Targeted therapies in NSCLC beyond EGFR and ALK
|
|
|
- Tyler Adams
- 5 years ago
- Views:
Transcription


1 Targeted therapies in NSCLC beyond EGFR and ALK David Planchard (MD, PhD) Department of Cancer Medicine Thoracic Unit Gustave Roussy Villejuif (France)






2 Great advances have been made in lung cancer therapy: targeting of oncogenic drivers Stratification for EGFR, ALK and histology EFGR-activating mutation ALK translocation EGFR WT/ALKnon-squamous EGFR WT/ALKsquamous Erlotinib Gefitinib Afatinib Exon 20 T790M Osimertinib Crizotinib Ceritinib Alectinib 4 6 cycles Platinum-based doublet +/ bevacizumab +/- maintenance 4 6 cycles Platinum-based doublet ALK, anaplastic lymphoma kinase; EGFR, epidermal growth factor receptor; WT, wild-type

3 Frequency of genetic alterations 1-year nationwide programme in France analysed samples F.Barlesi et al, lancet 2016
4 Out of EGFR and ALK there are many other potential driver mutations in lung adenocarcinoma Biomarker France (IFCT) Unknown/ wild type 50% EGFR (sensitizing) 10.1% KRAS 29% EGFR (resistance) 0.9% HER2 1% Cancer Genome Atlas Research Network MET amp ERBB2 amp HRAS 0.4% 2.2% 0.9% 2.2% RIT1 NRAS 0.4% RET fusion 0.9% NF1 MAP2K1 0.9% 8.3% ALK fusion 1.3% None ROS1 fusion 1.7% 24.4% ERBB2 1.7% MET ex14 4.3% BRAF 7.0% KRAS BRAF 2% (V600E 1.4%) EGFR 11.3% 32.2% ALK 5% PI3K 2% By including amplification of MET and ERBB2, MET exon 14 splicing mutations, RIT1 mutations, and NF1 loss-of-function mutations, the driver-positive group increases to ~75% of cases IFCT, French Cooperative Thoracic Intergroup. Barlesi F, et al. Lancet. 2016;387: Cancer Genome Atlas Research Network. Nature. 2014;511:
 Enriched in younger, never or light smokers with adenocarcinoma histology No overlap with other oncogenic drivers CD74-ROS1")
5 ROS1 rearrangements in NSCLC SLC34A2-ROS1 TPM3-ROS1 SDC4-ROS1 Present in ca. 1% of NSCLC cases (also found in some GBMs and cholangiocarcinomas) Enriched in younger, never or light smokers with adenocarcinoma histology No overlap with other oncogenic drivers CD74-ROS1 LRIG3-ROS1 EZR-ROS1 ROS1 GBM, glioblastoma. Bergethon K, et al. J Clin Oncol. 2012;30: Takeuchi K, et al. Nat Med. 2012;18:
6 Diagnostic Break-Apart FISH Assay for ROS1 Rearrangement Bergethon et al., JCO 30(8): , 2012
7 Signaling Pathways Activated by ROS1? Ligand(s) ECM Proteins ROS1 ROS1 PDK1 Akt PIP3 PI3K PIP2 IRS- 1/GAB1 SHP-1/2 TORC2 RAS VAV3 TORC1 MEK STAT 3 Cdc42 Rho S6K1 rs6 4E-BP1 elf4e ERK Adapted from Acquaiva et al., Biochim Biophys Acta 1795(1): 37-52, 2009


8 ROS1 Encodes a Receptor Tyrosine Kinase ROS1 ROS1 ALK LTK PTK7 Brock TG, Receptors and Tyrosine Kinases

9 Crizotinib: Inhibitor of c-met, ALK and ROS1 Co-crystal structure of crizotinib (PF ) bound to c-met Kinase IC 50 (nm) mean* Selectivity ratio c-met 8 ALK X ROS1 60 7X RON 80 10X Axl X X Tie X Trk A X Trk B X Abl 1, X IRK 2, X Lck 2, X Sky >10,000 >1,000X VEGFR2 >10,000 >1,000X PDGFRβ >10,000 >1,000X Camidge et al, ASCO 2014 Cui et al. J Med Chem 54: , 2011 and Pfizer data on file


10 Significant Responses to Crizotinib in Patients with ROS1-Positive NSCLC Baseline After 3 months of crizotinib Bergethon et al., JCO 30(8): , 2012

11 Rapid Responses to Crizotinib in Patients with ROS1-Positive NSCLC Baseline After 4 weeks of crizotinib Image courtesy of Ignatius Ou
 36 (72) CR, n (%) 3 (6) PR, n (%) 33 (66) SD, n (%) 9 (18) DOR, median (95% CI), mo PFS, median (95% CI), mo 17.6 (14.5 NR) 19.2 (14.4 NR) 80 100 OS, median (95% CI), mo 12.")
12 Crizotinib and ROS1+ patients Change from baseline (%) patients (6%) CR 33 patients (66%) PR 9 patients (18%) SD PD SD PR CR * Overall response rate: 72% M A Best response N = 50 ORR, n (%) 36 (72) CR, n (%) 3 (6) PR, n (%) 33 (66) SD, n (%) 9 (18) DOR, median (95% CI), mo PFS, median (95% CI), mo 17.6 (14.5 NR) 19.2 (14.4 NR) OS, median (95% CI), mo 12.7 ( ) NR, not reached. Shaw AT, et al. N Engl J Med. 2014;371:

13 AcSé Crizotinib : objectives Single biomarker tests in the 15 malignancies To identify patients with an advanced malignancy presenting a crizotinib-target alteration and to generate epidemiological data Gilles Vassal et al, ESMO-ECCO 2015
14 Tumor ALK ALK MET ROS1 ALK MET transloc. amp. amp. transloc. mut. mut. ALCL 50% Colorectal 2,40% 3,60% 3,30% NSCLC 4% 3,50% 3% Breast 2,40% Gastric and 6% oesogastric junction Cholangiocarcinoma 9% Ovary 12% Renal cell carcinoma 2% 10,10% 13% Hepatocarcinoma 2,30% Neuroblastoma 3% Inflammatory myofibroblastic tumor 50% 10% Rhabdomyosarcoma 28% Glioblastoma 45% Thyroid 2% 11% 8% Spitzoid melanoma 10% 17% Gilles Vassal et al, ESMO-ECCO % 30% Crizotinib Inhibitor of ALK, MET and ROS1 Indication ALK+ NSCLC Targets altered in more than 15 malignancies in adults and children


15 1 uterine leiomyosarcoma - ALK translocation, 1 pancreatic cancer - ROS1 mutation, 1 neuroblastoma - ROS1mutation, 1 kidney cancer - ROS1 amplification, 3 NSCLC - MET mutation, 1 NSCLC - ALK mutation, 1 NSCLC - ALK amplification, 1 SCLC - MET mutation + ROS1 mutation, 1 adenoca. ouraque - MET amplification, 1 cholangiocarcinoma - MET amplification, 1 gallbladder - MET amplification, 1 B lymphoma, large cell - ALK translocation, 1 carcinoma of the esophagus - MET amplification, 1 sarcomatoid carcinoma hail - ALK translocation, 1 unknown primary carcinoma. - ALK translocation. Results : 24 cohorts STOP STOP STOP Gilles Vassal et al, ESMO-ECCO 2015
![Tumor shrinkage at best response Best response ORR = 26/36 72 % [55% ; 86%] DCR = 32/36 89](/docs-images/85/92375912/images/16-0.jpg "% [74% ; 97%] 44% PFS at 12 months Results: ROS1+ NSCLC Gilles Vassal et al, ESMO-ECCO")
16 Tumor shrinkage at best response Best response ORR = 26/36 72 % [55% ; 86%] DCR = 32/36 89 % [74% ; 97%] 44% PFS at 12 months Results: ROS1+ NSCLC Gilles Vassal et al, ESMO-ECCO 2015
17 Comparison of crizotinib efficacy across studies on ROS1+ NSCLC Profile (N = 50) EUROS1 2 (N = 31) AcSé 3 (N = 36) Trial Phase 1 expansion Retrospective Phase 2 Ethnicity Global (42% Asian) Europe France Diagnostic Local FISH Local FISH FISH Response rate 72% 80% 72% Median PFS, months % at 12 months Median follow-up, months 16.4?? NA EMA, European Medicines Agency; FDA, Food and Drug Administration; FISH, fluorescent in situ hybridization; NA, not applicable. 1. Shaw AT, et al. N Engl J Med. 2014;371: Mazières J, et al. J Clin Oncol. 2015;33: Vassal G, et al. ECCO 2015; abstract 12LBA.
18 The FDA and EMA approved crizotinib for the treatment of ROS1+ NSCLC (March and August 2016, respectively)

 Proportion of progression-free 0.8 0.6 0.4 0.")
 20 (67) CR 1 (3) 1 (3) PR 19 (59) 19 (59) SD 6 (19) 6 (19) PD 2")
 NE 4 (6) 2 (7) DCR")
19 Ceritinib in ROS1-rearranged NSCLC: a Korean nationwide phase II study Baseline 5 months Baseline 3 months -66% PR CR 1.0 Progression-free survival Best response, n (%) All patients (N=32) Crizotinib-naïve (N=30) Proportion of progression-free All patients (n = 32) Crizontinib-naïve patients (n = 30) ORR 20 (62) 20 (67) CR 1 (3) 1 (3) PR 19 (59) 19 (59) SD 6 (19) 6 (19) PD 2 (6) 2 (6) Duration (months) NE 4 (6) 2 (7) DCR (CR+PR+SD) 26 (81) 26 (87) Lim S, et al. Presented at ESMO Abstract 1205PD.

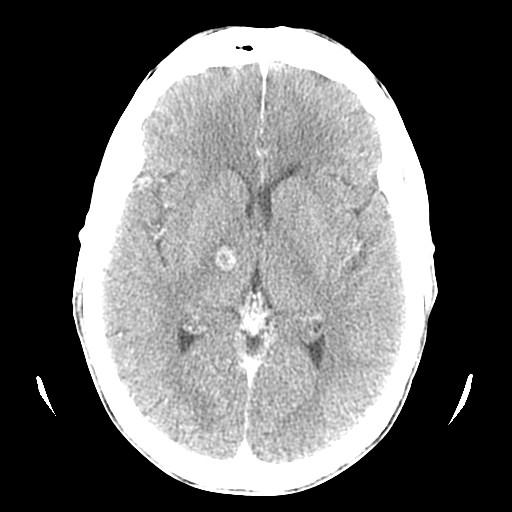
20 Acquired Resistance to Crizotinib from a Mutation in CD74 ROS1 Acquired resistance to crizotinib from a mutation in CD74-ROS1. N Engl J Med Jun 20;368(25):
21 Overcoming Crizotinib Resistance in Advanced ROS1+ NSCLC WT ROS1 G2032R Trials Alectinib 1 3,700 nm --- None not active Ceritinib nm 277 nm Phase 2 (SIGNATURE) Brigatinib nm 322 nm Investigator initiated trials Lorlatinib nm 167 nm Phase 2 Cabozantinib 2 2 nm 13.5 nm Phase 2 (MSKCC) Foretinib 4 ~3 nm 50 nm None Crizotinib nm 254 nm Phase 1 (PROFILE 1001) 1 Kodama et al., Mol Cancer Ther 13: , 2014; 2 Katayama et al., Clin Cancer Res 21(1): , 2015; 3 Zou et al., AACR-EORTC-NCI, 2013; 4 Davare et al., PNAS 110(48): , 2013


 Biopsy S1986 MTB")
22 ROS1 - Acquired Resistance to Crizotinib Ba/F3 EZR ROS1 100 crizotinib ceritinib lorlatinib % Cell Viability Drug Concentration (nm) Biopsy S1986 MTB Francesco Facchinetti et al, CCR 2015
23 Sensitivity of the CD74 ROS1 mutant reintroduced Ba/F3 cells to crizotinib or ceritinib Ryohei Katayama et al, CCR 2015
24 Cabozantinib (XL184) overcomes crizotinib resistance caused by the mutations in CD74 ROS1 cmet/ret/vascular endothelial growth factor (VEGFR) inhibitor cabozantinib Ryohei Katayama et al, CCR 2015

25 Modeling theoretical sensitivity of ROS1 patients according to their mutational status Francesco Facchinetti et al, CCR 2015
26 Frequency of genetic alterations 1-year nationwide programme in France analysed samples F.Barlesi et al, lancet 2016

27 Inhibition of BRAF V600 Kinase RTKs P P SOS Grb2 P P SHC P P RAS Dabrafenib Vemurafenib BRAF V600 BRAF CRAF MEK PI3K/AKT/mTOR pathway ERK1/2 p90rsk MSK1 Proliferation, Growth, Survival
 to an aspartic acid (D) V600K from a valine (V) to a lysine (K) V600R from a valine (V) to an arginine (R)")
28 V600E mutation results in an amino acid substitution at position 600 in BRAF, from a valine (V) to a glutamic acid (E) V600D from a valine (V) to an aspartic acid (D) V600K from a valine (V) to a lysine (K) V600R from a valine (V) to an arginine (R)


29 BRAF inhibitors: quick tumour responses in PET scans and clinically Before After 2 weeks Before After 2 weeks Images courtesy of Grant McArthur and Rod Hicks, Peter MacCallum Cancer Centre, Melbourne, Australia.
 Vemurafenib + cetuximab (N = 27) 19 10 26 CR, n (%) 0 0 0 PR, n (%) 8 (42) 0 1 (4) SD, n (%) 8 (42) 5 (50) 18 (69) PD, n (%) 2 (11) 5 (50) 7 (27) Missing data, n (%) 1 (5) 0 0 OR, n (%) [95% CI]")
![8 (42) [20 67] 0 1 (4) [< 1 20] Target tumour diameter sum (% change from baseline) 100 80 60 40 20 0 20 40 60 80 100 NSCLC cohort mpfs: 7.3 months (95% CI 3.5 10.](/docs-images/85/92375912/images/30-2.jpg "8) a Patients with several pre-specified cancers were enrolled into the study, including NSCLC and colorectal cancer.")
30 Vemurafenib in NSCLC with BRAF V600 mutations Basket trial (multiple non-melanoma cancers) Variable Patients with 1 postbaseline assessment, n NSCLC a (N = 20) Colorectal cancer a Vemurafenib (N = 10) Vemurafenib + cetuximab (N = 27) CR, n (%) PR, n (%) 8 (42) 0 1 (4) SD, n (%) 8 (42) 5 (50) 18 (69) PD, n (%) 2 (11) 5 (50) 7 (27) Missing data, n (%) 1 (5) 0 0 OR, n (%) [95% CI] 8 (42) [20 67] 0 1 (4) [< 1 20] Target tumour diameter sum (% change from baseline) NSCLC cohort mpfs: 7.3 months (95% CI ) a Patients with several pre-specified cancers were enrolled into the study, including NSCLC and colorectal cancer. CI, confidence interval; CR, complete response; mpfs, median PFS; OR, overall response; PD, progressive disease; PFS, progression-free survival; PR, partial response; SD, stable disease. Hyman DM, et al. N Engl J Med. 2015;373:



31 BRAF V600E and Vemurafenib B.Besse, Gustave Roussy
32 BRF study design Multicohort, non-randomized, open-label phase 2 study Cohort A (dabrafenib monotherapy) planned n = 60 Interim futility analysis Stage IV NSCLC BRAF V600E ECOG PS platinum-based chemotherapy Dabrafenib 150 mg b.i.d. Stage 1 n = 20 Stage 2 n = 20 Expansion n = 20 n = 78 ( 2nd line) Cohort B (combination dabrafenib + trametinib) planned n = 40 Stage IV NSCLC BRAF V600E ECOG PS prior treatments 1 platinum-based chemotherapy Dabrafenib 150 mg b.i.d. Trametinib 2 mg q.d. Stage 1 n = 20 Cohort C (combination dabrafenib + trametinib in 1st line) planned n = 25 Stage 2 n = 20 n = 57 (2nd 4th line) Stage IV NSCLC BRAF V600E ECOG PS 0 2 No prior treatment Dabrafenib 150 mg b.i.d. Trametinib 2 mg q.d. n = 34 ENROLLMENT COMPLETED b.i.d., twice daily; ECOG, Eastern Cooperative Oncology Group; PS, performance status; q.d., once daily. Planchard D, et al. Lancet Oncol. 2016;17: Planchard D, et al. Lancet Oncol. 2016;17:
33 380 Dabrafenib monotherapy: maximum reduction Maximum percent reduction from baseline measurement Best Confirmed confirmed Response response PR SD PD NE Best response 2nd line (N = 78) Response rate (confirmed CR + PR) 32% 95% CI ( ) DCR (CR + PR + SD) 56% 95% CI ( ) DCR, disease control rate; NE, not evaluable. Planchard D, et al. Lancet Oncol. 2016;17:
34 Dabrafenib monotherapy: Progression-free survival (independent review) No. at risk PFS Time from first dose (months) Independent PFS: 5.5 months (95% CI ) Planchard D, et al. Lancet Oncol. 2016;17:
 ECOG PS2 Adenocarcinoma, BRAFV600E, T3N3M1b (pleural, pulmonary, lymph")

35 Dabrafenib Activity in BRAF V600E NSCLC 72 year old white female, 2 nd line, former smoker, 10 pack years (stop in1985) ECOG PS2 Adenocarcinoma, BRAFV600E, T3N3M1b (pleural, pulmonary, lymph nodes) Progression after one line of platinum-pemetrexed October weeks of Dabrafenib Baseline CT-Scan. Mazieres et al, Hôpital Larrey CHU Toulouse ECOG PS0 D.Planchard et al, ESMO 2014



36 Unique residual disease in the lower left lung Discussion for a local treatment 2 years after the start of dabrafenib J. Mazieres et al, Hôpital Larrey CHU Toulouse D.Planchard et al, ESMO 2014 ECOG PS:0 Asymptomatic Very good safety profile (rare episodes of fever) September 2014

37 Acquired resistance to BRAF inhibition: many hypotheses Johannessen CM, et al. Nature. 2010;468: Nazarian R, et al. Nature. 2010;468: Poulikakos PI, et al. Nature. 2011;480: Shi H, et al. Nature Commun. 2012;3:724. Straussman R,et al. AACR. 2012;abstract Villanueva J, et al. Cancer Cell. 2010;18: Wagle N, et al. J Clin Oncol. 2011;29:

38 Wagle N, et al. J Clin Oncol. 2011;29:
39 Dabrafenib P RTKs P SOS P P Grb2 SHC P P RAS BRAF V600 BRAF CRAF PI3K/AKT/mTOR pathway MEK ERK1/2 Trametinib p90rsk MSK1 Proliferation, growth, survival Luke JJ, Ott PA. Drug Healthc Patient Saf. 2014;24:77-88.
40 Rationale for combination of dabrafenib + trametinib Dabrafenib + trametinib was more efficacious than BRAF-inhibitor monotherapy in BRAF V600-mutant melanoma dabrafenib + trametinib demonstrated clinically meaningful and significantly superior efficacy while reducing the risk of cutaneous squamous cell carcinoma COMBI-d 1 COMBI-v 2 Dabrafenib + trametinib (n = 211) Dabrafenib + placebo (n = 212) Dabrafenib + trametinib (n = 351) Vemurafenib (n = 350) Median OS, months Median PFS, months ORR, n (%) 144 (69) 112 (53) 226 (64) 180 (51) Median DOR, months DOR, duration of response; ORR, overall response rate. 1. Long GV, et al. Lancet. 2015;386: Robert C, et al. N Engl J Med. 2015;372:30-9.
41 Dabrafenib + trametinib: best confirmed response Investigator assessment (n = 57) Independent assessment (n = 57) ORR (CR + PR), n (%) [95% CI] 36 (63) [49 76] 36 (63) [49 76] Best response, n (%) CR PR SD a PD Non-CR/non-PD b NE 2 (4) 34 (60) 9 (16) 7 (12) 0 5 (9) 0 36 (63) 4 (7) 8 (14) 3 (5) 6 (11) DCR (CR + PR + SD), n (%) [95% CI] 45 (79) [66 89] 43 (75) [62 86] a SD is defined as meeting SD criteria for 12 weeks. b Patients were non-measurable by independent review committee. Planchard D, et al. Lancet Oncol. 2016;17:
42 Maximum reduction from baseline measurement (%) Dabrafenib + trametinib: maximum change in target lesion Best confirmed response Maximum change in target lesion by best investigatorassessed confirmed response CR PR SD PD NE ORR: 63% (95% CI 49 76) Patients NE patients either had no post-baseline CT scan or discontinued before 12 weeks without documented progression. Planchard D, et al. Lancet Oncol. 2016;17:
43 Dabrafenib + trametinib: progression-free survival Progression-free survival by investigator assessment PFS, median (95% CI), mo Progressions or deaths, n (%) Investigator assessment 9.7 ( ) 32 (56) Independent assessment 8.6 ( ) 34 (60) Time from first dose (months) No. at risk No. censored Dashed lines represent 95% CIs. Median follow-up of 11.6 months. Planchard D, et al. Lancet Oncol. 2016;17:

")
 PR at Week 6 with 54%")
 CDDP, cisplatin. Planchard D, et al.")
44 61-year-old woman, never smoked Dabrafenib + trametinib: case study 1 Adenocarcinoma with pleural effusion, liver metastases, 4th line (CDDP-pemetrexed, docetaxel, gemcitabine) Baseline (July 2014) Dabrafenib + trametinib +25 months (August 2016) PR at Week 6 with 54% reduction (confirmed and still response, 73% +25 months) CDDP, cisplatin. Planchard D, et al. Gustave Roussy Villejuif.


 +27 months (July 2016) PR at Week")
 Planchard D, et al.")
45 Dabrafenib + trametinib: case study 2 59-year-old man, former smoker, 70 packs/year Adenocarcinoma with irradiated brain metastases, 2nd line (1st line carboplatin + pemetrexed) Dabrafenib + trametinib Baseline (July 2014) +27 months (July 2016) PR at Week 6 with 70% reduction (confirmed and still response, 80% +27 months) Planchard D, et al. Gustave Roussy Villejuif.
46 Dabrafenib + trametinib vs dabrafenib monotherapy: adverse events Category Dabrafenib + trametinib Dabrafenib monotherapy AEs, n (%) All grades Grade 3 All grades Grade 3 General Pyrexia 26 (46) 1 (2) 30 (36) 2 (2) Asthenia 18 (32) 2 (4) 25 (30) 3 (4) Decreased appetite 17 (30) 0 24 (29) 1 (1) Chills 13 (23) 1 (2) 13 (15) 1 (1) Peripheral oedema 13 (23) 0 Arthralgia 11 (19) 0 14 (17) 1 (1) Skin Dry skin 15 (26) 1 (2) 19 (23) 0 Rash 12 (21) 1 (2) 17 (20) 1 (1) Hyperkeratosis 6 (10) 1 (2) 25 (30) 1 (1) Basal-cell carcinoma 2 (2) 1 (2) 4 (5) 4 (5) Squamous-cell carcinoma 2 (4) 2 (4) 10 (12) 10 (12) Skin papilloma 22 (26) 0 Digestive Nausea 23 (40) 0 23 (27) 1 (1) Vomiting 20 (35) 0 17 (20) 1 (1) Diarrhoea 19 (33) 1 (2) 14 (17) 1 (1) Planchard D, et al. Lancet Oncol. 2016;17: Planchard D, et al. Lancet Oncol. 2016;17:
47 Dabrafenib + trametinib provided an important treatment option for patients with BRAF V600E-mutant NSCLC With greater clinical activity compared with dabrafenib monotherapy Based on investigator assessment Dabrafenib + trametinib 1 (n = 57) Dabrafenib monotherapy 2 (n = 78) ORR, % (95% CI) 63 (49 76) 33 (23 45) DCR, % (95% CI) 79 (66 89) 58 (46 67) Median PFS, mo (95% CI) 9.7 ( ) 5.5 ( ) Median DOR, mo (95% CI) 9.0 ( ) a 9.6 ( ) The safety profile was manageable and similar to previous experience in melanoma a One-half of responses were ongoing at data cut-off. 1. Planchard D, et al. Lancet Oncol. 2016;17: Planchard D, et al. Lancet Oncol. 2016;17:

48 MET activation: amplification and/or exon 14 mutation/skipping Implicated in tumour cell migration, invasion, proliferation, and angiogenesis MET testing Mechanisms of MET activation amplification, point mutations, deletions MET amplification poor prognosis in NSCLC resistance to EGFR TKI 1 4% of lung NSCLC MET exon 14 mutation 3 4% of nonsquamous NSCLCs 20 30% of sarcomatoid lung carcinomas TKI, tyrosine kinase inhibitors. Ou SH, et al. J Thorac Oncol. 2011;6: Cancer Genome Atlas Research Network. Nature. 2014;511:
49 Tumour shrinkage seen with crizotinib treatment in intermediate and high MET cohorts Change from baseline (%) Best percent change from baseline in target tumour lesions by patient Low MET n = Intermediate MET n = MET/CEP7 ratio 5 High MET n = 6 ORR, % (95% CI) 0 (0 84) 17 (0 64) 67 (22 96) PD SD PR CR Threshold for partial response Camidge DR, et al. ASCO J Clin Oncol. 2014;32:5s (suppl; abstract 8001).


50 8/16/ /9/2011 3/27/2014 a MET/CEP7 ratio: >5 Duration of response: 31+ months Images: G. Shapiro DFCI

![49%] DCR = 15/25 60 % [41%;79%] No correlation observed between](/docs-images/85/92375912/images/51-2.jpg "the number of MET copies and best response (p=0,10). G.")
51 The French national AcSé Program Results: METAMP NSCLC Tumor shrinkage at best response Best response ORR = 7/25 28 % [12% ; 49%] DCR = 15/25 60 % [41%;79%] No correlation observed between the number of MET copies and best response (p=0,10). G.Vassal et al 2015
52 Tumour shrinkage observed with capmatinib treatment in intermediate and high MET cohorts Best response n (%) GCN < 4 (n = 17) GCN 4 and < 6 (n = 12) GCN 6 (n = 15) CR PR 0 2 (17) 7 (47) SD 8 (47) 3 (25) 5 (33) PD 5 (29) 3 (25) 2 (13) Unknown 4 (24) 4 (33) 1 (7) ORR 0 2 (17) 7 (47) 95% CI DCR 95% CI 8 (47) (42) (80) Best % change from baseline cmet GCN < 4 n/n (%) = 11/17 (64.7%) Best % change from baseline cmet GCN 4 and < 6 n/n (%) = 7/12 (58.3%) Best % change from baseline cmet GCN 6 n/n (%) = 12/15 (80.0%) GCN, gene copy number. Schuler M, et al. ASCO J Clin Oncol. 2016;34 Suppl:abstract 9067.

53 Prevalence of MET Exon 14 Mutations in NSCLC Awad MM, et al, J Clin Oncol Jan 4.
54 Normal MET Signaling HGF/SF Exon 14 Mutated/Skipped Cbl P Ub Ub Ub TKD Ex14 TKD Ex14 P Tyr1003 P P P P P TKD TKD Ex14 skipping P P P Grb2 P P Receptor Activation (Ras/MAPK, PI3K/Akt, Src, STAT3) Receptor internalization Receptor degradation Exon 14 mutation/skipping Loss of c-cbl binding site Decreased ubiquitination Impaired receptor degradation Increased MET signaling Awad MM, J Clin Oncol Jan 19.
55 Prognosis of MET Exon 14 Mutant NSCLC MET exon 14 wild type MET exon 14 mutant METΔ14 occurred mutually exclusively with known driver mutations but tended to coexist with MET amplification or copy number gain (p<0.001) Tong, JH, et al Clin Cancer Res Feb 4.
 of 36 patient with")

56 MET 14 skipping in pulmonary sarcoma Eight (22%) of 36 patient with pulmonary sarcoma. One with a concurrent PIK3CA mutation Liu et al. JCO
 Best OR, n (%) CR 0 Crizotinib PR 8 (44%) SD 9 (50%) Unconfirmed CR/PR a 5 (28%) Crizotinib PD 0 Indeterminate b 1 (6%) ORR 8 (44%) 95% CI 22 69 a Of the 5 patients, 2 await")
57 MET exon 14-mutant NSCLC may respond to treatment with c-met inhibitors such as crizotinib and cabozantinib Cabozantinib Antitumour activity of crizotinib (PROFILE 1001 study) Response-evaluable population (n = 18) Best OR, n (%) CR 0 Crizotinib PR 8 (44%) SD 9 (50%) Unconfirmed CR/PR a 5 (28%) Crizotinib PD 0 Indeterminate b 1 (6%) ORR 8 (44%) 95% CI a Of the 5 patients, 2 await confirmation, 3 cannot be confirmed. b This patient discontinued therapy in cycle 1; response imaging could not be performed but response-evaluable per protocol. Drilon AE, et al. ASCO J Clin Oncol. 2016;34 Suppl:abstract 108. Frampton GM, et al. Cancer Discov. 2015;5: Paik PK, et al. Cancer Discov. 2015;5: Waqar SN, et al. J Thorac Oncol. 2015;10:e Paik et al. Cancer Discovery
58 Antitumor Activity and Safety of Crizotinib in Patients with Advanced MET Exon 14-Altered Non-Small Cell Lung Cancer 20 ORR: 44% (95% CI: 22 69), n=8/18 % change from baseline * * Partial response (PR), confirmed Stable disease (SD): includes 4 unconfirmed PRs concurrent MET Amplification -100 Central testing for both MET exon 14 alterations and high-level MET amplification via ThermoFisher Scientific Inc., Ion Torrent (Cancer Genetics, CA) Presented by: Alexander Drilon MD
 51-year-old female EGFR L858R / MET AMP First scan post-treatment Baseline Kollmannsberger ASCO 2015")
59 Early signs of glesatinib clinical activity in NSCLC patients with MET copy gain or METex14del mutations 76-year-old male METex14del (+) 70-year-old female METex14del (+) 51-year-old female EGFR L858R / MET AMP First scan post-treatment Baseline Kollmannsberger ASCO 2015 Abstract 2589.
60 RET rearrangements 1 2% of unselected NSCLCs Clinical features: young, never or former light cigarette smokers 5 KIF5B RET exon 12 3 kinase KIF5B-RET fusions kinase Intact tyrosine kinase domain fused to an upstream gene partner most common: KIF5B others: CCDC6, NCOA4, TRIM33, KIAA1468 exon 8 exon 11 kinase kinase kinase kinase Result in ligand-independent dimerization and downstream growth pathway activation CCDC6 exon 12 kinase CCDC6-RET Oncogenic in vitro and in vivo NCOA4 kinase NCOA4-RET TRIM33 kinase TRIM33-RET Drilon A, et al. Cancer Discov. 2013;3: Kohno T, et al. Nat Med. 2012;18: Lipson D, et al. Nat Med. 2012;18: Saito M, et al. Carcinogenesis. 2014;35: Suehara Y, et al. Clin Cancer Res. 2012;18: Takeuchi K, et al. Nat Med. 2012;18:
61 Multi-kinase inhibitors targeting RET activity Compound Target KDR IC50 (nm) RET IC50 (nm) Cabozantinib KDR/MET 1 7 Vandetanib KDR/EGFR 2 5 Ponatinib ABL/Pan-RTK 2 1 Lenvatinib KDR 4 2 Sorafenib RAF/VEGF 21 6

 44 (7/16) Confirmed 38 (6/16) Unconfirmed 6 (1/16)")
 DOR, median (range), mo 8 (5.")
 Drilon AE, et al. ASCO 2015. J Clin Oncol.")
62 Best response (%) Response to cabozantinib in patients with RET-rearranged lung adenocarcinomas Confirmed PR SD Stage 1 (N = 16) 90 Best response Stage 1 (N = 16) PR, % (n/n) 44 (7/16) Confirmed 38 (6/16) Unconfirmed 6 (1/16) SD, % (n/n) 56 (9/16) ORR, % (95% CI) 38 (95% CI 15 65) ORR 12wks 36 (95% CI 13 65) DOR, median (range), mo 8 ( months) Baseline 4 weeks PFS (95% CI), mo 7 (95% CI 5 NA) Drilon AE, et al. ASCO J Clin Oncol. 2015;33 Suppl:abstract 8007.

63 A Drilon et al, ASCO 2015 Response to Cabozantinib 46-year-old female never smoker with CLIP1-RET-rearranged lung adenocarcinoma baseline 4 weeks received cabozantinib as first-line therapy confirmed partial response lasting 19 months
64 Phase 2 study to evaluate efficacy and safety of vandetanib in RET-rearranged NSCLC Maximum tumour shrinkage from baseline (%) KIF5B-RET CCDC6-RET Unknown-RET n = 19, ITT population Efficacy according to RET fusion All (n = 19) KIF5B-RET (n = 10) CCDC6-RET (n = 6) Unknown (n = 3) ORR, % (95% CI) 47 (24 71) 20 (3 56) 83 ( ) 67 (9 99) DCR, % (95% CI) 90 (67 99) 90 ( ) 100 (54 100) 67 (9 99) Median PFS, mo (95% CI) 4.7 ( ) 2.9 ( ) 8.3 ( ) 4.7 ( ) 1-year OS, % (95% CI) 47 (21 69) 42(11 71) 67 (5 95) 33 (1 77) ITT, intention-to-treat. Seto T, et al. ASCO J Clin Oncol. 2016;34 Suppl:abstract 9012.
65 Treatment n Response rate (%) Vandetanib (Seto 2016) Vandetanib (Lee 2016) Vandetanib (Gautschi 2016) Vandetanib (Horiike 2016) Cabozantinib (Drilon 2015) Cabozantinib (Gautschi 2016) Sunitinib (Gautschi 2016) Lenvatinib (Velcheti 2016) Overview of RET studies PFS (months) OS (months) % 1yr OS NR Drilon AE, et al. ASCO J Clin Oncol. 2015;33 Suppl:abstract Gautshi O, et al. ASCO J Clin Oncol. 2016;34 Suppl:abstract Lee SH, et al. ASCO J Clin Oncol. 2016;34 Suppl:abstract Seto T, et al. ASCO J Clin Oncol. 2016;34 Suppl:abstract Horiike A, et al. ESMO Abstract 1203PD. Velcheti V, et al. ESMO Abstract 1204PD.
 20 15 10 5 NTRK1 NTRK2 NTRK3 ROS1 ALK Detectable in the clinic FISH RNAseq DNA-based NGS 0 Select fusions are")
66 Trk prone to fusion proteins, similar to ALK, that induce constitutive activation of cell signalling Oncogenic drivers across a variety of cancers upstream partner can provide dimerization domains and ligand-independent signalling activation of downstream pathways Prevalence (%) NTRK1 NTRK2 NTRK3 ROS1 ALK Detectable in the clinic FISH RNAseq DNA-based NGS 0 Select fusions are clinically actionable responses to targeted therapy can be dramatic and durable PTC, papillary thyroid cancer; CRC, colorectal cancer. Drilon A, et al. AACR 2016:abstract CT007. Farago AF, et al. J Thorac Oncol. 2015;10:
 as nextgeneration ALK inhibitor Later discovered to have potent TrkA/B/C and ROS1 activity Trk and ROS1 prone to fusion proteins, similar to")
67 Entrectinib: a First-in-Class Trk Inhibitor Target TrkA TrkB TrkC ROS1 ALK IC50* (nm) Initially discovered by Nerviano Medical Sciences (NMS) as nextgeneration ALK inhibitor Later discovered to have potent TrkA/B/C and ROS1 activity Trk and ROS1 prone to fusion proteins, similar to ALK, that induce constitutive activation of cell signaling Entrectinib demonstrates inhibition of its RTK targets and downstream effectors in the PLCγ, MAPK and PI3K/AKT pathways * Biochemical kinase assay
 Alexander Drilon et al,")
68 Antitumor Activity (phase I studies) Alexander Drilon et al, AACR 2016

69 Duration of Clinical Benefit PTC: Papillar y thyroid cancer, CRC: colorectal cancer Alexander Drilon et al, AACR 2016





70 Baseline Day 26: - 47% response Day 155: - 77% response Anna F. Farago et al, JTO 2015





71 Baseline Day 26 Day 155

72 Current Directions
73 Principales mutations/insertions de HER2 Insertion de l exon 20 de 3 à 12 pdb. Entre les codons 775 and 881 : 12 pdb : 83% entrainant une insertion de 4 AA(YVMA). Insertion de 3 pdb 8% Mutations ponctuelles exon 20 : L755S et G776C 8%. Mutations de l exon 17 : G660D, V659E. Arcila ME, CCR 2012 Yamamoto H, JNCI 2014

74 Afatinib, efficace sur modèle préclinique 3 réponses objectives De Greve, Lung Cancer 2012


75 HER2 gene Polysomy Baseline After 2 months June 22, 2005 After 4 months Aug 31, 2005 Nov 8, 2005 Cappuzzo NEJM, 2006




76 Prédominance de femmes, non fumeurs, adénocarcinomes Mazières J, JCO 2013
77 Patients de stade IV traités avec des anti-her2 Patient 1 st line T Best disease response 1 VIN-HER PR 2 CAR-PAC-TRAS SD 3 TXT-MASA PD 4 VIN-TRAS PR 5 CAR-PAC-TRAS PR 6 VIN-TRAS PR 7 VIN-TRAS SD 8 LAP PD 9 NVB-HER PR 2 nd line T Best disease response 3rd line T Best disease response 4th line T Best disease response 10 LAP PD TRAS-VIN PR AFA SD CAR-TRAS SD 11 VIN-TRAS PD 12 DOC-TRAS PR 13 VIN-TRAS PR AFA PR 14 VIN-TRAS PR AFA SD 15 VIN-TRAS SD PAC-TRAS SD 16 TRAS PR SD: Stable Disease, PR: Partial Response, PD: Progressive disease, NE: non evaluated Conventional treatment: CAR: Carboplatin, PAC: Paclitaxel, VIN: Vinorelbin, DOC: Docetaxel. HER2 specific treatments: TRAS: Trastuzumab, LAP: Lapatinib, AFA: Afatinib, MASA: masatinib Taux de controle de la maladie : 96% pour le trastuzumab (n = 15), 100 % pour afatinib (n = 4).
78 Aberrant ERBB activation by: Gene amplification Receptor overexpression Somatic mutations EGFR:EGFR HER2:EGFR HER2:HER3 HER2:HER2 HER2:HER4 ERBB receptor dimerization Kinase activation Neratinib PI3K RAS PI3K Pathway AKT RAF MEK MAPK Pathway Downstream signal transduction Temsirolimus mtor ERK Nucleus Tumor growth, survival and spread Cell cycle control and proliferation Cell survival and decreased apoptosis Cellular migration and metastasis Angiogenesis B.Besse et al, ESMO 2014
79 Targeting HER2 aberrations HER2 mutations in 1 4% and HER2 amplifications in 2 5% of lung ADC Change from baseline (%) Dacomitinib (pan-her inhibitor) (HER2-mutated or amplified NSCLC) Partial response n = 30 HER2 mutation HER2 amplification Only 3/26 of HER2-mutant patients had a response (ORR 12%) Change in sum LD (%) PD PD PD Neratinib (pan-her inhibitor) ± temsirolimus (mtor inhibitor) (HER2-mutated NSCLC) PD SD SD PD SD * * SD SD SD SD PD * 30% threshold for reduction in tumour burden (response) Neratinib Neratinib + temsirolimus Partial response 0 (0) 3 (21)* SD SD SD SD SD SD SD SD SD SD SD PR PR PR 21% ORR and mpfs of 4 months * Patients had < 20% increase in tumour burden, but were considered PD due to the appearance of new lesions Kris MG, et al. Ann Oncol. 2015; 26: Besse B, et al. Presented at ESMO Abstract LBA 39.
80 And other targetable mutations Gene Alteration Histology Frequency (%) Inhibitor (Phase 1 and 2) BRAF Mutation, fusion ADC 1 3 Vemurafenib, dabrafenib, dabrafenib + trametinib ROS1 Chromosomal rearrangement ADC 1 2 Crizotinib (approved), ceritinib, cabozantinib, entrectinib, lorlatinib, DS-6051b MET Amplification, exon14 splicing ADC 1 4 (amplifications) 2 4 (mutations) Crizotinib, cabozantinib, tivantinib, capmatinib, volitinib, onartuzumab, glesatinib RET Fusion ADC 1 2 Carbozantinib, sunitinib, sorafenib, lenvatinib, vandetanib, ponatinib, alectinib, apatinib NTRK Fusion ADC < 1 Entrectinib, LOXO-101, cabozantinib, DS-6051b, merestinib HER2 Mutation (exon 20), amplification ADC 1 4 Trastuzumab, neratinib + temsirolimus, afatinib, lapatinib, dacomitinib KRAS Mutation ADC Selumetinib, trametinib PIK3CA Mutation, amplification SCC 15 (amplifications) (mutations) LY , PQR309, AZD2014, GDC-0032, AZD8186, IPI-549, BYL719 FGFR1 Amplification SCC 20 FGFR2-3 Mutation SCC 3 Lucitanib, nintedanib, dovitinib, AZD4547 FGFR1-3 Fusion SCC 3.5 DDR2 Mutation SCC 4 Dasatinib

81 Hyman DM, et al. N Engl J Med. 2015;373: Gautschi O, et al. J Thorac Oncol. 2015;10: Planchard D, et al. Lancet Oncol. 2016;17: Planchard D, et al. Lancet Oncol. 2016;17:
82 In summary. Diagnostic workup Molecular profiling 1. Multidisciplinary discussion to determine optimal procedure for tissue procedure 2. Biopsy 3. Morphology 4. Review of patient and tumour data Integrated NGS-based assay to detect mutations, amplifications, and translocations Patient selection Treatment EGFR ALK BRAF ROS1 RET MET exon 14mut/Amp NTRK1/2/3 HER2 No actionable alterations 1. Firstgeneration EGFR TKI 2. Thirdgeneration EGFR TKI 1. Crizotinib 2. 2nd or 3nd ALK TKI (Ceritinib, alectinib, Brigatinib) Dabrafenib + trametinib Vemurafenib Crizotinib Ceritinib Lorlatinib Cabozantinib Cabozantinib Vandetanib Sunitinib Crizotinib Cabozantinib Glesatinib Entrectinib Trastuzumab Neratinib+/- Temsirolimus Afatinib Dacomatinib Chemotherapy or immunotherapy Treatment cessation Subsequent therapies Treatment until response, progressive disease, or unacceptable adverse effects Therapy switch/combination based on re-biopsies or liquid therapy Adapted from Thomas A, et al. Nat Rev Clin Oncol. 2015;12:






")





83 Thoracic Molecular Tumor Board ON- PURPOSE FRESH TUMOR BIOSPSY & PATHOLOGY CONTROL MOLECULAR PROFILING (CGH & NGS) MOLECULAR TUMOR BOARD Since 2010 TREATMENT Max 21 calendar days

84 Acknowledgments Jean-Charles SORIA Benjamin BESSE Thierry LE CHEVALIER THANK YOU



85 ALK+ TKI + Immunotherapy.? EGFR+
 a Fusion Confirmed response (n) ORR (%) NTRK1/3 3/3 100% PD PR CR Clinical response to entrectinib NTRK1- rearranged NSCLC Baseline Day 26: 47%")
86 Entrectinib: study of a first-in-class Trk inhibitor in various previously treated solid tumours Tumour reduction (%) Best response in TKI treatment-naïve NTRK-, ROS1-, and ALK-rearranged solid tumours (n = 24) a Fusion Confirmed response (n) ORR (%) NTRK1/3 3/3 100% PD PR CR Clinical response to entrectinib NTRK1- rearranged NSCLC Baseline Day 26: 47% response Day 155: 77% response ROS1 12/14 86% a Patients with ALK different tumour 4/7 types were 57% included in this study, including NSCLC, mammary analogue secretory carcinoma, and renal cell carcinoma. Images courtesy of A. Shaw and A. Farago, Massachusetts General Hospital. Drilon A, et al. AACR 2016:abstract CT007. Farago AF, et al. J Thorac Oncol. 2015;10:
87 ROS inhibitors ALK/ROS1 inhibitors Crizotinib Ceritinib Brigatinib (AP26113) Entrectinib (RXDX-101) Lorlatinib Non-ALK inhibitor DS6051b (inhibitor of the tyrosine kinases ROS1 and NTRKs)
88 Overview of the side-effects of the combination therapy with vemurafenib and cobimetinib Squamous cell carcinoma Increased CK Alopecia Arthralgia QTc prolongation Hyperkeratosis BRAFinhibitor Nausea Diarrhoea Exanthema Sensitivity to light Fatigue Liver function test* MEKinhibitor Serous retinopathy Ejection fraction Ejection fraction *Liver function tests including AST and ALT. Includes chorioretinopathy and retinal detachment. CK, creatine kinase; QTc, corrected QT interval. Provided by Prof. Dummer. Gibney GT, et al. Nat Rev Clin Oncol. 2013;10: Grimaldi AM, et al. Curr Opin Oncol. 2014;26: Larkin J, et al. N Engl J Med. 2014;371: ; 2014;26: Larkin J, et al. Lancet Oncol.2014;15:
Stratégies thérapeutiques optimales en cas de positivité HER2, BRAF, ALK
 Stratégies thérapeutiques optimales en cas de positivité HER2, BRAF, ALK David Planchard (MD, PhD) Department of Cancer Medicine Thoracic Unit Gustave Roussy Villejuif (France) Disclosure Slide AstraZeneca,
Stratégies thérapeutiques optimales en cas de positivité HER2, BRAF, ALK David Planchard (MD, PhD) Department of Cancer Medicine Thoracic Unit Gustave Roussy Villejuif (France) Disclosure Slide AstraZeneca,
Targeted therapies for advanced non-small cell lung cancer. Tom Stinchcombe Duke Cancer Insitute
 Targeted therapies for advanced non-small cell lung cancer Tom Stinchcombe Duke Cancer Insitute Topics ALK rearranged NSCLC ROS1 rearranged NSCLC EGFR mutation: exon 19/exon 21 L858R and uncommon mutations
Targeted therapies for advanced non-small cell lung cancer Tom Stinchcombe Duke Cancer Insitute Topics ALK rearranged NSCLC ROS1 rearranged NSCLC EGFR mutation: exon 19/exon 21 L858R and uncommon mutations
The oncologist s point of view: the promise and challenges of increasing options for targeted therapies in NSCLC
 The oncologist s point of view: the promise and challenges of increasing options for targeted therapies in NSCLC Egbert F. Smit Department of Thoracic Oncology, Netherlands Cancer Institute, and Department
The oncologist s point of view: the promise and challenges of increasing options for targeted therapies in NSCLC Egbert F. Smit Department of Thoracic Oncology, Netherlands Cancer Institute, and Department
Beyond ALK and EGFR: Novel molecularly driven targeted therapies in NSCLC Federico Cappuzzo AUSL della Romagna, Ravenna, Italy
 Beyond ALK and EGFR: Novel molecularly driven targeted therapies in NSCLC Federico Cappuzzo AUSL della Romagna, Ravenna, Italy Oncogenic drivers in NSCLC Certain tumours arise as a result of aberrant activation
Beyond ALK and EGFR: Novel molecularly driven targeted therapies in NSCLC Federico Cappuzzo AUSL della Romagna, Ravenna, Italy Oncogenic drivers in NSCLC Certain tumours arise as a result of aberrant activation
Molecular Targets in Lung Cancer
 Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Other Driver Mutations: cmet, B-RAF, RET, NTRK
 Other Driver Mutations: cmet, B-RAF, RET, NTRK Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology and Medical Director, Memorial Cancer Institute Clinical Professor of Medicine Herbert Wertheim College
Other Driver Mutations: cmet, B-RAF, RET, NTRK Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology and Medical Director, Memorial Cancer Institute Clinical Professor of Medicine Herbert Wertheim College
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD. Mount Carrigain 2/4/17
 Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Drug Resistance in ALK- and ROS1-Rearranged Lung Cancers. Alice T. Shaw, MD PhD Director, Center for Thoracic Cancers September 16, 2017
 Drug Resistance in ALK- and ROS1-Rearranged Lung Cancers Alice T. Shaw, MD PhD Director, Center for Thoracic Cancers September 16, 2017 ALK and ROS1 are Related Tyrosine Kinases, and Both are Targeted
Drug Resistance in ALK- and ROS1-Rearranged Lung Cancers Alice T. Shaw, MD PhD Director, Center for Thoracic Cancers September 16, 2017 ALK and ROS1 are Related Tyrosine Kinases, and Both are Targeted
OTRAS DIANAS MOLECULARES TRATABLES. Rosario García Campelo Servicio de Oncología Médica Complejo Hospitalario Universitario A Coruña, CHUAC
 OTRAS DIANAS MOLECULARES TRATABLES Rosario García Campelo Servicio de Oncología Médica Complejo Hospitalario Universitario A Coruña, CHUAC A propósito de un caso. Mujer 34 años Fumadora ocasional < 10
OTRAS DIANAS MOLECULARES TRATABLES Rosario García Campelo Servicio de Oncología Médica Complejo Hospitalario Universitario A Coruña, CHUAC A propósito de un caso. Mujer 34 años Fumadora ocasional < 10
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
7/6/2015. Cancer Related Deaths: United States. Management of NSCLC TODAY. Emerging mutations as predictive biomarkers in lung cancer: Overview
 Emerging mutations as predictive biomarkers in lung cancer: Overview Kirtee Raparia, MD Assistant Professor of Pathology Cancer Related Deaths: United States Men Lung and bronchus 28% Prostate 10% Colon
Emerging mutations as predictive biomarkers in lung cancer: Overview Kirtee Raparia, MD Assistant Professor of Pathology Cancer Related Deaths: United States Men Lung and bronchus 28% Prostate 10% Colon
K-Ras signalling in NSCLC
 Targeting the Ras-Raf-Mek-Erk pathway Egbert F. Smit MD PhD Dept. Pulmonary Diseases Vrije Universiteit VU Medical Centre Amsterdam, The Netherlands K-Ras signalling in NSCLC Sun et al. Nature Rev. Cancer
Targeting the Ras-Raf-Mek-Erk pathway Egbert F. Smit MD PhD Dept. Pulmonary Diseases Vrije Universiteit VU Medical Centre Amsterdam, The Netherlands K-Ras signalling in NSCLC Sun et al. Nature Rev. Cancer
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer.
 Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Nouvelles stratégies Prise en charge en cas d altération oncogénique
 Nouvelles stratégies Prise en charge en cas d altération oncogénique David Planchard (MD, PhD) Department of Cancer Medicine Thoracic Unit Gustave Roussy Villejuif (France) Disclosure Slide Consultancy
Nouvelles stratégies Prise en charge en cas d altération oncogénique David Planchard (MD, PhD) Department of Cancer Medicine Thoracic Unit Gustave Roussy Villejuif (France) Disclosure Slide Consultancy
Corporate Medical Policy
 Corporate Medical Policy Molecular Analysis for Targeted Therapy for Non-Small Cell Lung File Name: Origination: Last CAP Review: Next CAP Review: Last Review: molecular_analysis_for_targeted_therapy_for_non_small_cell_lung_cancer
Corporate Medical Policy Molecular Analysis for Targeted Therapy for Non-Small Cell Lung File Name: Origination: Last CAP Review: Next CAP Review: Last Review: molecular_analysis_for_targeted_therapy_for_non_small_cell_lung_cancer
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Disclosures Genomic testing in lung cancer
 Disclosures Genomic testing in lung cancer No disclosures Objectives Understand how FISH and NGS provide complementary data for the evaluation of lung cancer Recognize the challenges of performing testing
Disclosures Genomic testing in lung cancer No disclosures Objectives Understand how FISH and NGS provide complementary data for the evaluation of lung cancer Recognize the challenges of performing testing
Beyond ALK and EGFR: Novel Molecularly Driven Targeted Therapies in NSCLC
 Beyond ALK and EGFR: Novel Molecularly Driven Targeted Therapies in NSCLC Simon Ekman, MD, PhD Senior Consultant in Oncology, Associate Professor Dept. of Oncology Karolinska University Hospital Stockholm,
Beyond ALK and EGFR: Novel Molecularly Driven Targeted Therapies in NSCLC Simon Ekman, MD, PhD Senior Consultant in Oncology, Associate Professor Dept. of Oncology Karolinska University Hospital Stockholm,
OTRAS TERAPIAS BIOLÓGICAS EN CPNM: Selección y Secuencia Óptima del Tratamiento
 OTRAS TERAPIAS BIOLÓGICAS EN CPNM: Selección y Secuencia Óptima del Tratamiento Dolores Isla Servicio de Oncología Médica HCU Lozano Besa de Zaragoza 2008 Selection Factors in Advanced NSCLC ( 8y ago)
OTRAS TERAPIAS BIOLÓGICAS EN CPNM: Selección y Secuencia Óptima del Tratamiento Dolores Isla Servicio de Oncología Médica HCU Lozano Besa de Zaragoza 2008 Selection Factors in Advanced NSCLC ( 8y ago)
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement. Reference Slides Introduction
 Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
Targeted therapy in NSCLC: do we progress? Prof. Dr. V. Surmont. Masterclass 27 september 2018
 Targeted therapy in NSCLC: do we progress? Prof. Dr. V. Surmont Masterclass 27 september 2018 Outline Introduction EGFR TKI ALK TKI TKI for uncommon driver mutations Take home messages The promise of
Targeted therapy in NSCLC: do we progress? Prof. Dr. V. Surmont Masterclass 27 september 2018 Outline Introduction EGFR TKI ALK TKI TKI for uncommon driver mutations Take home messages The promise of
MET as a novel treatment target- the story of the sleeping beauty. Balazs Halmos M.D. Montefiore Medical Center/Albert Einstein College of Medicine
 MET as a novel treatment target- the story of the sleeping beauty Balazs Halmos M.D. Montefiore Medical Center/Albert Einstein College of Medicine MET as a novel treatment target MET as an oncogene MET
MET as a novel treatment target- the story of the sleeping beauty Balazs Halmos M.D. Montefiore Medical Center/Albert Einstein College of Medicine MET as a novel treatment target MET as an oncogene MET
Improving outcomes for NSCLC patients with brain metastases
 Improving outcomes for NSCLC patients with brain metastases Martin Schuler West German Cancer Center, Essen, Germany In Switzerland, afatinib is approved as monotherapy for patients with non-small cell
Improving outcomes for NSCLC patients with brain metastases Martin Schuler West German Cancer Center, Essen, Germany In Switzerland, afatinib is approved as monotherapy for patients with non-small cell
Joachim Aerts Erasmus MC Rotterdam, Netherlands. Drawing the map: molecular characterization of NSCLC
 Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Inhibidores de EGFR Noemi Reguart, MD, PhD Hospital Clínic Barcelona IDIPAPS
 Inhibidores de EGFR Noemi Reguart, MD, PhD Hospital Clínic Barcelona IDIPAPS Driver Mutations to Classify Lung Cancer Unknown 36% KRAS 25% EGFR 15% ALK 4% HER2 2% Double Mut 2% BRAF 2% PIK3CA
Inhibidores de EGFR Noemi Reguart, MD, PhD Hospital Clínic Barcelona IDIPAPS Driver Mutations to Classify Lung Cancer Unknown 36% KRAS 25% EGFR 15% ALK 4% HER2 2% Double Mut 2% BRAF 2% PIK3CA
Response and resistance to BRAF inhibitors in melanoma
 Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
RXDX-101 & RXDX-102. Justin Gainor, MD February 20 th, 2014
 RXDX-101 & RXDX-102 Justin Gainor, MD February 20 th, 2014 Background Chromosomal fusions are important oncogenic drivers in NSCLC - ALK Rearrangements (4-6%) - ROS1 Rearrangements (1-2%) - RET Rearrangements
RXDX-101 & RXDX-102 Justin Gainor, MD February 20 th, 2014 Background Chromosomal fusions are important oncogenic drivers in NSCLC - ALK Rearrangements (4-6%) - ROS1 Rearrangements (1-2%) - RET Rearrangements
Molecular Testing in Lung Cancer
 Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Expanding Therapeutic Options for Cancer Patients with Comprehensive Profiling Alexander Drilon MD
 Expanding Therapeutic Options for Cancer Patients with Comprehensive Profiling Alexander Drilon MD Clinical Director, Early Drug Development Service Memorial Sloan Kettering Cancer Center COI Disclosure
Expanding Therapeutic Options for Cancer Patients with Comprehensive Profiling Alexander Drilon MD Clinical Director, Early Drug Development Service Memorial Sloan Kettering Cancer Center COI Disclosure
D Ross Camidge, MD, PhD
 i n t e r v i e w D Ross Camidge, MD, PhD Dr Camidge is Director of the Thoracic Oncology Clinical Program and Associate Director for Clinical Research at the University of Colorado Cancer Center in Aurora,
i n t e r v i e w D Ross Camidge, MD, PhD Dr Camidge is Director of the Thoracic Oncology Clinical Program and Associate Director for Clinical Research at the University of Colorado Cancer Center in Aurora,
1.Basis of resistance 2.Mechanisms of resistance 3.How to overcome resistance. 13/10/2017 Sara Redaelli
 Dott.ssa Sara Redaelli 13/10/2017 1.Basis of resistance 2.Mechanisms of resistance 3.How to overcome resistance Tumor Heterogeneity: Oncogenic Drivers in NSCLC The Promise of Genotype-Directed Therapy
Dott.ssa Sara Redaelli 13/10/2017 1.Basis of resistance 2.Mechanisms of resistance 3.How to overcome resistance Tumor Heterogeneity: Oncogenic Drivers in NSCLC The Promise of Genotype-Directed Therapy
Targeted Therapy for NSCLC: EGFR and ALK Fadlo R. Khuri, MD
 EGFR and ALK Fadlo R. Khuri, MD President, American University of Beirut Professor of Medicine July 26, 2018 A great year end! Targeted Therapy for NSCLC: Evolving Landscape of Lung Adenocarcinoma NSCLC
EGFR and ALK Fadlo R. Khuri, MD President, American University of Beirut Professor of Medicine July 26, 2018 A great year end! Targeted Therapy for NSCLC: Evolving Landscape of Lung Adenocarcinoma NSCLC
Personalized Medicine: Lung Biopsy and Tumor
 Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Changing demographics of smoking and its effects during therapy
 Changing demographics of smoking and its effects during therapy Egbert F. Smit MD PhD. Dept. Pulmonary Diseases, Vrije Universiteit Medical Centre, Amsterdam, The Netherlands Smoking prevalence adults
Changing demographics of smoking and its effects during therapy Egbert F. Smit MD PhD. Dept. Pulmonary Diseases, Vrije Universiteit Medical Centre, Amsterdam, The Netherlands Smoking prevalence adults
Personalized Therapies for Lung Cancer. Questions & Answers
 Personalized Therapies for Lung Cancer Questions & Answers What are Personalized Therapies for lung cancer? Like people, no two lung cancer tumors are the same. Personalized medicine (also known as precision
Personalized Therapies for Lung Cancer Questions & Answers What are Personalized Therapies for lung cancer? Like people, no two lung cancer tumors are the same. Personalized medicine (also known as precision
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Personalized Genetics
 Personalized Genetics Understanding Your Genetic Test Results Tracey Evans, MD September 29, 2017 Genetics 101 Punnett Square Genetic Pedigree 2 Genetics 101 Punnett Square Genetic Pedigree 3 It s not
Personalized Genetics Understanding Your Genetic Test Results Tracey Evans, MD September 29, 2017 Genetics 101 Punnett Square Genetic Pedigree 2 Genetics 101 Punnett Square Genetic Pedigree 3 It s not
NSCLC 2 nd and further line therapies. Egbert F. Smit MD PhD. Dept. Thoracic Oncology, Netherlands Cancer Institute
 NSCLC 2 nd and further line therapies Egbert F. Smit MD PhD. Dept. Thoracic Oncology, Netherlands Cancer Institute e.smit@nki.nl ESMO Guidelines 2016: Treatment of Stage IV nonsquamous NSCLC at progression
NSCLC 2 nd and further line therapies Egbert F. Smit MD PhD. Dept. Thoracic Oncology, Netherlands Cancer Institute e.smit@nki.nl ESMO Guidelines 2016: Treatment of Stage IV nonsquamous NSCLC at progression
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
I. Diagnosis of the cancer type in CUP
 Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
NSCLC: Terapia medica nella fase avanzata. Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza
 NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
2 nd line Therapy and Beyond NSCLC. Alan Sandler, M.D. Oregon Health & Science University
 2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
ALK positive Lung Cancer. Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan
 ALK positive Lung Cancer Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan Objectives What is ALK translocation? What drugs are used in what sequence? How many times
ALK positive Lung Cancer Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan Objectives What is ALK translocation? What drugs are used in what sequence? How many times
Efficacy of larotrectinib in adolescents and young adults with TRK fusion cancer
 Efficacy of larotrectinib in adolescents and young adults with TRK fusion cancer Soledad Gallego, 1 Valentina Boni, 2 Ulrik Lassen, 3 Anna Farago, 4 Wafik El-Deiry, 5 David Hong, 6 Blanca López-Ibor, 2
Efficacy of larotrectinib in adolescents and young adults with TRK fusion cancer Soledad Gallego, 1 Valentina Boni, 2 Ulrik Lassen, 3 Anna Farago, 4 Wafik El-Deiry, 5 David Hong, 6 Blanca López-Ibor, 2
Non-Small Cell Lung Cancer:
 Non-Small Cell Lung Cancer: Where We Are Today Sila Shalhoub, PharmD PGY2 Oncology Pharmacy Resident Shalhoub.Sila@mayo.edu Pharmacy Grand Rounds September 26, 2017 2017 MFMER slide-1 Objectives Identify
Non-Small Cell Lung Cancer: Where We Are Today Sila Shalhoub, PharmD PGY2 Oncology Pharmacy Resident Shalhoub.Sila@mayo.edu Pharmacy Grand Rounds September 26, 2017 2017 MFMER slide-1 Objectives Identify
ALK Inhibition: From Biology to Approved Therapy for Advanced Non-Small Cell Lung Cancer
 ALK Inhibition: From Biology to Approved Therapy for Advanced Non-Small Cell Lung Cancer Dr. Ben Solomon Medical Oncologist, Thoracic Oncology Peter MacCallum Cancer Centre Melbourne, Australia Dr. D.
ALK Inhibition: From Biology to Approved Therapy for Advanced Non-Small Cell Lung Cancer Dr. Ben Solomon Medical Oncologist, Thoracic Oncology Peter MacCallum Cancer Centre Melbourne, Australia Dr. D.
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016
 Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC
 1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD
 State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD Professor and Chair Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Nothing to disclose DISCLOSURE Objectives Lung
State of the Art Treatment of Lung Cancer Ravi Salgia, MD, PhD Professor and Chair Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Nothing to disclose DISCLOSURE Objectives Lung
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
14,30 18,20. II Sessione. Moderatori: Giovanni Apolone, Roberto Labianca
 14,30 18,20 II Sessione Moderatori: Giovanni Apolone, Roberto Labianca 15,10 15,30 Ca polmonare (never smokers): attualità e prospettive di ricerca Giulio Metro Ca polmonare (never smokers): attualità
14,30 18,20 II Sessione Moderatori: Giovanni Apolone, Roberto Labianca 15,10 15,30 Ca polmonare (never smokers): attualità e prospettive di ricerca Giulio Metro Ca polmonare (never smokers): attualità
Personalized Treatment Approaches for Lung Cancer
 Personalized Treatment Approaches for Lung Cancer California Thoracic Society 2018 Annual Carmel Conference January 27, 2018 Matthew Gubens, MD, MS Associate Professor of Medicine Chair, Thoracic Oncology
Personalized Treatment Approaches for Lung Cancer California Thoracic Society 2018 Annual Carmel Conference January 27, 2018 Matthew Gubens, MD, MS Associate Professor of Medicine Chair, Thoracic Oncology
DM Seminar. ALK gene rearrangements & ALK targeted therapy in NSCLC Dr Sarat
 DM Seminar ALK gene rearrangements & ALK targeted therapy in NSCLC Dr Sarat Introduction Discovery of activating mutations in kinase domain of epidermal growth factor receptor (EGFR) opened a new era of
DM Seminar ALK gene rearrangements & ALK targeted therapy in NSCLC Dr Sarat Introduction Discovery of activating mutations in kinase domain of epidermal growth factor receptor (EGFR) opened a new era of
Clinical response to entrectinib in a patient with NTRK1-rearranged non-small cell lung cancer (NSCLC)
") Clinical response to entrectinib in a patient with NTRK1-rearranged non-small cell lung cancer (NSCLC) Anna F. Farago, Manish Patel, Todd M. Bauer, Stephen V. Liu, Alexander Drilon, Jennifer Wheler, Sai-Hong
Clinical response to entrectinib in a patient with NTRK1-rearranged non-small cell lung cancer (NSCLC) Anna F. Farago, Manish Patel, Todd M. Bauer, Stephen V. Liu, Alexander Drilon, Jennifer Wheler, Sai-Hong
ASCO Highlights and Controversies in advanced Lung Cancer. Torino, 11 giugno 2015
 ASCO 2015 Highlights and Controversies in advanced Lung Cancer Torino, 11 giugno 2015 Paolo Bironzo AOU S Luigi Gonzaga - Orbassano Scuola di Specializzazione in Oncologia Medica Università di Torino What
ASCO 2015 Highlights and Controversies in advanced Lung Cancer Torino, 11 giugno 2015 Paolo Bironzo AOU S Luigi Gonzaga - Orbassano Scuola di Specializzazione in Oncologia Medica Università di Torino What
CURRENT STANDARD OF CARE OF LUNG CANCER. Maroun El-Khoury, MD Consultant Oncologist/Hematologist American Hospital Dubai President of Medical staff
 CURRENT STANDARD OF CARE OF LUNG CANCER Maroun El-Khoury, MD Consultant Oncologist/Hematologist American Hospital Dubai President of Medical staff Biopsy: Establish Diagnosis, Determine Histologic Subtype,
CURRENT STANDARD OF CARE OF LUNG CANCER Maroun El-Khoury, MD Consultant Oncologist/Hematologist American Hospital Dubai President of Medical staff Biopsy: Establish Diagnosis, Determine Histologic Subtype,
Personalised Healthcare (PHC) with Foundation Medicine (FMI) Fatma Elçin KINIKLI, FMI Turkey, Science Leader
 with Foundation Medicine (FMI) Fatma Elçin KINIKLI, FMI Turkey, Science Leader") Personalised Healthcare (PHC) with Foundation Medicine (FMI) Fatma Elçin KINIKLI, FMI Turkey, Science Leader Agenda PHC Approach Provides Better Patient Outcome FMI offers Comprehensive Genomic Profiling,
Personalised Healthcare (PHC) with Foundation Medicine (FMI) Fatma Elçin KINIKLI, FMI Turkey, Science Leader Agenda PHC Approach Provides Better Patient Outcome FMI offers Comprehensive Genomic Profiling,
Opzioni terapeutiche nel paziente ALK-traslocato
 Opzioni terapeutiche nel paziente ALK-traslocato Giulio Metro S.C. Oncologia Medica Ospedale Santa Maria della Misericordia, Azienda Ospedaliera di Perugia Carcinoma del polmone non microcitoma: quali
Opzioni terapeutiche nel paziente ALK-traslocato Giulio Metro S.C. Oncologia Medica Ospedale Santa Maria della Misericordia, Azienda Ospedaliera di Perugia Carcinoma del polmone non microcitoma: quali
MET skipping mutation, EGFR
 New NSCLC biomarkers in clinical research: detection of MET skipping mutation, EGFR T790M, and other important biomarkers Fernando López-Ríos Laboratorio de Dianas Terapéuticas Hospital Universitario HM
New NSCLC biomarkers in clinical research: detection of MET skipping mutation, EGFR T790M, and other important biomarkers Fernando López-Ríos Laboratorio de Dianas Terapéuticas Hospital Universitario HM
Targeted therapy beyond EGFR/ALK Focus on ROS1, RET, NTRK, BRAF, MET. Byoung Chul Cho, M.D., Ph.D.
 Targeted therapy beyond EGFR/ALK Focus on ROS1, RET, NTRK, BRAF, MET Byoung Chul Cho, M.D., Ph.D. DISCLOSURE Research funding: Novartis, Bayer, AstraZeneca, MOGAM Institute, Dong-A ST, Champions Oncology,
Targeted therapy beyond EGFR/ALK Focus on ROS1, RET, NTRK, BRAF, MET Byoung Chul Cho, M.D., Ph.D. DISCLOSURE Research funding: Novartis, Bayer, AstraZeneca, MOGAM Institute, Dong-A ST, Champions Oncology,
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC. Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy
 PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care
 Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
EGFR Mutation-Positive Acquired Resistance: Dominance of T790M
 Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Individualized therapy in lung cancer Where are we in 2012?
 UNIVERSITY OF OF TORINO DEPARTMENT OF ONCOLOGY Individualized therapy in lung cancer Where are we in 2012? Giorgio V. Scagliotti University of Torino Professor of Medical Oncology Department of Oncology
UNIVERSITY OF OF TORINO DEPARTMENT OF ONCOLOGY Individualized therapy in lung cancer Where are we in 2012? Giorgio V. Scagliotti University of Torino Professor of Medical Oncology Department of Oncology
Targeted Therapies for Advanced NSCLC
 Targeted Therapies for Advanced NSCLC Current Clinical Developments Friday, June 3, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016 ASCO Annual Meeting
Targeted Therapies for Advanced NSCLC Current Clinical Developments Friday, June 3, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016 ASCO Annual Meeting
Supplementary Online Content
 Supplementary Online Content Kris MG, Johnson BE, Berry LD, et al. Using Multiplexed Assays of Oncogenic Drivers in Lung Cancers to Select Targeted Drugs. JAMA. doi:10.1001/jama.2014.3741 etable 1. Trials
Supplementary Online Content Kris MG, Johnson BE, Berry LD, et al. Using Multiplexed Assays of Oncogenic Drivers in Lung Cancers to Select Targeted Drugs. JAMA. doi:10.1001/jama.2014.3741 etable 1. Trials
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Disclosure of Relevant Financial Relationships NON-SMALL CELL LUNG CANCER: 70% PRESENT IN ADVANCED STAGE
 MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
Slide 1. Slide 2 Maintenance Therapy Options. Slide 3. Maintenance Therapy in the Management of Non-Small Cell Lung Cancer. Maintenance Chemotherapy
 Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
Quale sequenza terapeutica nella malattia EGFR+
 Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with
Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with
Targeting Acquired Resistance to EGFR Kinase Inhibitors: Beyond T790M Mutation
 Targeting Acquired Resistance to EGFR Kinase Inhibitors: Beyond T790M Mutation James Chih-Hsin Yang, MD, PhD National Taiwan University Hospital National Taiwan University Cancer Center Taipei, Taiwan
Targeting Acquired Resistance to EGFR Kinase Inhibitors: Beyond T790M Mutation James Chih-Hsin Yang, MD, PhD National Taiwan University Hospital National Taiwan University Cancer Center Taipei, Taiwan
BRAF Inhibitors in Metastatic disease. Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia
 Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
MANEJO ACTUAL DEL PACIENTE CON CPNM CON REORDENACIONES ALK/ROS O MUTACIONES EN EGFR Rosario García Campelo Complejo Hospitalario Universitario A
 MANEJO ACTUAL DEL PACIENTE CON CPNM CON REORDENACIONES ALK/ROS O MUTACIONES EN EGFR Rosario García Campelo Complejo Hospitalario Universitario A Coruña The seventies IMAGINE The eighties The Ninety 2000
MANEJO ACTUAL DEL PACIENTE CON CPNM CON REORDENACIONES ALK/ROS O MUTACIONES EN EGFR Rosario García Campelo Complejo Hospitalario Universitario A Coruña The seventies IMAGINE The eighties The Ninety 2000
Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC)
") Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC) Suresh S. Ramalingam, MD Director of Thoracic Oncology Associate Professor Emory University Atlanta,
Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC) Suresh S. Ramalingam, MD Director of Thoracic Oncology Associate Professor Emory University Atlanta,
Lung Cancer Update 2016 BAONS Oncology Care Update
 Lung Cancer Update 2016 BAONS Oncology Care Update Matthew Gubens, MD, MS Assistant Professor Chair, Thoracic Oncology Site Committee UCSF Helen Diller Family Comprehensive Cancer Center Disclosures Consulting
Lung Cancer Update 2016 BAONS Oncology Care Update Matthew Gubens, MD, MS Assistant Professor Chair, Thoracic Oncology Site Committee UCSF Helen Diller Family Comprehensive Cancer Center Disclosures Consulting
Integration of Genomics Into Clinical Pathways. Precision Medicine and Decision Support
 Integration of Genomics Into Clinical Pathways Precision Medicine and Decision Support Faculty Andrew Hertler, MD, FACP Chief Medical Officer New Century Health Andrew Hertler, MD, FACP is employed by
Integration of Genomics Into Clinical Pathways Precision Medicine and Decision Support Faculty Andrew Hertler, MD, FACP Chief Medical Officer New Century Health Andrew Hertler, MD, FACP is employed by
Treatment of ALK Positive Advanced NSCLC Fiona Blackhall PhD FRCP Medical Oncologist Manchester, UK
 Treatment of ALK Positive Advanced NSCLC Fiona Blackhall PhD FRCP Medical Oncologist Manchester, UK ESMO The Christie Preceptorship in Lung Cancer March 2017 2017 : Similar incidence in women & men ADC
Treatment of ALK Positive Advanced NSCLC Fiona Blackhall PhD FRCP Medical Oncologist Manchester, UK ESMO The Christie Preceptorship in Lung Cancer March 2017 2017 : Similar incidence in women & men ADC
Targeted Cancer Therapies
 Targeted Cancer Therapies Primary Care Training Programme 14 th February 2018 Sin Chong Lau Consultant in Medical Oncology Financial Disclosure Honoraria: Amgen, Pfizer, Roche, Sanofi, Servier Meetings:
Targeted Cancer Therapies Primary Care Training Programme 14 th February 2018 Sin Chong Lau Consultant in Medical Oncology Financial Disclosure Honoraria: Amgen, Pfizer, Roche, Sanofi, Servier Meetings:
Osimertinib Activity in Patients With Leptomeningeal Disease From Non-Small Cell Lung Cancer: Updated Results From the BLOOM Study
 Osimertinib Activity in Patients With Leptomeningeal Disease From Non-Small Cell Lung Cancer: Updated Results From the BLOOM Study Abstract 9002 Yang JC, Kim DW, Kim SW, Cho BC, Lee JS, Ye X, Yin X, Yang
Osimertinib Activity in Patients With Leptomeningeal Disease From Non-Small Cell Lung Cancer: Updated Results From the BLOOM Study Abstract 9002 Yang JC, Kim DW, Kim SW, Cho BC, Lee JS, Ye X, Yin X, Yang
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making
 Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making November 20, 2014 Capturing Value in Next Generation Sequencing Symposium Douglas Johnson MD, MSCI Vanderbilt-Ingram
Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making November 20, 2014 Capturing Value in Next Generation Sequencing Symposium Douglas Johnson MD, MSCI Vanderbilt-Ingram
Leading the Way to Precision Care: Molecular Diagnostics and Therapeutics in Lung Cancers. Mark G Kris, MD Memorial Sloan Kettering New Amsterdam USA
 Leading the Way to Precision Care: Molecular Diagnostics and Therapeutics in Lung Cancers Mark G Kris, MD Memorial Sloan Kettering New Amsterdam USA Molecular Therapeutics in Lung Cancers Financial Disclosures
Leading the Way to Precision Care: Molecular Diagnostics and Therapeutics in Lung Cancers Mark G Kris, MD Memorial Sloan Kettering New Amsterdam USA Molecular Therapeutics in Lung Cancers Financial Disclosures
Sequencing in EGFR-Mutated NSCLC: Does Order Matter?
 Sequencing in EGFR-Mutated NSCLC: Does Order Matter? Maximilian J. Hochmair, MD Otto Wagner Hospital Vienna, Austria Disclosures Honoraria: AstraZeneca, AbbVie, Pfizer, Boehringer Ingelheim, Roche, MSD,
Sequencing in EGFR-Mutated NSCLC: Does Order Matter? Maximilian J. Hochmair, MD Otto Wagner Hospital Vienna, Austria Disclosures Honoraria: AstraZeneca, AbbVie, Pfizer, Boehringer Ingelheim, Roche, MSD,
Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung
 Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung Noemi Reguart,MD, PhD Hospital Clinic de Barcelona Barcelona, Spain SC-CRP-02660 Conversations in Oncology 2018 is a standalone
Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung Noemi Reguart,MD, PhD Hospital Clinic de Barcelona Barcelona, Spain SC-CRP-02660 Conversations in Oncology 2018 is a standalone
REPORT ASCO 2018 CHICAGO: RESPIRATORY ONCOLOGY Johan Vansteenkiste / Christophe Dooms, Univ. Hospital KU Leuven and Leuven Lung Cancer Group
 1 REPORT ASCO 2018 CHICAGO: RESPIRATORY ONCOLOGY Johan Vansteenkiste / Christophe Dooms, Univ. Hospital KU Leuven and Leuven Lung Cancer Group OUR 10 MESSAGE HIGHLIGHTS 1/ Advanced NSCLC 1 st line: IO
1 REPORT ASCO 2018 CHICAGO: RESPIRATORY ONCOLOGY Johan Vansteenkiste / Christophe Dooms, Univ. Hospital KU Leuven and Leuven Lung Cancer Group OUR 10 MESSAGE HIGHLIGHTS 1/ Advanced NSCLC 1 st line: IO
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007
 Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
Carcinoma de Tiroide: Teràpies Diana
 Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Dr. Andres Wiernik. Lung Cancer
 Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Thoracic and head/neck oncology new developments
 Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
Clinical Updates and Issues: Advanced Non-Small Cell Lung Cancer
 Clinical Updates and Issues: Advanced Non-Small Cell Lung Cancer Tracy Ruegg, MSN, ARNP, AOCN Miami Cancer Institute formerly of The Ohio State University Comprehensive Cancer Center James Cancer Hospital
Clinical Updates and Issues: Advanced Non-Small Cell Lung Cancer Tracy Ruegg, MSN, ARNP, AOCN Miami Cancer Institute formerly of The Ohio State University Comprehensive Cancer Center James Cancer Hospital
Discovery of Essential Growth Drivers in Cancer Brings Magical Drugs to Patients
 Discovery of Essential Growth Drivers in Cancer Brings Magical Drugs to Patients Hiroyuki Mano, MD, PhD Department of Cellular Signaling, Graduate School of Medicine, The University of Tokyo, Japan What
Discovery of Essential Growth Drivers in Cancer Brings Magical Drugs to Patients Hiroyuki Mano, MD, PhD Department of Cellular Signaling, Graduate School of Medicine, The University of Tokyo, Japan What
Tissue or Liquid Biopsy? ~For Diagnosis, Monitoring and Early detection of Resistance~
 16 th Dec. 2016. ESMO Preceptorship Program Non-Small-Cell Lung Cancer @Singapore Tissue or Liquid Biopsy? ~For Diagnosis, Monitoring and Early detection of Resistance~ Research Institute for Disease of
16 th Dec. 2016. ESMO Preceptorship Program Non-Small-Cell Lung Cancer @Singapore Tissue or Liquid Biopsy? ~For Diagnosis, Monitoring and Early detection of Resistance~ Research Institute for Disease of