GI Tumor Board 3/8/2018. Case #1 IDEA. Case #1 Question #1 What is the next step in management?
|
|
|
- Erik Farmer
- 5 years ago
- Views:
Transcription


1 GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case #1 70yo F without significant PMH presents w/3 months of diarrhea and RLQ abdominal pain CT: cecal mass with mesenteric adenopathy, no distant disease Colonoscopy: partially obstructing tumor in cecum biopsy positive for adenocarcinoma Undergoes right hemicolectomy. Surgical path: 8.5cm low grade adenocarcinoma pt3/pn2a 6/53 LN positive, negative margins, MSI high. Case #1 Question #1 IDEA 1. Test expanded RAS and BRAF 2. Treat with adjuvant FOLFOX for 3 months 3. Treat with adjuvant FOLFOX for 6 months 4. Treat with adjuvant CAPOX for 3 months 5. Treat with adjuvant CAPOX for 6 months 1



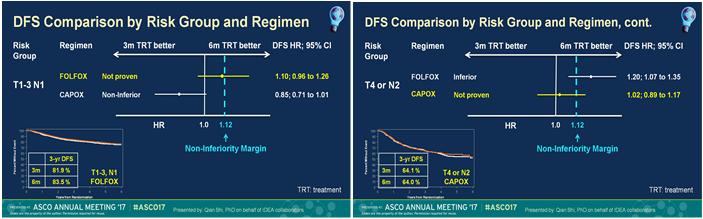
2 3m vs 6m Low risk High risk FOLFOX CAPOX Low risk High risk FOLFOX CAPOX 2



3 IDEA Clinical Consensus: Risk-based approach to adjuvant chemotherapy in stage III colon cancer Case #1 Question #2 In this patient with stage III colon cancer, would BRAF status change your approach to adjuvant therapy? 1. Yes 2. No Case #1 continued Patient completed 6 months of adjuvant FOLFOX with discontinuation of oxaliplatin after cycle 9 due to sensory neuropathy CT scan 2 months after completion of adjuvant FOLFOX reveals a 1.8cm liver lesion which on retrospect review may have been faintly present on preoperative imaging Molecular profiling reveals RAS wt, BRAF wt, MSI high Case #1 Question #3 1. Surgical resection of liver metastasis 2. Liver directed therapy (eg SIRT, RFA, SBRT) 3. FOLFIRI 4. PD 1 inhibitor 3

4 Case #1 Take Home Points In patients with T1 T3,N1 disease, consider 3 months of adjuvant therapy. Pre planned subgroup analysis showed non inferiority of 3 vs 6 months of adjuvant therapy. For patients with T4 or N2 disease, discuss risks and benefits of 3 vs 6 months of adjuvant therapy. Non inferiority was not met in this subgroup 3 months confers significantly less neurotoxicity Consider toxicity profiles when deciding between CAPOX AND FOLFOX Case #2 A 62yo M w/no significant PMH presents with 3 month history of epigastric pain with associated anorexia. CT reveals hypodense mass in pancreatic head with >180 0 encasement of the superior mesenteric artery EUS FNA confirms pancreatic adenocarcinoma. Case #2 Question #1 1. Start FOLFIRINOX 2. Start gemcitabine/nab paclitaxel 3. Radiation oncology consultation 4. Surgical oncology consultation 4


5 Case #2 Clinical Course Patient receives 6 months of gemcitabine/nab paclitaxel CT scans after 2 and 4 months of treatment showed stable disease Patient developed grade 3 sensory neuropathy and nab paclitaxel is discontinued during cycle 6 CT scan after 6 th month still showed stable disease and no evidence of distant disease Case #2 Question #2 1. Surgical resection 2. Chemoradiation 3. SBRT 4. Continue chemotherapy with gemcitabine alone 5. Continue chemotherapy but change regimen 6. Treatment break 5
6 LAP07 Assess OS with chemotherapy vs chemoradiotherapy in locally advanced pancreatic cancer with progression free disease after gemcitabine based therapy LAP07 Evaluate effect of Erlotinib on OS in locally advanced pancreatic cancer Gemcitabine vs Gemcitabine + Erlotinib Hammel, P et al JAMA. 315(17); Case #2 Clinical Course Patient elected to take a break from chemotherapy Subsequent imaging about 4 months later shows metastatic progression to the liver and peritoneum He continues to have symptomatic sensory neuropathy Case #2 Question #3 1. FOLFIRNOX 2. FOLFIRI 3. FOLFOX 4. 5FU/nanoliposomal irinotecan 6


7 NAPOLI 1 NAPOLI 1 OS Case #2 Take Home Points There is no standard of care best option for locally advanced pancreatic adenocarcinoma Both frontline regimens of FOLFIRINOX and Gem/nab paclitaxel are reasonable options based on extrapolation from randomized trial data in the metastatic setting Chemoradiotherapy has not been proven to improve OS compared to chemotherapy alone in locally advanced pancreatic cancer following gemcitabine based therapy Nanoliposomal Irinotecan in combination with fluorouracil extends survival in patients with metastatic pancreatic ductal adenocarcinoma who previously received gemcitabine based chemotherapy compared to fluorouracil. Case #3 63yo woman presents with fatigue and jaundice CT scan reveals biliary dilation and mass distally ERCP confirms a CBD stricture and brushings are positive for adenocarcinoma ECOG PS 0 7

8 Case #3 Question #2 1. Chemotherapy gemcitabine and cisplatin 2. Chemoradiation with capecitabine 3. Surgery Case #3 followup Patient undergoes whipple resection Pathology confirms a 2.5cm moderately differentiated extrahepatic cholangiocarcinoma 1/18 Lymph nodes are positive Negative margins Case #3 Question #2 1. Chemotherapy capecitabine 2. Chemotherapy gemcitabine and cisplatin 3. Chemotherapy with gemcitabine/capecitabine > chemoradiation with capecitabine 4. Chemoradiation with capecitabine BILCAP 8

9 BILCAP Future directions ACTICCA 1 adjuvant therapy for resected cholangio or GB cancer original design = gem/cis vs placebo > based on BILCAP > gem/cis vs capecitabine Primary endpoint DFS Case #3 Take Home Points Capecitabine improves median overall survival compared to surveillance in patients with biliary tract cancer following macroscopic complete resection Unclear whether multi drug regimens and incorporation of chemoradiation add benefit in the adjuvant setting Case #4 62 yo woman presents with upper GI bleeding EGD reveals a large ulcerative gastric mass positive for adenocarcinoma EUS reveals T3N1 disease Diagnostic laparoscopic evaluation with cytology of peritoneal washings is negative 9

10 Case #4 Question #1 1. Surgery 2. ECF 3. EOX 4. FOLFOX 5. FLOT 6. chemoradiation MAGIC Trial Perioperative Chemotherapy MAGIC > FLOT FLOT FLTO FTLO FTOL FOLT FOTL TFLO TFOL TLOF TLFO TOLF TOFL OLFT OLTF OTLF OTFL OFLT OFTL LFTO LFOT LTOF LTFO LOTF LOFT 10

11 FLOT4 Toxicity UK OE05 Trial of neoadjuvant chemo UK OE05 Trial of neoadjuvant chemo 11
12 Case #4 Clinical Course Patient received FOLFOX with perioperative intent Repeat imaging shows stable to slight improvement She undergoes surgical resection Pathology reveals a Tumor Regression Score of 3 = Poor response Minimum or no treatment effect; extensive residual cancer cells Case #4 Question #2 1. Adjuvant chemo same regimen as pre operative 2. Adjuvant chemo switch regimen to different from pre operative 3. No adjuvant therapy 4. Chemoradiation Case #4 Take Home Points FLOT chemotherapy is a new peri operative chemotherapy regimen option for gastric cancer Based on toxicity profile select patients carefully True benefit of adjuvant component of perioperative therapy remains unclear 12
Pancreatic Adenocarcinoma
 Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Overview. What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013
 What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
Pancreatic Cancer Where are we?
 Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Reference No: Author(s) 12/05/16. Approval date: committee. June Operational Date: Review:
 12/05/16. Approval date: committee. June Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
NCCN Guidelines for Hepatobiliary Cancers V Web teleconference on 10/24/17
 Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Esophageal and GEJ Cancers. Case Presentations
 Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
GASTROINTESTINAL MALIGNANCIES
 Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Alliance A Alliance SWOG ECOG/ACRIN - NRG
 Preoperative chemotherapy and chemotherapy plus hypofractionated radiation therapy for borderline resectable adenocarcinoma of the head of the pancreas Alliance A021501 Alliance SWOG ECOG/ACRIN - NRG Clinical
Preoperative chemotherapy and chemotherapy plus hypofractionated radiation therapy for borderline resectable adenocarcinoma of the head of the pancreas Alliance A021501 Alliance SWOG ECOG/ACRIN - NRG Clinical
Adjuvant/neoadjuvant systemic treatment of colorectal cancer
 5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
Frank Burton Memorial Update on Pancreato-biliary Cancers
 Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Pancreatic Cancer: Medical Therapeutic Approaches
 Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
The 2010 Gastrointestinal Cancers Symposium Oral Abstract Session: Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract
 The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy
 Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Gallbladder Cancer. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Gallbladder Cancer GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: September 2006 This guideline is a statement of
Gallbladder Cancer GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: September 2006 This guideline is a statement of
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran
 Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
Cholangiocarcinoma. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Upper GI. Oesophageal & Gastric Cancer. Tumour Group: Regimen name / acronym Cisplatin/5-FU with concomitant RT. Place in therapy
 Tumour Group: Upper GI Tumour Type: Oesophageal & Gastric Cancer Primary Cisplatin/5-FU with concomitant RT Alternative Regimen: Oxaliplatin/ 5FU with concomitant RT (FOLFOX6-RT) Cisplatin Carboplatin
Tumour Group: Upper GI Tumour Type: Oesophageal & Gastric Cancer Primary Cisplatin/5-FU with concomitant RT Alternative Regimen: Oxaliplatin/ 5FU with concomitant RT (FOLFOX6-RT) Cisplatin Carboplatin
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
Thursday, March 17, pm ET
 Virtual Molecular Tumor Board Host: MedStar Georgetown University Hospital Leader: Dr. John Marshall Thursday, March 17, 2016 5 pm ET Patient 1 The information contained in these slides is provided for
Virtual Molecular Tumor Board Host: MedStar Georgetown University Hospital Leader: Dr. John Marshall Thursday, March 17, 2016 5 pm ET Patient 1 The information contained in these slides is provided for
Fabienne Warmerdam Zuyderland
 GE Fabienne Warmerdam Zuyderland Disclosure ASCO 2017 travelgrant Pfizer CRC ADJUVANT Less is more? More is More! 1 Less is more? Perspectief INT-0035 stadium III (niets vs 5-FU) 6.5-jaars OS 46% vs. 60%
GE Fabienne Warmerdam Zuyderland Disclosure ASCO 2017 travelgrant Pfizer CRC ADJUVANT Less is more? More is More! 1 Less is more? Perspectief INT-0035 stadium III (niets vs 5-FU) 6.5-jaars OS 46% vs. 60%
Reference No: Author(s) Approval date: 12/05/16. Committee. June Operational Date: Review:
 Approval date: 12/05/16. Committee. June Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Biliary Tract Cancer (BTC) Dr Colin Purcell, Consultant Medical Oncologist on behalf of the GI Oncologists Group, Cancer
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Biliary Tract Cancer (BTC) Dr Colin Purcell, Consultant Medical Oncologist on behalf of the GI Oncologists Group, Cancer
Imaging techniques in the diagnosis, staging and follow up of GI cancers. Moderators: Banke Agarwal, MD and Paul Schultz, MD
 Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
GI ONCOLOGY CLINICAL TRIALS AT UCDAVIS
 G ONCOLOGY CLNCAL TRALS AT UCDAVS Version: DECEMBER 2017 Please contact us with any questions or any potential clinical patients Edward Kim, MD/PhD email: jhkim@ucdavis.edu pager: 916-816-4059 May Cho,
G ONCOLOGY CLNCAL TRALS AT UCDAVS Version: DECEMBER 2017 Please contact us with any questions or any potential clinical patients Edward Kim, MD/PhD email: jhkim@ucdavis.edu pager: 916-816-4059 May Cho,
Hot Topic in tema di neoplasie del Colon: Durata ottimale della chemioterapia adiuvante nei tumori del Colon
 Convegno Nazionale AIOM Giovani 2018 News in Oncology Hot Topic in tema di neoplasie del Colon: Durata ottimale della chemioterapia adiuvante nei tumori del Colon Daniele Rossini U.O. di Oncologia Medica
Convegno Nazionale AIOM Giovani 2018 News in Oncology Hot Topic in tema di neoplasie del Colon: Durata ottimale della chemioterapia adiuvante nei tumori del Colon Daniele Rossini U.O. di Oncologia Medica
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
ASCO Poster Review PANCREATIC CANCER
 ASCO Poster Review PANCREATIC CANCER Dr.ssa Michela Squadroni U.O. Oncologia Humanitas Gavazzeni Bergamo TOPICAL ISSUES Gemcitabine/Nab-paclitaxel and FOLFIRINOX comparison Neoadjuvant and perioperative
ASCO Poster Review PANCREATIC CANCER Dr.ssa Michela Squadroni U.O. Oncologia Humanitas Gavazzeni Bergamo TOPICAL ISSUES Gemcitabine/Nab-paclitaxel and FOLFIRINOX comparison Neoadjuvant and perioperative
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Pancreatic Ductal Adenocarcinoma. Razvan Popescu Tumor Center Aarau Switzerland
 Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Median Survival of Patients With Pancreatic Cancer Localized/ Resectable 15-24 months 10% Locally Advanced 6-15 months 30%
Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Median Survival of Patients With Pancreatic Cancer Localized/ Resectable 15-24 months 10% Locally Advanced 6-15 months 30%
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy
 Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m B a y e r
 EXPERTS KNOWLEDGE SHARE with Prof. Köhne, Dr. Modest and Dr. Vecchione Madrid (Spain) Sunday September 10 th 2017 S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m
EXPERTS KNOWLEDGE SHARE with Prof. Köhne, Dr. Modest and Dr. Vecchione Madrid (Spain) Sunday September 10 th 2017 S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m
Optimal adjuvant therapy for colon cancer is FOLFOX for 6 cycles YES
 Optimal adjuvant therapy for colon cancer is FOLFOX for 6 cycles YES Bassel F. El-Rayes 1 Background Standard of care for resected stage III colon cancer is six months of adjuvant oxaliplatin-based therapy
Optimal adjuvant therapy for colon cancer is FOLFOX for 6 cycles YES Bassel F. El-Rayes 1 Background Standard of care for resected stage III colon cancer is six months of adjuvant oxaliplatin-based therapy
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)
 in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)") Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
ARROCase: Borderline Resectable Pancreatic Cancer
 ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Cancer diagnosis and treatments- brief overview of the changing paradigm.
 Cancer diagnosis and treatments- brief overview of the changing paradigm. Pranshu Bansal MD New Mexico Cancer Center Identifying cancer in clinic Most common cancers are lung, breast, colon, prostate and
Cancer diagnosis and treatments- brief overview of the changing paradigm. Pranshu Bansal MD New Mexico Cancer Center Identifying cancer in clinic Most common cancers are lung, breast, colon, prostate and
CHOLANGIOCARCINOMA (CCA)
") CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
COLORECTAL CANCER. Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program
 COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
Phase II trial of capecitabine plus nab-paclitaxel in patients with metastatic pancreatic adenocarcinoma
 Original Article Phase II trial of capecitabine plus nab-paclitaxel in patients with metastatic pancreatic adenocarcinoma Werner Scheithauer 1, Gabriela Kornek 1, Gerald Prager 1, Nadja Stranzl 1, Friedrich
Original Article Phase II trial of capecitabine plus nab-paclitaxel in patients with metastatic pancreatic adenocarcinoma Werner Scheithauer 1, Gabriela Kornek 1, Gerald Prager 1, Nadja Stranzl 1, Friedrich
Disclosure. Nothing to Disclose Will not be discussing off label use of any of the medications
 Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Slide 1. Slide 2. Slide 3 Pancreatic Cancer- Case #1. Endoscopic management of GI malignancy. Endoscopic approaches in GI malignancy- Agenda
 Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Pancreatic Ca Update
 Pancreatic Ca Update Caio Max S. Rocha Lima, M.D. M. Robert Cooper Professor in Medical Oncology Co-leader GI Oncology and Co-leader Phase I Program Wake Forest School of Medicine E-mail:crochali@wakehealth.edu
Pancreatic Ca Update Caio Max S. Rocha Lima, M.D. M. Robert Cooper Professor in Medical Oncology Co-leader GI Oncology and Co-leader Phase I Program Wake Forest School of Medicine E-mail:crochali@wakehealth.edu
INTERACTIVE SESSION 2
 INTERACTIVE SESSION 2 2 patients with lung metastases, with complete response after oncologic treatment - Clinical Case Presentation: Dr. Esther Casado Dr. Sergi Call - Expert Opinion: Dr. Raúl Embún Dr.
INTERACTIVE SESSION 2 2 patients with lung metastases, with complete response after oncologic treatment - Clinical Case Presentation: Dr. Esther Casado Dr. Sergi Call - Expert Opinion: Dr. Raúl Embún Dr.
A Brief Overview of Screening and Management of Colorectal Cancer
 A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Jonathan Dickinson, LCL Xeloda
 Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Cáncer de Páncreas: Optimización del tratamiento sistémico
 Cáncer de Páncreas: Optimización del tratamiento sistémico Alfredo Carrato Hospital Universitario Ramón y Cajal, Madrid 16 de Mayo de 2015 Pancreatic cancer screening There is a latency period of about
Cáncer de Páncreas: Optimización del tratamiento sistémico Alfredo Carrato Hospital Universitario Ramón y Cajal, Madrid 16 de Mayo de 2015 Pancreatic cancer screening There is a latency period of about
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Personal Profile. Name: 劉 XX Gender: Female Age: 53-y/o Past history. Hepatitis B carrier
 Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Pancreatic Cancer: Light at the End of the (Very Long) Tunnel
 Tunnel") Pancreatic Cancer: Light at the End of the (Very Long) Tunnel Daniel Renouf, MD, MPH, FRCPC Medical Oncologist, BC Cancer Agency University of British Columbia Objectives 1. Discuss recent updates in systemic
Pancreatic Cancer: Light at the End of the (Very Long) Tunnel Daniel Renouf, MD, MPH, FRCPC Medical Oncologist, BC Cancer Agency University of British Columbia Objectives 1. Discuss recent updates in systemic
What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015
 What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015 Eileen M. O Reilly, M.D. Associate Director David M. Rubenstein Center Pancreatic Cancer Research
What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015 Eileen M. O Reilly, M.D. Associate Director David M. Rubenstein Center Pancreatic Cancer Research
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Caring for a Patient with Colorectal Cancer. Objectives. Poll question. UNC Cancer Network Presented on 10/15/18. For Educational Use Only 1
 Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Treatment outcomes and prognostic factors of gallbladder cancer patients after postoperative radiation therapy
 Korean J Hepatobiliary Pancreat Surg 2011;15:152-156 Original Article Treatment outcomes and prognostic factors of gallbladder cancer patients after postoperative radiation therapy Suzy Kim 1,#, Kyubo
Korean J Hepatobiliary Pancreat Surg 2011;15:152-156 Original Article Treatment outcomes and prognostic factors of gallbladder cancer patients after postoperative radiation therapy Suzy Kim 1,#, Kyubo
NAACCR Webinar Series 4/5/2018 COLLECTING CANCER DATA: PANCREAS
 COLLECTING CANCER DATA: PANCREAS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: PANCREAS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Is There a New Standard of Care for Adjuvant Therapy in Colon Cancer? When is 3 Months Enough?
 Is There a New Standard of Care for Adjuvant Therapy in Colon Cancer? When is 3 Months Enough? Jeffrey Meyerhardt, MD, MPH Dana-Farber Cancer Institute Boston, MA 1 Disclosure Ad Board: Genentech Honorarium:
Is There a New Standard of Care for Adjuvant Therapy in Colon Cancer? When is 3 Months Enough? Jeffrey Meyerhardt, MD, MPH Dana-Farber Cancer Institute Boston, MA 1 Disclosure Ad Board: Genentech Honorarium:
Clinical trials updates: current and future cholangiocarcinoma trials
 U C L C A N C E R I N S T I T U T E Clinical trials updates: current and future cholangiocarcinoma trials John Bridgewater UCL Cancer Institute AMMF Information Day Imperial College, 10 May 2016 U C L
U C L C A N C E R I N S T I T U T E Clinical trials updates: current and future cholangiocarcinoma trials John Bridgewater UCL Cancer Institute AMMF Information Day Imperial College, 10 May 2016 U C L
Clinical Research in Rare Cancers. Friday 10 th February Matt Seymour & Nicola Keat
 Clinical Research in Rare Cancers Friday 10 th February 2012 Matt Seymour & Nicola Keat Rare cancer is a common disease Rare Cancer : [prevalence
Clinical Research in Rare Cancers Friday 10 th February 2012 Matt Seymour & Nicola Keat Rare cancer is a common disease Rare Cancer : [prevalence
Disclosures. GI Cancers for the Boards. Esophageal Cancer. Esophageal Cancer: Risk Factors
 Disclosures GI Cancers for the Boards Peter C. Enzinger, MD Dana-Farber Cancer Institute Major GI Malignancies: Esophageal Cancer Gastric Cancer Pancreatic Cancer Colorectal Cancer Less Common GI Malignancies:
Disclosures GI Cancers for the Boards Peter C. Enzinger, MD Dana-Farber Cancer Institute Major GI Malignancies: Esophageal Cancer Gastric Cancer Pancreatic Cancer Colorectal Cancer Less Common GI Malignancies:
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
HeavilyTreated mcrc..whats next?
 ESMO Preceptorship Programme Gastrointestinal Cancer 20-22 October 2016,Singapore Dr Surendra Pal Chaudhary Dept of Medical Oncology Dr BR Ambedkar Instituite Rotary Cancer Hospital All India Institute
ESMO Preceptorship Programme Gastrointestinal Cancer 20-22 October 2016,Singapore Dr Surendra Pal Chaudhary Dept of Medical Oncology Dr BR Ambedkar Instituite Rotary Cancer Hospital All India Institute
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
L oncologo Alberto Zaniboni
 COME TRATTARE LA NEOPLASIA LOCALMENTE AVANZATA BORDERLINE PER RESECABILITA L oncologo Alberto Zaniboni Oncologia Medica Fondazione Poliambulanza - Brescia Pancreatic cancer deaths in 2030 Pancreatic cancer
COME TRATTARE LA NEOPLASIA LOCALMENTE AVANZATA BORDERLINE PER RESECABILITA L oncologo Alberto Zaniboni Oncologia Medica Fondazione Poliambulanza - Brescia Pancreatic cancer deaths in 2030 Pancreatic cancer
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal