Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
|
|
|
- Marcus Dustin Reynolds
- 5 years ago
- Views:
Transcription





1 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014
2 New onset Crohn s Disease 10 year old girl presents with background of vague abdominal discomfort, low grade fevers, lack of weight gain (1 year), poor linear growth (<2 cm in 1 year) Rapid deterioration! Within 2-3 weeks: anorexia, weight loss (3 kg), fatigue, fevers, transient E. nodosum




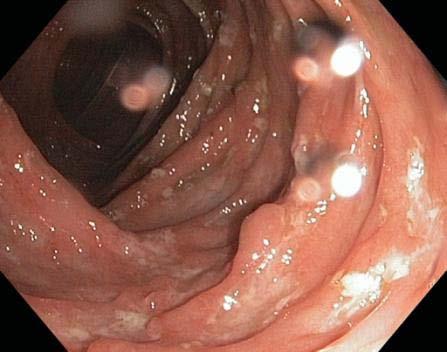



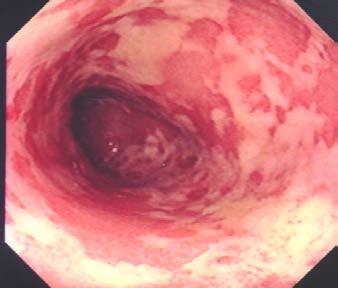
3 Ileocolonic Crohn Disease at first evaluation (Paris: L3 + L4a) Discontinuous disease Deep ulcers in transverse colon and ileum (20 cm) Small round and linear ulcers in stomach (+ve granuloma)
4 Current medical therapies for pediatric Crohn s disease to consider for this girl Treating active luminal disease anti-tnfα antibodies Maintaining remission of luminal disease anti-tnfα antibodies azathioprine/mp corticosteroids methotrexate enteral nutrition sulfasalazine (5-ASA) Level one evidence of efficacy based on multi-item measures of disease activity
5 Outline: Medical management and strategies to enhance mucosal healing The spectrum of Crohn disease What are our current treatment goals pratically? Strategizing to achieve such goals
6 Outline The spectrum of Crohn diseases Current treatment goals Strategizing to achieve such goals






7 Inflammatory bowel disease Ulcerative Colitis Clinical Phenotypes Crohn Diseases A SPECTRUM of related disorders
8 Levine, Griffiths et al, Inflamm Bowel Dis 2011; 17 : Paris Classification of Pediatric IBD Crohn Disease Location Behavior Modifiers L1 - Terminal Ileum B1 Inflammatory L4a, L4b and L4ab L2 Colon B2 Stricturing P - Perianal L3 Ileocolon B3 Penetrating Growth B2B3 G0, G1 Severity? Not classified for CD Age (years) A1a < 10 A1b 10-<17
9 Spectrum of pediatric Crohn s diseases: classification by macroscopic disease location Colon only 35% Terminal ileum +/- cecum 4% Jejunum/ proximal ileum 7% ile c Colon only 22% Terminal ileum +/- cecum 29% Ileocolonic 55% Children aged <10 years at diagnosis Ileocolonic 40% Data from Hospital for Sick Children, Toronto: Sherlock M, DDW 2011 Jejunum/ proximal ileum 12% Children aged >10 years but < 15 years at diagnosis
10 Pariente et al. Inflamm Bowel Dis 2011;17: Crohn s: A progressive disease Progression of digestive damage and inflammatory activity Digestive Damage Stricture Fistula/abscess Surgery Stricture Inflammatory Activity (CDAI, CDEIS, PCR) Disease Diagnosis Early onset Disease Pre-clinical Clinical
11 Crohn s diseases vs ulcerative colitis Chronically active inflammation (variations in activity) More truly a disease of exacerbations and remissions
12 Spectrum of disease Crohn Disease severity (with traditional therapies prior to 2000) Global symptom severity during 5-year follow-up Mild sx only Moderate exacerbations Chronically Severe (Despite immunemodulators and often enteral nutrition) Chronically severe then resection Pre-pubertal Children from the Greater Toronto Area No change comparing (Griffiths, Gut 1993) versus
13 Outline The spectrum of Crohn diseases Current treatment goals Strategizing to achieve such goals
14 Goals of treatment in paediatric Crohn s disease CURRENT TRADITIONAL TREATMENT GOALS TREATMENT GOALS Achieve and maintain mucosal healing Induce and maintain clinical remission (symptom control) Facilitate growth (a marker of success of therapy) Deep remission (minimize pan-intestinal damage)
15 Why have treatment goals have moved beyond symptoms? Recognition of the discrepancy between symptoms and status of intestine in Crohn s disease Greater appreciation of the chronic, continuous inflammation present in Crohn s disease with traditional therapies Greater access to means of re-evaluating healing (MRE; ultrasound; endoscopy; fecal inflammatory biomarkers) Availability of therapies able to achieve mucosal healing






16 Reassessment ileocolonoscopy in an 8 ½ year old with 5 years disease duration: on azathioprine followed clinically Ascending colon Cecum Transverse colon Upper descending colon sigmoid ileum
17 Practical questions in treating to target of mucosal healing Can we predicted progression or non-progression of disease? Can we make use of biomarkers (e.g. fecal calprotectin) or repeated colonoscopic examinations to monitor patients better? If we re-evaluate regularly via ileocolonoscopy and MR enterography..should we step-up treatment (i.e. biologics) in presence of macroscopic disease irrespective of symptoms? Should we use biologics (anti-tnf) more readily and earlier even in very young children?n
18 Outline The spectrum of Crohn diseases Current treatment goals Strategizing to achieve mucosal healing
19 Index patient: Ileocolonic Crohn Disease at first evaluation (Paris: L3 + L4a) Discontinuous disease Deep ulcers in transverse colon and ileum (20 cm) Small round and linear ulcers in stomach (+ve granuloma)
20 Managing Crohn s disease: top-down (early anti-tnf) or step-up? Exclusive enteral nutrition or corticosteroids followed by immunomodulator for maintenance? OR Early use of anti-tnf as induction and maintenance?
21 Pediatric Crohn s disease Guidelines: induction and maintenance ECCO/ESPGHAN Ruemmele F et al, J Crohn Colitis 2014 Exclusive Enteral Nutrition (EEN) is recommended as first line therapy to induce remission in children with active luminal CD [EL1] 96% agreement Oral corticosteroids are recommended for inducing remission in children with moderate to severe active luminal CD if EEN is not an option [EL2 (Pediatrics), EL1 (Adults)] 96% agreement Thiopurines or methotrexate are recommended as options for maintenance of steroid-free remission in children at risk for poor disease outcome [EL2 (pediatrics), EL1 (adults)] 96% agreement
22 Pediatric Crohn s disease Guidelines: induction and maintenance ECCO/ESPGHAN Ruemmele F et al, J Crohn Colitis 2014 Anti-TNF therapy is recommended for inducing and maintaining remission in children with chronically active luminal CD despite prior optimized immunomodulator therapy [EL2] 100% agreement Anti-TNF therapy is recommended for inducing remission in children with active steroid-refractory disease [EL2] 100% agreement Consider as primary therapy for selected children at high risk for poor outcome Anti-TNF therapy is recommended as primary induction and maintenance therapy for children with active perianal fistulizing disease in combination with appropriate surgical intervention [EL2] 84% agreement
23 In light of our treatment goals, what concepts should influence recommendations? Comparative abilities of therapies to heal intestine Whether timing matters, if one class of therapy is more effective Benefit vs risk considerations
24 What concepts should influence recommendations? Comparative abilities of therapies to heal intestine Whether timing matters, if one class of therapy is more effective Benefit vs risk considerations
25 Steroids: Infrequent mucosal healing despite clinical remission % % Patients % Complete healing in 12% Endoscopy worsened in 9% 0 Endoscopic Remission No Endoscopic Remission Clinical remission with steroids is not associated with mucosal healing Endoscopic status in patients with clinical remission after 7 weeks of prednisolone 1 mg/kg daily (n=131; 92% of total population) Modigliani R et al. Gastroenterology. 1990;98:811.

26 Open-label study with EEN: Simplified endoscopic scores before and after Grover et al, J Gastroenterol 2013
27 Mucosal healing with thiopurines and with biologics: prospective data Complete mucosal healing* at week SONIC Proportion of Patients (%) p=0.023 p< p= /109 28/93 47/107 AZA + placebo IFX + placebo IFX+ AZA *No remaining visible lesions at week 26 endoscopy Colombel J, et al. N Engl J Med 2010;362:


28 Azathioprine results in mucosal healing: previous observational data Pre-azathioprine 24 months post-azathioprine D Haens et al, GI Endoscopy 1999
29 What concepts should influence recommendations? Comparative abilities of therapies to heal intestine Whether timing matters, if one class of therapy is more effective Benefit vs risk considerations
30 Response and remission with anti-tnf therapy by duration of Crohn s Disease % in CDAI Response or Remission 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 90% 75% 68% 62% 55% 57% 50% 47% 44% 37% 37% 36% 36% 33% 29% 24% n=19 n=35 n=19 n=35 n=20 n=22 n=20 n=22 n=45 n=55 n=45 n=55 n=131 n=98 n=131 n=98 <1 Year 1-<2 years 2-<5 years >=5 years Response Placebo Response Remission Placebo Remission Colombel et al, NEJM 2007 PRECISE trial (certolizumab)
31 Response to infliximab induction in luminal inflammatory pediatric Crohn s disease 9% 11% Single-centre experience: 195 patients Significant covariates Covariate OR (95% CI) 80% Time from diagnosis to IFX induction (Years) Early IFX (<18mo from diagnosis) 0.79 ( ) 7.01 ( ) Male 2.24 ( ) No Response Partial Response (PGA) Complete Response (PGA, PCDAI 10) Church P, et al: Inflamm Bowel Dis 2014

32 Primary non-response uncommon in inflammatory CD: beware established stenosis ALTERNATE TREATMENT: surgical resection
33 Early Biologic Therapy versus conventional Management Steroids Steroids + AZA MTX Conventional therapy (n=66) Newly diagnosed, antimetabolite, anti-tnf, or steroid-naïve CD patients (n=133) + IFX Early aggressive (n=67) IFX (0,2,6 weeks) + AZA + (episodic) IFX Steroids D Haens et al. Lancet 2008;371:660
34 Proportion of Patients Receiving Infliximab % of Patients Numbers for the top down group indicate patients who required episodic IFX Week Top Down Step Up D Haens G et al. Lancet 2008.
35 Early Biologic Therapy vs Conventional Management of Crohn s Disease Complete endoscopic remission (absence of ulcers) after 2 years of treatment 100 Patients (%) ** **p=0.003 (n=26) Early aggressive (n=23) Conventional therapy D Haens et al. Lancet 2008;371:660
36 CCFA RISK Stratification Study New Onset Pediatric Crohn s Disease Walters TD, Gastroenterology 2014 TREATMENT in first 3 months Crohn s disease: 552 children with complete data and 1 yr f/u Anti-TNFα only n = 68 Early IM only n=248 Propensity Score Matching No early immunotherapy n = 236 Anti-TNFα only IM only n = 68 No early immunotherapy
37 Characteristics at Diagnosis of Propensity Score Matched Sample Feature Median Age (IQR) Anti-TNFα only (N=68) 13.8 yrs ( ) IM only (N=68) 11.3 yrs ( ) No Early immunotherapy (N=68) 11.5 ( ) p-value Paris age <10 years 9 (13%) 8 (12%) 7 (10%) 0.87 Male (n,%) 46 (68%) 34 (50%) 44 (65%) 0.08 Location Therapy in the first 3 months L1 (n, %) 67 (20%) 37 (23%) 30 (18%) L2 (n, %) 85 (26%) 48 (29%) 37 (22%) L3 (n, %) 181 (54%) 79 (48%) 102 (60%) 0.21 PCDAI >30 42 (62%) 42 (62%) 41 (60%) 0.98 Presence perianal 16 (24%) 12 (18%) 12 (18%) 0.61 disease Deep ulceration 41 (60%) 41 (60%) 41 (60%) 1.0 CRP (X ULN) 5.09 ( ) 5.85 ( ) 6.00 ( ) 0.45 ESR, platelet count, albumin, Ht z-score also part of the model, all
38 Walters TD, Gastroenterology 2014 Subsequent therapies Initial Therapy IM but not anti-tnf by 3 months Neither IM nor anti-tnf by 3 months Additional Agents added 3 to 6 months Additional Agents added 6 to 12 months 6 anti-tnf 14 anti-tnf 19 IM 8 anti-tnf 3 IM + anti- TNF 8 IM 5 anti-tnf 4 IM + anti- TNF Total Additional Anti-TNF use 3 to 12 months 20 anti-tnf (29%) (27 IM) 13 anti-tnf 7 IM + anti- TNF (29%)
39 12 Month Outcomes for the three early therapy approaches: PCDAI 10 without resection Therapy Achieved steroid-free, surgery- free remission by 12 months anti-tnf by 3 months 85% IM by 3 months 60% No immune therapy by 3 months 54% ARR NNT Anti-TNF vs IM 25% 4 Chi squ p = Walters TD, Gastroenterology 2014
40 Interpretation In clinically similar populations of children with Crohn s disease, early (<3 mon) therapy with anti-tnfα was superior to early IM or no early immunotherapy despite later addition of those agents: PCDAI remission, CRP, growth It doesn t mean that everyone should get anti-tnfα therapy, rather that we need to better define further characteristics of patients that are at risk of progressive disease without such therapy
41 Concerns about early anti-tnf therapy in children Some patients would be overtreated some have mild/non-progressive disease Limited extent of disease? Safety concerns Secondary loss of response: importance of sustaining response Cost and access Exit strategy?
42 Our practice: timing of anti-tnf therapy in pediatric Crohn s Disease Steroid-refractory (but inflammatory) disease (usually colonic CD) Accelerated fashion i.e. after corticosteroids/enteral nutrition help clinically but as a maintenance alternative to immunemodulators As initial treatment in select patients, considering disease location and extent Severe perianal fistulizing disease Extensive, severe colonic disease concomitantly with steroids Delayed recognition of disease, growth impairment When immunemodulator fails to achieve steroid-free sustained remission
43 Positioning of anti-tnf: exposure to immunomodulators prior to infliximab Number of Patients Azathioprine 16 Methotrexate 14 None Year of IFX Induction Church P, Inflamm Bowel Dis 2014 Single-centre experience: 195 patients


 Church P, et al")
44 Durability of response Secondary Loss of Responsiveness Complete loss of benefit from IFX after significant benefit had been obtained, despite adjustment of dose and/or dosing interval Individualization of regimen (dose escalation or interval shortening) was common especially in first 1-2 years of maintenance therapy (standard of care) Church P, et al Inflamm Bowel Dis 2014
45 Height improves significantly when potential remains at time of anti-tnf induction 0,4 0,2 Mean Height Z-Score 0,0-0,2-0,4-0,6-0,8-1,0 All patients Tanner 1/2 only Tanner 4/5 only -1,2-1,4 Diagnosis Induction 1 year 2 years Church P, et al Accepted, Inflamm Bowel Dis


46 Anti-TNF-α Antagonists Chimeric monoclonal antibody Humanized monoclonal antibody Infliximab IV infusion Adalimumab Subcutaneous injection
47 ANTI-TNF induction and maintenance therapy of pediatric Crohn disease: infliximab and adalimumab trials Infliximab (REACH) N=112 (mean age 13.3 years) (Hyams et al, Gastroenterology 2007) Adalimumab N=188 (mean age 13.5 years) (Hyams et al, Gastroenterology 2012) Prior anti-tnf treatment None (all anti-tnf naïve) Included 83 pts with secondary Loss of response /intolerance to infliximab Concomitant IM during study Response rate (drop in PCDAI >/= 15) after induction 99% throughout (thiopurines usually) 62% from start to week 26; 46% after week 26 88% at week 10 87% of anti-tnf naïve patients Remission rate at week 26 60% of week 10 responders randomized to 5 mg/kg q 8 weekly maintenance Remission rate at week 52 56% of week 10 responders randomized to 5 mg/kg q 8 weekly maintenance 63% of anti-tnf naïve week 4 responders randomized to high dose for body weight q 2 weeks 46% of anti-tnf naïve week 4 responders randomized to high dose for body weight q 2 weeks
48 Safety concerns : neoplasia risk Thiopurines alone Anti-TNF alone Anti-TNF in combination with thiopurines

49 Hepatosplenic T- cell lymphoma occurrences Estimated Risks: Males <35 yrs on Thiopurines: 1/7404 Males <35 yrs on Thiopurines + Anti-TNF: 1/3534 Kotlyar et al, Clin Gastroenterol Hepatol. 2011; 1: cases in IBD (35 male) 18 on anti TNF therapy + thiopurine (17 male) 19 on thiopurine therapy alone Age (mean 26) 1-24 infusions (8 had <3 infusions) 10 8 # Cases Anti-TNF + 6MP/AZA Dec 2006 Mar 2007 Sept 2007 April 2008 Dec 2008

50 Efficacy... and.safety
51 Important with either top-down or step-up More attention to biomarkers (serologic and fecal) and re-evaluation of intestine (MRE/colonoscopy) Need for predictors of such aggressive progression and of mild disease
52 STORI trial: Time to confirmed relapse 52 patients with confirmed relapse 44 relapses during first year Louis E, et al. Gastroenterology 2012; 42: 63-70




53 Canadian Children s IBD Network 10 academic centres, where children at first assessed for suspected IBD The Canadian Children Inflammatory Bowel Disease Network: A Joint Partnership of CIHR and the CH.I.L.D Foundation
54
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD
 Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Mono or Combination Therapy with. Individualized Approach
 Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL
 INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
How to use infliximab?
 How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
The Best of IBD at UEGW (Crohn s)
") The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Withdrawal of drug therapy in patients with quiescent Crohn s disease
 Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Endpoints for Stopping Treatment in UC
 Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
IBD Understanding Your Medications. Thomas V. Aguirre, MD Santa Barbara GI Consultants
 IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Medical Management of Inflammatory Bowel Disease
 Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Treatment of Pediatric IBD: What is Different?
 Treatment of Pediatric IBD: What is Different? January 13, 2017 Michael Kappelman MD, MPH University of North Carolina at Chapel Hill Overview Is Pediatric IBD the same disease? Treatment considerations
Treatment of Pediatric IBD: What is Different? January 13, 2017 Michael Kappelman MD, MPH University of North Carolina at Chapel Hill Overview Is Pediatric IBD the same disease? Treatment considerations
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease
 Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah
 John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Biologic Therapy for Inflammatory. Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida
 Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών. Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων
 Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
5/2/2018 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD
 5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
Implementation of disease and safety predictors during disease management in UC
 Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Immunogenicity of Biologic Agents and How to Prevent Sensitization
 Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Personalized Medicine in IBD
 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
New Perspectives on the Diagnosis and Management of IBD. Disclosures
 New Perspectives on the Diagnosis and Management of IBD Joel R. Rosh, MD Director, Pediatric Gastroenterology Goryeb Children's Hospital/Atlantic Health Professor of Pediatrics Icahn School of Medicine
New Perspectives on the Diagnosis and Management of IBD Joel R. Rosh, MD Director, Pediatric Gastroenterology Goryeb Children's Hospital/Atlantic Health Professor of Pediatrics Icahn School of Medicine
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Therapy for Inflammatory Bowel Disease
 Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
IBD in teenagers Biological and Transition
 IBD in teenagers Biological and Transition Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital Chelsea and Westminster Hospital Conflict of Interest None to declare Fee for presentation
IBD in teenagers Biological and Transition Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital Chelsea and Westminster Hospital Conflict of Interest None to declare Fee for presentation
How Safe and Effective is Infliximab in the Treatment of Children with Moderate to Severe Crohn s disease?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2011 How Safe and Effective is Infliximab
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2011 How Safe and Effective is Infliximab
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
How to Optimize Induction and Maintenance Responses: Definitions and Dosing Advances in Inflammatory Bowel Disease December 6, 2009
 How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R.
 UvA-DARE (Digital Academic Repository) Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R. Link to publication Citation for published version
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Highlights of DDW 2015: Crohn s disease
 Highlights of DDW 2015: Crohn s disease Mark S. Silverberg, MD, PhD, FRCPC Associate Professor of Medicine, University of Toronto Staff Gastroenterologist, Mount Sinai Hospital Senior Investigator, Lunenfeld-Tanenbaum
Highlights of DDW 2015: Crohn s disease Mark S. Silverberg, MD, PhD, FRCPC Associate Professor of Medicine, University of Toronto Staff Gastroenterologist, Mount Sinai Hospital Senior Investigator, Lunenfeld-Tanenbaum
Personalized Medicine in IBD: Where Are We in 2013
 Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Ulcerative Colitis Therapy. Faculty Disclosure. Acknowledgements 28/11/2013. Amy Morse November 30/13
 Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball
 Looking for the Crystal Ball") Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Agenda. Predictive markers in IBD. Management of ulcerative colitis. Management of Crohn s disease
 Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
Severe IBD: What to Do When Anti- TNFs Don t Work?
 Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review)
") Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Risk = probability x consequence
 Explaining Risks of IBD Therapy to Parents and Patients December 4, 2009 CCFA Advances in IBD Hollywood, FL Corey A. Siegel Assistant Professor of Medicine, Dartmouth Medical School Director, Dartmouth-Hitchcock
Explaining Risks of IBD Therapy to Parents and Patients December 4, 2009 CCFA Advances in IBD Hollywood, FL Corey A. Siegel Assistant Professor of Medicine, Dartmouth Medical School Director, Dartmouth-Hitchcock
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Slide 1 Medications in inflammatory bowel disease a primer for health care providers. Slide 2. Slide 3 Theory of pathogenesis. IBD - epidemiology
 Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM
 CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
Medical Management of Intestinal Strictures
 Medical Management of Intestinal Strictures Subrata Ghosh, FRCP, FRCPE, FRCPC, AGAF, FCAHS Professor of Translational Medicine Director of the Institute of Translational Medicine University of Birmingham,
Medical Management of Intestinal Strictures Subrata Ghosh, FRCP, FRCPE, FRCPC, AGAF, FCAHS Professor of Translational Medicine Director of the Institute of Translational Medicine University of Birmingham,
Selby Inflamm Bowel Dis. 2008:14:
 Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
The future of IBD therapeutic research
 The future of IBD therapeutic research Jean-Frederic Colombel, MD Director Susan and Leonard Feinstein IBD Clinical Center Icahn School of Medicine, Mount Sinai Hospital New York J-F Colombel has served
The future of IBD therapeutic research Jean-Frederic Colombel, MD Director Susan and Leonard Feinstein IBD Clinical Center Icahn School of Medicine, Mount Sinai Hospital New York J-F Colombel has served
Preventing post-operative recurrence
 Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Dr David Epstein Vincent Pallotti Hospital and University of Cape Town
 Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D.
 Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Scottish Medicines Consortium
 Scottish Medicines Consortium infliximab 100mg powder for intravenous infusion (Remicade ) No. (364/07) Schering-Plough UK Ltd 6 April 2007 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium infliximab 100mg powder for intravenous infusion (Remicade ) No. (364/07) Schering-Plough UK Ltd 6 April 2007 The Scottish Medicines Consortium (SMC) has completed its assessment
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY?
 WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
SYNOPSIS. Issue Date: 25 Oct 2011
 SYNOPSIS Issue Date: 25 Oct 2011 Name of Sponsor/Company Name of Finished Product Name of Active Ingredient(s) Janssen Research & Development STELARA Ustekinumab Protocol No.: Title of Study: Study Name:
SYNOPSIS Issue Date: 25 Oct 2011 Name of Sponsor/Company Name of Finished Product Name of Active Ingredient(s) Janssen Research & Development STELARA Ustekinumab Protocol No.: Title of Study: Study Name:
Lessons to learn from Crohn's disease clinical trials: implications for ulcerative colitis
 Lessons to learn from Crohn's disease clinical trials: implications for ulcerative colitis Aránzazu Jáuregui Amézaga, Elena Ricart, Julián Panés Department of Gastroenterology, Hospital Clínic de Barcelona,
Lessons to learn from Crohn's disease clinical trials: implications for ulcerative colitis Aránzazu Jáuregui Amézaga, Elena Ricart, Julián Panés Department of Gastroenterology, Hospital Clínic de Barcelona,
IBD Case Studies. David Rowbotham. Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital
 IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
Anti-TNF and cyclosporine are identical choices for severe ulcerative colitis refractory to steroid therapy CON Peter Laszlo LAKATOS Semmelweis
 Anti-TNF and cyclosporine are identical choices for severe ulcerative colitis refractory to steroid therapy CON Peter Laszlo LAKATOS Semmelweis University, 1st Department of Medicine Budapest June 13-15,
Anti-TNF and cyclosporine are identical choices for severe ulcerative colitis refractory to steroid therapy CON Peter Laszlo LAKATOS Semmelweis University, 1st Department of Medicine Budapest June 13-15,
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL
 NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
Il ruolo degli anticorpi anti farmaco nella pratica clinica
 Il ruolo degli anticorpi anti farmaco nella pratica clinica Daniela Pugliese, MD IBD Unit Complesso Integrato Columbus Gemelli Hospital Catholic University Foundation, Rome - Italy Therapeutic Drug monitoring
Il ruolo degli anticorpi anti farmaco nella pratica clinica Daniela Pugliese, MD IBD Unit Complesso Integrato Columbus Gemelli Hospital Catholic University Foundation, Rome - Italy Therapeutic Drug monitoring
Gionata Fiorino VEDOLIZUMAB E IBD. Un nuovo target terapeutico
 Gionata Fiorino VEDOLIZUMAB E IBD Un nuovo target terapeutico Anti cell adhesion molecules Danese S, NEJM 2011 6 Steps leukocyte recruitment Fiorino G. et al. 2010 Vedolizumab Blocks Fewer Biological Pathways
Gionata Fiorino VEDOLIZUMAB E IBD Un nuovo target terapeutico Anti cell adhesion molecules Danese S, NEJM 2011 6 Steps leukocyte recruitment Fiorino G. et al. 2010 Vedolizumab Blocks Fewer Biological Pathways
Crohn s
 Crohn s Disease David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology, and Nutrition Co-Director, Digestive Diseases Center @IBDMD Disclosures
Crohn s Disease David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology, and Nutrition Co-Director, Digestive Diseases Center @IBDMD Disclosures
Biologics, Novel Therapeutic Approaches in Inflammatory Bowel Diseases
 Biologics, Novel Therapeutic Approaches in Inflammatory Bowel Diseases Walter Reinisch Univ-Klinik für Innere Medizin III Abt. Gastroenterologie & Hepatologie AKH Wien The Biologic s evolution From availabilitydriven
Biologics, Novel Therapeutic Approaches in Inflammatory Bowel Diseases Walter Reinisch Univ-Klinik für Innere Medizin III Abt. Gastroenterologie & Hepatologie AKH Wien The Biologic s evolution From availabilitydriven
The Refractory Crohn s Disease
 The Refractory Crohn s Disease Patient David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and Nutrition
The Refractory Crohn s Disease Patient David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and Nutrition
Infliximab Therapy in Pediatric Patients 7 Years of Age and Younger
 ORIGINAL ARTICLE: GASTROENTEROLOGY Infliximab Therapy in Pediatric Patients 7 Years of Age and Younger Judith R. Kelsen, Andrew B. Grossman, Helen Pauly-Hubbard, Kernika Gupta, Robert N. Baldassano, and
ORIGINAL ARTICLE: GASTROENTEROLOGY Infliximab Therapy in Pediatric Patients 7 Years of Age and Younger Judith R. Kelsen, Andrew B. Grossman, Helen Pauly-Hubbard, Kernika Gupta, Robert N. Baldassano, and
OPTIMAL USE OF IMMUNOMODULATORS AND BIOLOGICS Edward V. Loftus, Jr., MD, FACG
 1C: Advances in Inflammatory Bowel Disease OPTIMAL USE OF IMMUNOMODULATORS AND BIOLOGICS Edward V. Loftus, Jr., MD, FACG narrow interpretation of this presentation topic would A be a discussion of dosing
1C: Advances in Inflammatory Bowel Disease OPTIMAL USE OF IMMUNOMODULATORS AND BIOLOGICS Edward V. Loftus, Jr., MD, FACG narrow interpretation of this presentation topic would A be a discussion of dosing
Assessing Response and Loss of Response to Biological Therapies in IBD
 CLINICAL AND SYSTEMATIC S nature publishing group 685 Assessing Response and Loss of Response to Biological Therapies in IBD Henit Yanai, MD 1 and Ste phe n B. Hanau e r, M D 2 OBJECTIVES: METHODS: RESULTS:
CLINICAL AND SYSTEMATIC S nature publishing group 685 Assessing Response and Loss of Response to Biological Therapies in IBD Henit Yanai, MD 1 and Ste phe n B. Hanau e r, M D 2 OBJECTIVES: METHODS: RESULTS:
Inflammatory bowel disease (IBD) Overview of the Paediatric investigation plans. Presented by: Richard Veselý. An agency of the European Union
 Overview of the Paediatric investigation plans. Presented by: Richard Veselý. An agency of the European Union") Inflammatory bowel disease (IBD) Overview of the Paediatric investigation plans Presented by: Richard Veselý An agency of the European Union Adalimumab - Crohn s disease Indication: Treatment of severe,
Inflammatory bowel disease (IBD) Overview of the Paediatric investigation plans Presented by: Richard Veselý An agency of the European Union Adalimumab - Crohn s disease Indication: Treatment of severe,
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art
 Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
Optimizing Immunomodulators and
 Optimizing Immunomodulators and Biologics i in Inflammatory Bowel Disease Sunanda Kane, MD, MSPH, FACG Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota,
Optimizing Immunomodulators and Biologics i in Inflammatory Bowel Disease Sunanda Kane, MD, MSPH, FACG Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota,
STELARA (ustekinumab) Clinical Study Report CNTO1275CRD3001
 Clinical Study Report CNTO1275CRD3001") SYNOPSIS Name of Sponsor/Company Janssen Research & Development* Name of Investigational Product STELARA (ustekinumab) * Janssen Research & Development is a global organization that operates through different
SYNOPSIS Name of Sponsor/Company Janssen Research & Development* Name of Investigational Product STELARA (ustekinumab) * Janssen Research & Development is a global organization that operates through different
Positioning New Therapies
 Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Pharmacotherapy of Inflammatory Bowel Disorder
 PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: Feb. 14, 2018 Last Revised: April 1, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: Feb. 14, 2018 Last Revised: April 1, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
Clinical Use of Measuring Trough Levels and Antibodies against Infliximab in Patients with Pediatric Inflammatory Bowel Disease
 Gut and Liver, Published online September 9, 2016 ORiginal Article Clinical Use of Measuring Trough Levels and Antibodies against Infliximab in Patients with Pediatric Inflammatory Bowel Disease So Yoon
Gut and Liver, Published online September 9, 2016 ORiginal Article Clinical Use of Measuring Trough Levels and Antibodies against Infliximab in Patients with Pediatric Inflammatory Bowel Disease So Yoon
Practical Risk Management Tools for Patients with IBD. Garth Swanson MD Rush University Medical Center
 Practical Risk Management Tools for Patients with IBD Garth Swanson MD Rush University Medical Center IBD Therapy Severity Tysabri Surgery Infliximab, i Adalimumab, Certilizumab Corticosteroids, Immunomodulators
Practical Risk Management Tools for Patients with IBD Garth Swanson MD Rush University Medical Center IBD Therapy Severity Tysabri Surgery Infliximab, i Adalimumab, Certilizumab Corticosteroids, Immunomodulators
Achieving Success in Ulcerative Colitis: the Role of Infliximab
 Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis