Renal and pulmonary Aspects of Birt-Hogg-Dubé syndrome
|
|
|
- Amberlynn Cox
- 5 years ago
- Views:
Transcription
1 Renal and pulmonary Aspects of Birt-Hogg-Dubé syndrome Paul Christiaan Johannesma
2 Renal and Pulmonary Aspects of Birt-Hogg-Dubé syndrome. Paul Christiaan Johannesma Thesis, Faculty of Medicine, VU University medical center, VU University, The Netherlands Proefschrift, faculteit der Geneeskunde, VU medisch centrum, Vrije Universiteit, Nederland isbn: Author: Paul Christiaan Johannesma Cover illustration: Arno Rozema Layout and printing: Off Page, Amsterdam Copyright P. C. Johannesma, Amsterdam, The Netherlands, 2016 All rights reserved. No parts of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, without written permission from the author or from the Publisher holding the comy right of the published articles. Publication of this thesis was financially supported by: Vrije Universiteit, afdeling Heelkunde Jeroen Bosch Ziekenhuis, ABN AMRO N.V., Jeroen Bosch Academie, Rijnstate Vriendenfonds, CARE10 HealthCare Products & Services, Myrovlytis Trust. The sponsors who are gratefully acknowledged, had no involvement in any stage of the study design, data collection, data-analysis, interpretation of the data or the decision to publish study results. The research presented in this thesis is part of the research program of the VUmc Cancer Center Amsterdam (VUmc- CCA). The studies were performed at the Department of Pulmonary Diseases and the Department of Urology of the VU University medical center, Amsterdam, The Netherlands.
3 VRIJE UNIVERSITEIT Renal and Pulmonary Aspects of Birt-Hogg-Dubé syndrome ACADEMISCH PROEFSCHRIFT ter verkrijging van de graad Doctor aan de Vrije Universiteit Amsterdam, op gezag van de rector magnificus prof.dr. V. Subramaniam, in het openbaar te verdedigen ten overstaan van de promotiecommissie van de Faculteit der Geneeskunde op vrijdag 30 september 2016 om 9.45 uur in de aula van de universiteit, De Boelelaan 1105 door Paul Christiaan Johannesma geboren te Amstelveen
4 promotoren: copromotoren: prof.dr. P.E. Postmus prof.dr. R.J.A. van Moorselaar dr. F.H. Menko dr. J.H.T.M. van Waesberghe
5 Voor mijn ouders
6 Table of Contents General introduction Chapter 1 Birt-Hogg-Dubé syndrome: a molecular and clinical overview. 15 Outline of the thesis 23 Part I Chapter 1.1 Chapter 1.2 Chapter 1.3 Chapter 1.4 Chapter 1.5 Pulmonary manifestations The pathogenesis of pneumothorax in Birt-Hogg-Dubé syndrome: a hypothesis. 33 Johannesma PC, Houweling AC, van Waesberghe JH, van Moorselaar RJ, Starink TM, Menko FH, Postmus PE. Respirology Nov;19(8): Presence of pulmonary cysts in BHD patients with and without a pneumothorax; a retrospective analysis of 61 patients. 41 Johannesma PC, van Waesberghe JHTM, Menko FH, van Moorselaar RJA, Paul MA, Starink ThM, Reinhard R, Houweling AC, van de Beek I, Jonker MA, Postmus PE. (Submitted). Radiological features of primary spontaneous pneumothorax patients with or without a mutation in FLCN. 51 Johannesma PC, van Waesberghe JHTM, Menko FH, van Moorselaar RJA, Paul MA, Starink ThM, Reinhard R, Houweling AC, van de Beek I, Jonker MA, Postmus PE. (Submitted). How reliable are clinical criteria in distinguishing between Birt-Hogg-Dubé syndrome and smoking as a cause for pneumothorax? 59 Johannesma PC, Thunnissen E, Postmus PE. Histopathology Jun;64(7): Risk of spontaneous pneumothorax due to air travel and diving in patients with Birt-Hogg-Dubé syndrome. 63 Johannesma PC, van der Wel JWT, Paul MA, Houweling AC, Jonker MA, van Waesberghe JHTM, Reinhard R, Starink ThM, van Moorselaar RJA, Menko FH, Postmus PE. SpringerLink 2016 (Accepted for publication)
7 Chapter 1.6 Chapter 1.7 Prevalence of Birt-Hogg-Dubé syndrome in patients with apparently primary spontaneous pneumothorax. 75 Johannesma PC, Reinhard R, Kon Y, Sriram JD, Smit HJ, van Moorselaar RJ, Menko FH, Postmus PE; on behalf of the Amsterdam BHD working group. Eur Respir J Apr;45(4): International guidelines for pneumothorax are not adequate for treatment of spontaneous pneumothorax in patients with Birt-Hogg-Dubé syndrome. 91 Johannesma PC, Paul MA, van Waesberghe JHTM, Jonker MA, Houweling AC, van de Beek I, van Moorselaar RJA, Menko FH, Postmus PE. (Submitted) Part ii Chapter 2.1 Chapter 2.2 Chapter 2.3 Renal manifestations Renal cancer and pneumothorax risk in Birt-Hogg-Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. 101 Houweling AC, Gijezen LM, Jonker MA, van Doorn MB, Oldenburg RA, van Spaendonck-Zwarts KY, Leter EM, van Os TA, van Grieken NC, Jaspars EH, de Jong MM, Bongers EM, Johannesma PC, Postmus PE, van Moorselaar RJ, van Waesberghe JH, Starink TM, van Steensel MA, Gille JJ, Menko FH. Br J Cancer Dec 6;105(12): Are lung cysts in renal cell cancer (RCC) patients an indication for FLCN mutation analysis? 119 Johannesma PC, Houweling AC, Menko FH, van de Beek I, Reinhard R, Gille JJ, van Waesberghe JHTM, Thunnissen E, Starink TM, Postmus PE, van Moorselaar RJ. Fam Cancer Apr;15(2): Renal imaging in 199 Dutch patients with Birt-Hogg-Dubé syndrome: Screening, compliance and outcome. 127 Johannesma PC, van de Beek I, Reinhard R, Leter EM, Rozendaal L, Starink ThM, Waesberghe JHTM, Horenblas S, Jonker MA, Menko FH, Postmus PE, Houweling AC, van Moorselaar RJA. (Submitted)
8 Part iii Chapter 3.1 Chapter 3.2 Relevant case reports and case series In-flight pneumothorax: diagnosis may be missed because of symptom delay. 141 Postmus PE, Johannesma PC, Menko FH, Paul MA. Am J Respir Crit Care Med Sep 15;190(6): Spontaneous pneumothorax as indicator for Birt-Hogg-Dubé syndrome in paediatric patients. 149 Johannesma PC, van den Borne BE, Gille JJ, Nagelkerke AF, van Waesberghe JT, Paul MA, van Moorselaar RJ, Menko FH, Postmus PE. BMC Pediatr Jul 3;14:171. Chapter 3.3 Lung cysts as indicator for Birt-Hogg-Dubé syndrome. 157 Johannesma PC, Thunnissen E, Postmus PE. Lung Feb;192(1): Chapter 3.4 Spontaneous pneumothorax as the first manifestation of a hereditary condition with an increased renal cancer risk. 161 Johannesma PC, Lammers JW, van Moorselaar RJ, Starink TM, Postmus PE, Menko FH. Ned Tijdschr Geneeskd. 2009;153:A581. Chapter 3.5 Facial fibrofolliculomas as indicator for renal cell cancer. 171 Johannesma PC, Starink TM, Van Moorselaar RJ, Postmus PE. Jpn J Clin Oncol Jun;44(6): Chapter 3.6 Bilateral renal tumour as indicator for Birt-Hogg-Dubé syndrome. 175 Johannesma PC, van Moorselaar RJ, Horenblas S, van der Kolk LE, Thunnissen E, van Waesberghe JH, Menko FH, Postmus PE. Case Rep Med. 2014;2014: Chapter 3.7 A de novo FLCN mutation in a patient with spontaneous pneumothorax and renal cancer; a clinical and molecular evaluation. 183 Menko FH, Johannesma PC, van Moorselaar RJ, Reinhard R, van Waesberghe JH, Thunnissen E, Houweling AC, Leter EM, Waisfisz Q, van Doorn MB, Starink TM, Postmus PE, Coull BJ, van Steensel MA, Gille JJ. Fam Cancer Sep;12(3):373-9.
9 Part iv summary, discussion and future perspectives Chapter 4.1 Summary of the thesis 199 Chapter 4.2 Nederlandse samenvatting (voor leken) 209 Chapter 4.3 Conclusions and future directions 217 Addendum Review committee 228 List of co-authors and affiliations 229 List of abbreviations 232 List of publications 234 List of scientific meetings 239 Grants and Awards 239 Acknowledgements Dankwoord 241 Curriculum Vitae Auctoris 248
10
11 "Een goed begin is het halve werk, maar een goed begin is maar de helft." (Adapted from: De Jeugd van Tegenwoordig, Album De Lachende Derde, Sterrenstof. Release: 5 november 2010)
12
13 general introduction
14
15 chapter 0.1 General introduction and outline of the thesis Paul C. Johannesma 1 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands
16 0.1 General introduction and outline of the thesis General introduction History In 1977, three Canadian physicians, Arthur Birt, Georgina Hogg, and James Dubé described a pedigree in which multiple family members had characteristic skin lesions, consisting of fibrofolliculomas, trichodiscomas and achrocordons (figure 1). 1 At present, Birt-Hogg-Dubé syndrome (BHD) is defined as an autosomal dominant condition, caused by germline mutations in the FLCN (folliculin) gene and clinically characterized by skin fibrofolliculomas, multiple lung cysts, spontaneous pneumothorax, and renal cancer (Online Mendelian Inheritance in Man #135150). Clinical diagnostic criteria proposed by the European BHD Consortium are outlined in figure 2. 2 Genetic and molecular aspects of Birt-Hogg-Dubé syndrome BHD is an autosomal dominant condition with high penetrance and variable expression. In 2001, a BHD-associated locus was mapped to chromosome 17p11.2 by linkage analysis. 3 4 Subsequently, - in 2002 in BHD probands truncating germline mutations were identified in a novel gene, folliculin (FLCN). 5 FLCN contains 14 exons and encodes folliculin, a protein of 579 amino acids that has no major homology to any other human protein. 6 Currently, in BHD kindreds, over 100 unique mutations in all coding regions of the FLCN gene have been reported in the LOVD mutation database ( 7 8 A hypermutable hot spot has been identified in a tract of eight cytosines in exon The majority of mutations are insertions/deletions, nonsense or Figure 1. Pedigree of the family described by Birt et al. (Adapted from Birt AR, et al. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatology 1977;113: ). 16
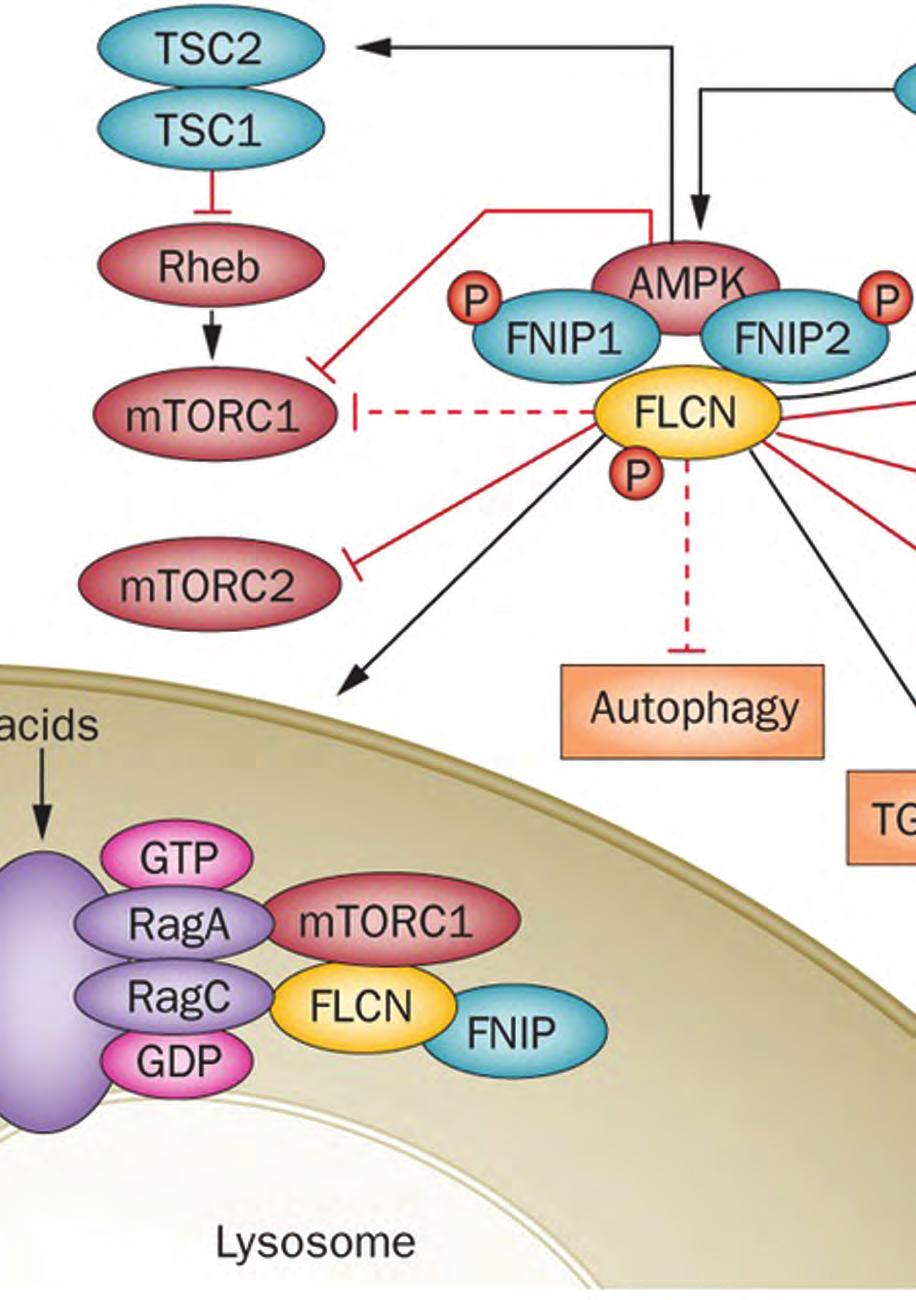
17 Panel: Diagnostic criteria for Birt-Hogg-Dubé syndrome (BHD; patients should fulfill one major or two minor criteria for diagnosis) 0.1 Major criteria At least five fibrofolliculomas or trichodiscomas, at least one histologically confirmed, of adult onset * Pathogenic FLCN germline mutation Minor criteria Multiple lung cysts: bilateral basally located lung cysts with no other apparent cause, with or without primary spontaneous pneumothorax Renal cancer: early onset (<50 years) or multifocal or bilateral renal cancer, or renal cancer of mixed chromophobe and oncocytic histology A frist-degree relative with BHD *Fibrofolliculoma and trichodiscoma are two possible presentations of the same lesion for the differential diagnosis, angiofibroma in tuberous sclerosis should be considered. Childhood- onset familial fibrofolliculoma or trichodiscoma without other syndromic features might be a distinct entity. General introduction and outline of the thesis Figure 2. Diagnostic criteria for BHD proposed by the European BHD Consortium (Adapted from Menko et al. Birt- Hogg-Dubé syndrome: diagnosis and management. Lancet Oncology 2009;10: ). splice-site mutations that result in a shift in the reading frame and/or introduction of a premature termination codon, indicating that loss of FLCN function is responsible for the clinical BHD. 13 However, the precise role of folliculin requires further elucidation. The functions of folliculin remain largely unknown, but are likely to include a tumor-suppressor function (figure 3). 14 The mammalian target of Rapamycine (mtor) signaling pathway has been implicated in the pathogenesis of several hereditary syndromes, including BHD. Several proteins, including FNIP1, FNIP 2, TSC1, TSC2 and AMPK, show an interaction with FLCN and abnormalities in the function of these are involved in genetic disorders showing partial clinical overlap with BHD. 15 Patients from a unique kindred with a germline FNIP1 defect is show facial skin lesions resembling those found in BHD. Patients with tuberous sclerosis complex due to TSC1 or TSC2 mutations have skin, lung and renal lesions, a combination of features which also characterizes BHD. 16 In ongoing studies the role of folliculin in multiple signaling pathways is investigated and these include TGFβ/BMP signaling, PGC-1α-driven mitochondrial biogenesis, TFE3/TFEB transcriptional regulation, cell polarity, Rho A signaling and regulation of the E-cadherin-LKB1-AMPK axis. 15 No clear genotype - phenotype correlations have been reported for BHD. 17 It has been proposed that in BHD patients with a cytosine deletion in the C8 tract in exon 11 of the FLCN gene, renal tumors are less frequent than in those with a cytosine insertion. Differences in frequency of pulmonary cysts, spontaneous pneumothorax, or fibrofolliculomas were not observed in this group. Another study observed a trend towards more pneumothoraces in BHD patients with FLCN mutations in exons 9 and 12 and an association between FLCN mutations in exon 9 and an increased number of pulmonary cysts have also been observed. 17

18 0.1 General introduction and outline of the thesis Figure 3. FLCN-FNIP axis and potential interactions with cellular pathways and processes. FLCN, FNIP and FNIP2 interact with AMPK and modulate mtor signaling. Tumor suppressors are red. FLCN interactors are green. Potential interactions of FLCN/FNIP1/FNIP2 with cellular pathways / processes are in yellow boxes. à indicates activation. - indicates inhibition.? indicates evidence for both inhibition and activation (Adapted from Schmidt LS. Birt-Hogg- Dubé syndrome: from gene discovery to molecularly targeted therapies. Fam Cancer 2013;12:357-64). Dermatological aspects of Birt-Hogg-Dubé syndrome The facial fibrofolliculomas typical for BHD are benign hair follicle tumors, consisting of epithelial strands emanating from the outer root sheath of a deformed hair follicle (figure 4). 21 These lesions usually appear after the age of 20 years, as multiple, dome-shaped, whitish papules in the face, neck and upper part of the back (figure 5). 22 Occasionally they involve the lips, buccal mucosa and gingiva. Fibrofolliculomas closely resemble angiofibromas and indeed, angiofibromas have been reported in BHD. 23 Other benign skin abnormalities possibly associated with BHD are acrochordons (skin tags) and lipomas. 24 Malignant skin lesions, including melanoma, have also been observed in BHD. The diagnosis of BHD associated fibrofolliculomas is based on both clinical presentation and histological examination. Biopsies and sectioning of on several levels show a unique histological pattern, which confirms the clinical diagnosis The penetrance of the skin lesions is age dependent and an estimated 80% of FLCN mutation carriers will develop skin fibrofolliculomas. Expression is quite variable: some patients have multiple facial papules whereas in other cases the lesions are minimal and will only be recognized by expert dermatological examination. 18
:609-10). Figure 5. Clinical facial fibrofolliculomas (Adapted from Menko et al.")

19 0.1 Figure 4. Fibrofolliculomas; hair follicle tumors, consisting of epithelial strands emanating from the outer root sheath of a deformed hair follicle. (Adapted from Johannesma et al. Facial fibrofolliculomas as indicator for renal cell cancer. Jpn J Clin Oncol. 2014;44(6):609-10). Figure 5. Clinical facial fibrofolliculomas (Adapted from Menko et al. Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncology 2009;10: ). General introduction and outline of the thesis For differential diagnosis tuberous sclerosis complex is important since the BHD associated fibrofolliculomas may be mistakenly classified as angiofibromas due to TSC. 2 Treatment of fibrofolliculomas is only needed for cosmetic reasons. Treatment options include hyfrecation (electrocoagulation), followed if necessary by curettage. Alternative possibilities are surgical removal, retinoic acid derivatives and ablative laser techniques (e.g. YAG, CO 2 ). Targeted local therapy by topical Rapamycin (mtor inhibitor) has no obvious effect. Pulmonary aspects of Birt-Hogg-Dubé syndrome Pneumothorax is defined as the presence of air in the pleural cavity. It is a common condition with a high incidence of between 1.2 and 18 cases per persons per year. If not due to an obvious external force (trauma, iatrogenic) the condition is described as spontaneous pneumothorax (SP). SP is subdivided into secondary SP (SSP), due to various forms of lung pathology, and primary SP (PSP) without an obvious underlying lung disease. 31 The first episode of PSP usually occurs in the third decade of life in males, who are often taller than age-matched controls, and the majority has a history of smoking. Smoking increases the risk of PSP more than 100 times. 32 PSP diagnosis is usually based on history and confirmed by a standard erect chest X-ray during inspiration. A chest CT is indicated in complicated cases, for example a recurrent or persistent air leak. In up to 90% of uncomplicated cases cystic structures, usually described as (subpleural) blebs and bullae, are found in the lung apices. In a subgroup of around 5-15% of PSP patients cystic abnormalities are 19
20 0.1 General introduction and outline of the thesis described in the apices and other areas of the lungs, also below the level of the main carina. Possibly in the latter group of patients the aetiology of pneumothorax differs from that in patients with abnormalities restricted to the apices. Overall 11.5% of patients with PSP report a positive family history of the disease. 35 Familial occurrence was described for the first time by Faber et al. 36 In 1991, Albolnik et al. postulated two modes of inheritance for familial primary spontaneous pneumothorax: autosomal dominant with reduced penetrance and X-linked recessive. 37 Hereditary predisposition for spontaneous pneumothorax can occur in specific syndromes including Marfan syndrome, homocystinuria, Ehlers-Danlos syndrome, α 1 -antitrypsin deficiency, tuberous sclerosis complex and Birt-Hogg-Dubé syndrome. The causes of hereditary predisposition for spontaneous pneumothorax are summarized in table Table 1. Causes of hereditary predisposition for spontaneous pneumothorax (adapted from Chiu et al. Familial spontaneous pneumothorax. Current Opin Pulm Med. 2006;12:268-72). Disease Gene(s) Chromosomal location Marfan syndrome Fibrillin 1 15q21.1 Homocystinuria Cystathionine β-synthase 21q22.3 Ehlers-Danlos syndrome Multiple Multiple α 1 -Antitrypsin deficiency α 1 -Antitrypsin 14q32.1 Birt-Hogg-Dubé syndrome Folliculin 17p11.2 SP may be the first and only apparent manifestation of BHD both in isolated and familial cases. In most BHD patients without pneumothorax chest X ray shows normal lung parenchyma but multiple lung cysts are commonly identified on CT, in about 90% of adult patients; approximately 50% of the cysts are located in the subpleural area and 50% in the parenchyma (figure 6A and B). 38 Zbar and colleagues found a 50-times increase in the risk of pneumothorax for BHD-affected individuals. 39 SP has been reported in BHD patients already at the age of 7 and 16 years, but the majority is over 18 years of age Although about 90% of BHD syndrome patients have these multiple cysts, lung function (measured by spirometry and diffusion capacity) is generally normal. 42 Thus, patients with pneumothorax due to BHD, usually have no preceding symptoms of pulmonary disease and are therefore likely to be diagnosed as having PSP. The risk of pneumothorax is about 25% and this risk is probably not due to specific gene defects since clear genotype phenotype correlations have thus far not been demonstrated. While the recurrence rate in common primary SP has been described up to 50% when treated in a conservative way, the recurrence rate of SP among BHD patients has been reported to be much higher, up to 75%, despite even less conservative types of treatment. The exact relationship between the presence of multiple lung cysts and the occurrence of PSP has not been clarified. Most but not all BHD who develop pneumothorax have multiple basal lung cysts The presence of cysts does not per se result in pneumothorax. 20
:1191-4).")
21 0.1 A Figure 6. Thoracic CT scan: lung cysts in basal parts of the lung in BHD patient (Adapted from Johannesma et al. The prevalence of Birt-Hogg-Dubé syndrome among patients with apparently primary spontaneous pneumothorax. Eur Respir J 2015;45(4):1191-4). Due to the variable expressivity of BHD, patients with only spontaneous pneumothorax, and without other clinical manifestations, might in fact have BHD. It is important to diagnose the syndrome in these apparently sporadic cases, since a diagnosis of BHD will lead to measures aimed at the early detection and treatment of renal cancer, not only in the proven carrier but also in possibly affected relatives. Thus far only one Chinese study described a prevalence of 9.8% of BHD in apparently common PSP. 46 Diagnosis of BHD in SP cases strongly depends on the demonstration of multiple lung cysts. However, in uncomplicated SP cases imaging is restricted to X ray and does not include a CT scan. Treatment of spontaneous pneumothorax is based on international guidelines. However, in BHD, the naturally history of pneumothorax may differ from that in sporadic cases and possibly treatment should be different for BHD associated pneumothorax, especially in complicated cases. 49 B General introduction and outline of the thesis Renal aspects of Birt-Hogg-Dubé syndrome Worldwide, renal cell carcinoma (RCC) accounts for about new cancer cases and cancer deaths annually, with a peak prevalence in the 6 th and 7 th decades, and a twofold excess of males to females The frequency of RCC has been increasing partly due to incidental cases detected by abdominal imaging. Epidemiological risk factors associated with RCC include cigarette smoking, obesity and hypertension. 52 Approximately 3% of RCC is due to hereditary predisposition and these hereditary cases include a dozen different syndromes. 53 The most common inherited syndromes associated with RCC are Von Hipple-Lindau disease, hereditary papillary renal cancer, hereditary leiomyomatosis and renal cancer, succinate dehydrogenase subunit mutations, chromosome 3 translocations, and Birt-Hogg-Dubé syndrome (BHD). 54 An overview of inherited disorders predisposing to RCC is given in table Hereditary RCCs differ from the far more common sporadic form in several aspects. Hereditary tumours often present at an early age, are more often multifocal and / or bilateral and may have a characteristic histology. 21
.")
22 0.1 General introduction and outline of the thesis In addition, they may be associated with syndromic features besides renal cell cancer and clearly, family history may be positive for RCC or features of the syndrome involved. 55 In BHD the risk of RCC is estimated to be about 15% with a mean age at diagnosis of 50 years (range years). 2 The most common histological subtype in sporadic RCC is clear cell RCC (ccrcc). 56 In BHD, the most common subtypes are hybrid oncocytic, chromophobe renal cell carcinoma and oncocytoma (figure 7). 20 However, other subtypes including ccrcc may also occur. Given the high degree of inter- and intra-familial variability of these features, it is likely that many cases of BHD associated RCC currently remain unrecognized. The prevalence of BHD in (familial) renal cancer has been investigated by Woodward et al. These authors found in selected patients (3/69) with RCC 4.3% of cases with FLCN mutations. 57 The main clinical consequence of a diagnosis of BHD is early diagnosis and treatment of renal cell cancer and therefore periodic renal imaging is advised for all FLCN mutation carriers Surveillance at regular intervals by MRI, is advised from the age of 20 (figure 8). A disadvantage of MRI is its availability and costs, which may lead to limited access in clinical practice. The role of ultrasound (US) in the early detection of renal tumours is a matter of debate due to limited sensitivity for the detection of small tumours. In general, BHD associated tumours are slowly growing tumours and the risk of distant metastasis is strongly dependent on the size of the tumour. Therefore, surgical treatment is recommended when the largest tumor reaches 3 cm in maximal diameter. 59 This guideline has previously been adopted for Figure 7. Reported histological subtypes of BHD associated renal tumours are hybrid oncocytic, chromophobe renal cell carcinoma and oncocytoma (Adapted from Houweling AC et al. Renal cancer and pneumothorax risk in Birt-Hogg- Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer Dec 6;105(12):1912-9). 22
23 0.1 Figure 8. Renal cell cancer on initial MRI (Johannesma et al. Prevalence of Birt-Hogg-Dubé syndrome in patients with apparently primary spontaneous pneumothorax. Eur Respir J Apr;45(4):1191-4). Von Hippel-Lindau disease and is now also recommended for BHD Local treatment should be nephron sparing due to the high risk of metachronic new primary tumours. Partial nephrectomy, and minimally invasive nephron sparing techniques such as cryoablation and radio frequency ablation (RFA) are options for local treatment. Since BHD patients are at lifelong risk for the development of new tumors, and cryoablation or RFA may complicate both long term evaluation and surgical management, nephron-sparing surgery thus far is the safest and most effective treatment for BHD associated RCC. General introduction and outline of the thesis Other clinical findings in Birt-Hogg-Dubé syndrome In BHD, many other clinical features besides fibrofolliculomas, pneumothorax and renal cell cancer have been observed, mainly in single case reports and small case series. Benign tumours with BHD include multinodular goitre, parotid gland adenoma, colorectal polyp and adenoma, neuraltissue tumour, trichoblastoma, connective tissue nevus, focal-cutaneous mucinosis, lipoma, angiolipoma and cutaneous leiomyoma. Malignant tumours include breast cancer, colorectal cancer, sarcoma of the leg, tonsillar cancer, lung cancer, melanoma, basal and squamous-cell skin cancer, dermatofibrosarcoma protuberans, cutaneous leiomyosarcoma and rhabdomyosarcoma. Although in 1975 Hornstein and Knickenberg described a relationship between fibrofolliculomas and colorectal polyps, this relationship remains uncertain. Also the suggested relationship between parotid oncocytomas and BHD remains unclear. Outline of the thesis The prevalence of BHD is unknown and the syndrome is likely unrecognized by doctors and patients as the skin signs are often mild and the pulmonary and renal symptoms of BHD are hard to distinguish from apparently common SP and sporadic RCC. Although over the last decade insight into the clinical manifestations of BHD has expanded, most knowledge is based on case reports and 23
24 0.1 General introduction and outline of the thesis small case series and not on large clinical datasets. Recognition of this syndrome is important to optimize the effectiveness of surveillance and treatment. The VU University Medical Center (VUmc) in Amsterdam, the Netherlands, is recognized as a NFU (Dutch Federation of University Medical Centers) expert center for BHD providing the unique opportunity of evaluating a large cohort of BHD families referred to the VUmc and its affiliated hospitals. We designed several clinical studies aimed at the pulmonary and renal manifestations of BHD. The thesis in subdivided into three parts. Part one: pulmonary manifestations, Part two: renal manifestations and Part three: relevant case reports. In chapter 1.1 we evaluated the association between BHD associated lung cysts and the development of spontaneous pneumothorax (SP). In chapter 1.2 we studied the role of chest computed tomography (CT) in diagnosis and management of BHD associated pneumothorax. We compared the radiological results of BHD patients with and without a history of (recurrent) SP, to evaluate a possible relationship between lung cysts in the development of SP. In chapter 1.3 we hypothesize that CT scanning in PSP patients could be a sensitive tool in diagnosing BHD in PSP patients. This would be highly clinically relevant since BHD is associated with an increased risk of renal cancer. Therefore we evaluated the findings of chest CT in a group of PSP patients without a detectable FLCN mutation and compared these to a group with a proven mutation in FLCN. In chapter 1.4 we discuss the reliability of clinical criteria in distinguishing between BHD and smoking as a cause for pneumothorax. In literature an increased prevalence of SP associated with air travel in patients with the interstitial cystic lung disease lymphangioleiomyomatosis (LAM) has been described. Based on these results we hypothesize in chapter 1.5 that BHD patients are also more prone to develop a SP during air travel or diving. This might have possible implications for clinical management for pulmonologists and lung surgeons. In chapter 1.6 we address the important clinical question whether all patients who present with primary spontaneous pneumothorax (PSP) should be evaluated for BHD. We reviewed the available thoracic CT scans in apparently PSP patients for the presence of basal cysts. In addition we perform FLCN mutation analysis in a randomly selected group of PSP patients. The recurrence rate of SP in BHD patients has been reported to be up to 75% despite different types of treatment. Therefore we evaluated the recurrence rate and different treatment options of SP in BHD patients comparted to SP patients without a pathogenic FLCN mutation in chapter 1.7. Part two: renal manifestations focuses on the renal manifestations of BHD. In chapter 2.1 we hypothesize that cysts under the main carina in patients diagnosed with sporadic RCC might be an important diagnostic clue in unmasking BHD. Therefore, we test in a pilot study a cohort of patients with formerly diagnosed RCC from the VU University Medical Center (VUmc) and the Netherlands Cancer Center (NKI-AvL). In literature renal MRI is recommended for renal surveillance in BHD patients from the age of 20. Unfortunately this suggestion is mainly based on expert opinion only and other genetic renal diseases. In chapter 2.2 we retrospectively evaluate the compliance to, and the outcomes of renal cancer surveillance in patients diagnosed with BHD in two Dutch centers (VUmc and NKI-AvL). Part three: relevant case reports contains several case reports and small case series. In chapter 3.1 we evaluate a case of missed diagnosis of pneumothorax in a BHD patient due to symptom delay. In chapter 3.2 we highlight SP as indicator for BHD in two pediatric patients. In chapter 3.3 and 24
25 chapter 3.4 we evaluate SP as first manifestation in BHD. In chapter 3.5 we discuss the importance of recognition of facial fibrofolliculomas as indicator for renal cell cancer. In chapter 3.6 we evaluate a patient with bilateral renal cancer as indicator for BHD. In chapter 3.7 we describe a de novo FLCN mutation in a patient with spontaneous pneumothorax and renal cancer. Finally, in part 4, the results of the previous chapters are discussed, put into perspective, and summarized. Table 2. Examples of inherited disorders predisposing to RCC (adapted from Maher ER. Genetics of familial renal cancers. Nephron Exp Nephrol 2011;118:e21-e26). Disorder Type of Rcc Associated tumours and other features VHL disease Clear cell Retinal and CNS haemangioblastoma, phaeochromocytoma, pancreatic tumours, visceral cysts Familial non-syndromic clear cell RCC Clear cell -? Gene and location VHL 3p25 HPRC1 Papillary (type 1) - MET 7q General introduction and outline of the thesis Hereditary leiomyomatosis and renal cancer Variable Cutaneous and uterine leiomyomas, leiomyosarcoma FH 1q25-32 Succinate dehydrogenase subunit mutations Variable Extra-adrenal and adrenal phaeochromocytoma, head and neck paraganglioma SDHB 1p36.1 p36 SDHD 11q23 BHD syndrome Variable Fibrofolliculomas, lung cysts and pneumothorax, colorectal polyps BHD/FLCN 17p11.2 Hyperparathyreoidismjaw tumour Papillary RCC, renal hamartomas, Wilms tumour Parathyroid tumours, fibro-osseous mandibular and maxillary tumours, renal cysts CD73/ HRPT2, 1q25 Chromosome 3 translocation Lynch syndrome Clear cell - Various (FHIT, NORE1A, etc.) Transitional cell carcinomas of the renal pelvis and ureter Colorectal cancer, endometrial cancer MSH2 2p22-p21, MLH1 3p21.3, PMS2 7p22.2, PMS1 2q31.3, MSH6 2p16 25
26 0.1 General introduction and outline of the thesis References 1. Birt AR, Hogg GR, Dubé WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatology 1977;113: Menko FH, van Steensel MAM, Giraud S, et al. Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncology 2009;10: Khoo SH, Bradley M, Wong FK, et al. Birt-Hogg- Dubé syndrome: mapping of a novel hereditary neoplasia gene to chromosome 17p12-q11.2. Oncogene 2001; Schmidt LS. Warren MB, Nickerson ML, et al. Birt-Hogg-Dubé syndrome, a genodermatosis associated with spontaneous pneumothorax and kidney neoplasia, maps to chromosome 17p11.2 Am J Hum Genet 2001;69: Nickerson ML, Warren MB, Toro JR, et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt Hogg Dubé syndrome. Cancer Cell. 2002; 2: Vocke CD, Yang Y, Pavlovich CP, et al. High frequency of somatic frameshift BHD gene mutations in Birt-Hogg-Dubé associated renal tumors. J Natl Cancer Inst 2005;97: LOVD v.3.0 Leiden Open Variation Database. Consulted on March 12, 2016 on 8. Wei MH, Blake PW, Shevchenko YO, et al. The folliculin mutation database: an online database of mutations associated with Birt-Hogg-Dubé syndrome. Hum Mutat 2009;30: Schmidt LS. Nickerson Warren MB, et al. Germline BHD-mutations spectrum and phenotype analysis of a large cohort of patients with Birt-Hogg-Dubé syndrome. Am J Hum Genet 2005;76: Toro JR, Wei MH, Glenn GM, et al. BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet 2008;45: Nickerson ML, Warren MB, Toro JR, et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg-Dubé syndrome. Cancer Cell : Khoo SJ, Giraud S, Kahnoski K, et al. Clinical and genetic studies of Birt-Hogg-Dubé syndrome. J Med Genet 2002;39: Schmidt LS. Birt-Hogg-Dubé syndrome: from gene discovery to molecularly targeted therapies. Fam Cancer ; 12(3): Linehan WM, Bratslavsky G, Pinto PA, et al. Molecular diagnosis and therapy of kidney cancer Annual Review of Medicine 2010;61: Schmidt LS, Lineham WM. Clinical features, genetics and potential therapeutic approaches for Birt-Hogg-Dubé syndrome. Expert Opin Orphan Drugs 2015;3(1): Taviera-DaSilva AM, Moss J. Clinical features, epidemiology, and therapy of lymphangioleiomyomatosis. Clin Epidemiol. 2015;7: Toro JR, Pautler SE, Stewart L, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med. 2007;175(10): Leter EM, Koopmans, AJ, Gille JJ, et al. Birt-Hogg- Dubé syndrome: clinical and genetic studies of 20 families. J Invest Dermatol. 2008;45: Kluger N, Giraud S, Coupier I, et al. Birt-Hogg- Dubé syndrome: clinical and genetic studies of 10 French families. Br J Dermatol. 2010;162: Houweling AC, Gijezen LM, Jonker MA, et al. Renal cancer and pneumothorax risk in Birt-Hogg-Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer 2011;35: Foucar K, Rosen T, Foucar E, et al. Fibrofolliculoma: a clinicopathologic study. Cutis 1981;28: Vernooij M, Claessens T, Luijten M, et al. Birt- Hogg-Dubé syndrome and the Skin. Familial Cancer 2013;12: Li S, Thangapazham RL, Wang JA, et al. Human TSC2-null fibroblast-like cells induce hair follicle neogeneis and hamartoma morphogenesis. Nat Commun. 2011;2: Vincent A, Farley M, Chan E, et al. Birt-Hogg- Dubé syndrome; a review of literature and the differential diagnosis of firm facials papules. J Am Acad Dermatol. 2003;49: Kahana M, Grossman E, Feinstein A, et al. Skin tags: a cutaneous marker for diabetes mellitus. Acta Derm Venereol. 1987;67(2): Cocciolone RA, Crotty KA, Andrews L, et al. Multiple desmoplastic melanomas in Birt-Hogg- 26
27 Dubé syndrome and a proposed signaling link between folliculin, the mtor pathway, and melanoma susceptibility. Arch Dermatol. 2010;146(11): Chung JY, Ramos-Caro FA, Beers B, et al. Multiple lipomas, angiolipomas, and parathyroid adenomas in a patient with Birt-Hogg-Dubé syndrome. Int J Dermatol. 1996;35(5): Starink TM, Kish LS, Meijer CJ. Familial multiple trichodiscomas: a clinicopathologic study. Arch Dermatol 1985;121: Farrant PB, Emerson R. Letter: Hyfrecation and currettage as a treatment for fibrofolliculomas in Birt-Hogg-Dubé syndrome. Dermatol Surg. 2007;33(10): Gambichler T, Wolter M, Altmeyer O, et al. Treatment of Birt-Hogg-Dubé syndrome with erbium: YAG lager. J Am Acad Dermatol. 2000;43(5 Pt 1): Bense L, Eklund G, Wiman LG. Smoking and the increased risk of contracting spontaneous pneumothorax. Chest 1987;92(6): Smit HJ, Chatrou M, Postmus PE. The impact of spontaneous pneumothorax, and its treatment, on the smoking behavior of young adult smokers. Respir Med. 1998;92(9): Donahue DM, Wright CD, Viale G, Mathisen DJ. Resection of pulmonary blebs and pleurodesis for spontaneous pneumothorax. Chest 1993; 104(6): Smit HJ, Wienk MA, Schreurs AJ, Schramel FM, Postmus PE. Do bullae indicate a predisposition for recurrent pneumothorax? Br J Radiol 2000;73(868): Chiu HT, Garcia CK. Familial spontaneous pneumothorax. Curr Opin Pulm Med. 2006;12(4): Faber E. Spontaneous pneumothorax in 2 siblings. Hospitalstid 1921;64: Albolnik IZ, Lossos IS, Zlotogora J, et al. On the inheritance of primary spontaneous pneumothorax. Am J Med Genet 1991;40(2): Johannesma PC, van Waesberghe JHTM, Reinhard R, et al. Chest CT for primary spontaneous pneumothorax (PSP): findings: Birt-Hogg-Dubé versus non-birt-hogg-dubé patients. Am J Resp Crit Care Med;189:A Zbar B, Alvord WG, Glenn G, et al. Risk of renal and colonic neoplasms and spontaneous pneumothorax in Birt-Hogg-Dubé syndrome. Cancer Epidemiol Biomarkers Prev. 2002;11(4): Bessis D, Giraud, Richard S, et al. A novel familial germline mutation in the initiator codon of the BHD gene in a patient with Birt-Hogg-Dubé syndrome. Br J Dermatol. 2006;155: Gunji Y, Akiyoshi T, Sato T, et al. Mutations in the Birt-Hogg-Dubé gene in patients with multiple lung cysts and recurrent pneumothorax. J Med Genet 2007;44: Tobino K, Hirai T, Johkoh T, et al. Differentation between Birt-Hogg-Dubé syndrome and lymphangioleimyomatosis: quantative analysis of pulmonary cysts on computed tomography of the chest in 66 females. Eur J Radiol. 2012:81: Pierce CW, Hull PR, Lemire EG, Marciniuk DD. Birt-Hogg-Dubé syndrome: an inherited cause of spontaneous pneumothorax. CMAJ 2011;183(9):E Verhaert LL. A young man with bilateral spontaneous pneumothorax. Case Rep Pulmonology. 2011;2011: Hopkins TG, Maher ER, Reid E, Marciniak SJ. Recurrent pneumothorax. Lancet 2011;377(9777): Ren HZ, Zhu CC, Yang C, et al. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax. Clin Genet 2008; 74(2): Agarwal PP, Gross BH, Holloway BJ, Seely J, Stark P, Kazerooni EA. Thoracic CT findings in Birt-Hogg-Dubé syndrome. AJR Am J Roentgenol 2011; 196(2): Gunji Y, Akiyoshi T, Sato T, Kurihara M, Tominaga S, Takahashi K, Seyama K. Mutations of the Birt Hogg Dubé gene in patients with multiple lung cysts and recurrent pneumothorax. J Med Genet 2007; 44(9): MacDuff A, Arnold A, Harvey J; BTS Pleural Disease Guideline Group. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline Thorax 2010; 65 Suppl 2:ii18-ii Maher ER. Genetics of familial renal cancers. Nephron Exp Nephrol 2011;118:e21-e Consulted on March 13th 2016; cancerresearchuk.org/cancerstats/typs/kidney/ incidence/index.htm#trend. 52. Lipworth L, Tarone RE, McLaughlin JK: The epidemiology of renal cell carcinoma. J Urol. 2006;176: General introduction and outline of the thesis 27
28 0.1 General introduction and outline of the thesis 53. Adeniran AJ, Shuch B, Humphrey PA. Hereditary Renal Cell Carcinoma Syndromes: Clinical, Pathologic, and Genetic Features. Am J Surg Pathol. 2015;39(12):e1-e Ho TH, Jonasch E. Genetic kidney cancer syndromes. J Natl Compr Canc Netw. 2014;12(9): Stamatakis L, Metwalli AR, Middelton LA, et al. Diagnosis and management of BHD-associated kidney cancer. Fam Cancer 2013;12(3): Pavlovich CP, Walther MM, Eyler RA, et al. Renal tumors in the Birt-Hogg-Dubé syndrome. Am J Surg Pathol. 2002; 26: Woodward ER, Ricketts C, Killick P, et al. Familial non-vhl clear cell (conventional) renal cell carcinoma: clinical features, segregation analysis, and mutation analysis of FLCN. Clin Cancer Res Sep 15;14(18): Choyke PL, Glenn GM, Walther MM, et al. Hereditary renal cancers. Radiology 2003;226: Jamis-Dow CA, Choyke PL, Jennings SB, et al. Small ( 3cm) renal masses: detection with CT versus US and pathologic correlation. Radiology 1996;198: Hall EJ, Brenner DJ. Cancer risks from diagnostic radiology. Br J Radiol 2008;81: Sodickson A, Baeyens PF, Andriole KP, et al. Recurrent CT, cumulative radiation exposure, and associated radioation-induced cancer risk from CT of adults. Radiology 2009;251: Walther MM, Choyke PI, Glenn G, et al. Renal cancer in families with hereditary renal cancer: prospective analysis of a tumor size threshold for renal parenchymal sparing surgery. J Urol 1999;161: Lonser RR, Glenn GM, Walther M, et al. Von Hippel- Lindau disease. Lancet 2003;361: Berger A, Crouzet S, Canes D, et al. Minimally invasive nephron-sparing surgery. Curr Opin Urol. 2008;18: Hornstein OP, Knickenberg M. Perifollicular fibromatosis cutis with polyps of the colon a cutaneo-intestinal syndrome sui generis. Arch Dermatol Res. 1975;253: Chung JY, Ramos-Caro FA, Beers B, et al. Multiple lipomas, angiolipomas and parathyroid adenomas in a patient with Birt-Hogg-Dubé syndrome. Int J Dermatol. 1996;35: Lui V, Kwan T, Page EH. Parotid oncocytoma in the Birt-Hogg-Dubé syndrome. J Am Acad Dermatol. 2000;43: Lindor NM, Hand J, Burch PA, et al. Birt-Hogg- Dubé syndrome: an autosomal dominant disorder with predisposition to cancers of the kidney, fibrofolliculomas, and focal cutaneous mucinosis. Int J Dermatol. 2001;40: Drummond C, Grigoris I, Dutta B. Birt-Hogg- Dubé syndrome and multinodular goiter. Austr J Dermatol. 2002;43: Welsch MJ, Krunic A, Medenica MM. Birt-Hogg- Dubé syndrome. Int J Dermatol. 2005;44: Palmirotta R, Donati P, Savonarola A, et al. Birt- Hogg-Dubé (BHD) syndrome: report of two novel germline mutations in the folliculin (FLCN) gene. Eur J Dermatol. 2008;18: Godbolt AM, Robertson IM, Weedon D, et al. Birt-Hogg-Dubé syndrome. Australas J Dermatol. 2003;44: Lamberti C, Schweiger N, Hartschuh W, et al. Birt-Hogg-Dubé syndrome: germline mutations in the (C) 8 mononucleotide tract of the BHD gene in a German patient. Acta Derm Venereol 2005;85: Imada K, Dianichi T, Yokomizo A, et al. Birt-Hogg- Dubé syndrome with clear-cell and oncocytic renal tumour and trichoblastoma associated with a novel FLCN mutation. Br J Dermatol. 2009;160: Walter P, Kirchhof B, Korge B, et al. Flecked chorioretinopathy associated with Birt-Hogg- Dubé syndrome. Graefes Arch Clin Exp Ohthalmol. 2997;235: Frantzen B, Rose C, Schulz T, et al. Hornstein- Knickenberg and Birt-Hogg-Dubé syndrome. Report of a case with spontaneous pneumothorax and aplaisa of the left carotid artery. Hautarzt 2001;52:
29
30

31 PART 1 Pulmonary manifestations
32
33 chapter 1.1 The pathogenesis of pneumothorax in Birt-Hogg-Dubé syndrome: a hypothesis Paul C. Johannesma 1, Arjan C. Houweling 2, JanHein T.M. van Waesberghe 3, R. Jeroen A. van Moorselaar 4, Theo M. Starink 5, Fred H. Menko 2 6, Pieter E. Postmus Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 3 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 4 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 5 Department of Dermatology, VU University Medical Center, Amsterdam, The Netherlands 6 Family Cancer Clinic, The Netherlands Cancer Institute, Amsterdam, The Netherlands 7 Department of Thoracic Oncology, Clatterbridge Cancer Centre, Liverpool Heart & Chest Hospital, University of Liverpool, Liverpool, United Kingdom Respirology 2014;19(8):
34 1.1 Pathogenesis of PTX in BHD syndrome Abstract The development and natural course of lung cysts in patients with Birt-Hogg-Dubé syndrome is still unclear and the relationship between the cysts and the development of pneumothorax has not been fully clarified. Based on the follow up results of thoracic imaging in 6 patients with Birt-Hogg- Dubé syndrome, we hypothesize that the pulmonary abnormalities of BHD patients are not due to a progressive degenerative disease. The decreased potential for stretching of the cysts wall and the extensive contact with the visceral pleura are likely to be responsible for rupture of the cyst wall resulting in the increased risk for pneumothorax in BHD patients. 34
35 Introduction Pneumothorax can be caused by a blunt or penetrating chest injury, or may occur without an identifiable cause and is then described as spontaneous pneumothorax (SP). If there is an obvious underlying lung disease it is classified as secondary SP. All other cases are described as primary SP (PSP), however, careful evaluation quite often reveals an underlying abnormality of the lungs, or pleura, possibly related to the development of SP. The most common of these findings is the presence of degenerative changes described as blebs, bullae or emphysema-like changes. 1 These lesions are especially found in areas with the highest degrees of pleural stress, the apices of both lungs. 2 In a subgroup of PSP patients somewhat comparable abnormalities are found in other parts of the lung, especially below the level of the main carina in the parenchyma as well as in the subpleural area. 3 These abnormalities are typical for the Birt-Hogg-Dubé syndrome. 4,5 Birt-Hogg- Dubé syndrome (BHD) is a rare hereditary syndrome first described in It is characterized by skin fibrofolliculomas, lung cysts, (recurrent) SP and renal cell cancer and is caused by germline mutations in the folliculin (FLCN) gene on chromosome 17p Almost every adult BHD patient has cysts in the lungs; however, the number detected on standard CT (slice thickness 3-5 mm) is much smaller in those who have not been diagnosed with a pneumothorax. 7 Around 50% of the cysts are located in the subpleural area. 8,9 It is unclear whether BHD-cysts are a sign of degeneration/ destruction of lung tissue like in lymphangioleiomyomatosis, Langerhans cell histiocytosis and bullae in emphysema. If degeneration plays a significant role in the development of SP in BHD one might expect an increase in number and/or size of the cysts over time. Information on the natural course of cyst development in BHD patients is very limited. We evaluated the natural course of pulmonary cysts in a patient previously treated for recurrent pneumothorax. In this case study we provide the results of repeated pulmonary imaging at an interval of 3 years and 8 months in a 47 year old male BHD patient with recurrent pneumothorax and multiple basal lung cysts and hypothesize on the causative mechanism of pneumothorax in BHD patients. 1.1 Pathogenesis of PTX in BHD syndrome Methods To evaluate the reproducibility of measurements of size and number of pulmonary cysts on CT we evaluated 5 additional BHD cases, in whom for clinical reasons thoracic CTs were repeated, within 1 year after the baseline thoracic CT. Thoracic CT scans were obtained using the 64-slice multi-detector CT system (Somatom Volume Zoom, Siemens, Erlangen, Germany) in three patients and a 256-slice multi detector CT system (Philips 256-slice Brilliance ICT, Best, The Netherlands) in two patients. Follow up of each patient was performed using the same CT system. All CT scans were made at the end of inspiration with the patient in the supine position; no intravenous contrast material was used. All images were digitally reconstructed with a section thickness of 3-5 mm. CT images were evaluated by one pulmonologist (observer). A pulmonary cyst was defined as an air-filled space with a sharply demarcated thin wall (<2mm). The observer assessed the CT images for the presence of pulmonary cysts. The size of each cyst was measured on the transversal maximum diameter. The levels of the slides of the follow up scan were equalized to the level of the baseline scan. All patients gave informed consent. 35
. There was no increase in number of cysts and the mean size (diameter) increased with a mean of 0.4 millimetres. Four of the patients had suffered from recurrent pneumothorax.")
36 1.1 Pathogenesis of PTX in BHD syndrome Results Findings on the CT scans were comparable to those on subsequent scans as is shown in 5 sets of CTs of 5 BHD control cases with CTs at a short interval (table 1). There was no increase in number of cysts and the mean size (diameter) increased with a mean of 0.4 millimetres. Four of the patients had suffered from recurrent pneumothorax. One was a former smoker, with a history of 23 pack-years. The recurrent pneumothorax and the CT-abnormalities in our index patient were the reasons to evaluate the possibility of a germline mutation in FLCN. A pathogenic splice site mutation was found (c a>g). The first pneumothorax at age 40 years was treated by VATS (in October 2006) the subsequent ipsilateral recurrences were treated by total pleurectomy (in May 2007) and chemical pleurodesis during VATS procedure (in September 2007) respectively. Table 1. Radiological characteristics of index patient and control group. Patient Mean size cysts (in mm) Number cysts (in mm) Initial fu Initial fu fu (months) PTX (n=) Smoking (in py) FLCN Mutation Index c a>g Control FLCN A>G Control FLCN.610_611DEL Control FLCN.1408_1418D Control FLCN.499C>T Control c.774_775delgtinscac The thoracic CT in the index patient revealed multiple lung cysts mainly in the basal parts of both lungs (figure 1). Despite the difference in slice thickness (5mm in the first CT versus 3mm in the second CT) only one additional lung cyst (from 36 to 37) was found on the CT after 44 months follow up. The size of the cysts was also not significantly different with a mean increase of 0.35 millimetres (range: minus 4.88 mm plus 4.45 mm), which is comparable to the findings in the control group (table 1). 36 Figure 1. Thoracic computed tomography (CT) in the index patient revealed multiple lung cysts mainly in the basal parts of both lungs.
37 Discussion The main finding of this case study was that within a period of 44 months there was no increase in size or number of pulmonary cysts. If cyst formation and pneumothorax are signs of a degenerative disease in BHD patients one might expect to see a higher prevalence of pneumothorax in older patients with BHD, which has not been reported in literature. 10 Little information is available on follow-up imaging of lung cysts in individual BHD patients. Although 44 months follow up is not very long, we found no indication of progression of the number and/or size of the cysts within this period. Ayo et al. reported a stable situation of the cysts in all four patients during a follow up period between 3 and 66 months. 11 Tobino et al. described no significant increase in size of the lung cysts in 3 patients who had undergone follow up CT scans with an interval between 7 and 24 months. This differs from other diseases with cystic changes such as pulmonary lymphangioleiomyomatosis (PLAM) and pulmonary Langerhans cell histiocytosis (PLCH). Both are known to be progressive disorders. 12 Despite the abnormalities in the lungs of BHD patients the lung function remains unaffected. This is consistent with the normal lung parenchyma found in most patients with resected cysts. 7 As most subpleural abnormalities in BHD patients are found in the lower parts of both lungs it is not very likely that pleural stress, as found in the apices of PSP patients, is causally related to the development of a pneumothorax. 2 It is much more likely that the explanation comes from the effect of the mutation in FLCN on the epithelial layer at the inside of the pleural cysts. Possibly the down regulation of folliculin results in increased cell-cell adhesion, as proposed by Medvetz and colleagues. 13 If the increased cell-cell adhesion of cells in an epithelial surface results in less potential to stretch, this might lead to rupture at the weakest spot of a continuous surface if the stretching force is strong enough. This hypothesis is supported by the hypothesis that growth of cysts is caused by fusion of smaller cysts by rupture of the wall between cysts resulting in larger cysts in which often still parts of interlobular septa are found 7. The areas in the lung where the largest stretching force occurs are the lower parts of the lung, as is reflected by the mobility of lung tumours. 14 Direct connection between a cyst wall and the visceral pleura will result in considerable stretching forces on the cyst wall adjacent to the pleura. If this results in rupture of this cyst wall one might expect rupture of the visceral pleura as well and subsequently the possibility of development of a pneumothorax. This visceral pleura cyst wall connection and rupture may even be the case in very small subpleural cysts not detectable by standard CT. 15 In conclusion: based on our observations and that of others it is unlikely t the pulmonary abnormalities of BHD patients are due to a progressive degenerative disease. It is much more likely that the trend of development and recurrence of pneumothorax in BHD is related to the lack of possibility of epithelial layers to stretch if forced to do so by connection to the visceral pleura. Follow-up of more BHD patients is needed to expand knowledge on the natural course of these cysts. This can be done by repeating thoracic CTs, for instance in cases with a recurrent or contralateral pneumothorax. To prove that especially the cysts in the lower parts of the lungs are responsible for development of a pneumothorax in BHD patients a therapeutic study is needed. A multicenter phase II study aiming at complete obliteration of the pleural space, such as can be achieved by extensive pleurectomy combined with chemical pleurodesis, should result in a much lower recurrence rate of pneumothorax in these patients. 1.1 Pathogenesis of PTX in BHD syndrome 37
38 1.1 Acknowledgements We thank the BHD families for their cooperation. Pathogenesis of PTX in BHD syndrome 38
39 Reference 1. Schramel FM, Postmus PE, Vanderschueren RG. Current aspects of spontaneous pneumothorax. Eur. Respir. J. 1997; 10(6): Casha AR, Manché A, Gatt R, Wolak W, Dudek K, Gauci M, Schembri-Wismayer P, Camilleri-Podesta MT, Grima JN. Is there a biomechanical cause for spontaneous pneumothorax? Eur. J. Cardiothorac. Surg. 2014; 45(6): Smit HJM, Wienk MAThP, Schreurs AJM, Schramel FM, Postmus PE. Do bullae indicate a predisposition to recurrent pneumothorax? Br. J. Radiol. 2000; 73(868): Ren HZ, Zhu CC, Yang C, Chen SL, Xie J, Hou YY, Xu ZF, Wang DJ, Mu DK, Ma DH, Wang Y, Ye MH, Ye ZR, Chen BF, Wang CG, Lin J, Qiao D, Yi L. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax. Clin. Genet. 2008; 74(2): Johannesma PC, Menko FH, Reinhard R, van Waesberghe JHTM, van Moorselaar RJA, Starink ThM, Postmus PE. Primary Spontaneous Pneumothorax: a pilot study on the frequency of FLCN mutation (Birt-Hogg-Dubé syndrome). Am. J. Resp. Crit. Care Med. 2014;189:A Schmidt LS. Birt-Hogg-Dubé syndrome: from gene discovery to moleculary targeted therapies. Fam. Cancer. 2013;12(3): Johannesma PC, van Waesberghe JHTM, Reinhard R, Gille JJP, van Moorselaar RJA, Houweling AC, Starink ThM, Menko FH, Postmus PE. Birt- Hogg-Dubé syndrome patients with and without pneumothorax: findings on chest CT. Am. J. Resp. Crit. Care Med. 2014;189: Kumasaka T, Hayashi T, Mitani K, Kataoka H, Kikkawa M, Tobino K, Kobayashi E, Gunji Y, Kunogi M, Kurihara M, Seyama K. Characterization of pulmonary cysts in Birt-Hogg-Dubé syndrome: histopathological and morphometric analysis of 229 pulmonary cysts from 50 unrelated patients. Histopathology. 2014; 65(1): Johannesma PC, van Waesberghe JHTM, Reinhard R, Gille JJP, van Moorselaar RJA, Houweling AC, Starink ThM, Menko FH, Postmus PE. Chest CT for primary spontaneous pneumothorax (PSP): findings: Birt-Hogg-Dubé versus non-birt-hogg- Dubé patients. Am. J. Resp. Crit. Care Med. 2014;189:A Toro JR, Pautler SE, Stewart L, Glenn GM, Weinreich M, Toure O, Wei MH, Schmidt LS, Davis L, Zbar B, Choyke P, Steinberg SM, Nguyen DM, Linehan WM. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg- Dubé syndrome. Am. J. Resp. Crit. Care Med. 2007; 175(10): Ayo DS, Aughenbaugh GL, Yi ES, Hand JL, Ryu JH. Cystic lung disease in Birt-Hogg-Dubé syndrome. Chest 2007; 132(2): Clarke BE. Cystic lung disease. J. Clin. Pathol. 2013;66(10): Medvetz DA, Khabibullin D, Hariharan V, Ongusaha PP, Goncharova EA, Schlechter T, Darling TN, Hofmann I, Krymskaya VP, Liao JK, Huang H, Henske EP. Folliculin, the product of the Birt-Hogg-Dubé tumor suppressor gene, interacts with the adherens junction protein p0071 to regulate cell-cell adhesion. PLoS One. 2012;7(11): e van Sörnsen de Koste JR, Lagerwaard FJ, Nijssen- Visser MR, Graveland WJ, Senan S. Tumor location cannot predict the mobility of lung tumors: a 3D analysis of data generated from multiple CT scans. Int J Radiat Oncol Biol. Phys. 2003; 56(2): Onuki T, Goto Y, Kuramochi M, Inagaki M, Bhunchet E, Suzuki K, Tanaka R, Furuya M. Radiologically indeterminate pulmonary cysts in Birt-Hogg-Dubé syndrome. Ann. Thoracic. Surg. 2014; 97(2): Pathogenesis of PTX in BHD syndrome 39
40
41 chapter 1.2 Presence of pulmonary cysts in BHD patients with and without a pneumothorax; a retrospective analysis of 61 patients Paul C. Johannesma 1, JanHein T.M. van Waesberghe 2, Fred H. Menko 3, R. Jeroen A. van Moorselaar 4, Marinus A. Paul 5, Theo M. Starink 6, Rinze Reinhard 2 7, Arjan C. Houweling 8, Marianne A. Jonker 9, Pieter E. Postmus 10 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 3 Family Cancer Clinic, The Netherlands Cancer Institute, Amsterdam, The Netherlands 4 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 5 Department of Thoracic Surgery, VU University Medical Center, Amsterdam, The Netherlands 6 Department of Dermatology, Leiden University Medical Center, Leiden, The Netherlands 7 Department of Radiology, Onze Lieve Vrouwen Gasthuis, Amsterdam, The Netherlands 8 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 9 Department of Epidemiology and Biostatistics, VU University Medical Center, Amsterdam, The Netherlands 10 Department of Thoracic Oncology, Clatterbridge Cancer Centre, Liverpool Heart & Chest Hospital, University of Liverpool, Liverpool, United Kingdom Submitted
42 1.2 Pulmonary cysts in BHD patients with / without PTX Abstract Introduction Multiple pulmonary cysts below the level of the carina are characteristic for Birt-Hogg-Dubé syndrome (BHD), an autosomal dominant condition caused by germline mutations in the folliculin (FLCN) gene. This autosomal dominant disorder clinically manifests in facial skin fibrofolliculomas, renal cell cancer (RCC), lung cysts and (recurrent) spontaneous pneumothorax (SP). Although the precise prevalence of BHD is unknown, two recent studies suggest that this syndrome is present in 5-10% of all PSP patients. The relationship between lung cyst characteristics and the development of (recurrent) SP is unknown. Chest computed tomography (CT) in this patient group might therefore be an useful tool for choice of treatment when developing a SP and might also play a role in advice of lifestyle. Material and methods We retrospectively collected the clinical data on all patients with a proven pathogenic FLCN mutation and an available thoracic CT. We scored on demographics and medical history for (recurrent) SP. The thoracic CT was reviewed for presence of abnormalities, and more specifically the presence of cystic abnormalities and/or air filled cavities. If these were found the size, number, location below and/or above level of main carina, in the parenchyma and/or subpleural area were noted. Results We included a total of 61 patients, 19 of them had a history of (recurrent) SP. We found a higher number of lung cysts among BHD patients with a history of (recurrent) SP. No differences were found in gender, size or location. We found no correlation between the number of cysts and age and no genotype phenotype correlation was found. Conclusion CT scanning of BHD patients may lead to detection of abnormalities characteristic for BHD. There seems to be a relationship between the number of cysts and development of (recurrent) SP. Chest CT in this patient group might therefore be an useful tool for choice of treatment when developing a SP and might also play a role in advice of lifestyle. 42
43 Introduction Birt-Hogg-Dubé syndrome (BHD) is an autosomal dominant condition caused by germline mutations in the folliculin (FLCN) gene. BHD is clinically characterized by skin fibrofolliculomas, pulmonary cysts, (recurrent) spontaneous pneumothorax (SP) and renal cell cancer. Clinical manifestations of BHD are variable and include patients and families with only skin, lung or renal abnormalities. 1 Two recent studies suggest that this syndrome is presented in 5-10% of all primary spontaneous pneumothorax (PSP) patients. 2 3 SP may be the first and only manifestation of BHD in isolated and familial cases. Most BHD patients have normal chest X-ray images but multiple lung cysts are commonly identified on CT. Multiple pulmonary cysts below the level of the carina, detected by thoracic CT, are characteristic for BHD as described in a few small thoracic CT studies and several sporadic case reports or small retrospective studies with a small number of included patients These studies show that most BHD patients (77-100%) have lung cysts, and it is assumed these to be related to the development of SP, although this occurs in a minority (33-39%) of all BHD patients. 8 Approximately 50% of these cysts are located in the subpleural area and 50% in the parenchyma Although about 90% of BHD syndrome patients have these multiple cysts, lung function (measured by spirometry and diffusion capacity) is generally normal. 9 Thus, patients with pneumothorax due to BHD often have no preceding symptoms of pulmonary disease and are therefore likely to be diagnosed as having PSP. For BHD mutation carriers it is relevant to know if for an individual there is a higher or lower risk of developing pulmonary complications, as this may affect their lifestyle, such as flying or diving. What the relationship between the on CT found abnormalities and the development of (recurrent) SP is, has not been described. In this study we compared the CT findings in BHD patients with and without a history of SP to evaluate whether there are CT-characteristics that differentiate BHD patients with SP from BHD patients without BHD. 1.2 Pulmonary cysts in BHD patients with / without PTX Materials and methods We retrospectively collected the clinical data on all patients with a proven pathogenic FLCN mutation and an available thoracic CT known in the VU University Medical Center. Exclusion criteria were clinical BHD without a proven FLCN mutation, secondary pneumothorax due to apparent underlying disease e.g. emphysema, traumatic or iatrogenic pneumothorax. Furthermore, deceased patients were excluded. One CT of the thorax of all the cases was scored, independently and blinded for final diagnosis, by an experienced pulmonologist (PEP) and an experienced radiologist (JHvW). Blinding for diagnosis was achieved by adding these cases to a much larger series of cases with a history of SP reviewed for other purposes. In case of multiple CTs the one in time closest to a pneumothorax episode was used, when available, after radiological resolution of the SP. For the BHD patients without a history of SP, the most recent available CT was used. We assumed, based on our prior study, that all radiological findings remained largely unchanged over time. 10 Scoring consisted of presence of abnormalities, and more specifically the presence of cystic abnormalities and/or air filled cavities. If these were found the size, number, location below and/or above level of main carina, in the parenchyma and/or subpleural area were noted. For FLCN mutation analysis genomic DNA was extracted from blood samples. Primers for the amplification and sequencing of the 14 exons were designed as detailed by Nickerson et al. PCR amplification was performed using a PE 9700 thermocycler (Applied Biosystems, Forster City, 43
44 1.2 Pulmonary cysts in BHD patients with / without PTX CA, USA). Sequencing reactions were performed using the Big Dye Terminator system (Applied Biosystems) and run on an ABI 3100XL or ABI 3730 genetic analyzer (Applied Biosystems). For the detection of deletions and duplications of one or more exons MLPA analysis was performed using MLPA kit P256 (MRC Holland, 11 All statistical analyses were performed using R software (version ). To compare the results of cysts on thoracic CT scans in BHD patients with and without history of (recurrent) SP, we used the Wilcoxon rank sum test with continuity correction. To evaluate a possible correlation between age and number of cyst and between number and size of cysts, we used the Spearman correlation test. A p-value of less than 0.05 was considered significant. All patients gave written informed consent for this study. The study was approved by the Ethics Committee of the VU University Medical Center. Results We included a total of 61 BHD patients with a proven pathogenic FLCN mutation, 27 of them were men and 34 of them were women. We included 19 BHD patients with a (recurrent) episode of SP and 42 BHD patients without a history of (recurrent) SP so far. We found in all included patients one or more lung cysts on thoracic CT. The mean number of cysts among BHD patients with a history of (recurrent) SP was 81.3 and the mean number of cysts among BHD patients without a history of (recurrent) SP was 19.0 cysts, this differed significantly between both groups (p<0.008). We found no significant difference in size, predominant distribution subpleurally or in the parenchyma, shape, or presence of small pulmonary artery and veins in the cysts. (table 1). As we found only a significant difference in number of cysts between both groups, we performed a subgroup analysis. The number of cysts did not significantly differ between men and women when both groups were taken together (figure 1; men=0 ; female =1). The scatter of cysts in number vary much more widely in the group of BHD patients with (recurrent) SP with a minimum of one cyst and a maximum of 250 cysts (mean number of pleural cysts 41.8 ± 37.0, mean number of parenchymal cysts 53 ± 45.9), compared to the group of BHD patients without a history of (recurrent) SP with a minimum of one cyst and a maximum of 80 cysts (mean number of pleural cysts 8.4 ± 9.1, mean number of parenchymal cysts 10.5 ± 11.6) (figure 2). We found no relationship (ρ=-0.027) between age and the number of cysts, which confirms the findings of our former published study. 14 Also when we perform this sub analysis in both groups separately, we found no relationship between age and the number of cysts (figure 3). The scatter in size between both groups are comparable, no predilection of size was found in both groups (figure 4). Also the presence of cysts above and under the carina did not differ between both groups (figure 5). Finally no genotype phenotype correlation was found in both groups. Discussion In this study we evaluated a group of 61 patients, 19 of them had a history of (recurrent) SP. We observed an important and significant difference between the two groups with respect to number of cysts. In the BHD patients with a history of (recurrent) SP we found a significant higher number of cysts in the lungs, both subpleurally and in the parenchyma. This might indicate that the visible 44
45 Table 1. Radiological characterisitics of cysts in BHD patients with a history of (recurrent) spontaneous pneumothorax and in BHD patients without a history of (recurrent) spontaneous pneumothorax. BHD+ Pneumothorax (sp)+ N=19 BHD+ Pneumothorax (sp) N=42 P-value Number of cysts (N=) 81.3 ( ) 19.0 ( ) 0,008 Distribution under main carina (%) Distribution left lung (%) Distribution right lung (%) Diameter <1cm (%) Diameter 1-2cm (%) Diameter >2cm (%) Distribution subpleural (%) Distribution parenchyma (%) Shape round (%) Shape oval (%) Abutting pulmonal artery/vein (%) Pulmonary cysts in BHD patients with / without PTX Figure 1. Number of cysts in male (0) and female (1) patients with BHD syndrome. cysts on thoracic CT are related to the development of SP in BHD patients. Compared to SP patients without a pathogenic FLCN mutation, lung cysts in BHD patients are smaller, are more equally distributed both subpleural and in the parenchyma and predominantly located in the lower parts of the lung. 12 Compared to e.g. lymphangioleiomyomatosis (LAM), lung cysts in BHD are typically described more uniform in size, multi-septated, round and diffuse in distribution. 13 The pathogenesis of lung cysts and the relationship with SP in BHD has not been fully clarified yet. A possible explanation can be the stretch hypotheses proposed by Kennedy et al. wherein they 45
46 1.2 Pulmonary cysts in BHD patients with / without PTX Figure 2. Number of cysts in patients with BHD but without a history of (recurrent) spontaneous pneumothorax (left) and number of cysts in patients with BHD and a history of (recurrent) spontaneous pneumothorax (right). Figure 3. Relationship between number of cysts and age. suggest that pulmonary cysts in BHD patients arise because of fundamental defects in cell-cell adhesion, leading to repeated respiration-induced physical stretch-induced stress and, over time, expansion of alveolar spaces particularly in regions of the lung with larger changes in alveolar volume and at weaker anchor points to the pleura. Whether this happens trough a destructive/ inflammatory program or a proliferative program, remains unclear. 14 Kumasaka et al analysed resected lung specimens of 50 BHD patients. 15 Out of 229 cysts that were found; 50% were located in the subpleural area and less than 5% abut on bronchioles. Based on this result we hypothesized that one of the consequences of the mutation in FLCN is the difficulty of respiratory epithelium to stretch, which likely will result in rupture of the wall of the cyst and leakage of air from inside the cyst to the surrounding area. If this is the lung parenchyma there will probably no problem occur, however if the cyst is in close connection with the overlying visceral pleura the air may leak through the as well ruptured pleura into the pleural cavity. This might create a small SP. If this ruptured cyst is in connection with the intrapulmonary airways, active leakage of more air 46
47 1.2 Figure 4. Relationship between size of cysts and development of spontaneous pneumothorax. Pulmonary cysts in BHD patients with / without PTX Figure 5. Presence of cysts above and under the carina. into the pleural cavity may follow, ultimately resulting in a symptomatic SP. Arguments to support this mechanism come from observed delayed SP after considerable atmospheric pressure changes, such as occur during flying Our observation in this study, that SP patients with BHD have much more cysts, supports the above described etiology as they have more possibilities to suffer from cyst rupture than the non-sp patients with BHD. In this study, we found no difference between the frequency of visible cysts in the subpleural area, in absolute numbers there certainly is. However, the presence of subpleural cysts might be underestimated as small cysts, due to the way CTs were done, will not be detected easily and these still could rupture On the other hand rupture of a small cyst will not that easily result in a symptomatic pneumothorax as the damage to the parenchyma, and consequently leakage of air, will be much smaller and absorption of intrapleural gas might cope with that. If we assume that the rupture of a subpleural cyst is the likely cause of the pneumothorax in BHD patients, these patients might also need a different approach for treatment than is assumed in current guidelines. As these cysts are found throughout the lungs with the majority in the lower 47
48 halves of the lungs, treatment to prevent recurrence should have as aim pleurodesis of the whole pleura visceralis, and not only in the apical region. As we showed in a different study, this can be done by extensive pleurectomy and/or talc pleurodesis Pulmonary cysts in BHD patients with / without PTX Unfortunately no genotype-phenotype association was found in this patient group. A history of spontaneous SP was somewhat more common among c a>g (4/19) and c.610_611delgcinsta. This is in line with another large study, wherein no genotype-phenotype correlation was found either. 20 Combining databases of BHD patients is needed to get more insight in possible prediposure for fenotype patterns. Based on 2 previous studies we hypothesized that BHD may not be as rare as assumed. 6 7 In addition to predisposing for a high risk of recurrent SP, BHD is also associated with a high risk of developing renal cell cancer with an estimated life time risk of around 15%. 21 If detected late, renal cancer is likely to have a fatal outcome. Since BHD is an autosomal dominant condition, early diagnosis enables screening for renal cancer in relatives of BHD patients who have a 50% chance of carrying the mutation in FLCN. Identification of these at risk relatives, by screening initiated after diagnosing BHD in an affected SP patient, was shown to result in earlier detection of renal cell cancer. 22 Early detection of a BHD in a patient presenting with SP may therefore be potentially life-saving not only for the patient but also for affected relatives. Although this is the first study in current literature that reviewed the relationship between lung cysts and SP among BHD patients, this study has a few limitations. The main limitation is the small number of patients we included. As this syndrome is relatively rare, it is difficult to gather a large cohort of patients. Although there seems to be a clear distinction on thoracic CT between BHD patients with and without a history of (recurrent) SP, the rarity of this syndrome may still lead to unawareness among doctors who have to evaluate these thoracic CT s. Although not all clinical information regarding smoking history, familial inheritance on pneumothorax and prior (surgical) treatment of pneumothorax was available, we suggest that thoracic imaging might play an important role in the prediction for development of pneumothorax in BHD patients. In conclusion: CT scanning of BHD patients may lead to detection of abnormalities characteristic for BHD. There seems to be a relationship between the number of cysts and development of (recurrent) SP. Chest CT in this patient group might therefore be an useful tool for choice of treatment when developing a SP and might also play a role in advice of lifestyle. Current pneumothorax guidelines might need to be discussed and revised. 48
49 References 1. Menko FH, van Steensel MAM, Giraud S, et al. Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncol 2009;10: Johannesma PC, Reinhard R, Kon Y, et al. Prevalence of Birt-Hogg-Dubé syndrome in patients with apparently primary spontaneous pneumothorax. Eur Respir J 2015; 45: Ren HZ, Zhu CC, Yang C, et al. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax Clin Genet 2008; 74: Bakan S, Kandemirli SG, Kilic F, et al. Birt-Hogg- Dubé syndrome: A diagnosis to consider in patients with renal cancer and pulmonary cysts. Diagn Interv Imaging Jan;97(1): Onuki T, Goto Y, Kuramochi M, Radiologically indeterminate pulmonary cysts in Birt-Hogg-Dubé syndrome. Ann Thorac Surg Feb;97(2): Seaman DM, Meyer CA, Gilman MD, et al. Diffuse cystic lung disease at high-resolution CT. AJR Am J Roentgenol Jun;196(6): Tobino K, Hirai T, Johkoh T, et al. Differentiation between Birt-Hogg-Dubé syndrome and lymphangioleiomyomatosis: quantitative analysis of pulmonary cysts on computed tomography of the chest in 66 females. Eur J Radiol Jun;81(6): Toro JR, Pautler SE, Stewart L, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med 2007;175: Gupta N, Seyama K, McCormack FX. Pulmonary manifestations of Birt-Hogg-Dubé syndrome. Fam Cancer. 2013;12: Johannesma PC, Houweling AC, van Waesberghe JH, et al. The pathogenesis of pneumothorax in Birt-Hogg-Dubé syndrome: a hypothesis. Respirology Nov;19(8): Nickerson, M.L., Warren, M.B., Toro, J.R. et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg-Dubé syndrome. Cancer Cell 2002: 2: Johannesma PC, van Waesberghe JHTM, Menko FH, et al. Radiological features of primary spontaneous pneumothorax patients with or without a mutation in FLCN. (Submitted) 13. Agarwal PP, Gross BH, Holloway BJ, et al. Thoracic CT findings in Birt-Hogg-Dubé syndrome. ARJ 2011;196; Kennedy JC, Khabibullin D, Henske EP. Mechanisms of pulmonary cyst pathogenesis in Birt-Hogg- Dubé syndrome: The stretch hypothesis. Semin Cell Dev Biol. 2016;52: Kumasaka T, Hayashi T, Mitani K, et al. Characterization of pulmonary cysts in Birt- Hogg-Dubé syndrome: histopathological and morphometric analysis of 229 pulmonary cysts from 50 unrelated patients. Histopathology. 2014;65: Johannesma PC, van de Beek I, van der Wel JWT, et al. Risk of spontaneous pneumothorax due to air travel and diving in patients with Birt-Hogg-Dubé syndrome. (SpringerPlus, in revision). 17. Postmus PE, Johannesma PC, Menko FH, et al. In-flight pneumothorax: diagnosis may be missed because of symptom delay. Am J Respir Crit Care Med Sep 15;190(6): Reference 18: Jawad H, Walker CM, Wu CC, Chung JH. Cystic interstitial lung diseases: recognizing the common and uncommon entities. Curr Probl Diagn Radiol. 2014;43(3): Johannesma PC, Paul MA, van Waesberghe JHTM, et al. International guidelines for pneumothorax are not adequate for treatment of spontaneous pneumothorax in patients with Birt-Hogg-Dubé syndrome. (Submitted) 20. Toro JR, Wei M-H, Glenn GM, et al. BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet 2008;45: Houweling AC, Gijezen LM, Jonker MA, et al. Renal cancer and pneumothorax risk in Birt-Hogg-Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer. 2011;105(12): Johannesma PC, Houweling AC, Menko FH, et al. Are lung cysts in renal cell cancer (RCC) patients an indication for FLCN mutation analysis? Fam Cancer. 6;15: Pulmonary cysts in BHD patients with / without PTX 49
50
51 chapter 1.3 Radiological features of primary spontaneous pneumothorax patients with or without a mutation in FLCN Paul C. Johannesma 1, JanHein T.M. van Waesberghe 2, Fred H. Menko 3, R. Jeroen A. van Moorselaar 4, Marinus A. Paul 5, Theo M. Starink 6, Rinze Reinhard 2,7, Arjan C. Houweling 8, Irma van de Beek 8, Hans J. Smit 9, Jincey D. Sriram 9, Marianne A. Jonker 10, Pieter E. Postmus 11 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 3 Family Cancer Clinic, The Netherlands Cancer Institute, Amsterdam, The Netherlands 4 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 5 Department of Thoracic Surgery, VU University Medical Center, Amsterdam, The Netherlands 6 Department of Dermatology, Leiden University Medical Center, Leiden, The Netherlands 7 Department of Radiology, Onze Lieve Vrouwen Gasthuis, Amsterdam, The Netherlands 8 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 9 Department of Pulmonary Diseases, Rijnstate Hospital, Arnhem, The Netherlands 10 Department of Epidemiology and Biostatistics, VU University Medical Center, Amsterdam, The Netherlands 11 Department of Thoracic Oncology, Clatterbridge Cancer Centre, Liverpool Heart & Chest Hospital, University of Liverpool, Liverpool, United Kingdom Submitted
52 1.3 Radiological features of PSP patients with / without Bhd Abstract Introduction In the past few years it has become apparent that several disorders with pulmonary involvement are associated with an increased risk of primary spontaneous pneumothorax (PSP). One of these disorders associated with a very high risk of recurring PSP, is the probably relatively common (5-10% of all PSP patients) cystic lung disease Birt-Hogg-Dubé (BHD) syndrome. As over 90% of these patients have cysts in basal parts of the lung, we hypothesized that the use of a low dose chest CT might be an effective way to detect this syndrome in patients presenting with an apparently isolated PSP. This is important as its inheritance is autosomal dominant, and is associated with a risk of renal cell cancer of approximately16-30%. Material and Methods We included 46 patients, 19 with a proven FLCN mutation and 27 without an identifiable FLCN mutation, with a history of spontaneous pneumothorax. We retrospectively evaluated the thoracic CT s for cystic abnormalities and/or air filled cavities, size, number and site (below and/or above level of main carina, presence in the parenchyma and/or subpleural area) were scored and compared to findings in a both groups Results We found a higher prevalence of recurrent episodes of SP among patients with a proven pathogenic FLCN mutation. Also the prevalence of (separate) episodes of SP in BHD patients was higher. The number of cysts in BHD patients was significantly higher in patients with a FLCN mutation. Also their distribution, location and size on thoracic CT differed significantly from patients without BHD syndrome. Conclusion CT scanning of PSP patients may by a useful tool in the detection of BHD in patients presenting with an apparently isolated PSP. 52
53 Introduction Idiopathic or primary spontaneous pneumothorax (PSP) is described as the presence of air in the pleural cavity without a known pulmonary abnormality. 1 Over time it has become clear that PSP might be the result of a number of pulmonary abnormalities, ranging from smoking related subpleurally located abnormalities 2 3, to inherited diseases like Marfan s syndrome, alpha-1-antitrypsin deficiency, Birt-Hogg-Dubé syndrome (BHD), lymphangioleiomyomatisis and homocysteinuria These conditions have in common that they may cause rupture of the visceral pleura, resulting in leakage of air into the pleural cavity and, depending on the amount of air in the pleural cavity, the development of a symptomatic pneumothorax. In current British Thoracic Society guidelines and the guidelines of the American College of Chest Physicians, recommendations on imaging of the lung parenchyma in PSP patients is very restricted In fact, for the first episode of pneumothorax the recommended diagnostic procedures are limited to taking history, physical examination and an erect chest-x-ray. 9 The rare conditions associated with an increased risk of SP may remain unrecognized following the current guidelines. A standardized more robust assessment of these patients might enable adequate diagnosis of these conditions and lead to a more effective treatment and disease management. As almost half of the PSP patients develop a recurrence, one of the main aims of guidelines on the diagnosis and treatment of PSP is the prevention of recurrence in patients prone to recurring PSP. One of the hereditary causes of pneumothorax, with a very high recurrence risk, is the relatively common Birt-Hogg-Dubé (BHD) syndrome, estimated to be present in 5-10% of PSP patients. Furthermore, prevention of recurrence of pneumothorax with standard approaches is in these patients very often ineffective. 13 Current guidelines recommend the use of chest CT for recurrent pneumothorax. We evaluated the findings of chest CT in a group of PSP patients without a detectable FLCN mutation and compared these to a group with a proven mutation in FLCN to evaluate whether CT scanning in PSP patients is a sensitive tool in diagnosing BHD in PSP patients. This would be highly clinically relevant since BHD is associated with an increased risk of renal cancer. 1.3 Radiological features of PSP patients with / without Bhd Materials and methods We evaluated the medical history of all FLCN mutation carriers known in the VU University Medical Center and the Rijnstate Hospital. The medical records of patients with a history of SP were examined (N=46). FLCN mutation negative patients with a history of PSP were recruited from a prospective study we performed previously 11, and retrospectively from the VUMC-database of PSP patients tested negative for the FLCN mutation. The clinical details and number of all pneumothorax episodes were collected of all patients in both groups (FLCN mutation positive and FLCN mutation negative). One CT-thorax of all the patients was scored independently by an experienced pulmonologist (PEP) and an experienced radiologist (JHvW) blinded for the final diagnosis. In case of multiple CTs the one made closest to the time of a pneumothorax episode was used, when available, after radiological resolution of the pneumothorax. For the mutation negative patients to be included, 53
54 1.3 Radiological features of PSP patients with / without Bhd the CT had to be performed within one year of the pneumothorax. We assumed, based on our prior study, that for the BHD cases this time interval is less relevant as the findings on chest CT have were found to remain largely unchanged over time. 14 Scoring consisted of presence of abnormalities, and more specifically the presence of cystic abnormalities and/or air filled cavities. If these were found the size, number, location below and/or above level of main carina, in the parenchyma and/ or subpleural area were noted. For FLCN mutation analysis genomic DNA was extracted from blood samples. Primers for the amplification and sequencing of the 14 exons were designed as detailed by Nickerson et al. PCR amplification was performed using a PE 9700 thermocycler (Applied Biosystems, Forster City, CA, USA). 15 Sequencing reactions were performed using the Big Dye Terminator system (Applied Biosystems) and run on an ABI 3100XL or ABI 3730 genetic analyzer (Applied Biosystems). For the detection of deletions and duplications of one or more exons MLPA analysis was performed using MLPA kit P256 (MRC Holland, All statistical analyses were performed using R software (version ). To compare the results of thoracic CT scans of SP patients with and without a FLCN mutation, we used the Wilcoxon test. A p-value of less than 0.05 was considered significant. The study was approved by the Ethics Committee of the VU University Medical Center. Results The main characteristics of the 46 included patients are summarized in table 1. We included 46 patients with a history of (recurrent) SP. All patients were tested for FLCN mutations between 2005 and We included 19 patients with a pathogenic FLCN mutation and 27 patients without a pathogenic FLCN mutation. In the included group of patients with a pathogenic FLCN mutation and a history of (recurrent) SP, the mean age at the first episode of PSP was 31.2 years. The number of patients with at least one recurrent episode was 68.4%. The mean number of episodes per patients was 3.5 with a maximum of twelve episodes. As we scored both lungs separately, we found at least one episode in the left lung in 72.2% of cases, 57.9% in the right lung and in 52.6% of cases at least one episode (separate moment) in both lungs (table 1). In the group of patients with (recurrent) SP (N=27) but without a detectable pathogenic FLCN mutation, the mean age at the first episode of PSP was 27.8 years and 59.3% of cases underwent at least one recurrent episode in the same lung. The mean number of episodes per patient was 1.5 episodes, with a maximum of four episodes. In total 59.2% occurred in the left lung, 55.6% in the right lung and in 18.5% of cases (at separate moments) in both lungs. In table two the results of the scored thoracic CT s are summarized. We found a large difference between the two groups of patients in the number of cysts. The number of cysts in BHD patients was significantly higher than in de group patients without BHD (p<0.001). We also found a significant difference in the distribution of the cysts, as the majority of cysts in BHD patients were found under the carina (p<0.001). Cysts in BHD patients are significant smaller (p<0.023), and are more equally distributed both subpleural and in the parenchyma (p<0.001). Also the presence of small pulmonary artery and veins in the cysts was only seen in the group of BHD patients (p<0.001). 54
55 Discussion Although the number of cases evaluated in this study is relatively small, we observed an important and significant difference between the two groups in respect to the type of abnormalities found. In the BHD patients the most commonly observed abnormality was the presence of one or more cysts in the parenchyma or adjacent to the visceral pleura, predominantly in the lower lobes. In contrast, in the FLCN mutation negative cases, we observed no abnormalities in the lower halves of the lung, nor abnormalities in the parenchyma far from the visceral pleura. Most of the abnormalities detected by CT were small (<2cm). This explains why these abnormalities could not be detected using a standard erect chest X-ray. The abnormalities found in the group of patients with a pathogenic FLCN mutation have in common a probably important attribute, likely to be associated with an increased risk of pneumothorax: spaces with trapped air. In the FLCN mutation negative cases the emphysema like changes in the apical parts are caused by accumulation of trapped air behind a one-way valve caused by conditions such as respiratory bronchiolitis. 16 The vast majority of air-filled cysts in BHD patients are not connected to the airways 17, resulting in trapped-air. Rapid changes in atmospheric pressure are likely to result in an increased chance of rupture of the wall of air-filled cavities or cysts potentially resulting in a spontaneous pneumothorax. Epidemiological data on weather conditions support this hypothesis 18 19, but also individual cases of pneumothorax related to exposure to large pressure changes have been reported. It is likely that in addition to air trapping other mechanisms play a role in the development of a pneumothorax. In the apical parts of the lung the pleural stress is high and abnormalities in that area are likely to increase the risk of rupture. 22 In BHD-patients the majority of cysts are located in the pleura in the lower lobes, which makes it likely that the wall of cysts connected to the visceral pleura rupture easily. 14 Important for this is the lack of stretching possibilities of the wall of lung cysts of BHD patients. 23 Based on 2 previous studies we hypothesized that BHD may not be as rare as assumed. In addition to predisposing for a high risk of recurrent pneumothorax, BHD is also associated with a high risk of developing renal cell cancer with an estimated life time risk of around 15% 24. If detected late, renal cancer is likely to have a fatal outcome. Since BHD is an autosomal dominant condition, early diagnosis enables screening for renal cancer in relatives of BHD patients who have a 50% chance of carrying the mutation in FLCN. Identification of these at risk relatives, by screening initiated after diagnosing BHD in an affected pneumothorax patient, was shown to result in earlier detection of renal cell cancer Early detection of a BHD in a patient presenting with SP may therefore be potentially life-saving not only for the patient but also for affected relatives. There are a few limitations to our study. The main limitation is the small number of patients we included. As this syndrome is relatively rare, it is difficult to gather a large cohort of patients. Although there seems to be a clear distinction on thoracic CT between BHD patients and patients without BHD, the rarity of this syndrome may still lead to unawareness among doctors who have to evaluate these thoracic CT s. Although not all clinical information regarding smoking history, familial inheritance on pneumothorax and prior (surgical) treatment of pneumothorax was available, 1.3 Radiological features of PSP patients with / without Bhd 55
56 we suggest that the radiological distinction between BHD and patients without BHD can easily be made on a low dose CT scan of the thorax. In conclusion: CT scanning of PSP patients may lead to detection of abnormalities characteristic for BHD. Current pneumothorax guidelines might need to be discussed and revised. 1.3 Radiological features of PSP patients with / without Bhd Figure 1. Boxplot and histogram, number of cysts. Patients with pathogenic FLCN mutation (BHD syndrome) compared to patients without a pathogenic FLCN mutation (no BHD syndrome). Table 1. Demographic results of all spontaneous pneumothorax patients, divided in patients with a pathogenic FLCN mutation and patients without a pathogenic FLCN mutation. Pathogenic FLCN mutation (N=19) No pathogenic FLCN mutation (N=27) Age in years (min-max) 31.2 (20-40) 27.8 (16-78) Number of patients with at least one recurrent episode of SP (=%) Mean number of episodes of SP (min-max) 3.5 (1-12) 1.5 (1-4) Side (Left : Right : Both) 73.7 : 57.9 : : 55.6 :
57 References 1. Kjæergaard H. Spontaneous pneumothorax in the apparently healthy. Acta Med Scand Suppl 1932; 43: Bense L, Lewander R, Eklund G, et al. Nonsmoking, non-alpha 1-antitrypsin deficiency-induced emphysema in nonsmokers with healed spontaneous pneumothorax, identified by computed tomography of the lungs. Chest 1993; 103: Mitlehner W, Friedrich M, Dissmann W. Value of computer tomography in the detection of bullae and blebs in patients with primary spontaneous pneumothorax. Respiration 1992; 59: Dyhdalo K, Farver C. Pulmonary histologic changes in Marfan syndrome: a case series and literature review. Am J Clin Pathol 2011; 136: Daniel R, Teba L. Spontaneous pneumothorax and alpha 1-antitrypsin deficiency. Respir Care 2000; 45: Toro JR, Pautler SE, Stewart L, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med 2007;175: Bass HN, LaGrave D, Mardach R, et al. Spontaneous pneumothorax in association with pyridoxine-responsive homocystinuria. J Inherit Metab Dis 1999; 20: Taveira-DaSilva AM, Moss J. Clinical features, epidemiology, and therapy of lymphangioleiomyomatosis. Clin Epidemiol Apr 7;7: MacDuff A, Arnold A, Harvey J, and the BTS Pleural Disease Guideline Group. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline Thorax 2010; 65 (suppl 2): ii Baumann MH, Strange C, Heffner JE. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest. 2001;119: Johannesma PC, Reinhard R, Kon Y, et al. Prevalence of Birt-Hogg-Dubé syndrome in patients with apparently primary spontaneous pneumothorax. Eur Respir J 2015; 45: Ren HZ, Zhu CC, Yang C, et al. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax Clin Genet 2008; 74: Johannesma PC, Jonker MA, van der Wel MA, et al. Management of spontaneous pneumothorax in patients with or without Birt Hogg Dubé syndrome. Eur Respir J 2014; 44: Suppl. 58, Johannesma PC, Houweling AC, van Waesberghe JHTM, van Moorselaar RJA, Starink ThM, Menko FH, Postmus PE. The pathogenesis of pneumothorax in Birt-Hogg-Dubé syndrome: a hypothesis. Respirology 2014; 19: Nickerson ML, Warren MB, Toro JR, et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg-Dubé syndrome. Cancer Cell Aug;2(2): Cottin V, Streichenberger N, Gamonde s J-P, et al. Respiratory bronchiolitis in smokers with spontaneous pneumothorax. Eur Respir J 1998; 12: Kumasaka T, Hayashi T, Mitani K, et al. Characterization of pulmonary cysts in Birt-Hogg-Dubé syndrome: histopathological and morphometric analysis of 229 pulmonarycysts from 50 unrelated patients. Histopathology 2014; 65: Haga T, Kurihara M, Kataoka H, Ebana H. Influence of wheather conditions on the onset of primary spontaneous pneumothorax: positive association with decreased atmospheric pressure. Ann Thorac Cardiovasc Surg 2013; 19: Scott GC, Berger R, McKean HE. The role of atmospheric pressure variation in the development of spontaneous pneumothoraces. Am Rev Resp Dis 1989; 139: Araki K, Okada Y, Kono Y, To M, To Y. Pneumothorax recurrence related to high-speed lift. Am J Med 2014; 127: e Postmus PE, Johannesma PC, Menko FH, Paul MA. In-flight pneumothorax: diagnosis may be missed due to delayed symptoms. Am J Resp Crit Care Med 2014; 190: Casha AR, Manché A, Gatt R, et al. Is there a biomechanical cause for spontaneous pneumothorax? Eur J Cardiothorac Surg Jun;45(6): Medvetz DA, Khabibullin D, Hariharan V, et al. Folliculin, the product of the Birt-Hogg-Dubé tumor suppressor gene, interacts with the adherens junction protein p0071 to regulate cell-cell adhesion. PLoS ONE 2012;7: e Houweling AC, Gijezen LM, Jonker MA, et al. Renal cancer and pneumothorax risk in Birt Hogg Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer 2011; 105: Johannesma PC, Houweling AC, Menko FH, et al. Are lung cysts in renal cell cancer (RCC) patients an indication for FLCN mutation analysis? Fam Cancer 2016;16: Radiological features of PSP patients with / without Bhd
58
59 chapter 1.4 How reliable are clinical criteria to distinguish between BHD and smoking as a cause for pneumothorax? Paul C. Johannesma 1, Erik Thunnissen 2, Pieter E. Postmus 1 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Pathology, VU University Medical Center, Amsterdam, The Netherlands Histopathology 2014;64(7)1045-6
60 We congratulate dr. Fabre and colleagues with their interesting study 1 as published reports of histopathology of lung tissue of BHD patients are limited. In this study a retrospective analysis was performed to compare histopathology and CT-imaging of 5 Birt-Hogg-Dubé (BHD) patients with a matched cohort of five assumed non-bhd - patients with a history of smoking and spontaneous pneumothorax (SP). 1.4 Clinical criteria for BHD syndrome Based on the study design and conclusion, we believe that some remarks should be made. It is unclear why the author assume that the SP in their cases in the control group were caused by smoking and not due to BHD. The final proof of non-bhd as causative factor is the lack of a pathogenic FLCN mutation in a patient with SP. It is difficult to conclude on clinical and/or radiological characteristics only, that SP is not caused by BHD. So far only in one study 102 unselected patients with SP were tested for a pathogenic mutation, ten cases (9.8%) with a mutation were found. 2 Although the characteristics of these 10 cases, and of 4 relatives with a mutation and SP, were not reported in a very detailed way, it is possible to conclude from this study that in at least 6 cases abnormalities (cysts) were found in the upper lung or apical part, three of these were (former) smokers. In 5 of these 6 cases the number of cysts was certainly < 10. In the study by Fabre et al. there were clear differences between BHD cases and assumed non-bhd controls. However, the findings of Ren et al. question the assumption of a lack of mutation as the characteristics of assumed non-bhd are overlapping with at least a number of BHD cases and it is therefore far from certain that the 5 control cases were really free of a mutation in FLCN. Furthermore the histopathological study by Furuya et al. confirms the presence of TTF-1 in BHD cases, although controls are lacking. 3 This suggests that TTF-1 staining patterns may be specific for BHD, while this is not necessarily the case, as the results of TTF-1 in controls in this study are not clearly mentioned. Furthermore it is far from certain that SP in a smoking BHD patient is always related to BHD and not to the same pathological mechanism as in smokers with SP but without BHD, at least in 1 of the 5 cases with BHD the authors report the same abnormalities as in the majority of the control group. The authors conclude that.pathologists should remain vigilant when assessing ruptured pulmonary bulla/bleb and bear in mind the possibility of BHD, especially in a non-smoking woman. Although the study design and results do not support this conclusion, we do not disagree that pathologists (and clinicians) should be aware of the possibility of BHD in non-smokers with SP. However, there is no reason to assume that gender is an important factor as the hereditary pattern is autosomal dominant and it is therefore unlikely to expect a female predominance. A female gender predilection is more related to a syndrome like pulmonary LAM. What is clear from this small study is that those with a typical CT pattern (many cysts, punched-out) would have been detected by CT at the time of SP, for those with a different pattern it remains unclear. Whether this should be sufficient evidence to change the diagnostic approach of patients with first time SP needs to be discussed. 4 60
61 References 1. Fabre A, Borie R, Debray MP, Crestaine B, Danel C. Distinguishing histological and radiological features between pulmonary cystic lung disease in Birt-Hogg- Dubé syndrome and tobacco-related spontaneous pneumothorax. Histopathology 2014;65: Ren HZ, Zhu CC, Yang C, et al. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax. Clin Genet 2008: Furuya M, Tanaka R, Koga S, et al. Pulmonary cysts of Birt-Hogg-Dubé syndrome: a clinicopathologic and immunohistochemical study of 9 families. Am J Surg Pathol. 2012;36(4): MacDuff A, Arnold A, Harvey J, et al. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline Thorax 2010;65 Suppl 2:ii Clinical criteria for BHD syndrome 61
62
63 chapter 1.5 Risk of spontaneous pneumothorax due to air travel and diving in patients with Birt-Hogg-Dubé syndrome Johannesma PC 1, van de Beek 2, van der Wel JWT 1, Paul MA 3, Houweling AC 2, Jonker MA 4, van Waesberghe JHTM 5, Reinhard R 5, Starink ThM 6, van Moorselaar RJA 7, Menko FH 8, Postmus PE 9 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 3 Thoracic Surgery, VU University Medical Center, Amsterdam, The Netherlands 4 Epidemiology and Biostatistics, VU University Medical Center, Amsterdam, The Netherlands 5 Radiology, VU University Medical Center, Amsterdam, The Netherlands 6 Dermatology, VU University Medical Center, Amsterdam, The Netherlands 7 Urology, VU University Medical Center, Amsterdam, The Netherlands 8 Family Cancer Clinic, Netherlands Cancer Institute, Amsterdam, The Netherlands 9 Clatterbridge Cancer Centre, Liverpool Heart & Chest Hospital, Department of Thoracic Oncology, University of Liverpool, Liverpool, United Kingdom Accepted for publication
64 Abstract Background and Objectives Birt-Hogg-Dubé syndrome is an autosomal dominant disorder characterized by skin fibrofolliculomas, lung cysts, spontaneous pneumothorax and renal cell cancer due to germline folliculin (FLCN) mutations. The aim of this study was to evaluate the incidence of spontaneous pneumothorax in patients with BHD during or shortly after air travel and diving. 1.5 Methods A questionnaire was sent to a cohort of 190 BHD patients and the medical files of these patients were evaluated. The diagnosis of BHD was confirmed by FLCN mutations analysis in all patients. We assessed how many spontaneous pneumothoraces (SP) occurred within one month after air travel or diving. Air travel / diving in BHD patients Results In total 158 (83.2%) patients returned the completed questionnaire. A total of 145 patients had a history of air travel. Sixty-one of them had a history of SP (42.1%), with a mean of 2.48 episodes (range 1-10). Twenty-four (35.8%) patients had a history of pneumothorax on both sides. Thirteen patients developed SP <1 month after air travel (9.0%) and 2 patients developed a SP <1 month after diving (3.7%). We found in this population of BHD patients a pneumothorax risk of 0.63% per flight and a risk of 0.33% per episode of diving. Symptoms possible related to SP were perceived in 30 patients (20.7%) after air travel, respectively in 10 patients (18.5%) after diving. Conclusion Based on the results presented in this retrospective study, exposure of BHD patients to considerable changes in atmospheric pressure associated with flying and diving may be related to an increased risk for developing a symptomatic pneumothorax. Symptoms reported during or shortly after flying and diving might be related to the early phase of pneumothorax. An individualized advice should be given, taking also into account patients preferences and needs. 64
65 Introduction Changes in atmospheric pressure are related to a higher incidence of spontaneous primary pneumothorax. Atmospheric pressure changes from day to day are usually small. However, during flying or diving significant changes in pressure will occur. Therefore it might be expected that patients with a predisposition for air trapping, such as cystic lesions not connected to the airways, have a considerable risk of developing a pneumothorax. Especially in diving, pulmonary barotrauma may result in serious complications. The increased risk of pneumothorax associated with changes in atmospheric pressure can be explained by a change in transpulmonary pressure in regions with air trapping, and not in direct connection with the airways, resulting in a higher pressure compared to the atmosphere Air trapping may be caused by peripheral airway inflammation with a checkvalve mechanism resulting in obstruction of the airway. 6 7 In addition, lung cysts, emphysematous blebs or bullae may predispose to air trapping. 8 Examples of diseases with cystic lesions in the lung are lymphangioleiomyomatosis (LAM) and Birt-Hogg-Dubé syndrome (BHD). BHD is an autosomal dominant condition caused by germline mutations in the folliculin (FLCN) gene, clinically characterized by skin fibrofolliculomas, pulmonary cysts, (recurrent) spontaneous pneumothorax and an increased risk of renal cell cancer. Pneumothorax may be the first and only manifestation of BHD both in isolated and familial cases. Approximately 90% of BHD patients show multiple lung cysts on standard CT. Lung function generally remains unaffected, demonstrated by normal spirometry and diffusion capacity. 9 Detailed analysis of resected lung specimens of 50 patients with BHD containing a total of 229 cysts was performed by Kumasaka and colleagues. Of the cysts, 50 % was located in the subpleural area and less than 5% abutted bronchioles. 10 These findings imply that almost all lung cysts in BHD patients are spaces filled with air without a direct connection to airways and therefore pressure changes outside the body will not rapidly affect the amount of air within the cyst. This situation of trapped air is comparable to a bag of chips during air travel. 11 According to Boyle s law the inverse relationship between pressure and volume for gas in a closed system at a constant temperature will result in an increased size of the cyst during flying and subsequently risk of rupture of the cyst wall. During diving the pressure increases and the the cyst will decrease in size reaching pressure equilibrium during the dive. However, after reaching pressure equilibrium during the period under water, the cyst will re-expand to its original size during ascent to the surface and the risk of rupture of the cyst wall is comparable to the situation during air travel. Few data are available regarding the prevalence of pneumothorax associated with air travel in patients with the interstitial cystic lung disease lymphangioleiomyomatosis (LAM). Two studies retrospectively reviewed the occurrence of spontaneous pneumothorax related to air travel in a group of patients with LAM and found an overall incidence of pneumothorax between 1.1 and per 100 flights. These findings raise the important clinical question whether BHD patients are as well prone to develop a spontaneous pneumothorax during air travel or after diving. As there is no clear definition of air travel related pneumothorax we evaluated the prevalence of spontaneous pneumothorax and adverse events in a period of one month both after air travel and after diving. 1.5 Air travel / diving in BHD patients 65
66 1.5 Air travel / diving in BHD patients Material and methods Study population We retrospectively approached patients diagnosed in our center with BHD, confirmed by FLCN mutation analysis. A survey including a letter summarising the study was sent to the last known address to collect information on demographic data, time since BHD diagnosis, medical history, use of cigarettes and inhaled soft drugs, history of spontaneous pneumothorax, number of SP episodes, side of SP, treatment of SP, air travel and diving behaviour within one month before the SP episode and adverse effects during/after flying and/or diving (dyspnoea, chest pain, palpitations, anxiety, fatigue, nausea, dizziness, haemoptysis, headache, blue hands, shackles and/ or light headedness). To increase the response rate, a second mailing was sent to non-responders after 6 weeks. The number of flights and the number of diving episodes was divided in none, 1-5 times, 6-10, or more than 20. Air travel was divided in continental and intercontinental. Depth during diving was categorized in 0-3 metres, 3-10 metres, more than 10 metres depth. Written consent was obtained from all subjects. Medical records of the responders were collected and reviewed for radiological evidence (chest X-ray and/or thoracic CT) of spontaneous pneumothorax. In addition information regarding type of treatment of the (recurrent) spontaneous pneumothorax was collected. Radiological studies for the presence of pneumothorax and lung cysts were reviewed by a radiologist and pulmonologist. The study was approved by the ethics committee of the VU University Medical Center. Results Demographics In total 158 (83.2%) patients completed and returned the questionnaire. Of this group, 9.5% was active smoker, 42.5% former smoker (mean: 19 pack years) and 7.6% had a history of inhaling drugs. In total 145 BHD patients reported having traveled by airplane at least once. We defined a flight as a single flight including one ascent and one descent. A total of 1582 single flights in Europe (mean 10.9 flights) and 946 single intercontinental flights (mean 6.5 flights) were reported. Fifty-four patients (34.2%) had ever dived, all for recreational purposes. The majority of this group had dived between 1-5 times at a depth between 0-3 meters (56.3%). Depth was categorized in 0-3 meters (87%), 3-10 meters (48.1%), >10 meters (14.8%) Thoracic CT in BHD patients with a history of spontaneous pneumothorax after air travel or diving A thoracic CT was available for 9 patients with a history of SP after air travel (N=8) or diving (N=1). The number of cysts on standard thoracic CT varied between 1 and 140, with a mean of 57.2 cysts. The majority of cysts was located in the basal parts of the lung equally divided subpleural and parenchymal (Table 2). Whether the number of lung cysts is significantly higher in this patients group, we scored the thoracic CT s of 42 patients with BHD and a history of air travel and/or diving, but without a history of (recurrent) pneumothorax. The number of cysts on thoracic CT varied between 2 and 33, with a mean of 19 cysts. The number of cysts in patients BHD and a history of 66
67 pneumothorax was significantly higher compared to the group of patients with BHD but without a history of pneumothorax (p<0.008). Adverse events during air travel and diving Complaints reported during air travel by BHD patients (N=145), included shortness of breath (4.1%), chest pain (6.2%), palpitations (2.8%), anxiety (9.7%), abnormal fatigue (3.4%), nausea (4.1%), dizziness (0.7%), abnormal headache (3.4%), abnormal chills (1.4%) and lightheadedness (4.8%). These subjective symptoms were reported in 30 patients (20.7%) during flight. In total 54 patients had ever dived, all recreational. Depth was categorized in 0-3 meters (87%), 3-10 meters (48.1%), >10 meters (14.8%).. Subjective symptoms were reported by 10 patients (18.5%) during diving: shortness of breath (11.1%), anxiety (3.7%), dizziness (1.9%), abnormal fatigue (1.9%), abnormal chills (1.9%), and hemoptysis (1.9%). 1.5 Spontaneous pneumothorax after air travel Sixty-one of 145 BHD patients (42.1%) had a history of both SP and air travel, with a mean of 2.48 episodes of SP (range 1-10). Twenty-four patients (39.3%) had a history of (separate) episodes of spontaneous pneumothorax on both sides. Thirteen of 145 BHD patients (9.0%) developed a SP <1 month after air traveling. 24.1% had travelled intercontinental. Two patients developed a SP two times within one months after air travel. One patient developed a SP three times. For 5 patients this was the first episode of SP. The time interval between flight and radiographic diagnoses of spontaneous pneumothorax are summarized in table 1. The diagnosis of pneumothorax was confirmed in all patients with chest X-ray, additional thoracic CT was performed in 5 patients. Retrospectively a thoracic CT was available in 8 patients (table 2). Although these patients did not undergo radiographic imaging of the chest prior to their flight, we assume that these patients developed a pneumothorax during air travel as these patients had no subjective symptoms of pneumothorax before their flight. We calculated a pneumothorax risk of 0.63% per flight. Air travel / diving in BHD patients Spontaneous pneumothorax after diving Two patients out of 54 that had ever dived (3,7%) developed a SP < 1 month after diving, both after diving at depth between 3-10 meters. Although these patients did not undergo radiographic imaging of the chest prior to their diving session, we assume that these patients developed a pneumothorax during ascending to the surface, as both patients had no subjective symptoms of pneumothorax before the diving session. The first patient dived between 6-10 times at a depth of 3-10 meters. After a diving session of 30 minutes, this patient developed his first pneumothorax within 0-5 days. The second patient developed her third episode of pneumothorax after her first diving session of maximum 30 minutes at a depth of 3-10 meters, within 0-5 days (table 3). Thoracic CT was available in one patient. Both patients were treated with a VATS procedure with surgical pleurodesis (table 4). We calculated a pneumothorax risk of 0.33% per episode of session. 67
68 Table 1. Characteristics of 13 BHD patients with (recurrent) SP after air travel. Patient number Destination prior to sp Number of flights in Europe Number of flights Intercontinental Recurrent episode of sp? Episode number of sp Type of imaging diagnosis sp Time interval (in days) 1.5 Air travel / diving in BHD patients 1 Unknown >20 >20 yes 2 X thorax Europe > yes 3 X Europe > yes 4 X thorax +CT Europe >20 >20 no 1 X thorax Intercontinental >20 >20 no 1 X thorax Intercontinental >20 >20 yes 4 X thorax +CT Intercontinental >20 >20 yes 2 X thorax Europe yes 10 X thorax Europe no 1 X thorax Europe >20 0 yes 2 X thorax +CT Europe > yes 2 X thorax Europe >20 >20 yes 2 X thorax +CT Intercontinental >20 >20 no 1 X thorax Europe >20 >20 no 1 X thorax Intercontinental >20 >20 yes 2 X thorax Intercontinental >20 >20 yes 3 X thorax +CT 0-5 Table 2. Imaging and treatment characteristics of 13 BHD patients with (recurrent) SP after air travel. Patient number Thoracic ct Available Number of cysts Prior sp Prior pleurodesis Treatment sp after air travel FLCN mutation 1 yes 5 yes yes Pleurodesis c.610_611delinsta 2 yes 1 yes no Pleurodesis c.499c>t 3 n/a # n/a # yes no Pleurectomy / pleurodesis c.250-?_1740+?del (del exon 5 14) 4 yes 99 no no Tube thoracostomy c.1285dupc 5 yes 140 no no Tube thoracostomy c.1408_1418del; p.gly470fs 5 yes 140 yes yes Pleurodesis c.1408_1418del; p.gly470fs 6 yes 4 yes no Pleurodesis c.619-1g>a 7 n/a # n/a # yes no Tube thoracostomy c a>g 8 yes 74 no no Pleurodesis c a>g 9 n/a # n/a # yes no Pleural rubbing c.610_611delinsta 10 yes 19 yes yes Pleurodesis c.610_611delinsta 11 n/a # n/a # yes no Pleural rubbing c.1065_1066delgcinsta 12 n/a # n/a # no no Tube thoracostomy c.610_611delinsta 13 yes 99 no no Tube thoracostomy c.1740dupc 13 yes 99 yes no Apical pleurectomy c.1740dupc 13 yes 99 yes no Total pleurectomy and pleurodesis c.1740dupc # Not Available 68
69 Table 3. Characteristics of 2 BHD patients with (recurrent) SP after diving. Patient number Total episodes of diving* Duration of diving prior to sp Type of imaging diagnosis sp Episode number of sp Depth of diving prior to sp Time interval (in days) minutes X thorax meters minutes X thorax meters 0-5 *All episodes at 3-10 meters depth Table 4. Imaging and treatment characteristics of 2 BHD patients with (recurrent) SP after diving. Patient number Thoracic ct Available Number of cysts Prior sp Prior pleurodesis Treatment sp after air travel FLCN mutation 1 n/a # n/a # no no Pleurodesis IVS9+6 C>T and IVS8+36G>A 2 yes 74 yes Tube thoracostomy Pleurodesis c a>g 1.5 #Not Available Discussion To date, our study is the largest air travel and diving survey of patients diagnosed with BHD. In this retrospective study we analyzed the self-reported history of air travel and diving of 158 patients diagnosed with BHD. In total 13/145 (9.0%) and 2/54 (3.7%) patients developed a spontaneous pneumothorax within one month after air travel or diving respectively. In total 30/145 (20.1%) and 10/54 (18.5%) of BHD patients experienced one or more adverse events during air travel and diving respectively. We calculated a pneumothorax risk of 0.63% per flight and a pneumothorax risk of 0.33% per diving session. The literature regarding the risk for pneumothorax related to diving in patients with lung cysts is extremely limited. However, several case reports suggest a relationship between a bulla and an increased risk for pneumothorax during ascent. So far, a standardised documentation of in-flight medical and surgical emergencies (IMEs) has not been established. 15 Recommendations by several speciality society guidelines and literature reviews addressing time to travel from pneumothorax diagnosis and or treatment vary widely and show some discrepancies, which is probably due to the limited number of studies on this subject. The British Thoracic Society (BTS) guideline recommends diving to be permanently avoided after an episode of spontaneous pneumothorax unless the patient has undergone bilateral surgical pleurectomy and the lung function and postoperative thoracic CT are normal. 14 Recommended time to travel from diagnosis and/or treatment for spontaneous pneumothorax varies between no time period noted up to 21 days after radiographic resolution. Currently, there are no guidelines for patients with cystic lung diseases. We show here that the incidence of pneumothorax in BHD associated with flying and diving might be higher than in the general population and therefore recommendations with respect to air travel and diving for patients with BHD have to be established. Pneumothorax occurring in-flight appears to be rare in the general population. Coker and colleagues described the results on 500 patients with a variety of lung diseases traveling by air. No in-flight emergencies, including pneumothoraces, were reported. 15 Air travel / diving in BHD patients 69
70 Sand and colleagues identified cases of in-flight medical emergencies in a retrospective study of two European airlines; no cases of pneumothorax were documented. 16 A recent evaluation among patients by Peterson and colleagues, showed also no pneumothorax as in-flight emergency. Between 1969 and 2012 a total of 38 episodes of pneumothorax during air travel are described in literature. 17 The majority of patients had the cystic lung disease LAM as underlying disease Air travel / diving in BHD patients Whether patients diagnosed with BHD are at an increased risk for developing spontaneous pneumothorax associated to air travel or diving is unknown. So far only little data concerning BHD and air travel are available. Hoshika and colleagues surveyed a small population with BHD syndrome (N=48). None of them had experienced air travel related pneumothorax, although the length of the pneumothorax free period after air travel was not specified. 19 Hu and colleagues reported an overview of 12 reports of in-flight pneumothoraces and associated outcomes but did not specify the disease characteristics of these patients. 17 In only one study the episode of pneumothorax during the flight was fatal. 20 LAM, like BHD is a pulmonary disease associated with lung cysts. So far two studies including LAM patients reported the incidence of pneumothorax during air travel. The first study found an in-flight pneumothorax risk of 2.2% among 308 LAM patients and an estimated pneumothorax risk for LAM patients of 4% per woman flying. 12 The second study among 449 LAM patients reported an incidence of 1.1 pneumothoraces per 100 flights and 2.9 pneumothoraces per 100 patients. 11 This is a higher incidence than we found in our study. An explanation could be that BHD patients have less cysts in their lungs, as they only appear under the carina. One may question whether a pneumothorax occurring days or weeks after the event with considerable atmospheric pressure change should be considered as related to that event. The size of the connection between airway and pleural cavity is likely to determine how fast a pneumothorax will increase in size and it may therefore take days to weeks before causing symptoms. 21 To determine whether a pneumothorax indeed occurred during or directly after air travel, imaging before and directly after air travel would be required. Our choice to make an inventory of SP within one month after air travel was arbitrary and based on the assumption that these episodes may be related to flying. Based on histological evaluation of the lung cysts in BHD patients this appears to be plausible. The location of the cysts in the periphery of the lungs, at least 50% is located subpleurally and the lack of a direct connection with the intrapulmonary airways supports this theory Based on these characteristics it is unlikely that rupture of a cyst will lead to a considerable flow of air into the pleural cavity. On the contrary, if a subpleural cyst ruptures the overlying visceral pleura has to rupture as well and resulting of the release of a very small amount of air into the pleural cavity. Larger amounts of air can only get there through damage of surrounding parenchyma and/or airways in the periphery adjacent to the ruptured cyst. Ultimately the size of the connection between airway and pleural cavity determines how fast a pneumothorax will increase in size and it may therefore take days to weeks before this will lead to symptoms. 21 The more reported association between LAM and pneumothorax after air travel might be related to the disease itself. Cysts in LAM are caused by air trapping behind an obstruction of the airways Rupture of these cysts is therefore more likely to include the airway resulting in a larger connection between airway and pleural cavity than in BHD and therefore leading to symptoms earlier. 70
71 So far, a standardised documentation of in-flight medical and surgical emergencies (IMEs) has not been established. 15 Recommendations by several speciality society guidelines and literature reviews addressing time to travel from pneumothorax diagnosis and or treatment vary widely and show some disagreement, which is probably due to a lack of evidence-based support structure. Recommended time to travel from diagnosis and/or treatment for spontaneous pneumothorax varies between no time period noted up to 21 days after radiographic resolution, but is not suitable for patients with cystic lung diseases. We show that the incidence of pneumothorax in BHD, and likely in other cystic lung disease as well, is much higher than in the general population and therefore recommendations with respect to air travel for patients with BHD have to be established. Based on our current data, we suggest that patients with BHD are likely to be at an increased risk for pneumothorax while flying. Possibly, it may take several days to weeks before a pneumothorax becomes symptomatic. Patients with BHD should be advised that the presence of any clinical symptoms such as shortness of breath or chest pain, during flying or shortly after air travel might indicate a (small) pneumothorax. This should preclude flying and these persons should immediately undergo appropriate radiologic testing, by chest X-ray or thoracic CT, before being approved for air travel or diving. In summary, SP in BHD patients after air travel and diving might occur more often than in the general population. We found a pneumothorax risk of 0.63% per flight and a pneumothorax risk of 0.33% per diving episode. Although BHD is not mentioned in the BTS and ACCP guideline for pneumothorax after air travel or diving, clinicians should be aware of the possible increased pneumothorax risk in BHD patients. An individualized advice should be given, taking also into account patients preferences and needs. Further research is required to address the exact rate of pneumothorax during and directly after air travel. Preferably, a healthy control group is used to address the pneumothorax rate in the general population. Since pneumothorax during diving is reported to be associated with serious complications, and screening for cysts has been suggested in professional divers, we recommend that BHD patients are evaluated and counselled on the potentially associated risk by a physician with experience in diving medicine. 1.5 Air travel / diving in BHD patients Acknowledgements We thank all the participants in this study for their extensive contribution. 71
72 1.5 Air travel / diving in BHD patients References 1. Scott GC, Berger R, McKean HE. The role of atmospheric pressure variation in the development of spontaneous pneumothoraces. Am Rev Respir Dis. 1989; 139(3): Suarez-Varel MM, Martinez-Selva MI, Llopis- Gonzalez A, et al. Spontaneous pneumothorax related with climatic characteristics in the Valencia area (Spain). Eur J Epidemiol. 2000; 16(2): Bense L. Spontaneous pneumothorax related to falls in atmospheric pressure. Eur J Respir Dis. 1984; 65(7): Bulajich B, Subotich D, Mandarich D, et al. Influence of atmospheric pressure, outdoor temperature, and weather phases on the onset of spontaneous pneumothorax. Ann Epidemiol. 2005; 15(3): Haga T, Kurihara M, Kataoka H, et al. Influence of weather conditions on the onset of primary spontaneous pneumothorax: positive association with decreased atmospheric pressure. Ann Thorac Cardiovasc Surg. 2013; 19(3): Smit HJ, Golding RP, Schramel FM, et al. Lung density measurements in spontaneous pneumothorax demonstrate airtrapping. Chest 2004; 125(6): Cottin V, Streichenberger N, Gamonde s JP, et al. Respiratory bronchiolitis in smokers with spontaneous pneumothorax. Eur Respir J. 1998; 12(3): Edmonds C, Lowry C, Pennefather J, eds. Pulmonary barotrauma. Diving and subaquatic medicine, 3rd edn. Sydney, Australia: Butterworth- Heinemann Medical, 1992: Johannesma PC, van Waesberghe JHTM, Reinhard R, et al. Chest CT for primary spontaneous pneumothorax (PSP): findings: Birt-Hogg-Dubé versus non-birt-hogg-dubé patients. Am J Resp Crit Care Med; 189:A Kumasaka T, Hayashi T, Mitani K, et al. Characterization of pulmonary cysts in Birt- Hogg-Dubé syndrome: histopathological and morphometric analysis of 229 pulmonary cysts from 50 unrelated patients. Histopathology 2014; 65(1): Baumann MH. Pneumothorax and air travel: lessons learned from a bag of chips. Chest 2009; 136(3): Taveira-DaSilva AM, Burstein D, Hathaway OM, et al. Pneumothorax after air travel in lymphangioleiomyomatosis, idiopathic pulmonary fibrosis, and sarcoidosis. Chest 2009; 136(3): Pollock-BarZiv S, Cohen MM, Downey GP, et al. Air travel in women with lymphangioleiomyomatosis. Thorax 2007; 62(2): MacDuff A, Arnold A, Harvey J; BTS Pleural Disease Guideline Group. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline Thorax 2010; 65 Suppl 2:ii Coker RK, Shiner RJ, Partridge MR. Is air travel safe in thorse with lung disease? Eur Respir J 2007; 30: Sand M, Bechera F-G, Sand D, et al. Surgical and medical emergencies on board European aircraft: a retrospective study of cases. Critical Care 2009; 13(1):R Peterson DC, Martin-Gill C, Guyette FX, et al. Outcomes of medical emergencies on commercial airline flights. N Engl J Med 2012; 368: Hu X, Cowl CT, Baqir M, et al. Air travel and pneumothorax. Chest 2014; 145(4): Hoshika Y, Kataoka H, Kurihara M, et al. Features of pneumothorax and risk of air travel in Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med 2012; 185:A Tiemensma M, Buys P, Wadee SA. Sudden death on an aeroplane. S Afr Med J. 2010; 100(3):
73
74
75 chapter 1.6 The prevalence of Birt-Hogg-Dubé syndrome among patients with apparently primary spontaneous pneumothorax Paul C. Johannesma 1, Rinze Reinhard 2, Yael Kon 3, Jincey D. Sriram 4, JanHein T.M. van Waesberghe 2, Marianne A. Jonker 5, Theo M. Starink 3, Arjan C. Houweling 6, Quinten Waisfisz 6, Johannes J.P. Gille 6, Erik Thunnissen 7, Hans J. Smit 4, R. Jeroen A. van Moorselaar 8, Fred H. Menko 9, Pieter E. Postmus 1 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 3 Department of Dermatology, VU University Medical Center, Amsterdam, The Netherlands 4 Department of Pulmonary Diseases, Rijnstate Hospital, Arnhem, The Netherlands 5 Department of Epidemiology and Biostatistics, VU University Medical Center, Amsterdam, The Netherlands 6 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 7 Department of Pathology, VU University Medical Center, Amsterdam, The Netherlands 8 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 9 Family Cancer Clinic, Netherlands Cancer Institute, Amsterdam, The Netherlands Eur Respir J 2015;45(4):1191-4
76 Abstract Introduction Primary spontaneous pneumothorax is a common condition often associated with apical lung blebs or bullae. Birt-Hogg-Dubé syndrome (BHD) is a rare autosomal dominant predisposition due to germline FLCN mutations and characterized by skin fibrofolliculomas, basally located lung cysts, pneumothorax and renal cell cancer. At present, evaluation of PSP patients generally does not include CT thorax. We hypothesized that a minority of PSP patients may in fact have underlying BHD. 1.6 Prevalence of BHD in PSP patients Material and methods We reviewed thoracic CT scans available for 69 apparently PSP patients for the presence of basal cysts. In addition, in 40 apparently common PSP patients we performed FLCN mutation analysis, thoracic CT scanning, renal MRI and skin examination. Results Among 69 PSP cases 7 (10.1%) had multiple basal cysts, indicating possible BHD. In two patients FLCN mutation analysis was performed which revealed a pathogenic mutation in both cases. Among the 40 patients with apparently common PSP three had pathogenic germline FLCN mutations and one of these had a positive family history for pneumothorax. All three patients had multiple basal lung cysts. Asymptomatic renal cell cancer was detected in a first-degree family member of an identified BHD patient. Conclusion Among patients with apparently PSP up to 5-10% may have underlying BHD. Thoracic CT scanning may reveal the multiple basal lung cysts typical for this syndrome. Periodic renal imaging is essential for BHD patients since this may lead to early detection and treatment of BHD-associated renal cell cancer. 76
77 Introduction Pneumothorax is defined as the presence of air in the pleural cavity. If not due to an obvious external force the condition is described as spontaneous pneumothorax (SP). This common clinical condition is subdivided into secondary SP (SSP), due to various forms of lung pathology and primary SP (PSP) without indication of an underlying lung disease, and diagnosis is usually based on history and chest X-ray. The first episode of PSP most commonly occurs in the third decade of life in males who are often taller than age-matched controls and the majority has a history of smoking. Smoking increases the risk of PSP more than 100 times. 1 For several reasons, such as recurrent or persistent air leak, a chest CT can be indicated for PSP patients. In up to 90% of uncomplicated cases cystic structures, usually described as (subpleural) blebs and bullae, are found in the lung apices. 2 In a subgroup of around 5-15% of PSP patients cystic abnormalities are described in other areas of the lungs, especially below the level of the main carina, and not only in the apices. 3 Possibly these patients have a different aetiology of pneumothorax than the patients with abnormalities restricted to the apices. Multiple cysts below the level of the main carina are characteristic for Birt-Hogg-Dubé syndrome (BHD, an autosomal dominant condition caused by germline mutations in the folliculin (FLCN) gene. BHD is clinically characterized by skin fibrofolliculomas, pulmonary cysts, recurrent pneumothorax and renal cell cancer. Clinical manifestations of BHD are variable and include patients and families with only skin, lung or renal abnormalities. SP may be the first and only manifestation of BHD in isolated and familial cases. Most BHD patients have normal chest X-ray images but multiple lung cysts are commonly identified on CT; approximately 50% of the cysts are located in the subpleural area and 50% in the parenchyma. 4 Although about 90% of BHD syndrome patients have these multiple cysts, lung function (measured by spirometry and diffusion capacity) is generally normal. 4 Thus, patients with pneumothorax due to BHD often have no preceding symptoms of pulmonary disease and are therefore likely to be diagnosed as having PSP In a prospective study in a Chinese population with apparently PSP testing for FLCN mutations was performed by Ren and colleagues. A total of 10 cases of BHD were confirmed among 102 PSP cases. Eight of these ten BHD cases had 10 or more cysts on CT, but unfortunately the exact location of the cysts was not reported. 10 These findings raise the important clinical question whether all patients who present with PSP should be evaluated for BHD. To address this issue, we evaluated the presence of cysts on pulmonary CT scans in PSP patients and performed FLCN mutation analysis in 2 patients with multiple cysts and in addition, we evaluated a group of 40 patients with apparently common PSP for underlying PSP. 1.6 Prevalence of BHD in PSP patients Patients and methods Patients Review of thoracic CTs We retrospectively collected data on all patients, who had been treated for PSP at a medical university and a general hospital (VU University Medical Center, Amsterdam and Rijnstate Hospital, Arnhem, the Netherlands) in the years Patients diagnosed with PSP according to the 77
78 criteria proposed by the British Thoracic Society were included when they were over the age of 18 years at the time of diagnosis. Exclusion criteria were secondary pneumothorax due to apparent underlying disease, traumatic or iatrogenic pneumothorax. Furthermore, deceased patients were excluded (figure 1). All thoracic CTs, made within 1 year before or after the PSP, were collected and scored by one pulmonologist (PEP) for the presence of abnormalities in the completely inflated lung or lungs. Clinical information was not available at the time of scoring. 1.6 Prevalence of BHD in PSP patients Evaluation for BHD characteristics For the second part of the study a questionnaire was sent to the last known address of in total 316 patients registered in the VUMC database under the diagnosis of PSP. Additional information on medical history (respiratory, dermatological, urological disease), any additional episodes of pneumothorax and treatment, treatment complications, history of smoking, history of drug use and family history of spontaneous pneumothorax were collected (n=93) (figure 1). All these participants (n=42) gave written informed consent. During an out-patient visit physical examination of the skin was performed by a dermatologist familiar with BHD, a blood sample was taken for FLCN mutation analysis and thoracic CT scanning was performed. In addition, all patients with a positive familial history for pneumothorax underwent an Figure 1. Flowchart study protocol BHD-P study. 78
79 renal MRI. Renal MRI was also offered to those in whom a pathogenic FLCN mutation was identified. Subsequently families of the patients diagnosed with BHD were invited for genetic counselling. This study was approved by the ethics committee of the VU University Medical Center (NL ). All patients provided written informed consent. Mutation analysis For FLCN mutation analysis genomic DNA was extracted from blood samples. Primers for the amplification and sequencing of the 14 exons were designed as detailed by Nickerson et al. 11 PCR amplification was performed using a PE 9700 thermocycler (Applied Biosystems, Forster City, CA, USA). Sequencing reactions were performed using the Big Dye Terminator system (Applied Biosystems) and run on an ABI 3100XL or ABI 3730 genetic analyzer (Applied Biosystems). For the detection of deletions and duplications of one or more exons MLPA analysis was performed using MLPA kit P256 (MRC Holland, Results CT evaluation of PSP patients The main characteristics of the 69 radiological scored patients are summarized in Table 1. Between 2000 and 2012 a total of 96 patients underwent one or more thoracic CT s for spontaneous pneumothorax. After exclusion of 6 non-evaluable cases (e.g. due to incomplete imaging of the thoracic CT) and 21 cases reclassified as having secondary SP, a total of 69 patients were eligible for scoring (figure 1). The mean age was 37.6 years, the recurrence rate was 28.2% and positive family history for SP was noted in 16.2% of cases. A family history for renal cell cancer or skin fibrofolliculomas was reported in none of the 316 medical records. Almost half of the patients had at least one cyst on thoracic CT, of which the majority was located above the carina. Among the 69 cases with PSP scored for lung cysts on thoracic CT, 14 patients (20.3%) showed one or more cysts below the carina. In 7 patients >50% of the lung cysts were present below the carina and therefore indicative for Birt-Hogg-Dubé syndrome (figure 2). In two of these patients the diagnosis BHD syndrome had been confirmed previously by FLCN mutation analysis. For the other 5 patients FLCN mutation analysis was not available. The main characteristics of the 7 patients are summarized in Table 2. Two patients had a history of renal cell cancer. The first patient with 1.6 Prevalence of BHD in PSP patients Table 1. Characteristics of primary spontaneous pneumothorax patients with available thoracic CT. Main characteristics of the 69 psp patients with available thoracic ct n (%) Male gender 52 (75.4) 1 cysts on thoracic CT 32 (46.4) 1 more cysts above carina 28 (40.6) 1 cysts under carina 14 (20.3) Mean number of cysts above carina 5.37 Mean number of cysts under carina % of cysts under carina 7 (10.1) 79

80 A B 1.6 Figure 2. High resolution computed tomography of the chest of a non-tested PSP patient, clinically suspected for Birt- Hogg-Dubé syndrome. The coronal and transversal coupe show multiple round and oval thin-walled pulmonary cysts of varying sizes, localized mostly in the lower lobes of both lungs. Prevalence of BHD in PSP patients Table 2. Characteristics of the seven spontaneous pneumothorax patients with >50% of cysts under the carina. Patient Gender (Age at first psp) Recurrence of psp Number of recurrences of psp Number of lung cysts under carina (%) of cysts under carina Renal cell cancer (Age at diagnosis) Fibrofolliculomas Positive family history of sp FLCN mutation 1 M (24) yes % Yes (44) no no c.510c>g; p.tyr170x) 2 F (20) yes % no no no c.610_611delgcinsta p.ala240x 3 M (62) no % n/a n/a n/a Not tested 4 M(75) no % Yes (74) n/a n/a Not tested 5 M (20) yes % n/a n/a n/a Not tested 6 M (29) no % n/a n/a n/a Not tested 7 F (52) no % n/a n/a No Not tested a proven pathogenic FLCN mutation had spontaneous pneumothorax at age 24 and developed renal cell cancer at the age of 44. After needle biopsy, histopathology showed a chromophobe renal cell carcinoma. The patient was treated with radiofrequency ablation (RFA). For the second patient with renal cell carcinoma, FLCN mutation analysis was not available. This patient with an unremarkable medical history - was evaluated for haematuria at the age of 74. Computed tomography (CT) of the abdomen showed an interpolar tumour in the right kidney (diameter of 10 cm) with lymph nodes metastasis and therefore classified as T3N2M1. The tumour was removed during an uncomplicated total nephrectomy procedure. Histopathology showed a chromophobe renal cell carcinoma, Fuhrman grade 4. Twelve months later the patient developed a spontaneous pneumothorax. 80
81 Evaluation for presence of BHD In total 93 patients returned a completed questionnaire and 42 of them gave written informed consent to be contacted for further studies (outlined in the right arm of Figure 1). The final study group consisted of 40 cases after exclusion of two patients with extensive bullous emphysema on thoracic CT who were reclassified as having SSP. The main characteristics of the 40 patients are summarized in Table 3. Three patients had a pathogenic FLCN mutation (7.5%, 95% confidence interval 1.5% 20.3%). Details of these patients are provided in Table 4 and the pedigrees are shown in Figure 3. The FLCN mutations detected in these patients were a nonsense mutation, c.610_611delgcinsta (p.ala240x), a frameshift mutation, c.1408_1418del (p.gly470fs) and a splice site mutation, c a>g. The thoracic imaging performed in these three patients is shown in Figure 4. For index patient B the histological picture of a basal lung cyst for which bullectomy was performed is shown in Figure 5. Family members of the three probands with BHD were invited for genetic counselling and given the option for pre-symptomatic DNA testing and further clinical evaluation. We identified four additional FLCN mutation carriers (one in families A and B and two in family C). Renal MRI in a first- 1.6 Table 3. Main characteristics of the 40 BHD-P study participants. Main characteristics of the 40 study participants n (%) Male gender 25 (62.5) History of smoking 29 (72.5) Pack years (range) 7.68 (1-50) History of drug abuse 11 (27.5) Mean age at first pneumothorax (range) 33.8 (18-78) Recurrence of pneumothorax 19 (47.5) Mean number of recurrences (range) 1.6 (1-12) Positive family history of pneumothorax 7 (17.5) Pathogenic FLCN mutation 3 (7.5) Prevalence of BHD in PSP patients Table 4. Characteristics of the three spontaneous pneumothorax patients who had pathogenic FLCN mutations. Patient (Fam. no) Gender (Age first psp) Delay between first symptom (psp) and final diagno- Recusis BHD(in rrence months) of psp Number of recurrences of psp Number of lung cysts Renal tumor ff Smoking history flcn mutation 1 (84) F (20) 243 yes 8 13 no Minimal* no c.610_611delgcinsta (p.ala240x) 2 (85) M (26) 153 yes no Minimal* no c.1408_1418del (p.gly470fs) 3 (94) M (40) 81 yes 3 74 no no no c a>g * Very subtle minimal facial skin lesions, probably fibrofolliculomas. Clinical diagnoses, skin biopsy for histopathology not performed. 81
82 A 1.6 Prevalence of BHD in PSP patients B Figure 3. Pedigrees of families A, B and C. Symbols: in black: right upper quadrant: pneumothorax, right lower: multiple lung cysts, left upper: skin fibrofolliculomas, left lower: renal cell cancer; Family A, patient II-7 and family B, patient III-6: affected according to family history. C 82




83 A B 1.6 C Figure 4. High resolution computed tomography of the chest in the three patients with proven BHD revealed multiple round and oval thin-walled pulmonary cysts of varying sizes, localized mostly in the lower lobes, which abutted to or enclosed the proximal portions of lower pulmonary arteries and veins. Prevalence of BHD in PSP patients A B Figure 5. Histopathology of a lung cyst of the index patient of family B. The cyst walls are completely lined by pneumocytes. The inner surfaces of the cysts stained positively for TTF-1 expression. 83
 in the lower pole of the right kidney, compatible with a small renal cell cancer.")
84 1.6 Prevalence of BHD in PSP patients Figure 6. Renal CT scan in patient III-IV, family C, showed a 15-mm solid mass (arrow) in the lower pole of the right kidney, compatible with a small renal cell cancer. degree relative in family C who was a proven FLCN mutation carrier revealed a 15-mm solid mass in the lower pole of the right kidney, compatible with a small renal cell cancer, shown in Figure 6. The patient underwent an uncomplicated nephron sparing therapy revealing a clear cell renal cell carcinoma. The outcomes of all investigations are summarized in Table 4. Among the 37 cases with PSP who showed no pathogenic FLCN mutation, blebs and bullae in the apical lung parts were seen in 21 (56.8%) patients, in none of these patients cysts were found in the basal parts of the lungs. The six patients without pathogenic FLCN mutation but with a positive family history for PSP showed no skin abnormalities or abnormalities on renal MRI. Discussion In this study we evaluated a group of 40 PSP patients with apparently common PSP for the presence of BHD and found three (7.5) positive cases, which is in line with the findings previously reported for a Chinese population group by Ren et al. 10 All three cases had the typical pulmonary features of BHD, i.e. multiple lung cysts, localized in the basal parts of the lungs. Apical blebs and bullae which are common in non-hereditary PSP were absent in these three cases. In contrast, among the 37 non-hereditary PSP cases 21 patients (56.8%) showed these apical lung abnormalities. Our retrospective evaluation of CTs of PSP patients underscores these findings since among 69 patients seven had predominantly basal lung cysts and two of these had proven BHD. This also indicates that in the common PSP study group indicating that the prevalence of BHD among PSP patients may be up to 5-10%. The three patients with a pathogenic FLCN mutation had undergone one or more thoracic CT s prior to our study. Although in retrospect lung cysts were visible on these scans, BHD was not suspected previously. With current knowledge, the multiple lung cysts combined with the recurrent episodes of pneumothorax would have been a reason to consider FLCN analysis at an earlier stage. A positive family 84
85 history for SP could also have been a reason for the treating pulmonologist to consider referring a patient to a clinical genetics outpatient clinic, but this is not recommended in current BTS or ACCP guidelines. Among the group of 69 PSP patients scored for the presence of lung cysts, we found in 7 patients (10.1%) a majority of cysts located under the carina. BHD was confirmed by FLCN mutation analysis in two patients and was clinically suspected in five patients. Among these seven patients, renal cell cancer was found in two patients, one of whom had a pathogenic FLCN mutation. The histopathology in the second patient revealed a chromophobic renal cell tumour, which is suggestive for BHD. Pneumothorax, the occurrence of air in the pleural cavity, is a common condition with a high incidence of between 1.2 and 18 cases per persons per year. 13 The diagnosis is suggested by patient s history and findings on physical examination and is in most cases confirmed by a standard erect chest X-ray during inspiration. Thoracic CT scanning is currently only recommended for uncertain or complex cases. 14 In PSP subpleural blebs/bullae are found among more than 76% of patients during video-assisted thoracoscopic surgery. 14 These cysts cannot be visualized by standard chest X-ray and the relationship between these blebs/bullae and the development of pneumothorax has not been fully clarified. 15 Following the current guidelines, underlying lung pathology as cause for SP might remain undiagnosed. Although cystic lesions on CT scanning in PSP patients have been reported, the location of these cysts has not been studied extensively. 16 In a rather dated study a prevalence of cystic structures present only below the level of the carina was reported in 8.4% (5 out 59 cases). 3 Whether these abnormalities were related to a different aetiology was not investigated at that time. The expression of BHD is variable and patients may present with isolated pneumothorax The variation in clinical presentation is probably not due to specific gene defects since clear genotype phenotype correlations have thus far not been demonstrated in this syndrome. Patients with BHD who develop pneumothorax have multiple basal lung cysts in the majority of cases, although the presence of cysts does not per se result in pneumothorax. Approximately 90% of BHD patients have these lung cysts whereas only 24% of BHD cases develop a pneumothorax. 16 The relationship between these cysts and the pathogenesis of pneumothorax has not been clarified yet. In our cohort of BHD families most probands were referred by their dermatologist after the diagnosis of multiple skin fibrofolliculomas. On reviewing these families we found many cases with pneumothorax that had been diagnosed initially as having common PSP This is to be expected given the lack of pulmonary symptoms and normal lung function in BHD patients. 20 Therefore, we hypothesized that common PSP may be diagnosed in cases that in fact have BHD. Furthermore there might be an overlap in radiological abnormalities between BHD- and smoking related PSP BHD is reported to be increased in patients who report a positive family history for pneumothorax. There are several strengths and limitations of our study. This is the first study in a European population. As the selection of cases for further testing in this study was done by voluntary participation, the tested group (N=40) might be different from the standard PSP population although the mean age, recurrence rate and percentage with a positive history for SP was comparable to the initial selected PSP group of 316 patients and in none of the included patients a family history of renal cancer was present (which would assumedly have resulted in a higher chance of participation to the study). Our 1.6 Prevalence of BHD in PSP patients 85
86 retrospective evaluation of CTs of PSP patients more or less confirms our earlier findings and might implicate that the prevalence of abnormalities indicating potential BHD on CTs of PSP patients is around 5-10%. This percentage is comparable to the (limited) available literature. In the study by Ren and colleagues, eight confirmed BHD patients had 10 or more lung cysts; two had one and three cysts, respectively. This observation shows that multiple basal lung cysts may be absent in BHD patients and we and others have made the same observation. The association of BHD with multiple lung cysts was previously shown in a Japanese study in eight patients with multiple lung cysts, seven of whom had had recurrent pneumothorax, five of them had BHD. 27 Other authors have selected patients with familial pneumothorax and demonstrated that familial pneumothorax without other signs of BHD may indeed indicate BHD. 1.6 Prevalence of BHD in PSP patients Patients with BHD have an increased risk of renal cell cancer. We calculated a 16% renal cancer risk until the age of 70 years. 17 Periodic renal imaging may result in early detection and treatment of BHD associated renal cell cancer. Therefore diagnosing BHD as early as possible may have consequences not only for the BHD patient presenting with pneumothorax, but also for their relatives. Indeed, a first-degree relative of one of the three probands carrying the FLCN mutation identified in our proband had an early stage solid small renal cell tumour and was treated successfully. Calculations based on literature and our database indicate that of 100 BHD cases diagnosed through the presence of SP around 60 cases of RCC will be detected during lifelong follow-up by MRI of the affected PSP patients and detected family members. 31 The three cases reported in our study lacked other signs of the syndrome. None had the typical skin fibrofolliculomas and two had a negative family history for pneumothorax. Absence of skin abnormalities and a negative family history for pneumothorax therefore do not exclude BHD and DNA testing may therefore be needed to diagnose this syndrome. The suspicion of BHD would have been much higher if at the time of diagnosis of PSP additional thoracic CT imaging would have been analysed for the presence of basal cysts. The main limitations of our study are the low response rate and a possible selection of cases. The response rate was low, since only 40 out of a total group of 316 patients (9.9%) were fully examined. Patients who were invited for the study may preferentially have opted for this possibility due to certain characteristics for example young age at diagnosis, high recurrence rate or a positive family history for the disease. In addition, after being informed on the characteristics of BHD patients with skin lesions or with a personal or family history of pneumothorax of renal cancer may have encouraged individuals to participate. As the results of the group of 40 patients is comparable both with the scored thoracic CT group (N=69) and the much larger study by Ren and colleagues in consecutive cases with PSP, selection bias may not have been a major factor in our study. An important argument to diagnose BHD at an early stage might be the high recurrence rate of PSP which might prompt a different and more aggressive therapeutic approach. 32 Based on these results we advocate that prospective studies should lead to further insights in the prevalence of BHD in PSP, any differences in response to therapy of pneumothorax and the optimal diagnostic tools in diagnosing BHD among apparently non hereditary PSP cases. The most attractive diagnostic routine for PSP patients may consist of thoracic CT as the first test, followed by 86
87 dermatological examination, family history taking and FLCN mutation analysis in patients suspected for BHD based on the findings on CT scan or their (family) history. In summary, BHD among apparently PSP patients is probably not a rare event. In our PSP group we identified a FLCN mutation in 3/40 (7.5%) patients. Although Birt-Hogg-Dubé is not mentioned in the BTS and ACCP guideline for pneumothorax, clinicians should be aware of this disease in the apparently common spontaneous pneumothorax population. Further research is required to address the question whether current diagnostic procedures in spontaneous pneumothorax should be changed, in order to allow detection of BHD - with its corresponding increased risk on RCC at an early stage. 1.6 Prevalence of BHD in PSP patients 87
88 1.6 Prevalence of BHD in PSP patients References 1. Bense L, Eklund G, Wiman LG. Smoking and the increased risk of contracting spontaneous pneumothorax. Chest 1987;92(6): Donahue DM, Wright CD, Viale G, Mathisen DJ. Resection of pulmonary blebs and pleurodesis for spontaneous pneumothorax. Chest 1993; 104(6): Smit HJ, Wienk MA, Schreurs AJ, Schramel FM, Postmus PE. Do bullae indicate a predisposition for recurrent pneumothorax? Br J Radiol 2000;73(868): Johannesma PC, van Waesberghe JHTM, Reinhard R, Gille JJP, van Moorselaar RJA, Houweling AC, Menko FH, Postmus PE. Chest CT for primary spontaneous pneumothorax (PSP): findings: Birt- Hogg-Dubé versus non-birt-hogg-dubé patients. Am J Resp Crit Care Med;189:A Johannesma PC, Lammers JW, van Moorselaar RJ, Starink ThM, Postmus PE, Menko FH. Spontaneous pneumothorax as the first manifestation of a hereditary condition with an increased renal cancer risk. Ned. Tijdschr Geneeskd. 2009;153:A Pierce CW, Hull PR, Lemire EG, Marciniuk DD. Birt-Hogg-Dubé syndrome: an inherited cause of spontaneous pneumothorax. CMAJ 2011;183(9):E Verhaert LL. A young man with bilateral spontaneous pneumothorax. Case Rep Pulmonology. 2011;2011: Hopkins TG, Maher ER, Reid E, Marciniak SJ. Recurrent pneumothorax. Lancet 2011;377(9777): Johannesma PC, Thunnissen E, Postmus E. Lung cysts as indicator for Birt-Hogg-Dubé syndrome. Lung 2014l1952(1): Ren HZ, Zhu CC, Yang C, Chen SL, Xie J, HouYYm, Xu ZF, Wang DJ, Mu DK, Ma DH, Wang Y, Ye ZR, Chen BF, Wang CG, Lin J, Qiao D, Yi L. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax. Clin Genet 2008; 74(2): Nickerson ML, Warren MB, Toro JR, Matrosova V, Glenn G, Turner ML, Duray P, Merino M, Choyke P, Pavlovich CP, Sharma N, Walther M, Munroe D, Hill R, Maher E, Greenberg C, Lerman MI, Linehan WM, Zbar B, Schmidt LS. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg- Dubé syndrome. Cancer Cell 2002; 2(2): Baumann MH, Strange C, Heffner JE, Light R, Kirby TJ, Klein J, Luketich D, Panacek EA, Sahn SA, for the ACCP Pneumothorax Consensus group. Management of Spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest 2001;119(2): Sahn SA, Heffner JE. Spontaneous pneumothorax. N Engl J Med 2000; 342(12): MacDuff A, Arnold A, Harvey J; BTS Pleural Disease Guideline Group. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline Thorax 2010; 65 Suppl 2:ii18-ii Schramel FM, Postmus PE, Vanderschueren RG. Current aspects of spontaneous pneumothorax. Eur Respir J 1997; 10(6): Lesur O, Delorme N, Fromaget JM, Bernadac P, Polu JM. Computed tomography in the etiologic assessment of idiopathic spontaneous pneumothorax. Chest 1990;98(2): Toro JR, Pautler SE, Stewart L, Glenn GM, Weinreich M, Toure O, Wei MH, Schmidt LS, Davis L, Zbar B, Choyke P, Steinberg SM, Nguyen DM, Linehan WM. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg- Dubé syndrome. Am J Respir Crit Care Med 2007; 175(10): Houweling AC, Gijezen LM, Jonker MA, van Doorn MB, Oldenburg RA, van Spaendonck-Zwarts KY, Leter EM, van Os TA, van Grieken NC, Jaspars EH, de Jong MM, Bongers EM, Johannesma PC, Postmus PE, van Moorselaar RJ, van Waesberghe JH, Starink TM, van Steensel MA, Gille JJ, Menko FH. Renal cancer and pneumothorax risk in Birt- Hogg-Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer 2011; 105(12): Leter EM, Koopmans AK, Gille JJ, van Os TA, Vittoz GG, David EF, Jaspars EH, Postmus PE, van Moorselaar RJ, Craanen ME, Starink TM, Menko FH. Birt-Hogg-Dubé syndrome: clinical and genetic studies of 20 families. J Invest Dermatol 2008; 128(1): Sundaram S, Tasker AD, Morrell NW. Familial spontaneous pneumothorax and lung cysts due 88
89 to a Folliculin exon 10 mutation. Eur Respir J 2009; 33(6): Fabre A, Borie R, Debray MP, Crestani B, Danel C. Distinguishing the histological and radiological features of cystic lung disease in Birt-Hogg- Dubé syndrome from those of tobacco-related spontaneous pneumothorax. Histopathology (5): Johannesma PC, Thunnissen E, Postmus PE. How reliable are clinical criteria to distinguish between BHD and smoking as a cause for pneumothorax? Histopathology 2014;64(7): Fröhlich BA, Zeitz C, Mátyás G, Alkadhi H, Tuor C, Berger W, Russi EW. Novel mutations in the folliculine gene associated with spontaneous pneumothorax. Eur Respir J 2008;32(5): Agarwal PP, Gross BH, Holloway BJ, Seely J, Stark P, Kazerooni EA. Thoracic CT findings in Birt- Hogg-Dubé syndrome. AJR Am J Roentgenol 2011; 196(2): Menko FH, Johannesma PC, van Moorselaar RJ, Reinhard R, van Waesberghe JH, Thunnissen E, Houweling AC, Leter EM, Waisfisz Q, van Doorn MB, Starink TM, Postmus PE, Coull BJ, van Steensel MA, Gille JJ. A de novo FLCN mutation in a patient with spontaneous pneumothorax and renal cancer; a clinical and molecular evaluation. Fam Cancer 2013; 12(3): Tomassetti S, Carloni A, Chilosi M, Maffe A, Ungari S, Sverzellati N, Gurioli C, Casoni G, Romagnoli M, Gurioli C, Ravaglia C, Poletti V. Pulmonary features of Birt- Hogg-Dubé syndrome: cystic lesions and pulmonary histiocytoma. Respir Med 2011; 105(5): Gunji Y, Akiyoshi T, Sato T, Kurihara M, Tominaga S, Takahashi K, Seyama K. Mutations of the Birt Hogg Dubé gene in patients with multiple lung cysts and recurrent pneumothorax. J Med Genet 2007; 44(9): Graham RB, Nolasco M, Peterlin B, Garcia CK. Nonsense mutations in folliculin presenting as isolated familial spontaneous pneumothorax in adults. Am J Respir Crit Care Med 2005; 172(1): Painter JN, Tapanainen H, Somer M, Tukiainen P, Aittomaki K. A 4-bp deletion in the Birt-Hogg- Dubé gene (FLCN) causes dominantly inherited spontaneous pneumothorax. Am J Hum Genet 2005; 76(3): Yang CY, Wang HC, Chen JS, Yu CJ. Isolated familial pneumothorax in a Taiwanese family with Birt-Hogg-Dubé syndrome. J Postgrad Med 2013; 59(4): Johannesma PC, Houweling AC, Reinhard R, Thunnissen E, Menko FH, van Waesberghe JHTM, Paul MA, Horenblas S, van Moorselaar RJA, Postmus PE. Early detection of hereditary renal cell cancer by improved evaluation of spontaneous pneumothorax patients. Abstract ESMO congress (accepted) 32. Postmus PE, Johannesma PC, Menko FH, Paul MA. In-flight pneumothorax: diagnosis may be missed due to symptom delay. Am J Respir Crit Care Med Sep 15;190(6): Prevalence of BHD in PSP patients 89
90
91 chapter 1.7 International guidelines for pneumothorax are not adequate for treatment of spontaneous pneumothorax in patients with Birt-Hogg-Dubé syndrome Paul C. Johannesma 1, Marinus A. Paul 2, JanHein T.M. van Waesberghe 3, Marianne A. Jonker 4, Arjan C. Houweling 5, Irma van de Beek 5, Theo M. Starink 6, R. Jeroen A. van Moorselaar 7, Fred H. Menko 8, Pieter E. Postmus 9 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Thoracic Surgery, VU University Medical Center, Amsterdam, The Netherlands 3 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 4 Department of Epidemiology and Biostatistics, VU University Medical Center, Amsterdam, The Netherlands 5 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 6 Department of Dermatology, Leiden University Medical Center, Leiden, The Netherlands 7 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 8 Family Cancer Clinic, Netherlands Cancer Institute, Amsterdam, The Netherlands 9 Department of Thoracic Oncology, Clatterbridge Cancer Centre, Liverpool Heart & Chest Hospital, University of Liverpool, Liverpool, United Kingdom Submitted
92 Abstract An important genetic cause of spontaneous pneumothorax is Birt-Hogg-Dubé syndrome (BHD), caused by mutations in the folliculin (FLCN) gene. It is suggested that approximately % of all spontaneous pneumothorax (SP) patients may have this underlying disorder. As the recurrence rate of SP in BHD has been described to be as high as 75%, we evaluated the effect of different types of treatment. Current BTS and ACCP guidelines do not describe the treatment of SP in BHD patients as a separate entity. In this study we compared the results of treatment in a comparable group of BHD and non-bhd patients with (recurrent) SP. We found a recurrence rate of 64.5% after conservative treatment and a recurrence rate of 11.1% after invasive treatment of SP in BHD patients. This recurrence rate was significant higher when compared to patients without BHD. Therefore invasive treatment seems to be the better option for BHD patients with (recurrent) SP. Our results suggest that SP in BHD is an associated with a high recurrence rate after conservative treatment and an invasive therapy would therefore be the best approach in this group. 1.7 Treatment options for sp in BHD patients 92
93 Introduction Pneumothorax is defined as the presence of air in the pleural cavity. If not due to an obvious external force, the condition is described as spontaneous pneumothorax (SP). This common clinical condition is subdivided into secondary SP (SSP) - due to various forms of lung pathology - and primary SP (PSP) without indication of an underlying lung disease. This distinction is usually based on medical history and chest X-ray at first presentation. 1 In a minority of cases a positive family history is reported in individuals who present with a SP. A possible genetic cause of familial SP in this situation is the Birt-Hogg-Dubé syndrome (BHD), due to pathogenic mutations in FLCN. Two recent studies showed that approximately % of all SP patients may have an underlying pathogenic FLCN mutation. 2 3 While the recurrence rate in common primary SP has been described up to 50% when treated conservative, the recurrence rate of SP among BHD patients has been reported to be much higher, up to 75%, despite different types of treatment. 1 4 Current international pneumothorax guidelines e.g. by the British Thoracic Society (BTS) and the American College of Chest Physicians (ACCP), do not distinguish common SP due to BHD as separate entity, and also in current published literature the optimal treatment of SP in patients with BHD has not been evaluated so far. 1,5 Therefore we evaluated the recurrence rate and different treatment options of SP in BHD patients compared to SP patients without a pathogenic FLCN mutation. Material and methods We collected data by sending a questionnaire to 54 patients with a proven pathogenic FLCN mutation and a history of (recurrent) SP. Forty patients consented to the study and of 38 patients the medical treatment details were available (Table 1, Table 2). As a control group, we included 47 randomly selected primary SP patients, who tested negative for a mutation in FLCN. To complete the dataset, we collected all data from their medical charts, after written informed consent. All included patients had one or more episodes of SP. We scored on general demographics, number of episodes, side of SP, number of recurrences and type of treatment classified in conservative (one time needle aspiration or tube thoracostomy) or invasive (chemical - or mechanical pleurodesis, (partial) pleurectomy, lobectomy, bullectomy, or a combination of invasive treatment options). Both lungs were scored separately. The Chi-square test was used for the qualitative variables. All statistical analyses were performed using SPSS software (version 20, SPSS Inc., Chicago IL, USA). A p-value of less than 0.05 was considered significant. The study was approved by the Ethics Committee of the VU University Medical Center. 1.7 Treatment options for sp in BHD patients Results We found no significant difference in gender or mean age at first episode of SP between the FLCN mutation positive- and negative groups. The mean number of episodes of SP was significantly higher among patients with BHD, with a mean of 2.85 episodes versus 1.94 episodes in the non-bhd group. Also the number of episodes of pneumothorax in both lungs (not at the same time) or same lung was significantly higher in the group of 40 BHD patients (table 1). The mean age in the BHD and 93
94 Table 1. Spontaneous pneumothorax in BHD and non-bhd patients. FLCN mutation + FLCN mutation - P-value (N=) (%=) (N=) (%=) Included patients with available medical information and informed consent Male : Female 19 : : : : 38.3 NS # Mean age (min-max) 32.2 (14-54) 31.6 (16-78) NS # Mean number of spontaneous pneumothorax (min-max) 2.85 (1-10) 1.94 (1-5) < Treatment options for sp in BHD patients Diagnosed first episode SP in: Left lung Right lung Bilateral (same time) Both lungs; separate episodes Total first episodes (left + right sided pneumothorax) Total episodes of pneumothorax (left and right lung) Right lung Left lung # Not significant β Calculated with X 2 test <0.05 non-bhd group was almost the same; 32.2 years (14-54 years) versus 31.6 years of age (16-78 years). The mean number of SP was 2.85 (1-10 episodes) among BHD patients and was significantly higher compared to patients without BHD, with a mean of 1.94 episodes of SP (1-5). We studied the number of SP episodes for each FLCN mutation. The number of included patients carrying the same pathogenic FLCN mutation varied between 1 and 23 patients. The pathogenic nonsense mutation in exon 6 (c.610_611delgcinsta) was found most often and was identified in seven different families. In one family, eight relatives with a history of (recurrent) SP carried mutation c a>g with a history of (recurrent) SP. Recurrence of SP occurred in 64.5% BHD patients after conservative treatment, which was significant higher when compared to the SP patients without BHD with a recurrence rate of 48.6%. Immediate invasive treatment after a first episode of SP was performed in BHD patients more frequently when compared to SP patients without BHD (46.6% versus 31.5%, p<0.05). Various types of invasive treatment for pneumothorax showed good results in both BHD and non-bhd patient groups. Especially the long-term results (>12 months) after invasive treatment gave good results in the group of patients without BHD. Partial pleurectomy was not effective in all treated BHD patients 94
95 Table 2. Effect of type of treatment in BHD and non-bhd patients with a (recurrent) episode of SP. Number of included patients* (N=) Type of treatment not available (N=) 2 # 0 FLCN mutation + FLCN mutation - P-value β (N=) (%=) (N=) (%=) Choice of treatment after first SP (N= both lungs) Conservative Invasive 31/58 # /58 # /54 & /54 & 31.5 <0.05 Conservative treatment of first SP No recurrence Recurrence within 1 months Recurrence within 1-12 months Recurrence within >12 months Total recurrence Invasive treatment of first SP (via thoracoscopy or VATS) No recurrence Recurrence within 1 months Recurrence within 1-12 months Recurrence within >12 months Total recurrence No recurrence after treatment: Conservative (one time aspiration / tube thoracostomy) (Talc) pleurodesis Partial pleurectomy Total pleurectomy Bullectomy Lobectomy Combined invasive (bullectomy/ pleurectomy/pleurodesis) 11/31 7/31 4/31 9/31 20/31 24/27 1/27 0/27 2/27 3/27 12/53 20/28 0/3 4/4 0/2 NP $ 22/ NP $ /37 4/37 6/37 8/37 18/37 16/17 1/17 0/17 0/17 1/17 18/46 24/26 2/2 2/2 4/6 NP $ 4/ NP $ 57.1 <0.05 <0.05 <0.05 <0.05 NS # NS # <0.05 NS <0.05 NA & < Treatment options for sp in BHD patients *With completed information from questionnaire and patients charts and after informed consent. $ Not performed, & Not available, # Not significant β Calculated with X 2 test # See table 1. In total 60 included separated lungs. In two patients with one sided pneumothorax no type of treatment known, therefore 60-2=58 included lungs with known type of treatment. & See table 1 for inclusion. and also bullectomy resulted in recurrent episodes of SP in all BHD patients. Combined invasive treatment or total pleurectomy resulted in excellent results in BHD patients. In non BHD patients all type of invasive treatment resulted in good (long term) results. 95
96 1.7 Treatment options for sp in BHD patients Discussion In this study we compared a group of 54 pneumothorax patients with a pathogenic FLCN mutation with 47 pneumothorax patients without a pathogenic FLCN mutation. The main finding was the significant higher number of recurrent episodes of spontaneous pneumothorax in BHD patients compared to non-bhd patients, despite several types of treatment. We found a recurrence rate of 64.5% in our BHD cohort, which is comparable with current literature. 6 Invasive treatment as pleurodesis, total pleurectomy or a combination of both gave good results in both groups (table 2). Recurrent episodes of pneumothorax were found in all BHD patients after bullectomy and partial (apical) pleurectomy. This seems explainable, as cysts in the basal parts of the lung are, very likely, often responsible for pneumothorax, and bullectomy or partial pleurectomy is only performed in the lung apices. 7 8 In current literature very little information is available on treatment of pneumothorax among BHD patients. In some papers surgical intervention with resection and pleurodesis is suggested to be an acceptable option, even in BHD patients with a first episode of pneumothorax These suggestions are only based on the somewhat comparable (progressive) cystic lung disease lymphangioleiomyomatosis (LAM). 12 Pulmonary LAM is characterized by recurrent pneumothoraces (in 50-60% of mainly female patients), chylothorax, progressive dyspnoea and pleural effusions This progressive lung disorder differs from BHD as pneumothorax occurs in approximately 30% of FLCN mutation carriers, and the lung function remains unaffected despite multiple cysts in the basal parts of the lung. The similarity between LAM and BHD is the high recurrence rate of up to 75% for pneumothorax, comparable to the 64.5% recurrence rate we found in our BHD population. Current guidelines for the treatment of spontaneous pneumothorax differ enormously and are based on older literature (BTS, ACCP). 1 5 Recommendations on the treatment of interstitial lung diseases as BHD or LAM are not discussed in these pneumothorax guidelines. In a recently published Cochrane review on conservative versus interventional management for primary spontaneous pneumothorax it was concluded that there is no strong evidence for interventional management of PSP, despite widespread practice and recommendation. 15 So far no gender predilection has been found in BHD with regards to development of pneumothorax. Age and smoking status are not associated with pneumothorax in literature, in accordance with the observations in our cohort. The two largest studies among BHD patients found no genotype/ phenotype correlation between pathogenic FLCN mutation and spontaneous pneumothorax In our cohort we observed no clear differences between the 15 different pathogenic FLCN mutations and the number of episodes of pneumothorax, age and recurrence rates. We found no recurrent episodes of pneumothorax in two different FLCN mutations, but both mutations were found in only one patient respectively (data not shown). In conclusion: based on our observations a conservative treatment is not accurate in BHD patients who suffer from a high recurrence rate of spontaneous pneumothorax. All types of (combined) invasive treatments except for the more localized ones like bullectomy and partial pleurectomyappears to give better results for the treatment of spontaneous pneumothorax in BHD patients compared to an initinal conservative approach. A large international multicentre phase II study is needed to evaluate our results. Current pneumothorax guidelines might need to be discussed and revised. Based on our results we suggest spontaneous pneumothorax in BHD needs a different and more aggressive treatment for SP in BHD patients. 96
97 References 1. MacDuff A, Arnold A, Harvey J, on behalf of the BTS Pleural Disease Guideline Group. Management of spontaneous pneumothorax: British Thoracic Society pleural disease guideline Thorax 2010;65:ii18-ii Johannesma PC, Reinhard R, Kon Y, et al. Prevalence of Birt-Hogg-Dubé syndrome in patients with apparently primary spontaneous pneumothorax. Eur Respir J. 2015;45: Ren HZ, Zhu CC, Yang C, et al. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax. Clin Genet 2008;74: Gupta N, Seyama K, McCormack FX. Pulmonary manifestations of Birt-Hogg-Dubé syndrome. Fam Cancer 2013;13: Baumann MH, Strange C, Heffner JE, et al. Management of spontaneous pneumothorax: An American College of Chest Physicians Delphi Consensus Statement. Chest 2001;119: Toro JR, Pautler SE, Stewart L, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg- Dubé syndrome. Am J REspir Crit Care Med. 2007;175: Agarwal PP, Gross BHD, Holloway BJ, et al. Thoracic CT findings in Birt-Hogg-Dubé syndrome. AJR Am J Roentgenol. 2011;196; Johannesma PC, Houweling AC, van Waesberghe JHTM, et al. The pathogenesis of pneumothorax in Birt-Hogg-Dubé syndrome: a hypothesis. Respirology Nov;19(8): Rehman HU. Birt-Hogg-Dubé syndrome: report of a new mutation. Can Respir J 2012;19: Onuki T, Goto Y, Kuramochi M, et al. Radiologically indeterminate pulmonary cysts in Birt-Hogg-Dubé syndrome. Ann Thorac Surg 2014;97: Dal Sasso AA, Belém LC, Zanetti G, et al. Birt-Hogg- Dubé syndrome. State-of-the-art review with emphasis on pulmonary involvement. Respir Med. 2015;109: Taveirna-DaSilva AM, Moss J. Clinical features, epidemiology, and therapy of lymphangioleiomyomatosis. Clin Epidemiol 2015;7: Ruy JH, Moss J, Beck GJ, et al. The NHLBI lymphangioleiomyomatosis registry: characteristics of 230 patients at enrollment. Am J Respir Crit Care Med. 2006;173: McCormack FX. Lymphangioleiomyomatosis: a clinical update. Chest 2008;133: Ashby M, Haug G, Mulcahy P, et al. Conservative versus interventional management for primary spontaneous pneumothorax in adults. Cochrane Database Syst Rev. 2014;12:CD Houweling AC, Gijezen LM, Jonker MA, et al. Renal cancer and pneumothorax risk in Birt-Hogg-Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer 2011;105: Treatment options for sp in BHD patients 97
98
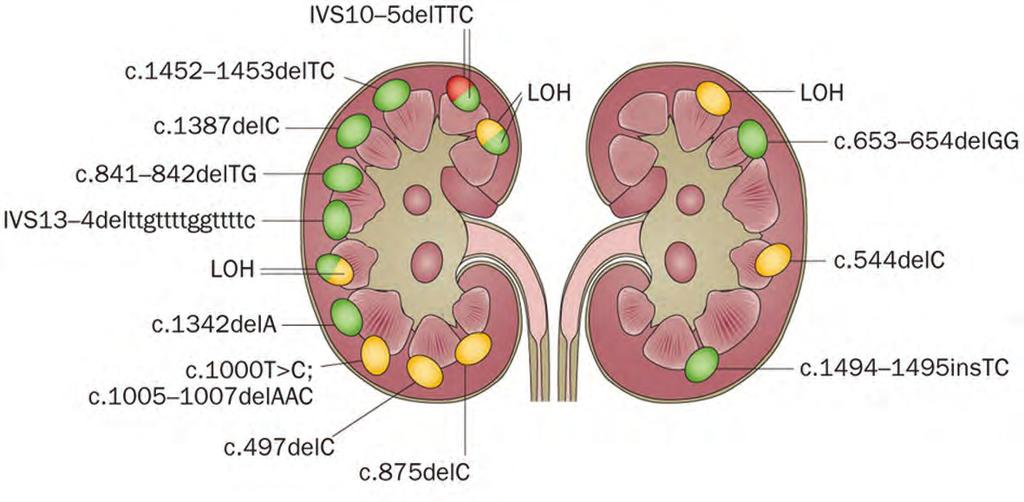
99 PART 2 Renal manifestations
100
101 chapter 2.1 Renal cancer and pneumothorax risk in birt-hogg-dubé syndrome (bhd); an analysis of 115 flcn mutation carriers from 35 bhd families arjan C. Houweling 1, Lieke M. Gijezen 2, Marianne A. Jonker 3, Martijn B. A. van Doorn 4, Rogier A. Oldenburg 5, Karin Y. van Spaendonck-Zwarts 6, Edward M. Leter 1, Theo A. van Os 7, Nicole C.T. van Grieken 8, Elisabeth H. Jaspars 8, Mirjam M. de Jong 6, Ernie M.H.F. Bongers 9, Paul C. Johannesma 10, Pieter E. Postmus 10, R. Jeroen A. van Moorselaar 11, JanHein T.M. van Waesberghe 12, Theo M. Starink 4, Maurice A.M. van Steensel 2, Johan J. P. Gille 1, Fred H. Menko 1 1 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Dermatology, GROW School for Oncology and Developmental Biology, Maastricht University Medical Center, Maastricht 3 Department of Mathematics, VU University, Amsterdam, The Netherlands 4 Department of Dermatology, VU University Medical Center, Amsterdam, The Netherlands 5 Department of Department of Clinical Genetics, Erasmus University Medical Center, Rotterdam 6 Department of Department of Genetics, University Medical Center Groningen, University of Groningen, Groningen 7 Department of Clinical Genetics, Academic Medical Center, Amsterdam 8 Department of Pathology, VU University Medical Center, Amsterdam, The Netherlands 9 Department of Department of Human Genetics, Radboud University Nijmegen Medical Center 10 Department of Pulmonology, VU University Medical Center, Amsterdam, The Netherlands 11 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 12 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands Br J Cancer 2011 Dec 6;105(12):1912-9
102 2.1 RCC and PTX risk in BHD patients Abstract Background Birt-Hogg-Dubé syndrome is an autosomal dominant condition caused by germline FLCN mutations, and characterized by fibrofolliculomas, pneumothorax and renal cancer. The renal cancer risk, cancer phenotype and pneumothorax risk of BHD have not yet been fully clarified. The main focus of this study was to assess the risk of renal cancer, the histological subtypes of renal tumours and the pneumothorax risk in BHD. Methods In this study we present the clinical data of 115 FLCN mutation carriers from 35 BHD families. Results Among 14 FLCN mutation carriers who developed renal cancer seven were <50 years at onset and/ or had multifocal / bilateral tumours. Five symptomatic patients developed metastatic disease. Two early-stage cases were diagnosed by surveillance. The majority of tumours showed characteristics of both eosinophilic variants of clear cell and chromophobe carcinoma. The estimated penetrance for renal cancer and pneumothorax was 16% (95% minimal confidence interval: 6-25%) and 29% (95% minimal confidence interval: 8-49%) at 70 years of age, respectively. The most frequent diagnosis in families without identified FLCN mutations was familial multiple discoid fibromas. Conclusion We confirmed a high yield of FLCN mutations in clinically defined BHD families, we found a substantially increased lifetime risk of renal cancer of 16% for FLCN mutation carriers. The tumours were metastatic in five out of 14 patients and tumour histology was not specific for BHD. We found a pneumothorax risk of 29%. We discuss the implications of our findings for diagnosis and management of BHD. 102
103 Introduction Birt-Hogg-Dubé syndrome (BHD, OMIM #135150) is an autosomal dominant condition characterized by fibrofolliculomas, pneumothorax, and renal tumours. BHD is caused by germline mutations in the FLCN gene encoding folliculin. 1 In the original kindred skin lesions were the only clinical manifestation. 2 Subsequently, renal cancer and pneumothorax were found to be part of the syndrome. 3 4 Furthermore, the risk for colorectal cancer might be slightly increased in FLCN mutation carriers. 5 The functions of folliculin have partly been clarified and might include a role in the mammalian target of rapamycin (mtor) pathway. 6 Whereas many BHD kindreds exhibit all three components of the syndrome, pneumothorax-only and renal-cancer-only families have also been described Among 69 patients with early-onset or familial clear cell renal cancer without further characteristics of BHD, germline FLCN mutations were found in 4% of cases. 9 In recent reviews, the variable clinical manifestations, molecular pathogenesis and management options for BHD were summarized. For optimal early detection and treatment of BHD-associated renal cancer, insight into the renal cancer risk and the clinical picture of these tumours is essential. Among cohorts of BHD patients a wide range of prevalence of kidney tumours has been observed, ranging from 6.5 to 34%. 13 The differences in prevalence are probably due to ascertainment in dermatological versus urological clinics and age at examination. Notably, the lifetime renal cancer risk for FLCN mutation carriers has not yet been established. In BHD, renal cancer is generally diagnosed at a relatively young age and commonly presents as bilateral and / or multifocal disease. The renal neoplasms typically found in BHD patients were described as hybrid tumours, containing elements of different histological subtypes, in particular chromophobe tumours and oncocytoma. However, other subtypes including clear cell renal carcinoma have also been reported. A 50 fold increased risk of spontaneous pneumothorax in BHD was reported. 16 Among cohorts of BHD patients the prevalence of pneumothorax ranged from 24-38%. 17 Again, ascertainment has varied for cohorts of patients and the lifetime risk of pneumothorax for FLCN mutation carriers has not yet been established. On CT examination of the thorax, more than 80% of adult BHD patients had multiple lung cysts, most often in the basal lung regions. 17 The presence of lung cysts is probably related to the increased risk for pneumothorax, which is often recurrent in BHD patients. A positive family history for pneumothorax was associated with an increased risk of pneumothorax and patients with a family history positive for renal cancer had an increased risk of having renal tumours. However, a family history of renal cancer was not associated with an increased pneumothorax risk. 13 Previously, we described 25 FLCN germline mutation carriers from 11 BHD families. 18 Here, we present an update of this cohort and add evaluation of 24 new kindreds with pathogenic FLCN mutations. In total, the clinical histories of 115 FLCN mutation carriers from 35 BHD families have been assessed. The main focus of this study was to assess the risk of renal cancer, the histological subtypes of renal tumours and the pneumothorax risk in BHD. Furthermore, we consider the yield of FLCN mutation analysis and the clinical phenotype in kindreds without FLCN mutations. 2.1 RCC and PTX risk in BHD patients 103
104 2.1 RCC and PTX risk in BHD patients Patients and methods Ascertainment of pedigrees The BHD database at VU University Medical Center currently lists more than 65 Dutch families referred for suspected BHD; 53 of these kindreds with completed family studies are considered in this report. Forty of these 53 families were referred to our center, while other Dutch clinical genetics centers contributed an additional 13 families with pathogenic FLCN mutations (Table 1). The index patient of 48 out of the 53 families was referred by a dermatologist after fibrofolliculomas were diagnosed. In three BHD families the index patient had renal cancer (BHD families 33, 35 and 63), in one kindred the proband had recurrent pneumothorax (BHD 29). One patient without an identifiable FLCN mutation was referred for multiple pulmonary cysts. For ascertainment of pedigrees, the proband was requested to inform family members by means of a written summary letter about BHD. After completion of the initial evaluation reminders were sent to probands aimed at complete ascertainment of family members. Table 1. Ascertainment of 115 FLCN mutation carriers from 35 BHD families considered in this study. Subdivision of families Clinical BHD & FLCN- mutation Clinical BHD without FLCN-mutation Other diagnoses Evaluation declined 40 families referred to our center for suspected BHD 1,# 13 FLCN- mutation-positive families from other centers 22 probands & 67 mutation-positive family members 13 probands & 13 mutation-positive family members Including families also described by in Leter et al., 2008 and Johannesma et al., Seven families (11, 17, 20, 24, 38, 45 and 50) had familial multiple discoid fibromas, described by Starink et al., 2011, in press; 2 index patients (26 and 39) were diagnosed with pulmonary emphysema and probable tuberous sclerosis complex and. # for calculation of renal cancer and pneumothorax penetrance the data of 86 FLCN mutation carriers from 21 kindreds for which complete family data were available were used Mutation analysis After informed consent genomic DNA was extracted from blood samples. Primers for the amplification and sequencing of the 14 exons were detailed previously by Nickerson et al. (2002). 1 PCR amplification was performed using a PE 9700 thermocycler (Applied Biosystems, Forster City, CA, USA). Sequencing reactions were performed using Big Dye Terminator (Applied Biosystems) and run on an ABI 3100 genetic analyzer (Applied Biosystems). For the detection of deletions and duplications of one or more exons the SALSA MLPA kit P256 obtained from MRC Holland was used ( Statistical analysis Conditional on the mutation status for different individuals, we assumed the various expressions of the BHD phenotype to be mutually independent and that for individual cases the risks for renal 104
105 cancer and pneumothorax and the ages at which these traits were expressed are independent. Finally, the penetrances of renal cancer and pneumothorax were assumed to be equal for male and female mutation carriers. For the estimates of the penetrance of pneumothorax and renal cancer we included 21 out of 22 FLCN-positive pedigrees investigated at our center. For these families medical records of all mutation carriers and information on untested relatives were available. Out of these 21 pedigrees, 20 were ascertained via a proband referred by a dermatologist. One proband (BHD 29) was referred by a pulmonologist for analysis of recurrent pneumothorax. Therefore, we included the proband data in the estimation of renal cancer and pneumothorax risks, with the exception of the proband referred for analysis of pneumothorax. Major problems of penetrance estimates are missing data and possible preferential testing of individuals affected with complications of BHD, i.e. renal cancer or pneumothorax. Indeed, if the mutation status and phenotype had been known for all individuals in all pedigrees the penetrance curves could have been assessed using the Kaplan-Meier estimator. Unfortunately, however, the mutation status or phenotype was not known for all family members. Excluding the individuals for whom the mutation status was unknown would likely lead to an overestimation of risk (see Figure 1A), assuming that non-affected individuals may be less willing to be genotyped. For our corrected risk estimation we assumed that a negative family history for renal cancer or pneumothorax in a close relative indeed reflects the absence of these complications in the untested relative. We imputed the missing data as follows: for every individual in the data set who was not genotyped the probability that he or she was a carrier was computed on the basis of the mutation status of his / her relatives. Subsequently, using this carrier probability it was sampled whether he or she was a mutation carrier or not. As a result, for every individual the mutation status was assigned and in combination with the phenotype Kaplan-Meier curves and confidence intervals were computed. This strategy of sampling the mutation status and estimating the penetrance functions by the Kaplan-Meier estimator was repeated times. Next, the mean of the estimated curves and upper and lower bounds of the confidence intervals were computed. These curves are plotted in Figure 1A and B for renal cancer and in Figure 1C for pneumothorax. By using this strategy the estimator will be asymptotically unbiased. The confidence interval found is slightly too narrow because there is a greater degree of uncertainty than would have been the case if the missing mutation statuses had actually been observed (as assumed after imputation). Therefore, the final confidence interval has a confidence of slightly less than 95%. Although the exact confidences of the intervals are not exactly known we included the calculated intervals in the figures in order to make those who would use the figures for consultation aware of the uncertainty of the given risk estimates. 2.1 RCC and PTX risk in BHD patients Results The characteristics of 53 families referred for suspected BHD are presented in Table 1. The main features of the BHD kindreds with pathogenic FLCN germline mutations are listed in Table 2. The mutations detected are depicted in Figure 2. Data on the renal tumours and pneumothorax are given in Tables 3 and 4, respectively. Among the 27 families with clinical BHD based on dermatological evaluation at our center, 22 had pathogenic FLCN mutations (mutation detection rate 81%). 105
106 2.1 RCC and PTX risk in BHD patients A Figure 1. (A) Estimate of the age-related penetrance function for renal cancer based on available data on both mutation carriers and their untested relatives till the age of 70: (continuous line n=86 mutation carriers and 84 untested relatives), together with the Kaplan-Meier estimator based on the known mutation carriers only at age 70: (n=86, red dashed line). (B) Estimate of the age-related penetrance function for renal cancer based on available data on both mutation carriers and their untested relatives together with a minimum 95% confidence interval. Estimated penetrance at age 70: 0.160, 95% minimal confidence interval: [0.0626, 0.259] (C) Estimation of the penetrance function of age at first pneumothorax and a minimum 95% confidence interval based on available data on both mutation carriers and their untested relatives (n=85 mutation carriers and 84 untested relatives). Estimated penetrance at age 70: 0.288, 95% minimal confidence interval: [ , 0.487]. B C Table 2. Main features of 115 FLCN mutation carriers from 35 BHD kindreds with pathogenic FLCN germline mutations. Fam. no. FLCN germline mutation No. of FLCN mutation carriers No. of mutation carriers with pneumothorax No. of mutation carriers with renal cancer BHD1 c.610_611delinsta BHD3 c.420delc BHD4 c.1285dupc BHD6 c.1285dupc BHD8 c.655dupg BHD12 c.1285dupc BHD14 c.610_611delinsta BHD15 c.619-1g>a BHD16 c.610_611delinsta BHD18 c.[1301-7_1304del11; 1323delCinsGA] BHD19 c.619-1g>a BHD22 c.1285dupc BHD23 c.319_320delgtinscac BHD27 c.1408_1418delgggagccctgt BHD29 c.610_611delinsta BHD30 c.1285dupc BHD31 c.610_611delinsta BHD32 c.469_471delttc BHD33 c.619-1g>a BHD35 c.1749_1753del BHD36 c.610_611delinsta BHD37 c.319_320delgtinscac
107 Table 2. Main (continued) features of 115 FLCN mutation carriers from 35 BHD kindreds with pathogenic FLCN germline mutations. Fam. no. FLCN germline mutation No. of FLCN mutation carriers No. of mutation carriers with pneumothorax No. of mutation carriers with renal cancer BHD40 c.1183_1198del BHD43 c.610_611delinsta BHD44 c.319_320delgtinscac BHD46 c.1408_1418delgggagccctgt BHD47 c a>g BHD48 c.1285dupc BHD49 c.1300g>c BHD51 c.1285dupc BHD53 c.871+3_ 871+4delGAinsTCCAGAT BHD57 c.250-?_1740+?del (del exon 5-14) BHD 62 c.1301-?_1740+?del (del exon 12-14) BHD 63 c.610_611delinsta BHD66 c.3g>a RCC and PTX risk in BHD patients Figure 2. Overview of the FLCN mutations identified in this study. N: nonsense, SS: splice site, F: Frame shift, Del: deletion, M: Missense. Exons are depicted as rectangles. The family numbers are shown after the mutations. Characteristics of the five families without a detectable FLCN mutation are summarized in Table 5; they include two families with an unclassified exon 1 deletion. Analysis of these exon 1 deletions is ongoing. In the cohort of our current study, no colorectal cancer was reported. Colorectal adenomas were diagnosed by colonoscopy in four FLCN mutation carriers (age 40, 42, 83, these patients were also included in our previous reports by Leter et al and Nahorski et al and age 44, not reported previously). Other malignancies than renal cancer were reported in 6 patients previously documented in Leter et al. (2008). 18 In addition to the patients reported by Leter et al. 2008, in five patients without renal 107
108 Table 3. Main features of 17 renal cancers in 14 FLCN germline mutation carriers from 12 BHD kindreds. 2.1 RCC and PTX risk in BHD patients Fam. no. M/F Age at diagnosis (yrs) Diagnosis # Clinical characteristics* Localisation Histology tnm Treatment Outcome BHD1 F 60 B 1 (L) 1 CC/Cph T1N0M0 T A (3) BHD6 M 39 A 1 (R) 1 Pap/CC T3N2M1 T & Im D (40) F 40 A a 1 (L) 2 CC/Cph T2N0M0 T A (7) BHD16 M 56 A 1 (R) 1 CC/Cph/Sa T3N0M1 T & Ch D (57) BHD23 M 51 A 1 (L) 1 CC/Cph T1N0M1 T & Ch & R D (52) BHD32 F 51 B 1 (R) 1 CC/Cph T1N0M0 P A (3) BHD33 M BHD35 M A B A B 2 (L) (R) 2 (R) (L) CC/Cph unknown CC unknown T3N0M0 T1N0M0 T1N0M0 T1N0M0 BHD37 F 52 A 1 1 CC TxNxM1 Rth D (52) BHD43 F 74 A 1 (L) 2 CC/Cph T1N0M0 T A (3) M 56 A 1 (R) 2 CC/Cph T1N0M0 T A (2) BHD44 F 43 A 1 (L) 1 CC/Cph TxNxM1 T & Me D (57) BHD46 M 50 A 1 (L) 1 unclassified b T1N0M0 - D (50) BHD63 M A B 2 (L) (R) 2 1 CC/Cph CC/Cph T2N0M0 T1N0M0 T P P P T P A (6) A (1) A (3) #: A: diagnosis after symptoms had developed; B: diagnosis after positive renal imaging of an asymptomatic individual * Localisation: Left column: 1/2: Unilateral/ Bilateral, in parentheses: L/ R: left-sided/ right-sided, Right column: 1: Unifocal, 2: multifocal. Histology: according to Lopez-Beltran et al., 2009; CC: clear cell, Pap: papillary, Cph chromophobe, Onc: oncocytoma; Sa: sarcomatoid component; CC/Cph: renal cell carcinoma with eosinophilic cytoplasm and characteristics of both CC en Cph, Ad: adenocarcinoma, classification not certain; TNM: classification according to tumour/ node/ metastasis status Treatment: T: total nephrectomy, P: partial nephrectomy; Ch: chemotherapy, Im: immunotherapy; Rth: radiotherapy A: alive, D: deceased; in parentheses: number of years of follow-up and age at death, respectively a : coincidental finding at medical examination for gastrointestinal complaints b : The tumour was found during autopsy and could not be reliably subclassified due to autolysis cancer, tumours were reported including non-melanoma skin cancer in two patients and single cases of melanoma, sarcoma, bladder and prostate cancer. The patient diagnosed with melanoma was also diagnosed with a sarcoma. Three patients with renal cancer were diagnosed with additional tumours. One patient had an oncocytic pituitary adenoma at age 9, a giant cell astrocytoma at age 12, pheochromocytoma at age 34 and renal cancer at age 34 and 35 (BHD 63, table 3). No evidence for other tumour susceptibility was found. The other two patients had gastric carcinoma at age 55 and renal cancer at age 56 (BHD 43, M, table 3) and prostate carcinoma and renal cancer at age 50 (BHD 46, table 3), respectively. Renal manifestations Fourteen out of 115 (12%) FLCN mutation carriers from 12 families were diagnosed with renal cancer. All available tumours were revised at our center by two pathologists. In addition, one mutation 108
109 Table 4. Main features of pneumothorax in 28 FLCN germline mutation carriers from 15 BHD kindreds. Fam. No. M/F Age at diagnosis* R/L* Clinical characteristics Episodes BHD1 F 44 L 1 M 30 R 1 BHD14 M 36 L 1 BHD15 F U U 1 BHD16 M 67 L 1 F 47 U 1 BHD18 M 22 U 1 BHD23 M 22 L 1 BHD29 1 M 25 # B 5 M 27 # B 1 Age at diagnosis of renal cancer BHD32 F 39 U 1 51 F U U 1 M 23 U 1 BHD33 M U U 1 BHD35 M 38 R 2 38 BHD37 F 48 B 1 51 F 29 R 1 BHD 63 M 37 B 1 BHD 62 M 53 L 7 M 27 L 1 M 42 B 3 BHD43 F 38 L 1 M 37 R 4 F 74 L 1 74 M 32 L 3 55 F 18 R 2 BHD57 M 31 L 1 F 33 R RCC and PTX risk in BHD patients Age at first episode of pneumothorax; U: Available records did not state exact age/clinical characteristics. R: right lung, L: left lung, B: Bilateral # Multiple cysts on CT 1: Described by Johannesma et al The relative diagnosed with a clear cell renal tumour was not tested for the FLCN mutation. Renal cancer: Age at diagnosis of renal cancer in patients with a history of pneumothorax Skin: FF: confirmed fibrofolliculoma, U: unknown carrier had renal oncocytoma (BHD 57). Five mutation carriers died of metastatic renal cancer (BHD 6, BHD 16, BHD 23, BHD 37, BHD 44, Table 3). All were diagnosed with renal cancer after symptoms had developed. The histological classification of the renal tumours according to the 109
110 Table 5. Characteristics of BHD probands without an identified FLCN mutation. 2.1 RCC and PTX risk in BHD patients BHD no. Sex & age of proband Clinical characteristics Family data Remarks BHD2 M 46 yrs Multiple fibrofolliculomas on the face, neck and trunk, starting at age 33 yrs BHD5 M 33 yrs Multiple fibrofolliculomas on thorax since childhood BHD9 M 34 yrs More than 100 skin lesions on the face, neck and trunk, fibrofolliculomas. Ulcerative colitis, sacroiliitis BHD25 F 70 yrs Multiple fibrofolliculomas at age 66 yrs BHD28 M 56 yrs Multiple fibrofolliculomas since age 40 yrs Colorectal cancer in mother Nephew had pneumothorax and died due to renal cancer Three unclassified variants in FLCN: exon 1 deletion &polymorphisms (IVS8+36G>A and IVS9+6C>T) # Unclassified variant in FLCN: IVS8+36G>A Unclassified variant in FLCN: exon 1 deletion # In BHD 2 an exon 1 deletion was detected in addition to two intronic FLCN variants, IVS9+6 C>T, and IVS8+36G>A. Variant IVS9+6 C>T was previously reported in a patient with suspected BHD who had multiple renal tumours and bilateral squamous papilloma of the eyelids 23. Both variants however, have since been reported to be rare polymorphisms ( lumc.nl/lovd2/shared1/home.php?select_db=flcn). WHO criteria is shown in Table Most of the tumours showed cells with granular / floccular eosinophilic cytoplasm, as can be seen in both clear cell carcinoma (formerly called the eosinophilic variant, Table 3) and chromophobe carcinoma. This eosinophilic cell variation is also often seen in sporadic clear cell carcinoma Since most tumours had mainly eosinophilic cytoplasm, with moderately sharp cell borders, a vague perinuclear halo and moderately enlarged nuclei, we classified them as intermediate between clear cell and chromophobe carcinoma (CC/Cph) (Table 3 and Figure 3). One of the tumours showed sarcomatoid changes, which can develop in both clear cell and chromophobe carcinoma (Table 3, BHD16). One other tumour had papillary structures in combination with clear cell changes (Table 3, BHD 6). Two additional patients from FLCN positive families but with unknown mutation carrier status (BHD1, and BHD42) were diagnosed with renal cancer. These two tumours also showed mixed chromophobe/clear cell histology. Two of the 14 renal tumours (BHD 1 and BHD 32, Table 3) were detected by surveillance. For one of these patients renal cancer was detected on the first ultrasound performed after the diagnosis BHD was made (BHD 32, Table 3). For the other patient renal cancer was detected by ultrasound four years after the preceding normal ultrasound / MRI (BHD1, Table 3); this latter patient did not undergo standard yearly surveillance after the initial imaging. 110
111 2.1 RCC and PTX risk in BHD patients Figure 3. Illustration of the histological pictures of renal cell carcinomas in our series. A: The most common pattern found, classified as clear cell/chromophobe. The tumour cells show eosinophilic cytoplasm, moderate nuclear pleiomorphism, vague perinuclear halos, no explicit cell borders and no vascular prominence. B: Classical picture of clear cell carcinoma, as can be seen in many of the tumours in our series, but mostly only in part of the tumour cells C: A clear cell/chromophobe renal cell carcinoma with partially clear cytoplasm, more prominent cell borders, no thick walled vessels D: Renal cell carcinoma with sarcomatoid changes (in the right part of the picture). Cutaneous manifestations Most FLCN mutation carriers (91/115, 79%), underwent dermatological evaluation (68 of which were evaluated by dermatologists at our center). Nineteen (21%) cases, aged years, had no cutaneous abnormalities; 14 (73%) of the patients without cutaneous manifestations were over age 40. Notably, one patient who presented with metastatic renal cancer at age 51 (BHD 23) had no cutaneous lesions. The youngest mutation carrier with histologically confirmed fibrofolliculomas was 25 years old (BHD 23). In five families without an identifiable FLCN mutation (BHD 2, 5, 9, 25 and 28) the clinical diagnosis BHD was based on histologically confirmed multiple fibrofolliculomas; in one of these kindreds both pneumothorax and renal cancer occurred (BHD 25, Table 5). In seven families without FLCN mutations the skin lesions consisted of multiple discoid fibromas of childhood onset (families 11, 17, 20, 24, 38, 45 and 50). In two of these families (24 and 45) a genealogical study showed common ancestry. No renal or pulmonary signs were present in these seven families, except for one case with pneumothorax. For two of these families the FLCN-locus was excluded by linkage analysis. 21 Pulmonary manifestations Among the 115 FLCN mutation carriers, 28 (24%)had a history of pneumothorax, recurrent in eight patients (Table 4). Four out of 28 patients with a previous pneumothorax were confirmed (former) smokers. The medical records of the other patients did not state a history of smoking. The mean age 111
112 2.1 RCC and PTX risk in BHD patients of the first pneumothorax was 36 years (range years). We did not systematically subject mutation carriers to CT-scanning of the lungs. For 12 FLCN mutation carriers the report of a CT-scan of the thorax was available. Scans were performed either to confirm suspected BHD or because of pulmonary complications of BHD. In five of these patients (aged years), multiple cysts were reported in one or both lungs. Of these, two had a history of recurrent or bilateral pneumothorax before the age of 30 years. In seven FLCN mutation carriers no pulmonary cysts were detected (age 23-71, four were over age 40). Cumulative renal cancer and pneumothorax risk The estimated renal cancer penetrance based on assessment of FLCN mutation carriers only was 0.20 at age 70 (red dashed line, Figure 1A). In contrast, when considering both tested and untested relatives, the estimated renal cancer penetrance at age 70 was 0.16 (continuous line, Figure 1A and Figure 1B). The estimated penetrance for the first episode of spontaneous pneumothorax was 29% (95% minimal confidence interval: 8-49%, Figure 1C) at 70 years, again considering information on both mutation carriers and their untested relatives. Discussion An important aim of this study was the estimation of renal cancer and pneumothorax penetrance in Birt-Hogg-Dubé syndrome. By incorporating data on relatives who did not undergo DNA testing we found an estimated penetrance for renal cancer of 16% and a penetrance for pneumothorax of 29% at the age of 70 years. The wide range of prevalence for renal cancer among cohorts of BHD reported in literature is %. The renal cancer risk we found of around 16% is at age 70 years is important for counselling of FLCN mutation carriers and their families ascertained in cancer family clinics. Future studies with larger patient groups and comparison between cohorts investigated in different populations may lead to further specification of the renal cancer risk. The clinical presentation, histological pattern and biological behaviour of renal cancer in FLCN mutation carriers are important for several reasons. First, a pathognomonic histological pattern would be helpful for early diagnosis. Previously, The European BHD Consortium proposed clinical diagnostic criteria for BHD which included early-onset, bilateral and multifocal renal tumours and a mixed chromophobe and oncocytic histological pattern. In addition, FLCN mutation analysis should be considered for patients who have familial cystic lung disease, familial pneumothorax, familial renal cancer, or any combination of spontaneous pneumothorax and kidney cancer. Notably, among 14 BHD patients in the current study who developed renal cancer, clinical signs of hereditary disease (age at onset <50 years and / or multifocal / bilateral tumours) were present in only seven cases. In addition, the histological picture of BHD- associated renal cancer in this cohort was not typical for this syndrome. Ten out of 14 renal tumours revised in this series were difficult to classify. None of them showed classical features of chromophobe renal cell carcinoma. Instead they mainly exhibited characteristics of both eosinophilic variants of clear cell cancer and chromophobe carcinoma. One of the tumours was a hybrid form of clear cell and papillary carcinoma and one showed sarcomatoid changes. These histological patterns can also be found in sporadic RCC. Therefore, late-onset unilateral, unifocal clear cell renal cancer also does not exclude BHD. 112
113 Furthermore, although BHD-associated renal tumours were reported to metastasize rarely, five of the 14 patients with renal cancer in our cohort developed metastatic disease underlining the importance of early detection of these renal tumours by surveillance. In recently diagnosed families not included in this report, we observed two BHD patients with renal cancer at the ages of 30 and in the early twenties respectively, underlining that surveillance for renal cancer should be offered to BHD patients from early age onward. Of the 115 FLCN mutation carriers 28 had a history of pneumothorax, frequently recurrent and bilateral. The mean ages at which pneumothorax and renal cancer occurred in our cohort were 36 years and 49 years, respectively. Among the 14 renal cancer patients described five had a history of pneumothorax (Table 3, 4), preceding renal cancer by several years in three patients (BHD 32, 37, 43, Table 4). Although an increased risk for renal cancer in BHD families with a positive history for pneumothorax has not been observed 13, bilateral, recurrent or familial pneumothorax may serve as an early indicator of BHD syndrome. 22 Since, in 1975, Hornstein and Knickenberg 23 described the combination of skin fibrofolliculomas and colorectal polyps it is a matter of debate whether BHD is associated with an increased risk of colorectal neoplasia. Whereas Zbar et al. found no significantly increased risk Khoo et al.32 proposed that the risk might apply to specific subgroups only. Nahorski et al. (2010) found evidence that the risk may be dependent on the FLCN genotype. Recently, in family BHD15, one of the FLCN mutation carriers developed symptomatic colonic cancer at age 62 years. Late-onset colorectal cancer has been diagnosed in several other FLCN mutation carriers from our BHD cohort not included in the present study. Although colorectal cancer may well be coincidental in these cases the current data call for further evaluation of the colorectal neoplasia risk in BHD. Among 27 families with clinical BHD (multiple fibrofolliculomas) evaluated at our center 22 had pathogenic FLCN mutations, i.e. a 81% yield for FLCN mutation analysis. Four patients referred for suspected BHD declined genetic testing. In two of the families (BHD 2 and 25 with clinical BHD but without a mutation in the coding region of FLCN, a deletion of exon 1 was observed. Exon 1 is the first of three non coding exons. The exact size and the effect of these deletions remains to be determined. Recently, after completion of our study, intragenic duplications and deletions were reported in patients with BHD after completion. 25 Using a luciferase reporter assay, this study also showed that expression was strongly reduced when exon 1 was deleted. Analysis of the pathogenicity and co-segregation of the deletions detected in our families are currently ongoing to prove pathogenicity. Therefore, these families were not included in the calculation of the penetrance for renal cancer and pneumothorax although the deletions are very likely to be pathogenic. In the current study, intragenic deletions were detected in two of the BHD families (BHD 57, 62), underlining the importance of MLPA or CGH analysis in patients with a clinical suspicion of BHD without an identifiable FLCN mutation. Nine patients referred for possible BHD were diagnosed with other conditions. One patient had probable tuberous sclerosis and one patient had pulmonary emphysema. Seven of the families were diagnosed with familial multiple discoid fibromas (FMDF). In 1985, one of the authors described this entity as a dominant condition distinct from BHD, showing childhood onset, preferential localisation 2.1 RCC and PTX risk in BHD patients 113
114 2.1 RCC and PTX risk in BHD patients of lesions on the ears, and distinct histology, which mimics the trichodiscomas in BHD. 26 Thus far no systemic complications have been noted for FMDF except for one patient with pneumothorax. We have now excluded involvement of the FLCN locus in two FMDF kindreds using linkage analysis. Currently, we use the renal cancer risk of around 16% by age 70 years for the counselling of patients to emphasize the importance of surveillance for renal cancer. Since according to our histological data, the renal cancers found in BHD were not evidently different from sporadic tumours, future studies are aimed at the classification of BHD associated renal cancer in comparison with sporadic disease are essential. Both the renal cancer risk and the pneumothorax risk (about 16% and 29% at age 70 years, respectively) are based on a large set of data using a model incorporating available data of family members not subjected to DNA testing. Evaluation of larger patients groups and patients from other populations may yield other penetrance figures in the future. The European BHD Consortium proposed FLCN mutation testing in patients with early-onset renal cancer (<50 years), in particular with multifocal or bilateral disease (or both) with chromophobe or oncocytic histology and in familial renal cancer cases. Age at diagnosis of (the first) renal cancer in our patient group was at or above 50 years of age in half of the patients and the tumour histology was mixed in most patients but included clear cell elements in all cases. Therefore, it will be important to study the yield of FLCN mutation testing using a wider set of criteria than proposed previously. The histology and molecular pathology of renal tumours are associated with their biological behaviour and reaction to systemic treatment of metastatic disease. Therefore, additional studies are needed to monitor the success of surveillance for renal cancer, the results of surgical or other forms of local treatment such as radiofrequency ablation and response to targeted therapies. 114
115 References 1. Nickerson ML, Warren MB, Toro JR, Matrosova V, Glenn G, Turner ML, Duray P, Merino M, Choyke P, Pavlovich CP, Sharma N, Walther M, Munroe D, Hill R, Maher E, Greenberg C, Lerman MI, Linehan WM, Zbar B, Schmidt LS (2002) Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt- Hogg-Dubé syndrome. Cancer Cell 2 (2): Birt AR, Hogg GR, Dubé WJ (1977) Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol 113 (12): Toro JR, Glenn G, Duray P, Darling T, Weirich G, Zbar B, Linehan M, Turner ML (1999) Birt-Hogg-Dubé syndrome - A novel marker of kidney neoplasia. Arch Dermatol 135 (10): Roth JS, Rabinowitz AD, Benson M, Grossman ME (1993) Bilateral Renal-Cell Carcinoma in the Birt-Hogg- Dubé syndrome. J Am Acad Dermatol 29 (6): Nahorski M, Lim DHK, Martin L, Gille JP, Mckay K, Rehal PK, Ploeger HM, van Steensel M, Tomlinson IP, Latif F, Menko FH, Maher ER (2010) Investigation of the Birt-Hogg-Dubé tumour suppressor gene (FLCN) in familial and sporadic colorectal cancer. J. Med. Genet. 47 (6): Hasumi Y, Baba M, Ajima R, Hasumi H, Valera VA, Klein ME, Haines DC, Merino MJ, Hong SB, Yamaguchi TP, Schmidt LS, Linehan WM (2009) Homozygous loss of BHD causes early embryonic lethality and kidney tumor development with activation of mtorc1 and mtorc2. Proc Natl Acad Sci 106 (44): Kunogi M, Kurihara M, Ikegami TS, Kobayashi T, Shindo N, Kumasaka T, Gunji Y, Kikkawa M, Iwakami S, Hino O, Takahashi K, Seyama K (2010) Clinical and genetic spectrum of Birt-Hogg-Dubé syndrome patients in whom pneumothorax and/or multiple lung cysts are the presenting feature. J Med Genet 47 (4): Painter JN, Tapanainen H, Somer M, Tukiainen P, Aittomäki K (2005) A 4-bp deletion in the Birt-Hogg-Dubé gene (FLCN) causes dominantly inherited spontaneous pneumothorax. Am J Hum Genet 76 (3): Woodward ER, Ricketts C, Killick P, Gad S, Morris MR, Kavalier F, Hodgson SV, Giraud S, Bressacde Paillerets B, Chapman C, Escudier B, Latif F, Richard S, Maher ER (2008) Familial non-vhl clear cell (conventional) renal cell carcinoma: Clinical features, segregation analysis, and mutation analysis of FLCN. Clin Cancer Res 14 (18): Graham RB, Nolasco M, Peterlin B, Garcia CK (2005) Nonsense mutations in folliculin presenting as isolated familial spontaneous pneumothorax in adults. Am J Respir Crit Care Med 172 (1): Menko FH, van Steensel MAM, Giraud S, Friis- Hansen L, Richard S, Ungari S, Nordenskjöld M, Hansen TV, Solly J, Maher ER (2009) Birt-Hogg- Dubé syndrome: diagnosis and management. Lancet Oncol 10 (12): Schmidt LS, Nickerson ML, Warren MB, Glenn GM, Toro JR, Merino MJ, Turner ML, Choyke PL, Sharma N, Peterson J, Morrison P, Maher ER, Walther MM, Zbar B, Linehan WM (2005) Germline BHD-mutation spectrum and phenotype analysis of a large cohort of families with Birt-Hogg-Dubé syndrome. Am J Hum Genet 76 (6): Toro JR, Wei MH, Glenn GM, Weinreich M, Toure O, Vocke C, Turner M, Choyke P, Merino MJ, Pinto PA, Steinberg SM, Schmidt LS, Linehan WM (2008) BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet 45 (6): Pavlovich CP, Grubb RL 3rd, Hurley K, Glenn GM, Toro J, Schmidt LS, Torres-Cabala C, Merino MJ, Zbar B, Choyke P, Walther MM, Linehan WM (2005) Evaluation and management of renal tumors in the Birt-Hogg-Dubé syndrome. J Urol 173 (5): Pavlovich CP, Walther MA, Eyler RA, Hewitt SM, Zbar B, Linehan WM, Merino MJ (2002) Renal tumors in the Birt-Hogg-Dubé syndrome. Am J Surg Pathol 26 (12): Zbar B, Alvord WG, Glenn G, Turner M, Pavlovich CP, Schmidt L, Walther M, Choyke P, Weirich G, Hewitt SM, Duray P, Gabril F, Greenberg C, Merino MJ, Toro J, Linehan WM (2002) Risk of renal and colonic neoplasms and spontaneous pneumothorax in the Birt-Hogg-Dubé syndrome. Cancer Epidemiol Biomarkers Prev 11 (4): Toro JR, Pautler SE, Stewart L, Glenn GM, Weinreich M, Toure O, Wei MH, Schmidt LS, Davis L, Zbar B, Choyke P, Steinberg SM, Nguyen DM, Linehan WM (2007) Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med 175 (10): Leter EM, Koopmans AK, Gille JJP, Van Os TAM, Vittoz GG, David EFL, Jaspars EH, Postmus PE, van Moorselaar 2.1 RCC and PTX risk in BHD patients 115
116 2.1 RCC and PTX risk in BHD patients RJA, Craanen ME, Starink TM, Menko FH (2008) Birt- Hogg-Dubé syndrome: Clinical and genetic studies of 20 families. J Invest Dermatol 128 (1): Lopez-Beltran A, Carrasco JC, Cheng L, Scarpelli M, Kirkali Z, Montironi R (2009) 2009 update on the classification of renal epithelial tumors in adults. International Journal of Urology 16 (5): Kummerlin I, ten Kate F, Smedts F, Horn T, Algaba F, Trias I, de la Rosette J, Laguna MP (2009) Diagnostic problems in the subtyping of renal tumors encountered by five pathologists. Pathol Res Pract 205 (1): Starink T.M., Houweling A.C., van Doorn M.B.A., Leter E.M., Jaspars E.H., van Moorselaar R.J.A., Postmus P.E., Johannesma P.C., van Waesberghe J.H., Ploeger M.H., Kramer M.T., Gille J.J.P., Waisfisz Q., Menko F.H. (2011) Familial multiple discoid fibromas: A look-alike of Birt-Hogg-Dubé syndrome not linked to the FLCN locus. J Am Acad Dermatol, in press. 22. Johannesma PC, Lammers JW, van Moorselaar RJ, Starink TM, Postmus PE, Menko FH (2009) Spontaneous pneumothorax as the first manifestation of a hereditary condition with an increased renal cancer risk. Ned Tijdschr Geneeskd 153 A Hornstein OP, Knickenberg M (1975) Perifollicular fi bromatosis cutis with polyps of the colon a cutaneo-intestinal syndrome sui generis. Arch Dermatol Res 253: Khoo SK, Giraud S, Kahnoski K, Chen J, Motorna O, Nickolov R, Binet O, Lambert D, Friedel J, Lévy R, Ferlicot S, Wolkenstein P, Hammel P, Bergerheim U, Hedblad MA, Bradley M, Teh BT, Nordenskjöld M, Richard S (2002) Clinical and genetic studies of Birt-Hogg-Dubé syndrome. J Med Genet 39(12): Benhammou JN, Vocke CD, Santani A, Schmidt LS, Baba M, Seyama K, Wu X, Korolevich S, Nathanson KL, Stolle CA, Linehan WM (2011) Identification of intragenic deletions and duplication in the FLCN gene in Birt-Hogg-Dubé syndrome. Genes Chromosomes Cancer 50 (6): Starink TM, Kisch LS, Meijer CJLM (1985) Familial Multiple Trichodiscomas - A clinicopathologic study. Arch Dermatol 121 (7):
117
118
119 chapter 2.2 Are lung cysts in renal cell cancer (Rcc) patients an indication for FLCN mutation analysis? Paul C. Johannesma 1, Arjan C. Houweling 2, Fred H. Menko 3, Irma van de Beek 2, Rinze Reinhard 4, Johan J.P. Gille 2, JanHein T.M. van Waesberghe 4, Erik Thunnissen 5, Theo M. Starink 6, Pieter E. Postmus 7, R Jeroen A van Moorselaar 8 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 3 Family Cancer Clinic, Netherlands Cancer Institute, Amsterdam, The Netherlands 4 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 5 Department of Pathology, VU University Medical Center, Amsterdam, The Netherlands 6 Department of Dermatology, Leiden University Medical Center, Leiden, The Netherlands 7 Department of Thoracic Oncology, Clatterbridge Cancer Centre, Liverpool Heart & Chest Hospital, University of Liverpool, Liverpool, United Kingdom 8 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands Fam Cancer 2016;15(2):
120 2.2 Lung cysts as indicator for BHD in rcc patients Abstract Renal cell cancer (RCC) represents 2-3% of all cancers and is the most lethal of the urologic malignancies, in a minority of cases caused by a genetic predisposition. Birt-Hogg-Dubé syndrome (BHD) is one of the hereditary renal cancer syndromes. As the histological subtype and clinical presentation in BHD are highly variable, this syndrome is easily missed. Lung cysts mainly under the carina - are reported to be present in over 90% of all BHD patients and might be an important clue in differentiating between sporadic RCC and BHD associated RCC. We conducted a retrospective study among patients diagnosed with sporadic RCC, wherein we retrospectively scored for the presence of lung cysts on thoracic CT. We performed FLCN mutation analysis in 8 RCC patients with at least one lung cysts under the carina. No mutations were identified. We compared the radiological findings in the FLCN negative patients to those in 4 known BHD patients and found multiple basal lung cysts were present significantly more frequent in FLCN mutation carriers and may be an indication for BHD syndrome in apparent sporadic RCC patients. 120
121 Introduction Renal cell carcinoma (RCC) represents 2-3% of all cancers and is the most lethal of the urologic malignancies. There has been an annual increase about 2% in the incidence, with 88,400 new cases of RCC worldwide in The incidence is approximately 5.8 per and the mortality is approximately 1.4 per Currently over 50% of RCC are detected incidentally, as only a minority (6-10%) of patients present with the classic triad; flank pain, gross haematuria and palpable abdominal mass. 3 These data underline the value of pre symptomatic identification and screening of patients with an increased risk for RCC. A genetic predisposition for renal cancer is currently estimated to be present in 3-5% of RCC patients, often showing recognisable features in addition to the increased risk for renal cancer. 4 A probably underdiagnosed autosomal dominant cancer disorder is the Birt- Hogg-Dubé syndrome (BHD), clinically characterized by skin fibrofolliculomas, lung cysts in >90% of cases, (recurrent) spontaneous pneumothorax (SP) and an increased lifetime risk for RCC between 16-35%. The gene associated with BHD encodes the protein folliculin (FLCN) which acts as a tumour suppressor and interacts with mtor and AMPK signalling pathways. 5 The incidence is estimated about 1 in people. 6 So far, two large studies described the phenotypes of a large cohort of families with BHD. The first study by Toro and colleagues showed 24 cases with a history of RCC. Of them 22/24 (91,7%) had multiple lung cysts on thoracic CT. In the remaining two patients, no thoracic CT scan was available. The second study performed in our University centre, we found 17 cases of RCC among a total of 115 FLCN mutation carriers. A thoracic CT was available in 13/17 (76.4%) which showed cysts in one or both lungs in all cases. In the other four cases no thoracic CT was available. 7 8 Therefore we hypothesized, that cysts under the main carina in patients with diagnosed with sporadic RCC might be an important diagnostic clue in unmasking Birt-Hogg-Dubé syndrome. We performed a pilot study to evaluate this hypothesis. 2.2 Lung cysts as indicator for BHD in rcc patients Material and Methods We retrospectively collected data on all patients (n=182), who had been diagnosed and treated for RCC in the years Patients diagnosed with RCC in our center were included when they were over the age of 18 years at the time of diagnosis. Exclusion criteria were metastasis in the kidney, no available thoracic CT or patients already known with a proven pathogenic FLCN mutation. Furthermore, deceased patients were excluded (Figure 1). All thoracic CT s, made in the period were collected and scored by one radiologist for the presence of one or more lung cysts, below the level of the carina. Furthermore we collected the clinical data on familial occurrence on SP, RCC and the history of SP. Clinical information was not available to the radiologist at the time of scoring. We compared the radiological data to that of 4 FLCN mutation carriers diagnosed with RCC and tested for potential significant differences in the number and size of lung cysts. Results Patient data: Proven FLCN mutation carriers (N=4) In our BHD cohort of 250 FLCN mutation carriers, 4 patients were diagnosed with BHD after the diagnosis of RCC and this enabled screening of their relatives. All 4 index patients had at diagnosis 121
122 2.2 Lung cysts as indicator for BHD in rcc patients Figure 1. Study in- / exclusion flowchart. one or more symptoms of the classic triad; flank pain, gross haematuria and/or a palpable abdominal mass at the time of diagnosis. All 4 patients had one or more RCC s on the abdominal CT. The mean age at time of diagnosis was 45.4 years of age (31-63 years). One patient had bilateral RCC and one patient had two renal tumours in one kidney. Histopathology showed RCC with clear cell and chromophobe elements in three patients and chromophobe elements only in one patient. A thoracic CT was performed in all four patients that showed between 1 and 51 lung cysts in the basal parts of the lung. Recurrent episodes of pneumothorax (3 episodes) occurred in one patient. Three patients had multiple fibrofolliculomas in the face and upper neck. The family history for SP was positive in three patients and was positive in two patients for RCC in two patients (table 1). FLCN negative RCC patients (N=8) For the evaluation for the potential presence of BHD in a sporadic RCC cohort, we included 182 patients with sporadic RCC in the medical history. Between 2003 and 2013 a total of 112 patients underwent one or more thoracic CT s, in the remaining 70 patients only a chest X-ray was performed. Eleven patients met our inclusion criteria. Of these eight patients gave informed consent for a one time visit at our outpatient clinic (figure 1). The mean age was 64.9 years (53-73 years) at time of diagnosis. On thoracic CT all eight patients had at least one cyst in the basal parts of the lung. Four patients had one cyst in the basal parts of the lung, three patients had two cysts in the basal parts of the lung and one patient had 5 cysts in the basal parts of the lung respectively. None of the patients had bilateral or multifocal RCC. The histopathology was clear cell in six patients, chromophobe in one patient and sarcomatoid in one patient. The patient with 5 lung cysts had a history of three 122
123 Table 1. Characteristics of 4 RCC patients with pathogenic FLCN mutation and 8 RCC patients without a pathogenic FLCN mutation. Fibrofolliculomas FLCN mutation Lung cysts (N=) sp in medical history (N=) Patient Rcc Fam. Predisposition Histopathology Treatment Diagnosis (age) Location sp Rcc 1 Chromophobe Partial 63 Left + right Yes c.774_775delgtinscac 2 Chromophobe Partial 31 Left (N=2) Yes c.499c>t 3 Chromophobe Partial 56 Left No c.610_611delgcinsta 4 Chromophobe RFA 41 Left Yes c.1552delc 5 Clearcell Partial 63 Right No No 6 Chromophobe Total 73 Right No No 7 Clearcell Total 60 Right No No 8 Clearcell Partial 53 Left No No 9 Sarcomatoid Total 62 Left No No 10 Clearcell Partial 73 Left No No 11 Clearcell Total 69 Right No No 12 Clearcell Partial 66 Left No No 2.2 Lung cysts as indicator for BHD in rcc patients 123
124 episodes of SP; the other 7 patients had never experienced a SP. The familial history for SP and RCC was negative in all eight patients. FLCN mutation analysis was performed; in none of the eight patients a pathogenic FLCN mutation was found (table 1). 2.2 Lung cysts as indicator for BHD in rcc patients Discussion To date, ten hereditary renal cancer syndromes have been defined, accounting for 3-5% of all RCCs. 4 Based on the reported increased presence of multiple lung cysts under the carina in BHD patients we performed FLCN mutation analysis in a pilot study setting among 8 patients with a history of RCC and one or more lung cysts in the basal parts of the lung on thoracic CT. Although the history of smoking was not available in all patients, it was possible to distinguish between smoking related bullae in the apical parts of the lung and lung cysts on thoracic CT, as described by Fabre et al. 9 We found no pathogenic FLCN mutations in this group. Although no pathogenic FLCN mutation is found in this group, BHD is not excluded as only in 81-84% of clinical BHD cases a pathogenic germline FLCN mutation is found. 10 We compared the analysed the radiological findings to those in 4 proven FLCN mutation carriers with renal cancer. We found that multiple basal lung cysts were present significantly more frequent in FLCN mutation carriers and may be an indication for further evaluation of BHD syndrome in apparently sporadic RCC patients. However, since solitary cysts were found in both groups, the absence of multiple cysts does not appear to be a specific marker for the absence of BHD, as one BHD patient had only one cyst on thoracic CT. We therefore advise that in all RCC patients at least a concise family history is taken for the presence of RCC or SP and the skin is evaluated for the presence of fibrofolliculomas. In the presence of a positive family history (SP or RCC) or multiple basal lung cysts further investigation of BHD is indicated (e.g. by dermatological evaluation or by DNA testing). The difficulty in unmasking BHD patients in apparently sporadic RCC patients is illustrated by the negative family history for pneumothorax and RCC in the two FLCN mutation carriers. Based on our results, we conclude that lung cysts in RCC patients can be an indicator for underlying Birt-Hogg-Dubé syndrome, although the absence of presence of solitary lung cysts doesn t equate to the diagnosis of BHD. Further evaluation in larger RCC cohorts is required to confirm our findings. 124
125 References 1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008L:GLOBOCAN Int J Cancer 2010;127: Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61: Lee CT, Katz J, Fearn PA, Russo P. Mode of presentation of renal cell carcinoma provides prognosticinformation. UrolOncol 2002;7: Verine J, Pluvinage A, Bousquet G, Lehmann-Che J, de Bazelaire C, Soufir N, et al. Hereditary renal cancer syndromes: An update of a systematic review. EurUrology 2010; 58: Baba M, Hong S-B, Sharma N, Warren MB, Nickerson ML, Iwamatsu A, et al. Folliculin encoded by the BHD gene interacts with a binding protein, FNIP1, and AMPK, and is involved in AMPK and mtor signaling. Proc Nat AcadSci USA 2006;103: Maffé A, Toschi B, Genuardi M. Birt-Hogg-Dubé syndrome (BHDS). Atlat Genet Cytogenet Oncol Haematol. 2014; 18(7): Houweling AC, Gijezen LM, Jonker MA, van Doorn MB, Oldenburg RA, van Spaendonck-Zwarts KY, et al. Renal cancer and pneumothorax risk in Birt- Hogg-Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer 2011;105: Toro JR, Schmidt LS, Nickerson ML, et al. Germline BHD-mutation spectrum and phenotype analysis of a large cohort of families with Birt-Hogg-Dubé syndrome. Am J Hum Genet. 2005;76: Fabre A, Borie R, Debray MP, Crestani B, Danel C. Distinguishing the histological and radiological features of cystic lung disease in Birt-Hogg- Dubé syndrome from those of tobacco-related spontaneous pneumothorax. Histopathology 2014;65(5): Menko FH, van Steensel MAM, Giraud S, Friis- Hansen L, Richard S, Ungari S, Nodenskjöld M, Hansen TvO, Solly J, Maher ER. Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncol 2009;10: Lung cysts as indicator for BHD in rcc patients 125
126
127 chapter 2.3 Renal imaging in 199 Dutch patients with Birt-Hogg-Dubé syndrome: screening, compliance and outcome Paul C. Johannesma 1, Irma van de Beek 2, Rinze Reinhard 3 4, Edward M. Leter 5, Rence Rozendaal 6, Theo M. Starink 7, JanHein T.M. van Waesberghe 3, Simon Horenblas 8, Marianne A. Jonker 9, Pieter E. Postmus 10, Arjan C. Houweling 2, R. Jeroen A. van Moorselaar 11 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 3 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 4 Department of Radiology, Onze Lieve Vrouwe Gasthuis, Amsterdam, The Netherlands 5 Department of Clinical Genetics, Maastricht University Medical Center, Maastricht, The Netherlands 6 Department of Pathology, VU University Medical Center, Amsterdam, The Netherlands 7 Department of Dermatology, Leiden University Medical Center, Leiden, The Netherlands 8 Urologic Oncology and Department of Urology, The Netherlands Cancer Institute, Amsterdam, The Netherlands 9 Department of Epidemiology and Biostatistics, VU University Medical Center, Amsterdam, The Netherlands 10 Department of Thoracic Oncology, Clatterbridge Cancer Centre, Liverpool Heart & Chest Hospital, University of Liverpool, Liverpool, United Kingdom 11 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands Submitted
128 2.3 Renal imaging in BHD patients Abstract Background information Birt-Hogg-Dubé syndrome (BHD) is an autosomal dominant disorder caused by germline mutations in the FLCN gene characterized by skin lesions, pneumothorax and an increased risk of renal cell cancer (RCC). Renal surveillance in BHD is recommended, but the optimal imaging method and screening interval remain to be defined. Local treatment is based on the 3 cm rule, which recommends surgical intervention when the (largest) lesion exceeds 3 cm in diameter. The aim of our study was to retrospectively evaluate the compliance with and outcomes of renal cancer surveillance in patients diagnosed with BHD in two centers. Methods Surveillance data of 199 patients diagnosed with BHD in two hospitals were collected. Data were collected form medical files and a questionnaire. In addition, we evaluated renal imaging follow up data and the medical records of 23 BHD patients with renal cell carcinoma (RCC). Results Initial screening for RCC was performed in 171/199 patients (86%) and follow up data were available from 117/171 patients (68%). A total follow-up period of 499 patient years was available. Of the patients that performed follow-up surveillance, 85% was investigated at least yearly and 96% at least every two years. A medical history of RCC was present in 23 patients, 38 tumours were diagnosed with a mean age of the first tumour of 51 years. In 21 tumours ultrasound (US) was performed. Eleven tumours sized 7-27 mm were visible on MR or CT and not detected using US. Conclusions Our data indicate that compliance to renal screening is relatively high and that US might be a sensitive, cheap and widely available imaging modality for detecting clinically relevant renal tumours in BHD patients, since no tumours exceeding 3 cm were missed with US. Follow up studies in BHD patient cohorts are required to further determine the optimal screening method and interval in BHD patients. 128
129 Introduction Birt-Hogg-Dubé syndrome (BHD, OMIM #315150) is an autosomal dominant condition characterized by fibrofolliculomas, lung cysts, spontaneous pneumothorax and renal tumours, due to germline mutations in the FLCN gene encoding folliculin. 1 In the initially reported family skin lesions were the only clinical manifestations. 2 Subsequently, renal cell carcinoma (RCC) and spontaneous pneumothorax were found to be part of the syndrome The functions of folliculin have partly been clarified and are likely to include a role in the mammalian target of rapamycin (mtor) pathway and in ciliary function Around 3-5% or of all RCCs are estimated to have a hereditary cause due to genetic predisposition. 9 Hereditary RCCs differ from the far more common sporadic form in several aspects. Hereditary tumours often present at an early age, are more often multifocal and / or bilateral and may have a characteristic histology. In addition, they may be associated with recognizable syndromic features besides renal cancer. In addition, the family history may be positive for RCC or syndromic clinical features. In BHD the prevalence of RCC is estimated to be 16-34% with a mean age at diagnosis of 50 years (range years) The most commonly reported histological subtypes of BHD associated renal tumours are hybrid oncocytic, chromophobe renal cell carcinoma and oncocytoma. However, other subtypes may also occur Given the high degree of inter- and intra familiail variability of these features, it is likely that many cases of hereditary RCC currently remain unrecognized. Renal surveillance in BHD patients has been recommended from age 20, preferably by annual MRI (Magnetic Resonance Imaging). This is based on the high sensitivity and the lack of radiation exposure. 17 However, its availability and cost may be limitations in clinical practice. The aim of our study is to retrospectively evaluate the compliance to, and the outcomes of renal cancer surveillance in patients diagnosed with BHD in two Dutch centers. 2.3 Renal imaging in BHD patients Patients and methods The suspected diagnosis of BHD in successively referred patients was based on patient and pedigree data and confirmed by FLCN mutation testing. The collection of family data and the methods of mutation analysis have been outlined in previous publications For the current study we collected data of 199 patients diagnosed with BHD at the VU University Medical Center and The Netherlands Cancer Institute. Our cohort includes both symptomatic index patients and healthy family members identified by pre-symptomatic DNA testing. We retrieved screening data from the medical files and we sent a questionnaire on performed surveillance in other medical institutions. Patients were included until June The study was approved by the ethical committee of the VU University Medical Center. We collected all available renal imaging follow up data and the medical records of 23 BHD patients with renal cell carcinoma (RCC). For evaluation of compliance with surveillance, we assessed initial screening and follow up surveillance data. Initial screening was defined as the first renal imaging after a maximum period of one year after the clinical or genetic diagnosis of BHD. Patients diagnosed with (symptomatic) RCC before the diagnosis of BHD were excluded, since their tumours were not detected by screening. Patients were included in the analysis of follow-up if de patient met the following criteria; The last screening from which data was available, was performed in 2013 or 2014, the questionnaire was returned and no screening was performed in 2013 or 2014 and the last screening was performed within one and a half years before death. 129

130 2.3 Renal imaging in BHD patients Results Screening compliance Initial screening was performed in 171 patients (86%) and follow-up data were available of 117 patients (68%). Figure 1 shows a flowchart of the population. Of the 27 patients excluded from analysis of followup, 10 were diagnosed with RCC before they were diagnosed with BHD, 2 decided not to undergo screening because of older age and 2 died within 1,5 years after the diagnosis of BHD. It was unclear whether or not initial screening was performed in 13 patients. No follow-up data was available for 54/174 patients, of which 16 had a recent diagnosis and initial screening was performed less than 1,5 year ago. The mean age of initial screening was 50 (median 51, range 20-83). The data of initial screening and follow-up screening are shown in table 1. Initial screening consisted predominantly of ultrasound (US) and MRI. The follow-up screening was predominantly performed by US. The total follow-up time was 499 patient years (mean 4,2; median 4; range 1-9). Most of the missed screening moments occurred in the first year of follow-up (12%). From the second to ninth year approximately 3-7% of patients per year missed a screening moment. Figure 1. Flow diagram of screening data in the study population. 130
131 Table 1. Overview of initial and follow-up screening per year. Initial screening (%) Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7 Year 8 Year 9 Total MRI + US 119 (69,6) US 9 (5,3) MRI 31(18,1) Other 18 (10,5) Unknown technique 3 (1,8) No screening (%) NA 14 (12,0) 3 (3,0) 5 (5,7) 4 (5,8) 2 (4,3) 2 (6,7) 1 (4,0) 1 (6,7) 0 CT, CT and US or CT and MRI Self-reported screening with questionnaire in which technique was not mentioned. NA: not applicable The majority of patients (99/117, 85%) was screened at least once a year, 112/117 patients (96%) were screened at least once every two years. Detected RCCs A total of 23 patients (13 male) had a medical history of RCC. The mean age at diagnosis of the first RCC was 51 (range 24-77). Ten patients developed RCC before they were diagnosed with BHD. Nine and five patients were diagnosed at initial screening and during follow-up respectively (one patient was diagnosed both at initial screening and follow-up). Eight patients were the first person in the family to be diagnosed with BHD. Six of them were already known with RCC at the time of diagnosis of BHD. The other 15 patients were diagnosed with BHD by (pre-)symtpomatic DNAtesting. Even though there are many missing data, the available data suggest that the majority of RCCs are asymptomatic. Table 2 shows tumour and patient characteristics. In total, 38 tumours were detected in 23 patients. Of one tumour no data was available since the treatment was performed 34 years ago. The histology of available tumours (n=25) was either chromophobe (32%), clearcell (32%), mixed chromophobe/clearcell (12%), papillary (12%), hybrid oncocytic/chromophobe (4%), sarcomatoid (4%) or unclassified (4%). There was a wide variability between the detection method(s) of these tumours. US was performed in 21 tumours. Ten tumours, sized 20 to 120 mm, were detected by US. Eleven tumours, sized 7 to 27 mm, were seen on MRI or CT and missed by US. Five patients died, of which four had metastic disease at the time of diagnosis of RCC. All four were diagnosed with RCC before they were diagnosed with BHD. No patients were diagnosed with metastasized RCC during follow-up after the BHD diagnosis. Local treatment of RCCs consisted of either total nephrectomy, partial nephrectomy, cryo-ablation or radio frequent ablation. All RCCs, except one, were treated independent of size. 2.3 Renal imaging in BHD patients 131
132 Table 2. Detected RCCs: tumour and patient characteristics. Gender Age at Tumour size diagnosis (mm) Moment of diagnosis Symptomatic Detected with Missed with Last screening Outcome 2.3 Renal imaging in BHD patients F (PA) 60 (PA) 20 (PA) 11 (PA) <BHD <BHD <BHD <BHD AS CT CT CT CT 7 years FU M <BHD S CT Metastasis at diagnosis, died M <BHD S CT + US Metastasis at diagnosis, died M Initial AS MRI (+2nd US) US 3 years FU F FU U US Unknown 5 years FU F (6 months later) Initial AS MRI MRI MRI F Initial AS MRI + CT NA M M US US Initial AS MRI + CT US (6 months before) Initial Initial Initial AS CT CT + US CT F Initial AS MRI US (2 months before) US US 4 years FU NA 4 years FU 3 years M <BHD U MRI + US Metastasis at diagnosis, died F FU U MRI US 1 year ago: MRI+US M Initial FU FU MRI +US MRI MRI+US US 1 year ago: MRI+US NA 2 years since last tumour M 69 3 Initial U MRI 3 years FU: tumour now 9 mm M FU U MRI + US 1 year ago: MRI + US M <BHD U MRI+US Metastasis at diagnosis, died NA 132
133 Table 2. Detected (continued) RCCs: tumour and patient characteristics. Gender Age at Tumour size diagnosis (mm) Moment of diagnosis Symptomatic Detected with Missed with Last screening Outcome F <BHD U MRI + US 10 years FU M (multifocal) (multifocal) <BHD AS CT Unknown F FU AS CT US 6 months before: US 1 year FU F (PA) <BHD S CT + US 21 years FU M M (PA) 23 (PA) 17 (PA) <BHD AS CT CT <BHD AS CT CT CT 2 years FU Died due to metastasis of other malignancy F Initial S CT 2 years FU Gender: F ; female, M; male Tumour size: reported as size on imaging when available. In case of both US and CT/MRI is size on CT or MRI reported. In case of both CT and MRI, the largest described size is reported. PA; size measured at pathology, no imaging size available. Moment of diagnosis: < BHD; Diagnosis of RCC before the diagnosis of BHD, FU; tumour diagnosed at follow-up, Initial; tumour diagnosed at initial screening, Outcome: NA; not applicable 2.3 Renal imaging in BHD patients Discussion To gain insight in optimal screening regimens in rare genetic cancer predisposition syndromes, it is crucial to study data of patient cohorts collected from specialized centers. We were able to collect data from 199 Dutch patients diagnosed with BHD in two Dutch centers. The recommended screening program in the Netherlands has changed over the years. Initial screening in BHD patients diagnosed at the VU University Medical Center, has consisted of both MRI and US followed by annual US Currently, initial screening consists of MRI only. The goal of initial screening by both MRI and US was to gain more insight in the optimal screening technique, since there are no evidence based guidelines for screening in BHD patients. The change to MRI only was based on expert opinion. As expected, the data show that a majority of initial screening consisted of both MRI and US (69,9%) and that a majority (54,3%) of follow-up screening consisted of US only. In some patients annual imaging is performed in the academic hospital. However, the majority of patients is screened in local or regional non-academic hospitals. This makes it difficult to be up to date about the screening compliance and outcomes. Using questionnaires, we tried to collect these data of as many patients as possible. The presented data show that at least 87% of the BHD patients performed initial screening. Excluding patients with a diagnosis of RCC before the diagnosis of BHD, and patients that died within 1,5 year after the diagnosis of BHD, this number increased to 91% (171/187). The true percentage might be slightly lower or higher, since no data was available from 13 patients. 133
134 2.3 Renal imaging in BHD patients Our cohort of patients with BHD participating in the screening program, is highly compliant to the recommended screening regimen (85%). The fact that the most missed screening moments were in the first year after initial screening, might be discussed during genetic counseling. A possible explanation is that patients are less aware of their own responsibility to organize the follow-up screening via their general practitioner. The number of patients declining screening and their reasons to do so remain unclear. The screening compliance is comparable to that described in patients with Lynch syndrome (87%) It has been established that that most renal masses in the general population grow slowly. In several studies the natural growth of presumed renal cancer in general (non-bhd) patients who were not surgical candidates due to comorbidity was examined. The annual growth rate of the renal masses was measured during active surveillance (AS) and was between cm / year, with a median follow-up of months One of these studies reported tumour size to be a predictor of tumour growth rate, with lower growth rates of renal masses <2.45 cm compared to masses >2.45 cm. 20 However Chawla et al. concluded that renal tumour size at presentation does not appear to be a reliable predictor for growth rate and to their opinion serial radiographic data alone are insufficient to predict the natural history of renal masses. 22 It is remarkable that during active surveillance some benign lesions (e.g., AML and oncocytoma) increased in size, while some biopsy-proven RCC s did not grow and, in some cases even decreased in size. 19 The biological behaviour of renal cell cancer in several hereditary tumour syndromes is, in most cases, reported to be indolent and metastases rarely occur at smaller tumour sizes. Taking into account the relatively high frequency of multiple or bilateral tumours, parenchymal sparing surgical treatment is important in patients with a hereditary predisposition for renal cancer. The aims of the treatment are local tumour control, preservation of renal function and prevention of metastatic disease. Nephron sparing treatment is often possible, as tumours in patients who undergo regular renal screening are usually discovered at a small size. Currently, the 3 cm rule, which recommends surgical intervention when the (largest) lesion exceeds 3 cm in diameter, is often applied to patients with Von Hippel Lindau disease, hereditary papillary renal cell cancer and BHD In a study among patients adhering to this 3 cm rule, no metastatic disease was reported with more than 10 years follow-up in 49 patients with hereditary renal cell cancer. It must be noted that in this study only 1 patient with BHD was included. 26 In our group of 23 BHD patients diagnosed with RCC, all but one patient underwent local treatment. In one patient, a tumour of 3 mm was detected. Three years later, this tumour was sized 9 mm and imaging was performed frequently. The treatment of tumours smaller than 3 cm was probably at the request of the patient due to anxiety for possible development of metastasis. Furthermore, the increasing availability of less invasive treatment options as radiofrequent ablation or cryotherapy might play a role in these decisions. When screening BHD patients, it is crucial to at least enable following the often recommended 3 cm rule. Therefore, no tumours larger than 3 cm should be missed by the applied screening technique and the screening interval must ensure that no tumours larger than 3 cm develop during the screening interval. The main techniques to be considered for imaging of renal tumours are CT, MRI and ultrasound. These imaging modalities each have their strengths and weaknesses. CT is a fast and robust 134
135 technique to display the kidneys three-dimensionally and with great anatomic detail. CT is the gold standard for the diagnosis and staging of renal cell carcinoma 29. Despite these qualities, the use of CT for annual surveillance would lead to unacceptably high cumulative radiation dose as patients will need many CT scans during their lifetime. 30 MRI is a technique that provides excellent soft tissue contrast without the use of radiation. It is powerful for the detection and characterization of focal renal lesions, various RCC subtypes can be differentiated and patency of blood vessels can be shown without the use of intravenous contrast. Drawbacks of MRI are long examination times (30-45 minutes), variations in quality and scan protocol, limited availability and high cost. 28 In some patients MRI cannot be performed due to contra-indications like claustrophobia, obesity, or the presence of metallic implants. US has the advantages that it is widely available, fast, cheap and without use of ionizing radiation. However small renal lesions can be missed due to limited spatial resolution of US depending on intrarenal location, isoechoic aspect of a lesion, large patient size or obscuring bowel gas Furthermore US depends on operator experience. Renal imaging with 1-3 year intervals has been proposed for BHD patients without renal lesions on initial imaging In our cohort, 11/21 tumours were missed by US. All missed tumours were smaller than 3 cm (largest 27 mm). Five of our patients were imaged within 1 year before diagnosis of RCC. One tumour larger than 3 cm (4 cm) was diagnosed within 1 year after a previous RCC in the same kidney, which was treated with a partial nephrectomy. One year prior, this tumour was not seen on both MRI and US. No metastatic disease occurred in this patient during a follow up period of 2 years. Based on the findings in our BHD cohort, US screening may be an adequate strategy since no relevant tumours were missed on US. However, a 40 mm tumour was found one year after imaging with MRI. This suggests that the screening interval might be too long. However, given the often indolent nature of BHD kidney cancer and the small number of patients, this remains to be further clarified. In addition, the total number of RCCs was relatively small and therefore, further evaluation in larger patient groups is required. Consistent with current literature, no metastatic disease occurred in patients with RCC <3 cm. 2.3 Renal imaging in BHD patients Conclusions Our main findings are that the vast majority of patients undergo initial screening and that 85% of patients in the screening program are compliant with yearly renal imaging. In our patient cohort no tumours larger than 3 cm visible on MRI or CT were missed with US and metastatic disease only occurred in tumours larger than 3 cm diagnosed at initial screening. Our findings are in line with the conclusions of Jamis-Dow et al that US is a sensitive method for detecting renal lesions larger than 3 cm in BHD patients. 31 It might be important to give more attention to the recommended screening program, especially the first follow-up moment after initial screening. Further studies are needed to determine whether our results for BHD patients in this study can be reproduced, preferably in a relatively large group of patients with screening by both MRI and ultrasound. 135
136 2.3 Renal imaging in BHD patients ReferenceS 1. Nickerson ML, Warren MB, Toro JR, et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg-Dubé syndrome. Cancer Cell 2002;2: Birt AR, Hogg GR, Dubé WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol. 1977;113: Chung JY, Ramos Caro FA, Beers B, et al. Multiple lipomas, angiolipomas, and parathyroid adenomas in a patient with Birt-Hogg-Dubé syndrome. Int J Dermatol 1996;35: Roth JS, Rabinowitz AD, Benson M, et al. Bilateral renal cell carcinoma in the Birt-Hogg-Dubé syndrome. J Am Acad Dermatol. 1993;29: Toro JR, Pautler SE, Stewart L, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med 2007;175: Hasumi Y, Baba M, Ajima R, et al. Homozygous loss of BHD causes early embryonic lethality and kidney tumor development with activation of mtorc1 and mtorc2. Proc Natl Acad Sci U.S.A. 2009;106: Hasumi Y, Baba M, Hasumi H, et al. Folliculin (Flcn) inactivation leads to murine cardiac hypertrophy through mtorc1 deregulation. Hum Mol Genet 2014;23: Luijten MN, Basten SG, Claessens T, et al. Birt- Hogg-Dubé syndrome is a novel ciliopathy. Hum Mol Genet 2013;22: Barrisford GW, Singer EA, Rosner IL, et al. Familial renal cancer: molecular genetics and surgical management. Int J Surg Oncol. 2011;2011: Houweling AC, Gijezen LM, Jonker MA, et al. Renal cancer and pneumothorax risk in Birt-Hogg-Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer 2011;105: Khoo SK, Giraud S, Kahnoski K, et al. Clinical and genetic studies of Birt-Hogg-Dubé syndrome. J Med Genet 2002;39: Toro JR, Wei MH, Glenn GM, et al. BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet 2008;45: Benusiglio PR, Giraud S, Deveaux S, et al. Renal cell tumour characteristics in patients with the Birt-Hogg-Dubé cancer susceptibility syndrome: a retrospective, multicentre study. Orphanet J Rare Dis 2014;9: Linehan WM, Pinto PA, Bratslavsky G, et al. Hereditary kidney cancer: unique opportunity for diseasebased therapy. Cancer 2009;115(10Suppl): Murakami T, Sano F, Huang Y, et al. Identification and characterization of Birt-Hogg-Dubé associated renal carcinoma. J Pathol 2007;211: Woodwared ER, Ricketts C, Killick P, et al. Familial non-vhl clear cell (conventional) renal cell carcinoma: clinical features, segregation analysis, and mutation analysis of FLCN. Clin Cancer Res. 2008;14: Menko FH, van Steensel MA, Giraud S, et al. Birt- Hogg-Dubé syndrome: diagnosis and treatment. Lancet Oncol 2009;10: Leter EM, Koopmans AK, Gille JJ, et al. Birt-Hogg- Dubé syndrome: clinical and genetic studies of 20 families. J Invest Dermatol. 2008;128: Newton K, Green K, Lalloo F, et al. Colonoscopy screening compliance and outcomes in patients with Lynch syndrome. Colorectal Dis 2015;17: Jewett MAS, Mattar K, Basiuk J, et al. Active surveillance of small renal masses: Progression patterns of early stage kidney cancer. Eur Urol 2011;60: Mason RJ, Abdolell M, Trottier G, et al. Growth kinetics of renal masses: Analysis of a prospective cohort of patients undergoing active surveillance. European Urology 2011;59: Abou Youssif T, Kassouf W, Steinberg J, et al. Active surveillance for selected patients with renal masses: updated results with long-term follow-up. Cancer 2007;110: Chawla SN, Crispen PL, Hanlon AL, et al. The natural history of observed enhancing renal masses: Metaanalysis and review of the world literature. The Journal of Urology 2006;175: Rosales JC, Haramis G, Moreno J, et al. Active surveillance for renal curtail neoplasms. J Urol 2010;183: Choyke PL, Glenn GM, McClellan WM, et al. Hereditary renal cancers. Radiology 2003;226:
137 26. Stamatakis L. Metwalli AR, Middelton LA, et al. Diagnosis and management of BHD-associated kidney cancer. Fam Cancer 2013;12: Herring JC, Enquist EG, Chernoff A, et al. Parenchymal sparing surgery in patients with hereditary renal cell carcinoma: 10-year experience. J Urol 2001;165: Walther MM, Choyke PL, Weiss G, et al. Parenchymal sparing surgery in patients with hereditary renal cell carcinoma. J Urol 1995;153: Sacco E, Pinto F, Totaro A, et al. Imaging of renal cell carcinoma: state of the art and recent advances. Urol Int 2011;86: Sodickson A, Baeyens PF, Andriole KP, et al. Recurrent CT, cumulative radiation exposure, and associated radiation-induced cancer risks from CT of adults. Radiology 2009;251: Jamis-Dow CA, Choyke PL, Jennings SB, et al. Small (< or = 3-cm) renal masses: detection with CT versus US and pathologic correlation. Radiology 1996;198: Renal imaging in BHD patients 137
138
139 PART 3 Relevant Case Series and Case Reports
140
141 chapter 3.1 In-flight pneumothorax: diagnosis will be missed due to symptom delay Pieter E. Postmus 1, Paul C. Johannesma 2, Fred H. Menko 3, Marinus A. Paul 4 1 Department of Thoracic Oncology, Clatterbridge Cancer Centre, Liverpool Heart & Chest Hospital, University of Liverpool, Liverpool, United Kingdom 2 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 3 Family Cancer Clinic, The Netherlands Cancer Institute, Amsterdam, The Netherlands 4 Department of Thoracic Surgery, VU University Medical Center, Amsterdam, The Netherlands Am J Respir Crit Care Med. 2014;190(6):704-5
142
143 Introduction Boyle s law describes the inverse relationship between pressure and volume for gas in a closed system at constant temperature. Based on this mechanism, an air-filled lung cyst will increase in size if brought in an environment with a lower atmospheric pressure. Patients with cystic lung disease might therefore be at risk of developing pneumothorax during air travel. Many persons have cystic changes in the lung, but the number of reported in-flight pneumothorax is very low. 1 This apparent discrepancy seems at first sight strange, but is in fact what one might expect. Any cystic airspace in the lung will not expand in size if connected to the bronchial tree, because there is no possibility to develop intracystic overpressure. However, if there is no connection between an air-filled cyst and the bronchial tree, the cyst will increase in size with 25-30% which may lead to rupture of the cyst. 2 This is not sufficient for developing pneumothorax, the visceral pleura needs to rupture as well. This may occur if a cyst is adjacent to the visceral pleura. But even then it is very unlikely that this will result in symptomatic pneumothorax within a few hours since there will be no or very little transport of air into the pleural cavity. We hypothesize that a pneumothorax developed during air travel will become symptomatic hours, or even more likely days, after air travel. We here report a patient with Birt-Hogg-Dubé syndrome who developed pneumothorax following air travel and was manifested later. 3.1 In-flight PTX in BHD patients Case report A 38-year-old male was diagnosed to have BHD after his uncle had been diagnosed with facial skin fibrofolliculomas. Three family members were found to carry the same pathogenic FLCN germline mutation, his father and brother are asymptomatic, but the patient s sister had a history of recurrent bilateral pneumothorax. The patient works for a commercial international firm and travels quite often, the mean number of flights per year during the last 6 years was 12. His first pneumothorax, at the age of 34, was treated by drainage through a chest tube. Within 2 months he developed a contralateral pneumothorax. Bilateral apical pleurectomy was performed. Four years later he flew transatlantic. He had no complaints during or after this flight. He visited, while still without complaints day after arrival one of the world s highest towers and used the speed lift to 410 m in around 45 seconds. After descent to sea level he noticed acute serious shortness of breath. Chest X-ray demonstrated a left-sided pneumothorax with considerable collapse in the basal part. He flew back to Europe with a Heimlich valve connected to a chest tube and was referred for additional treatment. As the last event occurred during a rapid change in atmospheric pressure (speed lift) and shortly after a transatlantic flight, he checked at home his old diaries for his flight pattern around the earlier episodes of pneumothorax. The first pneumothorax was diagnosed on December 17, 2010, complaints starting the day before diagnosis, he flew on the 8 th and 12 th that month within Europe. At discharge from the hospital there was radiological proof of complete resolution. His contralateral pneumothorax was diagnosed on January 31 after some shortness of breath starting the 30st, he flew transatlantic on the 17 th and 21 st the same month. 143
144 3.1 In-flight PTX in BHD patients Discussion BHD syndrome is autosomal dominant inherited, caused by germline mutations in the FLCN (folliculin) gene and is clinically characterized by facial fibrofolliculomas, pulmonary cysts, recurrent pneumothorax and an increased risk for renal cell cancer. 3 All BHD patients with (recurrent) pneumothorax have pulmonary cysts, especially in the lower lobes. The cysts are located both in the parenchyma and subpleural area. We analysed the lungs by CT of 18 other BHD patients with a history of at least one episode of pneumothorax, all patients had subpleural cysts and 50% of all cysts were located subpleural. 4 Very small subpleural cysts might have been missed on a standard CT. 5 Several studies on the role of atmospheric pressure changes showed that the interval after the trigger, assumed to be the change in atmospheric pressure, resulted with some delay into clustering of admitted patients with a spontaneous pneumothorax. 6 For instance Scott and colleagues reported a delay up to 4 days after a significant change in atmospheric pressure. 7 Considering the pressure changes during the subsequent flights as potential trigger for initiating rupture of a subpleural cyst, this implies that the interval between air travel and the diagnosis is respectively 5 and 9 days (1 st episode), respectively 10 and 14 days (2 nd episode) and 2 days or immediately after use of a speed lift (3 nd episode of pneumothorax). The latter gives a much faster change (68 hpa/min) in outside pressure than during ascent (<13.3 hpa/min) in commercial air travel 8 and might cause a rupture of a cyst by itself or, more likely based on start of patient s complaints, aggravate a small pneumothorax developed during the flight 2 days earlier. Hoshika and colleagues reported no relationship between development of spontaneous pneumothorax and 2142 flights among 48 BHD patients. 9 Three patients reported tightness of the chest. Unfortunately there were no details on the length of period after flying and the moment of becoming symptomatic of the pneumothoraces, this makes it uncertain whether there might have been a possible delay after the pressure change as in our patient. Striking is the reduction in number of flights in this series after the patients became aware of the underlying cause. Although the reported patient flew more than one week after complete resolution of his first pneumothorax, the character of the disease makes it questionable whether current BTS guidelines on pneumothorax and flying are applicable for these patients. 10 One of the hallmarks of pneumothorax in BHD patients is the high recurrence rate, 59% in 53 cases. 11 Rupture of a subpleural cyst is the likely cause of the pneumothorax in BHD patients. These cysts are found throughout the lungs with the majority in the lower halves of the lungs, this implies that treatment to prevent recurrence should have as aim pleurodesis of the whole pleura visceralis, not only in the apical region. This can be done by extensive pleurectomy and/or talc pleurodesis. From this perspective the initially performed bilateral apical pleurectomy after the pneumothorax in the reported patient is inadequate as was also found in our retrospective series. 11 Kumasaka et al analyzed resected lung specimens of 50 BHD patients. 12 Out of 229 cysts that were found; 50% were located in the subpleural area and less than 5% abut on bronchioles. Subpleural cyst are by definition far from the larger airways, so if a cyst would be connected to the bronchial tree the size of connection to the airways is very small, resulting in small volumes of air transported into the pleural cavity. Therefore it will probably take a long time before troublesome symptoms are present. This concept of delayed symptoms after the actual rupture of a cyst is probably as well relevant for other diseases with cystic changes in the lung, such as lymphangioleiomyomatosis or Langerhans cell histiocytosis assuming there is no (large) connection between airways and cyst. 144
145 Furthermore spontaneous resolution of a small pneumothorax after rupture of a subpleural cyst may occur if there is no active transport of gas into the pleural cavity. Evidence that this occurs in vivo comes from the presence of inflammation at the pleural side of the majority of the cysts 13 and the demonstration of pleural inflammation in patients with a pneumothorax. 14 In a survey among 190 patients with BHD we found that of the group with a previous pneumothorax, twelve other patients had a total of 13 episodes of pneumothorax within 31 days after a continental or intercontinental flight. 15 The interval between flying and diagnosis of pneumothorax was < 10 days in 6 cases, between 10 and 20 days in 4 and between 20 and 30 days in 3. This supports our hypothesis that the delay of becoming symptomatic should be taken into account if a relation between atmospheric pressure changes and pneumothorax is studied. Consequently BHD patients who have minimal chest symptoms after the first flight should be checked for pneumothorax before the return flight, because presence of pneumothorax, even if it is small, is a known risk factor for flying In-flight PTX in BHD patients 145
146 3.1 In-flight PTX in BHD patients References 1. Hu X, Cowl CT, Baqir M, Ryu JH. Air travel and pneumothorax. Chest 2014; 145: BTS statement. Managing passengers with respiratory disease planning air travel: British Thoracic Society recommendations. Thorax 2002; 57: Menko FH, van Steensel MA, Giraud S, Friis-Hansen L, Richard S, Ungari S, Nordenskjöld M, Hansen TV, Solly J, Maher ER; European BHD Consortium. Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncol 2009; 10: Johannesma PC, van Waesberghe JHTM, Reinhard R, Gille JJP, van Moorselaar RJA, Houweling AC, Starink ThM, Menko FH, Postmus PE. Birt- Hogg-Dubé syndrome patients with and without pneumothorax: findings on chest CT. Am J Resp Crit Care Med ajrccm-conference _ Meeting Abstracts.A Onuki T, Goto Y, Kuramochi M, Inagaki M, Bhunchet E, Suzuki K, Tanaka R, Furuya M. Radiologically indeterminate pulmonary cysts in Birt-Hogg-Dubé syndrome. Ann Thorac Surg 2014; 97: Haga T, Kurihara M, Kataoka H, Ebana H. Influence of wheather conditions on the onset of primary spontaneous pneumothorax: positive association with decreased atmospheric pressure. Ann Thorac Cardiovasc Surg 2013; 19: Scott GC, Berger R, McKean HE. The role of atmospheric pressure variation in the development of spontaneous pneumothoraces. Am Rev Resp Dis 1989; 139: Araki K, Okada Y, Kono Y, To M, To Y. Pneumothorax recurrence related to high-speed lift. Am J Med (in press) 9. Hoshika Y, Kataoka H, Kurihara M, Anod K, Sato T, Seyama K, Takahashi K. Features of pneumothorax and risk of air-travel in Birt-Hogg-Dubé syndrome (abstract). Am J Resp Crit Care Med 2012; 185: A Josephs LK, Coker RK, Thomas M, on behalf of the BTS air travel working group. Managing patients with stable respiratory disease planning air travel: a primary care summary of the British Thoracic Society recommendations. Prim Care Respir J 2013; 22: Johannesma PC, Jonker MA, van der Wel JWT, van Waesberghe JHTM, van Moorselaar RJA, Menko FH, Postmus PE. Management of spontaneous pneumothorax in patients with or without Birt- Hogg-Dubé syndrome [abstract[. ERS Kumasaka T, Hayashi T, Mitani K, Kataoka H, Kikkawa M, Tobino K, Kobayasha E, Gunji Y, Kunogi M, Kurihara M, Seyama K.Characterization of pulmonary cysts in Birt-Hogg-Dubé syndrome: histopathological and morphometric analysis of 229 pulmonary cysts from 50 unrelated patients. Histopathology (in press) 13. Furuya M, Tanaka R, Koga S, Yatabe Y, Gotoda H, Takagi S, Hsu Y-H, Fujii T, Okada A, Kuroda N, Moritani S, Mizino H, Nagashima Y,Nagaham K, Hiroshima K, Yoshino I, Nomura F, Aoki I, Nakatani Y. Pulmonary cysts of Birt-Hogg-Dubé syndrome: a clinicopathological and immunohistochemical study of 9 families. Am J Surg Pathol 2012; 36: Lichter I, Gwynne JF. Spontaneous pneumothorax in young subjects. A clinical and pathological study. Thorax 1971; 26: Johannesma PC, van der Wel JWT, Paul MA, Houweling AC, Jonker MA, van Waesberghe JHTM, van Moorselaar RJA, Menko FH, Postmus PE. Commercial air travel and diving in patients with Birt-Hogg-Dubé syndrome [abstract]. ACCP (submitted) 16. Ho BL. A case report of spontaneous pneumothorax during flight. Aviat Space Environ Med 1975; 46:
147
148
149 chapter 3.2 Spontaneous pneumothorax as indicator for Birt-Hogg-Dubé syndrome in pediatric patients Paul C. Johannesma 1, Ben E.E.M. van den Borne 2, Ad F. Nagelkerke 3, JanHein T.M. van Waesberghe 4, Marinus A. Paul 5, R. Jeroen A. van Moorselaar 6, Fred H. Menko 7 8, Pieter E. Postmus 1 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Pulmonary Diseases, Catharina Hospital, Eindhoven, The Netherlands 3 Department of Pediatrics, VU University Medical Center, Amsterdam, The Netherlands 4 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 5 Department of Thoracic Surgery, VU University Medical Center, Amsterdam, The Netherlands 6 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 7 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 8 Department of Clinical Genetics, The Netherlands Cancer Institute, Amsterdam, The Netherlands BMC Pediatr Jul 3;14:171
150 3.2 Abstract Background Birt-Hogg-Dubé syndrome (BHD) is a rare autosomal dominant inherited disorder caused by germline mutations in the folliculin (FLCN) gene. Clinical manifestations of the BHD syndrome include fibrofolliculomas, renal tumours, lung cysts and (recurrent) spontaneous pneumothorax. All clinical manifestations usually present in adults from the age 20 onward. SP as indicator for BHD in pediatric patients Material and methods Two non-related patients with a history of (recurrent) pneumothorax from the age of 14 and multiple basal lung cysts on thoracic CT were screened for a pathogenic FLCN mutation. Results A pathogenic FLCN mutation was found in both patients. No skin fibrofolliculomas or renal abnormities were found. Conclusion Although childhood occurrence of SP in BHD is rare, these two cases illustrate that BHD should be considered as cause of SP during childhood. 150
 spontaneous pneumothorax (SP) and renal cancer.")
 pneumothorax occurred from the age of 14. 3.")
151 Introduction Birt-Hogg-Dubé (BHD) is a rare tumor syndrome first described in The syndrome is characterized by skin fibrofolliculomas, lung cysts, (recurrent) spontaneous pneumothorax (SP) and renal cancer. The underlying germline mutation is located in the folliculin (FLCN) gene on chromosome 17p11.2. Although clinical manifestation usually appears after the age of 20, we here present two cases of BHD wherein episodes of (recurrent) pneumothorax occurred from the age of Patient presentation 1 A 14-year-old Caucasian apparently healthy boy, without any medical problems in the past, nonsmoker, was admitted to the Emergency Department for shortness of breath and right-sided chest pain which increased when bending over. He had no fever or other signs of influenza. Breath sounds over the right hemithorax were reduced. Routine laboratory tests showed no abnormalities. Chest x-ray showed a right-sided pneumothorax with a complete collapse of the lung. After drainage by catheter, thoracoscopic pleurodesis was performed. Approximately 8 months later he had recurrence of right-sided pneumothorax which was treated with a partial right-sided pleurectomy. In the subsequent 2 years he had 2 recurrences, both treated by drainage by catheter. Because of the recurrent episodes of pneumothorax a thoracic computed tomography of his chest was performed, which showed multiple cysts below the level of the carina in the parenchyma and subpleural, especially right sided. Because of the recurrent pneumothorax and the CT-abnormalities (CT-thorax, figure 1A, B) BHD was suspected. Genetic testing confirmed a pathogenic mutation of the FLCN gene (c _1177-3delctc). Skin fibrofolliculomas and renal abnormalities were absent in this patient. Subsequently other family members were counselled by the clinical geneticist. Three family members were also affected. (pedigree, figure 2) SP as indicator for BHD in pediatric patients A B Figure 1. (A) CT shows pneumothorax with intraparenchymal located cyst with small septa. (B) shows multiple cysts in the lower lobes (under the carina), in the same patient after treatment of the pneumothorax. 151
152 I 3.2 SP as indicator for BHD in pediatric patients Legend Figure 2. Edited pedigree of patient presentation 1. Generation identifier numbers (I-III) are located to the right of each generation. Each identifier numbers are listed below each family member (circle = female; square = male; solid symbol = pathogenic FLCN mutation carrier; open symbol = no pathogenic FLCN mutation carrier; slash-through symbol = deceased; arrow = proband). Patient presentation 2 A 19-year-old Caucasian male was presented at the Emergency Department for a recurrent rightsided pneumothorax, the first at age 14, treated by video-assisted-thoracoscopy surgery (VATS). A chest CT was made, which revealed a complete collapsed right lung with multiple bullae at the ventero-cranial side of the right lower lobe. An uncomplicated VATS procedure was performed by the thoracic surgeon. Although the thoracic CT showed multiple bullae, mainly in the basal parts of the right lung, no bullae were seen at operation. A total pleurectomy was performed. Two years later he was referred to our center for evaluation for BHD as it had been diagnosed in several family members (pedigree, figure 3). A chest CT was performed again, which showed several cysts in both lungs in the parenchyma and bullae mainly in the right lung (CT-thorax, figure 4A, B). Genetic testing confirmed a pathogenic mutation (c _1304del;1323delcinsga) of the FLCN gene that confirmed the diagnosis of BHD. Skin fibrofolliculomas and renal abnormalities were absent in this patient. Other family members had skin fibrofolliculomas, but no history of renal tumours or (recurrent) episodes of pneumothorax. ii III I II III Legend Figure 3. Edited pedigree of patient presentation 2. Generation identifier numbers (I-III) are located to the right of each generation. Each identifier numbers are listed below each family member (circle = female; square = male; solid symbol = pathogenic FLCN mutation carrier; open symbol = no pathogenic FLCN mutation carrier; slash-through symbol = deceased; arrow = proband). 152
 Figure shows lung cyst located subpleural in the right lower lobe, abutting the main fissure as shown after resolving of the pneumothorax.")
 SP.")
153 3.2 Discussion A Figure 4. (A) CT image of pneumothorax with cluster of lung cysts in the right lower lobe(4a). (B) Figure shows lung cyst located subpleural in the right lower lobe, abutting the main fissure as shown after resolving of the pneumothorax. We report here two pediatric patients with recurrent spontaneous pneumothorax, as part of the Birt-Hogg-Dubé (BHD) syndrome. Lung cysts were seen in both patients, predominantly located below the level of the carina, located in both the parenchyma and subpleural. We assume that these cysts are related to the (recurrent) SP. The incidence of pediatric primary and secondary SP is approximately 4 per males and 1.1. per females per year, suggesting that SP is probably less common than in adulthood. 1 2 The mean age at presentation in pediatric cases is between years and occurs commonly in tall, thin males. 3 A specific racial/ethnic predominance has not been described in literature. 2 The underlying cause in primary SP in adulthood is often unknown but can be caused by an underlying disorder like an inflammatory or connective tissue disease, infection, malignancy, foreign body aspiration or congenital malformation. 4 Subpleural bullae, mainly in the apex of the lung, are found in percent of adult patients during video-assisted thoracoscopic surgery (VATS) and thoracotomy. 5 Among non-smokers with a history of SP, 81 percent have bullae. 6 The general underlying aetiology of SP in childhood seems to be connective tissue changes, which predispose to spontaneous leaking of air from the airways into the pleural space. Several case series suggest a relation between subpleural blebs/bullae and the occurrence of SP. 2 7 The incidence of blebs and bullae detected on CT in children with SP is between 45% and 100%. 8 The clinical significance of these blebs and bullae remains unclear. 4 SP in pediatrics is often diagnosed on clinical suspicion, history and physical examination, confirmed by chest radiography. The additional value of chest CT is unclear. In the British Thoracic Society (BTS) guidelines a CT of the chest is indicated when chest radiography is negative despite of clinical signs for SP or for determining appropriate management strategies. Because blebs, bullae and cysts are only visible on CT, which is performed in a minority of cases, the diagnosis BHD is likely to be missed. Adult literature reports a recurrence rate in primary SP of approximately 30 percent, with a range of 16 to 52 percent. 9 In pediatrics a recurrence rate up to 61 percent has been reported and seems to be B SP as indicator for BHD in pediatric patients 153
154 higher compared to the adult data. 10 A smaller study by Ouanes-Berbes et al. reported a 19% overall recurrence rate over 7 year follow-up in a young adult cohort, with a 72 percent incidence of bullae SP as indicator for BHD in pediatric patients 154 Bullae and cysts have been associated in adults with the Birt-Hogg-Dubé syndrome, with a basal rather than apical distribution of bullae and cysts. The literature on the incidence of BHD syndrome in adults with SP is very limited. Ren and colleagues found a prevalence of 9.8% in 121 apparently spontaneous pneumothorax adult patients. 12 We found in our pilot study among 40 apparently primary spontaneous pneumothorax patients in 3 patients (7.5%) a pathogenic FLCN mutation. 13 SP has been reported twice in pediatric pathogenic FLCN-mutation carriers. The first patient had one episode of SP at age of 7 years. Chest CT was not performed. The second patient at age of 16 years, with a positive family history for SP, had in total 6 episodes of SP on both sides, multiple basal located cysts on chest CT were found. Birt-Hogg-Dubé syndrome [OMIM no ] is a rare autosomal dominant inherited disorder caused by germline mutations in the (FLCN) gene located on chromosome 17p11.2. The BHD gene codes for the protein folliculin which is expressed in skin tissue, nephrons and type 1 pulmonary alveolar epithelial cells. The function is not fully clarified yet, but it seems that folliculin acts as a cancer-inhibitory gene. 16 Clinically this syndrome consists of skin fibrofolliculomas, a 50-fold increased risk for development of (recurrent) SP, multiple lung cysts predominantly in the basal parts of the lung, renal cysts and renal cancer from the age of Therefore patients have to be lifelong screened annually by renal MRI or renal ultrasound. Because the clinical expression can vary, BHD syndrome cannot be excluded when no renal abnormalities or skin lesions are found. 18 The differential diagnosis of patients with multiple lung cysts include emphysema, cystic bronchiectasis, honeycomb change, cavitated infective nodules, pulmonary Langerhans cell histiocytosis (LCH), lymphangioleiomyomatosis (LAM), lymphocytic interstitial pneumonia (LIP), follicular bronchiolitis, amyloidosis, light chain deposition disease (LCDD) and the Birt-Hogg-Dubé (BHD) syndrome. 19 The cystic pattern in BHD differs from other lung diseases; multiple thin-walled pulmonary cysts of various sizes, predominately distributed to the lower medial and subpleural regions of the lung with cysts abutting or including the proximal portion of the lower pulmonary veins or arteries. Treatment of SP in pediatrics does not differ from adults and depends on size and underlying cause. Both BTS and American College of Chest Physicians (ACCP) have published different recommendations for treatment of primary SP in adults as well for pediatric patients. Multiple studies in adult literature advocate aspiration as a first treatment option in PSP. For secondary SP or recurrent SP the ACCP and BTS recommend tube thoracostomy and surgical recurrence prevention Whether treatment of pneumothorax in BHD patients need to be more aggressive than in idiopathic SP is still discussed. 18 In conclusion we report here two cases of Birt-Hogg-Dubé syndrome in children with recurrent pneumothorax. As SP in the pediatric population is relatively rare, BHD should be considered as underlying cause, especially when there is a positive family history for pneumothorax. BHD patients have an increased risk for developing renal cancer, therefore we suggest that easy accessible low dose chest CT and easy accessible genetic testing for BHD in pediatric patients with (recurrent) spontaneous pneumothorax should be performed, even when skin manifestation are absent. We suggest that more research on the prevalence of BHD in the pediatric population with a history of (recurrent) spontaneous pneumothorax is needed.
155 References 1. Healthcare Cost and Utilization Project (HCUP). Kids Inpatient Database (KID). 1997, 2000, 2003, Available at: kidoverview.jsp 2. Dotson K et al. Pediatric spontaneous pneumothorax. Pediatric Emergency Care 2012;28(7): Zgangjer M, Cizmic A, Pajic A, et al. Primary spontaneous pneumothorax in pediatric patients: our 7-year expercience. J Laparoendosc Adv Surg Tech A. 2010;20: Robinson PD, Cooper P, Ranganathan SC. Evidence-based management of pediatric primary spontaneous pneumothorax. Paediatr Respir Rev. 2009;10(3): Sahn SA, Heffner JE. Spontaneous pneumothorax. N Engl J Med Mar 23;342(12): Bense L, Lewander R, Eklund G, et al. Nonsmoking, non-alpha 1-antitypsin deficiencyinduced emphysema in non-smokers with healed spontaneous pneumothorax, identified by computed tomography of the lungs. Chest 1993;103: Smit HJ, Wienk MA, Schreurs AJ et al. Do bullae indicate a predisposition to recurrent pneumothorax? Br J Radiol 2000;73: O Lone E, Elphick HE, Robinson PJ. Spontaneous pneumothorax in children: when is invasive treatment indicated? Pediatr Pulmonol Jan;43(1): Schramel FM, Postmus PE, Vanderschueren RG. Current aspects of spontaneous pneumothorax. Eur Respir J 1997;10: Wilcox DT, Glick PL, Karamanoukian HL et al. Spontaneous pneumothorax: a single-institution:, 12-year experience in patients under 16 years of age. J Pediatr Surg 1995:30; Ouanes-Besbes L, Golli M, Knani J et al. Prediction of recurrent spontaneous pneumothorax: CT scan findings versus management features. Respir Med 2007;101: Ren H-Z, Zhu CC, Yang C, et al. Mutation Analysis of the FLCN gene in Chinese patients with sporadic and familial associated isolated primary spontaneous pneumothorax. Clin Genet 2008;74: Johannesma PC, Reinhard R, Kon Y, et al. The prevalence of Birt-Hogg-Dubé syndrome among patients with apparently common primary spontaneous pneumothorax. (submitted) 14. Bessis D, Giraud S, Richard S. A novel familial germline mutation in the initiator codon of the BHD gene in a patient with Birt-Hogg-Dubé syndrome. Br J Dermatol Nov;155(5): Gunji Y, Akiyoshi T, Sato T et al. Mutations of the Birt Hogg Dubé gene in patients with multiple lung cysts and recurrent pneumothorax. J Med Genet Sep;44(9): Toro JR, Wei MH, Glenn GM et al. BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet 2008;45: Houweling AC, Gijezen LM, Jonker MA, et al. Renal cancer and pneumothorax risk in Birt-Hogg- Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer Dec 6;105(12): Menko FH, van Steensel MA, Giraud S, et al. Birt- Hogg-Dubé syndrome: diagnosis and management. Lancet Oncol Dec;10(12): Clarke BE. Cystic lung disease. J Clin Pathol 2013 Oct;66(10): Johannesma PC, Thunnissen E, Postmus PE. Lung cysts as indicator for Birt-Hogg-Dubé. Lung 2014;192(1): Tobino K, Gunji Y, Kurihara M, et al. Characteristics of pulmonary cysts in Birt-Hogg-Dubé syndrome: Thin-section CT findings of the chest in 12 patients. European Journal of Radiology 2011;77: Kumasaka T, Hayashi T, Mitani K, et al. Characterization of pulmonary cysts in Birt- Hogg-Dubé syndrome: histopathological and morphometric analysis of 229 pulmonary cysts from 50 unrelated patients. Histopathology 2014 Jan 7. (in press) 23. MacDuff A, Arnold A, Harvey J et al. Management of spontaneous pneumothorax: British Thoracic Society pleural disease guideline Thorax 2010;65:ii SP as indicator for BHD in pediatric patients 155
156
157 chapter 3.3 Lung cysts as indicator for Birt-Hogg-Dubé syndrome Paul C. Johannesma 1, Erik Thunnissen 2, Pieter E. Postmus 1 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Pathology, VU University Medical Center, Amsterdam, The Netherlands Lung 2014;192(1):215-6
158 3.3 Lung cysts as indicator for BHD syndrome Abstract In this case we describe a patients with a history of recurrent pneumothorax. Based on CT-thorax and histopathology of the lung tissue, the Birt-Hogg-Dubé syndrome was suspected and confirmed after genetic testing. Recognizing this syndrome by pulmonologists and radiologists is very important as the risk on developing of renal cell cancer is high. A 38-year-old former Olympic swimmer was referred to our hospital due to recurrent pneumothorax. The patient was a non-smoker and had no positive family history for pneumothorax. From the age of 24 he developed 6 episodes of pneumothorax, three times on both sides. Treatment varied by VATS, talkage, pleurodesis, bullectomy and pleurectomy. A lung function test showed a normal function. High resolution computed tomography of the chest revealed multiple round and oval thin-walled pulmonary cysts of varying sizes, localized mostly in the lower lobes between, which abutted to or enclosed the proximal portions of lower pulmonary arteries and veins (Panel A,B,C). Histopathology, the cyst wall were completely lined by pneumocytes. The inner surfaces of the cysts stained positively for TTF-1 expression (Panel D,E), which might suggest that these cysts are distinctly different from nonspecific blebs or bullae. 1 A diagnosis of Birt-Hogg-Dubé syndrome (BHDS) was made after molecular testing. Birt-Hogg-Dubé syndrome BHDS [OMM no ] is a rare autosomal dominant inherited disorder caused by a mutation in the (FLCN) gene located on chromosome 17p11.2. BHD-patients have a 50-fold increased risk for development of (recurrent) spontaneous pneumothorax. Lung cysts are common in those with spontaneous pneumothorax. 2 Recognizing this disease is important as the risk on developing renal cell cancer is high and screening is indicated. References 1. Furuya M, Tanaka R, Koga S et al. Pulmonary cysts of Birt-Hogg-Dubé syndrome: A clinicopathologic and Immunohistochemical study of 9 families. Am J Surg Pathol. 2012;36: Menko FH, van Steensel MAM, Giraud S. et al. Birt- Hogg-Dubé syndrome: diagnosis and management. The Lancet Oncology 2009;10:



.")
159 3.3 Figure 1. Frontal view of high-resolution CT showing many round and oval thin-walled cysts mainly in the lower lobes. Figure 2. Cysts abutting pulmonary vessel (arrow). Lung cysts as indicator for BHD syndrome Figure 3. Cysts enclosing pulmonary vessel (arrow). Figure 4. Cysts walls lined by pneumocytes. Figure 5. Pneumocytes staining positive for TTF
160
161 chapter 3.4 Spontaneous pneumothorax as the first manifestation of a hereditary condition with an increased renal cancer risk Paul C. Johannesma 1, Jan-Willem J. Lammers 2, R. Jeroen A. van Moorselaar 3, Theo M. Starink 4, Pieter E. Postmus 1, Fred H. Menko 5, on behalf of Werkgroep Birt-Hogg-Dubé syndroom van het Centrum Familiaire Tumoren VUmc* *Hr. E.F.L. David, radioloog, hr. dr. J.J.P. Gille, klinisch moleculair geneticus, hr. P.C. Johannesma, student geneeskunde, hr. dr. E.M. Leter, klinisch geneticus, hr. dr. F.H. Menko, klinisch geneticus, hr. dr. R.J.A. van Moorselaar, uroloog, hr. H.M. Ploeger, patiënten coördinator, hr. prof. dr. P.E. Postmus, longarts, hr. prof. dr. Th.M. Starink, dermatoloog 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Pulmonary Diseases, Utrecht University Medical Center, Utrecht, The Netherlands 3 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 4 Department of Dermatology, VU University Medical Center, Amsterdam, The Netherlands 5 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands Ned Tijdschr Geneeskd. 2009;153:A581
162 3.4 Abstract Spontaneous pneumothorax may be due to Birt-Hogg-Dubé syndrome (BHD), an autosomal dominant predisposition for fibrofolliculomas, multiple lung cysts, pneumothorax and renal cancer. The syndrome is due to germline mutations in the FLCN (folliculin) gene. Clinical presentation is highly variable. Consequently, the syndrome is probably underdiagnosed. An illustrative kindred is presented in which the index patient had recurrent episodes of pneumothorax without apparent skin lesions or renal abnormalities. He had bilateral basally located lung cysts. Family members had fibrofolliculomas, lung cysts, pneumothorax and clear cell renal cancer. Recognition of BHD is important since mutation carriers can be offered surveillance for early detection and treatment of renal cancer. SP as indicator for rcc 162

.")
163 Dames en Heren, Een pneumothorax (klaplong) ontstaat als er lucht komt tussen de pariëtale en viscerale pleura. De long kan zich hierdoor niet meer volledig ontplooien. Pijn op de borst en kortademigheid zijn de meest voorkomende symptomen. Naar oorzaak wordt pneumothorax ingedeeld in 1) spontane pneumothorax, a) primair, zonder bekende oorzaak of b) secundair, als gevolg van een al bestaande longaandoening, 2) traumatische en 3) iatrogene pneumothorax. 1 Spontane pneumothorax kan een uiting zijn van het Birt-Hogg-Dubé syndroom (BHD). BHD wordt gekenmerkt door fibrofolliculomen van de huid, multipele longcysten, pneumothorax en nierkanker Herkenning van het syndroom is belangrijk voor de patiënt en voor de familie. Door jaarlijkse controle kan nierkanker in een vroeg stadium worden opgespoord en behandeld. In deze klinische les willen wij aan de hand van vier ziektegeschiedenissen uw aandacht vragen voor het Birt-Hogg-Dubé syndroom. Een positieve familie-anamnese voor pneumothorax leidde hier tot herkenning van het syndroom. Ziektegevallen Patiënt A, een niet-rokende vitale man van 26 jaar met een blanco voorgeschiedenis kwam eind juni 2007 op de spoedeisende hulp met kortademigheid en subfebriele temperatuursverhoging. Bij lichamelijk onderzoek was er rechts op de borst hypersonore percussie en verminderd ademgeruis. De thoraxfoto toonde een pneumothorax rechts. (Fig. 1A). Bij Video Assisted Thoracoscopic Surgery (VATS) werden in de rechter bovenkwab multipele bulleuze afwijkingen waargenomen. Behandeling vond plaats door talkage van de pleurabladen en zuigdrainage. In de weken daarop trad driemaal opnieuw een pneumothorax aan dezelfde zijde op. Het eerste recidief werd conservatief behandeld. Na het tweede recidief werd een restpleurectomie verricht gevolgd door zuigdrainage. Het derde recidief werd behandeld met opruwen van de pleura van de onderste thoraxhelft, talkage en zuigdrainage. Een week na ontslag traden opnieuw dyspnoeklachten op, nu bleek er een pneumothorax aan de linker zijde. Een CT-scan van de longen (Fig. 1B) toonde 3.4 SP as indicator for rcc A B Figuur 1. (A) Patiënt A. De röntgenfoto van de thorax toont een pneumothorax rechts. (B) Patiënt A. De CT-scan van de longen toont een pneumothorax rechts en bilaterale cysteuze longafwijkingen. 163


164 beiderzijds multipele cysteuze longafwijkingen, basaal meer uitgesproken dan apicaal. Behandeling vond plaats door middel van thoracotomie, bullectomie, pleurectomie, opruwing van het diafragma en zuigdrainage. Bij follow-up maakt patiënt het goed. Patiënt B, een 60-jarige man, maakte op de leeftijd van 47 jaar een dubbelzijdige pneumothorax door. Op een CT-scan van de longen waren multipele bullae in beide longen zichtbaar. Aan de gelaatshuid heeft patiënt multipele huidkleurig tot wittig doorschijnende papels, passend bij fibrofolliculomen. Histologisch onderzoek van één van deze laesies bevestigde deze diagnose (Fig. 2A, B). 3.4 SP as indicator for rcc A B Figuur 2. (A) Klinische aspect van multiple fibrofolliculomen in het gelaat bij patiënt B. (B) Histologische kenmerken van een fibrofolliculoom: proliferatie van het perifolliculaire bindweefsel en netvormig vertakkende epitheelstrengen. Patiente C, een niet-rokende vrouw zonder bijzondere medische voorgeschiedenis, kreeg op 34-jarige leeftijd een pneumothorax rechts. Behandeling vond plaats via drainage. Na drie dagen trad een recidief op. Als therapie werden drainage en pleurodese met talk toegepast. Een maand na ontslag uit het ziekenhuis trad een tweede recidief op. Een CT-scan van de thorax toonde beiderzijds in de longen dunwandige cysteuze afwijkingen. Bij mini-thoracotomie rechts werden twee grote en meerdere kleine bullae gezien, verspreid over de long, maar niet in de longtop. Er wordt een totale pleurectomie rechts verricht. Het postoperatieve beloop was voorspoedig. Dames en heren, De patiënten A, B en C zijn familieleden van elkaar. De stamboom is weergegeven in Figuur 4. Bij een paternale oom van de indexpatiënt, patiënt D, werd op de leeftijd van 48 jaar nierkanker geconstateerd. Er werd een thoraco-abdominale nefrectomie verricht, waarbij een groot tumorproces werd verwijderd. Histologisch betrof het een heldercellig carcinoom (Fig. 3, Fig. 4). Patiënt A werd wegens verdenking op Birt-Hogg-Dubé syndroom, op basis van het familiair voorkomen van pneumothorax door de longarts verwezen naar de klinisch geneticus. Patiënt bleek drager van een pathogene mutatie in exon 6 van het FLCN-gen (c.1065_1066delgcinsta). Zijn vader, patiënt B, bleek zoals verwacht ook drager van deze mutatie. Patiënt A had geen fibrofolliculomen; 164

165 Figuur 3. Histologisch beeld van het heldercellige niercarcinoom, opgetreden bij patiënt D. 3.4 SP as indicator for rcc Figuur 4. Stamboom van de beschreven familie. De indexpatiënt A is met pijl aangegeven. De zwarte symbolen geven de kenmerken van BHD aan: Pneumothorax, Fibrofolliculomen, en niercelkanker. de kans is groot, dat deze typerende huidverschijnselen bij hem later alsnog zullen optreden. Bij MRI en echoscopie van de nieren werden bij patiënt en bij zijn vader geen afwijkingen gevonden. Tot op heden hebben overige verwanten geen DNA-diagnostiek laten verrichten. BHD bij de patiënten C en D is een waarschijnlijkheidsdiagnose. Birt-Hogg-Dubé syndroom In 1977 beschreven drie Canadese artsen een grote familie met fibrofolliculomen, trichodiscomen en acrochordons. Vanaf de leeftijd van circa 25 jaar traden vooral in het gelaat multipele, kleine, witte papels op. 2 Nu staat het Birt-Hogg-Dubé syndroom bekend als een autosomaal dominant erfelijke aandoening, gekenmerkt door fibrofolliculomen van de huid, multipele longcysten, pneumothorax en nierkanker. BHD wordt veroorzaakt door kiembaanmutaties in het FLCN (folliculine)- gen, dat gelokaliseerd is op de korte arm van chromosoom 17 en codeert voor het eiwit folliculine. Het gen heeft kenmerken van een tumorsuppressor-gen en komt tot expressie in onder andere huid, longen en nieren
166 Bij patiënten met klinisch BHD kan in 70-80% van de gevallen een pathogene FLCN-mutatie worden aangetoond. Dragers van een pathogene FLCN-mutatie hebben een sterk variabele expressie. Zo zijn in families waarin alleen pneumothorax voorkwam - zonder fibrofolliculomen of niertumoren ook FLCN-mutaties gevonden SP as indicator for rcc Huid. De huidverschijnselen bestaan uit multipele 1-5 mm grote witte of huidkleurige papels, voornamelijk in het gelaat, maar ook in de hals en op de romp. Fibrofolliculomen zijn goedaardige haarfollikeltumoren die uitgaan van het bovenste gedeelte van de haarfollikel. Zij bestaan uit een proliferatie van het perifolliculaire bindweefsel en een epitheliale component met netvormig vertakkende epitheelstrengen. Trichodiscomen zijn een histologische variant van fibrofolliculomen 10 Indien om cosmetische redenen behandeling van de fibrofolliculomen wordt gewenst, kan met lasertechnieken vaak een tijdelijke remissie worden bereikt. Fibrofolliculomen zijn kenmerkend voor BHD: verwijzing van een patiënt met deze afwijkingen is daarom steeds aangewezen. Longen. Longcysten werden bij 80-90% van alle patiënten gevonden, vaker basaal dan apicaal gelegen. De longcysten zijn de oorzaak van het optreden van pneumothorax. Hoewel de meeste patiënten met BHD multipele longcysten hebben is de longfunctie als regel niet gestoord. Ongeveer 25% van de patiënten met BHD krijgt een pneumothorax, meestal voor de leeftijd van 50 jaar. Bij BHD is er een verhoogde kans op een recidief pneumothorax Pneumothorax bij BHD wordt behandeld zoals bij andere patiënten met spontane pneumothorax, ofwel conservatief ofwel invasief. Er is geen reden voor standaard onderzoek naar longcysten bij een individu met aanleg voor BHD. Dit onderzoek is wel nodig in omstandigheden met een verhoogde kans op een pneumothorax. Zo wordt een CT-scan van de thorax geadviseerd voorafgaand aan een operatie onder algemene narcose. Evaluatie door de longarts wordt ook geadviseerd in bijzondere situaties, zoals beroepskeuze voor piloot of diepzeeduiken als hobby. Roken wordt aan individuen met BHD sterk ontraden. Nieren. In 1993 werd niercelkanker voor het eerst geassocieerd met BHD. 12 FLCN-mutatiedragers hebben een sterk verhoogde kans op nierkanker. De prevalentie van nierkanker bij patienten met BHD loopt in verschillende studies echter sterk uiteen, van 6.5% tot 34%. 5 Evenals bij andere erfelijke vormen van nierkanker ontstaan de niertumoren bij BHD op relatief jonge leeftijd en treden zij vaak multifocaal en bilateraal op. Typerend voor BHD zijn chromofobe carcinomen en oncocytomen. Er worden vaak mengvormen van deze histologische typen gezien. Ook andere histologische vormen komen echter voor, waaronder het heldercellig niercarcinoom Voor vroege detectie en behandeling van nierkanker wordt bij FLCN-mutatiedragers een jaarlijks onderzoek verricht. Wij adviseren vanaf de leeftijd van 20 jaar eerst een MRI van de nieren en nierechoscopie en vervolgens jaarlijks alleen echoscopie en MRI op indicatie (bij moeilijke beoordeelbaarheid of bij mogelijke afwijkingen). Bij het vinden van nierkanker vindt na preoperatieve evaluatie zo mogelijk een niersparende operatie plaats. 166
167 Dames en Heren, Primaire SP komt ongeveer even vaak voor als secundaire SP. In de huisartsenpraktijk wordt bij 24 mannen per consulten per jaar en 10 per vrouwen spontane pneumothorax vastgesteld. 15 Primaire spontane pneumothorax treedt voornamelijk op bij lange, dunne jongens en mannen tussen de 10 en de 30 jaar. Roken is een belangrijke oorzakelijke factor. Bij de meeste patiënten worden bij thoracoscopie subpleurale bullae gevonden, vooral apicaal gelegen. De kans op een recidief pneumothorax is ongeveer 30%; de meeste recidieven treden binnen twee jaar na de eerste episode op. 16 Van secundaire spontane pneumothorax wordt gesproken, als de pneumothorax een complicatie is van een longziekte, in het bijzonder chronische obstructieve longziekte, longinfectie, longkanker, cystische fibrose, alfa-1-antitrypsine deficiëntie, sarcoïdose, Marfan syndroom, Ehlers Danlos syndroom, lymfangioleiomyomatose, tubereuze sclerose complex, en het Birt-Hogg-Dubé syndroom. 17 Tenslotte kan een pneumothorax optreden door een scherp of stomp thoraxtrauma of iatrogeen, in het bijzonder als complicatie bij het inbrengen van een centrale centrale lijn in de vena subclavia of bij het nemen van een pleurabiopt. 18 Bij ongeveer 10% van alle patiënten met een pneumothorax komt de aandoening familiair voor zonder enig ander verschijnsel. Verschillende vormen van overerving zijn hiervoor gesuggereerd (autosomaal dominant, X-chromosomaal recessief). Daarnaast kan familiair optreden van pneumothorax een uiting zijn van een erfelijk syndroom, waaronder het Birt-Hogg-Dubé syndroom. 19 Op basis van recente studies kan worden geschat, dat 15-25% van de familiaire gevallen berust op een FLCN-mutatie. In Nederland zijn op dit moment meer dan 30 families bekend, waarin BHD op basis van een pathogene FLCN-mutatie is aangetoond. De gegevens van een aantal van deze families zijn onlangs gepubliceerd. [4, 22] Recent is het Europees BHD Consortium opgericht www. europeanbhdconsortium.eu om het BHD syndroom beter in kaart te brengen en optimale methoden van diagnostiek, surveillance en behandeling te ontwikkelen. Er is een internationale patiëntenvereniging, met een website voor informatie: Vermoedelijk komt de aandoening vaker voor dan tot op heden wordt onderkend. Indien een patiënt een spontane pneumothorax krijgt zonder al bekende longziekte, dan kan het gaan om BHD. [23] Bij een dergelijke patiënt met pneumothorax zijn klinische aanwijzingen voor BHD multipele basaal gelegen longcysten en het voorkomen van pneumothorax in de familie. 19,20 In de besproken familie werden de voor het syndroom kenmerkende fibrofolliculomen van de huid en nierkanker gevonden bij het in kaart brengen van de familiegegevens. Door het vinden van een pathogene FLCN-mutatie werd de diagnose Birt-Hogg-Dubé syndroom bevestigd. Dames en heren, de hier gepresenteerde casus tonen, dat de eerste aanwijzing voor een bijzondere erfelijke aandoening kan worden verkregen door het nauwkeurig afnemen van een familieanamnese, door huisarts of behandelend specialist. 3.4 SP as indicator for rcc 167
168 3.4 SP as indicator for rcc References 1. Sahn SA, Heffner JE. Spontaneous pneumothorax. N Engl J Med 2000; 342: Birt AR, Hogg GR, Dubé WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol 1977;113: Khoo, S.K., Giraud, S., Kahnoski, K., Chen, J., Motorna, O., Nickolov, R. et al. Clinical and genetic studies of Birt-Hogg-Dubé syndrome. J. Med. Genet. 2002; 39: Leter EM, Koopmans AK, Gille JJP, van Os TAM, Vittoz GG, David EFL et al. Birt-Hogg-Dubé syndrome: clinical and genetic studies of 20 families. J Invest Dermatol 2008; 128: Toro JR, Wei M-H, Glenn GM, Weinreich M, Toure O, Vocke C, et al. BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet 2008; 45: Nickerson, ML, Warren MB,.Toro JR, Matrosova V, Glenn G, Turner ML et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt- Hogg-Dubé syndrome. Cancer Cell 2002; 2: Warren MB, Torres- Cabala CA, Turner ML, Merino MJ, Matrosova VY, Nickerson ML. Expression of Birt- Hogg-Dubé gene mrna in normal and neoplastic human tissues. Mod Pathol 2004;8: Graham RB, Nolasco, M, Peterlin, B, Garcia CK. Nonsense mutations in folliculin presenting as isolated familial spontaneous pneumothorax in adults. Am. J. Respir. Crit. Care Med. 2005; 172: Painter, J.N., Tapanainen, H., Somer, M. et al. A 4-bp deletion in the causes dominantly inherited spontaneous pneumothorax. Am. J. Hum. Genet. 2005; 76: Vincent A, Farley M, Chan E, James WD. Birt-Hogg- Dubé syndrome: a review of the literature and the differential diagnosis of firm facial papules. J. Am. Acad. Dermatol. 2003; 49: Toro JR, Pautler SE, Stewart, L, Glenn GM, Weinreich M, Toure O, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med 2007;175: Roth JS, Rabinowitz AD, Benson M., Grossman ME. Bilateral renal carcinoma in the Birt-Hogg-Dubé syndrome. J Am Acad Dermatol 1993; 29: Pavlovich CP, Grubb III RL, Hurley K, Glenn GM, Toro J, Schmidt LS Evaluation and management of renal tumors in the Birt-Hogg-Dubé syndrome. J Urol 2005; 173: Woodward ER, Ricketts C, Killick P, Gad S, Morris MR, Kavalier F. Familial non-vhl clear cell (conventional) renal cell carcinoma: clinical features, segregation analysis, and mutation analysis of FLCN. Clin. Cancer Res. 2008; 14: Gupta, D., Hansell, A., Nichols, T. et al. Epidemiology of pneumothorax in England. Thorax 2000; 55: Smit HJ, Devillé WL, Schramel FM, Schreurs JM, Sutedja TG, Postmus PE. Atmospheric pressure changes and outdoor temperature changes in relation to spontaneous pneumothorax. Chest 1999;116: Louis H, Los H, Lagendijk JH, de Graaff CS, Postmus PE. Spontane pneumothorax bij jonge vrouwen: mogelijk lymfangioleiomyomatose. Ned Tijdschr Geneeskd. 1997;141: Tan ECTH, Vliet, van der JA. Late (spannings) pneumothorax na het plaatsen van een centraalveneuze lijn. Ned. Tijdschr. Geneeskd. 1999; 143: Chiu HT, Garcia CK. Familial spontaneous pneumothorax. Curr Opin Pulm Med 2006;12: Gunji Y, Akiyoshi T, Sato T, Kurihara M, Tominaga S, Takahashi K et al Mutations of the Birt-Hogg-Dubé gene in patients with multiple lung cysts and recurrent pneumothorax. J Med Genet 2007; 44: Ren H-Z, Zhu C-C, Yang C, Chen S-L et al. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax. Clin Genet 2008; 74:
169
170
171 chapter 3.5 Facial fibrofolliculomas as indicator for renal cell cancer Paul C. Johannesma 1, Theo M. Starink 2, R. Jeroen A. van Moorselaar 3, Pieter E. Postmus 1 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Dermatology, VU University Medical Center, Amsterdam, The Netherlands 3 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands Jpn J Clin Oncol. 2014;44(6):609-10
.")

. Therefore she was referred for CT abdomen with i.v.")
. Partial nephrectomy followed and a clear cell tumour, Fuhrmann grade 2, was found.")
172 3.5 Fibrofolliculomas as indicator for BHD syndrome A 53-year old woman was referred to our hospital because of an increasing number of facial skin papules on her cheeks and ears. A biopsy was taken from several of these papules. The location of these lesions combined with the histology confirmed the diagnoses fibrofolliculomas (figure 1A+B). Except for facial papules since the age of 26 years, her medical history was unremarkable. The familial history was negative for renal cancer and spontaneous pneumothorax. She never smoked. Her father died of pancreatic cancer at the age of 73 years and her mother of cardiac failure at age 85. Based on the histology and location of the skin lesions, the patient was clinically diagnosed as having Birt-Hogg-Dubé syndrome (BHD). Therefore she was referred for CT abdomen with i.v. contrast, which showed a solid interpolar tumour in the lower pole of the right kidney, with a diameter of 19 mm, classified as T1N0Mx (figure 2). The slices through the basal parts of the lungs revealed multiple lung cysts (figure 3). Partial nephrectomy followed and a clear cell tumour, Fuhrmann grade 2, was found. This combination of skin fibrofolliculomas, renal cell cancer and cysts in the basal parts of the lungs is typical for the Birt-Hogg-Dubé syndrome (BHD), an autosomal dominantly inherited cancer disorder, caused by pathogenic FLCN mutations. Figure 1. Skin fibrofolliculomas. A B A B Figure 2. Renal tumour in the lower pole of the right kidney. 172
, which confirmed the clinical diagnosis at DNA level. Afterwards we identified four additional FLCN mutation carriers in her family.")
173 Figure 3. Thoracic CT: Multiple lung cysts in the basel parts of both lungs. Sequencing of the FLCN gene showed a pathogenic splice site mutation in exon 12 (c.[1301-7_1304; delcinsga]), which confirmed the clinical diagnosis at DNA level. Afterwards we identified four additional FLCN mutation carriers in her family. The family data are summarized in figure 4. Magnetic Resonance Imaging (MRI) showed no local recurrence of the removed renal tumour, respectively early detection of a new renal tumour during 18 months follow up after surgery. Lifetime frequent renal MRI will be performed in this patient. As the prevalence of renal cancer in BHD syndrome patients after initial renal imaging has been described in up to 27% of cases, BHD should be considered when facial fibrofolliculomas are diagnosed and consequently relatives should be stimulated to be screened for genetic testing. 3.5 Fibrofolliculomas as indicator for BHD syndrome Figure 4. Pedigree of the family. 173
174
175 chapter 3.6 Bilateral renal tumour as indicator for Birt-Hogg-Dubé syndrome Paul C. Johannesma 1, R. Jeroen A. van Moorselaar 2, Simon Horenblas 3, Lisette E. van der Kolk 4, Erik Thunnissen 5, JanHein T.M. van Waesberghe 6, Fred H. Menko 4 7, Pieter E. Postmus 1 1 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 3 Urologic Oncology and Department of Urology, The Netherlands Cancer Institute, Amsterdam, The Netherlands 4 Family Cancer Clinic, The Netherlands Cancer Institute, Amsterdam, The Netherlands 5 Department of Pathology, VU University Medical Center, Amsterdam, The Netherlands 6 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 7 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands Case Rep Med. 2014;2014:618675
176 Abstract Birt-Hogg-Dubé (BHD) syndrome is a cancer disorder caused by a pathogenic FLCN mutation characterized by fibrofolliculomas, lung cysts, pneumothorax, benign renal cyst and renal cell carcinoma (RCC). In this case we describe a patient with bilateral renal tumour and a positive familial history for pneumothorax and renal cancer. Based on this clinical presentation, the patient was suspected for BHD syndrome, which was confirmed after molecular testing. We discuss the importance of recognizing this autosomal dominant cancer disorder when a patient is presented at the urologist with a positive family history of chromophobe renal cell cancer, or a positive familial history for renal cell cancer and pneumothorax. 3.6 RCC as indicator for BHD syndrome 176
.")

177 Background Birt-Hogg-Dubé syndrome (BHDS), was originally described in 1977 and is nowadays known as a rare autosomal dominant cancer disorder characterized by fibrofolliculomas, lung cysts, pneumothorax, benign renal cyst and renal cell carcinoma (RCC). The mutated gene for BHD encodes the protein folliculin (FLCN) which acts as a tumour suppressor and interacts with mtor and AMPK signalling pathways. 1 Here we report a case of a patient with bilateral renal cancer and a positive familial history for pneumothorax and renal cancer. Based on the bilateral renal tumour and the positive family history for renal cancer and pneumothorax, Birt-Hogg-Dubé syndrome was suspected. Case report In March 2011, a 44-year-old Caucasian male was evaluated for urolithiasis. He had no physical complaints, no macroscopic haematuria or weight loss. His medical and social history were unremarkable, he never smoked. His father had been treated for colorectal cancer, his mother had three episodes of spontaneous pneumothorax and had been treated for a renal tumour. Physical examination of the abdomen showed no abnormalities. Routine laboratory tests were normal. Computed tomography (CT) of the abdomen showed an interpolar tumour in the left kidney, diameter 14 mm (figure 1A, arrow), and a second tumour in the upper pole of the right kidney, diameter 8 mm (figure 1B, arrow). After a needle biopsy of the largest tumour, revealing a chromophobe renal cell carcinoma (figure 2A+2B), the tumour in the left kidney was treated with radio frequency ablation (RFA). The CT findings in combination with the positive family history for renal cancer and his mother s episodes of pneumothorax suggested Birt-Hogg-Dubé (BHD) syndrome. Sequencing of the FLCN gene showed a pathogenic heterozygous frameshift mutation (c.155delc;p.leu518phefs*19) - which hasn t been described before in literature - and confirmed the diagnosis Birt-Hogg-Dubé syndrome. The index patient had neither siblings nor children. His 3.6 RCC as indicator for BHD syndrome A B Figure 1. Contrast enhanced CT shows in the arterial phase a hypervascular small lesion in both kidneys, representing two small chromophobe renal cell carcinomas. The tumour in left kidney (A) was treated by radiofrequency ablation (RFA), for the tumour in the right kidney (B) was follow up proposed. 177


178 A B 3.6 RCC as indicator for BHD syndrome Figure 2. Overview of needle biopsy of tumor in left kidney (A: Amplification X2.5) and detail (B: Amplification X40) of a chromophobe renal carcinoma. Overview of needle biopsy (A: amplification X2.5) and detail (B: amplification X40) of monotonous cellular pattern with mild nuclear pleomorphy and abundant partly eosinophilic cytoplasm with perinuclear halo, compatible with chromophobe renal cell carcinoma. parents died years ago, blood or tissue was not available for molecular testing. Frequent follow up by Magnetic Resonance Imaging (MRI) will be performed for evaluation of the small tumour in the right kidney and possible recurrence of the tumour in the left kidney. Discussion and conclusion Birt-Hogg-Dubé syndrome [OMIM #135150] is a rare autosomal dominant inherited disorder caused by a mutation in the FLCN gene located on chromosome 17p11.2, which acts as a tumour suppressor and probably interacts with mtor and AMPK signalling pathways. 1 BHD is clinically characterized by skin fibrofolliculomas, lung cysts, (recurrent) spontaneous pneumothorax and renal cancer.[2] In literature co-occurrence of BHD and a range of tumours, other than renal cancer, has been described, but so far a causal relationship between BHD and these benign and malignant tumours has not been proven. 2 Skin fibrofolliculomas are multiple, dome shaped, whitish papules located on the scalp, forehead, face and neck and are found in approximately 90% of families with confirmed BHD syndrome. Dermatologic consultation confirmed multiple fibrofolliculomas on the forehead and face of the index patient. Although cosmetic therapeutic options are limited, case reports suggest that laser ablation, using a YAG or fractional CO2 laser, gives temporary improvement. 3 BHD patients have a 50 fold higher risk to develop primary spontaneous pneumothorax (PSP) compared to the normal population. PSP in BHD patients occur usually after the age of 20, although it has been described already at the age of 7 years. 4 Up to 90% of BHD patients have multiple lung cysts, usually located in the basal regions. 5 In our clinic we found an estimated penetrance for pneumothorax of 29% (CI: 9-49%) at 70 years of age. BHD patients usually have a normal lung function and no pulmonary symptoms. A CT of the chest performed in our index patient showed no pulmonary cysts. 178
179 Renal cell cancer (RCC) is the most lethal of the urologic malignancies, with an estimated new cases diagnosed and patient deaths in 2008, worldwide. 6 RCC can be divided in sporadic and hereditary. The majority is of sporadic origin, presenting normally after the age of 60 as one lesion, while the hereditary type mainly presents as multifocal and bilateral at a far younger age. The most common hereditary renal cancer syndromes are associated with hereditary leiomyomatosis and renal cell carcinoma (HLRCC), Von Hippel-Lindau syndrome (VHL) and hereditary papillary renal carcinoma (HPRC). The prevalence of RCC in (familial) renal cancer is unknown and might be underestimated, since the majority (>80%) of the BHD index patients are referred by a dermatologist. In a large published series by Pavlovich et al., 34 of 124 individuals (27.4%) with genetic confirmed BHD had a median of 5 renal tumours at a mean age of 50.4 years (range years). 7 In a large series published by Toro et al, 34% of individuals with BHD had renal tumours. 5 The youngest patient with BHD who developed renal cancer was 20 years old. 8 Another study reported a history of renal cancer and metastasis in the same year in a patient with BHD at age In our Dutch study population published by Houweling et al., we found among 115 BHD patients, 14 patients with renal cancer, and calculated an estimated penetrance for renal cancer of 16% (CI: 6-26%) at 70 years of age. 10 Most lesions are a mixture of solid and cystic components. The largest published histological series of RCC among BHD patients demonstrates that these tumours contain both oncocytoma and chromophobe elements. 11 Houweling and colleagues confirmed these findings, as they found in the majority of RCC tumours, cells with granular/floccular eosinophillic cytoplasm, as can be seen in both clear cell carcinoma and chromophobe carcinoma. 10 As the risk of developing RCC is high, imaging and follow up at regular intervals is advised by MRI from the age of 20. The role of ultrasound (US) for detecting renal tumours is still extensively discussed in literature. Surgical treatment, is recommended before the largest tumour reaches 3 cm in maximal diameter, which is based on the VHL guideline. 9 Initially a nephron-sparing surgery should be ideally pursued, which can help prevent chronic renal insufficiency in this patient population. Minimally invasive nephron-sparing techniques such as cryoablation and radio frequency ablation (RFA) are generally accepted as treatment of choice in patients with a unifocal renal lesion. Since BHD patients are at lifelong risk for the development of new tumours, and cryoablation or RFA can complicate both the long term evaluation and surgical management, nephron-sparing surgery is so far the safest and most effective treatment for hereditary renal tumours. 12 In conclusion, in patients with a positive family history of chromophobe renal cell cancer or a positive family history for renal cell cancer and pneumothorax, the diagnosis BHD should be considered. Therefore we suggest easily accessible FLCN sequencing should be considered in patients and their family because of the high incidence of renal cancer in BHD patients. 3.6 RCC as indicator for BHD syndrome 179
180 3.6 RCC as indicator for BHD syndrome References 1. Baba M, Hong S-B, Sharma N, et al. Folliculin encoded by the BHD gene interacts with a binding protein, FNIP1, and AMPK, and is involved in AMPK and mtor signaling. Proc Nat Acad Sci USA 2006; 103: Menko FH, van Steensel MAM,Giraud S, et al. Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncol 2009; 10: Gambicher T, Wolter M, Altmeyer P, et al. Treatment of Birt-Hogg-Dubé syndrome with erbium : YAG laser. J Am Acad Dermatol 2000; 43: Zbar B, Alvord WG, Glenn G, et al. Risk of renal and colonic neoplasms and spontaneous pneumothorax in the Birt-Hogg-Dubé syndrome. Cancer Epidemiol Biomarkers Prev. 2002;11(4): Toro JR, Pautler SE, Stewart L, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg- Dubé syndrome. Am J Respir Crit Care Med 2007; 175: Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN Int J Cancer 2010;127: Pavlovich CP, Grubb RL 3rd, Hurley K, et al. Evaluation and management of renal tumors in the Birt-Hogg-Dubé syndrome. J Urol 2005; l173: Khoo SK, Giraud S, Kahnoski K, et al. Clinical and genetic studies of Birt-Hogg-Dubé syndrome. J Med Genet 2002; 39: Kluijt I, de Jong D, Teerstra HJ, et al. Early onset of renal cancer in a family with Birt-Hogg-Dubé syndrome. Clin Genet 2009; 75: Houweling AC, Gijezen LM, Jonker MA, et al. Renal cancer and pneumothorax risk in Birt-Hogg- Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer 2011;105(12): Pavlovich CP, Walther MM, Eyler RA, et al. Renal tumors in the Birt-Hogg-Dubé syndrome. Am J of Surg Pathol 2002; 26: Stamatakis L, Metwalli AR, Middelton LA, et al. Diagnosis and management of BHD-associated kidney cancer. Fam. Cancer 2013;12(3):
181
182
183 chapter 3.7 A de novo FLCN mutation in a patient with spontaneous pneumothorax and renal cancer; a clinical and molecular evaluation Fred H. Menko 1, Paul C. Johannesma 2, R. Jeroen A. van Moorselaar 3, Rinze Reinhard 4, Jan Hein van Waesberghe 4, Erik Thunnissen 5, Arjan C. Houweling 1, Edward M. Leter 1, Quinten Waisfisz 1, Martijn B. van Doorn 6, Theo M. Starink 6, Pieter E. Postmus 2, Barry J. Coull 7, Maurice A.M. van Steensel 7 8, Johan J.P. Gille 1 1 Department of Clinical Genetics, VU University Medical Center, Amsterdam, The Netherlands 2 Department of Pulmonary Diseases, VU University Medical Center, Amsterdam, The Netherlands 3 Department of Urology, VU University Medical Center, Amsterdam, The Netherlands 4 Department of Radiology, VU University Medical Center, Amsterdam, The Netherlands 5 Department of Pathology, VU University Medical Center, Amsterdam, The Netherlands 6 Department of Dermatology, VU University Medical Center, Amsterdam, The Netherlands 7 Department of Dermatology, GROW School for Oncology and Developmental Biology, Maastricht University Medical Centre, Maastricht; The Netherlands 8 Department of Clinical Genetics, GROW School for Oncology and Developmental Biology, Maastricht University Medical Centre, Maastricht; The Netherlands Fam. Cancer 2013;12(3):373-9
184 Abstract Birt-Hogg-Dubé syndrome (BHD) is an autosomal dominant condition due to germline FLCN (folliculin) mutations, characterized by skin fibrofolliculomas, lung cysts, pneumothorax and renal cancer. We identified a de novo FLCN mutation, c.499c>t (p.gln167x), in a patient who presented with spontaneous pneumothorax. Subsequently, typical skin features and asymptomatic renal cancer were diagnosed. Probably, de novo FLCN mutations are rare. However, they may be under-diagnosed if BHD is not considered in sporadic patients who present with one or more of the syndromic features. Genetic and immunohistochemical analysis of the renal tumour indicated features compatible with a tumour suppressor role of FLCN. The finding that mutant FLCN was expressed in the tumour might indicate residual functionality of mutant FLCN, a notion which will be explored in future studies. 3.7 de novo FLCN mutation in patient with SP and RCC 184
185 Introduction In 1977 Birt, Hogg and Dubé described a three-generation pedigree affected with multiple fibrofolliculomas. 1 Subsequently, it was shown that patients with Birt-Hogg-Dubé syndrome (BHD) can also develop renal cancer and pneumothorax. 2 3 The causative gene was mapped to chromosome 17p11.2 and germline mutations in the FLCN (folliculin) gene were identified in BHD families. 4 FLCN mutations have now been detected not only in classical BHD families but also in pneumothorax and renal cancer patients and families The spectrum of FLCN mutations has been outlined in detailed reports and summarized in two databases The function of folliculin is complex and involves several molecular pathways including mtor and vesicular transport The European BHD Consortium recently summarized diagnosis and management of this syndrome. 16 In autosomal dominant tumour syndromes a varying proportion of index patients have a de novo mutation, which is an alteration in a gene that is present for the first time in a family member as a result of a mutation in a germ cell of one of the parents, or a mutation that arises in the fertilized egg itself during early embryogenesis. For example, in Lynch syndrome (hereditary nonpolyposis colorectal cancer) about 1-5% of patients have de novo mutations in DNA mismatch repair genes 17, whereas in familial adenomatous polyposis de novo APC mutations occur in about 10-25% of cases. 18 The phenomenon of de novo mutations is important from a clinical point of view, since it implies that a negative family history for syndromic features does not exclude an autosomal dominant condition. To our knowledge, in BHD de novo mutations have thus far not been reported. Here we describe a patient who presented with spontaneous pneumothorax due to a de novo FLCN mutation. Subsequently, skin fibrofolliculomas were diagnosed and Magnetic Resonance Imaging (MRI) of the kidneys revealed a small left-sided renal cancer, treated by partial left nephrectomy. Histologically, the tumour was a chromophobe renal cancer. Since the molecular pathogenesis of renal cancer in BHD is incompletely understood, we analysed the tumour for loss of heterozygosity and expression of FLCN. Patients and methods Patient and family data The proband, a 30-year-old man, had recently been admitted to our hospital due to pneumothorax. He was referred to the department of clinical genetics by the dermatologist, who had identified multiple skin-coloured centro-facial papules histologically compatible with fibrofolliculomas typical for Birt-Hogg-Dubé syndrome (Fig. 1). We collected patient and family data and performed FLCN mutation analysis. In addition, renal imaging was performed by MRI and renal ultrasound. 3.7 de novo FLCN mutation in patient with SP and RCC Mutation analysis For FLCN mutation analysis genomic DNA was extracted from blood samples after the patient gave informed consent. Primers for the amplification and sequencing of the 14 exons were designed as detailed by Nickerson et al. 4 PCR amplification was performed using a PE 9700 thermocycler (Applied Biosystems, Forster City, CA, USA). Sequencing reactions were performed using the Big 185
 and run on an ABI 3100XL or ABI 3730 genetic analyzer (Applied Biosystems).")
186 Figure 1. Multiple smooth facial papules in the proband. 3.7 de novo FLCN mutation in patient with SP and RCC Dye Terminator system (Applied Biosystems) and run on an ABI 3100XL or ABI 3730 genetic analyzer (Applied Biosystems). For the detection of deletions and duplications of one or more exons MLPA analysis was performed using MLPA kit P256 (MRC Holland, Paternity confirmation To confirm paternity and exclude sample mix-up DNA samples of the patient and both parents were analysed using the Powerplex 16 system (Promega Madison, WI, USA). Molecular analysis of the renal tumour (a) Mutation analysis Genomic DNA was isolated from paraffin-embedded tumour material with the Macherey-Nagel kit for FFPE material (Macherey-Nagel, Düren, Germany) according to the manufacturer s instructions. Tumour tissue was isolated by needle scraping of macroscopically visible cancerous areas. Loss of heterozygosity was assessed by amplifying exon 6 using a Corbett Rotorgene 6000 (Qiagen, Venlo, the Netherlands) real-time system (primer sequences and conditions available on request). Sequencing reactions were performed with the PCR primers using the ABI BigDye terminator (v 1.1) kit according to the manufacturer s instructions and analyzed on an ABI 3100 capillary system (Applied Biosystems, Carlsbad, CA, USA). Sequence traces were assembled and examined using the PhredPhrap-Consed software package. The amplified tumour DNA was cloned into the pcr2.1-topo vector (Invitrogen, Groningen, The Netherlands) to determine whether the second hit had occurred in cis or in trans to the germline mutation. (b) Immunohistochemistry Procedures used for immunohistochemistry have been described in detail elsewhere. 19 Polyclonal FLCN antibody (rabbit) was a kind gift of professor Arnim Pause (McGill University, Montreal, Canada). Four µm formalin-fixed, paraffin-embedded (FFPE) sections of tumour sample, obtained during surgery, were deparaffinized in xylene and dehydrated through graded ethanol concentrations. Endogenous peroxidase activity was blocked by incubation in 3% (w/v) hydrogen peroxide (H 2 O 2 ) in methanol for 186

187 30 minutes, followed by microwave treatment using 10 mmol/l citrate buffer (ph 6) for 10 minutes (90W) to facilitate antigen retrieval. Non-specific protein binding was blocked using 3% bovine-serumalbumin in tris-buffered saline tween-20. Primary antibody was diluted in Dako Antibody diluent and incubated for 1 hour at room temperature. Secondary detection was done by use of the Envision detection system (Dako Netherlands BV, Heverlee, Belgium) for 30 minutes and bound antibody was visualized by using 3,3-diaminobenzidine (DAB) for 10 minutes. Tissue was counterstained with Gill II haematoxylin, dehydrated and coverslipped. Dako Washbuffer was used throughout for washing. Results Patient and family data Both parents and the two siblings of the proband were healthy. The multiple fibrofolliculomas in the proband which started to develop from the age of about 25 years are depicted in Fig. 1. A few weeks prior to referral the patient had been treated for left-sided spontaneous pneumothorax. He had experienced two previous episodes of left-sided spontaneous pneumothorax, at the ages of 19 and 22 years, treated by drainage and drainage plus tetracycline pleurodesis, respectively. A recent thoracic Computer Tomography (CT) showed a left-sided pneumothorax (Fig. 2) but no intrapulmonary cystic lesions apart from a small left-sided subpleural apical bleb. Since pneumothorax had recurred despite former drainage and pleurodesis, video-assisted thoracoscopic surgery was performed, which revealed a small rim of fibrosis in the left upper lobe probably due to collapsed bullae. Excision of the apex of the left upper lobe and pleurectomy were performed. Histologically, collapsed bullae associated with mild pleuritis, minor local emphysematous changes and a small rim of fibrosis with focal excentric intima fibrosis of the pulmonary artery were observed (Fig. 3). Abdominal MRI revealed a 18 mm left renal lesion which - notably - was not detected on renal ultrasound. The differential diagnosis was renal cancer or oncocytoma. A follow-up MRI with contrast made three months later showed that the lesion had not grown (Fig. 4). After weighing the various management options (follow-up, nephron sparing treatment) a left partial nephrectomy was performed, which revealed a pt1an0 chromophobe renal cancer (Fig. 5). 3.7 de novo FLCN mutation in patient with SP and RCC Figure 2. Left-sided pneumothorax; of note, pulmonary cysts were absent at all levels. 187

 in the collapsed resection specimen.")



188 A 3.7 de novo FLCN mutation in patient with SP and RCC B Figure 3. (A) 2,5x (H & E staining) overview of a lung bulla (asterisks) in the collapsed resection specimen. (B) and (C) (elastin and H & E stain, respectively) show thick elastotic alveolar walls and fibrosis in subpleural alveolar spaces and local marginal fibrotic thickening of the pleura. C Figure 4. The asymptomatic left renal tumour in the proband as revealed by MRI. Figure 5. Histopathology of the chromophobe kidney cancer (overview, 2.5x); the insert (40x) shows the monotonous cytonuclear appearance. 188
 wild type sequence. 3.")

189 Figure 6. Electropherogram of part of exon 6 of FLCN. (A) sequence of the DNA of the patient showing the FLCN mutation c.499c>t; due to the mutation codon 167, which is underlined, is changed from CAG encoding Gln into TAG encoding a stop; (B) wild type sequence. 3.7 de novo FLCN mutation in patient with SP and RCC Figure 7. Sequence traces of cloned FLCN exon 6 fragments amplified from tumor DNA showing the second hit mutation in the bottom panel, with a wild type sequence in the top for comparison. Since the sequence trace only shows one mutation (the second hit) and not the germ-line change (not shown due to space constraints), it must have occurred in trans to the germ line mutation. The reverse strand is shown as it had the best read quality. The 15bp deletion is shown in the shaded area and is emphasized with a continuous line. The dashed lines indicate how the sequence has changed. The intron-exon boundary is indicated by a vertical arrow. 189
 The kidney tumour shows pronounced staining, consistent with expression of one or both the mutant alleles.")
 Negative control, secondary antibody only on normal skin. Molecular data In the proband a pathogenic FLCN mutation c.499c>t, p.gln167x, located within exon 6 was identified (Fig.")


190 A B C D 3.7 de novo FLCN mutation in patient with SP and RCC Figure 8. Immunohistochemical staining of the renal tumor with a polyclonal FLCN antibody. (A) Unaffected kidney tissue of the proband. Strong FLCN expression throughout the kidney tubules, but not in a glomerulus. (B) The kidney tumour shows pronounced staining, consistent with expression of one or both the mutant alleles. (C) Positive control: normal skin from an unrelated healthy individual. Uniform staining in the epidermis and hair follicle as previously reported. Note the presence of FLCN in sebaceous glands. (D) Negative control, secondary antibody only on normal skin. Molecular data In the proband a pathogenic FLCN mutation c.499c>t, p.gln167x, located within exon 6 was identified (Fig. 6), which was absent in his parents and both siblings who had no signs of BHD. VNTR markers were tested in the patient and his parents. For all markers tested the patient showed one maternal and one paternal allele thus confirming paternity and excluding sample mix-up. Mutation analysis of the tumour indicated the presence of a second somatic hit, c.397-7_404del15, which deletes the exon 6 splice acceptor site and which is expected to result in exon skipping and production of a truncated protein. There was no material available for RNA isolation and therefore we were not able to analyze the consequences of the mutation. Subsequent cloning of amplified tumour DNA showed that the somatic mutation had occurred in trans to the germline mutation (Fig. 7). Immunohistochemical staining of the tumour showed robust FLCN expression; normal kidney tubules and skin also expressed FLCN (Fig. 8). Discussion Among the more than 35 BHD families with pathogenic germline FLCN mutations identified in our centre, most of which have been published 20 21, this is the only de novo FLCN mutation identified. This type of FLCN mutation, c.499c>t, p.gln167x, can be classified as pathogenic and causative of BHD since it leads to a premature stop. The FLCN mutation identified in this case has not been listed 190
191 in the FLCN mutation databases Since the proband had all three major manifestations of BHD, i.e. fibrofolliculomas, pneumothorax and renal cancer, a somatic mosaic of the FLCN mutation is unlikely. The absence of the mutation in both parents is consistent with a de novo mutation, but somatic mosaicism in one of the parents cannot be excluded. We cannot correlate the clinical expression in this patient to characteristics of the specific mutation since thus far, in BHD, no clear genotype-phenotype correlations have been found. To our knowledge, de novo FLCN mutations have not been reported previously. The frequency of de novo FLCN mutations is probably low, but may be under diagnosed if BHD is not considered in sporadic patients who show one or more of the syndromic clinical features. For clinical diagnosis the time scale for the various manifestations of BHD is also relevant. For example, pneumothorax may be the first manifestation in a patient who will develop fibrofolliculomas and / or renal cancer at a later age. If pneumothorax is the only manifestation the diagnosis BHD may easily be missed. In de novo cases, the absence of a positive family history for syndromic features increases the difficulty of recognizing the condition. Skin lesions may be absent in up to 20% of FLCN mutation carriers and if typical skin lesions are present they may not be recognized as marker lesions for the syndrome. Apart from the unusual cause of BHD in this patient - a de novo FLCN mutation - his clinical features are also remarkable and are therefore considered below in some detail. The recurrent spontaneous pneumothorax in this patient was initially interpreted as primary, which is the common form of this disease. The pathogenesis of primary spontaneous pneumothorax (PSP) is incompletely understood. Probably, PSP is associated with a focal inflammatory process related to the pleura and underlying lung. Small subpleural blebs or larger subpleural bullae, which are found in the majority of these patients, are only one feature of a complex and not fully understood pathogenetic mechanism. It remains unclear whether these emphysema-like changes are the cause of the air leak or merely a coincidental phenomenon. Subpleural blebs or bullae are also observed in about 15% of the normal population. In BHD, spontaneous pneumothorax has been linked directly to multiple bilateral and mostly basally located lung cysts, which are found in the majority of patients. In the patient described here thoracic CT did not show lung cysts but only a left apical subpleural bleb. The absence of lung cysts in a BHD patient who exhibits pneumothorax is remarkable: all 48 BHD patients with pneumothorax described by Toro et al. 24 had multiple lung cysts. However, in BHD, the occurrence of pneumothorax without lung cysts on thoracic CT has been described previously Thus, the relationship between lung cysts and pneumothorax in BHD has not yet been fully clarified. Few case studies have reported lung histopathology in BHD and in general the findings were nonspecific In the case described here the surgical specimen showed subpleural fibrosis in pre-existing alveolar walls associated with focal excentric intima fibrosis in a small pulmonary artery. Since these are morphologic changes of a small infarction, due to local hypoxia, a local infarction may have led to a local bulla. The molecular pathogenesis of renal cancer in BHD has been evaluated in a series of studies. Vocke et al. 31 demonstrated a second somatic FLCN mutation or loss of heterozygosity in the majority (70%) 3.7 de novo FLCN mutation in patient with SP and RCC 191
192 of 77 BHD-associated renal tumours. These findings were interpreted as supportive for a tumour suppressor role for FLCN. By immunohistochemical staining we detected strong FLCN expression. In theory, this could be due to expression in cells in which a wild type allele is still present. However, when sequencing cloned tumour DNA in order to determine whether the second hit we found was indeed in trans, we detected no wild type sequences. We therefore suggest that at least one of the mutant alleles is expressed in the tumour. The second hit mutation is predicted to result in skipping of exon 6 in which case the proper reading frame for FLCN is maintained. This mrna encodes for a mutant protein lacking the amino acids encoded by exon 6 and detected by the FLCN antibody, thus explaining the IHC result. As FLCN truncations are considered to result in a non-functional protein, our observations are consistent with a tumour suppressor role for FLCN. 3.7 de novo FLCN mutation in patient with SP and RCC An important goal of diagnosing BHD is prevention of disease burden and death due to renal cancer. In the present case, early diagnosis of a chomophobe renal cancer allowed curative surgical treatment. The renal tumour identified with MRI was not detected by renal ultrasound. Undoubtedly, MRI is more sensitive than ultrasound for the detection of small renal lesions and therefore MRI is generally advised for surveillance of individuals at high renal cancer risk. In summary, the case described here with a de novo FLCN mutation shows that BHD should be considered in patients with a negative family history who present with one or more of the syndromic features. We also showed that mutant FLCN can be expressed in BHD-associated renal cancer, raising the possibility that BHD-associated mutations do not result in complete loss of functionality. 192
193 References 1. Birt AR, Hogg GR, Dubé WJ Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol 1977;113: Roth JS, Rabinowitz AD, Benson M Bilateral renal cell carcinoma in the Birt-Hogg-Dubé syndrome. J Am Acad Dermatol 1993; 29: Zbar B, Alvord WG, Glenn G et al. Risk of renal and colonic neoplasms and spontaneous pneumothorax in the Birt-Hogg-Dubé syndrome. Cancer Epidemiol Biomarkers Prev. 2002; 11: Nickerson ML, Warren MB, Toro JR et al. Mutations in a novel gene lead to kidney tumours, lung wall defects, and benign tumours of the hair follicle in patients with the Birt-Hogg-Dubé syndrome. Cancer Cell 2002; 2: Graham RB, Nolasco M, Peterlin B et al Nonsense mutations in folliculin presenting as isolated familial spontaneous pneumothorax in adults. Am J Respir Crit Care Med 2005; 172: Painter JN, Tapanainen H, Somer M A 4-bp deletion in the Birt-Hogg-Dubé gene (FLCN) causes dominantly inherited spontaneous pneumothorax. Am J Hum Genet 2005; 76: Woodward ER, Ricketts C, Killick P et al. Familial non-vhl clear cell (conventional) renal cell carcinoma: clinical features, segregation analysis, and mutation analysis of FLCN. Clin Cancer Res 2008; 14: Schmidt LS, Nickerson ML, Warren MB et al. Germline BHD-mutation spectrum and phenotype analysis of a large cohort of families with Birt-Hogg-Dubé syndrome. Am J Hum Genet 2005; 76: Toro JR, Wei MH, Glenn GM et al BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet 2008; 45: Benhammou JN, Vocke CD, Santani A et al Identification of intragenic deletions and duplication in the FLCN gene in Birt-Hogg-Dubé syndrome. Genes Chromosomes Cancer 2011; 50: Wei MH, Blake PW, Shevchenko J, Toro JR The folliculin mutation database: an online database of mutations associated with Birt-Hogg-Dubé syndrome. Hum Mutat 2009; 30: E Lim DH, Rehal PK, Nahorski MS et al. A new locus-specific database (LSDB) for mutations in the folliculin (FLCN) gene. Hum Mutat 2010; 1: E van Steensel MA, van Geel M, Badeloe S et al. Molecular pathways involved in hair follicle tumor formation: all about mammalian target of rapamycin? Exp Dermatol 2009; 18: Hasumi Y, Baba M, Ajima R et al. Homozygous loss of BHD causes early embryonic lethality and kidney tumor development with activation of mtorc1 and mtorc2. Proc Natl Acad Sci USA 2009; 106: Nookala RK, Langemeyer L, Pacitto A et al. Crystal structure of folliculin reveals a hidden function in genetically inherited renal cancer. Open Biol 2012; 2: Menko FH, van Steensel MA, Giraud S et al European BHD Consortium. Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncol 2009; 10: Win AK, Jenkins MA, Buchanan DD et al. Determining the frequency of de novo germline mutations in DNA mismatch repair genes. J Med Genet 2011; 48: Aretz S, Uhlhaas S, Caspari R, Frequency and parental origin of de novo APC mutations in familial adenomatous polyposis. Eur J Hum Genet 2004; 12: Preston RS, Phil A, Claessens T et al. Absence of the Birt-Hogg-Dubé gene product is associated with increased hypoxia-inducible factor transcriptional activity and a loss of metabolic flexibility. Oncogene 2011; 30: Leter EM, Koopmans AK, Gille JJ et al Birt-Hogg- Dubé syndrome: clinical and genetic studies of 20 families. J Invest Dermatol 2008; 128: Houweling, AC, Gijezen, LM, Jonker MA et al. Renal cancer and pneumothorax risk in Birt Hogg Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families. Br J Cancer 2011; 105: Noppen, M. Spontaneous pneumothorax: epidemiology, pathophysiology and cause. Eur Resp Rev 2010; 19: de novo FLCN mutation in patient with SP and RCC 193
194 Grundy S, Bentley A, Tschopp J-M. Primary spontaneous pneumothorax: A diffuse disease of the pleura. Respiration 2012; 83: Toro JR, Pautler SE, Stewart L et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med 2007; 175: Fröhlich BA, Zeitz C, Mátyás G et al. Novel mutations in the folliculin gene associated with spontaneous pneumothorax. Eur Resp J 2008; 32: Kluger N, Giraud S, Coupier I et al. Birt-Hogg-Dubé syndrome: clinical and genetic studies of 10 French families. Br. J. Dermatol. 2010; 162: Butnor KJ & Guinee Jr DG Pleuropulmonary pathology in Birt-Hogg-Dubé syndrome. Am J Surg Pathol 2006; 30: Ayo DS, Aughenbaugh GL, Yi ES et al Cystic lung disease in Birt-Hogg-Dubé syndrome. Chest 2007; 132: Koga S, Furuya M, Takahashi Y et al Lung cysts in Birt-Hogg-Dubé syndrome: histopathological characteristics and aberrant sequence repeats. Pathol Internat 2009; 59: Furuya M, Tanaka R, Koga S et al. Pulmonary cysts of Birt-Hogg-Dubé: A clinicopathological and immunohistochemical study of 9 families. Am J of Surg Pathol 2012; 36: Vocke CD, Yang Y, Pavlovich CP et al. High frequency of somatic frameshift BHD gene mutations in Birt-Hogg-Dubé-associated renal tumors. J Natl Cancer Inst 2005; 97: de novo FLCN mutation in patient with SP and RCC 194
195
196

197 PART 4 Summary, discussion and future perspectives
Case Report Bilateral Renal Tumour as Indicator for Birt-Hogg-Dubé Syndrome
 Case Reports in Medicine, Article ID 618675, 4 pages http://dx.doi.org/10.1155/2014/618675 Case Report Bilateral Renal Tumour as Indicator for Birt-Hogg-Dubé Syndrome P. C. Johannesma, 1 R. J. A. van Moorselaar,
Case Reports in Medicine, Article ID 618675, 4 pages http://dx.doi.org/10.1155/2014/618675 Case Report Bilateral Renal Tumour as Indicator for Birt-Hogg-Dubé Syndrome P. C. Johannesma, 1 R. J. A. van Moorselaar,
Genetic Predisposition to Cancer
 Genetic Predisposition to Cancer Elena Castro, MD, PhD Prostate Cancer and GU tumours Unit Spanish National Cancer Research Centre Madrid, Spain Abstract 750O: Early detection of hereditary renal cell
Genetic Predisposition to Cancer Elena Castro, MD, PhD Prostate Cancer and GU tumours Unit Spanish National Cancer Research Centre Madrid, Spain Abstract 750O: Early detection of hereditary renal cell
Spontaneous pneumothorax as indicator for Birt- Hogg-Dubé syndrome in paediatric patients
 Spontaneous pneumothorax as indicator for Birt- Hogg-Dubé syndrome in paediatric patients Paul C Johannesma 1 Email: p.johannesma@vumc.nl Ben EEM van den Borne 2 Email: ben.vd.borne@catharinaziekenhuis.nl
Spontaneous pneumothorax as indicator for Birt- Hogg-Dubé syndrome in paediatric patients Paul C Johannesma 1 Email: p.johannesma@vumc.nl Ben EEM van den Borne 2 Email: ben.vd.borne@catharinaziekenhuis.nl
Spontaneous pneumothorax as indicator for Birt-Hogg-Dubé syndrome in paediatric patients
 Johannesma et al. BMC Pediatrics 2014, 14:171 CASE REPORT Open Access Spontaneous pneumothorax as indicator for Birt-Hogg-Dubé syndrome in paediatric patients Paul C Johannesma 1, Ben EEM van den Borne
Johannesma et al. BMC Pediatrics 2014, 14:171 CASE REPORT Open Access Spontaneous pneumothorax as indicator for Birt-Hogg-Dubé syndrome in paediatric patients Paul C Johannesma 1, Ben EEM van den Borne
A Japanese Family with Multiple Lung Cysts and Recurrent Pneumothorax: A Possibility of Birt-Hogg-Dubé Syndrome
 CASE REPORT A Japanese Family with Multiple Lung Cysts and Recurrent Pneumothorax: A Possibility of Birt-Hogg-Dubé Syndrome Hiroshi Ishii 1, Hiroaki Oka 1, Yuka Amemiya 1, Atsuko Iwata 1, Satoshi Otani
CASE REPORT A Japanese Family with Multiple Lung Cysts and Recurrent Pneumothorax: A Possibility of Birt-Hogg-Dubé Syndrome Hiroshi Ishii 1, Hiroaki Oka 1, Yuka Amemiya 1, Atsuko Iwata 1, Satoshi Otani
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 18 CBULP 2011 041 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 18 CBULP 2011 041 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Clinical and genetic study of a large Chinese family presented with familial spontaneous pneumothorax
 Original Article Clinical and genetic study of a large Chinese family presented with familial spontaneous pneumothorax Huajie Xing, Yanguo Liu, Guanchao Jiang, Xiao Li, Yanyan Hou, Fan Yang, Jun Wang Department
Original Article Clinical and genetic study of a large Chinese family presented with familial spontaneous pneumothorax Huajie Xing, Yanguo Liu, Guanchao Jiang, Xiao Li, Yanyan Hou, Fan Yang, Jun Wang Department
A rare association of parotid oncocytoma, lipoma, multinodular goitre and uterine adenomysosis
 ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 7 Number 2 A rare association of parotid oncocytoma, lipoma, multinodular goitre and uterine adenomysosis P Sinha, S Sharma, S Agarwal, R Ray
ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 7 Number 2 A rare association of parotid oncocytoma, lipoma, multinodular goitre and uterine adenomysosis P Sinha, S Sharma, S Agarwal, R Ray
Renal Cell Carcinoma: Genetics & Imaging Srinivasa R Prasad University of Texas San Antonio
 Renal Cell Carcinoma: Genetics & Imaging Srinivasa R Prasad University of Texas HSC @ San Antonio No financial disclosures Acknowledgements Dr. Peter Choyke, NIH My Gurus @ MIR, MGH 2004 WHO Taxonomy of
Renal Cell Carcinoma: Genetics & Imaging Srinivasa R Prasad University of Texas HSC @ San Antonio No financial disclosures Acknowledgements Dr. Peter Choyke, NIH My Gurus @ MIR, MGH 2004 WHO Taxonomy of
Birt-Hogg-Dubé Syndrome: Clinical and Genetic Studies of 20 Families
 ORIGINAL ARTICLE Birt-Hogg-Dubé Syndrome: Clinical and Genetic Studies of 20 Families Edward M. Leter 1,9, A. Karijn Koopmans 2,9, Johan J.P. Gille 1, Theo A.M. van Os 3, Gabriëlle G. Vittoz 1, Eric F.L.
ORIGINAL ARTICLE Birt-Hogg-Dubé Syndrome: Clinical and Genetic Studies of 20 Families Edward M. Leter 1,9, A. Karijn Koopmans 2,9, Johan J.P. Gille 1, Theo A.M. van Os 3, Gabriëlle G. Vittoz 1, Eric F.L.
Kidney Cancer Causes, Risk Factors, and Prevention
 Kidney Cancer Causes, Risk Factors, and Prevention Risk Factors A risk factor is anything that affects your chance of getting a disease such as cancer. Learn more about the risk factors for kidney cancer.
Kidney Cancer Causes, Risk Factors, and Prevention Risk Factors A risk factor is anything that affects your chance of getting a disease such as cancer. Learn more about the risk factors for kidney cancer.
Hereditary Leiomyomatosis and Renal Cell Carcinoma Variant of Reed s Syndrome - A Rare Case Report
 American Research Journal of Urology Volume 1, Issue 1, pp:26-30 Case Hereditary Leiomyomatosis and Renal Cell Carcinoma Variant of Reed s Syndrome - A Rare Case Manas Babu, Devesh Bansal, Sony Mehta,
American Research Journal of Urology Volume 1, Issue 1, pp:26-30 Case Hereditary Leiomyomatosis and Renal Cell Carcinoma Variant of Reed s Syndrome - A Rare Case Manas Babu, Devesh Bansal, Sony Mehta,
BHD mutations, clinical and molecular genetic investigations of Birt Hogg Dubé syndrome: a new series of 50 families and a review of published reports
 BHD mutations, clinical and molecular genetic investigations of Birt Hogg Dubé syndrome: a new series of 50 families and a review of published reports J R Toro, 1 M-H Wei, 1,2 G M Glenn, 1 M Weinreich,
BHD mutations, clinical and molecular genetic investigations of Birt Hogg Dubé syndrome: a new series of 50 families and a review of published reports J R Toro, 1 M-H Wei, 1,2 G M Glenn, 1 M Weinreich,
Birt-Hogg-Dubé Syndrome with Multiple Cysts and Recurrent Pneumothorax: Pathological Findings
 CASE REPORT Birt-Hogg-Dubé Syndrome with Multiple Cysts and Recurrent Pneumothorax: Pathological Findings Makoto Hayashi 1, Noboru Takayanagi 1, Takashi Ishiguro 1, Yutaka Sugita 1, Yoshinori Kawabata
CASE REPORT Birt-Hogg-Dubé Syndrome with Multiple Cysts and Recurrent Pneumothorax: Pathological Findings Makoto Hayashi 1, Noboru Takayanagi 1, Takashi Ishiguro 1, Yutaka Sugita 1, Yoshinori Kawabata
Renal cancer and pneumothorax risk in Birt Hogg Dubé syndrome; an analysis of 115 FLCN mutation carriers from 35 BHD families
 British Journal of Cancer (2011) 105, 1912 1919 All rights reserved 0007 0920/11 www.bjcancer.com Renal cancer and pneumothorax risk in Birt Hogg Dubé syndrome; an analysis of 115 FLCN mutation carriers
British Journal of Cancer (2011) 105, 1912 1919 All rights reserved 0007 0920/11 www.bjcancer.com Renal cancer and pneumothorax risk in Birt Hogg Dubé syndrome; an analysis of 115 FLCN mutation carriers
Birt Hogg Dubé syndrome: a case report and a review of the literature
 European Clinical Respiratory Journal ISSN: (Print) 2001-8525 (Online) Journal homepage: http://www.tandfonline.com/loi/zecr20 Birt Hogg Dubé syndrome: a case report and a review of the literature Dea
European Clinical Respiratory Journal ISSN: (Print) 2001-8525 (Online) Journal homepage: http://www.tandfonline.com/loi/zecr20 Birt Hogg Dubé syndrome: a case report and a review of the literature Dea
Information for You and Your Family
 Information for You and Your Family What is Prevention? Cancer prevention is action taken to lower the chance of getting cancer. In 2017, more than 1.6 million people will be diagnosed with cancer in the
Information for You and Your Family What is Prevention? Cancer prevention is action taken to lower the chance of getting cancer. In 2017, more than 1.6 million people will be diagnosed with cancer in the
Apoptosis and colorectal cancer. Studies on pathogenesis and potential therapeutic targets Koornstra, Jan
 University of Groningen Apoptosis and colorectal cancer. Studies on pathogenesis and potential therapeutic targets Koornstra, Jan IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
University of Groningen Apoptosis and colorectal cancer. Studies on pathogenesis and potential therapeutic targets Koornstra, Jan IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
Samer Ghosn, MD Associate professor, Derpartment of Dermatology American University of Beirut Medical Center. Follicular lesions
 Samer Ghosn, MD Associate professor, Derpartment of Dermatology American University of Beirut Medical Center Follicular lesions Introduction Follicular lesions are important to recognize: For proper management
Samer Ghosn, MD Associate professor, Derpartment of Dermatology American University of Beirut Medical Center Follicular lesions Introduction Follicular lesions are important to recognize: For proper management
UvA-DARE (Digital Academic Repository) The systemic right ventricle van der Bom, T. Link to publication
 The systemic right ventricle van der Bom, T. Link to publication") UvA-DARE (Digital Academic Repository) The systemic right ventricle van der Bom, T. Link to publication Citation for published version (APA): van der Bom, T. (2014). The systemic right ventricle. General
UvA-DARE (Digital Academic Repository) The systemic right ventricle van der Bom, T. Link to publication Citation for published version (APA): van der Bom, T. (2014). The systemic right ventricle. General
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Pulmonary Pathology of Birt-Hogg-Dubé (BHD) Syndrome Mitsuko FURUYA, Ikuma KATO, Reiko TANAKA, Yukio NAKATANI. Yokohama City University, Japan Chiba University, Japan
Enterprise Interest Nothing to declare Pulmonary Pathology of Birt-Hogg-Dubé (BHD) Syndrome Mitsuko FURUYA, Ikuma KATO, Reiko TANAKA, Yukio NAKATANI. Yokohama City University, Japan Chiba University, Japan
Case Based Learning Program
 Case Based Learning Program The Department of Urology Glickman Urological & Kidney Institute Cleveland Clinic Case Number 5 CBULP 2010 001 Case Based Urology Learning Program Editor: Associate Editor:
Case Based Learning Program The Department of Urology Glickman Urological & Kidney Institute Cleveland Clinic Case Number 5 CBULP 2010 001 Case Based Urology Learning Program Editor: Associate Editor:
Pulmonary features of Birt-Hogg-Dubé syndrome: Cystic lesions and pulmonary histiocytoma
 Respiratory Medicine (2011) 105, 768e774 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed Pulmonary features of Birt-Hogg-Dubé syndrome: Cystic lesions and pulmonary histiocytoma
Respiratory Medicine (2011) 105, 768e774 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed Pulmonary features of Birt-Hogg-Dubé syndrome: Cystic lesions and pulmonary histiocytoma
UvA-DARE (Digital Academic Repository) Intraarterial treatment for acute ischemic stroke Berkhemer, O.A. Link to publication
 Intraarterial treatment for acute ischemic stroke Berkhemer, O.A. Link to publication") UvA-DARE (Digital Academic Repository) Intraarterial treatment for acute ischemic stroke Berkhemer, O.A. Link to publication Citation for published version (APA): Berkhemer, O. A. (2016). Intraarterial
UvA-DARE (Digital Academic Repository) Intraarterial treatment for acute ischemic stroke Berkhemer, O.A. Link to publication Citation for published version (APA): Berkhemer, O. A. (2016). Intraarterial
Multimodality imaging in chronic coronary artery disease Maureen M. Henneman
 Multimodality imaging in chronic coronary artery disease Maureen M. Henneman 080237 Henneman boek.indb 1 03-11-2008 10:56:25 The studies described in this thesis were performed at the Department of Cardiology
Multimodality imaging in chronic coronary artery disease Maureen M. Henneman 080237 Henneman boek.indb 1 03-11-2008 10:56:25 The studies described in this thesis were performed at the Department of Cardiology
Identification of a novel duplication mutation in the VHL gene in a large Chinese family with Von Hippel-Lindau (VHL) syndrome
 syndrome") Identification of a novel duplication mutation in the VHL gene in a large Chinese family with Von Hippel-Lindau (VHL) syndrome L.H. Cao 1, B.H. Kuang 2, C. Chen 1, C. Hu 2, Z. Sun 1, H. Chen 2, S.S. Wang
Identification of a novel duplication mutation in the VHL gene in a large Chinese family with Von Hippel-Lindau (VHL) syndrome L.H. Cao 1, B.H. Kuang 2, C. Chen 1, C. Hu 2, Z. Sun 1, H. Chen 2, S.S. Wang
Risk of Renal and Colonic Neoplasms and Spontaneous Pneumothorax in the Birt-Hogg-Dubé Syndrome 1
 Vol. 11, 393 400, April 2002 Cancer Epidemiology, Biomarkers & Prevention 393 Risk of Renal and Colonic Neoplasms and Spontaneous Pneumothorax in the Birt-Hogg-Dubé Syndrome 1 Berton Zbar, 2 W. Gregory
Vol. 11, 393 400, April 2002 Cancer Epidemiology, Biomarkers & Prevention 393 Risk of Renal and Colonic Neoplasms and Spontaneous Pneumothorax in the Birt-Hogg-Dubé Syndrome 1 Berton Zbar, 2 W. Gregory
UvA-DARE (Digital Academic Repository) Bronchial Thermoplasty in severe asthma d'hooghe, J.N.S. Link to publication
 Bronchial Thermoplasty in severe asthma d'hooghe, J.N.S. Link to publication") UvA-DARE (Digital Academic Repository) Bronchial Thermoplasty in severe asthma d'hooghe, J.N.S. Link to publication Citation for published version (APA): d'hooghe, J. N. S. (2018). Bronchial Thermoplasty
UvA-DARE (Digital Academic Repository) Bronchial Thermoplasty in severe asthma d'hooghe, J.N.S. Link to publication Citation for published version (APA): d'hooghe, J. N. S. (2018). Bronchial Thermoplasty
Determinants of renal microvascular reactivity in rat models of diabetes mellitus and obesity. Marjon Troost-Roos
 Determinants of renal microvascular reactivity in rat models of diabetes mellitus and obesity Marjon Troost-Roos The studies presented in this thesis were performed at the Laboratory for Physiology of
Determinants of renal microvascular reactivity in rat models of diabetes mellitus and obesity Marjon Troost-Roos The studies presented in this thesis were performed at the Laboratory for Physiology of
Citation for published version (APA): Diederen, K. (2018). Pediatric inflammatory bowel disease: Monitoring, nutrition and surgery.
: Diederen, K. (2018). Pediatric inflammatory bowel disease: Monitoring, nutrition and surgery.") UvA-DARE (Digital Academic Repository) Pediatric inflammatory bowel disease Diederen, K. Link to publication Citation for published version (APA): Diederen, K. (2018). Pediatric inflammatory bowel disease:
UvA-DARE (Digital Academic Repository) Pediatric inflammatory bowel disease Diederen, K. Link to publication Citation for published version (APA): Diederen, K. (2018). Pediatric inflammatory bowel disease:
Citation for published version (APA): Lutke Holzik, M. F. (2007). Genetic predisposition to testicular cancer s.n.
: Lutke Holzik, M. F. (2007). Genetic predisposition to testicular cancer s.n.") University of Groningen Genetic predisposition to testicular cancer Lutke Holzik, Martijn Frederik IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite
University of Groningen Genetic predisposition to testicular cancer Lutke Holzik, Martijn Frederik IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite
Case Report Staged, Open, No-Ischemia Nephron-Sparing Surgery for Bilateral-Multiple Kidney Tumors in a Patient with Birt-Hogg-Dubé Syndrome
 Case Reports in Medicine Volume 2012, Article ID 639629, 6 pages doi:10.1155/2012/639629 Case Report Staged, Open, No-Ischemia Nephron-Sparing Surgery for Bilateral-Multiple Kidney Tumors in a Patient
Case Reports in Medicine Volume 2012, Article ID 639629, 6 pages doi:10.1155/2012/639629 Case Report Staged, Open, No-Ischemia Nephron-Sparing Surgery for Bilateral-Multiple Kidney Tumors in a Patient
Citation for published version (APA): Zeddies, S. (2015). Novel regulators of megakaryopoiesis: The road less traveled by
: Zeddies, S. (2015). Novel regulators of megakaryopoiesis: The road less traveled by") UvA-DARE (Digital Academic Repository) Novel regulators of megakaryopoiesis: The road less traveled by Zeddies, S. Link to publication Citation for published version (APA): Zeddies, S. (2015). Novel regulators
UvA-DARE (Digital Academic Repository) Novel regulators of megakaryopoiesis: The road less traveled by Zeddies, S. Link to publication Citation for published version (APA): Zeddies, S. (2015). Novel regulators
Building blocks for return to work after sick leave due to depression de Vries, Gabe
 UvA-DARE (Digital Academic Repository) Building blocks for return to work after sick leave due to depression de Vries, Gabe Link to publication Citation for published version (APA): de Vries, G. (2016).
UvA-DARE (Digital Academic Repository) Building blocks for return to work after sick leave due to depression de Vries, Gabe Link to publication Citation for published version (APA): de Vries, G. (2016).
Citation for published version (APA): de Groof, E. J. (2017). Surgery and medical therapy in Crohn s disease: Improving treatment strategies
: de Groof, E. J. (2017). Surgery and medical therapy in Crohn s disease: Improving treatment strategies") UvA-DARE (Digital Academic Repository) Surgery and medical therapy in Crohn s disease de Groof, E.J. Link to publication Citation for published version (APA): de Groof, E. J. (2017). Surgery and medical
UvA-DARE (Digital Academic Repository) Surgery and medical therapy in Crohn s disease de Groof, E.J. Link to publication Citation for published version (APA): de Groof, E. J. (2017). Surgery and medical
Citation for published version (APA): van der Paardt, M. P. (2015). Advances in MRI for colorectal cancer and bowel motility
: van der Paardt, M. P. (2015). Advances in MRI for colorectal cancer and bowel motility") UvA-DARE (Digital Academic Repository) Advances in MRI for colorectal cancer and bowel motility van der Paardt, M.P. Link to publication Citation for published version (APA): van der Paardt, M. P. (2015).
UvA-DARE (Digital Academic Repository) Advances in MRI for colorectal cancer and bowel motility van der Paardt, M.P. Link to publication Citation for published version (APA): van der Paardt, M. P. (2015).
UvA-DARE (Digital Academic Repository) What tumor cells cannot resist Ebbing, E.A. Link to publication
 What tumor cells cannot resist Ebbing, E.A. Link to publication") UvA-DARE (Digital Academic Repository) What tumor cells cannot resist Ebbing, E.A. Link to publication Citation for published version (APA): Ebbing, E. A. (2018). What tumor cells cannot resist: Mechanisms
UvA-DARE (Digital Academic Repository) What tumor cells cannot resist Ebbing, E.A. Link to publication Citation for published version (APA): Ebbing, E. A. (2018). What tumor cells cannot resist: Mechanisms
Dissecting Lyme borreliosis; Clinical aspects, pathogenesis and prevention Coumou, J.
 UvA-DARE (Digital Academic Repository) Dissecting Lyme borreliosis; Clinical aspects, pathogenesis and prevention Coumou, J. Link to publication Citation for published version (APA): Coumou, J. (2016).
UvA-DARE (Digital Academic Repository) Dissecting Lyme borreliosis; Clinical aspects, pathogenesis and prevention Coumou, J. Link to publication Citation for published version (APA): Coumou, J. (2016).
Tumor control and normal tissue toxicity: The two faces of radiotherapy van Oorschot, B.
 UvA-DARE (Digital Academic Repository) Tumor control and normal tissue toxicity: The two faces of radiotherapy van Oorschot, B. Link to publication Citation for published version (APA): van Oorschot, B.
UvA-DARE (Digital Academic Repository) Tumor control and normal tissue toxicity: The two faces of radiotherapy van Oorschot, B. Link to publication Citation for published version (APA): van Oorschot, B.
Functional abdominal pain disorders in children: therapeutic strategies focusing on hypnotherapy Rutten, J.M.T.M.
 UvA-DARE (Digital Academic Repository) Functional abdominal pain disorders in children: therapeutic strategies focusing on hypnotherapy Rutten, J.M.T.M. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Functional abdominal pain disorders in children: therapeutic strategies focusing on hypnotherapy Rutten, J.M.T.M. Link to publication Citation for published version
Cowden Syndrome PTEN Hamartoma Tumor Syndrome. ACCME/Disclosure. 1. Background. Outline
 MASSACHUSETTS GENERAL HOSPITAL HARVARD MEDICAL SCHOOL PATHOLOGY Cowden Syndrome PTEN Hamartoma Tumor Syndrome ACCME/Disclosure Vania Nosé, MD, PhD Professor of Pathology Director of Anatomic Pathology
MASSACHUSETTS GENERAL HOSPITAL HARVARD MEDICAL SCHOOL PATHOLOGY Cowden Syndrome PTEN Hamartoma Tumor Syndrome ACCME/Disclosure Vania Nosé, MD, PhD Professor of Pathology Director of Anatomic Pathology
Birt Hogg Dubé syndrome: a literature review and case study of a Chinese woman presenting a novel FLCN mutation
 Hao et al. BMC Pulmonary Medicine (2017) 17:43 DOI 10.1186/s12890-017-0383-9 CASE REPORT Open Access Birt Hogg Dubé syndrome: a literature review and case study of a Chinese woman presenting a novel FLCN
Hao et al. BMC Pulmonary Medicine (2017) 17:43 DOI 10.1186/s12890-017-0383-9 CASE REPORT Open Access Birt Hogg Dubé syndrome: a literature review and case study of a Chinese woman presenting a novel FLCN
University of Groningen. Functional outcome after a spinal fracture Post, Richard Bernardus
 University of Groningen Functional outcome after a spinal fracture Post, Richard Bernardus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from
University of Groningen Functional outcome after a spinal fracture Post, Richard Bernardus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from
Clinical Cancer Genetics
 Clinical Cancer Genetics Lisen Axell, MS, CGC University of Colorado Cancer Center Individuals with cancer Making surgical decisions (lump vs. mast) Making treatment decisions (XRT) Concerns for additional
Clinical Cancer Genetics Lisen Axell, MS, CGC University of Colorado Cancer Center Individuals with cancer Making surgical decisions (lump vs. mast) Making treatment decisions (XRT) Concerns for additional
Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R.
 UvA-DARE (Digital Academic Repository) Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Falling: should one blame the heart? Jansen, Sofie. Link to publication
 Falling: should one blame the heart? Jansen, Sofie. Link to publication") UvA-DARE (Digital Academic Repository) Falling: should one blame the heart? Jansen, Sofie Link to publication Citation for published version (APA): Jansen, S. (2015). Falling: should one blame the heart?
UvA-DARE (Digital Academic Repository) Falling: should one blame the heart? Jansen, Sofie Link to publication Citation for published version (APA): Jansen, S. (2015). Falling: should one blame the heart?
UvA-DARE (Digital Academic Repository) Toothbrushing efficacy Rosema, N.A.M. Link to publication
 Toothbrushing efficacy Rosema, N.A.M. Link to publication") UvA-DARE (Digital Academic Repository) Toothbrushing efficacy Rosema, N.A.M. Link to publication Citation for published version (APA): Rosema, N. A. M. (2015). Toothbrushing efficacy. General rights It
UvA-DARE (Digital Academic Repository) Toothbrushing efficacy Rosema, N.A.M. Link to publication Citation for published version (APA): Rosema, N. A. M. (2015). Toothbrushing efficacy. General rights It
Renal tumours: use of immunohistochemistry & molecular pathology. Dr Lisa Browning John Radcliffe Hospital Oxford
 Renal tumours: use of immunohistochemistry & molecular pathology Dr Lisa Browning John Radcliffe Hospital Oxford Renal tumours: the use of immunohistochemistry & molecular pathology Classification of RCC
Renal tumours: use of immunohistochemistry & molecular pathology Dr Lisa Browning John Radcliffe Hospital Oxford Renal tumours: the use of immunohistochemistry & molecular pathology Classification of RCC
Finding the balance between overtreatment and undertreatment of ductal carcinoma in situ Elshof, L.E.
 UvA-DARE (Digital Academic Repository) Finding the balance between overtreatment and undertreatment of ductal carcinoma in situ Elshof, L.E. Link to publication Citation for published version (APA): Elshof,
UvA-DARE (Digital Academic Repository) Finding the balance between overtreatment and undertreatment of ductal carcinoma in situ Elshof, L.E. Link to publication Citation for published version (APA): Elshof,
Novel insights into the complexity of ischaemic heart disease derived from combined coronary pressure and flow velocity measurements van de Hoef, T.P.
 UvA-DARE (Digital Academic Repository) Novel insights into the complexity of ischaemic heart disease derived from combined coronary pressure and flow velocity measurements van de Hoef, T.P. Link to publication
UvA-DARE (Digital Academic Repository) Novel insights into the complexity of ischaemic heart disease derived from combined coronary pressure and flow velocity measurements van de Hoef, T.P. Link to publication
Tobacco control policies and socio-economic inequalities in smoking cessation Bosdriesz, J.R.
 UvA-DARE (Digital Academic Repository) Tobacco control policies and socio-economic inequalities in smoking cessation Bosdriesz, J.R. Link to publication Citation for published version (APA): Bosdriesz,
UvA-DARE (Digital Academic Repository) Tobacco control policies and socio-economic inequalities in smoking cessation Bosdriesz, J.R. Link to publication Citation for published version (APA): Bosdriesz,
Citation for published version (APA): Braakhekke, M. W. M. (2017). Randomized controlled trials in reproductive medicine: Disclosing the caveats
: Braakhekke, M. W. M. (2017). Randomized controlled trials in reproductive medicine: Disclosing the caveats") UvA-DARE (Digital Academic Repository) Randomized controlled trials in reproductive medicine Braakhekke, M.W.M. Link to publication Citation for published version (APA): Braakhekke, M. W. M. (2017). Randomized
UvA-DARE (Digital Academic Repository) Randomized controlled trials in reproductive medicine Braakhekke, M.W.M. Link to publication Citation for published version (APA): Braakhekke, M. W. M. (2017). Randomized
Case 1 PLEASE TURN OFF YOUR CELL PHONES 3/28/2017. Disclosure of Relevant Financial Relationships. Disclosure of Relevant Financial Relationships
 PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose
PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose
Proteinuria-associated renal injury and the effects of intervention in the renin-angiotensinaldosterone
 University of Groningen Proteinuria-associated renal injury and the effects of intervention in the renin-angiotensinaldosterone system Kramer, Andrea Brechtsje IMPORTANT NOTE: You are advised to consult
University of Groningen Proteinuria-associated renal injury and the effects of intervention in the renin-angiotensinaldosterone system Kramer, Andrea Brechtsje IMPORTANT NOTE: You are advised to consult
St. Dominic s Annual Cancer Report Outcomes
 St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/23937 holds various files of this Leiden University dissertation. Author: Liu, Zhen Title: Exploring the interplay between TGF-β and VEGF signalling in
Cover Page The handle http://hdl.handle.net/1887/23937 holds various files of this Leiden University dissertation. Author: Liu, Zhen Title: Exploring the interplay between TGF-β and VEGF signalling in
INTER- AND INTRA INDIVIDUAL VARIATION IN EARPRINTS LYNN M EIJERM AN
 INTER- AND INTRA INDIVIDUAL VARIATION IN EARPRINTS LYNN M EIJERM AN Inter- and intra-individual variation in earprints Meijerman, Lynn Thesis University Leiden With Ref. ISBN-10: 90-806456-9-9 ISBN-13:
INTER- AND INTRA INDIVIDUAL VARIATION IN EARPRINTS LYNN M EIJERM AN Inter- and intra-individual variation in earprints Meijerman, Lynn Thesis University Leiden With Ref. ISBN-10: 90-806456-9-9 ISBN-13:
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Renal Parenchymal Neoplasms
 Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
UvA-DARE (Digital Academic Repository) Functional defecation disorders in children Kuizenga-Wessel, S. Link to publication
 Functional defecation disorders in children Kuizenga-Wessel, S. Link to publication") UvA-DARE (Digital Academic Repository) Functional defecation disorders in children Kuizenga-Wessel, S. Link to publication Citation for published version (APA): Kuizenga-Wessel, S. (2017). Functional defecation
UvA-DARE (Digital Academic Repository) Functional defecation disorders in children Kuizenga-Wessel, S. Link to publication Citation for published version (APA): Kuizenga-Wessel, S. (2017). Functional defecation
Enzyme replacement therapy in Fabry disease, towards individualized treatment Arends, M.
 UvA-DARE (Digital Academic Repository) Enzyme replacement therapy in Fabry disease, towards individualized treatment Arends, M. Link to publication Citation for published version (APA): Arends, M. (2017).
UvA-DARE (Digital Academic Repository) Enzyme replacement therapy in Fabry disease, towards individualized treatment Arends, M. Link to publication Citation for published version (APA): Arends, M. (2017).
Testicular microlithiasis and undescended testis. Joery Goede
 Testicular microlithiasis and undescended testis Joery Goede ISBN : 978-94-91082-02-3 Author : Joery Goede Lay-out : Ruth Visser, VisserVisuals, Amsterdam, the Netherlands Printing : Ridderprint, the Netherlands
Testicular microlithiasis and undescended testis Joery Goede ISBN : 978-94-91082-02-3 Author : Joery Goede Lay-out : Ruth Visser, VisserVisuals, Amsterdam, the Netherlands Printing : Ridderprint, the Netherlands
UvA-DARE (Digital Academic Repository) Obesity, ectopic lipids, and insulin resistance ter Horst, K.W. Link to publication
 Obesity, ectopic lipids, and insulin resistance ter Horst, K.W. Link to publication") UvA-DARE (Digital Academic Repository) Obesity, ectopic lipids, and insulin resistance ter Horst, K.W. Link to publication Citation for published version (APA): ter Horst, K. W. (2017). Obesity, ectopic
UvA-DARE (Digital Academic Repository) Obesity, ectopic lipids, and insulin resistance ter Horst, K.W. Link to publication Citation for published version (APA): ter Horst, K. W. (2017). Obesity, ectopic
Renal tumors of adults
 Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
Genetics and Genomics in Endocrinology
 Genetics and Genomics in Endocrinology Dr. Peter Igaz MD MSc PhD 2 nd Department of Medicine Faculty of Medicine Semmelweis University Genetics-based endocrine diseases I. Monogenic diseases: Multiple
Genetics and Genomics in Endocrinology Dr. Peter Igaz MD MSc PhD 2 nd Department of Medicine Faculty of Medicine Semmelweis University Genetics-based endocrine diseases I. Monogenic diseases: Multiple
Use of the comprehensive geriatric assessment to improve patient-centred care in complex patient populations Parlevliet, J.L.
 UvA-DARE (Digital Academic Repository) Use of the comprehensive geriatric assessment to improve patient-centred care in complex patient populations Parlevliet, J.L. Link to publication Citation for published
UvA-DARE (Digital Academic Repository) Use of the comprehensive geriatric assessment to improve patient-centred care in complex patient populations Parlevliet, J.L. Link to publication Citation for published
Renal Cancer. By Jamie Calderwood
 Renal Cancer By Jamie Calderwood ("Kidney Cancer")*1 ("What are the different types of kidney mass?")*2 What is it? Renal cancer is more commonly known as kidney cancer. Wilms tumor Another name for kidney
Renal Cancer By Jamie Calderwood ("Kidney Cancer")*1 ("What are the different types of kidney mass?")*2 What is it? Renal cancer is more commonly known as kidney cancer. Wilms tumor Another name for kidney
Molecular understanding of tamoxifen resistance in breast cancer. Renée de Leeuw
 Molecular understanding of tamoxifen resistance in breast cancer Renée de Leeuw Omslag ontworpen door: Theophile Suijkerbuijk (www.theophile.nl) Molecular understanding of tamoxifen resistance in breast
Molecular understanding of tamoxifen resistance in breast cancer Renée de Leeuw Omslag ontworpen door: Theophile Suijkerbuijk (www.theophile.nl) Molecular understanding of tamoxifen resistance in breast
University of Groningen. Diabetes mellitus and rhegmatogenous retinal detachment Fokkens, Bernardina Teunisje
 University of Groningen Diabetes mellitus and rhegmatogenous retinal detachment Fokkens, Bernardina Teunisje IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen Diabetes mellitus and rhegmatogenous retinal detachment Fokkens, Bernardina Teunisje IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
Citation for published version (APA): van de Vijver, S. J. M. (2015). Cardiovascular disease prevention in the slums of Kenya
: van de Vijver, S. J. M. (2015). Cardiovascular disease prevention in the slums of Kenya") UvA-DARE (Digital Academic Repository) Cardiovascular disease prevention in the slums of Kenya van de Vijver, Steven Link to publication Citation for published version (APA): van de Vijver, S. J. M. (2015).
UvA-DARE (Digital Academic Repository) Cardiovascular disease prevention in the slums of Kenya van de Vijver, Steven Link to publication Citation for published version (APA): van de Vijver, S. J. M. (2015).
UvA-DARE (Digital Academic Repository) Anorectal malformations and hirschsprung disease Witvliet, M.J. Link to publication
 Anorectal malformations and hirschsprung disease Witvliet, M.J. Link to publication") UvA-DARE (Digital Academic Repository) Anorectal malformations and hirschsprung disease Witvliet, M.J. Link to publication Citation for published version (APA): Witvliet, M. J. (2017). Anorectal malformations
UvA-DARE (Digital Academic Repository) Anorectal malformations and hirschsprung disease Witvliet, M.J. Link to publication Citation for published version (APA): Witvliet, M. J. (2017). Anorectal malformations
Citation for published version (APA): van Es, N. (2017). Cancer and thrombosis: Improvements in strategies for prediction, diagnosis, and treatment
: van Es, N. (2017). Cancer and thrombosis: Improvements in strategies for prediction, diagnosis, and treatment") UvA-DARE (Digital Academic Repository) Cancer and thrombosis van Es, N. Link to publication Citation for published version (APA): van Es, N. (2017). Cancer and thrombosis: Improvements in strategies for
UvA-DARE (Digital Academic Repository) Cancer and thrombosis van Es, N. Link to publication Citation for published version (APA): van Es, N. (2017). Cancer and thrombosis: Improvements in strategies for
Lung Cysts, Spontaneous Pneumothorax, and Genetic Associations in 89 Families with Birt-Hogg-Dubé Syndrome
 Lung Cysts, Spontaneous, and Genetic Associations in 89 Families with Birt-Hogg-Dubé Syndrome Jorge R. Toro 1, Stephen E. Pautler 2, Laveta Stewart 1, Gladys M. Glenn 1, Michael Weinreich 1, Ousmane Toure
Lung Cysts, Spontaneous, and Genetic Associations in 89 Families with Birt-Hogg-Dubé Syndrome Jorge R. Toro 1, Stephen E. Pautler 2, Laveta Stewart 1, Gladys M. Glenn 1, Michael Weinreich 1, Ousmane Toure
10/11/2018. Clinical and Surgical Management of VHL-Related Cysts and Cystic RCC. Outline. VHL Renal Manifestations. VHL Renal Manifestations
 Outline Clinical and Surgical Management of VHL-Related Cysts and Cystic RCC Mark W. Ball, MD Assistant Research Physician Attending Surgeon Urologic Oncology Branch, National Cancer Institute Prevalence
Outline Clinical and Surgical Management of VHL-Related Cysts and Cystic RCC Mark W. Ball, MD Assistant Research Physician Attending Surgeon Urologic Oncology Branch, National Cancer Institute Prevalence
Complex case Presentations
 Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Citation for published version (APA): Donker, M. (2014). Improvements in locoregional treatment of breast cancer
: Donker, M. (2014). Improvements in locoregional treatment of breast cancer") UvA-DARE (Digital Academic Repository) Improvements in locoregional treatment of breast cancer Donker, Mila Link to publication Citation for published version (APA): Donker, M. (2014). Improvements in
UvA-DARE (Digital Academic Repository) Improvements in locoregional treatment of breast cancer Donker, Mila Link to publication Citation for published version (APA): Donker, M. (2014). Improvements in
University of Groningen. Symptomatic and asymptomatic airway hyperresponsiveness Jansen, Desiree
 University of Groningen Symptomatic and asymptomatic airway hyperresponsiveness Jansen, Desiree IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite
University of Groningen Symptomatic and asymptomatic airway hyperresponsiveness Jansen, Desiree IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite
Insulin sensitivity of hepatic glucose and lipid metabolism in animal models of hepatic steatosis Grefhorst, Aldo
 University of Groningen Insulin sensitivity of hepatic glucose and lipid metabolism in animal models of hepatic steatosis Grefhorst, Aldo IMPORTANT NOTE: You are advised to consult the publisher's version
University of Groningen Insulin sensitivity of hepatic glucose and lipid metabolism in animal models of hepatic steatosis Grefhorst, Aldo IMPORTANT NOTE: You are advised to consult the publisher's version
Regulatory enzymes of mitochondrial B-oxidation as targets for treatment of the metabolic syndrome Bijker-Schreurs, Marijke
 University of Groningen Regulatory enzymes of mitochondrial B-oxidation as targets for treatment of the metabolic syndrome Bijker-Schreurs, Marijke IMPORTANT NOTE: You are advised to consult the publisher's
University of Groningen Regulatory enzymes of mitochondrial B-oxidation as targets for treatment of the metabolic syndrome Bijker-Schreurs, Marijke IMPORTANT NOTE: You are advised to consult the publisher's
Kael V. Mikesell, 1 Afif N. Kulaylat, 2 Keri J. Donaldson, 1 Brian D. Saunders, 2 and Henry S. Crist Introduction. 2.
 Hindawi Publishing Corporation Volume 2014, Article ID 753694, 5 pages http://dx.doi.org/10.1155/2014/753694 Case Report A Rare Soft Tissue Tumor Masquerading as a Parathyroid Adenoma in a Patient with
Hindawi Publishing Corporation Volume 2014, Article ID 753694, 5 pages http://dx.doi.org/10.1155/2014/753694 Case Report A Rare Soft Tissue Tumor Masquerading as a Parathyroid Adenoma in a Patient with
Clinical History. 29 yo woman with polyhydramnios Cardiac mass at fetal ultrasound At 35 weeks, newborn died 30 minutes after delivery
 CASE 1 a Clinical History 29 yo woman with polyhydramnios Cardiac mass at fetal ultrasound At 35 weeks, newborn died 30 minutes after delivery Interface between tumor and normal myocardium Smaller well-demarcated
CASE 1 a Clinical History 29 yo woman with polyhydramnios Cardiac mass at fetal ultrasound At 35 weeks, newborn died 30 minutes after delivery Interface between tumor and normal myocardium Smaller well-demarcated
Citation for published version (APA): Tjon-Kon-Fat, R. I. (2017). Unexplained subfertility: Illuminating the path to treatment.
: Tjon-Kon-Fat, R. I. (2017). Unexplained subfertility: Illuminating the path to treatment.") UvA-DARE (Digital Academic Repository) Unexplained subfertility Tjon-Kon-Fat, R.I. Link to publication Citation for published version (APA): Tjon-Kon-Fat, R. I. (2017). Unexplained subfertility: Illuminating
UvA-DARE (Digital Academic Repository) Unexplained subfertility Tjon-Kon-Fat, R.I. Link to publication Citation for published version (APA): Tjon-Kon-Fat, R. I. (2017). Unexplained subfertility: Illuminating
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/38594 holds various files of this Leiden University dissertation Author: Haan, Melina C. den Title: Cell therapy in ischemic heart disease models : role
Cover Page The handle http://hdl.handle.net/1887/38594 holds various files of this Leiden University dissertation Author: Haan, Melina C. den Title: Cell therapy in ischemic heart disease models : role
SCIENCE & TECHNOLOGY
 Pertanika J. Sci. & Technol. 24 (1): 225-230 (2016) SCIENCE & TECHNOLOGY Journal homepage: http://www.pertanika.upm.edu.my/ Case Study Parotid Oncocytoma in Birt-Hogg-Dubé Syndrome: A New Pitfall in 18
Pertanika J. Sci. & Technol. 24 (1): 225-230 (2016) SCIENCE & TECHNOLOGY Journal homepage: http://www.pertanika.upm.edu.my/ Case Study Parotid Oncocytoma in Birt-Hogg-Dubé Syndrome: A New Pitfall in 18
Endocrine Surgery. Characteristics of the Germline MEN1 Mutations in Korea: A Literature Review ORIGINAL ARTICLE. The Korean Journal of INTRODUCTION
 ORIGINAL ARTICLE ISSN 1598-1703 (Print) ISSN 2287-6782 (Online) Korean J Endocrine Surg 2014;14:7-11 The Korean Journal of Endocrine Surgery Characteristics of the Germline MEN1 Mutations in Korea: A Literature
ORIGINAL ARTICLE ISSN 1598-1703 (Print) ISSN 2287-6782 (Online) Korean J Endocrine Surg 2014;14:7-11 The Korean Journal of Endocrine Surgery Characteristics of the Germline MEN1 Mutations in Korea: A Literature
UvA-DARE (Digital Academic Repository) Hip and groin pain in athletes Tak, I.J.R. Link to publication
 Hip and groin pain in athletes Tak, I.J.R. Link to publication") UvA-DARE (Digital Academic Repository) Hip and groin pain in athletes Tak, I.J.R. Link to publication Citation for published version (APA): Tak, I. J. R. (2017). Hip and groin pain in athletes: Morphology,
UvA-DARE (Digital Academic Repository) Hip and groin pain in athletes Tak, I.J.R. Link to publication Citation for published version (APA): Tak, I. J. R. (2017). Hip and groin pain in athletes: Morphology,
Citation for published version (APA): Wolff, D. (2016). The Enigma of the Fontan circulation [Groningen]: Rijksuniversiteit Groningen
![Citation for published version (APA): Wolff, D. (2016). The Enigma of the Fontan circulation [Groningen]: Rijksuniversiteit Groningen](/thumbs/88/115374835.jpg "Citation for published version (APA): Wolff, D. (2016). The Enigma of the Fontan circulation [Groningen]: Rijksuniversiteit Groningen") University of Groningen The Enigma of the Fontan circulation Wolff, Djoeke IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
University of Groningen The Enigma of the Fontan circulation Wolff, Djoeke IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check
Citation for published version (APA): Owusu, E. D. A. (2018). Malaria, HIV and sickle cell disease in Ghana: Towards tailor-made interventions
: Owusu, E. D. A. (2018). Malaria, HIV and sickle cell disease in Ghana: Towards tailor-made interventions") UvA-DARE (Digital Academic Repository) Malaria, HIV and sickle cell disease in Ghana Owusu, E.D.A. Link to publication Citation for published version (APA): Owusu, E. D. A. (2018). Malaria, HIV and sickle
UvA-DARE (Digital Academic Repository) Malaria, HIV and sickle cell disease in Ghana Owusu, E.D.A. Link to publication Citation for published version (APA): Owusu, E. D. A. (2018). Malaria, HIV and sickle
The role of media entertainment in children s and adolescents ADHD-related behaviors: A reason for concern? Nikkelen, S.W.C.
 UvA-DARE (Digital Academic Repository) The role of media entertainment in children s and adolescents ADHD-related behaviors: A reason for concern? Nikkelen, S.W.C. Link to publication Citation for published
UvA-DARE (Digital Academic Repository) The role of media entertainment in children s and adolescents ADHD-related behaviors: A reason for concern? Nikkelen, S.W.C. Link to publication Citation for published
Apoptosis in (pre-) malignant lesions in the gastro-intestinal tract Woude, Christien Janneke van der
 malignant lesions in the gastro-intestinal tract Woude, Christien Janneke van der") University of Groningen Apoptosis in (pre-) malignant lesions in the gastro-intestinal tract Woude, Christien Janneke van der IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
University of Groningen Apoptosis in (pre-) malignant lesions in the gastro-intestinal tract Woude, Christien Janneke van der IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
Citation for published version (APA): Brinkman, J. W. (2007). Albuminuria as a laboratory risk marker: Methods evaluated s.n.
: Brinkman, J. W. (2007). Albuminuria as a laboratory risk marker: Methods evaluated s.n.") University of Groningen Albuminuria as a laboratory risk marker Brinkman, Jacoline Willijanne IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from
University of Groningen Albuminuria as a laboratory risk marker Brinkman, Jacoline Willijanne IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from
Genetic Risk Assessment for Cancer
 Genetic Risk Assessment for Cancer Jennifer Siettmann, MS CGC Certified Genetic Counselor Banner MD Anderson Cancer Center Objectives Describe the role of genetic counseling and genetic testing in patient
Genetic Risk Assessment for Cancer Jennifer Siettmann, MS CGC Certified Genetic Counselor Banner MD Anderson Cancer Center Objectives Describe the role of genetic counseling and genetic testing in patient
Molecular and mechanical functions of the intermediate filament protein GFAP Stassen, O.M.J.A.
 UvA-DARE (Digital Academic Repository) Molecular and mechanical functions of the intermediate filament protein GFAP Stassen, O.M.J.A. Link to publication Citation for published version (APA): Stassen,
UvA-DARE (Digital Academic Repository) Molecular and mechanical functions of the intermediate filament protein GFAP Stassen, O.M.J.A. Link to publication Citation for published version (APA): Stassen,
Cystic lung diseases 7/21/2017. Cystic Lung Diseases. CT definition of a lung cyst. Important clinical clues
 Cystic Lung Diseases Cystic lung diseases Aurelie Fabre Increased Awareness Spontaneous Pneumothorax High resolution imaging (HRCT) Multidisciplinary approach like interstitial lung disease CT definition
Cystic Lung Diseases Cystic lung diseases Aurelie Fabre Increased Awareness Spontaneous Pneumothorax High resolution imaging (HRCT) Multidisciplinary approach like interstitial lung disease CT definition
Pathology perspective of colonic polyposis syndromes
 Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Expert Interview: Inherited Susceptibility to Cancer with Dr. Nicoleta Voian
 Expert Interview: Inherited Susceptibility to Cancer with Dr. Nicoleta Voian ANNOUNCER OPEN: Welcome to CME on ReachMD. This segment, entitled Inherited Susceptibility to Cancer: What Do Primary Care Providers
Expert Interview: Inherited Susceptibility to Cancer with Dr. Nicoleta Voian ANNOUNCER OPEN: Welcome to CME on ReachMD. This segment, entitled Inherited Susceptibility to Cancer: What Do Primary Care Providers
Percutaneous coronary intervention in acute myocardial infarction: from procedural considerations to long term outcomes Delewi, R.
 UvA-DARE (Digital Academic Repository) Percutaneous coronary intervention in acute myocardial infarction: from procedural considerations to long term outcomes Delewi, R. Link to publication Citation for
UvA-DARE (Digital Academic Repository) Percutaneous coronary intervention in acute myocardial infarction: from procedural considerations to long term outcomes Delewi, R. Link to publication Citation for
CANCER GENETICS PROVIDER SURVEY
 Dear Participant, Previously you agreed to participate in an evaluation of an education program we developed for primary care providers on the topic of cancer genetics. This is an IRB-approved, CDCfunded
Dear Participant, Previously you agreed to participate in an evaluation of an education program we developed for primary care providers on the topic of cancer genetics. This is an IRB-approved, CDCfunded
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38506 holds various files of this Leiden University dissertation. Author: Nies, Jessica Annemarie Bernadette van Title: Early identification of rheumatoid
Cover Page The handle http://hdl.handle.net/1887/38506 holds various files of this Leiden University dissertation. Author: Nies, Jessica Annemarie Bernadette van Title: Early identification of rheumatoid
Multimodality Imaging of Anatomy and Function in Coronary Artery Disease. Joanne D. Schuijf
 Multimodality Imaging of Anatomy and Function in Coronary Artery Disease Joanne D. Schuijf The research described in this thesis was performed at the departments of Cardiology and Radiology of the Leiden
Multimodality Imaging of Anatomy and Function in Coronary Artery Disease Joanne D. Schuijf The research described in this thesis was performed at the departments of Cardiology and Radiology of the Leiden