Title: Chimeric Antigen Receptor T-Cell Therapy: Presenters: Promises and Challenges Date: Elizabeth Budde, MD, PhD
|
|
|
- Joy Garrison
- 5 years ago
- Views:
Transcription




1 Title: Chimeric Antigen Receptor T-Cell Therapy: Presenters: Promises and Challenges Date: Elizabeth Budde, MD, PhD Department of Hematology & HCT T Cell Therapeutics Research Laboratory Beckman Research Institute City of Hope National Medical Center Duarte, CA
2 DISCLOSURES Advisory board for Precision Biosciences, Promab Biotechnologies Research supports from Mustang Therapeutics, Amgen Inc, Merck & Co. Speaker Bureau for Kite Pharma, AstraZeneca, Gilead Inc.
3 Presentation Objectives Overview of CAR T mechanism of action Current status of relevant CAR T trials Toxicity management Patient screening and consultation CAR T therapy optimization

4 2017 A Year of CAR T Cell Breakthroughs FDA Approval for CD19-CAR T Therapy KYMRIAH August 30, 2017 Novartis Receives Approval For Acute Lymphoblastic Leukemia $475,000/cell product YESCARTA October 18, 2017 Kite/Gilead Receives Approval For Diffuse Large B Cell Lymphoma $373,000/cell product

5 Clinicaltrials.gov assessed on 3/15/2018 EMBO Molecular Medicine Volume 9, Issue 9, pages , 1 AUG 2017 Clinical Development of CAR T Cell Trials In 2018 (n=501) US: 194 China: 177 Europe: 82
6 Chapter 1: The Tool CART-Cell Therapy: Mechanism of Action
7 constitutive constitutive co-stimulation co-stimulation is provided is by provided the T cells by the between T cells the between scfv and the scfv cell and membrane, the cell membrane, which both which lifts both lifts themselves themselves 47. The development 47. The development of new combinations of new combinations the antigen-binding the antigen-binding domain away domain from away the membrane from the membrane of signalling of moieties signalling continues moieties with continues a view with to enhancing T cell function ing T cell 48. function However, 48. the However, benefits TCRs the of benefits includ-v.s. of essary to CARs bind essary antigen. to bind Members antigen. of Members the immunoglobulin of the immunoglobulin a view to enhanc- and provides and flexibility provides for flexibility the CAR for to the reorientate CAR to reorientate if nec- if necing multiple ing co-stimulatory multiple co-stimulatory domains into domains CARs into are CARs superfamily are superfamily excel in terms excel of flexibility, in terms of and flexibility, hinge regions and hinge regions not always not clear always and other clear factors and other such factors as the such target as the from target superfamily from superfamily members such members as CD8, such CD28 as CD8, and IgG CD28 and IgG antigen, the antigen, method the of method T cell production of T cell production and the and are often the used. are Assessments often used. Assessments of the relative of capacity the relative for capacity the for the TCR-mediated IR CAR-mediated IR a a Tumour cell b Tumour cell b Tumour cell Tumour cell T cell T cell T cell either T cell either naturally naturally occurring or occurring or from a transgenic from a transgenic mouse mouse TCR β2 MHCI Tumour peptide β TCR α β T cell γ ε ε δ γζ ε ε δ ζ CD3 complex CD3 complex Adapted from Kershaw et al, Nature Reviews Cancer 2013 β2 Extra and intracellular antigens α- β α- β Peptide processing required Restricted by patient s HLA Kd =10-6 to 10-4 M No ligand on HLA-negative tumor Non-immunogenic α b b MHCI Tumour peptide B cell antibody fromantibody from B cells B cells T cell B cell CD8 CD3ζ or FcεRIγ Tumour antigen Tumour antigen V H V L CD8 CD3ζ or FcεRIγ scfv T cell Direct arecognition a of extracellular Nature Reviews Cancer α- β α- β γ- δ- ε- γ- ζ δ- ε- ζ ζ V H V L ζ scfv T cell tumor-associated antigens Peptide processing not required HLA-independent, Kd = 10-9 to 10-6 M Immunogenicity might be a problem
 240, 1087-1098.")
8 Design & Engineering of CARs Costim 1 Costim 1 Signal 2 Signal 2 Signal 1 Costim 2 Eshhar 1993 Signal 1 Signal 1 Amelia E Firor; Alexander Jares; Yupo Ma; Exp Biol Med (Maywood) 240, with Modification
9 Not All CD19CARs Are Created Equal MSKCC JCAR-015 NCI KTE19 COH UPENN CTL-019 FHCRC/SCH JCAR017 CD28 CD28 CD28 4-1BB 4-1BB ζ ζ ζ ζ ζ ζ ζ ζ ζ ζ

10 The Common Process of CAR T Therapy cell engineering expansion and processing T cell activation CAR delivery PBMC collection lymphodepletion Variables: - the starting population: VST, subset enrichment/depletion, - manufacturing process activation method, cytokines, expansion time, - infused products: bulk or defined population,



11 Chapter 2: The Speed and Accidents Efficacy and Safety of Current Relevant CAR T-Cell Therapies
12 NHL ZUMA-1 (NCT ): Multicenter Phase II Trial of Axi-cel (sponsor: KITE Pharma/Gilead) JULIET (NCT ): Multicenter Phase II trial of Tisagenlecleucel (sponsor: Novartis) TRANSCEND NHL 001 (NCT ): Multicenter Phase I/II trial of Liso-cel (Sponsor: Juno Therapeutics/Celgene)
13 ZUMA-1 N = 111 NHL:CD19CARs JULIET N = 149 Costim domain CD28 4-1BB 4-1BB TRANSCEND N = 140 T cell type PBMC PBMC CD4: CD8 (1:1) 11 non-comforming ALC 100 /ul 300 /ul No requirement Cell dose 1-2M/kg M 100M (DL2S) Product success 99% 94% 98% (126/128) Product not given Patients Ref DLBCL, tfl, PMBCL R/R DLBCL tfl R/R DLBCL NOS tfl, FLgr3b high grade BCL Prior auto allowed allowed allowed CNS no no 2 nd CNS, allowed ECOG PS
14 NHL: Potential Best in Profile CR + durability+ Safety ZUMA-1 KTE-019 JULIET CTL-019 Lymphodepletion Flu/Cy Flu/Cy, Benda Flu/Cy TRANSCEND JCAR17 core group Best CR 54% (n=101) 40% (n = 81) 63% (n = 27) CR at 3 mos months 52% 32% 68% CR at 6 mos 36% 30% 50% Transplant 2 -> allohct 0% responders n/a CRS grade 3 12% 23% 0% (n=29) Grading Median TTO Lee s 2d (1-12) Penn scale 3d (1-9) NT grade 3 31% 12% 7% Grading Median TTO CTCAE4.03 5d (1-17) CTCAE4.03 n/a Lee s 5d (1-14) CTCAE d (3-23) Outpatient 0% 26% 20% (4/20) ASH 2017
 All: 9.2 mos (3.7, NR) PR: 2.1 mos (1.0, 5.")

15 Probability of Relapse Free (%) % Survival ZUMA-1 Duration of Response JULIET TRANSCEND (CORE) Median DoR: NR Pts at Mos From Onset of Response Risk, n At Risk CR: NR (5.0, NR) All: 9.2 mos (3.7, NR) PR: 2.1 mos (1.0, 5.0) Time from first response (months) CR PR All Median PFS 5.9 Mo -most pts with CR at Mo 6 remained in CR - 74% RFS at Mo 6 -No responders moved to HCT - Most pts achieving CR at Mo 3 remained in CR 80% CR at Mo 3 remain in CR at Mo 6 92% CR at Mo 6 remains in CR at a longer term ASH 2017
16 Other CAR T for NHL CAR No. of Sites Malignancy CD22 CAR at least 10 sites B-NHL, ALL CD30 CAR at least 7 sites HL, ALCL IgK CAR 1 (Baylor) B-NHL CD20 CAR at least 10 sites B-NHL CD7 CAR 1 TCL and T-ALL CD5 CAR 1 (Baylor) TCL CD4 CAR Being planned TCL CCR4 CAR Being planned TCL
17 CAR T Therapy for Lymphoma at COH Therapies in the following diseases DLBCL, tfl, PMBCL (3 sponsored trials, 1 COH trial, Yescarta) MCL (1 active sponsored trial, 1 COH trial being planned) CLL (1 active sponsored trial) CAR T Physician Team Stephen Forman Elizabeth Budde Alex Herrera Leslie Popplewell Tanya Siddiqi Jasmine Zain And others


18 Acute Lymphoblastic Leukemia Indication patients up to 25 years of age with ALL that is refractory or in second or later relapse.
19 Primary endpoint: ELIANA: Study Design International, multicenter, open-label, single-arm phase 2 study Pts (N =107) aged 3-21 yrs 5% BM lymphoblasts; no isolated extramedullary disease, no prior CD19-directed therapy, no prior gene therapy ORR (CR + CRi) within 3 mos; 4-wk maintenance of remission required (the null hypothesis, ORR 20%) Secondary endpoints MRD status, DoR, OS, cellular kinetics, safety Maude, et al. NEJM. 2018;378: Fludarabine 30 mg/m²/d IV QD x 4 Cyclophosphamide 500 mg/m²/d IV x 2 CTL x 10 6 /kg IV 50 kg x 10 8 IV if > 50 kg (n = 62 ) 17 pts discontinued before infusion: deaths (n = 7), manufacturing failures (n = 7), AEs (n = 3).
20 ELIANA: Baseline Characteristics at Enrollment Characteristic CTL019 (N = 107) Median age, yrs (range) 11 (3-23) Male, % 55 Prior allohct, n (%) 46 (61%) Median previous lines of therapy, n (range) 3 (1-8) Median marrow blast, % 74% (5% to 99%) Current disease status, % Primary refractory Chemotherapy refractory Relapsed Maude, et al. NEJM. 2018;378:
 with median stay of 7 days (range, 1-34) 10% mechanical ventilation 25% high dose vasopressors SL Maude")
21 Adverse Events of Special Interest within 8 Weeks after Infusion, Regardless of Relationship to Tisagenlecleucel.* ELIANA: Safety ICU admission 47% (35 of 75) with median stay of 7 days (range, 1-34) 10% mechanical ventilation 25% high dose vasopressors SL Maude et al. N Engl J Med 2018;378:
22 CD19CAR T Induced High CR Rates in B-ALL Trials Study N (txd) Age,yrs HSCT T cell Dose Lympho depletion CR% MRD-% Survival FHCRC (20-73) 37% M/kg Cy, Flu/Cy, Cy/E 93(F) -Flu/Cy group superior 86 SCH 45 (45) 12 (1-27) 62% M/kg Cy/Flu NA EFS 51% at 12 mos 89 CHOP (1.7-24) 66% 1M- 20M/kg Any 93 88(F) RFS 55% at 12 mos OS 79% NCIped 55 (52) 13 (4-30) 19% 1-3M/kg Cy, Cy/Flu 62 LFS 56% for MRD-CR* 55 median f/u -2.2 yrs MSKCC 51(50) ELIANA 107(75) 40 (22-74) 35% 11 (3-23) 56% 1-3M/kg Cy, Cy/Flu 82 DFS 27% MRD-CR # mos 2-5M/kg or M if >50kg Cy/Flu N: number at enrollment; Txd: treated with CAR T; F: flow cytometry RFS 59% at 12 mos OS 76% at 12 mos
23 Duration of Remission, Event-free Survival, and Overall Survival. ELIANA: DOR, OS and EFS Median follow-up: 13.1 months DOR: not reached (n = 61) 8 CR patients: allohct - 2 w/mrd+ - 2 w/ B cell recovery w/i 6 mos OS 76% EFS: 50% Relapse CD19 expression + 1 pt - 15 pts unknown 4 pts SL Maude et al. N Engl J Med 2018;378:

24 A Phase 1 Trial of CD22CAR T Cells for Pediatric and Young Adults with Rel/Ref CD22+ B Cell Malignancies (NCT ) Inclusion/Exclusion Criteria Pts aged 1-30 yrs 2 lines of prior therapies 100 days if prior allohct 30 days from prior CD19CAR with < 5% CAR T by flow CNS3 not allowed Fludarabine 25 mg/m²/d IV QD x 3 Cyclophosphamide 900 mg/m²/d IV x 1 N = 21 DL1: 3 x 10 5 /kg DL2: 1 x 10 6 /kg DL3: 3 x 10 6 /kg 23 patients enrolled 1 manufacturing failure 1 DLBCL Patient Characteristics median age 19 (7-30) All had at least one allohct; 17 had prior CD19 directed therapy; 15 CD19CAR T 10 CD19dim or CD19neg blasts Median marrow blast%: 70.5% No active CNS involvement Maude, et al. NEJM. 2018;378:
 - Most are MRD-ve (9/12) - Regardless prior CD19 CAR")
25 NCI-Ped CD22CAR Trial (NCT ) Toxicity - most common AE is CRS in 16 pts, 9 grade 1 and 7 grade 2. - Neurotoxicity: transient and reversible. No seizure - 1 grade 5 death due to gram negative sepsis - B cell aplasia in all CR patients Response - CR rate 73% in DL2 + DL3 (11/15 patients) - Most are MRD-ve (9/12) - Regardless prior CD19 CAR treatment - Correlates with CAR T expansion & B cell aplasia - DOR is 6 months Nature Medicine volume 24, pages (2018)
26 NCI-ped CD22CAR trial (NCT ) Relapse - 8/12 relapsed at months - diminished CD22 Ag density in 7 of 8 relapses no mutation identified Nature Medicine volume 24, pages (2018)
 Sequential approach CD22CAR T (day 1)+ CD19CAR T (day 14/15) at Tongji Hospital, China Bivalent approach CD19/CD22 CAR T at")
27 Trials using CAR T Cells targeting both CD19 & CD22 Duotargeting approach T cells transduced with CD19CAR and CD22CAR at Seattle Children s (PLAT-05 trial) Sequential approach CD22CAR T (day 1)+ CD19CAR T (day 14/15) at Tongji Hospital, China Bivalent approach CD19/CD22 CAR T at Stanford and NCI
28 CAR T for Acute Myeloid Leukemia Targets: CD123, CD33, NKG2D - Ideal target: only on leukemic stem cells No targets with a profile as favorable as CD19 or BCMA - Clonal heterogeneicity of LSCs. - Similarity of LSC with normal stem cells. - Lack of antigens with lineage specific expression - High risk for on-target, off tumor effects
29 A Phase 1 First-in-Human Clinical Trial Using CD123 CAR T for Patients with Rel/Ref AML and BPDCN (PI: Budde, COH) Manufacturi ng of Cell product ~ 2 weeks Manufacturing time: 13 to 16 day process Turnaround time ~ 21 days Success rate: 93% (13/14 products) AML cohort: 6 patients treated BPDCN cohort: 1 patient treated Budde et al. ASH 2017



 7000 6000 5000 4000")
30 UPN 167: ref AML, 47 F, 4 prior lines of treatment and prior MRD AlloSCT (sister), 200M Donor-CAR T cell infusion D0 D1 D5 D8 Tocilizumab: D5, D6, D7 Dex:D6, D8 IVIG: D7 D6 hypoxia, intubation, BAL-> adenovirus D10 extubation Ferritin (ng/ml)




31 UPN 167: Recovery of Hematopoiesis ANC >500 on d 22 Bone marrow examination last RBC transfusion on d17 last PLT transfusion on d10


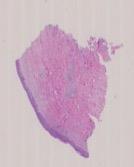


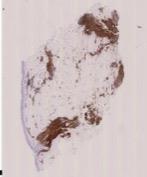
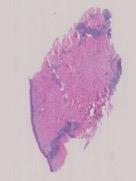


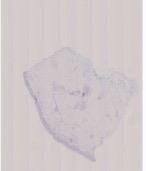






32 BPDCN Cohort: UPN 203 Pretreatment 72 y.o. man with BPDCN with disease progression after 5 cycles of SL Lymphodepletion D -5 to -3 Flu 25mg/m2/d Cy 300 mg/m2/d Pre D14 H&E CD123 CD4 CD56 CD3 Day 6 - Autologous CD123 CAR T D0, 100 x 10 6 D28 D14: skin biopsy -> NED D28: skin biopsy -> NED D28: bone marrow biopsy-> NED Budde et al. ASH 2017
33 CAR T Therapy for Acute Leukemia at COH Active Therapies for the following diseases ALL AML BPDCN CAR T Physician Team Stephen Forman Elizabeth Budde Samer Khaled Anthony Stein Guido Marcucci Joseph Rosenthal (ped) Weili Sun (ped) Ana Pawlowsky (ped) And others
34 CAR T in MM Targets: BCMA, CD19, SLAMF7 (CS1), NKG2D, CD56, CD70, CD38, CD138, CD44v6, IgKLC Study CAR/c ostim Dose + lymphodepletion Response AEs UPENN N=24 BCMA 4-1BB C1: M C2:10-50M+Cy C3: M+Cy ORR: 46% ORR in 100M: 53% gr3 CRS: 33% gr3 NT: 13% 2 DLT: gr 4 PRES 1 Gr4 hemorrhage and gr3 Cardiomyopathy CRB-401 N=21 BCMA 4-BB 50M 150M 450M 800M Flu/Cy ORR: 94% CR: 56% No DLT gr3 CRS: 10% NT: 0% Cohen AD, et al. ASH Abstract 505; Berdeja JG et al. ASH Abstract 740.
35 phase I trial of bb2121 anti-bcma CAR T- cell therapy in patients with R/R MM bb2121: 2nd-Generation Autologous T-cells transduced with lentiviral vector Anti-BCMA scfv VH α VL VL α VH R/R MM 3 prior lines of therapy or double-refractory MM >50% BCMA+ in dose escalation cohort Lymphodepletion: fludarabine 30 mg/m 2 /d x 3 cyclophosphamide 300 mg/m 2 /d x 3 Co-stim domain: 4-1BB T cell activation domain: CD3ζ 50, 150, 450, or 800 x 10 6 bb2121 CAR T-cells Berdeja JG, et al. ASH Abstract 740.
 Median time to best response, mos (range) Median time to CR, mos (range) Median duration of response, mos (range) Median PFS, mos (range) Pts (N =")
36 Pts (%) CRB-401: Depth of Response to bb2121 Over Time Responses continued to deepen in pts receiving x 10 6 CAR T-cells over median follow-up of 40 wks Outcome in Cohort CAR+ T-Cells Median time to first response, mos (range) Median time to best response, mos (range) Median time to CR, mos (range) Median duration of response, mos (range) Median PFS, mos (range) Pts (N = 18) 1.02 ( ) 3.74 ( ) 3.84 ( ) NR NR PFS at 6 mos, % 81 PFS at 9 mos, % 71 ORR in Cohorts CAR+ T-Cells ORR: 100% ORR: 94% MAY 2017 (N=15) OCT 2017 (N=18) Progression independent of tumor burden, bb2121 dose, CRS, bb2121 persistence (N = 4) CR 27% CR 56% VGPR 74% Berdeja JG et al. ASH Abstract 740. CR/sC R VGPR PR VGPR 89%
37 CRB-401: Conclusions Investigators conclude that bb2121 confers deep, durable responses at active doses ( x 10 6 CAR T cells) in heavily pretreated pts with R/R MM ORR: 94%, VGPR: 89%, CR: 56% 90% of evaluable pts MRD negative at 40 wks of follow-up PD in 4 pts; 3 of 3 evaluable patients remain BCMA positive at progression Safety profile of bb2121 manageable up to 800 x 10 6 CAR T-cell dose 2 cases of grade 3 CRS during dose escalation; resolved within 24 hours 1 case of delayed, reversible grade 4 neurotoxicity during dose expansion associated with TLS and CRS in patient with highest tumor burden Global pivotal phase II KarMMa trial evaluating bb2121 at doses of x 10 6 CAR T-cells open for enrollment (NCT ) Berdeja JG et al. ASH Abstract 740.
38 CAR T Therapy for MM at COH Targets: BCMA, CS-1 (coming) CAR T Physician Team Myo Htut Michael Rosenzweig And others
39 Chapter 3. CAR Repair Toxicity Management
40 CAR T Cell Therapy: Complications Commonly reported important adverse events On target off tumor effects, i.e. B cell aplasia (CD19CAR) Lymphodepletion chemo-related toxicity Tumor lysis syndrome Macrophage activation syndrome (HLH/MAS) Coagulopathy Cytokine release syndrome Neurotoxicity Infection

41 Cytokine Release Syndrome A constellation of inflammatory symptoms from cytokine elevations. Association with T cell activation and proliferation Association with clinical benefit and toxicity Jennifer N. Brudno, and James N. Kochenderfer Blood 2016;127:

42 Bone Marrow Blasts, % IL-6 (pg/ml) pg/ml IFNg (pg/ml) pg/ml Correlates of severe cytokine release syndrome (CRS) Temperature IL-6 IL 6 p<0.001 IFN-γ IFNg CR o NR p<0.001 No Severe CRS yes No Severe CRS Yes Temp Cytokine level: IFN-γ, IL-6 Tumor burden CAR T expansion M. L. Davila et al., Sci Transl Med 2014;6:224ra25 Maude SL et al. N Engl J Med 2014;371: N o Severe CRS P <.002 Ye s
43 CRS Grading Grade Clinical Signs and Symptoms Fever ± symptoms such as rigors, malaise, fatigue, anorexia, myalgias, arthalgias, nausea, vomiting, headache Hypotension responding to fluid resuscitation or one low dose pressor, or Hypoxia responding to 40% FiO2, or Grade 3 transaminitis, other grade 2 organ toxicity according to CTCAE v4.03 Hypotension requiring >3 hours of two pressors, or one pressor at high dose, or Hypoxia requiring >40% FiO2, or Grade 4 transaminitis, other grade 3 organ toxicity according to CTCAE v4.03 Requirement of mechanical ventilator support, or Grade 4 organ toxicity excluding grade 4 transaminitis 5 Death Lee DW et al. Blood 2014
44 CRS Management Goal: reduce serious CRS symptoms and signs, and prevent lifethreatening complications Tocilizumab is the first choice for CRS mitigation (selective grade 2, all grade 3 and 4 cases). humanized IgG1 anti-hil-6r mab, FDA approved in 8/ mg/kg iv over 1 hour x1, can repeat in 24 to 48 hours Would prophylactic tocilizumab increase safety without compromising efficacy? (likely not) What to do in tocilizumab refractory cases (no improvement after 2 doses of Tocilizumab)? - Steroids, Methylpred 2mg/kg/d or Dex 0.5mg/kg max 10mg/dose, quick taper. - Siltuximab, Etenercept, Roxilitinib, ibrutinib




45 Can result in patient death ROCKET trial: 5 cerebral edema FHCRC: 1 irreversible neurotoxicity (d10 to d122) MSKCC: 1 seizure ZUMA-1: 1 cerebral edema Neurologic Toxicity Presentation: headache, encephalopathy, delirium, aphasia, ataxia, confusion, hallucinations, headaches, tremor, seizure, obtundation. Last days to months Can occur independently from CRS or presence of CAR T cells in CSF. No correlation with CNS disease
46 Neurologic Toxicity Management Prophylaxis is common but efficacy is unknown Workup generally includes neurology consult, blood and cerebrospinal fluid analyses, neuro-imaging, and electroencephalography Gold standard of treatment is steroids Cytokine blockade can be given but its unknown if these are effective or detrimental (be cautious) Intervention is based on neurologic toxicity severity
47 Infection: Dancing with the devil Incidence: 23% FHCRC trials; 27% JULIET trial; 38% ZUMA-1; 41% ELIANA Pretreatment factors - impaired immune function - tissue damage from prior chemoregimens Treatment factors - cytopenia from lypmphodepletion, - immunosuppressive drugs such as toci/dex - ICU stay - hypogammaglobulinemia Other risk factors - ALL patients - >= 4 lines of prior therapies - Higher CAR dose - Severe CRS Hill et al.blood 2017
48 Infection: Dancing with the devil FHCRC cohort, N=133 Incidence: 23% Median Time to onset: 6 Bacterial 17% (N =22) Viral 11% (N = 11) Fungal 5% (N = 6) Fatal infection 4% ( n=5) ZUMA-1 cohort, N=108 Incidence: 38% Median Time to onset: 6 Bacterial 9% Viral 4% Unspecified 16% Severe infection 23% ID prophylaxis is recommended - lack of standard approach - autohct guideline - anti-fungal prophylaxis in pts with prior HCT Hill et al.blood 2017; Yescarta.com Budde and Zaia, Blood 2017
49 Chapter 4. CAR Service Patient Consultation
50 Patient Eligibility Considerations Timing of referral H/o AI, CVA, seizure Performance status Organ function Early referral is strongly encouraged - Product ready time 2-4 weeks unless off the shelf - Discussion of treatment strategies Might at increased risks for toxicity Excluded in trials ECOG 0-1 physically able to deal with CAR T toxicities
51 Patient Eligibility Considerations Requirement of ALC Prior CD19 treatment Prior Allogeneic HCT? Prior CAR T cut off of 100 ALC/ul in ZUMA ALC/ul in JULIET trial No impact on CD19CAR activity as long as tumor cells remain CD19+ No impact on efficacy Might increase infection risk (esp. aspergillus and viral infection) Might still respond to a different CAR T treatment CD19CAR -> CD22CAR or CTL119
52 What Is the Role of AlloHSCT if CR after CAR T Cell Therapy? - HSCT consolidation after CAR correlates with decreased relapsed rate in some studies but not others. NCI-ped B-ALL CD19CAR study Post CAR Allo Yes, N =21 Relapse (N, %) Transplant related Mortality Median LFS 2, 9% 5 (24%) Not reached 65% at 18 mos No, N=7 6, 86% N/A 4.9 months 14% at 9.8 mos OS MSKCC ALL trial, subsequent allohct did not improve OS (p = 0.8). Park et al. JCO 2017)
53 Chapter 5. CAR Improvement
 Jackson, H. J. et al. (2016) Driving CAR T-cells forward Nat. Rev. Clin. Oncol. doi:10.1038/nrclinonc.2016.36")
54 Approaches to Improve CAR T-cell Therapy More potent gene editing combination More regulated conditional switch Shorter delivery time Production time off the shelf (ips, NK- CAR, UCAR) Jackson, H. J. et al. (2016) Driving CAR T-cells forward Nat. Rev. Clin. Oncol. doi: /nrclinonc
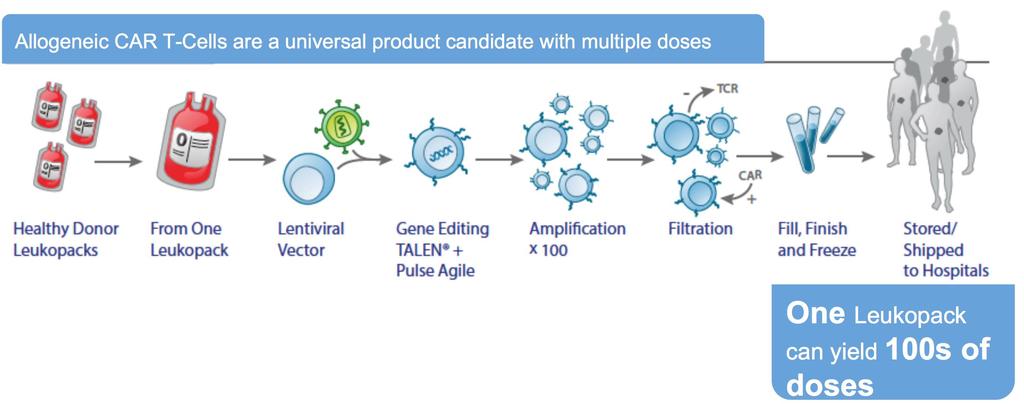
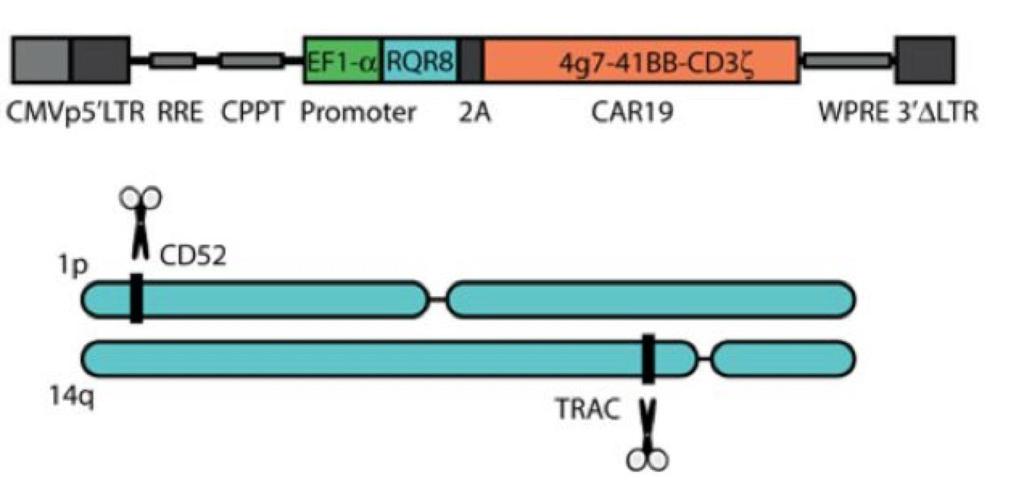
55 Off-The-Shelf UCART Cost: $4000 to 6000/treatment
56 UCART Clinical Trials Study CAR/c ostim Dose lymphodepletion Response AEs PALL N=5 CD19 4-1BB 20x10 6 or x10 6 /kg FC or FCA CRi: 100% CRS: 1gr1, 3gr2, 1gr3 GVH: 2gr1-skin NT: 0 3 died (2 PD, 1 HCT complication) CALM N=6 CD19 4-BB 6x10 6 FC or FCA CRi: 4/6 PD:1 CRS: 1 gr1, 4 gr2, 1 gr4 NT:1 gr1; GVHD: 1 gr1-skin 1 died on d15 due to gr4crs and sepsis AML N=1 CD BB 6.25x10 5 /kg FC n/a gr3 CRS, gr4cls BPDCN N=1 CD BB 6.25x10 5 /kg FC Not evaluable gr5 CRS, gr4cls gr3 lung infection Benjamin et al ASH 2017 Benjamin ASH 2017; Qasim ASH 2017; cellectis.com
57 Future Directions Bring CAR T therapy earlier in the disease treatment course - First salvage - Upfront? Can CAR T replace autologous transplant? ZUMA-7: phase 3 randomized trial, chemo-based vs CD19CAR Roles of CAR T as Maintenance - High risk patients DH-DLBCL in CR1 high risk ALL in CR1 with no donor Other indications - Follicular lymphoma, MCL, etc.
58 Conclusions Major advances have been made in the CAR T therapy. Understanding the biology and resistance mechanism is important for the design of the future versions of CARs. More non-cd19 targets are emergent. There is urgent need to design more potent, and safer CARs for patients. CAR T therapy should be given only in FACT accredited transplant centers for the time being.
59 Questions??????? Elizabeth Budde, MD, PhD Tel:
60 Quiz 1. Which of the following B-ALL patients is the best candidate to receive CD19CAR T therapy? A. 70 yo man with newly diagnosed CD19+ B-ALL, and COPD on 2L O2 at baseline, ECOG 3 B. 40 yo woman with refractory B-ALL, with CD19-ve disease after blinatumumab, ECOG 0, no comorbidities C. 30 yo man with newly diagnosed B-ALL, ECOG 0, no comorbidities D. 35 yo woman with refractory CD19+ B-ALL following a prior allohct, ECOG 1, no cormorbidities Answer: D
61 Quiz 2. Which of the following intervention is appropriate during CD19 CAR T therapy? A. Daily dexamethasone up to 4 mg per day B. Steroids should only be used in a patient with grade 4 encephalopathy if tocilizumab does not work. C. Patients can be followed on a weekly basis once they receive CAR T infusion. D. Tocilizumab is indicated if a patient develops persistent hypotension refractory to iv fluid. Answer: D
Title: Chimeric Antigen Receptor T Cell Therapy in Presenters: Lymphoma and Leukemia Date: Elizabeth Budde, MD, PhD
 Title: Chimeric Antigen Receptor T Cell Therapy in Presenters: Lymphoma and Leukemia Date: Tu m o r T c e ll Elizabeth Budde, MD, PhD Department of Hematology & HCT T Cell Therapeutics Research Laboratory
Title: Chimeric Antigen Receptor T Cell Therapy in Presenters: Lymphoma and Leukemia Date: Tu m o r T c e ll Elizabeth Budde, MD, PhD Department of Hematology & HCT T Cell Therapeutics Research Laboratory
CAR T Cell Therapy: What, When, How. Elizabeth Budde, MD, PhD Dept. of Hematology & HCT Beckman research Institute
 CAR T Cell Therapy: What, When, How Elizabeth Budde, MD, PhD Dept. of Hematology & HCT Beckman research Institute March 23, 2019 DISCLOSURES Advisory board: Promab Biotechnologies; Gilead, Roche Consultancy/Speaker
CAR T Cell Therapy: What, When, How Elizabeth Budde, MD, PhD Dept. of Hematology & HCT Beckman research Institute March 23, 2019 DISCLOSURES Advisory board: Promab Biotechnologies; Gilead, Roche Consultancy/Speaker
State of the art: CAR-T cell therapy in lymphoma
 State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
Objectives. Emily Whitehead 10/11/2018. Chimeric Antigen Recepetor T-Cells (CAR-T) CAR-T Therapy: The Past, The Present, and The Future
 CAR-T Therapy: The Past, The Present, and The Future") Objectives CAR-T Therapy: The Past, The Present, and The Future Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center Review indications for FDA approved CAR-T therapy
Objectives CAR-T Therapy: The Past, The Present, and The Future Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center Review indications for FDA approved CAR-T therapy
CAR-T Therapy: The Past, The Present, and The Future. Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center
 CAR-T Therapy: The Past, The Present, and The Future Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center Objectives Review indications for FDA approved CAR-T therapy
CAR-T Therapy: The Past, The Present, and The Future Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center Objectives Review indications for FDA approved CAR-T therapy
CAR T-Cell Therapy for Your Patients: What You Need To Know
 CAR T-Cell Therapy for Your Patients: What You Need To Know Marco L. Davila, MD, PhD Associate Member, Blood & Marrow Transplantation and Cellular Immunotherapy Medical Director Cell Therapy Facility H.
CAR T-Cell Therapy for Your Patients: What You Need To Know Marco L. Davila, MD, PhD Associate Member, Blood & Marrow Transplantation and Cellular Immunotherapy Medical Director Cell Therapy Facility H.
Exploiting the Immune System: Chimeric Antigen Receptor-T Cell Therapy for Hematologic Malignancies
 Exploiting the Immune System: Chimeric Antigen Receptor-T Cell Therapy for Hematologic Malignancies Maurice Alexander, PharmD, BCOP, CPP Clinical Specialist, Blood and Marrow Transplant UNC Bone Marrow
Exploiting the Immune System: Chimeric Antigen Receptor-T Cell Therapy for Hematologic Malignancies Maurice Alexander, PharmD, BCOP, CPP Clinical Specialist, Blood and Marrow Transplant UNC Bone Marrow
CAR T-Cell Therapy for Lymphoma: Assessing Long-Term Durability. Julie M. Vose, MD, MBA
 CAR T-Cell Therapy for Lymphoma: Assessing Long-Term Durability Julie M. Vose, MD, MBA Relevant Disclosures Research Funding: Kite Pharma/Gilead, JUNO/Celgene, Novartis Honorarium/Ad Boards: Novartis,
CAR T-Cell Therapy for Lymphoma: Assessing Long-Term Durability Julie M. Vose, MD, MBA Relevant Disclosures Research Funding: Kite Pharma/Gilead, JUNO/Celgene, Novartis Honorarium/Ad Boards: Novartis,
CAR-T CELLS: NEW HOPE FOR CANCER PATIENTS
 CAR-T CELLS: NEW HOPE FOR CANCER PATIENTS Natasha Kekre, MD, MPH, FRCPC Hematologist, Blood and Marrow Transplant Program, TOH Associate Scientist, Ottawa Hospital Research Institute Assistant Professor
CAR-T CELLS: NEW HOPE FOR CANCER PATIENTS Natasha Kekre, MD, MPH, FRCPC Hematologist, Blood and Marrow Transplant Program, TOH Associate Scientist, Ottawa Hospital Research Institute Assistant Professor
Immunocellular Therapies for Relapsed/ Refractory Heme Malignancies: A Focus on CAR T-Cell Therapy
 Immunocellular Therapies for Relapsed/ Refractory Heme Malignancies: A Focus on CAR T-Cell Therapy This transcript has been edited for style and clarity and includes all slides from the presentation. This
Immunocellular Therapies for Relapsed/ Refractory Heme Malignancies: A Focus on CAR T-Cell Therapy This transcript has been edited for style and clarity and includes all slides from the presentation. This
Chimeric Antigen Receptor - CAR T cell therapy. Frederick L. Locke, MD 2/17/2017
 Chimeric Antigen Receptor - CAR T cell therapy Frederick L. Locke, MD 2/17/2017 T cells are immune system cells that normally fight infection Each T cell recognizes a specific target T cells multiply and
Chimeric Antigen Receptor - CAR T cell therapy Frederick L. Locke, MD 2/17/2017 T cells are immune system cells that normally fight infection Each T cell recognizes a specific target T cells multiply and
CAR T CELL IMMUNOTHERAPY FOR ALL. Stephan Grupp, MD, PhD
 CAR T CELL IMMUNOTHERAPY FOR ALL Stephan Grupp, MD, PhD Disclosures Research and/or clinical trial support from Novartis, Servier, Vertex and Kite Study steering committees, consulting, or scientific advisory
CAR T CELL IMMUNOTHERAPY FOR ALL Stephan Grupp, MD, PhD Disclosures Research and/or clinical trial support from Novartis, Servier, Vertex and Kite Study steering committees, consulting, or scientific advisory
CARs vs. BiTE in ALL. David L Porter, MD Jodi Fisher Horowitz Professor University of Pennsylvania Health System Abramson Cancer Center
 CARs vs. BiTE in ALL David L Porter, MD Jodi Fisher Horowitz Professor University of Pennsylvania Health System Abramson Cancer Center Disclosure Information David L Porter Speaker and members of study
CARs vs. BiTE in ALL David L Porter, MD Jodi Fisher Horowitz Professor University of Pennsylvania Health System Abramson Cancer Center Disclosure Information David L Porter Speaker and members of study
Engineering an Immunity to Cancer: A New Era of Adoptive Cellular Therapy with Tisagenlecleucel (Kymriah) in Pediatric ALL
 in Pediatric ALL") Engineering an Immunity to Cancer: A New Era of Adoptive Cellular Therapy with Tisagenlecleucel (Kymriah) in Pediatric ALL Diana Schreier, Pharm.D., M.B.A. Pharmacy Grand Rounds October 17, 2017 2017 MFMER
Engineering an Immunity to Cancer: A New Era of Adoptive Cellular Therapy with Tisagenlecleucel (Kymriah) in Pediatric ALL Diana Schreier, Pharm.D., M.B.A. Pharmacy Grand Rounds October 17, 2017 2017 MFMER
R/R DLBCL Treatment Landscape
 An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
Applying Chimeric Antigen Receptor T cells (CAR-T) to hematologic malignancies
 to hematologic malignancies") Applying Chimeric Antigen Receptor T cells (CAR-T) to hematologic malignancies Anne W. Beaven, MD Associate Professor Duke University Medical Center Duke Debates April 21, 2017 Chimeric Antigen Receptor
Applying Chimeric Antigen Receptor T cells (CAR-T) to hematologic malignancies Anne W. Beaven, MD Associate Professor Duke University Medical Center Duke Debates April 21, 2017 Chimeric Antigen Receptor
Chimeric An+gen Receptor (CAR) Modified T Cell Therapy: Mee#ng the Unmet Need in Follicular Lymphoma
 Modified T Cell Therapy: Mee#ng the Unmet Need in Follicular Lymphoma") Chimeric An+gen Receptor (CAR) Modified T Cell Therapy: Mee#ng the Unmet Need in Follicular Lymphoma Stephen J. Schuster, M.D. Director, Lymphoma Program & Lymphoma Translational Research, Abramson Cancer
Chimeric An+gen Receptor (CAR) Modified T Cell Therapy: Mee#ng the Unmet Need in Follicular Lymphoma Stephen J. Schuster, M.D. Director, Lymphoma Program & Lymphoma Translational Research, Abramson Cancer
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities
: Cytokine release syndrome and neurological toxicities") Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
CAR T-Cell Therapy for Acute Lymphoblastic Leukemia: Identifying Appropriate Patients and Maximizing Outcomes. Shannon L.
 CAR T-Cell Therapy for Acute Lymphoblastic Leukemia: Identifying Appropriate Patients and Maximizing Outcomes Shannon L. Maude, MD, PhD CTL019 cell Lentiviral vector Anti-CD19 CAR construct CD19 Native
CAR T-Cell Therapy for Acute Lymphoblastic Leukemia: Identifying Appropriate Patients and Maximizing Outcomes Shannon L. Maude, MD, PhD CTL019 cell Lentiviral vector Anti-CD19 CAR construct CD19 Native
Abstract #163 Michael Kalos, PhD
 LONG TERM FUNCTIONAL PERSISTENCE, B CELL APLASIA AND ANTI LEUKEMIA EFFICACY IN REFRACTORY B CELL MALIGNANCIES FOLLOWING T CELL IMMUNOTHERAPY USING CAR REDIRECTED REDIRECTED T CELLS TARGETING CD19 Abstract
LONG TERM FUNCTIONAL PERSISTENCE, B CELL APLASIA AND ANTI LEUKEMIA EFFICACY IN REFRACTORY B CELL MALIGNANCIES FOLLOWING T CELL IMMUNOTHERAPY USING CAR REDIRECTED REDIRECTED T CELLS TARGETING CD19 Abstract
Reuben BENJAMIN, MD, PhD, Principal Investigator
 Preliminary Data on Safety, Cellular Kinetics and Anti Leukemic Activity of UCART19, an Allogeneic Anti-CD19 CAR T-cell Therapy in Adult and Pediatric Patients with CD19 + Relapsed/Refractory B-cell Acute
Preliminary Data on Safety, Cellular Kinetics and Anti Leukemic Activity of UCART19, an Allogeneic Anti-CD19 CAR T-cell Therapy in Adult and Pediatric Patients with CD19 + Relapsed/Refractory B-cell Acute
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities
: Cytokine release syndrome and neurological toxicities") Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
Current Applications and Future Directions of CAR-T cell therapies for B-cell Malignancies
 Current Applications and Future Directions of CAR-T cell therapies for B-cell Malignancies Nirav Shah, MD MSHP Assistant Professor of Medicine Medical College of Wisconsin 1 Financial Disclosure I currently
Current Applications and Future Directions of CAR-T cell therapies for B-cell Malignancies Nirav Shah, MD MSHP Assistant Professor of Medicine Medical College of Wisconsin 1 Financial Disclosure I currently
Conflict of Interest Natural Line of Defense: Update on Immunotherapy in Hematologic Malignancies. Immunogenicity of Cancer.
 Conflict of Interest Natural Line of Defense: Update on Immunotherapy in Hematologic Malignancies I have no professional/financial disclosures to report Katie Culos, PharmD BCOP Adult Stem Cell Transplant
Conflict of Interest Natural Line of Defense: Update on Immunotherapy in Hematologic Malignancies I have no professional/financial disclosures to report Katie Culos, PharmD BCOP Adult Stem Cell Transplant
(CAR) T Cell Therapy in Hematologic Malignancies
 T Cell Therapy in Hematologic Malignancies") Clinical Applications of Chimeric Antigen Receptor (CAR) T Cell Therapy in Hematologic Malignancies Valkal Bhatt PharmD. BCOP, BCPS Clinical Specialist Stem Cell Transplant Memorial Sloan Kettering Cancer
Clinical Applications of Chimeric Antigen Receptor (CAR) T Cell Therapy in Hematologic Malignancies Valkal Bhatt PharmD. BCOP, BCPS Clinical Specialist Stem Cell Transplant Memorial Sloan Kettering Cancer
Donor derived CD19 specific CAR + T cell therapy after haploidentical hematopoietic stem cell transplantation Laurence J.N. Cooper Hyatt Orlando
 Donor derived CD19 specific CAR + T cell therapy after haploidentical hematopoietic stem cell transplantation Laurence J.N. Cooper Hyatt Orlando International Airport Hotel December 3, 2015 (afternoon)
Donor derived CD19 specific CAR + T cell therapy after haploidentical hematopoietic stem cell transplantation Laurence J.N. Cooper Hyatt Orlando International Airport Hotel December 3, 2015 (afternoon)
REMS Program Live Training FOR TRAINING PURPOSES ONLY
 REMS Program Live Training FOR TRAINING PURPOSES ONLY This educational module contains information on selected YESCARTA -associated adverse reactions, including cytokine release syndrome and neurologic
REMS Program Live Training FOR TRAINING PURPOSES ONLY This educational module contains information on selected YESCARTA -associated adverse reactions, including cytokine release syndrome and neurologic
Chimeric Antigen Receptors (CAR)
") CAR Therapy In CLL Chimeric Antigen Receptors (CAR) 4-1BB (CD137) Costimulatory Domains: 0 1 2 PENN: 4-1BB MSKCC: CD28 USCD: CD28 Porter, D.L. et al Sci Trans Med 7:1-12, 2015 CD19 CAR T Cell Therapy For
CAR Therapy In CLL Chimeric Antigen Receptors (CAR) 4-1BB (CD137) Costimulatory Domains: 0 1 2 PENN: 4-1BB MSKCC: CD28 USCD: CD28 Porter, D.L. et al Sci Trans Med 7:1-12, 2015 CD19 CAR T Cell Therapy For
BiTE in ALL and AML. Ibrahim Aldoss, MD Assistant Professor, City of Hope Hematology and Hematopoietic Cell Transplantation
 BiTE in ALL and AML Ibrahim Aldoss, MD Assistant Professor, City of Hope Hematology and Hematopoietic Cell Transplantation Disclosure I am consultant for Helocyte and Speaker Bureau for JAZZ Immune system
BiTE in ALL and AML Ibrahim Aldoss, MD Assistant Professor, City of Hope Hematology and Hematopoietic Cell Transplantation Disclosure I am consultant for Helocyte and Speaker Bureau for JAZZ Immune system
B-Cell NHL and Hodgkin s Disease: Biologicals, Checkpoint Inhibitors, CAR-T cells
 B-Cell NHL and Hodgkin s Disease: Biologicals, Checkpoint Inhibitors, CAR-T cells Eduardo M. Sotomayor, MD Director, George Washington Cancer Center Professor, Department of Medicine George Washington
B-Cell NHL and Hodgkin s Disease: Biologicals, Checkpoint Inhibitors, CAR-T cells Eduardo M. Sotomayor, MD Director, George Washington Cancer Center Professor, Department of Medicine George Washington
Background. Outcomes in refractory large B-cell lymphoma with traditional standard of care are extremely poor 1
 2-Year Follow-Up and High-Risk Subset Analysis of ZUMA-1, the Pivotal Study of Axicabtagene Ciloleucel (Axi-Cel) in Patients with Refractory Large B Cell Lymphoma Abstract 2967 Neelapu SS, Ghobadi A, Jacobson
2-Year Follow-Up and High-Risk Subset Analysis of ZUMA-1, the Pivotal Study of Axicabtagene Ciloleucel (Axi-Cel) in Patients with Refractory Large B Cell Lymphoma Abstract 2967 Neelapu SS, Ghobadi A, Jacobson
Severe Neurotoxicity in the Phase 2 Trial of JCAR015 in Adult B-ALL (ROCKET Study): Analysis of Patient, Protocol and Product Attributes
: Analysis of Patient, Protocol and Product Attributes") Severe Neurotoxicity in the Phase 2 Trial of JCAR015 in Adult B-ALL (ROCKET Study): Analysis of Patient, Protocol and Product Attributes Mark J. Gilbert, MD Chief Medical Officer, Juno Therapeutics, Inc.
Severe Neurotoxicity in the Phase 2 Trial of JCAR015 in Adult B-ALL (ROCKET Study): Analysis of Patient, Protocol and Product Attributes Mark J. Gilbert, MD Chief Medical Officer, Juno Therapeutics, Inc.
Immune checkpoint inhibitors in lymphoma. Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust
 Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
Immunotherapy on the Horizon: Adoptive Cell Therapy
 Immunotherapy on the Horizon: Adoptive Cell Therapy Joseph I. Clark, MD, FACP Professor of Medicine Loyola University Chicago Stritch School of Medicine Maywood, IL June 23, 2016 Conflicts of Interest
Immunotherapy on the Horizon: Adoptive Cell Therapy Joseph I. Clark, MD, FACP Professor of Medicine Loyola University Chicago Stritch School of Medicine Maywood, IL June 23, 2016 Conflicts of Interest
ANCO: ASCO Highlights 2018 Hematologic Malignancies
 ANCO: ASCO Highlights 2018 Hematologic Malignancies Brian A. Jonas, M.D., Ph.D. UC Davis Comprehensive Cancer Center August 25, 2018 Brian Jonas, MD, PhD ANCO: ASCO Highlights 2018 Relevant financial relationships
ANCO: ASCO Highlights 2018 Hematologic Malignancies Brian A. Jonas, M.D., Ph.D. UC Davis Comprehensive Cancer Center August 25, 2018 Brian Jonas, MD, PhD ANCO: ASCO Highlights 2018 Relevant financial relationships
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Update: New Treatment Modalities
 ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
Abstract 861. Stein AS, Topp MS, Kantarjian H, Gökbuget N, Bargou R, Litzow M, Rambaldi A, Ribera J-M, Zhang A, Zimmerman Z, Forman SJ
 Treatment with Anti-CD19 BiTE Blinatumomab in Adult Patients With Relapsed/Refractory B-Precursor Acute Lymphoblastic Leukemia (R/R ALL) Post-Allogeneic Hematopoietic Stem Cell Transplantation Abstract
Treatment with Anti-CD19 BiTE Blinatumomab in Adult Patients With Relapsed/Refractory B-Precursor Acute Lymphoblastic Leukemia (R/R ALL) Post-Allogeneic Hematopoietic Stem Cell Transplantation Abstract
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain
 June 22-25, 2017 Madrid, Spain") Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Cytokine Release Syndrome and Neurotoxicity
 Cytokine Release Syndrome and Neurotoxicity Colette Chaney, RN,BSN,OCN Clinical Research Operations Manager Clinical Research Nurse Objectives Describe signs and symptoms of cytokine release syndrome and
Cytokine Release Syndrome and Neurotoxicity Colette Chaney, RN,BSN,OCN Clinical Research Operations Manager Clinical Research Nurse Objectives Describe signs and symptoms of cytokine release syndrome and
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA
 Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Preclinical Modeling of CART Cell and combination Immunotherapies
 Preclinical Modeling of CART Cell and combination Immunotherapies Saad S. Kenderian, MD Assistant Professor of Medicine, Immunology and Oncology Mayo Clinic College of Medicine July 19, 2017 2015 MFMER
Preclinical Modeling of CART Cell and combination Immunotherapies Saad S. Kenderian, MD Assistant Professor of Medicine, Immunology and Oncology Mayo Clinic College of Medicine July 19, 2017 2015 MFMER
Important new concerns or changes to the current ones will be included in updates of YESCARTA s RMP.
 PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN Summary of risk management plan for YESCARTA (axicabtagene ciloleucel) This is a summary of the risk management plan (RMP) for YESCARTA. The RMP details important
PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN Summary of risk management plan for YESCARTA (axicabtagene ciloleucel) This is a summary of the risk management plan (RMP) for YESCARTA. The RMP details important
IMMUNE EFFECTOR CELLS: CAR T AND OTHER CYTOTOXIC EFFECTOR CELLS OF THE IMMUNE SYSTEM
 IMMUNE EFFECTOR CELLS: CAR T AND OTHER CYTOTOXIC EFFECTOR CELLS OF THE IMMUNE SYSTEM Jennifer Peterson MSN, RN, OCN, BMTCN Jennifer Shamai MS, RN, AOCNS, BMTCN How the Experts Treat Hematologic Malignancies
IMMUNE EFFECTOR CELLS: CAR T AND OTHER CYTOTOXIC EFFECTOR CELLS OF THE IMMUNE SYSTEM Jennifer Peterson MSN, RN, OCN, BMTCN Jennifer Shamai MS, RN, AOCNS, BMTCN How the Experts Treat Hematologic Malignancies
Primer on Adoptive T cell Therapy. Saar Gill, MD, PhD University of Pennsylvania
 Primer on Adoptive T cell Therapy Saar Gill, MD, PhD University of Pennsylvania Presenter Disclosure Information Saar Gill The following relationships exist related to this presentation: Novartis, Research
Primer on Adoptive T cell Therapy Saar Gill, MD, PhD University of Pennsylvania Presenter Disclosure Information Saar Gill The following relationships exist related to this presentation: Novartis, Research
Lymphoma and CLL EHA Madrid Professor John G Gribben Centre for Haemato-Oncology Barts Cancer Institute, London, UK
 Lymphoma and CLL EHA Madrid 2017 Professor John G Gribben Centre for Haemato-Oncology Barts Cancer Institute, London, UK Conflicts of Interest J Gribben I have the following financial relationships to
Lymphoma and CLL EHA Madrid 2017 Professor John G Gribben Centre for Haemato-Oncology Barts Cancer Institute, London, UK Conflicts of Interest J Gribben I have the following financial relationships to
Chimeric antigen receptor T cell therapies for lymphoma
 Chimeric antigen receptor T cell therapies for lymphoma Jennifer N. Brudno and James N. Kochenderfer Abstract New therapies are needed for patients with Hodgkin or non-hodgkin lymphomas that are resistant
Chimeric antigen receptor T cell therapies for lymphoma Jennifer N. Brudno and James N. Kochenderfer Abstract New therapies are needed for patients with Hodgkin or non-hodgkin lymphomas that are resistant
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
4100: Cellular Therapy Essential Data Follow-Up Form
 4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
Immunotherapies in Acute Lymphoblastic Leukaemia. Professor David Ritchie Royal Melbourne Hospital
 Immunotherapies in Acute Lymphoblastic Leukaemia Professor David Ritchie Royal Melbourne Hospital Blinatumomab Cases Case 1: Mr BE 30 year old male Aged 17, diagnosed Philadelphia negative B-ALL in Nov
Immunotherapies in Acute Lymphoblastic Leukaemia Professor David Ritchie Royal Melbourne Hospital Blinatumomab Cases Case 1: Mr BE 30 year old male Aged 17, diagnosed Philadelphia negative B-ALL in Nov
Relapsed/Refractory Diffuse Large B-Cell Lymphoma John Kuruvilla, MD Princess Margaret Cancer Centre University of Toronto
 Relapsed/Refractory Diffuse Large B-Cell Lymphoma John Kuruvilla, MD Princess Margaret Cancer Centre University of Toronto Disclosures Research Support Employee Leukemia and Lymphoma Society US, Rasch
Relapsed/Refractory Diffuse Large B-Cell Lymphoma John Kuruvilla, MD Princess Margaret Cancer Centre University of Toronto Disclosures Research Support Employee Leukemia and Lymphoma Society US, Rasch
The KYMRIAH Experience
 The KYMRIAH Experience INDICATION KYMRIAH (tisagenlecleucel) is a CD19-directed genetically modified autologous T cell immunotherapy indicated for the treatment of patients up to 25 years of age with B-cell
The KYMRIAH Experience INDICATION KYMRIAH (tisagenlecleucel) is a CD19-directed genetically modified autologous T cell immunotherapy indicated for the treatment of patients up to 25 years of age with B-cell
CAR T-CELLS: ENGINEERING IMMUNE CELLS TO TREAT CANCER. Roman GALETTO, PhD 17 th Club Phase 1 Annual Meeting April 5 th Paris
 CAR T-CELLS: ENGINEERING IMMUNE CELLS TO TREAT CANCER Roman GALETTO, PhD 17 th Club Phase 1 Annual Meeting April 5 th 2018 - Paris Cellectis, 05-APR-2018 2 FORWARD-LOOKING STATEMENTS THIS PRESENTATION
CAR T-CELLS: ENGINEERING IMMUNE CELLS TO TREAT CANCER Roman GALETTO, PhD 17 th Club Phase 1 Annual Meeting April 5 th 2018 - Paris Cellectis, 05-APR-2018 2 FORWARD-LOOKING STATEMENTS THIS PRESENTATION
Treatments and Current Research in Leukemia. Richard A. Larson, MD University of Chicago
 Treatments and Current Research in Leukemia Richard A. Larson, MD University of Chicago 2 Acute (rapid progression) Myeloid Acute myeloid leukemia (AML) Acute promyelocytic leukemia (APL) Lymphoid Acute
Treatments and Current Research in Leukemia Richard A. Larson, MD University of Chicago 2 Acute (rapid progression) Myeloid Acute myeloid leukemia (AML) Acute promyelocytic leukemia (APL) Lymphoid Acute
Hematologic Malignancies: Top Ten Advances Impacting Clinical Practice
 Hematologic Malignancies: Top Ten Advances Impacting Clinical Practice Adam D. Cohen, MD Abramson Cancer Center University of Pennsylvania June 14, 2018 Please note that some of the studies reported in
Hematologic Malignancies: Top Ten Advances Impacting Clinical Practice Adam D. Cohen, MD Abramson Cancer Center University of Pennsylvania June 14, 2018 Please note that some of the studies reported in
Checkpoint Blockade in Hematology and Stem Cell Transplantation
 Checkpoint Blockade in Hematology and Stem Cell Transplantation Saad S. Kenderian, MD Assistant Professor of Medicine and Oncology Mayo Clinic College of Medicine October 14, 2016 2015 MFMER slide-1 Disclosures
Checkpoint Blockade in Hematology and Stem Cell Transplantation Saad S. Kenderian, MD Assistant Professor of Medicine and Oncology Mayo Clinic College of Medicine October 14, 2016 2015 MFMER slide-1 Disclosures
Society for Immunotherapy of Cancer (SITC)
") Society for Immunotherapy of Cancer (SITC) Current Status of Chimeric and Adoptive T cell Therapy Lawrence G. Lum, MD, DSc Karmanos Cancer Institute and Wayne State University Advances in Cancer Immunotherapy
Society for Immunotherapy of Cancer (SITC) Current Status of Chimeric and Adoptive T cell Therapy Lawrence G. Lum, MD, DSc Karmanos Cancer Institute and Wayne State University Advances in Cancer Immunotherapy
NY-ESO SPEAR T-cells in Synovial Sarcoma
 NY-ESO SPEAR T-cells in Synovial Sarcoma ASCO Update June 6, 2017 Disclaimer This presentation contains forward-looking statements, as that term is defined under the Private Securities Litigation Reform
NY-ESO SPEAR T-cells in Synovial Sarcoma ASCO Update June 6, 2017 Disclaimer This presentation contains forward-looking statements, as that term is defined under the Private Securities Litigation Reform
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham
 Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
ASCO Analyst & Investor Webcast. June 1, 2018
 ASCO Analyst & Investor Webcast June 1, 2018 June 1, 2018 NASDAQ: BLUE Forward Looking Statements These slides and the accompanying oral presentation contain forward-looking statements and information
ASCO Analyst & Investor Webcast June 1, 2018 June 1, 2018 NASDAQ: BLUE Forward Looking Statements These slides and the accompanying oral presentation contain forward-looking statements and information
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES!
 Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Allogeneic Hematopoietic Stem Cell Transplantation: State of the Art in 2018 RICHARD W. CHILDS M.D. BETHESDA MD
 Allogeneic Hematopoietic Stem Cell Transplantation: State of the Art in 2018 RICHARD W. CHILDS M.D. BETHESDA MD Overview: Update on allogeneic transplantation for malignant and nonmalignant diseases: state
Allogeneic Hematopoietic Stem Cell Transplantation: State of the Art in 2018 RICHARD W. CHILDS M.D. BETHESDA MD Overview: Update on allogeneic transplantation for malignant and nonmalignant diseases: state
Disclosure. Study was sponsored by Karyopharm Therapeutics No financial relationships to disclose Other disclosures:
 Combination of Selinexor with High-Dose Cytarabine and Mitoxantrone for Remission Induction in Acute Myeloid Leukemia is Feasible and Tolerable A Phase I Study (NCT02573363) Amy Y. Wang, Howie Weiner,
Combination of Selinexor with High-Dose Cytarabine and Mitoxantrone for Remission Induction in Acute Myeloid Leukemia is Feasible and Tolerable A Phase I Study (NCT02573363) Amy Y. Wang, Howie Weiner,
What should I ask my treatment team?
 TREATMENT TRANSFORMED Child portrayed is not a real KYMRIAH patient. DISCUSSION GUIDE What should I ask my treatment team? Making treatment decisions for relapsed or refractory cancer can be hard. Asking
TREATMENT TRANSFORMED Child portrayed is not a real KYMRIAH patient. DISCUSSION GUIDE What should I ask my treatment team? Making treatment decisions for relapsed or refractory cancer can be hard. Asking
What is the best approach to the initial therapy of PTCL? standards of treatment? Should all
 What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
CD19 Chimeric Antigen Receptor Therapy for Refractory Aggressive B-Cell Lymphoma
 biology of neoplasia CD19 Chimeric Antigen Receptor Therapy for Refractory Aggressive B-Cell Lymphoma Caron A. Jacobson, MD 1 ABSTRACT PURPOSE Anti-CD19 directed chimeric antigen receptor (CAR) T-cell
biology of neoplasia CD19 Chimeric Antigen Receptor Therapy for Refractory Aggressive B-Cell Lymphoma Caron A. Jacobson, MD 1 ABSTRACT PURPOSE Anti-CD19 directed chimeric antigen receptor (CAR) T-cell
What are the hurdles to using cell of origin in classification to treat DLBCL?
 What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
ACUTE LYMPHOBLASTIC LEUKEMIA
 ACUTE LYMPHOBLASTIC LEUKEMIA YOUNG ADULT PATIENT Highlights clonoseq Tracking (MRD) Testing in the peripheral blood revealed early signs of relapse post-transplant Patient achieved remission after CAR-T
ACUTE LYMPHOBLASTIC LEUKEMIA YOUNG ADULT PATIENT Highlights clonoseq Tracking (MRD) Testing in the peripheral blood revealed early signs of relapse post-transplant Patient achieved remission after CAR-T
Ohio State University, Columbus, OH.
 Complete Responses in Relapsed/ Refractory Acute Myeloid Leukemia (AML) Patients on a Weekly Dosing Schedule of XmAb 14045, a CD123 x CD3 T Cell-Engaging Bispecific Antibody: Initial Results of a Phase
Complete Responses in Relapsed/ Refractory Acute Myeloid Leukemia (AML) Patients on a Weekly Dosing Schedule of XmAb 14045, a CD123 x CD3 T Cell-Engaging Bispecific Antibody: Initial Results of a Phase
ANCO 2015: Treatment advances in acute leukemia
 ANCO 2015: Treatment advances in acute leukemia Michaela Liedtke, MD Stanford, CA September 12, 2015!" Disclosures Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Steering Committee
ANCO 2015: Treatment advances in acute leukemia Michaela Liedtke, MD Stanford, CA September 12, 2015!" Disclosures Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Steering Committee
Living Well with Myeloma Teleconference Series Thursday, March 24 th :00 PM Pacific/5:00 PM Mountain 6:00 PM Central/7:00 PM Eastern
 Living Well with Myeloma Teleconference Series Thursday, March 24 th 216 4: PM Pacific/5: PM Mountain 6: PM Central/7: PM Eastern Speakers Dr. Brian Durie, IMF Chairman Cedars Sinai Samuel Oschin Cancer
Living Well with Myeloma Teleconference Series Thursday, March 24 th 216 4: PM Pacific/5: PM Mountain 6: PM Central/7: PM Eastern Speakers Dr. Brian Durie, IMF Chairman Cedars Sinai Samuel Oschin Cancer
Management of high-risk diffuse large B cell lymphoma: case presentation
 Management of high-risk diffuse large B cell lymphoma: case presentation Daniel J. Landsburg, MD Assistant Professor of Clinical Medicine Perelman School of Medicine University of Pennsylvania January
Management of high-risk diffuse large B cell lymphoma: case presentation Daniel J. Landsburg, MD Assistant Professor of Clinical Medicine Perelman School of Medicine University of Pennsylvania January
Linfoma de Hodgkin. Novos medicamentos. Otavio Baiocchi CRM-SP
 Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Reduced-intensity Conditioning Transplantation
 Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Biogen Idec Oncology Pipeline. Greg Reyes, MD, PhD SVP, Oncology Research & Development
 Biogen Idec Oncology Pipeline Greg Reyes, MD, PhD SVP, Oncology Research & Development March 25, 2009 Biogen Idec Strategy in Lymphoma / Leukemia CLL RITUXAN NHL FC-RITUXAN GA101 RITUXAN-CVP RITUXAN-CHOP
Biogen Idec Oncology Pipeline Greg Reyes, MD, PhD SVP, Oncology Research & Development March 25, 2009 Biogen Idec Strategy in Lymphoma / Leukemia CLL RITUXAN NHL FC-RITUXAN GA101 RITUXAN-CVP RITUXAN-CHOP
-- Manufacturing Success Rate of 99 Percent in ZUMA-1 Pivotal Trial with a Median 17 Day Turnaround Time --
 Kite s Yescarta (Axicabtagene Ciloleucel) Becomes First CAR T Therapy Approved by the FDA for the Treatment of Adult Patients With Relapsed or Refractory Large B-Cell Lymphoma After Two or More Lines of
Kite s Yescarta (Axicabtagene Ciloleucel) Becomes First CAR T Therapy Approved by the FDA for the Treatment of Adult Patients With Relapsed or Refractory Large B-Cell Lymphoma After Two or More Lines of
Stem Cell Sources 2/22/13. Cellular Therapy Today and Tomorrow. Cellular Therapy in HCT. Bone Marrow
 2/22/13 Cellular Therapy Today and Tomorrow Robert S. Negrin, MD Division Chief, Stanford Bone and Marrow Transplant Program Professor of Medicine Cellular Therapy in Clinical Medicine Established Hematopoietic
2/22/13 Cellular Therapy Today and Tomorrow Robert S. Negrin, MD Division Chief, Stanford Bone and Marrow Transplant Program Professor of Medicine Cellular Therapy in Clinical Medicine Established Hematopoietic
Engineered TCR and CAR Immunotherapeutics 2015:
 : A comparative analysis of the landscape of and business opportunities with TCR and CAR antibodies, T cells, NK cells, TILs, DLIs and CTLs released by La Merie Publishing on March 10, 2015 La Merie Publishing
: A comparative analysis of the landscape of and business opportunities with TCR and CAR antibodies, T cells, NK cells, TILs, DLIs and CTLs released by La Merie Publishing on March 10, 2015 La Merie Publishing
An Introduction to Bone Marrow Transplant
 Introduction to Blood Cancers An Introduction to Bone Marrow Transplant Rushang Patel, MD, PhD, FACP Florida Hospital Medical Group S My RBC Plt Gran Polycythemia Vera Essential Thrombocythemia AML, CML,
Introduction to Blood Cancers An Introduction to Bone Marrow Transplant Rushang Patel, MD, PhD, FACP Florida Hospital Medical Group S My RBC Plt Gran Polycythemia Vera Essential Thrombocythemia AML, CML,
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Summary of Key AML Abstracts Presented at the American Society of Hematology (ASH) December 2-6, San Diego CA
 December 2-6, San Diego CA") Summary of Key AML Abstracts Presented at the American Society of Hematology (ASH) December 2-6, 2016 - San Diego CA ASH 2016 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://ash.confex.com/ash/2016/webprogram/start.html
Summary of Key AML Abstracts Presented at the American Society of Hematology (ASH) December 2-6, 2016 - San Diego CA ASH 2016 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://ash.confex.com/ash/2016/webprogram/start.html
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Lecture 17: Vaccines (Therapeutic and Prophylactic Types)
") Lecture 17: Vaccines (Therapeutic and Prophylactic Types) Therapeutic vaccines Bacillus Calmette Guerin (BCG; TheraCys) Very old agent initially developed as vaccine for MTB. Uses: Superficial bladder
Lecture 17: Vaccines (Therapeutic and Prophylactic Types) Therapeutic vaccines Bacillus Calmette Guerin (BCG; TheraCys) Very old agent initially developed as vaccine for MTB. Uses: Superficial bladder
2018 KSMO Immune Oncology Forum. Immune checkpoint inhibitors in hematologic. malignancies: evidences and perspectives 서울아산병원종양내과 홍정용
 2018 KSMO Immune Oncology Forum Immune checkpoint inhibitors in hematologic malignancies: evidences and perspectives 서울아산병원종양내과 홍정용 2018-07-18 Contents Introduction Immune checkpoint inhibtors in lymphomas
2018 KSMO Immune Oncology Forum Immune checkpoint inhibitors in hematologic malignancies: evidences and perspectives 서울아산병원종양내과 홍정용 2018-07-18 Contents Introduction Immune checkpoint inhibtors in lymphomas
Current Strategies for Relapsed/Refractory ALL in AYAs and Adults: Where We Are Now
 Current Strategies for Relapsed/Refractory ALL in AYAs and Adults: Where We Are Now Eunice S. Wang, MD Roswell Park Cancer Institute Buffalo, New York, United States Relapsed ALL Carries a Poor Prognosis
Current Strategies for Relapsed/Refractory ALL in AYAs and Adults: Where We Are Now Eunice S. Wang, MD Roswell Park Cancer Institute Buffalo, New York, United States Relapsed ALL Carries a Poor Prognosis
National Institute for Health and Care Excellence. Single Technology Appraisal (STA)
") Single Technology Appraisal (STA) Tisagenlecleucel-T for previously treated B-cell acute lymphoblastic Response to consultee and commentator comments on the draft remit and draft scope (pre-referral) Please
Single Technology Appraisal (STA) Tisagenlecleucel-T for previously treated B-cell acute lymphoblastic Response to consultee and commentator comments on the draft remit and draft scope (pre-referral) Please
Adoptive cell therapy and modulation of the tumour microenvironment: new insights from ASCO 2016
 Adoptive cell therapy and modulation of the tumour microenvironment: new insights from ASCO 2016 Leila Khoja 1,2 and Bishal Gyawali 3 1 Royal Free Hospital, Pond Street, London NW3 2QG, UK. 2 Astrazeneca
Adoptive cell therapy and modulation of the tumour microenvironment: new insights from ASCO 2016 Leila Khoja 1,2 and Bishal Gyawali 3 1 Royal Free Hospital, Pond Street, London NW3 2QG, UK. 2 Astrazeneca
Cytokine Release Syndrome and Neurotoxicity: Ongoing Efforts to Enhance Safety. Sattva S. Neelapu, MD
 Cytokine Release Syndrome and Neurotoxicity: Ongoing Efforts to Enhance Safety Sattva S. Neelapu, MD Disclosures Research support from Kite, Merck, BMS, Cellectis, Poseida, Karus, Acerta Advisory Board
Cytokine Release Syndrome and Neurotoxicity: Ongoing Efforts to Enhance Safety Sattva S. Neelapu, MD Disclosures Research support from Kite, Merck, BMS, Cellectis, Poseida, Karus, Acerta Advisory Board
Targeted Radioimmunotherapy for Lymphoma
 Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
One Day BMT Course by Thai Society of Hematology. Management of Graft Failure and Relapsed Diseases
 One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
How to Integrate the New Drugs into the Management of Multiple Myeloma
 How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
Bendamustine for Hodgkin lymphoma. Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service
 Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
BCMA-specific CAR T cells for Myeloma
 BCMA-specific CAR T cells for Myeloma Adam D. Cohen, MD Abramson Cancer Center University of Pennsylvania October 14, 2017 Chimeric antigen receptors - background w Combines recognition domain of antibody
BCMA-specific CAR T cells for Myeloma Adam D. Cohen, MD Abramson Cancer Center University of Pennsylvania October 14, 2017 Chimeric antigen receptors - background w Combines recognition domain of antibody
Summary... 2 IMMUNOTHERAPY IN CANCER... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 IMMUNOTHERAPY IN CANCER... 3 Sequencing analysis reveals baseline tumour T cell receptor and neo antigen load associates
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 IMMUNOTHERAPY IN CANCER... 3 Sequencing analysis reveals baseline tumour T cell receptor and neo antigen load associates
SUPPLEMENTAL APPENDIX
 SUPPLEMENTAL APPENDIX Table of Contents 1. Supplemental Tables 2. Supplemental Figures Nature Medicine: doi:1.138/nm.4441 Supplemental Table 1. Baseline Characteristics of Patients Treated with anti-cd22
SUPPLEMENTAL APPENDIX Table of Contents 1. Supplemental Tables 2. Supplemental Figures Nature Medicine: doi:1.138/nm.4441 Supplemental Table 1. Baseline Characteristics of Patients Treated with anti-cd22
Tumor Antigens in the Age of Engineered T cell Therapies
 Tumor Antigens in the Age of Engineered T cell Therapies September 30 th 2016 ESMO Preceptorship Course Amsterdam Carsten Linnemann, PhD Senior Scientist Kite Pharma EU B.V. Amsterdam Forward Looking Statements/Safe
Tumor Antigens in the Age of Engineered T cell Therapies September 30 th 2016 ESMO Preceptorship Course Amsterdam Carsten Linnemann, PhD Senior Scientist Kite Pharma EU B.V. Amsterdam Forward Looking Statements/Safe
Kymriah. Kymriah (tisagenlecleucel) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.101 Subject: Kymriah Page: 1 of 5 Last Review Date: September 20, 2018 Kymriah Description Kymriah
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.101 Subject: Kymriah Page: 1 of 5 Last Review Date: September 20, 2018 Kymriah Description Kymriah