Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
|
|
|
- Josephine Harrington
- 5 years ago
- Views:
Transcription

1 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1
2 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will be fine. Always remember that you are capable of doing more than what you think. Today is your day, so be the best that you could ever be. There are 2 parts to this tafreegh. The first is the lecture itself (15 pgs) and the second is a review from the book (7 pgs). Let s start! During the previous lectures, we discussed lymphomas. Lymphomas are tumors of mature lymphocytes. Leukemias can be either acute or chronic. Acute leukemia is a tumor of immature cells (blasts/proliferation of precursor cells). It is divided into myeloid and lymphoid. The defect of acute leukemia is within the bone marrow or the thymus (for T lymphoblastic leukemia, its maturation occurs in the thymus). Acute leukemia can have blasts in the bone marrow, and these immature cells can later pass on to the circulation (peripheral blood). The lesion in this type of leukemia is in the precursors/blasts. Chronic leukemia affects mature cells, involving partial maturation. In chronic myelogenous leukemia, the maturation of granulocytes over other lineages takes place. Polycythemia Vera involves the maturation of RBCs, leading to an increase in hemoglobin over other lineages (Partial maturation). In between, there is myelodysplastic syndrome (acute leukemia and chronic myeloproliferative neoplasm). Anything that affects the precursors will lead to acute leukemia. Anything that affects the mature cells is either lymphoma or chronic leukemia. 2
3 As we know, a normal myeloblast can divide and differentiate. The concept behind leukemia is that the myeloblast will not be able to differentiate to reach maturity. It may differentiate partially, or not at all. It s not able to complete all stages of maturation. For example, in myeloblastic leukemia, the predominant cell is the myeloblast. In promyelocytic leukemia, the predominant abnormal cell is the promyelocyte. These cells will not be able to differentiate into Neutrophils. Therefore, a patient with leukemia is most commonly seen with anemia, cytopenia, and neutropenia. The marrow is hypercellular, meaning that it is compacted with cells. However, there is no maturation. You have precursors, but no differentiation or maturation. The difference between a normal stem cell/myeloblast and a leukemic blast is that the normal stem cell can differentiate whereas the leukemic blast cannot. In the normal marrow, you shouldn t have more than 5% of stem cells. However in leukemia it can reach to 20-30% of abnormal blasts. So, in erythroblastic anemia, the majority of cells are erythroblasts. In monoblastic leukemia (acute myeloid leukemia), the majority of cells are monoblasts. All of these are acute myeloid leukemias because the myeloid lineage can give erythroid cells, megakaryocytes, monocytes, and neutrophils. 3
4 Myeloid / Lymphoid disorders Lymphoid: chronic or acute -Acute lymphoid leukemia: also known as: lymphoblastic leukemia (ALL) -Chronic lymphoid disorders: lymphomas, chronic lymphocytic leukemia, small lymphocytic lymphoma Myeloid: chronic or acute -Acute: more than 20% of the cells in the marrow are primitive cells (blasts) acute myeloid leukemia. -Chronic myeloproliferative neoplasm/myelodysplastic syndrome: less than 20% of cells in the bone marrow are blasts. (Partial differentiaton / maturation) Polycythemia vera, myelofibrosis, essential thrombocythemia are examples of chronic myeloproliferative disorders. Can a chronic myeloproliferative/myelodysplastic disorder transform into a higher stage acute leukemia? Yes. A patient may first have Polycythemia vera and 5% blasts (chronic). After a follow up, the patient may develop acute bone myeloid leukemia with more than 20% blasts. So this patient will be diagnosed with acute myeloid leukemia because the amount of blasts has increased to 20%. Remember, 20% is the magic number. In acute lymphoid leukemia (lymphoblastic leukemia), the number of blasts is not precise like in acute myeloid leukemia, but it is generally 30%. So more than 30% in the bone marrow this is acute lymphoblastic leukemia. Acute Myeloid Leukemia o There are subtypes within this leukemia. There are AMLs with recurrent genetic abnormalities, AMLs with features of myelodysplasia (compact disease), and AMLs that are therapy-related. o Sometimes, a patient with lymphoma who is treated with chemotherapy will develop cytopenia. In the marrow there are more 4

5 than 20% blasts, so the patient will have acute myeloid leukemia due to chemotherapy. So generally, patients with any cancer (colonic, breast, etc.) can develop leukemia from chemotherapy. This is what we call a therapy-related AML. o So far we ve mentioned 3 types of AML above. The last type of AML is one that does not have any of the above features. It does not fulfill the criteria of having genetic abnormalities, no features of myelodysplasia, and is not therapy- related. Let s say there is a patient who has an AML with recurrent genetic abnormalities, like translocations. If the amount of blasts is less than 20% would he be treated as AML or CML? We know this: AML: >20% blasts CML: <20% blasts BUT, in this case, even if the amount of blasts is below 20%, this patient would be treated as though he has AML because of the genetic abnormalities. Case: A year old patient was presented to you with cytopenia. What do you do? -CBC. -He is having symptoms of weakness, pallor, bleeding, fatigue, bruising. - Hemoglobin & platelet counts dropped Thrombocytopenia & anemia. - You do bone marrow biopsy and count the amount of blasts and it turns out 5
6 to be 10%. Is this acute? Well, we may think it is chronic because the amount of blasts is below 20%. But that doesn t stop there! Next, we must do a genetic study using cytogenetic or FISH analysis. The result shows that the patient has translocation (8; 21). In this case, you should treat the patient as if he has acute myeloid leukemia. - This is the significance of having subgroups for AML. If you find a translocation (genetic abnormality), but the blast count is less than 20%, you treat the patient as acute myeloid leukemia. The treatment and prognosis of AML differ from those of chronic myelogenous leukemia(cml) in part because the cellular differentiation is not the same; AML involves higher percentages of dedifferentiated and undifferentiated cells, including more blasts (myeloblasts, monoblasts, and megakaryoblasts). -Wikipedia The different subtypes of AML have varying prognoses. Those with AML of genetic abnormalities usually have a good prognosis. If AML is not specified, they will be classified according to their morphology. For specific types of AML, they are most preferably classified according to their cytogenetic abnormalities, not morphology. Morphology findings tend to be more subjective, whereas cytogenetic findings are more specific. When leukemias have normal cytogenetic findings, we can then classify them according to their morphology (erythroblastic/monoblastic leukemia). 6

.")
7 FAB (French American British) classification of acute myeloid leukemia: Classification of myeloproliferative neoplasm: If you have a patient with AML, the peripheral blood CBC should show cytopenia and a decrease in blood components. How can a clinician diagnose a patient with myeloproliferative neoplasm? By doing a CBC there should be cytosis in one lineage and cytopenia in another lineage. Case: Patient with chronic myelogenous leukemia CBC WBC count is 50,000 (high) Most of the cells are Neutrophils Patient may also have anemia or thrombocytopenia. In myeloproliferative neoplasm, there is a partial maturation (maturation of one lineage over other lineages). The first thing to do in any patient if you are suspecting myeloproliferative neoplasm is to look for Philadelphia chromosome t(9;22) Chronic Myelogenous Leukemia. Whenever the differential diagnosis is of a myeloproliferative disorder, you should rule out CML first (myeloproliferative spasm) by looking for t(9:22). CML has its own treatment, different from polycythemia vera and essential thrombocythemia. 7

 neoplasm: -Acute myeloid leukemia -Myeloid dysplastic syndromes in between, having features of acute leukemia and myeloid proliferative")
8 There are four main myeloproliferative diseases, which can be further categorized by the presence of the Philadelphia chromosome: -Wikipedia Myeloproliferative neoplasms are classified according to the presence/absence of the Philadelphia chromosome. If this chromosome is present CML. If this chromosome is absent Polycythemia Vera or Essential Thrombocythemia/thrombocytosis. Myelofibrosis then develops secondary to PV or ET. Myeloid (NON-lymphoid) neoplasm: -Acute myeloid leukemia -Myeloid dysplastic syndromes in between, having features of acute leukemia and myeloid proliferative neoplasms. -Chronic myeloproliferative disorders 8
9 Leukemia deals with precursors (B/T lymphoblastic leukemia). Leukemias may have double positivity or double negativity. For example, in T lymphoblastic leukemia, lymphoblasts are either CD4+/CD8+ or can be negative for both. For lymphomas, there is either CD4+ lymphoma or CD8+ lymphoma because lymphoma arises from mature cells whereas leukemia arises from immature cells. The stages of maturation starts with double negativity/positivity (immature) then in the peripheral blood there will be CD4+ OR CD8+ (mature). Antigens / markers expressed on cells allow us to differentiate between a mature and immature cell. Sometimes leukemia will look like lymphoma. So according to the markers of maturity, we can distinguish between them. Markers of immaturity: TdT (nuclear), CD 34 (cytoplasmic), CD 117 Blasts are positive for the myeloid-associated markers CD13, 14, CD15 or CD33, CD34 and negative for B or T lineage marker (CD3, CD10, CD19 and CD5). Taken from an online pdf, check it out! ~ ~ Lymphoid stem cells (primitive) found in the bone marrow produce lymphocytes. It expresses TdT, and CD 34 on the surface. However the mature cell does not have these markers (TdT, CD 34). Let s say you have a peripheral blood sample with a lesion. You look at the cells in the sample and see that they express CD34, CD19, and CD20. The cells are blasts (immature) and are abnormal because they re expressing mature and immature cells. So, this is lymphoblastic leukemia. * If it expresses CD34, CD19, CD20 B lymphoblast. * If it expresses CD4, CD8, CD3, TdT T lymphoblast. T & B lymphoblastic leukemia can t be easily differentiated from each other just by looking at them; so in conclusion, we look for markers of immaturity. CD 10,19, 20, 21, 22, 23 B cell markers CD 3, 4, 8, 5, 2, 7 T cell markers 9
10 CD3 a specific T cell marker. If you have a lymphocyte expressing CD3 and CD10, this is a T lymphocyte. CD3 is the only specific T cell marker. CD2 is not specific; it is seen on a T cell marker. CD5 is not specific because it is seen in both T and B lymphocytes (small subset of B cells mantle cells). Mantle cell lymphoma is CD5+. CD8 is a cytotoxic T cell. CD13, CD14, CD15 myeloid monocytic markers CD34 stem cell marker CD30 + in Hodgkin cells, Reed Sternberg cells, and activated B lymphocytes CD45 (+) common to all T / B lymphocytes, except Hodgkin cells (RS cells) *So when is CD45 (-)? In Hodgkin cells (RS cells) * CD45 is used when in this case: We take a biopsy from a patient, and the tumor looks poorly difffernetiated. Is it lymphoma, leukemia, or poorly differentiated carcinoma? Do CD 45. If the cells are positive for CD45, then it is a lymphoid neoplasm. * In conclusion, CD45 is a common lymphocyte marker. 10
11 11
12 If you are suspecting a patient with leukemia what should you do? First, start with taking a peripheral blood sample and a bone marrow biopsy. You find that cytopenia is very significant. You have to investigate this instead of just sending the patient home. You have a 6 year old presented to you with anemia: Hgb= 6 g/dl Platelet count = 50, 000 Do bone marrow biopsy. Peripheral blood: microcytic hypochromic anemia, no platelets. The lesion is in the bone marrow. The minimum requirements for someone with cytopenia are to do full blood count, bone marrow biopsy, and cytogenetic analysis. Take a bone marrow biopsy from the marrow of the patient. It is usually taken from the sternum or iliac crest in adults. This is done by using a needle and placing it within the marrow. The reason why we take a biopsy from these 2 bones is because the residual sites of the active marrow are found there. Biopsy from the sternum is more painful and has more complications than the iliac crest. After taking a sample, you aspire it with fluid (bone marrow aspirate). This will look like a peripheral blood sample but it actually represents the marrow. 2 Biopsies: 1. Bone marrow trephine needle biopsy aims at the bone, arrangement of cells, and the cellularity of the marrow. 2. The aspirate is just fluid, and examines the cells in thin spread. The details of the cells here are easier to examine and is used for flow cytometry. 12

 *This marrow (in the image) is")


13 The bone marrow is composed of adipose tissue and cells. This is important because you have to know the normal cellularity and the actual cellularity by examination. Normal cellularity = 100- age (+- 10) *This marrow (in the image) is normocellular for a 50 year old patient but hyper cellular for an 80 year old patient because the estimated cellularity shows that half of the marrow is fat and half of it is cells. So, this marrow is 50% cellular. So it is considered normocellular for a 50 year old. For an 80 year old, it s hyper cellular. 13



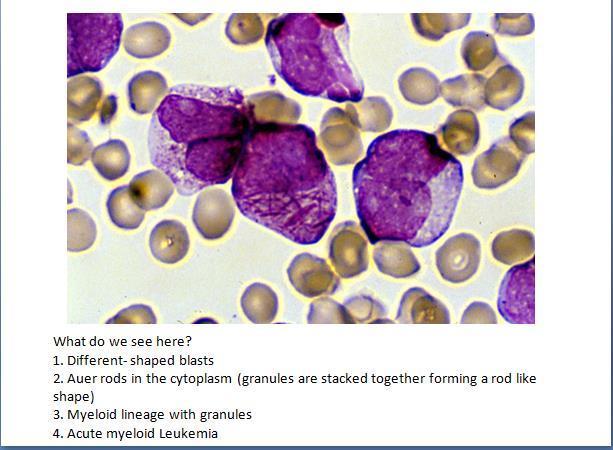
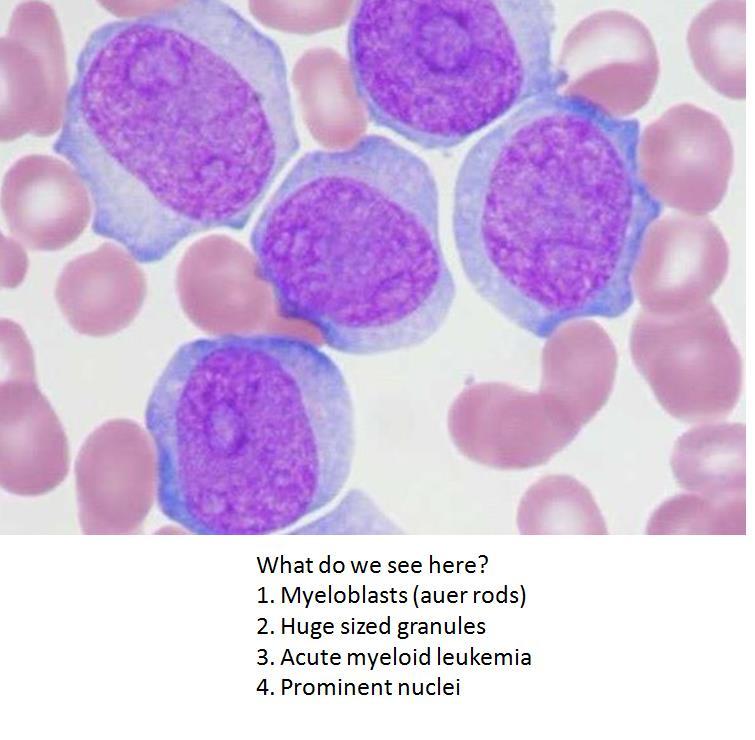
14 Leukemia has a 100% cellularity abnormal, regardless the age. So in this photo, the marrow is completely abnormal. This is seen in acute myeloid leukemia, myeloproliferative neoplasms, and myelodysplastic syndrome. In leukemia, the marrow is replaced by blasts (primitive cells). In a normal peripheral blood, there are RBC, platelets, and no precursors. You can see normal lymphocytes, and its size is almost 2x the RBC. It is round and smooth, and has a dark, clumped chromatin. Here, we see a blast. Normal lymphocytes are usually larger than RBCs by 2X. But here, its size is larger by 4-6X. The chromatin is not dark and is dispersed. Large amount of blasts in the blood and more than 20% in the bone marrow means that this is a lymphoblastic leukemia or acute myeloid leukemia. 14
15 15
16 16
17 Here, you ll find extra information from the book, for anyone who s interested. It s more of a review to all that was mentioned above. BOOK CORNER: ROBBINS: Pages Myeloid Neoplasms Arise from hematopoietic progenitors & give rise to clonal proliferations that replace the bone marrow. 3 categories: 1. Acute Myeloid Leukemia AML: Immature myeloid cells (blasts) accumulate in the marrow and replace normal elements; they frequently circulate the peripheral blood. 2. Myeloproliferative Disorders Neoplastic clone exhibits dysregulated growth. Involves the increase in formed elements (RBC / platelets / granulocytes) in the peripheral blood. 3. Myelodysplastic Disorders Disordered differentiation Dysplastic marrow precursors / peripheral blood cytopenias *Both myeloproliferative and myelodysplastic disorders can transform to Acute myeloid leukemia. *Some neoplasms have features of both myeloproliferative and myelodysplastic disorders. 17
18 Acute Myeloid Leukemia o Affects older adults (50 yrs.) o Closely resembles ALL & involves the replacement of the bone marrow elements with leukemic blasts. o Fatigue, pallor, abnormal bleeding, infections are symptoms in the newly diagnosed patients. o It is classified according to morphologic, histochemical, immunophenotypic, and karyoptypic findings. o Splenomegaly and lymphadenopathy occur to a lesser extent than in ALL. o AML is divided into 4 categories: - AMLs with genetic abberations - AMLs with dysplasia (which may arise from myelodysplastic syndromes) - AMLs occurring after genotoxic chemotherapy - AMLs without any of the above features. o Most tumors express a combination of myeloid associated antigens: CD13, CD14, CD15, CD64, CD117. o CD33 is expressed on pluripotent stem cells but is retained on myeloid progenitor cells. This marker distinguishes AML from ALL. 18



19 Myelodysplastic Syndromes o The bone marrow is replaced by the clonal progeny of a transformed multipotent stem cell that differentiates into red cells, granulocytes, and platelets. This occurs in an ineffective and disorderly manner. o Peripheral blood shows cytopenias. o The abnormal stem cell clone in the bone marrow is genetically unstable and can transform to AML. o Affects people within the ages of o Cytopenias may lead to anemias and hemorrhage. o It has a poor response to chemotherapy. 19

20 Chronic Myeloproliferative Disorders o Involves the hyperproliferation of neoplastic myeloid progenitors that can terminally differentiate. This results in an increase in the formed elements of the peripheral blood. o Hepatosplenomegaly o This disorder is associated with activating mutations in tyrosine kinases. o 4 diagnostic groups: Chronic myelogenous leukemia (CML), polycythemia vera, primary myelofibrosis, and essential thrombocythemia. o CML has an abnormality in the BCR-ABL fusion gene, producing an active BCR- ABL tyrosine kinase. 20
21 Chronic Myelogenous Leukemia Affects adults between ages It is always associated with the presence of a BCR-ABL fusion gene. (translocation 9;22) Fatigue, weakness, weight loss, splenomegaly What makes it distinct from other leukemias is the presence of the BCR- ABL fusion gene, which can be seen by karyotyping, FISH, or PCR assay. After some time, anemia, thrombocytopenia, cytogenicabnormalities, and the transformation into acute leukemia (blast crisis) may occur. This is the accelerated phase. Polycythemia Vera Excessive proliferation of erythroid, granulocytic, and megakaryocytic elements (panmyelosis). INCREASE IN RED CELL MASS / LOW LEVELS OF SERUM ERYTHROPOIETIN Increase in blood volume and viscosity Enlargement of liver and spleen Thromboses and infarctions are common in the heart, spleen, and kidneys. Hemorrhage abnormal platelet function. Usually occurs in the late middle age. Pruritus (itching), peptic ulceration, hypertension, headache, dizziness, GI symptoms, melena (GI bleeding), and hematemesis (vomiting of blood) are all symptoms. 21

22 Primary Myelofibrosis Extramedullary hematopoiesis (hematopoiesis in places outside the bone marrow like the spleen, liver, and lymph nodes. Splenomegaly and hepatomegaly This hematopoeisis is inefficient and disordered, leading to thrombocytopenia, anemia and neutropenia. Teardrop shaped red cells (poikilocytes) Nucleated erythroid precursors are present with immature white cells leukoerythroblastosis Primary Myelofibrosis 22
23 **SUMMARY - Myeloid Neoplasms** Myeloid tumors occur mainly in adults and fall into 3 major groups: Acute myeloid leukemias (AMLs) 1. Aggressive tumors comprised of immature myeloid lineage blasts, which replace the marrow and suppress normal hematopoiesis. 2. Associated with diverse acquired mutations that lead to expression of abnormal transcription factors, which interfere with myeloid differentiation. Myeloproliferative disorders 1. Increased production of formed myeloid elements, leading to high blood counts and extramedullary hematopoiesis. 2. Associated with mutations that activate tyrosine kinases, which mimic signals from normal growth factors. The most common pathogenic kinases are BCR-ABL & mutated JAK2. 3. All can transform to acute leukemia and to a spent phase of marrow fibrosis associated with anemia, thrombocytopenia, and splenomegaly. Myelodysplastic syndromes 1.Myeloid tumors characterized by disordered and ineffective hematopoiesis. 2. Manifest with 1 or more cytopenias and progress in 10% to 40% of cases to AML. Allow yourself to dream, And when you do, dream big. 23
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
2013 Pathology Student
 About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
WBCs Disorders. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
MYELOPROLIFARATIVE NEOPLASMS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
, FRCP(Edin).") MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم WBCs disorders *Slide 2: - we will focus on the disorders that are related to the # of WBCs - in children the # of lymphocyte is more than it in adults,sometimes more than neutrophils
بسم هللا الرحمن الرحيم WBCs disorders *Slide 2: - we will focus on the disorders that are related to the # of WBCs - in children the # of lymphocyte is more than it in adults,sometimes more than neutrophils
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
JAK2 V617F analysis. Indication: monitoring of therapy
 JAK2 V617F analysis BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
JAK2 V617F analysis BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
MPL W515L K mutation
 MPL W515L K mutation BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
MPL W515L K mutation BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Mixed Phenotype Acute Leukemias
 Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease
 The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
Blood Cell Identification: 2011-B Mailing: Acute Myeloid Leukemia (AML)
") Please Note: To view the Figures and Images contained within this education activity in color, access the electronic version of the reading. CASE HISTORY This peripheral blood smear is from a 51-year-old
Please Note: To view the Figures and Images contained within this education activity in color, access the electronic version of the reading. CASE HISTORY This peripheral blood smear is from a 51-year-old
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Leukemia and Myelodysplastic Syndromes
 Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
Neoplastic proliferation arising from white blood cells. Introductory remarks. Classification
 Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Hematopathology Case Study
 www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Flow Cytometry. Leukemia and Myelodysplastic Syndromes. Bone Marrow Aspirate and Biopsy
 Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Lenise Taylor, MN, RN, AOCNS, BMTCN BMT/Immunotherapy CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org History
Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Lenise Taylor, MN, RN, AOCNS, BMTCN BMT/Immunotherapy CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org History
Hematopathology Case Study
 Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
5/21/2018. Disclosures. Objectives. Normal blood cells production. Bone marrow failure syndromes. Story of DNA
 AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
Childhood Leukemia Early Detection, Diagnosis, and Types
 Childhood Leukemia Early Detection, Diagnosis, and Types Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
Childhood Leukemia Early Detection, Diagnosis, and Types Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Acute Lymphoblastic Leukaemia
 Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
رناد زكريا Dr. ahmad Dr. ahmad. P a g e 1
 5 رناد زكريا Dr. ahmad Dr. ahmad P a g e 1 Before we start. -This sheet was written according to section 2 s record and reviewed according to section 1 s record by Ruba Hussien with all thanks and I referred
5 رناد زكريا Dr. ahmad Dr. ahmad P a g e 1 Before we start. -This sheet was written according to section 2 s record and reviewed according to section 1 s record by Ruba Hussien with all thanks and I referred
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Peripheral Blood Smear: Diagnostic Clues and Algorithms
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Reactive and Neoplastic Lymphocytosis
 Reactive and Neoplastic Lymphocytosis Koranda A. Walsh, VMD, BS Assistant Professor, Clinical Pathobiology University of Pennsylvania School of Veterinary Medicine PLEASE NOTE: These notes are meant as
Reactive and Neoplastic Lymphocytosis Koranda A. Walsh, VMD, BS Assistant Professor, Clinical Pathobiology University of Pennsylvania School of Veterinary Medicine PLEASE NOTE: These notes are meant as
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Flow Cytometry. Bone Marrow Aspirate and Biopsy. Leukemia and Myelodysplastic Syndromes
 Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Elise Frans, MN, RN, CWON Oncology CNS University of Washington Medical Center delterzo@uw.edu 1 History & Physical Labs:
Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Elise Frans, MN, RN, CWON Oncology CNS University of Washington Medical Center delterzo@uw.edu 1 History & Physical Labs:
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
WHO Classification 7/2/2009
 Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Hematopathology Lab. Third year medical students
 Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Case #16: Diagnosis. T-Lymphoblastic lymphoma. But wait, there s more... A few weeks later the cytogenetics came back...
 Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
MYELOPROLIFERATIVE DISEASE. Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG
, MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG") MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
MS.4/ 1.Nov/2015. Acute Leukemia: AML. Abdallah Abbadi
 MS.4/ 1.Nov/2015. Acute Leukemia: AML Abdallah Abbadi Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising and hemorrhagic spots on her trunk
MS.4/ 1.Nov/2015. Acute Leukemia: AML Abdallah Abbadi Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising and hemorrhagic spots on her trunk
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Bone marrow histopathology in Ph - CMPDs. - the new WHO classification - Juergen Thiele Cologne, Germany
 Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Adult Acute leukemia. Matthew Seftel. August
 Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study
 Original Research Article Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study Priyanka Poonam 1*, N.K. Bariar 2 1 Tutor, Department of Pathology, Patna Medical
Original Research Article Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study Priyanka Poonam 1*, N.K. Bariar 2 1 Tutor, Department of Pathology, Patna Medical
Disorders of Blood Cells & Blood Coagulation
 Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor
: Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor") HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
Leukemias and Lymphomas Come From Normal Blood Cells
 Leukemias and Lymphomas Come From Normal Blood Cells by Steve Anderson, Ph.D. Steve Anderson has a Ph.D. in Immunology with 25 years experience in biomedical research. His scientific expertise includes
Leukemias and Lymphomas Come From Normal Blood Cells by Steve Anderson, Ph.D. Steve Anderson has a Ph.D. in Immunology with 25 years experience in biomedical research. His scientific expertise includes
When Cancer Looks Like Something Else: How Does Mutational Profiling Inform the Diagnosis of Myelodysplasia?
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
BLASTIC CRISIS AND MYELOFIBROSIS SIMULTANEOUS COMPLICATIONS IN A CASE OF CHRONIC MYELOCYTIC LEUKEMIA
 BLASTIC CRISIS AND MYELOFIBROSIS SIMULTANEOUS COMPLICATIONS IN A CASE OF CHRONIC MYELOCYTIC LEUKEMIA Abstract Pages with reference to book, From 151 To 153 Khalid Hassan ( Department of Pathology (Haematology)
BLASTIC CRISIS AND MYELOFIBROSIS SIMULTANEOUS COMPLICATIONS IN A CASE OF CHRONIC MYELOCYTIC LEUKEMIA Abstract Pages with reference to book, From 151 To 153 Khalid Hassan ( Department of Pathology (Haematology)
MS.4/ Acute Leukemia: AML. Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD
 MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
HASNA NADIA BT. HASAN SAZALLI JOSEPHIN SUZANA A/K JOHN ASIN LOW NORZUFIKAL BT. ZULKIFLY NURUL ALIYA BT ROSLAN MOHD SYAFFIQ BIN OTHMAN
 HASNA NADIA BT. HASAN SAZALLI JOSEPHIN SUZANA A/K JOHN ASIN LOW NORZUFIKAL BT. ZULKIFLY NURUL ALIYA BT ROSLAN MOHD SYAFFIQ BIN OTHMAN Anatomy of Bone Marrow Syaffiq Othman Bone Marrow Bone marrow is a
HASNA NADIA BT. HASAN SAZALLI JOSEPHIN SUZANA A/K JOHN ASIN LOW NORZUFIKAL BT. ZULKIFLY NURUL ALIYA BT ROSLAN MOHD SYAFFIQ BIN OTHMAN Anatomy of Bone Marrow Syaffiq Othman Bone Marrow Bone marrow is a
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES COPYRIGHTED MATERIAL SECOND EDITION
 VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
VETERINARY HEMATOLOGY ATLAS OF COMMON DOMESTIC AND NON-DOMESTIC SPECIES SECOND EDITION COPYRIGHTED MATERIAL CHAPTER ONE HEMATOPOIESIS GENERAL FEATURES All blood cells have a finite life span, but in normal
Acute Lymphoblastic and Myeloid Leukemia
 Acute Lymphoblastic and Myeloid Leukemia Pre- and Post-Disease Form Acute Lympoblastic Leukemia Mary Eapen MD, MS Acute Lymphoblastic Leukemia SEER Age-adjusted incidence rate 1.6 per 100,000 men and women
Acute Lymphoblastic and Myeloid Leukemia Pre- and Post-Disease Form Acute Lympoblastic Leukemia Mary Eapen MD, MS Acute Lymphoblastic Leukemia SEER Age-adjusted incidence rate 1.6 per 100,000 men and women
Leukemia and Myelodysplastic Syndromes
 Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS, BMTCN Oncology CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org Lymphoid 1 Myeloid 2 Diagnostic Evaluation of Blood Disorders
Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS, BMTCN Oncology CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org Lymphoid 1 Myeloid 2 Diagnostic Evaluation of Blood Disorders
Morfologia normale e patologica
 Morfologia normale e patologica Gina Zini Centro di Ricerca ReCAMH Dpt. Ematologia Università Cattolica S. Cuore - Roma EMATOLOGIA DI LABORATORIO: percorsi diagnostici e obiettivi clinici. Milano 11-12
Morfologia normale e patologica Gina Zini Centro di Ricerca ReCAMH Dpt. Ematologia Università Cattolica S. Cuore - Roma EMATOLOGIA DI LABORATORIO: percorsi diagnostici e obiettivi clinici. Milano 11-12
Primary myelofibrosis
 - It s a bone marrow fibrosis Primary myelofibrosis - It's type of myeloproliferative disease i.e. neoplastic proliferation of mature cell of myloid linage. - Its similar to chronic myloid leukemia (CML).
- It s a bone marrow fibrosis Primary myelofibrosis - It's type of myeloproliferative disease i.e. neoplastic proliferation of mature cell of myloid linage. - Its similar to chronic myloid leukemia (CML).
Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML
 reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Ordering Physician CLIENT,CLIENT. Collected REVISED REPORT
 HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Formation of Blood Cells
 Hematopoiesis Lecture Objectives Name organs responsible for hematopoiesis in the fetus. List the developmental stages of hematopoiesis both prenatally and postnatally. Outline the major steps of post
Hematopoiesis Lecture Objectives Name organs responsible for hematopoiesis in the fetus. List the developmental stages of hematopoiesis both prenatally and postnatally. Outline the major steps of post
Chronic Myelomonocytic Leukemia with molecular abnormalities SH
 Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone