Molecular Aspects of Colorectal Cancer for the Practicing Surgical Pathologist
|
|
|
- Tamsyn Tyler
- 6 years ago
- Views:
Transcription

1 Molecular Aspects of Colorectal Cancer for the Practicing Surgical Pathologist Murray Resnick MD PhD Vice Chief of Pathology, Director Anatomical Pathology Rhode Island and The Miriam Hospital Professor of Pathology Alpert School of Medicine, Brown University
2 KEY TOPICS Importance of Differentiating Microsatellite Stable from Instable Tumors Emphasizing IHC Methods Prognostic/Predictive Biomarkers in CRC Emphasizing MSI Next Generation Sequencing and Liquid Biopsy
3 Chromosomal Instability (CIN) Microsatellite Stable (MSS) Microsatellite Instability (MSI) Sporadic (85%) FAP (<1%) Sporadic (12-15%) Lynch Syndrome (3-4%) Acquired Germline Acquired Germline APC, p53 APC BRAF V600E MMR DCC, KRAS MLH1 methylation (MLH1, PMS2 Others MSH2, MSH6 EPCAM)
4 Why is MSI Colon Cancer Important? Identification of Lynch syndrome patients MSI status has prognostic significance and predictive significance for therapy MSI status is central to many of the molecular classification systems of CRC Pathologists often are first to identify MSI and are key in communicating forward
5 Lynch Syndrome (HNPCC) Most common hereditary CRC syndrome (3-4% of all CRC) Autosomal dominant Extracolonic (endometrium, ovary, renal pelvis, stomach, others) cancers common Colonic screening leads to decreased CRC and death!!! Screening of relatives critical Difficult to recognize clinically (family history not always obvious or available) Lynch CRCs arise from traditional adenomas
6 Sporadic MSI Tumors 10-15% of all colon cancer Phenotypically similar to LS tumors Right sided, older females Commonly arise from sessile serrated adenomas MLH1 deficient with wild type BRAF and MLH1 promotor hypermethylation arise from traditional adenomas (Farchoukh et al AJSP 2016)
7 Gross Morphological Aspects of MSI Tumors - Primarily right colon, bulky, less likely to have nodal or distal metastases Micro - Increased TILs, Crohn s like reaction - Poorly differentiated (High grade), medullary pattern - Signet ring and mucinous differentiation - Histologic heterogeneity (Jass et al Gut 1998, Greenson et al AJSP 2003)

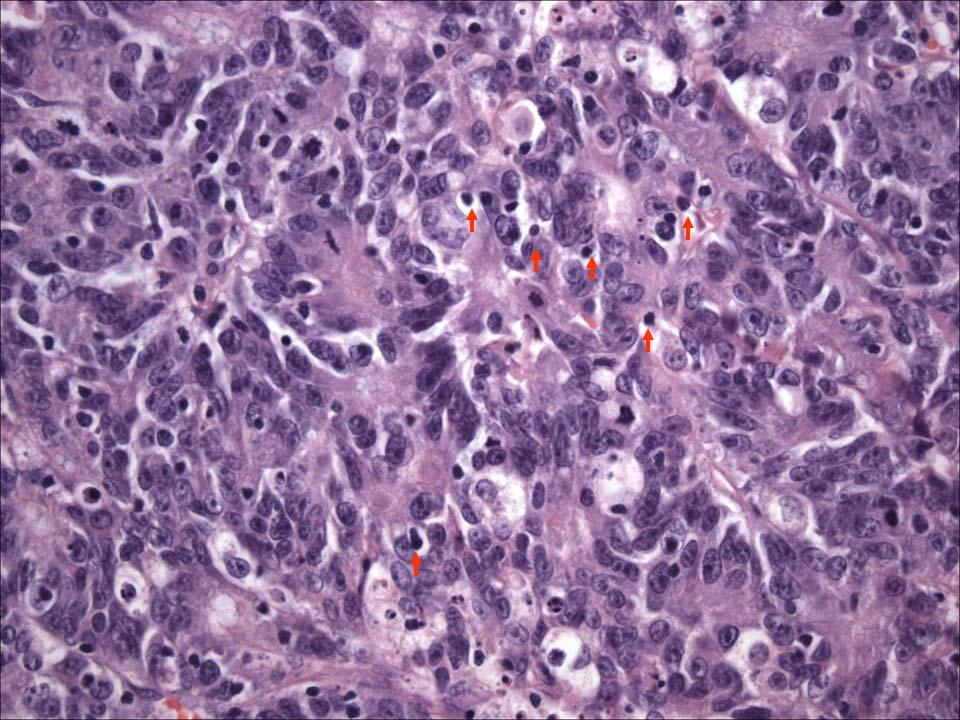



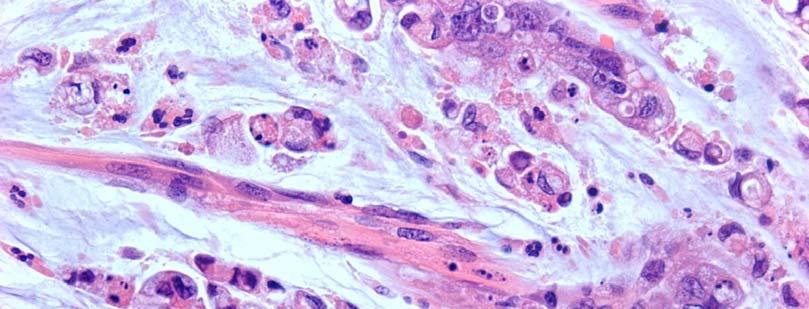

8 Show pics msi here

9 MSI Microsatellites are short nucleotide repeat sequences prone to replication errors by DNA polymerase Slippage causes insertion-deletion loops Mismatch repair (MMR) proteins correct this Errors result in varying lengths of these sequences If not corrected, second round of replication incorporates mutation frameshift mutations non functional protein

10 MSI is defined by the presence of new bands of tumor DNA not present in PCR components of normal DNA
 MSI-L (1 identified by PCR) MSS (0 identified by PCR) - dmmr - pmmr -")
11 Typically analyze 5 microsatellite markers: MSI-H (2 or more identified by PCR) MSI-L (1 identified by PCR) MSS (0 identified by PCR) - dmmr - pmmr - pmmr


12 MMR Proteins Two complexes MLH1/PMS2 and MSH2/MSH6 Stability of PMS2 and MSH6 depends upon these complexes Loss of MLH1 leads to loss of PMS2, loss of MSH2 leads to loss of MSH6 MLH1 and MSH2 are stable without complex (isolated loss of PMS2 or MSH6)
13 Universal MSI Testing of CRCs Universal testing all CRCs (Consensus Statement of US Multi-Society Task Force on CRC, EGAPP and other organizations) Universal testing all CRCs <70 and testing of >70 who meet Bethesda Guidelines slightly more cost effective option (35% fewer MMR tests than universal testing) (NCCN) Both are cost effective and have equal sensitivities for identifying LS Either MSI PCR or IHC MMR is valid
14 Principles of Lynch Syndrome/MSI Initial Screen Is tumor mismatch repair (MMR) deficient? Directly by IHC of MMR proteins Indirectly by measuring MSI status by PCR Directly/Indirectly using Next Generation Sequencing Is MMR deficiency indicative of LS or is this sporadic?
15 IHC vs MSI PCR Testing IHC Relatively cheap Rapid TAT Small amount of tumor and normal tissue Indirectly predicts MSI-H Results suggest MMR gene May be difficult to interpret MSI-PCR More expensive 2-5 days Need at least 40% tumor tissue Separates MSS, MSI-H, MSI-L



16 IHC Testing of MMR Proteins MLH-1 PMS-2










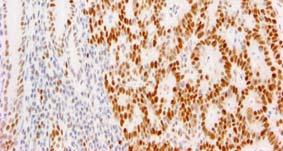















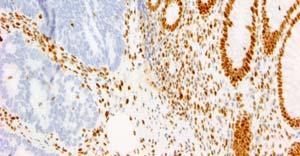










17 MLH1 PMS2 MSH2 MSH6
18 IHC Pattern Rate of results Clinical All proteins intact 80 85% most likely not LS MLH1 /PMS2 10% Sporadic (BRAF mutation/mlh1 promotor methylation) (80%) likely germline LS MLH1 (20%) MSH2 /MSH6 3% likely germline LS MSH2 MSH6 1% likely germline LS MSH6 PMS2 1% likely germline LS PMS2
19 MLH1 and PMS2 Absent (10% of CRC) Sporadic (80%) Lynch (20%) MLH1 hypermethylation (80%) BRAF mutation (70 %) MLH1 germline mutation

20 BRAF Mutations Threonine Kinase involved in the ras/raf/mek/erk pathway
21 BRAF Mutations Mutated in 15% of all CRC and 70% of MSI tumors with MLH1 loss Virtually exclusive for Lynch (rare reports in LS) Exon 15, point mutation in V600E (primarily) Has prognostic (poor) and possibly therapeutic significance BRAF mutations are uncommon in extracolonic tumors (endometrium)
 Others go directly to MLH1 promotor methylation")

22 MLH1 Promotor Methylation Perform for BRAF negative MLH1/PMS2 deficient tumors (30%) Others go directly to MLH1 promotor methylation (may be more cost effective but less readily available) If BRAF is not mutated and MLH1 promotor is not methylated refer to mutational analysis of MLH1
23 Isolated PMS2 Loss (5% of LS) PMS2 germline mutation or rarely Refer to PMS2 (and MLH1) mutational analysis MLH1 missense mutation resulting in non-functional, antigenically reactive protein
24 MSH2 and MSH6 Absent (35% of LS) Likely Lynch due to germline mutation of MSH2 Refer to MSH2 mutational analysis If genetic testing for MSH2 is normal refer to EPCAM (2% of LS)

25 MSH2 Loss Due to EPCAM Gene Mutations EPCAM gene is upstream from MSH2, mutation leads to MSH2 inactivation via CpG island methylation 25% of cases where MSH2 negative by IHC but germline MSH2 mutations not found (2-3% overall LS)
26 Isolated MSH6 loss (<5% of LS) Isolated MSH6 loss - likely MSH6 mutation rarely MSH2 mutation Refer to MSH6 mutational analysis Patients with MSH6 mutations may lack evidence of MSI by PCR or loss of MSH6 by IHC Patients with MSH6 loss by IHC may lack evidence of MSH6 mutations by genetic testing
27 Correlation Between MMR Loss and Germline Mutation Identification MLH1/PMS2-33% MLH1 mutation PMS2-56% PMS2 mutation MSH2/MSH6-66% MSH2 mutation MSH6-24% MSH6 mutation (Hampel et al J Clin Onc 2008) Reasons for MMR Deficient Germline Testing Negative 1. Two somatic MMR mutations 66% 2. LOH one allele, somatic mutation other 9% 3. False positive initial screen 20% (Haroldsdotter et al Gastroenterology 2014)
28 Rare and Unusual Molecular Scenarios MLH1 loss due to constitutional MLH1 hypermethylation of one allele in germline (MLH1 hypermethylation will be detectable in adjacent normal tissue) 0.6% of LS (Niessen et al Genes Chrom Cancer 2009) MSH2 rearrangement (inversion) not detectable by commonly used panels (Rhees et al Fam Cancer 2014) Biallelic somatic mutations in MMR genes (MLH1, MSH2) (Sourrouille et al Fam Cancer 2013, Mesenkamp et al Gastro 2014) Constituitonal MMR deficiency, biallelic germline mutation in one of four genes, very rare, high risk malignancies in childhood, CNS and colorectal, IHC negative in tumor and normal tissue (Wimmer et al J Med Gen 2014) Numerous others..
29 Practical Issues Related to MMR IHC Staining
30 IHC Staining Heterogeneity (Focal Weak Staining) Compare intensity to internal control (germinal center or basal normal epithelium) - Stain is adequate only if internal control positive If weaker (most common for MLH1) look at partner protein If PMS2 loss may suggest MLH1 mutation If PMS2, MSH2 or MSH6 weak likely related to somatic downregulation Focal/weak staining may be do to regional hypoxia, poor tissue fixation or older tissue blocks MOST consider 10% positivity as a cutoff



31




32 Aberrant Staining Patterns Cytoplasmic staining, dot-like nuclear or nucleolar staining (MLH1), perinuclear staining likely all technical and are regarded as negative Pai et al, AJSP 2016
33 Should We Be Performing IHC For MMR On Biopsy Or Resection Material? Biopsy preferable - If Lynch patient may undergo total colectomy, prophylactic hysterectomy/oopherectomy. - If rectal tumor preop chemoradiotherapy may completely ablate tumor.
34 Should We Stain Adenomas? Two large studies addressing testing of adenomas in Lynch patients (Pino et al JMD 2009, Walsh et al Mod Path 2012) Association between HG dysplasia, distal location, villous architecture and loss of staining, adenoma size over 10mm almost significant Not recommended as a screening tool for general population or for population fulfilling Revised Bethesda Guidelines!!!! In known LS families if tumor is not available and only large adenoma is, testing is appropriate, However Beware of False Negatives! (MSI late event)
35 MSI test MSS, MSI-L MSI-H No Further Testing BRAF mutated or promotor methylated CRC biopsy No loss of MMR proteins BRAF and/or promotor methylation test IHC test Loss of MLH1/PMS2 Loss of other MMR No BRAF mutation or promotor methylation Refer to Genetic Counseling, Consider Germline Testing
36 Pathologist s Role in MSI Testing Follow-Up Issue report explaining results and contact clinician to discuss whenever LS is a possibility, timeliness important Clinician needs to refer patient to geneticist We cannot reflexively order genetic testing, patient needs to consent Convincing patient to undergo genetic counseling is the largest barrier!! If clinical suspicion of LS is high consider ordering germline testing regardless of IHC and MSI testing results!!
37 Molecular Prognostic and Predictive Markers for CRC: State of the Art 2017 and Future Visions
 colon cancers (mostly prognosis) Stage IV (III) tumors (mostly")
38 Molecular Prognostic and Predictive Markers Which tumors needs to be tested? Stage II (III) colon cancers (mostly prognosis) Stage IV (III) tumors (mostly predictive)
39 CRC Prognostic/Predictive Biomarkers Multitude of studies based on: - Protein expression by IHC - Molecular mutational profile, MSI - Expression array mrna, mirna profile - Serum proteomic and DNA markers - Others
40 ASCP/CAP/AMP/ASCO Biomarker Guidelines 2017 Strongly recommends MSI testing of all stage II and above, screen for LS and prognosis, (and predictive) Strongly recommends BRAF (V600E) testing for stage II and above for prognostic stratification (BRAF status in the decision tree for EGFR targeted therapy is optional and still controversial) Strongly recommends KRAS and NRAS genotyping in all patients with metastatic CRC being considered for EGFR targeted therapy
41 MSI as a Prognostic Marker MSI Stage II have a more favorable outcome (Ribic et al NEJM 2003, Sargent et al JCO 2010) MSI Stage III slightly more favorable (Roth et al JNCI 2012, Sinicrope et al JCO 2013) BRAF Mutation attenuates MSI survival benefit WHO recommends poorly differentiated MSI-H tumors Should Not be graded as high grade!! - May not be valid for signet ring carcinomas (Kakar et al Mod Path 2005 Hartman et al AJSP 2013)

42 BRAF Mutation as a Prognostic Marker BRAF mutation is a poor prognostic factor for stage III and IV MSI and MSS tumors. (reviewed by Sinicrope FA et al Clin Gastroenterol Hepatol 2016)
43 MSI as a Predictive Marker Predicts poor response to 5FU therapy (Sargent et al JCO 2010) Addition of oxaliplatin (FOLFOX) negates adverse effects of MSI (Andre et al JCO 2015) Immune Checkpoint Therapy



44 The Immune Landscape of MSI Tumors Tumor Infiltrating Lymphocytes (TILs) CD3 Alexander J. Histopathological Identification of Colon Cancer with Microsatellite Instability. Am J. Pathol. 2001, 158:


45 T-cells are predominantly cytotoxic and activated in MSI Tumors Phillips, S. M. et al (2004), Tumour-infiltrating lymphocytes in colorectal cancer with microsatellite instability are activated and cytotoxic. Br J Surg, 91:


46 What attracts tumor infiltrating lymphocytes? Immunogenic neopeptides generated by abundant mutations Shia et al Modern Pathology, 2016
47 Why are MSI tumors (which are strongly immunogenic) not rejected by the host?


48 Checkpoint inhibitors CTLA4-CD80 - Ipilimumab MELANOMA 2011 Nature Reviews Cancer 12,


49 Immune Checkpoint Proteins PD1-PDL-1 Sitn.hms.harvard.edu

50
51 PD-1 Blockade in Tumors with Mismatch-Repair Deficiency Dung T. Le, M.D., Jennifer N. Uram, Ph.D., Hao Wang, Ph.D., Bjarne R. Bartlett, B.S., Holly Kemberling, R.N., Aleksandra D. Eyring, M.Pharm., Andrew D. Skora, Ph.D., Brandon S. Luber, Sc.M., Nilofer S. Azad, M.D., Dan Laheru, M.D., Barbara Biedrzycki, Ph.D., C.N.R.P., Ross C. Donehower, M.D., Atif Zaheer, M.D., George A. Fisher, M.D., Ph.D., Todd S. Crocenzi, M.D., James J. Lee, M.D., Ph.D., Steven M. Duffy, M.D., Richard M. Goldberg, M.D., Albert de la Chapelle, M.D., Ph.D., Minori Koshiji, M.D., Ph.D., Feriyl Bhaijee, M.D., Thomas Huebner, M.D., Ralph H. Hruban, M.D., Laura D. Wood, M.D., Ph.D., Nathan Cuka, M.D., Drew M. Pardoll, M.D., Ph.D., Nickolas Papadopoulos, Ph.D., Kenneth W. Kinzler, Ph.D., Shibin Zhou, M.D., Ph.D., Toby C. Cornish, M.D., Ph.D., Janis M. Taube, M.D., Robert A. Anders, M.D., Ph.D., James R. Eshleman, M.D., Ph.D., Bert Vogelstein, M.D., and Luis A. Diaz, Jr., M.D. N Engl J Med 372: June 25, 2015

52 Clinical Responses to Pembrolizumab Treatment. Le DT et al. N Engl J Med 2015;372:


53

54 Predictive Markers: EGFR Signaling Pathway Siddiqui & Piperdi Ann Surg Onc 2010 EGFR pathway overexpressed in over 80% of CRC EGF and other ligands activates KRAS and other signaling pathways leading to cellular proliferation, angiogenesis, migration and survival





55 RAS activating mutations predict poor response to anti-egfr therapy
56 ASCP/CAP/AMP/ASCO Biomarker Guidelines 2017 Strongly recommends MSI testing of all stage II and above, screen for LS and prognosis, (and predictive) Strongly recommends BRAF (V600E) testing for stage II and above for prognostic stratification (BRAF status in the decision tree for EGFR targeted therapy is optional and still controversial) Strongly recommends KRAS and NRAS genotyping in all patients with metastatic CRC being considered for EGFR targeted therapy

57 Pohl et al Dig Dis 2016
58 Future of Mutational Testing for Colorectal Cancer Mutations other than RAS, BRAF effect EGFR pathway and response to EGFR targeted therapy Novel therapies target these mutations CRC is driven by mutations in other pathways as well, some of which are being targeted Need for larger panels of mutation analysis (NGS) CRC with wild type KRAS develop novel mutations rendering anti-egfr ineffective over time following targeted therapy Need for continuous monitoring (LIQUID BIOPSY)

59 Role for Next Generation Sequencing in Colon Cancer Workup Colon Cancer Mutations By Frequency Cosmic Database 2016

60 Next Generation Sequencing (R Steven et al Biotechniques 2014) Rapid, sensitive and relatively inexpensive analysis: Multigene Mutation Panels Whole Exome, Whole Genome Transcriptome
61 NGS and the Future of Molecular Testing for CRC NGS is more sensitive and as prices continue to drop will become more cost-effective than existing mutational screening strategies for all stage II and greater CRC Mutation panels will cover all actionable mutations for targeted therapies Mutational analysis of LS (other polyposis and genetic syndromes) will be incorporated into NGS panels MSI status will be determined by NGS bioinformatic analysis


62 Detection of Circulating Tumor DNA in CRC Liquid Biopsies McDonald et al Sci Trans Med 2015
 as liquid biopsies for precision medicine")
 Circulating tumour cells and cell-free DNA in")
63 Key applications of circulating tumour cells (CTCs) and circulating tumour DNA (ctdna) as liquid biopsies for precision medicine Pantel, K. & Alix-Panabières, C. (2017) Circulating tumour cells and cell-free DNA in gastrointestinal cancer Nat. Rev. Gastroenterol. Hepatol.


64 Liquid Biopsy Market Projected at >10 Billion Dollars by 2020!!!
65 Circulating Tumor DNA in CRC Patients DNA levels in plasma are higher in CRC patients, decrease after therapy and increase again at tumor recurrence (Frattini et al 2005) Genotyping Cancer Alleles in ctdna KRAS mutant fragments are detected in the blood of patients with KRAS mutant tumors with high specificity and sensitivity (Bettegowda et al 2014) Tumor specific KRAS mutations in plasma have prognostic value (Spindler et al 2015) Monitoring Drug Resistance and Clonal Evolution RAS pathway mutations associated to acquired resistance to EGFR specific antibodies detected before disease progression is detected (Diaz et al, Misale et al 2012) ctdna used to track clonal evolution and targeted drug responses in CRC patients (Siravegna et al 2015) WGS of plasma of CRC patients treated with anti-egfr therapy reveals loss of APC chromosomal 5q22 region and amplifications in known genes involved with resistance of EGFR blockade such as MET, ERBB2 and KRAS (Mohan et al 2014)
66 Standard Biopsy Liquid Biopsy Time intensive Invasive Localized sampling of tissue Difficult to obtain in certain locations One point in time Quick and easily obtained Allows for continuous monitoring Better at detecting tumor heterogeneity?
67 Summary MSI status is an important prognostic and predictive marker and is central to many classification schemes of CRC With universal MSI testing we are responsible for guiding clinicians for further genetic work-up whenever LS is a consideration Current guidelines recommend testing for mutations in BRAF and genes governing the EGF-R pathway, however, the list of mutations to be tested will undoubtedly increase NGS will likely replace existing technologies for mutational analysis, MSI work-up and hereditary CRC work-up Liquid biopsies detecting ctdna will allow for real time monitoring of CRC mutational profiles


68 Thank You
69 Consensus Molecular Subtypes of CRC Guinney et al, Nature Medicine Evaluated the results of 6 CRC subtyping algorithms each developed independently using different gene expression data sets and analytical approaches -Total of 4151 patients including The Cancer Genome Atlas -Data included: -Clinical information and prognosis -Mutations and copy number analysis -Gene expression including mirna -Epigenetics -Proteomics
70 Proposed Taxonomy of CRC 2015 Tumor Subtype CMS1 MSI Immune CMS2 Canonical CMS3 Metabolic CMS4 Mesenchymal Proportion Precursor Genetic features Genetic drivers 14% 37% 13% 23% Serrated Tubular Unknown Serrated MSI, CIMP high hypermutation SCNA high Mixed MSI SCNA low, CIMP low SCNA high BRAF mutations APC KRAS mutation Unknown Gene expression signature Immune infiltration and activation WNT and MYC activation Metabolic deregulation Mesenchymal TGF-b activation angiogenesis Prognosis Good survival but poor after relapse Superior survival rate after relapse Intermediate Survival Worse relapse-free and overall survival
Development of Carcinoma Pathways
 The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Colorectal Carcinoma Reporting in 2009
 Colorectal Carcinoma Reporting in 2009 Overview Colorectal carcinoma- new and confusing AJCC TNM issues Wendy L. Frankel, M.D. Vice-Chair and Director of AP Department of Pathology The Ohio State University
Colorectal Carcinoma Reporting in 2009 Overview Colorectal carcinoma- new and confusing AJCC TNM issues Wendy L. Frankel, M.D. Vice-Chair and Director of AP Department of Pathology The Ohio State University
Molecular subtyping: how useful is it?
 Molecular subtyping: how useful is it? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics at the NCT-Partner Site Dresden CMTD Disclosure
Molecular subtyping: how useful is it? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics at the NCT-Partner Site Dresden CMTD Disclosure
Colon Cancer and Hereditary Cancer Syndromes
 Colon Cancer and Hereditary Cancer Syndromes Gisela Keller Institute of Pathology Technische Universität München gisela.keller@lrz.tum.de Colon Cancer and Hereditary Cancer Syndromes epidemiology models
Colon Cancer and Hereditary Cancer Syndromes Gisela Keller Institute of Pathology Technische Universität München gisela.keller@lrz.tum.de Colon Cancer and Hereditary Cancer Syndromes epidemiology models
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Microsatellite instability and other molecular markers: how useful are they?
 Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
A Review from the Genetic Counselor s Perspective
 : A Review from the Genetic Counselor s Perspective Erin Sutcliffe, MS, CGC Certified Genetic Counselor Cancer Risk Evaluation Program INTRODUCTION Errors in base pair matching that occur during DNA replication,
: A Review from the Genetic Counselor s Perspective Erin Sutcliffe, MS, CGC Certified Genetic Counselor Cancer Risk Evaluation Program INTRODUCTION Errors in base pair matching that occur during DNA replication,
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By. Magnitude of the Problem. Magnitude of the Problem. Cardinal Features of Lynch Syndrome
 GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual
Colon cancer: practical molecular diagnostics. Wade S. Samowitz, M.D. University of Utah and ARUP
 Colon cancer: practical molecular diagnostics Wade S. Samowitz, M.D. University of Utah and ARUP Disclosure Dr. Samowitz may receive royalties in the future related to the Ventana BRAF V600E antibody.
Colon cancer: practical molecular diagnostics Wade S. Samowitz, M.D. University of Utah and ARUP Disclosure Dr. Samowitz may receive royalties in the future related to the Ventana BRAF V600E antibody.
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Pr
 Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
Colorectal cancer Chapelle, J Clin Oncol, 2010
 Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Molecular Biomarkers in the Characterization & Treatment of Colorectal Carcinoma
 Molecular Biomarkers in the Characterization & Treatment of Colorectal Carcinoma Andrew C. Nelson, M.D., Ph.D. Divisions of Anatomic & Molecular Pathology Department of Laboratory Medicine & Pathology
Molecular Biomarkers in the Characterization & Treatment of Colorectal Carcinoma Andrew C. Nelson, M.D., Ph.D. Divisions of Anatomic & Molecular Pathology Department of Laboratory Medicine & Pathology
The Whys OAP Annual Meeting CCO Symposium September 20. Immunohistochemical Assessment Dr. Terence Colgan Mount Sinai Hospital, Toronto
 Immunohistochemical Assessment of Mismatch Repair Proteins in Endometrial Cancer: The Whys and How Terence J. Colgan, MD Head of Gynaecological Pathology, Mount Sinai Hospital, University of Toronto, Toronto.
Immunohistochemical Assessment of Mismatch Repair Proteins in Endometrial Cancer: The Whys and How Terence J. Colgan, MD Head of Gynaecological Pathology, Mount Sinai Hospital, University of Toronto, Toronto.
Molecular biology of colorectal cancer
 Molecular biology of colorectal cancer Phil Quirke Yorkshire Cancer Research Centenary Professor of Pathology University of Leeds, UK Rapid pace of molecular change Sequencing changes 2012 1,000 genomes
Molecular biology of colorectal cancer Phil Quirke Yorkshire Cancer Research Centenary Professor of Pathology University of Leeds, UK Rapid pace of molecular change Sequencing changes 2012 1,000 genomes
La genetica del carcinoma colo-rettale
 La genetica del carcinoma colo-rettale Ivana Cataldo Ospedale Ca Foncello, Treviso ARC-NET Centro di Ricerca Applicata sul Cancro AOUI, Verona OUTLINE What s new in colorectal cancer? Pathological Markers
La genetica del carcinoma colo-rettale Ivana Cataldo Ospedale Ca Foncello, Treviso ARC-NET Centro di Ricerca Applicata sul Cancro AOUI, Verona OUTLINE What s new in colorectal cancer? Pathological Markers
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO. CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS?
 INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
INMUNOTERAPIA EN CANCER COLORRECTAL METASTASICO CCRm MSI-H NUEVO ESTANDAR EN PRIMERA LINEA Y/O PRETRATADOS? V. Alonso Servicio de Oncologia Medica H. U. Miguel Servet Zaragoza MSI-H mcrc Clinical and Pathological
Universal Screening for Lynch Syndrome
 Universal Screening for Lynch Syndrome St. Vincent/Ameripath protocol proposal Lynch syndrome (HNPCC) 1/35 individuals with colorectal cancer has Lynch syndrome Over half individuals are >50 at time of
Universal Screening for Lynch Syndrome St. Vincent/Ameripath protocol proposal Lynch syndrome (HNPCC) 1/35 individuals with colorectal cancer has Lynch syndrome Over half individuals are >50 at time of
Anatomic Molecular Pathology: An Emerging Field
 Anatomic Molecular Pathology: An Emerging Field Antonia R. Sepulveda M.D., Ph.D. University of Pennsylvania asepu@mail.med.upenn.edu 2008 ASIP Annual Meeting Anatomic pathology (U.S.) is a medical specialty
Anatomic Molecular Pathology: An Emerging Field Antonia R. Sepulveda M.D., Ph.D. University of Pennsylvania asepu@mail.med.upenn.edu 2008 ASIP Annual Meeting Anatomic pathology (U.S.) is a medical specialty
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer
 status in Colorectal Cancer") Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Colorectal Cancer in 2017: From Biology to the Clinics. Rodrigo Dienstmann
 Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
Management of higher risk of colorectal cancer. Huw Thomas
 Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
Precision Genetic Testing in Cancer Treatment and Prognosis
 Precision Genetic Testing in Cancer Treatment and Prognosis Deborah Cragun, PhD, MS, CGC Genetic Counseling Graduate Program Director University of South Florida Case #1 Diana is a 47 year old cancer patient
Precision Genetic Testing in Cancer Treatment and Prognosis Deborah Cragun, PhD, MS, CGC Genetic Counseling Graduate Program Director University of South Florida Case #1 Diana is a 47 year old cancer patient
What Pathology can tell us in the approach of localized colorectal cancer
 What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
Molecular Diagnosis for Colorectal Cancer Patients
 Molecular Diagnosis for Colorectal Cancer Patients Antonia R. Sepulveda MD, PhD, FCAP October, 20, 2010 www.cap.org Welcome to the PHC Webinar Series This talk on The Molecular Diagnosis for Colorectal
Molecular Diagnosis for Colorectal Cancer Patients Antonia R. Sepulveda MD, PhD, FCAP October, 20, 2010 www.cap.org Welcome to the PHC Webinar Series This talk on The Molecular Diagnosis for Colorectal
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Hereditary Non Polyposis Colorectal Cancer(HNPCC) From clinic to genetics
 From clinic to genetics") From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
Molecular Testing Updates. Karen Rasmussen, PhD, FACMG Clinical Molecular Genetics Spectrum Medical Group, Pathology Division Portland, Maine
 Molecular Testing Updates Karen Rasmussen, PhD, FACMG Clinical Molecular Genetics Spectrum Medical Group, Pathology Division Portland, Maine Keeping Up with Predictive Molecular Testing in Oncology: Technical
Molecular Testing Updates Karen Rasmussen, PhD, FACMG Clinical Molecular Genetics Spectrum Medical Group, Pathology Division Portland, Maine Keeping Up with Predictive Molecular Testing in Oncology: Technical
High risk stage II colon cancer
 High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Lynch Syndrome. Angie Strang, PGY2
 Lynch Syndrome Angie Strang, PGY2 Background Previously hereditary nonpolyposis colorectal cancer Autosomal dominant inherited cancer susceptibility syndrome Caused by defects in the mismatch repair system
Lynch Syndrome Angie Strang, PGY2 Background Previously hereditary nonpolyposis colorectal cancer Autosomal dominant inherited cancer susceptibility syndrome Caused by defects in the mismatch repair system
Genetic testing all you need to know
 Genetic testing all you need to know Sue Clark Consultant Colorectal Surgeon, St Mark s Hospital, London, UK. Colorectal cancer Familial 33% Polyposis syndromes
Genetic testing all you need to know Sue Clark Consultant Colorectal Surgeon, St Mark s Hospital, London, UK. Colorectal cancer Familial 33% Polyposis syndromes
Introduction. Why Do MSI/MMR Analysis?
 Clinical Significance Of MSI, KRAS, & EGFR Pathway In Colorectal Carcinoma UCSF & Stanford Current Issues In Anatomic Pathology Introduction Microsatellite instability and mismatch repair protein deficiency
Clinical Significance Of MSI, KRAS, & EGFR Pathway In Colorectal Carcinoma UCSF & Stanford Current Issues In Anatomic Pathology Introduction Microsatellite instability and mismatch repair protein deficiency
LYNCH SYNDROME: IN YOUR FACE BUT LOST IN SPACE (MOUNTAIN)!
!") LYNCH SYNDROME: IN YOUR FACE BUT LOST IN SPACE (MOUNTAIN)! Kathryn Singh, MPH, MS, LCGC Associate Clinical Professor Assistant Director, Graduate Program in Genetic Counseling Division of Genetic and Genomic
LYNCH SYNDROME: IN YOUR FACE BUT LOST IN SPACE (MOUNTAIN)! Kathryn Singh, MPH, MS, LCGC Associate Clinical Professor Assistant Director, Graduate Program in Genetic Counseling Division of Genetic and Genomic
Content. Diagnostic approach and clinical management of Lynch Syndrome: guidelines. Terminology. Identification of Lynch Syndrome
 of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
MSI and other molecular markers: how useful are they? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany
 MSI and other molecular markers: how useful are they? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory boards for AMGEN, ROCHE I Speaker
MSI and other molecular markers: how useful are they? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory boards for AMGEN, ROCHE I Speaker
Marcatori biomolecolari dei carcinomi del colon-retto sporadici ed ereditari
 Marcatori biomolecolari dei carcinomi del colon-retto sporadici ed ereditari Milo Frattini XII Congresso AIFEG Villa Cagnola - Gazzada Schianno (VA) 16/17.10.2014 APC β-catenina APC Met (p16) Models of
Marcatori biomolecolari dei carcinomi del colon-retto sporadici ed ereditari Milo Frattini XII Congresso AIFEG Villa Cagnola - Gazzada Schianno (VA) 16/17.10.2014 APC β-catenina APC Met (p16) Models of
TumorNext-Lynch. genetic testing for hereditary colorectal or uterine cancer
 TumorNet-Lynch genetic testing for hereditary colorectal or uterine cancer What Are the Causes of Hereditary Colorectal Cancer? sporadic 70% familial 20% hereditary 10% Lynch syndrome, up to 4% Familial
TumorNet-Lynch genetic testing for hereditary colorectal or uterine cancer What Are the Causes of Hereditary Colorectal Cancer? sporadic 70% familial 20% hereditary 10% Lynch syndrome, up to 4% Familial
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors)
") Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors) Kael Mikesell, DO McKay-Dee Hospital May 14, 2015 Outline Update to DNA Testing
Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors) Kael Mikesell, DO McKay-Dee Hospital May 14, 2015 Outline Update to DNA Testing
M. Azzam Kayasseh,Dubai,UAE
 Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
Microsatellite instability and other molecular markers: how usefulare they? Pr Frédéric Bibeau, MD, PhD Pathology Department CHU de Caen France
 Microsatellite instability and other molecular markers: how usefulare they? Pr Frédéric Bibeau, MD, PhD Pathology Department CHU de Caen France Content - Colorectal cancer context - CRC molecular classification
Microsatellite instability and other molecular markers: how usefulare they? Pr Frédéric Bibeau, MD, PhD Pathology Department CHU de Caen France Content - Colorectal cancer context - CRC molecular classification
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
DIAGNOSTICS ASSESSMENT PROGRAMME Diagnostics consultation document
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE DIAGNOSTICS ASSESSMENT PROGRAMME Diagnostics consultation document Molecular testing strategies for Lynch syndrome in The National Institute for Health
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE DIAGNOSTICS ASSESSMENT PROGRAMME Diagnostics consultation document Molecular testing strategies for Lynch syndrome in The National Institute for Health
Lynch Syndrome Screening for Endometrial Cancer: Basic Concepts 1/16/2017
 1 Hi, my name is Sarah Kerr. I m a pathologist at Mayo Clinic, where I participate in our high volume Lynch syndrome tumor testing practice. Today I hope to cover some of the basics needed to understand
1 Hi, my name is Sarah Kerr. I m a pathologist at Mayo Clinic, where I participate in our high volume Lynch syndrome tumor testing practice. Today I hope to cover some of the basics needed to understand
Colorectal Cancer - Working in Partnership. David Baty Genetics, Ninewells Hospital
 Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
Policy Specific Section: Medical Necessity and Investigational / Experimental. October 14, 1998 March 28, 2014
 Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
Measure Description. Denominator Statement
 CMS ID/CMS QCDR ID: CAP 18 Title: Mismatch Repair (MMR) or Microsatellite Instability (MSI) Biomarker Testing to Inform Clinical Management and Treatment Decisions in Patients with Primary or Metastatic
CMS ID/CMS QCDR ID: CAP 18 Title: Mismatch Repair (MMR) or Microsatellite Instability (MSI) Biomarker Testing to Inform Clinical Management and Treatment Decisions in Patients with Primary or Metastatic
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
ADVANCES IN COLON CANCER
 ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
ADVANCES IN COLON CANCER Peter T. Silberstein, M.D., FACP Professor, Creighton University Chief Hematology/Oncology UNIVERSAL SCREENING FOR LYNCH SYNDROME OF ALL PATIENTS WITH COLON CANCER ADOPTED BY CHI
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
National Surgical Adjuvant Breast and Bowel Project (NSABP) Foundation Annual Progress Report: 2009 Formula Grant
 Foundation Annual Progress Report: 2009 Formula Grant") National Surgical Adjuvant Breast and Bowel Project (NSABP) Foundation Annual Progress Report: 2009 Formula Grant Reporting Period July 1, 2012 June 30, 2013 Formula Grant Overview The National Surgical
National Surgical Adjuvant Breast and Bowel Project (NSABP) Foundation Annual Progress Report: 2009 Formula Grant Reporting Period July 1, 2012 June 30, 2013 Formula Grant Overview The National Surgical
The molecular genetics of colorectal cancer
 1 Department of Gastroenterology, North Middlesex University Hospital, London, UK 2 Institute of Molecular Genetics, Cardiff University 3 Department of Gastroenterology, Queen s Hospital Romford, London,
1 Department of Gastroenterology, North Middlesex University Hospital, London, UK 2 Institute of Molecular Genetics, Cardiff University 3 Department of Gastroenterology, Queen s Hospital Romford, London,
Molecular Subtyping of Endometrial Cancer: A ProMisE ing Change
 Molecular Subtyping of Endometrial Cancer: A ProMisE ing Change Charles Matthew Quick, M.D. Associate Professor of Pathology Director of Gynecologic Pathology University of Arkansas for Medical Sciences
Molecular Subtyping of Endometrial Cancer: A ProMisE ing Change Charles Matthew Quick, M.D. Associate Professor of Pathology Director of Gynecologic Pathology University of Arkansas for Medical Sciences
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
BRAF Testing In The Elderly: Same As in Younger Patients?
 EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
Histo-prognostic factors what histopathology has to offer for clinical decision making
 Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
Molecular markers in colorectal cancer. Wolfram Jochum
 Molecular markers in colorectal cancer Wolfram Jochum Biomarkers in cancer Patient characteristics Tumor tissue Normal cells Serum Body fluids Predisposition Diagnostic marker Specific diagnosis Prognostic
Molecular markers in colorectal cancer Wolfram Jochum Biomarkers in cancer Patient characteristics Tumor tissue Normal cells Serum Body fluids Predisposition Diagnostic marker Specific diagnosis Prognostic
Case Study. Overview. Deleterious MLH1 mutation detected on sequencing 10/16/2014
 The Role of Next Generation Sequencing for Hereditary Cancer Syndromes: A Focus on Endometrial Cancer Laura J. Tafe, MD Assistant Professor of Pathology Assistant Director, Molecular Pathology Dartmouth-Hitchcock
The Role of Next Generation Sequencing for Hereditary Cancer Syndromes: A Focus on Endometrial Cancer Laura J. Tafe, MD Assistant Professor of Pathology Assistant Director, Molecular Pathology Dartmouth-Hitchcock
Diagnostics guidance Published: 22 February 2017 nice.org.uk/guidance/dg27
 Molecular testing strategies for Lynch syndrome in people with colorectal cancer Diagnostics guidance Published: 22 February 2017 nice.org.uk/guidance/dg27 NICE 2018. All rights reserved. Subject to Notice
Molecular testing strategies for Lynch syndrome in people with colorectal cancer Diagnostics guidance Published: 22 February 2017 nice.org.uk/guidance/dg27 NICE 2018. All rights reserved. Subject to Notice
NGS in tissue and liquid biopsy
 NGS in tissue and liquid biopsy Ana Vivancos, PhD Referencias So, why NGS in the clinics? 2000 Sanger Sequencing (1977-) 2016 NGS (2006-) ABIPrism (Applied Biosystems) Up to 2304 per day (96 sequences
NGS in tissue and liquid biopsy Ana Vivancos, PhD Referencias So, why NGS in the clinics? 2000 Sanger Sequencing (1977-) 2016 NGS (2006-) ABIPrism (Applied Biosystems) Up to 2304 per day (96 sequences
VENTANA MMR IHC Panel Interpretation Guide for Staining of Colorectal Tissue
 VENTANA MMR IHC Panel Interpretation Guide for Staining of Colorectal Tissue VENTANA anti-mlh1 (M1) Mouse Monoclonal Primary Antibody VENTANA anti-pms2 (A16-4) Mouse Monoclonal Primary Antibody VENTANA
VENTANA MMR IHC Panel Interpretation Guide for Staining of Colorectal Tissue VENTANA anti-mlh1 (M1) Mouse Monoclonal Primary Antibody VENTANA anti-pms2 (A16-4) Mouse Monoclonal Primary Antibody VENTANA
2018 National Academy of Medicine Annual Meeting
 2018 National Academy of Medicine Annual Meeting October 15, 2018 Targeting Cancer with Precision Prevention Ernest Hawk, M.D., M.P.H. What is Precision Prevention? The concept of precision medicine prevention
2018 National Academy of Medicine Annual Meeting October 15, 2018 Targeting Cancer with Precision Prevention Ernest Hawk, M.D., M.P.H. What is Precision Prevention? The concept of precision medicine prevention
Current and future applications of Molecular Pathology. Kathy Walsh Clinical Scientist NHS Lothian
 Current and future applications of Molecular Pathology Kathy Walsh Clinical Scientist NHS Lothian Molecular Pathology in Solid tumours Cancer type Genes tested Purpose Associated treatments Non small cell
Current and future applications of Molecular Pathology Kathy Walsh Clinical Scientist NHS Lothian Molecular Pathology in Solid tumours Cancer type Genes tested Purpose Associated treatments Non small cell
Colonic polyps and colon cancer. Andrew Macpherson Director of Gastroentology University of Bern
 Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Serrated Lesions in the Bowel Cancer Screening Programme
 Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Célia DeLozier-Blanchet
 The Genetics Consultation in OB-GYN : Hereditary cancers Célia DeLozier-Blanchet Division of Medical Genetics, Geneva University Hospital It is probable that all cancers are genetic! genetic vs. hereditary
The Genetics Consultation in OB-GYN : Hereditary cancers Célia DeLozier-Blanchet Division of Medical Genetics, Geneva University Hospital It is probable that all cancers are genetic! genetic vs. hereditary
Multistep nature of cancer development. Cancer genes
 Multistep nature of cancer development Phenotypic progression loss of control over cell growth/death (neoplasm) invasiveness (carcinoma) distal spread (metastatic tumor) Genetic progression multiple genetic
Multistep nature of cancer development Phenotypic progression loss of control over cell growth/death (neoplasm) invasiveness (carcinoma) distal spread (metastatic tumor) Genetic progression multiple genetic
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Genetic Testing for Familial Gastrointestinal Cancer Syndromes. C. Richard Boland, MD La Jolla, CA January 21, 2017
 Genetic Testing for Familial Gastrointestinal Cancer Syndromes C. Richard Boland, MD La Jolla, CA January 21, 2017 Disclosure Information C. Richard Boland, MD I have no financial relationships to disclose.
Genetic Testing for Familial Gastrointestinal Cancer Syndromes C. Richard Boland, MD La Jolla, CA January 21, 2017 Disclosure Information C. Richard Boland, MD I have no financial relationships to disclose.
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Should novel molecular therapies replace old knowledge of clinical tumor biology?
 Should novel molecular therapies replace old knowledge of clinical tumor biology? Danai Daliani, M.D. Director, 1 st Oncology Clinic Euroclinic of Athens Cancer Treatments Localized disease Surgery XRT
Should novel molecular therapies replace old knowledge of clinical tumor biology? Danai Daliani, M.D. Director, 1 st Oncology Clinic Euroclinic of Athens Cancer Treatments Localized disease Surgery XRT
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS
 CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
Beyond the APC era Alternative pathways to CRC. Jeremy R Jass McGill University
 Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
Colorectal Cancer in the Coming Years: What Can We Expect?
 Colorectal Cancer in the Coming Years: What Can We Expect? Clara Montagut, MD, PhD Hospital Universitari del Mar, Barcelona, Spain Memorial Sloan Kettering Cancer Center, New York, United States What Are
Colorectal Cancer in the Coming Years: What Can We Expect? Clara Montagut, MD, PhD Hospital Universitari del Mar, Barcelona, Spain Memorial Sloan Kettering Cancer Center, New York, United States What Are
COST ACTION CA IDENTIFYING BIOMARKERS THROUGH TRANSLATIONAL RESEARCH FOR PREVENTION AND STRATIFICATION OF COLORECTAL CANCER (TRANSCOLOCAN)
") COST ACTION CA17118 - IDENTIFYING BIOMARKERS THROUGH TRANSLATIONAL RESEARCH FOR PREVENTION AND STRATIFICATION OF COLORECTAL CANCER (TRANSCOLOCAN) Working group 1 management committee duties - Contribute
COST ACTION CA17118 - IDENTIFYING BIOMARKERS THROUGH TRANSLATIONAL RESEARCH FOR PREVENTION AND STRATIFICATION OF COLORECTAL CANCER (TRANSCOLOCAN) Working group 1 management committee duties - Contribute
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux
 Michel Ducreux") Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
Clinicopathologic Factors Identify Sporadic Mismatch Repair Defective Colon Cancers
 Anatomic Pathology / MORPHOLOGY IN MMR-DEFECTIVE COLON CANCER Clinicopathologic Factors Identify Sporadic Mismatch Repair Defective Colon Cancers Britta Halvarsson, MD, PhD, 1 Harald Anderson, PhD, 2 Katarina
Anatomic Pathology / MORPHOLOGY IN MMR-DEFECTIVE COLON CANCER Clinicopathologic Factors Identify Sporadic Mismatch Repair Defective Colon Cancers Britta Halvarsson, MD, PhD, 1 Harald Anderson, PhD, 2 Katarina
Biology of cancer development in the GI tract
 1 Genesis and progression of GI cancer a genetic disease Colorectal cancer Fearon and Vogelstein proposed a genetic model to explain the stepwise formation of colorectal cancer (CRC) from normal colonic
1 Genesis and progression of GI cancer a genetic disease Colorectal cancer Fearon and Vogelstein proposed a genetic model to explain the stepwise formation of colorectal cancer (CRC) from normal colonic
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
Pathology perspective of colonic polyposis syndromes
 Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University
 Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University") COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
Disclosures. Goals. Human Tissue as a Prognostic Biomarker 3/24/2017. Disclosure of Relevant Financial Relationships. Patient Prognosis Colon Cancer
 IMMUNOTHERAPY FOR GI MALIGNANCIES LEARNING FROM ZEBRAS Robert A. Anders, M.D., Ph.D. Associate Professor of Pathology Co Director, Tumor Microenvironment Laboratory Bloomberg Kimmel Institute for Cancer
IMMUNOTHERAPY FOR GI MALIGNANCIES LEARNING FROM ZEBRAS Robert A. Anders, M.D., Ph.D. Associate Professor of Pathology Co Director, Tumor Microenvironment Laboratory Bloomberg Kimmel Institute for Cancer
Agenda 8:30 AM. Jennifer L. Hunt
 Agenda Topic Introduction Terence J. Colgan Jennifer L. Hunt Time 8:30 AM Pre-analytic Variables in Molecular Testing Philip A. Branton 8:40 AM Carcinoma of Unknown Primary Site Is Gene Expression Profiling
Agenda Topic Introduction Terence J. Colgan Jennifer L. Hunt Time 8:30 AM Pre-analytic Variables in Molecular Testing Philip A. Branton 8:40 AM Carcinoma of Unknown Primary Site Is Gene Expression Profiling
Clonal evolution of human cancers
 Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana,
CANCER. Inherited Cancer Syndromes. Affects 25% of US population. Kills 19% of US population (2nd largest killer after heart disease)
") CANCER Affects 25% of US population Kills 19% of US population (2nd largest killer after heart disease) NOT one disease but 200-300 different defects Etiologic Factors In Cancer: Relative contributions
CANCER Affects 25% of US population Kills 19% of US population (2nd largest killer after heart disease) NOT one disease but 200-300 different defects Etiologic Factors In Cancer: Relative contributions
Objectives. Briefly summarize the current state of colorectal cancer
 Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Colorectal cancer molecular biology moves into clinical practice
 1 Department of Laboratory Medicine, University of Washington, Washington, USA 2 Clinical Research Division, Fred Hutchison Cancer Research Center, Washington, USA 3 Department of Medicine, University
1 Department of Laboratory Medicine, University of Washington, Washington, USA 2 Clinical Research Division, Fred Hutchison Cancer Research Center, Washington, USA 3 Department of Medicine, University
Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer
 s on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer Francis M. Giardiello, MD, 1 John I. Allen, 2 Jennifer E. Axilbund,
s on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer Francis M. Giardiello, MD, 1 John I. Allen, 2 Jennifer E. Axilbund,
Treatment of Advanced Colorectal Cancer
 Treatment of Advanced Colorectal Cancer Alexis D. Leal, M.D. Assistant Professor, GI Medical Oncology University of Colorado Cancer Center Disclosures None Objectives Review the basics of advanced colorectal
Treatment of Advanced Colorectal Cancer Alexis D. Leal, M.D. Assistant Professor, GI Medical Oncology University of Colorado Cancer Center Disclosures None Objectives Review the basics of advanced colorectal
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2018 Origination: 1/2004 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2018 Origination: 1/2004 Next Review: 1/2019 Policy Blue Cross and Blue Shield of Kansas
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%