FOLLICULAR LYMPHOMA. BHS course: indolent lymphoma 7 th february Ann Janssens MD, PhD Hematology UZ Leuven
|
|
|
- Janice Harrison
- 5 years ago
- Views:
Transcription
1 FOLLICULAR LYMPHOMA BHS course: indolent lymphoma 7 th february 2015 Ann Janssens MD, PhD Hematology UZ Leuven

2 Non Hodgkin Lymphoma Epidemiology US Marginal Zone MALT 8 % Follicular 22 % 20% Incidence FL Europe 5-7/ % 10% Others 6 % SLL/ CLL type anaplastic T/null 8 % 5.3% 2 % 1.1% M age 67y M 52.5% B 83% T/ NK 5% NOS 12% Mantle Cell 6 % 4.8% Lyplasmocytic ly 1.4% DLBCL 35 % 39.2% T-AILD 0.8% Péripheral T cell 7 % 2% lymphoblastic 2 % Burkitt 1 % 2% Non Hodgkin s Lymphoma Classification Project, Blood 1997 Go et al. EHA 2014, abstract
3 WHO: B-cell neoplasms Precursor B-cell neoplasm B-ALL, lymfoblastenlymfoom Mature B-cell neoplasms B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma B-cell prolymphocytic leukemia Lymphoplasmacytic lymphoma Splenic marginal zone B-cell lymphoma Hairy cell leukemia Plasma cell myeloma/plasmacytoma/mgus Extranodal marginal zone B-cell lymphoma (MALT) Nodal marginal zone B-cell lymphoma Follicular lymphoma Mantle cell lymphoma Diffuse large B-cell lymphoma Burkitt lymphoma/burkitt cell leukemia stage 3-4 at diagnosis 80% bone marrow invasion 50%

4 FL-cells are the malignant counterpart of normal germinal center B-cells


5 How to diagnose and stage a FL? Clinical data Personal history Clinical examination Blood examination Full blood count LDH 2 microglobulin HIV, hep B-C Histopathology Bone marrow/threphine Imaging

6 Diagnosis of FL on histopathology Lymph node biopsy Inguinal nodes not first choice due to reactive changes Cervical nodes are prefered A growing node is also prefered Fine needle aspiration DD reactive vs suspected H&N regio: DD epithelioma Core biopsy: no impression of Ln-strukture

7




8 FL immunohistochemistry CD20 Bcl-2 CD10




9 FL immunohistochemistry CD3 CD4 CD8



10 Follicular lymphoma: Grading Grade 1 Grade 2 Grade 3 Histological subtype Number of centroblasts/hpf Grade I 0 5 Grade II 6 15 Grade III > 15 Treat as a FL Grade IIIa Grade IIIb centrocytes still present centroblasts form solid sheets with no residual centrocytes Treat as a DLBCL




11 BONE MARROW EXAMINATION Bone marrow aspirate + biopsy + immunophenotyping + genetics For diagnosis or staging FL? Yes Unexplained cytopenia (disease related, autoimmune, drug related) Yes Confirming complete remission after treatment : Yes

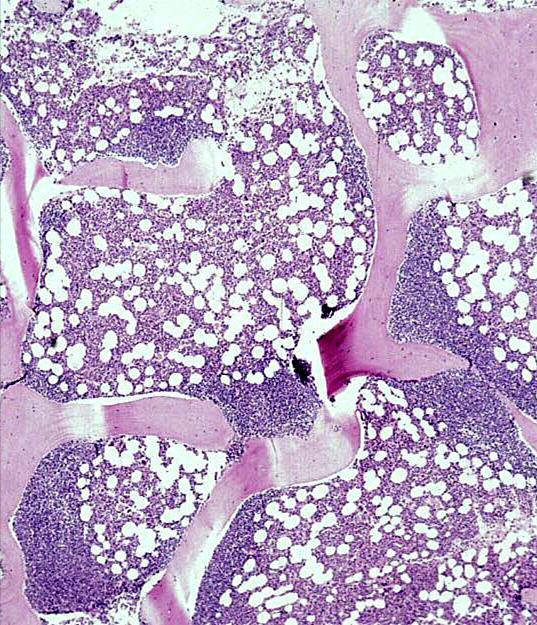
12 Bone marrow infiltration in FL CD20

13 T(14;18) genetic hallmark of FL + additional genetic abnormalities
14 How to diagnose and stage CLL? Clinical data Personal history: most asympthomatic, only 5% reveal B-symptoms Clinical examination: 25% lymphadenopathies, 15% organomegaly Blood examination: leukocytosis due to a lymphocytosis Histopathology Bone marrow/threphine Imaging: - CT-scan neck, thorax, abdomen & pelvis - PET-CT
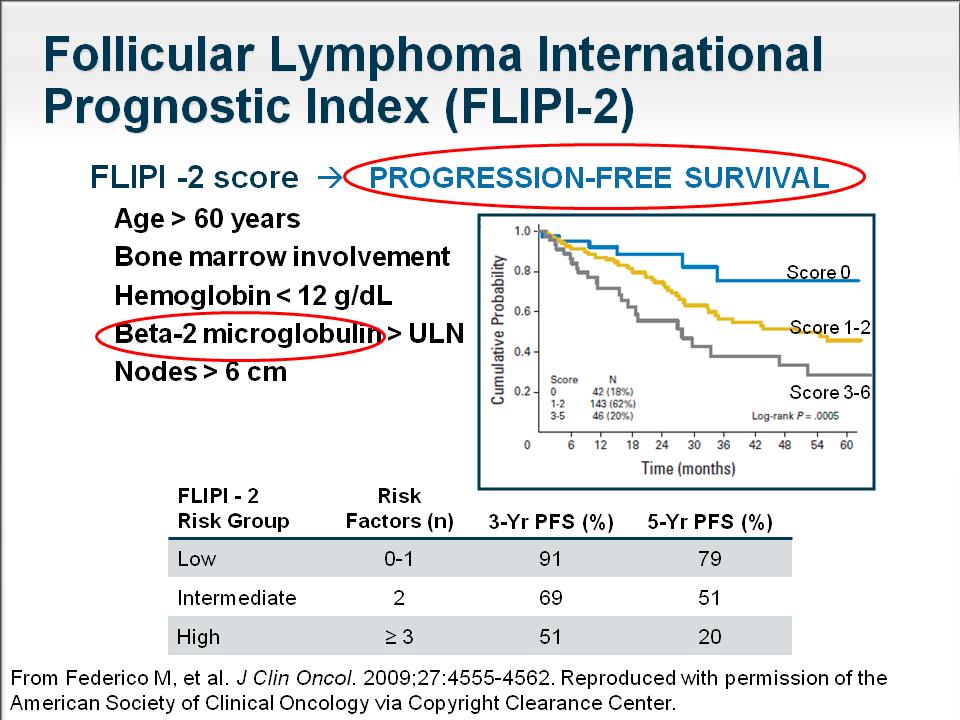
15 International prognostic index for follicular lymphoma ( FLIPI-index) Age :< of > 60 jaar Stage :I, II vs III, IV LDH :nl vs elevated Hb :> 12 vs <12 g/dl N of nodal sites :> 4 Number of Nodal sites > 4 LDH > normal Age > 60 N O L A S H Ann Arbor Stage III-IV Hemoglobin < 12

16 Follicular Lymphoma Survival according FLIPI-index 10 y OS 71% 51% 36% N= 1795 Solal-Celigny, P. et al. Blood 2004;104: Factors, n Risk Patients, % 5-Yr OS, % 10-Yr OS 0-1 Good Intermediate Poor
17


+ FLIPI: 2")
18 M, 51y, new diagnosis FL Male <60j Stage 4 Bone marrow + LDH nl Hb >12 B2 elevated T(14;18)+ FLIPI: 2 FLIPI2: 2


pos FLIPI: 2")
19 M, 60y, relapsing FL Male 60y Stage 4 Bone marrow + LDH nl Hb >12 B2 nl New Ln biopsy: FL grade 1-2 T(14;18)pos FLIPI: 2 FLIPI2: 1


20 Follicular lymphoma: Disease transformation Transformation to aggressive lymphoma in ±37% of patients in the 15y following diagnosis Lister, JCO, 2007
21 Probability of survival (%) Survival Patterns are Different for Indolent and Aggressive NHL 100 Indolent NHL (e.g. Follicular lymphoma) Aggressive NHL (e.g. Diffuse large B-cell lymphoma) Years The Non-Hodgkin s Lymphoma Classification Project. Blood 1997;89:





22 Treatment options for FL Radiotherapy Watchful waiting Chlorambucil, Cyclophosphamide High-dose therapy Kinase inhibitors Lenalidomide. Treatment modalities CIT= chemo + Mo Ab CVP CHOP Flu-combinations Bendamustine Monoclonal Ab
23 Follicular Lymphoma: Treatment stage I en II ( <3 nodi): involved field irradiation Stad III-IV: >60j en asymptomatisch Watch and wait 50% nood aan behandeling binnen de 24m 80 à 90% behandeld eerste 5 j ± 20% spontane remissies! Stad III-IV: <60j en >60j met symptomen Chlorambucil, CVP, CHOP, a-interferon Fludarabine en combinaties Rituximab, R-CVP of R-CHOP of R-FCM, Rituximab onderhoud Zevalin consolidatie Autologe transplantatie als consolidatie Allogene transplantatiediagnose
 (excessive")
24 Radiotherapy for localised FL Involved field radiotherapy 37% relapse free at 20y (Macmanus et al) 50% stage I cured, 25% stage II (MDACC) PFS influenced by tumor size < or > 3 cm and stage I vs II Relapses possible even after 30y, however rare > 10y 2% in-field failure-rate at 20 years 85% of failures in out-of-field nodal sites Extended field radiotherapy-tli (stage III-IV) (excessive toxicity, > secondary cancers) IFRT with chemotherapy (eradication occult disease) + Chl, CVP, CHOP, TROG/ALLLG trial ongoing: Involved field RT Gy with or without R-CVP x 6 ( ongoing till 2022)
25 Treatment guidelines: stage 1-2 RT preferred treatment of localized FL (36) Gy (no difference between 24-45Gy), involved field No data that show that RT is better than other treatment modalities, also not observation (no prospective trials, only retrospective data, data acquired before the R-era) If RT toxicity outweights the potential benefits then observation is a reasonable alternative Hiddemann et al, Leukemia, 2014 Dreyling et al, ESMO guidelines, Ann Oncol 2014 Kuruvilla et al, Canadian guidelines FL 1st line, Clin Lymph Myeloma Leuk 2015


26 LymphoCare database FL stage 1: 27% IFRT 28% CIT 12% R 23% Other R+ IFRT N= 471 Only 206 staged with a bone marrow Friedberg JW et al., JCO, 2009 and
27 Follicular Lymfoma Treatment stage I en II ( <3 nodi): involved field bestraling Stage III-IV: asymptomatic or/and low tumor burden Watch and wait 50% in need for treatment <24mo 80 à 90% treated in the coming 5y ± 20% spontaneous remissions! Stage III-IV: <60j en >60j met symptomen Chlorambucil, CVP, CHOP, a-interferon Fludarabine en combinaties Rituximab, R-CVP of R-CHOP of R-FCM, Rituximab onderhoud Zevalin consolidatie Autologe transplantatie als consolidatie Allogene transplantatiediagnose
28 Wait and see if No systemic symptoms < 3 nodal sites no bulky nodes No splenomegaly >16cm No effusions No compressive symptoms No circulating lymphoma cells No cytopenia No rapid disease progression No renal infiltration No bone lesions No life treatening organ involvement Impairment of qol Induction of myelosuppression, fatigue, secondary leukemia Impairment of collection of stem cells Induction of tumor resistance? Increasing risk of transformation????
 Higher risk of transformation if W&W??? Ardeshna et al, Lancet 2003")
29 Before R era: W&W vs Chl 3 trials W &W vs Promace-MOPP W & W vs predimustin W&W vs IFN-a No gain in OS mttt: 2.6y At 10y: 19% not treated ( 40% of >70y) Higher risk of transformation if W&W??? Ardeshna et al, Lancet 2003


30 R-era: W&W vs R stage II-IV, non-bulky ( ) Ardeshna et al, Lancet Oncol, 2014
 OS 3y W&W 94% R + MR 97% Will")


31 R-era: W&W vs R stage II-IV, non-bulky ( ) OS 3y W&W 94% R + MR 97% Will early treatment impair further treatment wit R or R- chemo? Improved psychological well-being in the R arms Time to chemo- or radiotherapy longer in the R-arm Ardeshna et al, Lancet Oncol, 2014


32 R-era: R with maintenance or retreatment Median follow-up: 4.5 y Till progression Kahl, JCO, 2014 Time to treatment failure identical

33 Low tumor burden GELF No systemic symptoms < 3 nodal sites of > 3cm no bulky nodes (< 7) No splenomegaly >16cm No vital organ compression No compressive symptoms > 5000 clonal lymphocytes No cytopenia Hb <10, plt <100000, PMN <1500 FLIPI low 17%, intermediate 47%, high 36% Kahl, JCO, 2014 GELF: Groupe pour l etude de lymphome folliculaire
34 2014 by American Society of Clinical Oncology Kahl B S et al. JCO 2014;32:
35 Treatment guidelines low tumor burden FL Observation if not fulfilling criteria for starting treatment according GELF-BLNI criteria If results of Ardeshna should be confirmed, R immediately as risk of relapse is reduced??? Hiddemann et al, Leukemia, 2014 Dreyling et al, ESMO guidelines, Ann Oncol 2014 Kuruvilla et al, Canadian guidelines FL 1st line, Clin Lymph Myeloma Leuk 2015
36 Follicular Lymphoma Treatment stad I en II ( <3 nodi): involved field bestraling ( relapsen mogelijk zelfs na 30j) Stad III-IV: >60j en asymptomatisch Watch and wait 50% nood aan behandeling binnen de 24m 80 à 90% behandeld eerste 5 j ± 20% spontane remissies! Stage III-IV: symptomatic and/or high tumor burden Chlorambucil, CVP, CHOP, a-interferon Fludarabine en combinaties, bendamustine Rituximab-chemo Rituximab maintenance Radio-immunotherapy (Zevalin) Autologeous transplantation Allogeneic transplantation

37 Marcus-trial: R-CVP vs CVP - PFS R-chemo is the standard of care for high tumor burden FL



38 Is one chemotherapeutic regimen better than another? R- CVP R- CHOP R-FM R- Benda

39 Primary Rituximab and MAintenance Study An intergroup international study co-ordinated by Untreated follicular NHL R-CVP 8 or R-CHOP 6 + 2R or R-FCM 6 + 2R or R-MCP 6 + 2R R A N D O M I Z E Rituximab maintenance 1 dose every 8 weeks for 24 months CR/PR Observation R-CHOP 74% R-CVP 23% R-FCM 3,5% PDs/SDs off study Salles G et al., JCO, 2011
40 pat enrolled National LymphoCare Study 80% at non academic sites Median age 61y F 52%, whites 91% Grade 1: 43%, grade 2: 29%, grade 3: 19% Stage I 17%, II 15%, III 29%, IV 37% Friedberg JW et al., JCO, 2009 and Initial Treatment Clincal trial 6% WW 18% Other 1% R-mono 14% XRT 5% Chemo 3% 500 pat grade 3: PFS & OS not significantly different between R-CHOP and R-CVP (median follow-up: 4.5 yrs) R-Chemo 53% R-CHOP 55% R-CVP 23.1% R-F 15.5% Other 6.4%

41 PFS in FL after 1st line treatment
42 Responses in FL according to 1 st line N= 534 M age 56 y treatment R-FM: more myelotoxicity and secondary malignancies TTF 3y OS R-CVP 46% 98% R-CHOP 64% 95% R-FM 61% 93% Federico, JCO, 2013
43 The Bright trial: BR vs RCVP/RCHOP in inhl and MCL Excluded: transformed disease, CLL-SLL, grade 3 FL Median age y inhl: BR 213, RCVP/CHOP 206 MCL BR 37, RCHOP 37% BR RCHOP RCVP ORR 97% 90% 83% CR 31% 23% 23% CR for BR or R-CVP/CHOP non inferior More nausea and emesis for BR, antiemetics equal Less neuropathy for BR Neutropenia > CHOP although more G-CSF use Lymphopenia > BR: 66 vs 33% Efficacy equal Toxicity different Flinn, ICML 2013, abstract 084

44

45
46
47
48 Treatment guidelines for FL with high tumor burden CIT except when chemotherapy is contraindicated F-based regimen no 1st line treatment due to toxicities No preference between R-CHOP, R-benda vs R- CVP Hiddemann et al, Leukemia, 2014 Dreyling et al, ESMO guidelines, Ann Oncol 2014 Kuruvilla et al, Canadian guidelines FL 1st line, Clin Lymph Myeloma Leuk 2015


49 after induction treatment consolidation maintenance? Radioimmunotherapy autosct R- maintenance

 Benefits seen in all 3")

50 Median follow-up: 73 mo PFS 6y favors R-arm: 59.2 vs 42.7% (p<0.0001) Benefits seen in all 3 FLIPI groups, CR increased after 2y of maintenance No difference in OS Salles et al, Lancet, 2011

51 Maintenance after 1st line R new standard of maintenace after induction when >PR Expensive Toxic. More infections More neutropenia maintenance Re-treatment
52 Rituximab maintenance in FL Infection-related adverse events in patients with follicular lymphoma treated with rituximab maintenance compared with observation Hazard ratio 1.99 ( CI ) Vidal et al, JNCI 2009 Van Oers: gr 3-4 infections: 9.7% vs 2.4%
 with minimal toxiciy and maintaining qol Johnson et al. J Clin Oncol. 1995;13:140-147. Years Treatment No. Treated RR, % Duration, Yrs Survival, Yrs First 204 88 2.6 9.")
53 Duration of remission in patients with indolent NHL No Curative treatment available for advanced stages First course Second Third Fourth course Goal of treatment: effective and durable disease control (OS-PFS) with minimal toxiciy and maintaining qol Johnson et al. J Clin Oncol. 1995;13: Years Treatment No. Treated RR, % Duration, Yrs Survival, Yrs First Second Third Fourth

54 Maintenance R in folliculair lymfoom na tweede respons op CHOP of R-CHOP Van Oers et al., Blood, 2006
 Period of previous remission Refractory to R-monotherapy or R-chemo Tolerance of previous")
55 Considerations for subsequent therapy Age Comorbidities Candidate for transplant? Previous treatment(s) Period of previous remission Refractory to R-monotherapy or R-chemo Tolerance of previous treatments Fit or unfit? Patient s preference
56 But not all patients respond to R or R-chemo 1 st line R SD and/or progression R (Gela phase 2) 27% R (Ardeshna) 27% 25% 1st line R-chemo SD and/or progression R-CVP 20% R-CHOP < 10% R-MCP 10% R-Benda < 10% 15% >2nd line R-chemo SD and/or progression R-CHOP 30% R-FCM 30% 30%

57 And some relapse or progress during maintenance R + R maintenance 1st line 20% SD and/or progression R-CHOP + IFNa 20% EORTC 20981: R/3m/24m 30% at <2.5y GLSG: R/6m 20% at <15m 25% during upfront and 1th relapse treatment approximately 70% of patients with inhl become refractory to rituximab
58 Treatment options for rituximab refractory inhl Radioimmunotherapy Monoclonal antibodies Hematopoietic transplantation Chemotherapy: bendamustine New drugs??? Immunomodulatory agents B-cell receptor signalling inhibitors mtor pathway inhibitors Proteasoom inhitors Histose deacetylase inhibitors Apoptosis inducing agents BH3mimetics
 74% CR 15% TTP 6.8m TTP for responders 8.")
59 RIT in R-refractory inhl 90 Y 90 Y 9o Y-ibrutumomab (Zevalin) N= 57 (54 FL) M age: 54y Median number of previous R/: 4 (1-9) 76% resistant to last chemo All no reponse or relapse <6m to R monotherapy 90 Y ORR (FL) 74% CR 15% TTP 6.8m TTP for responders 8.7m Witzig et al, JCO 2002, 20:
60 Bendamustine (Levact): active in R-refractory patients Relapsed/refractory indolent lymphoma 120 mg/m² d1-2 (n= 52) ORR 73%, CR 11%, remission duration 16m Relapsed/refractory indolent lymphoma: (n= 76), Refractory to R (61% FL ) ORR 77% CR 34%, response duration 9m (indolent) Alkylator refractory OR 66% R refractory indolent NHL (n=100) ( FL 62%) ORR 84% CR 32%, Respons duration 9.3m Cheson et al., JCO 2009
 10-20% secondary malignancies ( 10% t-mn) Indications for")
61 Autologeous stem cell transplantation Improve disease control with no impact on OS In RCT s longer PFS compared to control arm postremission IFN) but OS not changed ( chemo, Outcomes comparable if R before autotransplant Low transplant related mortality Transplant contamination by lymphoma (in vivo or ex vivo purging give better outcomes) 10-20% secondary malignancies ( 10% t-mn) Indications for autotx:??? go go patients (<70y without comorbidity) at first (???) relapse relapse within 24m after an anthracycline containing regimen No data on autotx in R-refractory patients If relapse <1y after treatment: dismal prognosis, candidate for allotx
62 Allogeneic stem cell transplantation The only curative treatment option for inhl! Advantages: Stem cells free of lymphoma and prior chemotherapy induced DNA damage Lower relapse rate Lower rate of secondary malignancies Graft vs lymphoma effect Plateau in relapses (20% at 3à 5y posttx) Disadvantages: Requirement of a HLA- matched donor TRM >20% (higher if chemo-r disease) cgvhd 50% RIC: better outcome >50y and more comorbidities Indications for allo Tx: No CR to upfront treatment Duration of response <2y Relapse after autologeous Tx, if bone marrow burden is high and disease is refractory but Better outcome if chemosensitive No data on allo Tx in R-refractory patients

 Target PD1-PDL1: pidilizumab ORR 19/35 with CR 14 Target CD137 (T), Kir (NK), CD47")

63 Chemo-free treatment for FL Kinase inhibitors lenalidomide Monoclonals Optimize dose and shedule of rituximab Other anti-cd20 monoclonals Combine anticd20 with anticd22, 80, 74, 37 Combine with G- or GM-CSF, IL2, IL-12, IFN-a Lenalidomide Combine with rituximab ( more CR, more neutropenia) Combine with GA-101 (GALEN phase 1b) Target PD1-PDL1: pidilizumab ORR 19/35 with CR 14 Target CD137 (T), Kir (NK), CD47 (phagocytosis) Bcl2-inhibitors Kinase inhibitors: Idelalisib in double Refr FL: ORR 57%, mdor 12.5 mo Ibrutinib R/R FL: ORR 56%, PFS 1y 50%, with R, with BR Bcl-2 antagonists Monoclonal antibodies Educational session FL EH 2014, G. Salles,
64 Overall Survival (%) Improving Survival of Follicular NHL: Impact of Antibody-Based Therapy OS by Treatment 1990s-2000s s Year N Death Estimate CHOP + Mab % ProMace % CHOP % Years After Registration Reprinted with permission American Society of Clinical Oncology. All rights reserved. Fisher RI, et al. J Clin Oncol. 2005; 23: s
65 FOLLICULAR LYMPHOMA Easy to treat. difficult to cure
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
Open questions in the treatment of Follicular Lymphoma. Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland
 Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Follicular Lymphoma. Michele Ghielmini. Oncology Institute of Southern Switzerland Bellinzona
 Follicular Lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona Conflicts of interest Astra Zeneca Roche Cellgene Mundipharma Janssen Gilead Bayer Abbvie FL remains an incurable
Follicular Lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona Conflicts of interest Astra Zeneca Roche Cellgene Mundipharma Janssen Gilead Bayer Abbvie FL remains an incurable
The case against maintenance rituximab in Follicular lymphoma. Jonathan W. Friedberg M.D., M.M.Sc.
 The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES
 How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting?
 Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
Follicular Lymphoma 2016:
 Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
SEQUENCING FOLLICULAR LYMPHOMA
 SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Challenges in the Treatment of Follicular Lymphoma
 Challenges in the Treatment of Follicular Lymphoma Prof. Michele Ghielmini Clinical Director Oncology Institute of Southern Switzerland Bellinzona ESMO guidelines 2014 (simplified) Low tumor burden High
Challenges in the Treatment of Follicular Lymphoma Prof. Michele Ghielmini Clinical Director Oncology Institute of Southern Switzerland Bellinzona ESMO guidelines 2014 (simplified) Low tumor burden High
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Lymphoma 101. Nathalie Johnson, MDPhD. Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University
 Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma
 12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
Is there still a role for autotransplant with follicular lymphoma in the rituximab era. Pr. Christian Gisselbrecht Hôpital Saint Louis Paris, France
 COSTEM Berlin September 8-11 211. Is there still a role for autotransplant with follicular lymphoma in the rituximab era. Pr. Christian Gisselbrecht Hôpital Saint Louis Paris, France World Health Organization
COSTEM Berlin September 8-11 211. Is there still a role for autotransplant with follicular lymphoma in the rituximab era. Pr. Christian Gisselbrecht Hôpital Saint Louis Paris, France World Health Organization
Indolent Lymphomas: Current. Dr. Laurie Sehn
 Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Targeted Radioimmunotherapy for Lymphoma
 Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
The case for maintenance rituximab in FL
 New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
eastern cooperative oncology group Michael Williams, Fangxin Hong, Brad Kahl, Randy Gascoyne, Lynne Wagner, John Krauss, Sandra Horning
 Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Patterns of Care in Medical Oncology. Follicular Lymphoma
 Patterns of Care in Medical Oncology Follicular Lymphoma CASE 1: A 72-year-old man with multiple comorbidities including COPD/asthma presents with slowly progressive cervical adenopathy. Bone marrow biopsy
Patterns of Care in Medical Oncology Follicular Lymphoma CASE 1: A 72-year-old man with multiple comorbidities including COPD/asthma presents with slowly progressive cervical adenopathy. Bone marrow biopsy
How to Refine Treatment Choice in Follicular Lymphoma: From Low-Tumor Burden to High-Risk Follicular Lymphoma
 How to Refine Treatment Choice in Follicular Lymphoma: From Low-Tumor Burden to High-Risk Follicular Lymphoma Peter A. Riedell, MD and Brad S. Kahl, MD Abstract Follicular lymphoma (FL) is the most common
How to Refine Treatment Choice in Follicular Lymphoma: From Low-Tumor Burden to High-Risk Follicular Lymphoma Peter A. Riedell, MD and Brad S. Kahl, MD Abstract Follicular lymphoma (FL) is the most common
Treatment Nodal Marginal Zone Lymphoma
 Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
C r h ist s op o h p e h r e R. R F l F ow o er e s, s M D, D M S
 1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
GLSG/OSHO Study Group. Supported by Deutsche Krebshilfe
 GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 18 July 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2012 MABTHERA 100 mg, concentrate for solution for infusion B/2 (CIP code: 560 600-3) MABTHERA 500 mg, concentrate
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2012 MABTHERA 100 mg, concentrate for solution for infusion B/2 (CIP code: 560 600-3) MABTHERA 500 mg, concentrate
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège. 14 th post-ash meeting, January 6 th 2011, Brussels
 Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Mantle Cell Lymphoma: Update in Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency
 Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Bendamustine: A Transversal * Chemotherapy Agent
 Bendamustine: A Transversal * Chemotherapy Agent Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, D.C., USA *Def Cutting across two lines, intersecting
Bendamustine: A Transversal * Chemotherapy Agent Bruce D. Cheson, M.D. Georgetown University Hospital Lombardi Comprehensive Cancer Center Washington, D.C., USA *Def Cutting across two lines, intersecting
1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes on the next page
 COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
Managing patients with relapsed follicular lymphoma. Case
 Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Brad S Kahl, MD. Tracks 1-21
 I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma
 How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
Low grade Non-Hodgkin Lymphoma: New Therapies & Updates
 Low grade Non-Hodgkin Lymphoma: New Therapies & Updates Craig A. Portell MD Assistant Professor of Medicine ivision of Hematology/Oncology University of Virginia Friday, April 28, 2017 Disclosures I have
Low grade Non-Hodgkin Lymphoma: New Therapies & Updates Craig A. Portell MD Assistant Professor of Medicine ivision of Hematology/Oncology University of Virginia Friday, April 28, 2017 Disclosures I have
Rituximab in the Treatment of NHL:
 New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
CLL: disease specific biology and current treatment. Dr. Nathalie Johnson
 CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
Head and Neck: DLBCL
 Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
TRANSPARENCY COMMITTEE OPINION. 8 November 2006
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 8 November 2006 MABTHERA 100 mg, concentrate for solution for infusion (CIP 560 600-3) Pack of 2 MABTHERA 500 mg,
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 8 November 2006 MABTHERA 100 mg, concentrate for solution for infusion (CIP 560 600-3) Pack of 2 MABTHERA 500 mg,
Outcomes of Treatment in Slovene Follicular Lymphoma Patients
 Original Study Outcomes of Treatment in Slovene Follicular Lymphoma Patients Tanja Juznic Setina, Simona Borstnar, Barbara Jezersek Novakovic Abstract The treatment outcomes of follicular lymphoma (FL)
Original Study Outcomes of Treatment in Slovene Follicular Lymphoma Patients Tanja Juznic Setina, Simona Borstnar, Barbara Jezersek Novakovic Abstract The treatment outcomes of follicular lymphoma (FL)
Diffuse Large B-Cell Lymphoma (DLBCL)
") Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma
 UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
Mathias J Rummel, MD, PhD
 I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
Bendamustine for relapsed follicular lymphoma refractory to rituximab
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine for relapsed follicular lymphoma refractory to rituximab Bendamustine for relapsed follicular lymphoma refractory to rituximab Contents Summary 1
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine for relapsed follicular lymphoma refractory to rituximab Bendamustine for relapsed follicular lymphoma refractory to rituximab Contents Summary 1
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
Lymphomas in Prof Paul Ruff Division of Medical Oncology
 Lymphomas in 2010 Prof Paul Ruff Division of Medical Oncology Most Common Lymphomas: ~90% B-cell and ~10% T-cell T lymphoblastic: 2% Marginal zone, nodal: 2% Other: 9% Burkitt: 2% Anaplastic large cell:
Lymphomas in 2010 Prof Paul Ruff Division of Medical Oncology Most Common Lymphomas: ~90% B-cell and ~10% T-cell T lymphoblastic: 2% Marginal zone, nodal: 2% Other: 9% Burkitt: 2% Anaplastic large cell:
Follicular Lymphoma: Updates and novel immune therapies
 Follicular Lymphoma: Updates and novel immune therapies Larry W. Kwak, M.D., Ph.D. Cancer Center Associate Director for Translational Research and Developmental Therapeutics Director, Toni Stephenson Lymphoma
Follicular Lymphoma: Updates and novel immune therapies Larry W. Kwak, M.D., Ph.D. Cancer Center Associate Director for Translational Research and Developmental Therapeutics Director, Toni Stephenson Lymphoma
Emerging targeted therapies for follicular lymphoma A future without chemotherapy
 Emerging targeted therapies for follicular lymphoma A future without chemotherapy Pier Luigi Zinzani Institute of Hematology L. e A. Seràgnoli University of Bologna FOLLICULAR LYMPHOMA: GENERAL ASPECTS
Emerging targeted therapies for follicular lymphoma A future without chemotherapy Pier Luigi Zinzani Institute of Hematology L. e A. Seràgnoli University of Bologna FOLLICULAR LYMPHOMA: GENERAL ASPECTS
How I treat High-risk follicular lymphoma
 How I treat High-risk follicular lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona 1) median OS raised from 10 to 18 y 2) advanced FL remains uncurable Stanford, n = 1334
How I treat High-risk follicular lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona 1) median OS raised from 10 to 18 y 2) advanced FL remains uncurable Stanford, n = 1334
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes
 Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
MANTLE CELL LYMPHOMA
 MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
POST ICML Indolent lymphomas relapse treatment
 POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
Mantle cell lymphoma An update on management
 Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
Notification to Implement Issued by pcodr: December 14, 2012
 PROVINCIAL FUNDING SUMMARY Bendamustine hydrochloride (Treanda) for indolent Non-Hodgkin Lymphoma and Mantle Cell Lymphoma (first-line and relapsed/refractory) perc Recommendation: Recommends For further
PROVINCIAL FUNDING SUMMARY Bendamustine hydrochloride (Treanda) for indolent Non-Hodgkin Lymphoma and Mantle Cell Lymphoma (first-line and relapsed/refractory) perc Recommendation: Recommends For further
Updates in the Treatment of Non-Hodgkin Lymphoma: ASH Topics
 Updates in the Treatment of Non-Hodgkin Lymphoma: ASH 2008 Joseph Tuscano, M.D. UC Davis Cancer Center 1 Topics Mantle Cell Lymphoma What is the standard of care for younger patients? (abstracts 581, 769,
Updates in the Treatment of Non-Hodgkin Lymphoma: ASH 2008 Joseph Tuscano, M.D. UC Davis Cancer Center 1 Topics Mantle Cell Lymphoma What is the standard of care for younger patients? (abstracts 581, 769,
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL
 Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Lymphoma- Med A-new drugs and treatments
 Lymphoma- Med A-new drugs and treatments Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Disclosures: Roche, Gilead Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Outline Lymphoma- what is
Lymphoma- Med A-new drugs and treatments Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Disclosures: Roche, Gilead Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Outline Lymphoma- what is
Choice of upfront treatment in the management of diffuse large B-cell lymphoma and follicular lymphoma
 Choice of upfront treatment in the management of diffuse large B-cell lymphoma and follicular lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Choice of upfront treatment in the management of diffuse large B-cell lymphoma and follicular lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bendamustine (Treanda) for Non-Hodgkin Lymphoma November 29, 2012
 for Non-Hodgkin Lymphoma November 29, 2012") pan-canadian Oncology Drug Review Final Clinical Guidance Report Bendamustine (Treanda) for Non-Hodgkin Lymphoma November 29, 2012 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bendamustine (Treanda) for Non-Hodgkin Lymphoma November 29, 2012 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Lymphocyte Predominant Hodgkin s Lymphoma. Case Presentation. How would you treat the patient?
 Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients
 Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Solomon Graf, MD February 22, 2013
 Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
State of the Art Treatment for Relapsed Mantle Cell Lymphoma
 Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
Clinical Commissioning Policy: Bendamustine with rituximab for relapsed and refractory mantle cell lymphoma (all ages)
") Clinical Commissioning Policy: Bendamustine with rituximab for relapsed and refractory mantle cell lymphoma (all ages) NHS England Reference: 170029P 1 NHS England INFORMATION READER BOX Directorate Medical
Clinical Commissioning Policy: Bendamustine with rituximab for relapsed and refractory mantle cell lymphoma (all ages) NHS England Reference: 170029P 1 NHS England INFORMATION READER BOX Directorate Medical
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009
 Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
The Clinical Characteristics and Treatment Response of Patients with Low Grade Non-Hodgkin Lymphoma
 The Egyptian Journal of Hospital Medicine (January 2019) Vol. 74 (4), Page 789-796 The Clinical Characteristics and Treatment Response of Patients with Low Grade Non-Hodgkin Lymphoma Ahmed Yosry El-Agamawi,
The Egyptian Journal of Hospital Medicine (January 2019) Vol. 74 (4), Page 789-796 The Clinical Characteristics and Treatment Response of Patients with Low Grade Non-Hodgkin Lymphoma Ahmed Yosry El-Agamawi,
Clinical Commissioning Policy Proposition: Bendamustine with rituximab for relapsed indolent non-hodgkin s lymphoma (all ages)
") Clinical Commissioning Policy Proposition: Bendamustine with rituximab for relapsed indolent non-hodgkin s lymphoma (all ages) Reference: NHS England 1607 1 First published: TBC Prepared by NHS England
Clinical Commissioning Policy Proposition: Bendamustine with rituximab for relapsed indolent non-hodgkin s lymphoma (all ages) Reference: NHS England 1607 1 First published: TBC Prepared by NHS England
OSCO/OU ASH-SABC Review. Lymphoma Update. Mohamad Cherry, MD
 OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA
 BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA General Non-Hodgkin s lymphomas (NHLs) encompass several unique malignant lymphoid disease entities that vary in clinical behavior, morphologic appearance,
BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA General Non-Hodgkin s lymphomas (NHLs) encompass several unique malignant lymphoid disease entities that vary in clinical behavior, morphologic appearance,
Angioimmunoblastic T-cell lymphoma: nobody knows what to do...
 Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Non-Hodgkin Lymphoma in Clinically Difficult Situations
 Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Lymphoma John P. Leonard, M.D.
 Lymphoma 2017 John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Vice Chairman, Department of Medicine Disclosures Consulting
Lymphoma 2017 John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Vice Chairman, Department of Medicine Disclosures Consulting
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center
 LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
Dr. Noelle O Rourke Beatson Oncology Centre, Glasgow RADIOTHERAPY FOR LYMPHOMA???
 Dr. Noelle O Rourke Beatson Oncology Centre, Glasgow RADIOTHERAPY FOR LYMPHOMA??? History of Radiotherapy 1895 Rontgen describes X-rays 1896 Becquerel radioactivity 1905 Radiation is used to treat tumours
Dr. Noelle O Rourke Beatson Oncology Centre, Glasgow RADIOTHERAPY FOR LYMPHOMA??? History of Radiotherapy 1895 Rontgen describes X-rays 1896 Becquerel radioactivity 1905 Radiation is used to treat tumours
Panel Discussion/References
 Follicular Lymphoma (FOLL) FOLL-B category designation for first-line therapy options for FL: Bendamustine + rituximab RCHOP RCVP Submission from Genentech to review the data related to obinutuzumab for
Follicular Lymphoma (FOLL) FOLL-B category designation for first-line therapy options for FL: Bendamustine + rituximab RCHOP RCVP Submission from Genentech to review the data related to obinutuzumab for
Il trattamento del Linfoma Follicolare in prima linea
 Il trattamento del Linfoma Follicolare in prima linea Dr.ssa Carola Boccomini SC Ematologia Dr. U. Vitolo AO Città della Salute e della Scienza Torino, Italy Median follow-up 3 years Median follow-up 6
Il trattamento del Linfoma Follicolare in prima linea Dr.ssa Carola Boccomini SC Ematologia Dr. U. Vitolo AO Città della Salute e della Scienza Torino, Italy Median follow-up 3 years Median follow-up 6
Transformed lymphoma: biology and treatment
 Transformed lymphoma: biology and treatment Silvia Montoto Centre for Haemato-Oncology Barts Cancer Institute 1.00 0.75 0.50 0.25 0.00 N =330 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 Years %Viability
Transformed lymphoma: biology and treatment Silvia Montoto Centre for Haemato-Oncology Barts Cancer Institute 1.00 0.75 0.50 0.25 0.00 N =330 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 Years %Viability
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University
 Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
CLL & SLL: Current Management & Treatment. Dr. Peter Anglin
 CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
CPAG Summary Report for Clinical Panel Policy 1630 Bendamustine-based chemotherapy for first-line treatment of Mantle cell lymphoma (MCL) in adults
 in adults") MANAGEMENT IN CONFIDENCE CPAG Summary Report for Clinical Panel Policy 1630 Bendamustine-based chemotherapy for first-line treatment of Mantle cell lymphoma (MCL) in adults The Benefits of the Proposition
MANAGEMENT IN CONFIDENCE CPAG Summary Report for Clinical Panel Policy 1630 Bendamustine-based chemotherapy for first-line treatment of Mantle cell lymphoma (MCL) in adults The Benefits of the Proposition
Recent Advances in the Treatment of Non-Hodgkin s Lymphomas
 671 Highlights of the NCCN 18th Annual Conference Recent Advances in the Treatment of Presented by Jeremy S. Abramson, MD, and Andrew D. Zelenetz, MD, PhD Abstract Non-Hodgkin s lymphomas (NHL) represent
671 Highlights of the NCCN 18th Annual Conference Recent Advances in the Treatment of Presented by Jeremy S. Abramson, MD, and Andrew D. Zelenetz, MD, PhD Abstract Non-Hodgkin s lymphomas (NHL) represent
MANAGEMENT OF LYMPHOMAS
 MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association