Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all)
|
|
|
- Ruby Dawson
- 5 years ago
- Views:
Transcription
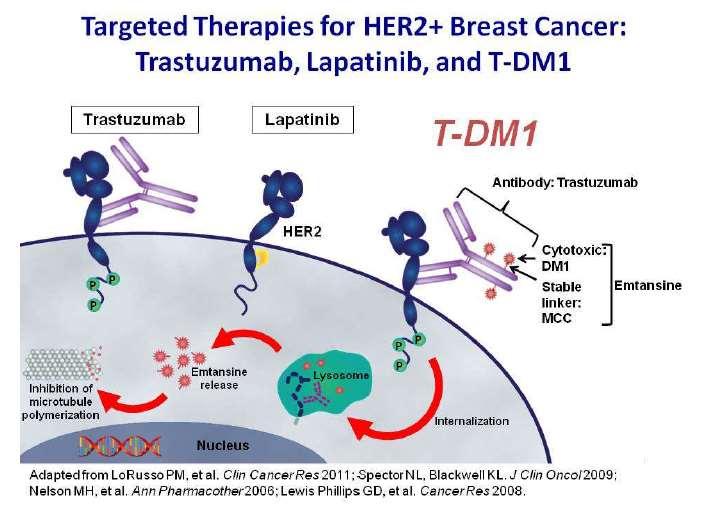
1 Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all) 8 November 2014 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky Lexington, KY

2 Slamon, et al. Science 1987;235:
3
4


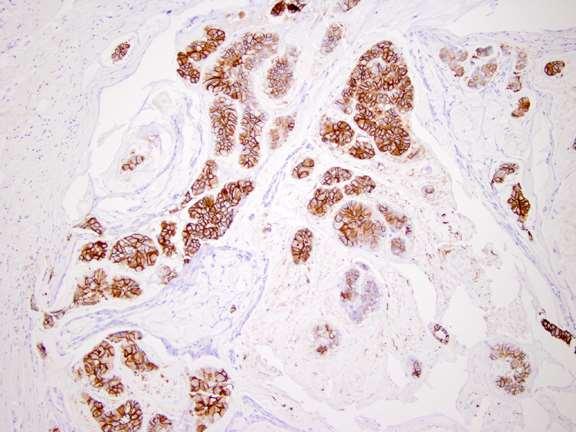
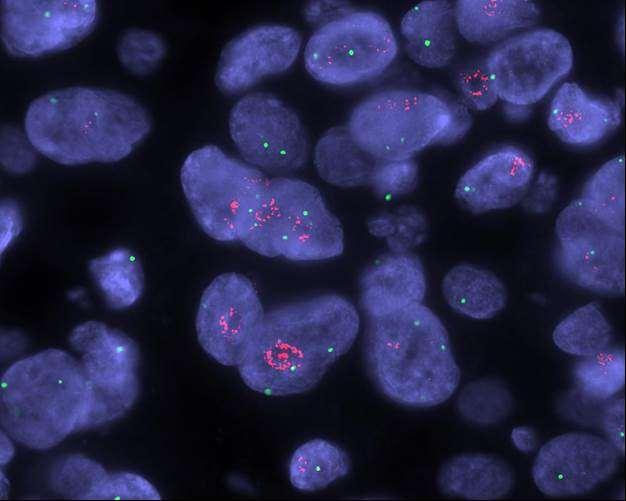
5 Focal HER2 Amplified Clones Amplified Not Amplified Not Amplified Amplified
 Trastuzumab.")
6 Fig. 2 Epitope binding of HER2 and EGFR therapeutic antibodies.(a) Trastuzumab. M X Sliwkowski, and I Mellman Science 2013;341: Published by AAAS
7 Large Phase III Adjuvant Trastuzumab Trials B31/N9831 CIRG 006 HERA: Chemo ± XRT AC T AC TH (AC T H) AC T* AC T*H T*C*H Observation H x 1 year H x 2 years A = doxorubicin C = cyclophosphamide T = paclitaxel H = trastuzumab T* = docetaxel C* = carboplatin
8 Arm 1 Arm 2 NSABP B-31 Control: AC T NCCTG N9831 Arm A Arm B Investigational: AC T+H Arm C = doxorubicin/cyclophosphamide (AC) 60/600 mg/m 2 q 3 wk x 4 = paclitaxel (T) 175 mg/m 2 q 3 wk x 4 = paclitaxel (T) 80 mg/m 2 /wk x 12 = trastuzumab (H) 4mg/kg LD + 2 mg/kg/wk x 51
 P<0.0001 No.")
9 % Event-Free San Antonio Breast Cancer Symposium, December 4-8, 2012 N9831/B-31 Disease-Free Survival AC P 81.4% 69.5% AC P+H 76.8% 64.9% 73.7% 62.2% 11.5% N Events AC P AC P+H HRadj=0.60 (95% CI: ) P< No. at risk Years from Randomization Perez, E et al., J Clin Oncol, 2014
 P<0.0001 No.")
10 % Survival San Antonio Breast Cancer Symposium, December 4-8, 2012 B-31/N9831 Overall Survival AC P 93.2% 89.8% 90.3% 84.3% 87.0% 79.4% AC P+H 84.0% 75.2% 8.8% =2.9% =5.5% =7.6% =8.8% N Events AC P AC P+H HRadj=0.63 (95% CI ) P< No. at risk Years from Randomization Perez, E et al., J Clin Oncol, 2014
11 Age Hormone Receptor Tumor Size Nodal Status Histologic Grade Factor <40 years years OS According to Subgroups ACTH vs. ACT (reference group) ER- and PR- ER+ or PR+ 0-2cm cm 5.1cm+ LN 0 LN 1-3 LN 4-9 LN 10+ Good Intermediate Poor N No. of Events ACT ACTH HR HR with 95% CI


12 Cumulative Incidence (%) Years from Randomization San Antonio Breast Cancer Symposium, December 4-8, 2012 B-31/N9831 Cumulative Incidence of Distant Recurrence as a First Event ER and/or PR Positive ER and PR Negative AC P 22.3% AC P 21.5% Δ= 9.6% 12.7% Δ=9.6% 11.9% AC P+H AC P+H N Events AC P AC P+H N Events AC P AC P+H
13 Does the degree of HER2 amplification correlate with the degree of benefit from trastuzumab?
14 Hazard Ratio of Benefit to Trastuzumab by HER2 FISH Ratio in NCCTG N9831 Ratio (N) p-value < 2.0 (156) p = (253) (515) (473) (328) p = 0.05 p = 0.03 p = p = (70) p = Hazard ratio Reinholz M, SABCS 2007, abstr 36
15 What is the benefit of using trastuzumab with a non-anthracycline containing regimen?
16 BCIRG 006 AC T 4 x AC 4 x Docetaxel 60/600 mg/m mg/m 2 Her2+ (Central FISH) N+ or high risk N- AC TH 4 x AC 4 x Docetaxel 60/600 mg/m mg/m 2 1 Year Trastuzumab N=3,222 Stratified by Nodes and Hormonal Receptor Status TCH 6 x Docetaxel and Carboplatin 75 mg/m 2 AUC 6 1 Year Trastuzumab
17 BCIRG 006 Disease Free Survival (median follow-up 65 months) Patients Events HR P AC-TH <0.001 TCH AC-T Slamon D, et al. NEJM 365: , 2011
18 What is the benefit of using trastuzumab after chemotherapy is finished?
19 HERA TRIAL DESIGN Accrual (n=5102) Women with locally determined HER2-positive invasive early breast cancer Surgery + (neo)adjuvant CT ± RT Centrally confirmed IHC 3+ or FISH+ and LVEF 55% Randomization OBSERVATION n=1698 After ASCO 2005, option of switch to Trastuzumab 1 year Trastuzumab 8 mg/kg 6 mg/kg 3 weekly schedule n= years Trastuzumab 8 mg/kg 6 mg/kg 3 weekly schedule n=1701 CT, chemotherapy; RT, radiotherapy
20 HERA: Disease Free Survival 53% of Observation received trastuzumab Goldhirsch A, et al. Lancet 382: ,2013
21 SUMMARY OF DFS ITT ANALYSES FOR 1 YEAR TRASTUZUMAB VS. OBSERVATION ACROSS ANALYSIS TIME POINTS Median follow-up (% follow-up time after selective crossover) 2005 (0%) 1 yr MFU 0.54 DFS benefit No. of DFS events 1 year trastuzumab vs observation 127 vs 220 P< (4.3%) 2 yrs MFU vs 321 P< (33.8%) 4 yrs MFU vs 458 P< (48.5%) 8 yrs MFU vs 570 P< Favours 1 year trastuzumab Favours observation HR (95% CI) Goldhirsch A, et al. Lancet 382: ,2013
22 SUMMARY OF OS ITT ANALYSES FOR 1 YEAR TRASTUZUMAB VS. OBSERVATION ACROSS ANALYSIS TIME POINTS Median follow-up (% follow-up time after selective crossover) 2005 (0%) 1 yr MFU 0.76 OS benefit No. of deaths 1 year trastuzumab vs observation 29 vs 37 P= (4.1%) 2 yrs MFU vs 90 P= (30.9%) 4 yrs MFU vs 213 P= (45.5%) 8 yrs MFU vs 350 P= Favours 1 year trastuzumab Favours observation HR (95% CI) Goldhirsch A, et al. Lancet 382: ,2013
23 So is it better to start trastuzumab sequentially after completion of chemotherapy or concurrently with taxane chemotherapy?
24 NCCTG N9831 Trial Incorporating Trastuzumab in Adjuvant Therapy Arm A HER2 positive (FISH ratio 2 or IHC 3+ >10%) n=3,505 R A N D O M I Z E T AC Arm B T AC Arm C T AC H H = AC (doxorubicin/cyclophosphamide 60/600 mg/m 2 q3w 4) = T (paclitaxel 80 mg/m 2 /wk 12) = H (trastuzumab 4 mg/kg loading + 2 mg/kg/wk 51)
 Perez EA et al.")
25 N9831: Sequential (B) vs. Concurrent (C) Perez EA et al. J Clin Oncol 29: , 2011
26 Efficacy Summary Randomized Adjuvant Trastuzumab Trials TRIAL Pts TREATMENT B31/N CIRG HERA FinHER PACS AC TH AC T AC TH TCH AC T chemo H chemo obs V/T+H FEC V/T FEC FEC/ET H FEC/ET DFS (%) HR P 74* 62 84** * * < < < at 3 years * - at 8 years ** - at 5.5years OS (%) HR P 84* 75 92** * * < NR
27 How long should trastuzumab be given in the adjuvant setting?
28 Current Trials Assessing Duration of Trastuzumab SOLD (Finland) PHARE (France) Short-HER (Italy) Hellenic Group (Greece) Persephone (Great Britain) HERA Docetaxel + Trast (nine weeks) FEC X 3 Docetaxel + Trast (nine weeks) FEC X 3 Trast (total 1 year) Chemotherapy + Trast X 12 months Chemotherapy + Trast X 6 months Docetaxel + Trast (nine weeks) FEC X 3 AC/FEC X 4 Taxane + Trast X 4 Trast (18 weeks) FEC X 4 Docetaxel + Trast Trast (total 12 months) FEC X 4 Docetaxel + Trast Trast (total 6 months) Chemotherapy + Trast X 12 months Chemotherapy + Trast X 6 months Chemotherapy Trast X 1 year Chemotherapy Trast X 2 years
29 Disease-free survival (%) HERA: DFS FOR 2 YEARS VS. 1 YEAR TRASTUZUMAB AT 8 YRS MFU % 86.7% 81.6% 81.0% 75.8% 76.0% 60 Trastuzumab 2 years 40 Trastuzumab 1 year 20 Pts Events HR (2 vs 1) 95% CI p-value 2 years ( ) year Years from randomization No. at risk Trastuzumab 2 years Trastuzumab 1 year Goldhirsch A, et al. Lancet 382: ,2013
30 PHARE* Study design trastuzumab 6 months R Stratification 1. ER pos / neg 2. Chemo: concurrent/sequential trastuzumab up to 12 months 1690 patients stop trastuzumab 1690 patients Clinical exam LVEF mos Mammography Up to 60 mos * Protocol of Herceptin Adjuvant with Reduced Exposure Pivot X, et al, Lancet Oncol 14: , 2013
31 Probability Disease Free Survival Events HR 95%CI p-value H 12m 176 H 6m ( ) Months At risk H-12m H 6m H-12m H-6m Pivot X, et al, Lancet Oncol 14: , 2013
32 Primary endpoint scenarii A Equivalent B 6 month Superior C PHARE trial D 6 month Non Inferior E HR 6 month Inferior Pivot X, et al, Lancet Oncol 14: , 2013
33 Cardiac Risk Assessment with Anthracycline based regimens
34 B-31/N9831 LVEF Evaluation Schedule Control AC x 4 Paclitaxel 0 mo. 3 mos. 6 mos. 9 mos. Investigational AC x 4 Trastuzumab + Paclitaxel 18 mos. 0 mo. 3 mos. 6 mos. 9 mos. 18 mos.
35 Asymptomatic Patients Rules for Trastuzumab Continuation Based on Serial LVEF Relationship of LVEF to LLN Absolute decrease of < 10% Absolute decrease of 10% 15% Absolute decrease of 15% Within normal limits Cont. Cont. Hold * 1% 5% below LLN Cont. Hold * Hold * 6% below LLN Cont. * Hold * Hold * * Repeat LVEF assessment after 4 weeks If criteria for continuation is met then resume trastuzumab If 2 consecutive holds (or a total of 3 holds occur) then discontinue trastuzumab LLN = lower limit of normal.
36 % NSABP B-31: 7 year cumulative incidence of cardiac events ACPH arm; 4.0% HR=3.30;P-value- = ACP arm; 1.3% Years Post Day 1 Cyc 5 Romond et al. J Clin Oncol 30: , 2012
37 B-31: Potential Risk Factors for Congestive Heart Failure Risk Factors No. of Pts No. with CHF (%) P value Relative risk (95% CI) Age < (2.3%) Ref. group (5.1%) ( ) (5.4%) 2.4 ( ) Hypertension medications No (3.0%) Yes (6.8%) ( ) Baseline LVEF < (12.9%) Ref. group (3.8%) ( ) (2.1%) 0.2 ( ) Left-sided tumor & radiation No (3.9%) Yes (3.4%) ( )
38 Cardiac Risk Score (based on evaluable cohort in NSABP B-31) [7.0 + (0.04 x Age in years) (0.1 x Baseline percent LVEF)] x Romond et al. J Clin Oncol 30: , 2012
39 Predicted Probability of CE % % % % % NSABP B-31 Cardiac Risk Assessment Cardiac Risk Score Romond et al. J Clin Oncol 30: , 2012
40 Examples: (a)age 45, LVEF=65%, CRS=48.3 (b)age 65, LVEF=55, CRS=86.1
41 Predicted Probability of CE % % % % % NSABP B-31: Examples of Cardiac Risk Assessment b a Cardiac Risk Score
42 Summary of Cardiac Dysfunction in the Large Adjuvant Trastuzumab Trials Trial Median Follow-up (years) Treatment Arms Class III/IV CHF (%) Cardiac Deaths NSABP B AC P + Trast AC P NCCTG N AC P+Trast AC P Trast AC P HERA 8 Chemo Trast Chemo Observation BCIRG AC D+Trast D+Carboplatin+Trast AC D A: doxorubicin; C: cyclophosphamide; P: paclitaxel; D: docetaxel
43 Low Risk and Node Negative Cancers
44 British Columbia Tumor Registry HER2 status Stage I Only (T1N0) n 10 yr RFS (%) HER HER P=0.21 Chia S et al. J Clin Oncol :

45 BCIRG 006 Node Negative Patients Valero et al, ASCO 2011, Abstr 553
46 BCIRG 006 Disease Free Survival Valero et al, ASCO 2011, Abstr 553
47 US Oncology Phase II Adjuvant Trial Docetaxel + Cyclophosphamide + Trastuzumab Open label, Phase II 493 patients registered Low risk HER2 positive operable breast cancer: T1-2, N0-1a LVEF 50% by MUGA or echo Treatment regimen: (4 chemotherapy cycles) Docetaxel 75 mg/m² day 1 Cyclophosphamide 600 mg/m² day 1 Trastuzumab 4 mg/kg (loading) then 2mg/kg day 1,8,15 Following completion of chemo: trastuzumab 6mg/kg q 21 days to complete 1 year targeted therapy Jones SE, et al. Lancet Oncol 14: , 2013

48 Baseline Patient Characteristics Jones SE, et al. Lancet Oncol 14: , 2013
49 US Oncology Phase II Adjuvant Trial Docetaxel + Cyclophosphamide + Trastuzumab Disease-free Survival Overall Survival Jones SE, et al. Lancet Oncol 14: , 2013
50 Study Design (APT Trial) HER2+ ER+ or ER- Node Negative < 3 cm Enroll P P P P P P P P P P P T T T T T T T T T T T PACLITAXEL 80 mg/m 2 + TRASTUZUMAB 2 mg/kg x 12 P T Planned N=400 T T T T T T T T T T T T T FOLLOWED BY 13 EVERY 3 WEEK DOSES OF TRASTUZUMAB (6 mg/kg)* *Dosing could alternatively be 2 mg/kg IV weekly for 40 weeks ** Radiation and hormonal therapy was initiated after completion of paclitaxel Tolaney S, et al. SABCS 2013, abstr S1-04
51 San Antonio Breast Cancer Symposium- Cancer Therapy and Research Center at UT Health Science Center--December 10-14, 2013 Patient Characteristics Age < Size of Primary Tumor T1a 0.5 cm T1b > T1c > T2 > Histologic Grade I Well differentiated II Moderately differentiated III Poorly differentiated HR Status (ER and/or PR) Positive Negative N % % 50% Tolaney S, et al. SABCS 2013, abstr S1-04
52 San Antonio Breast Cancer Symposium- Cancer Therapy and Research Center at UT Health Science Center- December 10-14, 2013 Recurrence-Free Survival (Probability) Recurrence-Free Interval 3-year RFI 95% Conf. Interval 99.2% 98.3% to >99.9% Recurrence Free Interval= Invasive Local/Regional Recurrence Distant Recurrence Death from Breast Cancer All patients Time (Months) Number at risk Tolaney S, et al. SABCS 2013, abstr S1-04
53 What about really small node negative breast cancers 1.0 cm (T1a/b)?

54 Subset DFS and OS results US Oncology Phase II Trial of TC + Trastuzumab Jones SE, et al. Lancet Oncol 14: , 2013
55 T1abN0M0 HER2+ Breast Cancers Kaiser Permanente Northern California 3.3 million members 16,975 new Breast Cancers diagnosed from 1/1/2000 to 12/31/2006 HER2, ER, PR IHC mandatory on all cases 2,168 HER2+ (IHC 3+ or FISH ratio >2.0) 237 T1a or T1b Fehrenbacher L, et al. J Clin Oncol 32: , 2014
56 Recurrences:T1a+bN0 HER2+ Median F/U 5.8 yrs N# T1aN0 116 T1bN0 121 T1abN0 237 Invasive Cancer Recurrence (%) (4) 3.5% (11) 9.1% (15) 6.3% Invasive Cancer Local Recurrence Only (%) (3) 2.6% (4) 3.3% (7) 2.9% Invasive Cancer Distant Recurrence (%) (1) 0.9% (7) 5.8% (8) 3.4% 5 year Relapse Free Interval (K-M) 97.4% (95% CI, 92.1.,99.1) 91.1% (95% CI,83.2,95.3) 94.2% (95% CI, 89.9, 96.7) 5 year Distant Relapse Free Interval (K-M) 99.1% (95% CI,93.9, 99.9) 94.0% (95% CI, 87.1, 97.3) 96.5% (95% CI, 92.8, 98.3) Fehrenbacher L, et al. J Clin Oncol 32: , 2014
57 Treatments Received by T1abN0M0 Received Chemo Received Trastuzumab Distant Recur No Chemo Distant Recur with Chemo All T1abN0 59/237 (24.9%) 20/237(8.4%) 5/178 (2.8%) 3/59 (5.1%) Pre /153 (2.6%) /84 (19.0%) T1aN0* 15/116 (12.9%) 8/116 (6.8%) 1/101 (1.0%) 0/15(0%) T1bN0 44/121 (36.3%) 12/121 (9.9%) 4/77 (5.2%) 3/44(6.8%) *Note:48% ER negative Fehrenbacher L, et al. J Clin Oncol 32: , 2014
58 NCCN Breast Cancer Guidelines (v ) T1/N0, HER2-positive Tumor Size Recommendation > 1cm Chemotherapy + trastuzumab* cm 0.5cm Consider chemotherapy + trastuzumab* No adjuvant therapy* * endocrine therapy if HR +
59 Recently Reported Adjuvant Trials
 Hormone Receptor Status NSABP/CIRG CONTACT TCH ± B FEC")
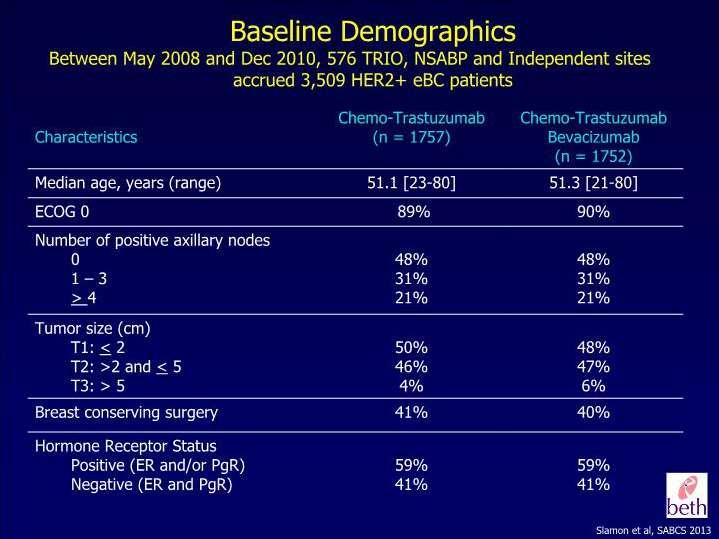
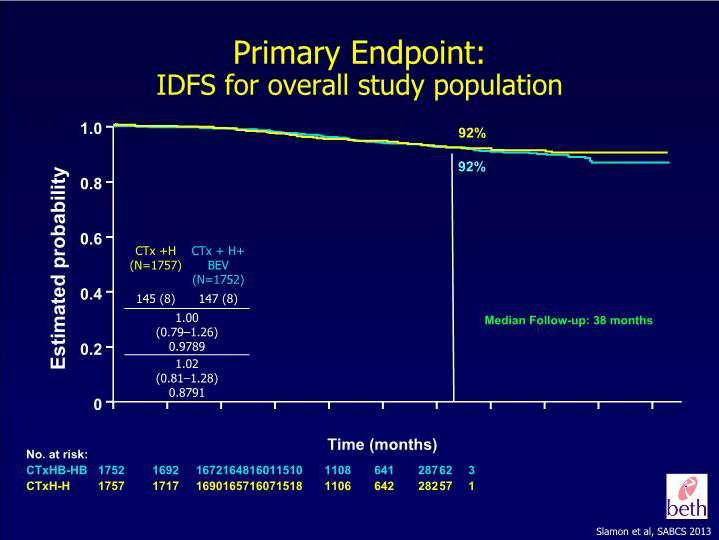
60 BETH TRIAL Node-Positive or High Risk Node- Negative Breast Cancer HER2 Positive by Central Testing STRATIFICATION Number of positive Nodes (0, ) Hormone Receptor Status NSABP/CIRG CONTACT TCH ± B FEC TH ± B
61
62
63 Does improved neo-adjuvant response predict improved disease-free and overall survival?
64 Collaborative Trials in Neoadjuvant Breast Cancer (CTNeoBC): Association of pcr with EFS in Her2+ Subtype HR=0.39, P* < HR=0.58, P* = HR=0.25, P* < pcr=ypt0/is ypn0 Cortazar P, et al. Lancet 384:164 72,2014



65 Lapatinib Lapatinib is an oral small-molecule dual inhibitor of ERBB1 and ERBB2 tyrosine kinase: Works intracellularly Binds reversibly to the cytoplasmic ATP-binding site of the kinase, thereby preventing receptor phosphorylation and activation Downstream signaling cascade
66 Phase III NeoALTTO Trial Eligibility criteria: Operable HER2 + breast cancer T > 2 cm LVEF 50% Stratify by: Tumor size ( 5 cm vs. > 5 cm) HR status (positive vs. negative) N status (0/1 vs. 2) R A N D O M I Z E (n = 455) Lapatinib a 1000 mg/day Trastuzumab 2 mg/kg/week (4-mg/kg loading dose) 18 cycles Paclitaxel 80 mg/m 2 /week 12 cycles starting at week 7 Lapatinib 1500 mg/day Paclitaxel 80 mg/m 2 /week 12 cycles starting at week 7 Trastuzumab 2 mg/kg/week (4-mg/kg loading dose) 18 cycles Paclitaxel 80 mg/m 2 /week 12 cycles starting at week 7 a 750 mg/day with paclitaxel S U R G E R Y Baselga J et al. Lancet 379: ,2012
67 NeoALTTO: Efficacy Lapatinib/ Trastuzumab (n = 152) Lapatinib (n = 154) Trastuzumab (n = 149) Pathologic CR, Breast 51% 25% 29.5% By hormone receptor status Positive 42% 16% 23% Negative 61% 34% 36.5% Total Pathologic CR, Breast +Nodes (n = 145) (n = 150) (n = 145) 47% 20% 28% Objective Response (n = 152) (n = 154) (n = 149) At week 6 67% 53% 30% At surgery 80% 74% 70.5% All differences between lapatinib/trastuzumab and trastuzumab alone are significant (P <.05). Baselga J et al. Lancet 379: ,2012.
68 ALTTO Adjuvant Lapatinib and/or Trastuzumab Treatment Optimization WILL DUAL ANTI-HER2 BLOCKADE IMPROVE DISEASE-FREE AND OVERALL SURVIVAL IN THE ADJUVANT SETTING?
.")
69 DESIGN 1: SEQUENTIAL ANTI-HER2 THERAPY AFTER ALL CHEMOTHERAPY (N= 4,613) 3-weekly Trastuzumab Lapatinib* All (neo)adjuvant chemo prior to anti-her2 therapy Weekly Trastuzumab wash out Lapatinib 12 weeks 6 wks 34 weeks 12 weeks Lapatinib + 3-weekly Trastuzumab 6 wks 34 weeks All patients: radiotherapy, if indicated (concomitant with targeted therapy). Hormone receptor-positive patients: endocrine therapy for at least 5 years. *The L alone arm was closed on 18 Aug 2011 following IDMC recommendation 52 weeks Tras alone: 8 mg/kg 6 mg/kg iv, q21 days Lap alone: 1500 mg po qd Tras Lap: T 4 mg/kg 2 mg/kg iv q7 days; L 1500 mg po qd Tras + Lap: T 8 mg/kg 6 mg/kg iv, q21 days; L 1000 mg po qd
70 DESIGN 2: CONCURRENT ANTI-HER2 THERAPY AFTER ANTHRACYCLINE-BASED CHEMOTHERAPY (N= 3,337) w-p or 3-w D 3-weekly Trastuzumab w-p or 3-w D Lapatinib* Anthracyclinebased chemo first Weekly w-p or 3-w D Trastuzumab wash out Lapatinib 12 weeks 6 wks 34 weeks w-p or 3-w D 12 weeks Lapatinib + 3-weekly Trastuzumab 6 wks 34 weeks w-p: weekly paclitaxel (80 mg/m 2 ); 3-w D: q3 weeks docetaxel ( mg/m 2 ) All patients: radiotherapy, if indicated (concomitant with targeted therapy). Hormone receptor-positive patients: endocrine therapy for at least 5 years. *The L alone arm was closed on 18 Aug 2011 following IDMC recommendation 52 weeks Tras alone: 4 mg/kg 2 mg/kg iv, q7 days 6 mg/kg iv, q21 days Lap alone: 750 mg po qd 1500 mg qd Tras Lap: T 4 mg/kg 2 mg/kg iv q7 days; L 1500 mg po qd Tras + Lap: T 4 mg/kg 2 mg/kg iv, q7 days 6 mg/kg iv, q21 days; L 750 mg po qd 1000 mg qd
71 DESIGN 2B: CONCURRENT ANTI-HER2 THERAPY WITH A NON-ANTHRACYCLINE CHEMOTHERAPY (N= 431) 3-w D + carbo 3-weekly Trastuzumab Nonanthracyclinebased chemo with anti-her2 therapy 3-w D + carbo Weekly 3-w D + carbo Trastuzumab Lapatinib* wash out Lapatinib 18 weeks 6 wks 28 weeks 3-w D + carbo 18 weeks Lapatinib + 3-weekly Trastuzumab 6 wks 28 weeks 3-w D: q3 weeks docetaxel (75 mg/m 2 ); carbo: carboplatin (AUC 6) All patients: radiotherapy, if indicated (concomitant with targeted therapy). Hormone receptor-positive patients: endocrine therapy for at least 5 years. *The L alone arm was closed on 18 Aug 2011 following IDMC recommendation 52 weeks Tras alone: 4 mg/kg 2 mg/kg iv, q7 days 6 mg/kg iv, q21 days Lap alone: 750 mg po qd 1500 mg qd Tras Lap: T 4 mg/kg 2 mg/kg iv q7 days; L 1500 mg po qd Tras + Lap: T 4 mg/kg 2 mg/kg iv, q7 days 6 mg/kg iv, q21 days; L 750 mg po qd 1000 mg qd
72 DISTRIBUTION OF THE STRATIFICATION Hormone Receptor Status FACTORS BY TREATMENT ARM L + T (N = 2,093) T L (N = 2,091) T (N = 2,097) Positive 1,203 (57%) 1,205 (58%) 1,200 (57%) Negative 890 (43%) 886 (42%) 897 (43%) Timing of chemotherapy Sequential (Design 1) 1,155 (55%) 1,143 (55%) 1,147 (55%) Concurrent (Design 2 and 2B) 938 (45%) 948 (45%) 950 (45%) Lymph Node Status Not applicable (neoadjuvant chemotherapy) 168 (8%) 170 (8%) 181 (9%) Node negative 845 (40%) 842 (40%) 844 (40%) 1-3 positive nodes 617 (29%) 617 (30%) 603 (29%) >=4 positive nodes 463 (22%) 462 (22%) 469 (22%)
73 DISTRIBUTION OF PATIENT CHARACTERISTICS BY TREATMENT ARM L + T (N = 2,093) T L 76 T (N = 2,097) (N = 2,091) Menopausal Status Premenopausal 908 (43%) 929 (44%) 908 (43%) Postmenopausal or male 1,185 (57%) 1,162 (56%) 1,189 (57%) Pathological primary tumor size - largest diameter of invasive component Missing cm 937 (45%) 938 (46%) 942 (46%) > 2cm to 5cm 1,002 (49%) 980 (48%) 990 (48%) > 5cm 127 (6%) 132 (6%) 127 (6%) Histologic grade Missing Gx: Differentiation cannot be assessed 79 (4%) 61 (3%) 59 (3%) G1: Well differentiated 51 (2%) 59 (3%) 48 (2%) G2: Moderately differentiated 774 (37%) 793 (38%) 744 (36%) G3: Poorly differentiated/undifferentiated 1,179 (57%) 1,171 (56%) 1,237 (59%)
74 DISEASE-FREE SURVIVAL (DFS) ANALYSIS MFU = 4.5 yrs * ** * 97.5% CI **p-value required for statistical significance Piccart-Gebhart M. ASCO 2014, LBA 4
 Pertuzumab.")
75 Fig. 2 Epitope binding of HER2 and EGFR therapeutic antibodies.(b) Pertuzumab. M X Sliwkowski, and I Mellman Science 2013;341: Published by AAAS
76 Randomized Phase II Study of Neoadjuvant Pertuzumab Plus Trastuzumab: NeoSphere Eligibility criteria: Operable or locally advanced/ inflammatory HER2 + breast cancer Chemonaive Primary tumors > 2 cm R A N D O M I Z E Docetaxel (T) Trastuzumab (H) (n = 107) Docetaxel (T) Trastuzumab (H) Pertuzumab (P) (n = 107) Trastuzumab (H) Pertuzumab (P) (n = 107) Docetaxel (T) Pertuzumab (P) (n = 96) All q 3 weeks 4 Primary endpoint: pcr rates Secondary endpoints including: clinical response S U R G E R Y FEC q 3 weeks 3 H q 3 weeks, cycles 5-17 FEC q 3 weeks 3 H q 3 weeks, cycles 5-17 T q 3 weeks 4 FEC q 3 weeks 3 H q 3 weeks, cycles 5-17 FEC q 3 weeks 3 H q 3 weeks, cycles 5-21 FEC: 5-fluorouracil/epirubicin/ cyclophosphamide Gianni et al. SABCS 2010; abstract S3-2.
77 NeoSphere: Efficacy of Neoadjuvant Pertuzumab Plus Trastuzumab Pathologic Complete Response TH (n = 107) THP (n = 107) HP (n = 107) TP (n = 96) pcr in Breast 29% 46% 17% 24% By Hormone Receptor Status ER + /PgR + 20% 26% 6% 17% ER /PgR 37% 63% 29% 30% By Nodal Status Node negative 21.5% 39% 11% 18% Node positive 7.5% 6.5% 6% 6% CR + PR + SD a 107 (100%) 106 (99%) 99 (92.5%) 94 (98%) a Investigator assessed T = docetaxel H = trastuzumab P = pertuzumab Gianni et al. SABCS 2010; abstract S3-2.
78 TRYPHAENA Cycles A FEC Docetaxel HER2-positive EBC centrally confirmed (n = 225) B C Pertuzumab + trastuzumab FEC Docetaxel Docetaxel Pertuzumab + trastuzumab Pertuzumab + trastuzumab S u r g e r y Trastuzumab to complete 1 year Carboplatin All 3 arms were experimental Study dosing q3w: FEC: 500 mg/m 2, 100 mg/m 2, 600 mg/m 2 Carboplatin: AUC 6 Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance Pertuzumab: 840 mg loading dose, 420 mg maintenance Docetaxel: 75 mg/m 2 (escalating to 100 mg/m 2 if tolerated, in Arms A and B only) Schneeweiss, et al. Annals Onc 24: ,2013
79 Pathologic complete response (%) TRYPHAENA: Pathologic complete response ypt0/is ypt0 ypn FEC+H+P x3 T+H+P x3 (n = 73) FEC x3 T+H+P x3 (n = 75) TCH+P x6 (n = 77) FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab Schneeweiss, et al. Annals Onc 24: ,2013
 FEC x3 T+H+P x3 (n = 75) TCH+P x6 (n = 77) ER, estrogen receptor; FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; PR, progesterone")
80 Pathologic complete response (%) Pathologic complete response by hormone receptor status ypt0/is ER- and PR-negative ER- and/or PR-positive FEC+H+P x3 T+H+P x3 (n = 73) FEC x3 T+H+P x3 (n = 75) TCH+P x6 (n = 77) ER, estrogen receptor; FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; PR, progesterone receptor; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab Schneeweiss, et al. Annals Onc 24: ,2013

81 Fig. 2 Epitope binding of HER2 and EGFR therapeutic antibodies.(d) T-DM1. M X Sliwkowski, and I Mellman Science 2013;341: Published by AAAS
82
83 NSABP B-50-I/GBG 77/Roche BO27938 Katherine: Study Schema Residual Invasive HER2 Positive Breast Cancer in Breast and/or Axillary Nodes after Neoadjuvant Taxane/Trastuzumab ± Anthracycline Randomization Trastuzumab 6 mg/kg q3wk x 14 doses T-DM1 3.6 mg/kg q3wk x 14 doses Radiation per standard guidance; hormone therapy if ER or PgR pos Accrual goal patients
84 A Final Question: Does the standard definition of HER2 positivity mean the same thing as a predictor of response to trastuzumab + chemotherapy in the adjuvant setting as it does for metastatic breast cancer?
85 B-31: distribution of cases according to central HER2 assay IHC=0 IHC=1 IHC=2 IHC=3 unk FISH Central assay negative FISH Paik, ASCO 2007, abstr 511
86 % Disease-Free NSABP B-31 Updated 2009 Disease Free Survival FISH Negative, IHC 0, 1+, 2+ Breast Cancer Pts. NSABP B-31:FISH Negative, IHC 0,1+,2+ ACT ACTH N #Event HR p-value HR=0.64, p= Time from Randomization
87 HER2 expression is a continuous variable HER2 by RT-PCR (relative to ref genes; log2) Hard to imagine that these two tumors respond differently to trastuzumab Cut-off Based on IHC/FISH Case Slide courtesy of S Paik
88
89 Summary of take-home messages Virtually all invasive breast cancers should be tested for HER2. HER2 testing must be done in laboratories with rigorous quality controls. Addition of one year of trastuzumab to adjuvant chemotherapy decreased the rate of breast cancer events by 25-40% in the large adjuvant trials. Focally positive cancers also derive similar benefit. The inclusion of pertuzumab along with trastuzumab and chemotherapy in pre-operative treatment of early stage disease is now a FDA approved standard of care. NCCN 2014 guidelines also provide for option to include pertuzumab concurrent with chemotherapy and trastuzumab in the adjuvant AC-TH and TCH regimens.
90 Summary of take-home messages Cardiac monitoring must be done in all patients treated with adjuvant trastuzumab with appropriate holds when indicated. Most patients recover normal ejection fractions if holding rules are followed. In B-31 the combination of age and baseline LVEF correlates with risk of CHF when trastuzumab/paclitaxel is used following AC. Radiation and hormone therapy may be given after chemotherapy concurrently with trastuzumab. Neo-adjuvant trials are appropriate for studying new targeted agents for specific patient subsets but appropriate patient selection for incorporating new agents in adjuvant trials is critical. The criteria of HER2 positivity for discerning adjuvant trastuzumab benefit is being studied further in a prospective randomized trial (NSABP B=47).

91 Thank you!
Treatment of Early Stage HER2-positive Breast Cancer
 Treatment of Early Stage HER2-positive Breast Cancer 3 November 2012 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky Lexington, KY Molecular Portrait
Treatment of Early Stage HER2-positive Breast Cancer 3 November 2012 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky Lexington, KY Molecular Portrait
The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?
 as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?") 1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
Novel Preoperative Therapies for HER2-Positive Breast Cancer. Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center
 Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Treatment of Early-Stage HER2+ Breast Cancer
 Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer
 Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA
 Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance
 Oncology Department Vall d Hebron University Hospital Barcelona. Spain Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance Javier Cortés June/2013 MD Anderson experience Buzdar et
Oncology Department Vall d Hebron University Hospital Barcelona. Spain Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance Javier Cortés June/2013 MD Anderson experience Buzdar et
Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre
 Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre Recurrence of HER2-positive breast cancer (A) Time to
Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre Recurrence of HER2-positive breast cancer (A) Time to
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012
 Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Existe-t-il un sous groupe à risque qui pourrait bénéficier d une modification de la durée de traitement par trastuzumab? X. Pivot CHRU De Besançon
 Existe-t-il un sous groupe à risque qui pourrait bénéficier d une modification de la durée de traitement par trastuzumab? X. Pivot CHRU De Besançon In 25 results of 4 Adjuvant Herceptin trials have definitively
Existe-t-il un sous groupe à risque qui pourrait bénéficier d une modification de la durée de traitement par trastuzumab? X. Pivot CHRU De Besançon In 25 results of 4 Adjuvant Herceptin trials have definitively
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2017 Relative Risk HER2-positive Breast
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2017 Relative Risk HER2-positive Breast
(Neo) Adjuvant systemic therapy for HER-2+ EBC
 Adjuvant systemic therapy for HER-2+ EBC") (Neo) Adjuvant systemic therapy for HER-2+ EBC F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESMO Board of Directors & NR Committee Chair ESO Breast Cancer Program
(Neo) Adjuvant systemic therapy for HER-2+ EBC F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESMO Board of Directors & NR Committee Chair ESO Breast Cancer Program
Non-Anthracycline Adjuvant Therapy: When to Use?
 Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
(NEO-)ADJUVANT THERAPY FOR HER-2+ EBC
ADJUVANT THERAPY FOR HER-2+ EBC") (NEO-)ADJUVANT THERAPY FOR HER-2+ EBC Rebecca Dent, MD FRCP (Canada) Senior Consultant, National Cancer Center Singapore Associate Professor, Duke-NUS www.abc-lisbon.org When to question a pathology report?
(NEO-)ADJUVANT THERAPY FOR HER-2+ EBC Rebecca Dent, MD FRCP (Canada) Senior Consultant, National Cancer Center Singapore Associate Professor, Duke-NUS www.abc-lisbon.org When to question a pathology report?
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Herceptin Pivotal Studies
 Herceptin Pivotal Studies Nuhad K Ibrahim, MD, FACP Associate Professor of Medicine Breast Medical Oncology Department MD Anderson Cancer Center Houston, TX, USAE-mail: nibrahim@mdanderson.org Herceptin
Herceptin Pivotal Studies Nuhad K Ibrahim, MD, FACP Associate Professor of Medicine Breast Medical Oncology Department MD Anderson Cancer Center Houston, TX, USAE-mail: nibrahim@mdanderson.org Herceptin
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives
 Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
The Expert Thoughts. Alessandra Fabi Oncologia Medica 1
 The Expert Thoughts Alessandra Fabi Oncologia Medica 1 My Thoughts Neoadjuvant: from the lessons of the history Adjuvant: Escalation and De-escalation Advanced and HER2+ : field for immunomodulation Brain
The Expert Thoughts Alessandra Fabi Oncologia Medica 1 My Thoughts Neoadjuvant: from the lessons of the history Adjuvant: Escalation and De-escalation Advanced and HER2+ : field for immunomodulation Brain
NeoadjuvantTreatment In BC When, How, Who?
 NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
Novel Preoperative Therapies for HER2-Positive Breast Cancer
 Key Findings to Date in the Neoadjuvant Therapy of H2+ Breast Cancer Novel Preoperative Therapies for H2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive
Key Findings to Date in the Neoadjuvant Therapy of H2+ Breast Cancer Novel Preoperative Therapies for H2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive
Update in the treatment of Her2- overexpressing breast cancers. Fabrice ANDRE Institut Gustave Roussy Villejuif, France
 Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER. Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx
 OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
Adjuvant Chemotherapy + Trastuzumab
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Chemotherapy + Trastuzumab (Optimal Drugs / Dosage / Trastuzumab) Adjuvant Chemotherapy (Optimal Drugs / Optimal Dosage
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Chemotherapy + Trastuzumab (Optimal Drugs / Dosage / Trastuzumab) Adjuvant Chemotherapy (Optimal Drugs / Optimal Dosage
PRO: Pathologic Complete Response Does Predict Outcome for Early Stage Breast Cancer Patients
 PRO: Pathologic Complete Response Does Predict Outcome for Early Stage Breast Cancer Patients Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute
PRO: Pathologic Complete Response Does Predict Outcome for Early Stage Breast Cancer Patients Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute
(Neo)Adjuvant Chemotherapy and biological Agents (essentials in HER2 and TN early breast cancer)
Adjuvant Chemotherapy and biological Agents (essentials in HER2 and TN early breast cancer)") (Neo)Adjuvant Chemotherapy and biological Agents (essentials in HER2 and TN early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Neoadjuvant
(Neo)Adjuvant Chemotherapy and biological Agents (essentials in HER2 and TN early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Neoadjuvant
Nadia Harbeck Breast Center University of Cologne, Germany
 Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA
 Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016
 Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016 Yes! Age disparities vary by tumor subtype Genomic risk prediction data in young women Adjuvant systemic therapy
Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016 Yes! Age disparities vary by tumor subtype Genomic risk prediction data in young women Adjuvant systemic therapy
Postoperative Adjuvant Chemotherapies. Stefan Aebi Luzerner Kantonsspital
 Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Highlights. Padova,
 Highlights P Pronzato Padova, 17.11.2012 Last 12 Months Main Meetings SABCS 2011 (San Antonio) EBCC 8 2012 (Wien) ASCO 2012 (Chicago) ESMO/ECCO 2012 (Wien) The Medical Oncology Job Risk Manager Strategy
Highlights P Pronzato Padova, 17.11.2012 Last 12 Months Main Meetings SABCS 2011 (San Antonio) EBCC 8 2012 (Wien) ASCO 2012 (Chicago) ESMO/ECCO 2012 (Wien) The Medical Oncology Job Risk Manager Strategy
Current and Future perspectives of HER2+ BC
 2018.4.6 GBCC Satellite symposium Current and Future perspectives of HER2+ BC Jee Hyun Kim, M.D., Ph.D. Seoul National University Bundang Hospital Seoul National University College of Medicine Disclaimer
2018.4.6 GBCC Satellite symposium Current and Future perspectives of HER2+ BC Jee Hyun Kim, M.D., Ph.D. Seoul National University Bundang Hospital Seoul National University College of Medicine Disclaimer
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
HER2-positive Breast Cancer
 HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer
 New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
Introduction. Approximately 20% of invasive breast cancers
 Introduction Approximately 2% of invasive breast cancers overexpress HER2 The current standard of care for neoadjuvant therapy is dual-targeted therapy with trastuzumab and pertuzumab plus chemotherapy
Introduction Approximately 2% of invasive breast cancers overexpress HER2 The current standard of care for neoadjuvant therapy is dual-targeted therapy with trastuzumab and pertuzumab plus chemotherapy
Considerations in Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
FDA Briefing Document Oncologic Drugs Advisory Committee Meeting. September 12, sbla /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc.
 Applicant: Genentech, Inc.") /51 FDA Briefing Document Oncologic Drugs Advisory Committee Meeting September 12, 2013 /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc. Disclaimer: The attached package contains background information
/51 FDA Briefing Document Oncologic Drugs Advisory Committee Meeting September 12, 2013 /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc. Disclaimer: The attached package contains background information
Target biologico e meccanismo d azione dei farmaci anti-her2: il continuum dal setting Neoadiuvante alla malattia metastatica
 Target biologico e meccanismo d azione dei farmaci anti-her2: il continuum dal setting Neoadiuvante alla malattia metastatica Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental
Target biologico e meccanismo d azione dei farmaci anti-her2: il continuum dal setting Neoadiuvante alla malattia metastatica Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
ASCO and San Antonio Updates
 ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
Systemic therapy: HER-2 update. Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven
 Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Treatment of HER-2 positive breast cancer
 EJC SUPPLEMENTS 6 (2008) 21 25 available at www.sciencedirect.com journal homepage: www.ejconline.com Treatment of HER-2 positive breast cancer Matteo Clavarezza, Marco Venturini * Ospedale Sacro Cuore
EJC SUPPLEMENTS 6 (2008) 21 25 available at www.sciencedirect.com journal homepage: www.ejconline.com Treatment of HER-2 positive breast cancer Matteo Clavarezza, Marco Venturini * Ospedale Sacro Cuore
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Appendix Four. Clinical effectiveness. Contents
 Appendix Four. Clinical effectiveness Contents 1. Treatment regimens and available trial data... 1 Treatment regimes in randomised controlled trials... 1 Trial outcomes as reported... 10 2. Increasing
Appendix Four. Clinical effectiveness Contents 1. Treatment regimens and available trial data... 1 Treatment regimes in randomised controlled trials... 1 Trial outcomes as reported... 10 2. Increasing
COME HOME Innovative Oncology Business Solutions, Inc.
 Innovative Oncology Business Solutions, Inc. Breast Cancer Diagnostic/Therapeutic Pathway V11, April 2015 Required Structured Data Fields: ICD9 Code Stage Staging Components Performance Status Treatment
Innovative Oncology Business Solutions, Inc. Breast Cancer Diagnostic/Therapeutic Pathway V11, April 2015 Required Structured Data Fields: ICD9 Code Stage Staging Components Performance Status Treatment
Adjuvant Chemotherapy TNBC & HER2 Subtype
 Adjuvant Chemotherapy TNBC & HER2 Subtype 2015.08.15 Gun Min Kim Yonsei Cancer Center Division of Medical Oncology Department of Internal Medicine Yonsei University College of Medicine gmkim77@yuhs.ac
Adjuvant Chemotherapy TNBC & HER2 Subtype 2015.08.15 Gun Min Kim Yonsei Cancer Center Division of Medical Oncology Department of Internal Medicine Yonsei University College of Medicine gmkim77@yuhs.ac
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY. Dr. Carlos Garbino
 EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
BREAST CANCER RISK REDUCTION (PREVENTION)
") BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Systemic Therapy Considerations in Inflammatory Breast Cancer
 Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Adjuvant chemotherapy in older breast cancer patients: how to decide?
 Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Dennis J Slamon, MD, PhD
 I N T E R V I E W Dennis J Slamon, MD, PhD Dr Slamon is Professor of Medicine, Chief of the Division of Hematology/Oncology and Director of Clinical and Translational Research at UCLA s David Geffen School
I N T E R V I E W Dennis J Slamon, MD, PhD Dr Slamon is Professor of Medicine, Chief of the Division of Hematology/Oncology and Director of Clinical and Translational Research at UCLA s David Geffen School
The HERA Study Team. Presented by Ian E. Smith
 Trastuzumab Following Adjuvant Chemotherapy in HER2-Positive Early Breast Cancer (HERA Trial): Disease-Free and Overall Survival after 2 Year Median Follow-Up The HERA Study Team Presented by Ian E. Smith
Trastuzumab Following Adjuvant Chemotherapy in HER2-Positive Early Breast Cancer (HERA Trial): Disease-Free and Overall Survival after 2 Year Median Follow-Up The HERA Study Team Presented by Ian E. Smith
Point of View on Early Triple Negative
 Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014
 MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
ASCO 2017 BREAST CANCER HIGHLIGHTS
 Post-ASCO 24 th June 2017, Dolce La Hulpe, Belgium ASCO 2017 BREAST CANCER HIGHLIGHTS Martine J. Piccart-Gebhart, MD, PhD Jules Bordet Institute, Brussels, Belgium Université Libre de Bruxelles Breast
Post-ASCO 24 th June 2017, Dolce La Hulpe, Belgium ASCO 2017 BREAST CANCER HIGHLIGHTS Martine J. Piccart-Gebhart, MD, PhD Jules Bordet Institute, Brussels, Belgium Université Libre de Bruxelles Breast
Adjuvant Systemic Therapy in Early Stage Breast Cancer
 Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Chemotherapy for Isolated Locoregional Recurrence
 Chemotherapy for Isolated Locoregional Recurrence Michelle Melisko MD Assistant Clinical Professor UCSF Helen Diller Family Comprehensive Cancer Center MBC and Improved Median Survival with New Therapies
Chemotherapy for Isolated Locoregional Recurrence Michelle Melisko MD Assistant Clinical Professor UCSF Helen Diller Family Comprehensive Cancer Center MBC and Improved Median Survival with New Therapies
Neoadjuvant and Adjuvant Therapy for HER2 Positive Disease
 ADJUVANT AND NEOADJUVANT THERAPY FOR HER2-POSITIVE DISEASE Neoadjuvant and Adjuvant Therapy for HER2 Positive Disease Stephen K. Chia, MD, FRCP(C) OVERVIEW Since the initial description of the HER2 proto-oncogene
ADJUVANT AND NEOADJUVANT THERAPY FOR HER2-POSITIVE DISEASE Neoadjuvant and Adjuvant Therapy for HER2 Positive Disease Stephen K. Chia, MD, FRCP(C) OVERVIEW Since the initial description of the HER2 proto-oncogene
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
XII Michelangelo Foundation Seminar
 XII Michelangelo Foundation Seminar Paradigm shift? The Food and Drug Administration collaborative project P. Cortazar, Silver Spring, USA FDA Perspective: Moving from Adjuvant to Neoadjuvant Trials in
XII Michelangelo Foundation Seminar Paradigm shift? The Food and Drug Administration collaborative project P. Cortazar, Silver Spring, USA FDA Perspective: Moving from Adjuvant to Neoadjuvant Trials in
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pertuzumab (Perjeta) Neoadjuvant Breast Cancer April 30, 2015
 Neoadjuvant Breast Cancer April 30, 2015") pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pertuzumab (Perjeta) Neoadjuvant Breast Cancer April 30, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Pertuzumab (Perjeta) Neoadjuvant Breast Cancer April 30, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Early Stage Disease. Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center
 SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
Non-anthracycline Adjuvant regimens in Early Breast Cancer. Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center
 Non-anthracycline Adjuvant regimens in Early Breast Cancer Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center Contents Role of Anthracyclines in adjuvant treatment EBCTCG2012
Non-anthracycline Adjuvant regimens in Early Breast Cancer Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center Contents Role of Anthracyclines in adjuvant treatment EBCTCG2012
Do we have to change our anti-cancer strategy in case of cardiac toxicity? Guy Jerusalem, MD, PhD
 Do we have to change our anti-cancer strategy in case of cardiac toxicity? Point of view of the oncologist Guy Jerusalem, MD, PhD CHU Sart Tilman Liège Anticancer therapy: cardiac toxicity New anticancer
Do we have to change our anti-cancer strategy in case of cardiac toxicity? Point of view of the oncologist Guy Jerusalem, MD, PhD CHU Sart Tilman Liège Anticancer therapy: cardiac toxicity New anticancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014
 Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
新竹馬偕紀念醫院癌症中心 乳癌化學治療藥物處方
 新竹馬偕紀念醫院癌症中心 乳癌化學治療藥物處方 文件修訂記錄 修正次數 修正日期 修正版別 修 改 內 容 1 2011.04.07 1.0 初次訂定 2 2013.05.08 2.0 修訂 3 2013.04.30 3.0 修訂 :Triple-Negative Breast Cancer 處方 新增 :Neoadjuvant-p7~8 4 2014.04.29 4.0 修訂 :FEC + Trastuzumab
新竹馬偕紀念醫院癌症中心 乳癌化學治療藥物處方 文件修訂記錄 修正次數 修正日期 修正版別 修 改 內 容 1 2011.04.07 1.0 初次訂定 2 2013.05.08 2.0 修訂 3 2013.04.30 3.0 修訂 :Triple-Negative Breast Cancer 處方 新增 :Neoadjuvant-p7~8 4 2014.04.29 4.0 修訂 :FEC + Trastuzumab
BIOLOGICAL THERAPIES FOR BREAST CANCER Updates from the 2005 San Antonio Breast Cancer Symposium
 Emerging trends and recommendations BIOLOGICAL THERAPIES FOR BREAST CANCER Updates from the 2005 San Antonio Breast Cancer Symposium Joseph Ragaz, MD, FRCPC Top-line summary Here, Oncology Exchange presents
Emerging trends and recommendations BIOLOGICAL THERAPIES FOR BREAST CANCER Updates from the 2005 San Antonio Breast Cancer Symposium Joseph Ragaz, MD, FRCPC Top-line summary Here, Oncology Exchange presents
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
SANDRA M. SWAIN. Washington Cancer Institute, Washington, District of Columbia, USA
 The Oncologist Early-Stage Breast Cancer: Clinical Update Chemotherapy: Updates and New Perspectives SANDRA M. SWAIN Washington Cancer Institute, Washington, District of Columbia, USA Key Words. Breast
The Oncologist Early-Stage Breast Cancer: Clinical Update Chemotherapy: Updates and New Perspectives SANDRA M. SWAIN Washington Cancer Institute, Washington, District of Columbia, USA Key Words. Breast
XII Michelangelo Foundation Seminar
 XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
Should pertuzumab be used as part of neoadjuvant treatment prior to the release of the APHINITY trial results?
 Commentary Should pertuzumab be used as part of neoadjuvant treatment prior to the release of the APHINITY trial results? Tom Wei-Wu Chen 1, Ching-Hung Lin 1,2, Chiun-Sheng Huang 3 1 Department of Oncology,
Commentary Should pertuzumab be used as part of neoadjuvant treatment prior to the release of the APHINITY trial results? Tom Wei-Wu Chen 1, Ching-Hung Lin 1,2, Chiun-Sheng Huang 3 1 Department of Oncology,
St Gallen 2017 controversies & consensus
 St Gallen 2017 controversies & consensus Shani Paluch-Shimon, MBBS, MSc Head, Breast Cancer Service for Young Women Breast Unit, Division of Oncology Sheba Medical Centre June 2017 St Gallen 2017 De-escalation
St Gallen 2017 controversies & consensus Shani Paluch-Shimon, MBBS, MSc Head, Breast Cancer Service for Young Women Breast Unit, Division of Oncology Sheba Medical Centre June 2017 St Gallen 2017 De-escalation
William J. Gradishar MD FACP FASCO
 Northwestern University Feinberg School of Medicine Highlights of Non-Endocrine Adjuvant Therapy SABCS 2018 William J. Gradishar MD FACP FASCO Betsy Bramsen Professor of Breast Oncology Chief- Hematology/Oncology
Northwestern University Feinberg School of Medicine Highlights of Non-Endocrine Adjuvant Therapy SABCS 2018 William J. Gradishar MD FACP FASCO Betsy Bramsen Professor of Breast Oncology Chief- Hematology/Oncology
London, 22 May 2006 Product Name: Herceptin Procedure no.: EMEA/H/C/278/II/0026 SCIENTIFIC DISCUSSION
 London, 22 May 2006 Product Name: Herceptin Procedure no.: EMEA/H/C/278/II/0026 SCIENTIFIC DISCUSSION 1 Introduction Trastuzumab is currently approved for the treatment of Her2 over-expressing metastatic
London, 22 May 2006 Product Name: Herceptin Procedure no.: EMEA/H/C/278/II/0026 SCIENTIFIC DISCUSSION 1 Introduction Trastuzumab is currently approved for the treatment of Her2 over-expressing metastatic
that the best available evidence has not demonstrated that pcr can predict long-term outcomes in the neoadjuvant setting.
 pcr in one arm of a randomized clinical trial comparing two neoadjuvant chemotherapies predicts for improved event-free or overall survival in that arm of the clinical trial. perc noted that the NeoALTTO
pcr in one arm of a randomized clinical trial comparing two neoadjuvant chemotherapies predicts for improved event-free or overall survival in that arm of the clinical trial. perc noted that the NeoALTTO
Breast Cancer: Chemotherapy and Novel Agents
 North Carolina Oncology Association & South Carolina Oncology Society Joint Membership Meeting ~ February 26 27, 2010 The Ballantyne Resort ~ Charlotte, NC Breast Cancer: Chemotherapy and Novel Agents
North Carolina Oncology Association & South Carolina Oncology Society Joint Membership Meeting ~ February 26 27, 2010 The Ballantyne Resort ~ Charlotte, NC Breast Cancer: Chemotherapy and Novel Agents
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
SANDRA M. SWAIN. Washington Cancer Institute, Washington, District of Columbia, USA
 The Oncologist Chemotherapy: Updates and New Perspectives SANDRA M. SWAIN Washington Cancer Institute, Washington, District of Columbia, USA Key Words. Breast cancer Chemotherapy Taxane Trastuzumab Ki-67
The Oncologist Chemotherapy: Updates and New Perspectives SANDRA M. SWAIN Washington Cancer Institute, Washington, District of Columbia, USA Key Words. Breast cancer Chemotherapy Taxane Trastuzumab Ki-67
Taxotere * and carboplatin plus Herceptin (trastuzumab) (TCH): the first approved non-anthracycline Herceptin-containing regimen 1
 (TCH): the first approved non-anthracycline Herceptin-containing regimen 1") Important data from BCIRG 006 Taxotere * and carboplatin plus Herceptin (trastuzumab) (TCH): the first approved non-anthracycline Herceptin-containing regimen 1 in the adjuvant treatment of HER2+ breast
Important data from BCIRG 006 Taxotere * and carboplatin plus Herceptin (trastuzumab) (TCH): the first approved non-anthracycline Herceptin-containing regimen 1 in the adjuvant treatment of HER2+ breast
Breast : ASCO Abstracts for Review
 Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Enfermedad con sobreexpresión de HER-2 neu
 Enfermedad con sobreexpresión de HER-2 neu Elsa Dalmau Parc Taulí Sabadell. Hospital Universitari. Enfermedad con sobreexpresión de HER-2 neu ÍNDICE Neoadyuvancia Adyuvancia Enfermedad avanzada Enfermedad
Enfermedad con sobreexpresión de HER-2 neu Elsa Dalmau Parc Taulí Sabadell. Hospital Universitari. Enfermedad con sobreexpresión de HER-2 neu ÍNDICE Neoadyuvancia Adyuvancia Enfermedad avanzada Enfermedad
(Neo-) Adjuvant chemotherapy and biological agents. Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology
 Adjuvant chemotherapy and biological agents. Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology") (Neo-) Adjuvant chemotherapy and biological agents Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Neoadjuvant treatment in triple negative and HER2 positive
(Neo-) Adjuvant chemotherapy and biological agents Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Neoadjuvant treatment in triple negative and HER2 positive
Stopping a cancer trial early: is it really for the benefit of patients? What about the quality of data?
 Stopping a cancer trial early: is it really for the benefit of patients? What about the quality of data? Pinuccia Valagussa Fondazione Michelangelo, Milano I have no relevant relationships to disclose
Stopping a cancer trial early: is it really for the benefit of patients? What about the quality of data? Pinuccia Valagussa Fondazione Michelangelo, Milano I have no relevant relationships to disclose
Triple Negative Breast Cancer: Part 2 A Medical Update
 Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Advanced HER2+ Breast Cancer: New Options and How to Deploy Them. José Baselga MD, PhD
 Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Rethinking neoadjuvant therapy: neoadjuvant therapy as a platform for drug development in HER2 positive breast cancer
 2016.04.29 GBCC luncheon symposium Rethinking neoadjuvant therapy: neoadjuvant therapy as a platform for drug development in HER2 positive breast cancer Seoul National University Bundang Hospital Seoul
2016.04.29 GBCC luncheon symposium Rethinking neoadjuvant therapy: neoadjuvant therapy as a platform for drug development in HER2 positive breast cancer Seoul National University Bundang Hospital Seoul
Post-ESMO 2012: Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich T.Rordorf, SAMO Luzern 1
 Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
The absolute benefit from chemotherapy for both older and younger patients appeared most significant in ER-negative populations.
 Hello, my name is Diane Hecht, and I am a Clinical Pharmacy Specialist at the University of Texas MD Anderson Cancer Center. It s my pleasure to talk to you today about the role of chemotherapy in this
Hello, my name is Diane Hecht, and I am a Clinical Pharmacy Specialist at the University of Texas MD Anderson Cancer Center. It s my pleasure to talk to you today about the role of chemotherapy in this
2
 1 2 Systematic review of published evidence PUBMED 1999-2017 ASCO 1999-2017 SABCS 1999-2017 ECCO/ESMO 1999-2017 3 Statement: Anthracycline/ taxane based chemotherapy 1. Budd GT et al. SWOG S0221: A Phase
1 2 Systematic review of published evidence PUBMED 1999-2017 ASCO 1999-2017 SABCS 1999-2017 ECCO/ESMO 1999-2017 3 Statement: Anthracycline/ taxane based chemotherapy 1. Budd GT et al. SWOG S0221: A Phase