LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
|
|
|
- Poppy Rogers
- 6 years ago
- Views:
Transcription
1 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University
2 OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish between Hodgkin and non-hodgkin lymphomas. Identify prognosis of leukemia and lymphoma. Interpret results of CBC, BM and radiology. Discuss treatment of leukemia and lymphoma.
3 Leukemia Definition: Leukemia is a group of malignant diseases in which genetic abnormalities in a hematopoietic cell give rise to unregulated clonal proliferation of cells. The result is a disruption of normal marrow function or marrow failure.
4 ETIOLOGY Unknown and is probably multi-factorial. Genetics and environmental factors: - CML a translocation bet. chromosome 9 and Increased risk in Down, Wiskott-Aldrich, Environmental factors e.g. ionizing radiation.
5 EPIDEMIOLOGY About 31% of childhood malignancy. Acute lymphoblastic leukemia (ALL): 75-80% Acute myeloid leukemia (AML): 15-20%. Chronic myeloid leukemia (CML): less than 5%. Chronic lymphocytic leukemia (CLL): not found in childhood.
6 Classification of Acute Lymphoblastic ACUTE LYMPHOBLASTIC LEUKEMIA (ALL): ALL-L1 morphology Precursor B-cell ALL ALL-L2 Precursor T-cell ALL. ALL B cell-l3 morphology (i.e., Burkitt's leukemia).
7 Classification of Acute Myeloid Leukemia ACUTE MYELOID LEUKEMIA (AML): (WHO) FAB (French-American-British) classification: AML (M0-M7).
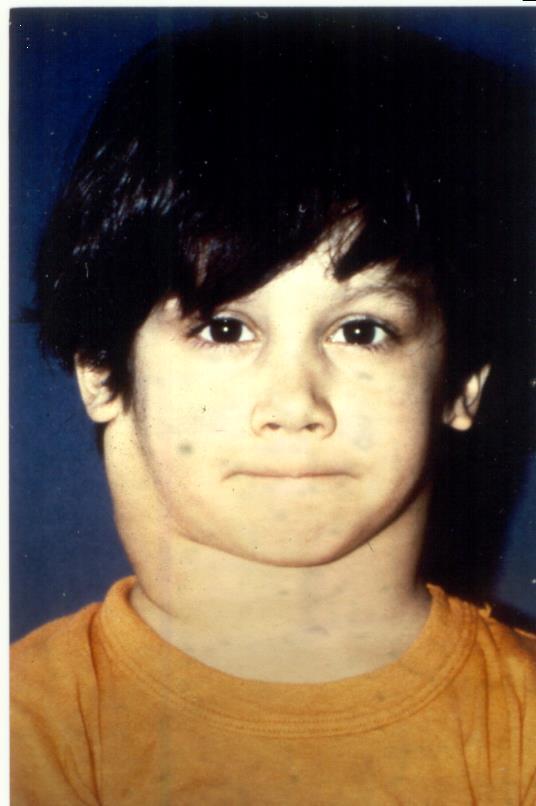
8 Clinical presentation General: fever, malaise, anorexia,.. Bone marrow infiltration: anemia, neutropenia and thrombocytopenia. Reticulo-endothelial infiltration: hepatosplenomegaly and lymphadenopathy. Other organ infiltration: CNS, testes also bone, skin, gingiva


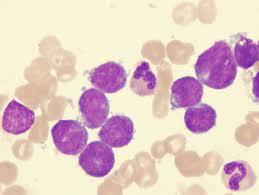

9
10 DIFFERENTIAL DIAGNOSIS Infection: Epstein-Barr virus, mycobacteria. Noninfectious: Aplastic anemia, JRA, SLE, ITP,.. Malignant diagnoses: lymphoma, neuroblastoma,.. Proliferation and accumulation of histiocytes e.g. Langerhans cell histiocytosis
11 LABORATORY AND IMAGING STUDIES CBC: low Hb and low plts are common. The WBC count (low, normal or high). The diagnosis is by finding of immature blast cells (blast morphology) on the peripheral blood smear or bone marrow aspirate (25%). Definitive diagnosis and typing requires the evaluation of cell surface markers (immunophenotype) by flow cytometry.
12 LABORATORY AND IMAGING cont. Cytogenetic analysis: Certain types have specific chromosomal abnormalities. A lumbar puncture to evaluate the possibility of CNS involvement. A chest x-ray to exclude an anterior mediastinal mass, which is commonly seen in T-cell ALL. Electrolytes, calcium, phosphorus, uric acid, and renal and hepatic function should be monitored in all patients.

13 Anterior mediastinal mass
14 Treatment of ALL Before starting treatment: Treat anemia, thrombocytopenia and infection. Hydration and allopurinol to protect renal function against tumour lysis syndrome.
15 Treatment of ALL Induction of remission: Eradication of the leukemic blasts and restoration of normal marrow function. Four weeks of 3-4 agents chemotherapy. Current induction achieve remission rates of 95%.
16 Treatment of ALL Consolidate remission: Blocks of intensive chemotherapy, but increased toxicity. CNS prophylaxis: Intrathecal chemotherapy to prevent CNS relapse.
17 Treatment of ALL Continuing maintenance therapy: Chemotherapy of modest intensity is continued up to 3 years from diagnosis. Co-trimoxazole is given routinely to prevent Pneumocystis carinii pneumonia.
18 Treatment of AML The treatment of AML different from ALL because: Non-myelosuppressive drugs (vincristine)not effective. The low-dose continuation therapy not helpful in AML. Induction is the most effective (two courses of drugs, 1 to 2 weeks apart) regardless of blood counts. Most experts recommend a stem cell transplantation in the first remission, except in Down syndrome and those with favorable cytogenetics.
19 General Prognostic Factors in ALL Based on: Age, initial WBC count, genetic characteristics, and response to induction therapy. Factor Age Gender Initial WBC count CNS or testicular disease at diagnosis Favorable (Lower Risk) years Females <50,000/mm 3 Absent Unfavorable (higher risk) <1 or 10 years Males 50,000/mm 3 Present Cytogenetic Response to therapy t(12;21) Rapid t(4;11), t(9;22) Slow
20 PROGNOSIS The overall cure rate for: 1- ALL 80%. Relapse occurs most commonly in the bone marrow, also in CNS, testes, 2- AML 50%. The prognosis for relapsed AML is poor.
21 Pediatric Lymphomas
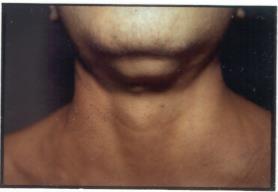
22 Cervical adenopathy
23 HODGKINS LYMPHOMA NON-HODGKINS (40%) (60%) LARGE CELL LYMPHOMA IMMUNOBLASTIC ANAPLASTIC LYMPHOBLASTIC LYMPHOMA BURKITT S LYMPHOMA (<15%) (30-40%) (40-50%) (50%) (50%)
24 NON-HODGKINS (NHL) Incidence/Etiology: 6% childhood cancer 60% of childhood lymphomas Peak age of 5-15; M:F ratio of 2.5:1 Increased with SCIDS, HIV, EBV post t-cell depleted BMT post solid organ transplant Geographic, viral, genetic & immunologic factors
25 Clinical Presentations Abdomen: (35%): pain, distention, jaundice, GI problems, mass. Head/neck (13%): lymphadenopathy, jaw swelling, single enlarged tonsil, nasal obstruction, rhinorrhea, Mediastinum (26%): SVC syndrome. CNS (rare): Headache, Vom., irritability, papilledema. + Fever, malaise, night sweats, wt. loss,
26 Prognosis **Unfavorable: Incomplete remission in first 2 months of treatment. Large tumor burden (LDH >1000). Stages III and IV: CNS or BM involvement. Relapse. **More favorable: Stage I or II, head/neck, peripheral nodes, GI tract.
27 NHL Treatment Surgery; for diagnostic or second look. Radiation Therapy: emergency airway obstruction or CNS complication or local control of residual mass. Chemotherapy: Combination chemo is usual, with overall cure rates %; high risk of tumor lysis and hyperuricemia. Relapse: Re-induction, followed by BMT
28 Hodgkin s Disease Immune system malignancy, involving B or T lymphocytes. Reed-Sternberg cells. Spread: slow, predictable, with extension to contiguous lymph nodes. Infiltration to non-lymphoid organs is rare.

29 Hodgkin s disease with Reed Sternberg cell
30 Incidence and Etiology Hodgkin s 5% of childhood cancers Bimodal peaks, at and >50; rare < 5 M:F ratio of 3:1 Increased in immunologic disorders, HIV, EBV
31 Types of Hodgkin s Lymphoma Nodular sclerosing: 40-60%, lower cervical, supraclavicular, mediastinal nodes. Mixed cellularity: 15-30%; advanced disease with extranodal involvement. Lymphocyte predominance: 5-15%, presents as localized disease. Lymphocyte depletion: <5%, widespread disease
32 Clinical Presentation Painless lymph node swelling; supraclavicular and cervical nodes (90%). Palpable non-tender, firm, mobile, rubbery nodes. Mediastinal adenopathy (60%); SVC Bulky: when mass is > 1/3 thorax diameter B symptoms: Fever of >38 C for 3 days, drenching night sweats, 10% weight loss within 6months.
33 I II III Hodgkin s Ann Arbor Staging Single lymph node region Two+ node regions on same side of diaphragm Nodes on both sides of diaphragm, or localized extra-lymphatic spread IV Diffuse or disseminated involvement of one+ extra-lymphatic organs or tissues
34 Prognosis FAVORABLE: <10, F, favorable subtypes (LP and NS) and Stage I non-bulky disease UNFAVORABLE: Persistently elevated ESR; LD histopathology; bulky disease--largest dimension >10cm; B symptoms;
35 Treatment and Prognosis Dependent on age, stage, and tumor burden Radiotherapy (RT) alone, Chemotherapy (CTX) alone. RT: varies from involved field for localized disease to extended field to total nodal irradiation. Most often multimodal therapy, with low-dose involved field RT and multi-agent CTX. Combined modality 70-90% cure.
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
WHAT ARE PAEDIATRIC CANCERS
 WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Easy Trick to Spot Leukemia for Pediatricians
 Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Leukemias. Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
 Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Lymphatic system component
 Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
Introduction Lymphatic system component Statistics Overview Lymphoma Non Hodgkin s Lymphoma Non- Hodgkin's is a type of cancer that originates in the lymphatic system. It is estimated to be the sixth most
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center
 LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
Leukemia and Myelodysplastic Syndromes
 Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
MS.4/ Acute Leukemia: AML. Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD
 MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Lymphatic System Disorders
 Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Aggressive Lymphomas - Current. Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre
 Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Pediatric cancer. Kleebsabai Sanpakit, MD. Hemato/Oncology division, Department of Pediatrics Faculty of Medicine Siriraj hospital
 Pediatric cancer เทคน คการให รห สโรค Siriraj Cancer ICD-O Registry ฉบ บม ออาช พ Kleebsabai Sanpakit, MD. Hemato/Oncology division, Department of Pediatrics Faculty of Medicine Siriraj hospital Different
Pediatric cancer เทคน คการให รห สโรค Siriraj Cancer ICD-O Registry ฉบ บม ออาช พ Kleebsabai Sanpakit, MD. Hemato/Oncology division, Department of Pediatrics Faculty of Medicine Siriraj hospital Different
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162
 Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162 Definition Pathophysiology Clinical signs and symptoms Biology and Diagnosis Different types of AL Prognosis and Treatment Malignant
Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162 Definition Pathophysiology Clinical signs and symptoms Biology and Diagnosis Different types of AL Prognosis and Treatment Malignant
Flow Cytometry. Leukemia and Myelodysplastic Syndromes. Bone Marrow Aspirate and Biopsy
 Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Lenise Taylor, MN, RN, AOCNS, BMTCN BMT/Immunotherapy CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org History
Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Lenise Taylor, MN, RN, AOCNS, BMTCN BMT/Immunotherapy CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org History
PEDIATRIC MALIGNANCIES
 PEDIATRIC MALIGNANCIES Martin Brecher, MD Roswell Park Cancer Institute Women & Children s Hospital of Buffalo! Oncology for Scientists Epidemiology 10% of childhood deaths, most common cause of death
PEDIATRIC MALIGNANCIES Martin Brecher, MD Roswell Park Cancer Institute Women & Children s Hospital of Buffalo! Oncology for Scientists Epidemiology 10% of childhood deaths, most common cause of death
Flow Cytometry. Bone Marrow Aspirate and Biopsy. Leukemia and Myelodysplastic Syndromes
 Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Elise Frans, MN, RN, CWON Oncology CNS University of Washington Medical Center delterzo@uw.edu 1 History & Physical Labs:
Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Elise Frans, MN, RN, CWON Oncology CNS University of Washington Medical Center delterzo@uw.edu 1 History & Physical Labs:
1 Introduction. 1.1 Cancer. Introduction
 Introduction 1 1.1 Cancer 1 Introduction Cancer is the most precarious disease characterized by uncontrolled proliferation of cells without any physiological demands of the organism. Cancer may be defined
Introduction 1 1.1 Cancer 1 Introduction Cancer is the most precarious disease characterized by uncontrolled proliferation of cells without any physiological demands of the organism. Cancer may be defined
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
Relapsed acute lymphoblastic leukemia. Lymphoma Tumor Board. July 21, 2017
 Relapsed acute lymphoblastic leukemia Lymphoma Tumor Board July 21, 2017 Diagnosis - Adult Acute Lymphoblastic Leukemia (ALL) Symptoms/signs include: Fever Increased risk of infection (especially bacterial
Relapsed acute lymphoblastic leukemia Lymphoma Tumor Board July 21, 2017 Diagnosis - Adult Acute Lymphoblastic Leukemia (ALL) Symptoms/signs include: Fever Increased risk of infection (especially bacterial
Lymphoma and Myeloma Kris3ne Kra4s, M.D.
 Lymphoma and Myeloma Kris3ne Kra4s, M.D. Hematologic Malignancies Leukemia Malignancy of hematopoie3c cells Starts in bone marrow, can spread to blood, nodes Myeloid or lymphoid Acute or chronic Lymphoma
Lymphoma and Myeloma Kris3ne Kra4s, M.D. Hematologic Malignancies Leukemia Malignancy of hematopoie3c cells Starts in bone marrow, can spread to blood, nodes Myeloid or lymphoid Acute or chronic Lymphoma
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
MANAGEMENT OF ACUTE LYMPHOBLASTIC LEUKEMIA. BY Dr SUBHASHINI 1 st yr PG DEPARTMENT OF PEDIATRICS
 MANAGEMENT OF ACUTE LYMPHOBLASTIC LEUKEMIA BY Dr SUBHASHINI 1 st yr PG DEPARTMENT OF PEDIATRICS Introduction The management of ALL, the most common childhood malignancy (1/3 rd of all malignancy), has
MANAGEMENT OF ACUTE LYMPHOBLASTIC LEUKEMIA BY Dr SUBHASHINI 1 st yr PG DEPARTMENT OF PEDIATRICS Introduction The management of ALL, the most common childhood malignancy (1/3 rd of all malignancy), has
Leukemia and Myelodysplastic Syndromes
 Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS, BMTCN Oncology CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org Lymphoid 1 Myeloid 2 Diagnostic Evaluation of Blood Disorders
Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS, BMTCN Oncology CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org Lymphoid 1 Myeloid 2 Diagnostic Evaluation of Blood Disorders
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Oncology
 Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Oncology - Introduction: Cancer is the most common cause of death from diseases in childhood but notice that most of
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Oncology - Introduction: Cancer is the most common cause of death from diseases in childhood but notice that most of
Low grade High grade , immune suppression chronic persistent inflammation viruses B-symptoms
 We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
Acute Lymphocytic Leukemia Early Detection, Diagnosis, and Types
 Acute Lymphocytic Leukemia Early Detection, Diagnosis, and Types Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
Acute Lymphocytic Leukemia Early Detection, Diagnosis, and Types Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
Hodgkin's Lymphoma. Symptoms. Types
 Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Hodgkin's lymphoma (Hodgkin's disease) usually develops in the lymphatic system, a part of the body's immune system. This system carries disease-fighting white blood cells throughout the body. Lymph tissue
Neoplastic proliferation arising from white blood cells. Introductory remarks. Classification
 Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Mantle-Cell Leukemia: Lessons in Life and Death
 Mantle-Cell Leukemia: Lessons in Life and Death James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation 60 y.o.
Mantle-Cell Leukemia: Lessons in Life and Death James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation 60 y.o.
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hematologic Malignancies. Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire
 Hematologic Malignancies Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire Objectives At the end of the session, the oncology nurse will be able to: Explain the pathophysiology
Hematologic Malignancies Anna Schaal, RN, MSN, arnp Norris Cotton Cancer Center Lebanon, New Hampshire Objectives At the end of the session, the oncology nurse will be able to: Explain the pathophysiology
Abstracting Hematopoietic Neoplasms
 CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
GOOD MORNING! July 3, 2014
 GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
MS.4/ 1.Nov/2015. Acute Leukemia: AML. Abdallah Abbadi
 MS.4/ 1.Nov/2015. Acute Leukemia: AML Abdallah Abbadi Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising and hemorrhagic spots on her trunk
MS.4/ 1.Nov/2015. Acute Leukemia: AML Abdallah Abbadi Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising and hemorrhagic spots on her trunk
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Cell Transplantation for Hodgkin Lymphoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_hodgkin_lymphoma
Corporate Medical Policy Hematopoietic Cell Transplantation for Hodgkin Lymphoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_hodgkin_lymphoma
 Page 1 of 9 Title Authored By Course No Contact Hours 2 ABCs of Lymphoma Anita Rothera RNC, BS, CDE LYM020108 Purpose The goal of this course is to help health care professionals learn about the different
Page 1 of 9 Title Authored By Course No Contact Hours 2 ABCs of Lymphoma Anita Rothera RNC, BS, CDE LYM020108 Purpose The goal of this course is to help health care professionals learn about the different
Adult Acute leukemia. Matthew Seftel. August
 Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
During past decades, because of the lack of knowledge
 Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
PROBLEMS OF THE HEMATOLOGICAL SYSTEM
 PROBLEMS OF THE HEMATOLOGICAL SYSTEM UNIT 5 Review A & P of Hematological system Outline focused exam Differentiate and start to evaluate diagnostic exams used to assess problems of the hematological system
PROBLEMS OF THE HEMATOLOGICAL SYSTEM UNIT 5 Review A & P of Hematological system Outline focused exam Differentiate and start to evaluate diagnostic exams used to assess problems of the hematological system
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Acute Lymphoblastic Leukaemia
 Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Lymphomas and multiple myeloma 12/23/2018 1
 60 Lymphomas and multiple myeloma 12/23/2018 1 Lymphomas Lymphoma is cancer of the lymphatic system. Lymphomas are subdivided into two main categories: Hodgkin's lymphoma (HL) and non- Hodgkin's lymphoma
60 Lymphomas and multiple myeloma 12/23/2018 1 Lymphomas Lymphoma is cancer of the lymphatic system. Lymphomas are subdivided into two main categories: Hodgkin's lymphoma (HL) and non- Hodgkin's lymphoma
Update in Lymphoma Imaging
 Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Acute Lymphoblastic and Myeloid Leukemia
 Acute Lymphoblastic and Myeloid Leukemia Pre- and Post-Disease Form Acute Lympoblastic Leukemia Mary Eapen MD, MS Acute Lymphoblastic Leukemia SEER Age-adjusted incidence rate 1.6 per 100,000 men and women
Acute Lymphoblastic and Myeloid Leukemia Pre- and Post-Disease Form Acute Lympoblastic Leukemia Mary Eapen MD, MS Acute Lymphoblastic Leukemia SEER Age-adjusted incidence rate 1.6 per 100,000 men and women
Cancer in Children. Dr Anant Sachdev Cancer Lead Berkshire East, GPSI Palliative Medicine
 Cancer in Children Dr Anant Sachdev Cancer Lead Berkshire East, GPSI Palliative Medicine 07976 608871 anant.sachdev@nhs.net Aim of this very short session! Facts and figures relating to Childrens Cancers
Cancer in Children Dr Anant Sachdev Cancer Lead Berkshire East, GPSI Palliative Medicine 07976 608871 anant.sachdev@nhs.net Aim of this very short session! Facts and figures relating to Childrens Cancers
Blood Cancers. Blood Cells. Blood Cancers: Progress and Promise. Bone Marrow and Blood. Lymph Nodes and Spleen
 Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Lymphoma Case Scenario 1
 Lymphoma Case Scenario 1 HISTORY: A 23-year-old healthy female presented with a month-long history of persistent headache of increasing severity. She noted episodic nausea and vomiting in association with
Lymphoma Case Scenario 1 HISTORY: A 23-year-old healthy female presented with a month-long history of persistent headache of increasing severity. She noted episodic nausea and vomiting in association with
Recommended Timing for Transplant Consultation
 REFERRAL GUIDELINES Recommended Timing for Transplant Consultation Published jointly by the National Marrow Donor Program /Be The Match and the American Society for Blood and Marrow Transplantation BeTheMatchClinical.org
REFERRAL GUIDELINES Recommended Timing for Transplant Consultation Published jointly by the National Marrow Donor Program /Be The Match and the American Society for Blood and Marrow Transplantation BeTheMatchClinical.org
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 24 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Aliyah Rahemtullah 1, Martin K Selig 1, Paola Dal Cin 2 and Robert P Hasserjian 1 Departments of Pathology,
Case 24 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Aliyah Rahemtullah 1, Martin K Selig 1, Paola Dal Cin 2 and Robert P Hasserjian 1 Departments of Pathology,
Childhood Leukemia Early Detection, Diagnosis, and Types
 Childhood Leukemia Early Detection, Diagnosis, and Types Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
Childhood Leukemia Early Detection, Diagnosis, and Types Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
CELL-MEDIATED IMMUNITY
 LECTURE #4 1 LYMPHATIC SYSTEM 2 CELL-MEDIATED IMMUNITY T-lymphocytes (activated in the thymus) identify aggressors and try to destroy them through the production of lymphokines (synthesized proteins) Killer
LECTURE #4 1 LYMPHATIC SYSTEM 2 CELL-MEDIATED IMMUNITY T-lymphocytes (activated in the thymus) identify aggressors and try to destroy them through the production of lymphokines (synthesized proteins) Killer
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Lymphocyte Predominant Hodgkin s Lymphoma. Case Presentation. How would you treat the patient?
 Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
First relapsed childhood ALL Role of chemotherapy
 First relapsed childhood ALL Role of chemotherapy Thirachit Chotsampancharoen, M.D. Division of Pediatric Hematology/Oncology Department of Pediatrics Prince of Songkla University Hat-Yai, Songkhla 25
First relapsed childhood ALL Role of chemotherapy Thirachit Chotsampancharoen, M.D. Division of Pediatric Hematology/Oncology Department of Pediatrics Prince of Songkla University Hat-Yai, Songkhla 25
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
WBCs Disorders. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
Lugano classification: Role of PET-CT in lymphoma follow-up
 CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
Understanding your diagnosis. Dr Graham Collins Consultant Haemtologist Oxford University Hospitals
 Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
SEVERE HYPERCALCEMIA SEVERE HYPERCALCEMIA A RARE AND UNUSUAL PRESENTATION OF ACUTE LYMPHOBLASTIC LEUKEMIA
 SEVERE HYPERCALCEMIA SEVERE HYPERCALCEMIA A RARE AND UNUSUAL PRESENTATION OF ACUTE LYMPHOBLASTIC LEUKEMIA Dr. Sowmiya Narayani. R. Junior Resident, Division Of Pediatric Hematology Oncology/ Pediatric
SEVERE HYPERCALCEMIA SEVERE HYPERCALCEMIA A RARE AND UNUSUAL PRESENTATION OF ACUTE LYMPHOBLASTIC LEUKEMIA Dr. Sowmiya Narayani. R. Junior Resident, Division Of Pediatric Hematology Oncology/ Pediatric
Consultation With the Specialist: Lymphomas Maria C. Velez. DOI: /pir
 Consultation With the Specialist: Lymphomas Maria C. Velez Pediatr. Rev. 2003;24;380 DOI: 10.1542/pir.24-11-380 The online version of this article, along with updated information and services, is located
Consultation With the Specialist: Lymphomas Maria C. Velez Pediatr. Rev. 2003;24;380 DOI: 10.1542/pir.24-11-380 The online version of this article, along with updated information and services, is located
Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD
 Photo by Tynan Studio Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD 96 Atlas of Childhood Cancer in Ontario (1985-2004) Chapter 6: Leukemia 6 Leukemia Atlas of Childhood
Photo by Tynan Studio Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD 96 Atlas of Childhood Cancer in Ontario (1985-2004) Chapter 6: Leukemia 6 Leukemia Atlas of Childhood
Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010
 Ryan Mattison, MD University of Wisconsin March 2, 2010") Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010 ALL Epidemiology 20% of new acute leukemia cases in adults 5200 new cases in 2007 Most are de novo Therapy-related
Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010 ALL Epidemiology 20% of new acute leukemia cases in adults 5200 new cases in 2007 Most are de novo Therapy-related
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Disclosures/COI. Cases in Hematopathology. Outline. Heme Path Findings Not to Miss. Normal Peripheral Smear 6/30/2016
 Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Indolent Lymphomas: Current. Dr. Laurie Sehn
 Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
NAACCR Webinar Series 1
 COLLECTING CANCER DATA: HEMATOPOIETIC AND LYMPHOID NEOPLASMS Jim Hofferkamp, CTR (jhofferkam@naaccr.org) Shannon Vann, CTR (svann@naaccr.org) Q&A Please submit all questions concerning webinar content
COLLECTING CANCER DATA: HEMATOPOIETIC AND LYMPHOID NEOPLASMS Jim Hofferkamp, CTR (jhofferkam@naaccr.org) Shannon Vann, CTR (svann@naaccr.org) Q&A Please submit all questions concerning webinar content
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA
 2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
HIV and Malignancy Alaka Deshpande, Himanshu Soni
 HIV and Malignancy Alaka Deshpande, Himanshu Soni Emergence of new infectious disease was documented in 1981. Within a short span of time it became a pandemic. It was Acquired Immunodeficiency Syndrome
HIV and Malignancy Alaka Deshpande, Himanshu Soni Emergence of new infectious disease was documented in 1981. Within a short span of time it became a pandemic. It was Acquired Immunodeficiency Syndrome
Lymphoma is a cancer that develops in the white blood cells (lymphocytes) of the lymphatic system, which is part of the body's immune system.
 of the lymphatic system, which is part of the body's immune system.") Scan for mobile link. Lymphoma Lymphoma is a cancer that develops in the white blood cells of the lymphatic system. Symptoms may include enlarged lymph nodes, unexplained weight loss, fatigue, night sweats
Scan for mobile link. Lymphoma Lymphoma is a cancer that develops in the white blood cells of the lymphatic system. Symptoms may include enlarged lymph nodes, unexplained weight loss, fatigue, night sweats
Leukemia And Lymphoma In The Nervous System
 Leukemia And Lymphoma In The Nervous System If you are searching for the book Leukemia and Lymphoma in the Nervous System in pdf format, then you've come to the right site. We presented complete variant
Leukemia And Lymphoma In The Nervous System If you are searching for the book Leukemia and Lymphoma in the Nervous System in pdf format, then you've come to the right site. We presented complete variant