RECOMMENDATIONS FOR USE OF IRRADIATED BLOOD COMPONENTS IN CANADA
|
|
|
- Samson Hodges
- 5 years ago
- Views:
Transcription
1 RECOMMENDATIONS FOR USE OF IRRADIATED BLOOD COMPONENTS IN CANADA Page 1
2 RECOMMENDATIONS FOR USE OF IRRADIATED BLOOD COMPONENTS IN CANADA BACKGROUND: The National Advisory Committee on Blood and Blood Products (NAC) is an interprovincial medical and technical advisory body to the provincial and territorial health ministries and Canadian Blood Services (CBS). The NAC mandate is to: Provide advice on matters pertaining to blood supply, including those directly affecting the practice of transfusion medicine in hospitals; Share information about blood and blood product utilization and utilization management efforts, and play a supportive role in the development of guidelines and recommendations for product use; Identify opportunities to optimize transfusion medicine practices; and On a jurisdictional level, provide leadership in the identification, design and implementation of blood utilization management initiatives for the optimization of patient care. The CBS Provincial Territorial Blood Liaison Committee (CBS PT BLC) requested that NAC develop recommendations and guidelines for the use of irradiated blood products for Canadian patients. NAC assembled an Irradiation working group to review current standards, published guidelines and recent literature on the indications for irradiated components and the quality of irradiated red cell components (RCCs) to facilitate recommendations for best practices. NAC s Irradiation working group also engaged representatives of Quebec s National Advisory Committee on Transfusion Medicine (CCNMT) and consulted with Canadian experts in transfusion medicine. This work was informed by guidelines published by the British Committee for Standards in Hematology (BCSH 2010) and the Australian and New Zealand Society of Blood Transfusion (ANZSBT 2011) as well as the Canadian Standards Association (CSA) and the Canadian Society for Transfusion Medicine (CSTM) standards, Council of Europe (COE) standards, and recent publications on the quality of stored red cells post irradiation. Upon review of the best-available information, the Irradiation working group has compiled recommendations regarding which patients should receive irradiated components, the age of the components at the time of irradiation and the length of storage post-irradiation. The latter recommendations are consistent with the COE standards and more restrictive than current American Association of Blood Banks (AABB), CSA and CSTM standards. Irradiation of blood components is a well-established intervention for the prevention of transfusion-associated graft-versus-host disease (TA-GVHD). There is a system cost of providing irradiated blood components to patients that includes higher production costs, time delays and damage to transfused red blood cells. In particular, recent publications have emphasized the importance of considering the age of a RCC at the time of irradiation and the length of storage post-irradiation. The working group has emphasized the importance of managing hospital inventories such that provision of irradiated RCCs is limited, to the extent feasible, to those Page 2
3 patients who have specific clinical indications for irradiated RCCs. Thereby minimizing exposure of the general patient population to irradiated RCCs. Data provided by CBS demonstrates some trends in irradiation practice in Canada over the past ten years. There has been a national increase in the percentage of irradiated RCCs from 4.5% ( ) to 6.7% ( ). There is considerable regional variation. The percentage irradiated RCC issued by CBS ranges from 2-18%, depending on the province. The percentage of irradiated RCC issued by Héma-Québec, in , was TA-GVHD is a rare, usually fatal, complication of transfusion resulting from the engraftment of transfused, immunocompetent, donor lymphocytes and subsequent damage to recipient tissues which are perceived as foreign by the engrafted lymphocytes. Patients at most risk include those who are severely immunocompromised and those who fail to recognize the transfused lymphocytes as foreign, due to HLA homology. Defining immunocompromised patient groups who should receive irradiated blood has been largely based on observational evidence, case reports, reviews and attempts to predict the degree of immunosuppression. As such, there is a lack of consistency in text books, publications and guidelines as to which patients must receive irradiated blood. Many authors address the lack of certainty by including a category of patients where there is uncertainty regarding the need for irradiated blood. In view of our growing knowledge of the poor quality of post-irradiation stored blood it behoves us to be thoughtful about our lists of clinical indications and avoid over stocking pre-storage irradiated blood. Finding a balance is difficult; however, recent observational evidence suggests that pre-storage leukoreduction reduces the risk of TA-GVHD and that the length of time since donation is relevant to the risk of TA-GVHD. In a recent systematic review of reported cases of TA-GVHD the authors report that greater than 94% of cases of TA-GVHD occur when the blood is less than 10 days old (Kopolovic et al, 2015). In a review of 290 cases referred to the Japanese Red Cross (JRC), from , 66 were deemed definite TA-GVHD, by microsatellite DNA analysis. The oldest blood transfused in these cases was 10 days for whole blood, 11 days for non-additive RCC and 14 days for RCC with added mannitol, adenine and phosphate (Uchida et al, 2013). In another report from the JRC, 96% of 51 cases received blood less than 96 hours old (Jawa et al, ). Thus, transfusion of blood stored for more than 14 days represents a potential risk mitigation strategy for patients in whom there is uncertainty regarding the degree of immune compromise. The potential risk mitigation afforded by leukoreduction is suggested by data from the Serious Hazards of Transfusion (SHOT) surveillance system in the United Kingdom (UK) where there have been no cases of TA-GVHD since the introduction of universal pre-storage leukoreduction in It should be noted, however, that 2 of 13 cases between 1996 and 2001 occurred in patients who received leukoreduced components. Furthermore, subsequent to the 2001 terrorist attacks a decision was made in the UK to increase blood stocks. The mean age of blood issued to hospitals after 2002 went from eight (8) days to days and this may have contributed to reduced risk of TA-GVHD (Williamson et al, 2007). Nonetheless, universal pre-storage leukoreduction is thought to afford some reduction in the risk of TA-GVHD Page 3
4 In defining patients who should receive irradiated cellular components, NAC has chosen to support the recommendations contained in the BCSH 2010 and ANZSBT 2011 guidelines while maintaining a cautious approach for top-up transfusions in neonates less than 1200 grams and neonatal exchange transfusion. For patient groups where the risk of TA-GVHD is uncertain, NAC has suggested the option of choosing pre-storage leukoreduced RCCs that are greater than 14 days post collection as a risk mitigation strategy in the absence of on-site irradiation. It is expected that this approach will reduce the need to maintain excessive stocks of irradiated blood in facilities that do not have an irradiator and minimize transfusion of irradiated stock RCCs to the general patient population. GENERAL RECOMMENDATIONS NAC supports the following general recommendations pertaining to the type of blood component that requires irradiation, information sharing and communications of a patient s requirement for irradiated blood components. In addition, NAC recommends voluntary alignment with the COE standards for the age of the units and post-irradiation storage conditions. Blood components that should be irradiated Recommendation: For at-risk patients, all red cell, platelet and granulocyte components should be irradiated, except cryopreserved red cells after deglycerolization. It is not necessary to irradiate fresh frozen plasma, cryoprecipitate or fractionated plasma. (Grade 1 recommendation; level B evidence, BCSH 2010) Age of the Units and Post-Irradiation Storage Conditions Recent evidence has shown that the age of RCCs at the time of irradiation is important and that prolonged storage of pre-irradiated units is associated with high potassium levels, in vitro hemolysis and decreased post-transfusion recovery. This has implications for patient safety as well as hospital inventory management practices. NAC is recommending voluntary alignment with the COE standards (17 th edition) which are more restrictive than the current North American standards (AABB, CSA and CSTM) and regulations (Health Canada and FDA). Current North American standards and regulations specify that RCCs shall have a maximum expiration time of 28 days after irradiation or shall retain the original outdate, whichever is shorter. There is no limit on the age of RCC at the time of irradiation. Contrariwise, the COE standards restrict the age of RCCs at the time of irradiation and the length of storage thereafter. Recommendation: Red cell components may be irradiated up to 28 days after collection. Irradiated cells must be transfused as soon as possible, but no later than 14 days after irradiation, and, in any case, no later than 28 days after collection. (Council of Europe Standards, 17 th edition, 2013) Page 4
5 Patient awareness Recommendation: The most responsible health care practitioner shall inform patients at risk of TA-GVHD of their need for irradiated blood components. (Grade 2 recommendation; level C evidence, BCSH 2010) Communication Recommendation: To ensure consistency of patient care across jurisdictions, particularly between hospital facilities that participate in the shared care of patients, a communications process facilitating sharing details of special transfusion requirements should be implemented and maintained. INVENTORY MANAGEMENT RECOMMENDATIONS As stated, prolonged storage of pre-irradiated units is associated with high potassium levels, invitro hemolysis and decreased post-transfusion recovery. Maintaining large inventories of irradiated red cells results in potentially harmful transfusion of irradiated red cells to patients who do not require irradiated cellular blood components. Proactive inventory management must take into consideration the perceived risk of TA-GVHD in the local patient population, the risks of transfusing irradiated red cells to patients who do not require irradiated cellular components and the logistics of providing irradiated components for elective transfusions. Recommendation: For elective transfusions reliance on a regional hub site for on-demand irradiation or pre-irradiated stock is recommended. Recommendation: Overstocking of pre-irradiated units for emergency transfusion is not recommended. If storage of pre-irradiated inventory is absolutely necessary, then obtain red cells that have been irradiated within 14 days of collection if possible. As described above, observational evidence from UK SHOT data (Williamson et al, 2007), a recent systematic review of 348 cases of TA-GVHD (Kopolovic et al, 2015) and three reviews of Japanese Red Cross data has provided some evidence for the risk mitigating effect of universal pre-storage leukoreduction and the transfusion of older RCCs with reduced lymphocyte viability (>14 days post donation) (Uchida et al, 2013) (Jawa et al, ). Recommendation: In the event of emergency transfusion in the absence of on-site irradiation or pre-storage irradiated inventory, pre-storage leukoreduced red cells that have been stored for more than 14 days should be provided Page 5
6 CLINICAL RECOMMENDATIONS To arrive at the following clinical recommendations NAC has drawn upon the BCSH 2010 and ANZSBT 2011 guidelines and a survey of current practices at Canadian hospitals with level three (3) neonatal intensive care units. See Appendix A for a quick reference of the clinical indications. Acquired immunodeficiency states Recommendation: There is no indication for irradiation of cellular blood components for adults or infants and children who are HIV antibody positive or who have AIDS. (Grade 2 recommendation; level B evidence, BCSH 2010; ANZSBT 2011) Acute leukemia Recommendation: It is not necessary to irradiate red cells or platelets for adults or children, except for HLA-selected platelets or donations from first- or second-degree relatives. (Grade 1 recommendation; level B evidence, BCSH 2010; ANZSBT 2011) Allogeneic bone marrow or peripheral blood stem cell transplantation Recommendation: All recipients of allogeneic hemopoietic stem cell transplantation (HSCT) must receive irradiated blood components from the time of initiation of conditioning chemoradiotherapy. (Grade 1 recommendation; level B evidence, BCSH 2010; ANZSBT 2011) Recommendation: Irradiated blood components should be continued while the patient continues to receive graft-versus-host disease (GVHD) prophylaxis, i.e. usually for 6 months post-transplant, or until the lymphocyte count is greater than 1x10 9 /L. If chronic GVHD is present or if continued immunosuppressive treatment is required, irradiated blood components should be given indefinitely. (Grade 2 recommendation; level C evidence, BCSH 2010) Recommendation: Allogeneic blood transfused to bone marrow and peripheral blood stem cell donors seven (7) days prior to or during the harvest should also be irradiated. (Grade 2 recommendation; level C evidence, BCSH 2010; ANZSBT 2011) Aplastic anemia Recommendation: In view of the recent switch from horse anti-thymocyte globulin (ATG) to the more immunosuppressive rabbit ATG, we now recommend use of irradiated blood components for aplastic anemia patients receiving immunosuppressive therapy with ATG (and/or alemtuzumab). (Grade 2 recommendation; level C evidence, BCSH 2010; ANZSBT 2011) Page 6
7 Recommendation: We cannot make a firm recommendation as to how long irradiated blood components should continue to be used after ATG administration. Autologous bone marrow or peripheral blood hemopoietic stem cell transplantation Recommendation: Patients undergoing bone marrow or peripheral blood stem cell harvesting for future autologous re-infusion should receive irradiated cellular blood components during and for seven (7) days before the bone marrow/stem cell harvest to prevent the collection of viable allogeneic T lymphocytes, which can potentially withstand cryopreservation. (Grade 2 recommendation; level C evidence, BCSH 2010; ANZSBT 2011) Recommendation: All patients undergoing autologous bone marrow transplant or peripheral blood stem cell transplant should receive irradiated cellular components from initiation of conditioning chemo/radiotherapy until three (3) months post-transplant (six months if total body irradiation was used in conditioning). (Grade 2 recommendation; level C evidence, BCSH 2010; ANZSBT 2011) Donations from family members and HLA-selected donors Recommendation: All transfusions from first- or second-degree relatives should be irradiated, even if the patient is immunocompetent. (Grade 1 recommendation; level B evidence, BCSH 2010) Recommendation: All HLA-selected platelets should be irradiated, even if the patient is immunocompetent. (Grade 2 recommendation; level C evidence, BCSH 2010) Lymphoma Recommendation: All adults and children with Hodgkin lymphoma at any stage of the disease should have irradiated red cells and platelets for life. (Grade 1 recommendation; level B evidence, BCSH 2010; ANZSBT 2011) Recommendation: All patients with non-hodgkins lymphoma on purine analogues and related drugs (see appendix A) should receive irradiated cellular blood components indefinitely (Grade 1 recommendation; level B evidence, BCSH 2010) (ANZSBT 2011) Local practices may be dictated by the ability of hospital transfusion medicine services to obtain the patient s drug history. The recommendation encourages the pharmacy to provide the patient s drug utilization information Page 7
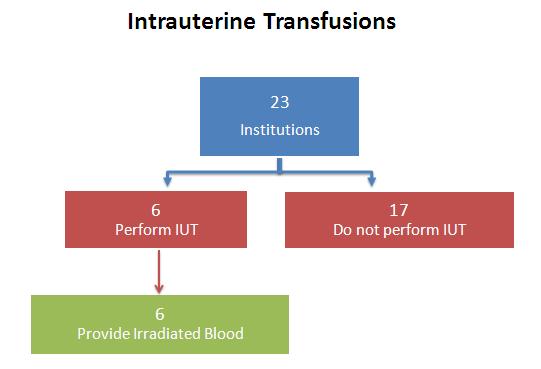
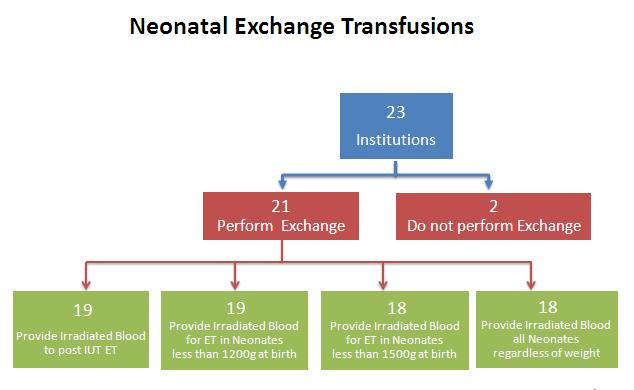
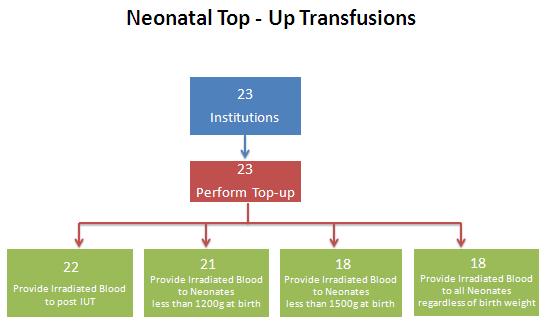
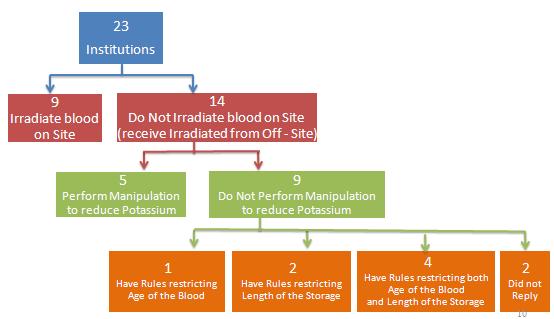
8 Neonatal Transfusions A survey was completed to better understand current practices in Canada regarding the use of irradiated blood components specifically for neonatal populations to inform NAC s recommendations. The survey focused on three clinical scenarios, namely, intrauterine transfusions, top-up transfusions and exchange transfusions in neonates. The survey was sent to the medical directors of transfusion medicine in level three (3) neonatal intensive care nurseries (according to the Neonatal Classification Tool developed in British Columbia). See Appendix B for the survey questions and Appendix C for survey results. The recommendations for neonatal transfusions are as follows: Intra-Uterine Transfusions (IUT): Recommendation: All components for IUT must be irradiated. To minimize the effect of potassium load, red cells for IUT must be used within five (5) days of donation and within 24 hours of irradiation. (Grade 1 recommendation; level B evidence, BCSH 2010) (ANZSBT 2011) Exchange Transfusion: Recommendation: Blood for neonatal exchange transfusion must be irradiated if there has been a previous IUT or if the donation comes from a first- or second-degree relative. (Grade 1 recommendation; level B evidence, BCSH 2010) (ANZSBT 2011) For other neonatal exchange transfusions, irradiation is recommended provided this does not unduly delay transfusion. (Grade 1 recommendation; level C evidence, BCSH 2010) Neonatal Top-up Transfusions: Recommendation: Irradiated cellular components are recommended for neonates who have received an IUT. (BCSH 2010) (ANZSBT 2011) Recommendation: Irradiated cellular components are recommended for top-up transfusions given to neonates less than four (4) months of age with very low birth weights of less than 1200 grams. (survey results; NAC working group and ANZSBT 2011) For top-up transfusions in neonates, NAC recognizes a lack of certainty in published guidelines and recommends that deviations from the aforementioned recommendation may be reflected in local policies that have been developed in consultation with neonatologists Page 8
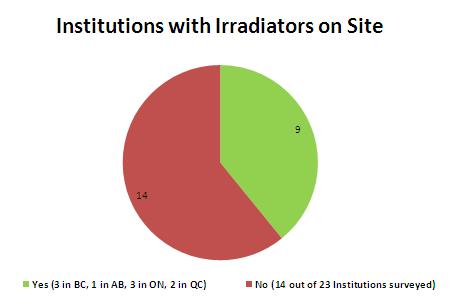
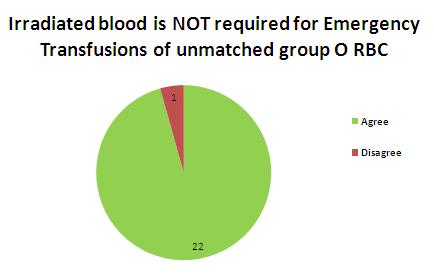
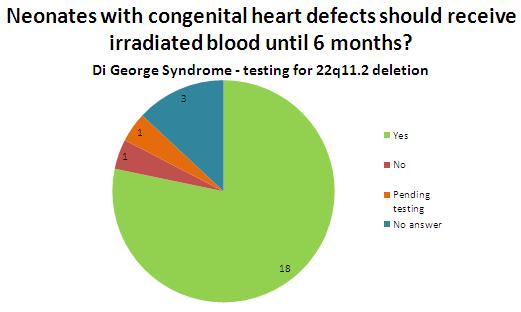
9 For facilities with on-site irradiators, aliquots of irradiated red cells should be irradiated at the time of issue. An alternative approach is recommended for those facilities without onsite irradiation. That is, the use of a single, sterile docked, adult unit for multiple neonates. This unit can be irradiated by the supplier or another hub-site hospital and should be rotated on a weekly basis. This is a practice that is evolving in pediatric centres where the concerns regarding donor exposure are thought to be subordinate to the risks of older blood irradiated prior to storage (Dr. Nancy Robitaille, CCNMT, personal communication). In these facilities, a neonatologist may request a dedicated unit when it is anticipated that the neonate will require many red blood cell transfusions. If that is the case and on-site irradiation is not available, consideration should be given to a procedure for saline replacement of the supernatant of aliquots that are prepared more than seven (7) days post irradiation of the parent unit. Recommendation: Where the patient is at particular risk from hyperkalemia, e.g. intrauterine or neonatal exchange transfusion, it is recommended that red cells be transfused within 24 hours of irradiation or that cells are washed. (BCSH 2010) (ANZSBT 2011) Emergency Transfusions: Recommendation: For emergency transfusions of unmatched group O, D-negative red cells for neonatal resuscitation due to obstetrical complications and/or accidents, irradiated cellular components are NOT required (survey results; NAC working group). Congenital Cardiac Abnormalities: Recommendation: All neonates with complex cardiac abnormalities should receive irradiated cellular components until 22q11.2 deletion associated with immunodeficiency states, which include DiGeorge Syndrome, have been excluded. If 22q11.2 deletion is confirmed, irradiated cellular components should be provided for life (survey results; NAC working group). Purine analogue drugs and other potent immunosuppressive drugs Recommendation: Patients treated with purine analogue drugs (fludarabine, cladribine and deoxycoformicin) should receive irradiated blood components indefinitely. (Grade 1 recommendation; level B evidence, BCSH 2010; ANZSBT 2011) Recommendation: The situation with other purine antagonists and new or related agents, such as bendamustine and clofarabine, is unclear, but use of irradiated blood components is recommended as these agents have a similar mode of action. Irradiated blood components should be used after alemtuzumab (anti-cd52) therapy. Their use after rituximab (anti-cd20) is not recommended at this time. As new potent immunosuppressive drugs and biological agents are introduced into practice there is a need for regular review of these recommendations Page 9
10 (Grade 2 recommendation; level C evidence, BCSH 2010) Recommendation: Where there is concern about the immunosuppressive potency of new drugs and uncertainty about the risk of TA-GVHD, in the absence of on-site irradiation or pre-storage irradiated inventory, pre-storage leukoreduced red cells that have been stored for more than 14 days should be provided. Routine surgery, solid tumors, organ transplantation, autoimmune disorders, acquired immunodeficiency Recommendation: It is not necessary to irradiate blood components for patients undergoing routine surgery, those with solid tumours, HIV infection, autoimmune diseases or after solid organ transplantation (unless alemtuzumab (anti-cd52) has been used in the conditioning regimen). The effects of new regimens of chemo- and immunotherapy entering clinical practice must continue to be monitored. (Grade 2 recommendation; level C evidence, BCSH 2010) Page 10
11 REFERENCES Annual Serious Hazards of Transfusion Medicine (SHOT) Report, (2014). Retrieved from Canadian Standards Association (CSA) Blood and Blood Components. Z (2015). Mississauga ON: Canadian Standards Association. Canadian Society for Transfusion Medicine (CSTM) Standards for Hospital Transfusion Services, Version 3, February Council of Europe, European Committee (Partial Agreement) on Blood Transfusion, Guide to the preparation, use and quality assurance of blood components. 17 th edition (2013). Guidelines on the use of irradiated blood components prepared by the British Committee for Standards in Haematology blood transfusion task force. British Journal of Haematology 152: 35-51, Guidelines for prevention of transfusion-associated graft-versus-host disease (TA-GVHD). Australian and New Zealand Society of Blood Transfusion Ltd., 1 st edition, January: 1-25, Jawa RS, Young DH, Stothert JC, Kulaylat MN and Landmark JD. Transfusion-associated graft versus host disease in the immunocompetent patient: an ongoing problem. Journal of Intensive Care Medicine 30(3): , Kopolovic I, Ostro J, Tsubota H, Lin Y, Cserti-Gazdewich CM, Messner HA, Keir AK, DenHollander N, Dzik WS and Callum J. A systematic review of transfusion-associated graftversus-host disease. Blood 126 (3): , July Rühl H, Bein G and Sachs UJH. Transfusion-associated graft-versus-host disease. Transfusion Medicine Reviews 23 (1): 62-71, Serrano K, Chen D, Hansen AL, Turner TR, Kurach JDR, Acker JP and Devine DV. The effect of timing of gamma-irradiation on hemolysis and potassium release in leukoreduced red cell concentrates stored in SAGM. Vox Sanguinis 106 (4): , Transfusion Medicine Medical Policy Manual, Irradiation of Blood Components Section 6.2, Version 3.0 (2015), British Columbia Provincial Blood Coordinating Office Uchida S, Tadokoro K, Takahashi M, Yahagi H, Satake M and Juji. Analysis of 66 patients with definitive transfusion-associated graft-versus-host disease and the effect of universal irradiation of blood. Transfusion Medicine, 23: , Williamson LM, Stainsby D, Jones H, et al. The impact of universal leukodepletion of the blood supply on hemovigilance reports of posttransfusion purpura and transfusion-associated graftversus-host disease. Transfusion 47 (8): , Zimmermann R, Schoetz AM, Frisch A, Hauck B, Weiss D, Strobel J and Echstein EtR. Influence of late irradiation on the in vitro RBC storage variables of leucoreduced RBCs in SAGM additive solution. Vox Sanguinis 100: , Page 11
12 APPENDIX A Quick Reference of Indications for Irradiated Blood Components Patient Category Condition Irradiated Pregnancy Intrauterine, fetal transfusion Neonates Neonatal exchange transfusion: Previous IUT All neonatal exchange transfusions provided it does not unduly delay transfusion Hematology Transplant Neonatal top-up transfusions Previous IUT Less than 4 months of age with very low birth weights (< 1200g) Consult local policies in uncertain situations Neonatal emergency transfusions: NOT required for unmatched group O, D-negative red cells Congenital cardiac abnormalities: Until 22q11.2 deletion has been excluded Confirmed 22q11.2 deletion Acute leukemia ONLY in these situations: HLA-selected platelets Donations from first- or second- degree relatives Aplastic Anemia Patients receiving immunosuppressive therapy with ATG (and/or alemtuzumab) Hodgkin s Lymphoma at any stage Non-Hodgkin s Lymphoma and being treated with purine analogues and related drugs Allogeneic haematopoietic stem cell or bone marrow transplant recipients, from the time of initiation of conditioning chemotherapy while the patient continues to receive GVHD prophylaxis, i.e. usually 6 months post transplant or until the lymphocyte count is greater than 1x10 9 /L. No Page 12
13 indefinitely if chronic GVHD is present or if continued immunosuppressive therapy is required Miscellaneous Allogeneic blood transfused to stem cell or bone marrow transplant donors for 7 days prior to and during the harvest Autologous stem cell or bone marrow transplant recipients from the initiation of conditioning chemo/radiation therapy to 3 months post-transplant Patients undergoing harvesting for future autologous reinfusion Patients known to have received potent immunosuppressive drugs. See table below. Directed Donation (from first- and second- degree relatives) HLA matched platelets Granulocyte transfusion Potent Immunosuppressive drugs thought to increase risk of GVHD GENERIC Name Fludarbine Cladribine or 2-CDA Deoxycoformicin Alemtuzumab (anti-cd52) Bendamustine Clofarabine TRADE Name Fludara Leustatin Pentostatin or Nipent Campath Treakisym, Ribomustin, Levact and Treanda Clolar Page 13
14 APPENDIX B Survey Questions 1. Please provide us with some information on your hospital. Note: Please answer the following questions for each hospital that you oversee. For example, if you are responsible for two hospitals, please complete this survey twice with responses specific to each institution. 1a. Name of institution. 1b. Level of care provided in your neonatal intensive care unit? Level 1 Level 2 Level 3 Use the BC NICU ClassificationTool_Perinatal Services BC.pdf classification scheme when determining your Level of Care. 1c. Which of the following types of transfusions are performed in your institution? (select all that apply) Intrauterine transfusion Neonatal exchange transfusion Neonatal top-up transfusion Emergency unmatched for neonatal resuscitation 2. Is there a policy requiring provision of irradiated cellular blood components for any of the following: 2a. Intrauterine transfusion? No Not performed at our hospital 2b. Top-up transfusion in neonates who (select all that apply) Have received intrauterine transfusion: Are less than 1200 grams at birth Are less than 1500 grams at birth All neonates (0-4 months) regardless of birth weight Not performed at our hospital 2c. Exchange transfusion in neonates who (select all that apply) Have received an intrauterine transfusion: Are less than 1200 grams at birth Are less than 1500 grams at birth All neonates (0-4 months) regarless of birth weight Not performed at our hospital 3. Is irradiation of cellular components for neonates done on site at your hospital? Page 14
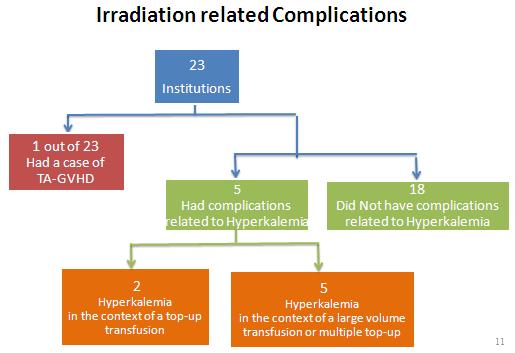
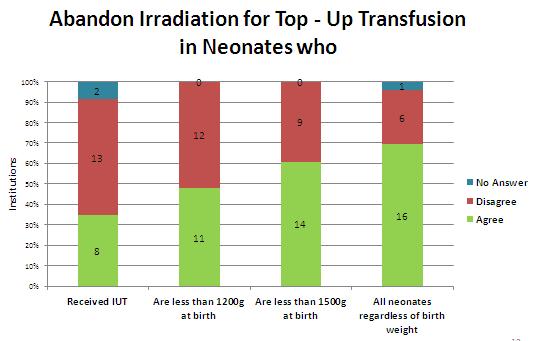
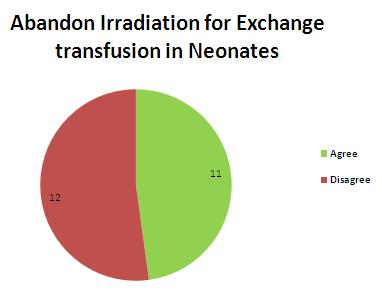
15 No 3a. If not, is there a manipulation of the red cell component to reduce the levels of potassium? No 3b. If not, are there rules restricting: (select all that apply) The age of the blood prior to irradiation The length of storage time post irradiation 4. To your knowledge, has there been a case of neonatal transfusion-associated graftversus-host disease (TA-GVHD) at your hospital? No 5. To your knowledge, have there been complications related to hyperkalemia in neonates receiving irradiated red cells? No 5a. In the context of a top-up transfusion? No 5b. In the context of a large volume transfusion (e.g. cardiac surgery) or multiple top-up transfusions in succession? No 6. Prolonged storage of pre-irradiated red cells is associated with high potassium levels and in-vitro hemolysis. UK SHOT data report only a single case of TA-GVHD since the introduction of universal pre-storage leukocyte reduction in With this in mind: 6a. Would you agree with abandonment of the irradiation requirement for top up transfusions in neonates, who: No 6b. Would you agree with abandonment of the irradiation requirement for neonatal exchange transfusion? No Page 15
16 7. Do you agree with the following statement: For emergency transfusions of unmatched group O, D negative red cells for neonatal resuscitation due to obstetric complications and / or accidents, irradiated cellular components are NOT required? No 8. Do you agree with the following statement: Although 22q11.2 deletion syndrome (encompasses DiGeorge Syndrome) is most commonly associated with conotruncal lesions, the variety of heart defects described in patients with this syndrome is extensive. In order to avoid missing a neonate or young infant with immunodeficiency, it is recommended that neonates and young infants with congenital heart defects receive irradiated cellular components up to 6 months of age, at which time those suspected of having 22q11.2 deletion syndrome should have been tested for this disorder. No 8a. Please indicate your comments, if any: 9. Do you think additional information is needed to improve strategies for preventing TA- GVHD and the usage of irradiation? No 9a. If yes, please indicate your suggestions (randomized controlled trials, systematic reviews, consensus conference, etc.) Page 16


17 APPENDIX C NAC 2016 National Survey Results - Irradiation Practices in Neonatal Transfusion Page 17
18 Page 18
19 Page 19
20 Page 20
21 Page 21
22 Page 22
23 Page 23
Guidelines for Gamma Irradiation of Blood Components
 AUSTRALIAN & NEW ZEALAND SOCIETY OF BLOOD TRANSFUSION INC. AUSTRALIAN RED CROSS BLOOD SERVICE NEW ZEALAND BLOOD SERVICE Guidelines for Gamma Irradiation of Blood Components Revised 2003 AN ZS B T Australian
AUSTRALIAN & NEW ZEALAND SOCIETY OF BLOOD TRANSFUSION INC. AUSTRALIAN RED CROSS BLOOD SERVICE NEW ZEALAND BLOOD SERVICE Guidelines for Gamma Irradiation of Blood Components Revised 2003 AN ZS B T Australian
GUIDELINES FOR IRRADIATED BLOOD COMPONENTS
 GUIDELINES FOR IRRADIATED BLOOD COMPONENTS 1. Policy Statement 2. Definitions 1.1 Blood transfusion services shall have a policy which indicates recipients who are to receive irradiated blood components.
GUIDELINES FOR IRRADIATED BLOOD COMPONENTS 1. Policy Statement 2. Definitions 1.1 Blood transfusion services shall have a policy which indicates recipients who are to receive irradiated blood components.
Transfusion-associated graft-versus-host disease
 CHAPTER 6 Transfusion-associated graft-versus-host disease Eric A. Gehrie, 1 Edward L. Snyder, 1 & Alex B. Ryder 2 1 Department of Laboratory Medicine, Yale School of Medicine, Yale University; and Blood
CHAPTER 6 Transfusion-associated graft-versus-host disease Eric A. Gehrie, 1 Edward L. Snyder, 1 & Alex B. Ryder 2 1 Department of Laboratory Medicine, Yale School of Medicine, Yale University; and Blood
Disclosures. Committee on Blood and Blood Products) Co-investigator CBS Small Project. in Solid Organ Transplant Recipients
 Co-investigator CBS Small Project. in Solid Organ Transplant Recipients") Neonatal Transfusion: Irradiation and CMV 6 th Annual Blood Matters Conference November 6 th, 2015 Disclosures Member of NAC (National Advisory Committee on Blood and Blood Products) Co-investigator CBS
Neonatal Transfusion: Irradiation and CMV 6 th Annual Blood Matters Conference November 6 th, 2015 Disclosures Member of NAC (National Advisory Committee on Blood and Blood Products) Co-investigator CBS
Blood Product Modifications: Leukofiltration, Irradiation and Washing
 1. Leukocyte Reduction Definitions and Standards: o Process also known as leukoreduction, or leukofiltration o Applicable AABB Standards, 25th ed. Leukocyte-reduced RBCs At least 85% of original RBCs
1. Leukocyte Reduction Definitions and Standards: o Process also known as leukoreduction, or leukofiltration o Applicable AABB Standards, 25th ed. Leukocyte-reduced RBCs At least 85% of original RBCs
Transfusion-Associated Graft-versus-Host Disease TRANSFUSION-ASSOCIATED GRAFT-VERSUS-HOST DISEASE
 TRANSFUSION-ASSOCIATED GRAFT-VERSUS-HOST DISEASE D H Pamphilon for the NBS Transfusion Medicine Clinical Policies Group. Membership: M F Murphy (Chair), A Copplestone, M Gesinde, S MacLennan, C Morgan,
TRANSFUSION-ASSOCIATED GRAFT-VERSUS-HOST DISEASE D H Pamphilon for the NBS Transfusion Medicine Clinical Policies Group. Membership: M F Murphy (Chair), A Copplestone, M Gesinde, S MacLennan, C Morgan,
A Review of Guidelines and Evidence for the Use of Irradiated Blood Products in Solid Tumor, Chemotherapy Patients. Chris Kim 11/29/12
 A Review of Guidelines and Evidence for the Use of Irradiated Blood Products in Solid Tumor, Chemotherapy Patients Chris Kim 11/29/12 Background Prevention of TAGVHD Irradiation: induces DNA crosslinks,
A Review of Guidelines and Evidence for the Use of Irradiated Blood Products in Solid Tumor, Chemotherapy Patients Chris Kim 11/29/12 Background Prevention of TAGVHD Irradiation: induces DNA crosslinks,
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Policy for the use of Irradiated blood products
 Policy for the use of Irradiated blood products SharePoint Location General Policies and Guidelines SharePoint Index Directory Haematology and Blood Transfusion Sub Area - Key words (for search purposes)
Policy for the use of Irradiated blood products SharePoint Location General Policies and Guidelines SharePoint Index Directory Haematology and Blood Transfusion Sub Area - Key words (for search purposes)
Specific Requirements
 Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
Specific Requirements AIMS Specific requirements your patients have for transfusion and how this is managed Classify which patients require: Irradiated components CMV negative components Washed components
CTYOMEGALOVIRUS (CMV) - BACKGROUND
 - BACKGROUND") CTYOMEGALOVIRUS (CMV) - BACKGROUND PURPOSE The flowing information provides guidance on the use of CMV negative blood components provided by the blood bank at the Royal Children s Hospital (RCH) including
CTYOMEGALOVIRUS (CMV) - BACKGROUND PURPOSE The flowing information provides guidance on the use of CMV negative blood components provided by the blood bank at the Royal Children s Hospital (RCH) including
with special requirements Contributes to: CQC Regulation 12 Consulted With Individual/Body Date Lead
 Special Requirements for Blood Transfusion Policy Register No: 16015 Status: Public Developed in response to: NHSBT & SaBTO guidance for patients with special requirements Contributes to: CQC Regulation
Special Requirements for Blood Transfusion Policy Register No: 16015 Status: Public Developed in response to: NHSBT & SaBTO guidance for patients with special requirements Contributes to: CQC Regulation
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
UKGS TRANSFUSION SERVICE PRODUCTS AND AVAILABILITY
 Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
QUICK REFERENCE Clinical Practice Guide on Red Blood Cell Transfusion
 QUICK REFERENCE 2012 Clinical Practice Guide on Red Blood Cell Transfusion Presented by the American Society of Hematology, adapted from Red Blood Cell Transfusion: A Clinical Practice Guideline from the
QUICK REFERENCE 2012 Clinical Practice Guide on Red Blood Cell Transfusion Presented by the American Society of Hematology, adapted from Red Blood Cell Transfusion: A Clinical Practice Guideline from the
Preventing CMV Transmission through Leukodepletion
 Preventing CMV Transmission through Leukodepletion Possibility & Facts Prof.S.B.Rajadhyaksha, MD,DTM,PGDMLS Head, Dept. of Transfusion Medicine Tata Memorial Hospital, Mumbai 1 Donor Leukocytes Linked
Preventing CMV Transmission through Leukodepletion Possibility & Facts Prof.S.B.Rajadhyaksha, MD,DTM,PGDMLS Head, Dept. of Transfusion Medicine Tata Memorial Hospital, Mumbai 1 Donor Leukocytes Linked
Zika Virus. Report to the Standing Committee on Health. Dr. Graham Sher Chief Executive Officer, Canadian Blood Services
 Dr. Graham Sher Chief Executive Officer, Services Dr. Dana Devine Chief Medical and Scientific Officer, Services Services Services is an arm s-length organization within the larger health-care system of
Dr. Graham Sher Chief Executive Officer, Services Dr. Dana Devine Chief Medical and Scientific Officer, Services Services Services is an arm s-length organization within the larger health-care system of
Transfusion-transmitted Cytomegalovirus
 Transfusion-transmitted Cytomegalovirus Can you confidently abandon CMV seronegative products in the modern era of pre-storage leukoreduction? Jeannie Callum, BA, MD, FRCPC Really? Are we still talking
Transfusion-transmitted Cytomegalovirus Can you confidently abandon CMV seronegative products in the modern era of pre-storage leukoreduction? Jeannie Callum, BA, MD, FRCPC Really? Are we still talking
Apheresis: Transfusion Indications. Sasha Wilson: Transfusion Senior Nurse
 Apheresis: Transfusion Indications Sasha Wilson: Transfusion Senior Nurse Apheresis: Transfusion Indications Focus of talk will be blood component transfusion in the context of apheresis procedures: Special
Apheresis: Transfusion Indications Sasha Wilson: Transfusion Senior Nurse Apheresis: Transfusion Indications Focus of talk will be blood component transfusion in the context of apheresis procedures: Special
5/1/2012 FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA IN CANADA
 FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA IN CANADA - 1 - FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA BACKGROUND: The National
FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA IN CANADA - 1 - FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA BACKGROUND: The National
Transfusion Medicine Update and Cases. OAP September 16, 2017
 Transfusion Medicine Update and Cases OAP September 16, 2017 Objectives 1. Explain the rationale for limiting the use of group O negative red cells. 2. List the indications for the use of irradiated and
Transfusion Medicine Update and Cases OAP September 16, 2017 Objectives 1. Explain the rationale for limiting the use of group O negative red cells. 2. List the indications for the use of irradiated and
FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA IN CANADA
 FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA IN CANADA - 1 - FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA BACKGROUND: The National
FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA IN CANADA - 1 - FRAMEWORK FOR APPROPRIATE USE AND DISTRIBUTION OF SOLVENT DETERGENT TREATED PLASMA BACKGROUND: The National
BLOOD TRANSFUSION. Dr Lumka Ntabeni
 BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
Blood Transfusion. What is blood transfusion? What are blood banks? When is a blood transfusion needed? Who can donate blood?
 What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
Blood & Blood Product Administration
 Approved by: Blood & Blood Product Administration Addendum to: Corporate Policy VII-B-397 Transfusion of Blood Components and Products- Pediatric/Neonate Gail Cameron Senior Director Operations, Maternal,
Approved by: Blood & Blood Product Administration Addendum to: Corporate Policy VII-B-397 Transfusion of Blood Components and Products- Pediatric/Neonate Gail Cameron Senior Director Operations, Maternal,
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem_cell_transplantation_for_waldenstrom_macroglobulinemia
Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem_cell_transplantation_for_waldenstrom_macroglobulinemia
Special Requirements Lab Matters. 18 th May Katy Cowan PBM Practitioner NHSBT
 Special Requirements Lab Matters. 18 th May 2016 Katy Cowan PBM Practitioner NHSBT Special requirements Frozen components and platelets HEV negative Irradiated CMV negative Frozen components and platelets
Special Requirements Lab Matters. 18 th May 2016 Katy Cowan PBM Practitioner NHSBT Special requirements Frozen components and platelets HEV negative Irradiated CMV negative Frozen components and platelets
TRANSFUSION ASSOCIATED DISEASE, RECALL, OR COMPLICATION INVESTIGATION POLICY I. FATALITIES AND COMPLICATIONS ASSOCIATED WITH TRANSFUSION:
 I. FATALITIES AND COMPLICATIONS ASSOCIATED WITH TRANSFUSION: A. TRANSFUSION RELATED FATALITY: FDA and MEDIC must be notified immediately, and subsequently in writing, when a possible transfusion related
I. FATALITIES AND COMPLICATIONS ASSOCIATED WITH TRANSFUSION: A. TRANSFUSION RELATED FATALITY: FDA and MEDIC must be notified immediately, and subsequently in writing, when a possible transfusion related
All institutions that transfuse blood components and products should implement national and local policies and written procedures for:
 5.0 GENERAL GUIDE TO GOOD TRANSFUSION PRACTICE Blood and the various components prepared or manufactured from it are biologic (in the case of blood cells, living human tissues) products intended for use
5.0 GENERAL GUIDE TO GOOD TRANSFUSION PRACTICE Blood and the various components prepared or manufactured from it are biologic (in the case of blood cells, living human tissues) products intended for use
Riposta immune versus stato immune
 Riposta immune versus stato immune Russell E. Lewis U.O. Malattie Infettive, Policlinico S. Orsola-Malpighi Dipartimento di Scienze Mediche e Chirurgiche Alma Mater Studiorum Università di Bologna Immunodeficiency
Riposta immune versus stato immune Russell E. Lewis U.O. Malattie Infettive, Policlinico S. Orsola-Malpighi Dipartimento di Scienze Mediche e Chirurgiche Alma Mater Studiorum Università di Bologna Immunodeficiency
PUO in the Immunocompromised Host: CMV and beyond
 PUO in the Immunocompromised Host: CMV and beyond PUO in the immunocompromised host: role of viral infections Nature of host defect T cell defects Underlying disease Treatment Nature of clinical presentation
PUO in the Immunocompromised Host: CMV and beyond PUO in the immunocompromised host: role of viral infections Nature of host defect T cell defects Underlying disease Treatment Nature of clinical presentation
Consent Laboratory Transfuse RBC
 Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Special Requirements Lab Matters. 21 st June Barrie Ferguson
 Special Requirements Lab Matters. 21 st June 2017 Barrie Ferguson Special requirements Patients requiring Methylene Blue or Solvent Detergent treated Fresh Frozen Plasma Patients requiring apheresis platelets
Special Requirements Lab Matters. 21 st June 2017 Barrie Ferguson Special requirements Patients requiring Methylene Blue or Solvent Detergent treated Fresh Frozen Plasma Patients requiring apheresis platelets
OneMatch Stem Cell and Marrow Network. Training Guide
 OneMatch Stem Cell and Marrow Network Training Guide What is OneMatch all about? OneMatch is a Canadian Program that matches and coordinates the collection of stem cells from potential donors to help save
OneMatch Stem Cell and Marrow Network Training Guide What is OneMatch all about? OneMatch is a Canadian Program that matches and coordinates the collection of stem cells from potential donors to help save
What s a Transplant? What s not?
 What s a Transplant? What s not? How to report the difference? Daniel Weisdorf MD University of Minnesota Anti-cancer effects of BMT or PBSCT [HSCT] Kill the cancer Save the patient Restore immunocompetence
What s a Transplant? What s not? How to report the difference? Daniel Weisdorf MD University of Minnesota Anti-cancer effects of BMT or PBSCT [HSCT] Kill the cancer Save the patient Restore immunocompetence
Carol Cantwell Blood Transfusion Laboratory Manager St Mary s Hospital, ICHNT
 Carol Cantwell Blood Transfusion Laboratory Manager St Mary s Hospital, ICHNT History Why is blood transfusion involved? What tests are performed in blood transfusion and why? What does a protocol look
Carol Cantwell Blood Transfusion Laboratory Manager St Mary s Hospital, ICHNT History Why is blood transfusion involved? What tests are performed in blood transfusion and why? What does a protocol look
Guide to the preparation, use and quality assurance of blood components
 Contents Foreword...3 Members of the European Committee (Partial Agreement) on Blood Transfusion... 8 Members of the GTS working group... 22 Members of the TS066 working group... 30 Recommendation No.
Contents Foreword...3 Members of the European Committee (Partial Agreement) on Blood Transfusion... 8 Members of the GTS working group... 22 Members of the TS066 working group... 30 Recommendation No.
5/9/2018. Bone marrow failure diseases (aplastic anemia) can be cured by providing a source of new marrow
 can be cured by providing a source of new marrow") 5/9/2018 or Stem Cell Harvest Where we are now, and What s Coming AA MDS International Foundation Indianapolis IN Luke Akard MD May 19, 2018 Infusion Transplant Conditioning Treatment 2-7 days STEM CELL
5/9/2018 or Stem Cell Harvest Where we are now, and What s Coming AA MDS International Foundation Indianapolis IN Luke Akard MD May 19, 2018 Infusion Transplant Conditioning Treatment 2-7 days STEM CELL
In The Name Of GOD ADVERSE REACTIONS OF TRANSFUSION
 In The Name Of GOD The 7 th international and 12 th national congress on quality improvement in clinical laboratories ADVERSE REACTIONS OF TRANSFUSION By Mehdi Allahbakhshian, PhD, Hematology and Blood
In The Name Of GOD The 7 th international and 12 th national congress on quality improvement in clinical laboratories ADVERSE REACTIONS OF TRANSFUSION By Mehdi Allahbakhshian, PhD, Hematology and Blood
Non-Medical Authorisation Course
 Non-Medical Authorisation Course November 2017 Authorising, Prescribing & Sampling Janice Smith Matron Transfusion Specialist Aims of this session To discuss and understand: Authorising blood / blood components
Non-Medical Authorisation Course November 2017 Authorising, Prescribing & Sampling Janice Smith Matron Transfusion Specialist Aims of this session To discuss and understand: Authorising blood / blood components
Rob Wynn RMCH & University of Manchester, UK. HCT in Children
 Rob Wynn RMCH & University of Manchester, UK HCT in Children Summary Indications for HCT in children Donor selection for Paediatric HCT Using cords Achieving engraftment in HCT Conditioning Immune action
Rob Wynn RMCH & University of Manchester, UK HCT in Children Summary Indications for HCT in children Donor selection for Paediatric HCT Using cords Achieving engraftment in HCT Conditioning Immune action
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 well structured and organized, provided perc with a much deeper understanding of patients experiences with relapse or refractory CLL/SLL and its treatment. perc deliberated upon the cost effectiveness
well structured and organized, provided perc with a much deeper understanding of patients experiences with relapse or refractory CLL/SLL and its treatment. perc deliberated upon the cost effectiveness
APPROACH TO RISK MANAGEMENT IN MEDICAL PRACTICE: STANDPOINT OF THE BLOOD TRASFUSION*
 11 APPROACH TO RISK MANAGEMENT IN MEDICAL PRACTICE: STANDPOINT OF THE BLOOD TRASFUSION* Hisami IKEDA** Asian Med. J. 44(1): 11 21, 2000 Abstract: In the field of blood transfusion, risk management is defined
11 APPROACH TO RISK MANAGEMENT IN MEDICAL PRACTICE: STANDPOINT OF THE BLOOD TRASFUSION* Hisami IKEDA** Asian Med. J. 44(1): 11 21, 2000 Abstract: In the field of blood transfusion, risk management is defined
2. Is therapy prescribed by, or in consultation with, a hematologist and/or oncologist?
 Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Colony Stimulating Factors (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Colony Stimulating Factors (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Chapter 13. DiGeorge Syndrome
 Chapter 13 DiGeorge Syndrome DiGeorge Syndrome is a primary immunodeficiency disease caused by abnormal migration and development of certain cells and tissues during fetal development. As part of the developmental
Chapter 13 DiGeorge Syndrome DiGeorge Syndrome is a primary immunodeficiency disease caused by abnormal migration and development of certain cells and tissues during fetal development. As part of the developmental
BMTCN REVIEW COURSE PRE-TRANSPLANT CARE
 BMTCN REVIEW COURSE PRE-TRANSPLANT CARE Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to edit the Master Experts
BMTCN REVIEW COURSE PRE-TRANSPLANT CARE Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to edit the Master Experts
Setting The setting was secondary care. The economic analysis was carried out in Canada.
 Allogeneic stem cell transplantation: an economic comparison of bone marrow, peripheral blood, and cord blood technologies Jacobs P, Hailey D, Turner R, MacLean N Record Status This is a critical abstract
Allogeneic stem cell transplantation: an economic comparison of bone marrow, peripheral blood, and cord blood technologies Jacobs P, Hailey D, Turner R, MacLean N Record Status This is a critical abstract
Stem cells. -Dr Dinesh Bhurani, MD, DM, FRCPA. Rajiv Gandhi Cancer Institute, Delhi, -Director, Department of Haematology and BMT
 Stem cells -Dr Dinesh Bhurani, MD, DM, FRCPA -Director, Department of Haematology and BMT Rajiv Gandhi Cancer Institute, Delhi, Flow of presentation Update on stem cell uses Haematopoietic stem cell transplantation
Stem cells -Dr Dinesh Bhurani, MD, DM, FRCPA -Director, Department of Haematology and BMT Rajiv Gandhi Cancer Institute, Delhi, Flow of presentation Update on stem cell uses Haematopoietic stem cell transplantation
Transfusion Medicine Best Practices: Indications for Blood Components
 Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Cell Transplantation for CLL and SLL File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_cll_and_sll 2/2001
Corporate Medical Policy Hematopoietic Cell Transplantation for CLL and SLL File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_cll_and_sll 2/2001
Policy for the use of Cytomegalovirus (CMV) negative blood products
 negative blood products") Policy for the use of Cytomegalovirus (CMV) negative blood products SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory Cancer and Specialist Care Sub Area Haematology and Blood
Policy for the use of Cytomegalovirus (CMV) negative blood products SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory Cancer and Specialist Care Sub Area Haematology and Blood
RITUXAN (rituximab and hyaluronidase human)
") Drug Prior Authorization Guideline RITUXIMAB products J9310 RITUXAN (rituximab and hyaluronidase human) PA9847 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria
Drug Prior Authorization Guideline RITUXIMAB products J9310 RITUXAN (rituximab and hyaluronidase human) PA9847 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Autoimmune Diseases File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_autoimmune_diseases
Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Autoimmune Diseases File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_autoimmune_diseases
The role of HLA in Allogeneic Hematopoietic Stem Cell Transplantation and Platelet Refractoriness.
 The role of HLA in Allogeneic Hematopoietic Stem Cell Transplantation and Platelet Refractoriness. Robert Liwski, MD, PhD, FRCPC Medical Director HLA Typing Laboratory Department of Pathology Dalhousie
The role of HLA in Allogeneic Hematopoietic Stem Cell Transplantation and Platelet Refractoriness. Robert Liwski, MD, PhD, FRCPC Medical Director HLA Typing Laboratory Department of Pathology Dalhousie
Hematopoietic Stem Cell Therapy
 Hematopoietic Stem Cell Therapy Grace Totoe, MBChB, SBB CME August 2012 Accra-Ghana Hematopoietic Stem Cells Cells capable of self renewal and differentiation into all blood cell lineages Objectives Historical
Hematopoietic Stem Cell Therapy Grace Totoe, MBChB, SBB CME August 2012 Accra-Ghana Hematopoietic Stem Cells Cells capable of self renewal and differentiation into all blood cell lineages Objectives Historical
Atgam (lymphocyte immune globulin, anti-thymocyte globulin [equine])
![Atgam (lymphocyte immune globulin, anti-thymocyte globulin [equine])](/thumbs/83/88936551.jpg "Atgam (lymphocyte immune globulin, anti-thymocyte globulin [equine])") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.20.01 Subject: Atgam Page: 1 of 5 Last Review Date: June 24, 2016 Atgam Description Atgam (lymphocyte
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.20.01 Subject: Atgam Page: 1 of 5 Last Review Date: June 24, 2016 Atgam Description Atgam (lymphocyte
High Intensity Chemotherapy Guidelines for Haematology Patients at ASPH
 High Intensity Chemotherapy Guidelines for Haematology Patients at ASPH Contents: Page No. 1. Overview 2 2. Admission 3 3. Admission Checklist 5 4. Inpatient management during chemotherapy 6 5. Inpatient
High Intensity Chemotherapy Guidelines for Haematology Patients at ASPH Contents: Page No. 1. Overview 2 2. Admission 3 3. Admission Checklist 5 4. Inpatient management during chemotherapy 6 5. Inpatient
BMTCN Review Course Basic Concepts and Indications for Transplantation How the Experts Treat Hematologic Malignancies Las Vegas, NV, March 10, 2016
 BMTCN Review Course Basic Concepts and Indications for Transplantation How the Experts Treat Hematologic Malignancies Las Vegas, NV, March 10, 2016 David Rice, PhD, RN, NP Director, Professional Practice
BMTCN Review Course Basic Concepts and Indications for Transplantation How the Experts Treat Hematologic Malignancies Las Vegas, NV, March 10, 2016 David Rice, PhD, RN, NP Director, Professional Practice
NAC Work Plan 2016/2017
 Contingency initiatives led by the NAC Blood Shortages Working Group(BSWG) National Plan for the Management of Shortages of Labile Blood Components Plan for a national mock blood shortage (red phase) which
Contingency initiatives led by the NAC Blood Shortages Working Group(BSWG) National Plan for the Management of Shortages of Labile Blood Components Plan for a national mock blood shortage (red phase) which
BLOOD COMPONENT SUPPORT OF RhD NEGATIVE INDIVIDUALS
 REASON FOR ISSUE: Review of section 4 along with changes in requirement to inform TMS in respect of authorisation process (in Appendix A) DCR16969. 1. INTRODUCTION of RhD positive blood components to an
REASON FOR ISSUE: Review of section 4 along with changes in requirement to inform TMS in respect of authorisation process (in Appendix A) DCR16969. 1. INTRODUCTION of RhD positive blood components to an
All you wanted to know about transfusion support for transplants
 All you wanted to know about transfusion support for transplants Dr Dora Foukaneli NHSBT and Addenbrooke s Hospital Cambridge When / why / why not? What ABO group? Do other groups matter? Transplantation
All you wanted to know about transfusion support for transplants Dr Dora Foukaneli NHSBT and Addenbrooke s Hospital Cambridge When / why / why not? What ABO group? Do other groups matter? Transplantation
Federica Galaverna, 1 Daria Pagliara, 1 Deepa Manwani, 2 Rajni Agarwal-Hashmi, 3 Melissa Aldinger, 4 Franco Locatelli 1
 Administration of Rivogenlecleucel (Rivo-cel, BPX-501) Following αβ T- and B-Cell Depleted Haplo-HSCT in Children With Transfusion-Dependent Thalassemia Federica Galaverna, 1 Daria Pagliara, 1 Deepa Manwani,
Administration of Rivogenlecleucel (Rivo-cel, BPX-501) Following αβ T- and B-Cell Depleted Haplo-HSCT in Children With Transfusion-Dependent Thalassemia Federica Galaverna, 1 Daria Pagliara, 1 Deepa Manwani,
Stem Cell Transplantation for Severe Aplastic Anemia
 Number of Transplants 10/24/2011 Stem Cell Transplantation for Severe Aplastic Anemia Claudio Anasetti, MD Professor of Oncology and Medicine Chair, Blood and Marrow Transplant Dpt Moffitt Cancer Center
Number of Transplants 10/24/2011 Stem Cell Transplantation for Severe Aplastic Anemia Claudio Anasetti, MD Professor of Oncology and Medicine Chair, Blood and Marrow Transplant Dpt Moffitt Cancer Center
Kymriah. Kymriah (tisagenlecleucel) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.101 Subject: Kymriah Page: 1 of 5 Last Review Date: September 20, 2018 Kymriah Description Kymriah
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.101 Subject: Kymriah Page: 1 of 5 Last Review Date: September 20, 2018 Kymriah Description Kymriah
Clinical Policy: Idelalisib (Zydelig) Reference Number: ERX.SPA.269 Effective Date:
 Reference Number: ERX.SPA.269 Effective Date:") Clinical Policy: (Zydelig) Reference Number: ERX.SPA.269 Effective Date: 12.01.18 Last Review Date: 11.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Zydelig) Reference Number: ERX.SPA.269 Effective Date: 12.01.18 Last Review Date: 11.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
General Terms: Appendix B. National Marrow Donor Program and The Medical College of Wisconsin
 Glossary of Terms This appendix is divided into two sections. The first section, General Terms, defines terms used throughout the CIBMTR data collection forms. The second section, FormsNet TM 2 Terms,
Glossary of Terms This appendix is divided into two sections. The first section, General Terms, defines terms used throughout the CIBMTR data collection forms. The second section, FormsNet TM 2 Terms,
QUICK REFERENCE Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP)
") QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
QUICK REFERENCE 2011 Clinical Practice Guideline on the Evaluation and Management of Immune Thrombocytopenia (ITP) Presented by the American Society of Hematology, adapted from: The American Society of
DEPARTMENT OF HEALTH AND SENIOR SERVICES PO BOX 360 TRENTON, N.J
 JON S. CORZINE Governor DEPARTMENT OF HEALTH AND SENIOR SERVICES PO BOX 360 TRENTON, N.J. 08625-0360 www.nj.gov/health HEATHER HOWARD Commissioner TO: FROM: Public Health Council Heather Howard Commissioner
JON S. CORZINE Governor DEPARTMENT OF HEALTH AND SENIOR SERVICES PO BOX 360 TRENTON, N.J. 08625-0360 www.nj.gov/health HEATHER HOWARD Commissioner TO: FROM: Public Health Council Heather Howard Commissioner
Hematopoietic Stem Cells, Stem Cell Processing, and Transplantation
 Hematopoietic Stem Cells, Stem Cell Processing, and Joseph (Yossi) Schwartz, M irector, Hemotherapy and Stem Cell Processing Facility Bone Marrow Can Cure: Leukemia Lymphoma Multiple Myeloma Genetic iseases:
Hematopoietic Stem Cells, Stem Cell Processing, and Joseph (Yossi) Schwartz, M irector, Hemotherapy and Stem Cell Processing Facility Bone Marrow Can Cure: Leukemia Lymphoma Multiple Myeloma Genetic iseases:
Clinical Policy: Donor Lymphocyte Infusion
 Clinical Policy: Reference Number: PA.CP.MP.101 Effective Date: 01/18 Last Review Date: 11/16 Coding Implications Revision Log This policy describes the medical necessity requirements for a donor lymphocyte
Clinical Policy: Reference Number: PA.CP.MP.101 Effective Date: 01/18 Last Review Date: 11/16 Coding Implications Revision Log This policy describes the medical necessity requirements for a donor lymphocyte
L 256/32 Official Journal of the European Union
 L 256/32 Official Journal of the European Union 1.10.2005 COMMISSION DIRECTIVE 2005/61/EC of 30 September 2005 implementing Directive 2002/98/EC of the European Parliament and of the Council as regards
L 256/32 Official Journal of the European Union 1.10.2005 COMMISSION DIRECTIVE 2005/61/EC of 30 September 2005 implementing Directive 2002/98/EC of the European Parliament and of the Council as regards
ADULT TRANSFUSION GUIDELINES ORDERED COMPONENT
 ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
Neutrophil Recovery: The. Posttransplant Recovery. Bus11_1.ppt
 Neutrophil Recovery: The First Step in Posttransplant Recovery No conflicts of interest to disclose Bus11_1.ppt Blood is Made in the Bone Marrow Blood Stem Cell Pre-B White cells B Lymphocyte T Lymphocyte
Neutrophil Recovery: The First Step in Posttransplant Recovery No conflicts of interest to disclose Bus11_1.ppt Blood is Made in the Bone Marrow Blood Stem Cell Pre-B White cells B Lymphocyte T Lymphocyte
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy. Megan Boysen Osborn, MD, MHPE
 Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
Bone Marrow Transplantation and the Potential Role of Iomab-B
 Bone Marrow Transplantation and the Potential Role of Iomab-B Hillard M. Lazarus, MD, FACP Professor of Medicine, Director of Novel Cell Therapy Case Western Reserve University 1 Hematopoietic Cell Transplantation
Bone Marrow Transplantation and the Potential Role of Iomab-B Hillard M. Lazarus, MD, FACP Professor of Medicine, Director of Novel Cell Therapy Case Western Reserve University 1 Hematopoietic Cell Transplantation
Hepatitis E and the English blood supply
 Hepatitis E and the English blood supply Mhairi Webster Microbiology Senior Scientist National Transfusion Microbiology Reference Laboratory With thanks to Dr Alan Kitchen Hepatitis E virus Small, non-enveloped
Hepatitis E and the English blood supply Mhairi Webster Microbiology Senior Scientist National Transfusion Microbiology Reference Laboratory With thanks to Dr Alan Kitchen Hepatitis E virus Small, non-enveloped
An Overview of Blood and Marrow Transplantation
 An Overview of Blood and Marrow Transplantation October 24, 2009 Stephen Couban Department of Medicine Dalhousie University Objectives What are the types of blood and marrow transplantation? Who may benefit
An Overview of Blood and Marrow Transplantation October 24, 2009 Stephen Couban Department of Medicine Dalhousie University Objectives What are the types of blood and marrow transplantation? Who may benefit
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand
 Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
Diagnosis of CMV infection UPDATE ECIL
 UPDATE ECIL-4 2011 Recommendations for CMV and HHV-6 management in patients with hematological diseases Per Ljungman, Rafael de la Camara, Hermann Einsele, Dan Engelhard, Pierre Reusser, Jan Styczynski,
UPDATE ECIL-4 2011 Recommendations for CMV and HHV-6 management in patients with hematological diseases Per Ljungman, Rafael de la Camara, Hermann Einsele, Dan Engelhard, Pierre Reusser, Jan Styczynski,
efs.sante.fr The best blood donor and blood product for each patient: an evolving role for haemovigilance? Pierre Tiberghien Etablissement Français du
 The best blood donor and blood product for each patient: an evolving role for haemovigilance? Pierre Tiberghien Etablissement Français du Sang, St-Denis Université de Franche-Comté, Besançon France Transfusion
The best blood donor and blood product for each patient: an evolving role for haemovigilance? Pierre Tiberghien Etablissement Français du Sang, St-Denis Université de Franche-Comté, Besançon France Transfusion
Summary of Changes Page BMT CTN 1205 Protocol Amendment #4 (Version 5.0) Dated July 22, 2016
 Dated July 22, 2016") Page 1 of 8 Date: July 22, 2016 Summary of Changes Page BMT CTN 1205 Protocol #4 Dated July 22, 2016 The following changes, and the rationale for the changes, were made to the attached protocol in this
Page 1 of 8 Date: July 22, 2016 Summary of Changes Page BMT CTN 1205 Protocol #4 Dated July 22, 2016 The following changes, and the rationale for the changes, were made to the attached protocol in this
CHAPTER 2 PROTOCOL DESIGN
 CHAPTER 2 PROTOCOL DESIGN CHAPTER 2 PROTOCOL DESIGN 2.1 ELIGIBILITY CRITERIA Participants fulfilling the following criteria will be eligible for enrollment in the protocol: 1. Participant is diagnosed
CHAPTER 2 PROTOCOL DESIGN CHAPTER 2 PROTOCOL DESIGN 2.1 ELIGIBILITY CRITERIA Participants fulfilling the following criteria will be eligible for enrollment in the protocol: 1. Participant is diagnosed
Database on Blood Safety 2009 in ECO Member States
 Database on Blood Safety 2009 in ECO Member States Section 1: Administrative Information Information provided by: 1.1 Name: 1.2 Title: 1.3 Position: 1.4 Organization: 1.5 Address: 1.6 Country: 1.7 Tel.
Database on Blood Safety 2009 in ECO Member States Section 1: Administrative Information Information provided by: 1.1 Name: 1.2 Title: 1.3 Position: 1.4 Organization: 1.5 Address: 1.6 Country: 1.7 Tel.
New Advances in Transfusion EM I LY CO BERLY, M D
 New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
An Approach to the Patient Refractory to Platelets Transfusion. Harold Alvarez, MD
 Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
Transfusion reactions illustrated
 Transfusion reactions illustrated Chapter 1 Transfusion practice 1 Procedure of transfusion practice In general, transfusion-associated incidents occur due to multiple errors, most of which occur in the
Transfusion reactions illustrated Chapter 1 Transfusion practice 1 Procedure of transfusion practice In general, transfusion-associated incidents occur due to multiple errors, most of which occur in the
Initial Recommendation for Ibrutinib (Imbruvica) for Mantle Cell Lymphoma perc Meeting: June 16, pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 4
 for Mantle Cell Lymphoma perc Meeting: June 16, pcodr PAN-CANADIAN ONCOLOGY DRUG REVIEW 4") although ibrutinib was associated with significant improvements in PFS and QoL, adverse events such as fatigue and bleeding were still observed in patients who received ibrutinib. perc concluded that overall,
although ibrutinib was associated with significant improvements in PFS and QoL, adverse events such as fatigue and bleeding were still observed in patients who received ibrutinib. perc concluded that overall,
Radiation Injury Treatment Network: Planning for the worst, using experience from hematology & transplantation
 Radiation Injury Treatment Network: Planning for the worst, using experience from hematology & transplantation Daniel Weisdorf, MD University of Minnesota Radiation Injury Treatment Network weisd001@umn.edu
Radiation Injury Treatment Network: Planning for the worst, using experience from hematology & transplantation Daniel Weisdorf, MD University of Minnesota Radiation Injury Treatment Network weisd001@umn.edu
Immunizing the Immunocompromised. Leilani T. Sanchez, MD, DPPS, DPIDSP Crowne Plaza Galleria Manila, 21 February 2013
 Immunizing the Immunocompromised Leilani T. Sanchez, MD, DPPS, DPIDSP Crowne Plaza Galleria Manila, 21 February 2013 WHO World Health Statistics 2012 2 Immunizing the Immunocompromised Leilani T. Sanchez
Immunizing the Immunocompromised Leilani T. Sanchez, MD, DPPS, DPIDSP Crowne Plaza Galleria Manila, 21 February 2013 WHO World Health Statistics 2012 2 Immunizing the Immunocompromised Leilani T. Sanchez
Pharmacy Prior Authorization
 Pharmacy Prior Authorization MERC CARE (MEDICAID) Colony Stimulating Factors (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Pharmacy Prior Authorization MERC CARE (MEDICAID) Colony Stimulating Factors (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
midostaurin should be extended to patients who are deemed fit to receive intensive induction and consolidation, regardless of age.
 midostaurin should be extended to patients who are deemed fit to receive intensive induction and consolidation, regardless of age. perc deliberated on the toxicity profile of midostaurin and noted that
midostaurin should be extended to patients who are deemed fit to receive intensive induction and consolidation, regardless of age. perc deliberated on the toxicity profile of midostaurin and noted that
Overview of Aplastic Anemia. Overview of Aplastic Anemia. Epidemiology of aplastic anemia. Normal hematopoiesis 10/6/2017
 Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Dedicated to Gordon. Stem Cell Transplantation: The Journey
 Dedicated to Gordon Stem Cell Transplantation: The Journey 1949 Jacobson et al: Radioprotection by lead shielding of the spleen of a lethally irradiated animal 1951 Lorenz et al: Radiation protection
Dedicated to Gordon Stem Cell Transplantation: The Journey 1949 Jacobson et al: Radioprotection by lead shielding of the spleen of a lethally irradiated animal 1951 Lorenz et al: Radiation protection
Patient Input CADTH COMMON DRUG REVIEW
 CADTH COMMON DRUG REVIEW Patient Input LETERMOVIR (PREVYMIS) (Merck Canada Inc.) Indication: Text Indicated for the prophylaxis of cytomegalovirus (CMV) infection or disease in adult CMV-seropositive recipients
CADTH COMMON DRUG REVIEW Patient Input LETERMOVIR (PREVYMIS) (Merck Canada Inc.) Indication: Text Indicated for the prophylaxis of cytomegalovirus (CMV) infection or disease in adult CMV-seropositive recipients
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_ transplantation_for_primary_amyloidosis 2/2001 11/2018 11/2019 11/2018 Description
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_ transplantation_for_primary_amyloidosis 2/2001 11/2018 11/2019 11/2018 Description
Hematopoietic Stem Cell Transplant in Sickle Cell Disease- An update
 Hematopoietic Stem Cell Transplant in Sickle Cell Disease- An update Dr Chirag A Shah Diplomate American Board of Hematology and Medical Oncology Director, Dept of Hemato-Oncology and Stem Cell Transplant
Hematopoietic Stem Cell Transplant in Sickle Cell Disease- An update Dr Chirag A Shah Diplomate American Board of Hematology and Medical Oncology Director, Dept of Hemato-Oncology and Stem Cell Transplant
AETNA BETTER HEALTH Non-Formulary Prior Authorization guideline for Colony Stimulating Factor (CSF)
") AETNA BETTER HEALTH Non-Formulary Prior Authorization guideline for Colony Stimulating Factor (CSF) Colony Stimulating Factor (CSF) Neupogen (filgrastim; G-CSF), Neulasta (peg-filgrastim; G-CSF); Neulasa
AETNA BETTER HEALTH Non-Formulary Prior Authorization guideline for Colony Stimulating Factor (CSF) Colony Stimulating Factor (CSF) Neupogen (filgrastim; G-CSF), Neulasta (peg-filgrastim; G-CSF); Neulasa
UKALL14. Non-Myeloablative Conditioning Regimen (1/1) Date started (dd/mm/yyyy) (Day 7) Weight (kg) BSA (m 2 )
 Date started (dd/mm/yyyy) (Day 7) Weight (kg) BSA (m 2 )") Non-Myeloablative Conditioning Regimen (1/1) started (dd/mm/yyyy) (Day 7) BSA (m 2 ) Weight (kg) Please enter the daily dose given in the table below: Day Fludarabine (mg) Melphalan (mg) Alemtuzumab (mg)
Non-Myeloablative Conditioning Regimen (1/1) started (dd/mm/yyyy) (Day 7) BSA (m 2 ) Weight (kg) Please enter the daily dose given in the table below: Day Fludarabine (mg) Melphalan (mg) Alemtuzumab (mg)