ASCO Poster Review PANCREATIC CANCER
|
|
|
- Fay Carr
- 5 years ago
- Views:
Transcription
1 ASCO Poster Review PANCREATIC CANCER Dr.ssa Michela Squadroni U.O. Oncologia Humanitas Gavazzeni Bergamo
2 TOPICAL ISSUES Gemcitabine/Nab-paclitaxel and FOLFIRINOX comparison Neoadjuvant and perioperative treatment New drugs, immunotherapy Genomics and molecular biology

 342 patients with metastatic/locally advanced pancreatic cancer Median")
3 Gemcitabine-Nabpaclitaxel and FOLFIRINOX comparison (first line) AIOM post ASCO Potential first line treatment: FOLFIRINOX or Gemcitabine and Nab-paclitaxel Which one should we use? No comparative prospective trial 861 patients with metastatic pancreatic cancer Median OS 8.5 vs 6.7 months (Gem/Nab-paclitaxel vs Gem) 342 patients with metastatic/locally advanced pancreatic cancer Median OS 11.1 vs 6.8 months (FOLFIRINOX vs Gem)

4
5 Kim S. et al Retrospective cohort study from US oncologist record PATIENTS selection: Metastatic pancreatic cancer Treated from april to december 2015 with Gem/Nab-paclitaxel or FOLFIRINOX Not enrolled in clinical trial COMPARISON First line therapy: Gem/Nab-paclitaxel vs FOLFIRINOX Second line therapy: Gem/Nab-paclitaxel vs FOLFIRINOX treated with second line 654 patients analyzed, median follow-up 10.7 months Gem/Nab-paclitaxel: 337 (51.5%) vs FOLFIRINOX: 317 (48.5%)
 than patients treated with FOLFIRINOX Similar percentage of second line chemotherapy (36.")
.")
6 RESULTS Patients treated with gem-abraxane were Older (median age 64 vs 59) Worst clinical condition(ecog % vs 9.2%; more comorbidities) than patients treated with FOLFIRINOX Similar percentage of second line chemotherapy (36.1 vs 41% gem abraxane vs FOLFIRINOX) Toxicity: incidence of any grade 3-4 toxicity were similar in Gem-Abraxane and FOLFIRINOX (35% vs 33.6%, p 0.57). Nausea/vomiting, diarrhea, stomatitis and fatigue more frequent in FOLFIRINOX Non statistically significant difference in term of OS by first and second line between Gem-Abraxane and FOLFIRINOX
7 Gemcitabine-Nabpaclitaxel and FOLFIRINOX comparison (second line) AIOM post ASCO 30-40% of patients do not receive second line chemotherapy Many phase II trials and retrospective analysis Nanoliposomal irinotecan is the only validated drug for second line chemotherapy (NAPOLI-1 Wang-Gillam et al; Lancet 2016) 417 patients randomized, 117 5FU+NALIRI, 151 NALIRI, 151 5FU Median OS 6.1 vs 4.2 months (5FU/NALIRI vs 5FU) No difference between monotherapy (NALIRI and 5FU)

8 FOLFIRINOX or Nab-Paclitaxel based second line? Phase II and retrospectitve data supporting potential role of both FOLFIRINOX and Nab-paclitaxel based chemotherapy in second line setting

9
 GnP")
10 AIM of the study Comparison of second line mfolfirinox after Gem/Abraxane and Gem/Nab-paclitaxel after mfolfirinox Similar patients characteristics (age, ECOG performance Status, metastatic sites, primary tumor site and biliary stent presence) GnP N=25




11 RESULTS No statistically significant difference in term of OS and PFS and DCR
12 Neoadjuvant and perioperative therapy Phase II trials, retrospective analysis and meta analysis support neoadjuvant treatment (chemotherapy and chemoradiotherapy) Phase III trials are ongoing Adjuvant chemotherapy improves survival in pts treated with preoperative treatment (Roland et al; Ann Surg Oncol 2015) Why neoadjuvant? Patients selection Tumor shrinkage to improve R0 resection rate Better delivery of chemotherapy and radiotherapy
13 Neoadjuvant therapy Neoadjuvant therapy is not a standard yet, but it should be considered in locally advanced and border line resectable pancreatic cancer (3rd St. Gallen Gastrointestinal Cancer Conference; 2017)
14 Neoadjuvant therapy UNSOLVED QUESTIONS Which chemotherapy Chemotherapy alone or chemoradiotherapy Treatment duration Postoperative treatment

15
16
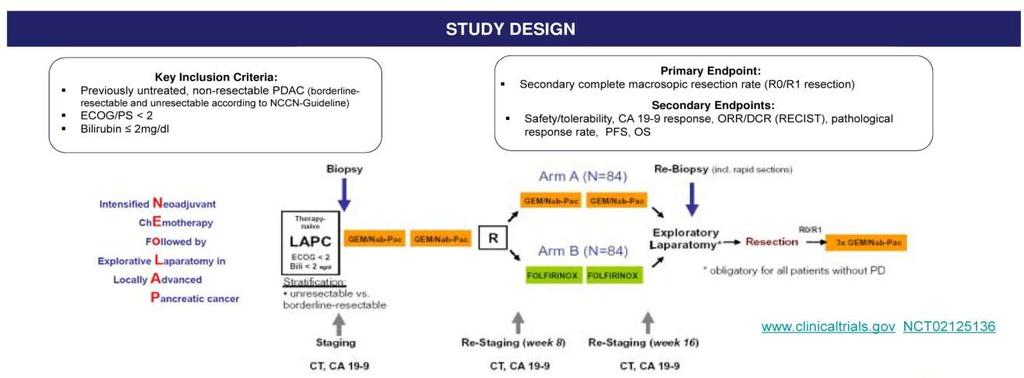
17 RESULTS Interim analysis About 70% in both arms had borderline resectable disease After induction chemotherapy 22.6 % of patients discontinued therapy (mainly progressive disease, and adverse events) 68% of patients completed treatment after randomization No survival data available Preliminary results of randomized patients Arm A nabpac/gem (N=42) DCR (%) PD(%) 7 11 Exploratory laparotomy (%) R0/R1 resection (%) RO/R1 resection (of surgically explored pts) 11/23 13/21 CONCLUSIONS ARMB FOLFIRINOX (N=44) Both FOLFIRINOX and nabpac/gem are effective and feasible High disease control rate (90%) Promising surgical conversion rates

18

 Of 160 NACRT pts 153 completed treatment (96%) 139 underwent surgery")
19 AIM of the study: evaluate the impact of neoadjuvant chemoradiotherapy (NACRT) on perioperative and long term clinical outcome Retrospective analysis 290 pts from 2006 to 2016: 160 treated with neoadjuvant CRT and 130 with upfront surgery) Of 160 NACRT pts 153 completed treatment (96%) 139 underwent surgery (87%)
 Favourable pathological effect (lower N+ rate and higher R0 resection")
20 RESULTS CONCLUSIONS High rate of treatment completion (96%) Long term better survival in NACRT (with the exception of arterial invasive tumor) Favourable pathological effect (lower N+ rate and higher R0 resection rate)

21
22 Potential novel therapy AIOM post ASCO New chemotherapy combinations Biological agents Moleculer/genomics driven treatment Immunotherapy

23 Novel Chemotherapy Combination AIOM post ASCO

24 Multicentric phase I/II trial investigating the substituion of CPT11 or Oxaliplatin with Nab-paclitaxel in FOLFIRINOX Primary Endpoint: To assess the activity of NabFOLFIRI and NabFOLFOX in first line in term of ORR Secondary Endpoint: Clinical Benefit, PFS, OS, Safety profile Inclusion Criteria: Age >18 and < 75 years Metastatic disease Non prior chemotherapy o radiotherapy for advanced cancer Performance Status ECOG 0-1
25 RESULTS Best Overall Response TUMOR ASSESSMENT Arm A (Nab-FOLFIRI) %(N) CR 0 0 PR 31%(13) 31%(13) SD 38%(16) 49%(17) ArmB (Nab-FOLFOX) No significant difference in term of CBR and ORR Grade 3 toxicity was 24% and 50% for NabFOLFIRI and nabfolfox respectively Grade 4 toxicity was 17% and 5% for NabFOLFIRI and nabfolfox respectively PD 26%(11) 12%(5) Not assessed 5%(2) 12%(5%) CBR (CR+PR+SD) 69%(29) 71%(30%) Nab-FOLFIRI PFS 6 month, OS 13.6 months Nab-FOLFOX PFS 5.6 months, OS 10.5 months CONCLUSION NabFOLFIRI and NabFOLFOX could represent a potential alternative firts line CT (achieving similar OS and PFS rate of FOLFIRINOX; with lower toxicity rate) Need for further investigation and validation (phase III trial)

26 Immunotherapy?
 or abstract (44%) Fifty four trials met criteria for further")
27 Analyzing the efficacy and safety of immunotherapy in pancreatic ductal adenocarcinoma (PDA): a systematic review and meta-analysis Babiker HM, et al. Meta-analysis and review of published and presented data of immunotherapy in pancreatic cancer Many data derive from ongoing trials (16%) or abstract (44%) Fifty four trials met criteria for further analysis (39 metastic, 12 adjuvant and 3 neoadjuvant) Modest activity and inconclusive data Need for further investigation!
: CAFs promote tumor growth and favour immunosuppression Myeloid cells: induce dense stromal cell reaction,")
28 Pancreatic cancer microenvironment Pancreatic stellate cells and fibroblasts: produce ECM (collagen,laminin, fibronectin). Reduce therapeutic sensitivity Inflammatory fibroblasts (CAF: cancer asociated fibroblasts): CAFs promote tumor growth and favour immunosuppression Myeloid cells: induce dense stromal cell reaction, and immunosoppressive microenvoronment. Immune infiltrate is mainly constituted by myeloid suppressor cells. Possible correlation with fibrosis T cells: not clear correlation and presence in pancreatic cancer. About a quarter present CD4 and CD8, but functional cells are rare No benefit from T cell regulatory immunotherapy Possibility to enhance immunotherapy acitivy in pancreatic cancer Use of chemotherapy to enhance antigen expression Repletion of myeloid cells (in order to reduce fibrosis and imunosuppression) Recruitment and augmentation of T cells expressione

29 Immunotherapy?
30 Phase II randomized trial of double immunotherapy (Durvalumab and Tremelimumab) + Chemotherapy (gemcitabine/nab-paclitaxel) vs Gemcitabine /Nab-paclitaxel PRIMARY ENDPOINT: Overall Survival SECONDARY ENDPOINT: PFS, ORR, safety and toxicity Rational for immunotherapy and chemotherapy in pancreatic cancer Durvalumab: specific binding PD L-1 Tremelimumab: anti CTLA-4 antibody Cancer associated fibroblast (CAF)reduce immunotherapy activity and nab paclitaxel induce CAF depletion Chemotherapy may induce antigens expression Double immunotherapy (anti PDL1 and CTLA-4) has sinergistic activity in mouse models
31 RESULTS Preliminary data from safety run in (11 patients enrolled) Median follow-up of 8.3 months Toxicity: 1 patient had grade 3 colitis Most common grade 2 toxicity:fatigue, anemia, abnormal WBC and lipase, hyponatremia Efficacy: 8/11 (73%) had partial response, median duration of 7.4 months Median PFS 7.9 months Median OS not reached, 6 Months survival rate 80% CONCLUSION Data of safety run in showed interesting acivity and acceptable toxicity profile Phase II trial is ongoing (planned enrollment of 130 patients)

32

33 Genetic profile of pancreatic cancer Most common genetic mutation: KRAS, TP53, CDKN2A, SMAD4, RNF43, ARID1A, TGFbR2, GNAS, RREB1, and PBRM1 KRAS mutation in > 90% pancreatic cancer 10% harbor mutation in BRCA1/2, PALB 2 and ATM MMR gene mutation could be observed BRAF mutation and mtor pathway activation are frequent in KRAS WT

34 Therapeutical and clinical implication Potential therapeutic target -BRCA, PALB2 (platinum sensitivity, potential PARP inhibitor sensitivity) -BRAF -Currently no other potential target Pihlak R. et al. Cancers 2018 PROPOSED GENOMIC CLASSIFICATION On the basis of mutational status and clinical characteristics BAYLEY (Nature 2016): - Squamous and adenosquamous - Pancreatic progenitor - Immunogenic - ADEX (aberrantly differentiated endocrine exocrine) WADDEL (Nature 2015) - Stable - Scaterred - Locall rearranged - Unstable. MOFFITT - Basal like - Classical

35 Genomic and molecular biology
36 BACKGROUND AND AIM OFTHE STUDY Pancreatic cancer can have BRCA 1/2 mutation and other homologous recombinant paththway genes. AIM of the study is to investigate the therapeuthic prognostic significance of these mutations 3030 patients analyzed comparing carriers and non carrieris of BRCA 1/2, PALB2 and ATM deletereous mutations (4.6% of patients had germline mutation) Comparison of clinical outcome with chemotherapy according to mutational status
 When analyzed post-folfirinox era, 40 patients with these mutation had better outcome than 668 non carriers (adjusted HR 0.62, p=0.")
37 RESULTS Relative distribution of BRAC1/2, PALB and ATM mutations in 139 (4.6%) patients with deletereous mutations Survival benefit slightly better in patients with mutation (14.3 vs 11.3 months, p=0.07) When analyzed post-folfirinox era, 40 patients with these mutation had better outcome than 668 non carriers (adjusted HR 0.62, p=0.0062) CONCLUSIONS BRCA1/2, PALB2 and ATM mutation is present in about 5% of patients, In post-folfirinox era pts with mutation had longer survival Development of trial incorporating this information could have potential value for PDAC (olaparib? Other treatment)

38
39 MultiOmic: gemonic,proteomic and phspoproteomic analysis AIM of the study: to define frequency of genetic and proteomic mutation in primary tumor and metastatic site and identify potential differences between them To explore potential moleculal target for treatment Methods 505 patients, tumor sample analyzed according to Perthera reports 182 primary sites and 323 metastatic site
40 RESULTS The 4 most common mutations seen in pancreatic cancer (SMAD4, CDKN2Am p53 and KRS ) were similar between primary and metastatic site Proportion of actionable mutations was similar between groups Within metastatic site specific tissue pattern expression was observed (liver vs lung higher TUBB3 and lower PTEN mutation) CONCLUSION No statistically significant difference in specific gene mutation observed between primary tumor and metastatic site Confirm the reason of early metastatization Potential molecular target even in early disease Non need for rebiopsy
41 CONCLUSION Gemcitabine-Nabpaclitaxel and FOLFIRINOX comparison o Comparison in real life shows similar activity both in first and second line o NB different patients characteristics and toxicity profile Neoadjuvant and perioperative treatment o FOLFIRINOX and Gem-Nabpaclitaxel potentially active in LAPC o Long term benefit confirmed with preoperative CT-RT o New treatment/schedules under investigation (Gem/Nabp+RT) and Phase III clinicl trial New drugs, immunotherapy o Nab FOLFOx/Nab FOLFIRI o Excaping immunotherapy resistance (immunotherapy and chemotherapy combination) o Other moleculer treatment under evaluation (immunotherapy, olaparib) Genomics and molecular biology o Prognostic and predictive role o Potential molecular target identification
Pancreatic Adenocarcinoma
 Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Cancer: Light at the End of the (Very Long) Tunnel
 Tunnel") Pancreatic Cancer: Light at the End of the (Very Long) Tunnel Daniel Renouf, MD, MPH, FRCPC Medical Oncologist, BC Cancer Agency University of British Columbia Objectives 1. Discuss recent updates in systemic
Pancreatic Cancer: Light at the End of the (Very Long) Tunnel Daniel Renouf, MD, MPH, FRCPC Medical Oncologist, BC Cancer Agency University of British Columbia Objectives 1. Discuss recent updates in systemic
Pancreatic Cancer: Medical Therapeutic Approaches
 Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
Future Perspectives in mpca. Michel Ducreux, MD, PhD Gustave Roussy Villejuif, France
 Future Perspectives in mpca Michel Ducreux, MD, PhD Gustave Roussy Villejuif, France Number of Novel Therapies and Targets in Pancreatic Cancer Are Expanding Garrido-Laguna I, et al. Nat Rev Clin Oncol.
Future Perspectives in mpca Michel Ducreux, MD, PhD Gustave Roussy Villejuif, France Number of Novel Therapies and Targets in Pancreatic Cancer Are Expanding Garrido-Laguna I, et al. Nat Rev Clin Oncol.
Keynote Lecture 1 Advances in Molecular Biology of Pancreatic Cancer: Understanding Genetic Complexity and Molecular Heterogeneity
 Keynote Lecture 1 Advances in Molecular Biology of Pancreatic Cancer: Understanding Genetic Complexity and Molecular Heterogeneity Volker Ellenrieder, MD, PhD University Hospital Gӧttingen Gӧttingen, Germany
Keynote Lecture 1 Advances in Molecular Biology of Pancreatic Cancer: Understanding Genetic Complexity and Molecular Heterogeneity Volker Ellenrieder, MD, PhD University Hospital Gӧttingen Gӧttingen, Germany
Pancreatic Ca Update
 Pancreatic Ca Update Caio Max S. Rocha Lima, M.D. M. Robert Cooper Professor in Medical Oncology Co-leader GI Oncology and Co-leader Phase I Program Wake Forest School of Medicine E-mail:crochali@wakehealth.edu
Pancreatic Ca Update Caio Max S. Rocha Lima, M.D. M. Robert Cooper Professor in Medical Oncology Co-leader GI Oncology and Co-leader Phase I Program Wake Forest School of Medicine E-mail:crochali@wakehealth.edu
Dr Roopinder Gillmore July 2017
 Dr Roopinder Gillmore July 2017 Resectable Borderline / locally advanced Metastatic 15-20% 15-20% 60-70% 22-28 months 9-15 months 6-12 months Does the patient have resectable disease?? Definitely not
Dr Roopinder Gillmore July 2017 Resectable Borderline / locally advanced Metastatic 15-20% 15-20% 60-70% 22-28 months 9-15 months 6-12 months Does the patient have resectable disease?? Definitely not
Overview. What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013
 What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
Unità Operativa di Oncologia Medica Direzione Scientifica Istituto Tumori Giovanni Paolo II Bari.
 Unità Operativa di Oncologia Medica Direzione Scientifica Istituto Tumori Giovanni Paolo II Bari n.silvestris@oncologico.bari.it LAPACT mffox + PEGPH20 (SWOG study) COMPASS trial Immune landscape ABSTRACT
Unità Operativa di Oncologia Medica Direzione Scientifica Istituto Tumori Giovanni Paolo II Bari n.silvestris@oncologico.bari.it LAPACT mffox + PEGPH20 (SWOG study) COMPASS trial Immune landscape ABSTRACT
Update on Pancreatic Cancer
 Update on Pancreatic Cancer Farshid Dayyani, MD, PhD Associate Clinical Professor, Department of Medicine, UC Irvine School of Medicine February 2 nd, 2018 Overview Current Systemic Treatments Adjuvant
Update on Pancreatic Cancer Farshid Dayyani, MD, PhD Associate Clinical Professor, Department of Medicine, UC Irvine School of Medicine February 2 nd, 2018 Overview Current Systemic Treatments Adjuvant
Pancreatic Ductal Adenocarcinoma. Razvan Popescu Tumor Center Aarau Switzerland
 Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Median Survival of Patients With Pancreatic Cancer Localized/ Resectable 15-24 months 10% Locally Advanced 6-15 months 30%
Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Median Survival of Patients With Pancreatic Cancer Localized/ Resectable 15-24 months 10% Locally Advanced 6-15 months 30%
Adjuvant therapy in pancreatic cancer Monotherapy for whom? JL VAN LAETHEM, MD,PhD
 Adjuvant therapy in pancreatic cancer Monotherapy for whom? JL VAN LAETHEM, MD,PhD Efficacy Parameters in adjuvant monochemotherapy Randomized studies in resectable PDAC Regimen DFS HR (p) OS HR (p) 5-yr-OS
Adjuvant therapy in pancreatic cancer Monotherapy for whom? JL VAN LAETHEM, MD,PhD Efficacy Parameters in adjuvant monochemotherapy Randomized studies in resectable PDAC Regimen DFS HR (p) OS HR (p) 5-yr-OS
Pancreas Cancer ASCO Poster Review
 Bologna, 9 Febbraio 2019 AIOM POST ASCO GI REVIEW Updates and News from the GI Cancers Symposium in San Francisco Pancreas Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Medica Fondazione Policlinico
Bologna, 9 Febbraio 2019 AIOM POST ASCO GI REVIEW Updates and News from the GI Cancers Symposium in San Francisco Pancreas Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Medica Fondazione Policlinico
GI Tumor Board 3/8/2018. Case #1 IDEA. Case #1 Question #1 What is the next step in management?
 GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
Disclosures. Immunotherapyin Head & NeckCancer. Actual landscape of systemic treatment in HNSCC. Head andneckcanceris an immunogeneic tumor
 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
The 2010 Gastrointestinal Cancers Symposium Oral Abstract Session: Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract
 The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
Reference No: Author(s) 12/05/16. Approval date: committee. June Operational Date: Review:
 12/05/16. Approval date: committee. June Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
L oncologo Alberto Zaniboni
 COME TRATTARE LA NEOPLASIA LOCALMENTE AVANZATA BORDERLINE PER RESECABILITA L oncologo Alberto Zaniboni Oncologia Medica Fondazione Poliambulanza - Brescia Pancreatic cancer deaths in 2030 Pancreatic cancer
COME TRATTARE LA NEOPLASIA LOCALMENTE AVANZATA BORDERLINE PER RESECABILITA L oncologo Alberto Zaniboni Oncologia Medica Fondazione Poliambulanza - Brescia Pancreatic cancer deaths in 2030 Pancreatic cancer
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreas Cancer Update Systemic Treatments
 Pancreas Cancer Update Systemic Treatments Carlos R Becerra. Baylor University Medical Center Stage Distribution for Pancreas Cancer in the US (24-21) 1 9 8 7 Axis Title 6 5 4 53 3 28 2 1 9 11 Localized
Pancreas Cancer Update Systemic Treatments Carlos R Becerra. Baylor University Medical Center Stage Distribution for Pancreas Cancer in the US (24-21) 1 9 8 7 Axis Title 6 5 4 53 3 28 2 1 9 11 Localized
Immunotherapy in non-small cell lung cancer
 Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO
 Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
Pancreatic Cancer Where are we?
 Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Improving the Outcome of Patients with Metastatic Pancreatic Cancer
 Improving the Outcome of Patients with Metastatic Pancreatic Cancer Philip Agop Philip, MD, PhD, FRCP Professor of Oncology and Pharmacology Karmanos Cancer Center Wayne State University Detroit, MI Median
Improving the Outcome of Patients with Metastatic Pancreatic Cancer Philip Agop Philip, MD, PhD, FRCP Professor of Oncology and Pharmacology Karmanos Cancer Center Wayne State University Detroit, MI Median
New targets in endometrial and ovarian cancer
 New targets in endometrial and ovarian cancer SAMO Interdisciplinary Workshop on Gynecologic Tumors Luzern, January 16-17, 2016 C. Sessa IOSI Bellinzona Outline New targets in ovarian cancer - Cell cycle
New targets in endometrial and ovarian cancer SAMO Interdisciplinary Workshop on Gynecologic Tumors Luzern, January 16-17, 2016 C. Sessa IOSI Bellinzona Outline New targets in ovarian cancer - Cell cycle
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Tumors in the Randomized German AIO study KRK-0306
 FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First- Line Treatment for Patients with Metastatic Colorectal Cancer (mcrc): Analysis of Patients with KRAS-Mutated Tumors in the Randomized German
FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First- Line Treatment for Patients with Metastatic Colorectal Cancer (mcrc): Analysis of Patients with KRAS-Mutated Tumors in the Randomized German
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Treatment Approaches for Pancreatic Cancer: Hope on the Horizon Disclosures
 Treatment Approaches for Pancreatic Cancer: Hope on the Horizon Michael Pishvaian, MD, PhD Director, Phase I Program Assistant Professor Lombardi Comprehensive Cancer Center Georgetown University Disclosures
Treatment Approaches for Pancreatic Cancer: Hope on the Horizon Michael Pishvaian, MD, PhD Director, Phase I Program Assistant Professor Lombardi Comprehensive Cancer Center Georgetown University Disclosures
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
Liver and Biliary Tract Cancers Critical Review
 Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015
 Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
Third Quarter 2015 Earnings Call. November 9, 2015
 Third Quarter 2015 Earnings Call November 9, 2015 Forward-Looking Statements All of the statements in this presentation that are not statements of historical facts constitute forward-looking statements
Third Quarter 2015 Earnings Call November 9, 2015 Forward-Looking Statements All of the statements in this presentation that are not statements of historical facts constitute forward-looking statements
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy
 Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy Dr. David B. Page Providence Portland Medical Center Earle A. Chiles Research Institute Funding & Disclosures
Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy Dr. David B. Page Providence Portland Medical Center Earle A. Chiles Research Institute Funding & Disclosures
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
Colon Cancer ASCO Poster Review
 Rome, February 11 th 2017 AIOM POST ASCO GI Review Colon Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Policlinico GB Rossi Azienda Ospedaliero Universitaria Integrata di Verona Me Before Me After
Rome, February 11 th 2017 AIOM POST ASCO GI Review Colon Cancer ASCO Poster Review Lisa Salvatore UOC Oncologia Policlinico GB Rossi Azienda Ospedaliero Universitaria Integrata di Verona Me Before Me After
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Ca Cardias e Stomaco: le diversita e le terapie
 XXII Riunione Nazionale I.T.M.O. Ca Cardias e Stomaco: le diversita e le terapie Maria Di Bartolomeo s.s. Oncologia Medica Gastroenterologica Fondazione IRCCS Istituto Nazionale Tumori Milano OUTLINE History
XXII Riunione Nazionale I.T.M.O. Ca Cardias e Stomaco: le diversita e le terapie Maria Di Bartolomeo s.s. Oncologia Medica Gastroenterologica Fondazione IRCCS Istituto Nazionale Tumori Milano OUTLINE History
LA CHEMIOTERAPIA DI I LINEA
 DECIDERE LA CHEMIOTERAPIA ADIUVANTE E DELLA MALATTIA METASTATICA LA CHEMIOTERAPIA DI I LINEA Michele Reni Department of Medical Oncology IRCCS Ospedale San Raffaele Milan, Italy 1930 1940 1950 1960 1970
DECIDERE LA CHEMIOTERAPIA ADIUVANTE E DELLA MALATTIA METASTATICA LA CHEMIOTERAPIA DI I LINEA Michele Reni Department of Medical Oncology IRCCS Ospedale San Raffaele Milan, Italy 1930 1940 1950 1960 1970
New Avenues for the development and evaluation of therapy: Complex, multi-pronged, not one size fitting all
 New Avenues for the development and evaluation of therapy: Complex, multi-pronged, not one size fitting all Antoine Yver MD MSC Senior VP & Head Oncology Global Medicines Development AstraZeneca, Gaithersburg
New Avenues for the development and evaluation of therapy: Complex, multi-pronged, not one size fitting all Antoine Yver MD MSC Senior VP & Head Oncology Global Medicines Development AstraZeneca, Gaithersburg
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
Team Progress Updates. SU2C Pancreatic Dream Team: Cutting Off the Fuel Supply: A New Approach in the Treatment of Pancreatic Cancer
 SU2C Pancreatic Dream Team: Cutting Off the Fuel Supply: A New Approach in the Treatment of Pancreatic Cancer Cancer of the pancreas is one of the deadliest forms of cancer, with a five-year survival rate
SU2C Pancreatic Dream Team: Cutting Off the Fuel Supply: A New Approach in the Treatment of Pancreatic Cancer Cancer of the pancreas is one of the deadliest forms of cancer, with a five-year survival rate
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
Rectal cancer: Poster Session Review
 AIOM PostASCO GI Roma, 5-6 febbraio 2016 Rectal cancer: Poster Session Review Sara Lonardi SS Trattamento Multidisciplinare Tumori Colorettali - UOC Oncologia Medica 1 Dipartimento di Oncologia Clinica
AIOM PostASCO GI Roma, 5-6 febbraio 2016 Rectal cancer: Poster Session Review Sara Lonardi SS Trattamento Multidisciplinare Tumori Colorettali - UOC Oncologia Medica 1 Dipartimento di Oncologia Clinica
Carla van Herpen Medical Oncologist Immunotherapyin Head & NeckCancer
 Carla van Herpen Medical Oncologist 01-10-2016 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial,
Carla van Herpen Medical Oncologist 01-10-2016 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial,
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
Κίκα Πλοιαρχοπούλου. Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών
 Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Triple-Negative Breast Cancer
 June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
ESMO Preceptorship Breast Cancer. Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia
 ESMO Preceptorship Breast Cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia Outline Rational for immune-based therapy in BC How to
ESMO Preceptorship Breast Cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia Outline Rational for immune-based therapy in BC How to
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
ESMO 13th World Congress on Gastrointestinal Cancer
 ESMO 13th World Congress on Gastrointestinal Cancer 22-25 June, 2011 Barcelona, Spain INTRODUCTION The ESMO World Congress on Gastrointestinal Cancer took place in Barcelona from the 22nd until the 25th
ESMO 13th World Congress on Gastrointestinal Cancer 22-25 June, 2011 Barcelona, Spain INTRODUCTION The ESMO World Congress on Gastrointestinal Cancer took place in Barcelona from the 22nd until the 25th
Breast Cancer: ASCO Poster Review
 Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Cáncer de Páncreas: Optimización del tratamiento sistémico
 Cáncer de Páncreas: Optimización del tratamiento sistémico Alfredo Carrato Hospital Universitario Ramón y Cajal, Madrid 16 de Mayo de 2015 Pancreatic cancer screening There is a latency period of about
Cáncer de Páncreas: Optimización del tratamiento sistémico Alfredo Carrato Hospital Universitario Ramón y Cajal, Madrid 16 de Mayo de 2015 Pancreatic cancer screening There is a latency period of about
Best Practices and Promising Agents in Pancreatic Cancer. This program is supported by educational grants from Celgene Corporation and Incyte.
 Best Practices and Promising Agents in Pancreatic Cancer This program is supported by educational grants from Celgene Corporation and Incyte. About These Slides Users are encouraged to use these slides
Best Practices and Promising Agents in Pancreatic Cancer This program is supported by educational grants from Celgene Corporation and Incyte. About These Slides Users are encouraged to use these slides
TGFβR1 Kinase Inhibitor
 TGFβR1 Kinase Inhibitor Galunisertib, LY2157299 H 2 0 Prud homme GJ 1 ; Flavell RA, et al 2 Drug Discovery Platform: Cancer Angiogenesis and Tumor Microenvironment/Immuno-Oncology A Phase 1b/2 Dose-Escalation
TGFβR1 Kinase Inhibitor Galunisertib, LY2157299 H 2 0 Prud homme GJ 1 ; Flavell RA, et al 2 Drug Discovery Platform: Cancer Angiogenesis and Tumor Microenvironment/Immuno-Oncology A Phase 1b/2 Dose-Escalation
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS
 CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands
 What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
Oral Communications & Posters
 Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Pancreatic cancer from the past to the future
 Pancreatic cancer from the past to the future Darren Sigal, MD Scripps Clinic Pancreas and Bile Duct Cancer Group Division of Hematology/Oncology Scripps Clinic Pancreas and Bile Duct Cancer Group 1 Objectives
Pancreatic cancer from the past to the future Darren Sigal, MD Scripps Clinic Pancreas and Bile Duct Cancer Group Division of Hematology/Oncology Scripps Clinic Pancreas and Bile Duct Cancer Group 1 Objectives
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy
 Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
SBRT in Pancreas Cancer Role of The Radiosurgery Society
 SBRT in Pancreas Cancer Role of The Radiosurgery Society Anand Mahadevan MD FRCS FRCR Chairman Division of Radiation Oncology Geisinger Health System, Danville, PA, USA. Past President and Chairman: The
SBRT in Pancreas Cancer Role of The Radiosurgery Society Anand Mahadevan MD FRCS FRCR Chairman Division of Radiation Oncology Geisinger Health System, Danville, PA, USA. Past President and Chairman: The
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Update on PARP inhibitors: opportunities and challenges in cancer therapy
 Update on PARP inhibitors: opportunities and challenges in cancer therapy Vanda Salutari Unità di Ginecologia Oncologica Fondazione Policlinico Universitario A. Gemelli vanda.salutari@policlinicogemelli.it
Update on PARP inhibitors: opportunities and challenges in cancer therapy Vanda Salutari Unità di Ginecologia Oncologica Fondazione Policlinico Universitario A. Gemelli vanda.salutari@policlinicogemelli.it
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
Synergistic combinations of targeted immunotherapy to combat cancer
 Synergistic combinations of targeted immunotherapy to combat cancer Myung Ah Lee, M.D., Ph. D Division of Medical Oncology, Hepato-biliary pancreatic cancer center Seoul St. Mary s hospital, The Catholic
Synergistic combinations of targeted immunotherapy to combat cancer Myung Ah Lee, M.D., Ph. D Division of Medical Oncology, Hepato-biliary pancreatic cancer center Seoul St. Mary s hospital, The Catholic
Atezolizumab Is a Humanized Anti-PDL1 Antibody That Inhibits the Binding of PD-L1 to PD-1 and B7.1
 Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Keynote Lecture 2 Targeting the Tumor Microenvironment in Pancreatic Cancer
 Keynote Lecture 2 Targeting the Tumor Microenvironment in Pancreatic Cancer E. Gabriela Chiorean, MD University of Washington Fred Hutchinson Cancer Research Center Seattle, Washington, United States Learning
Keynote Lecture 2 Targeting the Tumor Microenvironment in Pancreatic Cancer E. Gabriela Chiorean, MD University of Washington Fred Hutchinson Cancer Research Center Seattle, Washington, United States Learning
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer
 Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Phase II trial of capecitabine plus nab-paclitaxel in patients with metastatic pancreatic adenocarcinoma
 Original Article Phase II trial of capecitabine plus nab-paclitaxel in patients with metastatic pancreatic adenocarcinoma Werner Scheithauer 1, Gabriela Kornek 1, Gerald Prager 1, Nadja Stranzl 1, Friedrich
Original Article Phase II trial of capecitabine plus nab-paclitaxel in patients with metastatic pancreatic adenocarcinoma Werner Scheithauer 1, Gabriela Kornek 1, Gerald Prager 1, Nadja Stranzl 1, Friedrich
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker
 Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
A Fully Integrated Cancer Company.
 A Fully Integrated Cancer Company. Jefferies Global Healthcare Conference June 3, 2014 Robert Mulroy, President and CEO Forward Looking Statements To the extent that statements contained in this presentation
A Fully Integrated Cancer Company. Jefferies Global Healthcare Conference June 3, 2014 Robert Mulroy, President and CEO Forward Looking Statements To the extent that statements contained in this presentation