Emerging immune biomarkers. Athanasios Kotsakis MD, PhD Ast. Professor of Medical Oncology School of Medicine, University of Crete
|
|
|
- Edmund Greene
- 5 years ago
- Views:
Transcription
1 Emerging immune biomarkers Athanasios Kotsakis MD, PhD Ast. Professor of Medical Oncology School of Medicine, University of Crete
2 Disclosure: none
3 Cancer Immunotherapy Immunotherapy, mainly anti PD 1/PD L1 agents have been approved for the treatment of many tumor types such as melanoma, NSCLC, urothelial cancer, SCCHN and others BUT what about Toxicity and Cost?? Avoid toxic effects of the treatment to patients who will not benefit from such a therapy Spare money
4 A biomarker is defined as: European Medicines Agency: Biomarkers are tests that can be used to follow body processes and diseases in humans and animals. They can be used to predict how a patient will respond to a medicine or whether they have, or are likely to develop, a certain disease 1 European Medicines Agency. Accessed March 2, Could be: - prognostic: are biological characteristics that are objectively measured and evaluated to predict the course of a disease or - predictive: is a clinical or biologic characteristic that provides information on the likely benefit from treatment


:1753-1760. 2. Rundle A.")


5 Distinct types of biomarkers Physical features 2,3 Molecular variations 4 Cellular features 5 Histology Molecular Variations image adapted from: com/research education/braf/metastatic melanoma/mutations 1. OECD Policy Paper Accessed October 31, Okonkwo OC et al. Neurology. 2014;83(19): Rundle A. Cancer Epidemiol Biomarkers Prev. 2005;14(1): NCCN. Clinical Practice Guidelines in Melanoma, V Accessed February 11, NCCN. Clinical Practice Guidelines in Oncology-Breast Cancer, V Accessed February 11, Spector N et al. Breast Cancer Res. 2007;9(2): Menni C et al. Diabetes. 2013;62(12):




6 Immune-biomarkers are indicators of immune activity Immune-biomarkers are measures of activity within the tumor microenvironment, differing from established gene mutation biomarkers, such as BRAF and EGFR. As components and regulators of the immune response, immune-biomarkers include: Tumor-infiltrating immune cells Secreted peptides Cell surface proteins Immunosuppressive cells Evaluating multiple immune-biomarkers may provide a more realistic representation of the tumor microenvironment, as well as a more accurate and comprehensive assessment of clinical relevance. 15




7 Exploratory immune-biomarkers New immune-biomarkers are now being investigated across tumor types: The field of immune-biomarkers aims to characterize the ongoing g interactions between the immune system and cancer. 16
, CD4+ (Th cells/cd4+ Tregs), CD8+ (CTLs/CD8+ Tregs), CD20+ (B cells) or FoxP3+ (T regulatory cell marker).")

8 Tumor infiltrating lymphocytes (TILs) TILs are evaluated in 1. Hematoxylin and Eosin stained tissue sections 2. Immunostained for CD3+ (T cells), CD4+ (Th cells/cd4+ Tregs), CD8+ (CTLs/CD8+ Tregs), CD20+ (B cells) or FoxP3+ (T regulatory cell marker). Intratumoral lymphocytes (itils) were defined as intraepithelial mononuclear cells within tumor cell nests or in direct contact with tumor cells and are reported as the percentage of the tumor epithelial nests that contain infiltrating lymphocytes. y Stromal lymphocytes y (stils) are defined as the percentage of tumor stroma area that contains a lymphocytic infiltrate without direct contact to tumor cells.

9 Mandal R., et al JCI Insight. 2016;1(17):e89829
10 Mandal R., et al JCI Insight. 016;1(17):e89829 We find that both HPV+ and HPV HNSCC tumors are among the most highly immune infiltrated cancer types.
11 TILs in SCCHN: Prognostic value Increased levels of TILs (mononuclear cells) Associated with better DFS and DSS (Qiaoshi Xu et al., 2017, Translational Oncology Vol 10, no 1, pp 10-16)
12 TILs in SCCHN : Predictive value Tumor infiltrating lymphocytes predict response to definitive chemoradiotherapy in head and neck cancer High density of CD3 + and CD8 + TILs correlates with better OS, PFS, LFFS, DMFS (Balermpas P et al., 2014,BJC 110, )


13 HPV positive HNSCC had the highest levels of Treg infiltration, with HPV negative HNSCC having the second highest CD56 dim NK cell infiltration ti correlated ltdstrongly with overexpression of the KIR inhibitory receptor genes KIR2DL1 and KIR2DL3
14 higher levels of Treg infiltration were associated with superior OS Could be attributed to the ability of these cells to dampen inflammatory processes required for tumor survival/growth

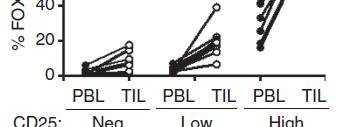
15 intratumoral Treg are more immunosuppressive than circulating Treg
16 Mutational load
17 Haddad R, et al Journal of Clinical Oncology 35, no. 15_suppl (May 2017) Background: Somatic mutational load (ML) is associated with response to anti CTLA 4 and PD 1/ L1 immunotherapies in select tumors, due to formation of neoepitopes not subject to central immune tolerance. Neoepitopes specific to HPV, EBV virus infection are also present in some HNSCC. An IFNγ gene expression profile (GEP) characteristic ti of tumor inflammation is also related ltdto response to anti PD 1/ L1 therapy. This study evaluated relationships between ML and clinical outcome and independent predictive values of ML and GEP in patients with HNSCC treated with pembrolizumab. Methods: Whole exome sequencing (WES) and GEP were assessed in FFPE tumor specimens of patients with HNSCC (KEYNOTE 012; subsets of B1 [PD L1 +, n = 34] and B2 [PD L1 + /, n = 73] cohorts). ML, neoantigen load (NL), HPV/EBV status and clonality were assessed by standard WES analytical methods. GEP score is a weighted sum of normalized expression values of 18 genes. Statistical testing of ML and response, and ML and GEP relationship by HPV/EBV status was prespecified. Results: There were 73 patients identified as HPV and EBV (n = 25 in B1; n = 48 in B2). In HPV and EBV patients in B1 and B2 cohorts, respectively, associations between ML and objective response (OR) (P = and 0.055; AUROC 0.89 and 0.63), and GEP and OR (P = and 0.01; AUROC 0.82 and 0.74) were statistically significant. In combined cohorts of HPV and EBV patients, ML and GEP were significantly associated with OR (P = and 0.002; AUROC 0.70 and 0.76, respectively). ML and GEP were only weakly correlated (r = 0.173). In a joint model, ML was significantly associated with response (p = 0.020) after adjusting for GEP (also significant, p = 0.006). NL and clonality weighted ML were also significantly associated with response (P = and 0.006, respectively). In HPV + or EBV + subjects, OR association was not significant for ML, possibly due to a dominance of viral vs somatic neoepitopes; GEP was significant, ifi likely l due to tumor inflammation. Conclusions: ML and GEP are independently d predictive of response to pembrolizumab in HPV /EBV patients with HNSCC; GEP was predictive regardless of viral status. ML and GEP may have utility in characterizing responses to anti PD 1 therapies and novel cancer regimens in HNSCC. Clinical trial information: NCT
 6009 6009 Background: Somatic mutational load (ML) is associated with response to anti CTLA 4 and PD 1/ L1 immunotherapies in select tumors, due to formation of neoepitopes not")
18 Haddad R, et al Journal of Clinical Oncology 35, no. 15_suppl (May 2017) Background: Somatic mutational load (ML) is associated with response to anti CTLA 4 and PD 1/ L1 immunotherapies in select tumors, due to formation of neoepitopes not subject to central immune tolerance. Neoepitopes specific to HPV, EBV virus infection are also present in some HNSCC. An IFNγ gene expression profile (GEP) characteristic ti of tumor inflammation is also related ltdto response to anti PD 1/ L1 therapy. This study evaluated relationships between ML and clinical outcome and independent predictive values of ML and GEP in patients with HNSCC treated with pembrolizumab. Methods: Whole exome sequencing (WES) and GEP were assessed in FFPE tumor specimens ML and objective of patients response with HNSCC (OR) (KEYNOTE (P = ; subsets and 0.055; of B1 [PD L1 AUROC +, n 0.89 = 34] and B2 0.63), [PD L1 and + /, n GEP = 73] cohorts). ML, and neoantigen OR (P = load (NL), and HPV/EBV 0.01; AUROC status and 0.82 clonality and were 0.74) assessed were statistically by standard WES significant. analytical methods. GEP score is a weighted sum of normalized expression values of 18 genes. Statistical testing of ML and response, and ML and GEP relationship by HPV/EBV status was prespecified. Results: There were 73 patients identified as HPV and EBV (n = 25 ML in B1; and n = GEP 48 in were B2). In only HPV weakly and EBV correlated patients in B1 and B2 cohorts, respectively, associations between ML and objective response (OR) (P = and 0.055; AUROC 0.89 and 0.63), and GEP ML and OR GEP (P = may have and 0.01; utility AUROC in characterizing 0.82 and 0.74) were responses statistically to anti significant. PD 1 therapies In combined and cohorts novel of HPV and EBV patients, ML and GEP were significantly cancer regimens associated in with HNSCC OR (P = and 0.002; AUROC 0.70 and 0.76, respectively). ML and GEP were only weakly correlated (r = 0.173). In a joint model, ML was significantly associated with response (p = 0.020) after adjusting for GEP (also significant, p = 0.006). NL and clonality weighted ML were also significantly associated with response (P = and 0.006, respectively). In HPV + or EBV + subjects, OR association was not significant for ML, possibly due to a dominance of viral vs somatic neoepitopes; GEP was significant, ifi likely l due to tumor inflammation. Conclusions: ML and GEP are independently d predictive of response to pembrolizumab in HPV /EBV patients with HNSCC; GEP was predictive regardless of viral status. ML and GEP may have utility in characterizing responses to anti PD 1 therapies and novel cancer regimens in HNSCC. Clinical trial information: NCT
19 Higher levels of tobacco mutational signature is associated with higher tumor mutational g g g burden, consistent with results reported in NSCLC However, tobacco mutational signature correlated inversely with the degree of T cell infiltrate, immune cell infiltrate, and IFN γ signaling Tumors with high levels of immune cell (HR = 0.66, P = 0.023), T cell (HR = 0.53, P = ) and CD8+ T cell (HR = 0.67, P = 0.029) infiltration were associated with better OS. Increasing level of tobacco mutational signature was associated with poorer survival (P = 0.005)
20 PD-L1 as a predictive biomarker
21 Nivolumab for SCCHN CheckMate 141: Overall Survival OS (%) No. at risk Median OS, mo (95% CI) HR (97.73% CI) P value Nivolumab (n = 240) 7.5 (5.5, 9.1) 0.70 Standard Therapy (n = 121) 5.1 (4.0, 6.0) (0.51, 0.96) 1-year OS rate (95% CI) 36.0% (28.5, 43.4) 16.6% 6% (8.6, Standard Therapy Nivolumab ) Months Nivolumab Standard Therapy 0.01 Adapted from Ferris et al. NEJM 2016; doi: /NEJM0a Abbreviations and references can be found in the speaker notes.
22 Nivolumab for SCCHN CheckMate 141: Overall Survival by PD-L1 Expression PD-L1 Expression 1% No. of Median OS No. of Patient mo (95% Deaths s CI) Nivolumab ( ) Standard Therapy ( ) PD-L1 Expression <1% No. of No. of Median OS Patients Deaths mo (95% CI) Nivolumab ( ) Standard Therapy ( ) Overall Surviv val (% of patien nts) No. at Risk Hazard ratio for death, 0.55 (95% CI, ) Standard Therapy Nivolumab Months Hazard ratio for death, 0.89 (95% CI, ) 30 Nivolumab Standard Therapy Months Nivolumab Standard 61 Therapy Estimates for OS HR for PD-L1 expression levels of 5% and 10% are similar to those for 1%. Adapted from Ferris et al. NEJM 2016; doi: /NEJM0a Abbreviations and references can be found in the speaker notes.
23 HNSCC Cohorts of Nonrandomized, Phase 1b KEYNOTE-012 Trial Biomarker analysis A Phase 1b Study of Pembrolizumab in Patients With HPV-Positive and HPV-Negative Head and Neck Cancer Patient population R/M HNSCC Measurable disease (RECIST v1.1) ECOG PS 0-1 PD-L1 positive (initial cohort) PD-L1 positive or PD-L1 negative (expansion cohort) Initial Cohort B N=60 Pembrolizumab 10 mg/kg q2w Expansion Cohort B2 N=132 Pembrolizumab 200 mg q3w Treat for 24 months or until progression or intolerable toxicity Pre-treatment samples collected for biomarker analyses Pre-treatment biomarker levels were correlated with efficacy outcomes (ORR, PFS, OS; central imaging vendor review) HNSCC = recurrent or metastatic squamous cell carcinoma; ORR = overall response rate; OS = overall survival; PD-L1 = programmed death ligand 1; PFS = progression-free survival; q2w = every 2 weeks; q3w = every 3 weeks; RECIST v1.1 1 = Response Evaluation Criteria In Solid Tumors version Chow LQ et al. J Clin Oncol. 2016;34(15;suppl): abstract For Internal Use Only
24 KEYNOTE-012: Overall Response by PD-L1 Status 1 PD-L1 Status Nonresponders, n Responders, n ORR % (95% CI) P TPS (tumor cells) PD-L1 positive PD-L1 negative (12 26) 26) (10 30) P values based on logistic regression one-sided testing. CI = confidence interval; CPS = combined positive score; ORR = overall response rate; PD-L1 = programmed death ligand 1; TPS = tumor proportion score. 1. Chow LQ et al. J Clin Oncol. 2016;34(15;suppl): abstract For Internal Use Only
25 KEYNOTE-012: Overall Response by PD-L1 Status 1 Incorporation of inflammatory cells improves ability to detect responders PD-L1 Status Nonresponders, n Responders, n ORR % (95% CI) P TPS (tumor cells) PD-L1 positive PD-L1 negative (12 26) 26) (10 30) CPS (either tumor and/or inflammatory cells) PD-L1 positive PD-L1 negative (15 28) (1 19) P values based on logistic regression one-sided testing. CI = confidence interval; CPS = combined positive score; ORR = overall response rate; PD-L1 = programmed death ligand 1; TPS = tumor proportion score. 1. Chow LQ et al. J Clin Oncol. 2016;34(15;suppl): abstract For Internal Use Only
26 KEYNOTE-012: Progression-free Survival by PD-L1 Status 1 og ess o ee Su a by Saus TPS (tumor cells) CPS (tumor and inflammatory cells) 1.00 P = P = Sur rvival Probab bility PD-L1+ PD-L1 Surv vival Probab bility PD-L1+ PD-L Time, days Time, days TPS< TPS CPS< CPS Median (95% CI) PD-L1 positive, 63 days (58 98) PD-L1 negative, 62 days (59 67) P values based on logistic regression one-sided testing. CI = confidence interval; CPS = combined positive score; PD-L1 = programmed death ligand 1; TPS = tumor proportion score. 1. Chow LQ et al. J Clin Oncol. 2016;34(15;suppl): abstract For Internal Use Only Median (95% CI) PD-L1 positive, 64 days (59 98) PD-L1 negative, 60 days (51 66)
27 KEYNOTE-012: Overall Survival by PD-L1 Status 1 TPS (tumor cells) CPS (tumor and inflammatory cells) 1.00 P = P = Survival Prob bability PD-L1+ PD-L1 Survival Prob bability PD-L1+ PD-L Time, days Time, days TPS< TPS CPS< CPS Median (95% CI) PD-L1 positive, 290 days ( ) PD-L1 negative, 246 days ( ) Median (95% CI) PD-L1 positive, 303 days ( ) PD-L1 negative, 151 days (84 247) P values based on logistic regression one-sided testing. CI = confidence interval; CPS = combined positive score; PD-L1 = programmed death ligand 1; TPS = tumor proportion score. 1. Chow LQ et al. J Clin Oncol. 2016;34(15;suppl): abstract For Internal Use Only
28 Challenges to use PD L1 as biomarker: Fluctuation in expression at different time points Variation within tumor tissue Lack of uniformity in cutoff points employed in different trials, in kit and antibodies used for the detection of PD L1 expression Where to look for them: TC, IC or both? Responses in PD L1 negative tumors OR No response even in highly PD L1 positive tumors While there are many doubts about how perfect PD L1 testing is, there is a belief it plays a role for enrichment!!
29 PD-L2 as a predictive biomarker
30
31 Jennifer H. Yearley et al, Clin Cancer Res; 23(12) June 15, 2017
32 KEYNOTE-012: Overall Response by PD-L2 Status 1 PD-L2 expression on tumor and inflammatory cells is predictive of response to pembrolizumab Samples from172 patients were evaluated for PD-L2 expression CPS (tumor and/or inflammatory cells) Nonresponders, Responders, ORR n n %(95% CI) PD-L (15 31) PD-L (4 20) P P values based on logistic regression one-sided testing. CI = confidence interval; CPS = combined positive score; ORR = overall response rate; PD-L2 = programmed death ligand For Internal Use Only

 PD-L1 Negative n ORR % (95% CI) n = 3 PD-L1 /")
 between PD-L1 and PD-L2 expression 33 For Internal Use Only 1.")
 3 0 (0 71) PD-L2 39 10 (3 24) 22 9 (1 29) High")
33 KEYNOTE-012: Correlation of PD-L1, PD-L2, and Response 1 Data suggest that PD-L2 predicts clinical outcome in pembrolizumab treated pts n=172 n = 39 PD-L1+/ PD-L2 n = 22 PD-L1 / PD-L2 n = 108 PD-L1+/ PD-L2+ PD-L1 Positive n ORR % (95% CI) PD-L1 Negative n ORR % (95% CI) n = 3 PD-L1 / PD-L2+ Significant association (P<0.001) between PD-L1 and PD-L2 expression 33 For Internal Use Only 1. Chow LQ et al. J Clin Oncol. 2016;34(15;suppl): abstract PD-L (16 32) 3 0 (0 71) PD-L (3 24) 22 9 (1 29) High response in PD-L1 positive/ PD-L2 positive tumors
34 HPV status t as a predictive biomarker
35
36 Nivolumab for SCCHN CheckMate 141: Overall Survival OS (%) No. at risk Median OS, mo (95% CI) HR (97.73% CI) P value Nivolumab (n = 240) 7.5 (5.5, 9.1) 0.70 Standard Therapy (n = 121) 5.1 (4.0, 6.0) (0.51, 0.96) 1-year OS rate (95% CI) 36.0% (28.5, 43.4) 16.6% 6% (8.6, Standard Therapy Nivolumab ) Months Nivolumab Standard Therapy 0.01 Adapted from Ferris et al. NEJM 2016; doi: /NEJM0a Abbreviations and references can be found in the speaker notes.
37 Nivolumab for SCCHN CheckMate 141: Overall Survival by p16 Status t p16-positive p16-negative No. of No. of Median OS No. of No. of Median OS Patients Deaths mo (95% CI) Patients Deaths mo (95% CI) Nivolumab ( ) Nivolumab (3.0 NA) Standard Therapy ( ) Standard Therapy ( ) Hazard ratio for death, 0.56 (95% CI, 0.32 Hazard ratio for death, 0.73 (95% CI, ) ) patients) Overall Survival (% of Standard Therapy Nivolumab No. at Risk Months Nivolumab Standard Therapy Nivolumab Standard Therapy Months mos appeared longer for patients treated with nivolumab than standard therapy regardless of p16 status Adapted from Ferris et al. NEJM 2016; doi: /NEJM0a Abbreviations and references can be found in the speaker notes.
38 IFN γ signature


39 FOR INTERNAL USE ONLY; NOT TO BE SHARED OR DISTRIBUTED TO ANYONE OUTSIDE THE COMPANY
40 T-Cell Inflamed Phenotype Gene Expression Signatures Predict Benefit from Pembro across Multiple Tumor Types Patients enrolled FFPE tumor in clinical study tissue NanoString Gene expression data RNA Evaluate genes and signatures associated with anti-pd-1 response Collected at baseline prior to receiving anti-pd-1 therapy Transcripts for genes of interest are counted 680 genes on platform immune focused (custom design) six IFN-γ regulated genes with a gene signature panel IFN-γ (6 gene) significantly associated with ORR, PFS (IFN CXCL9, CXCL10, IDO1, HLA-DRA, STAT1 - Nanostring) Consistent data across CRC, Esophageal, Biliary, Anal and Ovarian 40 For Internal Use Only
41 Inflamed-phenotype gene expression signatures to predict benefit from the anti-pd-1 antibody pembrolizumab in PD-L1+ head and neck cancer patients Tanguy Y. Seiwert et al abstr 6017 They investigated 4 multi-gene expression signatures previously described in melanoma and gastric patients (pts). FFPE-extracted RNA was analyzed on the NanoString ncounter system which is being developed as a companion diagnostic Interferon γ γ signature correlated strongly with the previously independently discovered inflamed/mesenchymal HNSCC intrinsic subtype

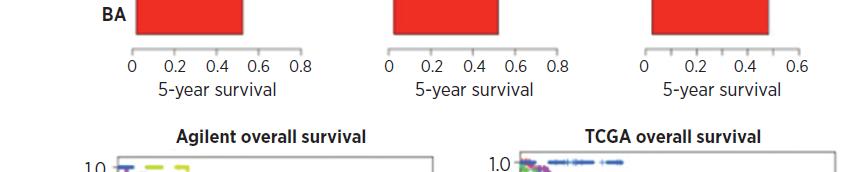
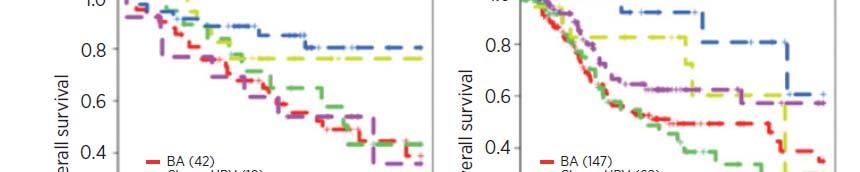
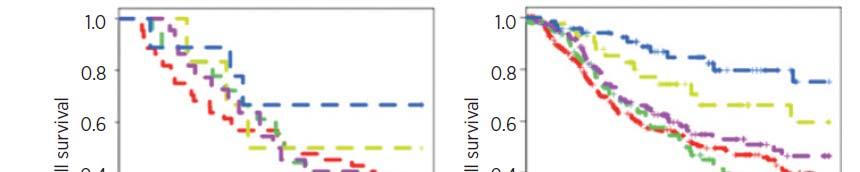
42 IMS subtype is characterized among others by CD8+ T-cell infiltration
43 Seiwert TY et al, Lancet Oncol Jul;17(7): The gene expression composite score provided a positive predictive value of 40% and a negative predictive value of 95% th ti f ti t ith ll i th bi k l t d the proportion of patients with an overall response in the biomarker selected population was nearly double that seen in the trial overall
44 KEYNOTE-012: Progression-free Survival and Overall Survival by IFN- 6-gene esg Signature auescoe Score 1 Progression-free Survival Overall Survival 1.00 IFN- Score < Q1 IFN- Score Q IFN- Score < Q1 IFN- Score Q1 Su urvival Proba ability Su urvival Proba ability Time, days IFN- Score < Q IFN- Score Q Time, days IFN- Score < Q IFN- Score Q Signature score was associated with improved PFS and OS Nonresponder Q1 defined as IFN = interferon; OS = overall survival; PFS = progression-free survival. 1. Chow LQ et al. J Clin Oncol. 2016;34(15;suppl): abstract For Internal Use Only
45
46 Slide 20 Presented By Drew Pardoll at 2015 ASCO Annual Meeting
47 T cell inflamed phenotype (TCIP) defined by a 12 gene chemokine signature (CCL2, CLL3, CLL4, CCL5, CCL8, CCL18, CCL19, CCL21, CXCL9, CXCL10, CXCL11 and CXCL13) was evaluated in a cohort of 134 HNSCC from the University of Chicago and 424 HNSCC samples from TCGA The presence of the TCIP was associated with infiltration of CD8+ cells in a subset of HNSCCs; 21% of HPV negative tumors were TCIP high and 51% of HPV positive tumors were TCIP high. The TCIP high phenotype was associated with mesenchymal subtype and higher prevalence of PD L1 expression, suggesting that this phenotype could represent the sensitivity to anti PD1/PD L1 therapies.
48 Inflamed phenotype correlates with Immune escape mechanisms Presented by T. Seiwert ESMO 2016
49
50 Conclusion Immunotherapy is active in SCCHN Identification of pts who will more likely benefit from ICI Most research is focused in TME Intensive research in this field; PD L1, PD L2, IFN γ gene signature and others have been proposed p The role of peripheral blood?? Lot of suppressive Treg, MDSC subpopulations have been suggested as potential biomarkers for response
51 Thank you
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Predictive Biomarkers for Pembrolizumab. Eric H. Rubin, M.D.
 Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Disclosures. Immunotherapyin Head & NeckCancer. Actual landscape of systemic treatment in HNSCC. Head andneckcanceris an immunogeneic tumor
 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS
 CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker
 Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
ICLIO National Conference
 ICLIO National Conference Immuno-oncology In The Clinic Today Lee Schwartzberg, MD, FACP Executive Director, West Cancer Center Chief, Division of Hematology/Oncology University of Tennessee Health Science
ICLIO National Conference Immuno-oncology In The Clinic Today Lee Schwartzberg, MD, FACP Executive Director, West Cancer Center Chief, Division of Hematology/Oncology University of Tennessee Health Science
Immunotherapy in head and neck cancer and MSI in solid tumors
 Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
News from ASCO. Niven Mehra, Medical Oncologist. Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital
 News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy
: Biomarkers for Immunotherapy") Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Merck ASCO 2015 Investor Briefing
 Merck ASCO 2015 Investor Briefing Forward-Looking Statement This presentation includes forward-looking statements within the meaning of the safe harbor provisions of the U.S. Private Securities Litigation
Merck ASCO 2015 Investor Briefing Forward-Looking Statement This presentation includes forward-looking statements within the meaning of the safe harbor provisions of the U.S. Private Securities Litigation
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Emerging Tissue and Serum Markers
 Emerging Tissue and Serum Markers for Immune Checkpoint Inhibitors Kyong Hwa Park MD, PhD Medical Oncology Korea University College of Medicine Contents Immune checkpoint inhibitors in clinical practice
Emerging Tissue and Serum Markers for Immune Checkpoint Inhibitors Kyong Hwa Park MD, PhD Medical Oncology Korea University College of Medicine Contents Immune checkpoint inhibitors in clinical practice
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies. Eric H. Rubin, MD Merck Research Laboratories
 Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Update on the development of immune checkpoint inhibitors
 Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Carla van Herpen Medical Oncologist Immunotherapyin Head & NeckCancer
 Carla van Herpen Medical Oncologist 01-10-2016 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial,
Carla van Herpen Medical Oncologist 01-10-2016 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial,
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal. Gabriela Sousa Oncologia Médica IPO Coimbra
 O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy in non-small cell lung cancer
 Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Immunotherapy for Breast Cancer Clinical Development
 Immunotherapy for Breast Cancer Clinical Development Laurence Buisseret, MD, PhD Breast Cancer Translational Research Laboratory Institut Jules Bordet Université Libre de Bruxelles (ULB) ESMO preceptorship
Immunotherapy for Breast Cancer Clinical Development Laurence Buisseret, MD, PhD Breast Cancer Translational Research Laboratory Institut Jules Bordet Université Libre de Bruxelles (ULB) ESMO preceptorship
Colorectal Cancer in 2017: From Biology to the Clinics. Rodrigo Dienstmann
 Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Immune Checkpoints. PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich
 Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-028 Study
 Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
New Paradigms for Treatment of. Erminia Massarelli, MD, PHD, MS Clinical Associate Professor
 New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
Recent Advances in Lung Cancer: Updates from ASCO Updates from ESMO, AACR and ASCO
 Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
The head and neck cancer immune landscape and its immunotherapeutic implications
 The head and neck cancer immune landscape and its immunotherapeutic implications Rajarsi Mandal,, Timothy A. Chan, Luc G.T. Morris JCI Insight. 2016;1(17):e89829. https://doi.org/10.1172/jci.insight.89829.
The head and neck cancer immune landscape and its immunotherapeutic implications Rajarsi Mandal,, Timothy A. Chan, Luc G.T. Morris JCI Insight. 2016;1(17):e89829. https://doi.org/10.1172/jci.insight.89829.
Predicting outcome in metastatic breast cancer
 Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
Immunotherapy on the Horizon
 Immunotherapy on the Horizon Andrew L. Coveler Assistant Professor of Medicine, Division of Oncology University of Washington Assistant Member Fred Hutchinson Cancer Research Center Image: NASA.gov 1 2
Immunotherapy on the Horizon Andrew L. Coveler Assistant Professor of Medicine, Division of Oncology University of Washington Assistant Member Fred Hutchinson Cancer Research Center Image: NASA.gov 1 2
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
A biomarker-driven approach for the development of the ICOS agonist antibody, JTX-2011 Heather A. Hirsch
 A biomarker-driven approach for the development of the ICOS agonist antibody, JTX-2011 Heather A. Hirsch On behalf of Jounce Therapeutics JTX-2011 team Immuno-Oncology Biomarkers: Today s Imperatives for
A biomarker-driven approach for the development of the ICOS agonist antibody, JTX-2011 Heather A. Hirsch On behalf of Jounce Therapeutics JTX-2011 team Immuno-Oncology Biomarkers: Today s Imperatives for
Cancer Immunotherapy Patient Forum. for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015
 Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Immunotherapy in breast cancer. Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy
 Immunotherapy in breast cancer Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy Outline Rational for immune-based therapy in breast cancer Immunogenic chemotherapy Targeting immune
Immunotherapy in breast cancer Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy Outline Rational for immune-based therapy in breast cancer Immunogenic chemotherapy Targeting immune
We re Reaching Ludicrous Speed: New Immunotherapy Oncology Medications
 We re Reaching Ludicrous Speed: New Immunotherapy Oncology Medications Adam Peele, PharmD, BCPS, BCOP Oncology Pharmacy Manager Cone Health Disclosures Merck Pharmaceuticals Speaker s Bureau 1 Objectives
We re Reaching Ludicrous Speed: New Immunotherapy Oncology Medications Adam Peele, PharmD, BCPS, BCOP Oncology Pharmacy Manager Cone Health Disclosures Merck Pharmaceuticals Speaker s Bureau 1 Objectives
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
ESMO PRECEPTORSHIP IN IMMUNO-ONCOLOGY
 ESMO PRECEPTORSHIP IN IMMUNO-ONCOLOGY LUGANO, MAY 4-5, 2018 Clinical development in ovarian cancer C. Sessa, CH CONTENT Rationale for immunotherapy in ovarian cancer Clinical data with single agent immune
ESMO PRECEPTORSHIP IN IMMUNO-ONCOLOGY LUGANO, MAY 4-5, 2018 Clinical development in ovarian cancer C. Sessa, CH CONTENT Rationale for immunotherapy in ovarian cancer Clinical data with single agent immune
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
THE SEARCH FOR BIOMARKERS IN BLADDER CANCER
 THE SEARCH FOR BIOMARKERS IN BLADDER CANCER CDDP and IO WORLD ALEJO RODRÍGUEZ-VIDA MD PhD Consultant Medical Oncologist Associate Professor Hospital del Mar, Barcelona November 23 rd 2018 DISCLOSURE OF
THE SEARCH FOR BIOMARKERS IN BLADDER CANCER CDDP and IO WORLD ALEJO RODRÍGUEZ-VIDA MD PhD Consultant Medical Oncologist Associate Professor Hospital del Mar, Barcelona November 23 rd 2018 DISCLOSURE OF
Atezolizumab Is a Humanized Anti-PDL1 Antibody That Inhibits the Binding of PD-L1 to PD-1 and B7.1
 Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Head and Neck Cancer Update Sandro V Porceddu
 Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Innovation in Prevention, Early Detection & Diagnosis of Colorectal Cancer Heidelberg Workshop Session VI, Oncology Pipeline June 6, 2014
 Innovation in Prevention, Early Detection & Diagnosis of Colorectal Cancer Heidelberg Workshop Session VI, Oncology Pipeline June 6, 2014 Bernd Mueller MSD Sharp & Dohme, Germany Normal Immune Surveillance:
Innovation in Prevention, Early Detection & Diagnosis of Colorectal Cancer Heidelberg Workshop Session VI, Oncology Pipeline June 6, 2014 Bernd Mueller MSD Sharp & Dohme, Germany Normal Immune Surveillance:
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Highlights from AACR 2015: The Emerging Potential of Immunotherapeutic Approaches in Non-Small Cell Lung Cancer
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Merck Oncology Overview. The Development of MSI-H Cancer Therapy. Development of Anti-Cancer Drugs Forum Tokyo, Japan, 18, February 2017
 Merck Oncology Overview The Development of MSI-H Cancer Therapy Development of Anti-Cancer Drugs Forum Tokyo, Japan, 18, February 217 Andrew Joe, MD Executive Director, Late Stage Oncology Merck & Co.,
Merck Oncology Overview The Development of MSI-H Cancer Therapy Development of Anti-Cancer Drugs Forum Tokyo, Japan, 18, February 217 Andrew Joe, MD Executive Director, Late Stage Oncology Merck & Co.,
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment
 Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Immunotherapy in NSCLC Pathologist role
 Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
The head and neck cancer immune landscape and its immunotherapeutic implications
 The head and neck cancer immune landscape and its immunotherapeutic implications Rajarsi Mandal, 1,2,3 Yasin Şenbabaoğlu, 4 Alexis Desrichard, 1,3 Jonathan J. Havel, 1,3 Martin G. Dalin, 1,3 Nadeem Riaz,
The head and neck cancer immune landscape and its immunotherapeutic implications Rajarsi Mandal, 1,2,3 Yasin Şenbabaoğlu, 4 Alexis Desrichard, 1,3 Jonathan J. Havel, 1,3 Martin G. Dalin, 1,3 Nadeem Riaz,
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates
 Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Immune Therapy in Clear Cell Ovarian Cancer (ITICC) Hal Hirte Canadian Cancer Clinical Trials Group
 Hal Hirte Canadian Cancer Clinical Trials Group") Immune Therapy in Clear Cell Ovarian Cancer (ITICC) Hal Hirte Canadian Cancer Clinical Trials Group Results of Phase II Study of Durvalumab and Tremelimumab in recurrent clear cell ovarian cancer Trial
Immune Therapy in Clear Cell Ovarian Cancer (ITICC) Hal Hirte Canadian Cancer Clinical Trials Group Results of Phase II Study of Durvalumab and Tremelimumab in recurrent clear cell ovarian cancer Trial
The PD-1 pathway of T cell exhaustion
 The PD-1 pathway of T cell exhaustion SAMO 18.3.2016 Overview T cell exhaustion Biology of PD-1 Mechanism Ligands expressed on tumor cell and on non-tumor cells other receptor pairs Biomarkers for apd-1/pd-l1
The PD-1 pathway of T cell exhaustion SAMO 18.3.2016 Overview T cell exhaustion Biology of PD-1 Mechanism Ligands expressed on tumor cell and on non-tumor cells other receptor pairs Biomarkers for apd-1/pd-l1
Neoplasie della testa e del collo e trattamenti combinati
 Neoplasie della testa e del collo e trattamenti combinati 2 nd Young Sicilian Oncologists Day: Linee Guida AIOM, Appropriatezza e Medicina di precisione Messina 12-13 Ottobre 2017 NERINA DENARO denaro.n@ospedale.cuneo.it
Neoplasie della testa e del collo e trattamenti combinati 2 nd Young Sicilian Oncologists Day: Linee Guida AIOM, Appropriatezza e Medicina di precisione Messina 12-13 Ottobre 2017 NERINA DENARO denaro.n@ospedale.cuneo.it
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Presenter Disclosure Information
 Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
PLENARY SESSION 1: CLINICAL TRIAL DESIGN IN AN ERA OF HORIZONTAL DRUG DEVELOPMENT Industry Perspective
 PLENARY SESSION 1: CLINICAL TRIAL DESIGN IN AN ERA OF HORIZONTAL DRUG DEVELOPMENT Industry Perspective Davy Chiodin, VP - Regulatory Science, QA and Compliance, Acerta Pharma (A Member of the AstraZeneca
PLENARY SESSION 1: CLINICAL TRIAL DESIGN IN AN ERA OF HORIZONTAL DRUG DEVELOPMENT Industry Perspective Davy Chiodin, VP - Regulatory Science, QA and Compliance, Acerta Pharma (A Member of the AstraZeneca
2019 ASCO-SITC. Nektar Therapeutics Investor & Analyst Call. March 1, 2019
 Nektar Therapeutics Investor & Analyst Call March 1, 2019 This presentation includes forward-looking statements regarding Nektar s proprietary drug candidates, the timing of the start and conclusion of
Nektar Therapeutics Investor & Analyst Call March 1, 2019 This presentation includes forward-looking statements regarding Nektar s proprietary drug candidates, the timing of the start and conclusion of
Immunotherapy in lung cancer. Saurabh maji
 Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Fattori predittivi di efficacia ed interpretazione della risposta all immunoterapia. Dott. Matteo Brighenti Oncologia Cremona
 Fattori predittivi di efficacia ed interpretazione della risposta all immunoterapia Dott. Matteo Brighenti Oncologia Cremona AREA DI RICERCA CLINICA EPIDEMIOLOGICA ONCOLOGIA CREMONA mos in 4 phase III
Fattori predittivi di efficacia ed interpretazione della risposta all immunoterapia Dott. Matteo Brighenti Oncologia Cremona AREA DI RICERCA CLINICA EPIDEMIOLOGICA ONCOLOGIA CREMONA mos in 4 phase III
Current experience in immunotherapy for metastatic renal cell carcinoma
 Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current practice, needs and future directions in immuno-oncology research testing
 Current practice, needs and future directions in immuno-oncology research testing Jose Carlos Machado IPATIMUP - Porto, Portugal ESMO 2017- THERMO FISHER SCIENTIFIC SYMPOSIUM Immune Therapies are Revolutionizing
Current practice, needs and future directions in immuno-oncology research testing Jose Carlos Machado IPATIMUP - Porto, Portugal ESMO 2017- THERMO FISHER SCIENTIFIC SYMPOSIUM Immune Therapies are Revolutionizing
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Evan J. Lipson, M.D.
 Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
International Society of Breast Pathology. Immune Targeting in Breast Cancer. USCAP 2017 Annual Meeting
 International Society of Breast Pathology USCAP 2017 Annual Meeting Immune Targeting in Breast Cancer Ashley Cimino-Mathews, MD Assistant Professor of Pathology and Oncology The Johns Hopkins Hospital
International Society of Breast Pathology USCAP 2017 Annual Meeting Immune Targeting in Breast Cancer Ashley Cimino-Mathews, MD Assistant Professor of Pathology and Oncology The Johns Hopkins Hospital
Is There a Future for Immunotherapy in Head and Neck Cancer?
 CME Is There a Future for Immunotherapy in Head and Neck Cancer? Course Director Barbara Ann Burtness, MD Message From the Course Director Full faculty details inside Dear Colleague, The management of
CME Is There a Future for Immunotherapy in Head and Neck Cancer? Course Director Barbara Ann Burtness, MD Message From the Course Director Full faculty details inside Dear Colleague, The management of
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Molecular mechanisms of the T cellinflamed tumor microenvironment: Implications for cancer immunotherapy
 Molecular mechanisms of the T cellinflamed tumor microenvironment: Implications for cancer immunotherapy Thomas F. Gajewski, M.D., Ph.D. Professor, Departments of Pathology and Medicine Program Leader,
Molecular mechanisms of the T cellinflamed tumor microenvironment: Implications for cancer immunotherapy Thomas F. Gajewski, M.D., Ph.D. Professor, Departments of Pathology and Medicine Program Leader,
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Liver and Biliary Tract Cancers Critical Review
 Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
Lung Cancer Update 2016 BAONS Oncology Care Update
 Lung Cancer Update 2016 BAONS Oncology Care Update Matthew Gubens, MD, MS Assistant Professor Chair, Thoracic Oncology Site Committee UCSF Helen Diller Family Comprehensive Cancer Center Disclosures Consulting
Lung Cancer Update 2016 BAONS Oncology Care Update Matthew Gubens, MD, MS Assistant Professor Chair, Thoracic Oncology Site Committee UCSF Helen Diller Family Comprehensive Cancer Center Disclosures Consulting
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Lung Cancer Immunotherapy
 Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
Highlights STOMACH CANCER
 UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria