IMMUNE CHECKPOINT BLOCKADE FOR NSCLC. Marina Chiara Garassino
|
|
|
- Myrtle Weaver
- 5 years ago
- Views:
Transcription

1 IMMUNE CHECKPOINT BLOCKADE FOR NSCLC Marina Chiara Garassino

2 Cells of the Immune System Innate immune system: Involving proteins (chemokines and cytokines) and cells, is considered to be the first line of immune defense and does not generate an antigen-specific response 1,2 Mast cell B cell Adaptive immune system: Mediated by B and T cells is highly specific and capable of generating an antigen-specific response 1,2 Macrophage NK cell DC Basophil γδ T cell Antibodies Induction requires presentation of antigens by cells of the innate immune system Complement protein Eosinophil T cell Neutrophil NKT cell Granulocytes CD4 + cell CD8 + cell Innate Immunity (rapid response) Adaptive Immunity (slow response, memory) Adapted from Dranoff G. 1 DC, dendritic cell; NK, natural killer. 1. Dranoff G. Nat Rev Cancer. 2004;4(1): Janeway CA, et al. Immunobiology: The Immune System in Health and Disease. 6th ed. New York, NY: Garland Science; 2004.

3 The cycle of cancer immunity Chen D & Mellman I, Immunity ,1
:400-404. Fritsch EF, et al. Oncoimmunology.")
4 Mutational Load Creates Neoantigens Stephens PJ, et al. Nature. 2012;486(7403): Fritsch EF, et al. Oncoimmunology. 2014;3:e29311

5 Explanation of the Molecular Mechanisms of Checkpoint Inhibitors and Other Key Emerging Immunologic Strategies Chen L, et al. Nat Rev Immunol. 2013;13(4):
:227-242.")
6 Chen L, et al. Nat Rev Immunol. 2013;13(4): Co-Signalling in T cells



7 Anti-cancer immunity in humans is segregated into three main phenotypes Immune-excluded Immune-desert Inflamed
8 Anti-cancer immunity in humans is segregated into three main phenotypes Immune-excluded Clinical responses to immunotherapy uncommon Immune-desert Non-inflamed tumor, will not respond to immunotherapy Inflamed Tumors most likely to respond to immunotherapy Can we increase the patient population that responds to Immunotherapy?

9 What is a PDL1 Positive Tumor? Atezolizumab Durvalumab 25% / 90%

.")
 of 4 assay are analitically similar for tumour cel,")
10 Blueprint PD-L1 IHC Assay Comparison Project Partnership between industry and academia to provide information on analytical correlation of 4 PD-L1assays. Aim: compare analytical staining factors reported as percentages of stained cells TC and IC between four PD-L1 IHC systems (22 C3, 28-8, SP142, SP263). Results and Conclusions Mean Tumour Proportion score (TPS per case based on three readers Data points represent the mean score from three pathologist for each assay on each case 3 (22C3, 28-8 and SP 263) of 4 assay are analitically similar for tumour cel, staining Methods: assessment 39 sample of NSCLC stained with all four investigational use only assays and assessed by 3 trained pathologists from the two diagnostic companies (2 Ventana/Roche and 1 Dako/Agilent).
 can achieve an analytical performance close to PD-L1 assays in a set of NSCLC cases 22C3, 28-8 and SP263 assays highly")
 LDTs concordant as compared to reference assays for tumor cell staining Methods: 41 resected NSCLC selected to have various expression levels of PD-L1 IHC performed in 7 centers (3 with Dako AS")
11 Multicentric French harmonization study for PD-L1 IHC testing in non-small cell lung cancer Aim: To evaluate the analytical correlation between 28-8, 22C3 and SP263 PD-L1 assays across various centers Results and Conclusions To determine if laboratory developed tests (LDT) can achieve an analytical performance close to PD-L1 assays in a set of NSCLC cases 22C3, 28-8 and SP263 assays highly concordant (51.8%) LDTs concordant as compared to reference assays for tumor cell staining Methods: 41 resected NSCLC selected to have various expression levels of PD-L1 IHC performed in 7 centers (3 with Dako AS Link 48, 2 with Ventana Benchmark Ultra and 2 with Leica Bond III) 22C3, 28-8, E1L3N, SP142, SP263 clones used in each center either as assays on dedicated platform (22C3, 28-8, SP263) or LDT
12 First Line treatment
13
14
15
16
17
18


 PD-L1 expression Secondary Outcome Measures: OS, PFS, disease-related symptom improvement: in all subjects with any")

19 CA : nivolumab monotherapy in chemotherapy-naïve patients CheckMate 026: Nivolumab monotherapy N=1325 Key Inclusion Criteria Stage IV or recurrent NSCLC No prior systemic anticancer therapy Measurable disease per RECIST 1.1 Tumor PD-L1+ ( 1% by IHC) ECOG PS 1 No known EGFR/ALK mutations sensitive to available targeted inhibitor therapy No untreated CNS metastases No autoimmune disease R Nivolumab 3 mg/kg IV Q2W Optional Crossover* Squamous NSCLC Gemcitabine + Cisplatin Gemcitabine + Carboplatin Paclitaxel + Carboplatin Non-Squamous NSCLC Pemetrexed + Cisplatin Pemetrexed + Carboplatin Until disease progression or unacceptable toxicity Start Date: March 2014 Estimated Study Completion Date: January 2018 Primary Completion Date: July 2016 Status: Ongoing, not recruiting Study Sponsor: Bristol-Myers Squibb Primary Outcome Measures: PFS in subjects with strong (ie, 5%) PD-L1 expression Secondary Outcome Measures: OS, PFS, disease-related symptom improvement: in all subjects with any PD-L1 tumor expression; OS, ORR, DOR and TTR: in subjects with strong (ie, 5%) PD-L1 expression * Permitted if crossover eligibility criteria met, including progression confirmed by independent radiology review Investigator s choice of chemotherapy administered in 3-week cycles up to a maximum of 6 cycles of IV injection until disease progression, unacceptable toxicity, or completion of 6 cycles, whichever comes first. Please refer to the Oncology Clinical Trials Platform for the most up-to-date clinical trial information. Abbreviations and references can be found in the speaker notes. LOCAL APPROVAL MAY BE REQUIRED BEFORE EXTERNAL USE. REFER TO LOCAL GUIDELINES.
20 CA : nivolumab monotherapy in chemotherapy-naïve patients OS (%) PFS (%) OS and PFS (in Patients With 5% PD-L1+) % in the chemotherapy arm had subsequent nivolumab therapy 43.6% in the nivolumab arm had subsequent systemic therapy Chemotherapy All randomized patients ( 1% PD-L1+): HR=1.07 (95% CI: 0.86, 1.33) Nivolumab No. of patients at risk: Months Nivolumab Chemotherapy Nivolumab Chemotherapy Months Nivolumab (n = 211) LOCAL APPROVAL MAY BE REQUIRED BEFORE EXTERNAL USE. REFER TO LOCAL GUIDELINES. Chemotherapy (n = 212) Median PFS, months (95% CI) 4.2 (3.0, 5.6) 5.9 (5.4, 6.9) 1-year PFS rate, % HR=1.15 (95% CI: 0.91, 1.45), P= Median OS, months (95% CI) 14.4 (11.7, 17.4) 13.2 (10.7, 17.1) 1-year OS rate, % Adapted from Socinski M, et al. Oral presentation at ESMO Abstract LBA7. Abbreviations, references and additional footnotes can be found in the speaker notes HR=1.02 (95% CI: 0.80, 1.30)
: HR=1.07 (95% CI: 0.86, 1.33) Nivolumab 0 0 3 6 9 12 15 18 21 24 27 30 No.")
21 CA : nivolumab monotherapy in chemotherapy-naïve patients OS (%) PFS (%) OS and PFS (in Patients With 5% PD-L1+) % in the chemotherapy arm had subsequent nivolumab therapy 43.6% in the nivolumab arm had subsequent systemic therapy Chemotherapy All randomized patients ( 1% PD-L1+): HR=1.07 (95% CI: 0.86, 1.33) Nivolumab No. of patients at risk: Months Nivolumab Chemotherapy Nivolumab Chemotherapy Months Nivolumab (n = 211) Chemotherapy (n = 212) Median PFS, months (95% CI) 4.2 (3.0, 5.6) 5.9 (5.4, 6.9) 1-year PFS rate, % HR=1.15 (95% CI: 0.91, 1.45), P= Median OS, months (95% CI) 14.4 (11.7, 17.4) 13.2 (10.7, 17.1) 1-year OS rate, % HR=1.02 (95% CI: 0.80, 1.30) Adapted from Socinski M, et al. Oral presentation at ESMO Abstract LBA7. Abbreviations, references and additional footnotes can be found in the speaker notes. LOCAL APPROVAL MAY BE REQUIRED BEFORE EXTERNAL USE. REFER TO LOCAL GUIDELINES. 75
22 Total exome mutations (mutations/mb) CA : nivolumab monotherapy in chemotherapy-naïve patients exploratory TMB analysis Total Exome Mutations vs Genes in FoundationOne Panel* FoundationOne panel* (mutations/mb) Samples from the TMB analysis in CheckMate 026 were not tested at Foundation Medicine; however, an exploratory in silico analysis (i.e. virtual bioinformatic approach) evaluating 315 genes in the FoundationOne panel suggested a correlation with total exome mutations *Based on in silico analysis filtering on 315 genes in FoundationOne comprehensive genomic profile (Foundation Medicine, Inc, Cambridge, MA, USA) Adapted from Peters S, et al. Oral presentation at AACR. 2017_CT082. Abbreviations, references and additional footnotes can be found in the speaker notes. LOCAL APPROVAL MAY BE REQUIRED BEFORE EXTERNAL USE. REFER TO LOCAL GUIDELINES. 87
23 CA : nivolumab monotherapy in chemotherapy-naïve patients exploratory TMB analysis Progression-free survival (%) PFS by Tumor Mutation Burden Subgroup High TMB Low/medium TMB Median PFS, months (95% CI) Nivolumab n = (5.1, NR) Chemotherapy n = (4.2, 8.5) HR = 0.62 (95% CI: 0.38, 1.00) Median PFS, months (95% CI) Nivolumab n = (2.8, 5.4) Chemotherapy n = (5.5, 8.6) HR = 1.82 (95% CI: 1.30, 2.55) Nivolumab Months No. at Risk Nivolumab Chemotherapy Chemotherapy Chemotherapy Nivolumab Months Adapted from Peters S, et al. Oral presentation at AACR. 2017_CT082. Abbreviations, references and additional footnotes can be found in the speaker notes. LOCAL APPROVAL MAY BE REQUIRED BEFORE EXTERNAL USE. REFER TO LOCAL GUIDELINES. 93
24 CA : nivolumab monotherapy in chemotherapy-naïve patients exploratory TMB analysis OS (%) OS by Tumor Mutation Burden Subgroup High TMB Low/medium TMB Nivolumab n = 47 Chemotherapy n = 60 Nivolumab n = 111 Chemotherapy n = No. at Risk Nivolumab Chemotherapy 0 Median OS, months (95% CI) 68% received nivolumab as crossover and/or post-study treatment 18.3 (11.4, NR) 18.8 (11.3, NR) HR = 1.10 (95% CI: 0.64, 1.88) 1-y OS rate = 64% vs 60% Chemotherapy Nivolumab Months Median OS, months (95% CI) 55% received nivolumab as crossover and/or post-study treatment 12.7 (9.9, 16.1) 13.2 (9.5, 15.2) HR = 0.99 (95% CI: 0.71, 1.40) 1-y OS rate = 54% vs 53% Months Chemotherapy Nivolumab Adapted from Peters S, et al. Oral presentation at AACR. 2017_CT082. Abbreviations, references and additional footnotes can be found in the speaker notes. LOCAL APPROVAL MAY BE REQUIRED BEFORE EXTERNAL USE. REFER TO LOCAL GUIDELINES. 95
25 CA : nivolumab monotherapy in chemotherapy-naïve patients exploratory TMB analysis PFS (%) PFS by TMB Subgroup and PD-L1 Expression 100 Nivolumab Arm 100 Chemotherapy Arm 75 High TMB, PD-L1 50% No. at Risk High TMB, PD-L1 50% High TMB, PD-L1 1 49% 25 Low/medium TMB, PD-L1 50% 0 Low/medium TMB, PD-L1 50% High TMB, PD-L1 1 49% Low/medium TMB, PD-L1 1 49% Months Low/medium TMB, PD-L1 1 49% High TMB, PD-L1 1 49% Low/medium TMB, PD-L1 50% Months Low/medium TMB, PD-L1 1 49% High TMB, PD-L1 50% Adapted from Peters S, et al. Oral presentation at AACR. 2017_CT082. Abbreviations, references and additional footnotes can be found in the speaker notes. LOCAL APPROVAL MAY BE REQUIRED BEFORE EXTERNAL USE. REFER TO LOCAL GUIDELINES. 99


26 CheckMate 227: Nivolumab monotherapy or in combination with ipilimumab or chemotherapy A Phase 3 Study of Nivolumab and Nivolumab in Combination with Ipilimumab or Chemotherapy Versus Chemotherapy in Subjects With Stage IV NSCLC N=2220 Key Inclusion Criteria Stage IV or recurrent NSCLC No prior systemic therapy for advanced disease PD-L1 IHC testing with results ECOG PS 1 EGFR WT and ALK negative CNS metastases permitted if adequately treated 2 weeks prior to randomization Stratification Factor Histology (SQ versus NSQ) PD-L1+ ( 1%) Randomize 1:1:1 PD-L1- (<1%) Nivolumab monotherapy 240 mg Q2W Nivolumab 3 mg/kg Q2W + Ipilimumab 1 mg/kg Q6W Chemotherapy Nivolumab 3 mg/kg Q2W + Ipilimumab 1 mg/kg Q6W Nivolumab 360 mg Q3W + Chemotherapy Start Date: August 2015 Estimated Completion Date: December 2020 Estimated Primary Completion Date: January 2018 Status: Recruiting Sponsor: Bristol-Myers Squibb Chemotherapy Primary Endpoint: OS and PFS Secondary Endpoints: ORR, disease-related symptom improvement by week 12 Adapted from Socinski, et al. Presentation at ESMO. 2016_LBA7. Please refer to the Oncology Clinical Trials Platform for the most up-to-date clinical trial information. Abbreviations, references and additional footnotes can be found in the speaker notes. 107 LOCAL APPROVAL MAY BE REQUIRED BEFORE EXTERNAL USE. REFER TO LOCAL GUIDELINES.

27 Chemotherapy Enhances Anti-Cancer Immune Response: Rational Partner for Immunotherapy Increasing T-cell penetrance in the tumor Eliminating immunosuppressive cells: T-regulatory cells Enhancing effector T-cell function Enhancing maturation and activation of dendritic cells toward antigen presentation Improving recognition of tumor antigens by T-cell Inducing immunogenic cell death Eliminating immunosuppressive cells: T-regs, myeloid-derived suppressor cells, M2 macrophages
28
29
30
31
32
33
34
35
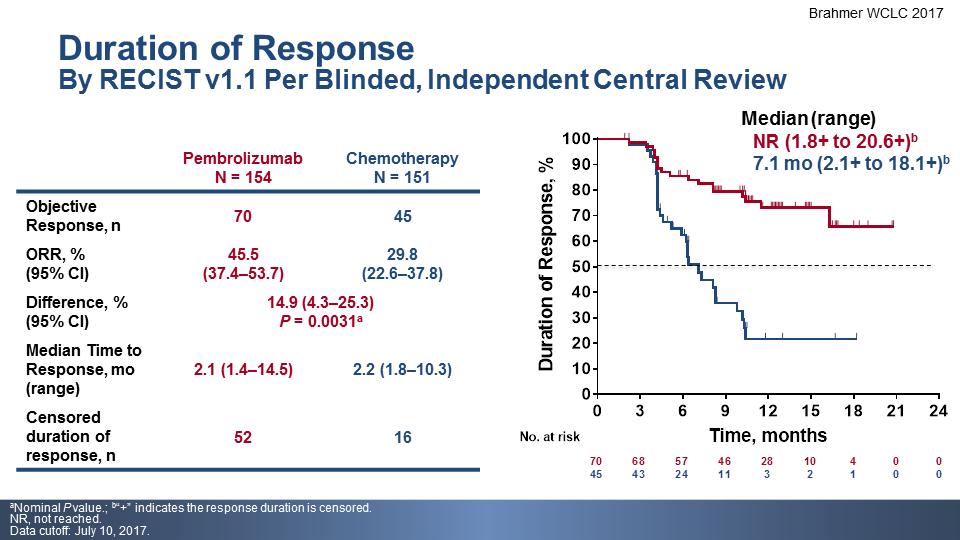
36 O S, % O S, % Plus chemotherapy in NSCLC Keynote -024 Keynote -021 G All NSCLC Histologies PD-L1 TPS 50% Median OS Pembro: 30 months Chemo: 14.2 months HR 0.63 (95%CI, ) Non-squamous NSCLC Any PD-L1 TPS Median OS Pembro +PC: NR Chemo: 20.9 months HR 0.59 (95%CI, ) % 54.8% 51.5% 34.5% N o. a t ris k T im e, m o n th s P em bro C h e m o N o. a t r is k Median (95% CI) NR (22.8 mo NR) 20.9 mo (14.9 NR) T im e, m o n th s 18-mo rate 70% 56%
37 Survival follow-up IMpower150 study design Maintenance therapy (no crossover permitted) Stage IV or recurrent metastatic non-squamous NSCLC Chemotherapy-naive a Tumour tissue available for biomarker testing Any PD-L1 IHC status Stratification factors: Sex PD-L1 IHC expression Liver metastases N = 1202 R 1:1:1 Arm A Atezolizumab b + Carboplatin c + Paclitaxel d 4 or 6 cycles Arm B Atezolizumab b + Carboplatin c + Paclitaxel d + Bevacizumab e 4 or 6 cycles Arm C (control) Carboplatin c + Paclitaxel d + Bevacizumab e 4 or 6 cycles Atezolizumab b Atezolizumab b + Bevacizumab e Bevacizumab e Treated with atezolizumab until PD by RECIST v1.1 or loss of clinical benefit AND/OR Treated with bevacizumab until PD by RECIST v1.1 The principal question is to assess whether the addition of atezolizumab to Arm C provides clinical benefit a Patients with a sensitising EGFR mutation or ALK translocation must have disease progression or intolerance of treatment with one or more approved targeted therapies. b Atezolizumab: 1200 mg IV q3w. c Carboplatin: AUC 6 IV q3w. d Paclitaxel: 200 mg/m 2 IV q3w. e Bevacizumab: 15 mg/kg IV q3w. Reck M, et al. IMpower150 PFS analysis Presented at ESMO IO 2017
38 INV-assessed PFS in ITT-WT (Arm B vs Arm C) Arm B: atezo + bev + CP Arm C: bev + CP HR, (95% CI: 0.517, 0.737) P < Minimum follow-up: 9.5 mo Median follow-up: ~15 mo 6.8 mo (95% CI: 6.0, 7.1) 8.3 mo (95% CI: 7.7, 9.8) INV, investigator. Data cutoff: September 15, 2017 Reck M, et al. IMpower150 PFS analysis Presented at ESMO IO 2017
39 INV-assessed PFS in ITT-WT (Arm B vs Arm C) Arm B: atezo + bev + CP Arm C: bev + CP 67% 56% 37% Minimum follow-up: 9.5 mo Median follow-up: ~15 mo 18% INV, investigator. Data cutoff: September 15, 2017 Reck M, et al. IMpower150 PFS analysis Presented at ESMO IO 2017
40 INV-assessed PFS in Teff-high WT (Arm B vs Arm C) Landmark PFS, % Arm B: atezo + bev + CP Arm C: bev + CP 6-month 72% 57% 12-month 46% 18% HR, (95% CI: 0.377, 0.675) P < Minimum follow-up: 9.5 mo 6.8 mo (95% CI: 5.9, 7.4) 11.3 mo (95% CI: 9.1, 13.0) INV, investigator. Data cutoff: September 15, 2017 Reck 50 M, et al. IMpower150 PFS analysis Presented at ESMO IO 2017
41

42
43
44 Conclusions 1 line For PD-L1>50% pembro is the standard of care For PD-L1<50% chemo is the standard of care The use of TMB COULD be important for defining a further subset Starting with IO seems the better strategy First line could rapidly change in the next months in combination with anti CTLA4 and chemotherapy We will have a problem in sequencing the right treatment for the right patients Patient empowerment will be crucial
45 Second line
46 Three drugs approved Nivolumab Pembrolizumab (PD-L1>1%) Atezolizumab

47 KEYNOTE-010: Pembrolizumab vs docetaxel Herbst RS, Presented December 20, 2015
48 KEYNOTE-010: Pembrolizumab vs docetaxel: OS Time (months) Grade 3 5 treatment-related adverse events were less common with pembrolizumab than with docetaxel: 13% of patients given 2 mg/kg, 16% given10 mg/kg, and 35% of patients given docetaxel). Herbst RS, Lancet 2016; 387:
49 OS (%) OS (%) Nivolumab VERSO docetaxel OS (3 anni di follow-up) CheckMate 017 (SQ NSCLC) Nivolumab (n = 135) Docetaxel (n = 137) HR (95% CI): 0.62 (0.48, 0.80) CheckMate 057 (non-sq NSCLC) Nivolumab (n = 292) Docetaxel (n = 290) HR (95% CI): 0.73 (0.62, 0.88) y OS = 24% 2-y OS = 8% 3-y OS = 6% Months No. of patients at risk 1-y OS = 42% Δ18% 2-y OS = 23% Δ15% Nivolumab Docetaxel CI = confidence interval; HR = hazard ratio 3-y OS = 16% Δ10% Months No. of patients at risk Nivolumab Docetaxel Δ12% 1-y OS = 39% y OS = 51% 2-y OS = 16% 2-y OS = 29% Δ13% 3-y OS = 9% 3-y OS = 18% Δ9%
50 Overall survival (%) Overall survival (%) Overall survival (%) CHECKMATE-057 study: OS Nivolumab vs docetaxel 100 1% PD-L1 expression 100 5% PD-L1 expression % PD-L1 expression 90 mos (mo) 90 mos (mo) 90 mos (mo) Nivolumab Docetaxel Nivolumab Docetaxel Nivolumab 19.9 Docetaxel Nivolumab Docetaxel Nivolumab Docetaxel Nivolumab Docetaxel 10 0 HR (95% CI) (0.43, 0.79) Time (months) 10 0 HR (95% CI) (0.30, 0.62) Time (months) 10 0 HR (95% CI) (0.27, 0.58) Time (months) Borghaei H, et al. N Engl J Med 2015;373: (suppl appendix)


51 Barlesi F et al, Annals of Oncology (2016) 27 (6): /annonc/mdw435; adapted from ESMO 2016 presentation available at ; last access 7/11/2016
52 Barlesi F et al, Annals of Oncology (2016) 27 (6): /annonc/mdw435; adapted from ESMO 2016 presentation available at ; last access 7/11/2016
53 Barlesi F et al, Annals of Oncology (2016) 27 (6): /annonc/mdw435; adapted from ESMO 2016 presentation available at ; last access 7/11/2016
54 Barlesi F et al, Annals of Oncology (2016) 27 (6): /annonc/mdw435; adapted from ESMO 2016 presentation available at ; last access 7/11/2016
55 Barlesi F et al, Annals of Oncology (2016) 27 (6): /annonc/mdw435; adapted from ESMO 2016 presentation available at ; last access 7/11/2016


56 Landmark 2-year overall survival in OAK Overall survival (OS) in ITT850 LTS, long-term survivors. a 27 atezolizumab- and 49 docetaxel-arm patients were censored prior to 24 months and excluded from this analysis. Data cutoff: 23 January, Satouchi, et al. WCLC 2017
57 OS (%) OS (%) Chechmate 057 (Nivolumab) Niv o Doc 1% PD-L1 expression level Median OS (mo) Nivo 17.2 Doc HR (95% CI)=0.59 (0.43, 0.82) OS by PD-L1 expression: <1% PD-L1 expression level Median OS(mo) Nivo 10.4 Doc Niv o 20 Doc HR 10(95% CI)=0.90 (0.66, 1.24) Time (months) > % 1 PD-L1 HR 0.59 < % 1 PD-L1 HR 0.90 Keynote 10 (Pembrolizumab).Rizvi NA, et al. Lancet Oncol 2015 R Herbst et al. Lancet 2016 Barlesi, et al. ESMO 2016 OAK Trial (Atezolizumab) TC3 or IC3 HR: 0.41 TC0 and IC0% HR: 0.75 PD-L1 > 50% HR: 0.53 PD-L1 < 1% HR: 0.76 In the II line setting, do we really select patients according a more favorable HR? Courtesy of C. Bennati
58 Duration
59 PFS (%) CM 152- PFS From Randomization a Median, months (95% CI) PFS rate, % 6-month 1-year Continuous tx NR (NR) year tx b 10.3 (6.4, 15.2) HR: 0.42 (95% CI: 0.25, 0.71) No. at risk Continuous tx 1-year tx Time post-randomization (months) a Patients who did not have PD at randomization; minimum/median follow-up time post-randomization, 10.0/14.9 months b With optional retreatment allowed at PD NR = not reached; tx = treatment
 100 SD Continuous tx Median, months (95% CI) NR (5.6, NA) 1-year tx b 9.6 (4.5, 12.6) HR: 0.44 (95% CI: 0.17, 1.09) 80 80 60 60 40 40 20 20 0 0 3 6 9 12 15 18 21 24 No.")
60 PFS (%) PFS (%) Same for RP and SD 100 CR/PR Continuous tx 1-year tx b,c Median, months (95% CI) NR (NR) 10.6 (4.8, NA) HR: 0.45 (95% CI: 0.24, 0.85) 100 SD Continuous tx Median, months (95% CI) NR (5.6, NA) 1-year tx b 9.6 (4.5, 12.6) HR: 0.44 (95% CI: 0.17, 1.09) No. at risk Time post-randomization (months) Continuous tx year tx Time post-randomization (months)
61 OS (%) Do not stop the treatment OS Median, months (95% CI) 6-month OS rate, % 1-year Continuous tx NR (NR) year tx b 23.2 (23.2, NA) HR: 0.63 (95% CI: 0.33, 1.20) No. at risk Continuous tx 1-year tx Time post-randomization (months) a Patients who did not have PD at randomization; minimum/median follow-up time post-randomization, 10.0/14.9 months b With optional retreatment allowed at PD
62 Change in target lesion size from randomization (%) Tumor Burden Change of Target Lesions in Retreated Patients Tumor burden change in target lesions following retreatment a,b 100 Type of PD n (%) Target lesions only 12 (35) Non-target lesions only 1 (3) New lesions only 14 (41) 0 Target lesions and new lesions 4 (12) 20 Non-target lesions and new lesions 1 (3) 40 Target lesions, non-target lesions, and new lesions 2 (6) Start of retreatment % change truncated to 100% Days since randomization a Patients with PD in target lesions only; b n = 11: 1 patient without further assessment after retreatment start was excluded 75
63 FUTURE
64 Resistances Innate resistance: non responders from the beginning Adaptative resistance Progressing during the treatment
65 Innate resistance Low mutational burden Associated genes to MHC I (es. B2 microglobulina) e MHC II HLA-loss IPRES (innate anti PD-1 resistance) signature trascrittomica correlate alla EMT JAK1/2 mutations IFNγ IFNγ signalling alterations PTEN loss/ PI3K
66 Tumors Use Complex, Overlapping Mechanisms to Evade and Suppress the Immune System 3 2 Priming and Activation CD28/B7.1, CD137/CD137L OX40/OX40L, CD27/CD70 HVEM, GITR, IL-2, IL-12 CTLA4/B7.1 PD-L1/PD-1 PD-L1/B7.1 Prostaglandins Cancer antigen presentation TNF-, IL-1 IFN-, CD40L/CD40 CDN, ATP HMGB1, TLR IL-10, IL-4, IL-13 Lymph node Tumour Stimulatory factors Blood vessel Trafficking of T cells to tumours CX3CL1, CXCL9, CXCL1 CCL5 Infiltration of T cells into tumours LFA1/ICAM1 Selectins VEGF Endothelin-B receptor Recognition of cancer cells by T cells T cell receptor Reduced pmhc on cancer cells Release of cancer cell antigens Immunogenic cell death Tolergenic cell death Inhibitors Killing of cancer cells IFN-, T-cell granule content TIM-3/phospholipids PD-L1/PD-1 PD-L1/B7.1 IDO TGF- BTLA VISTA LAG-3 Arginase MICA/MICB B7-H4 7 Chen DS and Mellman I. Immunity Jul 25;39(1):1-10.
 Routy JP, et al. Int J Tryptophan Res.")
67 Kynurenine Pathway IFNgamma AHR (Anche il recettore della diossina) Routy JP, et al. Int J Tryptophan Res. 2016;9:67-77.
68 Kynurenine Pathway IFNgamma AHR (Anche il recettore della diossina) Routy JP, et al. Int J Tryptophan Res. 2016;9:67-77.
69 Percentage Change in Target Lesions Epacadostat Plus Pembrolizumab Phase 1/2 Advanced NSCLC (Patients With 0 2 Prior Lines of Treatment) ORR=14/36 (39%): 2 CRs (6%), 12 PRs (33%) TPS, tumor proportion score Gangadhar TC, et al. J Clin Oncol. 2017;35(Suppl 4): Abstract 9014.
70 Practical conclusions 1. Test for PD-L1 (with the right antibody) 2. For patients PD-L1 (TPS)>50% pembro represents the standard of care (INFLAMED) for first line treatment 3. Stay tuned for 1 lines (look KN189, CM226, Mystic, IMPOWER 150) and critically «think» to the right sequence 4. Combinations could be the future for IMMUNE EXCLUDED and IMMUNE DESERT 5. For second line IO represents «a» standard of care 6. Kanyurenine pathway seem to be promising in the treatment of NSCLC 7. Multiple other targets are now under investigation
71 Thank you very grazie
Clinical Need and diagnostic challenge-the upcoming landscape of checkpointinhibitors
 Clinical Need and diagnostic challenge-the upcoming landscape of checkpointinhibitors ESP/ESMO Marina Chiara GARASSINO Amsterdam 2017 September, 4th 29 European Congress of Pathology Disclosures BMS ROCHE
Clinical Need and diagnostic challenge-the upcoming landscape of checkpointinhibitors ESP/ESMO Marina Chiara GARASSINO Amsterdam 2017 September, 4th 29 European Congress of Pathology Disclosures BMS ROCHE
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018
 Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER
 PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal. Gabriela Sousa Oncologia Médica IPO Coimbra
 O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
Immunoterapia di 1 linea Evidenze e Prospettive Future
 Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Non-Small Cell Lung Cancer Webinar. Thursday, September 13, p.m. EDT
 Non-Small Cell Lung Cancer Webinar Thursday, September 13, 2018 1 2 p.m. EDT 1 2 Webinar Faculty Julie R. Brahmer, MD Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Patrick Forde, MD Johns
Non-Small Cell Lung Cancer Webinar Thursday, September 13, 2018 1 2 p.m. EDT 1 2 Webinar Faculty Julie R. Brahmer, MD Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Patrick Forde, MD Johns
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Recent Advances in Lung Cancer: Updates from ASCO Updates from ESMO, AACR and ASCO
 Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
Alessandro Inno. IRCCS Ospedale Sacro Cuore Don Calabria Negrar, Verona
 GRUPPO C Coordinatore: Diego Signorelli Ruolo dei checkpoint inhibitors nelle neoplasie polmonari: le evidenze scientifiche e l inserimento dei checkpoint inhibitors nell algoritmo decisionale del NSCLC
GRUPPO C Coordinatore: Diego Signorelli Ruolo dei checkpoint inhibitors nelle neoplasie polmonari: le evidenze scientifiche e l inserimento dei checkpoint inhibitors nell algoritmo decisionale del NSCLC
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
esmo.org ESMO IMMUNO-ONCOLOGY CONGRESS 2017
 ESMO IMMUNO-ONCOLOGY CONGRESS 2017 Primary PFS and safety analyses of a randomised Phase III study of carboplatin + paclitaxel +/ bevacizumab, with or without atezolizumab in 1L non-squamous metastatic
ESMO IMMUNO-ONCOLOGY CONGRESS 2017 Primary PFS and safety analyses of a randomised Phase III study of carboplatin + paclitaxel +/ bevacizumab, with or without atezolizumab in 1L non-squamous metastatic
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Atezolizumab Is a Humanized Anti-PDL1 Antibody That Inhibits the Binding of PD-L1 to PD-1 and B7.1
 Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer
 Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer Benjamin Besse, MD, PhD Chair, EORTC Lung Group Chair, Gustave Roussy Thoracic Unit Villejuif, France What
Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer Benjamin Besse, MD, PhD Chair, EORTC Lung Group Chair, Gustave Roussy Thoracic Unit Villejuif, France What
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
LATEST DEVELOPMENT IN LUNG CANCER IMUNOTHERAPY & INSIGHTS TO THE DAILY CLINICAL PRACTICE
 LATEST DEVELOPMENT IN LUNG CANCER IMUNOTHERAPY & INSIGHTS TO THE DAILY CLINICAL PRACTICE Solange Peters MD-PhD Head Medical Oncology and Thoracic Clinic Oncology Department Lausanne University Hospital
LATEST DEVELOPMENT IN LUNG CANCER IMUNOTHERAPY & INSIGHTS TO THE DAILY CLINICAL PRACTICE Solange Peters MD-PhD Head Medical Oncology and Thoracic Clinic Oncology Department Lausanne University Hospital
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Medical Treatment of Advanced Lung Cancer
 Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Emerging biomarkers for immunotherapy in lung cancer
 Emerging biomarkers for immunotherapy in lung cancer Prof Keith M Kerr Department of Pathology Aberdeen University Medical School, Aberdeen Royal Infirmary Aberdeen, UK Why Do We Need Biomarkers for Immunotherapy?
Emerging biomarkers for immunotherapy in lung cancer Prof Keith M Kerr Department of Pathology Aberdeen University Medical School, Aberdeen Royal Infirmary Aberdeen, UK Why Do We Need Biomarkers for Immunotherapy?
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung
 Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung Noemi Reguart,MD, PhD Hospital Clinic de Barcelona Barcelona, Spain SC-CRP-02660 Conversations in Oncology 2018 is a standalone
Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung Noemi Reguart,MD, PhD Hospital Clinic de Barcelona Barcelona, Spain SC-CRP-02660 Conversations in Oncology 2018 is a standalone
The Role of Immuno-Oncology Biomarkers in Lung Cancer
 The Role of Immuno-Oncology Biomarkers in Lung Cancer Vamsidhar Velcheti, MD, FACP Staff Physician, Associate Director Center for Immuno-Oncology Research Taussig Cancer Institute Cleveland Clinic November
The Role of Immuno-Oncology Biomarkers in Lung Cancer Vamsidhar Velcheti, MD, FACP Staff Physician, Associate Director Center for Immuno-Oncology Research Taussig Cancer Institute Cleveland Clinic November
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker
 Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Lung Cancer Immunotherapy
 Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Immunotherapy in Patients with Non-Small Cell Lung Cancer
 LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
Media Release. Basel, 07 December 2017
 Media Release Basel, 07 December 2017 Phase III IMpower150 study showed Tecentriq (atezolizumab) and Avastin (bevacizumab) plus chemotherapy reduced the risk of disease worsening or death by 38 percent
Media Release Basel, 07 December 2017 Phase III IMpower150 study showed Tecentriq (atezolizumab) and Avastin (bevacizumab) plus chemotherapy reduced the risk of disease worsening or death by 38 percent
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
INNOVATION IN LUNG CANCER MANAGEMENT. Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy
 INNOVATION IN LUNG CANCER MANAGEMENT Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy FIRST-LINE THERAPY FOR METASTATIC NSCLC IN 216 Stratification for EGFR, ALK
INNOVATION IN LUNG CANCER MANAGEMENT Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy FIRST-LINE THERAPY FOR METASTATIC NSCLC IN 216 Stratification for EGFR, ALK
Biologic Basis of Immunotherapy in Lung Cancer
 Biologic Basis of Immunotherapy in Lung Cancer Andrew R. Haas, MD, PhD Director, Interventional Pulmonary and Thoracic Oncology Perelman School of Medicine of the University of Pennsylvania Philadelphia,
Biologic Basis of Immunotherapy in Lung Cancer Andrew R. Haas, MD, PhD Director, Interventional Pulmonary and Thoracic Oncology Perelman School of Medicine of the University of Pennsylvania Philadelphia,
Fattori predittivi di efficacia ed interpretazione della risposta all immunoterapia. Dott. Matteo Brighenti Oncologia Cremona
 Fattori predittivi di efficacia ed interpretazione della risposta all immunoterapia Dott. Matteo Brighenti Oncologia Cremona AREA DI RICERCA CLINICA EPIDEMIOLOGICA ONCOLOGIA CREMONA mos in 4 phase III
Fattori predittivi di efficacia ed interpretazione della risposta all immunoterapia Dott. Matteo Brighenti Oncologia Cremona AREA DI RICERCA CLINICA EPIDEMIOLOGICA ONCOLOGIA CREMONA mos in 4 phase III
Immunotherapy in non-small cell lung cancer
 Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Immunotherapeutic Advances in the Treatment of Metastatic Non-Small Cell Lung Cancer
 Immunotherapeutic Advances in the Treatment of Metastatic Non-Small Cell Lung Cancer Srinivasa R. Sanikommu, MD, and Kathryn F. Mileham, MD Abstract Lung cancer remains the leading cause of cancer-related
Immunotherapeutic Advances in the Treatment of Metastatic Non-Small Cell Lung Cancer Srinivasa R. Sanikommu, MD, and Kathryn F. Mileham, MD Abstract Lung cancer remains the leading cause of cancer-related
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
Media Release. Basel, 17 May 2018
 Media Release Basel, 17 May 2018 Phase III IMpower150 study showed Roche s Tecentriq and Avastin plus carboplatin and paclitaxel helped people with a specific type of metastatic lung cancer live significantly
Media Release Basel, 17 May 2018 Phase III IMpower150 study showed Roche s Tecentriq and Avastin plus carboplatin and paclitaxel helped people with a specific type of metastatic lung cancer live significantly
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Take home message. Emilio Bria. II SESSIONE: Immunoterapia nel tumore del polmone
 II SESSIONE: Immunoterapia nel tumore del polmone Take home message Emilio Bria Oncologia, Dipart. di Medicina, Università di Verona, Az. Osp. Univ. Int., Verona emilio.bria@univr.it Roma, 28 Marzo 2017
II SESSIONE: Immunoterapia nel tumore del polmone Take home message Emilio Bria Oncologia, Dipart. di Medicina, Università di Verona, Az. Osp. Univ. Int., Verona emilio.bria@univr.it Roma, 28 Marzo 2017
Predictive Biomarkers for Pembrolizumab. Eric H. Rubin, M.D.
 Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
Second-line treatment for advanced NSCLC
 UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
Quale sequenza terapeutica nella malattia EGFR+
 Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with
Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with
INMUNOTERAPIA II. Dra. Virginia Calvo
 INMUNOTERAPIA II Dra. Virginia Calvo LBA53. IMpower130. Progression-free survival (PFS) and safety analysis from a randomised phase 3 study of carboplatin + nab-paclitaxel (CnP) with o without atezolizumab
INMUNOTERAPIA II Dra. Virginia Calvo LBA53. IMpower130. Progression-free survival (PFS) and safety analysis from a randomised phase 3 study of carboplatin + nab-paclitaxel (CnP) with o without atezolizumab
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016
 Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Strengths and Weaknesses of PD-L1 testing: Pathology perspective
 Strengths and Weaknesses of PD-L1 testing: Pathology perspective Prof Keith M Kerr Department of Pathology Aberdeen University Medical School, Aberdeen Royal Infirmary Foresterhill, Aberdeen Disclosures
Strengths and Weaknesses of PD-L1 testing: Pathology perspective Prof Keith M Kerr Department of Pathology Aberdeen University Medical School, Aberdeen Royal Infirmary Foresterhill, Aberdeen Disclosures
Personalized Treatment Approaches for Lung Cancer
 Personalized Treatment Approaches for Lung Cancer California Thoracic Society 2018 Annual Carmel Conference January 27, 2018 Matthew Gubens, MD, MS Associate Professor of Medicine Chair, Thoracic Oncology
Personalized Treatment Approaches for Lung Cancer California Thoracic Society 2018 Annual Carmel Conference January 27, 2018 Matthew Gubens, MD, MS Associate Professor of Medicine Chair, Thoracic Oncology
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
INMUNOTERAPIA I. Dra. Virginia Calvo
 INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
Understanding Options: When Should TKIs be Considered?
 Advanced Stage Squamous NSCLC: Evolution and Increasing Complexity of the Therapeutic Landscape Understanding Options: When Should TKIs be Considered? David R. Gandara, MD University of California Davis
Advanced Stage Squamous NSCLC: Evolution and Increasing Complexity of the Therapeutic Landscape Understanding Options: When Should TKIs be Considered? David R. Gandara, MD University of California Davis
Immunotherapy in NSCLC
 Immunotherapy in NSCLC Enriqueta Felip Hospital Vall d Hebron University, Barcelona SAMO Interdisciplinary Workshop on Chest Tumors Lucerne, January 27 217 Immunotherapy in NSCLC: Outline 1 st line as
Immunotherapy in NSCLC Enriqueta Felip Hospital Vall d Hebron University, Barcelona SAMO Interdisciplinary Workshop on Chest Tumors Lucerne, January 27 217 Immunotherapy in NSCLC: Outline 1 st line as
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer") Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Giorgio V. Scagliotti University of Torino Department of Oncology
 Giorgio V. Scagliotti University of Torino Department of Oncology giorgio.scagliotti@unito.it The immune system Strategy to modulate/boost the immune system Check point inhibitors The clinical data Toxicity
Giorgio V. Scagliotti University of Torino Department of Oncology giorgio.scagliotti@unito.it The immune system Strategy to modulate/boost the immune system Check point inhibitors The clinical data Toxicity
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al -
 Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
IMpower150: an exploratory analysis of efficacy outcomes in patients with EGFR mutations
 IMpower150: an exploratory analysis of efficacy outcomes in patients with EGFR mutations Tony Mok, 1 Mark A. Socinski, 2 Martin Reck, 3 Robert Jotte, 4,5 Darren Wan-Teck Lim, 6 Federico Cappuzzo, 7 Francisco
IMpower150: an exploratory analysis of efficacy outcomes in patients with EGFR mutations Tony Mok, 1 Mark A. Socinski, 2 Martin Reck, 3 Robert Jotte, 4,5 Darren Wan-Teck Lim, 6 Federico Cappuzzo, 7 Francisco
1st line chemotherapy and contribution of targeted agents
 ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
Nuevos horizontes en inmunología: Atezolizumab. Dra. Margarita Majem Hospital de la Santa Creu i Sant Pau Barcelona
 Nuevos horizontes en inmunología: Atezolizumab Dra. Margarita Majem Hospital de la Santa Creu i Sant Pau Barcelona ATEZOLIZUMAB Ac monoclonal IgG1 humanizado anti-pd-l1 Unión a PD-L1. Bloquea interacción
Nuevos horizontes en inmunología: Atezolizumab Dra. Margarita Majem Hospital de la Santa Creu i Sant Pau Barcelona ATEZOLIZUMAB Ac monoclonal IgG1 humanizado anti-pd-l1 Unión a PD-L1. Bloquea interacción
Stato dell arte dell immunoterapia. Il Paziente con NSCLC Francesco Ferraù Oncologia Medica Ospedale S.Vincenzo, Taormina
 I CONVEGNO REGIONALE SIFO MEETING DI PRIMAVERA IL FARMACISTA CLINICO E I NUOVI MODELLI DI CURA Taormina, 11/12/13 maggio 217 Stato dell arte dell immunoterapia. Il Paziente con NSCLC Francesco Ferraù Oncologia
I CONVEGNO REGIONALE SIFO MEETING DI PRIMAVERA IL FARMACISTA CLINICO E I NUOVI MODELLI DI CURA Taormina, 11/12/13 maggio 217 Stato dell arte dell immunoterapia. Il Paziente con NSCLC Francesco Ferraù Oncologia
NSCLC: Terapia medica nella fase avanzata. Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza
 NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
AACR 2018 Investor Meeting
 AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Lung cancer PD-L1 testing clinical impact
 Lung cancer PD-L1 testing clinical impact Korinna Jöhrens Institute for pathology Carl Gustav Cars Universitätsklinikum Dresden, Germany Medical consultant QuIP Immune therapy with checkpoint-inhibitors
Lung cancer PD-L1 testing clinical impact Korinna Jöhrens Institute for pathology Carl Gustav Cars Universitätsklinikum Dresden, Germany Medical consultant QuIP Immune therapy with checkpoint-inhibitors
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Immune Checkpoint Inhibitors: Basics and Results
 Immune Checkpoint Inhibitors: Basics and Results Christoph Zielinski Comprehensive Cancer Center Medical University Vienna General Hospital, Vienna, Austria and Central European Cooperative Oncology Group
Immune Checkpoint Inhibitors: Basics and Results Christoph Zielinski Comprehensive Cancer Center Medical University Vienna General Hospital, Vienna, Austria and Central European Cooperative Oncology Group
IMpower132: PFS and Safety Results with 1L Atezolizumab + Carboplatin/Cisplatin + Pemetrexed in Stage IV Non-Squamous NSCLC
 IMpower132: PFS and Safety Results with 1L Atezolizumab + Carboplatin/Cisplatin + Pemetrexed in Stage IV Non-Squamous NSCLC Vassiliki A. Papadimitrakopoulou, 1 Manuel Cobo, 2 Rodolfo Bordoni, 3 Pascale
IMpower132: PFS and Safety Results with 1L Atezolizumab + Carboplatin/Cisplatin + Pemetrexed in Stage IV Non-Squamous NSCLC Vassiliki A. Papadimitrakopoulou, 1 Manuel Cobo, 2 Rodolfo Bordoni, 3 Pascale
NSCLC with squamous histology: Current treatment and new options on horizon
 NSCLC with squamous histology: Current treatment and new options on horizon Prof. Yasser A.Kader Professor of Oncology Faculty of Medicine, Cairo University 2015 Lung Cancer: Incidence and Mortality New
NSCLC with squamous histology: Current treatment and new options on horizon Prof. Yasser A.Kader Professor of Oncology Faculty of Medicine, Cairo University 2015 Lung Cancer: Incidence and Mortality New
The role of immune checkpoint inhibitors in non-small cell lung cancer
 Review Article Page 1 of 9 The role of immune checkpoint inhibitors in non-small cell lung cancer Tiffany L. George 1, Erin M. Bertino 2 1 Divisions of Hematology and Medical Oncology, 2 Division of Medical
Review Article Page 1 of 9 The role of immune checkpoint inhibitors in non-small cell lung cancer Tiffany L. George 1, Erin M. Bertino 2 1 Divisions of Hematology and Medical Oncology, 2 Division of Medical
ESMO IO Congress 2017, Geneva. Roche Analyst Call. Thursday, 7 December 2017
 ESMO IO Congress 2017, Geneva Roche Analyst Call Thursday, 7 December 2017 This presentation contains certain forward-looking statements. These forward-looking statements may be identified by words such
ESMO IO Congress 2017, Geneva Roche Analyst Call Thursday, 7 December 2017 This presentation contains certain forward-looking statements. These forward-looking statements may be identified by words such
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf
 MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
ALK positive Lung Cancer. Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan
 ALK positive Lung Cancer Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan Objectives What is ALK translocation? What drugs are used in what sequence? How many times
ALK positive Lung Cancer Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan Objectives What is ALK translocation? What drugs are used in what sequence? How many times
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
IMUNOTERAPIA NO CÂNCER DE PULMÃO: PRINCÍPIOS
 IMUNOTERAPIA NO CÂNCER DE PULMÃO: PRINCÍPIOS Dr. Gilberto de Castro Junior Professor Colaborador Livre-Docente Faculdade de Medicina da USP. Serviço de Oncologia Clínica - Instituto do Câncer do Estado
IMUNOTERAPIA NO CÂNCER DE PULMÃO: PRINCÍPIOS Dr. Gilberto de Castro Junior Professor Colaborador Livre-Docente Faculdade de Medicina da USP. Serviço de Oncologia Clínica - Instituto do Câncer do Estado
Immunotherapy in lung cancer. Saurabh maji
 Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,