Introduction. Objective. Critical Questions Addressed
|
|
|
- Magnus Walton
- 5 years ago
- Views:
Transcription
1
2
3 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1: What is the evidence for LDL C and non-hdl C goals for the secondary prevention of ASCVD? CQ2: LDL C and Non-HDL C Goals in Primary Prevention CQ3: For primary and secondary prevention, what is the impact on lipid levels, effectiveness, and safety of specific cholesterol-modifying drugs used for lipid management in general and in selected subgroups?
4 Key Findings RCTs indicated a consistent reduction in ASCVD events from statin therapy in both secondary and primary prevention Relative reduction in ASCVD risk is consistent for primary and secondary prevention and for various patient subgroups Absolute reduction in ASCVD events is proportional to baseline absolute ASCVD risk Statin therapy reduces ASCVD events across the spectrum of baseline LDL C levels >70 mg/dl Extent of relative-risk reductions for ASCVD is proportional to the degree of LDL C lowering observed on statin therapy. Therefore, more intensive statin therapy could reduce risk more than moderate-or lower-intensity statin therapy No ASCVD event reduction in those with New York Heart Association (NYHA) class II-IV heart failure Receiving maintenance hemodialysis
5 Key Findings NO RCT evidence to support titrating cholesterol-lowering drug therapy to achieve target LDL C or non-hdl-c levels As per the ATP III guidelines: Clinicians use targets such as LDL C <70 mg/dl and LDL C <100 mg/dl for secondary and primary ASCVD prevention (non-hdl C targets are 30 mg/dl higher) without hard evidence No evidence to support addition of non-statin hypolipidemics for CV risk reduction Available RCT evidence indicates a clear net absolute benefit of initiation of moderate-to-intensive statin therapy at a baseline estimated 10-year ASCVD risk of 7.5%. When baseline ASCVD risk is 5.0% to <7.5%, there is still net absolute benefit with moderate-intensity statin therapy. A risk-benefit discussion is even more important for individuals with this range of ASCVD risk The net benefit of high-intensity statin therapy appears to be marginal in such individuals.
6 Key Findings In adults with and without CHD/CVD who received more intensive compared to less intensive statin therapy or placebo, relative risk reductions per 1 mmol/l (38.7 mg/dl) LDL C reduction were: For major coronary events: 24% For nonfatal myocardial infarction: 27% Total mortality: 10% per 1 mmol/l Risk for CVD mortality: 14% For coronary revascularization: 24% 23% to 28% relative reductions in CVD risk per 39 mg/dl (1 mmol/l) reduction in LDL C were observed after 1 year to beyond 5 years of statin treatment
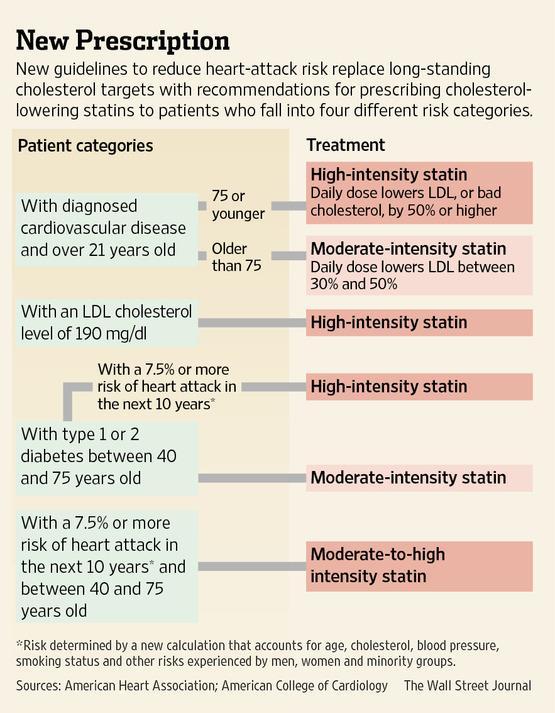
7 Recommendations High-intensity statin therapy Lowers LDL C by approximately 50% Indications: Secondary prevention in patients <75 years age LDL-C 190 mg/dl at baseline Diabetics y with LDL C 70 to189 mg/dl and without clinical ASCVD but with estimated 10- year ASCVD risk of 7.5% Non-diabetics y with estimated 10-year ASCVD risk of 7.5% Moderate-intensity statin therapy Lowers LDL C by approximately 30% to <50% Indication: Secondary prevention in patients <75 years age or those not tolerating high doses of statins LDL-C 190 mg/dl at baseline in those not tolerating high doses of statins All diabetics y with LDL C 70 to189 mg/dl and without clinical ASCVD Non-diabetics y with estimated 10 year ASCVD risk of 7.5%
8 Intensity of Statin Therapy High-Intensity Statin Therapy Daily dose lowers LDL-C on average, by approximately 50% Atorvastatin (40 ) 80 mg Rosuvastatin 20 (40) mg Moderate-Intensity Statin Therapy Daily dose lowers LDL-C on average, by approximately 30% to <50% Atorvastatin 10 (20) mg Rosuvastatin (5) 10 mg Simvastatin mg Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2-4 mg Low-Intensity Statin Therapy Daily dose lowers LDL-C on average, by <30% Simvastatin 10 mg Pravastatin mg Lovastatin 20 mg Fluvastatin mg Pitavastatin 1 mg Specific statins and doses are noted in bold that were evaluated in Statins and doses that are approved by the U.S. FDA but were not tested in the RCTs reviewed are listed in italics. Evidence from 1 RCT only: down-titration if unable to tolerate atorvastatin 80 mg in IDEAL Although simvastatin 80 mg was evaluated in RCTs, initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy, including rhabdomyolysis.
9 What s New in the Guideline Focus on ASCVD Risk Reduction: 4 statin benefit groups A New Perspective on LDL C and/or Non-HDL C Treatment Goals Global Risk Assessment for Primary Prevention Safety Recommendations
10 4 Statin Benefit Groups 1. Patients with clinical ASCVD 2. Primary elevations of LDL C >190 mg/dl 3. Diabetics aged 40 to 75 years with LDL C 70 to189 mg/dl and without clinical ASCVD, or 4. Without clinical ASCVD or diabetes with LDL C 70 to189 mg/dl and estimated 10-year ASCVD risk >7.5% Treatment decisions in selected individuals who are not included in the 4 statin benefit groups may be informed by other factors as recommended by the Risk Assessment Work Group guideline.
11 Patients with Clinical ASCVD Clinical ASCVD: Acute coronary syndromes, History of MI, Stable or unstable angina, Coronary or other arterial revascularization, Stroke or TIA, Peripheral arterial disease presumed to be of atherosclerotic origin Recommendations: In women and men 75 years of age High-intensity statin therapy as first-line therapy, unless contraindicated In individuals with clinical ASCVD >75 years of age Evaluate the potential for ASCVD risk-reduction benefits and for adverse effects, drug-drug interactions and consider patient preferences, when initiating a moderateor high-intensity statin. It is reasonable to continue statin therapy in those who are tolerating it When either high-intensity statin therapy is contraindicated or when characteristics predisposing to statin-associated adverse effects are present, moderate-intensity statin should be used as the second option, if tolerated
12 Primary Prevention in Adult 21 Years with LDL C 190 mg/dl 10-year ASCVD risk estimation is not required Observational data has shown significant reductions in ASCVD events without achieving specific LDL C targets Recommendations Use high-intensity statin therapy unless contraindicated For individuals unable to tolerate high-intensity statin therapy, use the maximum tolerated statin intensity After the maximum intensity of statin therapy has been achieved, addition of a non-statin drug may be considered to further lower LDL C Evaluate the potential for ASCVD risk reduction benefits, adverse effects, drug-drug interactions, and consider patient preferences
13 Diabetics aged 40 to 75 years with LDL C 70 to 189 mg/dl and without clinical ASCVD In adults with diabetes without CVD, moderate-dose statin therapy, compared with placebo/control, reduced the RR for CVD events by 27% per 38.7 mg/dl LDL C reduction In adults aged 40 to 75 years with diabetes and >1 risk factor, fixed moderate-dose statin therapy that achieved a mean LDL C 72 mg/dl reduced the RR for CVD by 37% Diabetics often have lower LDL C levels than those without diabetes "Goal" directed therapy often encourages use of a lower statin dose than is supported by the RCTs Non-statin drugs may be added to address low HDL C or high triglycerides, for which RCT evidence of an ASCVD event reduction is lacking
14 Diabetics aged 40 to 75 years with LDL C 70 to 189 mg/dl and without clinical ASCVD Recommendations Giving a maximally-tolerated statin intensity should receive primary emphasis Moderate-intensity statin therapy should be initiated or continued for adults 40 to 75 years of age with diabetes mellitus High-intensity statin therapy is reasonable for adults 40 to 75 years of age with diabetes mellitus with a 7.5% estimated 10- year ASCVD risk unless contraindicated. In adults with diabetes mellitus, who are <40 or >75 years of age Evaluate the potential for ASCVD benefits and for adverse effects, for drugdrug interactions, and to consider patient preferences when deciding to initiate, continue, or intensify statin therapy
15 Primary Prevention in Individuals without Diabetes Mellitus & With LDL C 70 to 189 mg/dl In men and postmenopausal women aged 40 to 75 years without CHD/CVD, moderate-dose statin therapy reduces the RR for CVD by 24 25% compared with placebo For those with a 5% to <7.5% estimated 10-year ASCVD risk Potential for adverse effects may outweigh the potential for ASCVD risk reduction benefit when high-intensity statin therapy is used in this risk group With moderate-intensity statin therapy the ASCVD risk reduction clearly exceeds the potential for adverse effects. In individuals 40 to 75 years of age with <5% estimated 10-year ASCVD risk, the net benefit from statin therapy over a 10-year period may be small. Additional factors may also be considered to inform treatment decision No primary prevention RCT data available for individuals 21 to 39 years of age and few data were available for individuals >75 years of age.
16 Primary Prevention in Individuals without Diabetes Mellitus & With LDL C 70 to 189 mg/dl Recommendations: Pooled Cohort Equations should be used to estimate 10-year ASCVD risk If estimated 10-year ASCVD risk 7.5% treat with moderate- to high-intensity statin therapy It is reasonable to offer treatment with a moderate-intensity statin if estimated 10-year ASCVD risk is 5% to <7.5% In adults with LDL C <190 mg/dl who are not otherwise identified in a statin benefit group, or for whom after quantitative risk assessment a risk- based treatment decision is uncertain, additional factors may be considered to inform treatment decision making. These factors may include primary LDL C >160 mg/dl or other evidence of genetic hyperlipidemias, family history of premature ASCVD with onset <55 years in a first degree male relative or <65 years in a first degree female relative, high sensitivity-creactive protein >2 mg/l, CAC score 300 Agatston units or 75 percentile for age, sex, and ethnicity, ABI <0.9, or lifetime risk of ASCVD.
17 Individuals >75 Years of Age A larger amount of data supports the use of moderateintensity statin therapy for secondary prevention in individuals with clinical ASCVD >75 years of age. Initiation of statins for primary prevention of ASCVD in individuals >75 years of age requires consideration of additional factors, including increasing comorbidities, safety considerations, and priorities of care A discussion of the potential ASCVD risk reduction benefits, risk of adverse effects, drug-drug interaction, and patient preferences precede the initiation of statin therapy for primary prevention in older individuals.
18 New LDL C and/or Non-HDL C Treatment Goals LDL-C lowering provides benefit irrespective of baseline levels Lack of RCT evidence to support continued use of specific LDL C and/or non- HDL C treatment targets RCTs either compared fixed doses of statins with placebo or untreated controls, or compared fixed doses of higher-intensity statins with moderateintensity statins Benefit : Risk ratio not in favor of prescribing non-statin therapy to achieve treatment gaols Non-statin therapies do not provide acceptable ASCVD risk reduction benefits AIM-HIGH demonstrated the futility of adding niacin in individuals with low HDL C and high triglycerides, and ACCORD demonstrated the futility of adding fenofibrate in persons with diabetes
19 New LDL C and/or Non-HDL C Treatment Goals Use of LDL C targets may result in under-treatment with evidencebased statin therapy or overtreatment with nonstatin drugs that have not been shown to reduce ASCVD events in RCTs (even though the drug may additionally lower LDL C and/or non-hdl C) Implications of treating to an LDL C goal may mean that a suboptimal dose of statin is used because the goal has been achieved, or that adding a non-statin therapy to achieve a specific target results in down-titration of the evidence-based dose of statin for safety reasons Appropriate intensity of statin therapy should be used to reduce ASCVD risk in those most likely to benefit
20 Global Risk Assessment for Primary Prevention Estimated absolute 10-year risk of ASCVD (defined as nonfatal MI, CHD death, nonfatal and fatal stroke) should be used to guide the initiation of statin therapy Pooled Cohort Equations to be used for estimating 10-year ASCVD risk Applicable to African-American and non-hispanic white men and women 40 through 79 years of age with or without diabetes who have LDL C levels 70 to 189 mg/dl May underestimate the risk for persons from some race/ethnic groups, especially American Indians, some Asian Americans (e.g., of south Asian ancestry), and some Hispanics (e.g., Puerto Ricans) May overestimate the risk for others, including some Asian Americans (e.g., of east Asian ancestry) and some Hispanics (e.g., Mexican Americans). For those with clinical ASCVD or with LDL C 190 mg/dl who are already in a statin benefit group, it is not appropriate to estimate 10-year ASCVD risk
21 Benefit: Risk Analysis Potential ASCVD risk reduction benefits Relative risk reduction of ~30% for moderate-intensity statin or ~45% for high-intensity statin therapy. Potential adverse effects. Excess risk of diabetes 1 year incidence of new onset diabetes: ~0.1 excess case per 100 individuals with moderate-intensity statin ~0.3 excess cases per 100 individuals with high-intensity statin Long-term adverse effects of statin-associated cases of diabetes over a 10-year period are unclear and are unlikely to be equivalent to an MI, stroke, or ASCVD death Myopathy (~0.01 excess case per 100) and hemorrhagic stroke (~0.01 excess case per 100) make minimal contributions to excess risk from statin therapy
22 Important Considerations Asian ancestry may also influence the initial choice of statin intensity Decreasing the statin dose may be considered when 2 consecutive values of LDL C are <40 mg/dl. However, no data was identified that suggests an excess of adverse events occurred when LDL C levels were below this level. Those who develop diabetes during statin therapy should be encouraged to adhere to a heart healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce their risk of ASCVD events. Do an initial fasting lipid panel (total cholesterol, triglycerides, HDL C, and calculated LDL C), followed by a second lipid panel 4 to 12 weeks after initiation of statin therapy and then every 3 to 12 months as clinically indicated. Statins used in combination with other cholesterol-lowering drug therapies might require more intensive monitoring.
23 Grey Areas Pooled Cohort Equations not validated for Indians May underestimate the ASCVD risk Recommendations may not apply to non-diabetic Indians with LDL-C between mg/dl Lack of clarity on younger adults (<40 years of age) who have a low estimated 10-year ASCVD risk, but a high lifetime ASCVD risk based on single strong factors or multiple risk factors

24 Statin use in Heart Failure & Hemodialysis
25
26 Intensive Statin Therapy

27 % reduction in MACE Reduction in MACE with Statins S LIPID CARE HPS WOSCOPS AFCAPS ASCOT-LA JUPITER Enas EA. How to beat the heart disease epidemic among South Asians. Downers Grove, 2005
28 Benefits Intensive Statin Therapy Trials using Atorvastatin 80 mg/d in Randomized Placebo Controlled Study # of subjects Treatment (mg/d) Decrease in LDL-C AVERT (2000) 314 x 18M Atorvastatin 80 * >115 mg/dl 36% Decrease in MACE MIRACLE (2001) 3,086 X 4M Atorvastatin 80* mg/dl 26% ALLIANCE (2004) 2,442 x 53M Atorvastatin 80* mg/dl 17% PROVE-IT (2004) 4,162 x 24M Atorvastatin 80* mg/dl 16% REVERSAL (2005) 654 x18m Atorvastatin 80* mg/dl IDEAL (2005) 8,888 x 56 M TNT (2005) 10,001 x 53 Atorvastatin 80 vs. simvastatin 20 Atorvastatin 80 vs. 10 mg mg/dl 13% < mg/dl Halted progression of atherosclerosis 22% SPARCLE (2006) 4,071 x 57M Atorvastatin 80* mg/dl SAGE (2007) 893 Atorvastatin 80* NA 26% Stroke 16-31% 29; 67% in death * Placebo controlled Enas EA, CSI Cochin, Cardiology Update 2009
29 Meta-analysis trials comparing intensive versus moderate statin therapy LDL changes Baseline Standard therapy Intensive therapy TNT PROVE IT-TIMI IDEAL A-to-Z Pooled Cannon CP. J Am Coll Cardiol 2006;48:438-45
30 Risk reduction vs. Atorvastatin 10 mg (%) TNT: Atorvastatin 80 mg vs.10 mg Reduces Cardiovascular Risk 0 Nonfatal MI Fatal and nonfatal stroke Revasc Hospitalization for CHF Angina % P= % P= % P=.02 28% P< % P=.01 Incremental risk reductions vs. Atorvastatin 10 mg Previously, in ASCOT-LLA, Atorvastatin 10 mg significantly reduced risk of MI, stroke, revascularization, and angina in primary prevention patients 1 1. Sever PS, et al. Lancet. 2003;361: LaRosa JC, et al. N Engl J Med. 2005;352:
31 Meta-analysis trials comparing intensive versus moderate statin therapy Risk of ALT and or AST >10 x ULN* Trial Standard dose ALT and or AST >10 x ULN High dose TNT 0.18% 1.2% PROVE IT-TIMI % 3.3% IDEAL 0.16% 1.37% A-to-Z 0.36% 0.84% *Cannon CP. J Am Coll Cardiol 2006;48:438-45
32 Efficacy and Safety of Statin Treatment: A Prospective Meta-analysis of Data from 90,056 Participants in 14 Randomised Trials A 40 mg/dl increase in LDL-C or non-hdl-c confer a 40% increase in CVD risk beginning with an LDL of 40 mg/dl A 40 mg/dl reduction in LDL-C statin therapy safely reduces the 5-year incidence of MACE ( major adverse CVD events such as MI stroke, CVD deaths ) and CARP (coronary artery revascularization procedures) by 20%, irrespective of the initial lipid profile. The reduction in MACE will be higher with greater LDL-C reduction (see next slide) The absolute benefit relates chiefly to an individual's absolute risk of such events and to the absolute reduction in LDL-C achieved. Baigent C. Lancet 2005;366:
33 Reduction in MACE from Lowering LDL-C with Statins for 5 years in 1000 Patients Major Cardiovascular Events* Secondary prevention Primary prevention LDL-C reduction RRR ARR RRR ARR 40 mg/dl 20% 48/ % 25/ mg/dl 40% 96/ % 50/ mg/dl 60% 144/ % 75/ mg/dl 80% 192/ % 100/1000 * Includes coronary artery revascularization procedures Baigent C. Lancet 2005;366:

 Q2((70) Q3 (83) Q4 (97) Q5")

34 % of patients TNT Study Post Hoc Analysis: Rates of MACE According to the Achieved LDL Quintiles P=< Q1(54) Q2((70) Q3 (83) Q4 (97) Q5 (122) (Mean LDL-C in mg/dl) MACE = Major Acute Cardiovascular Events Larosa JC. Am J Cardiol 2007;100:
35 TNT Study Post Hoc Analysis No. patients Quintiles Range Mean +SD Atorva 10 mg Atorva 80 mg Total 1 < , < ,403 1, < , , < , ,030 5 > , ,984 Larosa JC. Am J Cardiol 2007;100:
36 Can LDL-C be too low? Benefits of Aggressive versus Modest LDL-C Reduction in the PROVE-IT Study Achieved LDL (mg/dl) Risk reduction CI (Referent) 1 > % > % <40 39% Viviott SD. J Am J cardiol 2005;46:1411
37 Statin Safety: Muscle Toxicity Myopathy is a general term for all potential muscle problems Symptomatic myopathy- refers to all complaints referable to skeletal muscle and include cramps, pain, or weakness Asymptomatic myopathy- refers to CK elevation without complaints referable to skeletal muscle Clinically important rhabdomyolysis refers to muscle symptoms with CK elevation with change in renal function Mild CK elevation- <10 times ULN Moderate CK elevation- >10 times but <50 times ULN Severe CK elevation- >50 times ULN Thompson PD. Am J Cardiol 2006;97:69C-76C.
38 Not All Statins Are Created Equal Atorvastatin has been studied most extensively at doses ranging from 10 mg to 80 mg, for safety, efficacy and outcome Greater benefits at higher doses (80 mg/dl) clearly demonstrated with atorvastatatin Atorvastatin studies led to changes in NCEP guidelines Atorvastatin has received approval from US FDA for primary and secondary prevention
39 Side Effects of Intensive Statin Therapy Trials using Atorvastatin 80 mg/d Trial # of subjects and follow-up ALT/AST >3 x ULN CK>3 x ULN Newman et al 2000) 4,798 (variable) 26 (0.6%) 2 (0.06%) PROVE-IT (2004) 2,099 for 2 years 20 (0.6%) NA TNT (2005) 4,995 x 4.9 years 60 (1.2%) 0 IDEAL (2005) 4,439 x (1.38%) 0 SPARCLE (2006) 2,365 x 4.9 years 51 (2.2%) 2 (0.08%) Total atorvastatin 18, (1.43%) 4 (0.024%) Enas EA, CSI Cochin, Cardiology Update 2009
40 How safe is Intensive statin Therapy? 100 times safer than diabetic medications! 100 times safer than low-dose Aspirin!!
41 When Does the Benefit Outweigh the Risk of Aspirin in Primary Prevention? MEN WOMEN Age group 10- year risk of MI is 10- year risk of Stroke is years 4% 3% years 9% 8% years 12% 11% USPSTF. Ann Intern Med 2009;150:
42 Key Points (1) Efficacy The optimum LDL-C is currently standardized at 40 mg/dl For every 1 mg/dl increase from 40 mg/dl, confers a 1% higher risk for CVD; those with 70 mg/dl have a 30% higher risk compared to people with optimum LDL-C Regression of atherosclerosis requires an LDL-C <70 mg/dl, non-hdl-c <100 mg/dl and a systolic blood pressure <115 mm Hg The LDL-C target is <100 mg/dl for Asian Indians and <70 mg/dl for those with CVD, diabetes, metabolic syndrome and chronic kidney disease Intensive statin therapy may be often required to achieve these goals Intensive LDL-C lowering yields superior benefits than moderate lowering The CVD risk reduction is directly proportional to the absolute reduction in LDL- C and not the statin dose; A 50 mg/dl reduction in LDL-C and/or non-hdl-c confers a 50% reduction in CVD after 5 years of treatment.
43 Key Points (2) Remarkable Safety Asymptomatic transaminase elevations are not associated with an increased risk of liver disease or hepatotoxicity The risk of significant transaminase elevation with atorvastatin 80mg is 1.4% compared to 5.3% for fenofibrate The risk of liver failure with statin therapy is one in a million essentially same as the general population The risk of muscle toxicity is low 3 fatal and 30 non-fatal rhabdomyolysis cases per million person-years Statin toxicity is not related to the LDL-lowering efficacy Statin toxicity is driven by the blood concentrations of the statin, which in turn may be related to the dose of the specific statin used, drug interactions and or genetic susceptibility More than 80% of statin associated myopathy is attributable to concomitant use of fibrates or CPY3A4 inhibitors
44 Key Points (3) Comparison of High-dose Statins Toxicity varies among high doses of different statins The risks outweighs the benefits for simvastatin 80 mg; compared with 40 mg/d simvastatin 80 mg is associated with 700% increase in myopathy only a 7% additional LDL-C reduction. The JUPITER Trial has demonstrated the benefits and safety of lowering LDL-C rosuvastatin 20 mg/d to <55 mg/dl in nearly 5,000 patients and <40 mg/dl in 2,500 patients. Atorvastatin 80 mg /d reduces the risk of MI stroke, heart failure, and CARPs by about 25%, compared with atorvastatin 10 mg/d, with minimal risk AST/ALT >3x ULN - 1.4%; CK >10x ULN % Intensive statin therapy with Atorvastatin 80 mg/day or Rosuvastatin 20mg/day appears be 100 times safer than 81 mg /d of aspirin, which has a significant risk of GI bleeding requiring transfusion (1-3%) and hemorrhagic stroke (0.01%).
45 Key Points (4) Statins for High TG and Diabetes Non-HDL-C is a better predictor of CVD risk than LDL-C in patients with high TG, which spuriously lowers LDL-C The non-hdl-c targets is set at 30 mg/dl higher than the LDL-C target Intensive statin therapy can lower non-hdl-c by >50% (the same magnitude as LDL-C reduction) in patents with high TG. Intensive statin therapy is more effective than fibrates in lowering non- HDL-C Reducing non-hdl-c by 50% reduces the CVD risk by 50 % but lowering TG has not been shown to reduce CVD risk to-date Among patients with diabetics, statin therapy would prevent 9,250 MACE per million person-years of therapy in primary prevention, with minimal risk.
46 Key Points (5) Use of Statin Ahead of Aspirin in Primary Prevention In primary prevention, the benefits outweighs the risk for statins but for aspirin, the risks and benefits balances each other or may be even harmful. The benefit of aspirin in primary prevention of CVD in patients with diabetes is very small and risk high For every CVD event prevented with aspirin, one major GI bleeding is produced The risk benefit analysis supports the use of statin far ahead of aspirin in primary prevention of CVD Physicians should recognize and communicate to their patients that treatment of chronic conditions like high cholesterol and high blood pressure is lifelong.
47 High-Dose Atorvastatin Safety and benefits established for 80 mg/dl dose in more than 15,000 subjects High-dose atorvastatin therapy is more effective than usual dose therapy in lowering LDL-C and MACE In a person with an LDL-C 220 mg/dl, an 80 mg dose can decrease LDL-C by 120 mg/dl (55%) with a resultant 60% reduction in CVD risk in 5 years No increase in muscle toxicity with higher doses
48 Efficacy and Safety of Statin Treatment: Prospective Meta-analysis of Data from 90,056 Participants in 14 Randomised Trials Efficacy and Safety of Statin Treatment: Prospective Meta-analysis of Data from 90,056 Participants in 14 Randomised Trials The risk reduction achieved is only half in the first 2 years and may be double (40% reduction in MACE for 40 mg/dl decrease in LDL-C) These findings reinforce the need to consider prolonged statin treatment with substantial LDL-C reductions in all patients at high risk for any type of major vascular event Benefits of statins outweigh the risk in all but a very small group who are at high risk of complications There is no evidence that statins increases the incidence of cancer or hemorrhagic stroke Baigent C. Lancet 2005;366:
49 Indications for Atorvastatin Prevention of CVD Angina, MI, CARP, stroke To improve lipid profile in familial and nonfamilial dyslipidemia Fredrickson Types IIa, IIb, III & IV Pediatric dyslipidemia (in Asian Indians) LDL-C >160 mg/dl LDL-C >130 mg/dl with Positive family history or >2 risk factors Atorvastatin PI
50 Summary Statins Extensively studied for efficacy, safety, and clinical outcome Consistently reduce, LDL-C, non-hdl-c, and TG Significantly reduce fatal and nonfatal MACE in patients with and without CAD or CVD Significantly reduce first and subsequent MACE and CARP when used alone or in combination with other agents Benefits documented in children, adults, elderly, men, and women A 80 mg/dl decrease in LDL results in at least 40% reduction in MACE High dose statin therapy is more effective than usual dose therapy in lowering LDL-C and MACE Baigent C. Lancet 2005;366:
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
LAMIS (Livalo in AMI Study)
") JCR 2018. 12. 8 LAMIS (Livalo in AMI Study) Young Joon Hong Division of Cardiology, Chonnam National University Hospital Gwangju, Korea Trend of hypercholesterolemia in Korea < Prevalence of hypercholesterolemia
JCR 2018. 12. 8 LAMIS (Livalo in AMI Study) Young Joon Hong Division of Cardiology, Chonnam National University Hospital Gwangju, Korea Trend of hypercholesterolemia in Korea < Prevalence of hypercholesterolemia
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation,
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation,
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Observations on US CVD Prevention Guidelines. Donald M. Lloyd-Jones, MD ScM FACC FAHA
 Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Disclosure. A New Partnership. Objectives 03/27/2014. What is the main way you have obtained information about the 2013 ACC/AHA Cholesterol Guideline?
 Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
REAL-CAD. : Cardiovascular benefit of pitavastatin in stable coronary artery disease
 REAL-CAD : Cardiovascular benefit of pitavastatin in stable coronary artery disease Soo-Joong Kim M.D., PhD. Department of Cardiology, Internal Medicine, Kyung Hee University Hospital I have nothing to
REAL-CAD : Cardiovascular benefit of pitavastatin in stable coronary artery disease Soo-Joong Kim M.D., PhD. Department of Cardiology, Internal Medicine, Kyung Hee University Hospital I have nothing to
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
Major recommendations for statin therapy for ASCVD prevention
 2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
Calculating RR, ARR, NNT
 Calculating RR, ARR, NNT In a trial RR = Event rate (eg # of people with one stroke/ total people) in treatment group/event rate in the control group. ARR = Event rate in control group minus the event
Calculating RR, ARR, NNT In a trial RR = Event rate (eg # of people with one stroke/ total people) in treatment group/event rate in the control group. ARR = Event rate in control group minus the event
Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
2.3 CONTACT HOURS. Managing. By Kristine Anne Scordo, PhD, RN, ACNP-BC, FAANP
 2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin
 and Fixed-dose Combination Products Containing a Statin") Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin Final Report Update 5 November 2009 This report reviews information about the comparative
Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin Final Report Update 5 November 2009 This report reviews information about the comparative
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
NEW GUIDELINES FOR CHOLESTEROL
 NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
2/10/2016. Perspectives on the 2013 ACC/AHA Cholesterol Guidelines. Disclosures. ATP-III Update 2004
 Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Objec ves To discuss the process of formulation of guidelines and how this may differ among professional societies 5/14/15
 Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
Cholesterol Medicines New & Old: What to Use When
 Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Is it an era for statin for life?
 Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Supplementary Online Content
 Supplementary Online Content Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and
Supplementary Online Content Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
Game Strategy: High Intensity Statin in Stroke. K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018
 Game Strategy: High Intensity Statin in Stroke K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018 No Disclosures Are you Mind Full or Mindful? Objectives 1. Discuss the correlation between
Game Strategy: High Intensity Statin in Stroke K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018 No Disclosures Are you Mind Full or Mindful? Objectives 1. Discuss the correlation between
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
JAMA. 2011;305(24): Nora A. Kalagi, MSc
: Nora A. Kalagi, MSc") JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
Drug Class Review on HMG-CoA Reductase Inhibitors (Statins)
") Drug Class Review on HMG-CoA Reductase Inhibitors () Final Report June 2004 Mark Helfand, MD, MPH Susan Carson, MPH Cathy Kelley, PharmD Oregon Evidence-based Practice Center Oregon Health & Science University
Drug Class Review on HMG-CoA Reductase Inhibitors () Final Report June 2004 Mark Helfand, MD, MPH Susan Carson, MPH Cathy Kelley, PharmD Oregon Evidence-based Practice Center Oregon Health & Science University
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Implementation of CV Risk and. Dyslipidemia Guidelines. Impact on Americans 11/25/2014. Summary Implementing new. Dyslipidemia Guidelines
 Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Understanding US Lipid Guidelines-2013:
 Presentation to NLA Symposium: May 3 2014 Understanding US Lipid Guidelines-2013: Neil J. Stone MD, MACP, FACC Bonow Professor of Medicine Feinberg School of Medicine Northwestern University Chicago, Il
Presentation to NLA Symposium: May 3 2014 Understanding US Lipid Guidelines-2013: Neil J. Stone MD, MACP, FACC Bonow Professor of Medicine Feinberg School of Medicine Northwestern University Chicago, Il
Changing lipid-lowering guidelines: whom to treat and how low to go
 European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes?
 Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi