Complex case Presentations
|
|
|
- Lionel Sharp
- 5 years ago
- Views:
Transcription
1
2 Complex case Presentations
3 Case Presentations April 2016 Lisa M Pickering

4 Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical nephrectomy Chromophobe renal cell carcinoma Sarcomatoid features G2 pt3an0m0 Leibovich score: 6 Adjuvant SORCE trial: (sorafenib 1 or 3 years v placebo)

5 Case presentations: chromophobe renal carcinoma One year later August 2010: Routine CT Retroperitoneal lymph node relapse Hb 109 g/l, Alb 27 g/l
6 Case presentations: chromophobe renal carcinoma One year later August 2010: Routine CT Retroperitoneal lymph node relapse Hb 109 g/l, Alb 27 g/l Resected 6/11 retroperitoneal LN positive for chromphobe RCC. No extracapsular spread Taken off trial SHOULD HE HAVE ANY FURTHER THERAPY? 1. Pazopanib 2. Sunitinib 3. Different systemic therapy 4. Radiotherapy 5. Surveillance
7 Panel discussion
8 Case presentations: chromophobe renal carcinoma One year later August 2010: Routine CT Retroperitoneal lymph node relapse Hb 109 g/l, Alb 27 g/l Resected 6/11 retroperitoneal LN positive for chromphobe RCC. No extracapsular spread Taken off trial WE CHOSE: 1. Pazopanib 2. Sunitinib 3. Different systemic therapy 4. Radiotherapy 5. Surveillance
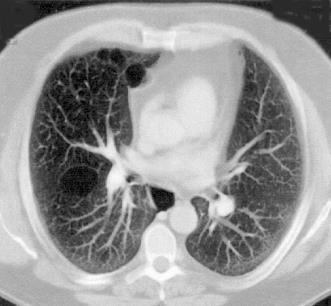
9 Case presentations: chromophobe renal carcinoma Four years later (March 2014) Six months after previous CT scan Symptomatic dysphagia Mediastinal lymph node relapse Note: Four years to relapse despite apparent high risk features
10 Case presentations: chromophobe renal carcinoma Four years later (March 2014) Six months after previous CT scan Symptomatic dysphagia Mediastinal lymph node relapse Note: Four years to relapse despite apparent high risk features MANAGEMENT OPTIONS 1. Pazopanib 2. Sunitinib 3. Radiotherapy 4. Resection 5. Surveillance

11 Panel discussion Resectable Arguments to reseque?
12 Case presentations: chromophobe renal carcinoma Four years later (March 2014) Six months after previous CT scan Symptomatic dysphagia Mediastinal lymph node relapse Note: Four years to relapse despite apparent high risk features WE CHOSE: 1. Pazopanib 2. Sunitinib 3. Radiotherapy 4. Resection (Renal cell carcinoma) 5. Surveillance
13 Case presentations: chromophobe renal carcinoma 6 weeks later (May 2014) First surveillance scan after surgery No recurrence Does he need any further therapy? POSSIBLE OPTIONS 1. Pazopanib 2. Sunitinib 3. Other systemic therapy 4. Radiotherapy 5. Surveillance
14 Panel discussion
15 Case presentations: chromophobe renal carcinoma 6 weeks later (May 2014) First surveillance scan after surgery No recurrence Does he need any further therapy? WE CHOSE: 1. Pazopanib 2. Sunitinib 3. Other systemic therapy 4. Radiotherapy 5. Surveillance
16 Case presentations: chromophobe renal carcinoma Another 6 weeks later (July 2014) Dysphagia++ Repeat CT scan Mediastinal lymph node recurrence No other sites of disease
17 Case presentations: chromophobe renal carcinoma Another 6 weeks later (July 2014) Dysphagia++ Repeat CT scan Mediastinal lymph node recurrence No other sites of disease MANAGEMENT OPTIONS 1. Pazopanib 2. Sunitinib 3. Other systemic therapy 4. Radiotherapy 5. Re-resection
18 Panel discussion
19 Case presentations: chromophobe renal carcinoma Another 6 weeks later (July 2014) Dysphagia++ Repeat CT scan Mediastinal lymph node recurrence No other sites of disease WE CHOSE: 1. Pazopanib 2. Sunitinib 3. Other systemic therapy 4. Radiotherapy 5. Re-resection
20 Case presentations: chromophobe renal carcinoma 12 weeks later (October 2014) Clinically improved Repeat CT scan Mediastinal lymph node reduction
21 Case presentations: chromophobe renal carcinoma January 2015 Sunitinib 50mg 4 / 2 Ongoing symptomatic benefit Radiological: incremental response Toxicities from treatment: supportive measures insitgated POSSIBLE MANAGEMENT STRATEGIES 1. Dose reduction 2. Schedule alteration 3. Change to pazopanib 4. Change to axitinib 5. Surgery 6. Radiotherapy 7. Treatment interruption
22 Panel discussion
23 Case presentations: chromophobe renal carcinoma January 2015 Sunitinib 50mg 4 / 2 Ongoing symptomatic benefit Radiological: incremental response Toxicities from treatment: supportive measures insitgated WE CHOSE: 1. Dose reduction 2. Schedule alteration 3. Change to pazopanib 4. Change to axitinib 5. Surgery 6. Radiotherapy 7. Treatment interruption

24 Case presentations: chromophobe renal carcinoma By September 2015 Further clinically improvement Complete resolution of disease and no new sites Ongoing toxicities on 37.5mg 2/1
25 Case presentations: chromophobe renal carcinoma By September 2015 Further clinically improvement Complete resolution of disease and no new sites Ongoing toxicities on 37.5mg 2/1 OPTIONS 1. Dose reduction 2. Schedule alteration 3. Change to pazopanib 4. Change to axitinib 5. Surgery 6. Radiotherapy 7. Treatment interruption
26 Panel discussion
27 Case presentations: chromophobe renal carcinoma By September 2015 Further clinically improvement Complete resolution of disease and no new sites Ongoing toxicities on 37.5mg 2/1 OPTIONS 1. Dose reduction 2. Schedule alteration 3. Change to pazopanib 4. Change to axitinib 5. Surgery 6. Radiotherapy 7. Treatment interruption
28 STAR Trial, UK CLRN Ph II/III RCT Controlled-trials.com ISRCTN mrcc N = 1000 Clear cell predominant First line ECOG PS 0/1c R A N D O M I S E Sunitinib or Pazopanib Conventional Schedule Sunitinib or Pazopanib Interrupted Schedule 1 Endpoint: PFS 2 Endpoints: OS, ORR, duration of response, safety, QoL
29 Complex Case Discussion Axel Bex The Netherlands Cancer Institute Division of Surgical Oncology Urology Amsterdam, The Netherlands

 ct1a cn0 left kidney 2.9 cm R.E.N.A.L. complexity score 5 (low)")
30 Male, 64 years Previous history : DVT due to factor V Leiden disease 07/ 2008 Bilateral renal tumours considered sporadic given his age of 56 years at diagnosis and absent family history ct1b cn0 cm0 right kidney 4.5 cm located in mid to lower pole in the hilar area R.E.N.A.L. complexity score 8 (medium) ct1a cn0 left kidney 2.9 cm R.E.N.A.L. complexity score 5 (low)
31 Panel discussion Idea on diagnosis Biopsy? Which side to start with?
 after biopsy of the left kidney pt1b pn0 cm0 clear-cell RCC Fuhrman grade 3 right kidney, margin microscopically positive Biopsy left kidney clear-cell RCC Fuhrman")
32 08/ 2008 after multidisciplinary tumour board Open partial nephrectomy right kidney with trial-based sentinel node and locoregional lymph node dissection and radiofrequency ablation (RFA) after biopsy of the left kidney pt1b pn0 cm0 clear-cell RCC Fuhrman grade 3 right kidney, margin microscopically positive Biopsy left kidney clear-cell RCC Fuhrman grade 3
33 10/ months after surgery Metachronous solitary lung metastasis and mediastinal lymph node ipsilateral pulmonary artery LN station 10
34 Panel discussion Need for biopsy? Surgery? Medical treatment?


35 10/ months after surgery Metachronous solitary lung metastasis and mediastinal lymph node ipsilateral pulmonary artery LN station 10 12/2010: metastasectomy of a 1.2 cm solitary clear-cell metastasis and hilar lymph node dissection with a single lymph node metastasis
36 01/ months after initial surgery 24 months after metastasectomy Suspected bilateral recurrence
37 Panel discussion Need for biopsy? Surgery? Medical treatment?
38 01/ months after initial surgery 24 months after metastasectomy Suspected bilateral recurrence Multidisciplinary decision to perform repartial nephrectomy on the right kidney and a percutaneous RFA left 03/2013: partial nephrectomy right kidney for a clear-cell recurrence, Fuhrman grade 2, margin positive!
39 Panel discussion What to do? Nephrectomy right kidney and RFA left kidney in a previously metastatic patient with high-risk of progression? Bilateral RFA?
40 Multidisciplinary tumour board What to do? Nephrectomy right kidney and RFA left kidney in a previously metastatic patient with high-risk of progression? Bilateral RFA? bilateral RFA
 for a 6 mm clear-cell")
41 08/ months after previous (first) metastasectomy 23 months after RFA for local recurrences 0.8 cm new pulmonary lesion 10/2015: video assisted thoracoscopic metastasectomy (VATS) for a 6 mm clear-cell metastasis




42 01/2016 gross hematuria after exercise Multifocal contrast enhancing lesions in the rght renal pelvis, ureter and in the bladder at the orifice 02/2016 TUR-B and attempted ureterorenoscopy: clear-cell RCC
43 Next options? Locoregional recurrence 27 months after RFA for a previous local recurrence but only 5 months after last metastasectomy for distant disease CT chest and abdomen 04/2016: no evidence of further systemic disease. Serum creatinine 108 µmol/l, GFR (MDRD-4) 60 ml/min/1.7 Consider rapid progression and start systemic therapy? Nephroureterectomy for local control and delay of systemic therapy?
44 Panel discussion Please help Dr Bex.
45 Case Presentations April 2016 B Rini
46 RCC in a Solitary Kidney 60 year-old-man, ECOG 0 Congenital solitary left kidney PMH: Hypertension, controlled with medication to 130/85 mmhg; no other PMH Dec. 2009: 2 month history of painless hematuria 5 kg weight loss in the past month




47 RCC in a Solitary Kidney Abd-US: hypoechoic area (4 x 3 x 3.2 cm) within the left kidney CT-Scan: Abd: diffuse infiltrative mass (5 cm) involving the upper pole of the left kidney; renal vein thrombus, perinephric lymph nodes; Thorax: bilateral indeterminate 2-5 mm pulmonary nodules
48 Panel discussion 1) partial nephrectomy 2) kidney biopsy to confirm clear cell RCC, then neoadjuvant VEGFR TKI 3) radical nephrectomy + hemodialysis
49 RCC in a Solitary Kidney Renal biopsy -> clear cell carcinoma, Fuhrman grade 2/4 (March - July 2010) phase II clinical trial with sunitinib (Jul 10): PR with 30% volume reduction. No lung changes. (Jul 10): Surgery: Partial left nephrectomy + vein thrombectomy Pathology: clear cell histology, grade 2/4, pt3, neg. margins Post-Op complications: ARF + fluid overload (No HD required); ARF resolved

50 RCC in a Solitary Kidney Follow up 6 months (Jan 11) CT: 1.7 cm non-occlusive thrombus Left RV. Lung nodules stable
51 Panel discussion 1) thrombectomy 2) restart sunitinib 3) radical nephrectomy + hemodialysis


52 RCC in a Solitary Kidney (Mar 11) Surgery: tumor thrombus resection + RV replacement with tubularized pericardial graft (Jul 11) CT: Renal hilar, pelvis, RV and soft tissue infiltration with tumor recurrence. No disease elsewhere. No viable resection possible
: Stable Disease.")

53 RCC in a Solitary Kidney (Jul 11) Sunitinib 50mg PO (4/2 schedule) with mild treatment-related skin toxicity. (Dec 11): Stable Disease. Sunitinib alteration to 2/1 schedule due to grade 2-3 HFS. Hypertension medication adjustment. (June 14) Locoregional PD with Post-renal failure due to left ureteric obstruction Percutaneous nephrostomy tube placed.
54 Panel discussion 1) Switch to axitinib 2) radical nephrectomy + hemodialysis 3) Other
 Last Visit Clinically well. ECOG 0-1 CT Scan: stable disease.")
55 RCC in a Solitary Kidney (June 14) STOP Sunitinib. Start Axitinib 5 mg bid. (August 14) Last Visit Clinically well. ECOG 0-1 CT Scan: stable disease.
56 RCC in a Solitary Kidney June 14: Axitinib 5mg BID -> 6mg BID; well tolerated with initial regression. Oct 15: Pt with progression in kidney causing renal failure requiring dialysis. Only gross disease is in solitary remaining kidney
57 Panel discussion 1) Radical nephrectomy NED/dialysis 2) Change systemic therapy to nivolumab

58 RCC in a Solitary Kidney 11/24/2015: Left open radical nephrectomy, removal left JJ ureteral stent, RPLND pathology revealed 11cm clear cell renal cell carcinoma, grade 3/4, pt3an0mx with negative margins, two lymph nodes were negative. April 2016
59 Panel discussion Please help Dr Rini.
60 Case Presentations April 2016 JJ Patard

61 Case presentation: bilateral and multifocal renal tumors 56 yrs old man No personal medical past history No familial kidney disease past history Incidental diagnosis of bilateral renal tumors Normal chest CT scan

62 Case presentation: bilateral and multifocal renal tumors 1 large hyper vascular hilar tumor in the right kidney RENAL score 11p At least 2 tumors in the left kidney RENAL Score 6 a Serum creatinin: 0.80 mg/dl MDRD GFR: 100 ml/min
63 Panel discussion Clear cell RCC? Oncocytoma? Papillary RCC? Chromophobe carcinoma? Other?
64 Panel discussion Role of biopsy? Is it reliable in case of multiple tumors? Will it change surgical strategy? Once surgery is decided, what to do? Double left partial nephrectomy first? Right partial nephrectomy first? Right radical nephrectomy first?
65 Case presentation: bilateral and multifocal renal tumors In the real life, the patient underwent a left renal biopsy six month earlier Result: Oncocytoma, an expectant follow-up had been advised The tumors have grown and the patient is asking for a second medical opinion Question to the panel: is the previous diagnosis of oncocytoma going to change your surgical management?
66 bilateral and multifocal renal tumors, practical management We started by left partial nephrectomy There were indeed 5 renal tumors ++ All the tumors were excised with negative margins WIT: 25 minutes No significant post op morbidity Serum creatinine at discharge: 0.95 mg/dl (MDRD GFR: 82 ml/min) Panel discussion; the limits of pre op imaging in case of multiple small renal tumors





67 bilateral and multifocal renal tumors, histological results left side Tumor 1 Tumor 2 Tumor 3 Tumor 4 Final Histological pathology (Pr N Rioux Leclercq): hybrid tumor (oncocytoma + chromophobe carcinoma) Question to the panel: will it change your mind for right side management?
68 bilateral and multifocal renal tumors, right side management We decided a partial nephrectomy WIT 30 minutes Estimated Blood loss: 800 ml Non intra operative complications Day 1 Gross haematuria Malaise, tachycardia, Hb: 7 g/dl Peri renal drainage > 400 ml Questions to the panel: Immediate re operation for surgical haemostasis? Immediate total nephrectomy? CT +- embolization? Blood transfusion and expectant management?

69 bilateral and multifocal renal tumors, panel discussion: BHD syndrome
70 bilateral and multifocal renal tumors, panel discussion: BHD syndrome Oncocytic hybrid tumors 50% chromophobe RCCs 34% Clear cell RCCs 9% Oncocytomas 5% Papillary RCCs 2%
71
Presentation of Cases /Audience Voting/Panel/Discussion
 Presentation of Cases /Audience Voting/Panel/Discussion JJ Patard Tim O Brien Ninth European International Kidney Cancer Symposium Dublin 25-26 April 2014 Clinical case 1 63 years old women Medical past
Presentation of Cases /Audience Voting/Panel/Discussion JJ Patard Tim O Brien Ninth European International Kidney Cancer Symposium Dublin 25-26 April 2014 Clinical case 1 63 years old women Medical past
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
GUIDELINES ON RENAL CELL CARCINOMA
 GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
Guidelines on Renal Cell
 Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Renal Cell Cancer. Clinical case study 1 & 2. Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland
 Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Manchester Cancer. Guidelines for the management of renal cancer
 Guidelines for the management of renal cancer Approved by the urology pathway board September 2014 To be reviewed September 2016 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Guidelines for the management of renal cancer Approved by the urology pathway board September 2014 To be reviewed September 2016 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management
: Diagnosis and Management") RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
SBRT for lung metastases: Case report
 SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
NEPHRECTOMY AUDIT. OCTOBER 1998-SEPTEMBER 2005 Dr. Sanjeev Bandi MBBS., FRCSI., FRACS(Urology) Mater Misericordiae Hospital, Mackay, Qld 4740
 Mater Misericordiae Hospital, Mackay, Qld 4740") NEPHRECTOMY AUDIT OCTOBER 1998-SEPTEMBER 2005 Dr. Sanjeev Bandi MBBS., FRCSI., FRACS(Urology) Mater Misericordiae Hospital, Mackay, Qld 4740 This audit has been performed in conjunction with the data requirements
NEPHRECTOMY AUDIT OCTOBER 1998-SEPTEMBER 2005 Dr. Sanjeev Bandi MBBS., FRCSI., FRACS(Urology) Mater Misericordiae Hospital, Mackay, Qld 4740 This audit has been performed in conjunction with the data requirements
Indications For Partial
 Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Tratamiento adyuvante y neoadyuvante del cáncer renal en Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet.
 Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Vincenzo Ficarra 1,2,3. Associate Editor BJU International
 Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
EAU GUIDELINES ON RENAL CELL CARCINOMA
 EAU GUIDELINES ON RENAL ELL ARINOMA (Limited text update March 2016) B. Ljungberg (hair), K. Bensalah, A. Bex (Vice-chair), S. anfield, R.H. Giles (Patient Organisation Representative), M. Hora, M.A. Kuczyk,
EAU GUIDELINES ON RENAL ELL ARINOMA (Limited text update March 2016) B. Ljungberg (hair), K. Bensalah, A. Bex (Vice-chair), S. anfield, R.H. Giles (Patient Organisation Representative), M. Hora, M.A. Kuczyk,
Medical Management of Renal Cell Carcinoma
 Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
RENAL CANCER GUIDELINES
 Greater Manchester and Cheshire Cancer Network RENAL CANCER GUIDELINES Agreed by Urology CSG: July 2010 Review Date: July 2012 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Greater Manchester and Cheshire Cancer Network RENAL CANCER GUIDELINES Agreed by Urology CSG: July 2010 Review Date: July 2012 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Cabozantinib for untreated locally advanced or metastatic renal cell carcinoma Final scope Remit/appraisal objective To appraise
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Cabozantinib for untreated locally advanced or metastatic renal cell carcinoma Final scope Remit/appraisal objective To appraise
Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma
 ONCOLOGY LETTERS 9: 125-130, 2015 Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma KEIICHI ITO 1, KENJI SEGUCHI 1, HIDEYUKI SHIMAZAKI 2, EIJI TAKAHASHI
ONCOLOGY LETTERS 9: 125-130, 2015 Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma KEIICHI ITO 1, KENJI SEGUCHI 1, HIDEYUKI SHIMAZAKI 2, EIJI TAKAHASHI
Clinical/Surgical trials that will change my practice
 Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 18 CBULP 2011 041 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 18 CBULP 2011 041 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
GUIDELINES ON RENAL CELL CANCER
 20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO
 REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer
 Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Case(s): How to Deal with Mixed Response Giuseppe Procopio
: How to Deal with Mixed Response Giuseppe Procopio") Case(s): How to Deal with Mixed Response Giuseppe Procopio Fondazione IRCCS Istituto Nazionale dei Tumori, Milano Disclosures Advisory: Astellas, Bayer, GSK Consultant: Pfizer, Novartis Background Mixed
Case(s): How to Deal with Mixed Response Giuseppe Procopio Fondazione IRCCS Istituto Nazionale dei Tumori, Milano Disclosures Advisory: Astellas, Bayer, GSK Consultant: Pfizer, Novartis Background Mixed
Role and extension of lymph node dissection in kidney, bladder and prostate cancer. Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017
 Moderator: Dr A. Noujem 30 th March 2017") Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
I Kid(ney) You Not: Updates on Renal Cell Carcinoma
 You Not: Updates on Renal Cell Carcinoma") Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Recent Developments in Research on Kidney Cancer: Highlights from Urological and Oncological Congresses in 2007
 european urology supplements 7 (2008) 494 507 available at www.sciencedirect.com journal homepage: www.europeanurology.com Recent Developments in Research on Kidney Cancer: Highlights from Urological and
european urology supplements 7 (2008) 494 507 available at www.sciencedirect.com journal homepage: www.europeanurology.com Recent Developments in Research on Kidney Cancer: Highlights from Urological and
Small Renal Mass Guidelines. Clif Vestal, MD USMD Arlington, Texas
 Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
Lymphadenectomy in RCC: Yes, No, Clinical Trial?
 Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
David N. Robinson, MD
 David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Atezolizumab Adjuvant Study: Medical Oncologist Perspective. Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center
 Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
Reference No: Author(s) Approval date: June Committee. Operational Date: July Review:
 Approval date: June Committee. Operational Date: July Review:") Reference No: Title: Author(s) Systemic anti-cancer therapy (SACT) guidelines for renal cell cancer Dr Alison Clayton Consultant Medical Oncologist & Dr Jane Hurwitz Consultant Medical Oncologist, Cancer
Reference No: Title: Author(s) Systemic anti-cancer therapy (SACT) guidelines for renal cell cancer Dr Alison Clayton Consultant Medical Oncologist & Dr Jane Hurwitz Consultant Medical Oncologist, Cancer
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
CASE REPORT. Introduction. Case series reports. J Thorac Dis 2012;4(S1): DOI: /j.issn s003
: DOI: /j.issn s003") CASE REPORT Lost in time pulmonary metastases of renal cell carcinoma: complete surgical resection of metachronous metastases, 18 and 15 years after nephrectomy Kosmas Tsakiridis 1, Aikaterini N Visouli
CASE REPORT Lost in time pulmonary metastases of renal cell carcinoma: complete surgical resection of metachronous metastases, 18 and 15 years after nephrectomy Kosmas Tsakiridis 1, Aikaterini N Visouli
Surgical Management of Renal Cancer. David Nicol Consultant Urologist
 Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5)
") SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
St. Dominic s Annual Cancer Report Outcomes
 St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense?
 Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
John Fitzpatrick Memorial Lecture. John Fitzpatrick Memorial lecture
 John Fitzpatrick Memorial Lecture John Fitzpatrick Memorial Lecture John M Fitzpatrick, 1948 2014 Head of Research at the Irish Cancer Society Professor of Surgery and Consultant Urologist at the Mater
John Fitzpatrick Memorial Lecture John Fitzpatrick Memorial Lecture John M Fitzpatrick, 1948 2014 Head of Research at the Irish Cancer Society Professor of Surgery and Consultant Urologist at the Mater
Salvage surgery after energy ablation for renal masses
 Salvage surgery after energy ablation for renal masses Jose A. Karam, Christopher G. Wood, Zachary R. Compton, Priya Rao*, Raghunandan Vikram, Kamran Ahrar and Surena F. Matin Departments of Urology, *Pathology,
Salvage surgery after energy ablation for renal masses Jose A. Karam, Christopher G. Wood, Zachary R. Compton, Priya Rao*, Raghunandan Vikram, Kamran Ahrar and Surena F. Matin Departments of Urology, *Pathology,
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Renal Parenchymal Neoplasms
 Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Challenges in RCC surgery. Treatment Goals. Surgical challenges. Management options in VHL associated RCCs
 Management options in VHL associated RCCs Challenges in RCC surgery JJ PATARD, MD, PhD Paris XI University Observation, Radical nephrectomy, Renal parenchymal sparing surgery, Open, laparoscopic, robotic
Management options in VHL associated RCCs Challenges in RCC surgery JJ PATARD, MD, PhD Paris XI University Observation, Radical nephrectomy, Renal parenchymal sparing surgery, Open, laparoscopic, robotic
Patient Selection for Surgery in RCC with Thrombus. E. Jason Abel, M.D.
 Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Is renal cryoablation becoming an effective alternative to partial nephrectomy?
 Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
AUA Guidelines Renal Mass and Localized Kidney Cancer
 AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic
 Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic renal cell carcinoma Wassim Kassouf, Leonardo L. Monteiro, Darrel E. Drachenberg, Adrian S. Fairey,
Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic renal cell carcinoma Wassim Kassouf, Leonardo L. Monteiro, Darrel E. Drachenberg, Adrian S. Fairey,
The Incidental Renal Mass in the Primary Care Setting
 The Incidental Renal Mass in the Primary Care Setting Adele M. Caruso, MSN, CRNP Adult Nurse Practitioner The Perelman School of Medicine at the University of Pennsylvania Abstract There are approximately
The Incidental Renal Mass in the Primary Care Setting Adele M. Caruso, MSN, CRNP Adult Nurse Practitioner The Perelman School of Medicine at the University of Pennsylvania Abstract There are approximately
Renal and ureteral involvement in Erdheim-Chester disease: analysis of a single centre cohort
 Renal and ureteral involvement in Erdheim-Chester disease: analysis of a single centre cohort Gaia Manari, Davide Gianfreda, Andrea Posteraro, Alessandro A. Palumbo and Augusto Vaglio Nephrology Unit and
Renal and ureteral involvement in Erdheim-Chester disease: analysis of a single centre cohort Gaia Manari, Davide Gianfreda, Andrea Posteraro, Alessandro A. Palumbo and Augusto Vaglio Nephrology Unit and
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
INTEGRATION OF SURGERY AND SYSTEMIC THERAPY FOR ADVANCED RENAL CELL CARCINOMA IN THE TARGETED THERAPY ERA
 INTEGRATION OF SURGERY AND SYSTEMIC THERAPY FOR ADVANCED RENAL CELL CARCINOMA IN THE TARGETED THERAPY ERA Dr. Michael J. Metcalfe PGY-4 Department of Urologic Sciences University of British Columbia October
INTEGRATION OF SURGERY AND SYSTEMIC THERAPY FOR ADVANCED RENAL CELL CARCINOMA IN THE TARGETED THERAPY ERA Dr. Michael J. Metcalfe PGY-4 Department of Urologic Sciences University of British Columbia October
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
What is the role of partial nephrectomy in the context of active surveillance and renal ablation?
 What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients
 Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Management of Locally Reccurent Renal Cell Carcinoma. Jose A. Karam, MD, FACS Assistant Professor Department of Urology
 Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
UnusalPresentationofMetastasisfromaRenalCellCarcinoma-A CaseReportwithReviewofLiterature
 Global Journal of Medical Research: K Interdisciplinary Volume 18 Issue 8 Version 1.0 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Online ISSN: 2249-4618 &
Global Journal of Medical Research: K Interdisciplinary Volume 18 Issue 8 Version 1.0 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Online ISSN: 2249-4618 &
Patient Reported Weight Loss Predicts Recurrence Rate in Renal Cell Cancer Cases after Nephrectomy
 DOI:10.22034/APJCP.2018.19.4.891 RESEARCH ARTICLE Editorial Process: Submission:01/04/2017 Acceptance:09/11/2017 Patient Reported Weight Loss Predicts Recurrence Rate in Renal Cell Cancer Cases after Nephrectomy
DOI:10.22034/APJCP.2018.19.4.891 RESEARCH ARTICLE Editorial Process: Submission:01/04/2017 Acceptance:09/11/2017 Patient Reported Weight Loss Predicts Recurrence Rate in Renal Cell Cancer Cases after Nephrectomy
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Kidney Cancer Session
 New Frontiers in Urologic Oncology September 12 th, 2015 Kidney Cancer Session Moderator: Philippe E. Spiess, M.D. Invited Faculty Members: Wade J. Sexton, MD Jeremiah J. Morrissey, PhD Agenda for Session
New Frontiers in Urologic Oncology September 12 th, 2015 Kidney Cancer Session Moderator: Philippe E. Spiess, M.D. Invited Faculty Members: Wade J. Sexton, MD Jeremiah J. Morrissey, PhD Agenda for Session
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation. Basics. What is Percutaneous Ablation? Where are your kidneys?
 Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
Cytoreductive Nephrectomy
 Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Role of imaging in RCC. Ultrasonography. Solid lesion. Cystic RCC. Solid RCC 31/08/60. From Diagnosis to Treatment: the Radiologist Perspective
 Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic
Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy?
 Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
Section Activity Activity Description Details Reference(s)
") Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
Surgeons Perspective: LN as a Draining Pattern. Jose A. Karam, MD, FACS Associate Professor Department of Urology
 Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA
 1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 11/17/2012 Radiology Quiz of the Week # 99 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 11/17/2012 Radiology Quiz of the Week # 99 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Wilms Tumor and Neuroblastoma
 Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
All India Institute of Medical Sciences, New Delhi, INDIA. Department of Pediatric Surgery, Medical Oncology, and Radiology
 All India Institute of Medical Sciences, New Delhi, INDIA Department of Pediatric Surgery, Medical Oncology, and Radiology Clear cell sarcoma of the kidney- rare renal neoplasm second most common renal
All India Institute of Medical Sciences, New Delhi, INDIA Department of Pediatric Surgery, Medical Oncology, and Radiology Clear cell sarcoma of the kidney- rare renal neoplasm second most common renal
Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma of Thyroid
 Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
Case Reports in Urology Volume 2013, Article ID 651081, 4 pages http://dx.doi.org/10.1155/2013/651081 Case Report Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
LONG-TERM SURGICAL OUTCOMES OF 1018 PATIENTS WITH EARLY STAGE NSCLC IN ACOSOG Z0030 (ALLIANCE) TRIAL
 TRIAL") LONG-TERM SURGICAL OUTCOMES OF 1018 PATIENTS WITH EARLY STAGE NSCLC IN ACOSOG Z0030 (ALLIANCE) TRIAL Stacey Su, MD; Walter J. Scott, MD; Mark S. Allen, MD; Gail E. Darling, MD; Paul A. Decker, MS; Robert
LONG-TERM SURGICAL OUTCOMES OF 1018 PATIENTS WITH EARLY STAGE NSCLC IN ACOSOG Z0030 (ALLIANCE) TRIAL Stacey Su, MD; Walter J. Scott, MD; Mark S. Allen, MD; Gail E. Darling, MD; Paul A. Decker, MS; Robert
Solitary Contralateral Adrenal Metastases after Nephrectomy for Renal Cell Carcinoma
 Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
Surgically Discovered Xanthogranulomatous Pyelonephritis Invading Inferior Vena Cava with Coexisting Renal Cell Carcinoma
 Case Study TheScientificWorldJOURNAL (2009) 9, 5 9 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2009.6 Surgically Discovered Xanthogranulomatous Pyelonephritis Invading Inferior Vena Cava with Coexisting
Case Study TheScientificWorldJOURNAL (2009) 9, 5 9 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2009.6 Surgically Discovered Xanthogranulomatous Pyelonephritis Invading Inferior Vena Cava with Coexisting
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
RCC in ADPKD / CKD / ESRD
 RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Urology An introduction to cut up DR J R GOEPEL
 Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient
Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.
 Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
Advanced & Metastatic Renal Cell Carcinoma
 Advanced & Metastatic Renal Cell Carcinoma An Update G. Renzulli January 2013 1 Overview of Cancers of the Kidney 2 Global Epidemiology 3 Global Epidemiology of Kidney Cancer 4 Globally, kidney cancer
Advanced & Metastatic Renal Cell Carcinoma An Update G. Renzulli January 2013 1 Overview of Cancers of the Kidney 2 Global Epidemiology 3 Global Epidemiology of Kidney Cancer 4 Globally, kidney cancer