Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012
|
|
|
- Julie Austin
- 6 years ago
- Views:
Transcription



1 Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory University, Chief of Hematology and Medical Oncology, Georgia Cancer Center for Excellence, Grady Memorial Hospital
2 Abstracts Delayed inhibition of HER2 in early stage breast cancer (Abstract S4-7) HER2-directed agents in the neoadjuvant setting (S5-6, S5-4, S5-1) Management of patients non-responsive to pre-operative therapy (Abstracts S3-2, S3-6)
3 Results of a randomized, double-blind, multicenter, placebo-controlled (TEACH) study of adjuvant lapatinib in women with early stage ErbB2-overexpressing breast cancer Goss et al Abstract S4-7
4 Study rationale At the time that results of the adjuvant trastuzumab trials were made available, many countries worldwide did not have access to trastuzumab TEACH trial designed to determine The natural history of HER2-positive breast cancers and whether there was continued recurrences overtime Whether delayed anti-her2 therapy with lapatinib would decrease these delayed recurrences if they occurred
5 TEACH trial design Stage 1-3c primary breast cancer HER2+ (3+ or FISH+) No prior trastuzumab (Neo) adjuvant chemotherapy Appropriate endocrine therapy Stratification: Time from diagnosis 4 vs >4 years Lymph node + vs ER+ and/or PR+ vs ER-, PR- RANDOMIZE Lapatinib 1500mg qd X 1 year n = 3147 Placebo qd X 1 year Diagnosis 4 years
6 TEACH: Endpoints and statistics Primary endpoint: DFS Hypothesis: Lapatinib will decreases recurrence by 23% (requires HR of 0.769), assuming an annual recurrence rate of 7% in the lapatinib arm and 10% in the placebo arm
7 TEACH: Baseline characteristics Lapatinib N = 1571 Placebo N = 1576 Median age Median time from initial diagnosis 2.7 years 2.75 years Years since initial diagnosis: 4 years 71% 72% > 4 years 29% 28% 0 1 year 20% 21% Hormone receptor status: ER and/or PR + 59% 59% ER, PR-negative 41% 41% Lymph node status: Positive 56% 56%
8 TEACH RESULTS: Ongoing Risk of Recurrence from Diagnosis in Placebo Arm Year(s) Disease-free Patients (%) Number of patients at risk Placebo % % % % % % % % % % 8
9 TEACH: K-M Plot of DFS According to Hormone Receptor (HR) Status in untreated (placebo) ITT Population ER/PgR+ve ER/PgR -ve 0.0 Number of patients at risk HR+ placebo HR placebo
10 TEACH Primary Endpoint: K-M Plot of DFS in ITT Population Time From Randomization HR 0.83 ( ); p=0.053 a Lapatinib Placebo Median Follow up: 4 years 0.0 Number of patients at risk Lapatinib 1500 mg Placebo a p value based on 2-sided stratified log-rank test
11 TEACH: K-M Plot of OS in ITT Population Time From Randomization Lapatinib Placebo HR 0.99 ( ); p=0.966 a Lapatinib (n=1571) Placebo (n=1576) Died, n (%) 92 (6%) 97 (6%) 0.0 Number of patients at risk Lapatinib 1500 mg Placebo a p value based on 2-sided stratified log-rank test. 11
12 TEACH: Forest Plot of DFS for Subgroups in ITT Population L=lapatinib; P=placebo. 12
13 TEACH: K-M Plot of DFS According to Hormone Receptor (HR) Status in treated ITT Population ER/PgR+ve: HR 0.98 ( ); p=0.886 a ER/PgR-ve: HR 0.68 ( ); p=0.006 a 0.0 Number of patients at risk HR+ lapatinib 1500 mg HR+ placebo HR lapatinib 1500 mg HR placebo a p value based on 2-sided stratified log-rank test.
14 TEACH: K-M Plot of DFS in Confirmed FISH+ Population Time From Randomization HR 0.82 ( ); p=0.04 a Lapatinib Placebo 0.0 Number of patients at risk Lapatinib 1500 mg Placebo a p value based on 2-sided stratified log-rank test.
15 TEACH: Sites of BRCA Recurrences and Second Primaries in Confirmed FISH+ Population Lapatinib 1500 mg (n=1230) Placebo (n=1260) Any recurrence of disease, second primary or contralateral BRCA, n (%) 157 (13%) 208 (17%) Local recurrence 24 (2%) 37 (3%) Regional recurrence 19 (2%) 25 (2%) Distant recurrence 102 (8%) 133 (11%) CNS 12 (<1%) 20 (2%) Contralateral BRCA 10 (<1%) 13 (1%) Second primary malignancy 22 (2%) 24 (2%)
16 TEACH: Time-to-First BRCA Recurrences in Confirmed FISH+ Population Lapatinib 1500 mg (n=1230) Placebo (n=1260) Any recurrence or contralateral BRCA, n (%) a 137 (11%) 183 (15%) Patients with recurrence at yearly time points, % 1 yr 3.7% 6% 2 yr 7.9% 10.5% 3 yr 10.6% 13.2% Any recurrence HR (95% CI) 0.79 ( ) 2-sided stratified log-rank p value b Patients with CNS recurrence at yearly time points, % 1 yr 0.5% 0.7% 3 yr 1.1% 1.3% CNS recurrence HR (95% CI) 0.66 (0.33, 1.34) 2-sided stratified log-rank p value b a Events not included were death and second primary cancer (competing risk). b p value stratified by time from initial diagnosis, HR status, and lymph node involvement.
17 TEACH: Adverse events Lapatinib associated with more AEs, especially diarrhea and rash 20% drug discontinuation on lapatinib arm No significant difference in cardiac events between the two arms Lapatinib associated with elevated LFTs in 8% of patients
18 TEACH: conclusions Patients with HER2+ cancers who do not receive trastuzumab remain at an ongoing risk of recurrence up to 10 years (regardless of HR status) DFS was not significantly improved with delayed lapatinib in the ITT population but did benefit patients: With ER/PR-negative cancers Within one year of diagnosis
19 Neoadjuvant Pertuzumab and Trastuzumab Concurrent or Sequential with an Anthracycline-Containing or Concurrent with an Anthracycline-Free Standard Regimen: A Randomized Phase II Study (TRYPHAENA) Schneeweiss et al Abstract S5-6
20 Primary study objective To make a preliminary assessment of the tolerability of neoadjuvant treatment with pertuzumab and trastuzumab plus anthracycline-taxanebased or carboplatin-taxane-based standard chemotherapy regimens in HER2-positive EBC EBC, early breast cancer; HER2, human epidermal growth factor receptor
21 Study design Cycles A FEC Docetaxel HER2-positive EBC centrally confirmed (n = 225) B C Pertuzumab + trastuzumab FEC Docetaxel Docetaxel Pertuzumab + trastuzumab Pertuzumab + trastuzumab S u r g e r y Trastuzumab to complete 1 year Carboplatin All 3 arms were experimental Study dosing q3w: FEC: 500 mg/m 2, 100 mg/m 2, 600 mg/m 2 Carboplatin: AUC 6 Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance Pertuzumab: 840 mg loading dose, 420 mg maintenance Docetaxel: 75 mg/m 2 (escalating to 100 mg/m 2 if tolerated, in Arms A and B only) AUC, area under the plasma concentration-time curve; EBC, early breast cancer; FEC, 5-fluorouracil, epirubicin, cyclophosphamide
22 Study endpoints Primary endpoint: Cardiac safety Symptomatic LVSD (grade 3) LVEF declines ( 10 percentage points and below 50%) Secondary endpoints: Toxicity pcr (defined as the absence of invasive tumor residues in the breast at surgery; remaining in situ lesions allowed; ypt0/is) Study was not powered for formal comparison between arms Clinical response rate Rate of breast-conserving surgery Disease-free survival and overall survival Biomarker evaluation LVEF, left ventricular ejection fraction; LVSD, left ventricular systolic dysfunction; pcr, pathologic complete response
23 Baseline characteristics in the safety population FEC+H+P x3 T+H+P x3 n = 72 FEC x3 T+H+P x3 n = 75 TCH+P x6 n = 76 Median age, years (range) 49.0 (27 77) 49.0 (24 75) 50.0 (30 81) ECOG PS 0, n (%) 1, n (%) ER and/or PR positive, n (%) ER and PR negative, n (%) Disease type, n (%) Operable Locally advanced Inflammatory HER2 IHC 0 and 1+, n (%) 2+, n (%) 3+, n (%) HER2 FISH positive, n (%) FISH negative, n (%) Unknown, n (%) 65 (91.5) 6 (8.5) 39 (53.4) 34 (46.6) 53 (72.6) 15 (20.5) 5 (6.8) 1 (1.4) 5 (6.8) 67 (91.8) 69 (94.5) 0 (0.0) 4 (5.5) 66 (88.0) 9 (12.0) 35 (46.7) 40 (53.3) 54 (72.0) 17 (22.7) 4 (5.3) 0 (0.0) 1 (1.3) 74 (98.7) 69 (92.0) 1 (1.3) 5 (6.7) 67 (88.2) 9 (11.8) 40 (51.9) 37 (48.1) 49 (63.6) 24 (31.2) 4 (5.2) 0 (0.0) 2 (2.6) 75 (97.4) 73 (94.8) 2 (2.6) 2 (2.6) ECOG PS, Eastern Cooperative Oncology Group performance status; ER, estrogen receptor; FEC, 5-fluorouracil, epirubicin, cyclophosphamide; FISH, fluorescence in situ hybridization; H, trastuzumab; IHC, immunohistochemistry; P, pertuzumab; PR, progesterone receptor; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
24 Cardiac events during neoadjuvant treatment FEC+H+P x3 T+H+P x3 n = 72 FEC x3 T+H+P x3 n = 75 TCH+P x6 n = 76 Symptomatic LVSD (grade 3), n (%) 0 (0.0) 2 (2.7) 0 (0.0) LVSD (all grades), n (%) 4 (5.6) 3 (4.0) 2 (2.6) LVEF decline 10% points and below 50%, n (%) 3 (4.2) 4 (5.3) 3 (3.9) FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; LVEF, left ventricular ejection fraction; LVSD, left ventricular systolic dysfunction; P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
25 Mean change in LVEF 8 Central readings FEC+H+P x3 T+H+P x3 (n = 72) FEC x3 T+H+P x3 (n = 75) TCH+P x6 (n = 76) 6 Mean absolute change in LVEF (%) Cycle Patients with assessment, n Neoadjuvant Adjuvant End of treatment 15 FEC+H+P x3 T+H+P x3 10 FEC x3 T+H+P x3 16 TCH+P x6 FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; LVEF, left ventricular ejection fraction; P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
26 10 most common grade 3 adverse events excluding cardiac events during neoadjuvant treatment Adverse event, n (%) FEC+H+P x3 T+H+P x3 n = 72 FEC x3 T+H+P x3 n = 75 TCH+P x6 n = 76 Neutropenia 34 (47.2) 32 (42.7) 35 (46.1) Febrile neutropenia 13 (18.1) 7 (9.3) 13 (17.1) Leukopenia 14 (19.4) 9 (12.0) 9 (11.8) Diarrhea 3 (4.2) 4 (5.3) 9 (11.8) Anemia 1 (1.4) 2 (2.7) 13 (17.1) Thrombocytopenia 0 (0.0) 0 (0.0) 9 (11.8) Vomiting 0 (0.0) 2 (2.7) 4 (5.3) Fatigue 0 (0.0) 0 (0.0) 3 (3.9) Alanine aminotransferase inc. 0 (0.0) 0 (0.0) 3 (3.9) Drug hypersensitivity 2 (2.8) 0 (0.0) 2 (2.6) FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; inc., increased; P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
27 Pathologic complete response Pathologic complete response (%) ypt0/is FEC+H+P x3 T+H+P x3 (n = 73) 57.3 FEC x3 T+H+P x3 (n = 75) 66.2 TCH+P x6 (n = 77) FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
28 Pathologic complete response Pathologic complete response (%) ypt0/is 50.7 FEC+H+P x3 T+H+P x3 (n = 73) FEC x3 T+H+P x3 (n = 75) ypt0 ypn TCH+P x6 (n = 77) 51.9 FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
 83.8 TCH+P x6 (n = 77) 50.")
29 Pathologic complete response by hormone receptor status Pathologic complete response (%) ER- and PR-negative FEC+H+P x3 T+H+P x3 (n = 73) 65.0 ER- and/or PR-positive 48.6 FEC x3 T+H+P x3 (n = 75) 83.8 TCH+P x6 (n = 77) 50.0 ypt0/is ER, estrogen receptor; FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; PR, progesterone receptor; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
30 Summary and conclusions Results from TRYPHAENA indicate a low incidence of symptomatic and asymptomatic LVSD across all arms Concurrent administration of pertuzumab plus trastuzumab with epirubicin resulted in similar cardiac tolerability compared with sequential administration or the anthracycline-free regimen Neutropenia, febrile neutropenia, leukopenia, and diarrhea were most frequently reported adverse events (grade 3) across all arms Regardless of chemotherapy chosen, the combination of pertuzumab with trastuzumab in the neoadjuvant setting resulted in high pcr rates (57 66%) Lower PCR in HR-positive versus HR-negative TRYPHAENA supports the ongoing APHINITY study, a Phase III trial to evaluate pertuzumab and trastuzumab plus standard chemotherapy in the adjuvant setting (NCT )
31 Comparison of survival according to pathological complete response (pcr) in patients with HER2-positive breast cancer receiving neoadjuvant chemotherapy with and w/o trastuzumab compared to patients with HER2-negative tumors, Loibl et al Abstract S5-4
32 TECHNO Study - Overall Survival pcr no pcr EC x4 Paclitaxel + Trastuzumab x4 Untch et al. J Clin Oncol 2011; 29:3351
33 Objectives Definition of three subgroups: HER2-positive with trastuzumab HER2-positive without trastuzumab HER2-negative Compare DDFS and OS in these subgroups: pcr vs. no pcr hormone receptor positive and -negative tumors
34 Methods All neoadjuvant trials with follow-up were included Known HER2 status (locally or centrally assessed) Hormone receptor positivity was defined as 10% cells positive for estrogen and/or progesterone receptor (locally or centrally assessed) pcr defined as no invasive and no non-invasive residuals in breast and lymph nodes (ypt0 ypn0) Adjustment for trial
35 All patients 6377 Eligible with known HER2-status 4387 HER2 negative HER2 positive HER2 positive 3060 w/o trastuzumab with trastuzumab pcr no pcr pcr no pcr pcr no pcr pcr-rate* pcr-rate* pcr-rate* 14.8% 17.9% 27.3% *ypt0 ypn0
 years % ct1-3 87 cn+ 53")

36 Patients Characteristics Age median 49 (22-81) years % ct cn+ 53 Ductal invasive 82 Grading 3 40 Hormone receptor positive 66 HER2-negative 70
37 DDFS and OS in the three subgroups vs vs P=0.040 P=0.382 vs vs P=0.142 P=0.103 n= 662 HER2+ with trastuzumab n= 3060 HER2 negative n= 665 HER2+; no trastuzumab
38 DDFS and OS by pcr HER2-negative pcr pcr no pcr no pcr Log-rank p<0.001 Log-rank p<0.001
39 DDFS and OS by pcr HER2-positive Without Trastuzumab pcr pcr no pcr no pcr Log-rank p=0.007 Log-rank p=0.037
40 DDFS and OS by pcr HER2-positive with Trastuzumab pcr pcr no pcr no pcr Log-rank p<0.001 Log-rank p=0.001
41 No pcr OS analysis by pcr pcr vs vs p=0.295 p=0.384 Log-rank vs vs p=0.058 p=0.134 Arm N Events Arm N Events positive w trast positive w trast positive w/o trast positive w/o trast negative negative n= 662 HER2+ with trastuzumab n= 3060 HER2 negative n= 665 HER2+; no trastuzumab
42 DDFS and OS in Hormone Receptor-positive vs vs P=0.606 P=0.795 vs vs P=0.614 P=0.652 n= 662 HER2+ with trastuzumab n= 3060 HER2 negative n= 665 HER2+; no trastuzumab
43 DDFS and OS in Hormone Receptor Negative vs p=0.012 vs p=0.123 vs p=0.059 vs p=0.029 n= 662 HER2+ with trastuzumab n= 3060 HER2 negative n= 665 HER2+; no trastuzumab
44 Summary Patients with HER2-positive primary breast cancer treated with trastuzumab and chemotherapy achieve a higher pcr rate DDFS and OS was significantly better with pcr in HER2- negative, HER2-positive non- trastuzumab and HER2-positive trastuzumab patients In pcr patients OS tended to be superior with trastuzumab compared to HER2-positive, non-trastuzumab and HER2- negative patients In particular HER2-positive, hormone receptor negative patients have a better DDFS and OS compared to HER2- positive, non-trastuzumab and HER2-negative patients

45 Neoadjuvant chemotherapy adapted by interim response improves overall survival of primary breast cancer patients Results of the GeparTrio trial. von Minckwitz et al Abstract 3-2
46 Aims To take advantage from the in vivo chemosensitivity test situation of neoadjuvant treatment To develop specific treatment strategies for patients with or without response to 2 cycles TAC: Responding patients: treatment intensification by increased cycle number Non-responding patients: switch to non-cross resistant treatment
47 GeparTrio Trial Design N=2072 Core biopsy: uni/bilateral ct2-4a-d cn0-3 size 2 cm* *low risk patients were excluded (T2 + ER/PR pos. + cno + G1/2 + > 35 yrs) NC R Sonography CR/ PR R NX TACx6 response- guided arms conventional arms TACx6 TACx8 von Minckwitz et al, JNCI 100: 542, 2008 von Minckwitz et al. JNCI 100; 552, 2008
48 Short Term Efficacy (pcr = ypt0 ypn0) Responder Non-Responder N=1344 N=604 30% P=0.27 P= % 10% TACx6 TACx8 TACx6 TAC-NX von Minckwitz et al, JNCI 100: 542, 2008 von Minckwitz et al. JNCI 100; 552, 2008
49 Objectives Primary: Pathologic response (responder) Sonographic response (non-responder) Secondary (actual with median follow up of 62 months): To determine 5-year DFS and OS To examine treatment effects by breast cancer phenotype (post-hoc analysis)
50 Study Population Characteristic Conventional Response-guided TACx6 TACx8 or TAC-NX N=1025 N=987 % % Age < 40 years ct> 40 mm ct4a-c ct4d cn Lobular type Grade HR-negative HER2-positive
51 DFS and OS after conventional (TACx6) vs. response-guided (TACx8/TAC-NX) treatment Median follow up 62 months
52 Adjusted Analysis for DFS Variable Group HR p-value Treatment Response-guided Age 40 years T-stage ct <0.001 T-size <40 mm cn negative 0.56 <0.001 Histological type lobular Grade HR positive 0.49 <0.001 HER2 negative
53 DFS after TACx6 vs TACx8 in responding patients
54 DFS after TACx6 vs TAC-NX in non-responding patients

55 Subgroup analysis comparing DFS after conventional vs response-guided treatment
56 Breast Cancer phenotypes (St. Gallen definition*) Phenotype Definition Conventional Response-guided % % Luminal A HR+, HER2-, G1/ Luminal B (HER2-) HR+, HER2-, G Luminal B (HER2+) HR+, HER HER2+ (non-luminal) HR-, HER Triple-negative HR-, HER Missing N=181 N=227 *Goldhirsch A, Ann Oncol 2011
 Luminal B")
 Triple-negative (N=211)")
57 pcr (%) pcr Rates by Subtype Luminal A (N=572) Luminal B (HER2-) Luminal B (HER2+) HER2+ (non-luminal) Triple-negative (N=211) (N=281) (N=178) N=362)
58 DFS in Luminal A tumors by pcr by treatment
59 DFS in Luminal B (HER2-) by pcr by treatment
60 DFS in Luminal B (HER2+) tumors by pcr by treatment
61 DFS in HER2+(non-luminal) tumors by pcr by treatment
62 DFS in Triple Negative Tumors by pcr by treatment
63 Conclusion Interim response-guided (longer or sequential) neoadjuvant chemotherapy improved survival. Treatment effects on survival derived from luminal-type tumors. This treatment effect could not be predicted by pcr as these tumors have lower pcr rates and their prognosis does not depend on pcr. Patients with HER2+ or triple-negative tumors did not benefit from response-guided treatment. pcr is highly prognostic in these subgroups. Lack of treatment effect on pcr rate corresponds to lack of long term treatment.

 Huober et al Abstract")
64 NEOADJUVANT CHEMOTHERAPY OF PACLITAXEL WITH OR WITHOUT RAD001 - RESULTS OF THE NON-RESPONDER PART OF THE GEPARQUINTO STUDY (GBG 44) Huober et al Abstract 3-6
65 Introduction HER2- Non-Responder The oral signal transduction inhibitor everolimus (RAD001 = Rad), binds selectively to mtor (mammalian target of rapamycin) mtor is an intracellular protein kinase controlling cellular proliferation of activated T-lymphocytes and neoplastic cells. In vitro synergistic reactions with Rad and several chemotherapeutic drugs including paclitaxel were observed1 Additional neoadjuvant treatment strategies are needed for patients without early clinical response 1 O`Reilly T et al. Anti-Cancer Drugs 2011


66 HER2- Non-Responder Study Design HER-2 negative Pw Core biopsy 2nd core NC R Surgery R EC +/- B RAD001 Pw RAD +/- Bevacizumab T +/- B PR CR/ +/- Bevacizumab E = Epirubicin C = Cyclophosphamide T = Docetaxel B = Bevacizumab Pw = Paclitaxel, weekly (80 mg/m2: day 1 q day 8-12 weeks) R = RAD001 (5 mg / day from day 13 after a dose escalation starting from 2.5 mg every other day to 5mg every day)
67 HER2- Non-Responder Patients & Tumor Characteristics Pw Pw+Rad N=198 N=197 age (median yrs) Age < 40 years (%) palpable T-size (median mm) % % ct 4 (a-c) inflammatory cn lobular type hormone receptor positive grade
68 HER2- Non-Responder 10% 9% 8% 7% 6% 5% 4% 3% pcr (no invasive & no non-invasive residuals in breast & nodes based on central pathology report review N=395) P= % 5.6% 3.6% 1% 0% N=11 N= % % Pw n= 198 Pw+Rad n=197
69 HER2- Non-Responder pcr Rates According to Secondary Endpoint Definitions no invasive residuals in breast & nodes (ypt0/tis, ypn0) Houston 20% 20% 18% 18% P= % 15% 13% 13% 10% 10% 8% 8% no invasive residuals in breast (ypt0/tis) NSABP P= % 6.1% 5% 7.1% 3% 5.1% 3% 6.6% 0% 0% Pw Pw+Rad Pw Pw+Rad
 100% 90%")

70 HER2- Non-Responder ccr+cpr (clinical complete and partial response at surgery n=379) 100% 90% 80% 70% 60% 50% 40% 30% P= % 52.2% 20% % % 10% 0% Pw n= 195 Pw+Rad n=184
71 HER2- Non-Responder Conclusions pcr rate is low (4.6%) in patients not responding to the initial 4 cycles of neoadjuvant chemotherapy with or without Bev Addition of Rad to 12 weeks paclitaxel did not improve pcr rate in these patients (Pw 5.6% vs. Pw+Rad 3.6%; P=0.476) Toxicity was higher in the group treated with Rad DFS and OS have to be awaited because pcr might not be the appropriate endpoint (high number HR+) A large biomarker program is ongoing to identify predictive markers
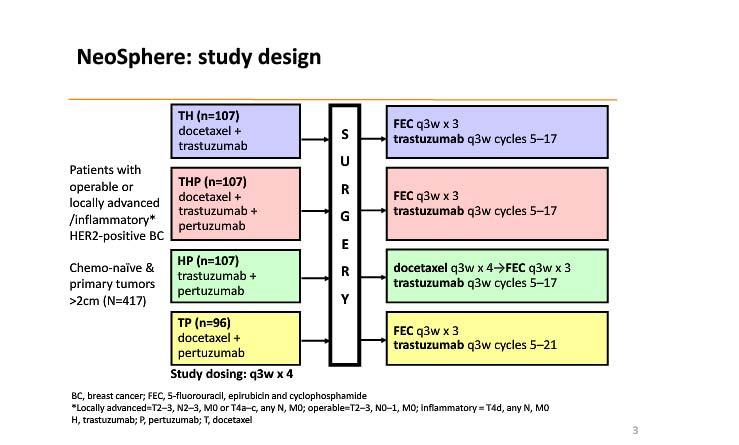
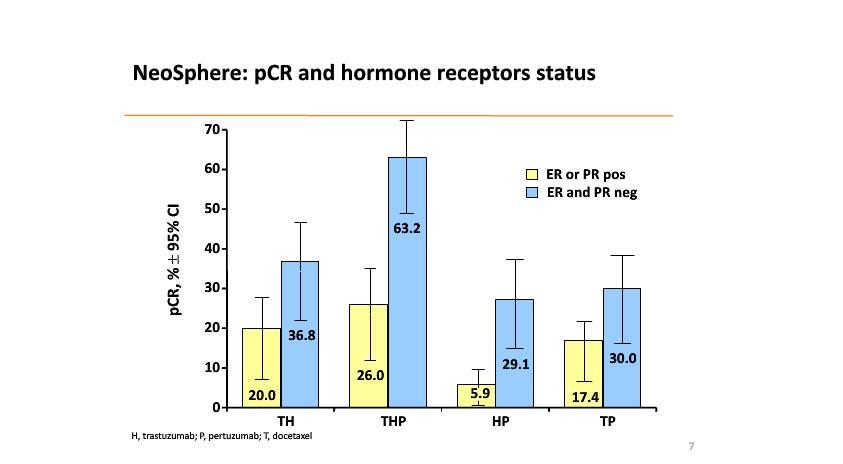
72 Neo-adjuvant pertuzumab and trastuzumab: Biomarker analyses of a 4-arm randomized phase 2 trial (NeoSphere) in patients with HER2-positive breast cancer Gianni et al Abstract S5-1
73
74
75
76 NeoSphere: Correlative results PI3-kinase mutations were not associated with rate of PCR No role for truncated forms of HER2, including p95 HER2 in predicting PCR IGF1R, HER3, PTEN and EGFR were higher in ER-positive cancers, while HER2 was higher in ER-negative breast cancers
77 Practice changing? Potentially important: Late recurrences in HER2-positive breast cancers Confirmatory: Decreased incidence (and importance) of PCR in HR-positive, HER2-positive breast cancers Equivalence of anthracycline and non-anthracycline containing regimens in HER2-positive breast cancers Dual targeting of HER2 superior to single agents in preoperative setting Depressing: Poor outcome for patients with TNBC who do not obtain a PCR and Lack of improvement in PCR rate with non-resistant chemotherapeutics and novel agents
The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?
 as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?") 1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance
 Oncology Department Vall d Hebron University Hospital Barcelona. Spain Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance Javier Cortés June/2013 MD Anderson experience Buzdar et
Oncology Department Vall d Hebron University Hospital Barcelona. Spain Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance Javier Cortés June/2013 MD Anderson experience Buzdar et
Novel Preoperative Therapies for HER2-Positive Breast Cancer. Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center
 Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
PRO: Pathologic Complete Response Does Predict Outcome for Early Stage Breast Cancer Patients
 PRO: Pathologic Complete Response Does Predict Outcome for Early Stage Breast Cancer Patients Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute
PRO: Pathologic Complete Response Does Predict Outcome for Early Stage Breast Cancer Patients Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer
 Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer
 New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA
 Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA
 Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
Novel Preoperative Therapies for HER2-Positive Breast Cancer
 Key Findings to Date in the Neoadjuvant Therapy of H2+ Breast Cancer Novel Preoperative Therapies for H2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive
Key Findings to Date in the Neoadjuvant Therapy of H2+ Breast Cancer Novel Preoperative Therapies for H2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive
Highlights. Padova,
 Highlights P Pronzato Padova, 17.11.2012 Last 12 Months Main Meetings SABCS 2011 (San Antonio) EBCC 8 2012 (Wien) ASCO 2012 (Chicago) ESMO/ECCO 2012 (Wien) The Medical Oncology Job Risk Manager Strategy
Highlights P Pronzato Padova, 17.11.2012 Last 12 Months Main Meetings SABCS 2011 (San Antonio) EBCC 8 2012 (Wien) ASCO 2012 (Chicago) ESMO/ECCO 2012 (Wien) The Medical Oncology Job Risk Manager Strategy
NeoadjuvantTreatment In BC When, How, Who?
 NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
Nadia Harbeck Breast Center University of Cologne, Germany
 Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all)
") Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all) 8 November 2014 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky
Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all) 8 November 2014 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky
Treatment of Early-Stage HER2+ Breast Cancer
 Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives
 Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pertuzumab (Perjeta) Neoadjuvant Breast Cancer April 30, 2015
 Neoadjuvant Breast Cancer April 30, 2015") pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pertuzumab (Perjeta) Neoadjuvant Breast Cancer April 30, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pertuzumab (Perjeta) Neoadjuvant Breast Cancer April 30, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Lo Studio Geparsepto. Alessandra Fabi Oncologia Medica 1
 Lo Studio Geparsepto Alessandra Fabi Oncologia Medica 1 nab-paclitaxel Versus Solvent-Based Paclitaxel in Neoadjuvant Chemotherapy for Early Breast Cancer (GeparSepto GBG 69): A Randomised, Phase III Trial
Lo Studio Geparsepto Alessandra Fabi Oncologia Medica 1 nab-paclitaxel Versus Solvent-Based Paclitaxel in Neoadjuvant Chemotherapy for Early Breast Cancer (GeparSepto GBG 69): A Randomised, Phase III Trial
FDA Briefing Document Oncologic Drugs Advisory Committee Meeting. September 12, sbla /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc.
 Applicant: Genentech, Inc.") /51 FDA Briefing Document Oncologic Drugs Advisory Committee Meeting September 12, 2013 /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc. Disclaimer: The attached package contains background information
/51 FDA Briefing Document Oncologic Drugs Advisory Committee Meeting September 12, 2013 /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc. Disclaimer: The attached package contains background information
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
San Antonio Breast Cancer Symposium, December 5-9, San Antonio Breast Cancer Symposium, December 5-9, 2017
 San Antonio Breast Cancer Symposium, December 5-9, 2017 Survival analysis of the prospectively randomized phase III GeparSepto trial comparing neoadjuvant chemotherapy with weekly nab-paclitaxel with solvent-based
San Antonio Breast Cancer Symposium, December 5-9, 2017 Survival analysis of the prospectively randomized phase III GeparSepto trial comparing neoadjuvant chemotherapy with weekly nab-paclitaxel with solvent-based
Breast : ASCO Abstracts for Review
 Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre
 Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre Recurrence of HER2-positive breast cancer (A) Time to
Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre Recurrence of HER2-positive breast cancer (A) Time to
Taking NeoadjuvantTreatment into the Clinic
 Taking NeoadjuvantTreatment into the Clinic The Data and the Challenges Karen A Gelmon MD FRCPC Professor Medicine University of British Columbia Medical Oncologist BC Cancer Agency NeoadjuvantTherapy
Taking NeoadjuvantTreatment into the Clinic The Data and the Challenges Karen A Gelmon MD FRCPC Professor Medicine University of British Columbia Medical Oncologist BC Cancer Agency NeoadjuvantTherapy
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Rethinking neoadjuvant therapy: neoadjuvant therapy as a platform for drug development in HER2 positive breast cancer
 2016.04.29 GBCC luncheon symposium Rethinking neoadjuvant therapy: neoadjuvant therapy as a platform for drug development in HER2 positive breast cancer Seoul National University Bundang Hospital Seoul
2016.04.29 GBCC luncheon symposium Rethinking neoadjuvant therapy: neoadjuvant therapy as a platform for drug development in HER2 positive breast cancer Seoul National University Bundang Hospital Seoul
Treatment of Early Stage HER2-positive Breast Cancer
 Treatment of Early Stage HER2-positive Breast Cancer 3 November 2012 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky Lexington, KY Molecular Portrait
Treatment of Early Stage HER2-positive Breast Cancer 3 November 2012 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky Lexington, KY Molecular Portrait
BREAST CANCER RISK REDUCTION (PREVENTION)
") BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
Dennis J Slamon, MD, PhD
 I N T E R V I E W Dennis J Slamon, MD, PhD Dr Slamon is Professor of Medicine, Chief of the Division of Hematology/Oncology and Director of Clinical and Translational Research at UCLA s David Geffen School
I N T E R V I E W Dennis J Slamon, MD, PhD Dr Slamon is Professor of Medicine, Chief of the Division of Hematology/Oncology and Director of Clinical and Translational Research at UCLA s David Geffen School
Systemic Therapy Considerations in Inflammatory Breast Cancer
 Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
(Neo)Adjuvant Chemotherapy and biological Agents (essentials in HER2 and TN early breast cancer)
Adjuvant Chemotherapy and biological Agents (essentials in HER2 and TN early breast cancer)") (Neo)Adjuvant Chemotherapy and biological Agents (essentials in HER2 and TN early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Neoadjuvant
(Neo)Adjuvant Chemotherapy and biological Agents (essentials in HER2 and TN early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Neoadjuvant
Non-Anthracycline Adjuvant Therapy: When to Use?
 Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Impact of BMI on pathologic complete response (pcr) following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer
 following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer") Impact of BMI on pathologic complete response (pcr) following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer Rachna Raman, MD, MS Fellow physician University of Iowa hospitals and clinics
Impact of BMI on pathologic complete response (pcr) following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer Rachna Raman, MD, MS Fellow physician University of Iowa hospitals and clinics
that the best available evidence has not demonstrated that pcr can predict long-term outcomes in the neoadjuvant setting.
 pcr in one arm of a randomized clinical trial comparing two neoadjuvant chemotherapies predicts for improved event-free or overall survival in that arm of the clinical trial. perc noted that the NeoALTTO
pcr in one arm of a randomized clinical trial comparing two neoadjuvant chemotherapies predicts for improved event-free or overall survival in that arm of the clinical trial. perc noted that the NeoALTTO
Point of View on Early Triple Negative
 Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017
 TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
Systemic therapy: HER-2 update. Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven
 Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
HER2-positive Breast Cancer
 HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cortazar P, Zhang L, Untch M, et al. Pathological
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cortazar P, Zhang L, Untch M, et al. Pathological
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2017 Relative Risk HER2-positive Breast
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2017 Relative Risk HER2-positive Breast
Overview of nab-paclitaxel in Breast Cancer
 Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
Adjuvant Chemotherapy + Trastuzumab
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Chemotherapy + Trastuzumab (Optimal Drugs / Dosage / Trastuzumab) Adjuvant Chemotherapy (Optimal Drugs / Optimal Dosage
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Chemotherapy + Trastuzumab (Optimal Drugs / Dosage / Trastuzumab) Adjuvant Chemotherapy (Optimal Drugs / Optimal Dosage
Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory University, Chief of
 Review of triple negative breast cancer and new agents GASCO Review of SABCS 2014 January 10 th 2015, Atlanta, GA Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology
Review of triple negative breast cancer and new agents GASCO Review of SABCS 2014 January 10 th 2015, Atlanta, GA Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology
Triple Negative Breast Cancer: Part 2 A Medical Update
 Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
2014 San Antonio Breast Cancer Symposium Review
 2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
Introduction. Approximately 20% of invasive breast cancers
 Introduction Approximately 2% of invasive breast cancers overexpress HER2 The current standard of care for neoadjuvant therapy is dual-targeted therapy with trastuzumab and pertuzumab plus chemotherapy
Introduction Approximately 2% of invasive breast cancers overexpress HER2 The current standard of care for neoadjuvant therapy is dual-targeted therapy with trastuzumab and pertuzumab plus chemotherapy
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
XII Michelangelo Foundation Seminar
 XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER. Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx
 OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Systemic Therapy for Locally Advanced Breast Cancer
 Systemic Therapy for Locally Advanced Breast Cancer Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology National University Cancer Institute, Singapore Clinical Care Senior Principal
Systemic Therapy for Locally Advanced Breast Cancer Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology National University Cancer Institute, Singapore Clinical Care Senior Principal
The absolute benefit from chemotherapy for both older and younger patients appeared most significant in ER-negative populations.
 Hello, my name is Diane Hecht, and I am a Clinical Pharmacy Specialist at the University of Texas MD Anderson Cancer Center. It s my pleasure to talk to you today about the role of chemotherapy in this
Hello, my name is Diane Hecht, and I am a Clinical Pharmacy Specialist at the University of Texas MD Anderson Cancer Center. It s my pleasure to talk to you today about the role of chemotherapy in this
Roche s Perjeta regimen approved in Europe for use before surgery in early stage aggressive breast cancer
 Media Release Basel, 31 July, 2015 Roche s Perjeta regimen approved in Europe for use before surgery in early stage aggressive breast cancer The approval is based on the benefit seen with the Perjeta regimen
Media Release Basel, 31 July, 2015 Roche s Perjeta regimen approved in Europe for use before surgery in early stage aggressive breast cancer The approval is based on the benefit seen with the Perjeta regimen
Breast cancer treatment
 Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
The Expert Thoughts. Alessandra Fabi Oncologia Medica 1
 The Expert Thoughts Alessandra Fabi Oncologia Medica 1 My Thoughts Neoadjuvant: from the lessons of the history Adjuvant: Escalation and De-escalation Advanced and HER2+ : field for immunomodulation Brain
The Expert Thoughts Alessandra Fabi Oncologia Medica 1 My Thoughts Neoadjuvant: from the lessons of the history Adjuvant: Escalation and De-escalation Advanced and HER2+ : field for immunomodulation Brain
10/15/2012. Inflammatory Breast Cancer vs. LABC: Different Biology yet Subtypes Exist
 Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
Neoadjuvant therapy a new pathway to registration?
 Neoadjuvant therapy a new pathway to registration? Graham Ross, FFPM Clinical Science Leader Roche Products Ltd Welwyn Garden City, UK (full time employee) Themes Neoadjuvant therapy Pathological Complete
Neoadjuvant therapy a new pathway to registration? Graham Ross, FFPM Clinical Science Leader Roche Products Ltd Welwyn Garden City, UK (full time employee) Themes Neoadjuvant therapy Pathological Complete
Lecture 5. Primary systemic therapy: clinical and biological endpoints
 Lecture 5 Primary systemic therapy: clinical and biological endpoints Valentina Guarneri, M.D., Ph.D. Primary systemic therapy in breast cancer Firstly introduced d into clinical i l practice in 70s for
Lecture 5 Primary systemic therapy: clinical and biological endpoints Valentina Guarneri, M.D., Ph.D. Primary systemic therapy in breast cancer Firstly introduced d into clinical i l practice in 70s for
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY. Dr. Carlos Garbino
 EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
(NEO-)ADJUVANT THERAPY FOR HER-2+ EBC
ADJUVANT THERAPY FOR HER-2+ EBC") (NEO-)ADJUVANT THERAPY FOR HER-2+ EBC Rebecca Dent, MD FRCP (Canada) Senior Consultant, National Cancer Center Singapore Associate Professor, Duke-NUS www.abc-lisbon.org When to question a pathology report?
(NEO-)ADJUVANT THERAPY FOR HER-2+ EBC Rebecca Dent, MD FRCP (Canada) Senior Consultant, National Cancer Center Singapore Associate Professor, Duke-NUS www.abc-lisbon.org When to question a pathology report?
Targe:ng HER2 in Metasta:c Breast Cancer in 2014
 Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Update in the treatment of Her2- overexpressing breast cancers. Fabrice ANDRE Institut Gustave Roussy Villejuif, France
 Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Advanced HER2+ Breast Cancer: New Options and How to Deploy Them. José Baselga MD, PhD
 Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
(Neo) Adjuvant systemic therapy for HER-2+ EBC
 Adjuvant systemic therapy for HER-2+ EBC") (Neo) Adjuvant systemic therapy for HER-2+ EBC F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESMO Board of Directors & NR Committee Chair ESO Breast Cancer Program
(Neo) Adjuvant systemic therapy for HER-2+ EBC F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESMO Board of Directors & NR Committee Chair ESO Breast Cancer Program
Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016
 Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016 Yes! Age disparities vary by tumor subtype Genomic risk prediction data in young women Adjuvant systemic therapy
Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016 Yes! Age disparities vary by tumor subtype Genomic risk prediction data in young women Adjuvant systemic therapy
Role of chemotherapy in BRCA and Triple negative breast cancer. Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos
 Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Post-ESMO 2012: Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich T.Rordorf, SAMO Luzern 1
 Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
Media Release. FDA grants Roche s Perjeta accelerated approval for use before surgery in people with HER2-positive early stage breast cancer
 Media Release Basel, 1 October 2013 FDA grants Roche s Perjeta accelerated approval for use before surgery in people with HER2-positive early stage breast cancer The Perjeta regimen is the first treatment
Media Release Basel, 1 October 2013 FDA grants Roche s Perjeta accelerated approval for use before surgery in people with HER2-positive early stage breast cancer The Perjeta regimen is the first treatment
Disease Update: Metastatic Breast Cancer
 Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Existe-t-il un sous groupe à risque qui pourrait bénéficier d une modification de la durée de traitement par trastuzumab? X. Pivot CHRU De Besançon
 Existe-t-il un sous groupe à risque qui pourrait bénéficier d une modification de la durée de traitement par trastuzumab? X. Pivot CHRU De Besançon In 25 results of 4 Adjuvant Herceptin trials have definitively
Existe-t-il un sous groupe à risque qui pourrait bénéficier d une modification de la durée de traitement par trastuzumab? X. Pivot CHRU De Besançon In 25 results of 4 Adjuvant Herceptin trials have definitively
Roohi Ismail-Khan, MD, MS
 Roohi Ismail-Khan, MD, MS Associate Member Department of Breast Oncology H. Lee Moffitt Cancer Center Associate Professor University of South Florida Department of Oncological Sciences September 27, 2018
Roohi Ismail-Khan, MD, MS Associate Member Department of Breast Oncology H. Lee Moffitt Cancer Center Associate Professor University of South Florida Department of Oncological Sciences September 27, 2018
St Gallen 2017 controversies & consensus
 St Gallen 2017 controversies & consensus Shani Paluch-Shimon, MBBS, MSc Head, Breast Cancer Service for Young Women Breast Unit, Division of Oncology Sheba Medical Centre June 2017 St Gallen 2017 De-escalation
St Gallen 2017 controversies & consensus Shani Paluch-Shimon, MBBS, MSc Head, Breast Cancer Service for Young Women Breast Unit, Division of Oncology Sheba Medical Centre June 2017 St Gallen 2017 De-escalation
Corporate Medical Policy
 Corporate Medical Policy Pertuzumab for Treatment of Malignancies File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pertuzumab_for_treatment_of_malignancies 2/2013 4/2017 4/2018 6/2017
Corporate Medical Policy Pertuzumab for Treatment of Malignancies File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pertuzumab_for_treatment_of_malignancies 2/2013 4/2017 4/2018 6/2017
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer
 The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy
 Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
pertuzumab 420mg concentrate for solution for infusion vial (Perjeta ) SMC No. (1121/16) Roche Products Limited
 SMC No. (1121/16) Roche Products Limited") pertuzumab 420mg concentrate for solution for infusion vial (Perjeta ) SMC No. (1121/16) Roche Products Limited 05 February 2016 The Scottish Medicines Consortium (SMC) has completed its assessment of
pertuzumab 420mg concentrate for solution for infusion vial (Perjeta ) SMC No. (1121/16) Roche Products Limited 05 February 2016 The Scottish Medicines Consortium (SMC) has completed its assessment of
Emerging Agents in HER2-positive Disease. Mary Cianfrocca, DO Director, Breast Oncology Program Banner MD Anderson Cancer Center Gilbert, AZ
 Emerging Agents in HER2-positive Disease Mary Cianfrocca, DO Director, Breast Oncology Program Banner MD Anderson Cancer Center Gilbert, AZ Signal Transduction by the HER Family and Potential Mechanisms
Emerging Agents in HER2-positive Disease Mary Cianfrocca, DO Director, Breast Oncology Program Banner MD Anderson Cancer Center Gilbert, AZ Signal Transduction by the HER Family and Potential Mechanisms
NEW ZEALAND DATA SHEET
 NEW ZEALAND DATA SHEET 1. PRODUCT NAME Perjeta 420 mg concentrate for solution for infusion. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Perjeta is supplied as a single-use vial containing 14 ml of preservative-free
NEW ZEALAND DATA SHEET 1. PRODUCT NAME Perjeta 420 mg concentrate for solution for infusion. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Perjeta is supplied as a single-use vial containing 14 ml of preservative-free
AUSTRALIAN PRODUCT INFORMATION Perjeta (pertuzumab)
") AUSTRALIAN PRODUCT INFORMATION Perjeta (pertuzumab) 1. NAME OF THE MEDICINE Pertuzumab 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Perjeta 420 mg concentrate for intravenous infusion. For the full list
AUSTRALIAN PRODUCT INFORMATION Perjeta (pertuzumab) 1. NAME OF THE MEDICINE Pertuzumab 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Perjeta 420 mg concentrate for intravenous infusion. For the full list
What to do after pcr in different subtypes?
 What to do after pcr in different subtypes? Luca Moscetti Breast Unit Università degli Studi di Modena e Reggio Emilia Policlinico di Modena, Italy Aims of neoadjuvant therapy in breast cancer Primary
What to do after pcr in different subtypes? Luca Moscetti Breast Unit Università degli Studi di Modena e Reggio Emilia Policlinico di Modena, Italy Aims of neoadjuvant therapy in breast cancer Primary
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Highlights in Metastatic Breast Cancer From the 2011 San Antonio Breast Cancer Symposium (SABCS)
") February 2012 A SPECIAL MEETING REVIEW EDITION Volume 10, Issue 2, Supplement 2 Highlights in Metastatic Breast Cancer From the 2011 San Antonio Breast Cancer Symposium (SABCS) December 6 10, 2011 San
February 2012 A SPECIAL MEETING REVIEW EDITION Volume 10, Issue 2, Supplement 2 Highlights in Metastatic Breast Cancer From the 2011 San Antonio Breast Cancer Symposium (SABCS) December 6 10, 2011 San
Adjuvant Chemotherapy TNBC & HER2 Subtype
 Adjuvant Chemotherapy TNBC & HER2 Subtype 2015.08.15 Gun Min Kim Yonsei Cancer Center Division of Medical Oncology Department of Internal Medicine Yonsei University College of Medicine gmkim77@yuhs.ac
Adjuvant Chemotherapy TNBC & HER2 Subtype 2015.08.15 Gun Min Kim Yonsei Cancer Center Division of Medical Oncology Department of Internal Medicine Yonsei University College of Medicine gmkim77@yuhs.ac
PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND!
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari
 Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
FEC-T plus trastuzumab & pertuzumab
 Page 1 of 5 Indication Treatment Intent Frequency and number of cycles Monitoring parameters pre-treatment The neoadjuvant treatment of locally advanced, inflammatory or early HER2 positive breast cancer
Page 1 of 5 Indication Treatment Intent Frequency and number of cycles Monitoring parameters pre-treatment The neoadjuvant treatment of locally advanced, inflammatory or early HER2 positive breast cancer
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
Accelerated approval of Perjeta for neoadjuvant use also converted to full approval
 Media Release Basel, 21 December 2017 FDA approves Roche s Perjeta (pertuzumab) for adjuvant treatment of specific type of early breast cancer Accelerated approval of Perjeta for neoadjuvant use also converted
Media Release Basel, 21 December 2017 FDA approves Roche s Perjeta (pertuzumab) for adjuvant treatment of specific type of early breast cancer Accelerated approval of Perjeta for neoadjuvant use also converted