Is there still a role for autotransplant with follicular lymphoma in the rituximab era. Pr. Christian Gisselbrecht Hôpital Saint Louis Paris, France
|
|
|
- Erik O’Brien’
- 5 years ago
- Views:
Transcription






1 COSTEM Berlin September Is there still a role for autotransplant with follicular lymphoma in the rituximab era. Pr. Christian Gisselbrecht Hôpital Saint Louis Paris, France
2 World Health Organization (WHO) Classification of Lymphoid Neoplasms: B-Cell Neoplasms Precursor B-cell neoplasm Precursor B-lymphoblastic leukemia/lymphoma (precursor B-cell acute lymphoblastic leukemia) Mature (peripheral) B-cell neoplasms B-cell CLL/SLL B-cell PLL Lymphoplasmacytic lymphoma Plasmacytoma, plasma cell myeloma HCL Marginal zone B-cell lymphoma Marginal zone B-cell lymphoma of MALT Nodal marginal zone lymphoma (+/- monocytoid B-cells) (Jaffe et al. Oncol. 1998;9 zone (suppl 5):S25). Ann Splenic marginal B-cell FL Follicular : 22% Grade 1, -5 centroblasts/hpf Grade 2, 6-15 centroblasts/hpf Grade 3, >15 centroblasts/hpf 3a, >15 centroblasts, but centrocytes still present 3b, centroblasts from solid sheets with no residual centrocytes Variants Cutaneous follicle center MCL Mantle cell DLCL Diffuse Large Cell Mediastinal (thymic) large B-cell lymphoma Intravascular lymphoma Primary effusion lymphoma
3 FOLLICULAR LYMPHOMA REQUIRING TREATMENT Prog 1 Diagnosis Prog 2 Auto Follow up Interval smaller Nb of phases Other treatments Nb of Chemo High tumor burden Cross over make analysis of survival benefit related to treatments almost impossible Histologic transformation Time in years 3-5%
4 Each recurence is associated Impaired quality of life Diminution of quality of response Diminution of duration of remission Diminution of life expectancy Basis for consolidation therapy
5 TREATMENT OF LYMPHOMA NHL Consolidation Options Poor Risk Chemo + Rituximab CR PR ASCT Ibritumomab Tiuxetan No treatment Rituximab
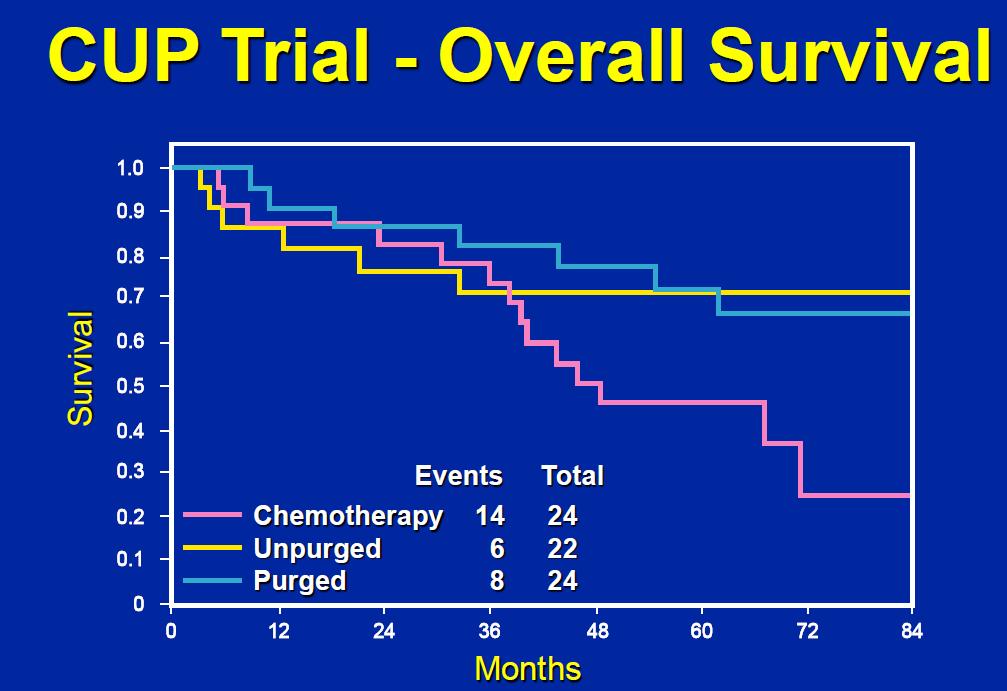
6 Before Rituximab CUP Trial for Follicular Lymphoma Progression-Free Survival 1. Probability.8 Chemotherapy Unpurged Purged Events Total EBMT registry.4 First CR n= Patients at: Chemotherapy Unpurged Purged Schouten HC et al. J Clin Oncol. 23;21: Months Other responses n=
7
8 RELAPSES GELF 86 (111pts)- GELF 94 (144pts) SALVAGE WITH OR WITHOUT AUTOLOGOUS STEM CELL TRANSPLANTATION Rohatiner et al. Gela studies 11.5 y 13 y AZS Rohatiner et al. Myeloablative Therapy With Autologous Bone Marrow Transplantation for Follicular Lymphoma at the Time of Second or Subsequent Remission: Long-Term Follow-Up. J Clin Oncol 27;25:2554 Sebban et al
9 Does Rituximab make a difference at relapse? What is the Impact of first line Treatment? Poor Risk Chemo + Rituximab salvage with rituximab Maintenance after chemo ASCT after response to salvage CR PR ASCT Ibritumomab Tiuxetan No treatment Rituximab
10 Intergroup phase III trial: study design NO first line RITUXIMAB R A N D O M I Z E D CHOP every 21 days maximum 6 cycles Rituximab + CHOP every 21 days maximum 6 cycles CR PR R A N D O M I Z E D Observation Rituximab maintenance* 2 EORTC Data Center *375mg/m every 3 months for 2 years or until relapse 25 Van Oers MHJ, et al.november (Blood. 26;18:3295-
11 Progression-free survival (%) Intergroup phase III trial: PFS from second randomization all patients MabThera maintenance median: 51.6 months Overall log-rank test: p<.1 Hazard ratio:.4 O N Years Number of patients at risk EORTC Data Center 1 2 Observation median: 15. months Treatment Observation MabThera 25 Van Oers MHJ, et al.november (Blood. 26;18:3295-
12 Intergroup phase III trial: PFS from second randomization by induction regimen Progression-free survival after CHOP Median 42. months Median 11.6 months Overall log-rank test: p<.1; HR:.3 O N Years Number of patients at risk : EORTC Data Center 4 Progression-free survival (%) Progression-free survival (%) Subgroups according to induction treatment Progression-free survival after R-CHOP Median 51.9 months Median 23.1 months Overall log-rank test: p=.4; HR: Years 1 4 Treatment Observation MabThera O N Number of patients at risk : Treatment Observation MabThera 25 Van Oers MHJ, et al.november (Blood. 26;18:3295-
13 Intergroup phase III trial: PFS from second randomization by response to induction Progression-free survival after CR Progression-free survival (%) Progression-free survival (%) Subgroups according to response quality after induction Median 51.6 months Median 14.5 months Overall log-rank test: p=.9; HR:.38 1 O N Number of patients at risk : Years EORTC Data Center Median 45.4 months Median 15.6months Overall log-rank test: p<.1; HR: Progression-free survival after PR Treatment Observation MabThera O N Years Number of patients at risk : Treatment Observation MabThera 25 Van Oers MHJ, et al.november (Blood. 26;18:3295-
14 GELF-86 & GELF-94 Design CHVP arm months CHVP+Ifn arm Interferon alpha 5MU S.C. 3 times a week for 18 months PBSC reinjection 94 CHVP regimen TBI Adriamycine 25mg/m2 J1 Endoxan 6mg/m2 J1 Teniposide 6mg/m2 J1 Prednisone 4mg/m2 J1 à J5 6 CHOP+ASCT arm Sebban et al CHOP regimen Cyclophosphamide + Etoposide
15 Treatments according to Studies Gelf-86 Gelf % 92% 1% 1% 11% 1% Yes 2% 47% Alone With chemotherapy No Unknown 1% 1% 98% - 9% 38% 52% 1% Yes 38% 39% No Unknown 57% 5% 59% 1% Number of patients Salvage chemotherapy Yes No Unknown Rituximab: no maintenance High-dose therapy with ASCT

16 RELAPSES GELF 86 (111pts)- GELF 94 (144pts) SALVAGE WITH OR WITHOUT AUTOLOGOUS STEM CELL TRANSPLANTATION Sebban et al Bertrand Coiffier et al ASH 27
17 Survival after Relapse or PD
18 Rituximab at time of Salvage Van Oers et al. Our study R-CHOP M. van Oers M, et al: Rituximab maintenance improves clinical outcome of relapsed/resistant follicular non-hodgkin lymphoma in patients both with and without rituximab during induction: results of a prospective randomized phase 3 intergroup trial. Blood 26;18:
19 EBMT LYM1 <3 <3 <21 28 <3 Days FL in CR/VGPR 2, 3 2 MabThera 375mg/m weekly x 4 2 R No treatment PBPC collection After any treatment CR or VGPR n=46 MabThera 375mg/m q 2 month x4 High-dose therapy BEAM R Observation alone
20 EBMT GELA GOELAMS study in FL: EBMT LYM1 R purging + RR maintenancemaintenance Pts Nb 69 Median PFS NR@ 6.4 y 69 R purging No R y 4.3 y 3.34 y 5y PFS 62.9 % 56 % 46 % 37.6 % 5y OS 79.5 % 8.5 % 84.8 % 78.4 % Ruth Pettengell et al: Blood (ASH) : Abstract 3567
21 Does rituximab maintenance in first line will change the place of autotransplantation?
22 P R IMA : s tu dy de s ig n INDUCTION MAINTENANCE Rituximab maintenance 375 mg/m2 every 8 weeks for 2 years Registration High tumor burden untreated follicular lymphoma Immunochemotherapy 8 x Rituximab + 8 x CVP or 6 x CHOP or 6 x FCM CR/CRu PR PD/SD off study Random 1:1* Observation * Stratified by response after induction, regimen of chemo, and geographic region Frequency of clinical, biological and CT-scan assessments identical in both arms Five additional years of follow-up Salles G et al Lancet 211; 377: 42 51
23 P rim a ry e n dpo in t (P F S ) m e t a t th e pla n n e d in te rim a n a ly s is Rituximab maintenance significantly reduced the risk of progression by 5% Progression-free rate 1. 82% Rituximab maintenance N= Observation N=513 66%.4 stratified HR=.5 95% CI.39;.64 p< Time (months) Patients at risk Salles G et al Lancet 211; 377: 42 51
24 B e n e fit s o f ritu x im a b m a in te n a n c e s e e n in a ll m a jo r s u b -g ro u ps e v a lu a te d Category N Hazard ratio* All < FLIPl R-FCM CR/CRu PR Subgroup All Age FLIPl Index Hazard ratio FLIPl = 2 FLIPl 3 Induction Chemotherapy Response to Induction R-CHOP R-CVP 2 1 Favors maintenance Favors observation 95% CIs 3 Salles G et al Lancet 211; 377: * Non-stratified analysis
25 R e s po n s e s t a tu s a t e n d o f m a in te n a n c e Observation n = 398 * Rituximab n = 389 * 162 (4.7%) 79 (2.3%) Stable disease (SD) 1 (.3%) (%) Partial response (PR) 29 (7.3%) 28 (7.2%) 19 (47.7%) 26 (66.8%) n = 19 n = 258 Patients remaining in CR/CRu 153 (56%) 29 (75%) Patients converting from PR/SD to CR/CRu 37 (3%) 49 (45%) Progressive disease (PD) Complete response (CR/CRu) Response: end of Induction Maintenance The quality of response remains a major parameter * Patients not evaluated/missing data: respectively 16 and 22 pts not evaluated in the rituximab maintenance arm: 2 pts Salles G et al Lancet 211; 377: 42 51
26
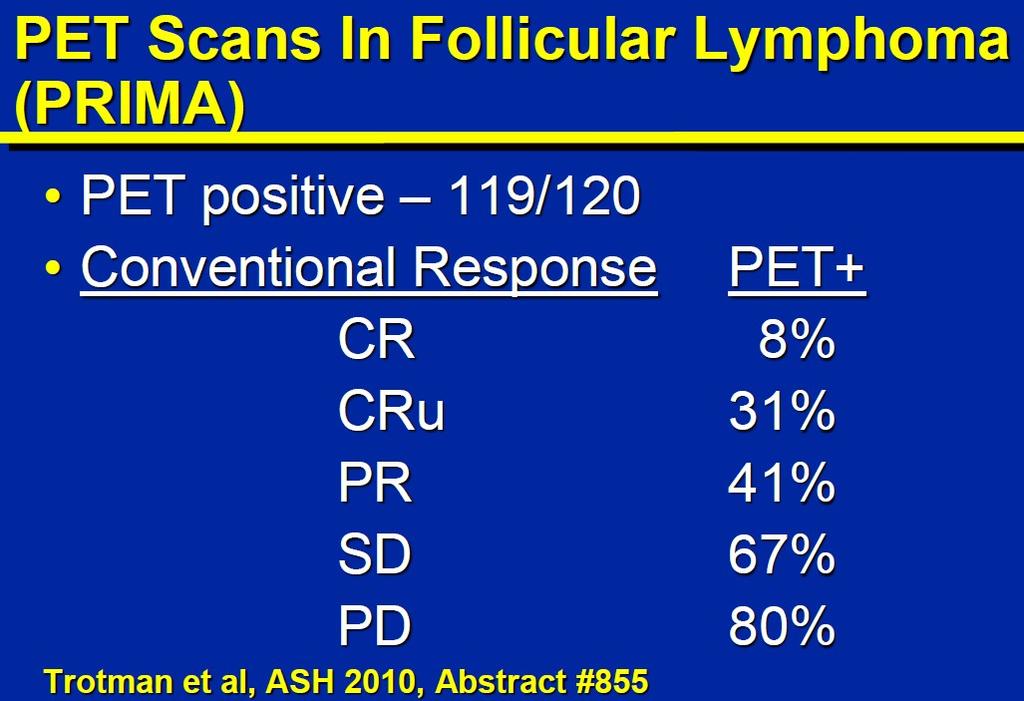
27 Post treatment PET-CT is predictive of patient outcome in follicular lymphoma Analysis of PET-CT in PRIMA study Trotman J et al JCO 211 on line
28 After first line therapy Bachy E, Brice P et al. JCO 29 GELF 86
29 FL2 study design CR : 6% EFS: 63% Arm A 6 months R 12 months Staging including CT-scan and bone marrow biopsy CR : 75% EFS: 78% Arm B D1 Cyclophosphamide 6 mg/m2 D1 Doxorubicin 25 mg/m2 D1 Etoposide 1 mg/m2 D1-D5 Prednisone 4 mg/m2 every month for 6 months (arm A & B) then every 2 months in arm A α-ifn 2b, 4.5 MU tiw for 18 months (3MU if aged 7 yr) Rituximab: 375 mg/m2 Salles G, et al. Blood 28; 112:
30 FL2 study Response to treatment After first line in rituximab treated patients Salles G, et al. Blood 28; 112: Bachy E, Brice P et al. JCO 29
31 FL 2: Patient outcome according to transplantation at first progression: ----transplanted patients (n=42); non-transplanted patients(n=111). Event free survival (P=.5). Overall survival (P=.3) transplantation in follicular lymphoma Steven Le Gouill et al Haematologica 211,
32 FL 2: Patients outcome according to frontline therapy and use of transplantation at first progression (---- transplanted patients and non-transplanted patients Event free survival for patients who fail R-CHVP-I (P=.52). Overall survival for patients who fail R-CHVP-I (P=.52). transplantation in follicular lymphoma Steven Le Gouill et al Haematologica 211,
33
34 Conclusion ASCT is still the best therapy after 1st relapse for most patients with follicular lymphoma, in each situation: before and during rituximab era. Best treatment if histologic transformation Consolidation with ASCT is even more appropiate for patients failing rituximab treatment and can be selected earlier with PET-SCAN. It can be challenged by new therapy or new monoclonal antibodies ASCT is also challenged by RIC allo for survival But improving progression free survival is the first step for: THE LONG WAY FOR CURE
35
36 Allogeneic BMT for Low-Grade Lymphoma Disease-Free Survival After BMT Percentage 1 High Treatment-Related Mortality Low Probability of Relapse van Besien K et al. Blood. 1998;92: Years After BMT 5 6
 6 4 Auto-unpurged (n = 596) Auto-purged (n = 13) 2 1 2 3 4 5 years (K. Van Besien et al.")
37 Adjusted Probability, % LYMPHOME FOLLICULAIRE AUTO/ ALLO SURVIE SANS RECHUTE REGISTRE ABMTR 1 8 Allogeneic (n = 175) 6 4 Auto-unpurged (n = 596) Auto-purged (n = 13) years (K. Van Besien et al., Blood, 23)
38 CONCLUSION We have new tools To improve survival A reasonable objective Survival has improved over the last 25 years as a result of sequential application of effective therapies even before monoclonal antibodies era. The chance for long term cure an idealistic goal.
39 Basis for a maintenance therapy Sustain the disease in ongoing remission Delay disease progression Improve the extent of response attained Extend the interval until next therapy Improve the QOL Improve the survival
40 Response to treatment After first line therapy Bachy E, Brice P et al. JCO 29
41 The Follicular Lymphoma International Prognostic Index (FLIPI): Overall survival Solal-Céligny P, et al. Blood 24; 14: Probability of survival 1. Good ( 1).8 Intermediate (2).6 Poor (3 5).4.2 P <.1 N = 1,795 Risk group Months AGE < 6 vs. 6 No. of factors Patients (%) 5-year (%) 1-year (%) Relative risk HEMOGLOBIN 12g/dL vs. < 12g/dL Intermediate vs. > ULN 1 SERUM LDH36LEVEL ULN91 2 ANN ARBOR37STAGE I II vs. 78III IV Poor 3 Good NUMBER OF NODAL SITES INVOLVED 4 vs. >
42 IMPROVEMENT OF SURVIVAL IN FOLLICULAR LYMPHOMA PATIENTS Swenson et coll. JCO 25

43 LOW GRADE LYMPHOME - Treatment Options? Wait and watch RIC Allograft Radiotherapy Radio immuntherapy Relapse Autograft Monochemotherapy? New drugs Polychemotherapy CT CT +/- Monoclonal Antibodies CT + IFN CT + RT Immunomodulator agents Vaccines
44 LYMPHOMA : HISTOLOGIC TYPES (adapted from the Non-Hogkin s classification project, 1997) Indolent lymphoma (low risk) Small lymphocytic (CLL) Lymphoplasmocytoid Marginal zone B-cell, MALT Marginal zone B-cell, nodal Follicular all grades Aggressive lymphoma (intermediate risk) Mantle cell Diffuse large B-cell Primary mediastinal large B-cell 6. % 3.6 % 2.4 % Peripheral T-cell, all types Anaplastic large T / null cell Very aggressive lymphomas (high risk) Burkitt s High grade B-cell, Burkitt like Precursor T-lymphoblastic % % % % % 7. % 2.4 % < 1 % 2.1 % 1.7 %
45 LYMPHOMES FOLLICULAIRES EN RECHUTE RÉPONDEURS AU TRAITMENT DE SAUVETAGE CHOP: RITUXIMAB D ENTRETIEN VERSUS OBSERVATION: SURVIE SANS PROGRESSION 1 Median PFS: Maintenance = 38 months Observation = 15 months P <.1 Percentage 8 6 Maintenance 4 2 O Observation P <.1 N Number of patients at risk: Years 5 Observation Rituximab maintenance Van Oers MHJ, et al. (Blood. 26;18:3295-
46 Rituximab en traitement d entretien (1/3) EORTC 2981 : Survie Sans Progression 1 Réduction de 45 % du risque de rechute à 6 ans Entretien Rituximab 6 Hazard ratio:, ms 1 44 ms Observation p<,1 (années) O O N N Nombre Nombrede depatients patients à risque à risque : : Observation Observation Rituximab Rituximab Van Oers / Etude EORTC 2981: Blood 26; Van Oers / Etude EORTC 2981: ASH 28
47 Rituximab en traitement d entretien (2/3) EORTC 2981 : Survie Sans Progression Analyse par sous-groupes : traitement d induction 1 CHOP induction Hazard ratio:.37 5 R-CHOP induction 1 médiane: 52,7 ms Médiane : 36,8 ms 2 2 p<,1 Hazard ratio =,37 1 O N Médiane : 11,6 ms Nombre de patients à risque : (années) 8 Observation Rituximab A 6 ans : réduction de 63 % du risque de rechute 1 O N p=,43 Hazard ratio =,69 Médiane : 23, ms Nombre de patients à risque (années) Observation Rituximab A 6 ans : réduction de 31 % du risque de rechute Van Oers / Etude EORTC 2981: Blood 26; Van Oers / Etude EORTC 2981: ASH 28
48 Rituximab en traitement d entretien (3/3) EORTC 2981 : Survie sans progression depuis la 2ème randomisation Analyse par sous-groupes : réponse à l induction 1 RC après induction 9 RP après induction Médiane : 52,7 ms Médiane : 41,8 ms Médiane : 14,4 ms p=,3 (années) O N Nombre de patients à risque : Observation Rituximab A 6 ans : + 38 mois de SSP et réduction de 64% du risque de rechute p=,6 O N Médiane : 15,6 ms Nombre de patients à risque : (years) Observation Rituximab A 6 ans : + 26 mois de SSP et réduction de 54 % du risque de rechute Van Oers / Etude EORTC 2981: Blood 26; Van Oers / Etude EORTC 2981: ASH 28
49 Event-free survival after relapse/pd
50 Rituximab treated No maintenance
 then every 2 months in arm A α-ifn 2b, 4.5 MU tiw for 18 months (3MU if aged 7 yr) Rituximab: 375 mg/m2 Salles G, et al.")
51 FL2 study design Arm A 6 months R 12 months Staging including CT-scan and bone marrow biopsy Arm B D1 Cyclophosphamide 6 mg/m2 D1 Doxorubicin 25 mg/m2 D1 Etoposide 1 mg/m2 D1-D5 Prednisone 4 mg/m2 every month for 6 months (arm A & B) then every 2 months in arm A α-ifn 2b, 4.5 MU tiw for 18 months (3MU if aged 7 yr) Rituximab: 375 mg/m2 Salles G, et al. Blood 24; 14:Abstract 16.
52 FL 2: Outcome of patients calculated from the time of first progression (n=175). Event free survival; the 3 and 5 year EFS rates are 5% (95%IC; 42-58%) and 26% (95%IC; 14-39%), respectively Overall survival; the 3 and 5 year OS rates are 72% (95%IC;64-78%) and 52% (95%IC; 36-66%). transplantation in follicular lymphoma Steven Le Gouill et al Haematologica 211,
53 FL 2: Patients outcome according to frontline therapy and use of transplantation at first progression: ---- transplanted patients and non-transplanted patients 3a: Event free survival for patients who fail CHVP-I (P=.2). 3b: Overall survival for patients who fail CHVP-I (P=.5) transplantation in follicular lymphoma Steven Le Gouill et al Haematologica 211,
54 4. Patient outcome according to the period of progression and use of transplantation at first progression (---- transplanted patients and non-transplanted patients). 4a: Event free survival of primary refractory patients (P=.2). 4b: Event free survival of patients who progressed or relapsed after completion of their first-line treatment: (P=.11). transplantation in follicular lymphoma Steven Le Gouill et al Haematologica 211,
55
56
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes
 Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
Open questions in the treatment of Follicular Lymphoma. Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland
 Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
The case against maintenance rituximab in Follicular lymphoma. Jonathan W. Friedberg M.D., M.M.Sc.
 The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES
 How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting?
 Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
The case for maintenance rituximab in FL
 New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
TRANSPARENCY COMMITTEE OPINION. 8 November 2006
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 8 November 2006 MABTHERA 100 mg, concentrate for solution for infusion (CIP 560 600-3) Pack of 2 MABTHERA 500 mg,
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 8 November 2006 MABTHERA 100 mg, concentrate for solution for infusion (CIP 560 600-3) Pack of 2 MABTHERA 500 mg,
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 18 July 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2012 MABTHERA 100 mg, concentrate for solution for infusion B/2 (CIP code: 560 600-3) MABTHERA 500 mg, concentrate
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2012 MABTHERA 100 mg, concentrate for solution for infusion B/2 (CIP code: 560 600-3) MABTHERA 500 mg, concentrate
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma
 12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
Autologous SCT in FL No!
 COSTEM 2011 Controversies in Stem Cell Transplantation and Cellular Therapies Berlin, September 10 th, 2011 Autologous SCT in FL No! Ulrich Dührsen Department of Hematology Follicular lymphoma Positioning
COSTEM 2011 Controversies in Stem Cell Transplantation and Cellular Therapies Berlin, September 10 th, 2011 Autologous SCT in FL No! Ulrich Dührsen Department of Hematology Follicular lymphoma Positioning
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
Targeted Radioimmunotherapy for Lymphoma
 Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Rituximab in the Treatment of NHL:
 New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
Follicular Lymphoma. Michele Ghielmini. Oncology Institute of Southern Switzerland Bellinzona
 Follicular Lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona Conflicts of interest Astra Zeneca Roche Cellgene Mundipharma Janssen Gilead Bayer Abbvie FL remains an incurable
Follicular Lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona Conflicts of interest Astra Zeneca Roche Cellgene Mundipharma Janssen Gilead Bayer Abbvie FL remains an incurable
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients
 Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center
 What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
eastern cooperative oncology group Michael Williams, Fangxin Hong, Brad Kahl, Randy Gascoyne, Lynne Wagner, John Krauss, Sandra Horning
 Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
How I treat High-risk follicular lymphoma
 How I treat High-risk follicular lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona 1) median OS raised from 10 to 18 y 2) advanced FL remains uncurable Stanford, n = 1334
How I treat High-risk follicular lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona 1) median OS raised from 10 to 18 y 2) advanced FL remains uncurable Stanford, n = 1334
MANTLE CELL LYMPHOMA
 MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
SEQUENCING FOLLICULAR LYMPHOMA
 SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
Brad S Kahl, MD. Tracks 1-21
 I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
The treatment of DLBCL. Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona
 The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
Challenges in the Treatment of Follicular Lymphoma
 Challenges in the Treatment of Follicular Lymphoma Prof. Michele Ghielmini Clinical Director Oncology Institute of Southern Switzerland Bellinzona ESMO guidelines 2014 (simplified) Low tumor burden High
Challenges in the Treatment of Follicular Lymphoma Prof. Michele Ghielmini Clinical Director Oncology Institute of Southern Switzerland Bellinzona ESMO guidelines 2014 (simplified) Low tumor burden High
Mathias J Rummel, MD, PhD
 I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
The role of stem cell transplant for lymphoma in 2017
 DOI: 10.1002/hon.2396 SUPPLEMENT ARTICLE The role of stem cell transplant for in 2017 John G. Gribben Barts Cancer Institute, Queen Mary University of London, London, UK Correspondence John G. Gribben,
DOI: 10.1002/hon.2396 SUPPLEMENT ARTICLE The role of stem cell transplant for in 2017 John G. Gribben Barts Cancer Institute, Queen Mary University of London, London, UK Correspondence John G. Gribben,
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma
 How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
Front-line treatment in young. Role of maintenance therapy. Rome 2017 Prof Le Gouill S.
 Front-line treatment in young patients with MCL: Role of maintenance therapy Rome 2017 Prof Le Gouill S. Is there a need for maintenance for young MCL patients? Is there a need for maintenance for young
Front-line treatment in young patients with MCL: Role of maintenance therapy Rome 2017 Prof Le Gouill S. Is there a need for maintenance for young MCL patients? Is there a need for maintenance for young
Outcomes of Treatment in Slovene Follicular Lymphoma Patients
 Original Study Outcomes of Treatment in Slovene Follicular Lymphoma Patients Tanja Juznic Setina, Simona Borstnar, Barbara Jezersek Novakovic Abstract The treatment outcomes of follicular lymphoma (FL)
Original Study Outcomes of Treatment in Slovene Follicular Lymphoma Patients Tanja Juznic Setina, Simona Borstnar, Barbara Jezersek Novakovic Abstract The treatment outcomes of follicular lymphoma (FL)
AHSCT in Hodgkin lymphoma - indication and challenges. Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital
 AHSCT in Hodgkin lymphoma - indication and challenges Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital AHSCT in Hodgkin Lymphoma The role of AHSCT in HL Mobilisation failure
AHSCT in Hodgkin lymphoma - indication and challenges Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital AHSCT in Hodgkin Lymphoma The role of AHSCT in HL Mobilisation failure
Follicular Lymphoma 2016:
 Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
Advances in molecular biology diagnostic and treatment of B-cell malignancies: indolent B-cell lymphoma
 Annals of Oncology 16 (Supplement 2): ii99 ii104, 2005 doi:10.1093/annonc/mdi724 Advances in molecular biology diagnostic and treatment of B-cell malignancies: indolent B-cell lymphoma M. Dreyling, C.
Annals of Oncology 16 (Supplement 2): ii99 ii104, 2005 doi:10.1093/annonc/mdi724 Advances in molecular biology diagnostic and treatment of B-cell malignancies: indolent B-cell lymphoma M. Dreyling, C.
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Radiotherapy in DLCL is often worthwhile. Dr. Joachim Yahalom Memorial Sloan-Kettering, New York
 Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Aggressive lymphomas ASH Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV
 Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
What are the hurdles to using cell of origin in classification to treat DLBCL?
 What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
Lymphoma- Med A-new drugs and treatments
 Lymphoma- Med A-new drugs and treatments Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Disclosures: Roche, Gilead Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Outline Lymphoma- what is
Lymphoma- Med A-new drugs and treatments Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Disclosures: Roche, Gilead Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Outline Lymphoma- what is
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas. Original Policy Date
 MP 7.03.13 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
MP 7.03.13 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013
Patterns of Care in Medical Oncology. Follicular Lymphoma
 Patterns of Care in Medical Oncology Follicular Lymphoma CASE 1: A 72-year-old man with multiple comorbidities including COPD/asthma presents with slowly progressive cervical adenopathy. Bone marrow biopsy
Patterns of Care in Medical Oncology Follicular Lymphoma CASE 1: A 72-year-old man with multiple comorbidities including COPD/asthma presents with slowly progressive cervical adenopathy. Bone marrow biopsy
Mantle Cell Lymphoma: Update in Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency
 Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège. 14 th post-ash meeting, January 6 th 2011, Brussels
 Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University
 Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Non-Hodgkin Lymphoma in Clinically Difficult Situations
 Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Managing patients with relapsed follicular lymphoma. Case
 Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Radiotherapy in aggressive lymphomas. Umberto Ricardi
 Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Mantle cell lymphoma An update on management
 Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes on the next page
 COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
The role of rituximab for maintenance therapy in
 COUNTERPOINTS Current Controversies in Hematology and Oncology Counterpoints Is Maintenance Therapy Necessary in Low-Grade Lymphoma? Maintenance therapy with rituximab has been shown to prolong progression-free
COUNTERPOINTS Current Controversies in Hematology and Oncology Counterpoints Is Maintenance Therapy Necessary in Low-Grade Lymphoma? Maintenance therapy with rituximab has been shown to prolong progression-free
Hematopoietic Cell Transplantation for Non-Hodgkin's Lymphomas
 Medical Policy Manual Transplant, Policy No. 45.23 Hematopoietic Cell Transplantation for Non-Hodgkin's Lymphomas Next Review: September 2018 Last Review: December 2017 Effective: January 1, 2018 IMPORTANT
Medical Policy Manual Transplant, Policy No. 45.23 Hematopoietic Cell Transplantation for Non-Hodgkin's Lymphomas Next Review: September 2018 Last Review: December 2017 Effective: January 1, 2018 IMPORTANT
Lymphocyte Predominant Hodgkin s Lymphoma. Case Presentation. How would you treat the patient?
 Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma
 UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
Rituximab and Combination Chemotherapy in Treating Patients With Non- Hodgkin's Lymphoma
 Page 1 of 5 Home Search Study Topics Glossary Search Full Text View Tabular View No Study Results Posted Related Studies Rituximab and Combination Chemotherapy in Treating Patients With Non- Hodgkin's
Page 1 of 5 Home Search Study Topics Glossary Search Full Text View Tabular View No Study Results Posted Related Studies Rituximab and Combination Chemotherapy in Treating Patients With Non- Hodgkin's
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
clinical practice guidelines
 Annals of Oncology 22 (Supplement 6): vi59 vi63, 2011 doi:10.1093/annonc/mdr388 Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
Annals of Oncology 22 (Supplement 6): vi59 vi63, 2011 doi:10.1093/annonc/mdr388 Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
Indolent Lymphomas: Current. Dr. Laurie Sehn
 Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Jonathan W Friedberg, MD, MMSc
 I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand
 Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
How to Refine Treatment Choice in Follicular Lymphoma: From Low-Tumor Burden to High-Risk Follicular Lymphoma
 How to Refine Treatment Choice in Follicular Lymphoma: From Low-Tumor Burden to High-Risk Follicular Lymphoma Peter A. Riedell, MD and Brad S. Kahl, MD Abstract Follicular lymphoma (FL) is the most common
How to Refine Treatment Choice in Follicular Lymphoma: From Low-Tumor Burden to High-Risk Follicular Lymphoma Peter A. Riedell, MD and Brad S. Kahl, MD Abstract Follicular lymphoma (FL) is the most common
BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA
 BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA General Non-Hodgkin s lymphomas (NHLs) encompass several unique malignant lymphoid disease entities that vary in clinical behavior, morphologic appearance,
BACKGROUND INFORMATION ON NON-HODGKIN S LYMPHOMA General Non-Hodgkin s lymphomas (NHLs) encompass several unique malignant lymphoid disease entities that vary in clinical behavior, morphologic appearance,
Lymphomas in Prof Paul Ruff Division of Medical Oncology
 Lymphomas in 2010 Prof Paul Ruff Division of Medical Oncology Most Common Lymphomas: ~90% B-cell and ~10% T-cell T lymphoblastic: 2% Marginal zone, nodal: 2% Other: 9% Burkitt: 2% Anaplastic large cell:
Lymphomas in 2010 Prof Paul Ruff Division of Medical Oncology Most Common Lymphomas: ~90% B-cell and ~10% T-cell T lymphoblastic: 2% Marginal zone, nodal: 2% Other: 9% Burkitt: 2% Anaplastic large cell:
Lymphoma 101. Nathalie Johnson, MDPhD. Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University
 Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Advances in the management of follicular lymphoma
 Hematology Meeting Reports 2007; 1(5):43 51 Advances in the management of follicular lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland, Oncologia medica, Bellinzona, Switzerland Corresponding
Hematology Meeting Reports 2007; 1(5):43 51 Advances in the management of follicular lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland, Oncologia medica, Bellinzona, Switzerland Corresponding
Medical Policy Manual. Date of Origin: May Topic: Hematopoietic Stem-Cell Transplantation for Non- Hodgkin Lymphomas
 Medical Policy Manual Topic: Hematopoietic Stem-Cell Transplantation for Non- Hodgkin Lymphomas Section: Transplant Policy No: 45.23 Date of Origin: May 2010 Last Reviewed Date: September 2013 Effective
Medical Policy Manual Topic: Hematopoietic Stem-Cell Transplantation for Non- Hodgkin Lymphomas Section: Transplant Policy No: 45.23 Date of Origin: May 2010 Last Reviewed Date: September 2013 Effective
EBMT2008_22_44:EBMT :29 Pagina 454 CHAPTER 30. HSCT for Hodgkin s lymphoma in adults. A. Sureda
 EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 454 * CHAPTER 30 HSCT for Hodgkin s lymphoma in adults A. Sureda EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 455 CHAPTER 30 HL in adults 1. Introduction
EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 454 * CHAPTER 30 HSCT for Hodgkin s lymphoma in adults A. Sureda EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 455 CHAPTER 30 HL in adults 1. Introduction
MANAGEMENT OF LYMPHOMAS
 MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin s Lymphomas
 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin s Lymphomas Policy Number: 8.01.20 Last Review: 7/2014 Origination: 7/2002 Next Review: 7/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin s Lymphomas Policy Number: 8.01.20 Last Review: 7/2014 Origination: 7/2002 Next Review: 7/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue
Blood Cancers. Blood Cells. Blood Cancers: Progress and Promise. Bone Marrow and Blood. Lymph Nodes and Spleen
 Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
GLSG/OSHO Study Group. Supported by Deutsche Krebshilfe
 GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
FOLLICULAR LYMPHOMA. BHS course: indolent lymphoma 7 th february Ann Janssens MD, PhD Hematology UZ Leuven
 FOLLICULAR LYMPHOMA BHS course: indolent lymphoma 7 th february 2015 Ann Janssens MD, PhD Hematology UZ Leuven Non Hodgkin Lymphoma Epidemiology US 1998-2011 Marginal Zone MALT 8 % Follicular 22 % 20%
FOLLICULAR LYMPHOMA BHS course: indolent lymphoma 7 th february 2015 Ann Janssens MD, PhD Hematology UZ Leuven Non Hodgkin Lymphoma Epidemiology US 1998-2011 Marginal Zone MALT 8 % Follicular 22 % 20%
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Rituximab in lymphoma: A systematic review and consensus practice guideline from Cancer Care Ontario
 Cancer Treatment Reviews (2007) 33, 161 176 available at www.sciencedirect.com journal homepage: www.elsevierhealth.com/journals/ctrv ANTI-TUMOUR TREATMENT Rituximab in lymphoma: A systematic review and
Cancer Treatment Reviews (2007) 33, 161 176 available at www.sciencedirect.com journal homepage: www.elsevierhealth.com/journals/ctrv ANTI-TUMOUR TREATMENT Rituximab in lymphoma: A systematic review and
Clinical Policy Bulletin: Hematopoietic Cell Transplantation for Non- Hodgkin's Lymphoma
 : Go Clinical Policy Bulletin: Hematopoietic Cell Transplantation for Non- Hodgkin's Lymphoma Number: 0494 Policy *Please see amendment forpennsylvaniamedicaid at theend of thiscpb. I. Autologous Hematopoietic
: Go Clinical Policy Bulletin: Hematopoietic Cell Transplantation for Non- Hodgkin's Lymphoma Number: 0494 Policy *Please see amendment forpennsylvaniamedicaid at theend of thiscpb. I. Autologous Hematopoietic
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas
 Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Policy Number: Original Effective Date: MM.07.018 04/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO 03/27/2015 Section:
Hematopoietic Stem-Cell Transplantation for Non-Hodgkin Lymphomas Policy Number: Original Effective Date: MM.07.018 04/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO 03/27/2015 Section:
Confronto Real world e studi registrativi
 Confronto Real world e studi registrativi V. Pavone San Giovanni Rotondo 8 Novembre 2018 U.O Ematologia Az.Osp.Card.G.Panico MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY
Confronto Real world e studi registrativi V. Pavone San Giovanni Rotondo 8 Novembre 2018 U.O Ematologia Az.Osp.Card.G.Panico MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY
Update: New Treatment Modalities
 ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL):
:") Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Traitement des lymphomes diffus à grandes cellules B
 Traitement des lymphomes diffus à grandes cellules B Corinne HAIOUN Unité Hémopathies Lymphoïdes- CHU Henri Mondor Université Paris Est Créteil DES Hématologie Février 2012 On February 10th, the merging
Traitement des lymphomes diffus à grandes cellules B Corinne HAIOUN Unité Hémopathies Lymphoïdes- CHU Henri Mondor Université Paris Est Créteil DES Hématologie Février 2012 On February 10th, the merging
Treatment Nodal Marginal Zone Lymphoma
 Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Diffuse Large B-Cell Lymphoma (DLBCL)
") Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009
 Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Autologous Stem Cell Transplanation as First line Treatment? (Against) Joan Bladé Berlin, September 9 th, 2011
 Joan Bladé Berlin, September 9 th, 2011") Autologous Stem Cell Transplanation as First line Treatment? (Against) Joan Bladé Berlin, September 9 th, 2011 Significant impact of ASCT before the availability of novel agents? Randomized trials: Single
Autologous Stem Cell Transplanation as First line Treatment? (Against) Joan Bladé Berlin, September 9 th, 2011 Significant impact of ASCT before the availability of novel agents? Randomized trials: Single
Disclosures WOJCIECH JURCZAK
 Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA
Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA
Place de la radiothérapie dans les CBPC métastatiques
 Place de la radiothérapie dans les CBPC métastatiques Cecile Le Péchoux, 12 ème Biennale Monégasque de Cancérologie, 2016 IOT Institut d Oncologie Thoracique CBPC metastatique Rapid doubling time, early
Place de la radiothérapie dans les CBPC métastatiques Cecile Le Péchoux, 12 ème Biennale Monégasque de Cancérologie, 2016 IOT Institut d Oncologie Thoracique CBPC metastatique Rapid doubling time, early
Solomon Graf, MD February 22, 2013
 Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
Allogeneic Transplantation for Follicular Lymphoma: Does One Size Fit All?
 Clinical Review Allogeneic Transplantation for Follicular Lymphoma: Does One Size Fit All? Mehdi Hamadani and Mary M. Horowitz Medical College of Wisconsin; and Center for International Blood and Marrow
Clinical Review Allogeneic Transplantation for Follicular Lymphoma: Does One Size Fit All? Mehdi Hamadani and Mary M. Horowitz Medical College of Wisconsin; and Center for International Blood and Marrow
THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982)
") EORTC Lymphoma Group THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982) J. Thomas, C. Fermé, E.M. Noordijk, H. Eghbali and M. Henry-Amar 7th International
EORTC Lymphoma Group THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982) J. Thomas, C. Fermé, E.M. Noordijk, H. Eghbali and M. Henry-Amar 7th International
CPAG Summary Report for Clinical Panel Policy 1630 Bendamustine-based chemotherapy for first-line treatment of Mantle cell lymphoma (MCL) in adults
 in adults") MANAGEMENT IN CONFIDENCE CPAG Summary Report for Clinical Panel Policy 1630 Bendamustine-based chemotherapy for first-line treatment of Mantle cell lymphoma (MCL) in adults The Benefits of the Proposition
MANAGEMENT IN CONFIDENCE CPAG Summary Report for Clinical Panel Policy 1630 Bendamustine-based chemotherapy for first-line treatment of Mantle cell lymphoma (MCL) in adults The Benefits of the Proposition
Overview. Table of Contents. A Canadian perspective provided by Isabelle Bence-Bruckler, MD, FRCPC
 2 A C A N A D I A N P E R S P E C T I V E Volume 2 November 2005 Overview The International Conference on Malignant Lymphoma (ICML) is held every three years in Lugano, Switzerland. ICML started nearly
2 A C A N A D I A N P E R S P E C T I V E Volume 2 November 2005 Overview The International Conference on Malignant Lymphoma (ICML) is held every three years in Lugano, Switzerland. ICML started nearly