UPDATE IN HOSPITAL MEDICINE FOR THE FLORIDA INTERNIST
|
|
|
- Joseph French
- 5 years ago
- Views:
Transcription

1 UPDATE IN HOSPITAL MEDICINE FOR THE FLORIDA INTERNIST ANKUSH K BANSAL, MD, FACP, SFHM, FABDA LOCUM TENENS HOSPITALIST 09 SEPTEMBER 2016 ANNUAL SCIENTIFIC MEETING 2016 FLORIDA CHAPTER, AMERICAN COLLEGE OF PHYSICIANS OCEAN REEF CLUB KEY LARGO, FL

2 DISCLOSURE OF FINANCIAL RELATIONSHIPS Ankush K Bansal Has disclosed relationships with an entity producing, marketing, reselling, or distributing health care goods or services consumed by, or used on, patients. Hospitalist Employment: Hospitalists Plus Stock Holdings: TelaDoc, iselectmd Telemedicine Independent Contractor: HealthTap, WellnessFX, WellVia Solutions, American Well, Video Medicine
3 Medical Therapy for Ureteric Colic Robert Pickard, Kathryn Starr, Graeme MacLennan, Thomas Lam, Ruth Thomas, Jennifer Burr, Gladys McPherson, Alison McDonald, Kenneth Anson, James N'Dow, Terry Clark, Mary Kilonzo, Katie Gillies, Kirsty Shearer, Charles Boachie, Sarah Cameron, John Norrie, Samuel McClinton Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial Lancet 386 (2015): DOI: /S (15)
4 Introduction Ureteric colic: episodic severe abdominal pain due to sustained contraction of ureteric smooth muscle as a kidney stone passes down the ureter into bladder USA statistics: 550,000 ER visits at cost of $3 billion Usual diagnostic & treatment course but may need drainage & stone removal by endoscopy or ESWL Tamsulosin (α-adrenoceptor antagonist) Nifedipine (calcium-channel stabilizer) use of either agent termed Medical Expulsive Therapy (MET) RCTs 1,2 show statistically significant benefit of either agent over placebo for spontaneous stone passage. Nevertheless, MET adopted as part of routine expectant management - Kidney Intl 83 (2013): Campschroer, T et al. Alpha blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev 4 (2014): CD Seitz, C. et al. Medical therapy to facilitate the passage of stones: what is the evidence. Eur Urol 56 (2009):
5 Study Design SUSPEND trial Spontaneous Urinary Stone Passage Enabled by Drugs Goal: Does tamsulosin or nifedipine increase likelihood of spontaneous stone passage with no need for further intervention? If so, which drug was better? Multi-center, randomized, placebo-controlled, modified intention to treat (primary outcome) Adults aged years. Stone 10 mm in either ureter on CT KUB. 24 hospitals in United Kingdom Conducted 11 January 2011 to 20 December 2013 (2.94 years) Remote randomization 1:1:1 to : Tamsulosin 0.4 mg Nifedipine 30 mg Placebo 28 capsules each participant all capsules over-encapsulated by one independent source Followed up to 4 weeks Analyzed by: Center/hospital stone size ( 5 mm or >5 mm) stone location (upper, mid, lower)
6 Exclusion Criteria Need immediate intervention by clinical assessment Sepsis egfr <30 ml/min Already on or unable to take α-blocker or calcium-channel stabilizer Age >65 because then nifedipine dose-titration is recommended. Procedure Participants self-administered medication until: Spontaneous stone passage Agreed need for intervention 4 weeks passed DID NOT verify medication adherence Follow up questionnaires at home at 4 and 12 weeks Case report forms in clinic or by phone at 4 and 12 weeks NO mandatory testing Serious adverse effects reported as occurred
7 Powered for hypothesis that: number of participants with stone passage in tamsulosin group would be 10% higher than in nifedipine group. Comparisons: MET against placebo Tamsulosin against nifedipine Tamsulosin against placebo Nifedipine against placebo 90% power, Type 1 error of 5%: Need 1062 participants (354 in each group) but: Inflated to 1200 to allow 10% loss to follow up. 17 excluded to ineligibility 14 lost to follow up = 1136 (97%) in primary analysis
8 Outcomes Primary: spontaneous stone passage at 4 weeks (no need for intervention to assist with stone passage at 4 weeks) Secondary: Pain by number of days of analgesic use (participant-reported) and visual analogue scale at 4 weeks Time to stone passage assessed by imaging Health status by SF-36 questionnaire Safety by participant report of medication discontinuation due to adverse effects Health outcomes by EQ-5D questionnaire (not reported in this paper) Health care resource use and participant cost (not reported in this paper)

9 Baseline Characteristics
10 Results 80% in placebo group did not need further intervention by 4 weeks 81% in tamsulosin group did not need further intervention by 4 weeks (ARR 1.3%, p=0.73) NNT=77 80% in nifedipine group did not need further intervention by 4 weeks (ARR 0.5%, p=0.88) NNT=200 Consistent findings across 3 groups (gender, stone size, stone location) Between nifedipine or tamsulosin and placebo, p=0.78 Between nifedipine and tamsulosin, p=0.77 Also: NO difference in stone passage at 12 weeks 7% in tamsulosin group had intervention planned 6% in nifedipine group had intervention planned 7% in placebo group had intervention planned NO differences in secondary outcomes of analgesic use, time to stone passage, health status between groups Adverse events: Nifedipine: 3 participants 1 had right groin pain, diarrhea, vomiting; 1 had malaise, headache, chest pain; 1 had chest pain, dyspnea, left arm pain Placebo: 1 participant headache, dizziness, lightheadedness

11 Primary Outcome Results
12 Subgroup Analyses

13 Pain and Time to stone passage (adjusted)
14 Conclusion Tamsulosin 0.4 mg and nifedipine 30 mg are no better than placebo at decreasing need for further treatment for stone clearance at 4 weeks and 12 weeks in those with expectantly managed ureteric colic. No evidence that either drug reduced pain, hastened time to stone passage, or improved health state. Therefore, these drugs should not be offered in ureteric colic when managed expectantly.
15 IVC Filter + AC vs AC alone in PE recurrence Patrick Mismetti, Silvy Laporte, Olivier Pellerin, Pierre-Vladimir Ennezat, Francis Couturaud, Antoine Elias, Nicolas Falvo, Nicolas Meneveau, Isabelle Quere, Pierre-Marie Roy, Olivier Sanchez, Jeannot Schmidt, Christophe Seinturier, Marie-Antoinette Sevestre, Jean-Paul Beregi, Bernard Tardy, Philippe Lacroix, Emilie Presles, Alain Leizorovicz, Hervé Decousus, Fabrice-Guy Barral, Guy Meyer, PREPIC2 Study Group Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone on risk of recurrent pulmonary embolism: A randomized clinical trial JAMA 313 (2015): DOI: /jama
16 Introduction Sharp increase in use of IVC filters in last 30 years, including as add-on to anti-coagulation 1-3 Unclear benefit to risk analysis in literature regarding adding retrievable inferior vena cava filter to anticoagulation for acute venous thromboembolism (DVT, PE) 1. Stein, PD et al. Twenty-one-year trends in the use of inferior vena cava filters. Arch Intern Med 164 (2004): Stein, PD et al. Increasing use of vena cava filters for prevention of pulmonary embolism. Am J Med 124 (2011): Spencer, FA et al. A population-based study of inferior vena cava filters in patients with acute venous thromboembolism. Arch Intern Med 170 (2010):
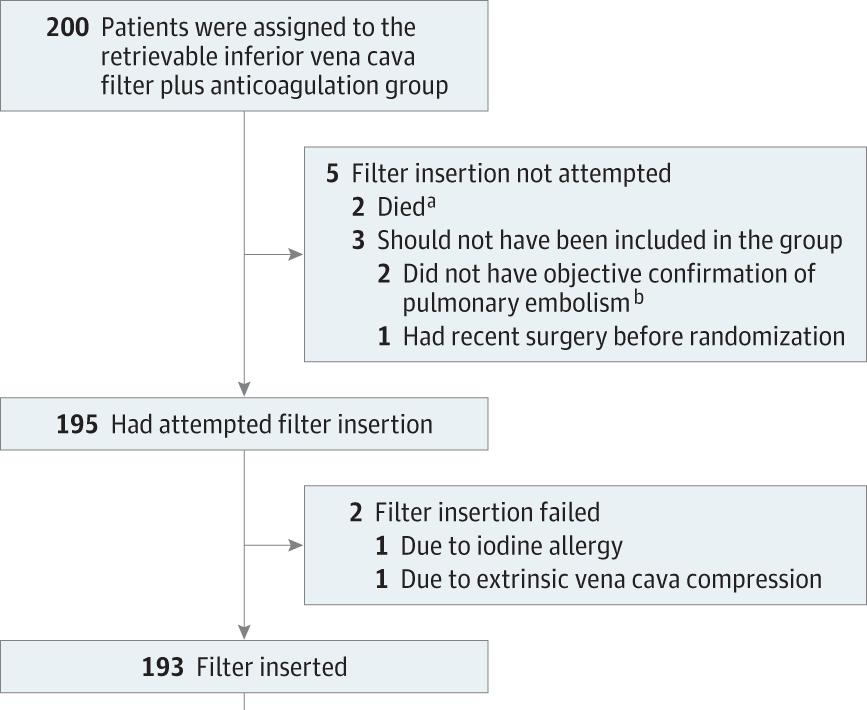
17 Study Design PREPIC2 trial Prévention du Risque d'embolie Pulmonaire par Interruption Cave 2 Goal of this study: Evaluate efficacy and safety of retrievable IVC filters + anti-coagulation vs anti-coagulation alone for preventing PE recurrence in patients with acute PE and high risk of recurrence. Multi-center, randomized, open-label, blinded end-point, intention to treat trial with 6 month follow up 17 centers (hospital & ambulatory follow up) in France Conducted August 2006 to January 2013 (6.5 years) Hospitalized patients, aged 18 Acute, symptomatic PE with LE vein thrombosis (deep or superficial) and 1 severity criterion: Age >75 Active cancer Chronic cardiac or respiratory insufficiency Ischemic stroke with leg paralysis 3 days to 6 months before randomization DVT involving iliocaval segment or bilateral 1 sign of RV dysfunction or myocardial injury RV dilation or pulmonary HTN on echo or abnormal BNP, N-terminal pro-bnp, troponin T or I Diagnosis by: PE spiral CT, V/Q, or pulmonary angio DVT of LE bilateral compression ultrasound or venography Randomization to: Retrievable IVC filter implantation + anti-coagulation (200) Anti-coagulation alone without IVC filter (199)
18 Exclusion Criteria Transient or permanent contraindication to anti-coagulation Recurrent VTE despite adequate anti-coagulant therapy IVC filter already inserted or could not insert filter due to vena caval thrombosis Patient already on full-dose anti-coagulation >72 hours before randomization Non-cancer surgery in prior 3 months or cancer surgery in prior 10 days Allergy to iodinated contrast Serum creatinine >2.04 mg/dl Life expectancy <6 months Pregnant Procedure Randomization by central IVR for concealed allocation, stratified by center and CrCl (Cockgroft-Gault) Full-dose anti-coagulation for minimum 6 months for all patients (thereafter at investigator discretion) Used any injectable anti-coagulant followed by vitamin K antagonist ASAP (unless cancer) Placement of retrievable IVC filter in filter group (randomized) within 72 hours (36 hours delay if thrombolyzed) - by IR Filter retrieval at 3 months from placement in filter group by vascular/interventional radiology (IR) Cavography before and after filter placement Abdominal x-ray hours after placement Ultrasound or venography prior to filter retrieval to detect filter thrombosis Cavography after retrieval Follow up visits at 3 and 6 months Immediate reporting of S/S suggesting VTE or bleeding between visits

19 8% incidence in primary efficacy outcome based on prior studies on rates of recurrent fatal PE and case fatality rates of VTE. Prior study 82% risk reduction in recurrent PE with permanent IVC filter + AC vs AC alone. Powered for hypothesis: 75% risk reduction of primary outcome in filter group. 80% power: Need 200 patients per group. Mean time from randomization to filter insertion attempt: 1.5 days ± 0.6


20

21

22
23 Outcomes Primary: fatal or symptomatic, recurrent pulmonary embolism at 3 months Secondary: Fatal or symptomatic, recurrent PE at 6 months New or recurrent, symptomatic DVT at 3 or 6 months Major bleeding Death from any cause at 3 and 6 months Filter complications (from insertion to retrieval) Thrombosis Migration Tilting Penetration of vena cava wall Access site hematoma Infection
24 Results Filters placed in 193 patients. Retrieved in 153 of 164 in those attempted At 3 months: 3% of those in filter group had recurrent PE all were fatal 1.5% of those in no filter group had recurrent PE 2 of 3 cases were fatal No difference between two groups (p=0.50) Results same at 6 months 1 additional PE recurrence in each group between 3 and 6 months No difference between two groups in other outcomes (DVT, major bleeding, all-cause death) Adverse events: Filter thrombosis 1.6% Access site hematoma 2.6% Retrival failure 5.7% Cardiac arrest during filter insertion 1 patient In control group: 6 required filter insertion 4 because of planned procedure/surgery 2 because of bleeding complication

25
26 Conclusion Compared with anti-coagulation alone, placement of a retrievable inferior vena cava filter for 3 months in addition to anti-coagulation provided no benefit in terms of pulmonary embolism recurrence or mortality in patients presenting with acute symptomatic pulmonary embolism. Previous studies showed that filters do not reduce overall mortality NEJM 338 (1998): ; Circulation 112 (2005): Therefore, use of a retrievable filter when the patient can be treated with anti-coagulation is not supported. Notes: Low rate of events in control group was consistent with contemporary care so full-dose anti-coagulation is likely effective in patients at high risk for recurrence. Further, those at high risk for recurrence are often also at high risk of major bleeding. Single source & model of filter. Lack of evidence of efficacy difference between retrievable filter models. Excluded those with anti-coagulation contraindication or recurrence due to ethical considerations. But included those with hemodynamic instability.
27 Screening for Occult Cancer in First Unprovoked VTE Marc Carrier, Alejandro Lazo-Langner, Sudeep Shivakumar, Vicky Tagalakis, Ryan Zarychanski, Susan Solymoss, Nathalie Routhier, James Douketis, Kim Danovitch, Agnes Lee, Gregoire Le Gal, Philip Wells, Daniel Corsi, Timothy Ramsay, Doug Coyle, Isabelle Chagnon, Zahra Kassam, Hardy Tao, Marc Rodger, SOME Investigators Screening for occult cancer in unprovoked venous thromboembolism NEJM 373 (2015): DOI: /NEJMoa
28 Introduction VTE (DVT and PE) is 3 rd most common cardiovascular disorder 1-3 Provoked: transient risk factor (trauma, surgery, prolonged immobility, pregnancy, puerperium) Unprovoked: no strong transient risk factor or overt cancer 10% patients with unprovoked VTE are diagnosed with cancer within 1 year. 60% are diagnosed soon after DVT. Then, incidence of cancer diagnosis declines and returns to general population rate after 1 year. Some studies have shown that adding CT abdomen & pelvis and/or tumor marker measurement to standard testing (labs, CXR) may significantly increase occult cancer detection rate. 1. Cohen, AT et al. Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost 98 (2007): White, RH. The epidemiology of venous thromboembolism. Circulation 107 (2003): S1: I4-I8. 3. Anderson, FA et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism: the Worcester DVT study. Arch Intern Med 151 (1991):
29 Study Design SOME trial Screening for Occult Malignancy in patients with idiopathic venous thromboembolism Goal of this study: Assess efficacy of screening strategy for occult cancer including comprehensive CT of abdomen & pelvis in patients with first, unprovoked VTE. Multi-center, randomized controlled, open-label, intention to treat, with sensitivity analysis (exclude non-adherent) 9 centers (hospital & ambulatory follow up) in Canada Conducted October 2008 to April 2014 (5.5 years) Patients with new diagnosis of first, unprovoked, symptomatic VTE referred to a thrombosis clinic Unprovoked: No known overt cancer Not currently pregnant No thrombophilia (acquired or hereditary) No previous unprovoked VTE In last 3 months did not have: Paralysis Paresis Plaster immobilization of LE Confinement to bed 3 days Major surgery Randomization with stratification according to center and age (<50, 50) within 21 days of VTE diagnosis.
30 Exclusion Criteria Age <18 Refusal/inability to provide informed consent Contrast allergy GFR <60 Claustrophobia/agoraphobia Mass >130 kg Ulcerative colitis Glaucoma Procedure Randomization by web to ensure concealment Limited screening: H&P, CBC, CMP, CXR Also sex-specific screening if not done in previous year per USPSTF and CTFPHC Female: Breast exam, mammography if age >50, Pap & pelvic for age Male: Prostate exam, PSA if age >40 Limited + CT Bowel prep followed by: Virtual colonoscopy & gastroscopy Biphasic enhanced CT liver & pancreas Uniphasic unenhanced CT bladder Abnormal findings investigated by local physician Followed for 1 year, assessed at fixed intervals Checklist new cancer diagnosis, recurrent VTE, other adverse events If suspected cancer, required biopsy confirmation If recurrent VTE, objective tests for confirmation
31 Previous studies: 6.1% have occult cancer at time of diagnosis of unprovoked VTE At 12 months, prevalence was 10% Power: 80% to detect RR of 75% (ARR 3%) if CT added Null: limited + CT would miss as many as limited alone Need sample size of 798. Assumed 8% non-adherence, so sample = 862 (854 patients)


32
33 Outcomes Primary: confirmed cancer that was missed by screening and detected by end of 1-year follow up period Secondary: Total number of cancers diagnosed Total number of early cancers (by TNM system of WHO) diagnosed by: Occult cancer screening Subsequent 1-year follow up 1-year cancer-related mortality 1-year overall mortality Time to cancer diagnosis (Kaplan-Meier analysis) Incidence of recurrent VTE
34 Results Of 854 total randomized subjects, 3.9% had new diagnosis of occult cancer by 1-year follow up. 3.2% in limited screening group 4.5% in limited screening plus CT group No difference between groups (p=0.28) Analysis: 20% of occult cancers were missed by limited screening strategy. 26% of occult cancers were missed by limited screening plus CT No difference between groups (p=1.0) The best case with CT added to limited screening: NNT = 91 No difference between groups in mean time to cancer diagnosis 4.2 months in limited screening vs 4.0 months in limited screening plus CT (p=0.88) No difference in cancer-related mortality (1.4% vs 0.9%, p=0.75)
35


36
37 Conclusion Routine screening with CT abdomen & pelvis did not provide clinical benefit. Prevalence of occult cancer was low in first, unprovoked VTE.
38 Summary For expectantly managed ureteric colic, neither tamsulosin nor nifedipine reduced the chance of needing further treatment for stone passage at 4 and 12 weeks. Additionally, neither reduced pain, hastened time to stone passage, or improved health. In patients with acute, symptomatic pulmonary embolism who have no contraindication to anti-coagulant therapy, retrievable inferior vena cava filters added no benefit with respect to recurrence or mortality. In patients with first, unprovoked venous thromboembolism, screening for occult cancer with CT beyond an H&P, basic labs, age-specific screening, and chest x-ray provided no clinical benefit with respect to time to cancer diagnosis or cancer-specific mortality. Moral of the story: Less IS More.

39 Questions? Thank You. Ankush Bansal drakb1 AnkushBansal
Management of Pulmonary Embolism. Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School
 Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Supplementary Online Content
 Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT
 VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
Venous Thromboembolic Disease Update
 Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Alpha blockers have no role in renal colic
 Alpha blockers have no role in renal colic HARRY WINKLER Director, section of Endourology Kidney stone center Dept.of Urology Sheba Medical Center Financial and Other Disclosures Off-label use of drugs,
Alpha blockers have no role in renal colic HARRY WINKLER Director, section of Endourology Kidney stone center Dept.of Urology Sheba Medical Center Financial and Other Disclosures Off-label use of drugs,
THROMBOEMBOLIC EVENTS AFTER IVC FILTER PLACEMENT IN TRAUMA PATIENTS. Lidie Lajoie, MD SUNY Downstate Department of Surgery December 20, 2012
 THROMBOEMBOLIC EVENTS AFTER IVC FILTER PLACEMENT IN TRAUMA PATIENTS Lidie Lajoie, MD SUNY Downstate Department of Surgery December 20, 2012 Background Trauma Patients at High Risk for VTE Spain, D.A.,
THROMBOEMBOLIC EVENTS AFTER IVC FILTER PLACEMENT IN TRAUMA PATIENTS Lidie Lajoie, MD SUNY Downstate Department of Surgery December 20, 2012 Background Trauma Patients at High Risk for VTE Spain, D.A.,
IRB protocol Yair Lev, MD 11/25/08
 IRB protocol Yair Lev, MD 11/25/08 Abdominal and Pelvic CT as a screening modality for occult malignant disease in unprovoked Venous Thromboembolism: A randomized, controlled prospective study. A. Study
IRB protocol Yair Lev, MD 11/25/08 Abdominal and Pelvic CT as a screening modality for occult malignant disease in unprovoked Venous Thromboembolism: A randomized, controlled prospective study. A. Study
abstract n engl j med 373;8 nejm.org August 20,
 The new england journal of medicine established in 1812 August 20, 2015 vol. 373 no. 8 Screening for Occult Cancer in Unprovoked Venous Thromboembolism Marc Carrier, M.D., Alejandro Lazo Langner, M.D.,
The new england journal of medicine established in 1812 August 20, 2015 vol. 373 no. 8 Screening for Occult Cancer in Unprovoked Venous Thromboembolism Marc Carrier, M.D., Alejandro Lazo Langner, M.D.,
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC
 David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC") Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski. Department of Surgery Grand Rounds March 24, 2008
 Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski Department of Surgery Grand Rounds March 24, 2008 History of Vena Cava Filters Virchow-1846-Proposes PE originate from veins
Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski Department of Surgery Grand Rounds March 24, 2008 History of Vena Cava Filters Virchow-1846-Proposes PE originate from veins
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/188/20915 holds various files of this Leiden University dissertation. Author: Flinterman, Linda Elisabeth Title: Risk factors for a first and recurrent venous
Cover Page The handle http://hdl.handle.net/188/20915 holds various files of this Leiden University dissertation. Author: Flinterman, Linda Elisabeth Title: Risk factors for a first and recurrent venous
I am NOT: Disclosures. The Problem of the Con-Position Non Thinking! Against New Ideas. Against New Therapies. Against Endovascular Therapies
 Inferior Vena Cava Filters: Disclosures A Love /Hate (Mostly Hate) Relationship Lack of Political Correctness Gregory L. Moneta, M.D. Professor and Chief, Vascular Surgery Oregon Health & Science University
Inferior Vena Cava Filters: Disclosures A Love /Hate (Mostly Hate) Relationship Lack of Political Correctness Gregory L. Moneta, M.D. Professor and Chief, Vascular Surgery Oregon Health & Science University
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
Inferior Vena Cava Filters
 Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
INFERIOR VENA CAVA FILTERS QUIZ 10 QUESTIONS MAY 5, 2014
 INFERIOR VENA CAVA FILTERS QUIZ 10 QUESTIONS MAY 5, 2014 QUESTION 1 1. Anatomically Transposition of the IVC is observed in what % of individuals A) 1-5% B).2-.05% C) 3-5% D) 5-10% ANSWER QUESTION 1 Answer
INFERIOR VENA CAVA FILTERS QUIZ 10 QUESTIONS MAY 5, 2014 QUESTION 1 1. Anatomically Transposition of the IVC is observed in what % of individuals A) 1-5% B).2-.05% C) 3-5% D) 5-10% ANSWER QUESTION 1 Answer
Top Ten Reasons For Failure To Prevent Postoperative Thrombosis
 Top Ten Reasons For Failure To Prevent Postoperative Thrombosis Joseph A. Caprini, MD, MS, FACS, RVT, FACCWS Louis W. Biegler Chair of Surgery NorthShore University HealthSystem, Evanston, IL Clinical
Top Ten Reasons For Failure To Prevent Postoperative Thrombosis Joseph A. Caprini, MD, MS, FACS, RVT, FACCWS Louis W. Biegler Chair of Surgery NorthShore University HealthSystem, Evanston, IL Clinical
Institute of Cellular Medicine, Newcastle University, Newcastle, UK 2. Health Services Research Unit, University of Aberdeen, Aberdeen, UK 3
 Use of drug therapy in the management of symptomatic ureteric stones in hospitalised adults: a multicentre, placebo-controlled, randomised controlled trial and cost-effectiveness analysis of a calcium
Use of drug therapy in the management of symptomatic ureteric stones in hospitalised adults: a multicentre, placebo-controlled, randomised controlled trial and cost-effectiveness analysis of a calcium
Understanding thrombosis in venous thromboembolism. João Morais Head of Cardiology Division and Research Centre Leiria Hospital Centre Portugal
 Understanding thrombosis in venous thromboembolism João Morais Head of Cardiology Division and Research Centre Leiria Hospital Centre Portugal Disclosures João Morais On the last year JM received honoraria
Understanding thrombosis in venous thromboembolism João Morais Head of Cardiology Division and Research Centre Leiria Hospital Centre Portugal Disclosures João Morais On the last year JM received honoraria
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Update in Hospital Medicine. Disclosures 10/30/2017. none Oregon Chapter ACP Scientific Meeting
 Update in Hospital Medicine 2017 Oregon Chapter ACP Scientific Meeting DATE: November 4, 2017 PRESENTED BY: Joel Papak, MD FACP Disclosures none 1 How well do you think you keep up with the medical literature?
Update in Hospital Medicine 2017 Oregon Chapter ACP Scientific Meeting DATE: November 4, 2017 PRESENTED BY: Joel Papak, MD FACP Disclosures none 1 How well do you think you keep up with the medical literature?
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
CHAPTER 2 VENOUS THROMBOEMBOLISM
 CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Management of Cancer Associated Thrombosis (CAT) where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth
 where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth") Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Clinical Guide - Suspected PE (Reviewed 2006)
") Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Simplified approach to investigation of suspected VTE
 Simplified approach to investigation of suspected VTE Diagnosis of DVT and PE THSNA 2016, Chicago 15 April 2016 Clive Kearon, McMaster University, Canada Relevant Disclosures Research Support/P.I. Employee
Simplified approach to investigation of suspected VTE Diagnosis of DVT and PE THSNA 2016, Chicago 15 April 2016 Clive Kearon, McMaster University, Canada Relevant Disclosures Research Support/P.I. Employee
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Proper Diagnosis of Venous Thromboembolism (VTE)
") Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS
 EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center
 Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION
 IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION Resident(s): George Athanasatos Attending(s): Daniel Golwyn Program/Dept: Interventional Radiology CHIEF
IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION Resident(s): George Athanasatos Attending(s): Daniel Golwyn Program/Dept: Interventional Radiology CHIEF
Epidermiology Early pulmonary embolism
 Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Pulmonary Embolism Pathway
 Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
What is the real place of venous echo Doppler in aircrew member flying rehabilitation after a thromboembolism event?
 89 th ASMA ANNUAL SCIENTIFIC MEETING DALLAS- May 6-10, 2018 What is the real place of venous echo Doppler in aircrew member flying rehabilitation after a thromboembolism event? S BISCONTE (1), V MARICOURT
89 th ASMA ANNUAL SCIENTIFIC MEETING DALLAS- May 6-10, 2018 What is the real place of venous echo Doppler in aircrew member flying rehabilitation after a thromboembolism event? S BISCONTE (1), V MARICOURT
IVC filter retrieval program effects on retrieval rates and number of patients lost to follow-up
 IVC filter retrieval program effects on retrieval rates and number of patients lost to follow-up Aliaksei Salei, MD; Joel Raborn, MD; Padma P. Manapragada, MD; Ahmed Kamel Abdel Aal, MD/PhD; AJ Gunn, MD
IVC filter retrieval program effects on retrieval rates and number of patients lost to follow-up Aliaksei Salei, MD; Joel Raborn, MD; Padma P. Manapragada, MD; Ahmed Kamel Abdel Aal, MD/PhD; AJ Gunn, MD
Top 5 (or so) Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE
 Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE") Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Bath, Philip M.W. and England, Timothy J. (2009) Thighlength compression stockings and DVT after stroke. Lancet. ISSN (In Press)
 Thighlength compression stockings and DVT after stroke. Lancet. ISSN (In Press)") Bath, Philip M.W. and England, Timothy J. (2009) Thighlength compression stockings and DVT after stroke. Lancet. ISSN 0140-6736 (In Press) Access from the University of Nottingham repository: http://eprints.nottingham.ac.uk/1087/1/lancet_clots_1_20090522_4.pdf
Bath, Philip M.W. and England, Timothy J. (2009) Thighlength compression stockings and DVT after stroke. Lancet. ISSN 0140-6736 (In Press) Access from the University of Nottingham repository: http://eprints.nottingham.ac.uk/1087/1/lancet_clots_1_20090522_4.pdf
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies
 VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information
 Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Duration of anticoagulation
 Duration of anticoagulation P. Fontana Service d angiologie et d hémostase Hôpitaux Universitaires de Genève Pomeriggio formativo in coagulazione, Bellinzona, 19.10.2017 Conflict of interest AstraZeneca,
Duration of anticoagulation P. Fontana Service d angiologie et d hémostase Hôpitaux Universitaires de Genève Pomeriggio formativo in coagulazione, Bellinzona, 19.10.2017 Conflict of interest AstraZeneca,
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
Clinical Guide - Inferior Vena Cava Filters (Reviewed 2006)
") Clinical Guide - Inferior Vena Cava Filters (Reviewed 2006) Principal Developer: V. Oliva Secondary Developers: W. Geerts Background The treatment of choice for deep venous thrombosis (DVT) and pulmonary
Clinical Guide - Inferior Vena Cava Filters (Reviewed 2006) Principal Developer: V. Oliva Secondary Developers: W. Geerts Background The treatment of choice for deep venous thrombosis (DVT) and pulmonary
The Evidence Base for Treating Acute DVT
 The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
Recurrence risk after anticoagulant treatment of limited duration for late, second venous thromboembolism
 ARTICLES Coagulation & its Disorders Recurrence risk after anticoagulant treatment of limited duration for late, second venous thromboembolism Tom van der Hulle, Melanie Tan, Paul L. den Exter, Mark J.G.
ARTICLES Coagulation & its Disorders Recurrence risk after anticoagulant treatment of limited duration for late, second venous thromboembolism Tom van der Hulle, Melanie Tan, Paul L. den Exter, Mark J.G.
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
VTE in the Trauma Population
 VTE in the Trauma Population Erik Peltz, D.O. February 11 th, 2015 * contributions from Eduardo Gonzalez, M.D. University of Colorado T-32 Research Fellow The problem. VTE - Scope of the Problem One of
VTE in the Trauma Population Erik Peltz, D.O. February 11 th, 2015 * contributions from Eduardo Gonzalez, M.D. University of Colorado T-32 Research Fellow The problem. VTE - Scope of the Problem One of
Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community
 Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Venous Thrombo-Embolism. John de Vos Consultant Haematologist RSCH
 Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Direct oral anticoagulants to prevent VTE recurrence: full or reduced dosage? MA Sevestre CHU Amiens
 Direct oral anticoagulants to prevent VTE recurrence: full or reduced dosage? MA Sevestre CHU Amiens Faculty disclosure Marie Antoinette Sevestre I disclose the following financial relationships: Paid
Direct oral anticoagulants to prevent VTE recurrence: full or reduced dosage? MA Sevestre CHU Amiens Faculty disclosure Marie Antoinette Sevestre I disclose the following financial relationships: Paid
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
Cover Page The handle http://hdl.handle.net/1887/40114 holds various files of this Leiden University dissertation Author: Exter, Paul L. den Title: Diagnosis, management and prognosis of symptomatic and
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Duration of Therapy for Venous Thromboembolism
 Duration of Therapy for Venous Thromboembolism Michael B Streiff, MD FACP Associate Professor of Medicine and Pathology Medical Director, Johns Hopkins Anticoagulation Service Chairman, VTE Guideline Committee
Duration of Therapy for Venous Thromboembolism Michael B Streiff, MD FACP Associate Professor of Medicine and Pathology Medical Director, Johns Hopkins Anticoagulation Service Chairman, VTE Guideline Committee
to anticoagulation in patients with acute venous thromboembolism, their benefit-risk ratio is unclear.
 Research Original Investigation Effect of a Retrievable Inferior Vena Cava Filter Plus Anticoagulation vs Anticoagulation Alone on Risk of Recurrent Pulmonary Embolism A Randomized Clinical Trial Patrick
Research Original Investigation Effect of a Retrievable Inferior Vena Cava Filter Plus Anticoagulation vs Anticoagulation Alone on Risk of Recurrent Pulmonary Embolism A Randomized Clinical Trial Patrick
Approach to Thrombosis
 Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
HISTORICALLY, INSERTION
 ORIGINAL INVESTIGATION A Population-Based Study of Inferior Vena Cava Filters in Patients With Acute Venous Thromboembolism Frederick A. Spencer, MD; Shannon M. Bates, MD; Robert J. Goldberg, PhD; Darleen
ORIGINAL INVESTIGATION A Population-Based Study of Inferior Vena Cava Filters in Patients With Acute Venous Thromboembolism Frederick A. Spencer, MD; Shannon M. Bates, MD; Robert J. Goldberg, PhD; Darleen
A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism
 Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
Cardiol Ther (2018) 7:1 13 https://doi.org/10.1007/s40119-018-0107-0 REVIEW A Review of the Role of Non-Vitamin K Oral Anticoagulants in the Acute and Long-Term Treatment of Venous Thromboembolism Andrew
Frequently Asked Questions about Cancer Associated Thrombosis
 + Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
+ Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP)
") The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
Duration of Anticoagulant Therapy. Linda R. Kelly PharmD, PhC, CACP September 17, 2016
 Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Deep Vein Thrombosis
 Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Mutidisciplinary cooperation on VTE prevention and managment
 Mutidisciplinary cooperation on VTE prevention and managment TAO YANG Dpartment of vascular surgery Shanxi DAYI Hospita Tai yuan Shanxi China Disclosure Speaker name: Tao Yang... I have the following potential
Mutidisciplinary cooperation on VTE prevention and managment TAO YANG Dpartment of vascular surgery Shanxi DAYI Hospita Tai yuan Shanxi China Disclosure Speaker name: Tao Yang... I have the following potential
PE service. 65 years old lady. What would you do next? Risk stratification. What would you do next? Regional College Lecture PE Management
 PE service Regional College Lecture PE Management Update in medicine (Eastern) Cambridge 29 th June 2017 Dr Rachel M Limbrey DM FRCP University Hospital Southampton NHS Foundation Trust Ambulatory acute
PE service Regional College Lecture PE Management Update in medicine (Eastern) Cambridge 29 th June 2017 Dr Rachel M Limbrey DM FRCP University Hospital Southampton NHS Foundation Trust Ambulatory acute
Deep vein thrombosis and its prevention in critically ill adults Attia J, Ray J G, Cook D J, Douketis J, Ginsberg J S, Geerts W H
 Deep vein thrombosis and its prevention in critically ill adults Attia J, Ray J G, Cook D J, Douketis J, Ginsberg J S, Geerts W H Authors' objectives To systematically review the incidence of deep vein
Deep vein thrombosis and its prevention in critically ill adults Attia J, Ray J G, Cook D J, Douketis J, Ginsberg J S, Geerts W H Authors' objectives To systematically review the incidence of deep vein
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach
 Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Duration anticoagulation VTE. Clinical case WGA april 2017 Dr Borgoens
 Duration anticoagulation VTE Clinical case WGA april 2017 Dr Borgoens Clinical case 70 y old, sedentary computer engineer 1 st episode intermediate high risk pulmonaryembolism(rv dysfunction, positives
Duration anticoagulation VTE Clinical case WGA april 2017 Dr Borgoens Clinical case 70 y old, sedentary computer engineer 1 st episode intermediate high risk pulmonaryembolism(rv dysfunction, positives
C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School
 Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
ARTEMIS. ARixtra (fondaparinux) for ThromboEmbolism prevention in. a Medical Indications Study. NV Organon Protocol 63129
 for ThromboEmbolism prevention in. a Medical Indications Study. NV Organon Protocol 63129") ARTEMIS ARixtra (fondaparinux) for ThromboEmbolism prevention in NV Organon Protocol 63129 a Medical Indications Study Objective To demonstrate efficacy and to assess safety of oncedaily subcutaneous (SC)
ARTEMIS ARixtra (fondaparinux) for ThromboEmbolism prevention in NV Organon Protocol 63129 a Medical Indications Study Objective To demonstrate efficacy and to assess safety of oncedaily subcutaneous (SC)
UC SF. Division of General Internal Medicine UNIVERSITY OF CALIFORNIA SAN FRANCISCO, DIVISION OF HOSPITAL MEDICINE
 Updates in the Management of Venous Thromboembolism Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic Venous Thromboembolism
Updates in the Management of Venous Thromboembolism Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic Venous Thromboembolism
Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren
 Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren Paul Kyrle Allgemeines Krankenhaus Wien Disclosures relevant for this presentation Consultancies, member of advisory boards, speaker
Spontane und Tumor-assoziierte VTE: womit wie lange antikoagulieren Paul Kyrle Allgemeines Krankenhaus Wien Disclosures relevant for this presentation Consultancies, member of advisory boards, speaker
Hydronephrosis. What is hydronephrosis?
 What is hydronephrosis? Hydronephrosis Hydronephrosis describes the situation where the urine collecting system of the kidney is dilated. This may be a normal variant or it may be due to an underlying
What is hydronephrosis? Hydronephrosis Hydronephrosis describes the situation where the urine collecting system of the kidney is dilated. This may be a normal variant or it may be due to an underlying
Prophylaxis for Hospitalized and Non-Hospitalized Medical Patients
 Prophylaxis for Hospitalized and Non-Hospitalized Medical Patients An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric
Prophylaxis for Hospitalized and Non-Hospitalized Medical Patients An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric
Preventing Blood Clots in Adult Patients
 Manchester Royal Eye Hospital Surgical Services Information for Patients Preventing Blood Clots in Adult Patients This leaflet will give you information on how to reduce the risk of developing blood clots
Manchester Royal Eye Hospital Surgical Services Information for Patients Preventing Blood Clots in Adult Patients This leaflet will give you information on how to reduce the risk of developing blood clots
Is Oral Rivaroxaban Safe and Effective in the Treatment of Patients with Symptomatic DVT?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Clinical Practice Committee Anticoagulation Bridging Document
 Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Diagnosis of Venous Thromboembolism
 Diagnosis of Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University of
Diagnosis of Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University of
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis. By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan
 Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Suspected Deep Vein Thrombosis (DVT) Assessment
 Assessment") CHI no... First name... DOB... /... /... Last name... Sex: c M c F Address...... Telephone... or attach addressograph label here Hospital/Location: c Hairmyres c Monklands c Wishaw Other (specify)... Ward/Base...
CHI no... First name... DOB... /... /... Last name... Sex: c M c F Address...... Telephone... or attach addressograph label here Hospital/Location: c Hairmyres c Monklands c Wishaw Other (specify)... Ward/Base...
October 2017 Pulmonary Embolism
 October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
Acute and long-term treatment of PE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Inferior Vena Cava Filter for DVT
 Inferior Vena Cava Filter for DVT Deep Vein Thrombosis A deep vein thrombosis (DVT) is a blood clot that forms in a deep vein. This is a serious condition that occurs more often than you might think. If
Inferior Vena Cava Filter for DVT Deep Vein Thrombosis A deep vein thrombosis (DVT) is a blood clot that forms in a deep vein. This is a serious condition that occurs more often than you might think. If
Chapter 1. Introduction
 Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150