Selective Internal Radiation Therapy (SIRT) A Novel Treatment for Inoperable Liver Tumours.
|
|
|
- Loraine Nelson
- 5 years ago
- Views:
Transcription

1 Selective Internal Radiation Therapy (SIRT) A Novel Treatment for Inoperable Liver Tumours. A/Prof Lourens Bester Interventional Radiologist University of New South Wales Sydney
2 Concept & Rationale. Objectives: Patient selection criteria. Overview of some clinical studies. Cases. On-going clinical studies. Integration of SIRT into the treatment paradigms for m-crc, mbreast, mnet & HCC.


3 Rationale behind SIRT Dual supply to the liver with the metastatic lesions supplied by the arterial system.. Most tumours and the Liver is sensitive to radiation. Parasitic effect of the tumour to protects the normal liver. The inflow of oxygenated blood is important as cancer cells are damaged by free radical formation from oxygen and therefore the embolic effect of SIRT should be less than with TACE and definitely less than with DEB. Gray et al, Annals of Oncology 2001


4 SIRT Approved as a therapeutic option by the FDA since 2002 SIR-Spheres = Yttrium 90 permanently bound to a Resin microsphere µm diameter Pure beta emission Half life 2.68 days Penetration 2-11 mm max. J Vasc Interv Radiol 2012; 23:
5 Liver Tolerance & Tumour Sensitivity to Radiation Gy SIRT Gy: Rectal Ca Kennedy A, Coldwell D, Nutting C et al. Pathology and microdosimetry in human livers after 90 Y-microspheres. Int J Rad Oncol Biol Phys 2004; 60(5):
6 Who gets SIRT? Primary Liver tumours: HCC / Cholangiocarcinoma as 1 st line or 2 nd line treatment or as combination therapy. Inoperable colorectal liver metastases in conjunction with chemotherapy or in the chemotherapy refractory setting as salvage therapy Secondary liver tumour from anywhere salvage therapy Metastatic Neuroendocrine tumours to the liver and liver dominant disease as 1 st line or 2 nd line treatment. Metastatic Breast Cancer that have progressed on polychemotherapy. Quality of life issues e.g. older patients / frail patients / patients with intolerable side-effects to the chemotherapy. Harring et.al. Int. J Hepatology 2011; epub. Khan et.al. Endocrine Rel Cancer 2011;18:53-73 Kennedy et al Am J Clin Oncol 2011
7 Who does not get SIRT? Limited hepatic reserve with clinical and pathological evidence of liver failure Pre-treatment Tc 99m -MAA lung shunt study demonstrating potential for >30Gy exposure to the lungs Pre-treatment hepatic angiogram demonstrating potential for deposition of microspheres in the GI tract or other organs that cannot be corrected by angiographic embolisation. Poor prognosticators Tumour volume 50-70% P= Tumour presentation (Infiltrative vs. Focal) P= AST & ALT > 5 x normal p= 0.03 Bilirubin > 35 µmol/l P= ECOG > 0 P= Albumin below 30 g/l + >50% infiltration of the liver by tumour p=0.01 Sangro et.al Hepatology 2011;57: Kennedy et.al.int J Radiation Onc Biol Phys 2007; 68:1:13-23 Ibrahim et al W J Gastro 2008;21: Kennedy et al. Int.Cong.on Anti-Cancer Therapy (ICACT) 2008 Abs Salem et al. J Vasc Interv Radiol 2006; 17:
8 Published data on liver tumours treated with SIR-Spheres Adenosquamous tongue Adrenal Breast Cancer of unknown primary Cervical Cholangiocarcinoma Colorectal Desmoplastic Small Round Cell Endometrial Gastric Gall bladder GI sarcoma GIST Hepatocellular carcinoma Hepatic angiosarcoma Lung Malignant melanoma Mouth Neuroendocrine tumour Ocular melanoma (uveal, choroidal etc) Oesophagus Ovarian Pancreatic Pharangeal Prostate Renal Sarcoma Squamous cell Thymus Thyroid Jiao. Eur J Surg Oncol 2007;33: Gulec. J Transl Med 2007;5:15. Jakobs. Eur Radiol 2007;17: Wong. JVIR 2005;16: Lim Int Med J 2005;35: Stuart. JVIR 2008;19: Bilbao. CIRSE 2007;Abs Gulec. World J Surg Oncol 2009;7:6.ePub. Gulec. AHPBA 2007;Abs 62. Cianni. La Radiologia Medica 2010;115: B oán. EANM 2005;Abs 295. Bailey. Australasian Radiol 2004; 48(2):A4. Yu. SIR 2006;Abs 17. Jakobs. WCIO 2006; Session L1. Whitney. J Surg Res 2009; epub. Subbiah. J Clin Oncol 2011; epub.
9 Overview of clinical studies.

10 Advances in Therapeutic Options for CRC Best Supportive care ~4-6 mo 5FU/LV/Capecitabine ~10-12 mo Oxaliplatin / Irinotecan + 5FU /LV/ Capecitabine ~15 mo ~20 mo 2 active drugs + biologicals 20.3 mo 2/3 active drugs + biologicals >24-26 mo 2/3 active drugs + biologicals SIRT SIRT mo Median Survival (months) 30
11 SIR-Spheres in 1 st -line Treatment of Colorectal Cancer Liver Metastases Investigator n Treatment ORR TTP/ PFS Survival Gray 74 SIR-Spheres + FUDR 44% 15.9 mo 39% at 2 yr FUDR 18% 9.7 mo 29% at 2 yr van Hazel 21 SIR-Spheres + 5FU/LV 91% 18.6 mo 29.4 mo 5FU/LV 0% 3.6 mo 12.8 mo P< Sharma 20 SIR-Spheres + FOLFOX4 90% 14.2 mo nr HR 0.33; P=0.025 Kosmider 19 SIR-Spheres +/- 84% 29.4 mo FOLFOX mo 37.8 mo Tie 31 SIR-Spheres + 91% 13.2 mo 30.7 mo FOLFOX4 phase II/III studies FOLFOX4 P=0.01 P=0.001 P=0.06 P< % mo m Gray et al. Ann Oncol 2001;12: van Hazel et al. J Surg Oncol 2004;88: Sharma et al. J Clin Oncol 2007;25: Kosmider et al. J Vasc Interv Radiol 2011; epub. Tie et al. ESMO, Ann Oncol 2010;21(Suppl 8): Abs Madajewicz et al. ASCO GI 2005; Abs 220. De Gramont et al. ASCO 2004; Abs Kalofonos et al. Ann Oncol 2005;16:






12 SIR-Spheres + FOLFOX4 in mcrc: CT Response Baseline CT scan pre-sirt CT scan 6 months post-sirt Sharma RA et al. Annals of Oncology 2006.
13 SIR-Spheres microspheres in 2 nd -line Chemotherapy m-crc. Investigator n Treatment ORR TTP/ PFS Survival van Hazel 25 SIR-Spheres + irinotecan 48% 6.0 mo 12.2 mo 9.2 mo Cove-Smith 33 SIR-Spheres + FOLFIRI 38% 9.5 mo 17.0 Kennedy 206 SIR-Spheres + 2 nd line nr nr 13.0 mo P<0.001 vs. >3 rd -line phase II/III studies 2 nd -line irinotecan 4 13% mo mo irinotecan + cetuximab 16 27% mo mo 3 rd -line panitumumab 9 14% mo mo Lim et al. BMC Cancer 2005;5:132. van Hazel et al. J Clin Oncol 2009;27: Cove-Smith, Wilson. WCGIC 2011; Abs P Reid et al. Eur J Cancer Suppl 2012;10(3): Kennedy et al. ASCO GI 2013; Abs Schoemaker et al. Brit J Cancer 2004;91: Van Cutsem et al. Brit J Cancer 2005;92: Seymour et al. Lancet 2007;370: Fuchs et al. JCO 2007;21: Sobrero et al. J Clin Oncol 2008;26: de Cerqueira Mathias et al. ECCO 2007;5: Abs P3055. Wilke et al. ECCO 2007;5: Abs P3025. Cunningham et al. N Engl J Med 2004;351: Hecht et al. Cancer 2007;110: Van Cutsem et al. J Clin Oncol 2007;25: Van Cutsem et al. Ann Oncol 2008;19:92 8. Muro et al. Jpn J Clin Oncol 2009;39:321 6.
14 SIR-Spheres + FOLFIRI in mcrc CT Response. Baseline CT scan pre-sirt CT scan 6 months post-sirt
15 SIRT in Chemorefractory CRC Liver Metastases Investigator n Treatment ORR SD TTP/ PFS Survival Prospective or Comparative studies: Hendlisz 44 Resin-Spheres + 5FU 10% 76% 5.0 mo 10.0 mo 5FU > salvage with 0% 35% 2.1 mo 7.3 mo P=0.001 HR 0.38 Resin-Spheres at PD /0.51; P=0.003 /0.03 ns Seidensticker 29 Resin-Spheres 41% 17% 5.5 mo 8.3 mo 29 supportive care (BSC) nr nr 2.1 mo 3.5 mo (matched-pairs) nr HR 0.26; P<0.001 Bester 224 Resin-Spheres nr nr nr 11.9 mo 29 conventional Tx/BSC nr nr nr 6.6 mo (comparative cohort) HR 0.50; P=0.001 Cosimelli 50 Resin-Spheres 24% 24% 4 mo 12.6 mo Hendlisz et al. J Clin Oncol 2010;28: Seidensticker et al. Cardiovasc Interv Radiol 2012; 35(5): Bester et al. J Vasc Interv Radiol 2011; epub. Cosimelli et al. Br J Cancer 2010;103:
16 SIRT in Chemorefractory CRC Liver Metastases Investigator n Treatment ORR SD TTP/PFS Survival Retrospective studies: Kennedy 606 Resin-Spheres nr nr nr 9.6 mo Sofocleous 18 Resin-Spheres 40% 5.1 mo 7.4 mo Coldwell 25 R-Spheres KRAS wild-type nr nr 9.0 mo not reached KRAS mutant nr nr 4.4 mo 7 mo Leoni 51 Resin-Spheres 53% nr 8 mo Jakobs 41 Resin-Spheres 17% 61% 5.9 mo 10.5 mo Cianni 41 Resin-Spheres 46% 36% 9.3 mo 11.8 mo Nace 51 Resin-Spheres 13% 64% nr 10.2 mo Cove-Smith 25/33 Resin-Spheres + chemo 20% 36% mo 13.2 mo Kennedy 208 Resin-Spheres 36% 55% responders 7.2 mo 10.5 mo non-responders/controls na na na 4.5 mo Kennedy et al. J Clin Oncol 2012; 30 (suppl): Abs Coldwell WCIO meeting 2012; Abs. 48. Sofocleous et al. J Vasc Interv Radiol 2012; 23 (Suppl): S70 Abs Leoni et al. ECR 2012; Abs. C Jakobs et al. J Vasc Intervent Radiol 2008; 19: Cianni et al. Cardio Interv Radiol 2009; 32: Nace et al. Int J Surg Oncol 2011; epub doi: /2011/ Cove-Smith Annals Oncol 2011; 22 (Suppl 5): v64 Abs. P Kennedy et al. Int J Radiat Oncol Biol Phys 2006; 65: P=0.0001
17 Belgium Multi-Center Study Hendlisz et al. J Clin Oncol 2010; 28: A phase II prospective randomised study comparing intraarterial injection of Yttrium-90 resin microspheres with continuous 5FU infusion versus continuous 5FU infusion alone. All patients have failed Oxaliplatin and Irinotecan based regimens. By design, patients in the control arm that received 5FU alone were able to receive Resin-Spheres as salvage therapy on disease progression, therefore overall survival was increased in both arms.
18 Conclusion The study met its primary end point by demonstrating that a single hepatic arterial injection of Yttrium 90 Resinmicrospheres added to a standard infusion of 5FU significantly extends the time to disease progression and median survival. Median survival in the SIRT arm was 10 months and in the 5FU arm who eventually also received SIRT was 7.3 months Hendlisz et al. J Clin Oncol 2010; 28:
19 German matched-pair analysis Seidensticker et al. Cardiovasc Interv Radiol 2012; 35(5): Matched-pair comparison of radioembolisation plus best supportive care versus best supportive care alone. Patients in this prospective phase II study had failed all chemotherapy options, and were matched with a contemporary pair by: 1. Tumour burden 2. Prior chemotherapy received 3. Synchronous vs. metachronous metastases 4. CEA >200 U/mL 5. Extrahepatic disease 6. Prior liver directed therapies.
20 Conclusion SIRT provides substantial clinical benefit as evidenced by a significant stabilisation in liver disease and prolonged survival of 8.3 months in patients with refractory mcrc for whom there are limited treatment options. Liver-directed treatment with Yttrium 90 Resinmicrospheres was the most significant independent predictor for prolonged PFS and overall survival on multivariate analysis Seidensticker et al. Cardiovasc Interv Radiol 2012; 35(5):
21 Australian retrospective comparative study. Bester et al. J Interv Radiol 2012; 23: Radioembolisation versus best supportive care in chemorefractory patients. Comparative retrospective study of survival outcomes and adverse events in chemorefractory patients.
22 Conclusion Radioembolisation is associated with an improved survival benefit. Whilst confounding factors may play a role, SIRT should be the treatment option of choice in the chemorefractory setting. The significant improvement in overall survival of 11.9 months in this study confirm the benefits demonstrated in two previous but smaller comparative studies by Hendlisz and Seidensticker. Bester et al. J Interv Radiol 2012; 23:
23 American Experience with Yttrium 90 in Chemorefractory Liver Metastases: Kennedy AS 90 Y microspheres for unresectable colorectal liver metastases: A multi-center study of 506 patients. ASCO Annual Meeting 2012, Journal of Clinical Oncology 2012; 30 (suppl): Abs. 358 Largest, most comprehensive study to date evaluating the use of Selective Internal Radiation Therapy (SIRT) in chemorefractory liver metastases from colorectal cancer. 606 patients (233 women; 373 men) at 10 institutions, who received a total of 966 SIRT treatments. All patients had failed 1 st -line, 93% had failed 2 line and 87% had failed 3 line of chemotherapy. 46% had previously received local-regional therapies (RFA, TACE etc.) The overall survival for these heavily pre-treated patients was 9.6 months from their first SIRT treatment.
24 Conclusion The U.S. experience confirms recently published data by Hendlisz, Seidensticker and Bester, who independently reported median overall survivals of 10.0, 8.3 and 11.9 months, respectively, in similar cohorts of patients with chemotherapy refractory disease. Kennedy AS 90 Y microspheres for unresectable colorectal liver metastases: A multi-center study of 506 patients. ASCO Annual Meeting 2012, Journal of Clinical Oncology 2012; 30 (suppl): Abs. 358

25 SIR-Spheres in Salvage Setting


26 Riad Salem Nortwestern Memorial Chicago

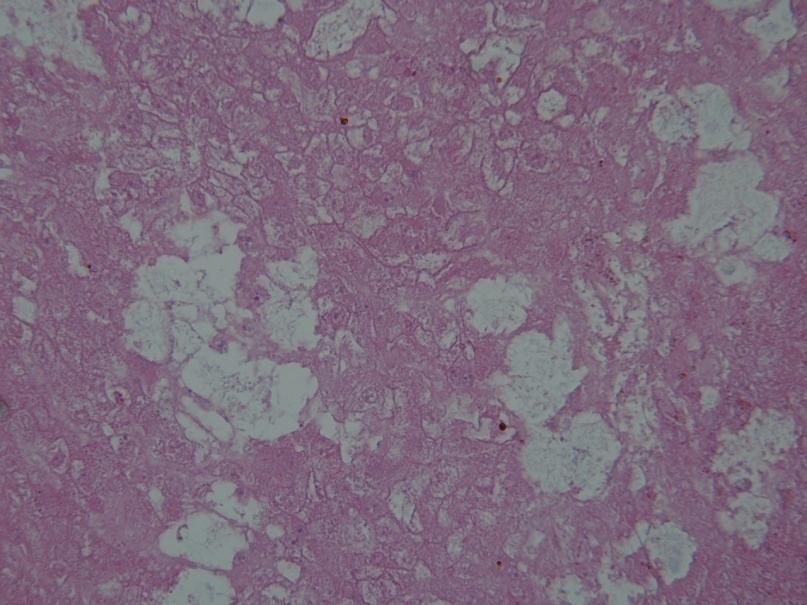
27 Sir-Spheres and Diffuse Parenchymal Changes Bester et. al. JMIRO 2011;55:

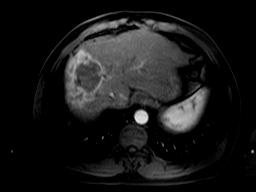
28 Capsular Retraction due to Hepatic Fibrosis and Portal Hypertension. Atassi et al, RadioGraphics 2008; 28: 81-99
29 Integrating SIRT into the mcrc treatment paradigm 10 20% Liver-only or liverpredominant mcrc Decrease RR > Radioembolisation > Radioembolisation <20% 1 st -line chemotherapy +/- Biologics 2 nd -line chemotherapy +/- Biologics VEGF n th -line chemotherapy +/- Biologics EGFR Chemorefractory? > Radioembolisation > Radioembolisation > Radioembolisation Clinical Trials / Regorafenib SIRT
30 Current ongoing SIRT studies: The goal is to investigate whether SIRT used in combination with chemotherapy can offer patient outcome advantages that are superior to chemotherapy alone. SIRFLOX = 1 st Line FOLFOX6 + SIRT vs. FOLFOX6 (Resin) with or without Bevacizumab. Open label multicentre RCT with PFS as the primary objective (518 Patients). FOXFIREGlobal / FOXFIRE = 1 st Line OxMdG + SIRT vs. OxMdG (Resin). RCT with overall survival as the primary objective (463 Patients). FOXFIRE bolt on to SIRFLOX powered for overall survival (981 P). EPOCH = Following failed 1 st line chemotherapy (Glass). RCT 2 nd line chemotherapy + SIRT vs. 2 nd line chemotherapy with PFS as the primary objective (360 Patients).
31 HCC
32 SIR-Spheres microspheres in Hepatocellular Carcinoma: European studies Investigator n Treatment ORR SD TTP/PFS Survival 1 st -line, advanced disease D Avola 35 SIR-Spheres nr nr nr 16 months 43 standard care nr nr nr 8 months P < st - or >2 nd -line Sangro 325 SIR-Spheres nr nr nr 12.8 months 52 in BCLC A (unresectable, non-ablatable) 24.4 months 87 in BCLC B 16.9 months 183 in BCLC C 10.0 months P < in Child A 14.9 months 57 in Child B 10.3 months P = Iñarrairaegui 72 SIR-Spheres 14% 80% nr 13 months statistically significant data D Avola et al. Hepato-Gastroenterology 2009;56: Sangro et al. Hepatology 2011;54: Iñarrairaegui et al. Int J Radiat Oncol Biol Phys 2010;77: Iñarrairaegui et al. Eur J Surg Oncol 2012; epub.
 not reached n = 52 n = 32 n = 39 n = 55 n = 48 n")

33 Clinical Outcomes of HCC Patients Treated with SIR-Spheres. Median Survival (months) not reached n = 52 n = 32 n = 39 n = 55 n = 48 n = 31 n = 183 n = 73 (unresectable) Candidates for TACE Poor Candidates Failed Contraindicated for TACE TACE/TAE for TACE Sangro et al. Hepatology 2011;54:868-78
34 SIR-Spheres microspheres in Hepatocellular Carcinoma: European Multi-Centre Analysis Investigator n Treatment Survival 1 st - or 2 nd -line, intermediate & advanced disease Sangro 199 in 1 5 nodule 16.8 months 125 in >5 nodules 10.0 months P < in no extra-hepatic disease 14.1 months 30 in extra-hepatic disease 7.4 months P = in ECOG months 145 in ECOG months 3 in ECOG months P < no prior surgical, locoregional or ablative procedure 12.5 months 143 prior surgical, locoregional or ablative procedure 12.8 months P = statistically significant data Sangro. Hepatology 2011;54:
35 SIR-Spheres microspheres in Hepatocellular Carcinoma: European Multi-Centre Analysis Investigator n Treatment ORR SD Survival 1 st - or >2 nd -line Sangro 183 SIR-Spheres nr nr 110 patent portal vein 9.3 months 44 branch PVT 10.8 months 32 main PVT 9.7 months P = P = Patent/Branch PVT vs. Main PVT Sangro et al. Int J Radiat Oncol Biol Phys 2006;66: Iñarrairaegui et al. J Vasc Interv Radiol 2010;21: Sangro et al. EASL, J Hepatol 2011; Abs. 650.
36 Integration of SIRT in the HCC BCLC staging classification and treatment schedule HCC PS 0 Child A PS 0 2 Child A B PS >2 Child C Stage 0 Very Early Stage Stage A Early Stage Stage B Intermediate Stage Stage C Advanced Stage Stage D End Stage single <2 cm or carcinoma in situ single nodule or 3 nodules <3 cm PS 0 multinodular; PS 0 portal vein invasion, N1 M1 or PS 1 2 PS >2 or Child C (unless within transplant criteria) portal pressure; bilirubin normal single 3 nodules <3 cm increased associated diseases no yes unilobar fewer nodules smaller burden failed TACE bilobar multinodular larger burden fit/suitable for SIRT i.e. liver-dominant; bilirubin <35 U/l Child A or <B7 OR fit/suitable for sorafenib Resection Liver Transplant Ablation TACE/SIRT SIRT SIRT/ sorafenib Sorafenib Symptoms Curative Treatments 5-year survival 40 70% 30% of patients at presentation RCTs median survival months 50% of patients at presentation survival <3 mo 20% of patients Andreana L, Isgrò G, Marelli L et al. Treatment of hepatocellular carcinoma (HCC) by intra-arterial infusion of radio-emitter compounds: Trans-arterial radioembolisation of HCC. Cancer Treat Rev 2011 Dec 12; epub doi: /j.ctrv Sangro B, Salem R, Kennedy A et al. Radioembolization for hepatocellular carcinoma: a review of the evidence and treatment recommendations. Am J Clin Oncol 2011; 34:
37 m-net
38 SIR-Spheres microspheres in Neuroendocrine Tumour Liver Metastases Investigator n Tx ORR SD Symp. PFS Median Survival Mixed cohort: >1 st -line to treatment-refractory disease Kennedy 148 SIR-Spheres 63.2% 22.7% nr 70 mo median King 34 SIR-Spheres + 5FU 50% 14.7% 55% nr 59% at 35.2 mo Saxena 48 SIR-Spheres 54% 23% nr nr 35 mo Cao 58 (+ 5FU) 39.2% 27.4% nr nr 36 mo Jahangir 73 SIR-Spheres nr nr nr 10.6 mo 55.2 mo Rhee Y microspheres [ 92 94% ] nr 22 γ & 28 mo McElmurray 10 SIR-Spheres 30% 70% nr 60% at 36 mo Jakobs 25 SIR-Spheres 20.8% 75% 92% nr 96% at 12 mo McGrath 26 SIR-Spheres 58.3% * 33% * 2 of 3 nr 69.1% at 17 mo Kennedy 18 SIR-Spheres 89% * nr nr 89% at 27 mo Coldwell Y microspheres 67% 33% 80% nr nr Kennedy et al. Am J Clin Oncol 2008;31: King et al. Cancer 2008;113:21 9. Saxena et al. Ann Surg 2010; 251: Cao et al. Br J Surg 2010;97: Jahangir et al. ASCO 2011; e Rhee et al. Ann Surg 2008;247: McElmurray et al. WCIO 2012; Abs 47. Jakobs et al. SIR 2010; Abs 30. McGrath et al. Emerging Trends in Radioembolization using Microspheres Kennedy et al. ABS Meeting Coldwell et al. WCGIC 2005; Abs O-00.
39 Integrating SIRT into the mnet treatment paradigm <10% Potentially curative Resectable resection or ablation Liver-only or liverpredominant mnet Debulking surgery TACE? Radioembolisation Radionuclide therapy Chemotherapy Liver only or liver dominant Metastasis to the whole body Kennedy AS et al. ICACT 2008
40 m-breast Cancer
41 SIR-Spheres microspheres in Breast Cancer Liver Metastases Investigator n Treatment ORR SD PFS Survival Treatment of progressive disease or chemo-refractory disease Coldwell 44 SIR-Spheres 47% 47% nr 86% at 14 mo post-sirt 17 mo post-lm Dx mbca studies >350 chemotherapy nr nr nr mo post-lm Dx Salvage of chemo-refractory disease Jakobs 30 SIR-Spheres 61% 35% (>8 wk) nr 11.7 mo ( mo) 3/16 down-sized to RFA Michl 40 SIR-Spheres 46% 58% 3.3 mo 8.2 mo Haug 58 SIR-Spheres 26% 63% nr 11.0 mo Cianni 52 SIR-Spheres 56% 35% 6.6 mo 11.5 mo 8.4 mo L retrospective data Coldwell D et al. Int J Radiat Oncol Biol Phys 2007;69: Eichbaum M et al. Breast Cancer Res Treat 2006;96: Pentheroudakis G et al. Breast Cancer Res Treat 2005;97: Jakobs TF et al. J Vasc Interv Radiol 2008;19: Hoffmann RT et al. Eur J Radiol 2010;74: Michl M et al. ASCO 2010; Abs Haug AR et al. J Nucl Med 2012;53: Cianni et al. Eur Pathol 2012; epub.
42 Adverse Events
43 Adverse events directly attributable to SIRFLOX Trial and Comparisons. Delayed SIRTspecific adverse events FOLFOX + SIR-Spheres Microspheres Kennedy et al IJROBP2009 Sharma et al JCO 2007 van Hazel et al JCO 2009 (n = 60) (n = 515) (n = 20) (n = 25) Biopsy confirmed gastric/duodenal ulceration Biopsy confirmed gastric/duodenal ulceration % % % % REILD Cholecystitis Pneumonitis 0 < Pancreatitis Learning curve effect: 4/6 cases from 2 inexperienced sites
44 SIRT Serious Adverse Events at St.Vincents Hospital (n = 536). SAE Incidence Characteristics Prevention/action Radiation 2.4 % (10%) non-target administration meticulous technique gastritis or immediate, severe ulceration unremitting pain Radiation <1% (0%) non-target administration meticulous technique pancreatitis immediate, severe unremitting pain Radiation 1.9% (0.1% non-target administration various cholecystitis right upper quadrant pain actions Radiation- 2.1% (2.0%) excess radiation to normal liver dosimetry/infiltration Induced Liver typically 6-12 weeks post-sirt Disease (RILD) Radiation no immediate symptoms MAA lung-shunt study Pneumonitis 0% (0.1%)
45 Conclusion. At present and while we waiting for the results of SIRFLOX, FOXFIRE, SARAH, SIRveNB, SIR step and SORAMIC trials to complete we have level 2 to 3 evidence to prove that SIRT is effective in combination with 1 st to N th line chemotherapy as well as in the salvage situation. SIRT can be performed in heavily pre-treated chemorefractory patients even if they had previously received local-regional therapies such as RFA,TACE,DEB or previous surgery. SIRT is effective in managing metastatic liver disease from any primary as long as it is radio-sensitive and hypervascular. As we gain experience in performing SIRT the adverse event profile will even further diminish.
46 DEBIRI American Initiated Multicentre Multinational Study Martin et.al. Ann Surg Oncol 2011 Single arm study of m-crc patients receiving DEBIRI. All patients had failed Oxaliplatin and Irinotecan based regimes and biological agents. Endpoints: Safety, Tolerance, Response rates and Overall survival. The study met its primary endpoints by demonstrating DEBIRI is: Safe and well tolerated. Response rate was 66% at 6/12 and 75% at 12/12 vs. a response rate of 10% reported for patients resistant to systemic chemotherapy. Overall survival 19 months vs. 8.6 months reported for patients resistant to systemic chemotherapy. Progression free survival 11 months vs. 4.6 months reported for patients resistant to systemic chemotherapy.
47 DEBIRI Italian phase 3 study comparing DEBIRI VS. FOLFIRI Fiorentini Anticancer Research 2012;32: Phase 3 prospective RCT. Endpoints: 1. Survival primary 2. Response 3. Recurrence 4. Toxicity 5. QoL 6. Influence of molecular markers The study met its primary and secondary endpoints at 50/12: 1. Median survival significantly longer for DEBIRI at 22/12 VS.15/12 FOLFIRI 2. PFS 7/12 VS. 4/12 3. Hepatic and extrahepatic progression in all patients 4. Acceptable toxic profile 5. Better QoL in DEBIRI group 6. Wild type KRAS appear to have better overall survival than the mutated KRAS
48 DEBIRI German phase 1 to 2 study CIRCE 2011 The study set out to answer three questions: 1. Will smaller beads achieve better tumour penetration? 2. Will DEBIRI produce significant tumour necrosis? Answers: 1. High grade uptake of smaller beads seen even with different grades of vascularization. 2. Complete tumour necrosis in majority of metastases but poor response in patients with more than 50% hypovascular tumour involvement.
49 The SIRFLOX Study! To assess the efficacy and safety of adding targeted radiation (SIR-Spheres microspheres) to standard-of-care systemic chemotherapy (FOLFOX6m + bevacizumab), compared to FOLFOX6m chemotherapy (+ bevacizumab) alone as 1 st -line therapy in patients with non-resectable colorectal liver metastases, with or without evidence of extra-hepatic metastases" Design: Prospective open-label, multi-centre, multi-national RCT" Eligible Patients:!!Unresectable liver-only or liver-predominant metastatic CRC" "No prior chemotherapy for mcrc" "Fit for combination therapy and SIRT" Stratify:!!Presence of extra- hepatic metastases" "Degree of liver involvement" "Institution" "Use of bevacizumab" Randomise! 1:1! n = 518! SIR-Spheres microspheres day 3 4, Cycle 1;" * oxaliplatin 60 mg/m 2 Cycles 1 3 in chemo-sirt arm;" C4/C1 bevacizumab from Cycle 4 in test arm, Cycle 1 " (or per institutional protocol) in control arm;" Primary endpoint: "Progression-free survival (PFS)" Sponsor: "Sirtex" PIs: "Prof. Peter Gibbs; Prof. Guy van Hazel" Status: "Currently enrolling" Secondary endpoints: "PFS in liver" "Overall survival" "Response rate" "Quality of life" "Recurrence rate "" "Toxicity "" "Resection rate"
50 The FOXFIRE Study! Can selective internal radiotherapy to liver metastases improve overall survival for patients treated with OxMdG (FOLFOX) chemotherapy as 1 st -line treatment of metastatic colorectal cancer?" Design: Prospective open-label, multi-centre, national (UK) RCT" Eligible Patients:!!Unresectable liver-only or liver-predominant metastatic CRC" "No prior chemotherapy for mcrc" "Fit for combination therapy and SIRT" Stratify:!!Presence of extra- hepatic metastases" "Degree of liver involvement" "Institution" "Use of biologic agent" Randomise! 1:1! n = <490! SIR-Spheres microspheres day 3 4, Cycle 2;" * oxaliplatin 60 mg/m 2 Cycles 2 4 in chemo-sirt arm;" C7/C1 use of a biologic agent is allowed from Cycle 7" " for test arm and at any time in control arm;" Primary endpoint:!overall survival" "(combined SIRFLOX-FOXFIRE cohort)" Sponsor: PIs: Status:!University of Oxford"!Dr. Ricky Sharma; Dr. Harpreet Wasan"!Currently enrolling" Secondary endpoints: "Progression-free survival (PFS)" "Liver-specific PFS" "Safety and toxicity" "Health economics " "Quality of life" "Response rate" "Liver resection rate" "Interval to and proportion receiving " ""2 nd -line chemotherapy" "Translational research"
51 FOXFIREGlobal! To assess the efficacy and safety of adding targeted radiation (SIR-Spheres microspheres) to standard-of-care systemic chemotherapy (FOLFOX6m + bevacizumab), compared to FOLFOX6m chemotherapy (+ bevacizumab) alone as 1st-line therapy in patients with non-resectable colorectal liver metastases, with or without evidence of extra-hepatic metastases" Design: Prospective open-label, multi-centre, multi-national RCT" Eligible Patients:!!Unresectable liver-only or liver-predominant metastatic CRC" "No prior chemotherapy for mcrc" "Fit for combination therapy and SIRT" Stratify:!!Presence of extra- hepatic metastases" "Degree of liver involvement" "Institution" "Use of bevacizumab" Randomise! 1:1! n = ! SIR-Spheres microspheres day 3 4, Cycle 1 or 2;" * oxaliplatin 60 mg/m 2 Cycles 1 3 in chemo-sirt arm;" C4/C1 bevacizumab from Cycle 4 in test arm, Cycle 1 " (or per institutional protocol) in control arm;" Primary endpoint: "Overall survival (OS)" Sponsor: "Sirtex" PIs: "Prof. Peter Gibbs;" Status: "About to start" Secondary endpoints: "PFS" "PFS in liver" "Response rate" "Quality of life "" "Toxicity "" "Resection rate" "Health Economics"
52 The SIR-step Study! To investigate whether an intensified maintenance treatment of SIR-Spheres microspheres + simplified chemotherapy has a benefit in terms of time to progression compared to simplified chemotherapy alone, in patients with stable disease after 3 months 1 st -line induction chemotherapy" Design: Prospective open-label, multi-centre, multi-national RCT" Eligible Patients:!!Unresectable liveronly or liver-predominant mcrc" "Controlled disease (PR or SD) after 3 months induction chemotherapy + bevacizumab" "Fit for combination therapy and SIRT" Stratify:!!Presence of extra- hepatic metastases" "Degree of liver involvement" "Use of bevacizumab" Primary endpoint:!time to progression (TTP1)" Sponsor:!Antwerp University Hospital " " "in collaboration with " "Belgian Group of Digestive Oncology "(BGDO) " PIs: Status: "Opens Q3 2012" "Prof. Marc Peeters; Dr. Marc van den Eynde" Randomise! 1:1! n = 162! SIR-Spheres microspheres day 3 4, Cycle 2;" >C3/C1 bevacizumab from >4 weeks post-sirt" in test arm and at any time in control arm;" TTP1 > TTP2 > Secondary endpoints: "TTP (liver-specific TTP, TTP2 and " " "global TTP) " "Progression-free survival" "Response rate" "Liver resection rate" "Safety and toxicity" "Overall survival" " ""
53 The SORAMIC Study Can the overall survival of patients with HCC be improved by combining sorafenib with RFA or SIR-Spheres microspheres? Design: Prospective open-label, multi-centre, multi-national (Europe) RCT Eligible Patients: Unresectable HCC BCLC stage A, B or C Child-Pugh class B7 Fit for sorafenib and microtherapy using RFA or SIRT Imaging sub-study Contrastenhanced CT Primovist - enhanced MRI Off Study BCLC stage 0 BCLC stage D <4 tumours <5 cm each Assign to study arm RFA local ablation group palliative group Randomise 11:10 n = 375 Randomise 1:1 n = 290 Primary endpoints: Imaging sub-study: Non-inferiority (1 st step) or superiority (2 nd step) of Primovist-enhanced MRI Local ablation: Time-to-recurrence Palliative: Overall survival Sponsor: University of Magdeburg PIs: Prof. Peter Malfertheiner; Prof. Jens Ricke Status: Currently enrolling Secondary endpoints: ٠۰ Quality of life ٠۰ Biomarker analysis Imaging sub-study: ٠۰ Detected lesions and diagnostic confidence Local ablation group: ٠۰ Detection of recurrence ٠۰ Safety and toxicity Palliative group: ٠۰ Safety and toxicity ٠۰ Overall survival for patients with or without PVT SIR-Spheres microspheres
54 The SIRveNIB Study To determine the difference, if any, in overall survival between SIR-Spheres microspheres and sorafenib in patients with unresectable HCC Design: Prospective open-label, multi-centre, multi-national (Asia Pacific) RCT Eligible Patients: Unresectable HCC BCLC stage B or C Child-Pugh class A or B 7 points ECOG performance status 0 1 Fit for sorafenib and SIRT Stratify: Presence of portal vein thrombosis Institution Randomise 1:1 n = 360 Primary endpoint: Overall survival Sponsor: Singapore General Hospital in collaboration with National Medical Research Council, Singapore National Cancer Centre, Singapore Singapore Clinical Research Institute and the Asia Pacific HCC Trials Group PI: Prof. Pierce Chow Secondary endpoints: ٠۰ Progression-free survival (PFS) in the liver and at any site ٠۰ Response rate ٠۰ Safety and toxicity ٠۰ Quality of life ٠۰ Liver resection rate ٠۰ Liver transplantation rate ٠۰ Time to disease progression Status: Currently enrolling SIR-Spheres microspheres
55 The SARAH Study To determine whether radioembolisation with SIR-Spheres microspheres is more effective on overall survival in advanced HCC than sorafenib Design: Prospective open-label, multi-centre, national (France) RCT Eligible Patients: Unresectable HCC BCLC stage C or BCLC stage A/B: New lesions post-radical therapy and unsuitable for further radical therapy or No objective response after 2 TACE sessions Child-Pugh class A or B 7 points ECOG performance status 0 1 Fit for sorafenib and SIRT Primary endpoint: Overall survival Sponsor: Assistance Publique Hôpitaux de Paris (AP-HP) PI: Prof. Valérie Vilgrain Status: Currently enrolling Stratify ECOG performance status Vascular invasion Prior TACE Institution Randomise 1:1 n = 400 Secondary endpoints: ٠۰ Safety and toxicity ٠۰ Quality of life ٠۰ Healthcare costs ٠۰ Progression-free survival (PFS) at 6 months SIR-Spheres microspheres
Role of SIRT Beyond First Line Therapy in Colorectal Cancer. Dr Toh Han Chong Division of Medical Oncology National Cancer Centre Singapore
 Role of SIRT Beyond First Line Therapy in Colorectal Cancer Dr Toh Han Chong Division of Medical Oncology National Cancer Centre Singapore MILESTONES IN THE TREATMENT OF COLON CANCER SIR-Spheres microspheres
Role of SIRT Beyond First Line Therapy in Colorectal Cancer Dr Toh Han Chong Division of Medical Oncology National Cancer Centre Singapore MILESTONES IN THE TREATMENT OF COLON CANCER SIR-Spheres microspheres
P < vs. 5FU/LV LD 0% 60.0% 3.6 months P < P = 0.113
 in Colorectal Cancer The following summarizes the key data within the broad clinical platform supporting the use of SIR-Spheres Y-9 resin microspheres in the treatment of liver metastases arising from
in Colorectal Cancer The following summarizes the key data within the broad clinical platform supporting the use of SIR-Spheres Y-9 resin microspheres in the treatment of liver metastases arising from
Guidelines for SIRT in HCC An Evolution
 Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
+ Radioembolization for ColoRectal Cancer Metastatic to the Liver
 + Radioembolization for ColoRectal Cancer Metastatic to the Liver Oct 4 th 2017 Alain Hendlisz, Institut Jules Bordet 1 st International Course on THERANOSTICS & MOLECULAR RADIOTHERAPY Indication and Rationale
+ Radioembolization for ColoRectal Cancer Metastatic to the Liver Oct 4 th 2017 Alain Hendlisz, Institut Jules Bordet 1 st International Course on THERANOSTICS & MOLECULAR RADIOTHERAPY Indication and Rationale
SIR-Spheres: Des essais cliniques à la pratique courante
 SIR-Spheres: Des essais cliniques à la pratique courante Un focus sur le traitement du mcrc en échappement thérapeutique Dr. Michaël Vouche, MD. PhD. Université Libre de Bruxelles Institut Jules Bordet
SIR-Spheres: Des essais cliniques à la pratique courante Un focus sur le traitement du mcrc en échappement thérapeutique Dr. Michaël Vouche, MD. PhD. Université Libre de Bruxelles Institut Jules Bordet
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
RADIOEMBOLIZZAZIONE NEI TUMORI EPATICI: STATO DELL ARTE. clic per modificare lo stile del sottotitolo dello schem
 XII Congresso Nazionale AIMN 2015 16-19 Aprile 2015 Rimini RADIOEMBOLIZZAZIONE NEI TUMORI EPATICI: STATO DELL ARTE clic per modificare lo stile del sottotitolo dello schem Marco Maccauro Nuclear Medicine
XII Congresso Nazionale AIMN 2015 16-19 Aprile 2015 Rimini RADIOEMBOLIZZAZIONE NEI TUMORI EPATICI: STATO DELL ARTE clic per modificare lo stile del sottotitolo dello schem Marco Maccauro Nuclear Medicine
in Hepatocellular Carcinoma
 in Hepatocellular Carcinoma The following summarises the key data supporting the use of SIR-Spheres Y-90 resin microspheres in the treatment of primary liver cancer due to hepatocellular carcinoma (HCC):
in Hepatocellular Carcinoma The following summarises the key data supporting the use of SIR-Spheres Y-90 resin microspheres in the treatment of primary liver cancer due to hepatocellular carcinoma (HCC):
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC?
 WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
SIRT for Intermediate and Advanced HCC
 Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC
 Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy?
 Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Identification and Management of post SIRT toxicities and complications
 Identification and Management of post SIRT toxicities and complications A/Prof. Lourens Bester Interventional Radiologist University of Notre Dame Sydney Disclosure Consultant and Proctor for SIRTEX Medical
Identification and Management of post SIRT toxicities and complications A/Prof. Lourens Bester Interventional Radiologist University of Notre Dame Sydney Disclosure Consultant and Proctor for SIRTEX Medical
SUMMARY OF THE SIRFLOX RESULTS
 SUMMARY OF THE SIRFLOX RESULTS The SIRFLOX study results on the combination of SIR-Spheres Y-90 resin microspheres with first-line chemotherapy were published in Journal of Oncology in early 2016. 1 There
SUMMARY OF THE SIRFLOX RESULTS The SIRFLOX study results on the combination of SIR-Spheres Y-90 resin microspheres with first-line chemotherapy were published in Journal of Oncology in early 2016. 1 There
NHS England. Cedar on behalf of NHS England Specialised Commissioning
 NHS England Evidence review: selective internal radiation therapy (SIRT) with ytrrium-90 microspheres for unresectable, liver-only or liver-dominant metastatic colorectal carcinoma who are chemotherapyrefractory
NHS England Evidence review: selective internal radiation therapy (SIRT) with ytrrium-90 microspheres for unresectable, liver-only or liver-dominant metastatic colorectal carcinoma who are chemotherapyrefractory
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE METASTASES
 LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
LIVER DIRECTED THERAPIES FOR PATIENTS WITH UNRESECTABLE COLORECTAL CANCER LIVER METASTASES Jaime R. Merchan, MD, MMSc Associate Professor of Medicine Division of Hematology-Oncology University of Miami
Description. Section: Therapy Effective Date: July 15, 2014 Subsection: Therapy Original Policy Date: June 7, 2012 Subject: Page: 1 of 23
 Last Review Status/Date: June 2014 Page: 1 of 23 Description Radioembolization (RE), referred to as selective internal radiation therapy or SIRT in older literature, is the intra-arterial delivery of small
Last Review Status/Date: June 2014 Page: 1 of 23 Description Radioembolization (RE), referred to as selective internal radiation therapy or SIRT in older literature, is the intra-arterial delivery of small
Evaluation of SIRFLOX Study Results. Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany
 Evaluation of SIRLX Study Results Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany ESM Guideline: Response is a Goal of Treatment Performance Status of the
Evaluation of SIRLX Study Results Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany ESM Guideline: Response is a Goal of Treatment Performance Status of the
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Unmet needs in intermediate HCC. Korea University Guro Hospital Ji Hoon Kim
 Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Radioembolisation (Yttrium-90 microspheres) for liver malignancies.
 for liver malignancies.") Radioembolisation (Yttrium-90 microspheres) for liver malignancies. M. Van den Eynde, R. Lhommel, P. Goffette, M.Peeters, P. Flamen, A. Hendlisz Radioembolisation using radioactive yttrium-90-labeled microspheres
Radioembolisation (Yttrium-90 microspheres) for liver malignancies. M. Van den Eynde, R. Lhommel, P. Goffette, M.Peeters, P. Flamen, A. Hendlisz Radioembolisation using radioactive yttrium-90-labeled microspheres
For personal use only
 Sirtex Medical Limited SARAH Clinical Study Results Investor Presentation Nigel Lange, Interim CEO Dr David N. Cade, CMO 24 April 2017 SIR-Spheres is a registered trademark of Sirtex SIR-Spheres Pty Ltd
Sirtex Medical Limited SARAH Clinical Study Results Investor Presentation Nigel Lange, Interim CEO Dr David N. Cade, CMO 24 April 2017 SIR-Spheres is a registered trademark of Sirtex SIR-Spheres Pty Ltd
Radioembolization for Primary and Metastatic Tumors of the Liver
 Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2017 Origination: 8/2006 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2017 Origination: 8/2006 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days
 94% of radiation delivered within 11 days") 100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES. Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí
 INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
SIRT in the Management of Metastatic Neuroendocrine Tumors
 SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
Radioembolization for Primary and Metastatic Tumors of the Liver
 Page: 1 of 28 Last Review Status/Date: September 2015 Description Radioembolization (RE), also referred to as selective internal radiotherapy (SIRT), is the intra-arterial delivery of small beads (microspheres)
Page: 1 of 28 Last Review Status/Date: September 2015 Description Radioembolization (RE), also referred to as selective internal radiotherapy (SIRT), is the intra-arterial delivery of small beads (microspheres)
Selective Internal Radiation Therapy (SIRT) in the multimodal approach to Hepatocellular Carcinoma
 in the multimodal approach to Hepatocellular Carcinoma") Selective Internal Radiation Therapy (SIRT) in the multimodal approach to Hepatocellular Carcinoma International Course on THERANOSTICS and MOLECULAR RADIOTHERAPY Brussels, 4 october 2017 Vincent Donckier
Selective Internal Radiation Therapy (SIRT) in the multimodal approach to Hepatocellular Carcinoma International Course on THERANOSTICS and MOLECULAR RADIOTHERAPY Brussels, 4 october 2017 Vincent Donckier
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Combined FOXFIRE Study Data Presented at ASCO Annual Meeting
 ASX/MEDIA RELEASE 6 th June 2017 Combined FOXFIRE Study Data Presented at ASCO Annual Meeting Sydney, Australia; 6 th June 2017 Sirtex Medical Limited (ASX:SRX) announces the oral abstract of the combined
ASX/MEDIA RELEASE 6 th June 2017 Combined FOXFIRE Study Data Presented at ASCO Annual Meeting Sydney, Australia; 6 th June 2017 Sirtex Medical Limited (ASX:SRX) announces the oral abstract of the combined
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
HCC with Intrahepatic Portal vein Tumour Should Be Treated by Systemic Therapy Rather Than Transarterial Therapy (Pros)
") HCC with Intrahepatic Portal vein Tumour Should Be Treated by Systemic Therapy Rather Than Transarterial Therapy (Pros) Yi-Hsiang Huang, MD, Ph.D. Professor, Division of Gastroenterology & Hepatology,
HCC with Intrahepatic Portal vein Tumour Should Be Treated by Systemic Therapy Rather Than Transarterial Therapy (Pros) Yi-Hsiang Huang, MD, Ph.D. Professor, Division of Gastroenterology & Hepatology,
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Disclosure. Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report:
 Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
Clinical Commissioning Policy Proposition:
 Clinical Commissioning Policy Proposition: Selective internal radiation therapy (SIRT) in the treatment of chemotherapy refractory and intolerant, unresectable metastatic colorectal cancer (Adults) Reference:
Clinical Commissioning Policy Proposition: Selective internal radiation therapy (SIRT) in the treatment of chemotherapy refractory and intolerant, unresectable metastatic colorectal cancer (Adults) Reference:
SIRT Dosimetry: Sometimes Less Is More
 SIRT Dosimetry: Sometimes Less Is More Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director, Radiation Oncology,
SIRT Dosimetry: Sometimes Less Is More Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director, Radiation Oncology,
Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases
 Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora silentio» Malignant
Radioembolization with Lipiodol for the Treatment of Hepatocellular Carcinoma and Liver Metastases Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora silentio» Malignant
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2018T0445O Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2018T0445O Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS
SIRveNIB Study Data Presented at ASCO Annual Meeting
 ASX/MEDIA RELEASE 5 th June 2017 SIRveNIB Study Data Presented at ASCO Annual Meeting Sydney, Australia; 5 th June 2017 Sirtex Medical Limited (ASX:SRX) announces the oral abstract of the SIRveNIB clinical
ASX/MEDIA RELEASE 5 th June 2017 SIRveNIB Study Data Presented at ASCO Annual Meeting Sydney, Australia; 5 th June 2017 Sirtex Medical Limited (ASX:SRX) announces the oral abstract of the SIRveNIB clinical
For personal use only
 ASX / MEDIA RELEASE 1 st June 2015 ASCO Peer Review Supports the Benefits of SIR-Spheres Y-90 Resin Microspheres in the Liver SIRFLOX results confirmed as both statistically significant and clinically
ASX / MEDIA RELEASE 1 st June 2015 ASCO Peer Review Supports the Benefits of SIR-Spheres Y-90 Resin Microspheres in the Liver SIRFLOX results confirmed as both statistically significant and clinically
MEDICAL POLICY SUBJECT: SELECTIVE INTERNAL RADIATION THERAPY (SIRT) FOR HEPATIC TUMORS. POLICY NUMBER: CATEGORY: Technology Assessment
 FOR HEPATIC TUMORS. POLICY NUMBER: CATEGORY: Technology Assessment") MEDICAL POLICY SUBJECT: SELECTIVE INTERNAL PAGE: 1 OF: 8 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including an
MEDICAL POLICY SUBJECT: SELECTIVE INTERNAL PAGE: 1 OF: 8 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including an
Embolotherapy for Cholangiocarcinoma: 2016 Update
 Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer
 Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer M Ducreux, MD, PhD Gustave Roussy Villejuif, FRANCE M Ducreux is a consultant to Biocompatibles
Role of loco-regional treatment in the medical and surgical management strategy of metastatic colorectal cancer M Ducreux, MD, PhD Gustave Roussy Villejuif, FRANCE M Ducreux is a consultant to Biocompatibles
Radioembolization for Primary and Metastatic Tumors of the Liver
 Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2018 Origination: 8/2006 Next Review: 8/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Radioembolization for Primary and Metastatic Tumors of the Liver Policy Number: 8.01.43 Last Review: 8/2018 Origination: 8/2006 Next Review: 8/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
NHS England Reference: P
 Clinical Commissioning Policy: Selective internal radiation therapy (SIRT) for chemotherapy refractory / intolerant metastatic colorectal cancer (adults) NHS England Reference: 170102P 1 NHS England INFORMATION
Clinical Commissioning Policy: Selective internal radiation therapy (SIRT) for chemotherapy refractory / intolerant metastatic colorectal cancer (adults) NHS England Reference: 170102P 1 NHS England INFORMATION
Damm et al. BMC Cancer (2016) 16:509 DOI /s x
 16:509 DOI /s x") Damm et al. BMC Cancer (2016) 16:509 DOI 10.1186/s12885-016-2549-x RESEARCH ARTICLE Open Access Y90 Radioembolization in chemo-refractory metastastic, liver dominant colorectal cancer patients: outcome
Damm et al. BMC Cancer (2016) 16:509 DOI 10.1186/s12885-016-2549-x RESEARCH ARTICLE Open Access Y90 Radioembolization in chemo-refractory metastastic, liver dominant colorectal cancer patients: outcome
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma
 Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of selective internal radiation therapy for primary liver cancer Selective internal
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of selective internal radiation therapy for primary liver cancer Selective internal
Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis?
 of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis?") Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis? Poster No.: C-1634 Congress: ECR 2014 Type: Authors: Keywords: DOI:
Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis? Poster No.: C-1634 Congress: ECR 2014 Type: Authors: Keywords: DOI:
Disclosures. Fees for Non CME/CE services received. agents: Bayer Healthcare. CT guided HDR Brachytherapy in Oligometastases
 CT guided HDR Brachytherapy in Oligometastases Jens Ricke Radiology and Nuclear medicine University of Magdeburg Disclosures Fees for Non CME/CE services received directlyfrom a commercial interest or
CT guided HDR Brachytherapy in Oligometastases Jens Ricke Radiology and Nuclear medicine University of Magdeburg Disclosures Fees for Non CME/CE services received directlyfrom a commercial interest or
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
Portal Vein Invasion and the Role of Liver Directed Therapy. Matthew S Johnson MD FSIR Indiana University May 6, 2016
 Portal Vein Invasion and the Role of Liver Directed Therapy Matthew S Johnson MD FSIR Indiana University May 6, 2016 Matthew Johnson, M.D., FSIR Stock: Endoshape Consultant/Advisory Board: Bayer, BTG,
Portal Vein Invasion and the Role of Liver Directed Therapy Matthew S Johnson MD FSIR Indiana University May 6, 2016 Matthew Johnson, M.D., FSIR Stock: Endoshape Consultant/Advisory Board: Bayer, BTG,
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Clinical Study Yttrium-90 Radioembolization for Colorectal Cancer Liver Metastases: A Single Institution Experience
 International Journal of Surgical Oncology Volume 20, Article ID 5726, 9 pages doi:0.55/20/5726 Clinical Study Yttrium-90 Radioembolization for Colorectal Cancer Liver Metastases: A Single Institution
International Journal of Surgical Oncology Volume 20, Article ID 5726, 9 pages doi:0.55/20/5726 Clinical Study Yttrium-90 Radioembolization for Colorectal Cancer Liver Metastases: A Single Institution
SIRTEX Lunch Symposium, Cebu, 23 Nov Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong
 SIRTEX Lunch Symposium, Cebu, 23 Nov 2013 Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong I will not talk on Mechanism of SIRT Data on efficacy of SIRT Epidemiology
SIRTEX Lunch Symposium, Cebu, 23 Nov 2013 Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong I will not talk on Mechanism of SIRT Data on efficacy of SIRT Epidemiology
Systemic Cytotoxic Therapy in advanced HCC
 Systemic Cytotoxic Therapy in advanced HCC Yeul Hong Kim Korea University Anam Hospital Cancer Center Hepatocellular Carcinoma : Overview Epidemiology Current Guideline : advanced HCC Cytotoxic Chemotherapy
Systemic Cytotoxic Therapy in advanced HCC Yeul Hong Kim Korea University Anam Hospital Cancer Center Hepatocellular Carcinoma : Overview Epidemiology Current Guideline : advanced HCC Cytotoxic Chemotherapy
MEDICAL POLICY SUBJECT: SELECTIVE INTERNAL RADIATION THERAPY (SIRT) FOR HEPATIC TUMORS
 FOR HEPATIC TUMORS") MEDICAL POLICY SUBJECT: SELECTIVE INTERNAL PAGE: 1 OF: 10 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including an
MEDICAL POLICY SUBJECT: SELECTIVE INTERNAL PAGE: 1 OF: 10 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including an
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
PRIOR AUTHORIZATION Prior authorization is required for BlueCHiP for Medicare members and recommended for Commercial products.
 Medical Coverage Policy Radioembolization for Primary and Metastatic Tumors of the Liver EFFECTIVE DATE: 10 06 2009 POLICY LAST UPDATED: 08 02 2016 OVERVIEW Radioembolization (RE), referred to as selective
Medical Coverage Policy Radioembolization for Primary and Metastatic Tumors of the Liver EFFECTIVE DATE: 10 06 2009 POLICY LAST UPDATED: 08 02 2016 OVERVIEW Radioembolization (RE), referred to as selective
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.11 T2 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Oxford Clinical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: CANCER 036.11 T2 Effective Date: May 1, 2018 Table of Contents Page INSTRUCTIONS
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain
 New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
soramic newsletter no. 1 / 2015
 Page 1 Message from the PIs Dear colleagues and friends; esteemed members of the SORAMIC study group, This newsletter is specifically dedicated to the prevention and treatment of radioembolization induced
Page 1 Message from the PIs Dear colleagues and friends; esteemed members of the SORAMIC study group, This newsletter is specifically dedicated to the prevention and treatment of radioembolization induced
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
Hepatocellular carcinoma: Intra-arterial treatments
 Hepatocellular carcinoma: Intra-arterial treatments Irene Bargellini U.O. Radiologia Interventistica Azienda Ospedaliero Universitaria Pisana IRENE BARGELLINI,MD UO RADIOLOGIA INTERVENTISTICA, AZIENDA
Hepatocellular carcinoma: Intra-arterial treatments Irene Bargellini U.O. Radiologia Interventistica Azienda Ospedaliero Universitaria Pisana IRENE BARGELLINI,MD UO RADIOLOGIA INTERVENTISTICA, AZIENDA
Chemosaturation: Indication, Technique and Outcome
 Chemosaturation: Indication, Technique and Outcome Thomas J Vogl, S Koch, B Gebauer, W Willinek, C Engelke, R Bruening, F Wacker, A Enk I D I R: Institute of Diagnostic and Interventional Radiology Goethe
Chemosaturation: Indication, Technique and Outcome Thomas J Vogl, S Koch, B Gebauer, W Willinek, C Engelke, R Bruening, F Wacker, A Enk I D I R: Institute of Diagnostic and Interventional Radiology Goethe
Y-Microspheres Radioembolization for Selective Internal Radiation Therapy of Primary and Metastatic Cancer in the Liver
 90 Y-Microspheres Radioembolization for Selective Internal Radiation Therapy of Primary and Metastatic Cancer in the Liver Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora
90 Y-Microspheres Radioembolization for Selective Internal Radiation Therapy of Primary and Metastatic Cancer in the Liver Pr Francesco Giammarile CHLS Lyon Faculté de Lyon Sud «Aut tace aut loquere meliora
DALLA CAPECITABINA AL TAS 102
 DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page
 Vol.69(1), Page") The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
Sirtex Medical Limited (ASX:SRX)
") Sirtex Medical Limited (ASX:SRX) Macquarie Australia Conference Mr Gilman Wong, CEO Dr David Cade, CMO Sydney, 8 th May 2014 SIR-Spheres is a registered trademark of Sirtex SIR-Spheres Pty Ltd 1 Understanding
Sirtex Medical Limited (ASX:SRX) Macquarie Australia Conference Mr Gilman Wong, CEO Dr David Cade, CMO Sydney, 8 th May 2014 SIR-Spheres is a registered trademark of Sirtex SIR-Spheres Pty Ltd 1 Understanding
Ruolo della interventistica per le secondarietà epatiche e di altre sedi
 Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Colon Cancer Molecular Target Agents
 Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Strategy for the treatment of metastatic CRC through the lines
 Strategy for the treatment of metastatic CRC through the lines I Congresso de Oncologia D Or 2013: Satellite Symposium, ROCHE David Cosgrove, MD Johns Hopkins University Disclosures No relevant financial
Strategy for the treatment of metastatic CRC through the lines I Congresso de Oncologia D Or 2013: Satellite Symposium, ROCHE David Cosgrove, MD Johns Hopkins University Disclosures No relevant financial
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
Radioembolization for Treatment of Salvage Patients with Colorectal Cancer Liver Metastases: A Systematic Review
 Radioembolization for Treatment of Salvage Patients with Colorectal Cancer Liver Metastases: A Systematic Review Charlotte E.N.M. Rosenbaum 1, Helena M. Verkooijen 1, Marnix G.E.H. Lam 1, Maarten L.J.
Radioembolization for Treatment of Salvage Patients with Colorectal Cancer Liver Metastases: A Systematic Review Charlotte E.N.M. Rosenbaum 1, Helena M. Verkooijen 1, Marnix G.E.H. Lam 1, Maarten L.J.
Section: Medicine Last Reviewed Date: July Policy No: 140 Effective Date: October 1, 2014
 Medical Policy Manual Topic: Radioembolization for Primary and Metastatic Tumors of the Liver Date of Origin: December 2, 2010 Section: Medicine Last Reviewed Date: July 2014 Policy No: 140 Effective Date:
Medical Policy Manual Topic: Radioembolization for Primary and Metastatic Tumors of the Liver Date of Origin: December 2, 2010 Section: Medicine Last Reviewed Date: July 2014 Policy No: 140 Effective Date:
SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER
 SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER SIR-Spheres*: A New Treatment Option for Non-Resectable Liver Tumors Treatment Overview SIRT: Selective Internal Radiation Therapy Concept
SELECTIVE INTERNAL RADIATION THERAPY FOR TREATMENT OF LIVER CANCER SIR-Spheres*: A New Treatment Option for Non-Resectable Liver Tumors Treatment Overview SIRT: Selective Internal Radiation Therapy Concept
Does it matter which chemotherapy regimen you partner with the biologic agents?
 Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
In- and exclusion criteria
 In- and exclusion criteria Kerstin Schütte Department of Gastroenterology, Hepatology and Infectious Diseases University of Magdeburg Overview: Study population Inclusion criteria I - General criteria
In- and exclusion criteria Kerstin Schütte Department of Gastroenterology, Hepatology and Infectious Diseases University of Magdeburg Overview: Study population Inclusion criteria I - General criteria
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS
 UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2017T0445N Effective Date: January 1, 2017 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Commercial Medical Policy IMPLANTABLE BETA-EMITTING MICROSPHERES FOR TREATMENT OF MALIGNANT TUMORS Policy Number: 2017T0445N Effective Date: January 1, 2017 Table of Contents Page INSTRUCTIONS
The ESMO consensus conference on metastatic colorectal cancer
 ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
HCC: Is it an oncological disease? - No
 June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
Sirtex Medical Limited
 Sirtex Medical Limited Lunch and Learn Clinician and Corporate Briefing Mr Nigel Lange, Interim CEO Dr David N. Cade, CMO mcrc Presenter: A/Prof Nick Pavlakis HCC Presenter: Prof Bruno Sangro Sydney, 2
Sirtex Medical Limited Lunch and Learn Clinician and Corporate Briefing Mr Nigel Lange, Interim CEO Dr David N. Cade, CMO mcrc Presenter: A/Prof Nick Pavlakis HCC Presenter: Prof Bruno Sangro Sydney, 2
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
EPIDEMIOLOGY. Long established risk factors for CCA: hepatobiliaryflukes, PSC, biliary tract cysts, epatolithiasis.
 EPIDEMIOLOGY Intrahepatic cholangiocarcinoma(icc) is the second most common (15%) primary liver cancer after hepatocellular carcinoma (HCC), with a rate of about 2.1/100,000 people per year in western
EPIDEMIOLOGY Intrahepatic cholangiocarcinoma(icc) is the second most common (15%) primary liver cancer after hepatocellular carcinoma (HCC), with a rate of about 2.1/100,000 people per year in western
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Safety of selective internal radiation therapy (SIRT) with yttrium-90 microspheres combined with systemic anticancer agents: expert consensus
 with yttrium-90 microspheres combined with systemic anticancer agents: expert consensus") Review Article Safety of selective internal radiation therapy (SIRT) with yttrium-90 microspheres combined with systemic anticancer agents: expert consensus Andrew Kennedy 1, Daniel B. Brown 2, Jonas Feilchenfeldt
Review Article Safety of selective internal radiation therapy (SIRT) with yttrium-90 microspheres combined with systemic anticancer agents: expert consensus Andrew Kennedy 1, Daniel B. Brown 2, Jonas Feilchenfeldt
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
Liver Directed Therapy for Hepatocellular Carcinoma
 Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer