Lipid Update and Case Studies: Comparing ATP III, AHA/ACC Guidelines and the National Lipid Association Recommendations 2017
|
|
|
- Abner Patrick
- 5 years ago
- Views:
Transcription
1 Lipid Update and Case Studies: Comparing ATP III, AHA/ACC Guidelines and the National Lipid Association Recommendations 2017 Chad Link, DO FACC Cardiologist Chairman Cardiology Section Sparrow TCI
2 Disclosures Speakers Bureau Actelion Pharmaceuticals, Bristol-Myers Squibb, Pfizer Clinical Research Support Sanofi Aventis
3 Patient Case #1-54 year old Hispanic male with type 2 diabetes, hypertension and CAD presents for an initial visit. He quit smoking 2 years ago and follows a low-calorie diet. - Medications: lisinopril 10 mg daily, atorvastatin 40 mg daily and aspirin 81 mg daily - Lipid Profile: TC 180 mg/dl, LDL-C 110 mg/dl, HDL-C 40 mg/dl, TG 150 mg/dl, LFTs NL
4 Patient Case #1 Is this patient to goal? What would be your recommendations? (54 Year Old, DM, CAD) (TC 180 mg/dl, LDL-C 110 mg/dl, HDL-C 40 mg/dl, TG 150 mg/dl on atorvastatin 20 mg) A. Continue current therapy. (ACC/AHA Guidelines) B. Adjust or change statin to a goal LDL of < 70 mg/dl (High risk patient- NLA Guidelines) C.Add additional lipid agents to regimen. D.Consider alternative therapy
5 Patient Case #1 Having determined his therapeutic LDL goal of < 70 mg/dl, how do you treat his hyperlipidemia? (54 Year Old, DM, CAD) (TC 180 mg/dl, LDL-C 110 mg/dl, HDL-C 40 mg/dl, TG 150 mg/dl on atorvastatin 20 mg) A. Continue atorvastatin 40 mg daily (ACC/AHA Guidelines) B. Increase to atorvastatin 80 mg daily (NLA Guidelines) C.Add ezetimibe 10 mg to atorvastatin 40 mg daily (NLA) D.Add niacin 1000 mg to atorvastatin 40 mg daily (NLA) E. Change to rosuvastatin 40 mg daily (NLA) F. Add alirocumab 75 mg 2x monthly to atorvastatin 40 mg daily
6 Objectives - Review Current Guidelines and Recommendations from the ACC/AHA, AACE and the National Lipid Association - Discuss Emerging Therapies in the Treatment of Hyperlipidemia - Case Studies
7 Summary of Recommendations - ATP III Summary ACC/AHA Guidelines - National Lipid Association lipid management approaches for ASCVD prevention
8 National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) Guidelines U.S. guidelines for the detection, evaluation, and treatment of hyperlipidemia in adults Developed by an expert panel for the National Heart, Lung, and Blood Institute (NHLBI) Division of National Institutes of Health (NIH) Long history of developing clinical practice guidelines First JNC report published 1976 ATP release history: ATP I First released in 1988 ATP II 1993 (LDL goal < 100 mg/dl) ATP III 2001 (LDL goal < 100 mg/dl and FRS)
9 U.S. Guidelines for Management of Dyslipidemias 2001 NCEP ATP III guidelines (TG < 150, DM CV risk, non HDL) 2004 NCEP ATP III implications ( LDL < 70 mg/dl optional) 2008 ADA/ACCF Consensus Statement on Lipoprotein Management in Patients with Cardiometabolic Risk ( LDL < 70 mg/dl) 2011 AHA/ACC guidelines for secondary prevention ( LDL < 70 mg/dl for high risk patients) 2012 AACE Guidelines for the Management of Dyslipidemia and Prevention of Atherosclerosis 2013 ATP IV Recommendations 2013 National Lipid Association Recommendations AACE = American Association of Clinical Endocrinologists, ACC = American College of Cardiology, ACCF = American College of Cardiology Foundation, ADA = American Diabetes Association, AHA= American Heart Association
10 ATP III Classification of Cholesterol Concentrations Lipoprotein Concentration (mg/dl) Interpretation TC < LDL-c < Desirable Borderline high High Optimal Near/above optimal Borderline high High Very high HDL-c <40 60 TG < Low High Normal Borderline high High Very high

11 ATP III Classification of Cholesterol Concentrations
12 ATP III Treatment Targets Primary Target: LDL-c Secondary Target: Non-HDL-c (Once LDL goal met and if TG 200) Exception: TG lowering is an immediate target if 500 mg/dl
13 NCEP ATP III: Determining LDL-c Goals Presence of ASCVD, DM <-YES NO-> 2 major CV risk factors* 10-year CHD risk: FRS High-Risk: <100mg/dL, optional <70mg/dL >20% 10-20% <10% High-Risk: <100mg/dL Mod-high Risk: <130mg/dL, optional <100mg/dL Moderate risk <130mg/dL Lower risk <160mg/dL
14 Major Studies Published Since 2001 Statin Trials - HPS - PROVE-IT - ASCOT - PROSPER - ALLHAT - TNT Non-Statin Trials - 2 Niacin trials - 2 Fibrate Trials - IMPROVE IT - Fourier Guidelines Update AT-4 -Finally! Seth Bilazarian, MD Theheart.org and Medscape.
15 ATP IV Guidelines 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults.
16 Scope of Guideline To identify whom to treat, with what treatment(s), and to consider how intensively the treatments should be used The recommendations were designed to be easy to use in the clinical setting The report does not provide for a comprehensive approach to the detection, evaluation, and treatment of lipid disorders as was done in the prior ATP III Report Guidelines Update AT-4 -Finally! Seth Bilazarian, MD Theheart.org and Medscape.
17 ACC/AHA (With NHLBI) Guidelines: 4 New Guidelines - Cholesterol Management - Risk assessment - Obesity - Lifestyle recommendations Guidelines Update AT-4 -Finally! Seth Bilazarian, MD Theheart.org and Medscape.
18 Atherosclerotic Disease Risk: What s new? CVA/ TIA (presumed to be atherosclerotic in origin) risk added to MI (especially important for African Americans and women) Newly developed race and sex specific equations Considered other markers. Did not add any. none merited inclusion. Four markers may be considered if uncertainty persists after use of equation. Family History (if known first degree relative male <55 or female <65) Hs-CRP (2 mg/l) CAC- strongest evidence is for this marker (300 Agatston units) ABI (< 0.9) Guidelines Update AT-4 -Finally! Seth Bilazarian, MD Theheart.org and Medscape.
19 Four Major Statin Benefit Groups 1. Does the patient have a history of heart disease (ASCVD) or stroke? 2. Is the LDL > 190 mg/dl? Do they have Familial Hyperlipidemia 3. Does the patient have DM, years old with an LDL of mg/dl without ASCVD? 4. Does the patient without DM or ASCVD have a global risk score > 7.5% for primary prevention of risk assessment?
20 ACC/AHA Statin Benefit Groups H=High intensity statin; M=Moderate intensity statin Individuals with clinical ASCVD without New York Heart Association class II-IV heart failure or receiving hemodialysis (H preferred; M if age >75 or if not candidate for H). Individuals with primary elevations of LDL-C 190 mg/dl (H preferred; M if not candidate for H). Individuals age years with diabetes, and LDL-C mg/dl without clinical ASCVD (M if 10 yr risk <7.5%; H if 7.5%). Individuals without clinical ASCVD or diabetes, who are age years with LDL-C mg/dl, and have an estimated 10-year ASCVD risk of 7.5% using Pooled Cohort Equations (M or H). Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
 Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin 20 40 mg Simvastatin 80 mg* Pravastatin 40 (80) mg Lovastatin 40 mg")
21 High- and Moderate-Intensity Daily Statin Therapy High Intensity (Lowers LDL-C 50%) Atorvastatin mg Rosuvastatin mg Bold = Tested in RCT and reviewed by Expert Panel Orange= Not tested in RCT reviewed by Expert Panel Moderate Intensity (Lowers LDL-C 30-50%) Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin mg Simvastatin 80 mg* Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg 2x/day Pitavastatin 2 4 mg Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
22 Efficacy of Intensive Lowering of LDL-C in Subjects with Low Baseline LDL-C Meta-analysis of RCT s of >1000 participants and 2 years treatment duration of more versus less intense statin trials involving 169,138 subjects The major vascular event reduction, among in those with baseline LDL-C <77mg/dL per further 39 mg/dl reduction was 29% (99% CI 2-48, p=0.007); in those with baseline LDL-C <70 mg/dl, similar reduction in LDL-C continued to demonstrate MVE reduction (RR 0.63, 99% CI , p=0.004). Cholesterol Treatment Trialists Collaboration. Lancet 2010;376: Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
23 ACC/AHA Perspective on Statin Therapy Statin intensity trials showed clear benefit for high intensity versus moderate intensity statins Because fixed doses, not dosage titrations, were employed, one should not assume that a dosage titration strategy is correct or that addition of nonstatins to achieve low LDL-C is indicated Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
24 ACC/AHA Perspective on Non-Statin Lipid Drug Therapy Non-statin drugs without demonstrated ASCVD risk reduction may favorably alter lipids but have an unfavorable risk/benefit ratio Niacin in AIM-HIGH and HPS-2 THRIVE Fibrates in ACCORD-Lipid, FIELD Lack of ASCVD event end-point data on ezetimibe CETP inhibitors torcetrapib and dalcetrapib The use of non-statin drugs should generally be avoided Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
25 Risk Calculators ACC/AHA Use Pooled Cohort Risk calculator in non- Hispanic Whites and non-hispanic African Americans age without ASCVD and not on statin therapy; may be considered in other populations Assessment of lifetime risk may be considered in those aged with no ASCVD and not at high short-term risk Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA

26
27 ACC/AHA Risk Calculator: Possible Overtreatment in Older Patients? Age Total cholesterol HDL cholesterol Systolic BP Treatment for HBP Diabetes Smoker 10-year ASCVD risk 60 AA No No No 7.5% 65 AA No No No 7.5% 60 C No No No 7.5% Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
28 CHD Events (%) CHD Event Rates in Secondary Prevention and ACS Trials y = x R² = p < HPS-P 4S-S LIPID-P HPS-S A2Z 20 CARE-P A2Z 80 TNT 10 LIPID-S PROVE-IT-AT TNT 80 IDEAL S20/40 IDEAL CARE-S A80 PROVE-IT-PR 4S-P LDL Cholesterol (mg/dl) Updated from - O Keefe, J. et al., J Am Coll Cardiol 2004;43:

29 Very Low LDL-C and Non-HDL-C in Statin Trials and Major CVD Event Risk On Treatment LDL- C, Non-HDL-C mg/dl Boekholdt et al. JACC 2014;64: Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
30 Recent Coronary IVUS Progression Trials Relationship between LDL-C and Progression Rate CAMELOT placebo REVERSAL pravastatin Median Change In Percent Atheroma Volume (%) Nissen S. JAMA REVERSAL atorvastatin ASTEROID rosuvastatin A-Plus placebo ACTIVATE placebo r 2 = 0.95 p< Mean Low-Density Lipoprotein Cholesterol (mg/dl)
31 CHD Events (%) CHD Event Rates in Secondary Prevention and ACS Trials y = x R² = p < HPS-P 4S-S LIPID-P HPS-S A2Z 20 CARE-P A2Z 80 TNT 10 LIPID-S PROVE-IT-AT TNT 80 IDEAL S20/40 IDEAL CARE-S A80 PROVE-IT-PR IMPROVE-IT 4S-P LDL Cholesterol (mg/dl) Updated from - O Keefe, J. et al., J Am Coll Cardiol 2004;43:
32 IMProved Reduction of Outcomes: Vytorin Efficacy International Trial A Multicenter, Double-Blind, Randomized Study to Establish the Clinical Benefit and Safety of Vytorin (Ezetimibe/Simvastatin Tablet) vs Simvastatin Monotherapy in High-Risk Subjects Presenting With Acute Coronary Syndrome
33 . National Lipid Association Guidelines
34 Overview of the NLA Recommendations 1. All preventive therapy begins with risk assessment and a provider-patient discussion of the pros and cons of therapy 2. Lifestyle therapy is at the basis of all ASCVD preventive recommendations, regardless of baseline risk 3. Judicious use of evidence-based drug therapy, particularly moderate and high-dose statins, is associated with optimal ASCVD risk reduction 4. When excessive circulating atherogenic cholesterol (non- HDL-cholesterol and LDL cholesterol) persists after appropriate lifestyle and statin therapy, the use of non-statin therapy may be considered 5. Long-term follow-up fostered by provider-patient communication is essential for optimal ASCVD prevention Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
35 NLA Risk ASCVD Category Risk Category Criteria Criteria Very High ASCVD Diabetes mellitus (type 1 or 2) 2 other major ASCVD risk factors; or Evidence of end-organ damage High 3 major ASCVD risk factors Diabetes mellitus (type 1 or 2) 0-1 other major ASCVD risk factor, and no evidence of end-organ damage Chronic kidney disease Stage 3B or 4 LDL-C 190 or non-hdl-c 220 mg/dl Moderate 2 major ASCVD risk factors For specific clinical features, high quantitative risk score or specific biomarker levels, consider reclassification to high risk Low 0-1 major ASCVD risk factor For specific clinical features, consider reclassification to moderate risk
36 NLA ASCVD Risk Categories, Levels for Consideration of Drug Therapy and Treatment Goals Risk Category Consider Drug Therapy Treatment Goal Very-high High Moderate Low Non-HDL-C /LDL-C Goal (mg/dl) Non-HDL-C/LDL-C Goal (mg/dl) <100 <70 <130 <100 <130 <100 <130 <100 For patients with ASCVD or diabetes mellitus, consider use of moderate or high intensity statins, irrespective of baseline atherogenic cholesterol levels. Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
37 NLA Perspective on Statin Therapy Statin therapy is the most potent and evidencebased approach to lowering atherogenic lipoproteins (non-hdl-c and LDL-C) Statin intensity trials showed clear benefit for high-intensity versus moderate-intensity statins Broad-based evidence supports lower is better concept, and provides an opportunity for clinicians to address residual risk above that addressed by appropriately-dosed statin therapy Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
38 NLA Perspective on Non-Statin Lipid Drug Therapy If non-hdl-c and LDL-C goals are not achieved with maximal tolerated statin therapy, the addition of nonstatin therapy should be considered to lower atherogenic cholesterol levels and to achieve goals Doctors can be instructed not to use niacin in patients on aggressive statin regimens As ezetimibe is safe and lowers atherogenic cholesterol, its use may be considered in selected patients with elevated non-hdl-c and/or LDL-C Resins may be considered in selected patients Meta-analyses of fibrate therapy in subgroups with atherogenic dyslipidemia suggest ASCVD risk reduction Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
39 Evidence Base: Summary ACC/AHA By limiting the scope to RCT of statins and metaanalyses of RCT, only the highest level of evidence on statins in defined populations is employed to assess ASCVD outcomes NLA By including evidence from RCT and other sources, a broader evidence base for clinical decision making is employed. This approach is consistent with the perspective of previous NCEP ATP s and the international community Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
40 Lipid Guideline Controversies: Common Threads Between ACC/AHA and NLA Lifestyle therapy is warranted for ASCVD risk reduction, whether or not drug therapy is used Patients with ASCVD, FH and diabetes are candidates for moderate or high-dose statins Risk calculators aid in, but do not take the place of clinical judgment Whether or not lipid goals are set, regular lipid follow-up is warranted to assess adherence Patient engagement in preventive care decision making aids in long-term adherence Lipid Guideline Controversies in 2014: The Decision is Yours Carl E. Orringer, MD, FACC, FNLA
41 Current problem Despite the widespread availability of statins, many patients fail to reach recommended LDL-C targets in clinical practice, even in combination with other lipid lowering agents and are unable achieve an LDL < 70 mg/dl. Numerous patients are often intolerant to statins and or high intensity statins due to various side effects (muscle aches, etc.)
42 Emerging Therapies PCSK9 Inhibitors.
43 Background: PCSK9 Inhibition PCSK 9 inhibitors are fully human monoclonal antibodies against PCSK9 which reduced LDL-C by up to 65% and was well tolerated in multiple randomized, placebo-controlled, phase 2 clinical trials of 12 weeks duration in over 1300 hypercholesterolemic patients. 1-4 The PCSK9 inhibitors are a new class of drugs that have been shown to dramatically lower LDL cholesterol levels. PCSK9 inhibitors are monoclonal antibodies (MABs). They inactivate a protein in the liver called proprotein convertase subtilisin kexin 9 (PCSK9). PCSK9 itself inactivates the needed receptors on the liver cell surface that transport LDL into the liver for metabolism (break down). Without these receptors, more LDL ("bad" cholesterol) remains in the blood. So, by inactivating PCSK9 via inhibition, more receptors are available to capture LDL for metabolism and removal from the blood.(5) 1. Lancet. 2012;380: Circulation. 2012;126: JAMA. 2012;308: Lancet. 2012;380:
44 LDL Receptor Function and Life Cycle For illustration purposes only Clinicaltrials.gov no. NCT

45 The Role of PCSK9 in the Regulation of LDL Receptor Expression For illustration purposes only Clinicaltrials.gov no. NCT
46 Impact of an PCSK9 mab on LDL Receptor Expression For illustration purposes only Clinicaltrials.gov no. NCT
47 LDL-C Mean ( SE) % Change from Baseline Change in Calculated LDL-C at 2 Weekly Intervals from Baseline to Week BASELINE WEEK 2 WEEK 4 WEEK 6 WEEK 8 WEEK 10 WEEK % - 5.1% % % % % Placebo SAR mg Q2W SAR mg Q2W SAR mg Q2W % % Mean percentage change in calculated LDL-C from baseline to weeks 2, 4, 6, 8, 10, and 12 in the modified intent-to-treat (mitt) population, by treatment group. Week 12 estimation using LOCF method. Clinicaltrials.gov no. NCT

48 % Patients Achieving Prespecified LDL-C Level Attainment of Prespecified LDL-C Levels at Week 12 (mitt Population) % LDL-C <100mg/dL % LDL-C <70mg/dL Placebo 50mg Q2W 100mg Q2W 150mg Q2W 200mg Q4W 300mg Q4W Clinicaltrials.gov no. NCT
 1 2 1 1 LS mean (SE) 2 median (Q1-Q3) Clinicaltrials.gov no.")
49 % Change from Baseline at Week 12 Changes in TG, HDL-C, and Apo AI from Baseline to Week 12 by Treatment Group (mitt Population) LS mean (SE) 2 median (Q1-Q3) Clinicaltrials.gov no. NCT
50 Summary of Treatment-Emergent Adverse Events (TEAEs) (Safety Population) Q2W dosing Placebo (N=31) 50mg (N=30) 100mg (N=31) Overview of all TEAEs no. 150mg (N=31) Q4W dosing 200mg (N=30) 300mg (N=30) Any TEAE Any treatment-emergent SAE Any TEAE leading to permanent treatment d/c AEs of special interest no. ALT or AST >3 x ULN Muscle (including pain, weakness) CK >10 x ULN Injection-site reactions occurred in the SAR groups only and were generally mild and non-progress Clinicaltrials.gov no. NCT
51 Summary and Conclusions PCSK9 inhibitors produced significant, dose-dependent LDL-C reductions Up to 72% LDL-C reduction with 150mg Q2W Improved ability to achieve LDL-C goal cut points LDL-C reductions were generally unaffected by baseline atorvastatin dose Consistent and robust reductions for all other Apo B containing lipoproteins Important reduction in Lp (a), consistent with prior studies Trend towards decreases in TG and increases in HDL-C and Apo AI vs placebo PCSK9 inhibitors are well tolerated No signals for persistent or prevalent clinical or laboratory adverse events including hepatic and muscle assessments. Clinicaltrials.gov no. NCT

52 Further Details An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School Article available at Slides available at
53 Trial Design 27,564 high-risk, stable patients with established CV disease (prior MI, prior stroke, or symptomatic PAD) Screening, Lipid Stabilization, and Placebo Run-in High or moderate intensity statin therapy (± ezetimibe) LDL-C 70 mg/dl or non-hdl-c 100 mg/dl Evolocumab SC 140 mg Q2W or 420 mg QM RANDOMIZED DOUBLE BLIND Placebo SC Q2W or QM Follow-up Q 12 weeks An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School Sabatine MS et al. Am Heart J 2016;173:94-101
54 Endpoints Efficacy Primary: CV death, MI, stroke, hosp. for UA, or coronary revasc Key secondary: CV death, MI or stroke Safety AEs/SAEs Events of interest incl. muscle-related, new-onset diabetes, neurocognitive Development of anti-evolocumab Ab (binding and neutralizing) TIMI Clinical Events Committee (CEC) Adjudicated all efficacy endpoints & new-onset diabetes Members unaware of treatment assignment & lipid levels An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School Sabatine MS et al. Am Heart J 2016;173:94-101

55 LDL Cholesterol (mg/dl) LDL Cholesterol Placebo Cohort of 11,077 patients who had all measurements through 120 weeks did not discontinue study drug did not D concomitant background lipid-lowering Rx Weeks An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School Evolocumab Similar data out to 4 years in OSLER-1 (JAMA Cardiology online)
56 Lower LDL-C Is Better Patients divided by quartile of baseline LDL-C and by treatment arm P< Q4 Q3 Q3 Q4 Q1 Q2 Q1 Q2 Placebo Evolocumab An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School
57 Safety Evolocumab (N=13,769) Placebo (N=13,756) Adverse events (%) Any Serious Allergic reaction Injection-site reaction Treatment-related and led to d/c of study drug Muscle-related Cataract Diabetes (new-onset) Neurocognitive Laboratory results (%) Binding Ab 0.3 n/a Neutralizing Ab none n/a New-onset diabetes assessed in patients without diabetes at baseline; adjudicated by CEC An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School
58 Summary for Evolocumab LDL-C by 59% Consistent throughout duration of trial Median achieved LDL-C of 30 mg/dl (IQR mg/dl) CV outcomes in patients already on statin therapy 15% broad primary endpoint; 20% CV death, MI, or stroke Consistent benefit, incl. in those on high-intensity statin, low LDL-C 25% reduction in CV death, MI, or stroke after 1 st year Long-term benefits consistent w/ statins per mmol/l LDL-C Safe and well-tolerated Similar rates of AEs, incl DM & neurocog events w/ EvoMab & pbo Rates of EvoMab discontinuation low and no greater than pbo No neutralizing antibodies developed An Academic Research Organization of Brigham and Women s Hospital and Harvard Medical School
59 .
60 . CASE STUDIES
61 Patient Case #2-75 year old African American male with a history of CABG x 3 in 2010 and HTN presents to your office for a routine physical examination - Medications: metoprolol XL100 mg daily, losartan 50 mg daily and aspirin 81 mg daily - Lipid Profile: TC 180 mg/dl, LDL-C 90 mg/dl, HDL-C 40 mg/dl, TG 200 mg/dl, LFTs NL
62 Patient Case #2 Which therapy if any would you institute in this patient? (75 yo, CAD- TC 180 mg/dl, LDL-C 90 mg/dl, HDL-C 40 mg/dl, TG 200 mg/dl) - A. Pravastatin 20 mg daily - B. Rosuvastatin 20 mg daily - C. Atorvastatin 40 mg daily - D. Lovastatin 20 mg daily - E. Alirocumab 75 mg 2x monthly - F. No Statin therapy is indicated. Continue diet and exercise.
63 Patient Case #3-40 year old Caucasian female with a history of DM and HTN presents to your office for a routine physical examination. Calculated Global Risk Index is 9%. - Medications: vasotec 20 mg daily and aspirin 81 mg daily - Lipid Profile: TC 180 mg/dl, LDL-C 100 mg/dl, HDL-C 50 mg/dl, TG 150 mg/dl, LFTs NL
64 Patient Case #3 Which therapy (if any) would you institute in this patient? (40, DM, global risk index 9%- TC 180 mg/dl, LDL-C 100 mg/dl, HDL-C 50 mg/dl, TG 150 mg/dl) - A. Pravastatin 40 mg daily - B. Rosuvastatin 20 mg daily - C. Atorvastatin 40 mg daily - D. Lovastatin 20 mg daily - E. Alirocumab 75 mg 2x monthly - F. No Statin therapy is indicated. Continue primary prevention strategies.
65 Patient Case #4-55 year old male with a history of CAD noted on cardiac catheterization in 2008 presents to your office for a routine physical examination - Medications: allopurinol 100 mg daily, losartan 50 mg daily, atorvastatin 40 mg and synthroid 75 mcg daily - Lipid Profile: TC 170 mg/dl, LDL-C 90 mg/dl, HDL-C 50 mg/dl, TG 150 mg/dl, LFTs NL
66 Patient Case #4 Which treatment plan would you institute in this patient? - A. Increase atorvastatin to 80 mg daily - B. Continue atorvastatin 40 mg daily - C. Continue atorvastatin 40 mg daily and add ezetimide 10 mg daily - D. Add Alirocumab 75 mg 2x monthly - E. Discontinue atorvastatin and start rosuvastatin 40 mg daily - F. Consult TCI Cardiology
67 Patient Case #5-72 year old female with a history of CAD, PVD and DM presents to your office for a routine follow-up. He has been intolerant to atorvastatin, rosuvastatin, simvastatin, pravastatin and pitvastatin due to muscle aches. - Medications: aspirin 81 mg daily, Lisinopril 10 mg daily, amlodipine 10 mg daily and Coenzyme Q 10 - Lipid Profile: TC 200 mg/dl, LDL-C 120 mg/dl, HDL-C 50 mg/dl, TG 150 mg/dl, LFTs NL
68 Patient Case #5 Which therapy if any would you institute in this patient? - A. ezetimibe 10 mg daily - B. alirocumab 75 mg SQ 2 x monthly - C. alirocumab 75 mg SQ 2 x monthly and ezetimide 10 mg daily - D. alirocumab 150 mg SQ 2 x monthly - E. None of the above (different therapy). - F. No Statin therapy is indicated.
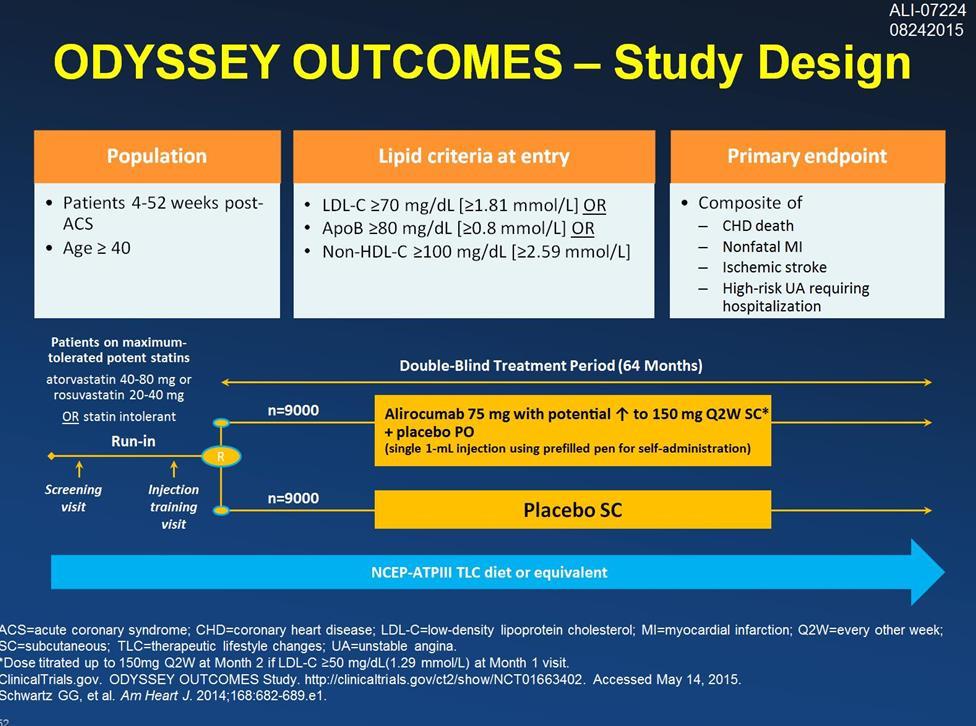
69 Final Thoughts For patients with established CAD, the recommended goal is < 70 mg/dl (ideal mg/dl? To be determined). ATP IV may be beneficial in treating primary prevention patients that may not otherwise be candidates for statin therapy. What is the ideal LDL target for patients with CAD? How low is too low? Awaiting outcomes trial data from Odyssey Outcomes Study due in 2017 in patients on a PCSK9 inhibitor.
70 . Thank you!
71 References Sitbon O et al. Circulation 2005 D Alonzo GE et al. Ann Intern Med 1991 Galie N et al. Eur Heart J Gaine SP et al. Lancet 1998 Barst RJ et al. J Am Coll Cardiol 2004 Simonneau G et al. JACC 2004 Barst RJ et al. J Am Coll Cardiol 2004 D Alonzo GE, et al. Ann Intern Med 1991;115: Peacock AJ. BMJ 2003 Gaine SP et al. Lancet 1998 Sitbon O et al. Am J Resp Crit Care Med 2008 Lin EE et al. Curr Hematol Rep 2005 McGoon M et al. Chest 2004 Stewart DJ et al. Ann Inter Med 1991 Vancheeswaran R et al. J Rheum 1994 Yoshibayashi M et al. Circulation 1991 Galiè N et al. Eur J Clin Invest 1996 Channick RN et al. Lancet 2001 Kato I et al. Cancer 2001 Bjoraker JA et al. Am J Respir Crit Care Med 1998 Humbert M et al. Am J Respir Crit Care Med 2006 Sitbon O et al. J Am Coll Cardiol 2002 Galie N et al. Eur Heart J 2004 Hachulla E et al Ann Rheum Dis 2004 McGoon M et al. Chest 2004 ATS. Am J Crit Care Med 2002 Galiè N et al. Lancet 2008 Humbert H et al. N Engl J Med 2004 Channick RN et al. Lancet 2001 Humbert H et al. N Engl J Med 2004 Galiè N et al. N Engl J Med 2005
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
MS Sabatine, RP Giugliano, AC Keech, PS Sever, SA Murphy and TR Pedersen, for the FOURIER Steering Committee & Investigators
 Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial
 Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
A Systemic Approach to Lipid Management Making Sense of the Fatty Debate
 A Systemic Approach to Lipid Management Making Sense of the Fatty Debate M Ranu Muttreja MD Aria Jefferson Health October 8, 2017 Historical Perspective Lipid Hypothesis Early 1900 s Anitschkow fed rabbits
A Systemic Approach to Lipid Management Making Sense of the Fatty Debate M Ranu Muttreja MD Aria Jefferson Health October 8, 2017 Historical Perspective Lipid Hypothesis Early 1900 s Anitschkow fed rabbits
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Cholesterol, guidelines, targets and new medications
 Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Statins and PCSK9 inhibitors for stroke prevention
 Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies
 Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
2/23/2018. Management of Hyperlipidemia Update on Guidelines and Novel Therapies. Burden of Heart Disease in U.S.
 Management of Hyperlipidemia Update on Guidelines and Novel Therapies SHARATH SUBRAMANIAN, MD, FACC February 24, 2018 Disclosures : None Burden of Heart Disease in U.S. https://www.cdc.gov/nchs/images/databriefs/251
Management of Hyperlipidemia Update on Guidelines and Novel Therapies SHARATH SUBRAMANIAN, MD, FACC February 24, 2018 Disclosures : None Burden of Heart Disease in U.S. https://www.cdc.gov/nchs/images/databriefs/251
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH
 PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus
 Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
2/10/2016. Patient-Centered Management of Dyslipidemia. No disclosures. What is Patient-Centered Management?
 Patient-Centered Management of Dyslipidemia Carl E. Orringer, MD, FACC, FNLA Associate Professor of Medicine University of Miami Miller School of Medicine President, National Lipid Association 1 No disclosures
Patient-Centered Management of Dyslipidemia Carl E. Orringer, MD, FACC, FNLA Associate Professor of Medicine University of Miami Miller School of Medicine President, National Lipid Association 1 No disclosures
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP
 Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES
 DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy
 PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for
Reducing Cardiovascular Risk Through Non-Statins. Kim K. Birtcher, PharmD Joseph Saseen, PharmD
 Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
LDL and the Benefits of Statin Therapy
 LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Prevention Updates and Paradigm Shifts
 Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Best Lipid Treatments
 Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual