CLL: from past to present from present to future
|
|
|
- Barbra Gordon
- 5 years ago
- Views:
Transcription


1 CLL: from past to present from present to future Ann Janssens MD, PhD Hematology UZ Leuven BHS course, 8 th february
2 2 Part1 Diagnosis Prognostic factors Part 2 Complications Treatment
3 B-cell neoplasms Precursor B-cell neoplasm B-ALL, B-lymfoblastenlymfoom Mature B-cell neoplasms >85% CLL/SLL B-cell prolymphocytic leukemia Follicular lymphoma Hairy cell leukemia Lymphoplasmacytic lymphoma Marginal zone B-cell lymphoma Extranodal MZL (gastric and non-gastric MALT) Splenic MZL Nodal MZL Plasma cell myeloma/plasmacytoma/mgus Mantle cell lymphoma Diffuse large B-cell lymphoma Burkitt lymphoma/burkitt cell leukemia
4 CLL is a Non Hodgkin lymphoma B cell lymphoma Mainly leukemic: B-ALL, CLL, MCL, B-PLL, SLVL, HCL Mainly nodal: FL, nodal MZL Nodal/extranodal: DLBCL, Burkitt, MALT Mainly bone marrow:waldenström, Multiple Myeloma T cell lymphoma Mainly leukemic: Mainly nodal: Nodal/extranodal: Mainly extranodal: T-ALL, LGL, T-PLL, ATLL, AITL, ALCL, peripheral T cell lymphoma NOS cutaneous lymphomas (mycosis fungoides), NK/T cell lymphoma, EATL, hepatosplenic lymphoma WHO classification of tumours of Haematopoietic and Lymphoid tissues, 4th ed., 2008






5 Hematological malignancies CLL is the most common form of adult leukemia in Western countries CML 4% CLL 11% NHL 50% AML 9% ALL 4% SEER Ho 7% MM 15%

6 Epidemiology of CLL US 4.2/ person-years median age 72y The Netherlands 3.8/ person-years 2/3 >65y at diagnosis M/F: 2/1 Van den Broek et al. Eur J Cancer 2012
7 How to diagnose and stage a lymphoma/cll? Clinical data Personal history Clinical examination Blood examination Histopathology Bone marrow/threphine Imaging
8 How to diagnose and stage CLL? Clinical data Personal history: most asymptomatic, only 5% reveal B-symptoms Clinical examination: 25% lymphadenopathies, 15% organomegaly Blood examination: leukocytosis due to a lymphocytosis Histopathology Bone marrow/threphine Imaging: X-ray thorax, echo abdomen, CT-scan neck, thorax, abdomen & pelvis, PET-CT?
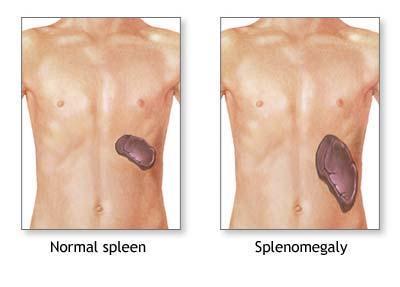
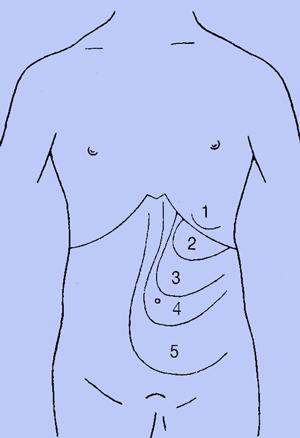
9 Clinical examination
10 How to diagnose and stage CLL? Clinical data Personal history: most asympthomatic, only 5% reveal B-symptoms Clinical examination: 25% lymphadenopathies, 15% organomegaly Blood examination: leukocytosis due to a lymphocytosis Histopathology Bone marrow/threphine Imaging: X-ray thorax, echo abdomen, CT-scan neck, thorax, abdomen & pelvis, PET-CT?



11 DIAGNOSIS OF CLL: 1:MORPHOLOGY BLOOD SMEAR CLL cell characterictics: small mature narrow border of cytoplasm dense nucleus with partially aggregated chromatin no discernible nucleoli Gumprecht nuclear shadows or smudge cells Microscopy blood smear: easy, rapid and inexpensive Hallek et al., Blood 2008, guidelines CLL, updating NCI-WG 1996
12 MORPHOLOGY CLL: GUMPRECHT NUCLEAR SHADOWS

13 DIAGNOSIS CLL 2: IMMUNOPHENOTYPE CLL score 3/5 CD5 positive CD19, CD23 positive CD20, CD79b low expression sig, k of l low expression FMC7 negative CLL 3 à 5/5 B-PLL 0 à 1/5 HC 0 à 1/5 FL, SLVL, MCL 0 à 2/5 Moreau, Am J Pathol 1997
14 How to diagnose and stage CLL? Clinical data Personal history: most asympthomatic, only 5% reveal B-symptoms Clinical examination: 25% lymphadenopathies, 15% organomegaly Blood examination: leukocytosis due to a lymphocytosis, morphology and immunophenotyping Bone marrow/ threphine Imaging: X-ray thorax, echo abdomen, CT-scan neck, thorax, abdomen & pelvis, PET-CT? Histopathology




15 DIAGNOSIS CLL: 3: MARROW EXAMINATION Bone marrow aspirate + biopsy + immunophenotyping + genetics For diagnosis or staging CLL? No Unexplained cytopenia (disease related, auto-immune, drug related) Yes Confirming complete remission after treatment in clinical trials: Yes



16 DIAGNOSIS CLL: 3: MARROW EXAMINATION Marrow aspirate/ biopsy not required for the diagnosis! CLL: > 30% of nucleated cells in the aspirate are lymphoid Diffuse or non-diffuse infiltration No prognostic value anymore Hallek et al., Blood 2008, guidelines CLL, updating NCI-WG 1996
17 How to diagnose and stage CLL? Clinical data Personal history: most asympthomatic, only 5% reveal B-symptoms Clinical examination: 25% lymphadenopathies, 15% organomegaly Blood examination: leukocytosis due to a lymphocytosis Histopathology Bone marrow/threphine Imaging: X-ray thorax, echo abdomen, CT-scan neck, thorax, abdomen & pelvis, PET-CT?
18 DIAGNOSIS CLL: 4: IMAGING Outsite clinical trials: Abdominal ultrasound: popular, clinician dependent In clinical trials: CT chest, abdomen and pelvis (before start and at the end of treatment) Positron emission tomography scan Not usefull in CLL, except when Richter transformation is suspected Hallek et al., Blood 2008, guidelines CLL, updating NCI-WG 1996

19 DIAGNOSIS CLL: 4:IMAGING??? Radiological investigation not needed for staging and response evaluation Eichhorst et al., Blood 2011 Pre- and posttreatment CT should be considered for patients treated with more intensive therapies. There is no role for routine surveillance CT in asymptomatic patients posttreatment. Oscier et al, Br J Haematol, 2012 Guidelines on diagnosis, investigation and management of CLL


20 Casus: F, 66 y Rai 0, Binet A
21 How to diagnose and stage CLL? Clinical data Personal history: most asympthomatic, only 5% reveal B-symptoms Clinical examination: 25% lymphadenopathies, 15% organomegaly Blood examination: leukocytosis due to a lymphocytosis Bone marrow/threphine Imaging: X-ray thorax, echo abdomen, CT-scan neck, thorax, abdomen & pelvis, PET-CT? Histopathology lymph node




22 DIAGNOSIS CLL: 5: LYMPH NODE BIOPSY Lymph node biopsy only necessary in case of difficult diagnosis Necessary to establish the diagnosis of Richter transformation Hallek et al., Blood 2008, guidelines CLL, updating NCI-WG 1996

23 Monoclonal B cell lymphocytosis Small Lymphocytic Lymphoma Chronic Lymphocytic Leukemia Clonal B cells < 5000/ l Clonal B cells < 5000/ l Clonal B cells > 5000/ l MBL + Lymphadenopathies Lymphadenopathies +/- 1%/y Organomegaly +/- Organomegaly +/- SLL/CLL Cytopenia due to marrow infiltration +/- Cytopenia due to marrow infiltration +/- Hallek et al. Blood 2008 Constitutional symptoms +/- Constitutional symptoms +/-




24 Clinical course CLL is highly variable 1/3 never requires treatment 1/3 requires treatment after an indolent phase 1/3 progressive from the onset with immediate need for treatment Dighiero et al, Am Soc Hematol Educ Program 2005

25 Can we predict clinical course? Can we predict overall survival? Can we predict treatment response? Can we predict duration of response?
26 Predictive and prognostic factors Clinical staging: Rai and Binet Lymphocyte doubling time IGVH mutational status CD38 Genomic aberrations Response to treatment 26


27 Clinical staging systems predict outcome Staging system Clinical features Lab results Median survival 0 low risk lymphocytosis 150m Rai I-II intermediate risk lymphadenopathy splenomegaly m III-IV high risk anemia thrombocytopenia 19m A <3 areas of lymphadenopathies nl Binet B >3 areas of lymphadenopathies 7y C anemia thrombocytopenia 2y Rai et al. Blood 1975 & 1987; Binet et al. Cancer 1981
28 Clinical staging and OS today Staging system Stage Median OS Anno 1975 N= 125 Rai 8 Median OS Anno 2009 N= 2397 Mayo 11 Median OS Anno 2011 N=1300 Czech Republic mo 130 mo 362 mo I 101 mo 106 mo 125 mo Rai II 71 mo 88 mo 120 mo III 19 mo 58 mo 72 mo Rai et al. Blood 1975 & 1987 Binet et al. Cancer 1981 Apelgren et al. Leuk Lymphoma 2006 Shanafelt et al. Cancer 2010 Doubek et al. Eur J Haematol 2011 Binet IV 19 mo 69 mo 104 mo Median OS Anno 1981 N= 295 Binet 10 Median OS Anno 2006 N=344 Sweden 12 A normal 100 mo B 7 y 55 mo C 2 y 45 mo
29 Lymphocyte doubling time < or > 12 months and mos Overleving B-CLL UZ Gent vgl >12m ( n= 164) verdubbelingstijd mos 233 mo <12m ( n= 61) en Binet mos staging 106 mo P < Percent Survival A en>12 m A en <12 m BC en >12m BC en <12m followup CLL database UZ Ghent

30 IGVH mutational status Remains stable over time Unmutated: 2% variation with germline Mutated: >2% variation with germline DNA sequencing was expensive, technically demanding, not widely available Search for surrogate markers Pepper et al. Br J Haematol 2011
31 CD38: surrogate marker for IGVH mutational status? Transmembrane protein Detected by flow cytometry CD38-IGV H discordance: 30% CD38 expression may vary: 25% Cut-off value not clearly defined ( %) Bimodal expression in some patients Pepper et al. Br J Haematol 2011
32 ZAP-70: surrogate marker for IGVH mutational status? Intracellular tyrosine kinase Detected by flow cytometry ZAP-70 -IGV H discordance: 7-30% ZAP-70 expression may vary: 5-10% Optimal cut-off value not defined No standardized test exist Pepper et al. Br J Haematol 2011


33 Genomic aberrations predict survival Conventional karyotyping Clonal aberrations in only 40-50% Better outcome if no vs clonal aberrations Better outcome if single vs complex aberrations FISH 13q14 deletion Trisomy 12 11q22 deletion 17p13 deletion Julliusson G et al. N Eng J Med 1990 Döhner H et al. N Eng J Med 2000
34 Genomic aberrations predict survival N= 325 untreated patients 100 % mttt mos 13q deletion 55 92m 133m trisomy m 114m 11q deletion 18 13m 79m Patients Surviving (%) q deletion 17p deletion 7 9m 32m 13q deletion 12q trisomy Normal 80% 0 17p deletion Mos Dohner et al. N Engl J Med 2000


35 Conventional karyotyping Clonal aberrations in only 40-50% Better outcome if no vs clonal aberrations Better outcome if single vs complex aberrations FISH 13q14 deletion Trisomy 12 11q22 deletion 17p13 deletion Conventional karyotyping with novel culture techniques Clonal aberrations in 80% Worse outcome if translocations or complex karyotype? Next generation sequencing p53, ATM NOTCH1, SF3B1, BIRC3 Julliusson G et al. N Eng J Med 1990, Döhner H et al. N Eng J Med 2000, Haferlach C et al. Leukemia 2007, Gaidano et al. Clin Invest 2012

36 Integrated mutational & cytogenetic analysis Rossi et al. Blood 2013
37 At diagnosis Chemorefractory 13q14 50% % ATM 15% P % NOTCH1 10% SF3B1 5-10% BIRC3 4% 13q14 50% % ATM 25% P53 40% NOTCH1 25% SF3B1 25% BIRC3 25% MYD88 3-5%
38 Response to treatment is a prognostic factor in first-line treatment Response to FCR as frontline treatment predicts OS Complete response Partial response Progressive disease Stable disease Hallek M, et al. Lancet 2010; 376: ; Hallek M, et al. CLL8 trial updated, Unpublished.
39 Response duration after 1st line treatment affects outcome Patients who relapse early after 1 st -line FC or FCR have a very poor prognosis Remission duration after 1 st -line treatment Median OS from 2 nd -line treatment >24 months 44.6 months months 20.3 months <12 months 13.1 months FC: 14,5%-24,5% Cumulative survival Remission <12 months (n=47) Remission >24 months (n=32) Remission months (n=45) 0.0 FCR: 7,6%-16% Overall survival Months Stilgenbauer S, Zenz T. Am Soc Hematol Educ Program 2010


40 Response to treatment is a prognostic factor in refractory patients Response to alemtuzumab in F-refractory patients Response to ofatumumab in F and A refractory patients Patient survival (%) m OS in responders 32 months Median OS all patients 16 months Keating et al. Blood, 2002 Wierda et al. Blood 2010

41 Minimal residual disease after 1 st line independent prognostic marker Moreno et al. Best Pract Res Clin Haematol 2010, Böttcher et al. J Clin Oncol 2012



42 Conclusion Part 1: Diagnostic and/or pretreatment work-up Mandatory Potential utility Personal and familial history Physical examination Biological fitness: PS, comorbidities Biological fitness: CGA Complete blood cell count Peripheral blood smear CLL score Serum chemistry: LDH, IG, Cr Parameters for hemolysis FISH: 17p deletion Virology: hep B, hep C, CMV, HIV Clinical staging: Rai-Binet CD38- ZAP-70 β2-microglobin IGV H mutational status FISH: 13q, t12, 11q Conventional karyotyping with novel culture techniques Bone marrow aspirate and biopsy CT neck, thorax, abdomen, pelvis PET-scan
43 43 Part1 Diagnosis Prognostic factors Part 2 Complications Treatment
44 CLL and complications Advanced or active disease Relapsing to refractory disease Disease or therapy related cytopenia Infections, disease or therapy related Auto-immune phenomena AIHA, ITP, PRCA, AIN Secondary malignancies Melanoma and non-melanoma skin cancer, cancer of respiratory tract, prostate, kidney, Transformation Richter s syndrome Prolymphocytic transformation

45 Auto-immune phenomena in 4-10% of CLL patients Treatment Corticoiden AIHA AIN AITP PRCA Immunosuppressive agents: cyclosporine, mycophenolate mofetil, azathioprine Monoclonal antibodies Splenectomy Myeloid growth factors TPO-agonists 45
46 Secondary malignancies Risk of a sec malignancy 2x compared to age and sex matched controls Melanoma and non-melanoma skin cancers Respiratory cancer Prostate Renal Transformation to a higher grade lymphoma : Richter s syndrome 46


47 Richter s syndrome Prolymphocytic transformation (PLL) Transformation to DLBCL (95%) or Hodgkin s lymphoma (5%) Characterized by an abrupt change in patient s condition, rapid, asymmetric enlargment of lymph nodes, extranodal involvement, increasing LDH, and sometimes a monoclonal gammapathy Progressive increase of prolymphocytes in blood and bone marrow Characterized by a worsening of cytopenia, increasing lymphadenopathies and organomegaly and refractoriness to conventional treatment

48 At diagnosis Richter transformation 13q14 50% % ATM 15% P % NOTCH1 10% SF3B1 5-10% BIRC3 4% 13q14 20% % ATM 25% P53 60% NOTCH1 30% SF3B1 5% BIRC3 0% MYD88 3-5%
 or progressive or symptomatic splenomegaly Massive (>10cm) or progressive or")
 Fever >38 C for >2w without infection Night sweats >1m Hallek et")
49 INDICATIONS FOR TREATMENT «primary = second line decisions» High tumorload Stage Rai 3-4 or Binet C Disease progression Lymphocyte doubling time of less than 6m Massive (>6 cm below costal margin) or progressive or symptomatic splenomegaly Massive (>10cm) or progressive or symptomatic lymphadenopathy Progressive marrow failure leading to cytopenia Auto-immune problems Disease related problems AIHA, AITP, PRCA poorly responsive to corticosteroids 10% weight loss in 6m Fatigue ( PS>+2) Fever >38 C for >2w without infection Night sweats >1m Hallek et al., Blood 2008






50 Treatment 50
51 Frontline treatment CLL Active or advanced disease No active or no advanced disease Wait and See 51

52 Fit or unfit? 52




53 Fit for what? 53
 Organ system Heart Blood pressure Vascular Respiratory Ear/nose/throat Upper gastrointestinal Lower")

54 Assessment of co-morbidity by CIRS Cumulative Illness rating scale CIRS captures numbers and severity of comorbidities CUMULATIVE ILLNESS RATING SCALE (CIRS) Organ system Heart Blood pressure Vascular Respiratory Ear/nose/throat Upper gastrointestinal Lower gastrointestinal Liver Renal Genitourinary Musculoskeletal Endocrine/metabolic Neurological Psychiatric If illness/impairment present, please specify: Score Total Score: Linn B, et al. J Am Geriatr Soc 1968; 16: Parmelee P, et al. J Am Geriatr Soc 1995; 43:




55 CIRS score measures medical fitness 25 Fit Unfit 20 Patients (%) CIRS total score Extermann M, et al. J Clin Oncol 1998; 16:
56 If >70y : screening for a geriatric risk prophile Triage risk screening tool (2)History or evidence of cognitive impairment (poor recall or not oriented) (1)Lives alone and/or no available caregiver (1) Difficulty walking/transferring or recent falls (1)Five or more medications (1) ED use in previous 30 days or hospitalization in previous 90 days If 1: go for comprehensive geriatric assessment Meldon et al,

57 Tools to evaluate functional age Polypharmacy Activities of daily living Instrumental ADL comprehensive geriatric assessment Time & Man-power consuming, Not reimbursed Social support FIT VULNERABLE FRAIL Comorbidities Not used in routine clinical practice Psychological status Nutritional status Minimental state Need for simple screening test Pallis A et al, Eur J Cancer,

58 Frontline treatment CLL CLL 8: FCR vs FC OR 95,1% vs 88,4% CR 44,1% vs 21,8% Active or advanced disease mpfs 51,8 vs 32 mo 17p deletion or p53 defect Fit for FCR Unfit for FCR FCR 3y OS 87% vs 83% Clinical trial Hallek et al., Lancet 2010;376;
59 CLL 10: FCR vs BR in physically fit patients with no 17p deletion 561 patients evaluable hematological toxicity: 90% vs 67% neutropenia: 81.7% vs 56.8% infections: 39% vs 25.4% ( p= 0.001) Median age 62 (33-82)y, CIRS 2 (0-6) Binet A 22%, B 38%, C 40% CR ORR MRD mpfs OS 2y TRM R N=284 Fludarabine- Cyclofosfamiderituximab Bendamustine- Cyclofosfamide FCR 47.4% 97.8% 55.2 mo 90.6% 3.9% BR 38.1% 97.8% 41.7 mo 92.2% 2.1% p = <0.01 0,897 N=280 Untreated CLL > 18 years CIRS <=6 CrCl >70ml/ Eichorst et al., ASH 2014, abstract M follow-up: 27.9 mo



60 Frontline treatment CLL Active or advanced disease Unfit for FCR? CIRS >6 CrCl <70 ml/ Active AIHA Recurrent infections 17p deletion or p53 defect Fit for FCR Unfit for FCR FCR BR Clinical trial 30% >65y 10% >70y Binet B or C CIRS 6 CrCl >70ml/ Janssens et al. Belg Hematol J, 2012



61 Frontline treatment CLL CLL 5: Chl vs F Active or advanced disease Median age y PFS 18 vs 19m OS 64 vs 46m Fit for FCR Unfit for FCR FCR OS 30% >65y 10% >70y Binet B or C CIRS 6 CrCl >70ml/ Something better than Chl??? Eichhorst, B. F. et al. Blood 2009;114:
62 First-Line Bendamustine vs Chl Response % B Chl Overall 62% 33% CR 27% 2% PR 35% 31% PFS (%) Log-rank test stratified according to Binet B/C: P <.0001 Gr 3-4 neutropenia: 43 vs 21% Gr 3-4 infections: 7 vs 3% Months 24 mpfs 21.5m mpfs 8.3m Median 40 Bendamustine (n = 162) Chlorambucil (n = 157) Knauf et al. Br J Haematol, 2012


63 CLL 11 for the slow go OR/CR mpfs 30/0% Chlorambucil 10.8 mo 66/8% CIRS >6 Or Cr Cl <70ml/ R Chlorambucil- Rituximab 15.7mo 75/22% Chlorambucil- GA mo Goede et al, ASCO, EHA, ICML, ASH


64 CLL 11: PFS GA 101 vs Chl Goede et al, NEJM, 2013


65 CLL 11: OS GA-101 vs Chl Goede et al, ASCO, EHA, ICML, ASH 2013 plenary

66 Results at ASH 2013 mpfs: 22.4 vs 13.1 mo N=525 18y, contraindication for fludarabine active disease, Not previously treated ECOG 0-2
67 OMB : PFS (IRC assessed) Hillmen et al, Lancet, accepted
 BR Chl / B Chl-R, Chl-GA-101 Chl-0 Clinical trial F / FR / FC RIC-alloBMT Clinical")
68 Frontline treatment CLL Active or advanced disease 17p deletion or p53 defect Fit for FCR Unfit for FCR Novel agents Clinical trial A A + HDMP FCR-FCA-CFAR FCR BR ( >65y) BR Chl / B Chl-R, Chl-GA-101 Chl-0 Clinical trial F / FR / FC RIC-alloBMT Clinical trial 68

 FA (Ib)/")
69 Treatment at Late relapse Refractory CLL Relapsing CLL Clinical trial Not confirmed by any clinical trial! Repeat previous treatment FC/FCR (Ib) FA (Ib)/ FCA (Iia/b abstract) BR (IIa) 69
 A + HDMP (IIb) R + HDMP (IIb) Clinical trial Alemtuzumab (IIa)")
 Not eligible for transplant: consider consolidation in")
70 Refractory or early relapse CLL 17p deletion - p53 defects Fludarabine refractory Fludarabine and Alemtuzumab refractory Relapse <24m after CIT Clinical trial A (IIa or b) A + HDMP (IIb) R + HDMP (IIb) Clinical trial Alemtuzumab (IIa) FCR-FA-FCA Ofatumumab (IIa) Clinical trial Repeat previous treatment if CR/nCR Go for another CIT combination Unmed medical need OS 13m PFS 4,5m Fit: RIC Allo-transplant (IIb or III) Not eligible for transplant: consider consolidation in clinical trial 70
 Clinical trial Alemtuzumab (IIa) FCR-FA-FCA Novel agents Ibrutinib Idelalisib/rituximab Venetoclax Ofatumumab (IIa) Clinical trial Repeat previous treatment if CR/nCR Go for another CIT")
71 Refractory or early relapse CLL 17p deletion - p53 defects Fludarabine refractory Fludarabine and Alemtuzumab refractory Relapse <24m after CIT Clinical trial A (IIa or b) A + HDMP (IIb) R + HDMP (IIb) Clinical trial Alemtuzumab (IIa) FCR-FA-FCA Novel agents Ibrutinib Idelalisib/rituximab Venetoclax Ofatumumab (IIa) Clinical trial Repeat previous treatment if CR/nCR Go for another CIT combination Fit: RIC Allo-transplant (IIb or III) Not eligible for transplant: consider consolidation in clinical trial 71

 after purine analogue or")


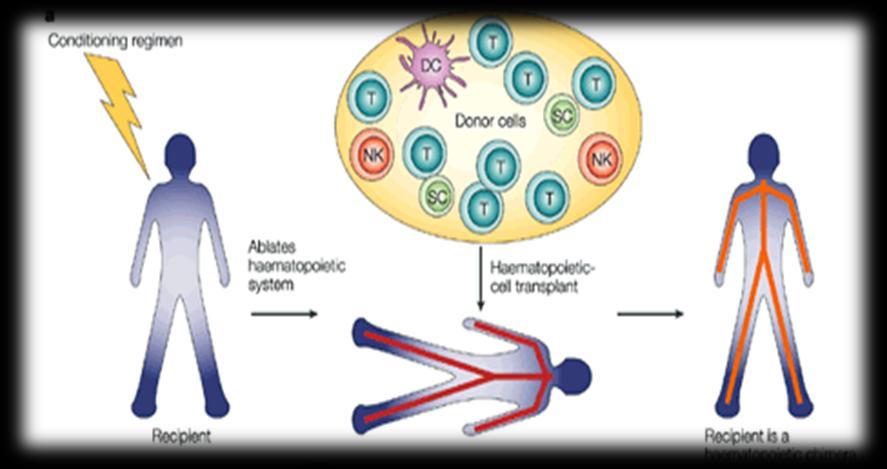
72 Allotranplantation in CLL EBMT guidelines for TX -Refractory CLL -Early relapse (within months) after purine analogue or combination therapy -p53 deletion/mutation requiring treatment Dreger et al, Blood, 2014 Don t use as a last desperate measure! Moreno, EHA 2012, educational 72
73 Dreger et al, Blood
 RP6530 d+y GS-9820 CC-292 ONO-4059")
74 BCR- antagonists Oral Inhibition of proliferation, migration, adhesion AMG 319 IPI-145 BAY TGR-1202 XL147 (panpi3k) RP6530 d+y GS-9820 CC-292 ONO
75 R/R no del 17p PFS = 81% 95% CI = [64%, 91%] R/R del 17p PFS = 53% 95% CI = [28%, 72%] Historical data: Median PFS 3-7 months R/R CLL patients by 17p status treated with ibrutinib (PCYC-1102-CA): Median PFS not reached (median f/u 22 mo)
76 R/R no del 17p OS = 87% R/R del 17p OS = 67% Historical data: Median OS months Survival in R/R CLL patients by del 17p status (PCYC-1102-CA): Median OS not Reached (median f/u 22 mo)
77 Byrd et al, NEJM 2013


78 Ibrutinib and response pattern 78

79 Ibrutinib: Aes in treatment naive CLL patients 79
 17 p del (n=9) ORR: 100%, CR 33%, PR 67% O Brien,")
80 Idelalisib+Rituximab in naive CLL, >65y Median age 71y Rituximab 8 weeks Idelalisib 2 x 150 mg/d continuously All patients ORR: 97% (CR 19%, PR 78%) 17 p del (n=9) ORR: 100%, CR 33%, PR 67% O Brien, ASCO 2013
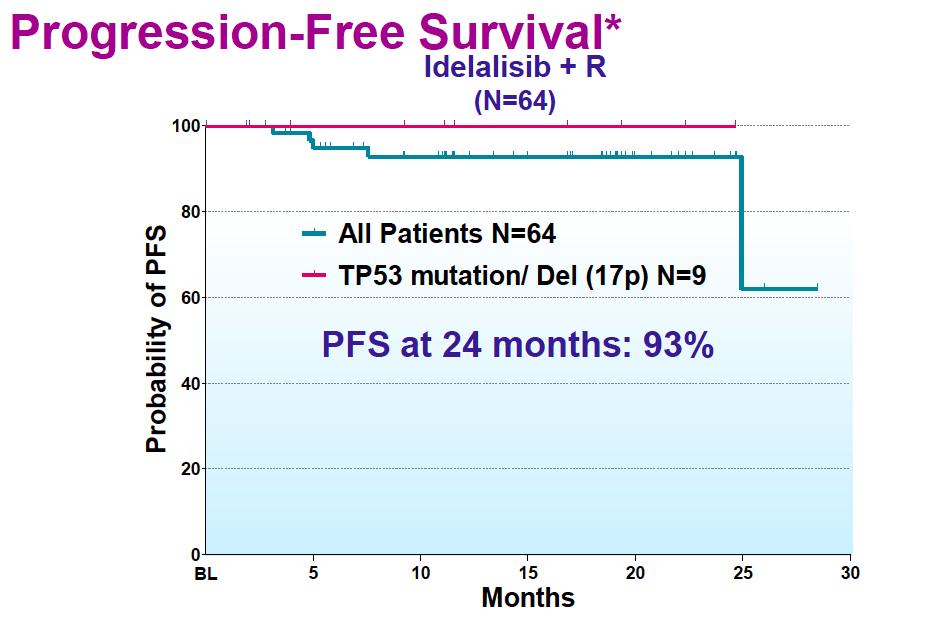
81 Idelalisib+Rituximab in naive CLL, >65y O Brien, ASCO 2013

82 Idelalisib in Rel/Ref CLL Flinn et al, ICML 2013, abstract 297 & Brown, ASCO 2013
83 Lenalidomide and 17p deletion N=103 Median age 63.6y 17p del 24% and p53 mut 39% ORR 38.5% ORR 40% for pat without and 35% for pat with p53 mut ORR 22.7% for pat with a 17pdel No difference in ORR for pat with or without p53 mutation Buhler et al, ICML 2013, abstract 058
 17p deletion 29%, F ref 32% ORR 85% (17p 88%, F Ref 75%) TLS 10%: dosing and sheduling modifications ongoing Nausea, diarrhea, fatigue, infections ( also")
84 ABT-199 in Rel/Ref CLL ABT-199: selective bcl-2inhibitor N=56 Median age 67y Median n of therapies: 3.5 (1-10) 17p deletion 29%, F ref 32% ORR 85% (17p 88%, F Ref 75%) TLS 10%: dosing and sheduling modifications ongoing Nausea, diarrhea, fatigue, infections ( also tested in FL, WM, MCL, DLBCL) Seymour et al, ICML 2013, abstract 057



85 CLL treatment: a chemotherapy-free road? Cytostatic agents Antibodies New anti- CD20 antibodies BCR antagonists Chimeric antigen receptors Immunomodulatory agents Bcl 2 inhibitors

86 86
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
Chronic lymphocytic Leukemia
 Chronic lymphocytic Leukemia after IwCLL, ICML and EHA 2017 Ann Janssens, MD, PhD Hematology, UZ Leuven Brussels, 14 september 2017 Front line treatment CLL Active or progressive disease No active or progressive
Chronic lymphocytic Leukemia after IwCLL, ICML and EHA 2017 Ann Janssens, MD, PhD Hematology, UZ Leuven Brussels, 14 september 2017 Front line treatment CLL Active or progressive disease No active or progressive
CLL Ireland Information Day Presentation
 CLL Ireland Information Day Presentation 5 May 2018 Professor Patrick Thornton Consultant Haematologist, Senior Lecturer RCSI, and Clinical Director Hermitage Medical Clinic Laboratory Chronic Lymphocytic
CLL Ireland Information Day Presentation 5 May 2018 Professor Patrick Thornton Consultant Haematologist, Senior Lecturer RCSI, and Clinical Director Hermitage Medical Clinic Laboratory Chronic Lymphocytic
FCR and BR: When to use, how to use?
 FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD
: Refresher Course for Hematologists Ekarat Rattarittamrong, MD") Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang-Mai University Outline
Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang-Mai University Outline
CLL: disease specific biology and current treatment. Dr. Nathalie Johnson
 CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
CLL & SLL: Current Management & Treatment. Dr. Peter Anglin
 CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto)
 and Dr. Matt Cheung (Staff Hematologist, University of Toronto)") CLL Updated March 2017 by Doreen Ezeife Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto) DISCLAIMER: The following
CLL Updated March 2017 by Doreen Ezeife Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto) DISCLAIMER: The following
Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division
 Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division University of Virginia Cancer Center The Clinical Continuum of CLL Early asymptomatic
Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division University of Virginia Cancer Center The Clinical Continuum of CLL Early asymptomatic
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
CLL what do I need to know as an Internist in Taimur Sher MD Associate Professor of Medicine Mayo Clinic
 CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
Investigation and Management of Chronic Lymphocytic Leukemia. James Johnston
 Investigation and Management of Chronic Lymphocytic Leukemia James Johnston Site Specific Clinics CLL Clinic (787-4454) Erin Elphee BN James Johnston Rajat Kumar Matt Seftel (transplant) Myeloma Clinic
Investigation and Management of Chronic Lymphocytic Leukemia James Johnston Site Specific Clinics CLL Clinic (787-4454) Erin Elphee BN James Johnston Rajat Kumar Matt Seftel (transplant) Myeloma Clinic
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
Chronic Lymphocytic Leukemia Update. Learning Objectives
 Chronic Lymphocytic Leukemia Update Ashley Morris Engemann, PharmD, BCOP, CPP Clinical Associate Adult Stem Cell Transplant Program Duke University Medical Center August 8, 2015 Learning Objectives Recommend
Chronic Lymphocytic Leukemia Update Ashley Morris Engemann, PharmD, BCOP, CPP Clinical Associate Adult Stem Cell Transplant Program Duke University Medical Center August 8, 2015 Learning Objectives Recommend
Advances in CLL 2016
 Advances in CLL 2016 The Geoffrey P. Herzig Memorial Symposium, Louisville, KY Kanti R. Rai, MD Northwell-Hofstra School of Medicine Long Island Jewish Medical Center New Hyde Park, NY Disclosures Member
Advances in CLL 2016 The Geoffrey P. Herzig Memorial Symposium, Louisville, KY Kanti R. Rai, MD Northwell-Hofstra School of Medicine Long Island Jewish Medical Center New Hyde Park, NY Disclosures Member
Highlights in chronic lymphocytic leukemia
 Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
CLL treatment algorithm and state of the art
 CLL treatment algorithm and state of the art Davide Rossi, M.D., Ph.D. Hematology IOSI - Oncology Institute of Southern Switzerland IOR - Institute of Oncology Research Bellinzona - Switzerland CLL subgroups
CLL treatment algorithm and state of the art Davide Rossi, M.D., Ph.D. Hematology IOSI - Oncology Institute of Southern Switzerland IOR - Institute of Oncology Research Bellinzona - Switzerland CLL subgroups
Clinical Overview: MRD in CLL. Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel
 Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
Risikoprofil-gesteuerte, individualisierte Therapiestrategien bei der CLL. Michael Hallek University of Cologne
 Risikoprofil-gesteuerte, individualisierte Therapiestrategien bei der CLL Michael Hallek University of Cologne 100 90 80 70 60 Substantial progress in CLL therapy in one decade 50 40 complete remissions
Risikoprofil-gesteuerte, individualisierte Therapiestrategien bei der CLL Michael Hallek University of Cologne 100 90 80 70 60 Substantial progress in CLL therapy in one decade 50 40 complete remissions
Georg Hopfinger 3. Med.Abt and LBI for Leukemiaresearch and Haematology Hanusch Krankenhaus,Vienna, Austria
 Chronic lymphocytic Leukemia Georg Hopfinger 3. Med.Abt and LBI for Leukemiaresearch and Haematology Hanusch Krankenhaus,Vienna, Austria georg.hopfinger@wgkk.at CLL Diagnosis and Staging Risk Profile Assessment
Chronic lymphocytic Leukemia Georg Hopfinger 3. Med.Abt and LBI for Leukemiaresearch and Haematology Hanusch Krankenhaus,Vienna, Austria georg.hopfinger@wgkk.at CLL Diagnosis and Staging Risk Profile Assessment
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia
 Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Improving Response to Treatment in CLL with the Addition of Rituximab and Alemtuzumab to Chemoimmunotherapy
 New Evidence reports on presentations given at ASH 2009 Improving Response to Treatment in CLL with the Addition of Rituximab and Alemtuzumab to Chemoimmunotherapy From ASH 2009: Chronic Lymphocytic Leukemia
New Evidence reports on presentations given at ASH 2009 Improving Response to Treatment in CLL with the Addition of Rituximab and Alemtuzumab to Chemoimmunotherapy From ASH 2009: Chronic Lymphocytic Leukemia
Management of CLL in the Targeted Therapy Era
 Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Update on Management of CLL. Presenter Disclosure Information. Chronic Lymphocytic Leukemia. Audience Response Question?
 Welcome to Master Class for Oncologists New York, NY May 14, 2010 Session 5: 4:20 PM - 5:00 PM Update on Management of CLL John C. Byrd, MD D Warren Brown Professor of Leukemia Research Professor of Medicine
Welcome to Master Class for Oncologists New York, NY May 14, 2010 Session 5: 4:20 PM - 5:00 PM Update on Management of CLL John C. Byrd, MD D Warren Brown Professor of Leukemia Research Professor of Medicine
MED B Form CLL. Johannes Schetelig. London 09/April/
 www.ebmt.org MED B Form CLL Johannes Schetelig London 09/April/2013 Content Update on CLL (15 ) Experiment with mini MED B CLL Assessment of pre-treatment in CLL Cytogenetics in CLL What is the IGVH-Gene
www.ebmt.org MED B Form CLL Johannes Schetelig London 09/April/2013 Content Update on CLL (15 ) Experiment with mini MED B CLL Assessment of pre-treatment in CLL Cytogenetics in CLL What is the IGVH-Gene
LEUCEMIA LINFATICA CRONICA
 LEUCEMIA LINFATICA CRONICA Gianluca Gaidano SCDU Ematologia Dipartimento di Medicina Traslazionale Università del Piemonte Orientale Novara Outline CLL biology and pathogenesis Prognostication and prediction
LEUCEMIA LINFATICA CRONICA Gianluca Gaidano SCDU Ematologia Dipartimento di Medicina Traslazionale Università del Piemonte Orientale Novara Outline CLL biology and pathogenesis Prognostication and prediction
CLL Biology and Initial Management. Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology
 CLL Biology and Initial Management Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology CLL- Epidemiology Most common adult leukemia 25-30% in western world Incidence in US 4.5
CLL Biology and Initial Management Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology CLL- Epidemiology Most common adult leukemia 25-30% in western world Incidence in US 4.5
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients
 MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November
MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November
CLL: What s New from ASH
 CLL: What s New from ASH John C. Byrd, MD D. Warren Brown Chair in Leukemia Research Professor of Medicine and Medicinal Chemistry Director, Division of Hematology The Ohio State University 2 Chronic Lymphocytic
CLL: What s New from ASH John C. Byrd, MD D. Warren Brown Chair in Leukemia Research Professor of Medicine and Medicinal Chemistry Director, Division of Hematology The Ohio State University 2 Chronic Lymphocytic
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
CHRONIC LYMPHOCYTIC LEUKEMIA
 CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: January, 2017 The recommendations contained in this guideline are a consensus of the Alberta Provincial Hematology Tumour Team synthesis of currently accepted
CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: January, 2017 The recommendations contained in this guideline are a consensus of the Alberta Provincial Hematology Tumour Team synthesis of currently accepted
Management of 17p Deleted CLL Patients in the Era of Targeted Therapy
 Management of 17p Deleted CLL Patients in the Era of Targeted Therapy Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November 11,
Management of 17p Deleted CLL Patients in the Era of Targeted Therapy Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November 11,
CHRONIC LYMPHOCYTIC LEUKEMIA
 CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: June, 2018 Copyright (2018) Alberta Health Services This material is protected by Canadian and other international copyright laws. All rights reserved. This
CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: June, 2018 Copyright (2018) Alberta Health Services This material is protected by Canadian and other international copyright laws. All rights reserved. This
We Can Cure Chronic Lymphocytic Leukemia with Current / Soon to be Approved Agents: CON ARGUMENT
 We Can Cure Chronic Lymphocytic Leukemia with Current / Soon to be Approved Agents: CON ARGUMENT Danielle M. Brander, MD Duke University Division of Hematologic Malignancies & Cell Therapy CLL & Indolent
We Can Cure Chronic Lymphocytic Leukemia with Current / Soon to be Approved Agents: CON ARGUMENT Danielle M. Brander, MD Duke University Division of Hematologic Malignancies & Cell Therapy CLL & Indolent
Quando e se è possibile e u/le o0enere una remissione completa
 Quando e se è possibile e u/le o0enere una remissione completa 1) Clinical heterogeneity Disease characteris:cs Pa:ent characteris:cs 2) Modern chemoimmunotherpy approaches 3) New mechanism- based treatment
Quando e se è possibile e u/le o0enere una remissione completa 1) Clinical heterogeneity Disease characteris:cs Pa:ent characteris:cs 2) Modern chemoimmunotherpy approaches 3) New mechanism- based treatment
CLL - venetoclax. Peter Hillmen St James s University Hospital Leeds 10 th May 2016
 CLL - venetoclax Peter Hillmen peter.hillmen@nhs.net St James s University Hospital Leeds 10 th May 2016 Pathophysiology of CLL: Proliferation vs Apoptosis Proliferation Apoptosis Ki-67 Expression Bcl-2
CLL - venetoclax Peter Hillmen peter.hillmen@nhs.net St James s University Hospital Leeds 10 th May 2016 Pathophysiology of CLL: Proliferation vs Apoptosis Proliferation Apoptosis Ki-67 Expression Bcl-2
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
ASH up-date: Changing the Standard of Care for Patients with. (or: Who to treat with What When?)
") ASH up-date: Changing the Standard of Care for Patients with B-cell Chronic Lymphocytic Leukaemia (or: Who to treat with What When?) Dr Anna Schuh, MD, PhD, MRCP, FRCPath Consultant and Senior Lecturer
ASH up-date: Changing the Standard of Care for Patients with B-cell Chronic Lymphocytic Leukaemia (or: Who to treat with What When?) Dr Anna Schuh, MD, PhD, MRCP, FRCPath Consultant and Senior Lecturer
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Aktuelle Therapiestandards und neue Entwicklungen bei der CLL Primärtherapie und Risikostratifikation
 Aktuelle Therapiestandards und neue Entwicklungen bei der CLL Primärtherapie und Risikostratifikation Dr. med. Petra Langerbeins Universitätsklinik Köln Deutsche CLL Studiengruppe (DCLLSG) OFFENLEGUNG
Aktuelle Therapiestandards und neue Entwicklungen bei der CLL Primärtherapie und Risikostratifikation Dr. med. Petra Langerbeins Universitätsklinik Köln Deutsche CLL Studiengruppe (DCLLSG) OFFENLEGUNG
REAL LIFE AMBULATORIALE E STUDI CLINICI RANDOMIZZATI NELLA PROGRAMMAZIONE TERAPEUTICA DELLA LEUCEMIA LINFATICA CRONICA.
 REAL LIFE AMBULATORIALE E STUDI CLINICI RANDOMIZZATI NELLA PROGRAMMAZIONE TERAPEUTICA DELLA LEUCEMIA LINFATICA CRONICA Roberta Murru Struttura Complessa Ematologia e Centro Trapianti Presidio Ospedaliero
REAL LIFE AMBULATORIALE E STUDI CLINICI RANDOMIZZATI NELLA PROGRAMMAZIONE TERAPEUTICA DELLA LEUCEMIA LINFATICA CRONICA Roberta Murru Struttura Complessa Ematologia e Centro Trapianti Presidio Ospedaliero
Chronic lymphocytic leukemia. E. Van Den Neste Cliniques UCL Saint-Luc, Brussels Post-ASH meeting January 2015
 Chronic lymphocytic leukemia E. Van Den Neste Cliniques UCL Saint-Luc, Brussels Post-ASH meeting January 2015 Disclosures Travelling to ASH: Roche Consulting services: Janssen Questions in CLL: answers
Chronic lymphocytic leukemia E. Van Den Neste Cliniques UCL Saint-Luc, Brussels Post-ASH meeting January 2015 Disclosures Travelling to ASH: Roche Consulting services: Janssen Questions in CLL: answers
Chronic lymphocytic leukemia
 Chronic lymphocytic leukemia How the Experts Treat Hematologic Malignancies Las Vegas, NV 3/2018 Tanya Siddiqi, MD Assistant Professor City of Hope National Medical Center Duarte, CA DISCLOSURES I am on
Chronic lymphocytic leukemia How the Experts Treat Hematologic Malignancies Las Vegas, NV 3/2018 Tanya Siddiqi, MD Assistant Professor City of Hope National Medical Center Duarte, CA DISCLOSURES I am on
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Update: Chronic Lymphocytic Leukemia
 ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
BENDAMUSTINE + RITUXIMAB IN CLL
 BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
Chronic lymphocytic leukemia
 Chronic lymphocytic leukemia Tanya Siddiqi, MD Assistant Professor City of Hope National Medical Center Duarte, CA How the Experts Treat Hematologic Malignancies Las Vegas, NV 3/2017 Disclosures Speaker
Chronic lymphocytic leukemia Tanya Siddiqi, MD Assistant Professor City of Hope National Medical Center Duarte, CA How the Experts Treat Hematologic Malignancies Las Vegas, NV 3/2017 Disclosures Speaker
Lymphoma 101. Nathalie Johnson, MDPhD. Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University
 Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
Lymphoma 101 Nathalie Johnson, MDPhD Division of Hematology Jewish General Hospital Associate Professor of Medicine, McGill University Disclosures Consultant and Advisory boards for multiple companies
accumulation the blood, marrow, lymph nodes, and spleen.
 Chronic Lymphocytic Leukemia accumulation of mature-appearing appearing lymphocytes in the blood, marrow, lymph nodes, and spleen. CLL cells are: monoclonal l B lymphocytes that express CD19. CD5, and
Chronic Lymphocytic Leukemia accumulation of mature-appearing appearing lymphocytes in the blood, marrow, lymph nodes, and spleen. CLL cells are: monoclonal l B lymphocytes that express CD19. CD5, and
Background. Approved by FDA and EMEA for CLL and allows for treatment without chemotherapy in all lines of therapy
 Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, Chronic Lymphocytic Leukemia. Paolo Ghia
 CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, 2013 Chronic Lymphocytic Leukemia Paolo Ghia CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, 2013
CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, 2013 Chronic Lymphocytic Leukemia Paolo Ghia CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, 2013
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL)
") Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
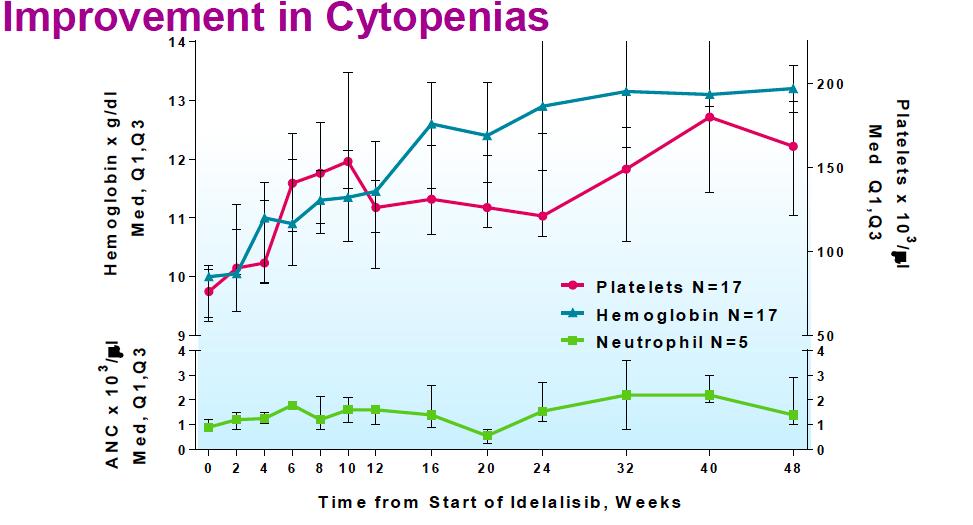
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL
 Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
UNMET NEEDS OF PATIENTS WITH CLL/SLL AND FL. June 6, 2018
 UNMET NEEDS OF PATIENTS WITH CLL/SLL AND FL June 6, 2018 0 PRESENTATION OVERVIEW IN CLL/SLL AND FL: Review patient heterogeneity and its connection to unmet needs Explore unmet needs within the CLL/SLL
UNMET NEEDS OF PATIENTS WITH CLL/SLL AND FL June 6, 2018 0 PRESENTATION OVERVIEW IN CLL/SLL AND FL: Review patient heterogeneity and its connection to unmet needs Explore unmet needs within the CLL/SLL
CLL: future therapies. Dr. Nathalie Johnson
 CLL: future therapies Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck Outline Treatment of relapsed
CLL: future therapies Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck Outline Treatment of relapsed
BR is an established treatment regimen for CLL in the front-line and R/R settings
 Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Treatment Nodal Marginal Zone Lymphoma
 Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
How I treat CLL up front
 How I treat How I treat CLL up front John G. Gribben Institute of Cancer, Queen Mary University of London, Barts and The London School of Medicine and Dentistry, London, United Kingdom Although chronic
How I treat How I treat CLL up front John G. Gribben Institute of Cancer, Queen Mary University of London, Barts and The London School of Medicine and Dentistry, London, United Kingdom Although chronic
UPDATES IN CHRONIC LYMPHOCYTIC LEUKEMIA TANYA SIDDIQI, MD
 UPDATES IN CHRONIC LYMPHOCYTIC LEUKEMIA TANYA SIDDIQI, MD DISCLOSURE Speaker s bureau: Pharmacyclics, Janssen, Seattle Genetics, Astra Zeneca Consultant: Juno therapeutics, Astra Zeneca, BeiGene, Pharmacyclics
UPDATES IN CHRONIC LYMPHOCYTIC LEUKEMIA TANYA SIDDIQI, MD DISCLOSURE Speaker s bureau: Pharmacyclics, Janssen, Seattle Genetics, Astra Zeneca Consultant: Juno therapeutics, Astra Zeneca, BeiGene, Pharmacyclics
Chronic Lymphocytic Leukemia: Prognostic Factors, Supportive Care Issues and Therapeutic Advances
 Chronic Lymphocytic Leukemia: Prognostic Factors, Supportive Care Issues and Therapeutic Advances 2017 Master Class Course John C. Byrd, MD D Warren Brown Chair of Leukemia Research Distinguished University
Chronic Lymphocytic Leukemia: Prognostic Factors, Supportive Care Issues and Therapeutic Advances 2017 Master Class Course John C. Byrd, MD D Warren Brown Chair of Leukemia Research Distinguished University
1. What to test. 2. When to test
 Biomarkers: the triad of questions 1. What to test 2. When to test 3. Who to test Biomarkers: the triad of questions 1. What to test 2. When to test 3. Who to test Impact of CLL biological features on
Biomarkers: the triad of questions 1. What to test 2. When to test 3. Who to test Biomarkers: the triad of questions 1. What to test 2. When to test 3. Who to test Impact of CLL biological features on
A Canadian Perspective on the Management of Chronic Lymphocytic Leukemia
 A Canadian Perspective on the Management of Chronic Lymphocytic Leukemia Douglas A. Stewart, MD, FRCP(C), 1 Christine Chen, MD, MEd, FRCP(C), 2 Laurie H. Sehn, MD, MPH, 3 Chaim Shustik, MD, FRCP(C) 4 1
A Canadian Perspective on the Management of Chronic Lymphocytic Leukemia Douglas A. Stewart, MD, FRCP(C), 1 Christine Chen, MD, MEd, FRCP(C), 2 Laurie H. Sehn, MD, MPH, 3 Chaim Shustik, MD, FRCP(C) 4 1
CLL: Future Therapies. Dr. Anca Prica
 CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
LEUCEMIA LINFATICA CRONICA: TERAPIA DEL PAZIENTE IN RECIDIVA
 CORSO TEORICO-PRATICO PER LA GESTIONE OTTIMALE DEI PAZIENTI AFFETTI DA LINFOMA MANTELLARE, LINFOMA FOLLICOLARE E LEUCEMIA LINFATICA CRONICA Torino, 21-23 Maggio 2018 LEUCEMIA LINFATICA CRONICA: TERAPIA
CORSO TEORICO-PRATICO PER LA GESTIONE OTTIMALE DEI PAZIENTI AFFETTI DA LINFOMA MANTELLARE, LINFOMA FOLLICOLARE E LEUCEMIA LINFATICA CRONICA Torino, 21-23 Maggio 2018 LEUCEMIA LINFATICA CRONICA: TERAPIA
Chronic Lymphocytic Leukemia: Current Concepts
 Review Chronic Lymphocytic Leukemia: Current Concepts EUN-MI YU 1, ADAM KITTAI 2 and IMAD A. TABBARA 1 1 Department of Hematology/ Oncology, George Washington University, Washington, DC, U.S.A.; 2 Department
Review Chronic Lymphocytic Leukemia: Current Concepts EUN-MI YU 1, ADAM KITTAI 2 and IMAD A. TABBARA 1 1 Department of Hematology/ Oncology, George Washington University, Washington, DC, U.S.A.; 2 Department
Management of Chronic Lymphatic Leukemia Beyond conventional therapy
 3 rd Young Hematologists Orientation Program SGPGI Lucknow August 18 th -19 th 218 Management of Chronic Lymphatic Leukemia Beyond conventional therapy Prof. Hari Menon. MD DM Department of Hemato-Oncology
3 rd Young Hematologists Orientation Program SGPGI Lucknow August 18 th -19 th 218 Management of Chronic Lymphatic Leukemia Beyond conventional therapy Prof. Hari Menon. MD DM Department of Hemato-Oncology
Dutch guidelines for diagnosis and treatment of chronic lymphocytic leukaemia 2011
 r e v i e w Dutch guidelines for diagnosis and treatment of chronic lymphocytic leukaemia 2011 A.P. Kater 1,*, S. Wittebol 2, M.E.D. Chamuleau 3, M. van Gelder 4, M.H. J van Oers 1,*, on behalf of the
r e v i e w Dutch guidelines for diagnosis and treatment of chronic lymphocytic leukaemia 2011 A.P. Kater 1,*, S. Wittebol 2, M.E.D. Chamuleau 3, M. van Gelder 4, M.H. J van Oers 1,*, on behalf of the
Brad S Kahl, MD. Tracks 1-21
 I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
L approccio terapeu-co. Maria Rosaria Villa U.O.C. Ematologia P.O. Ascalesi ASLNA1Centro
 L approccio terapeu-co Maria Rosaria Villa U.O.C. Ematologia P.O. Ascalesi ASLNA1Centro DISCLOSURE Nome: Maria Rosaria Cognome: Villa Impiego nell industria farmaceu7ca negli ul7mi 5 anni: NO Interssi
L approccio terapeu-co Maria Rosaria Villa U.O.C. Ematologia P.O. Ascalesi ASLNA1Centro DISCLOSURE Nome: Maria Rosaria Cognome: Villa Impiego nell industria farmaceu7ca negli ul7mi 5 anni: NO Interssi
BHS guidelines for the treatment of chronic lymphocytic leukaemia anno 2012
 4 Practice Guidelines BHS guidelines for the treatment of chronic lymphocytic leukaemia anno 2012 A. Janssens, E. Van Den Neste, W. Schroyens, M. André, A. Van Hoof, V. De Wilde, G. Verhoef, F. Offner,
4 Practice Guidelines BHS guidelines for the treatment of chronic lymphocytic leukaemia anno 2012 A. Janssens, E. Van Den Neste, W. Schroyens, M. André, A. Van Hoof, V. De Wilde, G. Verhoef, F. Offner,
What s on the Horizon for Chronic Lymphocytic Leukemia?
 What s on the Horizon for Chronic Lymphocytic Leukemia? Matthew S. Davids, MD, MMSc Associate Director Center for Chronic Lymphocytic Leukemia Assistant Professor of Medicine Harvard Medical School Dana
What s on the Horizon for Chronic Lymphocytic Leukemia? Matthew S. Davids, MD, MMSc Associate Director Center for Chronic Lymphocytic Leukemia Assistant Professor of Medicine Harvard Medical School Dana
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Chronic Lymphocytic Leukemia. Paolo Ghia
 Chronic Lymphocytic Leukemia Paolo Ghia Complex Karyotype: a novel predictive marker? Thompson PA et al. Cancer 2015 Complex karyotype superseded del(17p) Anderson MA et al. Blood 2017 Ibrutinib and Idela
Chronic Lymphocytic Leukemia Paolo Ghia Complex Karyotype: a novel predictive marker? Thompson PA et al. Cancer 2015 Complex karyotype superseded del(17p) Anderson MA et al. Blood 2017 Ibrutinib and Idela
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
MANTLE CELL LYMPHOMA
 MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo
 Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
BTK Inhibitors and BCL2 Antagonists
 BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
Hematology POCKET GUIDELINE. of Chronic Lymphocytic Leukemia in Belgium. Practical management
 POCKET GUIDELINE Hematology Practical management of Chronic Lymphocytic Leukemia in Belgium 1 2 POCKET GUIDELINE Hematology Practical management of Chronic Lymphocytic Leukemia in Belgium This pocket guideline
POCKET GUIDELINE Hematology Practical management of Chronic Lymphocytic Leukemia in Belgium 1 2 POCKET GUIDELINE Hematology Practical management of Chronic Lymphocytic Leukemia in Belgium This pocket guideline
Welcome & Introductions
 Living with Chronic Lymphocytic Leukemia (CLL) Welcome & Introductions Dr. Brander s slides are available for download at www.lls.org/programs Wednesday, July 12, 2017 1 Living with Chronic Lymphocytic
Living with Chronic Lymphocytic Leukemia (CLL) Welcome & Introductions Dr. Brander s slides are available for download at www.lls.org/programs Wednesday, July 12, 2017 1 Living with Chronic Lymphocytic
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
Patient Profile of CLL in 1L: the importance of appropriate therapy
 Patient Profile of CLL in 1L: the importance of appropriate therapy Pr Loic YSEBAERT Service d Hématologie Institut Universitaire du cancer de Toulouse-Oncopole Toulouse, FRANCE ysebaert.loic@iuct-oncopole.fr
Patient Profile of CLL in 1L: the importance of appropriate therapy Pr Loic YSEBAERT Service d Hématologie Institut Universitaire du cancer de Toulouse-Oncopole Toulouse, FRANCE ysebaert.loic@iuct-oncopole.fr
GVHD & GVL in the lymphoma setting: The case of CLL
 GVHD & GVL in the lymphoma setting: The case of CLL Peter Dreger Dept. Internal Medicine V University of Heidelberg EBMT: SCT for CLL 2000-2010 Update January 2012 allo auto 400 350 300 250 200 150 100
GVHD & GVL in the lymphoma setting: The case of CLL Peter Dreger Dept. Internal Medicine V University of Heidelberg EBMT: SCT for CLL 2000-2010 Update January 2012 allo auto 400 350 300 250 200 150 100
1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes on the next page
 COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
COME HOME Non-Hodgkin pathway development worksheet, v6 September 2014 1. Please review the following table, make any changes you think are necessary and highlight those changes. Feel free to put notes
Short Telomeres Predict Poor Prognosis in Chronic Lymphocytic Leukemia
 Short Telomeres Predict Poor Prognosis in Chronic Lymphocytic Leukemia L. Yang Internal Medicine Resident University of Manitoba Supervisor: Dr. J. Johnston Prognostic factors Clinical course is unpredictable
Short Telomeres Predict Poor Prognosis in Chronic Lymphocytic Leukemia L. Yang Internal Medicine Resident University of Manitoba Supervisor: Dr. J. Johnston Prognostic factors Clinical course is unpredictable
C r h ist s op o h p e h r e R. R F l F ow o er e s, s M D, D M S
 1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
1 Christopher R. Flowers, MD, MS Associate Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University School of Medicine Atlanta, Georgia 2 1 Anyone can get blood cancer One
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Small, mature-appearing appearing
 B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Disclosures I have nothing to disclose. Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center,
B-cell Chronic Lymphoproliferative Disorders of the Blood and Bone Marrow Disclosures I have nothing to disclose. Jeffrey L. Jorgensen, MD, PhD Department of Hematopathology, UT M.D. Anderson Cancer Center,
Lymphoma- Med A-new drugs and treatments
 Lymphoma- Med A-new drugs and treatments Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Disclosures: Roche, Gilead Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Outline Lymphoma- what is
Lymphoma- Med A-new drugs and treatments Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Disclosures: Roche, Gilead Silvia Montoto Lisbon, 19/03/2018 #EBMT18 www.ebmt.or Outline Lymphoma- what is