulation the blood, marrow, lymph nodes, and spleen.
|
|
|
- Laurel Williams
- 6 years ago
- Views:
Transcription
1
2 Chronic Lymphocytic Leukemia
3 accumulation of mature-appearing appearing lymphocytes in the blood, marrow, lymph nodes, and spleen.
4 CLL cells are: monoclonal l B lymphocytes that express CD19. CD5, and CD23 weak or no expression of surface immunoglobulin (Ig), CD20, CD79b, and FMC7
5 incidence of CLL varies throughout the world, highest in North America and rare in the Far East
6 The disease is rare in young people the incidence id rises in the fourth decade d and continues to rise exponentially mean age at diagnosis being 69.6 years and >80% of patients being >60 years
7 PATHOPHYSIOLOGY
8 Predisposing Factors no firm evidence linking an occupational exposure infection in the etiology of this disease? family history of CLL or another lymphoproliferative disorder is a strong risk factor for CLL
9 1 in 10 patients with ihcll has a family history of CLL or another lymphoproliferative disorder 30-fold increase in the risk of CLL in first-degree relatives of patients with CLL 13 to 18% of first-degree relatives have a peripheral g p p blood CD5+ monoclonal B-cell lymphocytosis
10 Patients with familial l CLL are -10 years younger than those with sporadic CLL Anticipation may occur in familial CLL with affected children being 15 to 20 years younger than their parents at diagnosis
11 There is no consistency in the clinical i l features of affected members with familial CLL
12 the CLL cell is a memory B cell two forms of CLL Pregerminal other having traversed lymphocyte and the germinal center lacking mutations of the and containing IgVHgene mutations
13 Abnormalities in Apoptosis defect in apoptosis typifies CLL with the majority of cells being long-lived Non cycling and in Go there is a small fraction of replicating cells in the lymph nodes and marrow that is responsible for disease progression
14
15 Genomic Abnormalities Conventional cytogenetic proved difficult because CLL cells have a very low proliferative index clonal chromosomal abnormalities are detected in -50% of cases
16 Analysis by Conventional Cytogenetic The most common clonal l abnormality was trisomy 12 (36%) structural abnormalities of chromosome 13(20%) structural abnormalities of chromosome 14 ( 16%)
17 The 13q abnormalities usually involved a 13q14 deletion (site of the Rb gene)
18 patients with abnormal karyotyping had a worse prognosis than those with normal cytogenetic, trisomy 12 was usually seen in those 15% of cases with CLL variants, (CLL /PLL) or "atypical" CLL
19 those with chromosome 14 abnormalities had the worst prognosis 11q22-q23 deletion have been detected in 13% of patients these patients had disease progression and poor survival
20 Analysis by Fluorescence in Situ Hybridization most present-day studies use FISH to identify if and quantify the genetic defects in CLL Evaluation of 325 CLL patients for deletions of 6q21, 11q22-q23,13q14, and 17p13;
21 268 (82%) had abnormalities i dlti deletion 13q1414 being most frequent (55%) deletion 11q22-q23 q23 (18%) trisomy 12q13 (16%), deletion 17p13 (7%) deletion 6q21 (7%)
22
23 The median survival times 17 p deletion 32 months 11q22-q23 deletion 79 months trisomy 12q 114 months normal karyotype 111 months 13q deletion 133 months
24 deletion 13q as the only abnormality had similar survival to those with normal chromosomes only one third required therapy
25 Patient with 17p1313 or 11q22-q23 23 deletions Have the poorest survival, more marked lymphadenopathy splenomegaly, and are more likely to be symptomatic with night sweats and likely to be symptomatic with night sweats and weight loss
26 correlation between genomic abnormalities and presence of IgV/I gene mutations and alterations in cell morphology
27
28 Clonal Evolution additional i chromosomal abnormalities develop with disease progression 16 to 39% incidence of new or additional chromosomal abnormalities, which develop over several years from initial diagnosis
29 By FISH analysis, one quarter of patients will have the development of new abnormalities after 5 years particularly in patients who are ZAP-70-positive, CD 38 positive, and those with un mutated IgVH
30 patients with un mutated IVH IgVH have an increased risk ik of developing deletions of llq22-q23 q23 or 17p13, those with mutated IgVH develop deletions of 13q
31 treatment with ih fludarabine increases the expression of p53-dependent genes, increasing the risk of selecting out 17pl3-deleted cells 42% of fludarabine-resistant CLL patients have either p53 mutations or deletions
32 CLINICAL FINDINGS
33 most CLL patients are elderly l -10% of patients t are <50 years old the presenting features are similar regardless of age 70 to 80% of patients are diagnosed incidentally and 70 to 80% of patients are diagnosed incidentally and they have early-stage
34 The most frequent complaint is fatigue or a vague sense of being unwell Less frequently: enlarged nodes or the development of an infection is the initial complaint.
35 Fever and weight loss are uncommon at presentation but may occur with advanced and drug- resistant disease
36 Enlargement of the cervical and supraclavicular l nodes occurs more frequently than axillary or inguinal lymphadenopathy mild to moderate enlargement of the spleen splenic infarction is uncommon
37 Less common manifestations: i enlargement of the tonsils abdominal masses due to mesenteric or retroperitoneal lymphadenopathy skin infiltration.
38 Anemia: related to marrow replacement or autoimmune hemolysis and aplasia bruising or bleeding secondary to : thrombocytopenia, acquired von Willebrand disease, or an acquired inhibitor to factor VIII
39 paraneoplastic syndrome nephrotic syndrome, paraneoplastic pemphigus, or angioedema
40 LABORATORY FINDINGS
41 Peripheral Blood The median lymphocyte count at diagnosis is /ml, in most patients there is a continuous increase in the p lymphocyte count over time
42 In half >12 months for the lymphocyte count to double cyclic fluctuations of up to 50 x 109/L can occur in the lymphocyte counts of untreated patient in others, the count may remain stable for years
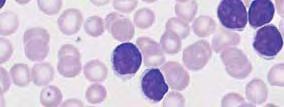
43 CLL cells: normal small to medium-sized i d lymphocytes clumped chromatin inconspicuous nucleoli small ring of cytoplasm
44 Smudge cells are commonly seen Appear to be caused by a decrease in vimentin Relationship between ~30% smudge cells And mutated IgVH and better prognosis than
45 French/American/British /B iti h classification Classical CLL: are small >90% of cells the cells are CLL/PLL: when 11 to 54% of e pro lymphocytes atypical CLL: >15% of the lymphocytes y are plasmoid or cleaved and <10% are prolymphocyts prolymphocytic leukemia: ~55% of the cells are pro lymphocytes,
46 There is always strong proliferation of the typical small lymphocytes, which are usually spread out diffusely.




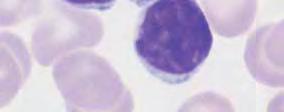
47 densely structured nuclei and little variation in CLL cells small cytoplasmic layer
48 Slightly eccentric enlargement of the cytoplasm in the lymphoplasmacytoid variant of CLL
49 large lymphocytes with irregularly l structured nucleus, well-defined nucleolus, and wide cytoplasm ( transitional form CLL/PLL)
50 Prolymphocytic leukemia of the T-cell series (T-PLL) with indented nuclei and nucleoli
51 Bone Marrow There are four patterns of marrow involvement in CLL Interstitial Nodular: the least common Mixed: most common Diffuse: effacement of the fat spaces by tumor, carries the worst prognosis
52 Immunophenotyping leukemic cells have the B-cell markers Cd19, Cd20 (low), Cd43, Cd79b (low), and, by definition, must be Cd5+ weak expression of sigm and sigd Cd23+ and Cd lo These cells are also Cd27+: Suggesting that these cells are memory B cells.
53 Recommendation for the use of five markers to differentiate t CLL from other B-cell malignancies Typical CLL should be: surface Ig (weak) Cd5+, Cd23+ Cd79b or Cd22 (weak) FMC7_
54 membrane Cd23 over expression is an activation marker may play a role in the decreased apoptosis observed in this disease is useful to differentiate CLL from mantle cell lymphoma
55 FMC7 is usually strongly expressed in hairy cell leukemia and prolymphocytic p y leukemia, 16% of CLL cases also stain positively those patients who are FMC7+have high levels of Surface IgM, low expression of Cd23, and poor prognosis
56 The Cd 5 antigen is most commonly associated with mature T cells and is expressed weakly on thymocytes Normal B cells carrying the CD 5 marker are located in the mantle zone of the lymph node, and in the peripheral blood
57 The Cd5 molecule l has been appears to be involved in the activation of T lymphocytes function of Cd5 on the B cell remains unknown
58 studies suggested that 5% of cases of CLL could be Cd5- These cases were more likely to be FMC7+, Cd23-, Cd11b+, and Cd13+ and had a poor prognosis
59
60 A score of 4 or 5 had an accuracy of 97 percent for the diagnosis of CLL, while most of the other non- CLL B-cell lymph proliferative diseases had scores of zero to two
61
62 Approximately 50% of patients had >30% Cd38+ cells, and these patients had un mutated IgVh and had a worse prognosis than those with <30% Cd38+ cells
63 Cd 38 acts as a receptor and enzyme and can produce cell replication and survival with a variety of signals Activation of Cd38+ cells, through slgm induces apoptosis and through IgD prolongs cell survival and induces differentiation
64 Cd38 can be measured easily by flow cytometry disagreement about the number of cells that are required to define positivity, with values ranging from 5 to 30% Moreover, the number of Cd38-positive cells can vary over time
65 ZAP-70 is a member of the Syk-ZAP-70 SkZAP protein ti kinase family is expressed in T and natural killer cells Is important in T-cell signaling recent evidence suggests that normal B cells may also express ZAP-70, particularly when activated
66 Gene expression studies in CLL have demonstrated that cells with unmutated IgVu have increased expression of ZAP to 90 % correlation between ZAP-70 expression and IgVh mutational status, whether ZAP-70 was measured by flow cytometry (>20% cells positive), Western blot analysis, or immunohistochemistry
67 ZAP-70 positivity iii correlates the presence of poor-risk cytogenetic, del llq22-q23, del and trisomy 12 and del 17 P13 unlike Cd38, the ZAP-70 status appears stable over time
68 Functional Immune Abnormalities 80% of patients have recurrent infections i sepsis being bi the major cause of death
69 CLL patients are susceptible to: typical bacterial infections opportunistic infections particularly if they have opportunistic infections, particularly if they have received nucleoside analogs or monoclonal antibodies
70 hypogammaglobulinemia li i is The major cause of infection, CLL patients also have abnormalities in T cells, complement, and neutrophil function
71 Hypogammaglobulinemia and agammaglobulinemia the severity increases with the duration and stage of disease The Ig levels are all decreased within the IgG class, reduced levels of IgG2 and IgG4 Correlate best with the risk of infection the decline in IgA levels is the most important predictor of infection
72 pathogenesis of the hypogammaglobulinemi: impaired B-cell function regulatory abnormalities of T cells suppress Ig secretion by normal B cells in vitro by CLL-derived natural killer (NK) cells
73 inversion i of the Thl T-helper to -suppressor cell ratio increase in the number of T-suppressor cells may correlate with the degree of hypogammaglobulinemia decreased T-helper function abnormality in abnormality in the large granular lymphocyte population
74 levels l of different complement components are decreased multiple defects in neutrophil function have been described
75 Autoimmune Manifestations CLL is the most common cause of autoimmune hemolytic anemia, causing 14% of cases 4to 25% of CLL patients develop AIHA with a warm-type antibody against the Rhesus system
76 the incidence id is higher hih in : Men, lymphocyte > and >60 years old
77 Immune thrombocytopenia t (ltp) occurs in 2% of patients t the diagnosis is based on increase in platelet size In the PBS and an increase in megakaryocytes in the marrow approximately one third of these patients with ITP have a positive Coombs test
78 Whether h autoimmune neutropenia occurs in CLL is unclear Pure red cell aplasia occurs in -1 % of cases and may Pure red cell aplasia occurs in -1 % of cases and may be caused by a T-cell mechanism
79 Nephrotic syndrome related to membranous or membranoproliferative acquired angioedema autoimmune blistering skin diseases
80 DIAGNOSIS
81 peripheral blood lymphocyte count >5 x 109 <55% of the cells being atypical Bcell specific differentiation antigens (CD19, CD20, and CD23) and be CD5+ bone marrow aspirate showing >30% lymphocytes y
82 INVESTIGATIONS AND STAGING
83 investigations complete blood count, review of the peripheral smear, and immunophenotyping are required for diagnosis
84 A marrow aspirate/ biopsy is not required for diagnosis but may be useful under the following circumstances: to establish the cause of anemia and thrombocytopenia for patients with Rai stage III or IV disease To confirm that there is no paratrabecular localization or cyclin Dl staining in atypical cases To assess the pattern of marrow infiltration, which is of prognostic value To assess response following chemotherapy
85 reticulocyte count Coombs test, renal and liver function tests LDH, serum protein electrophoresis and/or immunoelectrophoresis, and Ig levels. The plasma B-microglobulin level as this is a simple and important prognostic marker and an indicator of response to therapy
86 A baseline chest radiograph computed tomograph (CT) scans of the chest and abdomen will depend on clinical indications Positron emission tomography (PET) scans are not useful for staging in CLL Before starting chemotherapy screen for active viral infections (hepatitis Band C, cytomegalovirus)
87 Staging The Rai staging system is generally used in North America 7
88
89
90 several points should be made The staging is based on clinical i l examination i and not on CT scans patients with autoimmune cytopenia have a better prognosis than patients with cytopenia related to marrow packing The diagnosis of CLL was originally based on typical cell morphology peripherallymphocytosis
91 PROGNOSIS Ri Rai and Binet Staging the median survival of patients with stage A disease or in the low-risk group is > 10 years 40% of these patients will progress to a more advanced disease 50% of patients will require therapy at some point 25% will die from their diseas
92 Age and Sex 10% of CLL patients t are <50 years old clinical features and staging at presentation are similar To those > 50 years the proportion of deaths that can be attributed directly to CLL is greater for the younger age group
93 The male-to-female l ratio for CLL is 2:1 women are more likely l to have early-stage disease women have a better prognosis than men an increased incidence of IgVH mutated disease good prognostic genetic markers in women hormonal differences
94 lymphocyte Characteristics Morphology :20% of patients have atypical CLL or CLL/PLL more advanced stage. a higher h proliferative index trisomy 12 or deletion of 17p13 (p53 mutation). CD38+ aberrant cell morphology :an independent prognostic marker patients with >30% smudge cells have a better prognosis patients with >30% smudge cells have a better prognosis than with <30% smudge cells
95 Number Survival decreases with increasing lymphocyte count median survival is 8.6 years for a lymphocyte y count < years if the count is >40000
96 Doubling Time patients with a lymphocyte doubling time of <12 months have a significantly worse survival rate
97 Immune Markers increase in surface Igs,FMC7+, or increased intensity i of CD20 associated with atypical morphology trisomy 12 and poor prognosis
98 CD38+ has been associated with: shorter survival correlates with increasing Rai stage. intrathoracic and abdominal lymphadenopathy short doubling time increased,b2-microglobulin levels atypical morphology the CD38 status is useful to predict which patients within a particular clinical stage will progress
99 ZAP to 90% correlation between ZAp-70 expression and absence of IgVH mutations ZAP-70 positivity correlates moderately with CD38 positivity and the presence of poor-risk cytogenetics The median survivals for ZAP-70-positive and ZAP- 70-negative patients are 9.3 and 24.4 years
100 Molecular Genetics and Cytogenetics
101 p53 53, Ataxia Telangiectasia Mutation, Retinoblastoma Mutations ti of p53 :in 10 to 15% of patient t predictive of resistance to CTx The abnormality is associated with aberrant cell morphology and very poor survival ATM and Rb protein levels are reduced in 34 and 42% of patients these patients have advanced-stage disease and reduced survival
102 Marrow Histology Nodular growth patterns: 90 months interstitial titi growth patterns: 46months diffuse infiltration : median survival time of only 28 months Fibrosis of the marrow indicates an aggressive gg clinical course
103 The pattern of marrow involvement after chemotherapy is also prognostically important: nodular partial remission : persistent leukemia and have a shorter time to relapse compared to those in complete remission
104 Fludarabine Resistance Patients who do not respond to fludarabine or who relapse within 6 months of treatment have a median survival of 10 months with standard chemotherapy
105 Serum Markers Elevated B2microglobulin: i l b li predict resistance to chemotherapy Increased levels of LDH B2-microglobulin CD23, and TNF-a: patients who are at risk of disease progression.
106 TREATMENT one third of CLL patients never require therapy, one third need treatment as soon as they are seen, one third have disease progression over the years one third have disease progression over the years and require therapy at some point
107 With the possible exception of allogeneic hematopoietic i cell transplantation (HCT), CLL cannot be cured by current treatment options immediate versus delayed treatment strategies: no improvement in long-term survival with early treatment
108 indications to treat in CLL
109 Response Criteria and Minimal Residual Disease (MRD
110
111 MRD estimated that 25% of patients with a CR criteria will have MRD-positive disease same prognosis as those in PR? patients who achieve a marrow MRD-negative CR will have sustained remissions and perhaps improved survival
112 two-color (CD19/CD5) flowcytometry t to detect t MRD, with a sensitivity of one CLL cell in 1 x 10-2 leukocytes four-color (CD19/CD5/CD20/CD79b) flowcytometry can detect one CLL cell in 5 x 10-5 leukocytes new four-color (CD81/CD22/ CD19/CD5) flow - cytometry assay
113 ongoing studies are required to develop a simple and reproducible assay for MRD that can be used universally more intense treatments to achieve an MRD-negative Marrow?
114 Treatment options include purine analogs alkylating agents monoclonal antibodies combinations of these agents
115
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Prepared by: Dr.Mansour Al-Yazji
 C L L CLL Prepared by: Abd El-Hakeem Abd El-Rahman Abu Naser Ahmed Khamis Abu Warda Ahmed Mohammed Abu Ghaben Bassel Ziad Abu Warda Nedal Mostafa El-Nahhal Dr.Mansour Al-Yazji LEUKEMIA Leukemia is a form
C L L CLL Prepared by: Abd El-Hakeem Abd El-Rahman Abu Naser Ahmed Khamis Abu Warda Ahmed Mohammed Abu Ghaben Bassel Ziad Abu Warda Nedal Mostafa El-Nahhal Dr.Mansour Al-Yazji LEUKEMIA Leukemia is a form
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
CLL Biology and Initial Management. Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology
 CLL Biology and Initial Management Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology CLL- Epidemiology Most common adult leukemia 25-30% in western world Incidence in US 4.5
CLL Biology and Initial Management Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology CLL- Epidemiology Most common adult leukemia 25-30% in western world Incidence in US 4.5
Chronic Lymphocytic Leukemia Early Detection, Diagnosis, and Staging
 Chronic Lymphocytic Leukemia Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
Chronic Lymphocytic Leukemia Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Chronic Lymphocytic Leukemia (CLL)
") Page 1 of 10 PATIENT EDUCATION Chronic Lymphocytic Leukemia (CLL) Introduction Chronic lymphocytic leukemia (CLL) is a type of cancer of the lymphocytes (a kind of white blood cell). It is also referred
Page 1 of 10 PATIENT EDUCATION Chronic Lymphocytic Leukemia (CLL) Introduction Chronic lymphocytic leukemia (CLL) is a type of cancer of the lymphocytes (a kind of white blood cell). It is also referred
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Autoimmunity in CLL. Anne Silva, MD Hematology Fellows Conference
 Autoimmunity in CLL Anne Silva, MD Hematology Fellows Conference Case Presentation Mr. M is a 62 year old male with multiple medical problems including pulmonary sarcoidosis on steroids, was incidentally
Autoimmunity in CLL Anne Silva, MD Hematology Fellows Conference Case Presentation Mr. M is a 62 year old male with multiple medical problems including pulmonary sarcoidosis on steroids, was incidentally
CLL: disease specific biology and current treatment. Dr. Nathalie Johnson
 CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Global warming in the leukaemia microenvironment: Chronic Lymphocytic Leukaemia (CLL) Nina Porakishvili
 Nina Porakishvili") Global warming in the leukaemia microenvironment: Chronic Lymphocytic Leukaemia (CLL) Nina Porakishvili Working plan Case study; Epidemiology; Diagnosis; Immunobiology; Prognostication; Stratification
Global warming in the leukaemia microenvironment: Chronic Lymphocytic Leukaemia (CLL) Nina Porakishvili Working plan Case study; Epidemiology; Diagnosis; Immunobiology; Prognostication; Stratification
Investigation and Management of Chronic Lymphocytic Leukemia. James Johnston
 Investigation and Management of Chronic Lymphocytic Leukemia James Johnston Site Specific Clinics CLL Clinic (787-4454) Erin Elphee BN James Johnston Rajat Kumar Matt Seftel (transplant) Myeloma Clinic
Investigation and Management of Chronic Lymphocytic Leukemia James Johnston Site Specific Clinics CLL Clinic (787-4454) Erin Elphee BN James Johnston Rajat Kumar Matt Seftel (transplant) Myeloma Clinic
Chronic Lymphatic Leukemia Current Management Strategy
 Chronic Lymphatic Leukemia Current Management Strategy 463 80 Chronic Lymphatic Leukemia Current Management Strategy PK SASIDHARAN CHRONIC LYMPHATIC LEUKEMIA (CLL) CURRENT MANAGEMENT STRATEGY CLL is said
Chronic Lymphatic Leukemia Current Management Strategy 463 80 Chronic Lymphatic Leukemia Current Management Strategy PK SASIDHARAN CHRONIC LYMPHATIC LEUKEMIA (CLL) CURRENT MANAGEMENT STRATEGY CLL is said
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
How I treat CLL up front
 How I treat How I treat CLL up front John G. Gribben Institute of Cancer, Queen Mary University of London, Barts and The London School of Medicine and Dentistry, London, United Kingdom Although chronic
How I treat How I treat CLL up front John G. Gribben Institute of Cancer, Queen Mary University of London, Barts and The London School of Medicine and Dentistry, London, United Kingdom Although chronic
CLL Ireland Information Day Presentation
 CLL Ireland Information Day Presentation 5 May 2018 Professor Patrick Thornton Consultant Haematologist, Senior Lecturer RCSI, and Clinical Director Hermitage Medical Clinic Laboratory Chronic Lymphocytic
CLL Ireland Information Day Presentation 5 May 2018 Professor Patrick Thornton Consultant Haematologist, Senior Lecturer RCSI, and Clinical Director Hermitage Medical Clinic Laboratory Chronic Lymphocytic
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
Update: Chronic Lymphocytic Leukemia
 ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
This was a multicenter study conducted at 11 sites in the United States and 11 sites in Europe.
 Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Lymphatic system component
 Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Test Utilization: Chronic Lymphocytic Leukemia
 Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
CLL & SLL: Current Management & Treatment. Dr. Peter Anglin
 CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
Improving Response to Treatment in CLL with the Addition of Rituximab and Alemtuzumab to Chemoimmunotherapy
 New Evidence reports on presentations given at ASH 2009 Improving Response to Treatment in CLL with the Addition of Rituximab and Alemtuzumab to Chemoimmunotherapy From ASH 2009: Chronic Lymphocytic Leukemia
New Evidence reports on presentations given at ASH 2009 Improving Response to Treatment in CLL with the Addition of Rituximab and Alemtuzumab to Chemoimmunotherapy From ASH 2009: Chronic Lymphocytic Leukemia
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
GP CME. James Liang Consultant Haematologist. Created by: Date:
 GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
CELL-MEDIATED IMMUNITY
 LECTURE #4 1 LYMPHATIC SYSTEM 2 CELL-MEDIATED IMMUNITY T-lymphocytes (activated in the thymus) identify aggressors and try to destroy them through the production of lymphokines (synthesized proteins) Killer
LECTURE #4 1 LYMPHATIC SYSTEM 2 CELL-MEDIATED IMMUNITY T-lymphocytes (activated in the thymus) identify aggressors and try to destroy them through the production of lymphokines (synthesized proteins) Killer
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
The Lymphomas. An overview..
 The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
The Lymphomas An overview.. Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON The lymphomas are an important part of the history of medicine 1666 Magpighi publishes first recorded
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center
 LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
ACCME/Disclosures 4/13/2016. Clinical History
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
WBCs Disorders. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Multiple Myeloma 101: Understanding Your Labs
 Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Mathematical models of chronic lymphocytic leukemia
 Mathematical models of chronic lymphocytic leukemia Introduction to CLL Ibrutinib therapy understanding the kinetics Calculating personalized treatments Dominik Wodarz Department of Ecology and Evolutionary
Mathematical models of chronic lymphocytic leukemia Introduction to CLL Ibrutinib therapy understanding the kinetics Calculating personalized treatments Dominik Wodarz Department of Ecology and Evolutionary
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Volume 7, Issue 1 January 2012
 The Hong Kong College of Pathologists, Incorporated in Hong Kong with Limited Liability Volume 7, Issue 1 January 2012 Editorial note: Chronic lymphocytic leukaemia (CLL) is the commonest chronic lymphoproliferative
The Hong Kong College of Pathologists, Incorporated in Hong Kong with Limited Liability Volume 7, Issue 1 January 2012 Editorial note: Chronic lymphocytic leukaemia (CLL) is the commonest chronic lymphoproliferative
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Abstracting Hematopoietic Neoplasms
 CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
Neoplastic proliferation arising from white blood cells. Introductory remarks. Classification
 Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Primary Immunodeficiency
 Primary Immunodeficiency DiGeorge Syndrome Severe Combined Immunodeficiency SCID X-Linked Agammaglobulinemia Common variable immunodeficiency (CVID) IgA deficiency Hyper- IgM Syndrome Wiskott-Aldrich syndrome
Primary Immunodeficiency DiGeorge Syndrome Severe Combined Immunodeficiency SCID X-Linked Agammaglobulinemia Common variable immunodeficiency (CVID) IgA deficiency Hyper- IgM Syndrome Wiskott-Aldrich syndrome
Chronic Lymphocytic Leukemia Diagnosis and Management
 Chapter 2/Chronic Lymphocyte Leukemia 23 2 Chronic Lymphocytic Leukemia Diagnosis and Management Jamie D. Cavenagh, MD and T. Andrew Lister, MD CONTENTS INTRODUCTION EPIDEMIOLOGY ETIOLOGY CLINICAL AND
Chapter 2/Chronic Lymphocyte Leukemia 23 2 Chronic Lymphocytic Leukemia Diagnosis and Management Jamie D. Cavenagh, MD and T. Andrew Lister, MD CONTENTS INTRODUCTION EPIDEMIOLOGY ETIOLOGY CLINICAL AND
Blood Cell Identification: 2011-B Mailing: Acute Myeloid Leukemia (AML)
") Please Note: To view the Figures and Images contained within this education activity in color, access the electronic version of the reading. CASE HISTORY This peripheral blood smear is from a 51-year-old
Please Note: To view the Figures and Images contained within this education activity in color, access the electronic version of the reading. CASE HISTORY This peripheral blood smear is from a 51-year-old
Leukemias. Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
 Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
A heterogeneous collection of diseases characterised by hypogammaglobulinemia.
 1 Common variable immunodeficiency () A heterogeneous collection of diseases characterised by hypogammaglobulinemia. Although is the most common primary immune deficiency (PID) symptomatic in adults, it
1 Common variable immunodeficiency () A heterogeneous collection of diseases characterised by hypogammaglobulinemia. Although is the most common primary immune deficiency (PID) symptomatic in adults, it
MED B Form CLL. Johannes Schetelig. London 09/April/
 www.ebmt.org MED B Form CLL Johannes Schetelig London 09/April/2013 Content Update on CLL (15 ) Experiment with mini MED B CLL Assessment of pre-treatment in CLL Cytogenetics in CLL What is the IGVH-Gene
www.ebmt.org MED B Form CLL Johannes Schetelig London 09/April/2013 Content Update on CLL (15 ) Experiment with mini MED B CLL Assessment of pre-treatment in CLL Cytogenetics in CLL What is the IGVH-Gene
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Small, mature-appearing appearing
 B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Disclosures I have nothing to disclose. Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center,
B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Disclosures I have nothing to disclose. Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center,
CLL: What s New from ASH
 CLL: What s New from ASH John C. Byrd, MD D. Warren Brown Chair in Leukemia Research Professor of Medicine and Medicinal Chemistry Director, Division of Hematology The Ohio State University 2 Chronic Lymphocytic
CLL: What s New from ASH John C. Byrd, MD D. Warren Brown Chair in Leukemia Research Professor of Medicine and Medicinal Chemistry Director, Division of Hematology The Ohio State University 2 Chronic Lymphocytic
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL)
") Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
CLL what do I need to know as an Internist in Taimur Sher MD Associate Professor of Medicine Mayo Clinic
 CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
MS.4/ Acute Leukemia: AML. Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD
 MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Hematopathology Lab. Third year medical students
 Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Template for Reporting Results of Biomarker Testing of Specimens From Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma
 Template for Reporting Results of Biomarker Testing of Specimens From Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Version: CLLBiomarkers 1.0.0.2 Protocol Posting Date: June 2017
Template for Reporting Results of Biomarker Testing of Specimens From Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Version: CLLBiomarkers 1.0.0.2 Protocol Posting Date: June 2017
Outlines. Disclosures. Updates on B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow
 Updates on B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Sa A, Wang MD Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center, Houston,
Updates on B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Sa A, Wang MD Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center, Houston,
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Acute Myeloid Leukemia: A Patient s Perspective
 Acute Myeloid Leukemia: A Patient s Perspective Patrick A Hagen, MD, MPH Cardinal Bernardin Cancer Center Loyola University Medical Center Maywood, IL Overview 1. What is AML? 2. Who gets AML? Epidemiology
Acute Myeloid Leukemia: A Patient s Perspective Patrick A Hagen, MD, MPH Cardinal Bernardin Cancer Center Loyola University Medical Center Maywood, IL Overview 1. What is AML? 2. Who gets AML? Epidemiology
Younger patients with chronic lymphocytic leukemia benefit from rituximab treatment: A single center study in China
 1266 Younger patients with chronic lymphocytic leukemia benefit from rituximab treatment: A single center study in China ZHENSHU XU, JINYAN ZHANG, SHUNQUAN WU, ZHIHONG ZHENG, ZHIZHE CHEN and RONG ZHAN
1266 Younger patients with chronic lymphocytic leukemia benefit from rituximab treatment: A single center study in China ZHENSHU XU, JINYAN ZHANG, SHUNQUAN WU, ZHIHONG ZHENG, ZHIZHE CHEN and RONG ZHAN
Mantle-Cell Leukemia: Lessons in Life and Death
 Mantle-Cell Leukemia: Lessons in Life and Death James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation 60 y.o.
Mantle-Cell Leukemia: Lessons in Life and Death James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation 60 y.o.
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo
 Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
CHRONIC LYMPHOCYTIC LEUKEMIA
 CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: June, 2018 Copyright (2018) Alberta Health Services This material is protected by Canadian and other international copyright laws. All rights reserved. This
CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: June, 2018 Copyright (2018) Alberta Health Services This material is protected by Canadian and other international copyright laws. All rights reserved. This
Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto)
 and Dr. Matt Cheung (Staff Hematologist, University of Toronto)") CLL Updated March 2017 by Doreen Ezeife Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto) DISCLAIMER: The following
CLL Updated March 2017 by Doreen Ezeife Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto) DISCLAIMER: The following
The 1 World Congress on Controversies in Hematology (COHEM) Rome, September 2010
 Rome, September 2010") The 1 World Congress on Controversies in Hematology (COHEM) Rome, September 2010 Is the wait and watch philosophy still practical in the treatment of CLL even in younger patients? Expected to say NO Federico
The 1 World Congress on Controversies in Hematology (COHEM) Rome, September 2010 Is the wait and watch philosophy still practical in the treatment of CLL even in younger patients? Expected to say NO Federico
Acute Lymphoblastic Leukaemia
 Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology